
State of knowledge Sexual assault and domestic violence in the context of co-occurrence and re-victimisation
State of knowledge
State of knowledge | October 2015
Issue 13 | 2015
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
Acknowledgement of Country
ANROWS acknowledges the traditional owners of the land across Australia on which we work and live. We pay our respects to Aboriginal and Torres Strait Islander elders past, present and future; and we value Aboriginal and Torres Strait Islander history, culture and knowledge.
© ANROWS 2015
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box 6322, Alexandria NSW 2015 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
Sexual assault and domestic violence in the context of co-occurrence and re-victimisation:
State of knowledge paper / Peta, Cox.
Sydney: ANROWS, c2015.
Pages; 30 cm. (Landscapes: State of Knowledge: 13/2015)
I. Violence against women. II. Family violence. III. Victims of family violence – Services for. IV. Sexual abuse victims. V. Sex crimes.
I. Cox, Peta.
ISSN: 2204-9657 (print) 2204-9665 (online)
ISBN: 978-1-925372-26-7 (print) 978-1-925372-25-0 (online)
Creative Commons Licence
Attribution-Non Commercial

CC BY-NC
This licence lets others distribute, remix and build upon the work, but only if it is for non-commercial purposes and they credit the original creator/s (and any other nominated parties). They do not have to license their Derivative Works on the same terms.
Version 3.0 (CC Australia ported licence): View CC BY-NC Australia Licence Deed | View CC BY-NC 3.0 Australia Legal Code
Version 4.0 (international licence): View CC BY-NC 4.0 Licence Deed | View CC BY-NC 4.0 Legal Code
Prepared by
Dr Peta Cox, Senior Research Officer (Research Program), ANROWS
Author acknowledgement
My thanks to Jen Novak, Tony Fletcher, Erin Mackay and Ange Williams for their initial input and support with this project.
I also greatly appreciate valuable feedback from the two anonymous peer reviewers.
This work is part of the ANROWS Landscapes series. ANROWS Landscapes (State of knowledge papers) are medium length papers that scope current knowledge on an issue related to violence against women and their children. Papers will draw on empirical research, including research produced under ANROWS’s research program, and/or practice knowledge.
This paper addresses work covered in the ANROWS research project 1.6 “Sexual assault and domestic violence in the context of co-occurrence and re-victimisation”. Please consult the ANROWS website for more information on this project.
Contents
Overall characteristics of the corpus
Theories of re-victimisation and co-occurrence
Common disciplinary approaches
Theories, concepts and typologies
Methods used by researchers examining re-victimisation and co-occurrence
Life-course research: Key limitations
Cross-sectional research: Key limitations
Bias caused by population selection
Bias caused by incomplete reporting
Comparability: Inconsistent phenomena definitions
Undifferentiated categories of violence
Commonly used survey instruments
Comparability of study findings
Rates of re-victimisation and co-occurrence
Characteristics of incidents of intimate partner sexual violence
Risk factors for re-victimisation and co-occurrence
Relational and behavioural risk factors
Sub-populations with differential patterns of victimisation
Aboriginal and Torres Strait Islander women
Women from cultural and linguistically diverse (CALD) backgrounds
Women with low socio-economic status
Women who are, or who have been, incarcerated
Women who experience severe mental illness
Women who identify as lesbian, bisexual and/or queer
Women who work in the sex industry
Sub-populations of interest with limited existing research
Male repeat perpetrators of sexual assault and domestic violence: Repeat offenders
Community and professional attitudes towards re-victimisation and co-occurrence
Health impacts of re-victimisation and co-occurrence
Women’s engagement with legal and support services
Help-seeking: Non-legal services
Responses to women affected by re-victimisation and co-occurrence
Coordinated, multi-agency and integrated services responses
Recommendations and conclusion
Appendix A: Searched databases
Appendix B: Additional available literature
Intimate partner sexual violence rates
Executive summary
Scope of project
This state of knowledge paper aims to examine the intersection between sexual assault and domestic violence. In order to do this, it highlights similarities and differences in the causes, consequences and lived experience of two forms of concurrent victimisation. Within this paper, concurrent victimisation is understood to include re-victimisation (when a woman, over her lifetime, experiences both sexual assault and domestic violence) and intimate partner sexual violence (IPSV). This paper examines the complexity of these experiences in order to articulate the common impacts of domestic violence and sexual assault and to critically examine how the phenomenon of re-victimisation and IPSV can shift the ways in which we think about, and provide services for, women affected by domestic violence and sexual assault.
Method
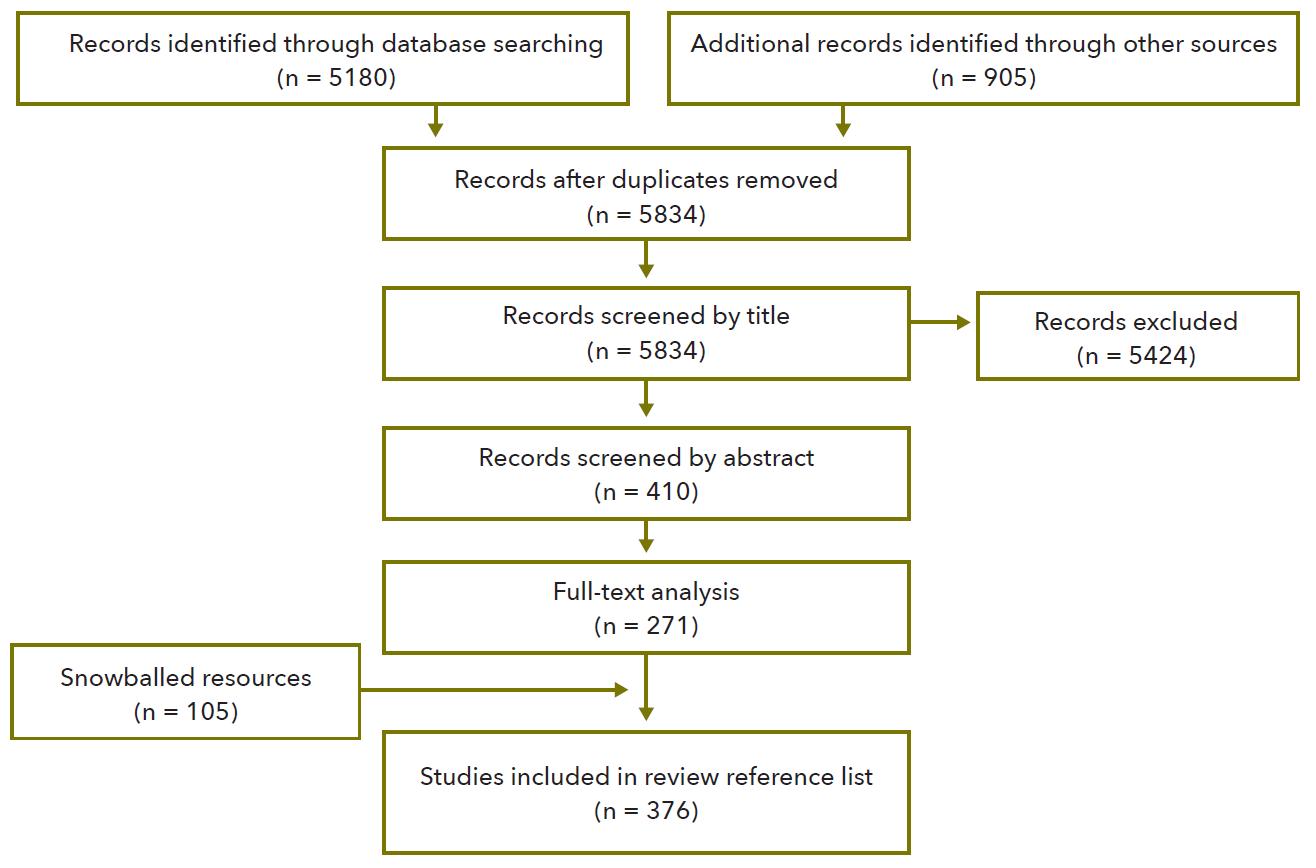
The review used a multi-staged, repeatable, search methodology. Academic and grey literature on (a) domestic violence (DV) and sexual assault (SXA) victimisations across the life course, and (b) intimate partner sexual violence was assessed. An initial corpus of 6715 sources were assessed, with 271 of these deemed within scope. After snowballing from relevant papers, a total of 333 papers were used in the review.
Key findings
The lack of longitudinal studies of re-victimisation reduces our ability to make conclusions about causal factors or the nature of victimisation over time.
Much of the available research on IPSV and re-victimisation is unable to be extrapolated to findings about the general population, as it focuses on non-representative groups such as women who were attending psychology clinics.
Regarding re-victimisation:
- Research indicates that women who experience child sexual abuse (CSA) are more likely to experience IPSV than women who have not experienced CSA.
- Similarly, women who have experienced CSA are more likely to experience DV (not limited to sexual violence) in their adult relationships.
- The relationship between CSA and adult victimisation is mediated to some extent by the severity of the abuse during childhood.
- Research on the frequency and impacts of re- victimisation in adulthood is more mixed.
Regarding IPSV:
- Across the reviewed studies, intimate partner sexual coercion was reported by between 24 percent and 62 percent of women, while intimate partner sexual assault was reported by between 1.7 percent and 46 percent of women.
- IPSV generally occurs in the context of other forms of violence and was often part of a larger pattern of coercive control in a relationship. IPSV should be considered a tactic of DV, and not a separate phenomenon.
- Alcohol abuse problems, frequent and normalised engagement with pornography and a history of sexual coercion were associated with IPSV perpetration in a current relationship.
- IPSV was often limited to emotional coercion, however when it was physically violent, it frequently resulted in injury.
- Heteronormative beliefs and conservative gender norms were associated with acceptance and experience of sexual coercion for both men and women.
- IPSV victims are less likely to seek help than victims of other forms of DV.
Regarding both re-victimisation and IPSV:
- Drug and alcohol use may be a precursor, consequence or risk factor associated with IPSV and re-victimisation. Similarly, emotional distress and psychiatric conditions may increase a person’s vulnerability to violence, place them in high risk contexts and/or may be a consequence of violence.
- A wide range of communities, including Aboriginal and Torres Strait Islander women, women from culturally and linguistically diverse backgrounds and women with a disability, have discrete patterns of victimisation, including distinct behaviours and norms that may increase the risk of victimisation.
- Normative understandings of what constitutes “real rape” affect how victims, perpetrators and bystanders interpret experiences of sexual assault. These norms particularly affect interpretations of IPSV incidents.
- Both IPSV and re-victimisation had significant physical and mental health consequences.
- DV and SXA services were often separated, with both service types finding victims of IPSV and women who had complex trauma histories to be particularly challenging client groups.
Key recommendations
The following recommendations are based on the research examined for this state of knowledge paper and can be made regarding the method and focus of future research.
ANROWS recommends that:
- As re-victimisation often occurs across violence types, researchers should, wherever possible, expand their examination of life course re-victimisation to multiple violence types.
- Longitudinal research is critical to understanding the complex pathways that result in repeated victimisation and IPSV. Such research is particularly important for understanding the lived experience of marginalised women (e.g. incarcerated women), as the intersections of disadvantage are even more complex for these populations(Poister, Tusher, & Cook, 2010). Put differently, “longitudinal research is needed to sort out risk factors, from consequences, from simple correlates” (Classen et al., 2005, p. 114).
- As has been noted for several decades now, one way of increasing the quality and comparability of research findings is for there to be consistent definitions of abusive behaviours used in IPSV and re-victimisation research. Such definitions would need to provide clarity to research participants about what was meant by “force” in relation to sexual activity, with distinctions made between physical threat and emotional/psychological coercion tactics.
- Future research should concentrate on relevant target groups. Many target groups have relatively small populations, making collecting data with population level surveys difficult. One exception to this is disability, which has a high prevalence and thus analysable data is likely to be able to be collected in all violence research. Most other sub-populations are likely to require dedicated surveys to get a sufficient sample to be statistically reliable.
- Although both qualitative and quantitative research is needed to inform Aboriginal and Torres Strait Islander family violence policy, priority should be given to quantitative research as current quantitative surveys like the Personal Safety Survey (PSS) are unable to provide prevalence estimates for this population.
The following recommendations are made regarding the service delivery environment and are based on the research findings reviewed in this paper.
ANROWS recommends that:
- Acknowledgement is made in policy and practice of weaknesses in our current research base, which means that we are heavily reliant on practice knowledge.
- Accurate and appropriate use of data and acknowledgement of data’s limitations is encouraged in policy, planning and service advocacy, so that when further evidence-based knowledge is available, it is welcomed and adopted.
- To address the stigma of IPSV, DV and SXA services continue to work to raise awareness of the impact of stigma on clients and staff.
- Judicial education and professional development work continues to be supported to ensure court and police sensitivity in IPSV cases, and to minimise the distress of the legal process to women who have experienced re- victimisation and/or IPSV.
- Where not already part of normal clinical practice, STI clinics be provided with training and materials to enable streamlined referrals to SXA and DV services.
- Trauma informed care (a model of care which puts at the centre of clinical practice the long term effects of victimisation) be supported through mainstream service provision and research investment.
- Large scale mental health campaigns promote gendered violence as a risk factor for poor mental health outcomes.
- All DV and SXA services be sufficiently resourced to further enrich cross-sector co-ordination (a full range of co- ordination strategies are possible, from referral pathways to fully integrated care).
- All DV and SXA services, as well as related services such as mental health and drug and alcohol programs, continue to work towards an integrated understanding of the impacts of the escalation or severity of CSA on adulthood in their engagements with both children and adults.
- Public education on violence against women acknowledges the distinct but intersectional dimensions of different forms of violence and its gendered impacts and characteristics.
- Providers of mainstream health and social services be sensitised to the possibility of IPSV and re-victimisation cases in their day to day work. An initial step towards this would be the promotion of existing IPSV screening tools to a wide range of mainstream frontline providers.
- Prevention programs not be funded by government if they implicitly or explicitly support victim blaming. Explanation of these actions should be given to campus unions to promote a similar stance in university campus programs.
- Professional development for workers in the violence against women field acknowledge the multi-faceted nature of abuse and emphasise the links between DV and SXA.
Introduction
State of play
Domestic violence and sexual assault are experienced by a large number of Australian women[1] and have significant and well-established health and welfare impacts. ANROWS has recently completed a research project examining the Australian Bureau of Statistics’ 2012 Personal Safety Survey (PSS) data, which showed that, since the age of 15, one in eight (13%) women in Australia have experienced at least one separate incident of both sexual violence and physical violence (Cox, 2015). As this paper demonstrates, many women have experienced both sexual assault (SXA) and domestic violence (DV) victimisation, either in the form of intimate partner sexual violence (IPSV) or re- victimisation across their life course.
Experiences of SXA and DV are complicated by the contexts in which such victimisation occurs, including the cultural meanings given to violence, and the curtailing action of some women due to the criminalisation of certain aspects of their lives. While such contextual aspects are critical in understanding the full impact of IPSV and re-victimisation, the variation and complexity of these intersections is only able to be briefly examined in this state of knowledge paper.
Despite significant co-occurrence, both researchers and practitioners have noted a continuing tendency to dichotomise SXA and DV into distinct concepts and responses, and to artificially separate women’s lived experience into the responsibility of one or other sector (Tellis, 2010). This theoretical and practical separation is particularly apparent in Australia, where the history of DV and SXA services are distinct.
In order to more fully understand DV and SXA, it is important to conceptualise them as interrelated experiences (Sabina & Ho, 2014). This paper adds to current understandings of this interrelatedness by examining the available research on patterns of violence against women that include both DV and SXA.[2] “Cross-type” re-victimisation and IPSV are both topics that have received limited research attention (Ferro, Carmeele & Saltzman, 2008). In the context of this state of knowledge paper it is important to note that such research may not fully reflect current Australian practice, especially in relation to engagements with priority populations or efforts to enhance the embedding of intersectional analysis in the work and philosophy of practitioners.
This paper notes that there is limited research on the characteristics of any types of violence in most sub-populations, with research on IPSV and re-victimisation particularly incomplete. Relatedly, a key weakness identified in the current research was the tendency to silo lived experience, so that the intersection of multiple sites of disadvantage and stigmatisation was not readily apparent within the literature. This limitation of the literature was, by nature of the building blocks available, mirrored in the state of knowledge paper.
Purpose of the paper
This paper aims to identify similarities and differences in the causes, consequences and lived experience of two forms of concurrent victimisation: namely, certain forms of repeat victimisation across the life course and sexual violence in an intimate relationship.
These two very specific types of violence are examined in this review. By doing this, we are able to examine the cross-over between experiences of domestic violence and sexual assault and thus appreciate its complexity.
Nature of the paper
This paper is an examination of the intersections between domestic violence and sexual assault. This intersection can occur in two ways:
- Re-victimisation – when a woman, over her lifetime, experiences both sexual assault and domestic violence.
- Co-occurring victimisation – when a woman experiences sexual assault by an intimate partner. This is also known as intimate partner sexual violence (IPSV).
Consistent with the focus of ANROWS, this paper is limited to examinations of instances and trajectories of violence that are experienced by adult women victims.
This state of knowledge paper is an examination of empirical literature. The inclusion of studies in the paper is not an endorsement of their methodology or approach, but is rather an acknowledgement that they are part of the currently available research.
State of knowledge method
Research questions
This literature review aims to answer the following questions:
- What do we know about when SXA and DV happen at the same time or when they happen at different times but to the same person, including lived experience and impacts?
- What do we know about the epidemiological and conceptual similarities and differences in the nature of sexual assault and domestic violence when they are experienced in the context of co-occurrence and re-victimisation?
- What do we know about what works in supporting survivors of both sexual assault and domestic violence?
Review method
The review used a multi-staged, repeatable, search methodology (see Table 1 on page 11).
The review began with a systematic search of a wide range of academic and grey literature databases (see Appendix A). Quantitative data was heavily represented in the available databases.
The metadata for all papers identified in the search were uploaded into bibliographic software. By examining the title and abstract of each paper, irrelevant articles were removed from the cohort (see Table 2 on page 12).
The search of the academic literature was supported by snowball searching on Google Scholar.
The review was limited to publications that were:
- published in the last ten years;
- empirical research, commentary and theoretical accounts;
- concerned with instances of co-occurring DV and SXA in the life of an adult female victim (including adolescent women in “dating” relationships);
- concerned with re-victimisation that began in childhood;
- accompanied by available abstracts;
- written in English; and
- studies of human subjects.
The review excluded publications that were more than 10 years old or focused on:
- low income countries;
- violence against men;
- child abuse, including paedophilia, not in the context of expressions of violence between adults or as part of a life course of violence that included abuse of an adult woman;
- violence in the context of war or conflict;
- sex trafficking;
- harmful cultural practices (e.g. forced marriage, female genital mutilation/cutting and wife inheritance);
- violence perpetrated by women; or
- the effect of DV on child welfare (where there is no consideration of an adult female victim).
Superseded publications were also excluded. Some papers published before 2005 have been included as part of the snowball searches – this has only occurred when more recent papers have indicated that the most up to date primary research is outside the time limit. In addition, a small number of older papers have been referenced when they are canonical studies or original theoretical pieces.
Table 1 Electronic search strategy
Topic
Key word (phrase searching)
Set 1: Sexual assault
Sexual assault OR Sexual violence OR Rape OR Indecent assault OR Unlawful sexual conduct OR Sex crime OR Date rape OR Acquaintance rape OR Sexual abuse OR Sexual attack OR Sexual force OR Sexual injury OR Attempted rape OR Sexual coercion OR Non-consensual sex OR Indecent exposure OR Sexual harassment OR Stalking
Set 2: Domestic violence
Intimate partner violence OR Domestic violence OR Domestic abuse OR Family violence OR Family abuse OR Dating abuse OR Battering OR Wife beating OR Wife battering OR Physical abuse OR Emotional abuse OR Psychological abuse OR Financial abuse OR Intimate terrorism OR Spouse abuse OR Spousal abuse
Set 3: Relationship between
Co-occur* OR Intersect* OR Poly-victimi$ation OR Concur* OR Simultaneous* OR Concomitance OR Overlap* OR Contemporaen* OR Compare OR Comparison OR Differences OR Similarities OR Correlations OR Risk factors OR Epistemology OR Cause OR Causation OR Epidemiology OR Typology OR Characteristics OR Responses OR Interventions OR Programs OR Instrument
Set 4: Final
Set 1 AND Set 2 AND Set 3
Limited to availability of abstracts, published 2005 to current, English language and humans.
Table 2 PRISMA Flow diagram
Overall characteristics of the corpus
A total of 271 articles were assessed in full text.
The methodological design of the studies in this paper was consistent with that found in other reviews of IPSV or re- victimisation literature, with the vast majority of studies being quantitative (see, for example, Classen, Palesh & Aggarwal, 2005; Martin, Taft & Resick, 2007; Messman-Moore & Long, 2003; Stockman, Lucea, & Campbell, 2013). Almost all studies included in this state of knowledge paper were retrospective, meaning that they asked people to report on things that had already happened. The majority of the papers were examinations of the prevalence of various types of assault and/or lifetime patterns of assault. Even when looking at the life course of victimisation, most research was cross-sectional (asking questions at one point in time only), with very little longitudinal research (Ludermir, Schraiber, D’Oliveira, França-Junior, & Jansen, 2008; Reyes & Foshee, 2013). Cross-sectional and retrospective survey designs are acknowledged as providing less reliable epidemiological findings than cohort studies that follow people over time. Research using cross-sectional methods cannot provide reliable evidence about whether variables are causally linked. Given this limitation, it is perhaps surprising that predictive modelling in the form of regression or path analysis was a common method of analysing the relationships between risk factors, albeit often with limited predictive utility. Behavioural self-report surveys, such as the Revised Conflict Tactics Scale or the Sexual Experiences Survey were the most common survey instruments (Koss et al., 2007).
Consistent with the nature of available research on DV and SXA more generally, the studies in this paper were primarily from the US (Martin, Taft, & Resick, 2007). Sample size varied from mid-twenties to tens of thousands. Consistent with study methodology, qualitative studies tended to have samples of less than 100, while national, representative studies generally had more than 1000 respondents. As with much behavioural science research, the researchers oversampled college students and under-sampled socially and/or economically disadvantaged communities and/or populations of interest (Christopher & Pflieger, 2007; Moreau, Boucher, Hébert, & Lemelin, 2015).
The corpus consisted primarily of research on IPSV. This seems a likely consequence of the narrow “cross-type” victimisation focus in the scope of the review. However, due to the proportionally small amount of research on “cross-type” re-victimisation; where content relates to this expression of violence and it isn’t under an identifying section heading, relevant words are highlighted to bring this content to the reader’s attention throughout this paper.
Definitions
Re-victimisation
Re-victimisation occurs when a person experiences multiple distinct instances of violence over their life course. In the context of this paper, re-victimisation is limited to instances where a woman experiences both DV and SXA across their lifetime. There are several scenarios that are examined:
- Women who had experienced both child sexual abuse (CSA) and DV, including DV in the context of cohabitating and dating relationships.
- Women who had experienced DV and adult SXA, not perpetrated in the same context (i.e. excluding IPSV).
- Women who had experienced IPSV and either:
- childhood sexual assault; or
- adult sexual assault perpetrated by a person other than the partner perpetrating IPSV.
The use of this “cross-type” definition of re-victimisation significantly reduces the range of re-victimisation types that are examined in this report. In doing so, we are able to focus on the intersection of DV and SXA which is a key aim of this project. However, it is noteworthy that much of the research on re-victimisation is limited to “single-type” repeated victimisation, which means that the corpus related to re-victimisation was relatively small.

We have included dating violence in this working definition. This was strategic and reflects a commitment to an inclusive understanding of intimate relationships. Dating violence occurs between non-cohabiting partners and in other “dating” relationships, and has significant similarities to other forms of intimate partner violence and sexual assault (Christopher & Pflieger, 2007; Chiara, Sabina & Ho, 2014). It is acknowledged, however, that dating violence in younger cohorts (e.g. young people in high school) can be qualitatively different to other forms of intimate partner violence, in part due to practical limitations on sexual intimacy (Noonan & Charles, 2009). As such, discretion has been used in this paper regarding the inclusion of research based on high school cohort data.
Co-occurrence
Domestic violence and sexual assault can occur in the same incident: specifically, this occurs when an intimate partner uses sexual violence. It is typically referred to as intimate partner sexual violence (IPSV) and is a both a form of domestic violence and a form of sexual assault (Macleod, 2014b).
IPSV is a common form of SXA, with intimate partners perpetrating most adult sexual assault (Black et al., 2011; Logan, Walker, & Cole, 2013; Tjaden & Thoennes, 2000). ANROWS’s additional analysis of the 2012 PSS has shown that “[s]ince the age of 15, 805,900 women were sexually assaulted by a male intimate partner: this is one out of every eleven women in Australia (9.2%)” (Cox, 2015).
In general, IPSV is characterised by “deliberate intimidation or coercion” and may either be pressure to perform sexual acts that the victim is not comfortable with, or to engage in acts at a time that they do not wish to do so (Cornelius & Resseguie, 2007; Macleod, 2014a; Shorey, Cornelius, & Bell, 2008). Not all forms of IPSV are criminalised (McOrmond- Plummer, Easteal & Levy-Peck, 2014).
After completing a meta-analysis of available studies, Bagwell-Gray et al (2015) suggested separating intimate partner sexual violence into:
- sexual assault – high force and high invasiveness, such as rape that uses physical force or threat of actual physical harm, which was found to be experienced by 36.1 percent of IPV survivors (n = 3178, 11 studies) (wide variation in prevalence rates: 9% to 91%);
- sexual coercion – low force and high invasiveness, where non-physical tactics of manipulation are used to obtain penetrative sex (including vaginal or anal penetration by penis, fingers or objects), which was found to be experienced by 24.9 percent of IPV survivors (wide variation in prevalence rates: 17.4% to 91%) (n = 1408, 5 studies);
- sexual abuse – low force and low invasiveness, where non-consensual dominating or humiliating tactics are used; and,
- forced sexual activity – high force and low invasiveness, physically forced, non-penetrative sex acts.
(Meta-analyses for sexual abuse or forced sexual activity were not possible) (Bagwell-Gray et al., 2015)
IPSV may occur in the context of any sexual behaviour (e.g. kissing, sexual touching, watching pornography, bondage scenes, oral sex, vaginal sex). IPSV may involve using sex, sexualised threat and sexualised humiliation as part of a larger pattern of coercive control of a partner (Logan, Cole, & Shannon, 2007).
IPSV involving force or threat rarely occurs in isolation, and is typically accompanied by other forms of violence (McOrmond-Plummer, 2014). Despite this co-occurrence, the nature of these assaults, as well as their impacts on the victim, has led researchers to classify IPSV as a distinct form of violence that differs from non-sexual physical and emotional DV (Miller, 2006; Spohn & Tellis, 2012).
Although IPSV is the more common term, this phenomena is referred to in different ways in the literature, often reflecting the theoretical approach of the researcher. Other common terms include:
- marital rape;
- sexual coercion;
- date rape/violence;
- intimate sexual violence;
- intimate partner sexual assault; and
- domestic sexual assault.
(Martin et al., 2007; Spohn & Tellis, 2012)
Theories of re-victimisation and co-occurrence
Over the past 30 years, researchers have developed many different explanations of why and how re- victimisation and IPSV occur (Martin et al., 2007). These theories provide the basis for academic work in the area and have become increasingly complex in order to accommodate a greater appreciation of the multifaceted nature of these types of violence (Brassard, Darveau, Péloquin, Lussier, & Shaver, 2014; Busby, Holman, & Walker, 2008).
Understanding the available explanatory models is important because such models provide the theoretical lens that determines what studies are undertaken in the first place. Explanatory models also affect the implementation of findings as they provide the basis from which violence, its causes and its prevention, are conceptualised (Clark & Quadara, 2010; Thomas & Fremouw, 2009; Vatnar & Bjørkly, 2008).
Key findings in this section:
- Research on re-victimisation and IPSV comes from a range of disciplines including psychology, social work, criminology, family studies and feminist studies.
- The models, concepts and typologies used to understand violence affect how research findings are interpreted.
- Approaches to IPSV and re-victimisation research can be roughly divided into:
- individualised approaches that understand violence as an personal maladjustment that is expressed and influenced by interpersonal dynamics; and
- societal approaches that understand violence as an issue that, while always occurring in the context of individual choice and action, reflects macro social inequalities.
- Individual approaches dominate research in this field.
Common disciplinary approaches
Theoretical approaches are often aligned with a specific academic discipline, although research may align with more than one discipline. Disciplines often have accepted accounts of the nature of reality (ontology) and consistent explanations of what counts as knowledge and how you should go about obtaining knowledge (epistemology and methodology) (Desai & Saltzman, 2001).
Some of the more common approaches found in the corpus were:
- Psychology is a significant scientific field characterised by concern with the mental and behavioural characteristics of groups or individuals. Research from this field that was identified in the corpus tended to presuppose that behaviours can be counted and that acting in a certain way was linked to the attitudes that a person had about that behaviour. To reflect this approach, methods used by psychologists tended to involve retrospective self-report of a participant’s actions and beliefs. The collected data frequently undergoes significant statistical analysis and is based in a positivist epistemology. Assessments of risk of both perpetration and victimisation tend to be calculated using actuarial measures and standardised tools. Research psychologists often assume that there is a knowable and mappable pathway for both victimisation and perpetration that can be measured against a “normal” person. Psychology research identified in this paper disproportionately uses US college samples and tends to promote individualised “treatment” as an appropriate response to violence.
- Social work is a field of intervention into systemic social inequality. Within the corpus, research from this field was characterised by both an understanding of disadvantage as a characteristic of inequitable social systems, and a concern with practical assistance to people most negatively affected by such systems. In addition, some social work approaches concentrated on establishing the value, and maximising the impact, of intervention (such as client advocacy, case work and community support) on the well-being of individuals and their communities.
- Criminology is the study of criminal behaviour, including its cause, patterns, consequence and prevention. Research from this field identified in the corpus tended to be concerned with effectiveness of mechanisms to minimise re-offending. In this context, a focus on “risk” was common –risk was understood in relation to the frequency and severity of violence, as well as the capacity and/or likelihood of rehabilitation (Salter, 2012). Researchers often used administrative data from justice systems in order to provide actuarial models of recidivism risk, with such work often positioning offending pathways as individual, rather than social, problems (Clark & Quadara, 2010). Criminology has a significant influence on SXA research and practice in Australia.
- Family studies is an approach which appears limited to certain schools within the US. Within the corpus, it is characterised by methods similar to those used by psychology, combined with values that are generally conservative and family-centric. Researchers are often influenced by psychoanalytic concepts, use more normative scripts of relationship development, place high value on keeping family units together and perceive actions in the family of origin as central to child development (Peterson& Bush, 2013). Family studies research frequently uses the Conflict Tactics Scale (CTS) and tends to promote a gender-neutral account of violence that presumes “mutual responsibility” for violence incidents.
- Feminist approaches may be embedded in a range of disciplines and methodologies. Feminist accounts of intimate partner violence tend to emphasise that violence occurs in the social context of embedded gender inequalities which are reflected and further established by gendered norms and behaviours (Shorey et al., 2008). Gendered violence is typically understood as a continuum from normative expressions of sexism to brutal assault (Kelly, 2013). Some researchers contextualise their work through an understanding of patriarchy as a key mechanism for providing the systemic social structures and gendered power relations that are critical aspects of violence against women (Hunnicut, 2009). Methods used by feminist researchers tend to emphasise the complexity of the lived experience of violence and value women’s stories – feminist methods are therefore more likely to be qualitative and participatory. Such approaches also increasingly examined the intersection of a range of forms of systemic disadvantage, so that meaningful acknowledgement is made about the similarities and differences in the experiences of violence by “otherised” women such as Aboriginal and Torres Islander women, women with a disability and lesbian women (Crenshaw, 1991; Parkinson & Zara, 2014). Consistent with other western English-speaking countries, in Australia these feminist approaches have had significant impact on the development and maturation of the DV sector and have also influenced government policy on violence against women (Ahrens, Dean, Rozee, & McKenzie, 2008; Cooper et al., 2008; Costello, 2005; Maas-DeSpain & Todahl, 2014).
Each approach provided the context for a variety of theories of the cause and nature of co-occurring DV and SXA.
Theories, concepts and typologies
Over the past 30 years, researchers have developed many different explanations of why and how re-victimisation and IPSV occur (Martin et al., 2007). These theories provide the basis for academic work in the area and have become increasingly complex in order to accommodate a greater appreciation of the multifaceted nature of these types of violence (Brassard, Darveau, Péloquin, Lussier, & Shaver, 2014; Busby, Holman, & Walker, 2008).
Understanding the available explanatory models is important because such models provide the theoretical lens that determines what studies are undertaken in the first place. Explanatory models also affect the implementation of findings as they provide the basis from which violence, its causes and its prevention, are conceptualised (Clark & Quadara, 2010; Thomas & Fremouw, 2009; Vatnar & Bjørkly, 2008).
The corpus revealed a large number of explanatory and descriptive theories of co-occurrence. Below is an outline of the models, concepts and typologies that dominated the selected literature. Please note that this section does not engage with the empirical support for any of the available explanatory models, but rather outlines the key ideas that are active in the field.
Theories
Four theories (macro frameworks that provide broad-scale explanation of a wide range of types of violence) were common in the corpus: the ecological model, the transmission of violence model, social learning theory and conflict theory. Some of these models are generally positioned as conceptually distinct and are not routinely used simultaneously.
The social ecological model, also known simply as the ecological model, understands that a person’s risk of gendered violence, including SXA and DV, is affected by factors at four levels – the individual, the relational, the communal and the societal (Conway et al., 2010). A minority of scholars also explicitly include biological factors in the model (Bronfenbrenner, 2005; Busby et al., 2008). The ecological model is a public health approach to interpersonal violence and therefore was developed to address and explain violence at a population level, and has been used widely in the violence against women field (Coulter & VandeWeerd, 2009; Heise, 1998). The model may be used to inform various community level interventions, including structural and attitudinal change and bystander intervention programs (Casey & Lindhorst, 2009; Moynihan, Banyard, Arnold, Eckstein, & Stapleton, 2010). The ecological model has been criticised for its lack of theoretical coherence, as well as for its positioning of gender inequality as one of several (rather than the underlying and key) factors which cause violence against women (Pease, 2008, 2014). If we consider the full range of research on SXA and DV (including that which is not informed by the ecological model) most DV and SXA research is concerned with the inner layers of the model – the interpersonal and individual – with less research completed on the broader community and societal influences on violence perpetration and victimisation (Vagi et al., 2013). Despite this, there is substantial research regarding the communal and social influences on violence against women (VAW), in the VAW field and in more general sociological and/or feminist research.
The theory of transmission of violence (also known as the “cycle of violence”) is a model of violent behaviour that asserts that experiences of violence in childhood create significant developmental problems and drastically increase the likelihood that the victim will act violently later in life (DeLisi, Caudill, & Trulson, 2014; Reckdenwald, Mancini, & Beauregard, 2013). The model is particularly common in accounts of the impact of CSA (Boivin, Lavoie, Hébert, & Gagné, 2012; Fergusson, Boden, & Horwood, 2006; Friesen et al., 2010; Reckdenwald et al., 2013). With the scope of this model, researchers may invoke a simplified account of direct “transmission” of violence or may engage more critically with the social norms and psychological impact of experiencing violent contexts.
Relatedly, social learning theory posits that violent behaviours are learnt through observation and imitation of the actions of others, especially parents (Busby et al., 2008; Feiring, Simon, Cleland, & Barrett, 2013; Monson & Langhinrichsen- Rohling, 1999; Shorey et al., 2008). It is the dominant theory to explain the relationship between child abuse and adult DV perpetration (Fang & Corso, 2008). An adult’s violent orientation is postulated to be more general than the specific forms of violence that were observed in childhood (Ireland & Smith, 2009). Research findings are mixed, with some statistical modelling of victimisation and perpetration across the life course showing very poor fit to the theory (Cyr, McDuff, & Wright, 2006). Social learning theory is frequently used in conjunction with theories of the intergenerational transmission of violence.
Conflict theories, such as the coercion hypothesis, presume that conflict is a normal part of all interpersonal relationships within this model. Adults try to diffuse conflict through influencing the other party, with some relationships having higher rates of conflict than others (Shorey et al., 2008). A range of tactics can be used to diffuse conflict, including aggression and violence (Dutton & Goodman, 2005; Shorey et al., 2008). This ontology forms the basis of the Conflict Tactics Scale and has been criticised for the normalisation of violence it may encourage.
Theories of violence provide a broad explanatory framework that informs and shapes research on IPSV and re-victimisation.
Concepts
Unlike “models” of violence which provide a general, but dynamic, explanation of violence; a “concept” is a static explanation that is more likely to relate to a specific scenario or community.
A wide range of concepts were used by scholars to provide a framework for understanding the nature of re-victimisation and IPSV. These concepts provide a lens for understanding the ontology of violence. Four of the most significant concepts are outlined below.
The concept of family violence is favoured by some Aboriginal and Torres Strait Islander women “as it encompasses all forms of violence in intimate, family and other relationships of mutual obligations and support” (Mitchell, 2011). Given the complex kin structures and family relationships active in many Aboriginal and Torres Strait Islander communities, this differentiation is important as the lived experience of violence may be different to that experienced by women living in more exclusive dyad or nuclear family structures. Harry Blagg has argued that the use of a distinct term enables the impact of colonisation and “settlement” to be embedded in the understanding of patterns of interpersonal violence (Blagg, Murray, Ray & Macarthy, 2000; Keel, 2004). The definition of family violence almost always includes sexual violence, including CSA and IPSV (Keel, 2004). Some Indigenous academics argue that we need a conceptualisation of intimate partner violence that is culture and law centric and which does not rely so heavily on Western psychological and sociological theorising (Hovane, 2007, 2014). However in some other contexts the term “family violence” has been criticised for reducing the focus on the gendered nature of violence, and potentially suggesting that it is family dynamic, rather than male perpetration, that is primarily responsible for violence against women (Tomison, 2000).
Coercive control is a key concept in DV research and is particularly significant for feminist research in the area. Coercive control describes a particular relationship dynamic that is typically understood as the most damaging form of violence between partners – one characterised by the use of multiple strategies of threat and violence to control the behaviours of one’s spouse (Stark, 2009, 2010). A range of violent behaviours such as sexual coercion, sexual degradation and sexual assault may be central to broader patterns of coercion (Logan et al., 2013; Macleod, 2014b; Tanha, Beck, Figueredo, & Raghavan, 2010). Coercive control is often contrasted to situational couple violence, which is defined as relationships where fighting may arise in a specific context, but where this aggression is typically mutual and not characterised by attempts to constrain the day to day activities of the other party. Some couples may not fit neatly into either category, and thus a continuum should be understood to exist between situational couple violence and coercive control (Maas-DeSpain & Todahl, 2014).
Typologies
Typologies of violence are a common way of differentiating and understanding IPSV and are a highly specific descriptive model of violence.
A typology of violence is a way of identifying key similarities in the lived experience of certain types of violence, such as the emotional impetus for a particular act or the relational impact of specific behaviours. Typologies enable us to note how different contextual and situational factors affect the way that violence occurs and are often based in in-depth qualitative analysis. The typologies identified as part of this paper examined the experience of IPSV from different perspectives and thus made different distinctions.
A common typology distinguishes between different contexts of assault (e.g. rape as a continuation of other violence in a relationship as compared to rape as an expression of sadistic sexual arousal), while others distinguish between physical assaults that are part of sexual activity and those that happen before sex (“make up” sex) (Bergen & Bukovec, 2006; Finkelhor & Yllö, 1987; Maas-DeSpain & Todahl, 2014; Martin et al., 2007).
These typologies place IPSV in the context of the dynamics of violent relationships.
Typologies have also been developed for:
- sexual coercion (Maas-DeSpain & Todahl, 2014; Martinet al., 2007);
- perpetrator characteristics (Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000; Monson & Langhinrichsen-Rohling, 1999; Shorey et al., 2008); and
- more general DV dynamics (Bair-Merritt, Ghazarian, Burrell, & Duggan, 2012; see also, Johnson, 2006).
Typologies are rarely used to explain re-victimisation, possibly because it is difficult to provide sufficient detail across multiple types of violence in a way that would enable a meaningful typology to be produced.
Comparing approaches
Researchers may combine certain models, concepts or typologies to give a more complete explanation of violence (e.g. coercive control might be a part of an ecological model of violence). However some theories do not map together, as the underlying assumptions are incompatible (e.g. conflict theories do not align easily with certain typologies of violence).
Overall, a distinction can be made between two broad approaches to DV and SXA that were evident in the corpus.
The individualised approach, which is dominant in this corpus, tends to understand violence as an individual maladjustment that is expressed and influenced by interpersonal dynamics. This approach generally has a methodological focus on quantitative statistical methods and presumes that, while gendered violence is problematic, conflict is inevitable and normal (Wangmann, 2011).
In contrast, the societal approach tends to understand violence against women as an issue that, while always occurring in the context of individual choice and action, reflects macro social inequalities. Researchers working in this approach use a wide range of methods including quantitative, qualitative and mixed method modalities. In comparison to researchers with a more individualised approach, these researchers are more likely to value the insights available through qualitative methods (Hamby, 2014). These researchers are also more likely to value personal narrative and to assert that gendered violence is fundamentally unacceptable (Tanha et al., 2010).
The two approaches have substantial epistemological and political tensions. In line with these different understandings of the nature of violence and what should (and should not) be done about it, they produce research using very different methods and use different samples with different definitions of DV and SXA (see above) (DeKeserdy & Schwartz, 2001). Combined with the distinct limitations of survey instruments used in each approach, the two approaches produce remarkably different study findings (Desai & Saltzman, 2001; Holtzworth- Munroe, 2005; Romans et al., 2007; Wangmann, 2011; Zweig, Dank, Yahner, & Lachman, 2013).
Methods used by researchers examining re-victimisation and co-occurrence
Overall, most research on IPSV and re-victimisation uses retrospective single assessment reports (Friesen, Woodward, Horwood, & Fergusson, 2010). Below is an examination of the limitations and biases that are common in the literature on concurrent DV and SXA victimisation. In keeping with a more “Public Health” approach to reviewing available literature, we provide extensive detail of the nature of these limitations – this detail is not meant to dissuade the reader from engaging with the available research, but rather it aims to provide the basis for understanding the constraints on the findings that are outlined in the body of the paper.
Life-course research: Key limitations
Life-course studies provide an actuarial examination of risk factors by mapping variables against certain outcomes and then modelling patterns of risk. These studies are particularly common within re-victimisation research. The resulting models are able to provide insight into pathways to recidivism and victimisation, however they are often inaccurate due to low base rates (i.e. not many people in the population experience the event of concern) and tend not to be able to accurately plot patterns of victimisation (Andersen, Hughes, Zou, & Wilsnack, 2014; Campbell, 2005; Dietrich, Smiley, & Frederick, 2007). Despite looking at lived experience over time, most research of re-victimisation is not longitudinal, which makes the examination of a set of events that happened over a long period of time methodologically precarious (Goodlin & Dunn, 2010).
Key findings in this section:
- The lack of longitudinal studies reduces our ability to make conclusions about causal factors or the nature of victimisation over time.
- Research on re-victimisation and IPSV often focuses on sub-populations that are not representative of the general population.
- The way that research questions are presented (and who they are presented to) significantly affects the research findings.
- The stigma of re-victimisation and IPSV may create bias in reporting.
- The use of inconsistent definitions makes comparing results across studies difficult.
- Commonly used survey instruments, such as the CTS, have significant limitations.
Cross-sectional research: Key limitations
Cross sectional research is a “snap shot” of lived experience at one time. It can be used to effectively show the pattern of victimisation across a population at a particular moment. However, it does not allow for any analysis of the causal relationship between variables (Classen, Palesh, & Aggarwal, 2005; Krebs, Breiding, Browne, & Warner, 2011; Rees et al., 2011). Controlled longitudinal research that provides for a comparison group is the best way of obtaining causal information (Rees et al., 2011). Cross-sectional research may not allow for a full understanding of the complexity of daily experience, especially of different forms of violence happening in the same context (McFarlane, 2007; Sullivan, McPartland, Armeli, Jaquier, & Tennen, 2012).
The cross-sectional research found in this corpus is almost all retrospective (i.e. collecting data about things that have already happened). Some of the key limitations of the types of retrospective studies used in the corpus are detailed below.
Bias caused by population selection
Bias occurs when there is a systemic pattern of inaccurate reporting. Bias is a major concern for researchers completing retrospective studies as researchers rely on a participant’s memory of historic events (Lalande & Bonanno, 2011). By understanding the potential for bias, certain types of limitations of the available research are contextualised.
Much of the available research on IPSV and re-victimisation is unable to be extrapolated to findings about the general population, with research being focused on non-representative groups such as women who were attending psychology clinics (Friesen et al., 2010).
As noted earlier, a large amount of research on IPSV and re-victimisation has been completed with college students, and so these findings may not be generalisable to the broader population (Zurbriggen, Gobin, & Freyd, 2010). In comparison to the general population, college students are more highly educated, are disproportionately from advantaged socio- economic backgrounds, are less likely to have a severe disability and are generally young adults.
Women have participated in more violence research than men, potentially due to the tendency for academics to select study populations that are either couples (predominantly heterosexual, and thus both men and women participate in equal number) or victims (primarily women participants) (Shorey et al., 2008). The lack of comparable data for women and men may restrict our ability to meaningfully identify and articulate the gendered nature of violent behaviours.
In addition, research on perpetrators is less common than research on victims. Most perpetrator research focuses on men who have been convicted of DV and/or SXA offences. Researchers note that this is likely to result in bias, as this group is atypical of men who perpetrate violence and the very nature of their incarceration may mean that these men are unable to report certain behaviours to researchers (Clark & Quadara, 2010).
The use of differing ways of selecting research participants also affects generalisability. The way that a sample is selected affects the research findings, which is likely to further entrench theoretical, epistemological and ontological differences in approaches to researching and understanding violence. In the case of research into re-victimisation and co-occurrence, a divide emerges between the findings of research based on samples of women who are known to have been victimised (e.g. women who are in women’s shelters) and findings from studies that use a sample of women from the general population, with women from the former reporting substantially higher rates of abuse, as well as reporting more severe violence with greater personal, psychological and health impacts (Romans, Forte, Cohen, Du Mont, & Hyman, 2007).
Relatedly, the way that a survey question is phrased makes a significant difference to reporting and thus to the findings of research. This was demonstrated in a research project where participants in a single birth cohort study were interviewed twice on the same day. In each interview, the participants were questioned using a differently worded violence questionnaire. The difference in the results was so large that they found opposite gendered patterns of violence – in one, men were the primary victims of IPV, while in the other, women were the more common victims (Langley, Martin, & Nada-Raja, 1997; Magdol et al., 1997; Romans et al., 2007).
Bias caused by incomplete reporting
Under-reporting is an important issue in all research on sensitive topics. Under-reporting in research occurs when a study participant has experienced something but, when asked, does not tell the researcher about it. Scholars have identified that social desirability is a major factor in the under-reporting of SXA and DV, with a sense of shame about victimisation and/or perpetration, fears about researcher response and gendered social scripts affecting what women and men report (Chiu et al., 2013; Ludermir et al., 2008; Martin et al., 2007). IPSV is more frequently under-reported than other forms of DV or SXA (Heenan, 2004; Wall, 2012). With awareness of this phenomenon, some researchers work extremely hard to develop surveys where the phrasing and structure enable people to answer questions in a way that feels comfortable and thus to reduce the impact of under-reporting on the research findings (DeKeserdy & Schwartz, 2001).
In addition, recall bias is a result of individuals being more likely to recall events that are memorable; what counts as memorable varies with personal and cultural factors (Casey & Nurius, 2005; Hetzel & McCanne, 2005; Sullivan et al., 2012). Although research is mixed, evidence suggests that gender non-conforming expressions of violence are often particularly salient: so that men tend to underestimate their own violence and overstate the violence of their female partners (although tending to see such violence as not serious), while women tend to overestimate their own violence and underestimate the violence of their male partners (Dobash & Dobash, 2004; Doroszewicz & Forbes, 2008). In addition, recall bias may be present in the form of trauma-related symptomology such as individuals not remembering distressing events (e.g., childhood sexual abuse) (DeKeserdy & Schwartz, 2001). Retrospective studies on IPSV and re-victimisation, especially those that ask about events a long time ago or which ask very specific questions about incidents that occur frequently, are more likely to be affected by recall bias (Desai & Saltzman, 2001; Gobin, Iverson, Mitchell, Vaughn, & Resick, 2013; Jennings, Zgoba, Maschi, & Reingle, 2014).
Comparability: Inconsistent phenomena definitions
Numerous commentators have identified that DV and SXA are inconsistently defined in the research literature (DeKeserdy & Schwartz, 2001; Ireland & Smith, 2009). Some definitional variation is important, as this supports a nuanced understanding of violence, especially when considering contexts where alternative manifestations of gendered violence may be present (Tapia, 2014). However the use of different definitions while examining similar populations (and in research aimed at answering similar questions) may impact the comparability and utility of findings (Desai & Saltzman, 2001; Ireland & Smith, 2009).
Much of the mainstream DV research is unable to be utilised for an examination of IPSV, as it is common for DV research to either exclude IPSV altogether or fail to differentiate IPSV from other forms of violence (Panuzio & Dilillo, 2010; Schewe, Riger, & Howard, 2006; White, McMullin, Swartout, Sechrist, & Gollehon, 2008). This limitation is slowly being addressed as commonly used instruments, such as the Revised Conflict Scale (CTS2 – see below for a description), now provide for a separate measure of IPSV.
Sexual violence is a particularly difficult concept to define, and the literature has “a significant and pervasive problem of a lack of specificity in definitions” (Logan et al., 2013, p. 115). Such definitional difficulties affect both “cross-type” re-victimisation and IPSV research as both require a robust definition of sexual violence. In a critical examination of terminology used to refer to IPSV in 49 research documents, it was identified that there was no common terminology used in this research (Bagwell-Gray, Messing, & Baldwin-White, 2015). Problematically, IPSV researchers use the same words to mean different things, and as a result, studies are confusingly inconsistent and ultimately difficult to pool (Hamby, 2014).
Definitional inconsistency is particularly acute in research on sexual coercion. Sexual coercion can be understood as a spectrum of behaviours between emotional coercion and physical force, with researchers defining the beginning of “coerced sex” at different points (Finkelhor & Yllö, 1987; Heenan, 2004). For instance, they may:
- include (or exclude) social pressure as a type of coercion;
- include (or exclude) sexual pressure as a type of IPSV;
- include (or exclude) sex that was initially unwanted and then became wanted as a type of IPSV;
- distinguish between sex that was wanted and sex that has been consented to;
- include only sex that was either physically or verbally coerced; and
- include only sex that was physically forced.
(Bagwell-Gray et al., 2015; Brousseau, Hébert, & Bergeron, 2012; Lehrer, Lehrer, & Koss, 2013; Logan et al., 2013; Maas-DeSpain & Todahl, 2014; Martin et al., 2007)
These definitional variations, more apparent in sexual coercion research but still present in DV and SXA research more generally, make it very difficult to meaningfully compare studies or to concretely or confidently understand the nature of IPSV or re-victimisation.
Undifferentiated categories of violence
In addition to definitional inconsistency, the methods used in some studies fail to distinguish between different forms of violence, thus making it more difficult to understand the extent or characteristics of IPSV and re-victimisation.
Earlier research on DV had a tendency to combine physical and sexual violence in relationships. This was a consequence of:
- survey instruments that did not differentiate the two type of assault; and
- the way that the data was presented at write up (Wangmann, 2011).
Such conflation both obscured the nature of DV and made it impossible to identify the prevalence of IPSV within these studied populations. This limitation was also common in the collection and representations of data for childhood abuse that were presented in re-victimisation research (Bonomi et al., 2008; Cannon, Bonomi, Anderson, Rivara, & Thompson, 2010).
In much of the currently available literature, there are significant difficulties in distinguishing between multiple incidents involving a single perpetrator and a single (or multiple) incident involving more than one perpetrator (Casey & Nurius, 2005; Koss et al., 2007; Logan et al., 2013). In some research, multi-perpetrator cases are excluded or coded like single perpetrator incidents. Multi-perpetrator domestic violence and sexual assault research is particularly hampered by these types of systemic data limitations (Salter, 2014).
Commonly used survey instruments
There are a range of instruments used to measure the incidence and prevalence of domestic and sexual violence, including instances of IPSV and/or re-victimisation (Garcia-Linares, Pico-Alfonso, & Sanchez-Lorente, 2005). The selection of survey instrument determines what data is collected and thereby shapes the understandings of violence that emerge from the research. While much of the critique of these instruments engages with how experiences of IPSV are captured using these survey instruments, such critique is equally applicable to re-victimisation research that engages with DV.
Behavioural checklists, such as the Conflict Tactics Scale (CTS) and Sexual Experiences Survey (SES), involve concrete descriptions of behaviours. Typically, the research participant rates how frequently a certain behaviour occurs in their intimate relationship(s), including “never” (Desai & Saltzman, 2001). At the analysis stage, behaviours are separated into more or less severe forms of violence/coercion, based on expectations of harm to the victim. The survey developers selected the survey wording very carefully in order to minimise under-reporting – for instance “forced sex” is not described as “rape” (Abbey, Parkhill, & Koss, 2005). Despite being a standardised measure, researchers have some capacity to vary the definitions used in these scales, resulting in variation that can make comparison of research with other studies using the same instrument impossible (Logan et al., 2013).
Partner-specific behavioural checklists are the most commonly used instruments for re-victimisation and IPSV research, with the corpus analysed for this state of knowledge paper demonstrating a dominance of the CTS and SES. Prior to the release of the Revised CTS (CTS2), the SES was used primarily for research involving IPSV (the original CTS did not ask about sexual violence), although the SES has also remained in use in a large number of studies that were published post the release of CTS2 (Koss et al., 2007). Research using the CTS and CTS2 remains very common in the literature, despite ongoing criticisms of the scales (Hegarty, Bush, & Sheehan, 2005; Logan et al., 2013; Wangmann, 2011).
There are a number of key limitations of these scales that are noteworthy given the dominance of these instruments in the available literature:
Scales like the CTS2 do not identify the context of the violence, thereby not accounting for the functionality of the violence within a relationship (Próspero & Vohra-Gupta, 2008). Similarly, such scales are unable to identify the temporal sequencing of the violence (i.e in what order things happened) and are therefore very limited in their ability to separate defensive/protective violence from acts of aggression (Bonomi, Holt, Martin, & Thompson, 2006; Cole, Logan, & Shannon, 2005; Shorey et al., 2008). In addition, such scales typically do not engage with the intent of the violence, its emotional impact or the extent of physical harm, thereby potentially erasing significant gendered and/or typological differences (Hegarty et al., 2005; Palmetto, Davidson, Breitbart, & Rickert, 2013).
The CTS tends to find that males perpetrate most IPSV but that there is gender parity in perpetration of physical violence. These findings, while consistent across studies that use the instrument, are inconsistent with other methods of examining the same phenomenon such as examinations of police arrest data, law enforcement data, witness data and almost all other forms of self-report (Hamby, 2014). There is significant ongoing debate about the meaning and implication of the gender symmetry reported using CTS2 (Doroszewicz & Forbes, 2008).
Consistent with other retrospective research, these scales are affected by recall bias. Such bias is particularly apparent when researchers interview couples, with extremely poor agreement between couples regarding the nature of the violence experienced in the relationship (Dobash, Dobash, Wilson, & Daly, 1992).
Different types of self-report behavioural checklists provide substantially different findings regarding the prevalence of violence (DeKeserdy & Schwartz, 2001). For example, in a study of refuge users (n=138) that compared the rate of IPSV calculated using the CTS2 and the revised Sexual Experiences Survey, it was found that the CTS2 calculated 16.7 percent more cases of IPSV (63% vs 73.2%) (Moreau et al., 2015). As Hamby (2014) notes, studies based on self-report behavioural checklists show a startling range of between 2 percent and 60 percent prevalence of violence in supposedly similar “general” community samples. This suggests that “our [measuring] technology is far from adequate” (Hamby, 2014, p. 151).
Comparability of study findings
Overall, research on re-victimisation and IPSV is difficult to collate into a coherent understanding of these phenomena. The use of different definitions and collection methods, as well as differences in study population mean that it is difficult to compare research findings or complete meta-analyses of the available data (Garcia-Linares et al., 2005; Pico-Alfonso et al., 2006). Researchers emphasise the need for validated instruments, while also pointing out that an over-reliance on established methods reinscribes certain understandings of violence that may not reflect lived experience (Desai & Saltzman, 2001; Hamby, 2014; Sørbø, Grimstad, Bjørngaard, Schei, & Lukasse, 2013).
Before proceeding to an examination of the study findings, let us reiterate that the extent of the limitations of the studies examined in this review are consistent with the limitations of other emerging fields of quantitative research. All research has methodological limitations, epistemological variation and definitional inconsistencies – by acknowledging these in detail we do not dismiss the value of this work, but rather provide a meaningful basis for understanding the exact nature of the available research.
This state of knowledge paper now turns to the specific findings of the corpus.
Rates of re-victimisation and co-occurrence
There is extensive research on the rate of IPSV and re-victimisation of women. This research provides conflicting evidence regarding the extent of these two phenomena, however researchers are consistent in identifying both types of victimisation affect a significant proportion of women.
There was significant overlap in re-victimisation and IPSV populations, with many women experiencing re-victimisation that included IPSV. This means, similar to the overlap between DV and SXA more generally, that IPSV and re-victimisation are two populations that are unable to be fully distinguished from each other, and should thus be considered both as combined and distinct phenomena.
This section examines statistics related to the rate, prevalence and extent of re-victimisation and IPSV. This section is limited to an outline of statistical findings and provides brief commentary on related methodological considerations.
As discussed earlier, research on the prevalence or rate of victimisation is subject to a range of methodological limitations. Although such limitations are significant, this work is still valuable as it enables us to scope the extent of the problem. Moreover, researchers in this field consistently acknowledge the key limitations of such research, including the issue of under-reporting, and make efforts to address these through sensitive interviewing and ongoing improvements in research design. While acknowledging that these statistics are likely to be underestimates of the extent of the violence, they are nonetheless our best insight into the scale of the phenomena.
Key findings in this section:
- Estimated rates of re-victimisation vary according to what patterns of violence are included in the research design.
- Women who experienced child sexual abuse (CSA) were more likely to experience IPSV than women who had not experienced CSA. Similarly, these women were more likely to experience DV (not limited to sexual violence) in their adult relationships.
- Research was more mixed regarding patterns of re-victimisation that included violence during adolescence.
- There was little research on re-victimisation rates for adult victimisation for separate DV and SXA incidents.
- Estimates of IPSV rates varied significantly depending on the definition of IPSV used for the research.
- In the research examined for this paper, intimate partner sexual coercion was reported by between 24 percent and 62 percent of women. Intimate partner sexual assault was reported by between 1.7 percent and 46 percent of women.
- Most women who had experienced IPSV did not consider that the incident was an assault.
- IPSV generally occurs in the context of other forms of violence.
Re-victimisation rates
As outlined earlier in this article “cross-type” re-victimisation occurs when a woman experiences separate incidents of SXA and DV that involve different perpetrators across her lifetime.
Re-victimisation is an endemic issue, with longitudinal studies indicating that more than half of female victims of childhood sexual abuse experience physical or sexual re-victimisation (n = 159) (Barnes, Noll, Putnam, & Trickett, 2009).
Despite this, re-victimisation should not be considered an inevitable consequence of initial victimisation, as approximately a third of women recover rapidly from CSA and do not experience ongoing traumatisation and most are not re-victimised (Hébert, Lavoie, Vitaro, McDuff, & Tremblay, 2008). The ANROWS additional analysis of the 2012 PSS indicated that 67.6 percent of all women in Australia who had experienced childhood abuse did not experience cohabiting partner violence as an adult (this is estimated to be 1.1 million women) (Cox, 2015).
Understanding the extent of re-victimisation requires an engagement with a range of scenarios of victimisation. This paper examines available literature on re-victimisation in the following scenarios:
- re-victimisation involving child sexual abuse and intimate partner sexual violence;
- re-victimisation involving child sexual abuse and adult domestic violence (in research where type of adult domestic violence was not identified);
- re-victimisation involving child and adolescent victimisation; and
- re-victimisation involving separated instances of domestic violence and non-intimate-partner sexual assault.
In keeping with the focus of this review on “cross-type” victimisation, we do not consider the rate of “same-type” re- victimisation (i.e. experience or witnessing of DV and later adult DV victimisation or CSA and then experiences of SXA as an adult). Given the scope of this project, examinations of the rates of CSA and adult IPSV are within scope as IPSV is a form of DV.
Child sexual abuse and adult domestic violence
Women who experience CSA are more likely than those who have not experienced CSA to experience DV in their adult relationships (Garcia-Linares et al., 2005; Pico-Alfonso et al., 2006). In a Canadian sample (n = 16993), in comparison to women who hadn’t experienced CSA, those who had were 2.44 times more likely to experience psychological DV and 2.75 times more likely to experience physical DV (Daigneault et al., 2009). In a smaller US study (n = 637), and in comparison to women who had not experienced DV, women who had experienced DV were five times as likely (5% vs 25%) to have experienced CSA (Seedat, Stein, & Forde, 2005).
Estimates of prevalence of re-victimisation involving CSA and DV vary significantly. The percentage range of all women research participants who identified experiencing both CSA and DV was between 25 percent (from a case control study of women attending STI clinics) and 40 percent (from a small Spanish cross-sectional study) (Garcia-Linares et al., 2005; Williams, Larsen, & McCloskey, 2010).
A minority of studies show no relationship between CSA victimisation and adult DV victimisation (Murphy, 2011; Renner & Whitney, 2012). For example, a population based cohort study of Australian women found a statistically insignificant increase in the rate of CSA (contact and no contact) and/or physical abuse (27% vs 36%) for women who had experienced IPV (Schei, Guthrie, Dennerstein, & Alford, 2006).
More general research on violence shows that forms of child abuse other than CSA also have an effect on adult victimisation. According to the 2012 PSS, over half a million women in Australia have experienced both abuse when they were a child as well as cohabiting partner violence. This is a third of all women in Australia who have experienced childhood abuse (Cox, 2015). In a research project involving 3201 women, those who had experienced either physical, sexual or emotional abuse as a child were about 7 times more likely to experience abuse as an adult, while those who had experienced all three types of abuse as a child were 36 times more likely to experience abuse as an adult (not limited to DV incidents). This research found a dose response, with women who had experienced more incidents of child abuse experiencing more incidents of abuse in adulthood (Chiu et al., 2013; see also Murphy, 2011). Some research suggests that a combination of CSA and other forms of childhood abuse has greater impact than CSA only, and a sample of 10,187 adolescents found that neglect was a stronger predictor than CSA for future DV victimisation (Cannon et al., 2010; Renner & Whitney, 2012). Such findings are consistent with older research which emphasises that the impact of CSA is altered by broader environmental factors, including other violent and neglectful behaviours (Briere & Elliott, 1994).
Additional relevant literature is outlined in Appendix B.
Child sexual abuse and intimate partner sexual violence
A subset of women who experience re-victimisation across childhood abuse and adult domestic violence are women who experience adult IPSV.
Women who experience CSA are more likely to experience domestic violence that involves IPSV than women who have not. In a large national stratified sample of Canadian men and women (n=16,993), it was found that women who had experienced CSA were 3.68 times more likely to experience IPSV than women who had not experienced CSA (Daigneault, Hébert, & McDuff, 2009). Similarly, after adjusting for demographic variables, in a study of Chinese university students (n=3388), participants were 2.04 times more likely to have experienced IPSV if they had a history of CSA (Chan, 2011). In a study of women who had recently obtained protection orders, one in three women had experienced both threatened/forced sex by their partner and sex before the age of 14: in contrast, one in five (19.8%) of these women had experienced CSA but not IPSV (Cole et al., 2005).
Child and adolescent victimisation
Researchers, particularly from the psych-sciences, consider adolescence[3] to be a distinct developmental phase (Shaffer & Kipp, 2013). Increased personal independence and sexual exploration mean that the nature and expression of violence in adolescence is distinct from that found in childhood or adulthood. Although some studies do not use this category, the research on young people in their teens and early-20s is a distinct aspect of the corpus and needs to be examined separately from research on child and adult victimisation (Levy-Peck, 2014a). Below we outline relevant research regarding adolescent female victims.
Estimates of adolescent dating violence are difficult to obtain, particularly given the difficulty of aligning research and community terminology and the commonality of “horseplay” and “wrestling” in this age group, which inflates the reported frequency of physical violence, especially when researchers use behavioural checklists such as the CTS that do not place acts of violence in context (Hamby & Turner, 2013; Levy-Peck, 2014a). When reports of violence are limited to incidents that result in injury or fear or have a sexual aspect; then rates of adolescent dating violence were found to be similar to those in general adult populations (Hamby & Turner, 2013). The US Centres for Disease Control and Prevention reports dating violence rates of between 7.6 percent and 12.2 percent (Eaton & Matamala, 2014; Eaton et al., 2012). In a study of 917 teenage girls, 3.9 percent were in long-term dating relationships where they experienced more than one incident of violence (Gagné, Lavoie, & Hébert, 2005).
In most studies, CSA is significantly associated with SXA in adolescence, however a minority of papers show no statistically significant relationship between childhood violence exposure and later victimisation (Barnes et al., 2009; Gagné et al., 2005; Littleton, 2014; Rich, Gidycz, & Warkentin, 2005). Similarly, adolescent women who have experienced CSA report high rates of dating violence (Miller, Breslau, et al., 2011). A small study of adolescent female CSA survivors (n=126) found dating violence rates of 45 percent for physical violence and 90 percent for psychological violence (Cyr et al., 2006). Adolescents with a history of CSA reported double the rate of dating violence victimisation than their non-abused peers (n=774) (Hébert et al., 2008).
Research is mixed regarding the effect of adolescent victimisation on adult sexual victimisation. Several studies indicate that adolescent victimisation was a stronger predictor of adult sexual victimisation than CSA (Classen et al., 2005; Gagné et al., 2005; Siegel & Williams, 2003; Smith, White, & Holland, 2003). However, for incarcerated women (n=484), adolescent sexual assault did not increase the risk of adult sexual assault in women who had also experienced CSA (Raj et al., 2008).
More than physical or sexual violence separately, the co- occurrence of adolescent sexual and physical dating violence is associated with DV victimisation in young adulthood (Miller, 2006; White & Smith, 2000).
Separated instances of adult sexual assault and domestic violence
There is very little research available regarding “cross-type” re-victimisation when all incidents occurred during adulthood. One of the few available studies examined re-victimisation of DV and military sexual trauma, and found a co-occurrence rate of 52.7 percent (see also Iverson, Mercado, Carpenter, & Street, 2013; Kelly, Skelton, Patel, & Bradley, 2011).
Some research is available, however, on re-victimisation when it includes only DV or SXA violence, with studies examining adult and adolescent SXA re-victimisation (Macy, 2007; Ranjbar & Speer, 2013; Rich et al., 2005) and experiences of DV in multiple consecutive relationships (Garcia-Linares et al., 2005; Vatnar & Bjørkly, 2008).
Co-occurrence rates
Domestic violence is characterised by a range of abusive tactics, one of which is IPSV. In research on IPSV, it is typical to distinguish between IPSV and other forms of physical violence and emotional abuse. Such separation enables us to understand the structures and mechanisms of violence in greater detail and to meaningfully examine the rate of IPSV in relationships. However, this type of conceptualisation of IPSV may de-emphasise the physically and emotionally violent aspects of IPSV incidents. The use of these distinctions in this section reflects the nature of the available research, and does not imply support for the conceptual separation of IPSV from other dynamics of DV.
A note on lived experience vs research definitions
Some women do not define their experience of sexual coercion as assault. In a study of college women (n = 1060), of those who had experienced behaviours that were categorised as sexual coercion:
- 49.5 percent said they were not victimised;
- 45.4 percent said that the incident was a “serious miscommunication”; and,
- 5.2 percent said they had experienced an assault.
(Orchowski, Untied, & Gidycz, 2013)
Even for forced sex, the lived understanding does not necessarily align with research categories. Between 30 percent and 47.9 percent of women who have experienced forced sex by an intimate partner identify the experience as rape (Littleton, Breitkopf, & Berenson, 2008; Logan et al., 2013). These findings have both research and practice implications: as noted by Bergen “[i]f they do not define their experiences as rape, women are unlikely to report the violence or seek outside assistance” (2006, p. 6).
At a research level, this lack of alignment requires careful and nuanced consideration of the findings: on the one hand, sexual coercion is one of several behaviours that constitute IPSV. It is the most common form of IPSV. When statistics on IPSV include sexual coercion, they may be inaccurately read as indicating a more brutal form of abuse. In this way, care needs to be taken not to accidentally exaggerate the extent or nature of the problem. On the other hand, however, evidence also points to the difficulty in women identifying sexual assault within relationship settings and the cognitive dissonance that such realisations may cause. In this context, while women may not identify their experiences as assault we must be careful not to presume that this means that such assaults are not traumatising, brutal or explicitly violent. The following quote from a participant in a New South Wales (NSW) qualitative study demonstrates some of the cognitive pressure that women may feel maintain certain understandings of their experiences: “I’d talk myself out of thinking that I’d been raped… My reaction was this can’t be true. You’re stupid, change your mind” (Parkinson & Reid, 2014, p. 139).
The nature of IPSV and the impact of such assaults is only ever partially visible through an engagement with research. In order to help the reader be sensitive to some of the constraints of empirical findings, in the discussion of prevalence, where possible, definitions have been noted and findings contextualised.
Intimate partner sexual violence
The following rates are for IPSV incidents only and do not reflect other forms of non-sexual violence that may occur in a relationship.
Within populations not limited to IPV survivors, intimate partner sexual coercion was reported by between 24 percent and 62 percent of women (Brousseau et al., 2012; Cole et al., 2005; Doroszewicz & Forbes, 2008; El-Bassel et al., 2007; Messing, Thaller, & Bagwell, 2014; Próspero & Vohra- Gupta, 2008; Sabina & Straus, 2008; Stockman et al., 2013). The highest rate of coercion was recorded in a study of 209 heterosexual couples, surveyed using the Sexual Experience Survey (Brousseau et al., 2012). The lowest rate was found in the largest study (n = 799), which examined women receiving Emergency Department care and used the CTS2 instrument (El-Bassel et al., 2007).
Intimate partner sexual assault was reported by between 1.7 percent and 46 percent of women (Black et al., 2011; Daigneault et al., 2009; Messing et al., 2014; Miller, 2006; Morokoff et al., 2009; Romans et al., 2007). The lowest rate of sexual assault was found in a Canadian population survey (n = 17,005) (Daigneault et al., 2009; Romans et al., 2007). Other representative samples have found rates of between 5.9 percent and 9.4 percent (Black et al., 2011; Miller, 2006). The highest rates were found in high risk populations, including women experiencing police involved IPV, and women who were recruited at sexual health and substance use clinics (Messing et al., 2014; Morokoff et al., 2009).
The Australian component of the International Violence Against Women Survey found that “[b]etween 5-7% of [respondents] who had a current or former partner had experienced [IPSV]” (Mouzos & Makkai, 2004; Wall, 2012). The 2012 PSS produces a slightly higher estimate, with 9.2% of women in Australia having reported ever having experienced sexual assault by an intimate partner they may or may not have been living with (Cox, 2015). A small (n = 233) prospective study of middle-aged Australian-born women found 1.3 percent of all women had experienced IPSV and 11.6 percent of women who experienced domestic violence in the last 12 months had experienced IPSV (Schei et al., 2006). There is very little research on IPSV in Aboriginal and Torres Strait communities, although it is generally understood to be a frequent part of family violence (Adams & Hunter, 2007).
Additional relevant literature is outlined in Appendix B.
Intimate partner sexual violence and non-sexual physical assault
The lived experience of domestic violence which involves the use of both IPSV and other forms of physical DV is both common and well documented (Spohn & Tellis, 2012). As noted above, both IPSV and other forms of physical DV contribute to the overall dynamic of DV, however research in this field frequently separates these forms of physical violence.
Many of the characteristics of IPSV mirror those of other forms of physical DV – the assaults typically occur in private, and are witnessed (if at all) by people known to both the perpetrator and victim (e.g. family and friends) and, when the abuse is more severe, they often result in physical injury (Tellis, 2010). Conversely, although most women who experience IPSV also experience other forms of physical violence, some researchers argue that the co-occurrence of IPSV and other forms of physical violence is a distinct form of violence that is different from either form by itself (Bagwell-Gray et al., 2015; Katz et al., 2008; White et al., 2008).
Reported rates of DV that include incidents of both IPSV and other forms of physical DV vary depending on study population, with between 64 percent and 100 percent of women who indicated that they were raped by their partner also reporting that they were physically abused by them (McFarlane, Malecha, Watson, et al., 2005; Smith, Thornton, DeVellis, Earp, & Coker, 2002; Vatnar & Bjørkly, 2008; White et al., 2008). Similarly, of women who have been physically assaulted by their partner, between 26.2 percent and 68 percent had experienced partner rape/sexual assault, with between 30 percent and 75 percent experiencing sexual victimisation (i.e. the range of actions from sexual coercion through to sexual assault) (Campbell et al., 2013; Cole et al., 2005; Krebs et al., 2011; Martin et al., 2007; McFarlane, Malecha, Gist, et al., 2005; Spiller et al., 2012).
Some women experience violent physical assault and sexual assault within the same incident. In 30 percent of cases of intimate partner rape (n = 124), women reported that they were physically assaulted in response to their own physical refusal of forced sex (McFarlane, Malecha, Watson et al., 2005). A study of help-seeking women found that 70 percent had experienced sexual violence and physical attack simultaneously (Vatnar & Bjørkly, 2008).
IPSV may also co-occur with other forms of physical violence when it occurs in the form of post-violence sexual assault. A research project with men arrested for physical assault of their partner found that 13.6 percent reported having made their partner have sex with them immediately after “a violent argument, even though she didn’t want to have sex” (Basile & Hall, 2011).
In a study of patterns of daily abuse, other forms of physical violence were 3.4 times more likely to occur on days when IPSV also occurred (in contrast, non-sexual physical abuse was 64 times more likely to occur on days when psychological abuse occurred) (Sullivan et al., 2012). Women who experienced both non-sexual and sexual domestic violence were more likely to be punched, kicked and be attacked with sharp objects (e.g. knives) than women who experienced non- sexual physical DV only (Garcia-Linares et al., 2005). In a sample of 449 mothers who were living in DV refuges and had experienced non-sexual physical DV, those who had also experienced IPSV were physically abused more than those who had not experienced IPSV (Spiller et al., 2012).
Overall, these findings suggest that when women experience IPSV and other forms of physical assault, the non-sexual physical assault is more physiologically damaging than if it occurred in a context where IPSV was not also being perpetrated.
Conclusion
Identifying the rate of re-victimisation or IPSV is difficult. Especially when using more inclusive definitions of violence, current research demonstrates high rates of IPSV and re- victimisation. Like other sensitive topics addressed through retrospective quantitative research, findings varied according to population, but also by which survey instrument was used. The extent of the variation limits our ability to understand the epidemiology of these patterns of victimisation, and thus restricts our ability to plan or respond to these issues.
Characteristics of incidents of intimate partner sexual violence
Key findings in this section:
- IPSV is an expression of DV.
- IPSV is often limited to emotional coercion, however when it was physically violent, it frequently resulted in injury.
- IPSV is often part of a larger pattern of coercive control in a relationship.
- Women are unlikely to fight back in an IPSV incident.
- IPSV often occurred at regular intervals over a long period of time.
“When you are raped by a stranger you live with a frightening memory.
When you are raped by your husband you live with your rapist.”
Research on the nature of the experience of IPSV demonstrates that it is often limited to emotional coercion but when it is physically violent, it frequently results in injury. The information below is largely limited to more severe forms of IPSV, and does not take into account the large number of sexually coercive incidents that are included in the rates of IPSV examined earlier in this paper.
(Comparable information on the nature of the experience of re-victimisation is extremely limited and thus not included in this paper.)
IPSV is one of many abusive tactics that are characteristic of domestic violence and for some women it is a tactic which is central to the violent dynamic of the relationship (Stack, 2010). Although IPSV is a physical act, many researchers separate it from other forms of physical violence: similarly, such violence (although emotionally abusive) is often conceptualised as distinct from emotional abuse that happens in other contexts.
Given these conceptual structures of the available research, it is therefore meaningful to say that research indicates that IPSV often co-occurs with other forms of physical and emotional violence (Sullivan et al., 2012). For example, in one investigation, almost all (98.2%) men arrested for physically assaulting their partner were sexually violent towards her, with very high rates of combined non-sexual physical violence, psychological abuse, stalking and sexual violence (96.8%) also reported (Basile & Hall, 2011). Similarly, in a study of 157 women who were seeking help for DV, 1.2 percent of women experienced psychological and sexual abuse (but not physical abuse), while no women experienced non-sexual physical abuse and sexual abuse (without emotional abuse): in contrast 35.2 percent experienced combined physical, emotional and sexual abuse (Vatnar & Bjørkly, 2008). This suggests that DV almost always involves a range of abuse methods, that emotional abuse is a common aspect of many violent scenarios, and that IPSV is a less common method of coercive control that may be indicative of more sustained structures of violence.
There is limited research on the temporal patterns of IPSV. Older research indicates that women raped by their partners experience an average of 1.6 rapes per year (Tjaden & Thoennes, 2000). More recent research suggests higher frequency, with one study finding that 40 percent of women in a Spanish cohort experiencing non-sexual physical DV were raped more than two times a month, and another finding that 38.9 percent of Norwegian women who were seeking help for DV having had unwanted sexual relationships with their partner at least once per week (Garcia-Linares et al., 2005; Vatnar & Bjørkly, 2008). When sexual assault and other forms of physical violence co-occur, the assault tends to happen in a repeated pattern of violence (Basile, 2008; Bergen & Bukovec, 2006; Schafran, 2010). For women who used illicit substances and were asked by researchers to keep a diary of their IPV abuse (n = 49), IPSV occurred on 4.1 percent of reporting days, making it the least common form of violence reported (Sullivan et al., 2012).
Violent and brutal sex acts are commonly reported by women who experience IPSV (Stack, 2010). A range of sex acts are reported, with multiple acts, especially sexual activity that includes both anal and vaginal penetration, more common in IPSV incidents than in assaults by strangers (Möller et al., 2012). In a sample of 56 women who had experienced repeated IPSV, the most common combination of sex acts was forced vaginal, oral and anal sex (37%), followed by forced vaginal sex only (23%) (Campbell et al., 2013). Women also frequently report being woken by their partner having sex with them and sex after a violent argument (Logan, Walker & Cole, 2013). There is currently insufficient evidence to determine how the brutality of an IPSV rape affects the impact of the assault on a woman’s wellbeing (Logan et al., 2013). IPSV also involves some specific forms of coercion related to sexuality and/or sexual activity, such as use of sexual degradation, sexual bargaining and threats of harm as a way of pressuring a woman to have sex (Logan et al., 2013).
As IPSV happens in established sexual relationships, the lived experience of sexual consent is complex as there are established patterns of sexual behaviour (Logan & Cole, 2011). Sexual routine, experiences of prior consensual activity and a presumption of continuous consent may create contexts where unwanted sex is agreed to, or where asking for sex to stop is not seen as a possibility (Clark & Quadara, 2010; Lazar, 2010; Schafran, 2010). Moreover, in the context of continual violence, it is arguable that all sex is non-consensual as the capacity for a woman to “freely consent” to sex may be fundamentally compromised (Logan & Cole, 2011; McOrmond-Plummer, 2014). As a participant in an Australian Institute of Family Studies (AIFS) research project said “… [b]ecause I was too terrified of him, that if I didn’t say yes to that, he would rape me. I agreed to it. But it wasn’t really agreeing, because I was agreeing under fear” (Clark & Quadara, 2010, p. 19). Similarly, a lawyer describing a case she represented of a woman who was charged with intentional murder after defending herself from her husband, wrote: “Her husband forced sex on her multiple times, and at a certain point in their marriage, she never had consensual sex with him again. Though she would resist at times, most of the time she was too fearful” (Stack, 2010, p. 540). The context of prior sexual consent, and the likelihood of IPSV being a repeated form of sexual violence, may make IPSV more traumatic than assaults by strangers or acquaintances (Kerr, 2014; Schafran, 2010).
Some research indicates that, when compared to women sexually assaulted by strangers or acquaintances, those who were assaulted by their partner were more likely to be physically injured (but not more likely to experience genital injuries) (Culbertson & Dehle, 2001; Möller et al., 2012). Women who experience IPSV were more likely to be strangled by their partner than women who experience non- sexual physical assault only (n = 432) (Messing et al., 2014). Physical injury may also occur when women are assaulted in response to resisting a sexual advance (McFarlane, 2007; Montoya et al., 2013).
IPSV does not, of course, need to involve physical injury (Kerr, 2014; McOrmond-Plummer, 2014). In addition to the simple materiality of the incident, IPSV may involve physical restraint and other embodied violence. For example, when examining physically forced sex, the use of physical restraint as a form of violence is more common than physical harm or verbal threats (n = 336) (Stermac, Del Bove, Brazeau, & Bainbridge, 2006).
Moreover, there is not a deterministic relationship between the nature of a woman’s resistance to IPSV and the severity of the crime. In a study that examined how women resisted IPSV, the most common mechanism was to remain immobile, followed by defending oneself, trying to escape, and trying to reason with the perpetrator (Garcia-Linares et al., 2005). Given that IPSV may occur in relationships with substantial histories of coercive control and violence, the ability for women to “resist” must always be understood with sensitivity to what types of actions are possible in the context of the violent relationship as a whole. As one women interviewed for an AIFS research project commented: “…usually he probably would just pin me down. He wasn’t violent, he just would hold me down. But if I tried to get away he would increase the pressure in order to keep me there so then it would hurt more” (Clark & Quadara, 2010, p. 36). At a physiological level, it is important to note that women may experience “tonic immobility” (freezing) during violent incidents, thus making resistance impossible – in such contexts, not resisting is symptomatic of the traumatic nature of the incident (Campbell, 2012).
Research indicates that IPSV is a common feature of cases of sustained DV that include aspects of coercive control (Tellis, 2010). Australian qualitative research found that women reporting IPSV described their violent relationships as characterised by reward and punishment exchanges and that their perpetrator relied on established sexual behaviour that normalised violence. This research also indicated that IPSV perpetration, including sexual coercion, was a deliberate and intentional act by perpetrators that should not be minimised or considered merely the consequence of a misunderstanding between partners (Clark & Quadara, 2010).
Finally, threats to kill a partner are more common in relationships that include IPSV than in other abusive relationships (Messing et al., 2014). In a study of 148 women who were seeking help from the justice system, and in comparison to the sub-group of women who were victims of physical violence from their partner, those who experienced IPSV were more likely to also experience a range of behaviours associated with femicide, including their partner threatening to kill them (OR 1.30) and threatening to harm their children (OR 4.56) (McFarlane, Malecha, Gist, et al., 2005). Moreover, IPSV is a risk factor for intimate partner homicide (Campbell, Webster & Glass, 2009; Palmer & Parekh, 2014; Sack, 2010).
Risk factors for re-victimisation and co-occurrence
Key findings in this section:
- The relationship between CSA and adult victimisation is mediated to some extent by the severity of the abuse during childhood.
- The emotional effects of violence may further increase a person’s vulnerability to future victimisation (e.g. through increased emotional dysregulation).
- Drug and alcohol use may be a precursor, consequence or risk factor associated with IPSV and re-victimisation.
- There was mixed evidence regarding the impact of sexual risk taking on the risk of IPSV and re-victimisation.
- The nature of an intimate relationship, including the length of the relationship and the way that partners routinely communicate, has been shown to impact on the expression of violence within the relationship.
Researchers have noted that while the social and political contexts of gendered relations affect the patterns of domestic and sexual violence within a society, individual instances of abuse are also affected by individual and relational characteristics (Goldscheid, 2006). These individual risk factors reflect the failures (and successes) of the systems in which a person is located, so a risk factor may be mitigated by appropriate care and support or exacerbated by the lack of it.
Moreover, it is broadly acknowledged that the aetiology of violence is extremely complex, involving the interactions between individual, inter-personal and societal factors (Krug, Mercy, Dahlberg, & Zwi, 2002; Martin et al., 2009). Such influences are not evenly distributed, with some sub- populations affected by different constellations of risk factors (Cattaneo & Goodman, 2005).
Given the reliance of IPSV and re-victimisation research on retrospective cross-sectional designs and the heavy disciplinary basis towards the psych-sciences and public health, it is particularly important to emphasise that risk factors are not the same as causal factors (Martin et al., 2007). The difference between causal and risk factors was described in a paper regarding sexual assault prevention for women with intellectual disabilities which said “none of these [risk factors], however, are known causes of sexual assault. Rather, women with these factors are more significantly burdened with sexual assault experiences”. This distinction is critical to avoid discussions of risk morphing into discussions of blame (Barger, Wacker, Macy & Parish, 2009, p.251; see also, McOrmond-Plummer, 2014).
Most of the research reviewed in this paper is only able to identify a correlation between particular life events or characteristics and violence. Unless further longitudinal research or research with dose-response findings is completed, causation will remain unclear. The surveyed research is almost all quantitative, with minimal qualitative research on risk factors identified through the search strategy.
Previous victimisation
Below is an outline of some of the factors that may augment the relationship between CSA and adult DV/SXA victimisation. As identified above, care should be taken when considering risk factors, as most research in this field is cross-sectional and thus cannot identify causal relationships between variables. In addition, most available research on re-victimisation has been deemed out of scope from this state of knowledge paper research as it typically examined same-type victimisation from childhood to adulthood (e.g. CSA to adult SXA) (Cuevas, Sabina, & Milloshi, 2012).
Research indicates a moderate to strong relationship between CSA and commonly researched forms of DV (physical, emotional and sexual) (Coid et al., 2001; Daigneault et al., 2009; Macy, 2007; Simmel, Postmus, & Lee, 2012; Whitfield, Anda, Dube, & Felitti, 2003).
The strength of the relationship between CSA and later DV (including IPSV) victimisation may be mediated by the extent of the abuse experienced as a child (Roodman & Clum, 2001). A range of characteristics of CSA are associated with a greater risk of adult DV victimisation, including that the CSA:
- was over a long period of time;
- occurred frequently;
- used force;
- involved penetration; and
- was perpetrated by a known person or guardian.
(Classen et al., 2005; Simmel et al., 2012; Tapia, 2014; Van Bruggen, Runtz, & Kadlec, 2006; Yoshihama & Horrocks, 2010)
Several studies identified a graded relationship between child abuse and DV (Jankowski, Leitenberg, Henning, & Coffey, 2002). For example, a study of 975 college undergraduates found that the frequency of interpersonal trauma as a child was correlated with the number of adult interpersonal victimisations (Pereda & Gallardo-Pujol, 2014).
In international predictive modelling research from the US and Canada, the pathway between childhood and adolescent SXA and adult sexual and DV victimisation is indirect (Fargo, 2009). A range of situational factors may increase the likelihood of a woman experiencing re-victimisation after CSA (Daigneault et al., 2009). These factors include:
- being incarcerated (Wolff, Shi, & Siegel, 2009);
- being poor (Poister, Tusher & Cook, 2010);
- adolescent and adult sexual behaviours including a greater number of partners (Messman-Moore & Long, 2003);
- having a recent victimisation (Classen et al., 2005); and
- experiencing Post-Traumatic Stress Disorder (PTSD) symptoms (Hetzel & McCanne, 2005).
Although research is currently not available, in the Australian context, such patterns may be compounded for certain disadvantaged sub-populations such as Aboriginal and Torres Strait Islander women.
Mediating factors, either in the characteristics of the CSA or the adult victimisation can only partially explain the relationship between CSA and later victimisation, with researchers acknowledging the vast complexity of victimisation experiences and the interdependence of risk factors (Simmel et al., 2012). Moreover, it is important to note that while the experience of abuse in childhood is traumatic, the impact of this may be mediated by appropriate and sensitive systems responses to children in need and the provision of ongoing support to women who have experienced abuse.
Psychological risk factors
(The psychological impact of re-victimisation and IPSV is discussed in detail in Sub-populations with differential patterns of victimisation and Health impacts of re-victimisation and co-occurrence sections of this paper.)
Research into psychological risk factors is almost exclusively based in individualised psychological methodologies. These approaches tend to look at risk without examining the impact of protective or systems responses in mitigating the ongoing impact of psychological risk and is consistent with the disciplinary background of this material. Moreover, such approaches are often focused on statistical trends and tend not to contextualise findings. The mirroring of this disciplinary norm in this paper does not in any way imply a judgement of behaviours or suggest that a woman is to blame for her victimisation.
A range of emotional states have been associated with both IPSV and re-victimisation. These are consistent with findings for other forms of VAW and include:
- externalising behaviours (socially inappropriate anger and other behaviours that are an expression of internal distress);
- poor emotional regulation (experiencing very strong and/or highly variable emotions);
- experiential avoidance (avoiding certain situations or experiences);
- anger;
- hostility; and
- shame.
(Armour & Sleath, 2014; Classen et al., 2005; Gibson & Leitenberg, 2001; Hébert et al., 2008; Messman-Moore, Walsh, & DiLillo, 2010)
Despite the lack of longitudinal research in this area, there is some research indicating that existing emotional volatility may impact on re-victimisation risk (Messman-Moore et al., 2010). Initial research suggests that self-sufficiency and a sense of mastery may protect against sexual re-victimisation (Macy, 2007).
There are several explanations of the mechanism that means that emotional dysregulation may be linked to later victimisation, however research is far from conclusive on whether these are true models (Macy, 2007). Each of these explanations provides a possible mechanism by which external, social and systemic factors may alter a woman’s risk of victimisation:
- For CSA victimisation to DV perpetration: Shame and guilt related to victimisation may predispose perpetrators to hostile responses to their partners and thus increase the risk of violence (Kernsmith, 2006).
- For CSA to DV re-victimisation: Effects of family of origin violence on norms of relationship are one possible explanation, however evidence is sparse (Busbyet al., 2008).
- For sexual re-victimisation, including IPSV: Women may try to regulate their emotional distress through behaviours that may increase their risk of victimisation (e.g. alcohol use, large numbers of sexual partners) (Messman-Moore et al., 2010).
- For gendered violence re-victimisation, including SXA and DV: Emotional dysregulation or trauma may affect a woman’s ability to process information, assess risk and act in a way to ameliorate risk, thereby increasing her susceptibility to victimisation(Messman-Moore, Ward, & Brown, 2009).
Post-Traumatic Stress Disorder (PTSD) is a common consequence of IPSV or re-victimisation. It is, however, also a significant risk factor for re-victimisation and has been shown to mediate the relationship between CSA and adult sexual victimisation (Arata, 2000; Iverson et al., 2011; Messman-Moore, Long, & Siegfried, 2000; Messman-Moore et al., 2009). There is some evidence that the relationship between PTSD and sexual assault may be explained by the symptomology of PTSD, in particular the moderating of distress through the increased use of drugs and alcohol (Messman-Moore et al., 2009). This relationship is less clear in the case of DV (including IPSV), with a small number of studies, including an interview and self-report study of women seeking help for DV, finding that the relationship between PTSD symptoms and childhood abuse was not mediated by DV experience (Gobin et al., 2013).
Relational and behavioural risk factors
Alcohol and other drugs
Consistent with research on VAW as a whole, research indicates that alcohol use may be a precursor, consequence or risk factor associated with IPSV and re-victimisation (Busch-Armendariz, DiNitto, Bell, & Bohman, 2010; Classen et al., 2005; Schewe et al., 2006). Evidence is mixed regarding the extent of the relationships between AOD use and re-victimisation or IPSV, and whether these associations are strong enough to be classed as causal (Macy, 2007).
Women’s patterns of alcohol and other drug use may, or may not, be problematic or addictive in nature. For some women, their use results in stigma and discrimination and may be classed as a criminal act. For these women, the nature of the risk associated with alcohol and other drug use is more complex than for those for whom alcohol use is socially sanctioned and where its impact on IPSV and re-victimisation appears limited to changes in the situational factors of an assault.
Disinhibition as a result of alcohol use is a situational risk factor as it may increase the risk of victimisation due to impaired danger assessment (Lutz-Zois, Phelps, & Reichle, 2011; Messman-Moore et al., 2009; Testa, Hoffman, & Livingston, 2010). There is a small amount of evidence that a history of victimisation (especially CSA) may negatively affect a woman’s capacity to assess situational risk (Fargo, 2009).
Due to its cognitive and physiological effects, alcohol intoxication by both men and women at the time of the incident is a major situational risk factor in dating IPSV, especially in women who already have a history of SXA (Chan, 2011; Filipas & Ullman, 2006; Littleton, 2014; Testa, VanZile-Tamsen, & Livingston, 2007). Australian and Norwegian qualitative evidence suggests that alcohol use is not a major aspect of IPSV in more established/cohabiting relationships (Clark & Quadara, 2010; Vatnar & Bjørkly, 2008). Research has found that men who perpetrate IPSV drink more than men who engaged in no violence, and women who experience rape in their relationships are more than twice as likely to have a substance use issue (Abbey, 2011; Gallagher, Hudepohl, & Parrott, 2010; Lacey, McPherson, Samuel, Powell Sears, & Head, 2013; White et al., 2008). These findings suggest that the overall patterns of substance use, rather than the nature of particular incidents, may put women at risk.
Women may also use alcohol to cope with their experiences of assault. A US study of 577 college women found that women who had experienced both CSA and the SXA as an adult were more likely to use this coping mechanism, although it is unclear what relationship this had to their re-victimisation experience (Filipas & Ullman, 2006).
Much less is known about the relationship between IPSV and illicit substance use, although there is evidence that women who have experienced IPSV or re-victimisation may increase their substance use as a way of helping them to cope with their trauma: such use may, or may not, cause problems for the woman in her day to day life. For example, in a study of 148 women, those who reported more than one IPSV incident were 3.5 times more likely to begin or increase their substance use than women who had experienced one incident only, suggesting a sub-population whose issues should be accommodated in treatment programs and harm minimisation drug and alcohol programs (McFarlane, Malecha, Gist, et al., 2005).
US research indicates that men who were convicted for IPSV were more likely than other sex offenders to use substances before they perpetrate a sex offence (Stalans, Hacker, & Talbot, 2010). This study was examining a population of convicted men, and thus has poor generalisability, with research on whether partner substance use is a risk factor for IPSV still considered equivocal (Hazen & Soriano, 2007).
Sexual behaviour
Certain sexual behaviours are associated with increased risk of re-victimisation and IPSV. Having more sexual partners, starting to have consensual sex at an earlier age, and/ or engaging in more sexual activity has been found to increase the likelihood of adolescent and adult IPSV and sexual re-victimisation (Kim-Godwin, Clements, McCuiston, & Fox, 2009; Macy, 2007; Stockman et al., 2013; Stockman et al., 2010; Young & Furman, 2008). Moreover, there is some evidence that sexual risk-taking mediates the relationship between CSA and adult SXA (Messman-Moore et al., 2009; Orcutt, Cooper, & Garcia, 2005). The implication of the latter findings are difficult to discern and unclear as they may simply indicate that individuals who engage in more sexual behaviours are being exposed to the same amount of risk than those who have less sex. At the same time, this more sexually active group are exposed more often, thus resulting in higher rates of victimisation.
Pregnancy
There is a dearth of research on the IPSV and re-victimisation experiences of pregnant women. The only study identified in this review to examine this population that was identified through the search method found pregnant women were approximately twice as likely to report bidirectional IPSV as IPSV victimisation only (Flanagan et al., 2014). This finding is inconsistent with more general DV and pregnancy research that identifies that pregnancy is a period of particular risk for escalation or initiation of intimate partner violence.
Relationship characteristics
The characteristics of an intimate relationship, such as the length of the relationship and the way that partners routinely communicate, have been shown to impact on the nature of violence within that relationship.
The expression of violence in a relationship is affected by the length of time a couple has been together. Casual sexual partners are likely to experience less endemic coercive sexual control, with men with casual sexual partners reporting the use of sexual coercion primarily in contexts of confusion and poor sexual negotiation skills (e.g. not being sure if their partner wants to have sex or not) (Eaton & Matamala, 2014; Rickert, Wiemann, Vaughan, & White, 2004; Wright, Norton, & Matusek, 2010). Over time, perpetrators of domestic violence tend to use more types of violence, which means that women who have been in abusive relationships of longer duration may be at more risk of co-occurrence of multiple types of violence (Thompson et al., 2006).
Research on whether being married[4] increases the risk of IPSV is mixed. In general, women who have ever been married are more likely to experience IPSV than women who have not been married (Arata & Lindman, 2002). When compared to married couples, research suggests that cohabiting couples are more likely to experience DV, although some studies show no statistically significant effect (Brownridge & Halli, 2001; DeKeseredy & Schwartz, 2008; Miller, 2006). Early marriage is associated with high rates of sexual coercion, possibly due to poor sexual consent negotiation skills (Hattery, 2009; Panuzio & Dilillo, 2010).
Leaving a relationship is a particularly risky time for IPSV, with women who have experienced IPSV frequently reporting incidents during the separation period. A small (n = 43) study of rural women in the US identified that three quarters (74%) were sexually assaulted when they indicated that they were planning to end the relationship (DeKeseredy & Schwartz, 2008). Such assaults may be possessive (an expression of control and ownership), reconciliatory (attempting to get back together through unwanted sex) or retaliatory (punishing a woman for leaving) (DeKeseredy, 2014).
Risk factor grouping
It is important to note that risk factors frequently accumulate in particular lives and communities. For instance, trauma- related responses, such as AOD use, withdrawing from social support and un-safe sexual behaviour, may occur at the same time and compound the effects of each other (Filipas & Ullman, 2006). Behavioural, personal and situational contexts may affect the risk of a person experiencing IPSV or re-victimisation.
Some researchers consider demographic characteristics to be another type of risk factor, with evidence that the risk of severe DV increases with certain demographic factors. In this report, this form of risk factor is addressed in a section on sub-population with differential patterns of victimisation. Some research, however, links more individualised risk factors with these socio-demographic factors, emphasising the complexity of lived experience of violence. For instance, in a study of 1402 randomly selected Spanish women, those who were on social security were 12.3 times more likely to experience emotional and sexual abuse (with or without physical abuse), than those who were not on welfare. Similarly, those who were divorced, separated or widowed were 8.7 times more likely to experience severe abuse than those who were married, and those who had three or more children were 5.4 times more likely to experience severe abuse than those who had no children (Ruiz-Pérez et al., 2006). Overall, the corpus demonstrates an ongoing intersection of disadvantage that complicates (and at time exacerbates) the lived experience of IPSV and re-victimisation.
Sub-populations with differential patterns of victimisation
There is limited research on the characteristics of any types of violence in most sub-populations (such as those in culturally and linguistically diverse communities, sexual minorities and other disadvantaged groups with proportionally small populations), with research on the specific forms of violence such as IPSV and re- victimisation particularly incomplete (Argento et al., 2014; Australian Bureau of Statistics, 2013a, 2013b; Heenan, 2004).
Findings are mixed regarding the extent, and indeed the existence, of a negative effect of minority status on IPSV and re-victimisation. A small number of studies have found equivalent prevalence rates of victimisation in minority groups and broader populations (McFarlane, Malecha, Gist, et al., 2005; Schewe et al., 2006). Most studies, however, find differences in the prevalence, nature and lived experience of violence by women in minority groups. Moreover, scholars note that culture (including the social norms of groups not normally thought of as “cultural”) affects both the meaning and experience of violence (Coker, Sanderson, Cantu, Huerta, & Fadden, 2008).
Research available on the prevalence and experiences of IPSV and re-victimisation in a range of sub-populations is outlined below. This section also acknowledges the behaviours and norms of these groups that may increase the risk of women experiencing IPSV or re-victimisation. The complexity of lived experience and the substantial overlap of populations means that a distinction between patterns of victimisation for IPSV and re-victimisation, or between these types of violence and VAW more generally, is somewhat artificial. While acknowledging this, in order to provide the most focused summary of available research, this section nonetheless focuses on sub-populations in relation to re-victimisation and IPSV as a way of constraining the scope of the review and noting patterns relevant to the specific topic of this paper. It is inevitable that this structuring of information will inadequately acknowledge the intersections of inequality and compounded disadvantage that may be experienced by some women whose lives are represented in multiple groups (Winters & Morgan, 2014).[5]
The sub-populations below have been highlighted in this review as they are communities where the broader social context affects the lived experience of IPSV and re-victimisation: specifically, where existing social disadvantage and distinct embodied life experience may compound and/or alter the prevalence and impact of re-victimisation and IPSV.
Aboriginal and Torres Strait Islander women
Aboriginal and Torres Strait Islander women are disproportionately affected by domestic, sexual and family violence, and family violence is considered an epidemic in these communities. Aboriginal and Torres Strait Islander women are 35 times more likely to be hospitalised as a result of family violence when compared to non-Aboriginal and Torres Strait Islander Australians (Cripps & McGlade, 2008; Productivity Commission, 2009). Violence in Indigenous communities occurs in a complex context of colonisation, dispossession and ongoing racism which makes Indigenous women particularly vulnerable to abuse (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010: Blagg, Bluett-Boyd, & Williams, 2015).
Although IPSV and CSA are acknowledged as a frequent aspect of family violence, primary research on the nature and extent of IPSV and re-victimisation in this population was not identified through this paper, potentially reflecting both the sparse amount of primary quantitative research in this area, and the relative focus of the search strategy on international sources (Adams & Hunter, 2007; Cripps, 2008; Northern Territory. Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse, 2007).
Interviews with Aboriginal women in New South Wales have identified the emotional impact of DV, and especially IPSV, as being similar to those found in the non-Aboriginal community (Heenan, 2004; Moore, 2002). As with the broader community, sexual violence perpetrated against Aboriginal women is often repeated (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010).
Indigenous women in rural or remote communities may be affected by a range of structural and service limitations, similar to those experienced by other women in these areas (Parkinson & Zara, 2014) (see Women who live in rural areas).
Women from cultural and linguistically diverse (CALD) backgrounds
There is significant variation in findings related to rates of domestic and sexual violence in migrant communities.[6] This variation is in part due to the challenge of creating methodologies that can accommodate the diversity of lived experience within and between different migrant communities (Mitchell, 2011; Tapia, 2014). There is very little research on the more narrow topics of IPSV or re-victimisation in migrant communities, with the full extent of the available literature on VAW out of scope for this review.
A range of practical and structural limitations affect the lived experience of violence by immigrants, including:
- Difficulties with English language that may affect help seeking or disclosure (Morash et al., 2007; Sabri, Barcelona de Mendoza, & Campbell, 2014).
- Limited financial independence (this may be due to a range of factors such as migration status, lack of recognition of previous qualification, low-paid employment or cultural or family reasons for not being in the workforce) that may reduce the capacity for women to leave their partners, (Morash et al., 2007).
- Cultural norms that may “emphasise a woman’s submissiveness, placing the needs of family before one’s own, and [where] stigma regarding divorce may present barriers to help-seeking” (Flicker et al., 2011, p. 1069; see also Sabri et al., 2014).
- Dependence on visas associated with their intimate relationship in order to stay in the country (Morash et al., 2007; Taylor & Putt, 2007).
Social disadvantage, including a “lack of support networks, socio-economic disadvantage, community pressure, and lack of knowledge about rights for victims” may increase the risk of SXA and DV, including IPSV (Allimant & Ostapiej- Piatkowski, 2011; Sabri et al., 2014). When women do report IPSV to police, they may have more difficulty than non- CALD women in obtaining protection orders or prosecuting their perpetrators, as a cultural defence may available to the perpetrator that enables them to indicate that they did not have criminal intent (Schafran, 2014). Moreover, some women may be ineligible for certain legal remedies due to their immigration status (Winters & Morgan, 2014).
Culturally specific gender norms may also affect the capacity for women to identify and/or disclose abuse, and may create contexts where traditional gender roles enable abuse (Liles et al., 2012; Morash et al., 2007; Parkinson & Reid, 2014; Rees & Pease, 2007; Sabri et al., 2014; Winters & Morgan, 2014).
There is mixed evidence regarding IPSV rates in immigrant communities, with some studies showing higher rates of IPSV in these populations, while others have found that lifetime sexual coercion rates were lower for women who were born overseas when compared to women of the same ethnic group who were born in the migration country (Cox, 2015; Hazen & Soriano, 2007; Möller et al., 2012).
Caution must be used when examining research regarding domestic and sexual violence in ethnic and migrant communities as conflation of violent behaviour with stereotypical accounts of particular communities may erase the complexity of lived experience and reinscribe racist (and in particular Islamophobic) discourses (Salter, 2014). Although there is some evidence that certain cultural identities may be associated with an increased risk of victimisation, this relationship may reflect broader patterns of disadvantage and risk such as population level differences in socio-economic status, education attainment, neighbourhood poverty or mental health status (Flicker et al., 2011; Palmetto, Davidson, Breitbart, & Rickert, 2013).
Women with disabilities[7]
The Australian peak body, Women with Disabilities Australia, notes that there is currently “inadequate recognition and response to the needs of those women and girls with disabilities who have experienced or are at risk of experiencing violence” (2013, p. 17).
Research on SXA, especially IPSV, experienced by women with physical disabilities is very limited (Plummer & Findley, 2012). In one of the few available studies, in comparison to women without disabilities, US women with severe physical disabilities were four times more likely to experience sexual assault (n= 6273) (Casteel, Martin, Smith, Gurka, & Kupper, 2008). A slightly larger (n= 7027) Canadian study of women with and without disabilities found that IPSV involving sexual assault was experienced by three times as many women with a disability (0.6% vs 0.2%) (Brownridge, 2006).
Women with physical disabilities are particularly vulnerable to assault by carers, with a US study of 84 women with physical disabilities finding that three percent had experienced sexual abuse by their primary personal assistant and eight percent had experienced abuse by another physical assistant (Oktay & Tompkins, 2004). Where women are dependent on a carer for assistance, including in key areas such as transportation or communication, accessing support or leaving a violent relationship may become particularly difficult (Davis, 2014; Plummer & Findley, 2012).
No studies were identified in this paper that examined the specific lived experience of IPSV or re-victimisation of women with intellectual disabilities. Research with professionals who work with people with an intellectual disability identify that this group is particularly vulnerable to sexual assault and assault within their domestic environment. Women with intellectual disabilities are also more likely to be part of other high-risk sub-populations such as women with low socio-economic status and women who experience severe mental illness (Barger et al., 2009; Hickson, Khemka, Golden & Chatzistyli, 2013). Women with intellectual disabilities are also “often socialised to be compliant […] and remain substantially more dependent on caregivers than nondisabled women” (Barger et al., 2009, p. 251).
As with some other sub-populations who experience multiple forms of disadvantage, Aboriginal and Torres Strait Islander women with disabilities find locating culturally appropriate and accessible services particularly difficult. As noted by a participant in Australian qualitative research on violence against Aboriginal women with disability: “people are just ignorant, and think that the disability [our] women have is being black and that their … disability isn’t even seen” (Cripps, Miller & Saxton-Barney, 2010). This quote highlights the challenges in making visible the experiences of women who are part of multiple highly disadvantaged sub-populations.
Research on IPSV for both women with disabilities and women with a mental illness is extremely limited, a pattern that may reflect societal norms that de-sexualise these two groups.
Young women
“…we began kissing, which I enjoyed but suddenly his hand was in my pants and I was extremely uncomfortable. He began fingering me and it was painful. [Afterwards] I was ashamed (we were in our school) and nervous someone would see us and think I was a slut.”
– Young woman aged 14 at the time
Adolescent women frequently experience dating sexual violence; over ten percent of young women having experienced forced sexual intercourse (Kim-Godwin et al., 2009). Within the adolescent cohort, rates of IPSV increase with age, with individuals who are over 18 more likely to experience IPSV (Kim-Godwin et al., 2009). This increase in victimisation is likely to reflect a larger proportion of women having become sexually active and the reduction in structural limitations to intimacy (e.g. having a licence, being permitted to be unsupervised in a bedroom etc.) (Noonan & Charles, 2009).
International research indicates that early adulthood (18-24 years) is a period of heightened risk of both rape and DV. In a US national representative sample (n = 9086), 37 percent of women who had been raped reported that their first incident occurred during this period. The same survey found that 47 percent of women who experienced DV reported that their first incident occurred at this age (Black et al., 2011). Some research also suggests that the early 30s are a period of heightened risk, particularly for IPSV perpetrated by cohabiting partners (Heenan, 2004). Research in Australia is more mixed, with findings from the 2012 PSS showing an increased risk of sexual assault for the 18-24 years age group, but the highest rate of partner violence occurring a little later (25-34 years) (Cox, 2015).
When examining women who have been assaulted more than once, a general population survey completed by female residents of Washington State found that those who were younger were more likely to have been assaulted by multiple perpetrators, while those who were older were more likely to experience violence by the same perpetrator (Casey & Nurius, 2005).
Women who are HIV positive
HIV and IPSV have been characterised as intersecting epidemics (Campbell et al., 2013; Stockman et al., 2013; Stockman et al., 2010; Tufts, Clements, & Wessell, 2010). Being forced to engage in behaviours that puts one at risk of HIV transmission is defined as a type of IPSV. In a meta- analysis of seven studies from the US that looked at IPSV and HIV risk behaviours (e.g. inconsistent condom use, having a HIV+ partner, having other STIs), six of the studies found a positive relationship between the two factors. Despite this, the paper identified no multivariate analysis that showed a statistically significant relationship between HIV infection/ risk behaviours and IPSV (Stockman et al., 2013).
For women with HIV or who have HIV+ partners, the impact of IPSV on their capacity to negotiate condom use may have significant health implications (Chamberlain & Levenson, 2012; Campbell et al., 2008; Macleod, 2014a).
As there are significantly fewer HIV+ women than men in Australia, HIV+ women may have difficulty finding health and support services that are sensitive to their needs (The Kirby Institute, 2015). Moreover, HIV+ women may face increased discrimination from service providers and the community in general due to the stigmatising context, or presumed context, of their seroconversion (e.g. injecting drug use or unsafe sex) (Lawless, Kippax & Crawford, 1996).
Women with low socio-economic status
Being unemployed and/or living in a low-income household are associated with higher rates of IPSV (Schumacher, Feldbau-Kohn, Slep, & Heyman, 2001; Vatnar & Bjørkly, 2008). In a prospective study of women who reported their violence to police, women who were unemployed were more likely than employed women to experience ongoing violence that included “physical aggression, sexual coercion or bodily injury” (Babcock & Deprince, 2013, p. 1396). In a random sample of Spanish women (n=1402), low income (OR 2.55) and poor social support (OR 12.28) were found to be associated with a combined intimate partner violence profile that included both emotional and sexual abuse (and may have involved physical abuse) (Ruiz-Pérez et al., 2006).
In a study that found a correlation between sexual or emotional abuse as a child and adult DV victimisation, low education attainment was the strongest predictive factor for adult DV victimisation (OR = 3.79, n= 637) (Seedat et al., 2005).
The financial and practical constraints of living in poverty, combined with the stigma and discrimination that may be experienced due to low socio-economic status, may reduce a woman’s capacity to seek support and/or leave a violent relationship (Cortis & Bullen, 2015).
Women who live in rural areas
“Where do you go? Your family doctor […] could be his best mate”
– Amanda
Rural communities have a number of characteristics that may increase women’s vulnerability to all forms of violence. These factors include:
- limited DV and/or SXA services;
- normalisation of violence; and
- the “tyranny of distance” that may increase the practical challenges of leaving a violent situation.
(DeKeseredy & Schwartz, 2008)
Some rural communities may be both close-knit and conservative, thus potentially perpetuating a culture that accepts IPSV (Parkinson & Zara, 2014). An interview study in the US (n=43) found that sexual assault in the context of relationship breakdown was routinely ignored for the “common good” of the community (DeKeseredy & Schwartz, 2008). More recent research indicates that IPSV in the context of separation is particularly common in these contexts (DeKeseredy, 2014; Rennison, DeKeseredy, & Dragiewicz, 2012). Moreover, there is some indication that the social isolation of gay and lesbian couples in socially conservative rural and remote contexts may negatively impact the capacity for IPSV survivors to access help and support (Ristock, 2014).
Rural communities may have higher rates of IPSV than urban communities: in Kentucky (n=213) 31 percent of women with protective orders reported being raped by their partner, that number rose to 36.8 percent when looking at women in rural areas (Logan, 2009). While research on rural communities is sparse, these initial studies suggest that women in these communities may be at higher risk of violence and may experience more negative impacts of that violence.
Women who are, or who have been, incarcerated
Women who have been incarcerated are a highly disadvantaged group who frequently have an extended history of contact with police. In the Australian context, Aboriginal and Torres Strait Islander women are disproportionately represented in prisons, and women prisoners have very high rates of drug dependence, mental illness and learning disability (Kilroy, 2014). For the US-based research described below, African America and Latina women are disproportionately represented. Researchers understand these racialised variations as reflective of the increased surveillance of particular populations, as well as interpreting them as a material impact of systemic racism (Baldry & Cunneen, 2014).
Incarcerated women have a higher rate of re-victimisation than poor urban women who have not been in prison, with statistical analysis also showing a stronger relationship between childhood and adult victimisation for incarcerated women (n=359) (Poister, Tusher & Cook, 2010).
A study of 50 NSW Aboriginal and Torres Strait Islander women prisoners found particularly high rates of CSA (over 75%) and adult SXA (approximately 50%) (Lawrie, 2003).
Women who have experienced CSA are twice as likely to be sexually victimised in prison when compared to women with no CSA history (Wolff, Blitz, Shi, Bachman, & Siegel, 2006; see also, Kilroy, 2014).
Even when they are out of prison, women who have been incarcerated have a higher rate of re-victimisation. Women who have been incarcerated (n = 484) and who had experienced IPSV were 3.1 times more likely to be assaulted by a friend and 2.4 times more likely to be sexually assaulted when they were a child (Raj et al., 2008). Unlike non-incarcerated women, incarcerated women report a greater proportion of adult sexual assaults by a stranger (12%) than by their partner (10%) (Raj et al., 2008).
Women who have been incarcerated face significant discrimination when they return to their communities. Difficulties in obtaining employment and accessing social services may impact on their ability to leave violent relationships, as well as their quality of life more generally (Decker, Spohn, Ortiz & Hedberg, 2014; Johnson, 2014).
Women who experience severe mental illness
Severe mental illness is associated with particularly high rates of CSA and SXA in adulthood (Meade et al., 2009; Shevlin et al., 2013).
Individuals who have histories of severe mental illness are particularly vulnerable to re-victimisation. This may be due to a range of factors including:
- the effects of psychosis, severe mental disturbance and the medications used to treat these states on perception of risk and danger;
- an inability to escape abuse when it happens in involuntary hospitalisation contexts; and
- reduced financial and social resources that in turn impact on the ability of women to escape violent relationships or contexts.
(Quadara, Stathopoulos, & Jenkinson, 2015)
Due to the lack of longitudinal research, there is limited understandings of the “direction” or exact nature of the link between mental illness and re-victimisation, however a bidirectional relationship where victimisation results in mental illness which in turn increases the risk of further victimisation is discussed in the clinical literature (Quadara, Stathopoulos, & Jenkinson, 2015).
A multivariate analysis of a representative sample of Australian women (n=4451) found that those that had experienced three or four types of gender-based violence (DV, stalking, sexual assault or rape) had a lifetime experience of clinically defined mental disorder that was 11 times greater than that of women who had no gender-based violence victimisation. Women with this high level of re-victimisation were also:
- ten times more likely to experience an anxiety disorder;
- sixteen times more likely to experience PTSD; and
- fifteen times more likely to attempt suicide. (Rees et al., 2011)
As this was a cross-sectional analysis, no inferences regarding the causal links between re-victimisation and mental health could be drawn.
There is substantial evidence that having a mental illness, and in particular psychotic illness, is a highly stigmatised identity (Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000; Watson, Corrigan, & Kosyluk, 2014). Women who are symptomatic may struggle to access services to assist them while simultaneously being in acute need of support. The long term effects of the social isolation that is often characteristic of severe mental illness may also result in women experiencing more severe impacts of violence.
(See also Risk factors for re-victimisation and co-occurrence, and Health impacts of re-victimisation and co-occurrence.)
Women who identify as lesbian, bisexual and/or queer
DV and IPSV in same-sex relationships may have different characteristics than DV in heterosexual relationships, in part due to the capacity for the threat of “outing” to be used as a tactic of coercive control (Freedner, Freed, Yang, & Austin, 2002; Potter, Fountain, & Stapleton, 2012). Research on DV in women’s same-sex relationships shows large variation in prevalence estimates, with available studies showing both significantly higher and significantly lower rates of victimisation than heterosexual women (Stoddard et al., 2009).
In an analysis of administrative data from GLBTIQ (gay, lesbian, bisexual, transgender, intersex and queer) anti- violence projects in the US, in comparison to other GLBTIQ intimate partner violence survivors, bisexual men and women were 1.6 times more likely to experience IPSV (from a male or female partner). The most common perpetrator of child or adult sexual assault of a lesbian is a man (Stoddard et al., 2009).
Women in same-sex relationships report significant concerns about experiencing prejudice and distress when seeking assistance related to DV (National Coalition of Anti-violence Programs, 2014). Lesbian women have less access to services than their heterosexual counterparts, potentially due to the limiting of some services to women who have children (of which, at a population level, lesbian women are less represented) and the provision of some services by religious groups that may not be, or may not be perceived to be, supportive of same-sex attracted women (Potter et al., 2012).
Large-scale and/or general population research on re-victimisation and IPSV rarely engages with women in same-sex relationships. This appears to be a methodological necessity, as even in a representative sample of 16,000 people, only 30 violent incidents involving same-sex partners were identified, thus making analysis statistically invalid (Messinger, 2011). Similarly, most of the ABS PSS data is unable to be reported for violence in same-sex relationships as the sample is too small to produce reliable estimates (Cox, 2015). In addition, and in keeping with gender norms which position women as incapable of rape, women may struggle to identify their experiences of same-sex IPSV as being a form of violence (Ristock, 2014).
Ongoing shifts in community attitudes towards people in same-sex relationships means that the levels of stigma and discrimination experienced by this sub-population may be reducing in relation to experiences by other sexual and gender minorities.
Transgender women and men
(Both transgender women and men are included in this paper as trans men may have experienced violence at a time when they presented as female and/or may have experienced gendered violence in a context where they were read by others as female.)
Transgender women and men experience high rates of violence in their lives, including SXA, DV and street based violence (Stotzer, 2009).
Transphobia has a significant impact on transgender survivors, with the lived experience of ongoing discrimination and prejudice and resultant distress likely to further compound the distress associated with victimisation. In a report on the experiences of IPV in the GLBTIQ communities in the US, the researchers noted that:
“In 2013 transgender survivors were more likely to experience physical violence and discrimination within IPV as well as police violence after incidents of intimate partner violence. Transphobia remains a formidable and dangerous reality for both the public and private lives of transgender individuals, creating barriers for access to essential services from anti-violence programs, law enforcement agencies, advocates, and medical professionals. Transphobia can also be a tactic of abuse that an abuser can use against a transgender partner. The barriers to accessing essential services for addressing violence in an intimate partner relationship have dangerous and sometimes deadly consequences for transgender survivors of IPV.” (National Coalition of Anti-violence Programs, 2014)
Trans individuals face a higher rate of IPSV than other groups in the GLBTIQ community, with 50 percent reporting having been raped by a partner (National Coalition of Anti-violence Programs, 2014).
Women who work in the sex industry
There is very little research regarding IPSV and re-victimisation of sex workers, however relationship patterns, including the potential to be in a relationship with an intimate partner who controls one’s work, may affect the patterns of victimisation in this population.
In a Canadian longitudinal study of 387 female sex workers with male partners, 26.2 percent had experienced physical and/or sexual abuse by their partner in the last 2 years. Of these women who had experienced abuse, 84.3 percent had experienced physical and/or sexual abuse as a child (Argento et al., 2014).
Sex workers have a higher risk of being sexually assaulted at work than other professionals. Much of this victimisation involves multiple criminal acts, including the combination of assault and theft (including not paying for a service). Street based sex workers are particularly vulnerable to this form of multiple victimisation (Jason, Hubbard, & Birch, 2013). Research in Queensland suggests that re-victimisation of sex workers is disproportionately distributed, with women in legal brothels least likely to be physically or sexually assaulted and women in street based sex work most likely to experience assault (Woodward, Fischer, Najman, & Dunne, 2004).
Women who experience sexual violence when engaging in sex work in criminalised jurisdictions have extremely limited access to the legal justice system because engagement with the police would require disclosure of illegal activity. Moreover, women who work in the sex industry may experience sustained discrimination from the community at large and service providers in particular, with stereotypes regarding the nature of sex work particularly destructive for women seeking help and support for work-based sexual assaults. As an example of the formalised discrimination against sex workers, the jail sentence given in relation to a victim of sexual assault who is identified as being a prostitute may be reduced as the judge is allowed to determine that the elements of “shame” and “defilement” may be “missing or diminished” (Clark, 2007, p. 21).
Debate on whether there is an association between prior victimisation and sex work victimisation remains unresolved in the literature and is an area of highly charged debate (Jason et al., 2013).
Sub-populations of interest with limited existing research
In the process of this review, a range of sub-populations were identified as likely to experience differential patterns of victimisation but for whom there was no or minimal dedicated research findings. Of particular interest were the following:
- Women who are homeless. Homelessness may create circumstances where women are particularly vulnerable to sexual violence, including contexts where they may feel obligated to have sex with a person who provides them with shelter (Christopher & Pflieger, 2007).
- Women who are polyamorous. Experiences of violence by women who have multiple partners are likely to be under-reported in the research literature as relationship structures (e.g. not cohabiting with all partners) may mean that certain relationships would be excluded from analysis.
- Women within the kink and BDSM communities. The dynamics and conceptualisations of IPSV in this community are likely to be distinct and may alter the lived experience and impact of re-victimisation and IPSV (for a brief discussion of this issue, see, McOrmond-Plummer, 2014; Ristock, 2014).
- Women who have intersex characteristics. There is no data available on this group within the GLBTIQ community.
Conclusion
A wide range of demographic factors have been shown to be associated with an increased risk of IPSV and re-victimisation. As with the risk factors described above, some of these factors may group together, with women who are identified in one sub-population category (e.g. having been incarcerated) more likely to be in others (e.g. having worked in the sex industry or used drugs and alcohol). The intersections between different demographic characteristics create distinct patterns of lived experience which need to be accounted for in public policy and service delivery.
Male repeat perpetrators of sexual assault and domestic violence: Repeat offenders
In this section:
- Most men who perpetrate sexual assault had not experienced CSA.
- Alcohol abuse problems, frequent and normalised engagement with pornography and a history of sexual coercion were associated with IPSV perpetration in a current relationship.
- Conservative gender norms were a contributing factor to perpetration.
Most of the research outlined in this paper has described the prevalence and victimisation patterns of IPSV and re-victimisation as they relate to women victims. This section describes research identified through the search strategy that examines male perpetrators who: engage in multiple types of perpetration; perpetrate violence against more than one woman; or perpetrate IPSV. While acknowledging that the perpetration of any man may contribute to a woman’s experience of re-victimisation, in order to keep within the scope of this review, this short examination of perpetrators is limited to repeat offenders.
The literature on perpetrators is distinct from that on victims as it has a different disciplinary focus, meaning the literature outlined below is a very partial picture of available research.
Recidivism refers to a return to perpetration after treatment and/or incarceration. Recidivists are a key sub-population of the broader group of people engaged in contexts of IPSV and re-victimisation, as these men may perpetrate multiple types of violence against a single woman and/or perpetrate violence against a range of women.
Much of the work on recidivism uses actuarial models to try to identify which men are more likely to re-offend. In an analysis used to develop an integrated theory of sexual recidivism, Jo Thakker (2012) notes several key risk factors for recidivism:
- general lack of sociality;
- sexual arousal associated with perpetration;
- attitudes and beliefs that are supportive of offending;
- difficulties with intimacy; and
- poor self-regulation.
In a meta-analysis of 20 longitudinal studies that examined risk and protective factors for perpetration of dating violence in adolescence, 53 risk factors were identified including the perpetrator’s mental health issues, aggressive thoughts, prior dating violence and the use of aggressive media (Vagi et al., 2012). Such research highlights the range of individualised risk factors that may influence repeated use of violence. Although such research indicates the existence of factors that increase the risk of perpetration it is important to emphasise that regardless of the contexts of their behaviour, perpetrators are responsible for their use of violence (McOrmond-Plummer, 2014).
Perpetrators of sexual assault may have been victims of abuse when they were children. In the limited number of cases where men then go on to perpetrate violence, the life-course of the perpetrator shows an alternative type of re-victimisation that crosses the victim-perpetrator division. Child sexual abuse has been associated with both adolescent sexual perpetration and adult sexual assault perpetration, however the extent of the relationship is still being examined (Reckwald, Mancini & Beauregard, 2013; Mathes, 2013). Although adolescent sexual perpetrators are more likely than other young men to have experienced CSA, the relationship is insufficient to be called a “risk factor” (and may be better described as a “risk marker”) (Mallie, Viljoen, Mordell, Spice, & Roesch, 2011, p. 412). Most CSA survivors do not perpetrate sexual assault, with more than 90 percent of adolescent sexual offenders not having experienced CSA (Nisbet, Wilson & Smallbone, 2004).
With regards to perpetrators of IPSV, there is little distinction in the backgrounds of men who are physically or sexually aggressive in their intimate relationships, with men who perpetrate both forms of violence frequently from family environments that were chaotic (White et al., 2008). In addition, a range of behaviours may co-occur and enable IPSV:
- Alcohol abuse problems are more common in men who sexually and physically abuse their female partners than in men who do not (White et al., 2008).
- Frequent and normalised engagement with pornography may provide a context of perceived constant sexual access (Clark & Quadara, 2010).
- Sexual coercion in a previous relationship is predictive of the same type of coercion in a current relationship (Brousseau et al., 2012; Vatnar & Bjorkly, 2008).
A perpetrator’s beliefs also affect their perpetration, with conservative gender norms being a contributing factor identified in a range of studies. For example, a study of 59 urban fathers showed that hypermasculinity was associated with IPSV and other forms of DV and child maltreatment (Guerrero, 2009), with hostility towards women also predictive of sexual recidivism (Stanlans et al., 2010).
Repeat perpetration is a complex area of research that is not able to be fully described in this paper.
Community and professional attitudes towards re-victimisation and co-occurrence
Key findings in this section:
- Normative understandings of “real rape” affect how people interpret narratives of sexual assault. They particularly affect interpretations of IPSV incidents.
- Heteronormative beliefs are associated with acceptance and experience of verbal sexual coercion for both men and women.
- Understandings of consent in established relationships affect how instances of IPSV were framed by victims and third parties.
“I remember my husband making me have sex with him one time when people were in the next room and none of them guys would come in and help me. And they knew he was hitting me, but they figured that he was my husband. If it were a stranger it would have been different”
– Grace, Rural Ohio
Attitudes, understandings and cultural framing affects an individual’s experience and conception of sexual assault and domestic violence (Addington & Rennison, 2008; Murphy, 2011). Social norms regarding sexuality, and sex within relationships in particular, may increase the negative impact of IPSV and/or re-victimisation on the wellbeing of the women who experience these forms of violence, with lack of community understanding being characterised as “one of the most injurious aspects of IPSV” (McOrmond-Plummer, 2014, p. 33).
Social paradigms affect what behaviours are understood as rape, including normative understandings of what constitutes “real rape” (i.e. the belief that a rape is more “real” if it is a physically violent assault by a stranger) (Addington & Rennison, 2008; Davis, 2014; Easteal, 2014; Kerr, 2014; Logan et al., 2013; McLean & Goodman-Delahunty, 2008; Raphael & Logan, 2009). “Real rapes” are also meant to create “real victims” – women who “scream during their rape […] forcibly resist their attackers […] report their rapes immediately […] remain vigilant following their attacks and […] avoid their assailants” (Long, 2009, p. 23). Many IPSV and re-victimisation survivors do not fit these stereotypes. Research has found that IPSV was consistently viewed by the community as both less serious and more justifiable than SXA committed by a stranger and acquaintance (Christopher & Pflieger, 2007).
For a range of populations, including victims and police officers, the likelihood that an incident of IPSV is considered a lie, or a “miscommunication” rather than an assault, increases with greater familiarity between the victim and the perpetrator (McLean & Goodman-Delahunty, 2008; Orchowski et al., 2013). In a study of 173 women who had experienced intimate partner violence, reactions of friends and family to disclosures of IPSV were generally negative, although this relationship was not as strong when there was evidence of positive coping strategies (Sullivan, Schroeder, Dudley, & Dixon, 2010).
Beliefs about sexuality and relationship norms also affect the risk of (re)victimisation (Niehaus, Jackson, & Davies, 2010). For both men and women, support of heteronormative beliefs is associated with acceptance and experience of being verbally pressured to have sex (Eaton & Matamala, 2014). Moreover, understandings of consent are complicated by a range of gendered and relational norms which may alter a person’s understanding or lived experience of IPSV (Martin et al., 2007; Spohn & Tellis, 2012; Wall, 2012). In both lived experience and court contexts, distinguishing between “wifely acquiescence” and rape can be difficult “precisely because coercion, pressure, aggression and ‘seduction’ remain culturally acceptable expressions of male [sexuality]” (Heenan, 2004, p. 9). Social scripts of heterosexuality normalise IPSV as part of accepted masculinity or as a standard characteristic of seduction, with these scripts apparent in the attitudes and behaviours of a range of populations including Australian young people (Flood & Kendrick, 2012; Noonan & Charles, 2009). Younger women rarely identify sexually coercive behaviours by boyfriends as sexual assault, and justify this violence through explanations that indicate that their own behaviour justified the assault or which emphasise some kind of extenuating circumstances (Christopher & Pflieger, 2007; Lloyd & Emery, 1999). Moreover, in instances where study participants looked at a hypothetical IPSV rape scenario, even participants who identified the event as rape tended not to believe that the “act was a violation of the wife’s rights” (Ferro, Cermele & Saltzman, 2008, p. 773).
Although legal understandings of consent in established relationships have altered significantly in the last 30 years, they remain imperfect and reflective of broader social understandings of the nature of sexual assault (Easteal, 2014). Until the 1980s, the concept of marital rape was not legally valid in Australia (Feerick & Easteal, 2005; Larcombe & Heath, 2012). Modern legal definitions of consent centre on establishing that the perpetrator was aware that the victim did not consent or that the perpetrator had wilful disregard for her consent (Feerick & Easteal, 2005). Despite this progress, the relationship between offender and victim remains a legitimate cause for reducing the jail sentence for sexual assault (Clark, 2007, p. 20). IPSV offences are difficult to prosecute, in large part because they typically happen in the context of consensual sexual relations before and after the assault, as well as patterns of sexual activity that are established and do not include verbalised consent (Easteal, 2014; Heenan, 2004; Logan et al., 2013; Martin et al., 2007). There is an ongoing need for feminist legal scholars to assert that women consent to specific acts of sex and not to sex in general with a particular person (or a particular class of person) – this advocacy is central to positioning IPSV as a criminal act that cannot be justified by the context of the assault (Ellison, 2010; McGlynn, 2010).
Attitudes towards violence construct the lived experience of violence, constraining a woman’s own emotional response to violence, her understanding of appropriate gendered behaviour and her ability to access legal responses.
Health impacts of re-victimisation and co-occurrence
Key findings in this section:
- The mental health impacts of re-victimisation and IPSV range from clinically significant symptoms (such as self-blame and shame) to severe mental illness (such as psychosis).
- The physical health impacts of re-victimisation and IPSV often continue after the abuse has stopped and include a range of injury and stress related conditions. Sexual health was particularly negatively impacted by IPSV.
The effect of violence varies between individuals, with women who have the same types of violence experiencing differing levels of ongoing impact and trauma. In addition, the characteristics of the violence, including its “severity, frequency, meaning and intention”, affect its impact on the victim (Hegarty & Roberts, 1998, p. 53). Like risk factors such as alcohol use and self-harm, many health impacts may be understood as being responses and manifestations of trauma (Kerr, 2014).
Below, we outline findings on the mental and physical health impacts of re-victimisation and IPSV.
In research which distinguishes between IPSV and other forms of physical violence, it has been found that IPSV, both by itself and in contexts where separate instances of non-sexual physical violence occur, has a greater burden of disease than physical DV only (Bonomi, Anderson, Rivara, & Thompson, 2007; Monson & Langhinrichsen-Rohling, 1999). These findings are based in medical, epidemiological and public health research which, while concerned with patterns of health and illness, does not readily engage with the broader social context of violence. Despite wanting to acknowledge the social dimensions of the effects of violence, in order to keep aligned with the methodology and epistemology of the studies examined, this section is aligned with a medicalised approach to the impacts of violence.
Mental health impacts
Clinically significant symptoms
Common clinically significant emotional difficulties and distress are a normal and expected response to trauma (Kerr, 2014; Palmer & Parekh, 2014). The following experiences are common in both IPSV and re-victimised populations:
- self-blame;
- guilt;
- low self-esteem; and
- shame.
(Johnson, 2005; Kelly & Stermac, 2012)
The cultural and personal meanings associated with IPSV result in women reporting intense feelings of shame – women who experience IPSV report more shame when compared to women who experience stranger rape; IPSV victims also experience more shame compared to women who experience DV that involves physical assault only (Messing et al., 2014; Palmer & Parekh, 2014; Temple, Weston, Rodriguez, & Marshall, 2007; Wall, 2012).
Shame may also impact on re-victimisation rates, with women who experience CSA more likely to be sexually re- victimised as adults if they experience more self-blame about their original abuse (OR = 1.7) (Tapia, 2014).
In comparison to women who experience non-sexual physical DV only, women who experience IPSV are more likely to experience clinically significant distress (n = 449) (Spiller et al., 2012). Moreover, children of women who experience IPSV are more likely to display disruptive behaviours than children whose mother has experienced physical abuse only (Kitzmann, Gaylord, Holt, & Kenny, 2003; Spiller et al., 2012).
The impact of clinically significant distress may be mitigated by appropriate health care responses. For instance, professionals engaging in victim-blaming may increase distress, as described by an interviewee in a UK qualitative study:
“I was also told by a psychiatrist that I should have fought harder, yelled louder, etc. Because I was blamed by two doctors who are suppose [sic] to help me – I began to blame myself and question maybe they are right. I still have difficulty overcoming this blame.”
Affective disorders
Consistent with other forms of VAW, the mental health effects of IPSV and re-victimisation are significant and may extend significantly beyond the period of trauma. These effects most commonly include:
- Depression.
- Anxiety.
- PTSD.
(Basile, Arias, Desai, & Thompson, 2004; Krebs et al., 2011; Ludermir et al., 2008)
In a Brazilian study, women who experienced IPSV were 3.88 times more likely to experience clinically diagnosable mental disorders (including, but not limited to, depression and anxiety) than women who had no DV victimisation. For women who experienced physical, sexual and emotional abuse, the odds ratio was 6.39 (Ludermir et al., 2008).
In comparison to women who were physically but not sexually abused by their partner, women who had experienced IPSV were more likely to experience depression, with one study showing a 61 percent increase in severe depression symptomology (Bonomi et al., 2007; Pico-Alfonso et al., 2006). Similarly, regression analysis of data from women who had experienced IPSV (n=57) showed that a history of childhood physical or sexual abuse and severity of IPSV independently contributed to depression, with these findings also mirrored in other studies (Koopman et al., 2007; Miller, 2006).
Women who had experienced IPSV reported a rate of suicide attempt and threat that was 5.3 times higher than women who had experienced solely physical abuse by an intimate partner (n=148) (McFarlane, Malecha, Gist, et al., 2005).
Re-victimisation compounds the psychological effect of previous trauma, with lifetime and current PTSD and depression more severe in this population (Casey & Nurius, 2005; Messman-Moore et al., 2010).
The experience of sexual assault by an intimate partner appears to be particularly traumatic, with women reporting more PTSD symptoms if they experience IPSV than if they experience non-sexual physical assault only (McFarlane, Malecha, Watson, et al., 2005; Messing et al., 2014). Women who experience IPSV in the form of sexual coercion report trauma symptomologies similar to adult rape survivors (Broach & Petretic, 2006). Even in cases where there was high severity of other forms of intimate partner violence, the presence of IPSV increased the severity, and was predictive of, PTSD symptoms, (Bennice, Resick, Mechanic, & Astin, 2003; Dutton, Kaltman, Goodman, Weinfurt, & Vankos, 2005; Sullivan et al., 2012).
Psychosis
A class analysis of victimisation patterns and psychosis found that women who experienced multiple victimisations across the life course were 6.43 times more likely to experience paranoia and 12.36 times more likely to experience auditory hallucinations than women with no abuse history (Shevlin et al., 2013). In addition, CSA victimisation, which is a common aspect of a re-victimisation life-course, is predictive of psychosis (Bebbington et al., 2011; Shevlin et al., 2013).
Given the significant mental health problems experienced by women who are exposed to IPSV, it is noteworthy that some research has found that, of women who were in abusive relationships, access to mental health services was less common or at best at equivalent levels, for IPSV survivors (Próspero & Vohra-Gupta, 2008).
(See also Sub-populations with differential patterns of victimisation.)
Both re-victimisation and IPSV are associated with many mental health conditions, including clinically significant distress, affective disorders and psychosis.
Physical health
General health
The physical health effects of IPSV and re-victimisation are significant, with long-term physical health consequences often continuing after the abuse has stopped (Andersen et al., 2014; Bonomi et al., 2007; Parekh & Williams, 2014).
Physical health conditions that have been shown to be associated with IPSV and/or re-victimisation include:
- urinary tract conditions;
- gastrointestinal disorders;
- headache;
- seizures;
- hypertension; and
- asthma.
(Campbell et al., 2002; Chiu et al., 2013; Sullivan et al., 2012)
Both IPSV and re-victimisation have complex impacts on the sympathetic and para-sympathetic nervous system (Patriquin, Wilson, Kelleher, & Scarpa, 2012). More specifically, there is some evidence that sexual re-victimisation affects cortisol levels and may in turn reduce the reactivity of the parasympathetic and sympathetic nervous systems (Friedman, Jalowiec, McHugo, Wang, & McDonagh, 2007; Miller, Chen, & Zhou, 2007).
Sexual health
In comparison to the research on general health effects, there is substantially more evidence of the negative sexual health consequences of IPSV. There is also an emerging body of evidence regarding the effects of re-victimisation on sexual health.
In an interview study of women who had experienced IPSV (n = 148), 20 percent identified that they had experienced a rape related pregnancy and 15 percent had attributed at least one sexual transmissible infection (STI) to IPSV. Of those women who experienced IPSV more than once, 1 in 5 (20%) had experienced bleeding from the vagina, with the same percentage experiencing bleeding from the rectum (McFarlane, Malecha, Watson, et al., 2005).
In a multinominal analysis of data from 432 women who had called the police due to an intimate partner assault, women who had experienced forced sex were 3.4 times as likely to experience miscarriage when compared to women who had not experienced IPSV. Within this sample, women who experienced forced sex were also 1.3 times more likely to experience PTSD (Messing et al., 2014).
Women who experience IPSV may have more difficulty negotiating condom use, with a study of women who use drugs finding that those who experienced IPSV were 3.3 times more likely to use condoms inconsistently (Palmer & Parekh, 2014; Panchanadeswaran et al., 2010). IPSV in dating relationships may increase the risk of STI transmission and pregnancy through increases in unprotected sex in non-fluid bonded relationships (Herman, 2009).
Sexual coercion appears to mediate the relationship between intimate partner violence and HIV transmission, however while bivariate analysis has shown a relationship between IPSV and HIV infection, no multivariate analysis has demonstrated this relationship (Stockman et al., 2013).
Women who have experienced IPSV were 2.7 times more likely to develop cervical cancer than women who had never experienced gendered violence, possibly due to increased transmission of the human papilloma virus (n = 4732) (Coker, Hopenhayn, DeSimone, Bush, & Crofford, 2009).
Re-victimisation also increases the risk of negative sexual health outcomes. In a study of 209 women who had experienced abuse only after the age of 12 years, those who had experienced no trauma, multiple single traumatic events and an ongoing and sustained experience of physical/sexual abuse had rate of ever having had an STI of two percent, nine percent and 44 percent respectively. The same groups had a rate of pregnancy of two percent, 15 percent and 33 percent, the vast majority of which were terminated (Green, Krupnick, Stockton, Goodman, & et al., 2005).
IPSV and re-victimisation may have a significant and long term negative effect on a woman’s well-being. Negative health outcomes are particularly apparent in the area of sexual health, with some evidence of higher rates of a range of gynaecological issues, including miscarriage, STI infection and cervical cancer.
Women’s engagement with legal and support services
Key findings in this section:
- Rates of reporting and engagement with the legal system for IPSV and re-victimisation were affected by the social context of the abuse, as well as difficulties with the legal system itself.
- IPSV victims were less likely to seek help than victims of other forms of DV.
Women who experience IPSV or re-victimisation may seek support from a both informal and formal sources. Accessing support, as well as engaging with the criminal justice system, can be important in maintaining a woman’s physical and emotional safety.
The corpus provided very limited research on help-seeking in relation to “cross-type” re-victimisation. As such, the following discussion is largely limited to IPSV.
Disclosure
“While I was ashamed of being battered [by my husband] – certainly in terms of the blame it accrued from others – the shame of being raped was more deeply excoriating; I did not think I would ever tell anybody”
Louise McOrmond-Plummer
The reactions of friends and family to disclosures of IPSV affect the lived experience of the violence.
In general, IPSV is associated with more negative social reaction than other forms of DV (Sullivan et al., 2010). A woman’s decision to disclose IPSV may be affected by her previous victimisation and responses to it, however research is mixed regarding whether a history of sexual assault increases or decreases the likelihood of future disclosure (Chiara Sabina & Ho, 2014; Simmel et al., 2012). In addition, willingness to disclose, as well as responses after disclosure are affected by a range of broader factors including the criminalisation of certain behaviours and stigma/discrimination based on race, sexuality, trans experience, occupation, HIV status and drug use.
The ANROWS additional analysis of the 2012 ABS PSS data found that “18.7% (46,800) of women sexually assaulted by their cohabiting partner have not told anyone about their most recent incident” (Cox, 2015).
Help-seeking: Non-legal services
Women who experience IPSV are less likely to seek help and/or support than women who experienced other forms of DV but not IPSV. In an additional analysis of the US Violence Against Women Survey data, women who experienced IPSV “sought help from significantly fewer sources” compared to women who experienced other forms of DV (Flicker et al., 2011, p. 1074). In several studies, once a woman had experienced more than one assault, the number of abusive acts was not related to help-seeking. This suggests that it is the types of abuse, rather than the amount of abuse, that determines help-seeking (Casey & Nurius, 2005; Flicker et al., 2011).
Additional analysis of the 2012 PSS data found that, of women who reported their most recent incident of sexual assault by a male was perpetrated by a cohabiting partner:
- 34.1% (85,300) sought support and advice from a friend/family member/work colleague/person providing pastoral care;
- 29.2% (73,200) sought support and advice from a counsellor/support worker/telephone hotline; and
- 25.5% (63,200) sought support and advice from GP/ health professional. (Cox, 2015)
Help-seeking may also be affected by the type of violence that a woman experiences. For instance, in a study of undergraduate college students (n = 200), participants who had experienced DV were less likely to access mental health services if they had experienced IPSV (Próspero & Vohra-Gupta, 2008). Disclosure may also be affected by a woman’s victimisation history. A victimisation history of repeated SXA in adolescence increased the likelihood of disclosure in college women by up to six times (n = 374) (Orchowski & Gidycz, 2012).
Help-seeking is also affected by existing and systemic disadvantage, including the material, practical and psychological impacts of discrimination associated with identity, ethnicity, health status or stigmatised behaviours. Women from marginalised communities may struggle to find services that align with their own interpretation of their lived experience, or may choose not to access services due to these fears. Some women, for example women with disabilities or women from CALD backgrounds, may require additional assistance to access support.
Overall, a woman’s capacity to access services is affected by a range of “individual, inter-personal and socio-cultural” factors that mould the way the woman recognises and conceptualises violence, her decision to seek help and the supports that she selects to use (Sabina & Ho, 2014, p. 202; see also, Kennedy et al., 2012; Liang, Goodman, Tummala- Narra, & Weintraub, 2005).
(See also Sub-populations with differential patterns of victimisation.)
Help-seeking: Legal system
“[It’s basically] domestics with a bit of sex thrown in”
Police officer, NSW.
Women tend to only report severe IPSV to police. Rates of reporting to police vary according to population and the form of sexual violence, with several studies finding a zero percent reporting rate for sexual coercion (Sabina & Ho, 2014). This is unsurprising given the high rates of women who do not perceive sexual coercion as an assault.
A woman’s decision to formally disclose their assault is affected by a range of factors including the relationship with the perpetrator, the severity of the victimisation, history of engagement with the police, and the location of the incident (Parekh & Williams, 2014; Thompson, Sitterle, Clay, & Kingree, 2007). Moreover, a woman’s capacity to report their experience of violence to police is affected by the context in which that violence occurs – for women who engage in criminalised activity (e.g. sex work in places where it is illegal, illicit drug use) reporting assaults to police may be practically impossible due to necessity to disclose criminalised activities. Socially stigmatised identities or behaviours may negatively impact a woman’s “believability” and presumed “moral character”, both of which have been shown to affect charging decisions (Spohn & Tellis, 2012, p. 177).
Most research indicates that women are less likely to report IPSV than non-sexual physical assault by an intimate partner to the police (Easteal, 2014; Mouzos & Makkai, 2004). Women who experienced IPSV were half as likely to seek help from police (OR = 0.48) or family (OR = 0.51) when compared to women who did not experience sexual victimisation but did experience other forms of DV (Flicker et al., 2011).
However, a minority of studies suggest that IPSV may result in higher police reporting rates. For instance, in a US study of abused women, 19.9 percent called the police in relation to a severe sexual coercion event (in contrast, 12.7% experienced a severe sexual coercion event but did not call the police in the last year). In comparison to other callers, women who were severely sexually assaulted were one and a half times more likely to call the police (OR = 1.58) (Bonomi et al., 2006).
Police reporting of IPSV is also lower than reporting sexual assault perpetrated by people other than an intimate partner (Fisher, Daigle, Cullen, & Turner, 2003; Möller et al., 2012).
In comparison to women raped by their partners:
- women who were raped by an acquaintance were 2.3 times more likely to report the incident to police; and
- women raped by a stranger were 5.2 times more likely to report. (Addington & Rennison, 2008)
In a psychological test which used a scenario exercise to assess a police officer’s attitudes about sexual assault, Australian police officers were more likely to consider a victim to be credible and to believe that she had been sexually assaulted if the scenario involved her being assaulted by an ex-boyfriend than by her husband (McLean & Goodman-Delahunty, 2008). The normative attitudes of practitioners throughout the legal system are important as they define and determine the results of criminal prosecutions. As Sack notes:
[most] practitioners are both sincere and well-meaning […] I believe that the fundamental explanation for the resistance to full implementation of [legal changes that acknowledge marital rape] rests in historical justifications for the toleration of domestic violence which we thought we had jettisoned long ago. Yet the legacy of these justifications continue to shape our beliefs about violence against women. Do we really believe that domestic violence is a crime?
In the context of community attitudes, IPSV is frequently difficult to prosecute (McGlynn, 2010). A study that examined agreement between police and prosecutors in Philadelphia rape cases found that prosecutors were more likely to agree to proceed with a case of stranger rape than IPSV (Holleran, Beichner, & Spohn, 2010). Additional analysis of the US National Survey of Violence Against Women showed that, while 29.7 percent of reported cases of sexual assault were perpetrated by an intimate partner, only 19 percent of convicted cases were for IPSV (Felson & Pare, 2007). A study comparing data from two large national crime victimisation studies found that case clearance was strongly predicted by the reporting of a co-occurring crime (Addington & Rennison, 2008).
The Aboriginal Family Violence and Legal Service Victoria notes that under-reporting of IPSV is a significant issue within Aboriginal and Torres Strait Islander communities (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010). Anecdotal evidence indicates that Aboriginal and Torres Strait Islander women often do not report assaults to police. Despite this, Aboriginal women are disproportionately represented as complainants in sexual assault cases, suggesting that the rate of assault is even more disproportionate than is currently reflected in available data (Keel, 2004). In addition, there is some evidence that Aboriginal women experience low rates of police response when they request assistance with multiple incidents (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010).
The available evidence suggests that the social context of IPSV and re-victimisation, as well as difficulties with the legal system itself, reduces the rates of reporting and engagement with the legal system for these types of violence. As Sack quips in her discussion of judicial responses to IPSV “[w] here intimate partner rape is concerned, the bad old days are surely still with us” (2010, p. 548).
Responses to women affected by re-victimisation and co-occurrence
Key findings in this section:
- DV and SXA services are often separated, with both service types finding victims of IPSV a particularly challenging client group.
- Joined-up services have substantial government support, however they sometimes have unexpected negative consequences such as the reduced provision of services to SXA victims.
- Health professionals are often a gateway to specialist violence services, however they generally have not received specialist training in the area.
- Evidence remains mixed regarding the efficacy of behaviour change perpetrator programs with very few programs addressing IPSV.
- Prevention programs, such as awareness campaigns and bystander programs, are typically implemented in university settings and often have a focus on IPSV in dating relationships.
- Education of professionals in the area of primary prevention is important, as is engaging young people in ongoing dialogues about the nature of sexual consent.
“We, in our own education, say that violence does not exist in isolation… why are we then providing a service to women in isolation?”
– Senior level management staff.
Service responses to women affected by re-victimisation and co-occurrence may be based in a range of orientations including feminist and empowerment approaches and social work methodologies (Conway et al., 2010). Within many of these, there is a political and practical commitment to enabling women to address their full history of abuse and for recovery to be defined as a sense of well-being rather than merely a lack of trauma-related pathology (Fotheringham & Tomlinson, 2009; Ranjbar & Speer, 2013). Evidence suggests that a large proportion of DV and SXA services users have a history of IPSV and/or re-victimisation, with a study of psychological and advocacy service users finding that about three quarters of their clients had experienced abuse as a child (Follette, Polusny, Bechtle & Naugle, 1996). In addition, a study of women in DV refuges found that eight out of ten women had experienced IPSV (Moreau et al., 2015).
There is limited evidence of the effectiveness of service responses to IPSV and re-victimisation (Macy, Johns, Rizo, Martin, & Giattina, 2011). Given the lack of directly relevant research, but in keeping with the focus of this study on the intersection between SXA and DV, this section is largely focused on service provision that addresses both DV and SXA. The minimal amount of content specific to IPSV and re-victimisation likely reflects the lack of services that address these forms of victimisation specifically – this implied service gap is problematic as the use of more generic support strategies may leave the needs of these survivors “unidentified and unaddressed” and may result in a narrowing of “the opportunities to develop safety and healing” (Winters, 2009, p.7; see also, McOrmond-Plummer, Easteal & Levy- Peck, 2014).
Australian domestic violence and sexual assault support services are often provided by distinct sets of professional organisations. The siloing of services may be understood as partially a consequence of the conceptual and practice histories of the DV and SXA sectors (Ristock, 2014; Wilcox, 2010). As Kerr notes, “[e]ven for those of us who work in the field, domestic abuse is sometimes seen as something separate from rape or sexual assault” (Kerr, 2014, p.90). This separation is common to a number of countries, including the US, and poses significant challenges in addressing the needs of women who have experienced both SXA and DV (Herz, Stroshine, & Houser, 2005; Macy, Giattina, Sangster, Crosby, & Montijo, 2009; McOrmond-Plummer, Easteal & Levy-Peck, 2014; Wilcox, 2010; Williamson, 2014).
In a study of service executives’ understandings of the characteristics of DV and SXA services, similar provisions, such as counselling, 24-hour crisis lines, support groups, children’s services and legal advocacy, were deemed important for users of both DV and SXA services. Medical and ER advocacy was largely considered useful for SXA survivors, while shelter services were understood as more important to survivors of domestic violence (Macy, Giattina, Montijo, & Ermentrout, 2010). Put differently, service providers tended to understand DV services as providing whole-of-life support while SXA services were seen as more likely to provide context-specific support (Fotheringham & Tomlinson, 2009).
A literature review on violence against women services found that the literature recommended that DV and SXA services have several similar characteristics. These included:
- a telephone hotline;
- legal advocacy;
- support groups; and
- individual counselling. (Macy et al., 2009)
Both types of service have an ultimate focus on ensuring women’s safety (Herz et al., 2005).
Despite the similarity in the ultimate goal of these services, it is important to note that the emotional needs of service users may vary with the type of violence experienced (Macy et al., 2011). Zweig and Burt (2007) observed that while a sense of control was important for women in domestic violence services, it did not predict how helpful women found sexual assault services (n = 1509).
Service executives acknowledged that the provision of combined services that were appropriate for both DV and SXA survivors was difficult (Macy et al., 2010). Individuals who have experienced IPSV were considered particularly challenging, with limited best practice guidance available (Macy et al., 2010). Despite this, the combining of services has been shown to be particularly valuable in improving the services to women who have experienced sexual violence, although its overall benefit to all types of survivor is less well established (Zweig & Burt, 2004).
The available literature regarding combined DV and SXA service provision is inconclusive. Some researchers emphasised that the experience of SXA and DV were different and thus require specialist services, while others argued that it was essential for DV and SXA services to collaborate (Fotheringham & Tomlinson, 2009; Macy et al., 2009). Some service representatives have raised concerns about the impact of combined SXA and DV service provision, which may negatively impact their funding arrangements and may result in SXA being subsumed under DV services (Fotheringham & Tomlinson, 2009). Many service and policy representatives consider that combined services dedicate inadequate attention and resources to sexual assault (Macy, Giattina, Parish, & Crosby, 2010).
For many DV service staff, IPSV is considered outside their area of expertise (Heenan, 2004; Macy et al., 2009; McOrmond-Plummer et al., 2014). Both DV and SXA workers may consider IPSV to more “properly” fit within the remit of workers in the other field, with US researchers noting a systemic lack of attention to IPSV found in both DV and SXA services (Bennice & Resick, 2003; Heenan, 2004; Levy-Peck, 2014b).
Both DV and SXA services acknowledge limited funding or capacity for services to marginalised women (Macy et al., 2010). In the Australian context, the compartmentalisation of services is of particular concern when addressing the needs of Aboriginal and Torres Strait Islander peoples, as the intricate histories of trauma in these communities mean that there is increased complexity in the service landscape (Cripps & McGlade, 2008). In addition, the needs of women who have experienced re-victimisation and/or IPSV and are unable to access mainstream violence services (e.g. women with severe communication or cognitive limitations), may be particularly poorly addressed in services which do not specialise in supporting women who have experienced violence (Barger et al., 2009).
Coordinated, multi-agency and integrated services responses
There is a growing consensus that women’s safety is best served when multiple bureaucratic and practical systems work together to provide the woman with the support services that she needs (Breckenridge, Rees, valentine, & Murray, 2015; Cattaneo & Goodman, 2005). Providing such services can be difficult for women who have experienced IPSV or re- victimisation, with service directors noting that providing services to women who have experienced both DV and SXA is a key challenge (Macy et al., 2010).
A range of coordinated approaches are available, including, but not limited to:
- whole of government policy coordination;
- recidivism risk assessments;
- safety planning;
- co-education across sectors;
- specialist workers to assist women to access services across sectors;
- multi-agency services; and
- “no wrong door” approaches.
(Breckenridge et al., 2015; Cooper et al., 2008; Macleod, 2014b; Salter, 2012)
Coordinated responses may also include access to services such as mental health or AOD programs that help to address issues that may occur at the same time or as a consequence of IPSV or re-victimisation (Macy et al., 2010). Another way of understanding potential coordinated responses is to imagine them as a continuum of coordination, from autonomous services with networking, through collaborative practice, streamlined referrals, cooperation (via regular communication about clients), coordination (agreed protocols) to integration (single system) (Wilcox, 2010; Potito, Day, Carson & O’Leary, 2009).
Although most research supports joined up services, some evidence indicates that the ability to meet the service needs of sexual assault victims but not domestic violence victims was improved when NGOs and legal services worked in collaboration (Zweig & Burt, 2003; for further review of literature on DV and SXA integrated responses, see Breckenridge et al., 2015).
In order for IPSV and re-victimisation to be adequately addressed, services need to simultaneously be consolidated and to provide specialist responses to the specific contexts of IPSV and re-victimisation (Bennice & Resick, 2003). Moreover, services need to be sensitive to the impacts of structural and attitudinal limitations on access to certain forms of coordinated response, including systemic restrictions due to limited accessibility and exclusion criteria based on a woman’s behaviour and/or health status (e.g. whether she uses injecting drugs) (Breckenridge et al., 2015). Researchers recommend that, as a first priority, there needs to be a shift in the Australian context so that there can be meaningful partnerships across services (Heenan, 2004).
Health professionals
“…many times victims present as domestic violence victims [although] in reality they’re both, but the other part doesn’t come out for a very long time”
– Research participant
Primary care professionals, such as general practitioners (GPs), are the gateway for many women into specialist DV or SXA services (Hegarty, Hindmarsh, & Gilles, 2000; Palmer & Parekh, 2014). Despite this, practitioners rarely receive training in DV and SXA, and are even less likely to be skilled in dealing with co-occurrence or re-victimisation (Maas-DeSpain & Todahl, 2014; Parkinson & Zara, 2014; Todahl & Walters, 2009).
In order for a GP to get a full picture of the DV that their patient is experiencing, it is important for them to assess both physical and sexual victimisation. A range of characteristics of this conversation may increase its helpfulness:
- Assurance of, and practices to ensure absolute maintenance of, confidentiality, especially in contexts where the GP sees other members of the woman’s family (including, potentially, the perpetrator of the violence).
- The provision of a comprehensive and sensitive discussion of IPSV may be assisted by using a validated screening tool.
- Asking separately and directly about IPSV may increase disclosure.
- Emphasising that the woman is believed may assist women to feel safe and supported.
- Explicitly identifying the described behaviours as IPSV may be helpful in contextualising the violence.
- Practitioners should be aware that a disclosure of physical violence may not include disclosure of IPSV, and that not mentioning IPSV does not necessarily mean that it is not happening.
- Capacity to engage in basic safety planning and referrals as required.
(Maas-DeSpain & Todahl, 2014; Palmer & Parekh, 2014; Parkinson & Reid, 2014; Spiller et al., 2012; Wall, 2012)
Researchers note that current screening methods could be improved by expanding the definition of IPSV to include not only intimate partner rape, but also sexual acquiescence, with the American College of Obstetrician and Gynaecologists providing detailed guidelines related to IPSV and reproductive coercion screening (Chamberlain & Levenson, 2012; Maas- DeSpain & Todahl, 2014; see also Williamson, 2014).
Treatment
Behavioural change perpetrator programs aim to stop men reoffending. Such programs are typically aimed at either SXA or DV perpetrators, with few structured in a way to acknowledge the high rate of co-occurrence in the form of IPSV. There is significant variation in the approaches used in these programs, however they tend to be didactic in nature (Nelson et al., 2010). Programs often have a high dropout rate, with a 50 percent completion rate considered typical (Day, O’Leary, Chung, & Justo, 2009).
Salter (2012) notes that perpetrator programs have little empirical support, with individual studies, literature reviews and meta-analyses showing no behavioural improvement in men who complete these programs. These traditional programs are particularly ineffective with high risk offenders, whose re-offending patterns are highly resistant to available intervention programs (Salter, 2012). Such equivocal evidence emphasises the need to improve interventions, rather than dismantle them (Campbell, 2005).
A minority of researchers promote interventions which provide couples with skills to improve communication and manage conflict (Mathes, 2013). Problematically, a sub set of these scholars recommend that victims should change their coping strategies as changes in the violent behaviour of their partner is unlikely (Sullivan et al., 2010).
Justice responses
This review identified significant legal debate on mainstream justice responses to IPSV. This discussion centred on how the law understands consent, and in particular, whether or not a presumption of ongoing consent is legally valid. Feminist legal scholars continue to advocate for the full removal of discussions of a woman’s sexual history from prosecutions of rape (Bergen, 2006; Clark, 2007; Ellison, 2010; McGlynn, 2010; Sack, 2010).
In addition, there is significant debate regarding whether restorative justice approaches are appropriate in these instances (Cripps & McGlade, 2008; Daly, 2006; McAlinden, 2008). Restorative justice approaches for youth sex offending show some promise, although initial research is limited in its ability to show changes in recidivism (Daly, Bouhours, Broadhurst, & Loh, 2013). Evaluation on circle sentencing impact has found no effect of the process on recidivism, however such research is not focused on DV, SXA or instances of their co-occurrence (Fitzgerald, 2008).
Prevention
Recent Australian initiatives such as Our Watch[8] are indicative of a consensus that prevention is necessary for ongoing changes in the epidemiology of violence.[9] Primary prevention, or stopping violence before it starts, is a priority of both practitioners and large policy bodies such as the US Centre for Disease Control (Martin et al., 2009). Despite this, very little research has engaged with the effectiveness of programs which address community attitudes, with research consistently focused on changes to individual behaviour (Sabina & Ho, 2014).
Prevention programs are unevenly distributed within communities, often along socio-economic lines. For instance, a US study of over 3000 counties found that having a top- ranked university in a county “was a significant predictor of the number of DV programs in the area” (Sabina & Ho, 2014, p. 214; Tiefenthaler, Farmer, & Sambira, 2005).
Research with young people emphasises the need for prevention activities to be tailored to the target audience (e.g. age, sex and ethnicity) and must address the relationship between normative gender roles and dating sexual violence (Noonan & Charles, 2009).
At a more individual level, a number of researchers have examined interventions that encourage women to enact “protective behaviours” or address victim “controllable” factors. These programs may support victim blaming and thus have limited support in the violence against women sector (Herman, 2009). Opponents of these programs note that by focusing on women’s “bad habits”, these programs support the power structures that enable gendered violence to happen in the first place (Lichtenstein, 2005). When programs do attempt to augment potential victim’s behaviours, such as intervening with women who have experienced CSA as a way of preventing adult sexual assault, these programs have been shown to have limited effectiveness (Hill et al., 2011; Macy, 2007).
Domestic violence and sexual assault bystander programs aim to provide people observing violence against women with the skills and confidence to intervene (Moynihan et al., 2010; Moynihan, Banyard, Arnold, Eckstein, & Stapleton, 2011). Dedicated bystander programs are particularly common on university campuses, with programs often combining SXA and DV prevention in the same campaign (Lichty, Campbell, & Schuiteman, 2008). Within the context of enabling successful bystander interventions, such programs often have an implicit engagement with gender norms and violence supporting attitudes.
Education
“[What’s needed is] education for the males – that females are not just a piece of equipment to be used whenever you want it.”
– Sexual offences and child abuse officer, NSW
Public education about DV happens in Australia in a range of ways, including sex education classes in schools and large scale public awareness campaigns. Public education on DV does not tend to focus on IPSV, despite IPSV being a major form of DV (Flicker et al., 2011).
Young people are particularly in need of education about sexual consent, with education on adolescent IPSV needing to be tailored to specific target groups and addressing the impact of traditional gender roles on sexual expectations and behaviours (Levy-Peck, 2014a; Noonan & Charles, 2009). Provision of such education varies significantly between schools and across jurisdictions.
Professional training, including of “grass roots” professionals interested in primary prevention, is also important. Very few practitioners receive comprehensive education in DV epidemiology or screening methods (Maas-DeSpain & Todahl, 2014; Martin et al., 2009; Todahl & Walters, 2009). In the Australian context, accredited vocational training is available in the area of DV, however equivalent training is not available for SXA – this reduces the professional development available to SXA and DV workers, as well as other front line service providers such as GPs (Macleod, 2014b; Parkinson & Zara, 2014). It is necessary to provide specialist training in order to ensure that appropriate responses are given to women from minority groups who experience IPSV or re- victimisation, including Aboriginal and Torres Strait Islander communities.
Overall, the available literature demonstrates responses to re-victimisation and IPSV that are across the full continuum of interventions – from primary prevention to tertiary responses. Most of these initiatives occur in the context of wider SXA and DV services, with the complex contexts of service delivery meaning that some clients may “fall through the cracks” between the sectors.
Recommendations and conclusion
“Effective response to IPSV [and re- victimisation] is the place where the movements to end and address domestic violence and sexualised violence come together”
Research on IPSV and re-victimisation is characterised by a range of systemic issues. A major ongoing issue in research in these areas is the siloing of research by type of assault (DV vs SXA) in a way that limits our understanding of women’s experiences when they cross these definitional boundaries (Sabina & Ho, 2014). The following recommendations are based in the research examined for this state of knowledge paper and can be made regarding the method and focus of future research.
ANROWS recommends that:
- As re-victimisation often occurs across violence types, researchers should, wherever possible, expand their examination of life course re-victimisation to multiple violence types.
- Longitudinal research is critical to understanding the complex pathways that result in repeated victimisation and IPSV. Such research is particularly important for understanding the lived experience of marginalised women (e.g. incarcerated women), as the intersections of disadvantage are even more complex for these populations (Poister, Tusher, & Cook, 2010). Put differently, “longitudinal research is needed to sort out risk factors, from consequences, from simple correlates” (Classen et al., 2005, p. 114).
- As has been noted for several decades now, one way of increasing the quality and comparability of research findings is for there to be consistent definitions of abusive behaviours used in IPSV and re-victimisation research. Such definitions would need to provide clarity to research participants about what was meant by “force” in relation to sexual activity, with distinctions made between physical threat and emotional/psychological coercion tactics.
- Future research should concentrate on relevant target groups. Many target groups have relatively small populations, making collecting data with population level surveys difficult. One exception to this is disability, which has a high prevalence and thus analysable data is likely to be able to be collected in all violence research. Most other sub- populations are likely to require dedicated surveys to get a sufficient sample to be statistically reliable.
- Although both qualitative and quantitative research is needed to inform Aboriginal and Torres Strait Islander family violence policy, priority should be given to quantitative research as current quantitative surveys like the PSS are unable to provide prevalence estimates for this population.
In order for IPSV and cross-type re-victimisation to be meaningfully addressed in the Australian context, it is necessary to provide coordinated SXA and DV services that occur in the context of supportive social service systems (Heenan, 2004). The following recommendations are made regarding the service delivery environment and are based on the research findings reviewed in this paper.
IPSV and “cross-type” re-victimisation are scenarios of violence which emphasise the inter-related nature of SXA and DV. This violence does not happen in silos or vacuums, rather it is a complex lived experience that crosses the conceptual lines which are frequently part of policy and service provision. Until there is full acknowledgement in the DV and SXA sectors that domestic violence and sexual assault are interdependent concepts, some of the instances of violence most in need of our attention will continue to be sidelined from mainstream responses (Sabina & Ho, 2014).
ANROWS recommends that:
- Acknowledgement is made in policy and practice of weaknesses in our current research base, which means that we are heavily reliant on practice knowledge.
- Accurate and appropriate use of data and acknowledgement of data’s limitations is encouraged in policy, planning and service advocacy, so that when further evidence-based knowledge is available, it is welcomed and adopted.
- To address the stigma of IPSV, DV and SXA services continue to work to raise awareness of the impact of stigma on clients and staff.
- Judicial education and professional development work continues to be supported to ensure court and police sensitivity in IPSV cases, and to minimise the distress of the legal process to women who have experienced re- victimisation and/or IPSV.
- Where not already part of normal clinical practice, STI clinics be provided with training and materials to enable streamlined referrals to SXA and DV services.
- Trauma informed care (a model of care which puts at the centre of clinical practice the long term effects of victimisation) be supported through mainstream service provision and research investment.
- Large scale mental health campaigns promote gendered violence as a risk factor for poor mental health outcomes.
- All DV and SXA services be sufficiently resourced to further enrich cross-sector co-ordination (a full range of co- ordination strategies are possible, from referral pathways to fully integrated care).
- All DV and SXA services, as well as related services such as mental health and drug and alcohol programs, continue to work towards an integrated understanding of the impacts of the escalation or severity of CSA on adulthood in their engagements with both children and adults.
- Public education on violence against women acknowledges the distinct but intersectional dimensions of different forms of violence and its gendered impacts and characteristics.
- Providers of mainstream health and social services be sensitised to the possibility of IPSV and re-victimisation cases in their day to day work. An initial step towards this would be the promotion of existing IPSV screening tools to a wide range of mainstream frontline providers.
- Prevention programs not be funded by government if they implicitly or explicitly support victim blaming. Explanation of these actions should be given to campus unions to promote a similar stance in university campus programs.
- Professional development for workers in the violence against women field acknowledge the multi-faceted nature of abuse and emphasise the links between DV and SXA.
Appendix A: Searched databases
EBSCO collections:
- Academic Search Premier;
- Aboriginal Australia;
- Health;
- Law;
- Psychology;
- Social Sciences – General, Statistics.
Proquest collections:
- ABI/Inform;
- PsychInfo;
- PsychArticles;
- Criminal Justice;
- Family Health;
- Health & Medical Complete;
- Health Management;
- Nursing & Allied Health Source;
- Psychology Journals;
- Research Library;
- Social Science Journals;
- Sociology.
Informit collections:
- Arts & humanities;
- Health;
- Indigenous peoples;
- Social Science.
JSTOR collections:
- Feminist & women’s studies;
- Health policy;
- Health sciences;
- Humanities;
- Law;
- Medicine and allied health;
- Psychology;
- Public health;
- Social studies;
- Social work;
- Sociology.
ANROWS collections:
- Bibliography of Australian Domestic Violence and Sexual Assault research.
Appendix B: Additional available literature
Re-victimisation
A variety of populations have been examined in relation to re-victimisation involving CSA and DV including:
- women attending health clinics (Williams et al., 2010);
- college students (Ménard & Pincus, 2014);
- women with severe mental illness (Meade et al., 2009); and
- women who were seeking help for DV (Vatnar & Bjørkly, 2008).
Research is predominately completed in the US, with some research from Spain (Garcia-Linares et al., 2005; Pico-Alfonso et al., 2006), Australia (Schei et al., 2006) and Norway (Vatnar & Bjørkly, 2008).
Intimate partner sexual violence rates
Overall there is extensive research on the rate of IPSV, typically in the context of estimating overall DV prevalence. Some examples of study populations are:
- women of various ethnicities (e.g. white, Hispanic, black) (McFarlane, Malecha, Watson, et al., 2005; Ramisetty-Mikler, Caetano, & McGrath, 2007);
- migrant communities (Liles et al., 2012; Morash, Bui, Zhang, & Holtfreter, 2007);
- people in same-sex relationships (Edwards et al., 2015; Stoddard, Dibble, & Fineman, 2009);
- pregnant women (Flanagan, Jaquier, Gordon, Moore, & Stuart, 2014);
- adolescents (Hess et al., 2013; Howard, Wang, & Yan, 2007; Sears & Byers, 2010; Zurbriggen et al., 2010); and
- women who are incarcerated (Raj et al., 2008).
Much of the research that used the CTS compared violence perpetration and victimisation rates for women and men, and thus provided significant gender comparisons (e.g. Dardis, Edwards, Kelley, & Gidycz, 2013). Population level studies include examination of IPSV rates in national representative samples (Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007) and adult women (Thompson et al., 2006).
Several studies used the CTS2 to compare rates of mild and severe sexual coercion.[10] Rates of severe sexual coercion and mild coercion varied with population group (represented below in brackets as severe: mild), including:
- US college women (2.2%: 27.8%) (Sabina & Straus, 2008);
- Polish college women (11%: 57%) (Doroszewicz & Forbes, 2008);
- women experiencing police involved DV (26.26%: 41.67%) (Messing et al., 2014);
- women receiving emergency department care (15%: 24% [any sexual coercion]) (El-Bassel et al., 2007); and
- US college women reporting on dating violence in adolescence (5.4%: 25.3%) (Bonomi, Anderson, Nemeth, Rivara, & Buettner, 2013).
Studies also examined particular abusive behaviours. Although the majority of research projects examined IPSV in a broad sense, and included sexual coercion, some were limited to, or explicitly separated, partner rape (Bergen & Bukovec, 2006; Finkelhor & Yllö, 1987; Logan, 2009; Maas-DeSpain & Todahl, 2014; Martin et al., 2007; McFarlane, 2007; Tellis, 2010). Research often focused on verbal coercion (Brousseau et al., 2012; Dutton & Goodman, 2005; Eaton & Matamala, 2014), with a small number of papers examining attempted rape (Möller, Bäckström, Söndergaard, & Helström, 2012) or forced sexual initiation (Campbell, Lucea, Stockman, & Draughon, 2013). Researchers also defined their research population by relationship type, with studies focusing on:
- dating IPSV (Doroszewicz & Forbes, 2008; Edwards et al., 2015; Foshee et al., 2007; Gagné et al., 2005; Katz, Moore, & May, 2008; Montoya, Coker-Appiah, Eng, Wynn, & Townsend, 2013; Reyes & Foshee, 2013; Sears & Byers, 2010);
- newly married couples (Panuzio & Dilillo, 2010); and,
- IPSV perpetrated by a married spouse (Martin et al., 2007).
Research has also examined the prevalence of IPSV in sub- sets of violence affected individuals, such as:
- women who are have been physically abused by their partner (Spiller, Jouriles, McDonald, & Skopp, 2012);
- women who have protection orders against their partner (Logan, 2009);
- men arrested for the physical assault of their female partner (Basile & Hall, 2011);
- women seeking assistance for SXA (Kennedy et al., 2012); and
- women who are residing in refuges (Spiller et al., 2012).
Although almost all studies were completed in the US, a small number of projects examined IPSV in other countries such as:
- Australia (Mouzos & Makkai, 2004; Schei et al., 2006);
- Spain (Pico-Alfonso et al., 2006);
- Japan (Yoshihama & Horrocks, 2010);
- Poland (Doroszewicz & Forbes, 2008); and
- Sweden (Möller et al., 2012).
References
Abbey, A. (2011). Alcohol’s role in sexual violence perpetration: Theoretical explanations, existing evidence and future directions. Drug and Alcohol Review, 30(5), 481-489.
Abbey, A., Parkhill, M. R., & Koss, M. P. (2005). The effects of frame of reference on responses to questions about sexual assault victimization and perpetration. Psychology of Women Quarterly, 29(4), 364-373.
Aboriginal Family Violence Prevention and Legal Service Victoria. (2010). Improving accessibility of the legal system for Aboriginal and Torres Strait Islander victims/survivors of family violence and sexual assault. Policy Paper Series: Paper 3 of 3. Collingwood, Vic: Aboriginal Family Violence Prevention and Legal Service Victoria.
Adams, R., & Hunter, Y. (2007). Surviving justice: Family violence, sexual assault and child sexual assault in remote Aboriginal communities in NSW. Indigenous Law Bulletin, 7(1), 26-28.
Addington, L. A., & Rennison, C. M. (2008). Rape co- occurrence: Do additional crimes affect victim reporting and police clearance of rape? Journal of Quantitative Criminology, 24(2), 205-226.
Ahrens, C. E., Dean, K., Rozee, P. D., & McKenzie, M. (2008). In F. L. Denmark & M. A. Paludi (Eds.), Psychology of women: A handbook of issues (2nd ed.). Westport, CT: Praeger Publishers.
Allimant, A., & Ostapiej-Piatkowski, B. (2011). Supporting women from CALD backgrounds who are victims/survivors of sexual violence: Challenges and opportunities for practitioners. Melbourne: Australian Institute of Family Studies.
Andersen, J. P., Hughes, T. L., Zou, C., & Wilsnack, S. C. (2014). Lifetime victimization and physical health outcomes among lesbian and heterosexual women. PLoS ONE, 9(7), e101939.
Arata, C. M. (2000). From child victim to adult victim: A model for predicting sexual revictimization. Child Maltreatment, 5(1), 28-38.
Arata, C. M., & Lindman, L. (2002). Marriage, child abuse, and sexual revictimization. Journal of Interpersonal Violence, 17(9), 953-971.
Argento, E., Muldoon, K. A., Duff, P., Simo, A., Deering,
K. N., & Shannon, K. (2014). High prevalence and partner correlates of physical and sexual violence by intimate partners among street and off-street sex workers. PLoS ONE, 9(7), 1-7.
Armour, C., & Sleath, E. (2014). Assessing the co-occurrence of intimate partner violence domains across the life-course: Relating typologies to mental health. European Journal of Psychotraumatology, 5.
Australian Bureau of Statistics. (2013a). Defining the data challenge for family, domestic and sexual violence. Canberra: ABS.
Australian Bureau of Statistics. (2013b). Personal Safety Survey, 2012. Canberra: ABS.
Babcock, R. L., & Deprince, A. P. (2013). Factors contributing to ongoing intimate partner abuse: Childhood betrayal trauma and dependence on one’s perpetrator. Journal of Interpersonal Violence, 28(7), 1385-1402.
Bagwell-Gray, M. E., Messing, J. T., & Baldwin-White, A. (2015). Intimate partner sexual violence: A review of terms, definitions, and prevalence. Trauma, Violence, & Abuse, 16(3), 316-335.
Bair-Merritt, M., Ghazarian, S., Burrell, L., & Duggan, A. (2012). Patterns of intimate partner violence in mothers at-risk for child maltreatment. Journal of Family Violence, 27(4), 287-294.
Baldry, E., & Cunneen, C. (2014). Imprisoned Indigenous women and the shadow of colonial patriarchy. Australian & New Zealand Journal of Criminology, 47(2), 276-298.
Barger, E., Wacker, J. Macy, R. & Parish, S. (2009). Sexual assault prevention for women with intellectual disabilities: A critical review of the evidence. Intellectual and Developmental Disabilities, 47(4), 249-262.
Barnes, J. E., Noll, J. G., Putnam, F. W., & Trickett, P. K. (2009). Sexual and physical revictimization among victims of severe childhood sexual abuse. Child Abuse & Neglect, 33(7), 412-420.
Basile, K. (2008). Histories of violent victimization among women who reported unwanted sex in marriages and intimate relationships: Findings from a qualitative study. Violence Against Women, 14(1), 29-52.
Basile, K., Arias, I., Desai, S., & Thompson, M. P. (2004). The differential association of intimate partner physical, sexual, psychological, and stalking violence and posttraumatic stress symptoms in a nationally representative sample of women. Journal of Traumatic Stress, 17(5), 413-421.
Basile, K., & Hall, J. E. (2011). Intimate partner violence perpetration by court-ordered men: Distinctions and intersections among physical violence, sexual violence, psychological abuse, and stalking. Journal of Interpersonal Violence, 26(2), 230-253.
Bebbington, P., Jonas, S., Kuipers, E., King, M., Cooper, C., Brugha, T., . . . Jenkins, R. (2011). Childhood sexual abuse and psychosis: Data from a cross-sectional national psychiatric survey in England. The British Journal of Psychiatry, 199(1), 29-37.
Bennice, J. A., & Resick, P. A. (2003). Marital rape history, research, and practice. Trauma, Violence, & Abuse, 4(3), 228-246.
Bennice, J. A., Resick, P. A., Mechanic, M., & Astin, M. (2003). The relative effects of intimate partner physical and sexual violence on post-traumatic stress disorder symptomatology. Violence and Victims, 18(1), 87.
Bergen, R.K. (2006). Marital rape: New research and directions. Retrieved from https://www.vawnet.org/Assoc_Files_VAWnet/AR_MaritalRapeRevised.pdf
Bergen, R. K., & Bukovec, P. (2006). Men and intimate partner rape: Characteristics of men who sexually abuse their partner. Journal of Interpersonal Violence, 21(10), 1375-1384.
Black, M. C., Basile, K., Breiding, M. J., Smith, S. G., Walters,
M. L., Merrick, M. T., . . . Stevens, M. R. (2011). National intimate partner and sexual violence survey: 2010 summary report. Atlanta, Ga: National Center for Injury Prevention and Control.
Blagg, H., Bluett-Boyd, N., & Williams, E. (2015). Innovative models in addressing violence against Indigenous women (State of knowledge paper 10). Sydney: ANROWS.
Blagg, H., Murray, R., Ray, D., & Macarthy, E. (2000). Crisis intervention in Aboriginal family violence: Strategies and models for Western Australia. Canberra: Department of the Prime Minister and Cabinet.
Boivin, S., Lavoie, F., Hébert, M., & Gagné, M.-H. (2012). Past victimizations and dating violence perpetration in adolescence: The mediating role of emotional distress and hostility. Journal of Interpersonal Violence, 27(4), 662-684.
Bonomi, A. E., Anderson, M. L., Nemeth, J., Rivara, F. P., & Buettner, C. (2013). History of dating violence and the association with late adolescent health. BMC Public Health, 13(1), 1-12.
Bonomi, A. E., Anderson, M. L., Rivara, F. P., Cannon, E. A., Fishman, P. A., Carrell, D., . . . Thompson, R. S. (2008). Health care utilization and costs associated with childhood abuse. Journal of General Internal Medicine, 23(3), 294-299.
Bonomi, A. E., Anderson, M. L., Rivara, F. P., & Thompson, R. S. (2007). Health outcomes in women with physical and sexual intimate partner violence exposure. Journal of Women’s Health, 16(7), 987-997.
Bonomi, A. E., Holt, V. L., Martin, D. P., & Thompson, R. S. (2006). Severity of intimate partner violence and occurrence and frequency of police calls. Journal of Interpersonal Violence, 21(10), 1354-1364.
Brassard, A., Darveau, V., Péloquin, K., Lussier, Y., & Shaver,
P. R. (2014). Childhood sexual abuse and intimate partner violence in a clinical sample of men: The mediating roles of adult attachment and anger management. Journal of Aggression, Maltreatment & Trauma, 23(7), 683-704.
Breckenridge, J., Rees, S., valentine, k., & Murray, S. (2015). Meta-evaluation of existing interagency partnerships, collaboration, coordination and/or integrated interventions and service responses to violence against women: State of knowledge paper 11. Sydney: ANROWS.
Briere, J. N., & Elliott, D. M. (1994). Immediate and long- term impacts of child sexual abuse. The Future of Children, 4(2), 54-69.
Broach, J. L., & Petretic, P. A. (2006). Beyond traditional definitions of assault: Expanding our focus to include sexually coercive experiences. Journal of Family Violence, 21(8), 477-486.
Bronfenbrenner, U. (2005). Making human beings human: Bioecological perspectives on human development. Thousand Oaks: Sage.
Brousseau, M. M., Hébert, M., & Bergeron, S. (2012). Sexual coercion within mixed-sex couples: The roles of sexual motives, revictimization, and reperpetration. The Journal of Sex Research, 49(6), 533-546.
Brownridge, D. A., & Halli, S. S. (2001). Explaining violence against women in Canada. Lanham, Md: Lexington Books.
Brownridge, D. A. (2006). Partner violence against women with disabilities Prevalence, risk, and explanations. Violence Against Women, 12(9), 805-822.
Busby, D. M., Holman, T. B., & Walker, E. (2008). Pathways to relationship aggression between adult partners. Family Relations, 57(1), 72-83.
Busch-Armendariz, N. B., DiNitto, D. M., Bell, H., & Bohman,
T. (2010). Sexual assault perpetrators’ alcohol and drug use: The likelihood of concurrent violence and post-sexual assault outcomes for women victims. Journal of Psychoactive Drugs, 42(3), 393-399.
Campbell, R. (2012). Fight, flight, or . . . freeze? Yes. Freeze. New York: Joyful Heart Foundation.
Campbell, J. (2005). Assessing dangerousness in domestic violence cases: History, challenges, and opportunities. Criminology & Public Policy, 4(4), 653-671.
Campbell, J. C., Baty, M. L., Ghandour, R. M., Stockman, J. K., Francisco, L., & Wagman, J. (2008). The intersection of intimate partner violence against women and HIV/AIDS: a review. International Journal of Injury Control and Safety Promotion, 15(4), 221-231.
Campbell, J., Jones, A. S., Dienemann, J., Kub, J., Schollenberger, J., O’Campo, P., Wynne, C. (2002). Intimate partner violence and physical health consequences. Archives of Internal Medicine, 162(10), 1157-1163.
Campbell, J., Lucea, M. B., Stockman, J. K., & Draughon, J.E. (2013). Forced sex and HIV risk in violent relationships. American Journal of Reproductive Immunology, 69, 41-44.
Campbell, J. C., Webster, D. W., & Glass, N. (2009). The danger assessment validation of a lethality risk assessment instrument for intimate partner femicide. Journal of Interpersonal Violence, 24(4), 653-674.
Cannon, E. A., Bonomi, A. E., Anderson, M., Rivara, F. P., & Thompson, R. S. (2010). Adult health and relationship outcomes among women with abuse experiences during childhood. Violence and Victims, 25(3), 291-305.
Casey, E., & Lindhorst, T. P. (2009). Toward a multi-level, ecological approach to the primary prevention of sexual assault: Prevention in peer and community contexts. Trauma, Violence, & Abuse, 10(2), 91-114.
Casey, E., & Nurius, P. S. (2005). Trauma exposure and sexual revictimization risk: Comparisons across single, multiple incident, and multiple perpetrator victimizations. Violence Against Women, 11(4), 505-530.
Casteel, C., Martin, S. L., Smith, J. B., Gurka, K. K., & Kupper,
L. L. (2008). National study of physical and sexual assault among women with disabilities. Injury Prevention, 14(2), 87-90.
Cattaneo, L. B., & Goodman, L. A. (2005). Risk factors for reabuse in intimate partner violence a cross-disciplinary critical review. Trauma, Violence, & Abuse, 6(2), 141-175.
Chamberlain, L., & Levenson, R. (2012). Addressing intimate partner violence, reproductive and sexual coercion: A guide for obstetric, gynecologic and reproductive health care settings. Washington, DC: American College of Obstetricians and Gynecologists.
Chan, K. L. (2011). Correlates of childhood sexual abuse and intimate partner sexual victimization. Partner Abuse, 2(3), 365-381.
Chiu, G. R., Lutfey, K. E., Litman, H. J., Link, C. L., Hall, S. A., & McKinlay, J. B. (2013). Prevalence and overlap of childhood and adult physical, sexual, and emotional abuse: A descriptive analysis of results from the Boston Area Community Health (BACH) survey. Violence & Victims, 28(3), 381-402.
Christopher, F. S., & Pflieger, J. C. (2007). Sexual aggression: The dark side of sexuality in relationships. Annual Review of Sex Research, 18, 115-142.
Clark, H., & Quadara, A. (2010). Insights into sexual assault perpetration: Giving voice to victim/survivors’ knowledge. (Research report 18). Melbourne: Australian Institute of Family Studies.
Clark, H. (2007). Judging rape: Public attitudes and sentencing.. Melbourne: Australian Centre for the Study of Sexual Assault.
Classen, C. C., Palesh, O. G., & Aggarwal, R. (2005). Sexual revictimization: A review of the empirical literature. Trauma, Violence & Abuse, 6(2), 103-129.
Coid, J., Petruckevitch, A., Feder, G., Chung, W.-S., Richardson, J., & Moorey, S. (2001). Relation between childhood sexual and physical abuse and risk of revictimisation in women: A cross-sectional survey. The Lancet, 358(9280), 450-454.
Coker, A. L., Hopenhayn, C., DeSimone, C. P., Bush, H. M., & Crofford, L. (2009). Violence against women raises risk of cervical cancer. Journal of Women’s Health, 18(8), 1179-1185.
Coker, A. L., Sanderson, M., Cantu, E., Huerta, D., & Fadden, M. K. (2008). Frequency and types of partner violence among Mexican American college women. Journal of American College Health, 56(6), 665-673.
Cole, J., Logan, T., & Shannon, L. (2005). Intimate sexual victimization among women with protective orders: Types and associations of physical and mental health problems. Violence & Victims, 20(6), 695-715.
Conway, P., Cresswell, J., Harmon, D., Pospishil, C., Smith, K., Wages, J., & Weisz, L. (2010). Using empowerment evaluation to facilitate the development of intimate partner and sexual violence prevention programs. Journal of Family Social Work, 13(4), 343-361.
Cooper, L., Anaf, J., & Bowden, M. (2008). Can social workers and police be partners when dealing with bikie-gang related domestic violence and sexual assault? European Journal of Social Work, 11(3), 295-311.
Cornelius, T. L., & Resseguie, N. (2007). Primary and secondary prevention programs for dating violence: A review of the literature. Aggression and Violent Behavior, 12(3), 364-375.
Cortis, N. & Bullen, J. (2015). Building effective policies and services to promote women’s economic security following domestic violence: State of knowledge paper 7. Sydney: ANROWS.
Costello, M. (2005). The disappearing ‘F’ word: Feminism and Australian Government violence against women policies? Women Against Violence: An Australian Feminist Journal, 17, 41-50.
Coulter, M., & VandeWeerd, C. (2009). Reducing domestic violence and other criminal recidivism: Effectiveness of a multilevel batterers intervention program. Violence & Victims, 24(2), 139-152.
Cox, P. (2015). Violence against women: Additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey, 2012, (ANROWS Horizons 1). Sydney: ANROWS.
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241-1299.
Cripps, K. (2008). Indigenous family violence: A statistical challenge. Injury, 39, Supplement 5, S25-S35.
Cripps, K., & McGlade, H. (2008). Indigenous family violence and sexual abuse: Considering pathways forward. Journal of Family Studies, 14(2-3), 240-253.
Cripps, K., Miller, L. & Saxton-Barney, J. (2010). Too hard to handle: Indigenous victims of violence with disabilities. Indigenous Law Bulletin, 7(21), 3.
Crisp, A. H., Gelder, M. G., Rix, S., Meltzer, H. I., & Rowlands, O. J. (2000). Stigmatisation of people with mental illnesses. The British Journal of Psychiatry, 177(1), 4-7.
Cuevas, C. A., Sabina, C., & Milloshi, R. (2012). Interpersonal victimization among a national sample of Latino women. Violence Against Women, 18(4), 377-403.
Culbertson, K. A., & Dehle, C. (2001). Impact of sexual assault as a function of perpetrator type. Journal of Interpersonal Violence, 16(10), 992-1007.
Cyr, M., McDuff, P., & Wright, J. (2006). Prevalence and predictors of dating violence among adolescent female victims of child sexual abuse. Journal of Interpersonal Violence, 21(8), 1000-1017.
Daigneault, I., Hébert, M., & McDuff, P. (2009). Men’s and women’s childhood sexual abuse and victimization in adult partner relationships: A study of risk factors. Child Abuse & Neglect, 33(9), 638-647.
Daly, K. (2006). Restorative justice and sexual assault: An archival study of court and conference cases. British Journal of Criminology, 46(2), 334-356.
Daly, K., Bouhours, B., Broadhurst, R., & Loh, N. (2013). Youth sex offending, recidivism and restorative justice: Comparing court and conference cases. Australian & New Zealand Journal of Criminology, 46(2), 241-267.
Dardis, C. M., Edwards, K. M., Kelley, E. L., & Gidycz, C. A. (2013). Dating violence perpetration: The predictive roles of maternally versus paternally perpetrated childhood abuse and subsequent dating violence attitudes and behaviors. Journal of Aggression, Maltreatment & Trauma, 22(1), 6-25.
Davis, M. (2014). Law enforcement response to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.). Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Day, A., O’Leary, P., Chung, D., & Justo, D. (2009). Integrated responses to domestic violence: Research and practice experiences in working with men. In A. Day, L. Forsythe, & K. Adams (Eds.), Domestic violence: Working with men: Research, practice experiences and integrated responses. Annandale, NSW: Federation Press.
Decker, S. H., Spohn, C., Ortiz, N. R., & Hedberg, E. (2014). Criminal stigma, race, gender and employment: An expanded assessment of the consequences of imprisonment for employment. Washington: National Institute of Justice.
DeKeseredy, W. S., & Schwartz, M. D. (2008). Separation/ divorce sexual assault in rural Ohio: Survivors’ perceptions. Journal of Prevention & Intervention in the Community, 36(1/2), 105-119.
DeKeseredy, W. S., & Schwartz, M. D. (2001). Definitional issues. In C.M. Renzetti, J.L. Edleson & R.K. Bergen (Eds.). Sourcebook on violence against women (2nd ed.) (pp. 23-34). Thousand Oaks, CA: Sage.
DeKeseredy, W. S. (2014). Separation/divorce sexual assault. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.). Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
DeLisi, M., Caudill, J. W., & Trulson, C. R. (2014). Does childhood sexual abuse victimization translate into juvenile sexual offending? New evidence. Violence and Victims, 29(4), 620-635.
Desai, S. & Saltzman, L. (2001). Measurement issues for violece against women. In C.M. Renzetti, J.L. Edleson & R.K. Bergen (Eds.). Sourcebook on violence against women (2nd ed.) (pp. 35-52). Thousand Oaks, CA: Sage.
Dietrich, A. M., Smiley, W. C., & Frederick, C. (2007). The roles of childhood maltreatment and psychopathy in sexual recidivism of treated sex offenders. Journal of Aggression, Maltreatment & Trauma, 14(3), 19-31.
Dobash, R. P., & Dobash, R. E. (2004). Women’s violence to men in intimate relationships: Working on a puzzle. British Journal of Criminology, 44(3), 324-349.
Dobash, R. P., Dobash, R. E., Wilson, M., & Daly, M. (1992). The myth of sexual symmetry in marital violence. Social Problems, 39(1), 71-91.
Doroszewicz, K., & Forbes, G. B. (2008). Experiences with dating aggression and sexual coercion among Polish college students. Journal of Interpersonal Violence, 23(1), 58-73.
Dutton, M. A., & Goodman, L. A. (2005). Coercion in intimate partner violence: Toward a new conceptualization. Sex Roles, 52(11-12), 743-756.
Dutton, M. A., Kaltman, S., Goodman, L. A., Weinfurt, K., & Vankos, N. (2005). Patterns of intimate partner violence: Correlates and outcomes. Violence and Victims, 20(5), 483-497.
Easteal, P. (2014). Advice for criminal justice staff and/or advocates to aid intimate partner sexual violence survivors. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Eaton, A., & Matamala, A. (2014). The relationship between heteronormative beliefs and verbal sexual coercion in college students. Archives of Sexual Behavior, 43(7), 1443-1457.
Eaton, D. K., Kann, L., Kinchen, S., Shanklin, S., Flint, K. H., Hawkins, J., . . . Wechsler, H. (2012). Youth risk behavior surveillance – United States, 2011. Morbidity and Mortality Weekly Report. Surveillance Summaries, 61(SS04), 1-162.
Edwards, K. M., Sylaska, K. M., Barry, J. E., Moynihan, M. M., Banyard, V. L., Cohn, E. S., . . . Ward, S. K. (2015). Physical dating violence, sexual violence, and unwanted pursuit victimization: A comparison of incidence rates among sexual-minority and heterosexual college students. Journal of Interpersonal Violence, 30(4), 580-600.
El-Bassel, N., Gilbert, L., Wu, E., Chang, M., Gomes, C., Vinocur, D., & Spevack, T. (2007). Intimate partner violence prevalence and HIV risks among women receiving care in emergency departments: Implications for IPV and HIV screening. Emergency Medicine Journal, 24(4), 255-259.
Ellison, L. (2010). Commentary on R v A (No 2). In R. Hunter, C. McGlynn & E. Rackley (Eds.). Feminist judgments: From theory to practice (pp. 206-210). Oxford: Hart Publishing.
Fang, X., & Corso, P. S. (2008). Gender differences in the connections between violence experienced as a child and perpetration of intimate partner violence in young adulthood. Journal of Family Violence, 23(5), 303-313.
Fargo, J. D. (2009). Pathways to adult sexual revictimization: Direct and indirect behavioral risk factors across the lifespan. Journal of Interpersonal Violence, 24(11), 1771-1791.
Feerick, C., & Easteal, P. W. (2005). Sexual assault by male partners: Is the licence still valid? Flinders Journal of Law Reform, 8(2), 185-207.
Feiring, C., Simon, V. A., Cleland, C. M., & Barrett, E. P. (2013). Potential pathways from stigmatization and externalizing behavior to anger and dating aggression in sexually abused youth. Journal of Clinical Child & Adolescent Psychology, 42(3), 309-322.
Felson, R. B., & Pare, P.-P. (2007). Does the criminal justice system treat domestic violence and sexual assault offenders leniently? JQ: Justice Quarterly, 24(3), 435-459.
Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2006). Examining the intergenerational transmission of violence in a New Zealand birth cohort. Child Abuse& Neglect, 30(2), 89-108.
Ferro, C., Cermele, J & Saltzman, A. (2008). Current perceptions of marital rape: Some good and some not-so-good news. Journal of Interpersonal Violence , 23(6), 764-779.
Filipas, H. H., & Ullman, S. E. (2006). Child sexual abuse, coping responses, self-blame, posttraumatic stress disorder, and adult sexual revictimization. Journal of Interpersonal Violence, 21(5), 652-672.
Finkelhor, D., & Yllö, K. (1987). License to rape: Sexual abuse of wives. New York: Holt, Rinehart and Winston.
Fisher, B. S., Daigle, L. E., Cullen, F. T., & Turner, M. G. (2003). Reporting sexual victimization to the police and others results from a national-level study of college women. Criminal Justice and Behavior, 30(1), 6-38.
Fitzgerald, J. (2008). Does circle sentencing reduce Aboriginal offending? Sydney: NSW Bureau of Crime Statistics and Research.
Flanagan, J. C., Jaquier, V., Gordon, K. C., Moore, T. M., & Stuart, G. L. (2014). Examining the prevalence, bidirectionality, and co-occurrence of sexual intimate partner violence among women during pregnancy and postpartum. Partner Abuse, 5(4), 407-419.
Flicker, S. M., Cerulli, C., Zhao, X., Tang, W., Watts, A., Xia, Y., & Talbot, N. L. (2011). Concomitant forms of abuse and help-seeking behavior among white, African American, and Latina women who experience intimate partner violence. Violence Against Women, 17(8), 1067-1085.
Flood, M. G., & Kendrick, V. (2012). “LOVEBiTES: Anevaluation of the LOVEBiTES and respectful relationships programs in a Sydney school”. Wollongong: University of Wollongong.
Follette, V. M., Polusny, M. A., Bechtle, A. E., & Naugle, A. E. (1996). Cumulative trauma: The impact of child sexual abuse, adult sexual assault, and spouse abuse. Journal of Traumatic Stress, 9(1), 25-35.
Foshee, V. A., Bauman, K. E., Linder, F., Rice, J., & Wilcher, R. (2007). Typologies of adolescent dating violence: Identifying typologies of adolescent dating violence perpetration. Journal of Interpersonal Violence, 22(5), 498-519.
Fotheringham, S., & Tomlinson, D. (2009). Identifying the potential for collaboration between women’s shelters and sexual assault centres: Comparing and contrasting the service delivery needs of clients. Currents, 8(1).
Freedner, N., Freed, L. H., Yang, Y. W., & Austin, S. B. (2002). Dating violence among gay, lesbian, and bisexual adolescents: Results from a community survey. Journal of Adolescent Health, 31(6), 469-474.
Friedman, M. J., Jalowiec, J., McHugo, G., Wang, S., & McDonagh, A. (2007). Adult sexual abuse is associated with elevated neurohormone levels among women with PTSD due to childhood sexual abuse. Journal of Traumatic Stress, 20(4), 611-617.
Friesen, M. D., Woodward, L. J., Horwood, L. J., & Fergusson, D. M. (2010). Childhood exposure to sexual abuse and partnership outcomes at age 30. Psychological Medicine, 40(4), 679-688.
Gagné, M.-H., Lavoie, F., & Hébert, M. (2005). Victimization during childhood and revictimization in dating relationships in adolescent girls. Child Abuse & Neglect, 29(10), 1155-1172.
Gallagher, K. E., Hudepohl, A. D., & Parrott, D. J. (2010). Power of being present: The role of mindfulness on the relation between men’s alcohol use and sexual aggression toward intimate partners. Aggressive Behavior, 36(6), 405-413.
Garcia-Linares, M. I., Pico-Alfonso, M. A., & Sanchez-Lorente, S. (2005). Assessing physical, sexual, and psychological violence perpetrated by intimate male partners toward women: A Spanish cross-sectional study. Violence and Victims, 20(1), 99-123.
Gibson, L. E., & Leitenberg, H. (2001). The impact of child sexual abuse and stigma on methods of coping with sexual assault among undergraduate women. Child Abuse & Neglect, 25(10), 1343-1361.
Gobin, R. L., Iverson, K. M., Mitchell, K., Vaughn, R., & Resick, P. A. (2013). The impact of childhood maltreatment on PTSD symptoms among female survivors of intimate partner violence. Violence and Victims, 28(6), 984-999.
Goldscheid, J. (2006). Domestic and sexual violence as sex discrimination: Comparing American and international approaches. Thomas Jefferson Law Review, 28(3), 355-397.
Goodlin, W. E., & Dunn, C. S. (2010). Three patterns of domestic violence in households: Single victimization, repeat victimization, and co-occurring victimization. Journal of Family Violence, 25(2), 107-122.
Green, B. L., Krupnick, J. L., Stockton, P., Goodman, L., Corcoran, C., & Petty, R. (2005). Effects of adolescent trauma exposure on risky behavior in college women. Psychiatry, 68(4), 363-378.
Griffing, S., Ragin, D. F., Morrison, S. M., Sage, R. E., Madry, L., & Primm, B. J. (2005). Reasons for returning to abusive relationships: Effects of prior victimization. Journal of Family Violence, 20(5), 341-348.
Guerrero, D. (2009). Hypermasculinity, intimate partner violence, sexual aggression, social support, and child maltreatment risk in urban, heterosexual fathers taking parenting classes. Child Welfare, 88(4), 135-155.
Hamby, S. (2014). Intimate partner and sexual violence research scientific progress, scientific challenges, and gender. Trauma, Violence, & Abuse, 15(3), 149-158.
Hamby, S., & Turner, H. (2013). Measuring teen dating violence in males and females: Insights from the national survey of children’s exposure to violence. Psychology of Violence, 3(4), 323-339.
Hattery, A. J. (2009). Sexual abuse in childhood: Intimate partner violence in adulthood – struggles for African American and white women. Race, Gender & Class, 16(1-2), 194-217.
Hazen, A. L., & Soriano, F. I. (2007). Experiences with intimate partner violence among Latina women. Violence Against Women, 13(6), 562-582.
Hébert, M., Lavoie, F., Vitaro, F., McDuff, P., & Tremblay, R. E. (2008). Association of child sexual abuse and dating victimization with mental health disorder in a sample of adolescent girls. Journal of Traumatic Stress, 21(2), 181-189.
Heenan, M. (2004). Just “keeping the peace”: A reluctance to respond to male partner sexual violence. Melbourne: Australian Institute of Family Studies.
Hegarty, K., Bush, R., & Sheehan, M. (2005). The composite abuse scale: Further development and assessment of reliability and validity of a multidimensional partner abuse measure in clinical settings. Violence and Victims, 20(5), 529-547.
Hegarty, K., Hindmarsh, E. D., & Gilles, M. T. (2000). Domestic violence in Australia: Definition, prevalence and nature of presentation in clinical practice. Medical Journal of Australia, 173(7), 363-367.
Hegarty, K., & Roberts, G. (1998). How common is domestic violence against women? The definition of partner abuse in prevalence studies. Australian and New Zealand Journal of Public Health, 22(1), 49-54.
Heise, L. L. (1998). Violence against women an integrated, ecological framework. Violence Against Women, 4(3), 262-290.
Herman, J. (2009). There’s a fine line…: Adolescent dating violence and prevention. Pediatric Nursing, 35(3).
Herz, D. C., Stroshine, M., & Houser, K. (2005). Exploring agreement on appropriate responses to domestic violence and sexual trauma across victim advocates, mental health service providers, and substance abuse treatment providers. Women & Criminal Justice, 16(4), 119-144.
Hess, K. L., Javanbakht, M., Brown, J. M., Weiss, R. E., Hsu, P., & Gorbach, P. M. (2013). Intimate partner violence and anal intercourse in young adult heterosexual relationships. Perspectives on Sexual & Reproductive Health, 45(1), 6-12.
Hetzel, M. D., & McCanne, T. R. (2005). The roles of peritraumatic dissociation, child physical abuse, and child sexual abuse in the development of posttraumatic stress disorder and adult victimization. Child Abuse & Neglect, 29(8), 915-930.
Hickson, L., Khemka, I., Golden, H., & Chatzistyli, A. (2013). Views and values of developmental disabilities and domestic violence/sexual assault support professionals regarding the prevention and handling of situations of abuse. Journal of Policy & Practice in Intellectual Disabilities, 10(3), 207-214.
Hill, J. M., Vernig, P. M., Lee, J. K., Brown, C., & Orsillo, S. M. (2011). The development of a brief acceptance and mindfulness- based program aimed at reducing sexual revictimization among college women with a history of childhood sexual abuse. Journal of Clinical Psychology, 67(9), 969-980.
Holleran, D., Beichner, D., & Spohn, C. (2010). Examining charging agreement between police and prosecutors in rape cases. Crime & Delinquency, 56(3), 385-413.
Holtzworth-Munroe, A. (2005). Female perpetration of physical aggression against an intimate partner: A controversial new topic of study. Violence and Victims, 20(2), 251-259.
Holtzworth-Munroe, A., Meehan, J. C., Herron, K., Rehman, U., & Stuart, G. L. (2000). Testing the Holtzworth-Munroe and Stuart (1994) batterer typology. Journal of Consulting and Clinical Psychology, 68(6), 1000.
Hovane, V. (2007). White privilege and the fiction of colour blindness: Implications for best practice standards for Aboriginal victims of family violence. Sydney: Australian Domestic and Family Violence Clearinghouse.
Hovane, V. (2015). Our story to tell: Aboriginal perspectives on domestic and family violence. ANROWS Footprints, 1, 13-17.
Howard, D. E., Wang, M. Q., & Yan, F. (2007). Prevalence and psychosocial correlates of forced sexual intercourse among US high school adolescents. Adolescence, 42(168), 629-643.
Hunnicutt, G. (2009). Varieties of patriarchy and violence against women: Resurrecting “patriarchy” as a theoretical tool. Violence Against Women, 15(5), 553-573.
Ireland, T. O., & Smith, C. A. (2009). Living in partner- violent families: Developmental links to antisocial behavior and relationship violence. Journal of Youth and Adolescence, 38(3), 323-339.
Iverson, K., Gradus, J. L., Resick, P. A., Suvak, M. K., Smith, K. F., & Monson, C. M. (2011). Cognitive–behavioral therapy for PTSD and depression symptoms reduces risk for future intimate partner violence among interpersonal trauma survivors. Journal of Consulting and Clinical Psychology, 79(2), 193.
Iverson, K., Mercado, R., Carpenter, S. L., & Street, A. E. (2013). Intimate partner violence among women veterans: Previous interpersonal violence as a risk factor. Journal of Traumatic Stress, 26(6), 767-771.
Jankowski, M. K., Leitenberg, H., Henning, K., & Coffey, P. (2002). Parental caring as a possible buffer against sexual revictimization in young adult survivors of child sexual abuse. Journal of Traumatic Stress, 15(3), 235-244.
Jason, P., Hubbard, P., & Birch, P. (2013). Sex worker victimization, modes of working, and location in New South Wales, Australia: A geography of victimization. The Journal of Sex Research, 50(6), 574-586.
Jennings, W. G., Zgoba, K. M., Maschi, T., & Reingle, J. M. (2014). An empirical assessment of the overlap between sexual victimization and sex offending. International Journal of Offender Therapy & Comparative Criminology, 58(12), 1466-1480.
Johnson, H. (2005). Assessing the prevalence of violence against women in Canada. Statistical Journal of the UN Economic Commission for Europe, 22(3/4), 225-238.
Johnson, M. P. (2006). Conflict and control gender symmetry and asymmetry in domestic violence. Violence Against Women, 12(11), 1003-1018.
Johnson, I. M. (2014). Economic impediments to women’s success on parole: “We need someone on our side”. The Prison Journal, 94(3), 365-387.
Katz, J., Moore, J., & May, P. (2008). Physical and sexual co victimization from dating partners: A distinct type of intimate abuse? Violence Against Women, 14(8), 961-980.
Keel, M. (2004). Family violence and sexual assault in Indigenous communities: “Walking the talk” (ACSSA Briefing No 4). Melbourne: Australian Institute of Family Studies.
Kelly, L. (2013). Surviving sexual violence. Cambridge: John Wiley & Sons.
Kelly, T. C., & Stermac, L. (2012). Intimate partner sexual assault against women: Examining the impact and recommendations for clinical practice. Partner Abuse, 3(1), 107-122.
Kelly, U. A., Skelton, K., Patel, M., & Bradley, B. (2011). More than military sexual trauma: Interpersonal violence, PTSD, and mental health in women veterans. Research in Nursing & Health, 34(6), 457-467.
Kennedy, A., Adams, A., Bybee, D., Campbell, R., Kubiak, S., & Sullivan, C. (2012). A model of sexually and physically victimized women’s process of attaining effective formal help over time: The role of social location, context, and intervention. American Journal of Community Psychology, 50(1/2), 217-228.
Kernsmith, P. (2006). Gender differences in the impact of family of origin violence on perpetrators of domestic violence. Journal of Family Violence, 21(2), 163-171.
Kerr, I. (2014). Counseling and advocacy perspectives on intimate partner sexual violence. In L. McOrmond Plummer,
J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Kilpatrick, D. G., Resnick, H. S., Ruggiero, K. J., Conoscenti, L. M., & McCauley, J. (2007). Drug-facilitated, incapacitated, and forcible rape: A national study. Charlston, SC: Medical University of South Carolina, National Crime Victims Research & Treatment Center.
Kilroy, D. (2014). Effective approaches to helping intimate partner sexual violence survivors in prison. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Kim-Godwin, Y. S., Clements, C., McCuiston, A., & Fox, J.A. (2009). Dating violence among high school students in southeastern North Carolina. The Journal of School Nursing, 25(2), 141-151.
The Kirby Institute. (2015). HIV, viral hepatitis and sexually transmissible infections in Australia Annual Surveillance Report 2015. Sydney: UNSW.
Kitzmann, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witnesses to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339.
Koopman, C., Ismailji, T., Palesh, O., Gore-Felton, C., Narayanan, A., Saltzman, K. M., . . . McGarvey, E. L. (2007). Relationships of depression to child and adult abuse and bodily pain among women who have experienced intimate partner violence. Journal of Interpersonal Violence, 22(4), 438-455.
Koss, M. P., Abbey, A., Campbell, R., Cook, S., Norris, J., Testa, M., . . . White, J. (2007). Revising the SES: A collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly, 31(4), 357-370.
Krebs, C., Breiding, M. J., Browne, A., & Warner, T. (2011). The association between different types of intimate partner violence experienced by women. Journal of Family Violence, 26(6), 487-500.
Krug, E. G., Mercy, J. A., Dahlberg, L. L., & Zwi, A. B. (2002). The world report on violence and health. The Lancet, 360(9339), 1083-1088.
Lacey, K. K., McPherson, M. D., Samuel, P. S., Powell Sears, K., & Head, D. (2013). The impact of different types of intimate partner violence on the mental and physical health of women in different ethnic groups. Journal of Interpersonal Violence, 28(2), 359-385.
Lalande, K. M., & Bonanno, G. A. (2011). Retrospective memory bias for the frequency of potentially traumatic events: A prospective study. Psychological Trauma: Theory, Research, Practice, and Policy, 3(2), 165-170.
Langley, J., Martin, J., & Nada-Raja, S. (1997). Physical assault among 21-year-olds by partners. Journal of Interpersonal Violence, 12(5), 675-684.
Larcombe, W., & Heath, M. (2012). Developing the common law and rewriting the history of rape in marriage in Australia: PGA v The Queen. Sydney Law Review, 34, 785-809.
Lawless, S., Kippax, S., & Crawford, J. (1996). Dirty, diseased and undeserving: The positioning of HIV positive women. Social Science & Medicine, 43(9), 1371-1377.
Lawrie, R. (2003). Speak out speak strong: Rising imprisonment rates of Aboriginal women. Indigenous Law Bulletin, 5(24), 5-7.
Lazar, R. (2010). Negotiating sex: The legal construct of consent in cases of wife rape in Ontario, Canada. Canadian Journal of Women and the Law, 22(2), 329-363.
Lehrer, J. A., Lehrer, E. L., & Koss, M. P. (2013). Unwanted sexual experiences in young men: Evidence from a survey of university students in Chile. Archives of Sexual Behavior, 42(2), 213-223.
Levy-Peck, J. (2014a). Addressing intimate partner sexual violence in teen relationships. In L. McOrmond Plummer,
J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers..
Levy-Peck, J. (2014b). The role of the advocate in addressing intimate partner sexual violence. In L. McOrmond Plummer,
J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Liang, B., Goodman, L., Tummala-Narra, P., & Weintraub, S. (2005). A theoretical framework for understanding help- seeking processes among survivors of intimate partner violence. American Journal of Community Psychology, 36(1-2), 71-84.
Lichtenstein, B. (2005). Domestic violence, sexual ownership, and HIV risk in women in the American deep south. Social Science & Medicine, 60(4), 701-714.
Lichty, L. F., Campbell, R., & Schuiteman, J. (2008). Developing a university-wide institutional response to sexual assault and relationship violence. Journal of Prevention & Intervention in the Community, 36(1/2), 5-22.
Liles, S., Usita, P., Irvin, V., Hofstetter, C., Beeston, T., & Hovell, M. (2012). Prevalence and correlates of intimate partner violence among young, middle, and older women of Korean descent in California. Journal of Family Violence, 27(8), 801-811.
Littleton, H. (2014). Interpersonal violence on college campuses: Understanding risk factors and working to find solutions. Trauma, Violence & Abuse, 15(4), 297-303.
Littleton, H., Breitkopf, C. R., & Berenson, A. (2008). Beyond the campus: Unacknowledged rape among low-income women. Violence Against Women, 14(3), 269-286.
Lloyd, S. A., & Emery, B. C. (1999). The dark side of courtship: Physical and sexual aggression. Thousand Oaks: Sage Publications.
Logan, T. (2009). The Kentucky Civil Protective Order Study: A rural and urban multiple perspective study of protective order violation consequences, responses and costs. Lexington: University of Kentucky, Department of Behavioral Science.
Logan, T., & Cole, J. (2011). Exploring the intersection of partner stalking and sexual abuse. Violence Against Women, 17(7), 904-924.
Logan, T., Cole, J. R., & Shannon, L. A. (2007). A mixed- methods examination of sexual coercion and degradation among women in violent relationships who do and do not report forced sex. Violence and Victims, 22(1), 71-94.
Logan, T., Walker, R., & Cole, J. (2013). Silenced suffering: The need for a better understanding of partner sexual violence. Trauma, Violence, & Abuse, 16, 111-135.
Long, J. M. (2009). Intimate partner sexual assault. In Washington Coalition of Sexual Assault Programs (Ed.), Intimate partner sexual violence: Sexual assault in the context of domestic violence. Olympia, WA: Washington Coalition of Sexual Assault Programs.
Ludermir, A. B., Schraiber, L. B., D’Oliveira, A. F. P. L., França- Junior, I., & Jansen, H. A. (2008). Violence against women by their intimate partner and common mental disorders. Social Science & Medicine, 66(4), 1008-1018.
Lutz-Zois, C. J., Phelps, C. E. R., & Reichle, A. C. (2011). Affective, behavioral, and social-cognitive dysregulation as mechanisms for sexual abuse revictimization. Violence and Victims, 26(2), 159-176.
Maas-DeSpain, A., & Todahl, J. L. (2014). Rape, sexual violence, and acquiescence in intimate relationships: Screening, assessment, and clinical decision making. Journal of Feminist Family Therapy, 26(1), 28-49.
Macleod, D. (2014a). Fatality and health risks associated with intimate partner sexual sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Macleod, D. (2014b). Real not rare: Cross-training for sexual assault and domestic violence workers to understand, recognize, and respond to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Macy, R. J. (2007). Sexual revictimization: Implications for social work practice. Families in Society, 88(4), 627-636.
Macy, R. J., Giattina, M., Sangster, T. H., Crosby, C., & Montijo, N. J. (2009). Domestic violence and sexual assault services: Inside the black box. Aggression & Violent Behavior, 14(5), 359-373.
Macy, R. J., Giattina, M. C., Montijo, N. J., & Ermentrout, D. M. (2010). Domestic violence and sexual assault agency directors’ perspectives on services that help survivors. Violence Against Women, 16(10), 1138-1161.
Macy, R. J., Giattina, M. C., Parish, S. L., & Crosby, C. (2010). Domestic violence and sexual assault services: Historical concerns and contemporary challenges. Journal of Interpersonal Violence, 25(1), 3-32.
Macy, R. J., Johns, N., Rizo, C. F., Martin, S. L., & Giattina, M. (2011). Domestic violence and sexual assault service goal priorities. Journal of Interpersonal Violence, 26(16), 3361-3382.
Magdol, L., Moffitt, T. E., Caspi, A., Newman, D. L., Fagan, J., & Silva, P. A. (1997). Gender differences in partner violence in a birth cohort of 21-year-olds: Bridging the gap between clinical and epidemiological approaches. Journal of Consulting and Clinical Psychology, 65(1), 68.
Mallie, A. L., Viljoen, J. L., Mordell, S., Spice, A., & Roesch, R. (2011). Childhood abuse and adolescent sexual re-offending: A meta-analysis. Child & Youth Care Forum, 40(5), 401-417.
Martin, E., Taft, C. T., & Resick, P. A. (2007). A review of marital rape. Aggression & Violent Behavior, 12(3), 329-347.
Martin, S. L., Coyne-Beasley, T., Hoehn, M., Mathew, M., Runyan, C. W., Orton, S., & Royster, L.-A. (2009). Primary prevention of violence against women. Violence Against Women, 15(1), 44-56.
Mathes, E. (2013). Why is there a strong positive correlation between perpetration and being a victim of sexual coercion? An exploratory study. Journal of Family Violence, 28(8), 783-796.
McAlinden, A. (2008). Restorative justice as a response to sexual offending: Addressing the failings of current punitive approaches. Sexual Offender Treatment, 3(1), 1-12.
McFarlane, J. (2007). Pregnancy following partner rape: What we know and what we need to know. Trauma, Violence & Abuse, 8(2), 127-134.
McFarlane, J., Malecha, A., Gist, J., Watson, K., Batten, E., Hall, I., & Smith, S. (2005). Intimate partner sexual assault against women and associated victim substance use, suicidality, and risk factors for femicide. Issues in Mental Health Nursing, 26(9), 953-967.
McFarlane, J., Malecha, A., Watson, K., Gist, J., Batten, E., Hall, I., & Smith, S. (2005). Intimate partner sexual assault against women: Frequency, health consequences, and treatment outcomes. Obstetrics & Gynecology, 105(1), 99-108.
McGlynn, C. (2010). R v A (No 2) Judgment. In R. Hunter, C. McGlynn & E. Rackley (Ed.), Feminist judgments: From theory to practice (pp. 211-227). Oxford: Hart Publishing.
McLean, R., & Goodman-Delahunty, J. (2008). The influence of relationship and physical evidence on police decision- making in sexual assault cases. Australian Journal of Forensic Sciences, 40(2), 109-121.
McOrmond-Plummer, L. (2014). Preventing secondary wounding by misconception: What professionals really need to know about intimate partner sexual violence. In
L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
McOrmond-Plummer. (2009). Considering the differences: Intimate partner sexual violence in sexual assault and domestic violence discourse. In Washington Coalition of Sexual Assault Programs (Ed.), Intimate partner sexual violence: Sexual assault in the context of domestic violence. Olympia, WA: Washington Coalition of Sexual Assault Programs.
McOrmond-Plummer, L., Easteal, P. & Levy-Peck, J.Y. (2014). The necessity of appropriate service response to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Meade, C. S., Kershaw, T. S., Hansen, N. B., & Sikkema, K. J. (2009). Long-term correlates of childhood abuse among adults with severe mental illness: Adult victimization, substance abuse, and HIV sexual risk behavior. AIDS and Behavior, 13(2), 207-216.
Ménard, K. S., & Pincus, A. L. (2014). Child maltreatment, personality pathology, and stalking victimization among male and female college students. Violence and Victims, 29(2), 300-316.
Messing, J. T., Thaller, J., & Bagwell, M. (2014). Factors related to sexual abuse and forced sex in a sample of women experiencing police-involved intimate partner violence. Health & Social Work, 39(3), 181.
Messinger, A. M. (2011). Invisible victims: Same-sex IPV in the national violence against women survey. Journal of Interpersonal Violence, 26(11), 2228-2243.
Messman-Moore, T. L., & Long, P. J. (2003). The role of childhood sexual abuse sequelae in the sexual revictimization of women: An empirical review and theoretical reformulation. Clinical Psychology Review, 23(4), 537-571.
Messman-Moore, T. L., Long, P. J., & Siegfried, N. J. (2000). The revictimization of child sexual abuse survivors: An examination of the adjustment of college women with child sexual abuse, adult sexual assault, and adult physical abuse. Child Maltreatment, 5(1), 18-27.
Messman-Moore, T. L., Walsh, K. L., & DiLillo, D. (2010). Emotion dysregulation and risky sexual behavior in revictimization. Child Abuse & Neglect, 34(12), 967-976.
Messman-Moore, T. L., Ward, R. M., & Brown, A. L. (2009). Substance use and PTSD symptoms impact the likelihood of rape and revictimization in college women. Journal of Interpersonal Violence, 24(3), 499-521.
Miller, D. (2006). The effects of childhood physical abuse or childhood sexual abuse in battered women’s coping mechanisms: Obsessive-compulsive tendencies and severe depression. Journal of Family Violence, 21(3), 185-195.
Miller, E., Breslau, J., Chung, W. J. J., Green, J. G., McLaughlin, K. A., & Kessler, R. C. (2011). Adverse childhood experiences and risk of physical violence in adolescent dating relationships. Journalof Epidemiology & Community Health, 65(11), 1006-1013.
Miller, G., Chen, E., & Zhou, E. S. (2007). If it goes up, must it come down? Chronic stress and the hypothalamic- pituitary-adrenocortical axis in humans. Psychological Bulletin, 133(1), 25.
Miller, J. (2006). A specification of the types of intimate partner violence experienced by women in the general population. Violence Against Women, 12(12), 1105-1131.
Mitchell, L. (2011). Domestic violence in Australia: An overview of the issues. Canberra: Parliamentary Library.
Möller, A. S., Bäckström, T., Söndergaard, H. P., & Helström, L. (2012). Patterns of injury and reported violence depending on relationship to assailant in female Swedish sexual assault victims. Journal of Interpersonal Violence, 27(16), 3131-3148.
Monson, C. M., & Langhinrichsen-Rohling, J. (1999). Sexual and nonsexual marital aggression: Legal considerations, epidemiology, and an integrated typology of perpetrators. Aggression and Violent Behavior, 3(4), 369-389.
Montoya, T., Coker-Appiah, D. S., Eng, E., Wynn, M. R., & Townsend, T. G. (2013). A qualitative exploration of rural African American youth perceptions about the effect of dating violence on sexual health. Journal of Child & Family Studies, 22(1), 48-62.
Moore, E. (2002). Not just court: Family violence in rural New South Wales: Aboriginal women speak out. Wagga Wagga: Centre for Rural Social Research.
Morash, M., Bui, H., Zhang, Y., & Holtfreter, K. (2007). Risk factors for abusive relationships: A study of Vietnamese American immigrant women. Violence Against Women, 13(7), 653-675.
Moreau, C., Boucher, S., Hébert, M., & Lemelin, J. (2015). Capturing sexual violence experiences among battered women using the revised sexual experiences survey and the revised conflict tactics scales. Archives of Sexual Behavior, 44(1), 223-231.
Morokoff, P. J., Redding, C. A., Harlow, L. L., Cho, S., Rossi, J. S., Meier, K. S., . . . Brown‐Peterside, P. (2009). Associations of sexual victimization, depression, and sexual assertiveness with unprotected sex: A test of the multifaceted model of HIV risk across gender. Journal of Applied Biobehavioral Research, 14(1), 30-54.
Mouzos, J., & Makkai, T. (2004). Women’s experiences of male violence: Findings from the Australian component of the International Violence Against Women Survey (IVAWS) (Research and Public Policy No 56). Canberra: Australian Institute of Criminology Canberra.
Moynihan, M. M., Banyard, V. L., Arnold, J. S., Eckstein, R. P., & Stapleton, J. G. (2010). Engaging intercollegiate athletes in preventing and intervening in sexual and intimate partner violence. Journal of American College Health, 59(3), 197-204.
Moynihan, M. M., Banyard, V. L., Arnold, J. S., Eckstein, R. P., & Stapleton, J. G. (2011). Sisterhood may be powerful for reducing sexual and intimate partner violence: An evaluation of the Bringing in the Bystander in-person program with sorority members. Violence Against Women, 17(6), 703-719.
Murphy, L. M. (2011). Childhood and adolescent violent victimization and the risk of young adult intimate partner violence victimization. Violence and Victims, 26(5), 593-607.
National Coalition of Anti-violence Programs. (2014). 2013 Report on lesbian, gay, bisexual, transgender, queer, and HIV-affected intimate partner violence. New York: National Coalition of Anti-violence Programs.
Nelson, A., Lewy, R., Ricardo, F., Dovydaitis, T., Hunter, A., Mitchell, A., . . . Kugel, C. (2010). Eliciting behavior change in a US sexual violence and intimate partner violence prevention program through utilization of Freire and discussion facilitation. Health Promotion International, 25(3), 299-308.
Niehaus, A. F., Jackson, J., & Davies, S. (2010). Sexual self- schemas of female child sexual abuse survivors: Relationships with risky sexual behavior and sexual assault in adolescence. Archives of Sexual Behavior, 39(6), 1359-1374.
Nisbet, I., Wilson, P., & Smallbone, S. (2004). A prospective longitudinal study of sexual recidivism among adolescent sex offenders. Sexual Abuse: A Journal of Research and Treatment, 16(3), 223-234.
Noonan, R. K., & Charles, D. (2009). Developing teen dating violence prevention strategies. Violence Against Women, 15(9), 1087-1105.
Northern Territory. Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse. (2007). Report of the Northern Territory Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse. Darwin: Department of the Chief Minister.
Oktay, J. S., & Tompkins, C. J. (2004). Personal assistance providers’ mistreatment of disabled adults. Health & Social Work, 29(3), 177-188.
Orchowski, L., & Gidycz, C. A. (2012). To whom do college women confide following sexual assault? A prospective study of predictors of sexual assault disclosure and social reactions. Violence Against Women, 18(3), 264-288.
Orchowski, L., Untied, A., & Gidycz, C. (2013). Factors associated with college women’s labeling of sexual victimization. Violence and Victims, 28(6), 940-958.
Orcutt, H. K., Cooper, M. L., & Garcia, M. (2005). Use of sexual intercourse to reduce negative affect as a prospective mediator of sexual revictimization. Journal of Traumatic Stress, 18(6), 729-739.
Palmer, C., & Parekh, V. (2014). Medical indicators and responses to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Palmetto, N., Davidson, L. L., Breitbart, V., & Rickert, V. I. (2013). Predictors of physical intimate partner violence in the lives of young women: Victimization, perpetration, and bidirectional violence. Violence and Victims, 28(1), 103-121.
Panchanadeswaran, S., Frye, V., Nandi, V., Galea, S., Vlahov, D., & Ompad, D. (2010). Intimate partner violence and consistent condom use among drug-using heterosexual women in New York City. Women & Health, 50(2), 107-124.
Panuzio, J., & Dilillo, D. (2010). Physical, psychological, and sexual intimate partner aggression among newlywed couples: Longitudinal prediction of marital satisfaction. Journal of Family Violence, 25(7), 689-699.
Parekh, V., & Williams, A. (2014). Forensic medical assessment in intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Parkinson, D., & Reid, S. (2014). “Invisible” intimate partner sexual violence: Prevention and intervention challenges. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Parkinson, D., & Zara, C. (2014). Issues faced by intimate partner sexual violence survivors in rural areas. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Patriquin, M. A., Wilson, L. C., Kelleher, S. A., & Scarpa, A. (2012). Psychophysiological reactivity to abuse-related stimuli in sexually revictimized women. Journal of Aggression, Maltreatment & Trauma, 21(7), 758-775.
Pease, B. (2014). Theorising men’s violence prevention policies. In N. Henry, & A. Powell (Eds.), Preventing sexual violence: Interdisciplinary approaches to overcoming a rape culture. London: Palgrave Macmillan.
Pease, B. (2008). Engaging men in men’s violence prevention: Exploring the tensions, dilemmas and possibilities. Australian Domestic & Family Violence Clearinghouse, (17), 1-20.
Pereda, N., & Gallardo-Pujol, D. (2014). One hit makes the difference: The role of polyvictimization in childhood in lifetime revictimization on a southern European sample. Violence and Victims, 29(2), 217-231.
Peterson, G. W., & Bush, K. R. (Eds.). Handbook of marriage and the family (3rd ed.). New York: Springer Science+Business.
Pico-Alfonso, M. A., Garcia-Linares, M. I., Celda-Navarro, N., Blasco-Ros, C., Echeburúa, E., & Martinez, M. (2006). The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: Depressive symptoms, posttraumatic stress disorder, state anxiety, and suicide. Journal of Women’s Health, 15(5), 599-611.
Plummer, S.-B., & Findley, P. A. (2012). Women with disabilities’ experience with physical and sexual abuse: Review of the literature and implications for the field. Trauma, Violence & Abuse, 13(1), 15-29.
Poister Tusher, C., & Cook, S. L. (2010). Comparing revictimization in two groups of marginalized women. Journal of Interpersonal Violence, 25(10), 1893-1911.
Potito, C., Day, A., Carson, E., & O’Leary, P. (2009). Domestic violence and child protection: Partnerships and collaboration. Australian Social Work, 62(3), 369-387.
Potter, S. J., Fountain, K., & Stapleton, J. G. (2012). Addressing sexual and relationship violence in the LGBT community using a bystander framework. Harvard Review of Psychiatry, 20(4), 201-208.
Productivity Commission. (2009). Overcoming Indigenous disadvantage: Key indicators 2009. Canberra: Steering Committee for the Review of Government Service Provision.
Próspero, M., & Vohra-Gupta, S. (2008). The use of mental health services among victims of partner violence on college campuses. Journal of Aggression, Maltreatment & Trauma, 16(4), 376-390.
Quadara, A., Stathopoulos, M., & Jenkinson, R. (2015). Establishing the connection (between alcohol and other drug use and sexual victimisation): State of knowledge paper. ANROWS Landscapes, 6.
Raj, A., Rose, J., Decker, M. R., Rosengard, C., Hebert, M. R., Stein, M., & Clarke, J. G. (2008). Prevalence and patterns of sexual assault across the life span among incarcerated women. Violence Against Women, 14(5), 528-541.
Ramisetty-Mikler, S., Caetano, R., & McGrath, C. (2007). Sexual aggression among white, black, and Hispanic couples in the US: Alcohol use, physical assault and psychological aggression as its correlates. The American Journal of Drug and Alcohol Abuse, 33(1), 31-43.
Ranjbar, V., & Speer, S. A. (2013). Revictimization and recovery from sexual assault: Implications for health professionals. Violence and Victims, 28(2), 274-287.
Raphael, J., & Logan, T. (2009). The use (and misuse) of data on rape: Understanding the rape denial campaign in America: Part I. Sexual Assault Reports, 13(1), 1-16.
Reckdenwald, A., Mancini, C., & Beauregard, E. (2013). The cycle of violence: Examining the impact of maltreatment early in life on adult offending. Violence and Victims, 28(3), 466-482.
Rees, S., & Pease, B. (2007). Domestic violence in refugee families in Australia. Journal of Immigrant & Refugee Studies, 5(2), 1-19.
Rees, S., Silove, D., Chey, T., Ivancic, L., Steel, Z., Creamer, M., . . . Forbes, D. (2011). Lifetime prevalence of gender- based violence in women and the relationship with mental disorders and psychosocial function. JAMA, 306(5), 513-521.
Renner, L. M., & Whitney, S. D. (2012). Risk factors for unidirectional and bidirectional intimate partner violence among young adults. Child Abuse & Neglect, 36(1), 40-52.
Rennison, C. M., DeKeseredy, W. S., & Dragiewicz, M. (2012). Urban, suburban, and rural variations in separation/ divorce rape/sexual assault: Results from the National Crime Victimization Survey. Feminist Criminology, 7(4), 282-297.
Reyes, H. L., & Foshee, V. A. (2013). Sexual dating aggression across grades 8 through 12: Timing and predictors of onset. Journal of Youth & Adolescence, 42(4), 581-595.
Rich, C. L., Gidycz, C. A., & Warkentin, J. B. (2005). Child and adolescent abuse and subsequent victimization: A prospective study. Child Abuse & Neglect, 29(12), 1373-1394.
Rickert, V. I., Wiemann, C. M., Vaughan, R. D., & White, J. W. (2004). Rates and risk factors for sexual violence among an ethnically diverse sample of adolescents. Archives of Pediatrics & Adolescent Medicine, 158(12), 1132-1139.
Ristock, J. (2014). Sexual assault in intimate same-sex relationships. In L. McOrmond Plummer, J.Y. Levy- Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Romans, S., Forte, T., Cohen, M. M., Du Mont, J., & Hyman, I. (2007). Who is most at risk for intimate partner violence? A Canadian population-based study. Journal of Interpersonal Violence, 22(12), 1495-1514.
Roodman, A. A., & Clum, G. A. (2001). Revictimization rates and method variance: A meta-analysis. Clinical Psychology Review, 21(2), 183-204.
Ruiz-Pérez, I., Plazaola-Castaño, J., Álvarez-Kindelán, M., Palomo-Pinto, M., Arnalte-Barrera, M., Bonet-Pla, Á., . . . Garralón-Ruiz, L. M. (2006). Sociodemographic associations of physical, emotional, and sexual intimate partner violence in Spanish women. Annals of Epidemiology, 16(5), 357-363.
Sabina, C., & Ho, L. Y. (2014). Campus and college victim responses to sexual assault and dating violence disclosure, service utilization, and service provision. Trauma, Violence, & Abuse, 15(3), 201-226.
Sabina, C., & Straus, M. A. (2008). Polyvictimization by dating partners and mental health among U.S. college students. Violence and Victims, 23(6), 667-682.
Sabri, B., Barcelona de Mendoza, V., & Campbell, J. (2014). Immigrant women and intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Sack, E. (2009). Is domestic violence a crime? Intimate partner rape as allegory, St John’s Journal of Legal Commentary, 24(3), 535-566.
Salter, M. (2012). Managing recidivism amongst high risk violent men (Issues paper 23). Sydney: Australian Domestic & Family Violence Clearinghouse.
Salter, M. (2014). Multi-perpetrator domestic violence. Trauma, Violence & Abuse, 15(2), 102-112.
Schafran, L. H. (2014). Intimate partner sexual violence and the courts. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Schafran, L. H. (2010). Risk assessment and intimate partner sexual abuse. Judicature, 93(4), 161-163.
Schei, B., Guthrie, J. R., Dennerstein, L., & Alford, S. (2006). Intimate partner violence and health outcomes in mid-life women: A population-based cohort study. Archives of Womens Mental Health, 9(6), 317-324.
Schewe, P., Riger, S., & Howard, A. (2006). Factors associated with domestic violence and sexual assault victimization. Journal of Family Violence, 21(7), 469-475.
Schumacher, J. A., Feldbau-Kohn, S., Slep, A. M. S., & Heyman, R. E. (2001). Risk factors for male-to-female partner physical abuse. Aggression and Violent Behavior, 6(2), 281-352.
Sears, H. A., & Byers, E. S. (2010). Adolescent girls’ and boys’ experiences of psychologically, physically, and sexually aggressive behaviors in their dating relationships: Co- occurrence and emotional reaction. Journal of Aggression, Maltreatment & Trauma, 19(5), 517-539.
Seedat, S., Stein, M. B., & Forde, D. R. (2005). Association between physical partner violence posttraumatic stress, childhood trauma, and suicide attempts in a community sample of women. Violence and Victims, 20(1), 87-98.
Shaffer, D., & Kipp, K. (2013). Developmental psychology: Childhood and adolescence. Belmont, CA: Cengage Learning.
Shevlin, M., O’Neill, T., Houston, J., Read, J., Bentall, R., & Murphy, J. (2013). Patterns of lifetime female victimisation and psychotic experiences: A study based on the UK Adult Psychiatric Morbidity Survey 2007. Social Psychiatry & Psychiatric Epidemiology, 48(1), 15-24.
Shorey, R. C., Cornelius, T. L., & Bell, K. M. (2008). A critical review of theoretical frameworks for dating violence: Comparing the dating and marital fields. Aggression and Violent Behavior, 13(3), 185-194.
Siegel, J. A., & Williams, L. M. (2003). Risk factors for sexual victimization of women: Results from a prospective study. Violence Against Women, 9(8), 902-930.
Simmel, C., Postmus, J. L., & Lee, I. (2012). Sexual revictimization in adult women: Examining factors associated with their childhood and adulthood experiences. Journal of Child Sexual Abuse, 21(5), 593-611.
Smith, P. H., Thornton, G. E., DeVellis, R., Earp, J., & Coker, A. L. (2002). A population-based study of the prevalence and distinctiveness of battering, physical assault, and sexual assault in intimate relationships. Violence Against Women, 8(10), 1208-1232.
Smith, P. H., White, J. W., & Holland, L. J. (2003). A longitudinal perspective ondating violence among adolescent and college-age women. American Journal of Public Health, 93(7), 1104-1109.
Sørbø, M. F., Grimstad, H., Bjørngaard, J. H., Schei, B., & Lukasse, M. (2013). Prevalence of sexual, physical and emotional abuse in the Norwegian mother and child cohort study. BMC Public Health, 13(1), 1-11.
Spiller, L. C., Jouriles, E. N., McDonald, R., & Skopp, N. A. (2012). Physically abused women’s experiences of sexual victimization and their children’s disruptive behavior problems. Psychology of Violence, 2(4), 401-410.
Spohn, C., & Tellis, K. (2012). The criminal justice system’s response to sexual violence. Violence Against Women, 18(2), 169-192.
Stalans, L. J., Hacker, R., & Talbot, M. E. (2010). Comparing nonviolent, other-violent, and domestic batterer sex offenders: Predictive accuracy of risk assessments on sexual recidivism. Criminal Justice and Behavior, 37(5), 613-628.
Stark, E. (2009). Rethinking coercive control. Violence Against Women, 15(12), 1509-1525.
Stark, E. (2010). Do violent acts equal abuse? Resolving the gender parity/asymmetry dilemma. Sex Roles, 62(3-4), 201-211.
Stermac, L., Del Bove, G., Brazeau, P., & Bainbridge, D. (2006). Patterns in sexual assault violence as a function of victim perpetrator degree of relatedness. Journal of Aggression, Maltreatment & Trauma, 13(1), 41-58.
Stockman, J., Lucea, M., & Campbell, J. (2013). Forced sexual initiation, sexual intimate partner violence and HIV risk in women: A global review of the literature. AIDS & Behavior, 17(3), 832-847.
Stockman, J. K., Campbell, J. C., & Celentano, D. D. (2010). Sexual violence and HIV risk behaviors among a nationally representative sample of heterosexual American women: The importance of sexual coercion. Journal of Acquired Immune Deficiency Syndromes (1999), 53(1), 136.
Stoddard, J. P., Dibble, S. L., & Fineman, N. (2009). Sexual and physical abuse: A comparison between lesbians and their heterosexual sisters. Journal of Homosexuality, 56(4), 407-420.
Stotzer, R. L. (2009). Violence against transgender people: A review of United States data. Aggression and Violent Behavior, 14(3), 170-179.
Sullivan, T. P., McPartland, T. S., Armeli, S., Jaquier, V., & Tennen, H. (2012). Is it the exception or the rule? Daily co- occurrence of physical, sexual, and psychological partner violence in a 90-day study of substance-using, community women. Psychology of Violence, 2(2), 154-164.
Sullivan, T. P., Schroeder, J. A., Dudley, D. N., & Dixon, J.M. (2010). Do differing types of victimization and coping strategies influence the type of social reactions experienced by current victims of intimate partner violence? Violence Against Women, 16(6), 638-657.
Tanha, M., Beck, C. J. A., Figueredo, A. J., & Raghavan, C. (2010). Sex differences in intimate partner violence and the use of coercive control as a motivational factor for intimate partner violence. Journal of Interpersonal Violence, 25(10), 1836-1854.
Tapia, N. D. (2014). Survivors of child sexual abuse and predictors of adult re-victimization in the United States: A forward logistic regression analysis. International Journal of Criminal Justice Sciences, 9(1), 64-73.
Taylor, N., & Putt, J. (2007). Adult sexual violence in Indigenous and culturally and linguistically diverse communities in Australia. Canberra: Australian Institute of Criminology.
Tellis, K. (2010). Rape as a part of domestic violence: A qualitative analysis of case narratives and official reports. El Paso, TX: LFB Scholarly Pub.
Temple, J. R., Weston, R., Rodriguez, B. F., & Marshall, L. L. (2007). Differing effects of partner and nonpartner sexual assault on women’s mental health. Violence Against Women, 13(3), 285-297.
Testa, M., Hoffman, J. H., & Livingston, J. A. (2010). Alcohol and sexual risk behaviors as mediators of the sexual victimization– revictimization relationship. Journal of Consulting and Clinical Psychology, 78(2), 249.
Testa, M., VanZile-Tamsen, C., & Livingston, J. A. (2007). Prospective prediction of women’s sexual victimization by intimate and nonintimate male perpetrators. Journal of Consulting & Clinical Psychology, 75(1), 52-60.
Thakker, J. (2012). An integrated theory of sexual recidivism. Sexual Abuse in Australia and New Zealand, 4(1), 41-52.
Thomas, T. A., & Fremouw, W. (2009). Moderating variables of the sexual “victim to offender cycle” in males. Aggression and Violent Behavior, 14(5), 382-387.
Thompson, M., Sitterle, D., Clay, G., & Kingree, J. (2007). Reasons for not reporting victimizations to the police: Do they vary for physical and sexual incidents? Journal of American College Health, 55(5), 277-282.
Thompson, R. S., Bonomi, A. E., Anderson, M., Reid, R. J., Dimer, J. A., Carrell, D., & Rivara, F. P. (2006). Intimate partner violence: Prevalence, types, and chronicity in adult women. American Journal of Preventive Medicine, 30(6), 447-457.
Tiefenthaler, J., Farmer, A., & Sambira, A. (2005). Services and intimate partner violence in the United States: A county‐level analysis. Journal of Marriage and Family, 67(3), 565-578.
Tjaden, P., & Thoennes, N. (2000). Full report of the prevalence, incidence, and consequences of violence against women series: Research report. Washington DC: U.S. Department of Justice.
Todahl, J. L., & Walters, E. (2009). Universal screening and assessment for intimate partner violence: The IPV Screen and Assessment Tier (IPV-SAT) Model. Journal of Feminist Family Therapy, 21(4), 247-270.
Tomison, A. (2000). Exploring family violence: Links between child maltreatment and domestic violence. NCPC Issues, 13(Winter).
Tufts, K. A., Clements, P. T., & Wessell, J. (2010). When intimate partner violence against women and HIV collide: Challenges for healthcare assessment and intervention. Journal of Forensic Nursing, 6(2), 66-73.
Vagi, K. J., Rothman, E. F., Latzman, N. E., Tharp, A. T., Hall, D. M., & Breiding, M. J. (2013). Beyond correlates: A review of risk and protective factors for adolescent dating violence perpetration. Journal of Youth and Adolescence, 42(4), 633-649.
Van Bruggen, L. K., Runtz, M. G., & Kadlec, H. (2006). Sexual revictimization: The role of sexual self-esteem and dysfunctional sexual behaviors. Child Maltreatment, 11(2), 131-145.
Vatnar, S., & Bjørkly, S. (2008). An interactional perspective of intimate partner violence: An in-depth semi-structured interview of a representative sample of help-seeking women. Journal of Family Violence, 23(4), 265-279.
Wall, L. (2012). The many facets of shame in intimate partner sexual violence. Melbourne: Australian Institute of Family Studies.
Wangmann, J. (2011). Different types of intimate partner violence: An exploration of the literature (Issues Paper 22). Sydney: Australian Domestic& Family Violence Clearinghouse.
Watson, A. C., Corrigan, P., & Kosyluk, K. (2014). Challenging stigma. In P. Byrn & A. Rosen (Eds.), Early Intervention in Psychiatry (pp. 358-372). Oxford: John Wiley & Sons.
Wekerle, C., Bennett, T., & Francis, K. (2013). Child sexual abuse and adolescent sexuality. In D.S. Bromberg & T.W. O’Donohue, (Eds.), Handbook of child and adolescent sexuality: developmental and forensic psychology. Oxford: Academic Press.
White, J., McMullin, D., Swartout, K., Sechrist, S., & Gollehon, A. (2008). Violence in intimate relationships: A conceptual and empirical examination of sexual and physical aggression. Children & Youth Services Review, 30(3), 338-351.
White, J., & Smith, P. H. (2000). Developmental antecedents of violence against women: A longitudinal perspective. Rockville, MD: National Criminal Justice Reference Service.
Whitfield, C. L., Anda, R. F., Dube, S. R., & Felitti, V. J. (2003). Violent childhood experiences and the risk of intimate partner violence in adults: Assessment in a large health maintenance organization. Journal of Interpersonal Violence, 18(2), 166-185.
Wilcox, K. (2010). Connecting systems, protecting victims: Towards vertical coordination of Australia’s response to domestic and family violence. University of New South Wales Law Journal, 33, 1013.
Williamson, E. (2014). Reproductive coercion. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Wilson, K. S., Silberberg, M. R., Brown, A. J., & Yaggy, S. D. (2007). Health needs and barriers to healthcare of women who have experienced intimate partner violence. Journal of women’s health, 16(10), 1485-1498.
Winters, M., & Morgan, I. (2014). Cross-cultural perspectives on intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Winters, M. (2009). Making the connections: Advocating for survivors of intimate Partner Sexual Violence. In Washington Coalition of Sexual Assault Programs (Ed.), Intimate partner sexual violence: Sexual assault in the context of domestic violence. Olympia, WA: Washington Coalition of Sexual Assault Programs.
Wolff, N., Blitz, C. L., Shi, J., Bachman, R., & Siegel, J. A. (2006). Sexual violence inside prisons: Rates of victimization. Journal of Urban Health, 83(5), 835-848.
Wolff, N., Shi, J., & Siegel, J. A. (2009). Patterns of victimization among male and female inmates: Evidence of an enduring legacy. Violence and Victims, 24(4), 469-484.
Women With Disabilities Australia. (2013). Background paper – National symposium on violence against women and girls with disabilities. Tasmania: WWDA.
Woodward, C., Fischer, J., Najman, J., & Dunne, M. (2004). Selling sex in Queensland 2003: A study of prostitution in Queensland. Milton, QLD: Prostitution Licensing Authority.
Wright, M. O., Norton, D. L., & Matusek, J. A. (2010). Predicting verbal coercion following sexual refusal during a hookup: Diverging gender patterns. Sex Roles, 62(9-10), 647-660.
Yoshihama, M., & Horrocks, J. (2010). Risk of intimate partner violence: Role of childhood sexual abuse and sexual initiation in women in Japan. Children & Youth Services Review, 32(1), 28-37.
Young, B. J., & Furman, W. (2008). Interpersonal factors in the risk for sexual victimization and its recurrence during adolescence. Journal of Youth and Adolescence, 37(3), 297-309.
Zurbriggen, E. L., Gobin, R. L., & Freyd, J. J. (2010). Childhood emotional abuse predicts late adolescent sexual aggression perpetration and victimization. Journal of Aggression, Maltreatment & Trauma, 19(2), 204-223.
Zweig, J. M., & Burt, M. R. (2003). Effects of interactions among community agencies on legal system responses to domestic violence and sexual assault in STOP-funded communities. Criminal Justice Policy Review, 14(2), 249-272.
Zweig, J. M., & Burt, M. R. (2004). Impacts of agency coordination on nonprofit domestic violence and sexual assault programs in communities with STOP formula grant funding. Violence and Victims, 19(5), 613-624.
Zweig, J. M., & Burt, M. R. (2007). Predicting women’s perceptions of domestic violence and sexual assault agency helpfulness. Violence Against Women, 13(11), 1149-1178.
Zweig, J. M., Dank, M., Yahner, J., & Lachman, P. (2013). The rate of cyber dating abuse among teens and how it relates to other forms of teen dating violence. Journal of Youth and Adolescence, 42(7), 1063-1077.
Endnotes
-
In this paper, when we refer to “women” we mean individuals who (a) self-identify as women, and/or (b) have lived or embodied experience as women. At the same time, it is acknowledged that almost all research examined in this review does not critically engage with the concept of “woman” and thus the nature of the study samples may not reflect this definition. ↑
-
This paper examines IPSV and re-victimisation in relation to a wide range of sub-populations including Aboriginal and Torre Strait Islander women, women from culturally and linguistically diverse backgrounds, women with low socio-economic status, women who work in the sex industry, lesbian and bisexual women, people who are transgender (inclusive of trans-men who experienced violence at a time when they identified as female and/ or experienced violence in a context where they were read by others as female), women who are alcohol or other drug dependent, women who are HIV positive, women with physical or intellectual disability, women who experience severe mental illness, women who are incarcerated and women who live in rural areas. ↑
-
Adolescence is understood in this review to mean the period after the onset of puberty and prior to adulthood. ↑
-
Marriage in these studies was limited to religious and secular marriages involving opposite sex partners. ↑
-
It should be acknowledged that, while essential for the representation of data in a literature review format, the separation of groups in this manner does a disservice to the complexity of lived experience. Discrimination and stigma are often more acute for women who identify as part of multiple groups (e.g. a woman who is homeless, HIV positive, works in the sex industry and injects drugs is likely to experience more discrimination and stigma when compared to a woman who is part of only one of these sub- populations). These highly marginalised women are likely to experience discrimination and stigma from both the general community and service providers, with the criminal aspect of certain dimensions of their lives likely to further compound the challenges of help-seeking in relation to experiences of victimisation. ↑
-
As the research outlined below is predominately from the US, it relates to migrant communities. In the Australian context, the category of CALD communities would include a wider range of women, including women who are refugees and those who live in certain cultural and/or religious communities. ↑
-
This section is limited to a discussion of women with physical and intellectual disability. Papers on women with psychiatric disability were placed in a separate category, namely “Women who experience severe mental illness”. ↑
-
Our Watch was founded under the First Action Plan of the National Plan to Reduce Violence against Women and their Children as Australia’s national organisation for preventing violence against women and their children. ↑
-
In light of the Royal Commission into Institutional Child Abuse in Australia, there has been increasing focus on programs which aim to prevent CSA. These programs, while potentially contributing to the reduction in re- victimisation, were outside the scope of this review and thus are unable to be discussed in this section. ↑
-
Intimate partner sexual assault is captured under the category of severe sexual coercion in the CTS2. ↑
State of knowledge
State of knowledge | October 2015
Issue 13 | 2015
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
Acknowledgement of Country
ANROWS acknowledges the traditional owners of the land across Australia on which we work and live. We pay our respects to Aboriginal and Torres Strait Islander elders past, present and future; and we value Aboriginal and Torres Strait Islander history, culture and knowledge.
© ANROWS 2015
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box 6322, Alexandria NSW 2015 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
Sexual assault and domestic violence in the context of co-occurrence and re-victimisation:
State of knowledge paper / Peta, Cox.
Sydney: ANROWS, c2015.
Pages; 30 cm. (Landscapes: State of Knowledge: 13/2015)
I. Violence against women. II. Family violence. III. Victims of family violence – Services for. IV. Sexual abuse victims. V. Sex crimes.
I. Cox, Peta.
ISSN: 2204-9657 (print) 2204-9665 (online)
ISBN: 978-1-925372-26-7 (print) 978-1-925372-25-0 (online)
Creative Commons Licence
Attribution-Non Commercial
CC BY-NC
This licence lets others distribute, remix and build upon the work, but only if it is for non-commercial purposes and they credit the original creator/s (and any other nominated parties). They do not have to license their Derivative Works on the same terms.
Version 3.0 (CC Australia ported licence): View CC BY-NC Australia Licence Deed | View CC BY-NC 3.0 Australia Legal Code
Version 4.0 (international licence): View CC BY-NC 4.0 Licence Deed | View CC BY-NC 4.0 Legal Code
Prepared by
Dr Peta Cox, Senior Research Officer (Research Program), ANROWS
Author acknowledgement
My thanks to Jen Novak, Tony Fletcher, Erin Mackay and Ange Williams for their initial input and support with this project.
I also greatly appreciate valuable feedback from the two anonymous peer reviewers.
This work is part of the ANROWS Landscapes series. ANROWS Landscapes (State of knowledge papers) are medium length papers that scope current knowledge on an issue related to violence against women and their children. Papers will draw on empirical research, including research produced under ANROWS’s research program, and/or practice knowledge.
This paper addresses work covered in the ANROWS research project 1.6 “Sexual assault and domestic violence in the context of co-occurrence and re-victimisation”. Please consult the ANROWS website for more information on this project.
Contents
Overall characteristics of the corpus
Theories of re-victimisation and co-occurrence
Common disciplinary approaches
Theories, concepts and typologies
Methods used by researchers examining re-victimisation and co-occurrence
Life-course research: Key limitations
Cross-sectional research: Key limitations
Bias caused by population selection
Bias caused by incomplete reporting
Comparability: Inconsistent phenomena definitions
Undifferentiated categories of violence
Commonly used survey instruments
Comparability of study findings
Rates of re-victimisation and co-occurrence
Characteristics of incidents of intimate partner sexual violence
Risk factors for re-victimisation and co-occurrence
Relational and behavioural risk factors
Sub-populations with differential patterns of victimisation
Aboriginal and Torres Strait Islander women
Women from cultural and linguistically diverse (CALD) backgrounds
Women with low socio-economic status
Women who are, or who have been, incarcerated
Women who experience severe mental illness
Women who identify as lesbian, bisexual and/or queer
Women who work in the sex industry
Sub-populations of interest with limited existing research
Male repeat perpetrators of sexual assault and domestic violence: Repeat offenders
Community and professional attitudes towards re-victimisation and co-occurrence
Health impacts of re-victimisation and co-occurrence
Women’s engagement with legal and support services
Help-seeking: Non-legal services
Responses to women affected by re-victimisation and co-occurrence
Coordinated, multi-agency and integrated services responses
Recommendations and conclusion
Appendix A: Searched databases
Appendix B: Additional available literature
Intimate partner sexual violence rates
Executive summary
Scope of project
This state of knowledge paper aims to examine the intersection between sexual assault and domestic violence. In order to do this, it highlights similarities and differences in the causes, consequences and lived experience of two forms of concurrent victimisation. Within this paper, concurrent victimisation is understood to include re-victimisation (when a woman, over her lifetime, experiences both sexual assault and domestic violence) and intimate partner sexual violence (IPSV). This paper examines the complexity of these experiences in order to articulate the common impacts of domestic violence and sexual assault and to critically examine how the phenomenon of re-victimisation and IPSV can shift the ways in which we think about, and provide services for, women affected by domestic violence and sexual assault.
Method
The review used a multi-staged, repeatable, search methodology. Academic and grey literature on (a) domestic violence (DV) and sexual assault (SXA) victimisations across the life course, and (b) intimate partner sexual violence was assessed. An initial corpus of 6715 sources were assessed, with 271 of these deemed within scope. After snowballing from relevant papers, a total of 333 papers were used in the review.
Key findings
The lack of longitudinal studies of re-victimisation reduces our ability to make conclusions about causal factors or the nature of victimisation over time.
Much of the available research on IPSV and re-victimisation is unable to be extrapolated to findings about the general population, as it focuses on non-representative groups such as women who were attending psychology clinics.
Regarding re-victimisation:
- Research indicates that women who experience child sexual abuse (CSA) are more likely to experience IPSV than women who have not experienced CSA.
- Similarly, women who have experienced CSA are more likely to experience DV (not limited to sexual violence) in their adult relationships.
- The relationship between CSA and adult victimisation is mediated to some extent by the severity of the abuse during childhood.
- Research on the frequency and impacts of re- victimisation in adulthood is more mixed.
Regarding IPSV:
- Across the reviewed studies, intimate partner sexual coercion was reported by between 24 percent and 62 percent of women, while intimate partner sexual assault was reported by between 1.7 percent and 46 percent of women.
- IPSV generally occurs in the context of other forms of violence and was often part of a larger pattern of coercive control in a relationship. IPSV should be considered a tactic of DV, and not a separate phenomenon.
- Alcohol abuse problems, frequent and normalised engagement with pornography and a history of sexual coercion were associated with IPSV perpetration in a current relationship.
- IPSV was often limited to emotional coercion, however when it was physically violent, it frequently resulted in injury.
- Heteronormative beliefs and conservative gender norms were associated with acceptance and experience of sexual coercion for both men and women.
- IPSV victims are less likely to seek help than victims of other forms of DV.
Regarding both re-victimisation and IPSV:
- Drug and alcohol use may be a precursor, consequence or risk factor associated with IPSV and re-victimisation. Similarly, emotional distress and psychiatric conditions may increase a person’s vulnerability to violence, place them in high risk contexts and/or may be a consequence of violence.
- A wide range of communities, including Aboriginal and Torres Strait Islander women, women from culturally and linguistically diverse backgrounds and women with a disability, have discrete patterns of victimisation, including distinct behaviours and norms that may increase the risk of victimisation.
- Normative understandings of what constitutes “real rape” affect how victims, perpetrators and bystanders interpret experiences of sexual assault. These norms particularly affect interpretations of IPSV incidents.
- Both IPSV and re-victimisation had significant physical and mental health consequences.
- DV and SXA services were often separated, with both service types finding victims of IPSV and women who had complex trauma histories to be particularly challenging client groups.
Key recommendations
The following recommendations are based on the research examined for this state of knowledge paper and can be made regarding the method and focus of future research.
ANROWS recommends that:
- As re-victimisation often occurs across violence types, researchers should, wherever possible, expand their examination of life course re-victimisation to multiple violence types.
- Longitudinal research is critical to understanding the complex pathways that result in repeated victimisation and IPSV. Such research is particularly important for understanding the lived experience of marginalised women (e.g. incarcerated women), as the intersections of disadvantage are even more complex for these populations(Poister, Tusher, & Cook, 2010). Put differently, “longitudinal research is needed to sort out risk factors, from consequences, from simple correlates” (Classen et al., 2005, p. 114).
- As has been noted for several decades now, one way of increasing the quality and comparability of research findings is for there to be consistent definitions of abusive behaviours used in IPSV and re-victimisation research. Such definitions would need to provide clarity to research participants about what was meant by “force” in relation to sexual activity, with distinctions made between physical threat and emotional/psychological coercion tactics.
- Future research should concentrate on relevant target groups. Many target groups have relatively small populations, making collecting data with population level surveys difficult. One exception to this is disability, which has a high prevalence and thus analysable data is likely to be able to be collected in all violence research. Most other sub-populations are likely to require dedicated surveys to get a sufficient sample to be statistically reliable.
- Although both qualitative and quantitative research is needed to inform Aboriginal and Torres Strait Islander family violence policy, priority should be given to quantitative research as current quantitative surveys like the Personal Safety Survey (PSS) are unable to provide prevalence estimates for this population.
The following recommendations are made regarding the service delivery environment and are based on the research findings reviewed in this paper.
ANROWS recommends that:
- Acknowledgement is made in policy and practice of weaknesses in our current research base, which means that we are heavily reliant on practice knowledge.
- Accurate and appropriate use of data and acknowledgement of data’s limitations is encouraged in policy, planning and service advocacy, so that when further evidence-based knowledge is available, it is welcomed and adopted.
- To address the stigma of IPSV, DV and SXA services continue to work to raise awareness of the impact of stigma on clients and staff.
- Judicial education and professional development work continues to be supported to ensure court and police sensitivity in IPSV cases, and to minimise the distress of the legal process to women who have experienced re- victimisation and/or IPSV.
- Where not already part of normal clinical practice, STI clinics be provided with training and materials to enable streamlined referrals to SXA and DV services.
- Trauma informed care (a model of care which puts at the centre of clinical practice the long term effects of victimisation) be supported through mainstream service provision and research investment.
- Large scale mental health campaigns promote gendered violence as a risk factor for poor mental health outcomes.
- All DV and SXA services be sufficiently resourced to further enrich cross-sector co-ordination (a full range of co- ordination strategies are possible, from referral pathways to fully integrated care).
- All DV and SXA services, as well as related services such as mental health and drug and alcohol programs, continue to work towards an integrated understanding of the impacts of the escalation or severity of CSA on adulthood in their engagements with both children and adults.
- Public education on violence against women acknowledges the distinct but intersectional dimensions of different forms of violence and its gendered impacts and characteristics.
- Providers of mainstream health and social services be sensitised to the possibility of IPSV and re-victimisation cases in their day to day work. An initial step towards this would be the promotion of existing IPSV screening tools to a wide range of mainstream frontline providers.
- Prevention programs not be funded by government if they implicitly or explicitly support victim blaming. Explanation of these actions should be given to campus unions to promote a similar stance in university campus programs.
- Professional development for workers in the violence against women field acknowledge the multi-faceted nature of abuse and emphasise the links between DV and SXA.
Introduction
State of play
Domestic violence and sexual assault are experienced by a large number of Australian women[1] and have significant and well-established health and welfare impacts. ANROWS has recently completed a research project examining the Australian Bureau of Statistics’ 2012 Personal Safety Survey (PSS) data, which showed that, since the age of 15, one in eight (13%) women in Australia have experienced at least one separate incident of both sexual violence and physical violence (Cox, 2015). As this paper demonstrates, many women have experienced both sexual assault (SXA) and domestic violence (DV) victimisation, either in the form of intimate partner sexual violence (IPSV) or re- victimisation across their life course.
Experiences of SXA and DV are complicated by the contexts in which such victimisation occurs, including the cultural meanings given to violence, and the curtailing action of some women due to the criminalisation of certain aspects of their lives. While such contextual aspects are critical in understanding the full impact of IPSV and re-victimisation, the variation and complexity of these intersections is only able to be briefly examined in this state of knowledge paper.
Despite significant co-occurrence, both researchers and practitioners have noted a continuing tendency to dichotomise SXA and DV into distinct concepts and responses, and to artificially separate women’s lived experience into the responsibility of one or other sector (Tellis, 2010). This theoretical and practical separation is particularly apparent in Australia, where the history of DV and SXA services are distinct.
In order to more fully understand DV and SXA, it is important to conceptualise them as interrelated experiences (Sabina & Ho, 2014). This paper adds to current understandings of this interrelatedness by examining the available research on patterns of violence against women that include both DV and SXA.[2] “Cross-type” re-victimisation and IPSV are both topics that have received limited research attention (Ferro, Carmeele & Saltzman, 2008). In the context of this state of knowledge paper it is important to note that such research may not fully reflect current Australian practice, especially in relation to engagements with priority populations or efforts to enhance the embedding of intersectional analysis in the work and philosophy of practitioners.
This paper notes that there is limited research on the characteristics of any types of violence in most sub-populations, with research on IPSV and re-victimisation particularly incomplete. Relatedly, a key weakness identified in the current research was the tendency to silo lived experience, so that the intersection of multiple sites of disadvantage and stigmatisation was not readily apparent within the literature. This limitation of the literature was, by nature of the building blocks available, mirrored in the state of knowledge paper.
Purpose of the paper
This paper aims to identify similarities and differences in the causes, consequences and lived experience of two forms of concurrent victimisation: namely, certain forms of repeat victimisation across the life course and sexual violence in an intimate relationship.
These two very specific types of violence are examined in this review. By doing this, we are able to examine the cross-over between experiences of domestic violence and sexual assault and thus appreciate its complexity.
Nature of the paper
This paper is an examination of the intersections between domestic violence and sexual assault. This intersection can occur in two ways:
- Re-victimisation – when a woman, over her lifetime, experiences both sexual assault and domestic violence.
- Co-occurring victimisation – when a woman experiences sexual assault by an intimate partner. This is also known as intimate partner sexual violence (IPSV).
Consistent with the focus of ANROWS, this paper is limited to examinations of instances and trajectories of violence that are experienced by adult women victims.
This state of knowledge paper is an examination of empirical literature. The inclusion of studies in the paper is not an endorsement of their methodology or approach, but is rather an acknowledgement that they are part of the currently available research.
State of knowledge method
Research questions
This literature review aims to answer the following questions:
- What do we know about when SXA and DV happen at the same time or when they happen at different times but to the same person, including lived experience and impacts?
- What do we know about the epidemiological and conceptual similarities and differences in the nature of sexual assault and domestic violence when they are experienced in the context of co-occurrence and re-victimisation?
- What do we know about what works in supporting survivors of both sexual assault and domestic violence?
Review method
The review used a multi-staged, repeatable, search methodology (see Table 1 on page 11).
The review began with a systematic search of a wide range of academic and grey literature databases (see Appendix A). Quantitative data was heavily represented in the available databases.
The metadata for all papers identified in the search were uploaded into bibliographic software. By examining the title and abstract of each paper, irrelevant articles were removed from the cohort (see Table 2 on page 12).
The search of the academic literature was supported by snowball searching on Google Scholar.
The review was limited to publications that were:
- published in the last ten years;
- empirical research, commentary and theoretical accounts;
- concerned with instances of co-occurring DV and SXA in the life of an adult female victim (including adolescent women in “dating” relationships);
- concerned with re-victimisation that began in childhood;
- accompanied by available abstracts;
- written in English; and
- studies of human subjects.
The review excluded publications that were more than 10 years old or focused on:
- low income countries;
- violence against men;
- child abuse, including paedophilia, not in the context of expressions of violence between adults or as part of a life course of violence that included abuse of an adult woman;
- violence in the context of war or conflict;
- sex trafficking;
- harmful cultural practices (e.g. forced marriage, female genital mutilation/cutting and wife inheritance);
- violence perpetrated by women; or
- the effect of DV on child welfare (where there is no consideration of an adult female victim).
Superseded publications were also excluded. Some papers published before 2005 have been included as part of the snowball searches – this has only occurred when more recent papers have indicated that the most up to date primary research is outside the time limit. In addition, a small number of older papers have been referenced when they are canonical studies or original theoretical pieces.
Table 1 Electronic search strategy
| Topic | Key word (phrase searching) |
|---|---|
| Set 1: Sexual assault | Sexual assault OR Sexual violence OR Rape OR Indecent assault OR Unlawful sexual conduct OR Sex crime OR Date rape OR Acquaintance rape OR Sexual abuse OR Sexual attack OR Sexual force OR Sexual injury OR Attempted rape OR Sexual coercion OR Non-consensual sex OR Indecent exposure OR Sexual harassment OR Stalking |
| Set 2: Domestic violence | Intimate partner violence OR Domestic violence OR Domestic abuse OR Family violence OR Family abuse OR Dating abuse OR Battering OR Wife beating OR Wife battering OR Physical abuse OR Emotional abuse OR Psychological abuse OR Financial abuse OR Intimate terrorism OR Spouse abuse OR Spousal abuse |
| Set 3: Relationship between | Co-occur* OR Intersect* OR Poly-victimi$ation OR Concur* OR Simultaneous* OR Concomitance OR Overlap* OR Contemporaen* OR Compare OR Comparison OR Differences OR Similarities OR Correlations OR Risk factors OR Epistemology OR Cause OR Causation OR Epidemiology OR Typology OR Characteristics OR Responses OR Interventions OR Programs OR Instrument |
| Set 4: Final Set 1 AND Set 2 AND Set 3 | Limited to availability of abstracts, published 2005 to current, English language and humans. |
Table 2 PRISMA Flow diagram
Overall characteristics of the corpus
A total of 271 articles were assessed in full text.
The methodological design of the studies in this paper was consistent with that found in other reviews of IPSV or re- victimisation literature, with the vast majority of studies being quantitative (see, for example, Classen, Palesh & Aggarwal, 2005; Martin, Taft & Resick, 2007; Messman-Moore & Long, 2003; Stockman, Lucea, & Campbell, 2013). Almost all studies included in this state of knowledge paper were retrospective, meaning that they asked people to report on things that had already happened. The majority of the papers were examinations of the prevalence of various types of assault and/or lifetime patterns of assault. Even when looking at the life course of victimisation, most research was cross-sectional (asking questions at one point in time only), with very little longitudinal research (Ludermir, Schraiber, D’Oliveira, França-Junior, & Jansen, 2008; Reyes & Foshee, 2013). Cross-sectional and retrospective survey designs are acknowledged as providing less reliable epidemiological findings than cohort studies that follow people over time. Research using cross-sectional methods cannot provide reliable evidence about whether variables are causally linked. Given this limitation, it is perhaps surprising that predictive modelling in the form of regression or path analysis was a common method of analysing the relationships between risk factors, albeit often with limited predictive utility. Behavioural self-report surveys, such as the Revised Conflict Tactics Scale or the Sexual Experiences Survey were the most common survey instruments (Koss et al., 2007).
Consistent with the nature of available research on DV and SXA more generally, the studies in this paper were primarily from the US (Martin, Taft, & Resick, 2007). Sample size varied from mid-twenties to tens of thousands. Consistent with study methodology, qualitative studies tended to have samples of less than 100, while national, representative studies generally had more than 1000 respondents. As with much behavioural science research, the researchers oversampled college students and under-sampled socially and/or economically disadvantaged communities and/or populations of interest (Christopher & Pflieger, 2007; Moreau, Boucher, Hébert, & Lemelin, 2015).
The corpus consisted primarily of research on IPSV. This seems a likely consequence of the narrow “cross-type” victimisation focus in the scope of the review. However, due to the proportionally small amount of research on “cross-type” re-victimisation; where content relates to this expression of violence and it isn’t under an identifying section heading, relevant words are highlighted to bring this content to the reader’s attention throughout this paper.
Definitions
Re-victimisation
Re-victimisation occurs when a person experiences multiple distinct instances of violence over their life course. In the context of this paper, re-victimisation is limited to instances where a woman experiences both DV and SXA across their lifetime. There are several scenarios that are examined:
- Women who had experienced both child sexual abuse (CSA) and DV, including DV in the context of cohabitating and dating relationships.
- Women who had experienced DV and adult SXA, not perpetrated in the same context (i.e. excluding IPSV).
- Women who had experienced IPSV and either:
- childhood sexual assault; or
- adult sexual assault perpetrated by a person other than the partner perpetrating IPSV.
The use of this “cross-type” definition of re-victimisation significantly reduces the range of re-victimisation types that are examined in this report. In doing so, we are able to focus on the intersection of DV and SXA which is a key aim of this project. However, it is noteworthy that much of the research on re-victimisation is limited to “single-type” repeated victimisation, which means that the corpus related to re-victimisation was relatively small.
We have included dating violence in this working definition. This was strategic and reflects a commitment to an inclusive understanding of intimate relationships. Dating violence occurs between non-cohabiting partners and in other “dating” relationships, and has significant similarities to other forms of intimate partner violence and sexual assault (Christopher & Pflieger, 2007; Chiara, Sabina & Ho, 2014). It is acknowledged, however, that dating violence in younger cohorts (e.g. young people in high school) can be qualitatively different to other forms of intimate partner violence, in part due to practical limitations on sexual intimacy (Noonan & Charles, 2009). As such, discretion has been used in this paper regarding the inclusion of research based on high school cohort data.
Co-occurrence
Domestic violence and sexual assault can occur in the same incident: specifically, this occurs when an intimate partner uses sexual violence. It is typically referred to as intimate partner sexual violence (IPSV) and is a both a form of domestic violence and a form of sexual assault (Macleod, 2014b).
IPSV is a common form of SXA, with intimate partners perpetrating most adult sexual assault (Black et al., 2011; Logan, Walker, & Cole, 2013; Tjaden & Thoennes, 2000). ANROWS’s additional analysis of the 2012 PSS has shown that “[s]ince the age of 15, 805,900 women were sexually assaulted by a male intimate partner: this is one out of every eleven women in Australia (9.2%)” (Cox, 2015).
In general, IPSV is characterised by “deliberate intimidation or coercion” and may either be pressure to perform sexual acts that the victim is not comfortable with, or to engage in acts at a time that they do not wish to do so (Cornelius & Resseguie, 2007; Macleod, 2014a; Shorey, Cornelius, & Bell, 2008). Not all forms of IPSV are criminalised (McOrmond- Plummer, Easteal & Levy-Peck, 2014).
After completing a meta-analysis of available studies, Bagwell-Gray et al (2015) suggested separating intimate partner sexual violence into:
- sexual assault – high force and high invasiveness, such as rape that uses physical force or threat of actual physical harm, which was found to be experienced by 36.1 percent of IPV survivors (n = 3178, 11 studies) (wide variation in prevalence rates: 9% to 91%);
- sexual coercion – low force and high invasiveness, where non-physical tactics of manipulation are used to obtain penetrative sex (including vaginal or anal penetration by penis, fingers or objects), which was found to be experienced by 24.9 percent of IPV survivors (wide variation in prevalence rates: 17.4% to 91%) (n = 1408, 5 studies);
- sexual abuse – low force and low invasiveness, where non-consensual dominating or humiliating tactics are used; and,
- forced sexual activity – high force and low invasiveness, physically forced, non-penetrative sex acts.
(Meta-analyses for sexual abuse or forced sexual activity were not possible) (Bagwell-Gray et al., 2015)
IPSV may occur in the context of any sexual behaviour (e.g. kissing, sexual touching, watching pornography, bondage scenes, oral sex, vaginal sex). IPSV may involve using sex, sexualised threat and sexualised humiliation as part of a larger pattern of coercive control of a partner (Logan, Cole, & Shannon, 2007).
IPSV involving force or threat rarely occurs in isolation, and is typically accompanied by other forms of violence (McOrmond-Plummer, 2014). Despite this co-occurrence, the nature of these assaults, as well as their impacts on the victim, has led researchers to classify IPSV as a distinct form of violence that differs from non-sexual physical and emotional DV (Miller, 2006; Spohn & Tellis, 2012).
Although IPSV is the more common term, this phenomena is referred to in different ways in the literature, often reflecting the theoretical approach of the researcher. Other common terms include:
- marital rape;
- sexual coercion;
- date rape/violence;
- intimate sexual violence;
- intimate partner sexual assault; and
- domestic sexual assault.
(Martin et al., 2007; Spohn & Tellis, 2012)
Theories of re-victimisation and co-occurrence
Over the past 30 years, researchers have developed many different explanations of why and how re- victimisation and IPSV occur (Martin et al., 2007). These theories provide the basis for academic work in the area and have become increasingly complex in order to accommodate a greater appreciation of the multifaceted nature of these types of violence (Brassard, Darveau, Péloquin, Lussier, & Shaver, 2014; Busby, Holman, & Walker, 2008).
Understanding the available explanatory models is important because such models provide the theoretical lens that determines what studies are undertaken in the first place. Explanatory models also affect the implementation of findings as they provide the basis from which violence, its causes and its prevention, are conceptualised (Clark & Quadara, 2010; Thomas & Fremouw, 2009; Vatnar & Bjørkly, 2008).
Key findings in this section:
- Research on re-victimisation and IPSV comes from a range of disciplines including psychology, social work, criminology, family studies and feminist studies.
- The models, concepts and typologies used to understand violence affect how research findings are interpreted.
- Approaches to IPSV and re-victimisation research can be roughly divided into:
- individualised approaches that understand violence as an personal maladjustment that is expressed and influenced by interpersonal dynamics; and
- societal approaches that understand violence as an issue that, while always occurring in the context of individual choice and action, reflects macro social inequalities.
- Individual approaches dominate research in this field.
Common disciplinary approaches
Theoretical approaches are often aligned with a specific academic discipline, although research may align with more than one discipline. Disciplines often have accepted accounts of the nature of reality (ontology) and consistent explanations of what counts as knowledge and how you should go about obtaining knowledge (epistemology and methodology) (Desai & Saltzman, 2001).
Some of the more common approaches found in the corpus were:
- Psychology is a significant scientific field characterised by concern with the mental and behavioural characteristics of groups or individuals. Research from this field that was identified in the corpus tended to presuppose that behaviours can be counted and that acting in a certain way was linked to the attitudes that a person had about that behaviour. To reflect this approach, methods used by psychologists tended to involve retrospective self-report of a participant’s actions and beliefs. The collected data frequently undergoes significant statistical analysis and is based in a positivist epistemology. Assessments of risk of both perpetration and victimisation tend to be calculated using actuarial measures and standardised tools. Research psychologists often assume that there is a knowable and mappable pathway for both victimisation and perpetration that can be measured against a “normal” person. Psychology research identified in this paper disproportionately uses US college samples and tends to promote individualised “treatment” as an appropriate response to violence.
- Social work is a field of intervention into systemic social inequality. Within the corpus, research from this field was characterised by both an understanding of disadvantage as a characteristic of inequitable social systems, and a concern with practical assistance to people most negatively affected by such systems. In addition, some social work approaches concentrated on establishing the value, and maximising the impact, of intervention (such as client advocacy, case work and community support) on the well-being of individuals and their communities.
- Criminology is the study of criminal behaviour, including its cause, patterns, consequence and prevention. Research from this field identified in the corpus tended to be concerned with effectiveness of mechanisms to minimise re-offending. In this context, a focus on “risk” was common –risk was understood in relation to the frequency and severity of violence, as well as the capacity and/or likelihood of rehabilitation (Salter, 2012). Researchers often used administrative data from justice systems in order to provide actuarial models of recidivism risk, with such work often positioning offending pathways as individual, rather than social, problems (Clark & Quadara, 2010). Criminology has a significant influence on SXA research and practice in Australia.
- Family studies is an approach which appears limited to certain schools within the US. Within the corpus, it is characterised by methods similar to those used by psychology, combined with values that are generally conservative and family-centric. Researchers are often influenced by psychoanalytic concepts, use more normative scripts of relationship development, place high value on keeping family units together and perceive actions in the family of origin as central to child development (Peterson& Bush, 2013). Family studies research frequently uses the Conflict Tactics Scale (CTS) and tends to promote a gender-neutral account of violence that presumes “mutual responsibility” for violence incidents.
- Feminist approaches may be embedded in a range of disciplines and methodologies. Feminist accounts of intimate partner violence tend to emphasise that violence occurs in the social context of embedded gender inequalities which are reflected and further established by gendered norms and behaviours (Shorey et al., 2008). Gendered violence is typically understood as a continuum from normative expressions of sexism to brutal assault (Kelly, 2013). Some researchers contextualise their work through an understanding of patriarchy as a key mechanism for providing the systemic social structures and gendered power relations that are critical aspects of violence against women (Hunnicut, 2009). Methods used by feminist researchers tend to emphasise the complexity of the lived experience of violence and value women’s stories – feminist methods are therefore more likely to be qualitative and participatory. Such approaches also increasingly examined the intersection of a range of forms of systemic disadvantage, so that meaningful acknowledgement is made about the similarities and differences in the experiences of violence by “otherised” women such as Aboriginal and Torres Islander women, women with a disability and lesbian women (Crenshaw, 1991; Parkinson & Zara, 2014). Consistent with other western English-speaking countries, in Australia these feminist approaches have had significant impact on the development and maturation of the DV sector and have also influenced government policy on violence against women (Ahrens, Dean, Rozee, & McKenzie, 2008; Cooper et al., 2008; Costello, 2005; Maas-DeSpain & Todahl, 2014).
Each approach provided the context for a variety of theories of the cause and nature of co-occurring DV and SXA.
Theories, concepts and typologies
Over the past 30 years, researchers have developed many different explanations of why and how re-victimisation and IPSV occur (Martin et al., 2007). These theories provide the basis for academic work in the area and have become increasingly complex in order to accommodate a greater appreciation of the multifaceted nature of these types of violence (Brassard, Darveau, Péloquin, Lussier, & Shaver, 2014; Busby, Holman, & Walker, 2008).
Understanding the available explanatory models is important because such models provide the theoretical lens that determines what studies are undertaken in the first place. Explanatory models also affect the implementation of findings as they provide the basis from which violence, its causes and its prevention, are conceptualised (Clark & Quadara, 2010; Thomas & Fremouw, 2009; Vatnar & Bjørkly, 2008).
The corpus revealed a large number of explanatory and descriptive theories of co-occurrence. Below is an outline of the models, concepts and typologies that dominated the selected literature. Please note that this section does not engage with the empirical support for any of the available explanatory models, but rather outlines the key ideas that are active in the field.
Theories
Four theories (macro frameworks that provide broad-scale explanation of a wide range of types of violence) were common in the corpus: the ecological model, the transmission of violence model, social learning theory and conflict theory. Some of these models are generally positioned as conceptually distinct and are not routinely used simultaneously.
The social ecological model, also known simply as the ecological model, understands that a person’s risk of gendered violence, including SXA and DV, is affected by factors at four levels – the individual, the relational, the communal and the societal (Conway et al., 2010). A minority of scholars also explicitly include biological factors in the model (Bronfenbrenner, 2005; Busby et al., 2008). The ecological model is a public health approach to interpersonal violence and therefore was developed to address and explain violence at a population level, and has been used widely in the violence against women field (Coulter & VandeWeerd, 2009; Heise, 1998). The model may be used to inform various community level interventions, including structural and attitudinal change and bystander intervention programs (Casey & Lindhorst, 2009; Moynihan, Banyard, Arnold, Eckstein, & Stapleton, 2010). The ecological model has been criticised for its lack of theoretical coherence, as well as for its positioning of gender inequality as one of several (rather than the underlying and key) factors which cause violence against women (Pease, 2008, 2014). If we consider the full range of research on SXA and DV (including that which is not informed by the ecological model) most DV and SXA research is concerned with the inner layers of the model – the interpersonal and individual – with less research completed on the broader community and societal influences on violence perpetration and victimisation (Vagi et al., 2013). Despite this, there is substantial research regarding the communal and social influences on violence against women (VAW), in the VAW field and in more general sociological and/or feminist research.
The theory of transmission of violence (also known as the “cycle of violence”) is a model of violent behaviour that asserts that experiences of violence in childhood create significant developmental problems and drastically increase the likelihood that the victim will act violently later in life (DeLisi, Caudill, & Trulson, 2014; Reckdenwald, Mancini, & Beauregard, 2013). The model is particularly common in accounts of the impact of CSA (Boivin, Lavoie, Hébert, & Gagné, 2012; Fergusson, Boden, & Horwood, 2006; Friesen et al., 2010; Reckdenwald et al., 2013). With the scope of this model, researchers may invoke a simplified account of direct “transmission” of violence or may engage more critically with the social norms and psychological impact of experiencing violent contexts.
Relatedly, social learning theory posits that violent behaviours are learnt through observation and imitation of the actions of others, especially parents (Busby et al., 2008; Feiring, Simon, Cleland, & Barrett, 2013; Monson & Langhinrichsen- Rohling, 1999; Shorey et al., 2008). It is the dominant theory to explain the relationship between child abuse and adult DV perpetration (Fang & Corso, 2008). An adult’s violent orientation is postulated to be more general than the specific forms of violence that were observed in childhood (Ireland & Smith, 2009). Research findings are mixed, with some statistical modelling of victimisation and perpetration across the life course showing very poor fit to the theory (Cyr, McDuff, & Wright, 2006). Social learning theory is frequently used in conjunction with theories of the intergenerational transmission of violence.
Conflict theories, such as the coercion hypothesis, presume that conflict is a normal part of all interpersonal relationships within this model. Adults try to diffuse conflict through influencing the other party, with some relationships having higher rates of conflict than others (Shorey et al., 2008). A range of tactics can be used to diffuse conflict, including aggression and violence (Dutton & Goodman, 2005; Shorey et al., 2008). This ontology forms the basis of the Conflict Tactics Scale and has been criticised for the normalisation of violence it may encourage.
Theories of violence provide a broad explanatory framework that informs and shapes research on IPSV and re-victimisation.
Concepts
Unlike “models” of violence which provide a general, but dynamic, explanation of violence; a “concept” is a static explanation that is more likely to relate to a specific scenario or community.
A wide range of concepts were used by scholars to provide a framework for understanding the nature of re-victimisation and IPSV. These concepts provide a lens for understanding the ontology of violence. Four of the most significant concepts are outlined below.
The concept of family violence is favoured by some Aboriginal and Torres Strait Islander women “as it encompasses all forms of violence in intimate, family and other relationships of mutual obligations and support” (Mitchell, 2011). Given the complex kin structures and family relationships active in many Aboriginal and Torres Strait Islander communities, this differentiation is important as the lived experience of violence may be different to that experienced by women living in more exclusive dyad or nuclear family structures. Harry Blagg has argued that the use of a distinct term enables the impact of colonisation and “settlement” to be embedded in the understanding of patterns of interpersonal violence (Blagg, Murray, Ray & Macarthy, 2000; Keel, 2004). The definition of family violence almost always includes sexual violence, including CSA and IPSV (Keel, 2004). Some Indigenous academics argue that we need a conceptualisation of intimate partner violence that is culture and law centric and which does not rely so heavily on Western psychological and sociological theorising (Hovane, 2007, 2014). However in some other contexts the term “family violence” has been criticised for reducing the focus on the gendered nature of violence, and potentially suggesting that it is family dynamic, rather than male perpetration, that is primarily responsible for violence against women (Tomison, 2000).
Coercive control is a key concept in DV research and is particularly significant for feminist research in the area. Coercive control describes a particular relationship dynamic that is typically understood as the most damaging form of violence between partners – one characterised by the use of multiple strategies of threat and violence to control the behaviours of one’s spouse (Stark, 2009, 2010). A range of violent behaviours such as sexual coercion, sexual degradation and sexual assault may be central to broader patterns of coercion (Logan et al., 2013; Macleod, 2014b; Tanha, Beck, Figueredo, & Raghavan, 2010). Coercive control is often contrasted to situational couple violence, which is defined as relationships where fighting may arise in a specific context, but where this aggression is typically mutual and not characterised by attempts to constrain the day to day activities of the other party. Some couples may not fit neatly into either category, and thus a continuum should be understood to exist between situational couple violence and coercive control (Maas-DeSpain & Todahl, 2014).
Typologies
Typologies of violence are a common way of differentiating and understanding IPSV and are a highly specific descriptive model of violence.
A typology of violence is a way of identifying key similarities in the lived experience of certain types of violence, such as the emotional impetus for a particular act or the relational impact of specific behaviours. Typologies enable us to note how different contextual and situational factors affect the way that violence occurs and are often based in in-depth qualitative analysis. The typologies identified as part of this paper examined the experience of IPSV from different perspectives and thus made different distinctions.
A common typology distinguishes between different contexts of assault (e.g. rape as a continuation of other violence in a relationship as compared to rape as an expression of sadistic sexual arousal), while others distinguish between physical assaults that are part of sexual activity and those that happen before sex (“make up” sex) (Bergen & Bukovec, 2006; Finkelhor & Yllö, 1987; Maas-DeSpain & Todahl, 2014; Martin et al., 2007).
These typologies place IPSV in the context of the dynamics of violent relationships.
Typologies have also been developed for:
- sexual coercion (Maas-DeSpain & Todahl, 2014; Martinet al., 2007);
- perpetrator characteristics (Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000; Monson & Langhinrichsen-Rohling, 1999; Shorey et al., 2008); and
- more general DV dynamics (Bair-Merritt, Ghazarian, Burrell, & Duggan, 2012; see also, Johnson, 2006).
Typologies are rarely used to explain re-victimisation, possibly because it is difficult to provide sufficient detail across multiple types of violence in a way that would enable a meaningful typology to be produced.
Comparing approaches
Researchers may combine certain models, concepts or typologies to give a more complete explanation of violence (e.g. coercive control might be a part of an ecological model of violence). However some theories do not map together, as the underlying assumptions are incompatible (e.g. conflict theories do not align easily with certain typologies of violence).
Overall, a distinction can be made between two broad approaches to DV and SXA that were evident in the corpus.
The individualised approach, which is dominant in this corpus, tends to understand violence as an individual maladjustment that is expressed and influenced by interpersonal dynamics. This approach generally has a methodological focus on quantitative statistical methods and presumes that, while gendered violence is problematic, conflict is inevitable and normal (Wangmann, 2011).
In contrast, the societal approach tends to understand violence against women as an issue that, while always occurring in the context of individual choice and action, reflects macro social inequalities. Researchers working in this approach use a wide range of methods including quantitative, qualitative and mixed method modalities. In comparison to researchers with a more individualised approach, these researchers are more likely to value the insights available through qualitative methods (Hamby, 2014). These researchers are also more likely to value personal narrative and to assert that gendered violence is fundamentally unacceptable (Tanha et al., 2010).
The two approaches have substantial epistemological and political tensions. In line with these different understandings of the nature of violence and what should (and should not) be done about it, they produce research using very different methods and use different samples with different definitions of DV and SXA (see above) (DeKeserdy & Schwartz, 2001). Combined with the distinct limitations of survey instruments used in each approach, the two approaches produce remarkably different study findings (Desai & Saltzman, 2001; Holtzworth- Munroe, 2005; Romans et al., 2007; Wangmann, 2011; Zweig, Dank, Yahner, & Lachman, 2013).
Methods used by researchers examining re-victimisation and co-occurrence
Overall, most research on IPSV and re-victimisation uses retrospective single assessment reports (Friesen, Woodward, Horwood, & Fergusson, 2010). Below is an examination of the limitations and biases that are common in the literature on concurrent DV and SXA victimisation. In keeping with a more “Public Health” approach to reviewing available literature, we provide extensive detail of the nature of these limitations – this detail is not meant to dissuade the reader from engaging with the available research, but rather it aims to provide the basis for understanding the constraints on the findings that are outlined in the body of the paper.
Life-course research: Key limitations
Life-course studies provide an actuarial examination of risk factors by mapping variables against certain outcomes and then modelling patterns of risk. These studies are particularly common within re-victimisation research. The resulting models are able to provide insight into pathways to recidivism and victimisation, however they are often inaccurate due to low base rates (i.e. not many people in the population experience the event of concern) and tend not to be able to accurately plot patterns of victimisation (Andersen, Hughes, Zou, & Wilsnack, 2014; Campbell, 2005; Dietrich, Smiley, & Frederick, 2007). Despite looking at lived experience over time, most research of re-victimisation is not longitudinal, which makes the examination of a set of events that happened over a long period of time methodologically precarious (Goodlin & Dunn, 2010).
Key findings in this section:
- The lack of longitudinal studies reduces our ability to make conclusions about causal factors or the nature of victimisation over time.
- Research on re-victimisation and IPSV often focuses on sub-populations that are not representative of the general population.
- The way that research questions are presented (and who they are presented to) significantly affects the research findings.
- The stigma of re-victimisation and IPSV may create bias in reporting.
- The use of inconsistent definitions makes comparing results across studies difficult.
- Commonly used survey instruments, such as the CTS, have significant limitations.
Cross-sectional research: Key limitations
Cross sectional research is a “snap shot” of lived experience at one time. It can be used to effectively show the pattern of victimisation across a population at a particular moment. However, it does not allow for any analysis of the causal relationship between variables (Classen, Palesh, & Aggarwal, 2005; Krebs, Breiding, Browne, & Warner, 2011; Rees et al., 2011). Controlled longitudinal research that provides for a comparison group is the best way of obtaining causal information (Rees et al., 2011). Cross-sectional research may not allow for a full understanding of the complexity of daily experience, especially of different forms of violence happening in the same context (McFarlane, 2007; Sullivan, McPartland, Armeli, Jaquier, & Tennen, 2012).
The cross-sectional research found in this corpus is almost all retrospective (i.e. collecting data about things that have already happened). Some of the key limitations of the types of retrospective studies used in the corpus are detailed below.
Bias caused by population selection
Bias occurs when there is a systemic pattern of inaccurate reporting. Bias is a major concern for researchers completing retrospective studies as researchers rely on a participant’s memory of historic events (Lalande & Bonanno, 2011). By understanding the potential for bias, certain types of limitations of the available research are contextualised.
Much of the available research on IPSV and re-victimisation is unable to be extrapolated to findings about the general population, with research being focused on non-representative groups such as women who were attending psychology clinics (Friesen et al., 2010).
As noted earlier, a large amount of research on IPSV and re-victimisation has been completed with college students, and so these findings may not be generalisable to the broader population (Zurbriggen, Gobin, & Freyd, 2010). In comparison to the general population, college students are more highly educated, are disproportionately from advantaged socio- economic backgrounds, are less likely to have a severe disability and are generally young adults.
Women have participated in more violence research than men, potentially due to the tendency for academics to select study populations that are either couples (predominantly heterosexual, and thus both men and women participate in equal number) or victims (primarily women participants) (Shorey et al., 2008). The lack of comparable data for women and men may restrict our ability to meaningfully identify and articulate the gendered nature of violent behaviours.
In addition, research on perpetrators is less common than research on victims. Most perpetrator research focuses on men who have been convicted of DV and/or SXA offences. Researchers note that this is likely to result in bias, as this group is atypical of men who perpetrate violence and the very nature of their incarceration may mean that these men are unable to report certain behaviours to researchers (Clark & Quadara, 2010).
The use of differing ways of selecting research participants also affects generalisability. The way that a sample is selected affects the research findings, which is likely to further entrench theoretical, epistemological and ontological differences in approaches to researching and understanding violence. In the case of research into re-victimisation and co-occurrence, a divide emerges between the findings of research based on samples of women who are known to have been victimised (e.g. women who are in women’s shelters) and findings from studies that use a sample of women from the general population, with women from the former reporting substantially higher rates of abuse, as well as reporting more severe violence with greater personal, psychological and health impacts (Romans, Forte, Cohen, Du Mont, & Hyman, 2007).
Relatedly, the way that a survey question is phrased makes a significant difference to reporting and thus to the findings of research. This was demonstrated in a research project where participants in a single birth cohort study were interviewed twice on the same day. In each interview, the participants were questioned using a differently worded violence questionnaire. The difference in the results was so large that they found opposite gendered patterns of violence – in one, men were the primary victims of IPV, while in the other, women were the more common victims (Langley, Martin, & Nada-Raja, 1997; Magdol et al., 1997; Romans et al., 2007).
Bias caused by incomplete reporting
Under-reporting is an important issue in all research on sensitive topics. Under-reporting in research occurs when a study participant has experienced something but, when asked, does not tell the researcher about it. Scholars have identified that social desirability is a major factor in the under-reporting of SXA and DV, with a sense of shame about victimisation and/or perpetration, fears about researcher response and gendered social scripts affecting what women and men report (Chiu et al., 2013; Ludermir et al., 2008; Martin et al., 2007). IPSV is more frequently under-reported than other forms of DV or SXA (Heenan, 2004; Wall, 2012). With awareness of this phenomenon, some researchers work extremely hard to develop surveys where the phrasing and structure enable people to answer questions in a way that feels comfortable and thus to reduce the impact of under-reporting on the research findings (DeKeserdy & Schwartz, 2001).
In addition, recall bias is a result of individuals being more likely to recall events that are memorable; what counts as memorable varies with personal and cultural factors (Casey & Nurius, 2005; Hetzel & McCanne, 2005; Sullivan et al., 2012). Although research is mixed, evidence suggests that gender non-conforming expressions of violence are often particularly salient: so that men tend to underestimate their own violence and overstate the violence of their female partners (although tending to see such violence as not serious), while women tend to overestimate their own violence and underestimate the violence of their male partners (Dobash & Dobash, 2004; Doroszewicz & Forbes, 2008). In addition, recall bias may be present in the form of trauma-related symptomology such as individuals not remembering distressing events (e.g., childhood sexual abuse) (DeKeserdy & Schwartz, 2001). Retrospective studies on IPSV and re-victimisation, especially those that ask about events a long time ago or which ask very specific questions about incidents that occur frequently, are more likely to be affected by recall bias (Desai & Saltzman, 2001; Gobin, Iverson, Mitchell, Vaughn, & Resick, 2013; Jennings, Zgoba, Maschi, & Reingle, 2014).
Comparability: Inconsistent phenomena definitions
Numerous commentators have identified that DV and SXA are inconsistently defined in the research literature (DeKeserdy & Schwartz, 2001; Ireland & Smith, 2009). Some definitional variation is important, as this supports a nuanced understanding of violence, especially when considering contexts where alternative manifestations of gendered violence may be present (Tapia, 2014). However the use of different definitions while examining similar populations (and in research aimed at answering similar questions) may impact the comparability and utility of findings (Desai & Saltzman, 2001; Ireland & Smith, 2009).
Much of the mainstream DV research is unable to be utilised for an examination of IPSV, as it is common for DV research to either exclude IPSV altogether or fail to differentiate IPSV from other forms of violence (Panuzio & Dilillo, 2010; Schewe, Riger, & Howard, 2006; White, McMullin, Swartout, Sechrist, & Gollehon, 2008). This limitation is slowly being addressed as commonly used instruments, such as the Revised Conflict Scale (CTS2 – see below for a description), now provide for a separate measure of IPSV.
Sexual violence is a particularly difficult concept to define, and the literature has “a significant and pervasive problem of a lack of specificity in definitions” (Logan et al., 2013, p. 115). Such definitional difficulties affect both “cross-type” re-victimisation and IPSV research as both require a robust definition of sexual violence. In a critical examination of terminology used to refer to IPSV in 49 research documents, it was identified that there was no common terminology used in this research (Bagwell-Gray, Messing, & Baldwin-White, 2015). Problematically, IPSV researchers use the same words to mean different things, and as a result, studies are confusingly inconsistent and ultimately difficult to pool (Hamby, 2014).
Definitional inconsistency is particularly acute in research on sexual coercion. Sexual coercion can be understood as a spectrum of behaviours between emotional coercion and physical force, with researchers defining the beginning of “coerced sex” at different points (Finkelhor & Yllö, 1987; Heenan, 2004). For instance, they may:
- include (or exclude) social pressure as a type of coercion;
- include (or exclude) sexual pressure as a type of IPSV;
- include (or exclude) sex that was initially unwanted and then became wanted as a type of IPSV;
- distinguish between sex that was wanted and sex that has been consented to;
- include only sex that was either physically or verbally coerced; and
- include only sex that was physically forced.
(Bagwell-Gray et al., 2015; Brousseau, Hébert, & Bergeron, 2012; Lehrer, Lehrer, & Koss, 2013; Logan et al., 2013; Maas-DeSpain & Todahl, 2014; Martin et al., 2007)
These definitional variations, more apparent in sexual coercion research but still present in DV and SXA research more generally, make it very difficult to meaningfully compare studies or to concretely or confidently understand the nature of IPSV or re-victimisation.
Undifferentiated categories of violence
In addition to definitional inconsistency, the methods used in some studies fail to distinguish between different forms of violence, thus making it more difficult to understand the extent or characteristics of IPSV and re-victimisation.
Earlier research on DV had a tendency to combine physical and sexual violence in relationships. This was a consequence of:
- survey instruments that did not differentiate the two type of assault; and
- the way that the data was presented at write up (Wangmann, 2011).
Such conflation both obscured the nature of DV and made it impossible to identify the prevalence of IPSV within these studied populations. This limitation was also common in the collection and representations of data for childhood abuse that were presented in re-victimisation research (Bonomi et al., 2008; Cannon, Bonomi, Anderson, Rivara, & Thompson, 2010).
In much of the currently available literature, there are significant difficulties in distinguishing between multiple incidents involving a single perpetrator and a single (or multiple) incident involving more than one perpetrator (Casey & Nurius, 2005; Koss et al., 2007; Logan et al., 2013). In some research, multi-perpetrator cases are excluded or coded like single perpetrator incidents. Multi-perpetrator domestic violence and sexual assault research is particularly hampered by these types of systemic data limitations (Salter, 2014).
Commonly used survey instruments
There are a range of instruments used to measure the incidence and prevalence of domestic and sexual violence, including instances of IPSV and/or re-victimisation (Garcia-Linares, Pico-Alfonso, & Sanchez-Lorente, 2005). The selection of survey instrument determines what data is collected and thereby shapes the understandings of violence that emerge from the research. While much of the critique of these instruments engages with how experiences of IPSV are captured using these survey instruments, such critique is equally applicable to re-victimisation research that engages with DV.
Behavioural checklists, such as the Conflict Tactics Scale (CTS) and Sexual Experiences Survey (SES), involve concrete descriptions of behaviours. Typically, the research participant rates how frequently a certain behaviour occurs in their intimate relationship(s), including “never” (Desai & Saltzman, 2001). At the analysis stage, behaviours are separated into more or less severe forms of violence/coercion, based on expectations of harm to the victim. The survey developers selected the survey wording very carefully in order to minimise under-reporting – for instance “forced sex” is not described as “rape” (Abbey, Parkhill, & Koss, 2005). Despite being a standardised measure, researchers have some capacity to vary the definitions used in these scales, resulting in variation that can make comparison of research with other studies using the same instrument impossible (Logan et al., 2013).
Partner-specific behavioural checklists are the most commonly used instruments for re-victimisation and IPSV research, with the corpus analysed for this state of knowledge paper demonstrating a dominance of the CTS and SES. Prior to the release of the Revised CTS (CTS2), the SES was used primarily for research involving IPSV (the original CTS did not ask about sexual violence), although the SES has also remained in use in a large number of studies that were published post the release of CTS2 (Koss et al., 2007). Research using the CTS and CTS2 remains very common in the literature, despite ongoing criticisms of the scales (Hegarty, Bush, & Sheehan, 2005; Logan et al., 2013; Wangmann, 2011).
There are a number of key limitations of these scales that are noteworthy given the dominance of these instruments in the available literature:
Scales like the CTS2 do not identify the context of the violence, thereby not accounting for the functionality of the violence within a relationship (Próspero & Vohra-Gupta, 2008). Similarly, such scales are unable to identify the temporal sequencing of the violence (i.e in what order things happened) and are therefore very limited in their ability to separate defensive/protective violence from acts of aggression (Bonomi, Holt, Martin, & Thompson, 2006; Cole, Logan, & Shannon, 2005; Shorey et al., 2008). In addition, such scales typically do not engage with the intent of the violence, its emotional impact or the extent of physical harm, thereby potentially erasing significant gendered and/or typological differences (Hegarty et al., 2005; Palmetto, Davidson, Breitbart, & Rickert, 2013).
The CTS tends to find that males perpetrate most IPSV but that there is gender parity in perpetration of physical violence. These findings, while consistent across studies that use the instrument, are inconsistent with other methods of examining the same phenomenon such as examinations of police arrest data, law enforcement data, witness data and almost all other forms of self-report (Hamby, 2014). There is significant ongoing debate about the meaning and implication of the gender symmetry reported using CTS2 (Doroszewicz & Forbes, 2008).
Consistent with other retrospective research, these scales are affected by recall bias. Such bias is particularly apparent when researchers interview couples, with extremely poor agreement between couples regarding the nature of the violence experienced in the relationship (Dobash, Dobash, Wilson, & Daly, 1992).
Different types of self-report behavioural checklists provide substantially different findings regarding the prevalence of violence (DeKeserdy & Schwartz, 2001). For example, in a study of refuge users (n=138) that compared the rate of IPSV calculated using the CTS2 and the revised Sexual Experiences Survey, it was found that the CTS2 calculated 16.7 percent more cases of IPSV (63% vs 73.2%) (Moreau et al., 2015). As Hamby (2014) notes, studies based on self-report behavioural checklists show a startling range of between 2 percent and 60 percent prevalence of violence in supposedly similar “general” community samples. This suggests that “our [measuring] technology is far from adequate” (Hamby, 2014, p. 151).
Comparability of study findings
Overall, research on re-victimisation and IPSV is difficult to collate into a coherent understanding of these phenomena. The use of different definitions and collection methods, as well as differences in study population mean that it is difficult to compare research findings or complete meta-analyses of the available data (Garcia-Linares et al., 2005; Pico-Alfonso et al., 2006). Researchers emphasise the need for validated instruments, while also pointing out that an over-reliance on established methods reinscribes certain understandings of violence that may not reflect lived experience (Desai & Saltzman, 2001; Hamby, 2014; Sørbø, Grimstad, Bjørngaard, Schei, & Lukasse, 2013).
Before proceeding to an examination of the study findings, let us reiterate that the extent of the limitations of the studies examined in this review are consistent with the limitations of other emerging fields of quantitative research. All research has methodological limitations, epistemological variation and definitional inconsistencies – by acknowledging these in detail we do not dismiss the value of this work, but rather provide a meaningful basis for understanding the exact nature of the available research.
This state of knowledge paper now turns to the specific findings of the corpus.
Rates of re-victimisation and co-occurrence
There is extensive research on the rate of IPSV and re-victimisation of women. This research provides conflicting evidence regarding the extent of these two phenomena, however researchers are consistent in identifying both types of victimisation affect a significant proportion of women.
There was significant overlap in re-victimisation and IPSV populations, with many women experiencing re-victimisation that included IPSV. This means, similar to the overlap between DV and SXA more generally, that IPSV and re-victimisation are two populations that are unable to be fully distinguished from each other, and should thus be considered both as combined and distinct phenomena.
This section examines statistics related to the rate, prevalence and extent of re-victimisation and IPSV. This section is limited to an outline of statistical findings and provides brief commentary on related methodological considerations.
As discussed earlier, research on the prevalence or rate of victimisation is subject to a range of methodological limitations. Although such limitations are significant, this work is still valuable as it enables us to scope the extent of the problem. Moreover, researchers in this field consistently acknowledge the key limitations of such research, including the issue of under-reporting, and make efforts to address these through sensitive interviewing and ongoing improvements in research design. While acknowledging that these statistics are likely to be underestimates of the extent of the violence, they are nonetheless our best insight into the scale of the phenomena.
Key findings in this section:
- Estimated rates of re-victimisation vary according to what patterns of violence are included in the research design.
- Women who experienced child sexual abuse (CSA) were more likely to experience IPSV than women who had not experienced CSA. Similarly, these women were more likely to experience DV (not limited to sexual violence) in their adult relationships.
- Research was more mixed regarding patterns of re-victimisation that included violence during adolescence.
- There was little research on re-victimisation rates for adult victimisation for separate DV and SXA incidents.
- Estimates of IPSV rates varied significantly depending on the definition of IPSV used for the research.
- In the research examined for this paper, intimate partner sexual coercion was reported by between 24 percent and 62 percent of women. Intimate partner sexual assault was reported by between 1.7 percent and 46 percent of women.
- Most women who had experienced IPSV did not consider that the incident was an assault.
- IPSV generally occurs in the context of other forms of violence.
Re-victimisation rates
As outlined earlier in this article “cross-type” re-victimisation occurs when a woman experiences separate incidents of SXA and DV that involve different perpetrators across her lifetime.
Re-victimisation is an endemic issue, with longitudinal studies indicating that more than half of female victims of childhood sexual abuse experience physical or sexual re-victimisation (n = 159) (Barnes, Noll, Putnam, & Trickett, 2009).
Despite this, re-victimisation should not be considered an inevitable consequence of initial victimisation, as approximately a third of women recover rapidly from CSA and do not experience ongoing traumatisation and most are not re-victimised (Hébert, Lavoie, Vitaro, McDuff, & Tremblay, 2008). The ANROWS additional analysis of the 2012 PSS indicated that 67.6 percent of all women in Australia who had experienced childhood abuse did not experience cohabiting partner violence as an adult (this is estimated to be 1.1 million women) (Cox, 2015).
Understanding the extent of re-victimisation requires an engagement with a range of scenarios of victimisation. This paper examines available literature on re-victimisation in the following scenarios:
- re-victimisation involving child sexual abuse and intimate partner sexual violence;
- re-victimisation involving child sexual abuse and adult domestic violence (in research where type of adult domestic violence was not identified);
- re-victimisation involving child and adolescent victimisation; and
- re-victimisation involving separated instances of domestic violence and non-intimate-partner sexual assault.
In keeping with the focus of this review on “cross-type” victimisation, we do not consider the rate of “same-type” re- victimisation (i.e. experience or witnessing of DV and later adult DV victimisation or CSA and then experiences of SXA as an adult). Given the scope of this project, examinations of the rates of CSA and adult IPSV are within scope as IPSV is a form of DV.
Child sexual abuse and adult domestic violence
Women who experience CSA are more likely than those who have not experienced CSA to experience DV in their adult relationships (Garcia-Linares et al., 2005; Pico-Alfonso et al., 2006). In a Canadian sample (n = 16993), in comparison to women who hadn’t experienced CSA, those who had were 2.44 times more likely to experience psychological DV and 2.75 times more likely to experience physical DV (Daigneault et al., 2009). In a smaller US study (n = 637), and in comparison to women who had not experienced DV, women who had experienced DV were five times as likely (5% vs 25%) to have experienced CSA (Seedat, Stein, & Forde, 2005).
Estimates of prevalence of re-victimisation involving CSA and DV vary significantly. The percentage range of all women research participants who identified experiencing both CSA and DV was between 25 percent (from a case control study of women attending STI clinics) and 40 percent (from a small Spanish cross-sectional study) (Garcia-Linares et al., 2005; Williams, Larsen, & McCloskey, 2010).
A minority of studies show no relationship between CSA victimisation and adult DV victimisation (Murphy, 2011; Renner & Whitney, 2012). For example, a population based cohort study of Australian women found a statistically insignificant increase in the rate of CSA (contact and no contact) and/or physical abuse (27% vs 36%) for women who had experienced IPV (Schei, Guthrie, Dennerstein, & Alford, 2006).
More general research on violence shows that forms of child abuse other than CSA also have an effect on adult victimisation. According to the 2012 PSS, over half a million women in Australia have experienced both abuse when they were a child as well as cohabiting partner violence. This is a third of all women in Australia who have experienced childhood abuse (Cox, 2015). In a research project involving 3201 women, those who had experienced either physical, sexual or emotional abuse as a child were about 7 times more likely to experience abuse as an adult, while those who had experienced all three types of abuse as a child were 36 times more likely to experience abuse as an adult (not limited to DV incidents). This research found a dose response, with women who had experienced more incidents of child abuse experiencing more incidents of abuse in adulthood (Chiu et al., 2013; see also Murphy, 2011). Some research suggests that a combination of CSA and other forms of childhood abuse has greater impact than CSA only, and a sample of 10,187 adolescents found that neglect was a stronger predictor than CSA for future DV victimisation (Cannon et al., 2010; Renner & Whitney, 2012). Such findings are consistent with older research which emphasises that the impact of CSA is altered by broader environmental factors, including other violent and neglectful behaviours (Briere & Elliott, 1994).
Additional relevant literature is outlined in Appendix B.
Child sexual abuse and intimate partner sexual violence
A subset of women who experience re-victimisation across childhood abuse and adult domestic violence are women who experience adult IPSV.
Women who experience CSA are more likely to experience domestic violence that involves IPSV than women who have not. In a large national stratified sample of Canadian men and women (n=16,993), it was found that women who had experienced CSA were 3.68 times more likely to experience IPSV than women who had not experienced CSA (Daigneault, Hébert, & McDuff, 2009). Similarly, after adjusting for demographic variables, in a study of Chinese university students (n=3388), participants were 2.04 times more likely to have experienced IPSV if they had a history of CSA (Chan, 2011). In a study of women who had recently obtained protection orders, one in three women had experienced both threatened/forced sex by their partner and sex before the age of 14: in contrast, one in five (19.8%) of these women had experienced CSA but not IPSV (Cole et al., 2005).
Child and adolescent victimisation
Researchers, particularly from the psych-sciences, consider adolescence[3] to be a distinct developmental phase (Shaffer & Kipp, 2013). Increased personal independence and sexual exploration mean that the nature and expression of violence in adolescence is distinct from that found in childhood or adulthood. Although some studies do not use this category, the research on young people in their teens and early-20s is a distinct aspect of the corpus and needs to be examined separately from research on child and adult victimisation (Levy-Peck, 2014a). Below we outline relevant research regarding adolescent female victims.
Estimates of adolescent dating violence are difficult to obtain, particularly given the difficulty of aligning research and community terminology and the commonality of “horseplay” and “wrestling” in this age group, which inflates the reported frequency of physical violence, especially when researchers use behavioural checklists such as the CTS that do not place acts of violence in context (Hamby & Turner, 2013; Levy-Peck, 2014a). When reports of violence are limited to incidents that result in injury or fear or have a sexual aspect; then rates of adolescent dating violence were found to be similar to those in general adult populations (Hamby & Turner, 2013). The US Centres for Disease Control and Prevention reports dating violence rates of between 7.6 percent and 12.2 percent (Eaton & Matamala, 2014; Eaton et al., 2012). In a study of 917 teenage girls, 3.9 percent were in long-term dating relationships where they experienced more than one incident of violence (Gagné, Lavoie, & Hébert, 2005).
In most studies, CSA is significantly associated with SXA in adolescence, however a minority of papers show no statistically significant relationship between childhood violence exposure and later victimisation (Barnes et al., 2009; Gagné et al., 2005; Littleton, 2014; Rich, Gidycz, & Warkentin, 2005). Similarly, adolescent women who have experienced CSA report high rates of dating violence (Miller, Breslau, et al., 2011). A small study of adolescent female CSA survivors (n=126) found dating violence rates of 45 percent for physical violence and 90 percent for psychological violence (Cyr et al., 2006). Adolescents with a history of CSA reported double the rate of dating violence victimisation than their non-abused peers (n=774) (Hébert et al., 2008).
Research is mixed regarding the effect of adolescent victimisation on adult sexual victimisation. Several studies indicate that adolescent victimisation was a stronger predictor of adult sexual victimisation than CSA (Classen et al., 2005; Gagné et al., 2005; Siegel & Williams, 2003; Smith, White, & Holland, 2003). However, for incarcerated women (n=484), adolescent sexual assault did not increase the risk of adult sexual assault in women who had also experienced CSA (Raj et al., 2008).
More than physical or sexual violence separately, the co- occurrence of adolescent sexual and physical dating violence is associated with DV victimisation in young adulthood (Miller, 2006; White & Smith, 2000).
Separated instances of adult sexual assault and domestic violence
There is very little research available regarding “cross-type” re-victimisation when all incidents occurred during adulthood. One of the few available studies examined re-victimisation of DV and military sexual trauma, and found a co-occurrence rate of 52.7 percent (see also Iverson, Mercado, Carpenter, & Street, 2013; Kelly, Skelton, Patel, & Bradley, 2011).
Some research is available, however, on re-victimisation when it includes only DV or SXA violence, with studies examining adult and adolescent SXA re-victimisation (Macy, 2007; Ranjbar & Speer, 2013; Rich et al., 2005) and experiences of DV in multiple consecutive relationships (Garcia-Linares et al., 2005; Vatnar & Bjørkly, 2008).
Co-occurrence rates
Domestic violence is characterised by a range of abusive tactics, one of which is IPSV. In research on IPSV, it is typical to distinguish between IPSV and other forms of physical violence and emotional abuse. Such separation enables us to understand the structures and mechanisms of violence in greater detail and to meaningfully examine the rate of IPSV in relationships. However, this type of conceptualisation of IPSV may de-emphasise the physically and emotionally violent aspects of IPSV incidents. The use of these distinctions in this section reflects the nature of the available research, and does not imply support for the conceptual separation of IPSV from other dynamics of DV.
A note on lived experience vs research definitions
Some women do not define their experience of sexual coercion as assault. In a study of college women (n = 1060), of those who had experienced behaviours that were categorised as sexual coercion:
- 49.5 percent said they were not victimised;
- 45.4 percent said that the incident was a “serious miscommunication”; and,
- 5.2 percent said they had experienced an assault.
(Orchowski, Untied, & Gidycz, 2013)
Even for forced sex, the lived understanding does not necessarily align with research categories. Between 30 percent and 47.9 percent of women who have experienced forced sex by an intimate partner identify the experience as rape (Littleton, Breitkopf, & Berenson, 2008; Logan et al., 2013). These findings have both research and practice implications: as noted by Bergen “[i]f they do not define their experiences as rape, women are unlikely to report the violence or seek outside assistance” (2006, p. 6).
At a research level, this lack of alignment requires careful and nuanced consideration of the findings: on the one hand, sexual coercion is one of several behaviours that constitute IPSV. It is the most common form of IPSV. When statistics on IPSV include sexual coercion, they may be inaccurately read as indicating a more brutal form of abuse. In this way, care needs to be taken not to accidentally exaggerate the extent or nature of the problem. On the other hand, however, evidence also points to the difficulty in women identifying sexual assault within relationship settings and the cognitive dissonance that such realisations may cause. In this context, while women may not identify their experiences as assault we must be careful not to presume that this means that such assaults are not traumatising, brutal or explicitly violent. The following quote from a participant in a New South Wales (NSW) qualitative study demonstrates some of the cognitive pressure that women may feel maintain certain understandings of their experiences: “I’d talk myself out of thinking that I’d been raped… My reaction was this can’t be true. You’re stupid, change your mind” (Parkinson & Reid, 2014, p. 139).
The nature of IPSV and the impact of such assaults is only ever partially visible through an engagement with research. In order to help the reader be sensitive to some of the constraints of empirical findings, in the discussion of prevalence, where possible, definitions have been noted and findings contextualised.
Intimate partner sexual violence
The following rates are for IPSV incidents only and do not reflect other forms of non-sexual violence that may occur in a relationship.
Within populations not limited to IPV survivors, intimate partner sexual coercion was reported by between 24 percent and 62 percent of women (Brousseau et al., 2012; Cole et al., 2005; Doroszewicz & Forbes, 2008; El-Bassel et al., 2007; Messing, Thaller, & Bagwell, 2014; Próspero & Vohra- Gupta, 2008; Sabina & Straus, 2008; Stockman et al., 2013). The highest rate of coercion was recorded in a study of 209 heterosexual couples, surveyed using the Sexual Experience Survey (Brousseau et al., 2012). The lowest rate was found in the largest study (n = 799), which examined women receiving Emergency Department care and used the CTS2 instrument (El-Bassel et al., 2007).
Intimate partner sexual assault was reported by between 1.7 percent and 46 percent of women (Black et al., 2011; Daigneault et al., 2009; Messing et al., 2014; Miller, 2006; Morokoff et al., 2009; Romans et al., 2007). The lowest rate of sexual assault was found in a Canadian population survey (n = 17,005) (Daigneault et al., 2009; Romans et al., 2007). Other representative samples have found rates of between 5.9 percent and 9.4 percent (Black et al., 2011; Miller, 2006). The highest rates were found in high risk populations, including women experiencing police involved IPV, and women who were recruited at sexual health and substance use clinics (Messing et al., 2014; Morokoff et al., 2009).
The Australian component of the International Violence Against Women Survey found that “[b]etween 5-7% of [respondents] who had a current or former partner had experienced [IPSV]” (Mouzos & Makkai, 2004; Wall, 2012). The 2012 PSS produces a slightly higher estimate, with 9.2% of women in Australia having reported ever having experienced sexual assault by an intimate partner they may or may not have been living with (Cox, 2015). A small (n = 233) prospective study of middle-aged Australian-born women found 1.3 percent of all women had experienced IPSV and 11.6 percent of women who experienced domestic violence in the last 12 months had experienced IPSV (Schei et al., 2006). There is very little research on IPSV in Aboriginal and Torres Strait communities, although it is generally understood to be a frequent part of family violence (Adams & Hunter, 2007).
Additional relevant literature is outlined in Appendix B.
Intimate partner sexual violence and non-sexual physical assault
The lived experience of domestic violence which involves the use of both IPSV and other forms of physical DV is both common and well documented (Spohn & Tellis, 2012). As noted above, both IPSV and other forms of physical DV contribute to the overall dynamic of DV, however research in this field frequently separates these forms of physical violence.
Many of the characteristics of IPSV mirror those of other forms of physical DV – the assaults typically occur in private, and are witnessed (if at all) by people known to both the perpetrator and victim (e.g. family and friends) and, when the abuse is more severe, they often result in physical injury (Tellis, 2010). Conversely, although most women who experience IPSV also experience other forms of physical violence, some researchers argue that the co-occurrence of IPSV and other forms of physical violence is a distinct form of violence that is different from either form by itself (Bagwell-Gray et al., 2015; Katz et al., 2008; White et al., 2008).
Reported rates of DV that include incidents of both IPSV and other forms of physical DV vary depending on study population, with between 64 percent and 100 percent of women who indicated that they were raped by their partner also reporting that they were physically abused by them (McFarlane, Malecha, Watson, et al., 2005; Smith, Thornton, DeVellis, Earp, & Coker, 2002; Vatnar & Bjørkly, 2008; White et al., 2008). Similarly, of women who have been physically assaulted by their partner, between 26.2 percent and 68 percent had experienced partner rape/sexual assault, with between 30 percent and 75 percent experiencing sexual victimisation (i.e. the range of actions from sexual coercion through to sexual assault) (Campbell et al., 2013; Cole et al., 2005; Krebs et al., 2011; Martin et al., 2007; McFarlane, Malecha, Gist, et al., 2005; Spiller et al., 2012).
Some women experience violent physical assault and sexual assault within the same incident. In 30 percent of cases of intimate partner rape (n = 124), women reported that they were physically assaulted in response to their own physical refusal of forced sex (McFarlane, Malecha, Watson et al., 2005). A study of help-seeking women found that 70 percent had experienced sexual violence and physical attack simultaneously (Vatnar & Bjørkly, 2008).
IPSV may also co-occur with other forms of physical violence when it occurs in the form of post-violence sexual assault. A research project with men arrested for physical assault of their partner found that 13.6 percent reported having made their partner have sex with them immediately after “a violent argument, even though she didn’t want to have sex” (Basile & Hall, 2011).
In a study of patterns of daily abuse, other forms of physical violence were 3.4 times more likely to occur on days when IPSV also occurred (in contrast, non-sexual physical abuse was 64 times more likely to occur on days when psychological abuse occurred) (Sullivan et al., 2012). Women who experienced both non-sexual and sexual domestic violence were more likely to be punched, kicked and be attacked with sharp objects (e.g. knives) than women who experienced non- sexual physical DV only (Garcia-Linares et al., 2005). In a sample of 449 mothers who were living in DV refuges and had experienced non-sexual physical DV, those who had also experienced IPSV were physically abused more than those who had not experienced IPSV (Spiller et al., 2012).
Overall, these findings suggest that when women experience IPSV and other forms of physical assault, the non-sexual physical assault is more physiologically damaging than if it occurred in a context where IPSV was not also being perpetrated.
Conclusion
Identifying the rate of re-victimisation or IPSV is difficult. Especially when using more inclusive definitions of violence, current research demonstrates high rates of IPSV and re- victimisation. Like other sensitive topics addressed through retrospective quantitative research, findings varied according to population, but also by which survey instrument was used. The extent of the variation limits our ability to understand the epidemiology of these patterns of victimisation, and thus restricts our ability to plan or respond to these issues.
Characteristics of incidents of intimate partner sexual violence
Key findings in this section:
- IPSV is an expression of DV.
- IPSV is often limited to emotional coercion, however when it was physically violent, it frequently resulted in injury.
- IPSV is often part of a larger pattern of coercive control in a relationship.
- Women are unlikely to fight back in an IPSV incident.
- IPSV often occurred at regular intervals over a long period of time.
“When you are raped by a stranger you live with a frightening memory.
When you are raped by your husband you live with your rapist.”
Research on the nature of the experience of IPSV demonstrates that it is often limited to emotional coercion but when it is physically violent, it frequently results in injury. The information below is largely limited to more severe forms of IPSV, and does not take into account the large number of sexually coercive incidents that are included in the rates of IPSV examined earlier in this paper.
(Comparable information on the nature of the experience of re-victimisation is extremely limited and thus not included in this paper.)
IPSV is one of many abusive tactics that are characteristic of domestic violence and for some women it is a tactic which is central to the violent dynamic of the relationship (Stack, 2010). Although IPSV is a physical act, many researchers separate it from other forms of physical violence: similarly, such violence (although emotionally abusive) is often conceptualised as distinct from emotional abuse that happens in other contexts.
Given these conceptual structures of the available research, it is therefore meaningful to say that research indicates that IPSV often co-occurs with other forms of physical and emotional violence (Sullivan et al., 2012). For example, in one investigation, almost all (98.2%) men arrested for physically assaulting their partner were sexually violent towards her, with very high rates of combined non-sexual physical violence, psychological abuse, stalking and sexual violence (96.8%) also reported (Basile & Hall, 2011). Similarly, in a study of 157 women who were seeking help for DV, 1.2 percent of women experienced psychological and sexual abuse (but not physical abuse), while no women experienced non-sexual physical abuse and sexual abuse (without emotional abuse): in contrast 35.2 percent experienced combined physical, emotional and sexual abuse (Vatnar & Bjørkly, 2008). This suggests that DV almost always involves a range of abuse methods, that emotional abuse is a common aspect of many violent scenarios, and that IPSV is a less common method of coercive control that may be indicative of more sustained structures of violence.
There is limited research on the temporal patterns of IPSV. Older research indicates that women raped by their partners experience an average of 1.6 rapes per year (Tjaden & Thoennes, 2000). More recent research suggests higher frequency, with one study finding that 40 percent of women in a Spanish cohort experiencing non-sexual physical DV were raped more than two times a month, and another finding that 38.9 percent of Norwegian women who were seeking help for DV having had unwanted sexual relationships with their partner at least once per week (Garcia-Linares et al., 2005; Vatnar & Bjørkly, 2008). When sexual assault and other forms of physical violence co-occur, the assault tends to happen in a repeated pattern of violence (Basile, 2008; Bergen & Bukovec, 2006; Schafran, 2010). For women who used illicit substances and were asked by researchers to keep a diary of their IPV abuse (n = 49), IPSV occurred on 4.1 percent of reporting days, making it the least common form of violence reported (Sullivan et al., 2012).
Violent and brutal sex acts are commonly reported by women who experience IPSV (Stack, 2010). A range of sex acts are reported, with multiple acts, especially sexual activity that includes both anal and vaginal penetration, more common in IPSV incidents than in assaults by strangers (Möller et al., 2012). In a sample of 56 women who had experienced repeated IPSV, the most common combination of sex acts was forced vaginal, oral and anal sex (37%), followed by forced vaginal sex only (23%) (Campbell et al., 2013). Women also frequently report being woken by their partner having sex with them and sex after a violent argument (Logan, Walker & Cole, 2013). There is currently insufficient evidence to determine how the brutality of an IPSV rape affects the impact of the assault on a woman’s wellbeing (Logan et al., 2013). IPSV also involves some specific forms of coercion related to sexuality and/or sexual activity, such as use of sexual degradation, sexual bargaining and threats of harm as a way of pressuring a woman to have sex (Logan et al., 2013).
As IPSV happens in established sexual relationships, the lived experience of sexual consent is complex as there are established patterns of sexual behaviour (Logan & Cole, 2011). Sexual routine, experiences of prior consensual activity and a presumption of continuous consent may create contexts where unwanted sex is agreed to, or where asking for sex to stop is not seen as a possibility (Clark & Quadara, 2010; Lazar, 2010; Schafran, 2010). Moreover, in the context of continual violence, it is arguable that all sex is non-consensual as the capacity for a woman to “freely consent” to sex may be fundamentally compromised (Logan & Cole, 2011; McOrmond-Plummer, 2014). As a participant in an Australian Institute of Family Studies (AIFS) research project said “… [b]ecause I was too terrified of him, that if I didn’t say yes to that, he would rape me. I agreed to it. But it wasn’t really agreeing, because I was agreeing under fear” (Clark & Quadara, 2010, p. 19). Similarly, a lawyer describing a case she represented of a woman who was charged with intentional murder after defending herself from her husband, wrote: “Her husband forced sex on her multiple times, and at a certain point in their marriage, she never had consensual sex with him again. Though she would resist at times, most of the time she was too fearful” (Stack, 2010, p. 540). The context of prior sexual consent, and the likelihood of IPSV being a repeated form of sexual violence, may make IPSV more traumatic than assaults by strangers or acquaintances (Kerr, 2014; Schafran, 2010).
Some research indicates that, when compared to women sexually assaulted by strangers or acquaintances, those who were assaulted by their partner were more likely to be physically injured (but not more likely to experience genital injuries) (Culbertson & Dehle, 2001; Möller et al., 2012). Women who experience IPSV were more likely to be strangled by their partner than women who experience non- sexual physical assault only (n = 432) (Messing et al., 2014). Physical injury may also occur when women are assaulted in response to resisting a sexual advance (McFarlane, 2007; Montoya et al., 2013).
IPSV does not, of course, need to involve physical injury (Kerr, 2014; McOrmond-Plummer, 2014). In addition to the simple materiality of the incident, IPSV may involve physical restraint and other embodied violence. For example, when examining physically forced sex, the use of physical restraint as a form of violence is more common than physical harm or verbal threats (n = 336) (Stermac, Del Bove, Brazeau, & Bainbridge, 2006).
Moreover, there is not a deterministic relationship between the nature of a woman’s resistance to IPSV and the severity of the crime. In a study that examined how women resisted IPSV, the most common mechanism was to remain immobile, followed by defending oneself, trying to escape, and trying to reason with the perpetrator (Garcia-Linares et al., 2005). Given that IPSV may occur in relationships with substantial histories of coercive control and violence, the ability for women to “resist” must always be understood with sensitivity to what types of actions are possible in the context of the violent relationship as a whole. As one women interviewed for an AIFS research project commented: “…usually he probably would just pin me down. He wasn’t violent, he just would hold me down. But if I tried to get away he would increase the pressure in order to keep me there so then it would hurt more” (Clark & Quadara, 2010, p. 36). At a physiological level, it is important to note that women may experience “tonic immobility” (freezing) during violent incidents, thus making resistance impossible – in such contexts, not resisting is symptomatic of the traumatic nature of the incident (Campbell, 2012).
Research indicates that IPSV is a common feature of cases of sustained DV that include aspects of coercive control (Tellis, 2010). Australian qualitative research found that women reporting IPSV described their violent relationships as characterised by reward and punishment exchanges and that their perpetrator relied on established sexual behaviour that normalised violence. This research also indicated that IPSV perpetration, including sexual coercion, was a deliberate and intentional act by perpetrators that should not be minimised or considered merely the consequence of a misunderstanding between partners (Clark & Quadara, 2010).
Finally, threats to kill a partner are more common in relationships that include IPSV than in other abusive relationships (Messing et al., 2014). In a study of 148 women who were seeking help from the justice system, and in comparison to the sub-group of women who were victims of physical violence from their partner, those who experienced IPSV were more likely to also experience a range of behaviours associated with femicide, including their partner threatening to kill them (OR 1.30) and threatening to harm their children (OR 4.56) (McFarlane, Malecha, Gist, et al., 2005). Moreover, IPSV is a risk factor for intimate partner homicide (Campbell, Webster & Glass, 2009; Palmer & Parekh, 2014; Sack, 2010).
Risk factors for re-victimisation and co-occurrence
Key findings in this section:
- The relationship between CSA and adult victimisation is mediated to some extent by the severity of the abuse during childhood.
- The emotional effects of violence may further increase a person’s vulnerability to future victimisation (e.g. through increased emotional dysregulation).
- Drug and alcohol use may be a precursor, consequence or risk factor associated with IPSV and re-victimisation.
- There was mixed evidence regarding the impact of sexual risk taking on the risk of IPSV and re-victimisation.
- The nature of an intimate relationship, including the length of the relationship and the way that partners routinely communicate, has been shown to impact on the expression of violence within the relationship.
Researchers have noted that while the social and political contexts of gendered relations affect the patterns of domestic and sexual violence within a society, individual instances of abuse are also affected by individual and relational characteristics (Goldscheid, 2006). These individual risk factors reflect the failures (and successes) of the systems in which a person is located, so a risk factor may be mitigated by appropriate care and support or exacerbated by the lack of it.
Moreover, it is broadly acknowledged that the aetiology of violence is extremely complex, involving the interactions between individual, inter-personal and societal factors (Krug, Mercy, Dahlberg, & Zwi, 2002; Martin et al., 2009). Such influences are not evenly distributed, with some sub- populations affected by different constellations of risk factors (Cattaneo & Goodman, 2005).
Given the reliance of IPSV and re-victimisation research on retrospective cross-sectional designs and the heavy disciplinary basis towards the psych-sciences and public health, it is particularly important to emphasise that risk factors are not the same as causal factors (Martin et al., 2007). The difference between causal and risk factors was described in a paper regarding sexual assault prevention for women with intellectual disabilities which said “none of these [risk factors], however, are known causes of sexual assault. Rather, women with these factors are more significantly burdened with sexual assault experiences”. This distinction is critical to avoid discussions of risk morphing into discussions of blame (Barger, Wacker, Macy & Parish, 2009, p.251; see also, McOrmond-Plummer, 2014).
Most of the research reviewed in this paper is only able to identify a correlation between particular life events or characteristics and violence. Unless further longitudinal research or research with dose-response findings is completed, causation will remain unclear. The surveyed research is almost all quantitative, with minimal qualitative research on risk factors identified through the search strategy.
Previous victimisation
Below is an outline of some of the factors that may augment the relationship between CSA and adult DV/SXA victimisation. As identified above, care should be taken when considering risk factors, as most research in this field is cross-sectional and thus cannot identify causal relationships between variables. In addition, most available research on re-victimisation has been deemed out of scope from this state of knowledge paper research as it typically examined same-type victimisation from childhood to adulthood (e.g. CSA to adult SXA) (Cuevas, Sabina, & Milloshi, 2012).
Research indicates a moderate to strong relationship between CSA and commonly researched forms of DV (physical, emotional and sexual) (Coid et al., 2001; Daigneault et al., 2009; Macy, 2007; Simmel, Postmus, & Lee, 2012; Whitfield, Anda, Dube, & Felitti, 2003).
The strength of the relationship between CSA and later DV (including IPSV) victimisation may be mediated by the extent of the abuse experienced as a child (Roodman & Clum, 2001). A range of characteristics of CSA are associated with a greater risk of adult DV victimisation, including that the CSA:
- was over a long period of time;
- occurred frequently;
- used force;
- involved penetration; and
- was perpetrated by a known person or guardian.
(Classen et al., 2005; Simmel et al., 2012; Tapia, 2014; Van Bruggen, Runtz, & Kadlec, 2006; Yoshihama & Horrocks, 2010)
Several studies identified a graded relationship between child abuse and DV (Jankowski, Leitenberg, Henning, & Coffey, 2002). For example, a study of 975 college undergraduates found that the frequency of interpersonal trauma as a child was correlated with the number of adult interpersonal victimisations (Pereda & Gallardo-Pujol, 2014).
In international predictive modelling research from the US and Canada, the pathway between childhood and adolescent SXA and adult sexual and DV victimisation is indirect (Fargo, 2009). A range of situational factors may increase the likelihood of a woman experiencing re-victimisation after CSA (Daigneault et al., 2009). These factors include:
- being incarcerated (Wolff, Shi, & Siegel, 2009);
- being poor (Poister, Tusher & Cook, 2010);
- adolescent and adult sexual behaviours including a greater number of partners (Messman-Moore & Long, 2003);
- having a recent victimisation (Classen et al., 2005); and
- experiencing Post-Traumatic Stress Disorder (PTSD) symptoms (Hetzel & McCanne, 2005).
Although research is currently not available, in the Australian context, such patterns may be compounded for certain disadvantaged sub-populations such as Aboriginal and Torres Strait Islander women.
Mediating factors, either in the characteristics of the CSA or the adult victimisation can only partially explain the relationship between CSA and later victimisation, with researchers acknowledging the vast complexity of victimisation experiences and the interdependence of risk factors (Simmel et al., 2012). Moreover, it is important to note that while the experience of abuse in childhood is traumatic, the impact of this may be mediated by appropriate and sensitive systems responses to children in need and the provision of ongoing support to women who have experienced abuse.
Psychological risk factors
(The psychological impact of re-victimisation and IPSV is discussed in detail in Sub-populations with differential patterns of victimisation and Health impacts of re-victimisation and co-occurrence sections of this paper.)
Research into psychological risk factors is almost exclusively based in individualised psychological methodologies. These approaches tend to look at risk without examining the impact of protective or systems responses in mitigating the ongoing impact of psychological risk and is consistent with the disciplinary background of this material. Moreover, such approaches are often focused on statistical trends and tend not to contextualise findings. The mirroring of this disciplinary norm in this paper does not in any way imply a judgement of behaviours or suggest that a woman is to blame for her victimisation.
A range of emotional states have been associated with both IPSV and re-victimisation. These are consistent with findings for other forms of VAW and include:
- externalising behaviours (socially inappropriate anger and other behaviours that are an expression of internal distress);
- poor emotional regulation (experiencing very strong and/or highly variable emotions);
- experiential avoidance (avoiding certain situations or experiences);
- anger;
- hostility; and
- shame.
(Armour & Sleath, 2014; Classen et al., 2005; Gibson & Leitenberg, 2001; Hébert et al., 2008; Messman-Moore, Walsh, & DiLillo, 2010)
Despite the lack of longitudinal research in this area, there is some research indicating that existing emotional volatility may impact on re-victimisation risk (Messman-Moore et al., 2010). Initial research suggests that self-sufficiency and a sense of mastery may protect against sexual re-victimisation (Macy, 2007).
There are several explanations of the mechanism that means that emotional dysregulation may be linked to later victimisation, however research is far from conclusive on whether these are true models (Macy, 2007). Each of these explanations provides a possible mechanism by which external, social and systemic factors may alter a woman’s risk of victimisation:
- For CSA victimisation to DV perpetration: Shame and guilt related to victimisation may predispose perpetrators to hostile responses to their partners and thus increase the risk of violence (Kernsmith, 2006).
- For CSA to DV re-victimisation: Effects of family of origin violence on norms of relationship are one possible explanation, however evidence is sparse (Busbyet al., 2008).
- For sexual re-victimisation, including IPSV: Women may try to regulate their emotional distress through behaviours that may increase their risk of victimisation (e.g. alcohol use, large numbers of sexual partners) (Messman-Moore et al., 2010).
- For gendered violence re-victimisation, including SXA and DV: Emotional dysregulation or trauma may affect a woman’s ability to process information, assess risk and act in a way to ameliorate risk, thereby increasing her susceptibility to victimisation(Messman-Moore, Ward, & Brown, 2009).
Post-Traumatic Stress Disorder (PTSD) is a common consequence of IPSV or re-victimisation. It is, however, also a significant risk factor for re-victimisation and has been shown to mediate the relationship between CSA and adult sexual victimisation (Arata, 2000; Iverson et al., 2011; Messman-Moore, Long, & Siegfried, 2000; Messman-Moore et al., 2009). There is some evidence that the relationship between PTSD and sexual assault may be explained by the symptomology of PTSD, in particular the moderating of distress through the increased use of drugs and alcohol (Messman-Moore et al., 2009). This relationship is less clear in the case of DV (including IPSV), with a small number of studies, including an interview and self-report study of women seeking help for DV, finding that the relationship between PTSD symptoms and childhood abuse was not mediated by DV experience (Gobin et al., 2013).
Relational and behavioural risk factors
Alcohol and other drugs
Consistent with research on VAW as a whole, research indicates that alcohol use may be a precursor, consequence or risk factor associated with IPSV and re-victimisation (Busch-Armendariz, DiNitto, Bell, & Bohman, 2010; Classen et al., 2005; Schewe et al., 2006). Evidence is mixed regarding the extent of the relationships between AOD use and re-victimisation or IPSV, and whether these associations are strong enough to be classed as causal (Macy, 2007).
Women’s patterns of alcohol and other drug use may, or may not, be problematic or addictive in nature. For some women, their use results in stigma and discrimination and may be classed as a criminal act. For these women, the nature of the risk associated with alcohol and other drug use is more complex than for those for whom alcohol use is socially sanctioned and where its impact on IPSV and re-victimisation appears limited to changes in the situational factors of an assault.
Disinhibition as a result of alcohol use is a situational risk factor as it may increase the risk of victimisation due to impaired danger assessment (Lutz-Zois, Phelps, & Reichle, 2011; Messman-Moore et al., 2009; Testa, Hoffman, & Livingston, 2010). There is a small amount of evidence that a history of victimisation (especially CSA) may negatively affect a woman’s capacity to assess situational risk (Fargo, 2009).
Due to its cognitive and physiological effects, alcohol intoxication by both men and women at the time of the incident is a major situational risk factor in dating IPSV, especially in women who already have a history of SXA (Chan, 2011; Filipas & Ullman, 2006; Littleton, 2014; Testa, VanZile-Tamsen, & Livingston, 2007). Australian and Norwegian qualitative evidence suggests that alcohol use is not a major aspect of IPSV in more established/cohabiting relationships (Clark & Quadara, 2010; Vatnar & Bjørkly, 2008). Research has found that men who perpetrate IPSV drink more than men who engaged in no violence, and women who experience rape in their relationships are more than twice as likely to have a substance use issue (Abbey, 2011; Gallagher, Hudepohl, & Parrott, 2010; Lacey, McPherson, Samuel, Powell Sears, & Head, 2013; White et al., 2008). These findings suggest that the overall patterns of substance use, rather than the nature of particular incidents, may put women at risk.
Women may also use alcohol to cope with their experiences of assault. A US study of 577 college women found that women who had experienced both CSA and the SXA as an adult were more likely to use this coping mechanism, although it is unclear what relationship this had to their re-victimisation experience (Filipas & Ullman, 2006).
Much less is known about the relationship between IPSV and illicit substance use, although there is evidence that women who have experienced IPSV or re-victimisation may increase their substance use as a way of helping them to cope with their trauma: such use may, or may not, cause problems for the woman in her day to day life. For example, in a study of 148 women, those who reported more than one IPSV incident were 3.5 times more likely to begin or increase their substance use than women who had experienced one incident only, suggesting a sub-population whose issues should be accommodated in treatment programs and harm minimisation drug and alcohol programs (McFarlane, Malecha, Gist, et al., 2005).
US research indicates that men who were convicted for IPSV were more likely than other sex offenders to use substances before they perpetrate a sex offence (Stalans, Hacker, & Talbot, 2010). This study was examining a population of convicted men, and thus has poor generalisability, with research on whether partner substance use is a risk factor for IPSV still considered equivocal (Hazen & Soriano, 2007).
Sexual behaviour
Certain sexual behaviours are associated with increased risk of re-victimisation and IPSV. Having more sexual partners, starting to have consensual sex at an earlier age, and/ or engaging in more sexual activity has been found to increase the likelihood of adolescent and adult IPSV and sexual re-victimisation (Kim-Godwin, Clements, McCuiston, & Fox, 2009; Macy, 2007; Stockman et al., 2013; Stockman et al., 2010; Young & Furman, 2008). Moreover, there is some evidence that sexual risk-taking mediates the relationship between CSA and adult SXA (Messman-Moore et al., 2009; Orcutt, Cooper, & Garcia, 2005). The implication of the latter findings are difficult to discern and unclear as they may simply indicate that individuals who engage in more sexual behaviours are being exposed to the same amount of risk than those who have less sex. At the same time, this more sexually active group are exposed more often, thus resulting in higher rates of victimisation.
Pregnancy
There is a dearth of research on the IPSV and re-victimisation experiences of pregnant women. The only study identified in this review to examine this population that was identified through the search method found pregnant women were approximately twice as likely to report bidirectional IPSV as IPSV victimisation only (Flanagan et al., 2014). This finding is inconsistent with more general DV and pregnancy research that identifies that pregnancy is a period of particular risk for escalation or initiation of intimate partner violence.
Relationship characteristics
The characteristics of an intimate relationship, such as the length of the relationship and the way that partners routinely communicate, have been shown to impact on the nature of violence within that relationship.
The expression of violence in a relationship is affected by the length of time a couple has been together. Casual sexual partners are likely to experience less endemic coercive sexual control, with men with casual sexual partners reporting the use of sexual coercion primarily in contexts of confusion and poor sexual negotiation skills (e.g. not being sure if their partner wants to have sex or not) (Eaton & Matamala, 2014; Rickert, Wiemann, Vaughan, & White, 2004; Wright, Norton, & Matusek, 2010). Over time, perpetrators of domestic violence tend to use more types of violence, which means that women who have been in abusive relationships of longer duration may be at more risk of co-occurrence of multiple types of violence (Thompson et al., 2006).
Research on whether being married[4] increases the risk of IPSV is mixed. In general, women who have ever been married are more likely to experience IPSV than women who have not been married (Arata & Lindman, 2002). When compared to married couples, research suggests that cohabiting couples are more likely to experience DV, although some studies show no statistically significant effect (Brownridge & Halli, 2001; DeKeseredy & Schwartz, 2008; Miller, 2006). Early marriage is associated with high rates of sexual coercion, possibly due to poor sexual consent negotiation skills (Hattery, 2009; Panuzio & Dilillo, 2010).
Leaving a relationship is a particularly risky time for IPSV, with women who have experienced IPSV frequently reporting incidents during the separation period. A small (n = 43) study of rural women in the US identified that three quarters (74%) were sexually assaulted when they indicated that they were planning to end the relationship (DeKeseredy & Schwartz, 2008). Such assaults may be possessive (an expression of control and ownership), reconciliatory (attempting to get back together through unwanted sex) or retaliatory (punishing a woman for leaving) (DeKeseredy, 2014).
Risk factor grouping
It is important to note that risk factors frequently accumulate in particular lives and communities. For instance, trauma- related responses, such as AOD use, withdrawing from social support and un-safe sexual behaviour, may occur at the same time and compound the effects of each other (Filipas & Ullman, 2006). Behavioural, personal and situational contexts may affect the risk of a person experiencing IPSV or re-victimisation.
Some researchers consider demographic characteristics to be another type of risk factor, with evidence that the risk of severe DV increases with certain demographic factors. In this report, this form of risk factor is addressed in a section on sub-population with differential patterns of victimisation. Some research, however, links more individualised risk factors with these socio-demographic factors, emphasising the complexity of lived experience of violence. For instance, in a study of 1402 randomly selected Spanish women, those who were on social security were 12.3 times more likely to experience emotional and sexual abuse (with or without physical abuse), than those who were not on welfare. Similarly, those who were divorced, separated or widowed were 8.7 times more likely to experience severe abuse than those who were married, and those who had three or more children were 5.4 times more likely to experience severe abuse than those who had no children (Ruiz-Pérez et al., 2006). Overall, the corpus demonstrates an ongoing intersection of disadvantage that complicates (and at time exacerbates) the lived experience of IPSV and re-victimisation.
Sub-populations with differential patterns of victimisation
There is limited research on the characteristics of any types of violence in most sub-populations (such as those in culturally and linguistically diverse communities, sexual minorities and other disadvantaged groups with proportionally small populations), with research on the specific forms of violence such as IPSV and re- victimisation particularly incomplete (Argento et al., 2014; Australian Bureau of Statistics, 2013a, 2013b; Heenan, 2004).
Findings are mixed regarding the extent, and indeed the existence, of a negative effect of minority status on IPSV and re-victimisation. A small number of studies have found equivalent prevalence rates of victimisation in minority groups and broader populations (McFarlane, Malecha, Gist, et al., 2005; Schewe et al., 2006). Most studies, however, find differences in the prevalence, nature and lived experience of violence by women in minority groups. Moreover, scholars note that culture (including the social norms of groups not normally thought of as “cultural”) affects both the meaning and experience of violence (Coker, Sanderson, Cantu, Huerta, & Fadden, 2008).
Research available on the prevalence and experiences of IPSV and re-victimisation in a range of sub-populations is outlined below. This section also acknowledges the behaviours and norms of these groups that may increase the risk of women experiencing IPSV or re-victimisation. The complexity of lived experience and the substantial overlap of populations means that a distinction between patterns of victimisation for IPSV and re-victimisation, or between these types of violence and VAW more generally, is somewhat artificial. While acknowledging this, in order to provide the most focused summary of available research, this section nonetheless focuses on sub-populations in relation to re-victimisation and IPSV as a way of constraining the scope of the review and noting patterns relevant to the specific topic of this paper. It is inevitable that this structuring of information will inadequately acknowledge the intersections of inequality and compounded disadvantage that may be experienced by some women whose lives are represented in multiple groups (Winters & Morgan, 2014).[5]
The sub-populations below have been highlighted in this review as they are communities where the broader social context affects the lived experience of IPSV and re-victimisation: specifically, where existing social disadvantage and distinct embodied life experience may compound and/or alter the prevalence and impact of re-victimisation and IPSV.
Aboriginal and Torres Strait Islander women
Aboriginal and Torres Strait Islander women are disproportionately affected by domestic, sexual and family violence, and family violence is considered an epidemic in these communities. Aboriginal and Torres Strait Islander women are 35 times more likely to be hospitalised as a result of family violence when compared to non-Aboriginal and Torres Strait Islander Australians (Cripps & McGlade, 2008; Productivity Commission, 2009). Violence in Indigenous communities occurs in a complex context of colonisation, dispossession and ongoing racism which makes Indigenous women particularly vulnerable to abuse (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010: Blagg, Bluett-Boyd, & Williams, 2015).
Although IPSV and CSA are acknowledged as a frequent aspect of family violence, primary research on the nature and extent of IPSV and re-victimisation in this population was not identified through this paper, potentially reflecting both the sparse amount of primary quantitative research in this area, and the relative focus of the search strategy on international sources (Adams & Hunter, 2007; Cripps, 2008; Northern Territory. Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse, 2007).
Interviews with Aboriginal women in New South Wales have identified the emotional impact of DV, and especially IPSV, as being similar to those found in the non-Aboriginal community (Heenan, 2004; Moore, 2002). As with the broader community, sexual violence perpetrated against Aboriginal women is often repeated (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010).
Indigenous women in rural or remote communities may be affected by a range of structural and service limitations, similar to those experienced by other women in these areas (Parkinson & Zara, 2014) (see Women who live in rural areas).
Women from cultural and linguistically diverse (CALD) backgrounds
There is significant variation in findings related to rates of domestic and sexual violence in migrant communities.[6] This variation is in part due to the challenge of creating methodologies that can accommodate the diversity of lived experience within and between different migrant communities (Mitchell, 2011; Tapia, 2014). There is very little research on the more narrow topics of IPSV or re-victimisation in migrant communities, with the full extent of the available literature on VAW out of scope for this review.
A range of practical and structural limitations affect the lived experience of violence by immigrants, including:
- Difficulties with English language that may affect help seeking or disclosure (Morash et al., 2007; Sabri, Barcelona de Mendoza, & Campbell, 2014).
- Limited financial independence (this may be due to a range of factors such as migration status, lack of recognition of previous qualification, low-paid employment or cultural or family reasons for not being in the workforce) that may reduce the capacity for women to leave their partners, (Morash et al., 2007).
- Cultural norms that may “emphasise a woman’s submissiveness, placing the needs of family before one’s own, and [where] stigma regarding divorce may present barriers to help-seeking” (Flicker et al., 2011, p. 1069; see also Sabri et al., 2014).
- Dependence on visas associated with their intimate relationship in order to stay in the country (Morash et al., 2007; Taylor & Putt, 2007).
Social disadvantage, including a “lack of support networks, socio-economic disadvantage, community pressure, and lack of knowledge about rights for victims” may increase the risk of SXA and DV, including IPSV (Allimant & Ostapiej- Piatkowski, 2011; Sabri et al., 2014). When women do report IPSV to police, they may have more difficulty than non- CALD women in obtaining protection orders or prosecuting their perpetrators, as a cultural defence may available to the perpetrator that enables them to indicate that they did not have criminal intent (Schafran, 2014). Moreover, some women may be ineligible for certain legal remedies due to their immigration status (Winters & Morgan, 2014).
Culturally specific gender norms may also affect the capacity for women to identify and/or disclose abuse, and may create contexts where traditional gender roles enable abuse (Liles et al., 2012; Morash et al., 2007; Parkinson & Reid, 2014; Rees & Pease, 2007; Sabri et al., 2014; Winters & Morgan, 2014).
There is mixed evidence regarding IPSV rates in immigrant communities, with some studies showing higher rates of IPSV in these populations, while others have found that lifetime sexual coercion rates were lower for women who were born overseas when compared to women of the same ethnic group who were born in the migration country (Cox, 2015; Hazen & Soriano, 2007; Möller et al., 2012).
Caution must be used when examining research regarding domestic and sexual violence in ethnic and migrant communities as conflation of violent behaviour with stereotypical accounts of particular communities may erase the complexity of lived experience and reinscribe racist (and in particular Islamophobic) discourses (Salter, 2014). Although there is some evidence that certain cultural identities may be associated with an increased risk of victimisation, this relationship may reflect broader patterns of disadvantage and risk such as population level differences in socio-economic status, education attainment, neighbourhood poverty or mental health status (Flicker et al., 2011; Palmetto, Davidson, Breitbart, & Rickert, 2013).
Women with disabilities[7]
The Australian peak body, Women with Disabilities Australia, notes that there is currently “inadequate recognition and response to the needs of those women and girls with disabilities who have experienced or are at risk of experiencing violence” (2013, p. 17).
Research on SXA, especially IPSV, experienced by women with physical disabilities is very limited (Plummer & Findley, 2012). In one of the few available studies, in comparison to women without disabilities, US women with severe physical disabilities were four times more likely to experience sexual assault (n= 6273) (Casteel, Martin, Smith, Gurka, & Kupper, 2008). A slightly larger (n= 7027) Canadian study of women with and without disabilities found that IPSV involving sexual assault was experienced by three times as many women with a disability (0.6% vs 0.2%) (Brownridge, 2006).
Women with physical disabilities are particularly vulnerable to assault by carers, with a US study of 84 women with physical disabilities finding that three percent had experienced sexual abuse by their primary personal assistant and eight percent had experienced abuse by another physical assistant (Oktay & Tompkins, 2004). Where women are dependent on a carer for assistance, including in key areas such as transportation or communication, accessing support or leaving a violent relationship may become particularly difficult (Davis, 2014; Plummer & Findley, 2012).
No studies were identified in this paper that examined the specific lived experience of IPSV or re-victimisation of women with intellectual disabilities. Research with professionals who work with people with an intellectual disability identify that this group is particularly vulnerable to sexual assault and assault within their domestic environment. Women with intellectual disabilities are also more likely to be part of other high-risk sub-populations such as women with low socio-economic status and women who experience severe mental illness (Barger et al., 2009; Hickson, Khemka, Golden & Chatzistyli, 2013). Women with intellectual disabilities are also “often socialised to be compliant […] and remain substantially more dependent on caregivers than nondisabled women” (Barger et al., 2009, p. 251).
As with some other sub-populations who experience multiple forms of disadvantage, Aboriginal and Torres Strait Islander women with disabilities find locating culturally appropriate and accessible services particularly difficult. As noted by a participant in Australian qualitative research on violence against Aboriginal women with disability: “people are just ignorant, and think that the disability [our] women have is being black and that their … disability isn’t even seen” (Cripps, Miller & Saxton-Barney, 2010). This quote highlights the challenges in making visible the experiences of women who are part of multiple highly disadvantaged sub-populations.
Research on IPSV for both women with disabilities and women with a mental illness is extremely limited, a pattern that may reflect societal norms that de-sexualise these two groups.
Young women
“…we began kissing, which I enjoyed but suddenly his hand was in my pants and I was extremely uncomfortable. He began fingering me and it was painful. [Afterwards] I was ashamed (we were in our school) and nervous someone would see us and think I was a slut.”
– Young woman aged 14 at the time
Adolescent women frequently experience dating sexual violence; over ten percent of young women having experienced forced sexual intercourse (Kim-Godwin et al., 2009). Within the adolescent cohort, rates of IPSV increase with age, with individuals who are over 18 more likely to experience IPSV (Kim-Godwin et al., 2009). This increase in victimisation is likely to reflect a larger proportion of women having become sexually active and the reduction in structural limitations to intimacy (e.g. having a licence, being permitted to be unsupervised in a bedroom etc.) (Noonan & Charles, 2009).
International research indicates that early adulthood (18-24 years) is a period of heightened risk of both rape and DV. In a US national representative sample (n = 9086), 37 percent of women who had been raped reported that their first incident occurred during this period. The same survey found that 47 percent of women who experienced DV reported that their first incident occurred at this age (Black et al., 2011). Some research also suggests that the early 30s are a period of heightened risk, particularly for IPSV perpetrated by cohabiting partners (Heenan, 2004). Research in Australia is more mixed, with findings from the 2012 PSS showing an increased risk of sexual assault for the 18-24 years age group, but the highest rate of partner violence occurring a little later (25-34 years) (Cox, 2015).
When examining women who have been assaulted more than once, a general population survey completed by female residents of Washington State found that those who were younger were more likely to have been assaulted by multiple perpetrators, while those who were older were more likely to experience violence by the same perpetrator (Casey & Nurius, 2005).
Women who are HIV positive
HIV and IPSV have been characterised as intersecting epidemics (Campbell et al., 2013; Stockman et al., 2013; Stockman et al., 2010; Tufts, Clements, & Wessell, 2010). Being forced to engage in behaviours that puts one at risk of HIV transmission is defined as a type of IPSV. In a meta- analysis of seven studies from the US that looked at IPSV and HIV risk behaviours (e.g. inconsistent condom use, having a HIV+ partner, having other STIs), six of the studies found a positive relationship between the two factors. Despite this, the paper identified no multivariate analysis that showed a statistically significant relationship between HIV infection/ risk behaviours and IPSV (Stockman et al., 2013).
For women with HIV or who have HIV+ partners, the impact of IPSV on their capacity to negotiate condom use may have significant health implications (Chamberlain & Levenson, 2012; Campbell et al., 2008; Macleod, 2014a).
As there are significantly fewer HIV+ women than men in Australia, HIV+ women may have difficulty finding health and support services that are sensitive to their needs (The Kirby Institute, 2015). Moreover, HIV+ women may face increased discrimination from service providers and the community in general due to the stigmatising context, or presumed context, of their seroconversion (e.g. injecting drug use or unsafe sex) (Lawless, Kippax & Crawford, 1996).
Women with low socio-economic status
Being unemployed and/or living in a low-income household are associated with higher rates of IPSV (Schumacher, Feldbau-Kohn, Slep, & Heyman, 2001; Vatnar & Bjørkly, 2008). In a prospective study of women who reported their violence to police, women who were unemployed were more likely than employed women to experience ongoing violence that included “physical aggression, sexual coercion or bodily injury” (Babcock & Deprince, 2013, p. 1396). In a random sample of Spanish women (n=1402), low income (OR 2.55) and poor social support (OR 12.28) were found to be associated with a combined intimate partner violence profile that included both emotional and sexual abuse (and may have involved physical abuse) (Ruiz-Pérez et al., 2006).
In a study that found a correlation between sexual or emotional abuse as a child and adult DV victimisation, low education attainment was the strongest predictive factor for adult DV victimisation (OR = 3.79, n= 637) (Seedat et al., 2005).
The financial and practical constraints of living in poverty, combined with the stigma and discrimination that may be experienced due to low socio-economic status, may reduce a woman’s capacity to seek support and/or leave a violent relationship (Cortis & Bullen, 2015).
Women who live in rural areas
“Where do you go? Your family doctor […] could be his best mate”
– Amanda
Rural communities have a number of characteristics that may increase women’s vulnerability to all forms of violence. These factors include:
- limited DV and/or SXA services;
- normalisation of violence; and
- the “tyranny of distance” that may increase the practical challenges of leaving a violent situation.
(DeKeseredy & Schwartz, 2008)
Some rural communities may be both close-knit and conservative, thus potentially perpetuating a culture that accepts IPSV (Parkinson & Zara, 2014). An interview study in the US (n=43) found that sexual assault in the context of relationship breakdown was routinely ignored for the “common good” of the community (DeKeseredy & Schwartz, 2008). More recent research indicates that IPSV in the context of separation is particularly common in these contexts (DeKeseredy, 2014; Rennison, DeKeseredy, & Dragiewicz, 2012). Moreover, there is some indication that the social isolation of gay and lesbian couples in socially conservative rural and remote contexts may negatively impact the capacity for IPSV survivors to access help and support (Ristock, 2014).
Rural communities may have higher rates of IPSV than urban communities: in Kentucky (n=213) 31 percent of women with protective orders reported being raped by their partner, that number rose to 36.8 percent when looking at women in rural areas (Logan, 2009). While research on rural communities is sparse, these initial studies suggest that women in these communities may be at higher risk of violence and may experience more negative impacts of that violence.
Women who are, or who have been, incarcerated
Women who have been incarcerated are a highly disadvantaged group who frequently have an extended history of contact with police. In the Australian context, Aboriginal and Torres Strait Islander women are disproportionately represented in prisons, and women prisoners have very high rates of drug dependence, mental illness and learning disability (Kilroy, 2014). For the US-based research described below, African America and Latina women are disproportionately represented. Researchers understand these racialised variations as reflective of the increased surveillance of particular populations, as well as interpreting them as a material impact of systemic racism (Baldry & Cunneen, 2014).
Incarcerated women have a higher rate of re-victimisation than poor urban women who have not been in prison, with statistical analysis also showing a stronger relationship between childhood and adult victimisation for incarcerated women (n=359) (Poister, Tusher & Cook, 2010).
A study of 50 NSW Aboriginal and Torres Strait Islander women prisoners found particularly high rates of CSA (over 75%) and adult SXA (approximately 50%) (Lawrie, 2003).
Women who have experienced CSA are twice as likely to be sexually victimised in prison when compared to women with no CSA history (Wolff, Blitz, Shi, Bachman, & Siegel, 2006; see also, Kilroy, 2014).
Even when they are out of prison, women who have been incarcerated have a higher rate of re-victimisation. Women who have been incarcerated (n = 484) and who had experienced IPSV were 3.1 times more likely to be assaulted by a friend and 2.4 times more likely to be sexually assaulted when they were a child (Raj et al., 2008). Unlike non-incarcerated women, incarcerated women report a greater proportion of adult sexual assaults by a stranger (12%) than by their partner (10%) (Raj et al., 2008).
Women who have been incarcerated face significant discrimination when they return to their communities. Difficulties in obtaining employment and accessing social services may impact on their ability to leave violent relationships, as well as their quality of life more generally (Decker, Spohn, Ortiz & Hedberg, 2014; Johnson, 2014).
Women who experience severe mental illness
Severe mental illness is associated with particularly high rates of CSA and SXA in adulthood (Meade et al., 2009; Shevlin et al., 2013).
Individuals who have histories of severe mental illness are particularly vulnerable to re-victimisation. This may be due to a range of factors including:
- the effects of psychosis, severe mental disturbance and the medications used to treat these states on perception of risk and danger;
- an inability to escape abuse when it happens in involuntary hospitalisation contexts; and
- reduced financial and social resources that in turn impact on the ability of women to escape violent relationships or contexts.
(Quadara, Stathopoulos, & Jenkinson, 2015)
Due to the lack of longitudinal research, there is limited understandings of the “direction” or exact nature of the link between mental illness and re-victimisation, however a bidirectional relationship where victimisation results in mental illness which in turn increases the risk of further victimisation is discussed in the clinical literature (Quadara, Stathopoulos, & Jenkinson, 2015).
A multivariate analysis of a representative sample of Australian women (n=4451) found that those that had experienced three or four types of gender-based violence (DV, stalking, sexual assault or rape) had a lifetime experience of clinically defined mental disorder that was 11 times greater than that of women who had no gender-based violence victimisation. Women with this high level of re-victimisation were also:
- ten times more likely to experience an anxiety disorder;
- sixteen times more likely to experience PTSD; and
- fifteen times more likely to attempt suicide. (Rees et al., 2011)
As this was a cross-sectional analysis, no inferences regarding the causal links between re-victimisation and mental health could be drawn.
There is substantial evidence that having a mental illness, and in particular psychotic illness, is a highly stigmatised identity (Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000; Watson, Corrigan, & Kosyluk, 2014). Women who are symptomatic may struggle to access services to assist them while simultaneously being in acute need of support. The long term effects of the social isolation that is often characteristic of severe mental illness may also result in women experiencing more severe impacts of violence.
(See also Risk factors for re-victimisation and co-occurrence, and Health impacts of re-victimisation and co-occurrence.)
Women who identify as lesbian, bisexual and/or queer
DV and IPSV in same-sex relationships may have different characteristics than DV in heterosexual relationships, in part due to the capacity for the threat of “outing” to be used as a tactic of coercive control (Freedner, Freed, Yang, & Austin, 2002; Potter, Fountain, & Stapleton, 2012). Research on DV in women’s same-sex relationships shows large variation in prevalence estimates, with available studies showing both significantly higher and significantly lower rates of victimisation than heterosexual women (Stoddard et al., 2009).
In an analysis of administrative data from GLBTIQ (gay, lesbian, bisexual, transgender, intersex and queer) anti- violence projects in the US, in comparison to other GLBTIQ intimate partner violence survivors, bisexual men and women were 1.6 times more likely to experience IPSV (from a male or female partner). The most common perpetrator of child or adult sexual assault of a lesbian is a man (Stoddard et al., 2009).
Women in same-sex relationships report significant concerns about experiencing prejudice and distress when seeking assistance related to DV (National Coalition of Anti-violence Programs, 2014). Lesbian women have less access to services than their heterosexual counterparts, potentially due to the limiting of some services to women who have children (of which, at a population level, lesbian women are less represented) and the provision of some services by religious groups that may not be, or may not be perceived to be, supportive of same-sex attracted women (Potter et al., 2012).
Large-scale and/or general population research on re-victimisation and IPSV rarely engages with women in same-sex relationships. This appears to be a methodological necessity, as even in a representative sample of 16,000 people, only 30 violent incidents involving same-sex partners were identified, thus making analysis statistically invalid (Messinger, 2011). Similarly, most of the ABS PSS data is unable to be reported for violence in same-sex relationships as the sample is too small to produce reliable estimates (Cox, 2015). In addition, and in keeping with gender norms which position women as incapable of rape, women may struggle to identify their experiences of same-sex IPSV as being a form of violence (Ristock, 2014).
Ongoing shifts in community attitudes towards people in same-sex relationships means that the levels of stigma and discrimination experienced by this sub-population may be reducing in relation to experiences by other sexual and gender minorities.
Transgender women and men
(Both transgender women and men are included in this paper as trans men may have experienced violence at a time when they presented as female and/or may have experienced gendered violence in a context where they were read by others as female.)
Transgender women and men experience high rates of violence in their lives, including SXA, DV and street based violence (Stotzer, 2009).
Transphobia has a significant impact on transgender survivors, with the lived experience of ongoing discrimination and prejudice and resultant distress likely to further compound the distress associated with victimisation. In a report on the experiences of IPV in the GLBTIQ communities in the US, the researchers noted that:
“In 2013 transgender survivors were more likely to experience physical violence and discrimination within IPV as well as police violence after incidents of intimate partner violence. Transphobia remains a formidable and dangerous reality for both the public and private lives of transgender individuals, creating barriers for access to essential services from anti-violence programs, law enforcement agencies, advocates, and medical professionals. Transphobia can also be a tactic of abuse that an abuser can use against a transgender partner. The barriers to accessing essential services for addressing violence in an intimate partner relationship have dangerous and sometimes deadly consequences for transgender survivors of IPV.” (National Coalition of Anti-violence Programs, 2014)
Trans individuals face a higher rate of IPSV than other groups in the GLBTIQ community, with 50 percent reporting having been raped by a partner (National Coalition of Anti-violence Programs, 2014).
Women who work in the sex industry
There is very little research regarding IPSV and re-victimisation of sex workers, however relationship patterns, including the potential to be in a relationship with an intimate partner who controls one’s work, may affect the patterns of victimisation in this population.
In a Canadian longitudinal study of 387 female sex workers with male partners, 26.2 percent had experienced physical and/or sexual abuse by their partner in the last 2 years. Of these women who had experienced abuse, 84.3 percent had experienced physical and/or sexual abuse as a child (Argento et al., 2014).
Sex workers have a higher risk of being sexually assaulted at work than other professionals. Much of this victimisation involves multiple criminal acts, including the combination of assault and theft (including not paying for a service). Street based sex workers are particularly vulnerable to this form of multiple victimisation (Jason, Hubbard, & Birch, 2013). Research in Queensland suggests that re-victimisation of sex workers is disproportionately distributed, with women in legal brothels least likely to be physically or sexually assaulted and women in street based sex work most likely to experience assault (Woodward, Fischer, Najman, & Dunne, 2004).
Women who experience sexual violence when engaging in sex work in criminalised jurisdictions have extremely limited access to the legal justice system because engagement with the police would require disclosure of illegal activity. Moreover, women who work in the sex industry may experience sustained discrimination from the community at large and service providers in particular, with stereotypes regarding the nature of sex work particularly destructive for women seeking help and support for work-based sexual assaults. As an example of the formalised discrimination against sex workers, the jail sentence given in relation to a victim of sexual assault who is identified as being a prostitute may be reduced as the judge is allowed to determine that the elements of “shame” and “defilement” may be “missing or diminished” (Clark, 2007, p. 21).
Debate on whether there is an association between prior victimisation and sex work victimisation remains unresolved in the literature and is an area of highly charged debate (Jason et al., 2013).
Sub-populations of interest with limited existing research
In the process of this review, a range of sub-populations were identified as likely to experience differential patterns of victimisation but for whom there was no or minimal dedicated research findings. Of particular interest were the following:
- Women who are homeless. Homelessness may create circumstances where women are particularly vulnerable to sexual violence, including contexts where they may feel obligated to have sex with a person who provides them with shelter (Christopher & Pflieger, 2007).
- Women who are polyamorous. Experiences of violence by women who have multiple partners are likely to be under-reported in the research literature as relationship structures (e.g. not cohabiting with all partners) may mean that certain relationships would be excluded from analysis.
- Women within the kink and BDSM communities. The dynamics and conceptualisations of IPSV in this community are likely to be distinct and may alter the lived experience and impact of re-victimisation and IPSV (for a brief discussion of this issue, see, McOrmond-Plummer, 2014; Ristock, 2014).
- Women who have intersex characteristics. There is no data available on this group within the GLBTIQ community.
Conclusion
A wide range of demographic factors have been shown to be associated with an increased risk of IPSV and re-victimisation. As with the risk factors described above, some of these factors may group together, with women who are identified in one sub-population category (e.g. having been incarcerated) more likely to be in others (e.g. having worked in the sex industry or used drugs and alcohol). The intersections between different demographic characteristics create distinct patterns of lived experience which need to be accounted for in public policy and service delivery.
Male repeat perpetrators of sexual assault and domestic violence: Repeat offenders
In this section:
- Most men who perpetrate sexual assault had not experienced CSA.
- Alcohol abuse problems, frequent and normalised engagement with pornography and a history of sexual coercion were associated with IPSV perpetration in a current relationship.
- Conservative gender norms were a contributing factor to perpetration.
Most of the research outlined in this paper has described the prevalence and victimisation patterns of IPSV and re-victimisation as they relate to women victims. This section describes research identified through the search strategy that examines male perpetrators who: engage in multiple types of perpetration; perpetrate violence against more than one woman; or perpetrate IPSV. While acknowledging that the perpetration of any man may contribute to a woman’s experience of re-victimisation, in order to keep within the scope of this review, this short examination of perpetrators is limited to repeat offenders.
The literature on perpetrators is distinct from that on victims as it has a different disciplinary focus, meaning the literature outlined below is a very partial picture of available research.
Recidivism refers to a return to perpetration after treatment and/or incarceration. Recidivists are a key sub-population of the broader group of people engaged in contexts of IPSV and re-victimisation, as these men may perpetrate multiple types of violence against a single woman and/or perpetrate violence against a range of women.
Much of the work on recidivism uses actuarial models to try to identify which men are more likely to re-offend. In an analysis used to develop an integrated theory of sexual recidivism, Jo Thakker (2012) notes several key risk factors for recidivism:
- general lack of sociality;
- sexual arousal associated with perpetration;
- attitudes and beliefs that are supportive of offending;
- difficulties with intimacy; and
- poor self-regulation.
In a meta-analysis of 20 longitudinal studies that examined risk and protective factors for perpetration of dating violence in adolescence, 53 risk factors were identified including the perpetrator’s mental health issues, aggressive thoughts, prior dating violence and the use of aggressive media (Vagi et al., 2012). Such research highlights the range of individualised risk factors that may influence repeated use of violence. Although such research indicates the existence of factors that increase the risk of perpetration it is important to emphasise that regardless of the contexts of their behaviour, perpetrators are responsible for their use of violence (McOrmond-Plummer, 2014).
Perpetrators of sexual assault may have been victims of abuse when they were children. In the limited number of cases where men then go on to perpetrate violence, the life-course of the perpetrator shows an alternative type of re-victimisation that crosses the victim-perpetrator division. Child sexual abuse has been associated with both adolescent sexual perpetration and adult sexual assault perpetration, however the extent of the relationship is still being examined (Reckwald, Mancini & Beauregard, 2013; Mathes, 2013). Although adolescent sexual perpetrators are more likely than other young men to have experienced CSA, the relationship is insufficient to be called a “risk factor” (and may be better described as a “risk marker”) (Mallie, Viljoen, Mordell, Spice, & Roesch, 2011, p. 412). Most CSA survivors do not perpetrate sexual assault, with more than 90 percent of adolescent sexual offenders not having experienced CSA (Nisbet, Wilson & Smallbone, 2004).
With regards to perpetrators of IPSV, there is little distinction in the backgrounds of men who are physically or sexually aggressive in their intimate relationships, with men who perpetrate both forms of violence frequently from family environments that were chaotic (White et al., 2008). In addition, a range of behaviours may co-occur and enable IPSV:
- Alcohol abuse problems are more common in men who sexually and physically abuse their female partners than in men who do not (White et al., 2008).
- Frequent and normalised engagement with pornography may provide a context of perceived constant sexual access (Clark & Quadara, 2010).
- Sexual coercion in a previous relationship is predictive of the same type of coercion in a current relationship (Brousseau et al., 2012; Vatnar & Bjorkly, 2008).
A perpetrator’s beliefs also affect their perpetration, with conservative gender norms being a contributing factor identified in a range of studies. For example, a study of 59 urban fathers showed that hypermasculinity was associated with IPSV and other forms of DV and child maltreatment (Guerrero, 2009), with hostility towards women also predictive of sexual recidivism (Stanlans et al., 2010).
Repeat perpetration is a complex area of research that is not able to be fully described in this paper.
Community and professional attitudes towards re-victimisation and co-occurrence
Key findings in this section:
- Normative understandings of “real rape” affect how people interpret narratives of sexual assault. They particularly affect interpretations of IPSV incidents.
- Heteronormative beliefs are associated with acceptance and experience of verbal sexual coercion for both men and women.
- Understandings of consent in established relationships affect how instances of IPSV were framed by victims and third parties.
“I remember my husband making me have sex with him one time when people were in the next room and none of them guys would come in and help me. And they knew he was hitting me, but they figured that he was my husband. If it were a stranger it would have been different”
– Grace, Rural Ohio
Attitudes, understandings and cultural framing affects an individual’s experience and conception of sexual assault and domestic violence (Addington & Rennison, 2008; Murphy, 2011). Social norms regarding sexuality, and sex within relationships in particular, may increase the negative impact of IPSV and/or re-victimisation on the wellbeing of the women who experience these forms of violence, with lack of community understanding being characterised as “one of the most injurious aspects of IPSV” (McOrmond-Plummer, 2014, p. 33).
Social paradigms affect what behaviours are understood as rape, including normative understandings of what constitutes “real rape” (i.e. the belief that a rape is more “real” if it is a physically violent assault by a stranger) (Addington & Rennison, 2008; Davis, 2014; Easteal, 2014; Kerr, 2014; Logan et al., 2013; McLean & Goodman-Delahunty, 2008; Raphael & Logan, 2009). “Real rapes” are also meant to create “real victims” – women who “scream during their rape […] forcibly resist their attackers […] report their rapes immediately […] remain vigilant following their attacks and […] avoid their assailants” (Long, 2009, p. 23). Many IPSV and re-victimisation survivors do not fit these stereotypes. Research has found that IPSV was consistently viewed by the community as both less serious and more justifiable than SXA committed by a stranger and acquaintance (Christopher & Pflieger, 2007).
For a range of populations, including victims and police officers, the likelihood that an incident of IPSV is considered a lie, or a “miscommunication” rather than an assault, increases with greater familiarity between the victim and the perpetrator (McLean & Goodman-Delahunty, 2008; Orchowski et al., 2013). In a study of 173 women who had experienced intimate partner violence, reactions of friends and family to disclosures of IPSV were generally negative, although this relationship was not as strong when there was evidence of positive coping strategies (Sullivan, Schroeder, Dudley, & Dixon, 2010).
Beliefs about sexuality and relationship norms also affect the risk of (re)victimisation (Niehaus, Jackson, & Davies, 2010). For both men and women, support of heteronormative beliefs is associated with acceptance and experience of being verbally pressured to have sex (Eaton & Matamala, 2014). Moreover, understandings of consent are complicated by a range of gendered and relational norms which may alter a person’s understanding or lived experience of IPSV (Martin et al., 2007; Spohn & Tellis, 2012; Wall, 2012). In both lived experience and court contexts, distinguishing between “wifely acquiescence” and rape can be difficult “precisely because coercion, pressure, aggression and ‘seduction’ remain culturally acceptable expressions of male [sexuality]” (Heenan, 2004, p. 9). Social scripts of heterosexuality normalise IPSV as part of accepted masculinity or as a standard characteristic of seduction, with these scripts apparent in the attitudes and behaviours of a range of populations including Australian young people (Flood & Kendrick, 2012; Noonan & Charles, 2009). Younger women rarely identify sexually coercive behaviours by boyfriends as sexual assault, and justify this violence through explanations that indicate that their own behaviour justified the assault or which emphasise some kind of extenuating circumstances (Christopher & Pflieger, 2007; Lloyd & Emery, 1999). Moreover, in instances where study participants looked at a hypothetical IPSV rape scenario, even participants who identified the event as rape tended not to believe that the “act was a violation of the wife’s rights” (Ferro, Cermele & Saltzman, 2008, p. 773).
Although legal understandings of consent in established relationships have altered significantly in the last 30 years, they remain imperfect and reflective of broader social understandings of the nature of sexual assault (Easteal, 2014). Until the 1980s, the concept of marital rape was not legally valid in Australia (Feerick & Easteal, 2005; Larcombe & Heath, 2012). Modern legal definitions of consent centre on establishing that the perpetrator was aware that the victim did not consent or that the perpetrator had wilful disregard for her consent (Feerick & Easteal, 2005). Despite this progress, the relationship between offender and victim remains a legitimate cause for reducing the jail sentence for sexual assault (Clark, 2007, p. 20). IPSV offences are difficult to prosecute, in large part because they typically happen in the context of consensual sexual relations before and after the assault, as well as patterns of sexual activity that are established and do not include verbalised consent (Easteal, 2014; Heenan, 2004; Logan et al., 2013; Martin et al., 2007). There is an ongoing need for feminist legal scholars to assert that women consent to specific acts of sex and not to sex in general with a particular person (or a particular class of person) – this advocacy is central to positioning IPSV as a criminal act that cannot be justified by the context of the assault (Ellison, 2010; McGlynn, 2010).
Attitudes towards violence construct the lived experience of violence, constraining a woman’s own emotional response to violence, her understanding of appropriate gendered behaviour and her ability to access legal responses.
Health impacts of re-victimisation and co-occurrence
Key findings in this section:
- The mental health impacts of re-victimisation and IPSV range from clinically significant symptoms (such as self-blame and shame) to severe mental illness (such as psychosis).
- The physical health impacts of re-victimisation and IPSV often continue after the abuse has stopped and include a range of injury and stress related conditions. Sexual health was particularly negatively impacted by IPSV.
The effect of violence varies between individuals, with women who have the same types of violence experiencing differing levels of ongoing impact and trauma. In addition, the characteristics of the violence, including its “severity, frequency, meaning and intention”, affect its impact on the victim (Hegarty & Roberts, 1998, p. 53). Like risk factors such as alcohol use and self-harm, many health impacts may be understood as being responses and manifestations of trauma (Kerr, 2014).
Below, we outline findings on the mental and physical health impacts of re-victimisation and IPSV.
In research which distinguishes between IPSV and other forms of physical violence, it has been found that IPSV, both by itself and in contexts where separate instances of non-sexual physical violence occur, has a greater burden of disease than physical DV only (Bonomi, Anderson, Rivara, & Thompson, 2007; Monson & Langhinrichsen-Rohling, 1999). These findings are based in medical, epidemiological and public health research which, while concerned with patterns of health and illness, does not readily engage with the broader social context of violence. Despite wanting to acknowledge the social dimensions of the effects of violence, in order to keep aligned with the methodology and epistemology of the studies examined, this section is aligned with a medicalised approach to the impacts of violence.
Mental health impacts
Clinically significant symptoms
Common clinically significant emotional difficulties and distress are a normal and expected response to trauma (Kerr, 2014; Palmer & Parekh, 2014). The following experiences are common in both IPSV and re-victimised populations:
- self-blame;
- guilt;
- low self-esteem; and
- shame.
(Johnson, 2005; Kelly & Stermac, 2012)
The cultural and personal meanings associated with IPSV result in women reporting intense feelings of shame – women who experience IPSV report more shame when compared to women who experience stranger rape; IPSV victims also experience more shame compared to women who experience DV that involves physical assault only (Messing et al., 2014; Palmer & Parekh, 2014; Temple, Weston, Rodriguez, & Marshall, 2007; Wall, 2012).
Shame may also impact on re-victimisation rates, with women who experience CSA more likely to be sexually re- victimised as adults if they experience more self-blame about their original abuse (OR = 1.7) (Tapia, 2014).
In comparison to women who experience non-sexual physical DV only, women who experience IPSV are more likely to experience clinically significant distress (n = 449) (Spiller et al., 2012). Moreover, children of women who experience IPSV are more likely to display disruptive behaviours than children whose mother has experienced physical abuse only (Kitzmann, Gaylord, Holt, & Kenny, 2003; Spiller et al., 2012).
The impact of clinically significant distress may be mitigated by appropriate health care responses. For instance, professionals engaging in victim-blaming may increase distress, as described by an interviewee in a UK qualitative study:
“I was also told by a psychiatrist that I should have fought harder, yelled louder, etc. Because I was blamed by two doctors who are suppose [sic] to help me – I began to blame myself and question maybe they are right. I still have difficulty overcoming this blame.”
Affective disorders
Consistent with other forms of VAW, the mental health effects of IPSV and re-victimisation are significant and may extend significantly beyond the period of trauma. These effects most commonly include:
- Depression.
- Anxiety.
- PTSD.
(Basile, Arias, Desai, & Thompson, 2004; Krebs et al., 2011; Ludermir et al., 2008)
In a Brazilian study, women who experienced IPSV were 3.88 times more likely to experience clinically diagnosable mental disorders (including, but not limited to, depression and anxiety) than women who had no DV victimisation. For women who experienced physical, sexual and emotional abuse, the odds ratio was 6.39 (Ludermir et al., 2008).
In comparison to women who were physically but not sexually abused by their partner, women who had experienced IPSV were more likely to experience depression, with one study showing a 61 percent increase in severe depression symptomology (Bonomi et al., 2007; Pico-Alfonso et al., 2006). Similarly, regression analysis of data from women who had experienced IPSV (n=57) showed that a history of childhood physical or sexual abuse and severity of IPSV independently contributed to depression, with these findings also mirrored in other studies (Koopman et al., 2007; Miller, 2006).
Women who had experienced IPSV reported a rate of suicide attempt and threat that was 5.3 times higher than women who had experienced solely physical abuse by an intimate partner (n=148) (McFarlane, Malecha, Gist, et al., 2005).
Re-victimisation compounds the psychological effect of previous trauma, with lifetime and current PTSD and depression more severe in this population (Casey & Nurius, 2005; Messman-Moore et al., 2010).
The experience of sexual assault by an intimate partner appears to be particularly traumatic, with women reporting more PTSD symptoms if they experience IPSV than if they experience non-sexual physical assault only (McFarlane, Malecha, Watson, et al., 2005; Messing et al., 2014). Women who experience IPSV in the form of sexual coercion report trauma symptomologies similar to adult rape survivors (Broach & Petretic, 2006). Even in cases where there was high severity of other forms of intimate partner violence, the presence of IPSV increased the severity, and was predictive of, PTSD symptoms, (Bennice, Resick, Mechanic, & Astin, 2003; Dutton, Kaltman, Goodman, Weinfurt, & Vankos, 2005; Sullivan et al., 2012).
Psychosis
A class analysis of victimisation patterns and psychosis found that women who experienced multiple victimisations across the life course were 6.43 times more likely to experience paranoia and 12.36 times more likely to experience auditory hallucinations than women with no abuse history (Shevlin et al., 2013). In addition, CSA victimisation, which is a common aspect of a re-victimisation life-course, is predictive of psychosis (Bebbington et al., 2011; Shevlin et al., 2013).
Given the significant mental health problems experienced by women who are exposed to IPSV, it is noteworthy that some research has found that, of women who were in abusive relationships, access to mental health services was less common or at best at equivalent levels, for IPSV survivors (Próspero & Vohra-Gupta, 2008).
(See also Sub-populations with differential patterns of victimisation.)
Both re-victimisation and IPSV are associated with many mental health conditions, including clinically significant distress, affective disorders and psychosis.
Physical health
General health
The physical health effects of IPSV and re-victimisation are significant, with long-term physical health consequences often continuing after the abuse has stopped (Andersen et al., 2014; Bonomi et al., 2007; Parekh & Williams, 2014).
Physical health conditions that have been shown to be associated with IPSV and/or re-victimisation include:
- urinary tract conditions;
- gastrointestinal disorders;
- headache;
- seizures;
- hypertension; and
- asthma.
(Campbell et al., 2002; Chiu et al., 2013; Sullivan et al., 2012)
Both IPSV and re-victimisation have complex impacts on the sympathetic and para-sympathetic nervous system (Patriquin, Wilson, Kelleher, & Scarpa, 2012). More specifically, there is some evidence that sexual re-victimisation affects cortisol levels and may in turn reduce the reactivity of the parasympathetic and sympathetic nervous systems (Friedman, Jalowiec, McHugo, Wang, & McDonagh, 2007; Miller, Chen, & Zhou, 2007).
Sexual health
In comparison to the research on general health effects, there is substantially more evidence of the negative sexual health consequences of IPSV. There is also an emerging body of evidence regarding the effects of re-victimisation on sexual health.
In an interview study of women who had experienced IPSV (n = 148), 20 percent identified that they had experienced a rape related pregnancy and 15 percent had attributed at least one sexual transmissible infection (STI) to IPSV. Of those women who experienced IPSV more than once, 1 in 5 (20%) had experienced bleeding from the vagina, with the same percentage experiencing bleeding from the rectum (McFarlane, Malecha, Watson, et al., 2005).
In a multinominal analysis of data from 432 women who had called the police due to an intimate partner assault, women who had experienced forced sex were 3.4 times as likely to experience miscarriage when compared to women who had not experienced IPSV. Within this sample, women who experienced forced sex were also 1.3 times more likely to experience PTSD (Messing et al., 2014).
Women who experience IPSV may have more difficulty negotiating condom use, with a study of women who use drugs finding that those who experienced IPSV were 3.3 times more likely to use condoms inconsistently (Palmer & Parekh, 2014; Panchanadeswaran et al., 2010). IPSV in dating relationships may increase the risk of STI transmission and pregnancy through increases in unprotected sex in non-fluid bonded relationships (Herman, 2009).
Sexual coercion appears to mediate the relationship between intimate partner violence and HIV transmission, however while bivariate analysis has shown a relationship between IPSV and HIV infection, no multivariate analysis has demonstrated this relationship (Stockman et al., 2013).
Women who have experienced IPSV were 2.7 times more likely to develop cervical cancer than women who had never experienced gendered violence, possibly due to increased transmission of the human papilloma virus (n = 4732) (Coker, Hopenhayn, DeSimone, Bush, & Crofford, 2009).
Re-victimisation also increases the risk of negative sexual health outcomes. In a study of 209 women who had experienced abuse only after the age of 12 years, those who had experienced no trauma, multiple single traumatic events and an ongoing and sustained experience of physical/sexual abuse had rate of ever having had an STI of two percent, nine percent and 44 percent respectively. The same groups had a rate of pregnancy of two percent, 15 percent and 33 percent, the vast majority of which were terminated (Green, Krupnick, Stockton, Goodman, & et al., 2005).
IPSV and re-victimisation may have a significant and long term negative effect on a woman’s well-being. Negative health outcomes are particularly apparent in the area of sexual health, with some evidence of higher rates of a range of gynaecological issues, including miscarriage, STI infection and cervical cancer.
Women’s engagement with legal and support services
Key findings in this section:
- Rates of reporting and engagement with the legal system for IPSV and re-victimisation were affected by the social context of the abuse, as well as difficulties with the legal system itself.
- IPSV victims were less likely to seek help than victims of other forms of DV.
Women who experience IPSV or re-victimisation may seek support from a both informal and formal sources. Accessing support, as well as engaging with the criminal justice system, can be important in maintaining a woman’s physical and emotional safety.
The corpus provided very limited research on help-seeking in relation to “cross-type” re-victimisation. As such, the following discussion is largely limited to IPSV.
Disclosure
“While I was ashamed of being battered [by my husband] – certainly in terms of the blame it accrued from others – the shame of being raped was more deeply excoriating; I did not think I would ever tell anybody”
Louise McOrmond-Plummer
The reactions of friends and family to disclosures of IPSV affect the lived experience of the violence.
In general, IPSV is associated with more negative social reaction than other forms of DV (Sullivan et al., 2010). A woman’s decision to disclose IPSV may be affected by her previous victimisation and responses to it, however research is mixed regarding whether a history of sexual assault increases or decreases the likelihood of future disclosure (Chiara Sabina & Ho, 2014; Simmel et al., 2012). In addition, willingness to disclose, as well as responses after disclosure are affected by a range of broader factors including the criminalisation of certain behaviours and stigma/discrimination based on race, sexuality, trans experience, occupation, HIV status and drug use.
The ANROWS additional analysis of the 2012 ABS PSS data found that “18.7% (46,800) of women sexually assaulted by their cohabiting partner have not told anyone about their most recent incident” (Cox, 2015).
Help-seeking: Non-legal services
Women who experience IPSV are less likely to seek help and/or support than women who experienced other forms of DV but not IPSV. In an additional analysis of the US Violence Against Women Survey data, women who experienced IPSV “sought help from significantly fewer sources” compared to women who experienced other forms of DV (Flicker et al., 2011, p. 1074). In several studies, once a woman had experienced more than one assault, the number of abusive acts was not related to help-seeking. This suggests that it is the types of abuse, rather than the amount of abuse, that determines help-seeking (Casey & Nurius, 2005; Flicker et al., 2011).
Additional analysis of the 2012 PSS data found that, of women who reported their most recent incident of sexual assault by a male was perpetrated by a cohabiting partner:
- 34.1% (85,300) sought support and advice from a friend/family member/work colleague/person providing pastoral care;
- 29.2% (73,200) sought support and advice from a counsellor/support worker/telephone hotline; and
- 25.5% (63,200) sought support and advice from GP/ health professional. (Cox, 2015)
Help-seeking may also be affected by the type of violence that a woman experiences. For instance, in a study of undergraduate college students (n = 200), participants who had experienced DV were less likely to access mental health services if they had experienced IPSV (Próspero & Vohra-Gupta, 2008). Disclosure may also be affected by a woman’s victimisation history. A victimisation history of repeated SXA in adolescence increased the likelihood of disclosure in college women by up to six times (n = 374) (Orchowski & Gidycz, 2012).
Help-seeking is also affected by existing and systemic disadvantage, including the material, practical and psychological impacts of discrimination associated with identity, ethnicity, health status or stigmatised behaviours. Women from marginalised communities may struggle to find services that align with their own interpretation of their lived experience, or may choose not to access services due to these fears. Some women, for example women with disabilities or women from CALD backgrounds, may require additional assistance to access support.
Overall, a woman’s capacity to access services is affected by a range of “individual, inter-personal and socio-cultural” factors that mould the way the woman recognises and conceptualises violence, her decision to seek help and the supports that she selects to use (Sabina & Ho, 2014, p. 202; see also, Kennedy et al., 2012; Liang, Goodman, Tummala- Narra, & Weintraub, 2005).
(See also Sub-populations with differential patterns of victimisation.)
Help-seeking: Legal system
“[It’s basically] domestics with a bit of sex thrown in”
Police officer, NSW.
Women tend to only report severe IPSV to police. Rates of reporting to police vary according to population and the form of sexual violence, with several studies finding a zero percent reporting rate for sexual coercion (Sabina & Ho, 2014). This is unsurprising given the high rates of women who do not perceive sexual coercion as an assault.
A woman’s decision to formally disclose their assault is affected by a range of factors including the relationship with the perpetrator, the severity of the victimisation, history of engagement with the police, and the location of the incident (Parekh & Williams, 2014; Thompson, Sitterle, Clay, & Kingree, 2007). Moreover, a woman’s capacity to report their experience of violence to police is affected by the context in which that violence occurs – for women who engage in criminalised activity (e.g. sex work in places where it is illegal, illicit drug use) reporting assaults to police may be practically impossible due to necessity to disclose criminalised activities. Socially stigmatised identities or behaviours may negatively impact a woman’s “believability” and presumed “moral character”, both of which have been shown to affect charging decisions (Spohn & Tellis, 2012, p. 177).
Most research indicates that women are less likely to report IPSV than non-sexual physical assault by an intimate partner to the police (Easteal, 2014; Mouzos & Makkai, 2004). Women who experienced IPSV were half as likely to seek help from police (OR = 0.48) or family (OR = 0.51) when compared to women who did not experience sexual victimisation but did experience other forms of DV (Flicker et al., 2011).
However, a minority of studies suggest that IPSV may result in higher police reporting rates. For instance, in a US study of abused women, 19.9 percent called the police in relation to a severe sexual coercion event (in contrast, 12.7% experienced a severe sexual coercion event but did not call the police in the last year). In comparison to other callers, women who were severely sexually assaulted were one and a half times more likely to call the police (OR = 1.58) (Bonomi et al., 2006).
Police reporting of IPSV is also lower than reporting sexual assault perpetrated by people other than an intimate partner (Fisher, Daigle, Cullen, & Turner, 2003; Möller et al., 2012).
In comparison to women raped by their partners:
- women who were raped by an acquaintance were 2.3 times more likely to report the incident to police; and
- women raped by a stranger were 5.2 times more likely to report. (Addington & Rennison, 2008)
In a psychological test which used a scenario exercise to assess a police officer’s attitudes about sexual assault, Australian police officers were more likely to consider a victim to be credible and to believe that she had been sexually assaulted if the scenario involved her being assaulted by an ex-boyfriend than by her husband (McLean & Goodman-Delahunty, 2008). The normative attitudes of practitioners throughout the legal system are important as they define and determine the results of criminal prosecutions. As Sack notes:
[most] practitioners are both sincere and well-meaning […] I believe that the fundamental explanation for the resistance to full implementation of [legal changes that acknowledge marital rape] rests in historical justifications for the toleration of domestic violence which we thought we had jettisoned long ago. Yet the legacy of these justifications continue to shape our beliefs about violence against women. Do we really believe that domestic violence is a crime?
In the context of community attitudes, IPSV is frequently difficult to prosecute (McGlynn, 2010). A study that examined agreement between police and prosecutors in Philadelphia rape cases found that prosecutors were more likely to agree to proceed with a case of stranger rape than IPSV (Holleran, Beichner, & Spohn, 2010). Additional analysis of the US National Survey of Violence Against Women showed that, while 29.7 percent of reported cases of sexual assault were perpetrated by an intimate partner, only 19 percent of convicted cases were for IPSV (Felson & Pare, 2007). A study comparing data from two large national crime victimisation studies found that case clearance was strongly predicted by the reporting of a co-occurring crime (Addington & Rennison, 2008).
The Aboriginal Family Violence and Legal Service Victoria notes that under-reporting of IPSV is a significant issue within Aboriginal and Torres Strait Islander communities (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010). Anecdotal evidence indicates that Aboriginal and Torres Strait Islander women often do not report assaults to police. Despite this, Aboriginal women are disproportionately represented as complainants in sexual assault cases, suggesting that the rate of assault is even more disproportionate than is currently reflected in available data (Keel, 2004). In addition, there is some evidence that Aboriginal women experience low rates of police response when they request assistance with multiple incidents (Aboriginal Family Violence Prevention and Legal Service Victoria, 2010).
The available evidence suggests that the social context of IPSV and re-victimisation, as well as difficulties with the legal system itself, reduces the rates of reporting and engagement with the legal system for these types of violence. As Sack quips in her discussion of judicial responses to IPSV “[w] here intimate partner rape is concerned, the bad old days are surely still with us” (2010, p. 548).
Responses to women affected by re-victimisation and co-occurrence
Key findings in this section:
- DV and SXA services are often separated, with both service types finding victims of IPSV a particularly challenging client group.
- Joined-up services have substantial government support, however they sometimes have unexpected negative consequences such as the reduced provision of services to SXA victims.
- Health professionals are often a gateway to specialist violence services, however they generally have not received specialist training in the area.
- Evidence remains mixed regarding the efficacy of behaviour change perpetrator programs with very few programs addressing IPSV.
- Prevention programs, such as awareness campaigns and bystander programs, are typically implemented in university settings and often have a focus on IPSV in dating relationships.
- Education of professionals in the area of primary prevention is important, as is engaging young people in ongoing dialogues about the nature of sexual consent.
“We, in our own education, say that violence does not exist in isolation… why are we then providing a service to women in isolation?”
– Senior level management staff.
Service responses to women affected by re-victimisation and co-occurrence may be based in a range of orientations including feminist and empowerment approaches and social work methodologies (Conway et al., 2010). Within many of these, there is a political and practical commitment to enabling women to address their full history of abuse and for recovery to be defined as a sense of well-being rather than merely a lack of trauma-related pathology (Fotheringham & Tomlinson, 2009; Ranjbar & Speer, 2013). Evidence suggests that a large proportion of DV and SXA services users have a history of IPSV and/or re-victimisation, with a study of psychological and advocacy service users finding that about three quarters of their clients had experienced abuse as a child (Follette, Polusny, Bechtle & Naugle, 1996). In addition, a study of women in DV refuges found that eight out of ten women had experienced IPSV (Moreau et al., 2015).
There is limited evidence of the effectiveness of service responses to IPSV and re-victimisation (Macy, Johns, Rizo, Martin, & Giattina, 2011). Given the lack of directly relevant research, but in keeping with the focus of this study on the intersection between SXA and DV, this section is largely focused on service provision that addresses both DV and SXA. The minimal amount of content specific to IPSV and re-victimisation likely reflects the lack of services that address these forms of victimisation specifically – this implied service gap is problematic as the use of more generic support strategies may leave the needs of these survivors “unidentified and unaddressed” and may result in a narrowing of “the opportunities to develop safety and healing” (Winters, 2009, p.7; see also, McOrmond-Plummer, Easteal & Levy- Peck, 2014).
Australian domestic violence and sexual assault support services are often provided by distinct sets of professional organisations. The siloing of services may be understood as partially a consequence of the conceptual and practice histories of the DV and SXA sectors (Ristock, 2014; Wilcox, 2010). As Kerr notes, “[e]ven for those of us who work in the field, domestic abuse is sometimes seen as something separate from rape or sexual assault” (Kerr, 2014, p.90). This separation is common to a number of countries, including the US, and poses significant challenges in addressing the needs of women who have experienced both SXA and DV (Herz, Stroshine, & Houser, 2005; Macy, Giattina, Sangster, Crosby, & Montijo, 2009; McOrmond-Plummer, Easteal & Levy-Peck, 2014; Wilcox, 2010; Williamson, 2014).
In a study of service executives’ understandings of the characteristics of DV and SXA services, similar provisions, such as counselling, 24-hour crisis lines, support groups, children’s services and legal advocacy, were deemed important for users of both DV and SXA services. Medical and ER advocacy was largely considered useful for SXA survivors, while shelter services were understood as more important to survivors of domestic violence (Macy, Giattina, Montijo, & Ermentrout, 2010). Put differently, service providers tended to understand DV services as providing whole-of-life support while SXA services were seen as more likely to provide context-specific support (Fotheringham & Tomlinson, 2009).
A literature review on violence against women services found that the literature recommended that DV and SXA services have several similar characteristics. These included:
- a telephone hotline;
- legal advocacy;
- support groups; and
- individual counselling. (Macy et al., 2009)
Both types of service have an ultimate focus on ensuring women’s safety (Herz et al., 2005).
Despite the similarity in the ultimate goal of these services, it is important to note that the emotional needs of service users may vary with the type of violence experienced (Macy et al., 2011). Zweig and Burt (2007) observed that while a sense of control was important for women in domestic violence services, it did not predict how helpful women found sexual assault services (n = 1509).
Service executives acknowledged that the provision of combined services that were appropriate for both DV and SXA survivors was difficult (Macy et al., 2010). Individuals who have experienced IPSV were considered particularly challenging, with limited best practice guidance available (Macy et al., 2010). Despite this, the combining of services has been shown to be particularly valuable in improving the services to women who have experienced sexual violence, although its overall benefit to all types of survivor is less well established (Zweig & Burt, 2004).
The available literature regarding combined DV and SXA service provision is inconclusive. Some researchers emphasised that the experience of SXA and DV were different and thus require specialist services, while others argued that it was essential for DV and SXA services to collaborate (Fotheringham & Tomlinson, 2009; Macy et al., 2009). Some service representatives have raised concerns about the impact of combined SXA and DV service provision, which may negatively impact their funding arrangements and may result in SXA being subsumed under DV services (Fotheringham & Tomlinson, 2009). Many service and policy representatives consider that combined services dedicate inadequate attention and resources to sexual assault (Macy, Giattina, Parish, & Crosby, 2010).
For many DV service staff, IPSV is considered outside their area of expertise (Heenan, 2004; Macy et al., 2009; McOrmond-Plummer et al., 2014). Both DV and SXA workers may consider IPSV to more “properly” fit within the remit of workers in the other field, with US researchers noting a systemic lack of attention to IPSV found in both DV and SXA services (Bennice & Resick, 2003; Heenan, 2004; Levy-Peck, 2014b).
Both DV and SXA services acknowledge limited funding or capacity for services to marginalised women (Macy et al., 2010). In the Australian context, the compartmentalisation of services is of particular concern when addressing the needs of Aboriginal and Torres Strait Islander peoples, as the intricate histories of trauma in these communities mean that there is increased complexity in the service landscape (Cripps & McGlade, 2008). In addition, the needs of women who have experienced re-victimisation and/or IPSV and are unable to access mainstream violence services (e.g. women with severe communication or cognitive limitations), may be particularly poorly addressed in services which do not specialise in supporting women who have experienced violence (Barger et al., 2009).
Coordinated, multi-agency and integrated services responses
There is a growing consensus that women’s safety is best served when multiple bureaucratic and practical systems work together to provide the woman with the support services that she needs (Breckenridge, Rees, valentine, & Murray, 2015; Cattaneo & Goodman, 2005). Providing such services can be difficult for women who have experienced IPSV or re- victimisation, with service directors noting that providing services to women who have experienced both DV and SXA is a key challenge (Macy et al., 2010).
A range of coordinated approaches are available, including, but not limited to:
- whole of government policy coordination;
- recidivism risk assessments;
- safety planning;
- co-education across sectors;
- specialist workers to assist women to access services across sectors;
- multi-agency services; and
- “no wrong door” approaches.
(Breckenridge et al., 2015; Cooper et al., 2008; Macleod, 2014b; Salter, 2012)
Coordinated responses may also include access to services such as mental health or AOD programs that help to address issues that may occur at the same time or as a consequence of IPSV or re-victimisation (Macy et al., 2010). Another way of understanding potential coordinated responses is to imagine them as a continuum of coordination, from autonomous services with networking, through collaborative practice, streamlined referrals, cooperation (via regular communication about clients), coordination (agreed protocols) to integration (single system) (Wilcox, 2010; Potito, Day, Carson & O’Leary, 2009).
Although most research supports joined up services, some evidence indicates that the ability to meet the service needs of sexual assault victims but not domestic violence victims was improved when NGOs and legal services worked in collaboration (Zweig & Burt, 2003; for further review of literature on DV and SXA integrated responses, see Breckenridge et al., 2015).
In order for IPSV and re-victimisation to be adequately addressed, services need to simultaneously be consolidated and to provide specialist responses to the specific contexts of IPSV and re-victimisation (Bennice & Resick, 2003). Moreover, services need to be sensitive to the impacts of structural and attitudinal limitations on access to certain forms of coordinated response, including systemic restrictions due to limited accessibility and exclusion criteria based on a woman’s behaviour and/or health status (e.g. whether she uses injecting drugs) (Breckenridge et al., 2015). Researchers recommend that, as a first priority, there needs to be a shift in the Australian context so that there can be meaningful partnerships across services (Heenan, 2004).
Health professionals
“…many times victims present as domestic violence victims [although] in reality they’re both, but the other part doesn’t come out for a very long time”
– Research participant
Primary care professionals, such as general practitioners (GPs), are the gateway for many women into specialist DV or SXA services (Hegarty, Hindmarsh, & Gilles, 2000; Palmer & Parekh, 2014). Despite this, practitioners rarely receive training in DV and SXA, and are even less likely to be skilled in dealing with co-occurrence or re-victimisation (Maas-DeSpain & Todahl, 2014; Parkinson & Zara, 2014; Todahl & Walters, 2009).
In order for a GP to get a full picture of the DV that their patient is experiencing, it is important for them to assess both physical and sexual victimisation. A range of characteristics of this conversation may increase its helpfulness:
- Assurance of, and practices to ensure absolute maintenance of, confidentiality, especially in contexts where the GP sees other members of the woman’s family (including, potentially, the perpetrator of the violence).
- The provision of a comprehensive and sensitive discussion of IPSV may be assisted by using a validated screening tool.
- Asking separately and directly about IPSV may increase disclosure.
- Emphasising that the woman is believed may assist women to feel safe and supported.
- Explicitly identifying the described behaviours as IPSV may be helpful in contextualising the violence.
- Practitioners should be aware that a disclosure of physical violence may not include disclosure of IPSV, and that not mentioning IPSV does not necessarily mean that it is not happening.
- Capacity to engage in basic safety planning and referrals as required.
(Maas-DeSpain & Todahl, 2014; Palmer & Parekh, 2014; Parkinson & Reid, 2014; Spiller et al., 2012; Wall, 2012)
Researchers note that current screening methods could be improved by expanding the definition of IPSV to include not only intimate partner rape, but also sexual acquiescence, with the American College of Obstetrician and Gynaecologists providing detailed guidelines related to IPSV and reproductive coercion screening (Chamberlain & Levenson, 2012; Maas- DeSpain & Todahl, 2014; see also Williamson, 2014).
Treatment
Behavioural change perpetrator programs aim to stop men reoffending. Such programs are typically aimed at either SXA or DV perpetrators, with few structured in a way to acknowledge the high rate of co-occurrence in the form of IPSV. There is significant variation in the approaches used in these programs, however they tend to be didactic in nature (Nelson et al., 2010). Programs often have a high dropout rate, with a 50 percent completion rate considered typical (Day, O’Leary, Chung, & Justo, 2009).
Salter (2012) notes that perpetrator programs have little empirical support, with individual studies, literature reviews and meta-analyses showing no behavioural improvement in men who complete these programs. These traditional programs are particularly ineffective with high risk offenders, whose re-offending patterns are highly resistant to available intervention programs (Salter, 2012). Such equivocal evidence emphasises the need to improve interventions, rather than dismantle them (Campbell, 2005).
A minority of researchers promote interventions which provide couples with skills to improve communication and manage conflict (Mathes, 2013). Problematically, a sub set of these scholars recommend that victims should change their coping strategies as changes in the violent behaviour of their partner is unlikely (Sullivan et al., 2010).
Justice responses
This review identified significant legal debate on mainstream justice responses to IPSV. This discussion centred on how the law understands consent, and in particular, whether or not a presumption of ongoing consent is legally valid. Feminist legal scholars continue to advocate for the full removal of discussions of a woman’s sexual history from prosecutions of rape (Bergen, 2006; Clark, 2007; Ellison, 2010; McGlynn, 2010; Sack, 2010).
In addition, there is significant debate regarding whether restorative justice approaches are appropriate in these instances (Cripps & McGlade, 2008; Daly, 2006; McAlinden, 2008). Restorative justice approaches for youth sex offending show some promise, although initial research is limited in its ability to show changes in recidivism (Daly, Bouhours, Broadhurst, & Loh, 2013). Evaluation on circle sentencing impact has found no effect of the process on recidivism, however such research is not focused on DV, SXA or instances of their co-occurrence (Fitzgerald, 2008).
Prevention
Recent Australian initiatives such as Our Watch[8] are indicative of a consensus that prevention is necessary for ongoing changes in the epidemiology of violence.[9] Primary prevention, or stopping violence before it starts, is a priority of both practitioners and large policy bodies such as the US Centre for Disease Control (Martin et al., 2009). Despite this, very little research has engaged with the effectiveness of programs which address community attitudes, with research consistently focused on changes to individual behaviour (Sabina & Ho, 2014).
Prevention programs are unevenly distributed within communities, often along socio-economic lines. For instance, a US study of over 3000 counties found that having a top- ranked university in a county “was a significant predictor of the number of DV programs in the area” (Sabina & Ho, 2014, p. 214; Tiefenthaler, Farmer, & Sambira, 2005).
Research with young people emphasises the need for prevention activities to be tailored to the target audience (e.g. age, sex and ethnicity) and must address the relationship between normative gender roles and dating sexual violence (Noonan & Charles, 2009).
At a more individual level, a number of researchers have examined interventions that encourage women to enact “protective behaviours” or address victim “controllable” factors. These programs may support victim blaming and thus have limited support in the violence against women sector (Herman, 2009). Opponents of these programs note that by focusing on women’s “bad habits”, these programs support the power structures that enable gendered violence to happen in the first place (Lichtenstein, 2005). When programs do attempt to augment potential victim’s behaviours, such as intervening with women who have experienced CSA as a way of preventing adult sexual assault, these programs have been shown to have limited effectiveness (Hill et al., 2011; Macy, 2007).
Domestic violence and sexual assault bystander programs aim to provide people observing violence against women with the skills and confidence to intervene (Moynihan et al., 2010; Moynihan, Banyard, Arnold, Eckstein, & Stapleton, 2011). Dedicated bystander programs are particularly common on university campuses, with programs often combining SXA and DV prevention in the same campaign (Lichty, Campbell, & Schuiteman, 2008). Within the context of enabling successful bystander interventions, such programs often have an implicit engagement with gender norms and violence supporting attitudes.
Education
“[What’s needed is] education for the males – that females are not just a piece of equipment to be used whenever you want it.”
– Sexual offences and child abuse officer, NSW
Public education about DV happens in Australia in a range of ways, including sex education classes in schools and large scale public awareness campaigns. Public education on DV does not tend to focus on IPSV, despite IPSV being a major form of DV (Flicker et al., 2011).
Young people are particularly in need of education about sexual consent, with education on adolescent IPSV needing to be tailored to specific target groups and addressing the impact of traditional gender roles on sexual expectations and behaviours (Levy-Peck, 2014a; Noonan & Charles, 2009). Provision of such education varies significantly between schools and across jurisdictions.
Professional training, including of “grass roots” professionals interested in primary prevention, is also important. Very few practitioners receive comprehensive education in DV epidemiology or screening methods (Maas-DeSpain & Todahl, 2014; Martin et al., 2009; Todahl & Walters, 2009). In the Australian context, accredited vocational training is available in the area of DV, however equivalent training is not available for SXA – this reduces the professional development available to SXA and DV workers, as well as other front line service providers such as GPs (Macleod, 2014b; Parkinson & Zara, 2014). It is necessary to provide specialist training in order to ensure that appropriate responses are given to women from minority groups who experience IPSV or re- victimisation, including Aboriginal and Torres Strait Islander communities.
Overall, the available literature demonstrates responses to re-victimisation and IPSV that are across the full continuum of interventions – from primary prevention to tertiary responses. Most of these initiatives occur in the context of wider SXA and DV services, with the complex contexts of service delivery meaning that some clients may “fall through the cracks” between the sectors.
Recommendations and conclusion
“Effective response to IPSV [and re- victimisation] is the place where the movements to end and address domestic violence and sexualised violence come together”
Research on IPSV and re-victimisation is characterised by a range of systemic issues. A major ongoing issue in research in these areas is the siloing of research by type of assault (DV vs SXA) in a way that limits our understanding of women’s experiences when they cross these definitional boundaries (Sabina & Ho, 2014). The following recommendations are based in the research examined for this state of knowledge paper and can be made regarding the method and focus of future research.
ANROWS recommends that:
- As re-victimisation often occurs across violence types, researchers should, wherever possible, expand their examination of life course re-victimisation to multiple violence types.
- Longitudinal research is critical to understanding the complex pathways that result in repeated victimisation and IPSV. Such research is particularly important for understanding the lived experience of marginalised women (e.g. incarcerated women), as the intersections of disadvantage are even more complex for these populations (Poister, Tusher, & Cook, 2010). Put differently, “longitudinal research is needed to sort out risk factors, from consequences, from simple correlates” (Classen et al., 2005, p. 114).
- As has been noted for several decades now, one way of increasing the quality and comparability of research findings is for there to be consistent definitions of abusive behaviours used in IPSV and re-victimisation research. Such definitions would need to provide clarity to research participants about what was meant by “force” in relation to sexual activity, with distinctions made between physical threat and emotional/psychological coercion tactics.
- Future research should concentrate on relevant target groups. Many target groups have relatively small populations, making collecting data with population level surveys difficult. One exception to this is disability, which has a high prevalence and thus analysable data is likely to be able to be collected in all violence research. Most other sub- populations are likely to require dedicated surveys to get a sufficient sample to be statistically reliable.
- Although both qualitative and quantitative research is needed to inform Aboriginal and Torres Strait Islander family violence policy, priority should be given to quantitative research as current quantitative surveys like the PSS are unable to provide prevalence estimates for this population.
In order for IPSV and cross-type re-victimisation to be meaningfully addressed in the Australian context, it is necessary to provide coordinated SXA and DV services that occur in the context of supportive social service systems (Heenan, 2004). The following recommendations are made regarding the service delivery environment and are based on the research findings reviewed in this paper.
IPSV and “cross-type” re-victimisation are scenarios of violence which emphasise the inter-related nature of SXA and DV. This violence does not happen in silos or vacuums, rather it is a complex lived experience that crosses the conceptual lines which are frequently part of policy and service provision. Until there is full acknowledgement in the DV and SXA sectors that domestic violence and sexual assault are interdependent concepts, some of the instances of violence most in need of our attention will continue to be sidelined from mainstream responses (Sabina & Ho, 2014).
ANROWS recommends that:
- Acknowledgement is made in policy and practice of weaknesses in our current research base, which means that we are heavily reliant on practice knowledge.
- Accurate and appropriate use of data and acknowledgement of data’s limitations is encouraged in policy, planning and service advocacy, so that when further evidence-based knowledge is available, it is welcomed and adopted.
- To address the stigma of IPSV, DV and SXA services continue to work to raise awareness of the impact of stigma on clients and staff.
- Judicial education and professional development work continues to be supported to ensure court and police sensitivity in IPSV cases, and to minimise the distress of the legal process to women who have experienced re- victimisation and/or IPSV.
- Where not already part of normal clinical practice, STI clinics be provided with training and materials to enable streamlined referrals to SXA and DV services.
- Trauma informed care (a model of care which puts at the centre of clinical practice the long term effects of victimisation) be supported through mainstream service provision and research investment.
- Large scale mental health campaigns promote gendered violence as a risk factor for poor mental health outcomes.
- All DV and SXA services be sufficiently resourced to further enrich cross-sector co-ordination (a full range of co- ordination strategies are possible, from referral pathways to fully integrated care).
- All DV and SXA services, as well as related services such as mental health and drug and alcohol programs, continue to work towards an integrated understanding of the impacts of the escalation or severity of CSA on adulthood in their engagements with both children and adults.
- Public education on violence against women acknowledges the distinct but intersectional dimensions of different forms of violence and its gendered impacts and characteristics.
- Providers of mainstream health and social services be sensitised to the possibility of IPSV and re-victimisation cases in their day to day work. An initial step towards this would be the promotion of existing IPSV screening tools to a wide range of mainstream frontline providers.
- Prevention programs not be funded by government if they implicitly or explicitly support victim blaming. Explanation of these actions should be given to campus unions to promote a similar stance in university campus programs.
- Professional development for workers in the violence against women field acknowledge the multi-faceted nature of abuse and emphasise the links between DV and SXA.
Appendix A: Searched databases
EBSCO collections:
- Academic Search Premier;
- Aboriginal Australia;
- Health;
- Law;
- Psychology;
- Social Sciences – General, Statistics.
Proquest collections:
- ABI/Inform;
- PsychInfo;
- PsychArticles;
- Criminal Justice;
- Family Health;
- Health & Medical Complete;
- Health Management;
- Nursing & Allied Health Source;
- Psychology Journals;
- Research Library;
- Social Science Journals;
- Sociology.
Informit collections:
- Arts & humanities;
- Health;
- Indigenous peoples;
- Social Science.
JSTOR collections:
- Feminist & women’s studies;
- Health policy;
- Health sciences;
- Humanities;
- Law;
- Medicine and allied health;
- Psychology;
- Public health;
- Social studies;
- Social work;
- Sociology.
ANROWS collections:
- Bibliography of Australian Domestic Violence and Sexual Assault research.
Appendix B: Additional available literature
Re-victimisation
A variety of populations have been examined in relation to re-victimisation involving CSA and DV including:
- women attending health clinics (Williams et al., 2010);
- college students (Ménard & Pincus, 2014);
- women with severe mental illness (Meade et al., 2009); and
- women who were seeking help for DV (Vatnar & Bjørkly, 2008).
Research is predominately completed in the US, with some research from Spain (Garcia-Linares et al., 2005; Pico-Alfonso et al., 2006), Australia (Schei et al., 2006) and Norway (Vatnar & Bjørkly, 2008).
Intimate partner sexual violence rates
Overall there is extensive research on the rate of IPSV, typically in the context of estimating overall DV prevalence. Some examples of study populations are:
- women of various ethnicities (e.g. white, Hispanic, black) (McFarlane, Malecha, Watson, et al., 2005; Ramisetty-Mikler, Caetano, & McGrath, 2007);
- migrant communities (Liles et al., 2012; Morash, Bui, Zhang, & Holtfreter, 2007);
- people in same-sex relationships (Edwards et al., 2015; Stoddard, Dibble, & Fineman, 2009);
- pregnant women (Flanagan, Jaquier, Gordon, Moore, & Stuart, 2014);
- adolescents (Hess et al., 2013; Howard, Wang, & Yan, 2007; Sears & Byers, 2010; Zurbriggen et al., 2010); and
- women who are incarcerated (Raj et al., 2008).
Much of the research that used the CTS compared violence perpetration and victimisation rates for women and men, and thus provided significant gender comparisons (e.g. Dardis, Edwards, Kelley, & Gidycz, 2013). Population level studies include examination of IPSV rates in national representative samples (Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007) and adult women (Thompson et al., 2006).
Several studies used the CTS2 to compare rates of mild and severe sexual coercion.[10] Rates of severe sexual coercion and mild coercion varied with population group (represented below in brackets as severe: mild), including:
- US college women (2.2%: 27.8%) (Sabina & Straus, 2008);
- Polish college women (11%: 57%) (Doroszewicz & Forbes, 2008);
- women experiencing police involved DV (26.26%: 41.67%) (Messing et al., 2014);
- women receiving emergency department care (15%: 24% [any sexual coercion]) (El-Bassel et al., 2007); and
- US college women reporting on dating violence in adolescence (5.4%: 25.3%) (Bonomi, Anderson, Nemeth, Rivara, & Buettner, 2013).
Studies also examined particular abusive behaviours. Although the majority of research projects examined IPSV in a broad sense, and included sexual coercion, some were limited to, or explicitly separated, partner rape (Bergen & Bukovec, 2006; Finkelhor & Yllö, 1987; Logan, 2009; Maas-DeSpain & Todahl, 2014; Martin et al., 2007; McFarlane, 2007; Tellis, 2010). Research often focused on verbal coercion (Brousseau et al., 2012; Dutton & Goodman, 2005; Eaton & Matamala, 2014), with a small number of papers examining attempted rape (Möller, Bäckström, Söndergaard, & Helström, 2012) or forced sexual initiation (Campbell, Lucea, Stockman, & Draughon, 2013). Researchers also defined their research population by relationship type, with studies focusing on:
- dating IPSV (Doroszewicz & Forbes, 2008; Edwards et al., 2015; Foshee et al., 2007; Gagné et al., 2005; Katz, Moore, & May, 2008; Montoya, Coker-Appiah, Eng, Wynn, & Townsend, 2013; Reyes & Foshee, 2013; Sears & Byers, 2010);
- newly married couples (Panuzio & Dilillo, 2010); and,
- IPSV perpetrated by a married spouse (Martin et al., 2007).
Research has also examined the prevalence of IPSV in sub- sets of violence affected individuals, such as:
- women who are have been physically abused by their partner (Spiller, Jouriles, McDonald, & Skopp, 2012);
- women who have protection orders against their partner (Logan, 2009);
- men arrested for the physical assault of their female partner (Basile & Hall, 2011);
- women seeking assistance for SXA (Kennedy et al., 2012); and
- women who are residing in refuges (Spiller et al., 2012).
Although almost all studies were completed in the US, a small number of projects examined IPSV in other countries such as:
- Australia (Mouzos & Makkai, 2004; Schei et al., 2006);
- Spain (Pico-Alfonso et al., 2006);
- Japan (Yoshihama & Horrocks, 2010);
- Poland (Doroszewicz & Forbes, 2008); and
- Sweden (Möller et al., 2012).
References
Abbey, A. (2011). Alcohol’s role in sexual violence perpetration: Theoretical explanations, existing evidence and future directions. Drug and Alcohol Review, 30(5), 481-489.
Abbey, A., Parkhill, M. R., & Koss, M. P. (2005). The effects of frame of reference on responses to questions about sexual assault victimization and perpetration. Psychology of Women Quarterly, 29(4), 364-373.
Aboriginal Family Violence Prevention and Legal Service Victoria. (2010). Improving accessibility of the legal system for Aboriginal and Torres Strait Islander victims/survivors of family violence and sexual assault. Policy Paper Series: Paper 3 of 3. Collingwood, Vic: Aboriginal Family Violence Prevention and Legal Service Victoria.
Adams, R., & Hunter, Y. (2007). Surviving justice: Family violence, sexual assault and child sexual assault in remote Aboriginal communities in NSW. Indigenous Law Bulletin, 7(1), 26-28.
Addington, L. A., & Rennison, C. M. (2008). Rape co- occurrence: Do additional crimes affect victim reporting and police clearance of rape? Journal of Quantitative Criminology, 24(2), 205-226.
Ahrens, C. E., Dean, K., Rozee, P. D., & McKenzie, M. (2008). In F. L. Denmark & M. A. Paludi (Eds.), Psychology of women: A handbook of issues (2nd ed.). Westport, CT: Praeger Publishers.
Allimant, A., & Ostapiej-Piatkowski, B. (2011). Supporting women from CALD backgrounds who are victims/survivors of sexual violence: Challenges and opportunities for practitioners. Melbourne: Australian Institute of Family Studies.
Andersen, J. P., Hughes, T. L., Zou, C., & Wilsnack, S. C. (2014). Lifetime victimization and physical health outcomes among lesbian and heterosexual women. PLoS ONE, 9(7), e101939.
Arata, C. M. (2000). From child victim to adult victim: A model for predicting sexual revictimization. Child Maltreatment, 5(1), 28-38.
Arata, C. M., & Lindman, L. (2002). Marriage, child abuse, and sexual revictimization. Journal of Interpersonal Violence, 17(9), 953-971.
Argento, E., Muldoon, K. A., Duff, P., Simo, A., Deering,
K. N., & Shannon, K. (2014). High prevalence and partner correlates of physical and sexual violence by intimate partners among street and off-street sex workers. PLoS ONE, 9(7), 1-7.
Armour, C., & Sleath, E. (2014). Assessing the co-occurrence of intimate partner violence domains across the life-course: Relating typologies to mental health. European Journal of Psychotraumatology, 5.
Australian Bureau of Statistics. (2013a). Defining the data challenge for family, domestic and sexual violence. Canberra: ABS.
Australian Bureau of Statistics. (2013b). Personal Safety Survey, 2012. Canberra: ABS.
Babcock, R. L., & Deprince, A. P. (2013). Factors contributing to ongoing intimate partner abuse: Childhood betrayal trauma and dependence on one’s perpetrator. Journal of Interpersonal Violence, 28(7), 1385-1402.
Bagwell-Gray, M. E., Messing, J. T., & Baldwin-White, A. (2015). Intimate partner sexual violence: A review of terms, definitions, and prevalence. Trauma, Violence, & Abuse, 16(3), 316-335.
Bair-Merritt, M., Ghazarian, S., Burrell, L., & Duggan, A. (2012). Patterns of intimate partner violence in mothers at-risk for child maltreatment. Journal of Family Violence, 27(4), 287-294.
Baldry, E., & Cunneen, C. (2014). Imprisoned Indigenous women and the shadow of colonial patriarchy. Australian & New Zealand Journal of Criminology, 47(2), 276-298.
Barger, E., Wacker, J. Macy, R. & Parish, S. (2009). Sexual assault prevention for women with intellectual disabilities: A critical review of the evidence. Intellectual and Developmental Disabilities, 47(4), 249-262.
Barnes, J. E., Noll, J. G., Putnam, F. W., & Trickett, P. K. (2009). Sexual and physical revictimization among victims of severe childhood sexual abuse. Child Abuse & Neglect, 33(7), 412-420.
Basile, K. (2008). Histories of violent victimization among women who reported unwanted sex in marriages and intimate relationships: Findings from a qualitative study. Violence Against Women, 14(1), 29-52.
Basile, K., Arias, I., Desai, S., & Thompson, M. P. (2004). The differential association of intimate partner physical, sexual, psychological, and stalking violence and posttraumatic stress symptoms in a nationally representative sample of women. Journal of Traumatic Stress, 17(5), 413-421.
Basile, K., & Hall, J. E. (2011). Intimate partner violence perpetration by court-ordered men: Distinctions and intersections among physical violence, sexual violence, psychological abuse, and stalking. Journal of Interpersonal Violence, 26(2), 230-253.
Bebbington, P., Jonas, S., Kuipers, E., King, M., Cooper, C., Brugha, T., . . . Jenkins, R. (2011). Childhood sexual abuse and psychosis: Data from a cross-sectional national psychiatric survey in England. The British Journal of Psychiatry, 199(1), 29-37.
Bennice, J. A., & Resick, P. A. (2003). Marital rape history, research, and practice. Trauma, Violence, & Abuse, 4(3), 228-246.
Bennice, J. A., Resick, P. A., Mechanic, M., & Astin, M. (2003). The relative effects of intimate partner physical and sexual violence on post-traumatic stress disorder symptomatology. Violence and Victims, 18(1), 87.
Bergen, R.K. (2006). Marital rape: New research and directions. Retrieved from https://www.vawnet.org/Assoc_Files_VAWnet/AR_MaritalRapeRevised.pdf
Bergen, R. K., & Bukovec, P. (2006). Men and intimate partner rape: Characteristics of men who sexually abuse their partner. Journal of Interpersonal Violence, 21(10), 1375-1384.
Black, M. C., Basile, K., Breiding, M. J., Smith, S. G., Walters,
M. L., Merrick, M. T., . . . Stevens, M. R. (2011). National intimate partner and sexual violence survey: 2010 summary report. Atlanta, Ga: National Center for Injury Prevention and Control.
Blagg, H., Bluett-Boyd, N., & Williams, E. (2015). Innovative models in addressing violence against Indigenous women (State of knowledge paper 10). Sydney: ANROWS.
Blagg, H., Murray, R., Ray, D., & Macarthy, E. (2000). Crisis intervention in Aboriginal family violence: Strategies and models for Western Australia. Canberra: Department of the Prime Minister and Cabinet.
Boivin, S., Lavoie, F., Hébert, M., & Gagné, M.-H. (2012). Past victimizations and dating violence perpetration in adolescence: The mediating role of emotional distress and hostility. Journal of Interpersonal Violence, 27(4), 662-684.
Bonomi, A. E., Anderson, M. L., Nemeth, J., Rivara, F. P., & Buettner, C. (2013). History of dating violence and the association with late adolescent health. BMC Public Health, 13(1), 1-12.
Bonomi, A. E., Anderson, M. L., Rivara, F. P., Cannon, E. A., Fishman, P. A., Carrell, D., . . . Thompson, R. S. (2008). Health care utilization and costs associated with childhood abuse. Journal of General Internal Medicine, 23(3), 294-299.
Bonomi, A. E., Anderson, M. L., Rivara, F. P., & Thompson, R. S. (2007). Health outcomes in women with physical and sexual intimate partner violence exposure. Journal of Women’s Health, 16(7), 987-997.
Bonomi, A. E., Holt, V. L., Martin, D. P., & Thompson, R. S. (2006). Severity of intimate partner violence and occurrence and frequency of police calls. Journal of Interpersonal Violence, 21(10), 1354-1364.
Brassard, A., Darveau, V., Péloquin, K., Lussier, Y., & Shaver,
P. R. (2014). Childhood sexual abuse and intimate partner violence in a clinical sample of men: The mediating roles of adult attachment and anger management. Journal of Aggression, Maltreatment & Trauma, 23(7), 683-704.
Breckenridge, J., Rees, S., valentine, k., & Murray, S. (2015). Meta-evaluation of existing interagency partnerships, collaboration, coordination and/or integrated interventions and service responses to violence against women: State of knowledge paper 11. Sydney: ANROWS.
Briere, J. N., & Elliott, D. M. (1994). Immediate and long- term impacts of child sexual abuse. The Future of Children, 4(2), 54-69.
Broach, J. L., & Petretic, P. A. (2006). Beyond traditional definitions of assault: Expanding our focus to include sexually coercive experiences. Journal of Family Violence, 21(8), 477-486.
Bronfenbrenner, U. (2005). Making human beings human: Bioecological perspectives on human development. Thousand Oaks: Sage.
Brousseau, M. M., Hébert, M., & Bergeron, S. (2012). Sexual coercion within mixed-sex couples: The roles of sexual motives, revictimization, and reperpetration. The Journal of Sex Research, 49(6), 533-546.
Brownridge, D. A., & Halli, S. S. (2001). Explaining violence against women in Canada. Lanham, Md: Lexington Books.
Brownridge, D. A. (2006). Partner violence against women with disabilities Prevalence, risk, and explanations. Violence Against Women, 12(9), 805-822.
Busby, D. M., Holman, T. B., & Walker, E. (2008). Pathways to relationship aggression between adult partners. Family Relations, 57(1), 72-83.
Busch-Armendariz, N. B., DiNitto, D. M., Bell, H., & Bohman,
T. (2010). Sexual assault perpetrators’ alcohol and drug use: The likelihood of concurrent violence and post-sexual assault outcomes for women victims. Journal of Psychoactive Drugs, 42(3), 393-399.
Campbell, R. (2012). Fight, flight, or . . . freeze? Yes. Freeze. New York: Joyful Heart Foundation.
Campbell, J. (2005). Assessing dangerousness in domestic violence cases: History, challenges, and opportunities. Criminology & Public Policy, 4(4), 653-671.
Campbell, J. C., Baty, M. L., Ghandour, R. M., Stockman, J. K., Francisco, L., & Wagman, J. (2008). The intersection of intimate partner violence against women and HIV/AIDS: a review. International Journal of Injury Control and Safety Promotion, 15(4), 221-231.
Campbell, J., Jones, A. S., Dienemann, J., Kub, J., Schollenberger, J., O’Campo, P., Wynne, C. (2002). Intimate partner violence and physical health consequences. Archives of Internal Medicine, 162(10), 1157-1163.
Campbell, J., Lucea, M. B., Stockman, J. K., & Draughon, J.E. (2013). Forced sex and HIV risk in violent relationships. American Journal of Reproductive Immunology, 69, 41-44.
Campbell, J. C., Webster, D. W., & Glass, N. (2009). The danger assessment validation of a lethality risk assessment instrument for intimate partner femicide. Journal of Interpersonal Violence, 24(4), 653-674.
Cannon, E. A., Bonomi, A. E., Anderson, M., Rivara, F. P., & Thompson, R. S. (2010). Adult health and relationship outcomes among women with abuse experiences during childhood. Violence and Victims, 25(3), 291-305.
Casey, E., & Lindhorst, T. P. (2009). Toward a multi-level, ecological approach to the primary prevention of sexual assault: Prevention in peer and community contexts. Trauma, Violence, & Abuse, 10(2), 91-114.
Casey, E., & Nurius, P. S. (2005). Trauma exposure and sexual revictimization risk: Comparisons across single, multiple incident, and multiple perpetrator victimizations. Violence Against Women, 11(4), 505-530.
Casteel, C., Martin, S. L., Smith, J. B., Gurka, K. K., & Kupper,
L. L. (2008). National study of physical and sexual assault among women with disabilities. Injury Prevention, 14(2), 87-90.
Cattaneo, L. B., & Goodman, L. A. (2005). Risk factors for reabuse in intimate partner violence a cross-disciplinary critical review. Trauma, Violence, & Abuse, 6(2), 141-175.
Chamberlain, L., & Levenson, R. (2012). Addressing intimate partner violence, reproductive and sexual coercion: A guide for obstetric, gynecologic and reproductive health care settings. Washington, DC: American College of Obstetricians and Gynecologists.
Chan, K. L. (2011). Correlates of childhood sexual abuse and intimate partner sexual victimization. Partner Abuse, 2(3), 365-381.
Chiu, G. R., Lutfey, K. E., Litman, H. J., Link, C. L., Hall, S. A., & McKinlay, J. B. (2013). Prevalence and overlap of childhood and adult physical, sexual, and emotional abuse: A descriptive analysis of results from the Boston Area Community Health (BACH) survey. Violence & Victims, 28(3), 381-402.
Christopher, F. S., & Pflieger, J. C. (2007). Sexual aggression: The dark side of sexuality in relationships. Annual Review of Sex Research, 18, 115-142.
Clark, H., & Quadara, A. (2010). Insights into sexual assault perpetration: Giving voice to victim/survivors’ knowledge. (Research report 18). Melbourne: Australian Institute of Family Studies.
Clark, H. (2007). Judging rape: Public attitudes and sentencing.. Melbourne: Australian Centre for the Study of Sexual Assault.
Classen, C. C., Palesh, O. G., & Aggarwal, R. (2005). Sexual revictimization: A review of the empirical literature. Trauma, Violence & Abuse, 6(2), 103-129.
Coid, J., Petruckevitch, A., Feder, G., Chung, W.-S., Richardson, J., & Moorey, S. (2001). Relation between childhood sexual and physical abuse and risk of revictimisation in women: A cross-sectional survey. The Lancet, 358(9280), 450-454.
Coker, A. L., Hopenhayn, C., DeSimone, C. P., Bush, H. M., & Crofford, L. (2009). Violence against women raises risk of cervical cancer. Journal of Women’s Health, 18(8), 1179-1185.
Coker, A. L., Sanderson, M., Cantu, E., Huerta, D., & Fadden, M. K. (2008). Frequency and types of partner violence among Mexican American college women. Journal of American College Health, 56(6), 665-673.
Cole, J., Logan, T., & Shannon, L. (2005). Intimate sexual victimization among women with protective orders: Types and associations of physical and mental health problems. Violence & Victims, 20(6), 695-715.
Conway, P., Cresswell, J., Harmon, D., Pospishil, C., Smith, K., Wages, J., & Weisz, L. (2010). Using empowerment evaluation to facilitate the development of intimate partner and sexual violence prevention programs. Journal of Family Social Work, 13(4), 343-361.
Cooper, L., Anaf, J., & Bowden, M. (2008). Can social workers and police be partners when dealing with bikie-gang related domestic violence and sexual assault? European Journal of Social Work, 11(3), 295-311.
Cornelius, T. L., & Resseguie, N. (2007). Primary and secondary prevention programs for dating violence: A review of the literature. Aggression and Violent Behavior, 12(3), 364-375.
Cortis, N. & Bullen, J. (2015). Building effective policies and services to promote women’s economic security following domestic violence: State of knowledge paper 7. Sydney: ANROWS.
Costello, M. (2005). The disappearing ‘F’ word: Feminism and Australian Government violence against women policies? Women Against Violence: An Australian Feminist Journal, 17, 41-50.
Coulter, M., & VandeWeerd, C. (2009). Reducing domestic violence and other criminal recidivism: Effectiveness of a multilevel batterers intervention program. Violence & Victims, 24(2), 139-152.
Cox, P. (2015). Violence against women: Additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey, 2012, (ANROWS Horizons 1). Sydney: ANROWS.
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241-1299.
Cripps, K. (2008). Indigenous family violence: A statistical challenge. Injury, 39, Supplement 5, S25-S35.
Cripps, K., & McGlade, H. (2008). Indigenous family violence and sexual abuse: Considering pathways forward. Journal of Family Studies, 14(2-3), 240-253.
Cripps, K., Miller, L. & Saxton-Barney, J. (2010). Too hard to handle: Indigenous victims of violence with disabilities. Indigenous Law Bulletin, 7(21), 3.
Crisp, A. H., Gelder, M. G., Rix, S., Meltzer, H. I., & Rowlands, O. J. (2000). Stigmatisation of people with mental illnesses. The British Journal of Psychiatry, 177(1), 4-7.
Cuevas, C. A., Sabina, C., & Milloshi, R. (2012). Interpersonal victimization among a national sample of Latino women. Violence Against Women, 18(4), 377-403.
Culbertson, K. A., & Dehle, C. (2001). Impact of sexual assault as a function of perpetrator type. Journal of Interpersonal Violence, 16(10), 992-1007.
Cyr, M., McDuff, P., & Wright, J. (2006). Prevalence and predictors of dating violence among adolescent female victims of child sexual abuse. Journal of Interpersonal Violence, 21(8), 1000-1017.
Daigneault, I., Hébert, M., & McDuff, P. (2009). Men’s and women’s childhood sexual abuse and victimization in adult partner relationships: A study of risk factors. Child Abuse & Neglect, 33(9), 638-647.
Daly, K. (2006). Restorative justice and sexual assault: An archival study of court and conference cases. British Journal of Criminology, 46(2), 334-356.
Daly, K., Bouhours, B., Broadhurst, R., & Loh, N. (2013). Youth sex offending, recidivism and restorative justice: Comparing court and conference cases. Australian & New Zealand Journal of Criminology, 46(2), 241-267.
Dardis, C. M., Edwards, K. M., Kelley, E. L., & Gidycz, C. A. (2013). Dating violence perpetration: The predictive roles of maternally versus paternally perpetrated childhood abuse and subsequent dating violence attitudes and behaviors. Journal of Aggression, Maltreatment & Trauma, 22(1), 6-25.
Davis, M. (2014). Law enforcement response to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.). Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Day, A., O’Leary, P., Chung, D., & Justo, D. (2009). Integrated responses to domestic violence: Research and practice experiences in working with men. In A. Day, L. Forsythe, & K. Adams (Eds.), Domestic violence: Working with men: Research, practice experiences and integrated responses. Annandale, NSW: Federation Press.
Decker, S. H., Spohn, C., Ortiz, N. R., & Hedberg, E. (2014). Criminal stigma, race, gender and employment: An expanded assessment of the consequences of imprisonment for employment. Washington: National Institute of Justice.
DeKeseredy, W. S., & Schwartz, M. D. (2008). Separation/ divorce sexual assault in rural Ohio: Survivors’ perceptions. Journal of Prevention & Intervention in the Community, 36(1/2), 105-119.
DeKeseredy, W. S., & Schwartz, M. D. (2001). Definitional issues. In C.M. Renzetti, J.L. Edleson & R.K. Bergen (Eds.). Sourcebook on violence against women (2nd ed.) (pp. 23-34). Thousand Oaks, CA: Sage.
DeKeseredy, W. S. (2014). Separation/divorce sexual assault. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.). Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
DeLisi, M., Caudill, J. W., & Trulson, C. R. (2014). Does childhood sexual abuse victimization translate into juvenile sexual offending? New evidence. Violence and Victims, 29(4), 620-635.
Desai, S. & Saltzman, L. (2001). Measurement issues for violece against women. In C.M. Renzetti, J.L. Edleson & R.K. Bergen (Eds.). Sourcebook on violence against women (2nd ed.) (pp. 35-52). Thousand Oaks, CA: Sage.
Dietrich, A. M., Smiley, W. C., & Frederick, C. (2007). The roles of childhood maltreatment and psychopathy in sexual recidivism of treated sex offenders. Journal of Aggression, Maltreatment & Trauma, 14(3), 19-31.
Dobash, R. P., & Dobash, R. E. (2004). Women’s violence to men in intimate relationships: Working on a puzzle. British Journal of Criminology, 44(3), 324-349.
Dobash, R. P., Dobash, R. E., Wilson, M., & Daly, M. (1992). The myth of sexual symmetry in marital violence. Social Problems, 39(1), 71-91.
Doroszewicz, K., & Forbes, G. B. (2008). Experiences with dating aggression and sexual coercion among Polish college students. Journal of Interpersonal Violence, 23(1), 58-73.
Dutton, M. A., & Goodman, L. A. (2005). Coercion in intimate partner violence: Toward a new conceptualization. Sex Roles, 52(11-12), 743-756.
Dutton, M. A., Kaltman, S., Goodman, L. A., Weinfurt, K., & Vankos, N. (2005). Patterns of intimate partner violence: Correlates and outcomes. Violence and Victims, 20(5), 483-497.
Easteal, P. (2014). Advice for criminal justice staff and/or advocates to aid intimate partner sexual violence survivors. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Eaton, A., & Matamala, A. (2014). The relationship between heteronormative beliefs and verbal sexual coercion in college students. Archives of Sexual Behavior, 43(7), 1443-1457.
Eaton, D. K., Kann, L., Kinchen, S., Shanklin, S., Flint, K. H., Hawkins, J., . . . Wechsler, H. (2012). Youth risk behavior surveillance – United States, 2011. Morbidity and Mortality Weekly Report. Surveillance Summaries, 61(SS04), 1-162.
Edwards, K. M., Sylaska, K. M., Barry, J. E., Moynihan, M. M., Banyard, V. L., Cohn, E. S., . . . Ward, S. K. (2015). Physical dating violence, sexual violence, and unwanted pursuit victimization: A comparison of incidence rates among sexual-minority and heterosexual college students. Journal of Interpersonal Violence, 30(4), 580-600.
El-Bassel, N., Gilbert, L., Wu, E., Chang, M., Gomes, C., Vinocur, D., & Spevack, T. (2007). Intimate partner violence prevalence and HIV risks among women receiving care in emergency departments: Implications for IPV and HIV screening. Emergency Medicine Journal, 24(4), 255-259.
Ellison, L. (2010). Commentary on R v A (No 2). In R. Hunter, C. McGlynn & E. Rackley (Eds.). Feminist judgments: From theory to practice (pp. 206-210). Oxford: Hart Publishing.
Fang, X., & Corso, P. S. (2008). Gender differences in the connections between violence experienced as a child and perpetration of intimate partner violence in young adulthood. Journal of Family Violence, 23(5), 303-313.
Fargo, J. D. (2009). Pathways to adult sexual revictimization: Direct and indirect behavioral risk factors across the lifespan. Journal of Interpersonal Violence, 24(11), 1771-1791.
Feerick, C., & Easteal, P. W. (2005). Sexual assault by male partners: Is the licence still valid? Flinders Journal of Law Reform, 8(2), 185-207.
Feiring, C., Simon, V. A., Cleland, C. M., & Barrett, E. P. (2013). Potential pathways from stigmatization and externalizing behavior to anger and dating aggression in sexually abused youth. Journal of Clinical Child & Adolescent Psychology, 42(3), 309-322.
Felson, R. B., & Pare, P.-P. (2007). Does the criminal justice system treat domestic violence and sexual assault offenders leniently? JQ: Justice Quarterly, 24(3), 435-459.
Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2006). Examining the intergenerational transmission of violence in a New Zealand birth cohort. Child Abuse& Neglect, 30(2), 89-108.
Ferro, C., Cermele, J & Saltzman, A. (2008). Current perceptions of marital rape: Some good and some not-so-good news. Journal of Interpersonal Violence , 23(6), 764-779.
Filipas, H. H., & Ullman, S. E. (2006). Child sexual abuse, coping responses, self-blame, posttraumatic stress disorder, and adult sexual revictimization. Journal of Interpersonal Violence, 21(5), 652-672.
Finkelhor, D., & Yllö, K. (1987). License to rape: Sexual abuse of wives. New York: Holt, Rinehart and Winston.
Fisher, B. S., Daigle, L. E., Cullen, F. T., & Turner, M. G. (2003). Reporting sexual victimization to the police and others results from a national-level study of college women. Criminal Justice and Behavior, 30(1), 6-38.
Fitzgerald, J. (2008). Does circle sentencing reduce Aboriginal offending? Sydney: NSW Bureau of Crime Statistics and Research.
Flanagan, J. C., Jaquier, V., Gordon, K. C., Moore, T. M., & Stuart, G. L. (2014). Examining the prevalence, bidirectionality, and co-occurrence of sexual intimate partner violence among women during pregnancy and postpartum. Partner Abuse, 5(4), 407-419.
Flicker, S. M., Cerulli, C., Zhao, X., Tang, W., Watts, A., Xia, Y., & Talbot, N. L. (2011). Concomitant forms of abuse and help-seeking behavior among white, African American, and Latina women who experience intimate partner violence. Violence Against Women, 17(8), 1067-1085.
Flood, M. G., & Kendrick, V. (2012). “LOVEBiTES: Anevaluation of the LOVEBiTES and respectful relationships programs in a Sydney school”. Wollongong: University of Wollongong.
Follette, V. M., Polusny, M. A., Bechtle, A. E., & Naugle, A. E. (1996). Cumulative trauma: The impact of child sexual abuse, adult sexual assault, and spouse abuse. Journal of Traumatic Stress, 9(1), 25-35.
Foshee, V. A., Bauman, K. E., Linder, F., Rice, J., & Wilcher, R. (2007). Typologies of adolescent dating violence: Identifying typologies of adolescent dating violence perpetration. Journal of Interpersonal Violence, 22(5), 498-519.
Fotheringham, S., & Tomlinson, D. (2009). Identifying the potential for collaboration between women’s shelters and sexual assault centres: Comparing and contrasting the service delivery needs of clients. Currents, 8(1).
Freedner, N., Freed, L. H., Yang, Y. W., & Austin, S. B. (2002). Dating violence among gay, lesbian, and bisexual adolescents: Results from a community survey. Journal of Adolescent Health, 31(6), 469-474.
Friedman, M. J., Jalowiec, J., McHugo, G., Wang, S., & McDonagh, A. (2007). Adult sexual abuse is associated with elevated neurohormone levels among women with PTSD due to childhood sexual abuse. Journal of Traumatic Stress, 20(4), 611-617.
Friesen, M. D., Woodward, L. J., Horwood, L. J., & Fergusson, D. M. (2010). Childhood exposure to sexual abuse and partnership outcomes at age 30. Psychological Medicine, 40(4), 679-688.
Gagné, M.-H., Lavoie, F., & Hébert, M. (2005). Victimization during childhood and revictimization in dating relationships in adolescent girls. Child Abuse & Neglect, 29(10), 1155-1172.
Gallagher, K. E., Hudepohl, A. D., & Parrott, D. J. (2010). Power of being present: The role of mindfulness on the relation between men’s alcohol use and sexual aggression toward intimate partners. Aggressive Behavior, 36(6), 405-413.
Garcia-Linares, M. I., Pico-Alfonso, M. A., & Sanchez-Lorente, S. (2005). Assessing physical, sexual, and psychological violence perpetrated by intimate male partners toward women: A Spanish cross-sectional study. Violence and Victims, 20(1), 99-123.
Gibson, L. E., & Leitenberg, H. (2001). The impact of child sexual abuse and stigma on methods of coping with sexual assault among undergraduate women. Child Abuse & Neglect, 25(10), 1343-1361.
Gobin, R. L., Iverson, K. M., Mitchell, K., Vaughn, R., & Resick, P. A. (2013). The impact of childhood maltreatment on PTSD symptoms among female survivors of intimate partner violence. Violence and Victims, 28(6), 984-999.
Goldscheid, J. (2006). Domestic and sexual violence as sex discrimination: Comparing American and international approaches. Thomas Jefferson Law Review, 28(3), 355-397.
Goodlin, W. E., & Dunn, C. S. (2010). Three patterns of domestic violence in households: Single victimization, repeat victimization, and co-occurring victimization. Journal of Family Violence, 25(2), 107-122.
Green, B. L., Krupnick, J. L., Stockton, P., Goodman, L., Corcoran, C., & Petty, R. (2005). Effects of adolescent trauma exposure on risky behavior in college women. Psychiatry, 68(4), 363-378.
Griffing, S., Ragin, D. F., Morrison, S. M., Sage, R. E., Madry, L., & Primm, B. J. (2005). Reasons for returning to abusive relationships: Effects of prior victimization. Journal of Family Violence, 20(5), 341-348.
Guerrero, D. (2009). Hypermasculinity, intimate partner violence, sexual aggression, social support, and child maltreatment risk in urban, heterosexual fathers taking parenting classes. Child Welfare, 88(4), 135-155.
Hamby, S. (2014). Intimate partner and sexual violence research scientific progress, scientific challenges, and gender. Trauma, Violence, & Abuse, 15(3), 149-158.
Hamby, S., & Turner, H. (2013). Measuring teen dating violence in males and females: Insights from the national survey of children’s exposure to violence. Psychology of Violence, 3(4), 323-339.
Hattery, A. J. (2009). Sexual abuse in childhood: Intimate partner violence in adulthood – struggles for African American and white women. Race, Gender & Class, 16(1-2), 194-217.
Hazen, A. L., & Soriano, F. I. (2007). Experiences with intimate partner violence among Latina women. Violence Against Women, 13(6), 562-582.
Hébert, M., Lavoie, F., Vitaro, F., McDuff, P., & Tremblay, R. E. (2008). Association of child sexual abuse and dating victimization with mental health disorder in a sample of adolescent girls. Journal of Traumatic Stress, 21(2), 181-189.
Heenan, M. (2004). Just “keeping the peace”: A reluctance to respond to male partner sexual violence. Melbourne: Australian Institute of Family Studies.
Hegarty, K., Bush, R., & Sheehan, M. (2005). The composite abuse scale: Further development and assessment of reliability and validity of a multidimensional partner abuse measure in clinical settings. Violence and Victims, 20(5), 529-547.
Hegarty, K., Hindmarsh, E. D., & Gilles, M. T. (2000). Domestic violence in Australia: Definition, prevalence and nature of presentation in clinical practice. Medical Journal of Australia, 173(7), 363-367.
Hegarty, K., & Roberts, G. (1998). How common is domestic violence against women? The definition of partner abuse in prevalence studies. Australian and New Zealand Journal of Public Health, 22(1), 49-54.
Heise, L. L. (1998). Violence against women an integrated, ecological framework. Violence Against Women, 4(3), 262-290.
Herman, J. (2009). There’s a fine line…: Adolescent dating violence and prevention. Pediatric Nursing, 35(3).
Herz, D. C., Stroshine, M., & Houser, K. (2005). Exploring agreement on appropriate responses to domestic violence and sexual trauma across victim advocates, mental health service providers, and substance abuse treatment providers. Women & Criminal Justice, 16(4), 119-144.
Hess, K. L., Javanbakht, M., Brown, J. M., Weiss, R. E., Hsu, P., & Gorbach, P. M. (2013). Intimate partner violence and anal intercourse in young adult heterosexual relationships. Perspectives on Sexual & Reproductive Health, 45(1), 6-12.
Hetzel, M. D., & McCanne, T. R. (2005). The roles of peritraumatic dissociation, child physical abuse, and child sexual abuse in the development of posttraumatic stress disorder and adult victimization. Child Abuse & Neglect, 29(8), 915-930.
Hickson, L., Khemka, I., Golden, H., & Chatzistyli, A. (2013). Views and values of developmental disabilities and domestic violence/sexual assault support professionals regarding the prevention and handling of situations of abuse. Journal of Policy & Practice in Intellectual Disabilities, 10(3), 207-214.
Hill, J. M., Vernig, P. M., Lee, J. K., Brown, C., & Orsillo, S. M. (2011). The development of a brief acceptance and mindfulness- based program aimed at reducing sexual revictimization among college women with a history of childhood sexual abuse. Journal of Clinical Psychology, 67(9), 969-980.
Holleran, D., Beichner, D., & Spohn, C. (2010). Examining charging agreement between police and prosecutors in rape cases. Crime & Delinquency, 56(3), 385-413.
Holtzworth-Munroe, A. (2005). Female perpetration of physical aggression against an intimate partner: A controversial new topic of study. Violence and Victims, 20(2), 251-259.
Holtzworth-Munroe, A., Meehan, J. C., Herron, K., Rehman, U., & Stuart, G. L. (2000). Testing the Holtzworth-Munroe and Stuart (1994) batterer typology. Journal of Consulting and Clinical Psychology, 68(6), 1000.
Hovane, V. (2007). White privilege and the fiction of colour blindness: Implications for best practice standards for Aboriginal victims of family violence. Sydney: Australian Domestic and Family Violence Clearinghouse.
Hovane, V. (2015). Our story to tell: Aboriginal perspectives on domestic and family violence. ANROWS Footprints, 1, 13-17.
Howard, D. E., Wang, M. Q., & Yan, F. (2007). Prevalence and psychosocial correlates of forced sexual intercourse among US high school adolescents. Adolescence, 42(168), 629-643.
Hunnicutt, G. (2009). Varieties of patriarchy and violence against women: Resurrecting “patriarchy” as a theoretical tool. Violence Against Women, 15(5), 553-573.
Ireland, T. O., & Smith, C. A. (2009). Living in partner- violent families: Developmental links to antisocial behavior and relationship violence. Journal of Youth and Adolescence, 38(3), 323-339.
Iverson, K., Gradus, J. L., Resick, P. A., Suvak, M. K., Smith, K. F., & Monson, C. M. (2011). Cognitive–behavioral therapy for PTSD and depression symptoms reduces risk for future intimate partner violence among interpersonal trauma survivors. Journal of Consulting and Clinical Psychology, 79(2), 193.
Iverson, K., Mercado, R., Carpenter, S. L., & Street, A. E. (2013). Intimate partner violence among women veterans: Previous interpersonal violence as a risk factor. Journal of Traumatic Stress, 26(6), 767-771.
Jankowski, M. K., Leitenberg, H., Henning, K., & Coffey, P. (2002). Parental caring as a possible buffer against sexual revictimization in young adult survivors of child sexual abuse. Journal of Traumatic Stress, 15(3), 235-244.
Jason, P., Hubbard, P., & Birch, P. (2013). Sex worker victimization, modes of working, and location in New South Wales, Australia: A geography of victimization. The Journal of Sex Research, 50(6), 574-586.
Jennings, W. G., Zgoba, K. M., Maschi, T., & Reingle, J. M. (2014). An empirical assessment of the overlap between sexual victimization and sex offending. International Journal of Offender Therapy & Comparative Criminology, 58(12), 1466-1480.
Johnson, H. (2005). Assessing the prevalence of violence against women in Canada. Statistical Journal of the UN Economic Commission for Europe, 22(3/4), 225-238.
Johnson, M. P. (2006). Conflict and control gender symmetry and asymmetry in domestic violence. Violence Against Women, 12(11), 1003-1018.
Johnson, I. M. (2014). Economic impediments to women’s success on parole: “We need someone on our side”. The Prison Journal, 94(3), 365-387.
Katz, J., Moore, J., & May, P. (2008). Physical and sexual co victimization from dating partners: A distinct type of intimate abuse? Violence Against Women, 14(8), 961-980.
Keel, M. (2004). Family violence and sexual assault in Indigenous communities: “Walking the talk” (ACSSA Briefing No 4). Melbourne: Australian Institute of Family Studies.
Kelly, L. (2013). Surviving sexual violence. Cambridge: John Wiley & Sons.
Kelly, T. C., & Stermac, L. (2012). Intimate partner sexual assault against women: Examining the impact and recommendations for clinical practice. Partner Abuse, 3(1), 107-122.
Kelly, U. A., Skelton, K., Patel, M., & Bradley, B. (2011). More than military sexual trauma: Interpersonal violence, PTSD, and mental health in women veterans. Research in Nursing & Health, 34(6), 457-467.
Kennedy, A., Adams, A., Bybee, D., Campbell, R., Kubiak, S., & Sullivan, C. (2012). A model of sexually and physically victimized women’s process of attaining effective formal help over time: The role of social location, context, and intervention. American Journal of Community Psychology, 50(1/2), 217-228.
Kernsmith, P. (2006). Gender differences in the impact of family of origin violence on perpetrators of domestic violence. Journal of Family Violence, 21(2), 163-171.
Kerr, I. (2014). Counseling and advocacy perspectives on intimate partner sexual violence. In L. McOrmond Plummer,
J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Kilpatrick, D. G., Resnick, H. S., Ruggiero, K. J., Conoscenti, L. M., & McCauley, J. (2007). Drug-facilitated, incapacitated, and forcible rape: A national study. Charlston, SC: Medical University of South Carolina, National Crime Victims Research & Treatment Center.
Kilroy, D. (2014). Effective approaches to helping intimate partner sexual violence survivors in prison. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Kim-Godwin, Y. S., Clements, C., McCuiston, A., & Fox, J.A. (2009). Dating violence among high school students in southeastern North Carolina. The Journal of School Nursing, 25(2), 141-151.
The Kirby Institute. (2015). HIV, viral hepatitis and sexually transmissible infections in Australia Annual Surveillance Report 2015. Sydney: UNSW.
Kitzmann, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witnesses to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339.
Koopman, C., Ismailji, T., Palesh, O., Gore-Felton, C., Narayanan, A., Saltzman, K. M., . . . McGarvey, E. L. (2007). Relationships of depression to child and adult abuse and bodily pain among women who have experienced intimate partner violence. Journal of Interpersonal Violence, 22(4), 438-455.
Koss, M. P., Abbey, A., Campbell, R., Cook, S., Norris, J., Testa, M., . . . White, J. (2007). Revising the SES: A collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly, 31(4), 357-370.
Krebs, C., Breiding, M. J., Browne, A., & Warner, T. (2011). The association between different types of intimate partner violence experienced by women. Journal of Family Violence, 26(6), 487-500.
Krug, E. G., Mercy, J. A., Dahlberg, L. L., & Zwi, A. B. (2002). The world report on violence and health. The Lancet, 360(9339), 1083-1088.
Lacey, K. K., McPherson, M. D., Samuel, P. S., Powell Sears, K., & Head, D. (2013). The impact of different types of intimate partner violence on the mental and physical health of women in different ethnic groups. Journal of Interpersonal Violence, 28(2), 359-385.
Lalande, K. M., & Bonanno, G. A. (2011). Retrospective memory bias for the frequency of potentially traumatic events: A prospective study. Psychological Trauma: Theory, Research, Practice, and Policy, 3(2), 165-170.
Langley, J., Martin, J., & Nada-Raja, S. (1997). Physical assault among 21-year-olds by partners. Journal of Interpersonal Violence, 12(5), 675-684.
Larcombe, W., & Heath, M. (2012). Developing the common law and rewriting the history of rape in marriage in Australia: PGA v The Queen. Sydney Law Review, 34, 785-809.
Lawless, S., Kippax, S., & Crawford, J. (1996). Dirty, diseased and undeserving: The positioning of HIV positive women. Social Science & Medicine, 43(9), 1371-1377.
Lawrie, R. (2003). Speak out speak strong: Rising imprisonment rates of Aboriginal women. Indigenous Law Bulletin, 5(24), 5-7.
Lazar, R. (2010). Negotiating sex: The legal construct of consent in cases of wife rape in Ontario, Canada. Canadian Journal of Women and the Law, 22(2), 329-363.
Lehrer, J. A., Lehrer, E. L., & Koss, M. P. (2013). Unwanted sexual experiences in young men: Evidence from a survey of university students in Chile. Archives of Sexual Behavior, 42(2), 213-223.
Levy-Peck, J. (2014a). Addressing intimate partner sexual violence in teen relationships. In L. McOrmond Plummer,
J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers..
Levy-Peck, J. (2014b). The role of the advocate in addressing intimate partner sexual violence. In L. McOrmond Plummer,
J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Liang, B., Goodman, L., Tummala-Narra, P., & Weintraub, S. (2005). A theoretical framework for understanding help- seeking processes among survivors of intimate partner violence. American Journal of Community Psychology, 36(1-2), 71-84.
Lichtenstein, B. (2005). Domestic violence, sexual ownership, and HIV risk in women in the American deep south. Social Science & Medicine, 60(4), 701-714.
Lichty, L. F., Campbell, R., & Schuiteman, J. (2008). Developing a university-wide institutional response to sexual assault and relationship violence. Journal of Prevention & Intervention in the Community, 36(1/2), 5-22.
Liles, S., Usita, P., Irvin, V., Hofstetter, C., Beeston, T., & Hovell, M. (2012). Prevalence and correlates of intimate partner violence among young, middle, and older women of Korean descent in California. Journal of Family Violence, 27(8), 801-811.
Littleton, H. (2014). Interpersonal violence on college campuses: Understanding risk factors and working to find solutions. Trauma, Violence & Abuse, 15(4), 297-303.
Littleton, H., Breitkopf, C. R., & Berenson, A. (2008). Beyond the campus: Unacknowledged rape among low-income women. Violence Against Women, 14(3), 269-286.
Lloyd, S. A., & Emery, B. C. (1999). The dark side of courtship: Physical and sexual aggression. Thousand Oaks: Sage Publications.
Logan, T. (2009). The Kentucky Civil Protective Order Study: A rural and urban multiple perspective study of protective order violation consequences, responses and costs. Lexington: University of Kentucky, Department of Behavioral Science.
Logan, T., & Cole, J. (2011). Exploring the intersection of partner stalking and sexual abuse. Violence Against Women, 17(7), 904-924.
Logan, T., Cole, J. R., & Shannon, L. A. (2007). A mixed- methods examination of sexual coercion and degradation among women in violent relationships who do and do not report forced sex. Violence and Victims, 22(1), 71-94.
Logan, T., Walker, R., & Cole, J. (2013). Silenced suffering: The need for a better understanding of partner sexual violence. Trauma, Violence, & Abuse, 16, 111-135.
Long, J. M. (2009). Intimate partner sexual assault. In Washington Coalition of Sexual Assault Programs (Ed.), Intimate partner sexual violence: Sexual assault in the context of domestic violence. Olympia, WA: Washington Coalition of Sexual Assault Programs.
Ludermir, A. B., Schraiber, L. B., D’Oliveira, A. F. P. L., França- Junior, I., & Jansen, H. A. (2008). Violence against women by their intimate partner and common mental disorders. Social Science & Medicine, 66(4), 1008-1018.
Lutz-Zois, C. J., Phelps, C. E. R., & Reichle, A. C. (2011). Affective, behavioral, and social-cognitive dysregulation as mechanisms for sexual abuse revictimization. Violence and Victims, 26(2), 159-176.
Maas-DeSpain, A., & Todahl, J. L. (2014). Rape, sexual violence, and acquiescence in intimate relationships: Screening, assessment, and clinical decision making. Journal of Feminist Family Therapy, 26(1), 28-49.
Macleod, D. (2014a). Fatality and health risks associated with intimate partner sexual sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Macleod, D. (2014b). Real not rare: Cross-training for sexual assault and domestic violence workers to understand, recognize, and respond to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Macy, R. J. (2007). Sexual revictimization: Implications for social work practice. Families in Society, 88(4), 627-636.
Macy, R. J., Giattina, M., Sangster, T. H., Crosby, C., & Montijo, N. J. (2009). Domestic violence and sexual assault services: Inside the black box. Aggression & Violent Behavior, 14(5), 359-373.
Macy, R. J., Giattina, M. C., Montijo, N. J., & Ermentrout, D. M. (2010). Domestic violence and sexual assault agency directors’ perspectives on services that help survivors. Violence Against Women, 16(10), 1138-1161.
Macy, R. J., Giattina, M. C., Parish, S. L., & Crosby, C. (2010). Domestic violence and sexual assault services: Historical concerns and contemporary challenges. Journal of Interpersonal Violence, 25(1), 3-32.
Macy, R. J., Johns, N., Rizo, C. F., Martin, S. L., & Giattina, M. (2011). Domestic violence and sexual assault service goal priorities. Journal of Interpersonal Violence, 26(16), 3361-3382.
Magdol, L., Moffitt, T. E., Caspi, A., Newman, D. L., Fagan, J., & Silva, P. A. (1997). Gender differences in partner violence in a birth cohort of 21-year-olds: Bridging the gap between clinical and epidemiological approaches. Journal of Consulting and Clinical Psychology, 65(1), 68.
Mallie, A. L., Viljoen, J. L., Mordell, S., Spice, A., & Roesch, R. (2011). Childhood abuse and adolescent sexual re-offending: A meta-analysis. Child & Youth Care Forum, 40(5), 401-417.
Martin, E., Taft, C. T., & Resick, P. A. (2007). A review of marital rape. Aggression & Violent Behavior, 12(3), 329-347.
Martin, S. L., Coyne-Beasley, T., Hoehn, M., Mathew, M., Runyan, C. W., Orton, S., & Royster, L.-A. (2009). Primary prevention of violence against women. Violence Against Women, 15(1), 44-56.
Mathes, E. (2013). Why is there a strong positive correlation between perpetration and being a victim of sexual coercion? An exploratory study. Journal of Family Violence, 28(8), 783-796.
McAlinden, A. (2008). Restorative justice as a response to sexual offending: Addressing the failings of current punitive approaches. Sexual Offender Treatment, 3(1), 1-12.
McFarlane, J. (2007). Pregnancy following partner rape: What we know and what we need to know. Trauma, Violence & Abuse, 8(2), 127-134.
McFarlane, J., Malecha, A., Gist, J., Watson, K., Batten, E., Hall, I., & Smith, S. (2005). Intimate partner sexual assault against women and associated victim substance use, suicidality, and risk factors for femicide. Issues in Mental Health Nursing, 26(9), 953-967.
McFarlane, J., Malecha, A., Watson, K., Gist, J., Batten, E., Hall, I., & Smith, S. (2005). Intimate partner sexual assault against women: Frequency, health consequences, and treatment outcomes. Obstetrics & Gynecology, 105(1), 99-108.
McGlynn, C. (2010). R v A (No 2) Judgment. In R. Hunter, C. McGlynn & E. Rackley (Ed.), Feminist judgments: From theory to practice (pp. 211-227). Oxford: Hart Publishing.
McLean, R., & Goodman-Delahunty, J. (2008). The influence of relationship and physical evidence on police decision- making in sexual assault cases. Australian Journal of Forensic Sciences, 40(2), 109-121.
McOrmond-Plummer, L. (2014). Preventing secondary wounding by misconception: What professionals really need to know about intimate partner sexual violence. In
L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
McOrmond-Plummer. (2009). Considering the differences: Intimate partner sexual violence in sexual assault and domestic violence discourse. In Washington Coalition of Sexual Assault Programs (Ed.), Intimate partner sexual violence: Sexual assault in the context of domestic violence. Olympia, WA: Washington Coalition of Sexual Assault Programs.
McOrmond-Plummer, L., Easteal, P. & Levy-Peck, J.Y. (2014). The necessity of appropriate service response to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Meade, C. S., Kershaw, T. S., Hansen, N. B., & Sikkema, K. J. (2009). Long-term correlates of childhood abuse among adults with severe mental illness: Adult victimization, substance abuse, and HIV sexual risk behavior. AIDS and Behavior, 13(2), 207-216.
Ménard, K. S., & Pincus, A. L. (2014). Child maltreatment, personality pathology, and stalking victimization among male and female college students. Violence and Victims, 29(2), 300-316.
Messing, J. T., Thaller, J., & Bagwell, M. (2014). Factors related to sexual abuse and forced sex in a sample of women experiencing police-involved intimate partner violence. Health & Social Work, 39(3), 181.
Messinger, A. M. (2011). Invisible victims: Same-sex IPV in the national violence against women survey. Journal of Interpersonal Violence, 26(11), 2228-2243.
Messman-Moore, T. L., & Long, P. J. (2003). The role of childhood sexual abuse sequelae in the sexual revictimization of women: An empirical review and theoretical reformulation. Clinical Psychology Review, 23(4), 537-571.
Messman-Moore, T. L., Long, P. J., & Siegfried, N. J. (2000). The revictimization of child sexual abuse survivors: An examination of the adjustment of college women with child sexual abuse, adult sexual assault, and adult physical abuse. Child Maltreatment, 5(1), 18-27.
Messman-Moore, T. L., Walsh, K. L., & DiLillo, D. (2010). Emotion dysregulation and risky sexual behavior in revictimization. Child Abuse & Neglect, 34(12), 967-976.
Messman-Moore, T. L., Ward, R. M., & Brown, A. L. (2009). Substance use and PTSD symptoms impact the likelihood of rape and revictimization in college women. Journal of Interpersonal Violence, 24(3), 499-521.
Miller, D. (2006). The effects of childhood physical abuse or childhood sexual abuse in battered women’s coping mechanisms: Obsessive-compulsive tendencies and severe depression. Journal of Family Violence, 21(3), 185-195.
Miller, E., Breslau, J., Chung, W. J. J., Green, J. G., McLaughlin, K. A., & Kessler, R. C. (2011). Adverse childhood experiences and risk of physical violence in adolescent dating relationships. Journalof Epidemiology & Community Health, 65(11), 1006-1013.
Miller, G., Chen, E., & Zhou, E. S. (2007). If it goes up, must it come down? Chronic stress and the hypothalamic- pituitary-adrenocortical axis in humans. Psychological Bulletin, 133(1), 25.
Miller, J. (2006). A specification of the types of intimate partner violence experienced by women in the general population. Violence Against Women, 12(12), 1105-1131.
Mitchell, L. (2011). Domestic violence in Australia: An overview of the issues. Canberra: Parliamentary Library.
Möller, A. S., Bäckström, T., Söndergaard, H. P., & Helström, L. (2012). Patterns of injury and reported violence depending on relationship to assailant in female Swedish sexual assault victims. Journal of Interpersonal Violence, 27(16), 3131-3148.
Monson, C. M., & Langhinrichsen-Rohling, J. (1999). Sexual and nonsexual marital aggression: Legal considerations, epidemiology, and an integrated typology of perpetrators. Aggression and Violent Behavior, 3(4), 369-389.
Montoya, T., Coker-Appiah, D. S., Eng, E., Wynn, M. R., & Townsend, T. G. (2013). A qualitative exploration of rural African American youth perceptions about the effect of dating violence on sexual health. Journal of Child & Family Studies, 22(1), 48-62.
Moore, E. (2002). Not just court: Family violence in rural New South Wales: Aboriginal women speak out. Wagga Wagga: Centre for Rural Social Research.
Morash, M., Bui, H., Zhang, Y., & Holtfreter, K. (2007). Risk factors for abusive relationships: A study of Vietnamese American immigrant women. Violence Against Women, 13(7), 653-675.
Moreau, C., Boucher, S., Hébert, M., & Lemelin, J. (2015). Capturing sexual violence experiences among battered women using the revised sexual experiences survey and the revised conflict tactics scales. Archives of Sexual Behavior, 44(1), 223-231.
Morokoff, P. J., Redding, C. A., Harlow, L. L., Cho, S., Rossi, J. S., Meier, K. S., . . . Brown‐Peterside, P. (2009). Associations of sexual victimization, depression, and sexual assertiveness with unprotected sex: A test of the multifaceted model of HIV risk across gender. Journal of Applied Biobehavioral Research, 14(1), 30-54.
Mouzos, J., & Makkai, T. (2004). Women’s experiences of male violence: Findings from the Australian component of the International Violence Against Women Survey (IVAWS) (Research and Public Policy No 56). Canberra: Australian Institute of Criminology Canberra.
Moynihan, M. M., Banyard, V. L., Arnold, J. S., Eckstein, R. P., & Stapleton, J. G. (2010). Engaging intercollegiate athletes in preventing and intervening in sexual and intimate partner violence. Journal of American College Health, 59(3), 197-204.
Moynihan, M. M., Banyard, V. L., Arnold, J. S., Eckstein, R. P., & Stapleton, J. G. (2011). Sisterhood may be powerful for reducing sexual and intimate partner violence: An evaluation of the Bringing in the Bystander in-person program with sorority members. Violence Against Women, 17(6), 703-719.
Murphy, L. M. (2011). Childhood and adolescent violent victimization and the risk of young adult intimate partner violence victimization. Violence and Victims, 26(5), 593-607.
National Coalition of Anti-violence Programs. (2014). 2013 Report on lesbian, gay, bisexual, transgender, queer, and HIV-affected intimate partner violence. New York: National Coalition of Anti-violence Programs.
Nelson, A., Lewy, R., Ricardo, F., Dovydaitis, T., Hunter, A., Mitchell, A., . . . Kugel, C. (2010). Eliciting behavior change in a US sexual violence and intimate partner violence prevention program through utilization of Freire and discussion facilitation. Health Promotion International, 25(3), 299-308.
Niehaus, A. F., Jackson, J., & Davies, S. (2010). Sexual self- schemas of female child sexual abuse survivors: Relationships with risky sexual behavior and sexual assault in adolescence. Archives of Sexual Behavior, 39(6), 1359-1374.
Nisbet, I., Wilson, P., & Smallbone, S. (2004). A prospective longitudinal study of sexual recidivism among adolescent sex offenders. Sexual Abuse: A Journal of Research and Treatment, 16(3), 223-234.
Noonan, R. K., & Charles, D. (2009). Developing teen dating violence prevention strategies. Violence Against Women, 15(9), 1087-1105.
Northern Territory. Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse. (2007). Report of the Northern Territory Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse. Darwin: Department of the Chief Minister.
Oktay, J. S., & Tompkins, C. J. (2004). Personal assistance providers’ mistreatment of disabled adults. Health & Social Work, 29(3), 177-188.
Orchowski, L., & Gidycz, C. A. (2012). To whom do college women confide following sexual assault? A prospective study of predictors of sexual assault disclosure and social reactions. Violence Against Women, 18(3), 264-288.
Orchowski, L., Untied, A., & Gidycz, C. (2013). Factors associated with college women’s labeling of sexual victimization. Violence and Victims, 28(6), 940-958.
Orcutt, H. K., Cooper, M. L., & Garcia, M. (2005). Use of sexual intercourse to reduce negative affect as a prospective mediator of sexual revictimization. Journal of Traumatic Stress, 18(6), 729-739.
Palmer, C., & Parekh, V. (2014). Medical indicators and responses to intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Palmetto, N., Davidson, L. L., Breitbart, V., & Rickert, V. I. (2013). Predictors of physical intimate partner violence in the lives of young women: Victimization, perpetration, and bidirectional violence. Violence and Victims, 28(1), 103-121.
Panchanadeswaran, S., Frye, V., Nandi, V., Galea, S., Vlahov, D., & Ompad, D. (2010). Intimate partner violence and consistent condom use among drug-using heterosexual women in New York City. Women & Health, 50(2), 107-124.
Panuzio, J., & Dilillo, D. (2010). Physical, psychological, and sexual intimate partner aggression among newlywed couples: Longitudinal prediction of marital satisfaction. Journal of Family Violence, 25(7), 689-699.
Parekh, V., & Williams, A. (2014). Forensic medical assessment in intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Parkinson, D., & Reid, S. (2014). “Invisible” intimate partner sexual violence: Prevention and intervention challenges. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Parkinson, D., & Zara, C. (2014). Issues faced by intimate partner sexual violence survivors in rural areas. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Patriquin, M. A., Wilson, L. C., Kelleher, S. A., & Scarpa, A. (2012). Psychophysiological reactivity to abuse-related stimuli in sexually revictimized women. Journal of Aggression, Maltreatment & Trauma, 21(7), 758-775.
Pease, B. (2014). Theorising men’s violence prevention policies. In N. Henry, & A. Powell (Eds.), Preventing sexual violence: Interdisciplinary approaches to overcoming a rape culture. London: Palgrave Macmillan.
Pease, B. (2008). Engaging men in men’s violence prevention: Exploring the tensions, dilemmas and possibilities. Australian Domestic & Family Violence Clearinghouse, (17), 1-20.
Pereda, N., & Gallardo-Pujol, D. (2014). One hit makes the difference: The role of polyvictimization in childhood in lifetime revictimization on a southern European sample. Violence and Victims, 29(2), 217-231.
Peterson, G. W., & Bush, K. R. (Eds.). Handbook of marriage and the family (3rd ed.). New York: Springer Science+Business.
Pico-Alfonso, M. A., Garcia-Linares, M. I., Celda-Navarro, N., Blasco-Ros, C., Echeburúa, E., & Martinez, M. (2006). The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: Depressive symptoms, posttraumatic stress disorder, state anxiety, and suicide. Journal of Women’s Health, 15(5), 599-611.
Plummer, S.-B., & Findley, P. A. (2012). Women with disabilities’ experience with physical and sexual abuse: Review of the literature and implications for the field. Trauma, Violence & Abuse, 13(1), 15-29.
Poister Tusher, C., & Cook, S. L. (2010). Comparing revictimization in two groups of marginalized women. Journal of Interpersonal Violence, 25(10), 1893-1911.
Potito, C., Day, A., Carson, E., & O’Leary, P. (2009). Domestic violence and child protection: Partnerships and collaboration. Australian Social Work, 62(3), 369-387.
Potter, S. J., Fountain, K., & Stapleton, J. G. (2012). Addressing sexual and relationship violence in the LGBT community using a bystander framework. Harvard Review of Psychiatry, 20(4), 201-208.
Productivity Commission. (2009). Overcoming Indigenous disadvantage: Key indicators 2009. Canberra: Steering Committee for the Review of Government Service Provision.
Próspero, M., & Vohra-Gupta, S. (2008). The use of mental health services among victims of partner violence on college campuses. Journal of Aggression, Maltreatment & Trauma, 16(4), 376-390.
Quadara, A., Stathopoulos, M., & Jenkinson, R. (2015). Establishing the connection (between alcohol and other drug use and sexual victimisation): State of knowledge paper. ANROWS Landscapes, 6.
Raj, A., Rose, J., Decker, M. R., Rosengard, C., Hebert, M. R., Stein, M., & Clarke, J. G. (2008). Prevalence and patterns of sexual assault across the life span among incarcerated women. Violence Against Women, 14(5), 528-541.
Ramisetty-Mikler, S., Caetano, R., & McGrath, C. (2007). Sexual aggression among white, black, and Hispanic couples in the US: Alcohol use, physical assault and psychological aggression as its correlates. The American Journal of Drug and Alcohol Abuse, 33(1), 31-43.
Ranjbar, V., & Speer, S. A. (2013). Revictimization and recovery from sexual assault: Implications for health professionals. Violence and Victims, 28(2), 274-287.
Raphael, J., & Logan, T. (2009). The use (and misuse) of data on rape: Understanding the rape denial campaign in America: Part I. Sexual Assault Reports, 13(1), 1-16.
Reckdenwald, A., Mancini, C., & Beauregard, E. (2013). The cycle of violence: Examining the impact of maltreatment early in life on adult offending. Violence and Victims, 28(3), 466-482.
Rees, S., & Pease, B. (2007). Domestic violence in refugee families in Australia. Journal of Immigrant & Refugee Studies, 5(2), 1-19.
Rees, S., Silove, D., Chey, T., Ivancic, L., Steel, Z., Creamer, M., . . . Forbes, D. (2011). Lifetime prevalence of gender- based violence in women and the relationship with mental disorders and psychosocial function. JAMA, 306(5), 513-521.
Renner, L. M., & Whitney, S. D. (2012). Risk factors for unidirectional and bidirectional intimate partner violence among young adults. Child Abuse & Neglect, 36(1), 40-52.
Rennison, C. M., DeKeseredy, W. S., & Dragiewicz, M. (2012). Urban, suburban, and rural variations in separation/ divorce rape/sexual assault: Results from the National Crime Victimization Survey. Feminist Criminology, 7(4), 282-297.
Reyes, H. L., & Foshee, V. A. (2013). Sexual dating aggression across grades 8 through 12: Timing and predictors of onset. Journal of Youth & Adolescence, 42(4), 581-595.
Rich, C. L., Gidycz, C. A., & Warkentin, J. B. (2005). Child and adolescent abuse and subsequent victimization: A prospective study. Child Abuse & Neglect, 29(12), 1373-1394.
Rickert, V. I., Wiemann, C. M., Vaughan, R. D., & White, J. W. (2004). Rates and risk factors for sexual violence among an ethnically diverse sample of adolescents. Archives of Pediatrics & Adolescent Medicine, 158(12), 1132-1139.
Ristock, J. (2014). Sexual assault in intimate same-sex relationships. In L. McOrmond Plummer, J.Y. Levy- Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Romans, S., Forte, T., Cohen, M. M., Du Mont, J., & Hyman, I. (2007). Who is most at risk for intimate partner violence? A Canadian population-based study. Journal of Interpersonal Violence, 22(12), 1495-1514.
Roodman, A. A., & Clum, G. A. (2001). Revictimization rates and method variance: A meta-analysis. Clinical Psychology Review, 21(2), 183-204.
Ruiz-Pérez, I., Plazaola-Castaño, J., Álvarez-Kindelán, M., Palomo-Pinto, M., Arnalte-Barrera, M., Bonet-Pla, Á., . . . Garralón-Ruiz, L. M. (2006). Sociodemographic associations of physical, emotional, and sexual intimate partner violence in Spanish women. Annals of Epidemiology, 16(5), 357-363.
Sabina, C., & Ho, L. Y. (2014). Campus and college victim responses to sexual assault and dating violence disclosure, service utilization, and service provision. Trauma, Violence, & Abuse, 15(3), 201-226.
Sabina, C., & Straus, M. A. (2008). Polyvictimization by dating partners and mental health among U.S. college students. Violence and Victims, 23(6), 667-682.
Sabri, B., Barcelona de Mendoza, V., & Campbell, J. (2014). Immigrant women and intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Sack, E. (2009). Is domestic violence a crime? Intimate partner rape as allegory, St John’s Journal of Legal Commentary, 24(3), 535-566.
Salter, M. (2012). Managing recidivism amongst high risk violent men (Issues paper 23). Sydney: Australian Domestic & Family Violence Clearinghouse.
Salter, M. (2014). Multi-perpetrator domestic violence. Trauma, Violence & Abuse, 15(2), 102-112.
Schafran, L. H. (2014). Intimate partner sexual violence and the courts. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Schafran, L. H. (2010). Risk assessment and intimate partner sexual abuse. Judicature, 93(4), 161-163.
Schei, B., Guthrie, J. R., Dennerstein, L., & Alford, S. (2006). Intimate partner violence and health outcomes in mid-life women: A population-based cohort study. Archives of Womens Mental Health, 9(6), 317-324.
Schewe, P., Riger, S., & Howard, A. (2006). Factors associated with domestic violence and sexual assault victimization. Journal of Family Violence, 21(7), 469-475.
Schumacher, J. A., Feldbau-Kohn, S., Slep, A. M. S., & Heyman, R. E. (2001). Risk factors for male-to-female partner physical abuse. Aggression and Violent Behavior, 6(2), 281-352.
Sears, H. A., & Byers, E. S. (2010). Adolescent girls’ and boys’ experiences of psychologically, physically, and sexually aggressive behaviors in their dating relationships: Co- occurrence and emotional reaction. Journal of Aggression, Maltreatment & Trauma, 19(5), 517-539.
Seedat, S., Stein, M. B., & Forde, D. R. (2005). Association between physical partner violence posttraumatic stress, childhood trauma, and suicide attempts in a community sample of women. Violence and Victims, 20(1), 87-98.
Shaffer, D., & Kipp, K. (2013). Developmental psychology: Childhood and adolescence. Belmont, CA: Cengage Learning.
Shevlin, M., O’Neill, T., Houston, J., Read, J., Bentall, R., & Murphy, J. (2013). Patterns of lifetime female victimisation and psychotic experiences: A study based on the UK Adult Psychiatric Morbidity Survey 2007. Social Psychiatry & Psychiatric Epidemiology, 48(1), 15-24.
Shorey, R. C., Cornelius, T. L., & Bell, K. M. (2008). A critical review of theoretical frameworks for dating violence: Comparing the dating and marital fields. Aggression and Violent Behavior, 13(3), 185-194.
Siegel, J. A., & Williams, L. M. (2003). Risk factors for sexual victimization of women: Results from a prospective study. Violence Against Women, 9(8), 902-930.
Simmel, C., Postmus, J. L., & Lee, I. (2012). Sexual revictimization in adult women: Examining factors associated with their childhood and adulthood experiences. Journal of Child Sexual Abuse, 21(5), 593-611.
Smith, P. H., Thornton, G. E., DeVellis, R., Earp, J., & Coker, A. L. (2002). A population-based study of the prevalence and distinctiveness of battering, physical assault, and sexual assault in intimate relationships. Violence Against Women, 8(10), 1208-1232.
Smith, P. H., White, J. W., & Holland, L. J. (2003). A longitudinal perspective ondating violence among adolescent and college-age women. American Journal of Public Health, 93(7), 1104-1109.
Sørbø, M. F., Grimstad, H., Bjørngaard, J. H., Schei, B., & Lukasse, M. (2013). Prevalence of sexual, physical and emotional abuse in the Norwegian mother and child cohort study. BMC Public Health, 13(1), 1-11.
Spiller, L. C., Jouriles, E. N., McDonald, R., & Skopp, N. A. (2012). Physically abused women’s experiences of sexual victimization and their children’s disruptive behavior problems. Psychology of Violence, 2(4), 401-410.
Spohn, C., & Tellis, K. (2012). The criminal justice system’s response to sexual violence. Violence Against Women, 18(2), 169-192.
Stalans, L. J., Hacker, R., & Talbot, M. E. (2010). Comparing nonviolent, other-violent, and domestic batterer sex offenders: Predictive accuracy of risk assessments on sexual recidivism. Criminal Justice and Behavior, 37(5), 613-628.
Stark, E. (2009). Rethinking coercive control. Violence Against Women, 15(12), 1509-1525.
Stark, E. (2010). Do violent acts equal abuse? Resolving the gender parity/asymmetry dilemma. Sex Roles, 62(3-4), 201-211.
Stermac, L., Del Bove, G., Brazeau, P., & Bainbridge, D. (2006). Patterns in sexual assault violence as a function of victim perpetrator degree of relatedness. Journal of Aggression, Maltreatment & Trauma, 13(1), 41-58.
Stockman, J., Lucea, M., & Campbell, J. (2013). Forced sexual initiation, sexual intimate partner violence and HIV risk in women: A global review of the literature. AIDS & Behavior, 17(3), 832-847.
Stockman, J. K., Campbell, J. C., & Celentano, D. D. (2010). Sexual violence and HIV risk behaviors among a nationally representative sample of heterosexual American women: The importance of sexual coercion. Journal of Acquired Immune Deficiency Syndromes (1999), 53(1), 136.
Stoddard, J. P., Dibble, S. L., & Fineman, N. (2009). Sexual and physical abuse: A comparison between lesbians and their heterosexual sisters. Journal of Homosexuality, 56(4), 407-420.
Stotzer, R. L. (2009). Violence against transgender people: A review of United States data. Aggression and Violent Behavior, 14(3), 170-179.
Sullivan, T. P., McPartland, T. S., Armeli, S., Jaquier, V., & Tennen, H. (2012). Is it the exception or the rule? Daily co- occurrence of physical, sexual, and psychological partner violence in a 90-day study of substance-using, community women. Psychology of Violence, 2(2), 154-164.
Sullivan, T. P., Schroeder, J. A., Dudley, D. N., & Dixon, J.M. (2010). Do differing types of victimization and coping strategies influence the type of social reactions experienced by current victims of intimate partner violence? Violence Against Women, 16(6), 638-657.
Tanha, M., Beck, C. J. A., Figueredo, A. J., & Raghavan, C. (2010). Sex differences in intimate partner violence and the use of coercive control as a motivational factor for intimate partner violence. Journal of Interpersonal Violence, 25(10), 1836-1854.
Tapia, N. D. (2014). Survivors of child sexual abuse and predictors of adult re-victimization in the United States: A forward logistic regression analysis. International Journal of Criminal Justice Sciences, 9(1), 64-73.
Taylor, N., & Putt, J. (2007). Adult sexual violence in Indigenous and culturally and linguistically diverse communities in Australia. Canberra: Australian Institute of Criminology.
Tellis, K. (2010). Rape as a part of domestic violence: A qualitative analysis of case narratives and official reports. El Paso, TX: LFB Scholarly Pub.
Temple, J. R., Weston, R., Rodriguez, B. F., & Marshall, L. L. (2007). Differing effects of partner and nonpartner sexual assault on women’s mental health. Violence Against Women, 13(3), 285-297.
Testa, M., Hoffman, J. H., & Livingston, J. A. (2010). Alcohol and sexual risk behaviors as mediators of the sexual victimization– revictimization relationship. Journal of Consulting and Clinical Psychology, 78(2), 249.
Testa, M., VanZile-Tamsen, C., & Livingston, J. A. (2007). Prospective prediction of women’s sexual victimization by intimate and nonintimate male perpetrators. Journal of Consulting & Clinical Psychology, 75(1), 52-60.
Thakker, J. (2012). An integrated theory of sexual recidivism. Sexual Abuse in Australia and New Zealand, 4(1), 41-52.
Thomas, T. A., & Fremouw, W. (2009). Moderating variables of the sexual “victim to offender cycle” in males. Aggression and Violent Behavior, 14(5), 382-387.
Thompson, M., Sitterle, D., Clay, G., & Kingree, J. (2007). Reasons for not reporting victimizations to the police: Do they vary for physical and sexual incidents? Journal of American College Health, 55(5), 277-282.
Thompson, R. S., Bonomi, A. E., Anderson, M., Reid, R. J., Dimer, J. A., Carrell, D., & Rivara, F. P. (2006). Intimate partner violence: Prevalence, types, and chronicity in adult women. American Journal of Preventive Medicine, 30(6), 447-457.
Tiefenthaler, J., Farmer, A., & Sambira, A. (2005). Services and intimate partner violence in the United States: A county‐level analysis. Journal of Marriage and Family, 67(3), 565-578.
Tjaden, P., & Thoennes, N. (2000). Full report of the prevalence, incidence, and consequences of violence against women series: Research report. Washington DC: U.S. Department of Justice.
Todahl, J. L., & Walters, E. (2009). Universal screening and assessment for intimate partner violence: The IPV Screen and Assessment Tier (IPV-SAT) Model. Journal of Feminist Family Therapy, 21(4), 247-270.
Tomison, A. (2000). Exploring family violence: Links between child maltreatment and domestic violence. NCPC Issues, 13(Winter).
Tufts, K. A., Clements, P. T., & Wessell, J. (2010). When intimate partner violence against women and HIV collide: Challenges for healthcare assessment and intervention. Journal of Forensic Nursing, 6(2), 66-73.
Vagi, K. J., Rothman, E. F., Latzman, N. E., Tharp, A. T., Hall, D. M., & Breiding, M. J. (2013). Beyond correlates: A review of risk and protective factors for adolescent dating violence perpetration. Journal of Youth and Adolescence, 42(4), 633-649.
Van Bruggen, L. K., Runtz, M. G., & Kadlec, H. (2006). Sexual revictimization: The role of sexual self-esteem and dysfunctional sexual behaviors. Child Maltreatment, 11(2), 131-145.
Vatnar, S., & Bjørkly, S. (2008). An interactional perspective of intimate partner violence: An in-depth semi-structured interview of a representative sample of help-seeking women. Journal of Family Violence, 23(4), 265-279.
Wall, L. (2012). The many facets of shame in intimate partner sexual violence. Melbourne: Australian Institute of Family Studies.
Wangmann, J. (2011). Different types of intimate partner violence: An exploration of the literature (Issues Paper 22). Sydney: Australian Domestic& Family Violence Clearinghouse.
Watson, A. C., Corrigan, P., & Kosyluk, K. (2014). Challenging stigma. In P. Byrn & A. Rosen (Eds.), Early Intervention in Psychiatry (pp. 358-372). Oxford: John Wiley & Sons.
Wekerle, C., Bennett, T., & Francis, K. (2013). Child sexual abuse and adolescent sexuality. In D.S. Bromberg & T.W. O’Donohue, (Eds.), Handbook of child and adolescent sexuality: developmental and forensic psychology. Oxford: Academic Press.
White, J., McMullin, D., Swartout, K., Sechrist, S., & Gollehon, A. (2008). Violence in intimate relationships: A conceptual and empirical examination of sexual and physical aggression. Children & Youth Services Review, 30(3), 338-351.
White, J., & Smith, P. H. (2000). Developmental antecedents of violence against women: A longitudinal perspective. Rockville, MD: National Criminal Justice Reference Service.
Whitfield, C. L., Anda, R. F., Dube, S. R., & Felitti, V. J. (2003). Violent childhood experiences and the risk of intimate partner violence in adults: Assessment in a large health maintenance organization. Journal of Interpersonal Violence, 18(2), 166-185.
Wilcox, K. (2010). Connecting systems, protecting victims: Towards vertical coordination of Australia’s response to domestic and family violence. University of New South Wales Law Journal, 33, 1013.
Williamson, E. (2014). Reproductive coercion. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Wilson, K. S., Silberberg, M. R., Brown, A. J., & Yaggy, S. D. (2007). Health needs and barriers to healthcare of women who have experienced intimate partner violence. Journal of women’s health, 16(10), 1485-1498.
Winters, M., & Morgan, I. (2014). Cross-cultural perspectives on intimate partner sexual violence. In L. McOrmond Plummer, J.Y. Levy-Peck, P. Easteal (Eds.), Intimate partner sexual violence: A multidisciplinary guide to improving services and support for survivors of rape and abuse. London: Jessica Kingsley Publishers.
Winters, M. (2009). Making the connections: Advocating for survivors of intimate Partner Sexual Violence. In Washington Coalition of Sexual Assault Programs (Ed.), Intimate partner sexual violence: Sexual assault in the context of domestic violence. Olympia, WA: Washington Coalition of Sexual Assault Programs.
Wolff, N., Blitz, C. L., Shi, J., Bachman, R., & Siegel, J. A. (2006). Sexual violence inside prisons: Rates of victimization. Journal of Urban Health, 83(5), 835-848.
Wolff, N., Shi, J., & Siegel, J. A. (2009). Patterns of victimization among male and female inmates: Evidence of an enduring legacy. Violence and Victims, 24(4), 469-484.
Women With Disabilities Australia. (2013). Background paper – National symposium on violence against women and girls with disabilities. Tasmania: WWDA.
Woodward, C., Fischer, J., Najman, J., & Dunne, M. (2004). Selling sex in Queensland 2003: A study of prostitution in Queensland. Milton, QLD: Prostitution Licensing Authority.
Wright, M. O., Norton, D. L., & Matusek, J. A. (2010). Predicting verbal coercion following sexual refusal during a hookup: Diverging gender patterns. Sex Roles, 62(9-10), 647-660.
Yoshihama, M., & Horrocks, J. (2010). Risk of intimate partner violence: Role of childhood sexual abuse and sexual initiation in women in Japan. Children & Youth Services Review, 32(1), 28-37.
Young, B. J., & Furman, W. (2008). Interpersonal factors in the risk for sexual victimization and its recurrence during adolescence. Journal of Youth and Adolescence, 37(3), 297-309.
Zurbriggen, E. L., Gobin, R. L., & Freyd, J. J. (2010). Childhood emotional abuse predicts late adolescent sexual aggression perpetration and victimization. Journal of Aggression, Maltreatment & Trauma, 19(2), 204-223.
Zweig, J. M., & Burt, M. R. (2003). Effects of interactions among community agencies on legal system responses to domestic violence and sexual assault in STOP-funded communities. Criminal Justice Policy Review, 14(2), 249-272.
Zweig, J. M., & Burt, M. R. (2004). Impacts of agency coordination on nonprofit domestic violence and sexual assault programs in communities with STOP formula grant funding. Violence and Victims, 19(5), 613-624.
Zweig, J. M., & Burt, M. R. (2007). Predicting women’s perceptions of domestic violence and sexual assault agency helpfulness. Violence Against Women, 13(11), 1149-1178.
Zweig, J. M., Dank, M., Yahner, J., & Lachman, P. (2013). The rate of cyber dating abuse among teens and how it relates to other forms of teen dating violence. Journal of Youth and Adolescence, 42(7), 1063-1077.
Endnotes
-
In this paper, when we refer to “women” we mean individuals who (a) self-identify as women, and/or (b) have lived or embodied experience as women. At the same time, it is acknowledged that almost all research examined in this review does not critically engage with the concept of “woman” and thus the nature of the study samples may not reflect this definition. ↑
-
This paper examines IPSV and re-victimisation in relation to a wide range of sub-populations including Aboriginal and Torre Strait Islander women, women from culturally and linguistically diverse backgrounds, women with low socio-economic status, women who work in the sex industry, lesbian and bisexual women, people who are transgender (inclusive of trans-men who experienced violence at a time when they identified as female and/ or experienced violence in a context where they were read by others as female), women who are alcohol or other drug dependent, women who are HIV positive, women with physical or intellectual disability, women who experience severe mental illness, women who are incarcerated and women who live in rural areas. ↑
-
Adolescence is understood in this review to mean the period after the onset of puberty and prior to adulthood. ↑
-
Marriage in these studies was limited to religious and secular marriages involving opposite sex partners. ↑
-
It should be acknowledged that, while essential for the representation of data in a literature review format, the separation of groups in this manner does a disservice to the complexity of lived experience. Discrimination and stigma are often more acute for women who identify as part of multiple groups (e.g. a woman who is homeless, HIV positive, works in the sex industry and injects drugs is likely to experience more discrimination and stigma when compared to a woman who is part of only one of these sub- populations). These highly marginalised women are likely to experience discrimination and stigma from both the general community and service providers, with the criminal aspect of certain dimensions of their lives likely to further compound the challenges of help-seeking in relation to experiences of victimisation. ↑
-
As the research outlined below is predominately from the US, it relates to migrant communities. In the Australian context, the category of CALD communities would include a wider range of women, including women who are refugees and those who live in certain cultural and/or religious communities. ↑
-
This section is limited to a discussion of women with physical and intellectual disability. Papers on women with psychiatric disability were placed in a separate category, namely “Women who experience severe mental illness”. ↑
-
Our Watch was founded under the First Action Plan of the National Plan to Reduce Violence against Women and their Children as Australia’s national organisation for preventing violence against women and their children. ↑
-
In light of the Royal Commission into Institutional Child Abuse in Australia, there has been increasing focus on programs which aim to prevent CSA. These programs, while potentially contributing to the reduction in re- victimisation, were outside the scope of this review and thus are unable to be discussed in this section. ↑
-
Intimate partner sexual assault is captured under the category of severe sexual coercion in the CTS2. ↑