
RESEARCH REPORT RECOVER – Reconnecting mothers and children after family violence: The child–parent psychotherapy pilot
Read the PDF version of the report
This report addresses work covered in the ANROWS research project RF.19.02 “RECOVER – Reconnecting mothers and children after violence: The child-parent psychotherapy pilot”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Plan Outcome 4 – Services meet the needs of women and their children experiencing violence.
Suggested citation:
Hooker, L., Toone, E., Wendt, S., Taft, A., & Humphreys, C. (2021). RECOVER – Reconnecting mothers and children after family violence: The child–parent psychotherapy pilot (Research report, 05). ANROWS.



Judith Lumley Centre, La Trobe University
Plenty Rd & Kingsbury Dr, Bundoora VIC
La Trobe Rural Health School, La Trobe University
Edwards Rd, Flora Hill VIC
Author acknowledgement
Thank you to all children, mothers, therapists and organisations who participated in RECOVER. Thank you to our industry partner, Berry Street, and Marg Hamley for early championing of the project, and Sally Watson (South Australian Branch, Australian Association for Infant Mental Health), Julie Larrieu (Tulane University), Chandra Ghosh Ippen (University of California) and Kjerstin Almqvist (Karlstad University) for sharing their knowledge. Thank you also to Dr Jess Ison for research assistance and support, including preparation of this document. We also extend our gratitude to our steering committee: Tom Bowerman (Berry Street), Vibhay Raykar (Goulburn Valley Health), Anita Morris (Department of Families, Fairness and Housing, Victoria) and Elizabeth Westrupp (Deakin University).
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732) and Lifeline (13 11 14).
Contents
Implications and recommendations for policymakers
Implications and guidance for practitioners and service providers
Part 1: State of knowledge review
1. How acceptable and feasible is CPP to the Australian context?
2. Do CPP therapists-in-training adhere to CPP model fidelity?
3. How effective is treatment by CPP therapists-in-training during the study?
Implications and recommendations for policymakers
Implications and guidance for practitioners and service providers
APPENDIX A: Keyword search terms and grey literature sites searched
APPENDIX B: Ovid MEDLINE search strategy
APPENDIX C: Grey literature search: Relevant websites
APPENDIX E: Summary table of included studies
APPENDIX F: Summary table of interventions identified
APPENDIX G: Intervention descriptions
Group work: Psychoeducational, psychotherapeutic
Psychotherapies: Individual, parent, dyadic
APPENDIX H: Maternal interview schedule
Key definitions
Concept
Definition
Cisgender
A person who identifies as the gender they were assigned at birth.
Dyad
A grouping of two participants. In this report we refer to a dyad as the caregiver and child receiving child–parent psychotherapy (CPP).
Dyadic interventions
Dyadic interventions (also referred to as mother–child, parent–child, child–parent, relational, infant–parent therapy) are a model of therapeutic or mental health and wellbeing care that engage both child and parent simultaneously and focus on their relationship as target for change.
Family violence
Family violence (FV) is defined by the Victorian Department of Families, Fairness and Housing (2018) as any violent, threatening, coercive or controlling behaviour that occurs in current or past family, domestic or intimate relationships. This includes not only physical injury but direct or indirect threats, sexual assault, emotional and psychological torment, economic control, damage to property, social isolation and any behaviour which causes a person to live in fear.
Intimate partner violence
Intimate partner violence (IPV) is defined as behaviour by a partner or ex-partner that includes physical, sexual and/or psychological abuse and controlling behaviours.
Practice champions
Leadership figures within an organisation who are skilled in a particular intervention and passionate about using evidence to inform practice. RECOVER practice champions supported the implementation of CPP in the clinical settings and reported back regularly to the research team.
Shadow pandemic
The increase in violence against women, especially IPV, since the outbreak of the COVID-19 pandemic.
Therapeutic readiness
Therapeutic readiness is a term initially coined in relation to the application of child psychiatry within community settings (Despert, 1949). It considers factors internal and external to the child and caregivers that are conducive to treatment engagement and success. CPP provides a foundational framework that equips clinicians to determine therapeutic readiness, considering child and family strengths and contextual risks (Lieberman et al., 2015, p. 265).
Trauma- and violence-informed care
Incorporates an understanding of the effects of trauma while accounting for intersecting impacts of systemic and interpersonal violence and structural inequalities (Wathen et al., 2021).
Executive summary
Background
Family violence, especially intimate partner violence (IPV), is prevalent in Australia (Australian Institute of Health and Welfare [AIHW], 2019). IPV is defined as behaviour by a partner or ex-partner that includes physical, sexual and/or psychological abuse and controlling behaviours (World Health Organization [WHO], 2013a). While people of all genders and sexualities can experience IPV, the focus of the RECOVER project is on IPV perpetrated by men in cisgender heterosexual couples and the harm it causes mothers
and children.
Globally, up to one in three women have experienced IPV in their lifetime. Higher rates of IPV are noted in low- and middle-income countries compared to high-income countries like Australia (WHO, 2021). In Australia, one in six women (and one in 17 men) report an experience of partner violence since the age of 15 years (Australian Bureau of Statistics [ABS], 2017). Women’s mental health, parenting and relationships with their children can be profoundly impacted by partner violence (Hooker, Kaspiew, & Taft, 2016; Humphreys et al., 2006; Trevillion et al., 2012). Couple relationships are complex and separations stressful, particularly when there has been violence in family relationships (Jones & Bunston, 2012). Separations after IPV are particularly fraught and often complicated by ongoing patterns of coercive control, harassment and physical dangers, including fatality risks to women and children (AIHW, 2019).
Twenty per cent of young Australian children experience poor mental health (AIHW, 2020), but less than 1 per cent of under four-year-olds receive treatment (Segal et al., 2018a).
Children’s mental health, wellbeing and the relationships that they depend upon for their development and recovery are all impacted by IPV (Humphreys et al., 2018; James-Hanman & Holt, 2021; Morris et al., 2015). These harms to health and wellbeing are extensive (Fitzpatrick et al., 2020; Trevillion et al., 2012; Vu et al., 2016), hampering the recovery of the mother–child relationship (Buchanan & Humphreys, 2021; Humphreys et al., 2006). Less is known about the impact of IPV use on father–child relationships, although these relationships too may be distorted (Mohaupt et al., 2020; Stover et al., 2020). Of all age groups, very young children are disproportionately affected by traumatic events and the most developmentally vulnerable to IPV-related physical dangers and relational harms (Lieberman, Chu et al., 2011; Lyons-Ruth et al., 2017). While the harms to older children and adolescents from family violence are well known (Evans et al., 2008; Kitzmann et al., 2003; Vu et al., 2016), the extent of burden to pre-school-aged children’s mental health from family violence is less clear (Howell et al., 2011; Orr et al., 2020). Twenty per cent of young Australian children experience poor mental health (AIHW, 2020, p. 87), but less than 1 per cent of under four-year-olds receive treatment (Segal et al., 2018a). Programs that include mothers and children together (dyadic interventions) show significant benefits (Anderson & van Ee, 2018). Child–parent psychotherapy (CPP) is an evidence-based dyadic intervention initially designed for young children and their mothers affected by IPV to strengthen their relationship and positively impact on their mental health (Lieberman et al., 2015).
Across several randomised controlled trials (RCTs), CPP has been shown to reduce child behavioural problems and maternal and child trauma and mental health symptoms (Cicchetti et al., 2000; Cicchetti et al., 2011; Ghosh Ippen et al., 2011; Lieberman, Van Horn & Ghosh Ippen, 2005; Lieberman et al., 2006), and improve attachment between mothers and children (Cicchetti et al., 1999; Toth 2002, 2006). CPP improves mental health outcomes in children and mothers simultaneously and treatment effects are maintained over time (Lieberman et al., 2015).
The state of knowledge review completed for this report identified very few evidence-based preventive treatments for mothers and children affected by IPV, especially in Australia. The present report identifies the need for suitable treatment for women and children exposed to IPV and reports on a pilot evaluation of CPP for this population in Australia.
Project aims and methodology
Aims
To test the feasibility of implementing CPP into the Australian context for children and their mothers affected by IPV.
Research questions:
- How acceptable and feasible is CPP to the Australian context?
- Do therapists adhere to CPP model fidelity?
- How effective is CPP treatment at improving maternal and child health and wellbeing outcomes?
About the intervention
Child–parent psychotherapy is a relationship-focused treatment for parents and young children who have experienced trauma (Lieberman et al., 2015). CPP originated in the psychoanalytic tradition of infant–parent psychotherapy and was designed for mother–child dyads affected by IPV, integrating a lens of social justice (Cerulli et al., 2021; Lieberman, 2004; Lieberman et al., 2015). Although CPP has since found application in other trauma populations, in this project, exposure to IPV is the trauma of focus. The goal of CPP is to support and strengthen the parent–child relationship, which acts as the vehicle to restore the child’s sense of safety, attachment, and social and emotional wellbeing. CPP is a manualised, flexible intervention, where the goals of treatment are co-designed with mothers and children. Treatment is offered by qualified therapists, weekly for up to 12 months or longer if needed and includes parent-and-child play sessions and collateral, parent-only reflective sessions. Through a range of modalities such as developmental guidance, insight-oriented interpretation and advocacy, treatment aims to help children and parents make sense of, and recover from, trauma (Lieberman et al., 2015). Opportunities for change are harnessed within spontaneous child–parent interactions. Parents are helped to understand the impact of trauma on their parenting and to confidently respond to their child’s behaviour as a form of communication (Lieberman et al., 2015; Lieberman et al., 2019). A detailed explanation of the RECOVER study background and methodology has been published elsewhere (Hooker et al., 2019).
Study sites and recruitment
Eleven community-based, clinical sites including specialist family violence services (with clinical services for children), child and adolescent mental health services (CAMHS), one enhanced maternal and child health centre with a multidisciplinary team and co-located infant mental health specialist, and one private perinatal psychiatry clinic participated in RECOVER and actively recruited suitable mother–child dyads for the study. These included four urban and seven rural/regional sites. Recruitment was staggered as new sites came on board and occurred over two waves – RECOVER 1 in 2018 and RECOVER 2 in 2019–20, with the welcome addition of ANROWS funding in the form of legacy funds from the former Luke Batty Foundation.
We looked for mother–child dyads using the following inclusion criteria:
- pre-school-aged child (3 to 5 years)
- English-speaking biological mothers
- recent exposure to IPV (past 12 months) and with advocacy support already received
- clinical signs of trauma (e.g. child presenting with emotional or behavioural issues/impaired mother–child interaction based on clinical assessment)
- therapeutic readiness: post-crisis situation, or not living with the person using violence.
Mixed methods evaluation
Program evaluation involved mixed methods, including:
- semi-structured interviews with CPP therapists, service managers and eligible women. Implementation theory (May & Finch, 2009) guided interview questions and data analysis
- therapists completed fidelity logbooks and documented the dose/number of treatment sessions completed
- maternal survey data and video-recorded free play between mothers and children before (T1), during treatment (T2) and after treatment (T3).
Key findings
Eighteen dyads consented to and received treatment, 15 completed the baseline (T1) survey and 10 mothers completed at least two surveys at two time points, T1 and either T2 or T3. The average age of mothers was 34 years, with children around four years of age. Forty per cent of women who completed the baseline survey were separated from their partners, over half of all women were not working in a paid job (53%), and 60% were on a pension. No women were Aboriginal or Torres Strait Islander, and all were Australian born. Two women were from rural locations and the remaining 13 were city based.
Therapists offered 293 CPP treatment sessions to 15 dyads during the project. The median number of sessions across all dyads was 23 (range 5 to 50). Treatment time was approximately six months. Forty in-depth interviews were completed, including 28 process and impact interviews with therapists (n=15) and managers (n=13), and 12 interviews with women completed after treatment.
She’s just a different child now.
(Mother, 3)
How acceptable and feasible is CPP to the Australian context?
CPP appears feasible for this population of mothers and children affected by IPV under certain conditions, despite the implementation barriers outlined below. The intervention was highly acceptable to study participants. All therapists reported that they found the CPP training enjoyable, and that the intervention suited their clinical needs; they noted swift and satisfying changes in their clients. In line with the concept of victims’ and survivors’ stages of change or readiness (Chang et al., 2006), despite seeking help, some women required alternative supports (e.g. acute mental health treatment) before the intensive dyadic treatment commenced. Managers reported that they felt pleased to be able to offer an evidence-based intervention for this under-serviced population. Therapists reported that children were often drivers of change in the dyadic relationship. The research highlighted that a range of systemic structures and processes need to be in place to enable CPP to occur.
Implementation enablers:
- CPP leaders within services that act as practice champions (or leaders) assisting implementation processes (e.g. recruitment, collaborations)
- therapists with family violence practice knowledge
- therapists with prior clinical experience, especially with young children
- organisations with established therapeutic services within their family violence service
- clear organisational clinical governance, and supportive policy and procedures
- systems that both support therapists and identify victims and survivors.
Implementation barriers:
- coincided with a time of escalating service delivery and service reform demands
- COVID-19 pandemic and impacts on families and clinical services
- limited organisational and workforce family violence knowledge and/or practice skills
- systems and practices that prioritise older children’s mental health needs
- poor collaborative links with family violence networks/referral options (especially in rural areas)
- crisis-driven systems, no time and/or resources to offer early intervention
- restricted access to qualified CPP workforce.
Do CPP therapists-in-training adhere to CPP model fidelity?
In total, eight therapists who provided CPP in the project completed fidelity logbooks for each dyad and recorded their perceived adherence to CPP goals at the completion of each dyadic session. Greater adherence to the model was reported in conveying a sense of hope and aid in developing a relationship with the dyad. Enhancement of safety in therapy was also high. Areas lacking in focus were client care coordination, supporting the child’s relationship with others and helping the dyad put the trauma into perspective. Urban sites reported greater fidelity and adherence to all CPP objectives compared to rural and small services.
How effective is CPP treatment delivered by CPP therapists-in-training during the study?
In the original Lieberman et. al trial (2005), CPP treatment comprised an average of 32 sessions completed by therapists experienced in CPP and delivered to 75 dyads. In our RECOVER study, therapists were still learning the CPP model and provided an average of 23 sessions. Ten RECOVER cases completed T1 and either T2 or T3 surveys and were used in the statistical analysis. Four dyad video interactions with complete data were double-coded and analysed.
In this study, all women reported substantial IPV from a male perpetrator, which reduced significantly after treatment (T3; p<0.005).
Differences across many study outcomes showed no statistically significant effect of treatment, however trends in positive directions were noted across most outcomes. These results are not surprising considering the small sample which limits any conclusions of causation and the effectiveness of CPP in this study. We found no statistically significant change in maternal emotional health, reflective functioning and parenting due to CPP. In addition, no significant changes were seen across child functioning and trauma symptoms, or mother–child attachment.
Two important outcome measures did change significantly, including parental warmth, which increased after treatment (p<0.028), and improved child emotions and behaviours (p<0.005).
I think the best part is … the joy of seeing children and their primary caregiver start to heal with each other and start to feel safe to – to express things to each other that previously they hadn’t been able to – or they had been communicating to each other in a way that had left either party feeling very isolated and alone … It is such a privilege to witness that. (Therapist 6)
Summary
CPP has been shown in several previous RCTs to be an effective dyadic treatment model for mothers and children exposed to IPV (Lieberman, Van Horn & Ghosh Ippen, 2005; Lieberman et al., 2006). The RECOVER project tests the feasibility of implementing this model in an Australian service setting for mother–child dyads affected by IPV, delivered by CPP therapists-in-training. We found that CPP is acceptable and feasible for this population and can be implemented into the Australian setting, in locations with established family violence system partnerships, service capacity to prioritise mental health and wellbeing responses for very young children, and strong clinical governance structures.
Although the intervention was delivered by CPP therapists-in-training and our sample size was too small to conclude efficacy, positive changes were found in child behaviour and parental warmth and reinforced by qualitative reports from women and therapists. Findings also show that women experienced less IPV post-intervention. This may be a natural reduction in abuse over time – from crisis to a more stable environment – rather than a true treatment effect, however, further research to explore this outcome with a larger sample is required.
With the high prevalence of IPV and the contributing “shadow pandemic” arising from the public health response to COVID-19 (Pfitzner et al., 2020) there is an overwhelming demand for evidence-based, relational therapy like CPP. An improved trauma- and violence-informed child mental health workforce is needed (Wathen et al., 2021). Systems reforms facilitating better non-government organisation and public child mental health partnerships and equity of mental health service delivery across the age range are also required for CPP to be expanded in CAMHS for this population of women and children.
I think it’s quite a pragmatic approach … It’s a broad model, it encompasses lots of different therapeutic approaches. It’s not a very limited focus, I think it sees the bigger picture. CPP takes into account the child, the parent, the systems and that’s what really helps. (Manager 6)
CPP is a feasible model for expansion for this population of children and women affected by IPV in Australia. This is especially so within the current family violence and mental health service system reform contexts at state and national levels. The model is also adaptable for families from conception through to children aged five who have experienced a wide range of family stresses and trauma and is in fact already being expanded to Aboriginal and Torres Strait Islander populations (Toone et al., 2021), perinatal child protection populations (Kong, 2021), broader populations within rural CAMHS (Raykar et al., 2021) and for use via telehealth in Australia (Fogarty et al., 2021). CPP can be delivered to children in their relationships with parents or caregivers who have used violence within relationships, with clear guidelines for assessing therapeutic readiness of families (Lieberman et al., 2015). CPP for IPV-exposed dyads is acceptable to clients and organisations, can be delivered in under six months, and will be increasingly available as more Australian therapists across non-government organisations; perinatal, child and adolescent mental health services; and private practitioners are trained in CPP and gain experience in skilled delivery. The CPP model of training and model of treatment delivery can equip services to better respond to young children and their caregiving relationships after violence and trauma, for the betterment of their lives and for future generations.
Implications and recommendations for policymakers
Implications
- Very young children’s mental health and wellbeing can be particularly impacted by IPV trauma, alongside those of their affected mothers.
- The mental health care needs of very young children are often overlooked in Australian service systems, as are the needs of IPV affected mother–child dyads.
- The way to restore young children’s mental health after IPV is within their safe relationships (as a first step this is often, but not always, with their mother).
- CPP is an evidence-based model for this population that is acceptable and increasingly feasible across settings within Australia.
- The CPP model of care also provides the theory, skills training and reflective supervision framework to build and sustain a mental health and wellbeing workforce for young children and parents/caregivers impacted by IPV trauma.
Recommendations
- Promote equity of mental health service delivery for children across the age range, to ensure responsive care is available for all children from earliest life.
- Invest in and expand the trauma- and violence-informed child mental health workforce that is growing in Australia, based on the CPP training and workforce development model.
- Develop a national trauma- and violence-informed child mental health and wellbeing practice framework, to guide safe engagement for children within all important caregiving relationships after IPV. This should be inclusive of both victim and survivor and perpetrator co-parents when safe, and across caregiver genders and sexualities.
Implications and guidance for practitioners and service providers
RECOVER has made considerable service impacts across project sites that can guide future care. RECOVER has:
- reinforced the value of tailoring services for IPV-exposed mothers and very young children previously missing out on care and/or identified service gaps for this age group
- highlighted the need to identify safe windows of therapeutic readiness for change with families
- identified that rural therapists/managers with less experience need more support to implement CPP
- operationalised trauma history assessment for children and caregivers referred to the service to better inform and tailor treatment plans for children and families
- facilitated the introduction of family violence screening at triage and realisation that family violence is prevalent among the clinical population
- facilitated partnerships between child mental health and family violence services
- highlighted the need for and value of building a
trauma- and violence-informed child mental health/therapeutic workforce - facilitated the training of further cohorts of CPP-qualified clinicians who are in turn now offering CPP across Victoria and South Australia (to Aboriginal and Torres Strait Islander families, migrant and refugee families, and some parents – mothers, fathers, caregivers – who have used violence in their relationships), as well as delivering CPP via telehealth
- developed a national community of practice, practice activities and knowledge translation.
Introduction
This report outlines the findings of the RECOVER project (“Reconnecting mothers and children after family violence: The child–parent psychotherapy pilot”). The study aimed to implement and evaluate the child–parent psychotherapy (CPP) model of care (Lieberman et al., 2015) for Australian women and children (<5 years) affected by intimate partner violence (IPV).
Intimate partner violence
IPV is defined as behaviour by a partner or ex-partner that includes physical, sexual and/or psychological abuse and controlling behaviours (World Health Organization [WHO], 2013a). Up to one in three women globally have experienced IPV in their lifetime (WHO, 2021), compared to one in six women in Australia (Australian Bureau of Statistics [ABS], 2017). One in 17 Australian men report experiencing IPV since the age of 15 years (ABS, 2017).
While people of all genders and sexualities can experience IPV, the focus of the RECOVER project is on IPV perpetrated by men in cisgender heterosexual couples and the harm it causes mothers and children – and in particular, fathers or other intimate partners/ex-partners as perpetrators of the violence, and victims and survivors as mothers (protective parent/caregiver) and children. All women can be at risk of IPV, and women from marginalised backgrounds can face heightened risk – for example, women with disability, First Nations women and women from migrant and refugee backgrounds (ABS, 2017). Partner violence is more prevalent among women of childbearing age (WHO, 2021), especially those with infants and young children; consequently, the violence impacts on both mothers and children simultaneously (WHO, 2013a).
Our study cohort replicates the population targeted in the original CPP trial (Lieberman, Van Horn et al., 2005). We note that future studies could expand to include diverse genders and sexualities, male victims and survivors, and parents and caregivers who are not the biological mother to reflect the expanding breadth of CPP practice (Iwaoka-Scott et al., 2015; Larrieu, 2018; Lieberman et al., 2019).
Effects on children
Children can be impacted by IPV in a range of ways depending on their age and stage of development. The impact and resilience of children depends on the severity and chronicity of IPV experienced, other adverse experiences in the home, and the availability and responsivity of caregivers (Fogarty, Giallo et al., 2019). Child abuse, including sexual abuse, is also associated with IPV (Bidarra et al., 2016; Holt et al., 2008).
Persistent fear and anxiety in children’s lives results in activation of prolonged stress responses, with detrimental structural and physiological changes in the developing brain (Cicchetti et al., 2011; National Scientific Council on the Developing Child, 2010). There is strong evidence outlining frequent externalising behavioural problems and post-traumatic stress, depression and anxiety in children due to IPV (Vu et al., 2016). Children’s mental and physical health is impacted by exposure to violence in the home (Orr et al., 2020), with up to 20 per cent of young children suffering from poor mental health (Australian Institute of Health and Welfare [AIHW], 2020; Lyons-Ruth et al., 2017; Westrupp et al., 2015). Consequently, children exposed to IPV may suffer a range of serious and ongoing socio-behavioural, physical, academic and mental health problems, including re-victimisation and perpetration of violence in their adulthood (Chan & Yeung, 2009; Felitti et al., 1998; Holt et al., 2008; Vu et al., 2016).
Infancy and early childhood are critically important developmental periods when children’s brains are particularly vulnerable to the harms of IPV. Recent Australian longitudinal evidence (in a sample of 615 mother–child dyads) shows that any IPV exposure from infancy to 10 years was associated with poorer child health outcomes (Gartland et al., 2021). Almost half of all children with mental health and language disorders had been exposed to IPV (Conway et al., 2020; Gartland et al., 2021).
Children living in separated families are often left to navigate complex relationships with other caregivers, including with fathers or other caregivers, on their own while they are still recovering from the impacts of IPV trauma (Morris et al., 2015). Children’s experiences of IPV and their relationships are often not discussed and the consequential harms to children often go unrecognised (Humphreys et al., 2011; Lamb et al., 2018; Morris et al., 2018).
Harms to women and the mother–child relationship
The maternal morbidity and mortality associated with IPV is well documented and understood. Harmful effects include significant mental health issues, physical illness and somatoform disorders, reproductive health problems, substance abuse disorders, chronic illness and disability (WHO, 2013a).
Becoming a parent is a stressful developmental phase (Lieberman, Ghosh Ippen et al., 2015) and can be made significantly harder in the context of IPV trauma. Women’s agency and confidence as a mother may be directly undermined by her partner through tactics of coercive control, impacting her experience of motherhood and the quality of mother–child relationships (Buchanan & Humphreys, 2021; Hooker, Samaraweera, et al., 2016; Katz, 2019).
The impacts of IPV on social isolation, including the mental health impacts of stress and trauma, may mean that mothers are understandably hampered in their capacity to sensitively and consistently respond to their children at times when their children are presenting with challenging behavioural symptoms of traumatic stress (Bancroft et al., 2012; Holt et al., 2008; Isobe et al., 2020). Along with the practical insults of IPV on mother–child relationships (Hooker, Samaraweera et al., 2016), mothers and children can also begin to misunderstand each other “as the child’s traumatic expectations interact with the (traumatic) expectations of the parents” (Lieberman et al., 2015, p. 21).
Family separations after IPV are also particularly fraught for women and children and often complicated by ongoing patterns of coercive control and physical dangers, including fatality risks to women and children (AIHW, 2019). Therefore, even when protective steps are taken by mothers, ongoing psychosocial stressors from men’s use of violence may continue to undermine mother–child relational recovery (Humphreys et al., 2018).
Treatment and support for women and children
Evidence reviews exploring treatment for victims and survivors of trauma and abuse (Barlow et al., 2015; Gillies et al., 2016; Howarth et al., 2016) have identified a lack of evidence-based interventions focused on IPV and the parent–child relationship. Quality parent–child or dyadic therapies favour interventions delivered to the (non-abusive) parent and child, rather than individual treatments (Graham-Bermann et al., 2007; Howarth et al., 2016).
One such intervention is CPP, an evidence-based intervention that was initially designed for pre-school-aged children and mothers affected by IPV. The intervention is adaptable across different populations, including a range of family constellations and culturally diverse populations, and across the entire 0- to 5-year-old age range (Lieberman et al., 2019; Shafiet al., 2019). CPP has been extensively evaluated across many randomised controlled trials (RCTs), with different traumatised parent–infant populations, including children with mothers experiencing domestic violence and depression, and children with a history of maltreatment/poor attachment (Ghosh Ippen et al., 2011; Lieberman, Van Horn et al., 2005; Lieberman et al., 2006; Lieberman et al., 2015). Findings show improvements in maternal and child trauma symptoms and mental health, child behaviour and the parent–child relationship (Hagan et al., 2017; Lieberman et al., 2015). Sustained benefits of CPP include decreased child behavioural problems and maternal distress to six months (Lieberman et al., 2006), and decreased parenting stress and attachment security to one year (Cicchetti et al., 2011; Stronach et al., 2013). In recent evidence from Guild et al. (2021), CPP participation of depressed mothers and infants enhanced maternal warmth and child problem behaviour six years post-intervention.
CPP is built on a psychodynamic model, the hallmark of which is the premise that learning and relational change can only occur within the context of safe relationships (e.g. the therapist–supervisor relationship, the therapist–mother relationship and the mother–child relationship). CPP is a flexible and non-didactic relational model of learning and treatment that is therefore inherently resource and time intensive. Questions on the accessibility and scalability of CPP have therefore been raised (Alto et al., 2021). Interestingly however, rates of attrition for CPP do not vary, irrespective of study population and/or socioeconomic status. This suggests intervention length is not a barrier to participation.
Alto et al. (2021) have reviewed the literature of other parenting and attachment interventions and have found that many studies do not provide attrition information, and those that do provide comparable attrition rates whether interventions are brief or longer term. There are mixed results about whether briefer dyadic or parenting intervention models can achieve comparable outcomes (Mountain et al., 2017; Shafi et al., 2019).
What is clear is that there is an urgent need for early intervention and secondary prevention programs for mothers and young children to arrest the detrimental consequences of IPV. Maternal functioning with a reduction in trauma symptoms is currently considered one of the best predictors of child outcomes (Graham-Bermann et al., 2011; McFarlane et al., 2014). In securely attached relationships, where the emotional and physical needs of children are consistently met, fewer child behavioural, language and school readiness problems are seen, compared with insecure mother–child attachments (Carpenter & Stacks, 2009; Guild et al., 2021). Children’s resilience to the negative impacts of IPV is enhanced when mothers’ health and wellbeing are supported (Fogarty, Giallo et al., 2019; Fogarty, Woolhouse et al., 2019). Interventions that jointly address maternal and child symptoms and their relationship with each other may have added benefit and arrest intergenerational trauma and abuse (Lieberman et al., 2015).
Study rationale
Interventions for women and children living with violence in Australia
Despite the clear evidence of harm, less than 1 per cent of all Australian children under five years receive formal mental health treatment (Segal et al., 2018). Australia’s mental health system does not have a focus on prevention and early intervention, with most people treated long after the onset of their symptoms (Productivity Commission, 2020). The mental health care needs of infants and young children are poorly identified, and the treatment that is offered frequently arises in crisis situations and/or is directed to older children and youths. Recent state and national inquiries and commissions have identified substantial service gaps or the “missing middle” (McGorry, 2021) between primary care (GP) and tertiary hospital/mental health bed-based services for all clients with mental health problems. This includes a lack of focus on the early years and young children needing more mental health support (Productivity Commission, 2020; State of Victoria, 2021). Consistent and comprehensive mental health services for those living in rural and regional areas are particularly lacking (Productivity Commission, 2020; State of Victoria, 2019, 2021). Rural areas also face the additional burden of fewer experienced mental health care professionals (Productivity Commission, 2020).
Modifiable risk factors for adult mental illness (like IPV) are prevalent and occur at the earliest stages of life (Guy et al., 2016; Orr et al., 2020). Challenges include the identification of young children as victims and survivors of IPV and subsequent mental health problems (Bunston et al., 2017), and service gaps and capacity in mental health systems. In addition, very few Australian individual, group or dyadic programs have been rigorously evaluated, identifying the benefits of interventions for abused women and children (Campo, 2015; Hooker et al., 2019). Suboptimal mental health care has been reported by women seeking mental health care after IPV (Marsden et al., 2020). Australian services that deliver IPV support for non-abusive parent and child populations, such as community-based individual counselling, group work and parenting programs, are often siloed, subject to the uncertainty of poor organisational clinical governance and government funding cycles, and not evidence-based (Campo, 2015; Hooker, Kaspiew & Taft, 2016).
Therefore, the RECOVER project outlined in this report sought to pilot an established trauma- and violence-informed relational intervention with strong evidence, the CPP model of care, across rural and urban settings. Although contemporary CPP can be provided across the 0- to 5-year-old age range, to a wide range of family contexts and caregiver genders and sexualities, to address a range of traumatic experiences, the focus of this project was to test the acceptability and feasibility of CPP for pre-school-aged children and mothers affected by IPV in an Australian context, drawing on the original CPP trial (Lieberman, Van Horn et al., 2005).
Research questions
The RECOVER project addressed the following research questions on the feasibility of CPP for a population of women and children affected by IPV.
1. How acceptable and feasible is CPP to the Australian context?
- How acceptable is the intervention for women and service providers?
- What are the barriers and facilitators to the implementation of the CPP model into services?
- What (if any) are the dyad recruitment and retention issues encountered?
- Are there process and impact differences between service providers across sites?
2. Do CPP therapists-in-training adhere to CPP model fidelity?
3. How effective is treatment delivered by CPP therapists-in-training during the study?
- Do women’s and children’s trauma symptoms differ before and after treatment?
- Does treatment improve the mother–child relationship?
Intervention description
Child–parent psychotherapy
CPP is an intervention for parents and young children who have experienced some form of trauma. Integrating theories of psychoanalysis, attachment theory and developmental psychology, CPP was developed to support children and their mothers affected by family violence. In addition to considering psychodynamic and relational processes, it privileges safety and the socioeconomic and cultural context of the family. Delivered in hour-long weekly sessions by specially trained therapists, treatment time can extend to 12 months, depending on family need (Lieberman et al., 2015; Lieberman et al., 2019). A CPP intervention comprises three phases:
- foundation phase: assessment and engagement sessions (4 to 6 weeks)
- core intervention phase (length varies depending on the need; approx. 20 to 32 weeks)
- recapitulation and termination phase: promoting sustainability (<8 weeks; Lieberman et al., 2015).
Family strengths and context, trauma type and developmental impact, and the child’s age all inform the structure and length of the CPP sessions. Therapy for infants includes actively engaging them in sessions and reflecting together with mothers to understand their infants’ expressions of distress and attempts to connect. Play-based therapy facilitates communication for toddlers and pre-school-aged children with their mothers using a range of objects, toys, and stories. Child-friendly spaces are provided alongside adult-friendly collateral or parent sessions for mothers (Lieberman, 2004; Lieberman, Chu et al., 2011; Lieberman et al., 2015; Lieberman, et al., 2020).
How child–parent psychotherapy works
CPP targets the mother–child relationship as the central change agent to restore the child’s health and development (Chu et al., 2021; Lieberman et al., 2015). Relationships may be seen as a “web of jointly constructed meanings” based on each participant’s perceptions of and actions toward one another (Lieberman, 2004; Lieberman et al. 2015). When mothers and children are exposed to IPV and overwhelmed by frightening experiences, their relationship suffers (Jones & Bunston, 2012; Levendosky et al., 2012). They can misunderstand each other’s intentions and actions and find it much more difficult to connect in a safe and rewarding way (Lieberman et al. 2015; Overbeek et al., 2019). The focus of CPP is therefore to change these misunderstandings so that relationship repair can occur, and mothers and children can return to safe and more rewarding patterns of relating (Bernstein et al., 2019; Lieberman et. al., 2015).
Therapists take time to get to know mothers and children, including their family’s strengths and cultural values. During this “foundation phase”, the therapist will map the history, nature and effects of violence and trauma on the child, mother and their relationship (Lieberman et. al., 2015, p. 55). In so doing, the mother and child will get an initial sense of how the therapist will work and decide whether they feel comfortable in proceeding. Treatment goals and plans are co-created using the CPP “Triangle of Explanations” (Figure 1), which links past trauma experiences. The triangle is developed with the mother and then, with her permission, communicated in an age-appropriate manner to the child directly.
Figure 1: The CPP Triangle of Explanations

An example of a triangle of explanation communicated to the child might be:
You saw mummy and daddy fighting. Daddy hurt mummy, and then he was gone [trauma/experience]. Since then you can’t sleep at night and don’t want to leave mummy’s side [behaviour]. You’ve been missing daddy while he is getting help with his angry feelings. And worried that you and your mummy will be safe and okay. Mummy and I will meet with you each week to talk and play to help you with big feelings so you can feel better inside [treatment plan].
Explaining the triangle to children in the above way ushers in the beginning of the core phase of CPP. Toddlers and pre-school-aged children often are able to add to the triangle or ask questions about events that have been troubling them, once they see that the space is for them. Children see their mother and their therapist as examples of adults working safely together, and even though frightening feelings may come up, no one gets hurt. Moments like this are often transformative for mothers too, as they may come to see the child’s behaviour as an attempt to communicate when words are not possible (Fraiberg et al., 1975; Lieberman & Van Horn, 2011; Lieberman et al., 2015; Lieberman et al., 2019).
Collateral sessions with the parent alone consider the impact that IPV (e.g. earlier maternal childhood traumas or “ghosts in the nursery”; Fraiberg et al., 1975) may have on the mother’s ability to parent (Lieberman, Padron et al., 2005). For example, a mother may find herself becoming frightened of her toddler’s loud tantrums and unable to set a limit. This may be an understandable response if she, for instance, has had an experience of being hurt by someone in the context of raised voices. The mother’s trauma response would be normalised and psychoeducation about normal toddler development provided. Exacerbating external stressors from IPV, like housing, poverty or court demands, would be considered. The therapist and mother may develop body-based emotional regulation strategies to calm her own trauma response (e.g. breathing exercises), and workshop alternative ways of engaging with her toddler’s feelings expressed through tantrums. Risk and safety are continuously monitored throughout treatment, and referral and advocacy provided as needed (Lieberman & Van Horn, 2011; Lieberman et al., 2015; Narayan et al., 2020). A core aspect of this phase of treatment is also to honour the child’s relationship with the frightening/absent caregiver (for example, in this population, their dad), understanding that children develop their sense of themselves based upon their relationship with all parents or caregivers present or absent in their lives. CPP also has protocols for inclusion of caregivers who use violence into parallel collateral or dyadic treatment where safe (Groves et al., 2015; Lieberman et al., 2015).
During this process of dyadic and collateral work, children and mothers become more active in shaping the therapeutic narrative. As the mother–child relationship is repaired, the triangle is changed over time. The trauma story begins to recede and more benevolent and hopeful experiences or “angels in the nursery” moments are built (Lieberman, Padron et al., 2005). The therapist’s role becomes less active, and eventually redundant. The mother and child and their recovery journey are honoured and the journey is concluded in the termination phase (Lieberman et al., 2015; Lieberman et al., 2020).
While there is a large body of evidence on the effectiveness of CPP, qualitative evidence is lacking to support improved implementation and gain clarity on participant experiences (especially children’s). The complex change mechanisms that occur due to CPP continue to be explored. The attachment relationship is, however, considered to be the main driver of change.
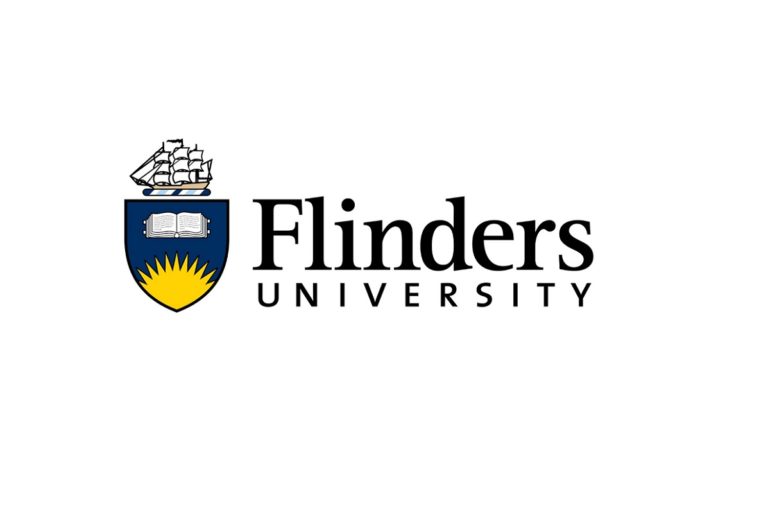
The program logic model (Figure 2) outlines the problem statement, consequences of the IPV on victims and survivors and associated factors, the relational CPP intervention and the theory of change proposed in the dyad.
Figure 2: CPP Program Logic Modela
aAdapted from the United Kingdom’s Domestic Abuse, Recovering Together (DART) program (Smith, 2016)
Child–parent psychotherapy training in Australia
CPP training in Australia is open to allied health and medical clinicians with experience in infant–parent mental health and currently employed within a clinical setting. The CPP training is conducted by an endorsed international CPP trainer from the United States. Training in CPP is currently delivered via a “learning collaborative model” (Ebert et al., 2012), an 18-month training model that centres on providing reflective case presentations with an international trainer and the establishment of local peer/supervision group presentations for learning (Lieberman et al., 2019). Specifically, the training comprises:
- seven days of core didactics and case-based competency building
- eighteen months of case-based consultation calls
- case-based participation in smaller local reflective supervision groups
It is expected that the smaller case-based reflective supervision groups will continue post-training as structures to sustain quality CPP delivery (or trauma- and violence-informed mental health/wellbeing care).
To date, two CPP Learning Collaborative (LC) models have been completed in Australia. The first LC was convened by the South Australian branch of the Australian Association for Infant Mental Health (AAIMH) in 2016–17, and the second was convened by Berry Street Victoria in 2017–19 in partnership with the RECOVER research project. A third LC commenced in 2020 and has been run completely online, with participants also learning to deliver CPP remotely. This current training is due to conclude in mid-2022. A fourth LC is due to commence in 2022. Training is funded in a range of ways:
- non-government organisations providing mental health and wellbeing care in the community with (now) ongoing funding to provide CPP to women and children affected by IPV
- public child and adolescent mental health services, or hospital-based therapeutic child protection services with professional development budgets for their staff or within their award structures
- individual private practitioners who self-fund training as part of their commitment to their professional development.
The child–parent psychotherapy workforce in Australia
The CPP workforce resembles the broader infant and child mental health and wellbeing workforce in Australia, consisting of clinicians across social work, occupational therapy, speech pathology, maternal and child health nursing, child psychotherapy, family therapy, psychology, perinatal and child psychiatry and paediatrics. Clinicians work in non-government organisations, child and adolescent mental health services, hospitals, child protection, private practice and local government settings. Two thirds of clinicians are situated in metropolitan areas. Most clinicians are situated within (or provide consultancy to) services that work with children who have experienced multiple adverse childhood and family experiences (including but not limited to family violence) and across statutory and non-statutory systems. To date, CPP in Australia has been delivered by this workforce to children and adoptive, foster-care, kith and kin care and biological parents. This includes CPP work with parents who are victims and survivors or perpetrators of sexual and family violence, including pregnant parents and or/where there is a risk of child removal.
Report structure
This report is divided into three main sections: Part 1: A systematic state of knowledge review; Part 2: Research process and methods; and Part 3: Research findings, including discussion and implications for policy and practice.
Part 1 outlines the current state of knowledge on family violence, the impact on children and suitable interventions for families to heal from abuse.
Part 2 provides insight into the research aims, methods, CPP training and therapeutic service sites. While maternal and child health and wellbeing outcomes were measured throughout the project, the feasibility of CPP implementation in the Australian context was the focus, rather than program efficacy. Eleven clinical partners were involved in the delivery of CPP. A thriving CPP community of practice was established.
Part 3 of the report focuses on the acceptability and feasibility of implementing CPP, barriers and enablers to implementation and the impacts the intervention has had on existing services. Practice implications and future research are also outlined. Findings provide policy and practice guidance on future therapeutic intervention work with families with young children exposed to family violence.
Part 1:
State of knowledge review
Context of this review
Our previous ANROWS Landscapes state of knowledge review explored literature on parenting in the context of domestic and family violence (Hooker, Kaspiew & Taft, 2016). In addition to identifying the prevalence, impacts and dynamics of abuse in families, it reviewed clinical trial-level evidence and other promising research on interventions to strengthen and support a positive and healthy mother–child relationship, post-IPV. Since publication, these results have informed future testing of interventions to support the recovery of abused women and children (Hooker et al., 2019).
The 2016 review identified a range of programs suitable for victim and survivor mothers and children to repair relationships and improve wellbeing. Intensive home visiting trials proved inconclusive with findings showing more targeted, IPV-specific therapy is needed for families. Other empowerment (Maternal Empowerment Program; Graham-Bermann et al., 2007), advocacy (Jouriles et al., 2009), psychoeducational (Circle of Security; Hoffman et al., 2006), psychotherapeutic (CPP; Lieberman, Van Horn et al., 2005) and trauma-focused cognitive behavioural therapy interventions (Cohen et al., 2011) were identified. Some relevant, non-trial interventions showed promise, yet lacked robust, ongoing evaluation due to a lack of funding (Bunston, 2008; Bunston, Pavlidis & Cartwright, 2016).
Psychotherapeutic interventions based on trauma that combined therapy for mothers and children together showed the most benefit. We subsequently recommended further development of effective interventions (like CPP) for mother–child victims and survivors of IPV, including measures of the parent–child relationship, in more pragmatic settings with representative samples, to fully understand what works to help women and children recover from IPV.
Existing review evidence
This RECOVER state of knowledge review builds on our previous evidence review outlined above (Hooker, Kaspiew & Taft, 2016). Prior to starting this study, we broadly explored recent (since 2016) literature or systematic reviews on interventions for families experiencing IPV.
Findings include separate reviews of evidence on children exposed to violence, pregnant women and mothers experiencing IPV, and interventions for fathers using violence.
A systematic review by Marie-Mitchell & Kostolansky (2019) on children’s outcomes associated with adverse childhood experiences identified that multicomponent/disciplinary-delivered interventions addressing parenting, mental health and social support for parents can reduce the impact of adverse childhood experiences and improve the parent–child relationship for pre-school-aged children (Marie-Mitchell & Kostolansky, 2019). Treating maternal mental health reduces mental health symptoms and behavioural problems in children (Marie-Mitchell & Kostolansky, 2019; Weissman et al., 2006) and is a strong argument for treating both mothers and children together in the aftermath of IPV.
Study heterogeneity and poor study quality limit review findings, although as described in earlier studies, Latzman et al. (2019) found programs targeting the non-offending parent had the largest effect. Programs with separate individual treatments for children and mothers were the least effective. Interventions based at home had a greater effect than clinic-based services (Latzman et al., 2019). Intensive home visiting interventions may decrease child behaviour problems in children exposed to IPV but overall, it remains unclear what IPV psychosocial interventions (and in what circumstances) are best for the promotion of child health and wellbeing (Latzman et al., 2019).
Austin et al.’s (2019) systematic review of interventions for women as parents in the context of IPV found it impossible to determine what interventions were most effective in addressing mothers’ needs. Study limitations found Austin et al. drawing similar inconclusive findings to Latzman et al. (2019). Earlier, Howell and colleagues looked at the unique needs of pregnant women exposed to partner violence (Howell et al., 2017). Despite the well-known negative effects associated with violence during pregnancy, very few interventions exist and those that do are limited to crisis-level interventions. Developmentally specific, strength- and theory-based interventions (like perinatal CPP) for pregnant women (and the foetus and newborn) exposed to IPV are urgently needed.
Interventions for fathers who use violence focused on increasing men’s accountability and empathy while decreasing violence, fostering positive fathering, and the father–child relationship (Labarre et al., 2016; Toone, 2018). Aims included promoting healthy interactions between father and child, and father and the child’s mother, including supporting the mother’s parenting. Program effectiveness was unclear due to a lack of quality program evaluation. Concerns were identified with fathers’ co-parenting and the potential for causing further harm to children and mothers when comprehensive safety and ongoing risk assessment is lacking (Labarre et al., 2016; Toone, 2018). However, going beyond dyadic mother–child interventions to also include fathers in children’s relational repair after violence can potentially improve father–child relationships and children’s sense of safety and wellbeing. More workforce training/skill development and organisational support for clinicians is needed to provide safe experiences and improved outcomes for victims and survivors (Toone, 2018).
Most similar to our current state of knowledge review, Anderson & van Ee (2018) revised treatment interventions for mothers and children (up to 18 years) exposed to IPV and attempted to document the theory of change. From 17 studies, multilevel, combination sessions (joint and separate) for mothers and their children seem most effective compared to individual- or joint-only programs. Benefits were gained from enhancing dyadic interactions. Authors have called for future research to test and replicate research identified in the review (including using the same outcome measures), in order to strengthen and consolidate the evidence (Anderson & van Ee, 2018; Howarth et al., 2015; Howarth et al., 2016).
Other reviews of research on program evaluations and interventions for families experiencing IPV do exist and have been described above; however, unique in comparison to other reviews, we searched the most recent (2015 to 2021) evidence on mothers and/or fathers and focused on pre-school-aged children.
Method
The purpose of this RECOVER state of knowledge review was to explore the nature and extent of global interventions (for parents and pre-school-aged children) to restore the parent–child relationship after IPV. We adopted a systematic, narrative literature review process to identify key themes across the evidence base.
Search strategy
In view of the previous systematic reviews completed on this topic, bibliographic databases were searched for peer-reviewed literature from the time of our previous ANROWS state of knowledge literature review (April 2015) to August 2019, with an updated search completed in May 2021. Databases include Medline (1946 onwards), CINAHL, SocIndex, Informit (Health & Family), PsycINFO and ProQuest. Using a modified PICO/PEO structure and Boolean AND/OR operators, the four main concepts explored were:
- population – child/parent
- intervention – treatment intervention/support
- exposure – intimate partner violence
- outcome – parent–child relationship.
Keywords and Medline search strategy are outlined in Appendices A and B.
To capture unpublished work including practice experiences, we explored the international and national grey literature/websites (see Appendix C) including Google Scholar. In addition, we hand-searched all references and citations (“snowballing”) of identified studies and reviews.
Eligibility criteria
The above search applied the following eligibility criteria to identified titles, abstracts and full-text articles.
Inclusions
- English language studies only from April 2015 to May 2021
- interventions with an IPV focus
- evaluation studies of a therapeutic intervention
- intervention at minimum addresses IPV, but may also address multiple risk factors/traumas
- population includes at least one of either pregnant women, mothers, fathers or both parents, and children aged from birth to 5 years
- interventions: either group, dyadic or individual therapy to support the parent–child relationship
- quantitative and qualitative evaluations of any design
Exclusions
- systematic reviews
- not evaluation of a therapeutic intervention
- not empirical study (e.g. commentaries, opinion pieces)
- studies without a parenting focus or parent–child outcome measure
- studies with the majority of children >5 years.
Data analysis
Based on the above eligibility criteria, all titles and abstracts were reviewed by two authors using Covidence software (Veritas Health Innovation) and inter-rater reliability was monitored using a predetermined article review template. If all inclusion criteria were met, articles were retrieved for full-text review, with items marked as unsure also included for full-text review.
Final full-text items were charted, and relevant data were extracted from each study (see Appendix F). Abstraction included study authors and year of publication, country of origin, setting, study design, data collection methods, sample details (participants and size), type of intervention and delivery method, comparison group details, outcomes assessed and evidence of effectiveness. Identified studies were synthesised and reported according to the delivery method and research design/hierarchy of evidence. The quality of the quantitative evidence was ordered as follows: randomised/quasi-randomised controlled trials (classed as high-quality evidence); non-randomised studies with a comparison group; non-randomised without comparison (pre–post observation studies); and finally, low-level quality for studies using single case study/series designs (classed as low-quality).
Results
Search results
We identified 34 articles, representing 29 separate interventions (see Appendices E and F) from April 2015 until May 2021. The search identified 2,027 records for assessment, with 22 additional records from grey literature and reference lists or citations of included studies. We excluded 1,655 from the title and abstract review, with 215 full texts potentially relevant for inclusion. After further application of eligibility criteria, we excluded 181 records (see PRISMA diagram in Appendix D for exclusion reasons) to reach our final 34 articles.
Articles included 10 RCTs and two ongoing trials (protocols only; 35%), two non-RCTs and 13 pre–post observational studies (44%) without a comparison group. Two papers reported on multiple pilot evaluations of the Attachment and Child Health (ATTACH) intervention, using a mix of RCT and non-RCT designs. The remaining involved qualitative research and case study evaluations (15%). More than two thirds of studies (68%) were published between 2015 and 2017, with only two papers identified since 2020.
Research was reported from eight countries with no quality trial-level evidence based in Australia. Australian evidence was restricted to two pre–post studies (Bunston, Eyre et al., 2016; Southwell, 2016) and one qualitative evaluation (Broady et al., 2017). Across all records identified, most articles (n=17) were from the United States (50%), and four (12%) each from Sweden and Canada. The United Kingdom and Australia published three each. Single studies were reported from Israel, India and the Netherlands. Urban settings dominated the research with no rural-only research identified. Four of the final 34 studies were conducted in both rural and urban settings (Broady et al., 2017; Domoney et al., 2019; Roopnarine & Dede Yildirim, 2018; Southwell, 2016), yet many settings were poorly described.
Significant heterogeneity in intervention type, comparison group used, target audience, delivery method and setting were noted across identified studies, making synthesis, comparisons and conclusions on best methods challenging. Group interventions made up most of the studies (53%), followed by dyadic/triadic interventions (23%), combination approaches (15%), and individual-only programs (9%; see Appendix G for various therapy descriptions). Some studies, for example, reported on group plus individual sessions with parents (Morales et al., 2015), while others used group plus dyadic interaction sessions with parents and children (Visser et al., 2015).
In this review we report studies according to intervention type (group, dyadic, individual or combined) and by study design to highlight the level and quality of the evidence.
1. Group treatment programs
Randomised/non-randomised controlled studies
RCTs offer the strongest design for measuring effectiveness and identifying the best methods of supporting women and children healing from IPV.
Of the 12 RCTs (including two RCT protocols and two studies without randomisation but including a control group), seven described group-based therapy (Feinberg et al., 2016; Graham-Bermann et al., 2015; Howell et al., 2015; Roopnarine & Dede Yildirim, 2018; Satyanarayana et al., 2016; Scott, 2017; Steele et al., 2019).
Interventions with the protective parent (mother) and child programs were most common and included maternal empowerment programs (MEP) with a parallel intervention for pre-school-aged children (Pre Kids’ Club; Graham-Bermann et al., 2015) and a group attachment-based intervention (Steele et al., 2019). In the Graham-Bermann et al. (2015) study, which included separate psychotherapeutic and educational group treatment for mothers and children, compared to a waitlist control group, female children in the treatment group showed improvements in internalising symptoms (depression/anxiety). Further analysis of these data and case notes indicated that 68 per cent of children developed re-experiencing symptoms during treatment, which spiked around the third session, resulting in recommendations to provide a minimum of 6 to 10 sessions for children to overcome these symptoms and prevent ongoing harm (Miller-Graff et al., 2016).
Howell et al. (2015) evaluated MEP only, a psychoeducational/advocacy intervention that aims to improve maternal mental health, parenting and self-efficacy. Significant improvements were seen in parenting behaviours compared to waitlist controls, with a reduction in corporal punishment immediately post-intervention and at six months follow-up (Grogan-Kaylor et al., 2019).
Scott’s (2017) protocol describes a trial underway evaluating two group-based parenting interventions: Mothers in Mind (MIM) and Caring Dads. MIM is a program for mothers and children that focuses on increasing maternal awareness of the impact of the IPV on the child and themselves, to positively influence parenting skills and competence. Caring Dads aims to prevent reoccurring IPV exposure for children by working with fathers (Scott, 2017). Program emphasis is on ending violence towards the child’s mother and improving child-centred fathering.
The other father-only group intervention was an integrated cognitive behavioural therapy (CBT) program for 177 IPV perpetrators with a dependence on alcohol (Satyanarayana et al., 2016). Satyanarayana et al. (2016) also found significantly less IPV perpetration among fathers attending the CBT treatment than controls. Spouses (mothers) also reported fewer mental health problems, however, no changes were seen in child behaviour or fathers’ alcohol consumption from baseline to three months follow-up.
Two studies described couple (mother and father) prevention interventions (Feinberg et al., 2016; Roopnarine & Dede Yildirim, 2018). Roopnarine and Dede Yildirim (2018) reported on 3,045 fathers from the Building Stronger Families psychoeducational intervention for vulnerable families, showing positive changes in paternal depression and IPV at 15 months post-intervention. Father–child relationships and child behaviour also improved, however self-report measures – especially fathers’ reporting on self and functioning – is a serious study limitation. Data from female participants were not reported in this article.
The Family Foundations psychoeducational program evaluated by Feinberg et al. (2016) is a transition to parenthood prevention intervention held pre- and postnatally over nine sessions (n=399). Outcomes focus on couple relationships, parenting quality, IPV and infant behaviour. After 10 months postpartum, better post-test levels compared with control couples were seen on more than two thirds of measures of co-parenting/parenting, parent mental health, child adjustment and partner violence. Effects on IPV were the largest, with strong trends in many other secondary outcomes. The large sample size and positive findings that reflect those of a previous pilot are study strengths, however, the mature and well-educated sample limits generalisations to all at-risk couples.
Pre–post observational studies (no controls)
Group therapy was again the most frequently reported type of intervention delivery in the observational studies identified. Six programs are described (Berry et al., 2019; Bunston, Eyre et al., 2016; McConnell et al., 2017; Pernebo et al., 2018, 2019; Rizo et al., 2018).
From Australia, Bunston, Eyre et al. (2016) reported on 30 dyads engaged in the Peek-a-Boo Club, a relational repair/psychotherapeutic intervention for infants and mothers impacted by partner violence. Improvements were seen in infant–maternal attachment and functioning, however clinical significance was uncertain, and authors suggest more comprehensive evaluation methods when testing the program in future.
Maternal mental health outcomes were the focus of Rizo et al.’s (2018) psychoeducational empowerment pilot study (MOVE: Mothers Overcoming Violence through Education and Empowerment). Mothers exposed to IPV reported significant improvements in depression and post-traumatic stress symptoms at both three- and six-month post-intervention time points.
The evaluation of the Family Vision coaching program (Berry et al., 2019) for 19 single mothers indicates that this type of group-based program for mothers is acceptable and feasible to implement in community settings, although statistical differences in pre–post outcomes on child–parent relationship measures and other parenting measures were not reported (Berry et al., 2019).
Caring Dads Safer Families (based on the Canadian Caring Dads model) was evaluated using a predominantly pre–post design. Using the fathering role to motivate men to examine and change their behaviour, Caring Dads explores men’s anger, family cohesion, co-parenting, domestic violence, perceptions of the child as a problem, use of corporal punishment, positive and involved parent–child relationship, self-centeredness and substance use. After two-hour weekly group sessions for 17 weeks, significant improvements in (father-reported) parental distress, parent–child dysfunction and parenting stress were shown. Partners’ and children’s reports enhanced the reliability of results which show promising evidence that the program can reduce risks to children and families (McConnell et al., 2017).
Pernebo et al. (2018) tested two group interventions and assessed outcome scores pre-intervention, post-intervention, six months later and 12 months later. Community-based psychoeducation and trauma-focused psychotherapy interventions both substantially reduced maternal trauma symptoms, although children benefited more from psychotherapy than the psychoeducation program. These treatment gains were sustained to 12 months with no increase in symptoms of IPV reported (Pernebo et al., 2019). Ongoing poor maternal mental health appears to hinder child recovery and children with high levels of trauma benefit most.
Qualitative research and other designs
Of all included studies, only one article focused solely on children. Pernebo and Almqvist’s (2016) qualitative paper explored nine pre-school-aged children’s experiences participating in a group psychotherapeutic intervention. Overwhelmingly positive responses ensued with themes around joy, security, relatedness, talking and competence. All children reported wishing to attend the group and no harmful effects were identified. Authors reinforce that young children (4 to 6 years) can contribute to research with valuable viewpoints that augment existing knowledge on interventions for women and children exposed to IPV (Pernebo & Almqvist, 2016).
Fathers reported on their experiences of the 18-week Taking Responsibility group (behaviour change) program, with a specific focus on fathers’ parenting and relationships with children (Broady et al., 2017). Twenty-one fathers reported that love for their children was a motivator to stop using violence, however, several group members considered themselves good fathers and failed to acknowledge that children were affected by the violence used. Despite this, children’s wellbeing and fathering may work as key leverage points for future interventions with men and children (Lamb et al., 2018).
The Parenting and Violence psychoeducational parenting program from Sweden (Kamal et al., 2017) aimed to improve parental awareness of children’s involvement in violence and minimise effects on child development and ongoing intergenerational trauma. Group therapy is offered separately for parents who are victims and survivors or perpetrators of IPV. Qualitative findings indicated that participants developed improved self-control, self-esteem and communication skills which had positive self-perceived effects on child wellbeing and behaviour.
2. Dyadic or joint treatment programs
Randomised/non-randomised controlled studies
Two dyadic studies used non-randomised controlled designs (Schechter et al., 2015; Waldman-Levi & Weintraub, 2015). The Family Intervention for Improving Occupational Performance program from Israel (Waldman-Levi & Weintraub, 2015) involved a dyadic crisis-based intervention for mothers and children, with an emphasis on dyadic interaction and play functioning. In the intervention arm, some significant differences were seen in mother–child interactions and play skills, but not playfulness. Video feedback with traumatised mothers and children (one to four years) in the Clinician Assisted Video Feedback Exposure Sessions (CAVES; Schechter et al., 2015) showed reduced parental negativity indicators towards their children, but not themselves, compared with non-traumatised mothers.
Letourneau et al. (2020) and Anis et al. (2020) report on the mixed pilot evaluation of the ATTACH program. The authors used both randomised controlled and non-randomised controlled designs to test the intervention with mothers and young children under 36 months of age. Although mostly dyadic, three of the 10 to 12 sessions offered included a triadic approach with a co-parent (father, relative, friend or other). Aside from Feinberg et al.’s (2016) Family Foundations study, these were the only two papers to report interventions that may have included the non-abusive (mostly mother) and abusive parent (father). Arguments for co-parent inclusion were to buffer maternal stress, offer social support and nurture attachment security. No mention of risk assessment or management of participant safety/ongoing IPV during therapy was explored in the papers. This information is needed if future interventions are to safely involve fathers who continue to parent children post-separation. The ATTACH evaluation showed significant improvements in overall reflective functioning and positive trends in enhanced parent–child attachment.
Pre–post observational studies (no controls)
We identified four dyadic studies using pre–post designs to test the effectiveness of two main interventions: CPP (Hagan et al., 2017; Lavi et al., 2015; Waters et al., 2015) and parent–child interaction therapy (PCIT; Herschell et al., 2017).
CPP has been evaluated extensively in the past using RCTs (Lieberman & Van Horn, 2005). In the above studies, further adaption/testing of CPP is reported against different samples and maternal outcomes. A pilot study of weekly perinatal CPP delivered to 64 pregnant women in the third trimester until infants were six months old (Lavi et al., 2015) found reduced depression and trauma symptoms from pre- to post-assessment. Women with lower feelings of attachment to the foetus demonstrated the greatest improvements in child-rearing attitudes and mental health (Lavi et al., 2015). Similar findings were reported by Waters et al. (2015) with Latina, low-income, pregnant women (n=52), indicating that the addition of a perinatal component to CPP may be a very useful intervention to consider in maternity service settings for pregnant women experiencing IPV – especially as very few interventions exist for pregnant women experiencing partner violence (Howell et al., 2017). However, further research using perinatal CPP is required with larger randomised and representative samples using comparison groups to show real effect.
Conflicting with other findings, Hagan et al. (2017) found trauma symptoms improved more in female children, in dyads (n=199) with fewer lifetime stressors, and among those who received fewer CPP sessions. These findings are inconsistent with previous research which has found no gender differences in effects (Hagan et al., 2017), and in other studies included in this review which reported improved benefits (mental health, trauma and behaviour symptoms) for those at greatest risk (Lavi et al., 2015; Pernebo et al., 2019). These conflicts reinforce the need for replication of studies and more research on the feasibility and efficacy of CPP.
Challenges were identified in the implementation of PCIT in a shelter population evaluated by Herschell et al. (2017), with high attrition (57%) and only nine of the 21 participant dyads completing treatment. Positive effects on child behaviour were seen but there were no improvements on parenting practices.
Qualitative research and other designs
In a case series study by Keeshin et al. (2015) with shelter participants (n=8), combination PCIT with individual parent training and dyadic sessions were acceptable to mothers and children (2 to 5 years). PCIT improved women’s parenting capacity including more positive communication and praise of children (Keeshin et al., 2015). However, shelter settings may not be suitable sites for intensive therapy due to women’s and children’s ongoing stressors at this time (e.g. leaving the shelter, relocating, changing schools; Herschell et al., 2017).
3. Individual treatment programs
Randomised/non-randomised controlled studies
Intensive nurse home visiting (HV) programs have shown promise in reducing child abuse and parenting behaviours but there have been inconsistent findings on their benefits for reducing IPV and its impact on mothers and children. In the United States, Jack et al. (2019) enrolled 492 socially disadvantaged pregnant women in a 2.5-year HV program that included an augmented IPV component comprising further assessment, tailored care and social supports. Although women’s quality of life improved in both control (usual HV care) and intervention groups at 24 months post-delivery, no differences across arms were seen. Caution is needed in interpreting these results as although this was a rigorously evaluated trial, fidelity to the augmented HV intervention was challenging and these results may reflect poor implementation, rather than poor intervention effect (Hooker & Taft, 2019).
Pre–post observational studies (no controls)
In a less rigorous design, HV was again evaluated in the United Kingdom by Domoney who tested For Baby’s Sake, a trauma-informed parenting program aimed at breaking the cycle of IPV and improving child outcomes. The intervention is offered to vulnerable families from pregnancy until children are two years old. Conclusive data are yet to be published; however, early findings indicate parents value the approach. More HV research to address IPV and improve the health and wellbeing of affected mothers, fathers and children is needed.
In response to unmet demand, an Australian community service organisation developed the yourtown Expressive Therapies Intervention (YETI) program in Queensland for disadvantaged families (Southwell, 2016). Set in refuge and family support services, YETI provides individual treatment for infants and young children that draws on theoretical frameworks including expressive, child-centred play and parent–child relationship therapy. Evaluation data over two years showed 85 children under 5 years attending, with 41 parents providing outcome data on child behaviour and mental health. Significant and promising results showed improvements in child behaviour and mental health, including child social functioning, self-confidence and the parent–child relationship. Although dropout rates were high, this is not unusual in vulnerable populations (Herschell et al., 2017) and this program can be delivered by non-specialist staff who receive regular clinical and operational supervision (Southwell, 2016).
Qualitative research and other designs
No qualitative/other papers were identified that reported individual treatments.
4. Combination treatment programs
Randomised/non-randomised controlled studies
Visser and colleagues (2015) from the Netherlands describe the HORIZON trial currently underway that includes preparatory group work with parents only, parallel groups for parents and children, and dyadic parent–child sessions based on trauma-focused CBT.
Fathers for Change (Stover, 2015) uses the fathering role as a motivator for change and integrates methods to reduce paternal substance abuse. Individual sessions and dyadic treatment with partners and children are offered over four months. Compared with controls (offered group drug counselling), the Fathers for Change participants completed more treatment sessions, described greater program satisfaction and were less intrusive in father–child interactions during free-play sessions. In addition, a trend in the reduction of IPV was seen in these fathers.
Pre–post observational studies (no controls)
Fathers for Change was also evaluated in 2017 in a feasibility study testing program implementation in a residential substance use disorder treatment setting (Stover et al., 2017). Participants generally engaged and were satisfied with the program, with a reduction in anger and emotional regulation problems. Fathers for Change is a feasible treatment for fathers using violence and substances within residential drug treatment facilities. Results of these preliminary studies show promise in the context of fathers’ co-parenting; however, authors acknowledge further evaluation of Fathers for Change and other parenting programs is warranted in this setting (Stover et al., 2017). Larger samples and testing the intervention in non-drug affected, mandated populations may also be beneficial.
Qualitative research and other designs
Morales et al. (2015) used a single case study design to describe the impact and cultural adaptability of SafeCare for Latina families (parent–infant interaction module), an HV program that aims to reduce child maltreatment and the impacts of IPV on parent–child interactions. A range of parenting and maternal health and wellbeing factors improved at one and three months post-treatment, with high levels of participant satisfaction. Assessing the suitability of programs across cultures is essential for program success, with further research needed to confirm that SafeCare is appropriate for Latina families (Morales et al., 2015).
Discussion
To inform the development of Australian programs and services and improve outcomes for women and children experiencing IPV, we conducted a comprehensive state of knowledge literature review of IPV interventions addressing the parent–child relationship for families exposed to IPV. This review builds on previous ANROWS research we have completed on parenting and domestic and family violence, including a 2016 scoping literature review exploring the nature of healing interventions for victim and survivor mothers and children (Hooker, Kaspiew & Taft, 2016).
Review limitations
Our review was restricted to English-only studies from April 2015 to May 2021. While every attempt was made to identify all published and unpublished work on interventions to heal the parent–child relationship among those experiencing IPV, the significant increase in research on this topic means we may have missed some of the evidence. In addition, this is a narrative review that has not included the rigour of other types of more systematic literature reviews, including a detailed analysis of the quality of the evidence. To address this, we have reported findings according to the levels of evidence to highlight the scope of the literature. Categories used to organise and describe studies (designs and delivery type: group, dyadic etc.) may have some overlap. The following discussion reports on common review themes and identifies evidence gaps for further research.
Focus on fathers
Since 2015, there appears to have been an explosion of research published on IPV and parent–child interaction, especially related to interventions for fathers. The significant variation in study type, design, intervention delivery method, setting, sample size and outcomes measured makes it difficult to make sound conclusions about what methods are best for supporting parents and children to restore relationships post-IPV. Trial-level evidence for programs (to support abused women and children) is reasonably strong, with good sample sizes, although in-depth analysis of the risk of bias was beyond the scope of this review. We agree with other researchers that the evidence base is underdeveloped and that more rigorous studies are required (Latzman et al., 2019).
The evidence on fathering interventions did not address earlier concerns highlighted in the literature about safety and ongoing IPV risk (Labarre et al., 2016; Toone, 2018). This was possibly due to the types of interventions for fathers we identified (e.g. primary prevention, clinical treatments) but ongoing risk assessment remains a high priority in interventions with fathers. Critique of father interventions was more directed to methodological issues and potential bias, for example where abusive men are self-reporting improvement in attitudes, knowledge and behaviour change. A small amount of qualitative or mixed methods research was identified but much more is needed to inform program feasibility (especially in rural areas) and to identify the essential elements of successful program implementation, in conjunction with future trials.
Relational interventions
Psychotherapeutic and psychoeducational interventions dominate the evidence, with some suggestion that longer term psychotherapy improves child, maternal and relationship outcomes. Overall, few studies reported on the sustained benefits of programs. Treating both mothers and children together appears optimal, as there is clear evidence that improvements in maternal mental health predict enhanced child functioning and mother–child relationships (Marie-Mitchell & Kostolansky, 2019). Brief interventions, while appealing to funding bodies and providers, may not be suitable for families exposed to IPV, especially children with high trauma symptoms who were reported to benefit most from treatment (Pernebo et al., 2019). Dyadic work is resource-intensive but may be the most cost-effective considering the harm IPV has on children, families and generations (Spangaro, 2017). Dyadic psychotherapy for mothers and children exposed to IPV has been recommended since 2013 (WHO, 2013b).
New studies are now combining treatments to include group, dyadic and individual sessions for pregnant women and all family members, however, the sustained and real benefit of group therapy over dyadic treatment remains unclear. Outcome measures seem to have expanded beyond child behaviour and mental health since the earlier review (Howarth et al., 2016) and call by Howarth et al. (2015) for more consistent use of outcomes in this field. However, outcomes remain clinically focused, and a lack of consensus remains on best measures/instruments to use.
Australian research needed
Very few studies originated in Australia, indicating a lack of evidence-based treatment options and research on IPV and parenting locally. The testing and replication of interventions identified in this and previous reviews are warranted. Psychotherapy or combined psychotherapy/educational programs that are jointly delivered to abused mothers and children may be of greater benefit than educational programs alone. Identification of contextual differences and cultural adaptation (including in rural settings) is essential for many of these interventions which have been tested in the United States, often with non-representative samples.
In late 2019, our research team was successful in obtaining ANROWS funding, with legacy funds from the former Luke Batty Foundation, to test the feasibility of implementing CPP into Australian rural and urban service settings. This funding extended existing research: Reconnecting Mothers and Children after Family Violence, or RECOVER, which had begun in 2017 through the Safer Families Centre for Research Excellence at the University of Melbourne. [1]
1. See https://www.saferfamilies.org.au/
Part 2:
Research process
Research questions
1. How acceptable and feasible is CPP for IPV-affected mother–child dyads to the Australian context?
- How acceptable is the intervention for women and service providers?
- What are the barriers and facilitators to the implementation of the CPP model into services?
- What (if any) are the dyad recruitment and retention issues encountered?
- Are there process and impact differences between service providers across sites?
2. Do CPP therapists-in-training adhere to CPP model fidelity?
3. How effective is CPP treatment delivered by CPP therapists-in-training during the study?
- Do women’s and children’s trauma symptoms differ before and after treatment?
- Does treatment improve the mother–child relationship?
Design
We used a concurrent, mixed methods feasibility study design to assess acceptability, implementation processes and effectiveness of CPP for RECOVER families. In addition to qualitative process evaluation, descriptive quantitative data on recruitment and implementation were collected. In a longitudinal, repeated measure design, outcome measures were assessed via parent survey at three time points: baseline (pre-intervention; T1), 12 weeks into the core CPP phase (midpoint; T2), and at the completion of the intervention (post; T3). Clinical data of measures were collected from service records. Practice champions were embedded within two services and supported recruitment and facilitated data collection. Practice champions are leadership staff within an organisation who are passionate about using evidence to inform practice and who support the implementation of new practices within the clinical environment.
Qualitative in-depth interviews with therapists and managers occurred mid- and post-intervention. Women were interviewed post-treatment. Direct observation of dyad interactions throughout treatment were recorded and assessed.
Participants
- CPP-trained therapists from Victoria and South Australia
- service managers
- practice champions
- mother–child dyads who have experienced IPV and meet the inclusion criteria.
Practice champion role
RECOVER practice champions included clinical leaders (one in a rural CAMHS, one in an urban family violence service) who advocated for CPP implementation and development within their respective services. These two practice champions (involved in the RECOVER 1 sites) were carried over to the RECOVER 2 settings. On a part-time basis, they maintained relationships with CPP international trainers, coordinated team supervision or mentoring, monitored CPP fidelity, and ensured that CPP and young children’s needs were kept on the agenda within multidisciplinary teams delivering a range of service offerings to different age groups. Both practice champions participated in the CPP national community of practice and in a monthly supervision phone call with CPP international trainers. The roles grew to provide peer support to each other and on one occasion, when a champion from one service took extended leave, there was an arrangement whereby the other provided CPP supervision to staff to ensure training requirements were met.
Study sites and recruitment process
In addition to clinical site therapists and managers, we sought eligible parent–child dyads from clinical services via intake systems. These study sites were chosen due to the accessibility of trained or trainee CPP therapists and service providers. As there is a shortage of staff qualified in CPP, most therapists underwent CPP training during the time of the study.
Eleven community-based, clinical sites including specialist family violence services (with clinical services for children), child and adolescent mental health services (CAMHS), one enhanced maternal and child health centre with a multidisciplinary team and co-located infant mental health specialist, and one private perinatal psychiatry clinic participated in RECOVER and actively recruited suitable mother–child dyads for the study.
Five urban, three rural and three regional service sites were chosen across Victoria and South Australia (Table 1). Recruitment periods at sites were approximately six months each for RECOVER 1 and 2, depending on workforce availability and capacity.
Table 1: CPP recruitment sites, location, phase and therapist qualifications (n=11)
Clinical site
Location
Australian state
RECOVER phase
Therapist base qualification
Family violence service
Urban
1 and 2
Child psychotherapist/psychologist
Family violence service
Regional
1
Social worker/psychologist
CAMHS
Regional
1 and 2
Mental health nurse/
social worker
CAMHS
South Australia
2
Social worker
CAMHS
Rural
South Australia
2
Social worker
CAMHS
Rural
South Australia
2
Occupational therapist
CAMHS
Urban
South Australia
2
Social worker
Take Two
Regional
Victoria
2
Social worker
Hospital child protection services (CPS)
Urban
South Australia
2
Psychologist
Private perinatal
psychiatric clinic
Urban
Victoria
2
Perinatal psychiatrist
Enhanced maternal and child health service (with co-located infant mental health specialist)
Urban
Victoria
2
Maternal and child health nurse
Dyads were recruited and received treatment through specialist family violence and CAMHS, in metropolitan and regional areas of Victoria and South Australia. Recruitment was staggered as new sites came on board and occurred over two waves – RECOVER 1 in 2018 and RECOVER 2 in 2019–2020, with the welcome addition of ANROWS funding (with legacy funds from the former Luke Batty Foundation). Due to organisational capacity, a smaller number of dyads were recruited from other services such as hospital-based therapeutic child protection services (CPS), a private perinatal psychiatric clinic and a local government maternal and child health service. Potential mother–child dyads entering services were screened by CPP therapists to determine participant eligibility for the project, describe the study and gain informed consent. In this study, the emphasis is on exploring feasibility rather than efficacy and in fact efficacy cannot be reliably tested when therapists are still learning the model and have not met the full training requirements for delivery of CPP.
Fathers’ consent
All service sites that participated in the study had existing procedures for obtaining parental consent (from both parents) to treat children, including consideration of court orders governing parental decision-making. The specialist family violence service sites (children’s clinical service) had additional decision-making procedures directing safe engagement with fathers who were perpetrators in consent conversations about their child’s need for treatment. This included procedures for initial conversations and decision-making with victim and survivor mothers about the risks and benefits of therapists engaging or not engaging fathers in consent conversations about their child’s treatment.
All sites implemented the CPP foundation fidelity requirements that provide specific direction for “Assessing Child Safety Risks to Engaging in Trauma-Informed Treatment” (Lieberman et al., 2015. p. 262), where risks are coded. These include considering whether “child has contact with a violent caregiver who is unaware that child is participating in trauma treatment” or “child has contact with a violent caregiver who denies the child’s experience of trauma” (Lieberman et al., 2015. p. 262). It is worth noting that in contemporary CPP practice, perpetrator co-parents would at minimum be included in consent conversations about their child’s treatment and assessed for suitability to be included via collateral parenting or parallel father–child dyadic sessions (Groves et al., 2007; Lieberman et al., 2015). However, in RECOVER, while fathers’ consent for child treatment was requested, they were not provided with CPP collateral parenting or dyadic treatment at the study sites.
Therapeutic readiness
A complex range of individual, relationship and organisational or ecological factors impact on participant readiness to take up interventions (Fogarty et al., 2020; Howarth et al., 2018). “Therapeutic readiness” is a term initially coined in relation to the application of child psychiatry within community settings (Despert, 1949). It considers what factors internal to the individual child and caregivers, versus factors external to the child and caregivers, are conducive to initiation and engagement in treatment. The authors of the current study initially attempted to describe the idea of therapeutic readiness by developing an inclusion criterion based on the concepts of 1) maternal “readiness to change” within situations of IPV (Humphreys et al., 2011); and 2) a definition of sufficient mother–child safety as “post-crisis situation, or not living with the person using violence”. However, CPP itself provides a foundational framework that equips clinicians to determine therapeutic readiness considering family strengths and contextual risks (Lieberman et al., 2015, p. 265). Over the duration of study implementation and continuing to date, services participating in the study have continued at a local level to expand implementation of CPP and refine concepts of therapeutic readiness for this population. This expansion has especially considered the realities experienced by families experiencing cycles of violence, some of whom will separate, re-partner or remain together. More work however is needed to integrate and consolidate this learning as part of a national trauma- and violence-informed child mental health framework.
Recruitment criteria
Inclusion criteria:
- pre-school-aged child (3 to 5 years)
- biological mother of the child
- English-speaking mother
- recent exposure to IPV (past 12 months)
- mother has received subsequent IPV assessment and advocacy support (risk assessment and safety
plan, counselling and referral to legal, housing,
healthcare services) - therapeutic readiness: post-crisis or not living with the person using violence
- clinical signs of trauma (e.g. a child presenting with emotional or behavioural issues/impaired mother–child interaction based on clinical assessment).
Exclusion criteria:
- mother–child dyads where the person using violence continues to use violence and live in the family home or there is insufficient safety
- mothers who have been substantiated/documented abusers of the child
- mothers who are currently dependent on alcohol and other drugs
- previous diagnosis of maternal intellectual disability
- significant maternal mental illness, for example, psychosis
- children with a significant intellectual disability and/or autism which interferes with their capacity for engagement in treatment.
Process evaluation
To assess program feasibility, Bowen et al. (2009) suggest there are eight core study aspects to evaluate. These are program acceptability, demand, implementation, practicality (costs), adaption, integration, expansion and limited efficacy testing. In this study, we evaluated acceptability, implementation and costs, in addition to fidelity, reach and dose.
Acceptability
We explored whether CPP was a suitable method of treatment for therapists and families receiving treatment. Suitability criteria included satisfaction with/appropriateness of the model, intervention length, content and types of questions used in the survey, intention to continue with the treatment, and the fit of CPP within the organisational culture.
Implementation
Therapeutic interventions to support women and children need to be sustainable. The collection of process data is an important aspect in the evaluation of complex interventions like RECOVER. Assessing the feasibility of CPP in the Australian context involves having a greater understanding of the barriers and enablers to implementation and program sustainability.
Theoretical framework
In this study, factors influencing integration of the CPP model were explored using May and Finch’s (2009) implementation framework: normalisation process theory (NPT). This socio-behavioural theory proposes four essential principles or constructs that explain the type of work people need to do to implement a new practice or intervention. These include coherence (sense-making work), cognitive participation (relational work), collective action (operational work) and reflexive monitoring (appraisal work; May & Finch, 2009). These NPT constructs have been used to frame data collection tools and support the intervention and process evaluation.
Intervention fidelity, reach and dose
CPP fidelity monitoring was essential due to the potential diversity of clinical presentations and program flexibility. The CPP manual describes a six-strand fidelity framework, which includes reflective practice, emotional process, dyadic relations, trauma framework, and procedural and content fidelity (Lieberman et al., 2015). Each CPP phase has detailed fidelity tools incorporating this framework, which were completed by clinicians. Clinicians completed specially designed fidelity logbooks (based on work by Almqvist [n.d.]) after each consultation, which indicate adherence to CPP goals. Throughout official CPP training, treatment fidelity was closely monitored through a review of process notes and regular clinical supervision. Clinical data were collected on maternal, child and/or dyad assessment; fidelity measures; and the intervention reach (number of eligible dyads offered CPP) and dose (sessions attended/delivered).
Practicality including costs
Parents were asked about costs incurred in attending treatment sessions to gain some insight into the burden on parents. A cost–benefit analysis of CPP was not undertaken.
Data management
Participants and therapists were given a unique ID code for use throughout the study. A secure, purpose-built online electronic database was used to record and store all data including participant and therapist details. Dyadic interaction was recorded using tablet devices. Onsite clinical researchers regularly collated intake, fidelity and survey data. All data were uploaded as electronic files to university research drives that are securely stored.
Data collection time points
Pre-intervention
Therapists collected baseline quantitative outcome measures using a maternal survey (and parent–child interaction, free-play recording) in the foundation phase of treatment and recorded dyad free-play sessions. Survey responses also captured women’s expectations of the treatment and outcomes that most suited their needs. Therapists documented fidelity, attendance rates and dose for each dyad at each session. Table 2 provides time points and outcomes measured.
Table 2: RECOVER project outcome measures and data collection time points
Mental health and wellbeing
Outcome measures
Pre
Mid
Post
Symptoms Checklist–90 Revised (SCL-90-R)
(Derogatis & Unger, 2010)
X
X
X
PTSD Symptom Scale–Interview (PSSI)
(Foa et al., 1993)
X
X
X
Composite Abuse Scale (CASR-SF)
(Ford-Gilboe et al., 2016)
X
X
Child functioning and trauma symptoms
Outcome measures
Pre
Mid
Post
Strengths and Difficulties Questionnaire (SDQ)
(Goodman, 2001)
X
X
X
Young Child PTSD Checklist (YCPC)
(Scheeringa & Haslett, 2010)
X
X
X
Parenting
Outcome measures
Pre
Mid
Post
Parental self-efficacy, warmth, irritability and consistency
(Zubrick et al., 2014)
X
X
X
Mother-child relationship
Outcome measures
Pre
Mid
Post
Parental Reflective Functioning Questionnaire (PRFQ)
(Luyten et al., 2009)
X
X
X
Recording of parent–child interaction assessed using
Coding of Attachment-Related Parenting (CARP)
(Matias et al., 2006)
X
X
X
Midpoint
While the true midpoint of a flexible, needs-based intervention is undetermined, findings from previous CPP studies suggest dyads require between 20 and 32 weeks of core therapy. Consequently, we defined our midpoint evaluation to be at 12 weeks. Researchers conducted process evaluation interviews with CPP therapists and managers, using NPT to explore feasibility, experiences and contextual factors related to implementation. Therapists also collected maternal reports of quantitative outcome measures and recorded direct observation of dyad free play.
Post-intervention
Researchers conducted impact evaluation interviews with mothers, therapists and managers, using NPT to explore feasibility, perceptions/experiences and contextual factors related to implementation. Quantitative outcome measures and dyad free-play recording were completed by therapists in the termination phase of treatment.
Outcome measures
The main focus of this study was on feasibility as CPP is an evidence-based intervention. However, we were interested in testing evaluation instruments with mothers and therapists and reporting any concerns and possible outcome changes. When deciding on outcome measures to use in this study, we considered 1) measures used in the original Lieberman (2015) trial and those recommended by CPP developers; 2) calls within the literature to expand assessment beyond child mental health and behaviour; 3) participant and therapist burden; 4) service provider capacity and experience (and alignment with existing measures used by services); 5) instrument and training costs; and 6) the age of children. The main outcomes of interest included maternal and child mental health and trauma (PTSD) symptoms and child behavioural problems. PTSD in 3- to 5-year-olds often manifests as behaviour problems and these were used as a basis for the description of the disorder (Table 2). Secondary outcomes measured recovery by assessing parenting (self-efficacy, warmth, irritability and consistency), reflective functioning (or the mother’s ability to hold the child’s mental states in mind), responsiveness and the mother–child relationship/interaction.
Analysis
All interviews were audio-recorded, transcribed by a professional transcription service, coded by two RECOVER researchers and analysed using an NPT lens. Process evaluation assessed the model’s feasibility and identified contextual program barriers and facilitators to inform future research. NVivo software was used to assist the analysis. Statistical analyses were completed using STATA Version 15. Proportions and means (with 95% CIs [confidence intervals]) were calculated to describe participant baseline characteristics, fidelity and feasibility measures. Paired samples t-tests compared mean scores at different time points. If data were not evenly distributed, medians, range and non-parametric tests were used. Survey responses with missing values were removed list-wise.
Dyad video recordings of free play were viewed and coded using a coding scheme specifically designed for observation of parent–child interaction called Coding of Attachment-Related Parenting (CARP; Matias et al., 2006). Domains included parental responsiveness, sensitivity and affect; child affect; and dyad mutuality. All recordings were double coded by researchers, with inter-rater reliability calculated. If parents did not consent to recording, then therapists made notes of parent–child interaction and these notes were then coded and analysed using the CARP guide.
Ethical considerations
Consent
Due to the nature of treatment, women’s consent to the project could only be obtained when it was clear that women and children required treatment. This was not evident until a thorough assessment of the dyad was made by an experienced therapist, after intake to one of the participating services. If women and children were deemed unsuitable or not ready for this specialist type of treatment, they were offered alternative support (e.g. case management, individual/group counselling). As such, therapists, rather than researchers, obtained informed consent and facilitated collection of clinical outcome data. Women were provided with a participant information statement and invited to ask questions about the research and sign the consent form for herself and her child to participate. However, all participants had clear instructions (in verbal and written form) that their participation was voluntary and that they could withdraw from the study at any stage without prejudice, disadvantage or interruption of treatment.
Vulnerable group
The clients are a vulnerable group, some of whom have potentially been traumatised by their experiences of violence. Experienced qualified clinicians delivered CPP and managed any potential distress. Researchers interviewed clients once post-treatment and adopted a distress protocol including information for referral. RECOVER researchers are trained and experienced in family violence identification and supportive debriefing in the event of participant distress.
When therapists and service managers were interviewed, they may have felt uncomfortable about discussing implementation in relation to their organisation, and concern that they could be identified. Clear information was provided to staff regarding privacy prior to consent, and all participant data were de-identified.
All ethical considerations and applications for approval of the research were guided by the WHO recommendations on ethics and safety for intervention research on violence against women (WHO, 2016).
Prior to research commencing, human research ethics committee approval was received (including all modifications) from La Trobe University (HEC17-108), Goulburn Valley Health (GVH 03/18), the Victorian Government Department of Health and Human Services (HHSD/19/234647), and South Australia’s Women’s and Children’s Health Network (HREC/19/WCHN/88).
Part 3:
Research findings
1. How acceptable and feasible is CPP to the Australian context?
Forty in-depth process and impact interviews were completed during the RECOVER project to assess program acceptability and feasibility: 28 interviews with therapists (n=15) and managers (n=13), and 12 interviews with women on the completion of treatment. Overwhelmingly, the intervention was acceptable to the majority of participants. Except for two women, all participants including therapists and managers reported CPP as a suitable treatment option for IPV-exposed families. In addition to asking women about the acceptability of the intervention, therapists were asked how acceptable CPP was for their clients and themselves.
Mothers
There are so few interventions for young children, with many being for older children, meaning CPP is quite unique. The majority of mothers found the program useful and acceptable. One mother called it “phenomenal” (Mother 3).
Those who found the program the most acceptable usually had a very good relationship with the therapist, as did their children. These dyads often received longer treatment and saw their children develop as well as their own confidence as a parent, as they learned how to manage their situation.
This experience, good has to come out of it and one of the things is connecting with her [the therapist] and having her support and my son just adores her, she’s been amazing. (Mother 6)
Therapists noted that mothers would often see the importance of CPP for their child but, through the therapeutic process, realise the impact on their own healing, as the program supports parental confidence and growth, as well as healing the dyad relationship. “It’s a lovely model to support mums and children.” (Therapist 6)
One mother described how she had previously been “covered in armour” protecting herself as a result of prolonged IPV. She attempted to shield her children from the abuse alongside her own stress and trauma. Working with the therapist helped her learn to express her inner feelings and emotions with her children and to reach out to support networks. “It helped me express who I am.” (Mother 11)
Women’s motivation to seek therapy was generally for the wellbeing of their child/ren after experiencing family violence-related trauma. They predominantly saw it as an opportunity to support their children emotionally and to improve their relationship with their children and their own parenting skills. Many mothers reported their child to be anxious and/or having attachment problems and hoped the program would help build the child’s confidence and improve communication, especially about their feelings. “I wanted to figure out how do I help her, then to help us.” (Mother 3)
The program allowed mothers to see how the therapist worked with the child, modelling a learning, reflective and relational practice, so they could learn to adopt these reflective strategies with their child.
They’re kind of getting to learn and say, “Oh, well I can try that, or the therapist did that, that didn’t work very well”, or whatever. There’s kind of a sense of teamwork like you’re trying stuff out and you might not always get it right, but sometimes it works and you know, there’s that kind of sense of us being in the struggle and sharing that struggle with mums and kids, and them not being alone and perhaps to feel that they can take some of what they learn back with them, out of the room, as well. (Manager 4)
The mothers themselves wanted to gain these skills.
For myself, it was about getting some tools and strategies to help my little girls to help them get an understanding of what their feelings were and how to help them with that when they were really struggling. (Mother 9)
However, some mothers were focused on supporting their children without fully grasping the impact CPP may have on them, as mothers. Women come into the program with their own trauma history (recent IPV and/or earlier trauma), which they often do not expect will be considered in the sessions. Some mothers may not want to share their history.
Interviews were captured with some women who disengaged early, before treatment even started. Mothers in this group (n=2) did not find the sessions acceptable, usually not connecting with the therapist and/or having an inconsistent experience with the therapist, and not finding the sessions as useful as they had expected. These reports were from one rural service which lacked established clinical governance structures and where therapists were still completing CPP training. “I didn’t get along with her – she was nice, but I didn’t feel like we were achieving anything … I just felt like my time was being wasted.” (Mother 2)
“It’s just had such an amazing impact on all three of us and I’d do it again and again just for the things that I learnt and the things my girls learnt and the things we learnt together. I feel like to a degree they got their mummy back.” (Mother 9)
Therapists recognised that women had to be “therapeutically ready” to take on an intensive intervention like CPP. Many clients had complex trauma in the family and therapists have a very short safety window at times with clients. In these cases, when
safety is not particularly well established, mums are really traumatised themselves and are quite often nominating that they don’t have the capacity to engage in long term – they can’t think about the logistics of engaging in a long-term therapeutic intervention. (Therapist 11)
Therefore, therapists learnt over the course of the pilot to assess readiness before they suggested CPP. If a mother had very recently experienced violence and was still focused on acute practicalities, she may not be ready to make a commitment. In some instances, the mother engaged briefly with the service and then after several months came back to engage in the longer service.
Several rural therapists suggested women were unable to engage in CPP for other reasons – for example, they may not understand the treatment, thinking the problem is the child, or being burdened themselves by life circumstances.
So you know the ideal of maybe seeing a family for four sessions over four weeks doesn’t happen. I think that that’s a – they want to stay involved, but they just can’t, they don’t have – what they talk about is not having the headspace to do four weeks in a row, or they’ve got big families, no car, you know poverty is a big thing. (Therapist 9)
I mean, we get a lot of parents who come in here and say “Come here and fix my child. It has nothing to do with me.” (Therapist 1)
While there were some concerns, in general the majority of therapists were very positive about CPP for dyads: “Yes they’ve been really positive. I’m not surprised, they come every week, they’ve been really engaged. I think it’s been quite acceptable to them.” (Therapist 10)
I think that the mother having to provide her own trauma history and her own attachment history was really hard for the mum that I’m working with, to understand. She’d come for therapy for her child, she really didn’t understand what it was that – why I was talking about her parents or her childhood or, you know, her past relationships with other men, who weren’t the father of this child. I had to spend a lot of time creating a shared understanding of why I needed that information and that I wasn’t just collecting information for information’s sake, or trying to snoop into her history. That was challenging and I think wouldn’t have been accepted if it was a less overt model of – I really like the overtness in this model. We’re very upfront about what it is that we’re doing and why, with clients, at all times. I think that that creates acceptability, where I think in other kinds of therapy that would be lacking. (Therapist 11)
Suitability of outcome measures
Maternal surveys captured a lot of information, including sensitive questions about women’s relationships, health and past abuse. One therapist was concerned that the survey questions might be upsetting for the client. However, she noted, “In actual fact it wasn’t a big deal at all, the women were very happy to fill out those questionnaires and it wasn’t a problem”, and further that “a lot of the mums have reported that they found doing the measures quite validating” (Therapist 6).
Women reported mixed feelings about the IPV Composite Abuse Scale questions in the survey. Some mothers reported that the survey questions about abuse and violence were not complex enough. “I think the survey or questions that you asked to do with trauma weren’t nuanced enough to pick up on complex trauma rather than sort of more situational.” (Mother 5) In contrast, in a few cases, mothers thought the questions were difficult. “It was intimidating [the questionnaire], I guess because a lot of time it’s not something you like to think about, it’s something you choose to forget.” (Mother 2) However, this was not the case for most participants.
Therapists reported that some mothers, on describing the IPV they had experienced, had concerns about being judged as poor parents within court contexts and/or being reported to child protection services. This is an issue not unique to CPP.
I think the family violence dynamic brings in something that’s a bit even hard for me to articulate. But it does … make it much harder for a mum to trust engaging with a service, and talking about their child, when they think that there’s even a remote possibility that their parenting will be judged as poor, and that that information will get back to a court environment, or that the father or violent person will be able to somehow access the information and use it to their advantage. And just what it’s like for women to live under risk, such high levels of risk all the time, makes it very hard to come to weekly appointments, and their kids are frequently sick for the same reason. So that’s what I’ve found. (Therapist 9)
Acceptability of CPP for therapists and managers
Managers found that CPP was beneficial for the individual therapist, but also for the broader organisation. The intervention was also something that created a sense of purpose and reward for therapists. “The clinicians have said to me, you know, basically it’s the highlight of their week.” (Manager 4) Further,
There’s a real sense of community in the intervention, then those little communities that you’re developing with each of the children and the mums. You know, there’s that sense that they’re finding it valuable, you know, that kind of sense that they’re feeling – these children are feeling more able to talk and mums, even amidst all the other demands they’ve got, are being able to show up. There’s something valuable that they seem to be getting out of it, which I think is very rewarding. (Manager 4)
Well, personally I think it’s an excellent model that sits very well with the work that we do. I’m a bit surprised why it has not been used more widely, maybe because of the resource-intensive nature of the work. (Manager 6)
Therapists were optimistic about CPP positively impacting children’s mental health and the impacts this would have across their lifespan. By addressing children’s mental health needs they are potentially dealing with trauma whereas if they did not access therapy, this trauma might manifest as they age.
I have trained in a lot of different therapeutic programs and to me, CPP – if I could only do one therapy with anyone and everyone, I would only do CPP because it just – it has the biggest ability, capacity, significance in changing within children … (Therapist 4)
Addressing child mental health was important to therapists and managers who were frustrated at times at the lack of early intervention work they could offer in their organisation. CPP filled this void.
… having worked in this area and in this region. There are so many children and young people that we see and come across and we go back to their files, and we look at when was the first time that they were referred or when did the difficulties start. It all points to the early years and so it’s overwhelming the evidence. The fact that we don’t do much about it when it’s needed, but when we try to intervene later on in life, the trauma that has already occurred is probably not addressed. (Manager 6)
One therapist felt CPP was a challenging intervention to offer for those who have less experience and suggested it should be a model that is only offered to experienced clinicians.
So I think it’s more probably a model that should be offered to senior clinicians especially clinicians that have had either experience or training in infant mental health or perinatal infant mental health. Or, therapy looking at reunification of parents and children that have been separated after child protection concerns. So yeah, I think it should be saved and targeted for those kinds of clinicians or therapists rather than a kind of generalist therapeutic model. (Therapist, 8)
CPP has been criticised in the past for its intensity and the time commitment and potential length of the intervention. One therapist felt this model of delivery was justified.
… the baby can’t wait and that mum – if we focus on mum’s therapeutic intervention, you know, the baby’s developmental processes are so much quicker than the mother’s that, you know, they will have developed post-traumatic stress disordered symptoms and difficulties and emotional dysregulation, so we can’t wait to treat the mother’s symptoms in order to treat the baby’s … The length is necessary and the intensity is necessary because the baby can’t wait. I actually feel quite good about that and the rationale for that, and why that length and intensity is required. I think that the families really benefit from that very close and caring relationship with someone who helps them think about their relationship and their baby and their mother in a different way. (Therapist 11)
Acceptability of CPP for children
Therapists and managers were positive about the acceptability of CPP for children. They noted that children were engaged in the program and at times they saw rapid improvements in a child’s mental health. Although a positive outcome for children, the process of healing could be difficult. One therapist noted CPP brings up issues that children have likely been encouraged to ignore or forget, and so it is a new experience to address this trauma.
I think they come and play but I think it’s hard as well because CPP speaks the unspeakable and we don’t kind of shy away from that. What I’ve noticed is a lot of those kids, people outside of the therapy room probably avoid talking about dad and so initially they’re quite surprised when we raise him and pretty quickly and when we continue that conversation. (Therapist 10)
However, others described the process as a positive experience for children, who would often drive the change required in the dyad’s relationship.
Some of them [the children] are just hanging out to have these conversations with their parents, and to be understood in a different way, like they usually come into appointments I guess and have their parents talk about them, and all their problems … (Therapist 2)
To engage with the child, therapists build a relationship with the mother. In particular, at the initial stages, the child may not be present so that the therapist is able to assess the needs of the mother and child through intensive sessions with the mother. Once that has been established, the therapist can then build a rapport with the child. “You walk into that waiting room and they’re excited to come in.” (Therapist 1)
Initially, some mothers thought their children did not need the program. Mothers regularly hoped that their children did not remember the family violence and were minimally impacted. However, “kids always remember more than what the mum would like them to or thought they were exposed to” (Therapist, 10). For some mothers, this was “confronting”, although the program allowed for a safe space where children could explore what they had experienced. For example,
I’ve been working with her [the mother] and her little boy for over a year now, and in the session just last week, he was raising this incident, and he knew that it was safe to raise, and he knew that his mum was supportive enough that he could raise it, and we could help him to talk about what he needed to talk about, which was his memory of this really frightening thing, and just how confusing this was for him … He was able to talk about this incident, in a lot of detail, that the mum and I were able to support him to slow down, to feel really safe. So he wanted to tell his story, but he knew that it was scary to talk about, so he and his little sister cuddled up on mum’s knee, and they all kind of did what they needed to feel safe and secure with each other, and to just visit this memory for a very short time, which was really upsetting; and talk about it, and then to be supported to feel safe again in the moment, and knowing that we can keep talking about it, that you know, we can do so together in a way that he’ll feel safe and supported, and not overwhelmed and re-traumatised … CPP is a beautiful intervention, in its ability to do that. (Therapist 6)
Although processing traumatic experiences may be distressing and confronting at times, CPP is a treatment that privileges hope and is led by the spontaneity of the child. CPP treatment experiences therefore can also be fun. Children reportedly enjoyed attending the intervention because of the focus on play.
The kids I see, they really love it. You know, that time of having time with their mum, where … you know, the session is that she speaks their language, in a way … through play, and also through language that’s connected to the playing. You know, it’s a time that’s for them, and so children love coming to the sessions. (Therapist 6)
In this environment, children are able to open up about their experiences. “I just find it gobsmacking how the children will respond if there’s an opportunity for them to be heard and be respected and know that their view is important.” (Therapist 7)
Mothers’ reports on children’s experiences
Activities initiated by the therapists allowed for children to express themselves via play, for example, how they felt about the violence they had seen and experienced. The mothers reported that their children’s behaviour generally improved both in public and in private, such as in behaviour and communication skills and the ability to identify and acknowledge their emotions.
… when she got comfortable and she started connecting to the dolls and she would act things out or draw pictures and say how she’d felt. I knew that was a turning point because she’s actually expressing herself instead of trying to hide it away. (Mother 4)
Those participants who managed to attend five or more sessions, especially those who attended for more than a few months, really saw the positive impact the program had on their children. “I think probably the most helpful thing for her [the child] was to express how she was feeling.” (Mother 3)
One woman spoke of her concerns with co-parenting and the impact this could have on her and her child’s recovery:
She’s very traumatised by all of this stuff and then the courts have gone and said, “Well 50/50 share with all parents, he deserves to be a dad”, even though the majority of the issues he’s caused. (Mother 8)
For those children that did not attend many sessions, mothers reported little improvement even if they thought their child enjoyed the experience with the therapist. This occurred in a rural setting without existing structures to support staff development, and mothers acknowledged it was most likely because they did not attend enough sessions for the program to have a long-term impact.
I think they were happy enough to be there. I don’t know exactly how much they took out of it. Obviously, we didn’t go enough times for them to have a great benefit from it. (Mother 7)
Implementing CPP
- What are the barriers and facilitators to the implementation of the CPP model into services?
In this study, we used NPT (May & Finch, 2009) as a guide to understand the barriers and facilitators to implementing CPP for dyads exposed to family violence across the many different clinical contexts. NPT is a behaviour-based theory that can be used to describe the actions or work required to implement and normalise new clinical practices in complex settings. The theory can be used in research design, data analysis or to support reporting (Hooker & Taft, 2016). The four core NPT principles or constructs provide a framework to understanding implementation processes, barriers and enablers and the work required to implement and sustain programs. Table 3 outlines in further detail the NPT principles and their application to the RECOVER project.
Table 3: Normalisation process theory and application to RECOVER
NPT construct
Examples of construct in
the clinical context
Identified implementation
barriers and enablers
Coherence
(sense-making work)
- Do individual participants see the need, benefit, value and importance of CPP?
- How do therapists make sense of the CPP work required?
Barriers:
- time of major organisational change and reforms
Enablers:
- Previous work with infants and young children
- when client need is evident
- family violence knowledge and skill
Cognitive participation (participation work)
- How do participants engage in the work?
- Are therapists using CPP resources and are they worthwhile?
- Is there evidence of commitment and continued support?
Barriers:
- workloads
- limited knowledge and skills
- structural barriers e.g. triage systems
- strict eligibility criteria
- COVID-19 pandemic
Enablers:
- Practice champions
- CPP training
- therapists seeing a change in dyads
- belief in the intervention
- CPP research tools
Collective action (operational work)
- Is there evidence of investment?
- Are therapists able to enact the intervention and its components in practice?
- What is the functionality of and relationship between the teams and DV services?
- How is the CPP work resourced, funded and supported by the organisation?
Barriers:
- few links and relationships with FV services
- lack of leadership/support
- structural barriers – lack of service equity for <5 years
- service funding
- access to trained therapists/movement of staff
Enablers:
- clinical governance and policy
- support for therapists and clients
- survey tools
- established therapeutic services/co-located hubs
Reflexive monitoring (appraisal work)
- How is CPP work monitored/reflected on?
- Is there monitoring of CPP work in meetings?
Barriers:
- structural barriers – small teams/services
Enablers:
- Fidelity logbooks
- CPP training and clinical supervision
Understanding CPP and family violence work (coherence)
Although all RECOVER therapists needed to be CPP trained or in training, the level of clinical experience varied across provider groups. Therapists who had existing experience in psychotherapy with young children were able to implement the program with more ease than those less experienced:
I think that for those people that already had existing expertise in that area, it’s been pretty easy, implementation, compared to those that were not familiar to talking to babies or young children or working in relationships. Also, in a family violence population, which has additional kinds of sensitivities, even to working with mums that may judge themselves, but when there’s family violence in the background, there’s extra difficulty. (Manager 4)
The workforce experience of CPP training to be able to deliver the intervention was met with positivity overall: “[The training is] one of the best training [programs] I’ve ever done and I feel like I’ve got a clear understanding of the model and how to do the therapy.” (Therapist 8)
Managers noted difficulty in their role managing staff if they as managers were not trained in CPP themselves.
I don’t really have a strong understanding of CPP but I’m the person responsible for making decisions around accepting referrals and you know talking with clinicians about the decisions that we make in terms of intervention. So, I think it would be helpful for team leaders and people supervising clinicians to have had the training or some more knowledge in CPP. (Manager ٢)
Therapists’ earlier training impacted how they approached the work and their level of confidence. Regardless of whether they were new to this model or had some previous dyad therapist training, their understanding of the work evolved over the length of the training.
Some therapists, including those working in child mental health services, did not have previous family violence education or the management skills to deal with adult women and the children affected by the abuse. Supportive systems were lacking to even identify those clients entering the service who were experiencing family violence.
I guess domestic violence has always been around but it’s not necessarily something that tertiary mental health services have necessarily thought about in terms of risk before either. (Therapist 1)
Recruitment coincided with a time of significant change and restructure for some organisations, notably changes due to the Royal Commission into Family Violence. Therapists were dealing with multiple system reforms and the piloting of other therapeutic treatment programs. Some therapists were involved in the delivery of multiple interventions or styles of therapy, in addition to CPP. For some, this was positive: “I think there’s massive overlap in a good way. I think the model and the approach is really relevant for the families that we are seeing.” (Therapist ١٠) Others found that engaging in multiple interventions made it difficult to learn and apply another intervention and could create confusion.
I think they have an understanding of it but I think they would probably consistently report to me that they want more, they want more [from the trainer], they want more exposure to [CPP]. (Therapist 10)
Clinicians struggled particularly in learning the model of CPP when situated in settings without adequate clinical governance structures. One participant discussed how her understanding improved once she had weekly supervision.
I think it’s improved. So I have regular supervision now. I’m getting weekly supervision now, and I’ve only had that for probably about six weeks. Seven weeks. And prior to that, I didn’t really get supervision, so I struggled with … I think I struggled with an understanding of CPP. (Therapist 9)
The CPP work appeared to be highly valued by therapists on the ground and to some extent the management structures. However, major changes to the organisational structure at one large urban site and the uncertainty of future program funding may have impacted on therapist investment and CPP engagement.
… it is unclear to what extent CPP will be taken up by the organisation in future. There remain key individuals that encourage involvement, however, most are on contracts ending soon. (Manager 4)
CPP participation and engagement (cognitive participation)
Therapists were generally highly engaged in the intervention. However, organisations that were able to support therapists, due to being a larger organisation or having supportive systems and adequate funding, saw staff with higher levels of engagement. This was particularly so at sites with a CPP practice champion, who promoted the CPP work and provided encouragement and support with recruitment queries, risk assessments and data collection.
When therapists observed positive changes in dyads, this encouraged engagement with the CPP work and organisational support for the model.
I was already able to see this mum thinking about and making connections between the child’s behaviour and their experiences and that was in the first session. So that was really good. (Therapist 1)
Aspects of the RECOVER eligibility criteria caused problems for some sites. Needing to recruit biological mothers limited those services that worked with children within the child protection system, not infrequently in the care of an alternative family member or foster carer. Also, in some cases of family violence, the mother had been murdered. Therapists noted that they used the principles of CPP in these cases, but they were not formally included in the RECOVER study. Similarly, requirements for the mother to have left the perpetrator were at times found to be unrealistic and not reflective of cycles of couple/family separation and repartnering.
In addition, the need to include pre-school-aged children was problematic for CAMHS. Child mental health services with clinical triage systems that prioritised certain client groups hampered recruitment and engagement with the intervention. When an older child presents in crisis, with more obvious signs of trauma, they tend to be triaged over a younger child, whose trauma may not be as recognisable to those without training in this area.
So it’s definitely not just adolescents. We’re getting eight- and nine-year-olds absconding from school and refusing school, and threatening suicide and self-harm as well. (Therapist 2)
This structural barrier to the recruitment of young children resulted in very few dyads recruited from the five CAMHS clinical sites. Additional structural barriers in CAMHS included a prior lack of family violence awareness in clients referred to the service, which prevented the identification of eligible dyads for the study. This was resolved over the life of the project.
Well, I think one of the major things has been that it has made us a whole lot more aware of family violence in our referrals. So we are now flagging with every single case and asking the question with every single case about family violence. And it’s really surprised me and a number on the team just – it’s almost every referral has some form of family violence involved with it. And that’s from the project, I think we’ve all just become much more aware of making sure yeah. (Manager 1)
Some clients wanted the father to be involved, however, fathers were not active participants in the study. “Some clients that would be ideal for CPP but it’s the dad, the dad’s the safe caregiver rather than the mum. The mum is not the perpetrator, it’s mum’s new boyfriend, but yes that gender thing as well.” (Therapist, 9)
A major barrier for therapists was excess workload and the crisis-driven nature of the clinical work.
… it’s across the board with our adolescents and all sorts of kids that are needing extra support. So our crisis presentations are the most heavy coming in, so I guess the ability to address those is priority. (Therapist 2)
Therapists at some sites were involved in multiple therapeutic modalities and had heavy caseloads.
Yeah. I mean I wonder whether as a team – because we’re learning in EMDR [eye movement desensitisation and reprocessing] and CPP and we’re trying to recruit clients for both, and work out which kids would be – and mum – would be suitable for which one. Whether if we were just doing CPP, whether we might have got more referrals for CPP, and been able to recruit more in. (Therapist 9)
The intervention is intensive, involving a substantial commitment to the client as well as commitments to weekly supervision. On top of this, therapists must adhere to the model itself which can take time to master. However, while this was an issue for some therapists, others found that CPP did fit into their workload. For example, when one therapist was asked, “How easy has it been to include CPP into your workload?” she simply replied, “Easy” (Therapist ٧).
In the later stages of the study, the COVID-19 pandemic caused further demands on services and interrupted service delivery to dyads, who spoke about the limitations of CPP via telehealth modalities. One mother called the impacts of COVID-19 “disastrous” (Mother 12). She explained that her child had started to open up in the sessions before COVID-19. The change to telehealth hindered the progress they had made. Difficulties included engaging the child to use the online modality, and setting up the lounge room to mirror the therapy space. At the end of the session, after working through some difficult topics, she would then have no reprieve or ability to change scenery, out of the new therapy space. However, due to the strong bond her child had with the therapist, they did still make some progress via telehealth.
While there were some issues incorporating CPP into organisations, over the length of the pilot, many of these issues were dealt with.
I guess we’ve been able to overcome that barrier because it’s a modality [CPP] that we see really help some clients and really works and we’ve been able to utilise it, you know, in our program very easily really. (Therapist 6)
How does the CPP work get done (collective action)?
The CPP resources and CPP training were valued by therapists, enhancing the operationalisation of the clinical work. In addition, the fidelity logbooks and other research tools aided adherence to CPP objectives.
The CPP resource manual provided therapists with the confidence and skill set to offer CPP.
The manual, Don’t Hit My Mummy, is very explicit about what skills you need to bring to it and how that looks in the room and what a port of entry is and how you intervene, so I think that I’ve learnt a huge amount in a fairly short space of time. (Therapist 11)
I use the manual a bit, when I’m working out what to do next I do look at the manual and use that, and the fidelity measures are quite good because they prompt you to make sure that you’re doing particular things through the different phases. (Therapist 2)
Outcome measure assessments as part of the RECOVER project supported therapists’ learning and guided their practice.
So I personally think it’s great. It’s got those parent–child observations in there and I do find the responses in the questionnaires helpful to kind of aid my understanding of where mum’s at and their understanding of the child and the difficulties. (Therapist, 10)
There were some difficulties for therapists in the smaller rural settings to engage in the intervention. Factors included rural therapists having less psychotherapy knowledge and skills and so they were being presented with new learning challenges. Rural therapists noted that travelling to the city for training could be difficult and was time-consuming. Lack of qualified staff was an issue for recruitment, and this was particularly heightened in rural areas. Larger urban organisations had greater funding and a range of therapists, and could train more senior and experienced staff.
I would say, the main issue is those folk in rural areas, that don’t have that additional kind of level of experience in working with infants and young children, have found it harder to engage and retain their – I think they’ve found it harder to engage and hold onto some of the clients that are coming through. I think it’s been harder for them, and also to recruit the dyads needed for the study. So, I think that’s about confidence. (Manager 4)
Rural workloads prevented extensive networking and promotion of the new therapy on offer.
I think management are a bit wary about going out and talking about what we do, just because the number of referrals is already way too overwhelming, and we don’t really want to be going out and drumming up any more work, I think that’s part of it. (Therapist 2)
One organisation created a specific role to link the services for childhood with family violence workers. Due to the connection already between the two areas in the organisation, CPP integrated seamlessly. However, inter-sector collaboration was restricted in rural areas. This interrupted referral pathways and, in particular, the offering of secondary support from family violence services to CAMHS.
I kind of thought that would be really different in the country, but my experience is agencies tend to work in silos more at times. So there’s not that collaborative approach or referrals that I would have expected coming in. (Therapist 9)
As mentioned above, the education levels and skills of the CPP therapists varied, with a variety of undergraduate professional qualifications. There was some concern from both therapists and managers about staff ability to work with young children. It was noted that the CPP model had excellent training and clear guidelines, which assisted the therapists.
It has given them the confidence to work with this age group. They had no prior experience with working with the under-fives and having gone through the training, I think it has been an important exercise in building capacity in the absence of any other training available in Australia that CAMHS can do that at this stage. (Manager 6)
All RECOVER therapists were trained or completing training in CPP. The training was met with an overwhelmingly positive response. “I think CPP – as a whole the training in CPP has been fantastic.” (Manager 6) Therapists also felt that the training was something that should be taken up by other clinicians. “I’d definitely recommend it to anyone, it’s a fantastic opportunity.” (Therapist 2)
Therapists found that the training was useful not only for learning CPP but also across their practice. While some therapists enjoyed the length of training, others found that it was burdensome alongside their busy workloads. Response to the CPP training and its application appeared to reflect the individual therapist’s background, as those who had a background in psychotherapy or infant training found they could understand and apply the techniques better than those who had no prior knowledge. Therapists were also applying the model as they continued through the training. Those with a clearer understanding of the training concepts were able to apply the model and therefore became proficient much more quickly. Therefore, they gained more experience, and the divide grew between those therapists and the therapists who did not have a psychotherapy background.
While different levels of experience could make CPP training difficult for some therapists, for others this was a welcome addition to their practice. For example, one manager noted that a particular therapist did not have extensive clinical mental health experience or child mental health experience. The training thus
[gave] her that kind of framework for working with those real young ones and the training and knowledge that you don’t get normally from doing short workshops. Like it’s been quite amazing to think that she is now in this position where she’s providing amazing intervention for these families. (Manager 1).
The ongoing training was also seen as positive, as therapists could bring questions they had to the group and discuss them each month. Therapists reported that they enjoyed the face-to-face teaching days and having this interactive learning with one another. Also, the teaching videos made by the CPP international trainer practising and modelling CPP with clients were singled out as positive learning tools. This training and organisational investment is needed to maintain the delivery of CPP. In this study, most organisations were very supportive of the project and happy to be offering CPP to clients.
I haven’t got enough people trained for sustainability, and I don’t want this investment that we’ve made to fall away. I think it’s been an important, valuable investment, but we absolutely need to invest further, to make the most of what we’ve already invested. So I probably need to train double what I’ve already trained, at least. Because obviously, you lose people, as well. (Manager 8)
Ongoing appraisal of CPP (reflexive monitoring)
All therapists offering CPP were accustomed to receiving clinical supervision and reflecting on cases and their practice. The fidelity logbook enhanced reflection, providing a practical tool to learn from and to support practice.
So I think even the nature of doing the logbook after each session, it kind of does keep you quite accountable and in the fidelity core intervention for the training, those headings that are in the logbook are expanded upon. (Therapist 10)
Staff also reflected on vicarious trauma and how this affected their work. While this might be something that therapists discuss in supervision, for some this was a more personal process. “I think that has to be something that’s more personal and separate to what would be provided at work.” (Therapist, 2) Peer discussions were viewed positively. These allowed therapists to discuss implementation issues and strategies. It also allowed staff to offer support to one another. Managers noted how positive this was and that in the future they would, ideally, have larger numbers of staff trained and delivering the program so there was a network of support.
It’s such a delight and privilege to be able to spend dedicated reflective time and [have] that built into a model where you can just really do deep dives into thinking about the experiences of children and women and also how we as clinicians get in the way and can get better and to foster that environment. (Manager 4)
Summary of implementation
The introduction of new clinical practices can be challenging. As outlined in this report there were many barriers outlined in participants’ responses to embedding CPP into their routines. Factors that enabled and challenged the implementation of CPP are as follows.
2. Do CPP therapists-in-training adhere to CPP model fidelity?
For each session, therapists completed a structured fidelity logbook assessing adherence to 17 CPP objectives according to the CPP manual and training (Lieberman, Ghosh Ippen et al., 2015). Responses to the items were made on a 0- to 3-point scale, with 3 indicating the highest level of adherence or satisfaction and 0 indicating no adherence. All eight therapists who provided CPP and treated RECOVER dyads completed logbooks, with data collated as the proportion of therapists adhering to CPP goals. Over 293 sessions, CPP therapists rated their own fidelity to the intervention as described in Table 4. Their rating of fidelity to CPP goals shows strong perceived adherence to most goals, especially conveying hope, developing relationships and enhancing safety, but less focus in other areas (in bold in Table 4). This included care coordination, supporting the child’s relationship with others and helping the dyad put the trauma into perspective. Adherence was greatest in conveying a sense of hope and developing a relationship with the dyad. Enhancement of safety in therapy was also high. Urban sites reported greater fidelity and adherence to all CPP objectives compared to rural and small services.
Table 4: Rates of adherence to CPP objectives (fidelity logbooks) reported by therapists (n=293)
CPP objectivesa
0–1 = No or low (%)
2 = moderate (%)
3 = significant (%)
1. Convey a sense of hope
6
30
64
2. Develop empathic relationship with family members
7
28
65
3. Enhance physical safety
24
39
37
4. Enhance safety – stabilisation (basic needs)
21
40
39
5. Enhance safety and consistency in therapy
10
28
62
6. Enhance safety within dyad relationship
11
35
54
7. Promote emotional reciprocity between mother and child
15
32
53
8. Coordinate care
37
43
20
9. Strengthen dyadic affect regulation capacity
24
31
45
10. Strengthen dyadic body-based regulation
25
39
36
11. Support child’s relationship with other important caregivers
31
43
26
12. Enhance understanding of the meaning of behaviour
11
31
58
13. Support child in returning to a normal developmental trajectory
20
30
50
14. Normalise the traumatic response
14
31
55
15. Support dyads in acknowledging the impact of trauma
22
28
50
16. Help dyad differentiate between then and now
25
29
46
17. Help dyad put the traumatic experience in perspective
26
29
45
a For CPP objectives, see pp. 215–223, 279–283 of the CPP manual (Lieberman, Ghosh Ippen et al., 2015).
Intervention dose
The length of each CPP treatment and intervention phase is flexible and depends on clinical assessment and dyad needs. Four dyads (27%) received a brief intervention (<10 sessions), and six dyads (40%) received a moderate dose (12 to 28 sessions). The remaining five dyads (33%) received more than 30 sessions, with one of these families receiving 50 treatment episodes over 18 months. The median number of sessions across all dyads was 23 (range 5 to 50) or less than six months of treatment time.
3. How effective is treatment by CPP therapists-in-training during the study?
Dyad characteristics
In this pilot, 18 families consented to CPP treatment and participation in the RECOVER study. Three dyads disengaged from the service before treatment began. Women who completed the T1 survey (n=15) were on average 34 years old. Children (n=15) were around four years of age
(Table 5). Forty per cent of women who completed the baseline survey were separated from their partners, 53 per cent were not working in a paid job, and 60 per cent were on a pension. No women were Aboriginal and/or Torres Strait Islander, and all were Australian born. Two women were from rural Victoria and the remaining 13 were from urban settings. As expected, all women reported substantial IPV from a male perpetrator.
Table 5: Participant characteristics (T1; n=15)
Children
Category
Characteristic
%
Mean age
(months; SD)
49.5 (13.5)
Gender
Male
53.0
Female
47.0
Mothers
Category
Characteristic
%
Mean age
(years; SD)
34.3 (6.3)
Birthplace
Australian born
100.0
Aboriginal and/or Torres Strait Islander
No
100.0
Marital status
Married
13.3
Living with partner
6.7
Have a partner but do not live together
26.7
Separated or divorced
40.0
Single
13.3
Highest level of education
Degree/higher degree
26.7
Diploma/apprenticeship
26.7
Completed secondary school to Year 12
26.6
Did not finish secondary school
20.0
Employment
Paid job
46.7
Not working in a paid job at the moment
53.3
Income source
Wages or salary
40.0
Pension or benefit
60.0
Health Care Card (low income)
Yes
80.0
Family income (AUD) before tax
<$800 per week
60.0
$800 to $1,900 per week
33.0
>$2,000 per week
7.0
Intimate partner violence
Definite IPV (CASR-SF ≥ 7)
100
Attrition and missing data
Table 6 outlines a comparison of baseline outcome scores between complete and attrited cases. No significant differences were seen between the two groups. Fifteen families (83.3%) completed a survey at baseline (T1) and 10 of these families (56%) completed surveys with matched data at T1 and either T2 or T3 time points. Missing survey data were less than 10 per cent and so this complete case data set (n=10) was used in the final data analysis. The small sample size reduces the statistical power to make meaningful conclusions from the quantitative data and as such we do not claim or conclude study effectiveness.
The quality of dyad free-play recordings (to assess mother–child relationships) varied greatly, with 13 recordings captured by therapists at T1 but only four dyad interactions captured at T1 and either T2 or T3. The latter four were used in the pre–post analysis (Table 7). The consistency of decision-making between coders was substantial (Cohen’s kappa=0.69).
Table 6: Attrition data and study variables of completed and attrited dyads
Phase
n
% attrition
Comment
Dyads consented to treatment
18
N/A
N/A
CPP assessment phase
3
17
Note: 2 of the 3 mothers did not complete the baseline survey
CPP foundation/core phase
5
28
All completed baseline survey
Mothers
Study outcomes at baseline
Completed (n=10) – Median (95% CI)a
Completed (n=10) – Range
Not completed (n=5) – Median (95% CI)a
Not completed (n=5) – Range
p-valueb
Global Severity Index (SCL-90-R)
2.17 (1.82 – 2.52)
1.30 – 2.79
2.13 (1.40 – 2.86)
1.04 – 2.38
0.423
PTSD Symptoms Scale–Interview
23.50 (15.94 – 31.06)
17.0 – 45.0
30.50 (18.95 – 42.05)
19.0 – 36.0
0.327
Composite Abuse Scale (CASR-SF)
24.0 (13.26 – 34.74)
0 – 52.0
28.00 (0.34 – 55.66)
0 – 36.0
0.423
Parenting
Study variables
Mean
SD
Mean
SD
p-valueb
Parenting self-efficacy
3.20 (2.39 – 4.01)
1.13
2.80 (2.24 – 3.56)
0.45
0.474
Parenting consistency
3.40 (3.17 – 3.63)
0.98
3.45 (2.78 – 4.12)
0.54
0.821
Parenting irritability
4.28 (2.35 – 6.21)
2.69
2.5 (1.67 – 3.33)
0.67
0.176
Parenting warmth
4.35 (3.98 – 4.72)
0.51
4.47 (4.13 – 4.81)
0.27
0.642
Child
Study variables
Mean
SD
Mean
SD
p-valueb
Total difficulties score (SDQ)
17.7 (13.32 – 22.08)
6.13
17.0 (10.61 – 23.39)
5.15
0.830
Young Child PTSD Checklist (YCPC) – PTSD symptoms
51.10 (41.56 – 60.64)
13.34
52.20 (29.67 – 74.73)
18.14
0.895
Young Child PTSD Checklist (YCPC) – Functional impairment
13.60 (10.12 – 17.08)
4.86
15.80 (7.27 – 24.33)
6.87
0.482
Mother–child relationship
Study variables – Parental Reflective Functioning (PRFQ)
Mean
SD
Mean
SD
p-valueb
Pre-mentalising
1.79 (1.35 – 2.22)
0.61
1.83 (1.10 – 2.64)
0.66
0.893
Certainty about mental states
3.78 (3.14 – 4.43)
0.90
4.00 (3.26 – 4.74)
0.60
0.638
Interest and curiosity
6.27 (5.88 – 6.66)
0.54
6.29 (5.82 – 6.76)
0.38
0.940
a 95% confidence interval.
b Nonparametric (Mann-Whitney U test) used for unevenly distributed data.
Baseline or T1 scores indicate that dyads were experiencing major mental health and trauma symptoms and parenting distress (Table 7).
The Global Severity Index, an indicator of overall maternal psychological distress, has a cut-off score of >1 (Olsen et al., 2006) to indicate severe distress. All women had scores well above this clinical cut-off at baseline and post treatment (100%). The PTSD Symptoms Scale Interview cut-off for a diagnosis of maternal PTSD is >23 (Foa et al., 2016). Over half of the sample had scores above this cut-off at baseline, which reduced to 40 per cent post-treatment. Scores did improve after treatment on all maternal mental health indicators but most variables did not significantly differ on statistical analysis between data collection time points. It is unclear why these mental health and trauma symptoms failed to change, however women did continue to experience violence from partners during the treatment which may have impacted on their mental health and wellbeing.
Parenting scores improved on most indicators post treatment –significantly so for enhanced parental warmth (p<0.028), but not for other parenting items: self-efficacy, consistency or irritability. Parental affection and feelings of closeness to the child may have altered over the dyadic treatment as CPP has a focus on enhancing parent understanding of the impact of violence on the child’s emotional health and behaviour. Parental warmth has also been demonstrated as a benefit of CPP (Chu et al., 2021; Guild et al., 2021) and other relevant IPV and parenting programs (Sousa et al., 2021).
Reduced IPV exposure was reported post treatment (p<0.029) on the short-form revised CAS. The higher the CAS score, the more IPV experienced. The high CAS scores reported here are to be expected for this population, as the CAS measures partner abuse in the past 12 months. At T1, this captures the significant violence women experienced while still living with their abusive partners. Although abuse has reduced post-treatment (when families were in safer environments), some women and almost all children were still seeing the perpetrator (co-parenting at weekends, etc.). At T3, women continue to report high rates of IPV (Table 7).
Children’s SDQ total difficulties score (combined emotional, conduct, peer and hyperactivity problems) reduced from a mean of 17.7 at T1 to 11.40 at T3 (p<0.005), indicating a significant reduction in child emotional and behavioural difficulties. Up to 80 per cent of children presented with high scores on the parent report SDQ, well above the 12 cut-off score for this age group. This proportion reduced to 50 per cent post-treatment, a clinically relevant change. Probable cut-off scores for the YCPC indicated that 90 per cent of children had probable PTSD (≥ 26 for PTSD symptoms, ≥ 4 for functioning) on beginning treatment which did not change post-CPP. While planned, we were unable to assess the impact of shorter versus longer term CPP treatment due to the small number of dyads included. The small sample size in this study is a limitation and prevents any claim of treatment efficacy, however, shifts in the desired direction can be seen across most mental health/trauma, parenting and relationship outcomes (Table 7).
Table 7: Pre- and post-CPP comparison of study variables: Complete cases (n=10)
Mothers
Study variables
Baseline CPP (T1) – Median (95% CI)a
Baseline CPP (T1) – Range
Post CPP (T3) – Median
(95% CI)a
Post CPP (T3) – Range
Diff (T3 – T1)
p-valuesb
Global Severity Index (SCL-90-R)
2.17 (1.82 – 2.52)
1.30 – 2.79
1.76 (1.24 – 2.28)
1.20 – 3.14
-0.41
0.307
PTSD Symptoms Scale–Interview (PSSI)
23.50 (15.94 – 31.06)
17.0 – 45.0
18.00 (10.16 – 25.84)
2.0 – 36.0
-5.50
0.091
Composite Abuse Scale (CASR-SF)
24.00 (13.26 – 34.74)
0.0 – 52.0
6.50 (0.42 – 12.58)
0.0 – 28.0
-16.1
0.029
Parenting
Study variables
Baseline CPP (T1) – Mean (95% CI)a
Baseline CPP (T1) – SD
Post CPP (T3) – Mean
(95% CI)a
Post CPP (T3) – SD
Diff (T3 – T1)
p-valuesb
Parenting self-efficacy
3.20 (2.39 – 4.01)
1.13
3.60 (2.83 – 4.37)
1.07
0.40
0.269
Parenting consistency
3.40 (3.17 – 3.63)
0.98
3.10 (2.72 – 3.48)
1.44
-0.30
0.181
Parenting irritability
4.28 (2.35 – 6.21)
2.69
3.32 (1.90 – 4.74)
1.98
-0.96
0.252
Parenting warmth
4.35 (3.98 – 4.72)
0.51
4.67 (4.41 – 4.92)
0.36
0.32
0.028
Child
Study variables
Baseline CPP (T1) – Mean (95% CI)a
Baseline CPP (T1) – SD
Post CPP (T3) – Mean
(95% CI)a
Post CPP (T3) – SD
Diff (T3 – T1)
p-valuesb
Total difficulties score (SDQ)
17.7 (13.32 – 22.08)
6.13
11.40 (7.21 – 15.59)
5.85
-6.30
0.005
Young Child PTSD Checklist (YCPC) – PTSD symptoms
51.10 (41.56 – 60.64)
13.34
49.4 (40.65 – 58.15)
12.23
-1.70
0.716
Young Child PTSD Checklist (YCPC) – Functional impairment
13.60 (10.12 – 17.08)
4.86
12.1 (9.01 – 15.18)
4.31
-1.50
0.346
Mother–child relationship
Study variables – Parental Reflective Functioning (PRFQ)
Baseline CPP (T1) – Mean (95% CI)a
Baseline CPP (T1) – SD
Post CPP (T3) – Mean
(95% CI)a
Post CPP (T3) – SD
Diff (T3 – T1)
p-valuesb
Pre-mentalising
1.79 (1.35 – 2.22)
0.61
1.63 (1.11 – 2.15)
0.73
-0.16
0.603
Certainty about mental states
3.78 (3.14 – 4.43)
0.90
4.10 (3.32 – 4.88)
1.08
0.32
0.147
Interest and curiosity
6.27 (5.88 – 6.66)
0.54
6.16 (5.69 – 6.63)
0.65
-0.11
0.571
Coding of Attachment Related Parenting (CARP; n=4)
Study variables – Parental Reflective Functioning (PRFQ)
Baseline CPP (T1) – Mean (95% CI)a
Baseline CPP (T1) – SD
Post CPP (T3) – Mean
(95% CI)a
Post CPP (T3) – SD
Diff (T3 – T1)
p-valuesb
Sensitivity
6.00 (3.75 – 8.25)
1.41
6.00 (2.82 – 9.18)
2.00
0
1.0
Positive parent affect
5.50 (3.91 – 7.09)
1.00
5.25 (2.53 – 7.97)
1.71
-0.25
0.634
Positive child affect
5.25 (3.73 – 6.77)
0.96
6.00 (4.70 – 7.30)
0.82
0.75
0.266
Mutuality
5.75 (3.75 – 7.75)
1.26
6.00 (3.75 – 8.25)
1.41
0.25
0.264
a 95% Confidence Interval.
b Nonparametric (Wilcoxon signed-rank test) used for unevenly distributed data.
Other results
At the T1 and T3 surveys, women were asked if they or their child had previously had any contact with the perpetrator (Figure 3). If so, the frequency of the contact was recorded (daily/weekly/fortnightly/monthly/greater than monthly). Mothers’ contact with perpetrators reduced over time (from 80% having contact down to 70%), however for those who did have contact, the frequency of contact increased. Children increasingly had frequent contact with the person using violence.
Figure 3: Participant contact with the person using violence by time point
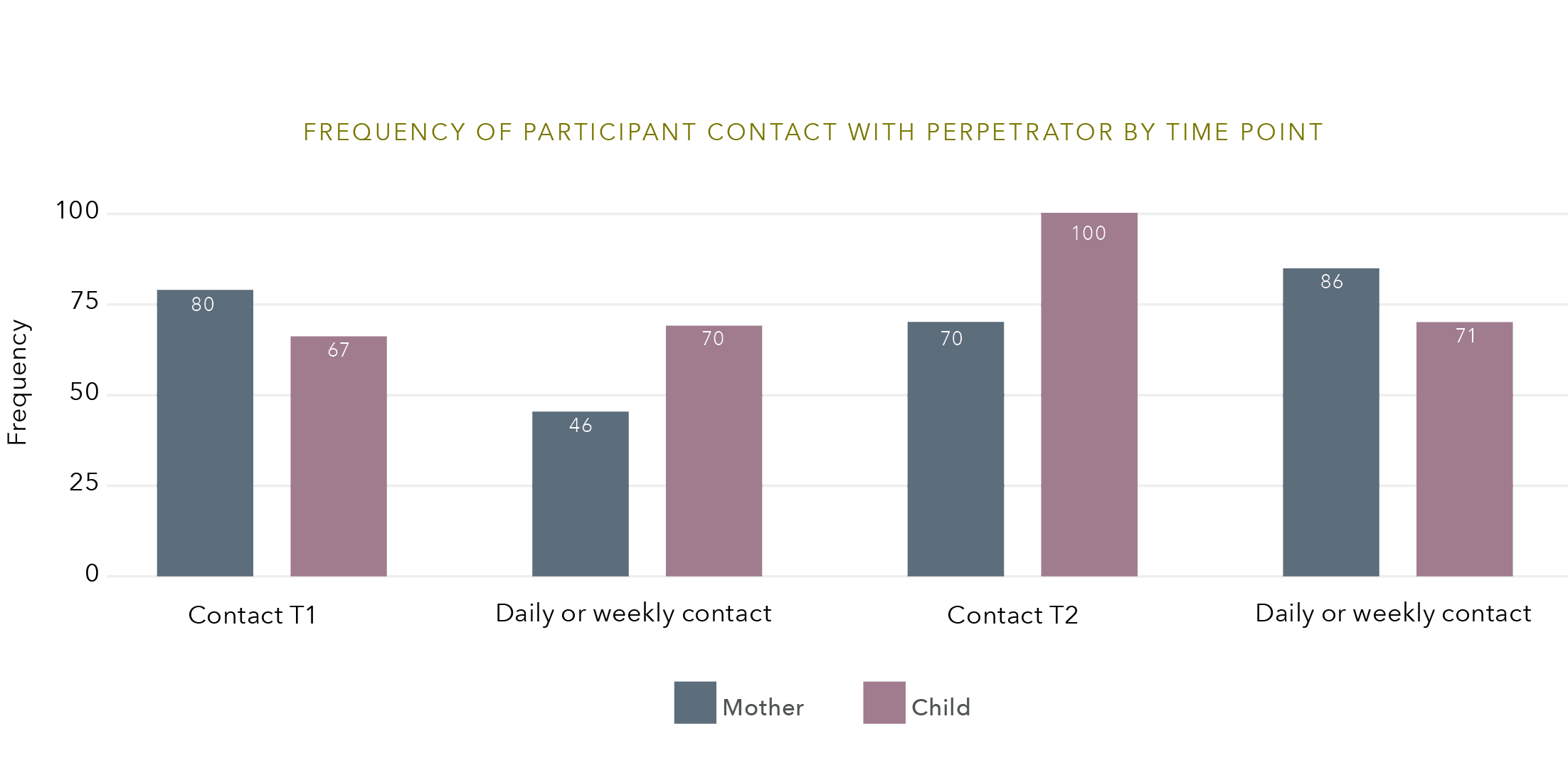
Time Point
Frequency – Mother
Frequency – Child
Contact T1
80
67
Daily or weekly contact
46
70
Contact T2
70
100
Daily or weekly contact
86
71
Costs of treatment
Most women reported minimal costs to receive CPP treatment from services (Table 8). Travel, fuel and public transport costs were the most common out-of-pocket expenses. One family received CPP from a private provider who charged professional fees.
Table 8: Costs to attend treatment each week (n=15)
By Amount per week
Amount per week (AUD)
%
Less than $50
64.3
$50 – $100
21.4
$101 – $200
14.3
>$200
0.0
By Cost Description
Cost description
%
Childcare
23.5
Travel/public transport
41.2
Loss of income
11.8
Other (e.g., parking, private treatment fees)
23.5
The CPP community of practice in Australia
Through training, peer supervision and clinical practice opportunities, this project developed and promoted a national CPP community of practice that aimed to build workforce capacity, enhance practice, and provide a vehicle for ongoing education and professional networking for those working in the field.
The RECOVER project established the CPP Australia Community of Practice (CPP AUS CoP), chaired as a collaboration between Berry Street, La Trobe University and the Australian Association for Infant Mental Health (AAIMH) South Australia. Following an initial meeting in late 2019 in Adelaide alongside the AAIMH National Conference, the CPP AUS CoP was open to 32 CPP clinicians who had completed training. Participants in attendance expressed interest in participating in a biannual CoP forum to share practice experiences and resources. With the onset of the COVID-19 pandemic in early 2020, the CPP AUS CoP held the first online forum for clinicians to share experiences of telehealth practice adaptations, followed by a forum on archetypal play with Dr Chandra Ghosh Ippen and a webinar on perinatal CPP with Dr Alicia Lieberman. CPP AUS CoP participants presented a symposium together at the 2021 World Association for Infant Mental Health (WAIMH) World Congress on local implementation innovations with CPP in Victoria and South Australia. In March 2022 another 28 clinicians across Victoria and South Australia will complete the CPP training and be invited to participate in future CPP community of practice events. Future directions include the establishment of a secure online communication resource and incorporating a yearly case-based symposium on themes of interest in CPP.
Discussion
This study examined the feasibility of implementing CPP for Australian mothers and children exposed to IPV and family violence. CPP is an evidence-based psychotherapeutic intervention for families experiencing trauma (Lieberman et al., 2015). Currently, in Australia, there is an inequity of mental health service provision for very young children (Segal et al., 2018) who are disproportionately affected by traumatic events in early life (Lieberman et al., 2011). Our state of knowledge review identified a gap in effective treatments available to young children and mothers who have experienced family violence. The high prevalence of IPV and the contributing “shadow pandemic” or increase in family violence due to COVID-19 (Pfitzner et al., 2020) means there will continue to be a high demand for relational dyadic therapies such as CPP. Factors associated with the COVID-19 pandemic such as public health measures to enforce home isolation, loss of income, greater alcohol and other drug use and worsening mental health have resulted in increased rates of all forms of violence against women, with greater calls for help (UN Women, 2020).
The RECOVER pilot of CPP in Australia, specifically for mothers and children experiencing family violence, suggests that CPP is acceptable and feasible to implement in the Australian setting, in certain locations. Factors enabling the implementation of CPP into clinical services include established family violence system partnerships, service capacity to prioritise mental health and wellbeing responses for very young children, and strong clinical governance structures.
The COVID-19 pandemic impacted aspects of recruitment late in the study and impaired CPP delivery with most therapy either put on hold or offered via telehealth, which was challenging for dyads and therapists. Staff were often moved to other acute clinical areas and client intake was restricted to crisis cases only. Evaluation of CPP delivery via telehealth is needed and guidelines for CPP delivery are currently being developed by the CPP Dissemination Team at the University of California, San Francisco (Ghosh Ippen, Chu & Lieberman, 2020).
The study was conducted at a time of significant system change across non-government and public mental health service systems in Victoria and South Australia. The timing of these reforms as well as limitations in family violence system partnerships or early childhood mental health referral pathways hindered recruitment of the target population and implementation of this intervention for that target population. This was especially pronounced in rural areas and compounded by increased service demands for older children and young people, and children in statutory care. In the face of this demand, most service sites were simply unable to prioritise young children presenting with the mental health sequelae of IPV trauma. Mental health workforce shortages were also pronounced within CAMHS but were also a feature across all rural settings. These long-standing systemic barriers to service provision earlier in life and earlier in the risk trajectory of a family have been documented elsewhere (State of Victoria, 2021).
Our RECOVER findings are consistent with other countries outside the United States that have tested CPP in their contexts (David & Schiff, 2015; Norlen et al., 2020). In Israel, feasibility research showed that aspects of the intervention, the international CPP training and organisational readiness promoted CPP implementation. Consistent with our findings, Israeli therapists were highly motivated to deliver the intervention when they observed the benefits to young children and caregivers. Limited supervision and vicarious trauma were the main inhibiting factors. Like our rural therapists, isolated or solo therapists who have limited access to established supervisory structures and work with traumatised populations may struggle to provide optimal care (McLean & McIntosh, 2021). These findings suggest that future implementation and scale-up of CPP delivery in rural areas will require planning to ensure that rural therapist selection is based on the presence of a minimum level of access to supervisory structures, and building CPP virtual teams, whereby rural therapists are partnered with other CPP therapist peers. This may be a partner in the same service, or an opportunity to partner therapists across public mental health and non-government organisations within a region. Cross-service service peer partnerships may also build collaboration between, for example, family violence and mental health service systems to support workforce retentions and wellbeing, in the service of promoting women’s and children’s safety and wellbeing.
In other CPP feasibility research, Swedish caregivers receiving CPP felt their confidence and parenting improved, with greater reflection and understanding of child behaviour and the trauma they had experienced (Norlen et al., 2020). Caregivers reported children’s enthusiasm and positive responses to treatment, indicating CPP as a helpful endeavour, even during difficult discussions. The CPP therapists were highly regarded. As we have found in RECOVER, mothers noticed significant changes in their children in terms of development and self-regulatory behaviours that enabled children to manage everyday situations (Norlen et al., 2020).
In the present study, the average duration of treatment was less than six months (median number of 23 sessions). Very little is known about how to assess which IPV-affected mother–child dyads benefit from briefer models of dyadic care, versus those dyads that may require a longer treatment. Current research evaluating a six-month course of CPP will help to clarify whether a shorter treatment course by trained CPP clinicians in established services can provide comparable positive outcomes (Cerulli et al., 2021). In the period following the conclusion of the RECOVER project, some Australian services have received ongoing funding to provide CPP for IPV-affected mother–child dyads and are delivering this as part of a tiered or stepped-care model to best target delivery to those families who can most benefit from a CPP intervention (Fogarty et al., 2021). It will be important to understand how these stepped-care models, delivered by CPP clinicians (more experienced in delivering the model), can impact on recruitment, retention and outcomes of families experiencing IPV.
In the original Lieberman et al. (2005) trial, CPP was delivered by clinicians experienced in CPP, who provided an average of 32 treatment sessions per dyad. In these circumstances, the CPP model demonstrated efficacy in child behaviour, child trauma and maternal avoidance symptoms, and most maternal and child health outcomes (Lieberman, Van Horn et al., 2005), and positive outcomes were sustained (Lieberman et al., 2006) and replicated in subsequent RCTs (Cicchetti, 1999, 2006; Toth, 2002, 2006). The RECOVER study was delivered by therapists learning the CPP model who provided an average of 23 treatment sessions per dyad. Although no significant changes were seen across several treatment domains, it is interesting to note that, given the limitations in session number and CPP experience level, there were still positive trends observed across most treatment outcomes. Positive outcomes in child emotions and behaviour and parental warmth were also observed, consistent with the original Lieberman et al. trial (2015) and other CPP studies. In the present study these quantitative outcomes were reinforced by complementary qualitative reports from women and therapists.
Most children involved in this study continued to be parented by multiple parents or caregivers, including fathers who had used violence, indicating a need for fathers to be safely offered CPP treatment with their child. Although fathers were included in treatment consent conversations, they were not included in the RECOVER intervention. Fathers’ participation in their children’s treatment, where safe, could be considered to improve father and child wellbeing outcomes (Groves et al., 2007; Iwaoka-Scott et al., 2015; Mohaupt et al., 2020). Given that CPP treatment delivery offers a pragmatic and careful risk assessment and intervention approach by clinicians skilled in engaging children and caregivers together, future CPP delivery could be expanded to include fathers who have previously used violence and wish to change, if sufficient supervision, organisational partnerships and support structures were built (Groves et al., 2007; Toone, 2018).
Our finding that women reported a reduction in IPV during treatment is new and has not been measured before in RCTs or other feasibility studies. In one instance, Lieberman, Diaz et al. (2011) completed chart audits within a study of perinatal CPP which revealed no further incidence of IPV post-treatment. Our small sample limits sound conclusions and the reduction in IPV observed in the current study may have occurred naturally over time despite the intervention. However, it is possible that therapist discussions with non-participating fathers who had used violence (to engage them in consent conversations about the impact of violence on their child and their children’s need for therapy) may have influenced their use of violent behaviour and impacted on the levels of IPV women experienced. Although research with fathers who use violence is limited (Cater & Forsell, 2014; Stover, 2015), some evidence does suggest that men’s relationships with their children may be influential in changing men’s behaviour (Broady et al., 2017; Stanley et al., 2012; Stover et al., 2020). Further research is needed to explore this possible positive effect on women’s and children’s safety.
What is needed to sustain CPP within organisations?
For CPP to be sustained within organisations, young children and their mothers affected by violence need to be identified and referred, and trained therapists need to be supported in regular supervision. Strong governance and collaborative networks are needed to address the many contextual strengths and risk factors impacting on IPV-affected dyads (Groves et al., 2007; Lieberman et al., 2015). This includes more work in building organisational capacity and practice guidance in the delivery of trauma- and violence-informed child mental health care. Guidelines should also cover therapeutic readiness assessment to support relational safety for children in the care of multiple victim and survivor and perpetrator parents or caregivers and build staff confidence in providing this form of care (Bunston, 2013; Humphreys et al., 2020; Stover, 2015; Toone, 2018).
Better service collaboration between family violence and mental health services is needed to sustain CPP practice for this population of IPV-affected mother–child dyads. Within the reform context that is driving collaboration between non-government organisations and mental health services (Productivity Commission, 2020; State of Victoria, 2016, 2021), we anticipate that CPP will readily find a place as an acceptable and effective intervention for mother–child dyads. While the RECOVER project was instrumental in establishing the Australian CPP community of practice, for the intervention to be scaled up and dyads to receive intervention benefits, more CPP-trained therapists are needed. Investment in an evidence-based program like CPP early in the child’s life course may prevent intergenerational mental health problems and abuse, which could provide future cost savings for society and the wider economy.
Conclusion
CPP for IPV-exposed dyads is acceptable to clients and organisations, can be delivered in under six months and is increasingly available as more Australian therapists are trained in the model.
The strengths of this project are the mixed methods evaluation design; use of subjective and objective evidence; delivery of CPP at multiple clinical sites; and the use of implementation theory to guide project design, research analysis and interpretation of findings. The triangulation of qualitative and quantitative data, including both maternal self-report outcome data and direct observation measures (video recordings), adds credibility to our findings. Multi-site studies allow for greater participation of clients and mitigate recruitment risk. Clinical sites across varied locations enabled a deeper understanding of CPP feasibility, with comparisons between different qualified therapists, geographic locations and clinical organisations.
In this study, NPT (May & Finch, 2009) guided the design of data collection tools, analysis and reporting. Using implementation theory helps explain the key mechanisms that prevent or promote the implementation of complex interventions. This provides an additional level of rigour to process evaluation research. NPT supports the identification of individual and organisational barriers to embedding and sustaining new clinical practices (May et al., 2018). These can then be acted upon to improve policy, address the knowledge-to-practice gap and ultimately enhance clinical outcomes.
However, there were several limitations to the RECOVER project. The small survey sample significantly increases our margin for error and means we had limited power to predict the true impacts of the intervention. The limited inclusion criteria and attempt to define therapeutic readiness with reference to a post-separation and post-violence window of safety for families was not reflective of the experiences of violence-cyclical families. Therapeutic readiness requires a more nuanced and flexible approach, and training in such an approach is in fact provided by the CPP training model. This study criteria may have significantly impacted our recruitment. Addressing this and the other identified service recruitment and implementation barriers will assist with obtaining greater participant numbers in future CPP studies to further test program efficacy and impacts.
While it was disappointing that we were unable to retain some dyads, attrition in therapeutic programs with vulnerable groups like CPP is not uncommon (Herschell et al., 2017). The lowest rate of attrition in a CPP study was 14 per cent (Lieberman et al., 2005). The highest rates have been in preventative CPP interventions with non-clinical-treatment-seeking samples (Alto et al., 2021). While attrition varies across CPP studies (14 to 40%), there are similar dropout rates across treatment (intervention and control) groups, indicating challenges with study participation in general, rather than a failing of CPP overall. Similar dyadic interventions report comparable or higher attrition rates, for example attachment and biobehavioural catch-up (22%; Alto et al., 2021) and parent–child interaction therapy (25 to 69%; Lanier et al., 2011).
There may be many reasons why families disengage from services. In our study, women reported their relationship with the therapist to be a key factor influencing their ongoing engagement and experience of program acceptability. Some rural therapists lacked experience engaging young children and were more isolated from supervisory support structures, which in turn may have impacted on their capacity to build the necessary skills in parental engagement needed for CPP delivery. In addition, women and children who have experienced IPV may continue to be exposed to post-separation violence and psychosocial stressors (Humphreys et al., 2018), impacting their availability for regular sessions. Therapists in this study reported families temporarily ceasing treatment during times of maternal ill health, crisis or ongoing abuse. However, it is worth noting that the lowest attrition rate of CPP across all populations tested was with a racially diverse population of IPV-affected dyads and this lower rate was for a CPP treatment that was longer in duration than that provided in the current study. The treatment was also provided by therapists already experienced in CPP working from within an established CPP clinic (Lieberman et al., 2015). Many of the reasons families disengage do not appear to be related to treatment length or acceptability of the intervention, however further research is needed to draw any strong conclusions. Greater research is needed to understand attrition in these groups and ways of intervening during changing windows of readiness with families.
More research is needed to ensure some standardisation of outcome measures across therapeutic intervention studies allowing for greater comparisons, and more emphasis on measuring outcomes that are actually meaningful to families (Howarth et al., 2021). Existing trials of CPP have been focused on a 12-month model of CPP treatment and this is a significant investment for families and agencies (Alto et al., 2021). Longer term psychotherapy treatments require a higher level of engagement from families, as it has been recommended that CPP should be offered as part of a tiered or stepped-care model to best target delivery to those families who can most benefit (Toone, 2015; Valentino, 2017). Current research and implementation projects are evaluating briefer (six-month) courses of CPP (Cerulli et al., 2021) or brief interventions including those conducted via telehealth that draw on skills gained in CPP workforce training cohorts (Giallo et al., 2021).
Since the inception of the current study CPP has already begun to disseminate more widely in Australia within a range of service settings. CPP for the population of mothers and children affected by IPV is feasible in some settings, however this was not the case in all areas, especially with the current escalation of systemic pressures on CAMHS that limit response capacity for young children. The following key messages apply for policymakers to ensure CPP becomes part of a suite of available evidence-based treatment options for young children and their mothers or caregivers affected by violence.
Implications and recommendations for policymakers
CPP is an evidence-based treatment that is feasible to implement and is acceptable to families and services. The comprehensive CPP training package provides the skills and reflective supervision framework to equip therapists to respond to children and their mothers affected by IPV.
In Australia, many young children experiencing family violence miss out on essential mental health care. Women who have experienced IPV are also often overlooked and yet when they are their child’s primary caregiver, their relationship with their child is an essential resource for children’s recovery and resilience after trauma. Children often also need help in their relationships with their fathers (or other caregivers) who are co-parenting them after using IPV, however there are currently a lack of service parameters and policies in place to enable workforces to provide this care.
Governments need to invest in early childhood mental health and wellbeing service delivery and to expand a trauma- and violence-informed child mental health and wellbeing workforce. This should include the development of a practice guide or framework to support child victims of violence and their families to recovery. CPP training can provide the foundation for the development of this workforce development and practice framework. Future service design should emphasise assessment for therapeutic readiness, workforce supervisory structures and inter-sector collaboration between public mental health and family violence services, especially in rural areas, to ensure returns from investment in workforce training and treatment delivery are maximised.
Implications
- Very young children’s mental health and wellbeing can be particularly impacted by IPV trauma, alongside those of their affected mothers.
- The mental health care needs of very young children are often overlooked in Australian service systems, as are the needs of IPV-affected mother–child dyads.
- The way to restore young children’s mental health after IPV is within their safe relationships (and as a first step this is often, but not always, with their mother).
- CPP is an evidence-based model for this population that is acceptable and increasingly feasible across settings within Australia.
- The CPP model of care also provides the theory, skills training and reflective supervision framework to build and sustain a mental health and wellbeing workforce for young children and parents/caregivers impacted by IPV trauma.
Recommendations
- Promote equity of mental health service delivery for children across the age range, to ensure responsive care is available for all children from earliest life.
- Invest in and expand the trauma- and violence-informed child mental health workforce that is growing in Australia, based on the CPP training and workforce development model.
- Develop a national trauma- and violence-informed child mental health and wellbeing practice framework, to guide safe engagement for children within all important caregiving relationships after IPV. This should be inclusive of both victim and survivor, and perpetrator co-parents when safe, and across caregiver genders and sexualities.
Implications and guidance for practitioners and service providers
RECOVER has made considerable service impacts across several project sites that can guide future care. RECOVER has:
- reinforced the value of tailoring services for IPV-exposed mothers and very young children previously missing out on care and/or identified service gaps for this age group
- highlighted the need to identify safe windows of therapeutic readiness for change with families
- identified that rural therapists/managers with less experience need more support to implement CPP
- operationalised trauma history assessment for children and caregivers referred to the service to better inform and tailor treatment plans for children and families
- facilitated the introduction of family violence screening at triage and realisation that family violence is prevalent among the clinical population
- facilitated partnerships between child mental health and family violence services
- highlighted the need for and value of building a trauma- and violence-informed child mental health/therapeutic workforce
- facilitated the training of further cohorts of CPP-qualified clinicians who are in turn now offering CPP across Victoria and South Australia (to Aboriginal and Torres Strait Islander families, migrant and refugee families, and some parents – mothers, fathers, caregivers – who have used violence in their relationships), as well as delivering CPP via telehealth
- developed a national community of practice, practice activities and knowledge translation.
Future research
Further research is needed to identify the most effective treatments for women and children who have been impacted by IPV. This includes better understanding therapeutic readiness for violence-cyclical families to intervene with children in multiple caregiving relationships. In addition, studies in future could expand the range of caregiver and family participants to include diverse genders and sexualities.
RECOVER has outlined that CPP is feasible and acceptable to participants in this study. However, further research is required to assess intervention efficacy in an Australian context, with a larger sample and delivered by a now larger and more CPP-experienced Australian workforce.
Very little research is available on young children’s experiences of psychotherapeutic treatment (Pernebo & Almqvist, 2016) and the mechanisms for change. There is a need to explore children’s participation experiences of CPP, and to better understand how children influence their own treatment and recovery.
In metropolitan and rural Victoria and South Australia, teams are already beginning to expand CPP practice across perinatal child protection populations, culturally and linguistically diverse families and Aboriginal and Torres Strait Islander families, and via telehealth. It will be important to understand the experiences of these client populations, what adaptations therapists are making in partnership with these families, and whether these locally adapted models are effective.
Better understanding these elements will enable a more precise delivery of CPP to families that can most benefit and will maximise return on investment, ensuring that young children affected by trauma not only recover but also thrive.
References
Alto, M. E., Ross, A. J., Handley, E. D., Manly, J. T., Guild, D. J., Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2021). Longitudinal outcomes of child–parent psychotherapy: Response to commentaries. Research on Child and Adolescent Psychopathology. https://doi.org/10.1007/s10802-021-00801-4
Anderson, K., & van Ee, E. (2018). Mothers and children exposed to intimate partner violence: A review of treatment interventions. International Journal of Environmental Research & Public Health, 15(9), 07. https://doi.org/10.3390/ijerph15091955
Anis, L., Letourneau, N., Benzies, K., Ewashen, C., & Hart, M. J. (2020). Effect of the attachment and child health parent training program on parent–child interaction quality and child development. Canadian Journal of Nursing Research, 52(2), 157–168. https://doi.org/10.1177/0844562119899004
Austin, A. E., Shanaham, M. E., Barrios, Y. V., & Macy, R. J. (2019). A systematic review of interventions for women parenting in the context of intimate partner violence. Trauma Violence & Abuse, 20(4), 498–519. https://doi.org/10.1177/1524838017719233
Australian Bureau of Statistics. (2017). Personal Safety Survey, Australia (cat. no. 4906.0). ABS. https://www.abs.gov.au/ausstats/abs
Australian Institute of Health and Welfare. (2020). Australia’s children. AIHW. https://www.aihw.gov.au/reports/children-youth/australias-children
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story 2019 – In brief. AIHW. https://www.aihw.gov.au/getmedia/b0037b2d-a651-4abf-9f7b-00a85e3de528/aihw-fdv3-FDSV-in-Australia-2019.pdf.aspx?inline=true
Bancroft, L., Silverman, J. G., & Ritchie, D. (2012). The batterer as parent: Addressing the impact of domestic violence on family dynamics (2nd ed.). Sage.
Barlow, J., Bennett, C., Midgley, N., Larkin, S. K., & Wei, Y. (2015). Parent–infant psychotherapy for improving parental and infant mental health. Cochrane Database of Systematic Reviews, 1, CD010534. https://doi.org/10.1002/14651858.CD010534.pub2
Bernstein, R. E., Timmons, A. C., & Lieberman, A. F. (2019). Interpersonal Violence, maternal perception of infant emotion, and child-parent psychotherapy. Journal of Family Violence, 34(4), 309–320. https://doi.org/10.1007/s10896-019-00041-7
Berry, V., Wilkinson, K., Farr, N., & Stimson, A. (2019). Assessing the feasibility of a parent life coaching intervention to support parents and children who have experienced domestic violence and abuse. Journal of Family Violence, 34(6), 493–506. https://doi.org/10.1007/s10896-019-00042-6
Bidarra, Z. S., Lessard, G., & Dumont, A. (2016). Co-occurrence of intimate partner violence and child sexual abuse: Prevalence, risk factors and related issues. Child Abuse & Neglect, 55, 10–21. https://doi.org/10.1016/j.chiabu.2016.03.007
Bowen, D. J., Kreuter, M., Spring, B., Cofta-Woerpel, L., Linnan, L., Weiner, D., Bakken, S., Kaplan, C. P., Squiers, L., Fabrizio, C., & Fernandez, M. (2009). How we design feasibility studies. American Journal of Preventive Medicine, 36(5), 452–457. https://doi.org/https://doi.org/10.1016/j.amepre.2009.02.002
Broady, T. R., Gray, R., Gaffney, I., & Lewis, P. (2017). “I miss my little one a lot”: How father love motivates change in men who have used violence. Child Abuse Review, 26(5), 328–338. https://doi.org/10.1002/car.2381
Buchanan, F., & Humphreys, C. (2021). Coercive control during pregnancy, birthing and postpartum: Women’s experiences and perspectives on health practitioners’ responses. Journal of Family Violence, 36(3), 325–335. https://doi.org/10.1007/s10896-020-00161-5
Bunston, W. (2008). Baby lead the way: Mental health group work for infants, children and mothers affected by family violence. Journal of Family Studies, 14(2–3), 334–341. https://doi.org/10.5172/jfs.327.14.2-3.334
Bunston, W. (2013). “What about the fathers?” Bringing “Dads on Board” with their infants and toddlers following violence. Journal of Family Studies, 19(1), 70–79. https://doi.org/10.5172/jfs.2013.19.1.70
Bunston, W., Eyre, K., Carlsson, A., & Pringle, K. (2016). Evaluating relational repair work with infants and mothers impacted by family violence. Australian and New Zealand Journal of Criminology, 49(1), 113–133. https://doi.org/10.1177/0004865814559925
Bunston, W., Franich-Ray, C., & Tatlow, S. (2017). A diagnosis of denial: How mental health classification systems have struggled to recognise family violence as a serious risk factor in the development of mental health issues for infants, children, adolescents and adults. Brain Sciences, 7(10), 133. https://doi.org/10.3390/brainsci7100133
Bunston, W., Pavlidis, T., & Cartwright, P. (2016). Children, family violence and group work: Some do’s and don’ts in running therapeutic groups with children affected by family violence. Journal of Family Violence, 31(1), 85–94. https://doi.org/10.1007/s10896-015-9739-1
Campo, M. (2015). Children’s exposure to domestic and family violence: Key issues and responses. Journal of the Home Economics Institute of Australia, 22(3), 33. https://doi.org/10.13140/RG.2.1.1759.1121
Cater, Å., & Forssell, A. M. (2014). Descriptions of fathers’ care by children exposed to intimate partner violence (IPV) – Relative neglect and children’s needs. 19(2), 185–193. https://doi.org/10.1111/j.1365-2206.2012.00892.x
Carpenter, G. L., & Stacks, A. M. (2009). Developmental effects of exposure to intimate partner violence in early childhood: A review of the literature. Children and Youth Services Review, 31(8), 831–839. https://doi.org/10.1016/j.childyouth.2009.03.005
Cerulli, C., Cicchetti, D., Handley, E. D., Manly, J. T., Rogosch, F. A., & Toth, S. L. (2021). Transforming the paradigm of child welfare. Development and Psychopathology, 33(2), 377–393. https://doi.org/10.1017/S0954579420002138
Chan, Y.-C., & Yeung, J. W.-K. (2009). Children living with violence within the family and its sequel: A meta-analysis from 1995–2006. Aggression and Violent Behavior, 14(5), 313–322. https://doi.org/10.1016/j.avb.2009.04.001
Chang, J. C., Dado, D., Ashton, S., Hawker, L., Cluss, P. A., Buranosky, R., & Scholle, S. H. (2006). Understanding behavior change for women experiencing intimate partner violence: Mapping the ups and downs using the stages of change. Patient Education and Counseling, 62(3), 330–339. https://dx.doi.org/10.1016/j.pec.2006.06.009
Child–Parent Psychotherapy. (2018). Research fact sheet. https://childparentpsychotherapy.com/wp-content/uploads/2018/01/CPP-research-fact-sheet-Jan-2018.pdf
Chu, A. T., Ippen, C. G., & Lieberman, A. F. (2021). It’s all about the relationship: The role of attachment in child–parent psychotherapy. Research on Child and Adolescent Psychopathology, 49(5), 591–593. https://doi.org/10.1007/s10802-020-00741-5
Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2006). Fostering secure attachment in infants in maltreating families through preventive interventions. Development and Psychopathology, 18(03), 623-649. https://doi.org/10.1017/s0954579406060329
Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2000). The efficacy of toddler-parent psychotherapy for fostering cognitive development in offspring of depressed mothers. Journal of Abnormal Child Psychology, 28(2), 135–148. https://doi.org/10.1023/a:1005118713814
Cicchetti, D., Rogosch, F. A., Toth, S. L., & Sturge-Apple, M. L. (2011). Normalizing the development of cortisol regulation in maltreated infants through preventive interventions. Development and Psychopathology, 23(03), 789–800. https://doi.org/10.1017/S0954579411000307
Cicchetti, D., Toth, S. L., & Rogosch, F. A. (1999). The efficacy of toddler-parent psychotherapy to increase attachment security in offspring of depressed mothers. Attachment & Human Development, 1(1), 34–66. https://doi.org/10.1080/14616739900134021
Cohen, J. A., Mannarino, A. P., & Iyengar, S. (2011). Community treatment of posttraumatic stress disorder for children exposed to intimate partner violence: A randomized controlled trial. Archives of Pediatrics Adolescent Medicine, 165(1), 16–21. https://doi.org/10.1001/archpediatrics.2010.247
Conway, L. J., Cook, F., Cahir, P., Brown, S., Reilly, S., Gartland, D., Mensah, F., & Giallo, R. (2020). Children’s language abilities at age 10 and exposure to intimate partner violence in early childhood: Results of an Australian prospective pregnancy cohort study. Child Abuse & Neglect, 104794. https://doi.org/10.1016/j.chiabu.2020.104794
David, P., & Schiff, M. (2015). Learning from bottom-up dissemination: Importing an evidence-based trauma intervention for infants and young children to Israel. Evaluation and Program Planning, 53, 18–24. https://doi.org/10.1016/j.evalprogplan.2015.07.012
Despert, J. L. (1949) Therapeutic readiness in child psychiatry. Psychiatry, 12(2), 153–158. https://doi.org/10.1080/00332747.1949.11022728
Derogatis, L. R., & Unger, R. (2010). Symptom Checklist-90–Revised. In The Corsini Encyclopedia of Psychology. John Wiley & Sons, Inc. https://doi.org/10.1002/9780470479216.corpsy0970
Domoney, J., Fulton, E., Stanley, N., McIntyre, A., Heslin, M., Byford, S., Bick, D., Ramchandani, P., MacMillan, H., Howard, L. M., & Trevillion, K. (2019). For baby’s sake: Intervention development and evaluation design of a whole-family perinatal intervention to break the cycle of domestic abuse. Journal of Family Violence, 34(6), 539–551. https://doi.org/10.1007/s10896-019-00037-3
Dowling, D. (2019). An independent practitioner’s introduction to child and adolescent psychotherapy: Playing with ideas. Routledge.
Ebert, L., Amaya-Jackson, L., Markiewicz, J., & Fairbank, J. A. (2012). Development and application of the NCCTS learning collaborative model for the implementation of evidence-based child trauma treatment. In R. K. McHugh & D. H. Barlow (Eds.). Dissemination and implementation of evidence-based psychological interventions (pp. 97–123). Oxford University Press.
Erford, B., & Bardhoshi, G. (2018). Introduction to group work: Historical perspectives and functional group models. In B. Erford (Ed.). Group Work (pp. 35–64). Routledge.
Evans, S., Davies, C., & DiLillo, D. (2008). Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggression and Violent Behavior, 13(2), 131–140. https://doi.org/
Feinberg, M. E., Jones, D. E., Hostetler, M. L., Roettger, M. E., Paul, I. M., & Ehrenthal, D. B. (2016). Couple-focused prevention at the transition to parenthood, a randomized trial: Effects on coparenting, parenting, family violence, and parent and child adjustment. Prevention Science, 17(6), 751–764. https://doi.org/10.1007/s11121-016-0674-z
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Fitzpatrick, K. M., Brown, S., Hegarty, K., Mensah, F., & Gartland, D. (2020). Physical and emotional intimate partner violence and women’s health in the first year after childbirth: An Australian pregnancy cohort study. Journal of Interpersonal Violence, 088626052093442. https://doi.org/10.1177/0886260520934426
Foa, E. B., Riggs, D. S., Dancu, C. V., & Rothbaum, B. O. (1993). Reliability and validity of a brief instrument for assessing post‐traumatic stress disorder. Journal of Traumatic Stress, 6(4), 459–473. https://doi/10.1002/jts.2490060405
Foa, E., McLean, C., Zang, Y. , Zhong, J., Rauch, S., Porter, K., Knowles, K., Powers, M. & Kauffman, B. (2016). Psychometric properties of the posttraumatic stress disorder symptom scale interview for DSM-5 (PSSI-5). Psychological Assessment, 28(10), 1159–1165. https://doi.org/10.1037/pas0000259
Fogarty, A., Giallo, R., Wood, C., Kaufman, J., & Brown, S. (2019). Emotional-behavioral resilience and competence in preschool children exposed and not exposed to intimate partner violence in early life. International Journal of Behavioral Development, 44(2), 97–106. https://doi.org/10.1177/0165025419830241
Fogarty, A., Savopoulos, P., Seymour, M., Cox, A., Williams, K., Petrie, S., Herman, S., Toone, E., Schroeder, K., & Giallo, R. (2021). Providing therapeutic services to women and children who have experienced intimate partner violence during the COVID-19 pandemic: Challenges and learnings. Child Abuse & Neglect, 105365. https://doi.org/10.1016/j.chiabu.2021.105365
Fogarty, A., Treyvaud, K., Savopoulos, P., Jones, A., Cox, A., Toone, E., & Giallo, R. (2020). Facilitators to engagement in a mother–child therapeutic intervention following intimate partner violence. Journal of Interpersonal Violence, 0886260520926316. https://doi.org/10.1177/0886260520926316
Fogarty, A., Woolhouse, H., Giallo, R., Wood, C., Kaufman, J., & Brown, S. (2019). Promoting resilience and wellbeing in children exposed to intimate partner violence: A qualitative study with mothers. Child Abuse & Neglect, 95, 104039. https://doi.org/10.1016/j.chiabu.2019.104039
Ford-Gilboe, M., Wathen, C. N., Varcoe, C., MacMillan, H. L., Scott-Storey, K., Mantler, T., Hegarty, K., & Perrin, N. (2016). Development of a brief measure of intimate partner violence experiences: The Composite Abuse Scale (Revised) – Short Form (CASR-SF). BMJ Open, 6(12). https://doi.org/10.1136/bmjopen-2016-012824
Fraiberg, S., Adelson, E., & Shapiro, V. (1975). Ghosts in the nursery: A psychoanalytic approach to the problems of impaired infant-mother relationships. Journal of the American Academy of Child Psychiatry, 14(3), 387-421. https://doi.org/10.1016/S0002-7138(09)61442-4
Gartland, D., Conway, L. J., Giallo, R., Mensah, F. K., Cook, F., Hegarty, K., Herrman, H., Nicholson, J., Reilly, S., Hiscock, H., Sciberras, E., & Brown, S. J. (2021). Intimate partner violence and child outcomes at age 10: A pregnancy cohort. Archives of Disease in Childhood. https://doi.org/10.1136/archdischild-2020-320321
Ghosh Ippen, C., Chu, A., & Lieberman, A. F. (2020). CPP & Telehealth: What we know and how it guides us. CPP https://childparentpsychotherapy.com/wp-content/uploads/2020/03/CPP-and-Telehealth-module1.pdf
Ghosh Ippen, C., Harris, W. W., Van Horn, P., & Lieberman, A. F. (2011). Traumatic and stressful events in early childhood: Can treatment help those at highest risk? Child Abuse & Neglect, 35(7), 504–513. https://doi.org/http://dx.doi.org/10.1016/j.chiabu.2011.03.009
Giallo, R., Fogarty, A., Savopoulos, P., Cox, A., Toone, E., Williams, K., Jones, A. & Treyvaud, K. (2021). Capturing the experiences of clinicians implementing a new brief intervention for parents and children who have experienced family violence in Australia. Health & Social Care in the Community. https://doi.org/10.1111/hsc.13587
Gillies, D., Maiocchi, L., Bhandari, A. P., Taylor, F., Gray, C., & O’Brien, L. (2016). Psychological therapies for children and adolescents exposed to trauma. Cochrane Database of Systematic Reviews, 2016(10), Article Cd012371. https://doi.org/10.1002/14651858.CD012371
Goodman, R. (2001). Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337–1345. https://doi.org/10.1097/00004583-200111000-00015
Graham-Bermann, S. A. (2006). Early intervention for children exposed to domestic violence. Grant funded by Blue Cross and Blue Shield of Michigan Foundation.
Graham-Bermann, S. A., Howell, K. H., Lilly, M., & DeVoe, E. (2011). Mediators and moderators of change in adjustment following intervention for children exposed to intimate partner violence. Journal of Interpersonal Violence, 26(9), 1815–1833. https://doi.org/10.1177/0886260510372931
Graham-Bermann, S. A., Lynch, S., Banyard, V., DeVoe, E. R., & Halabu, H. (2007). Community-based intervention for children exposed to intimate partner violence: An efficacy trial. Journal of Consulting Clinical Psychology & Psychotherapy, 75(2), 199. https://doi.org/10.1037/0022-006X.75.2.199
Graham-Bermann, S. A., Miller-Graff, L. E., Howell, K. H., & Grogan-Kaylor, A. (2015). An efficacy trial of an intervention program for children exposed to intimate partner violence. Child Psychiatry & Human Development, 46(6), 928–939. https://doi.org/10.1007/s10578-015-0532-4
Grogan-Kaylor, A., Galano, M. M., Howell, K. H., Miller-Graff, L., & Graham-Bermann, S. A. (2019). Reductions in parental use of corporal punishment on pre-school children following participation in the Moms’ Empowerment Program. Journal of Interpersonal Violence, 34(8), 1563–1582. https://doi.org/10.1177/0886260516651627
Groves, B. M., Van Horn, P., & Lieberman, A. F. (2007). Deciding on fathers’ involvement in their children’s treatment after domestic violence. In J. L. Edleson & O. J. Williams, Parenting by men who batter: New directions for assessment and intervention (pp. 65–84). https://doi.org/10.1093/acprof:oso/9780195309034.001.0001
Guild, D. J., Alto, M. E., Handley, E. D., Rogosch, F., Cicchetti, D., & Toth, S. L. (2021). Attachment and affect between mothers with depression and their children: Longitudinal outcomes of child–parent psychotherapy. Research on Child and Adolescent Psychopathology, 49(5), 563–577. https://doi.org/10.1007/s10802-020-00681-0
Guy, S., Furber, G., Leach, M., & Segal, L. (2016). How many children in Australia are at risk of adult mental illness? Australian & New Zealand Journal of Psychiatry, 50(12), 1146–1160. https://doi.org/10.1177/0004867416640098
Hagan, M. J., Browne, D. T., Sulik, M., Ippen, C. G., Bush, N., & Lieberman, A. F. (2017). Parent and child trauma symptoms during child–parent psychotherapy: A prospective cohort study of dyadic change. Journal of Traumatic Stress, 30(6), 690–697. https://doi.org/10.1002/jts.22240
Herschell, A., Scudder, A., Schaffner, K., & Slagel, L. (2017). Feasibility and effectiveness of parent–child interaction therapy with victims of domestic violence: A pilot study. Journal of Child & Family Studies, 26(1), 271–283. https://doi.org/10.1007/s10826-016-0546-y
Hoffman, K. T., Marvin, R. S., Cooper, G., & Powell, B. (2006). Changing toddlers’ and preschoolers’ attachment classifications: The Circle of Security intervention. Journal of Consulting Clinical Psychology & Psychotherapy, 74(6), 1017. https://doi.org/10.1037/0022-006X.74.6.1017
Holt, S., Buckley, H., & Whelan, S. (2008). The impact of exposure to domestic violence on children and young people: A review of the literature. Child Abuse & Neglect, 32(8), 797–810. https://doi.org/10.1016/j.chiabu.2008.02.004
Hooker, L., Kaspiew, R., & Taft, A. (2016). Domestic and family violence and parenting: Mixed method insights into impact and support needs: State of knowledge paper (ANROWS Landscapes 01/16). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/L1.16_1.8-Parenting-2.pdf
Hooker, L., Samaraweera, N., Agius, P., & Taft, A. (2016). Intimate partner violence and the experience of motherhood: A cross-sectional analysis of factors associated with a poor experience of motherhood. Midwifery, 34, 88–94. https://doi.org/10.1016/j.midw.2015.12.011
Hooker, L., & Taft, A. (2016). Using theory to design, implement and evaluate sustained nurse domestic violence screening and supportive care. Journal of Research in Nursing, 21(5–6), 432–442. https://doi.org/10.1177/1744987116649633
Hooker, L., & Taft, A. J. (2019). Incorporating intimate partner violence interventions in nurse home visitation programs. Journal of the American Medical Association, 322(11), 1103. https://doi.org/10.1001/jama.2019.10598
Hooker, L., Toone, E., Raykar, V., Humphreys, C., Westrupp, E., Morris, A., & Taft, A. (2019). Reconnecting mothers and children after violence (RECOVER): The Australian Child–Parent Psychotherapy feasibility project – Study protocol. BMJ Open, 9:e023653. https://doi.org/10.1136/bmjopen-2018-023653
Howarth, E., Moore, T. H., Shaw, A. R., Welton, N. J., Feder, G. S., Hester, M., MacMillan, H. L., & Stanley, N. (2015). The effectiveness of targeted interventions for children exposed to domestic violence: Measuring success in ways that matter to children, parents and professionals. Child Abuse Review, 24(4), 297–310. https://doi.org/10.1002/car.2408
Howarth, E., Moore, T. H. M., Stanley, N., MacMillan, H. L., Feder, G., & Shaw, A. (2018). Towards an ecological understanding of readiness to engage with interventions for children exposed to domestic violence and abuse: Systematic review and qualitative synthesis of perspectives of children, parents and practitioners. Health & Social Care in the Community. https://doi.org/10.1111/hsc.12587
Howarth, E., Moore, T. H., Welton, N. J., Lewis, N., Stanley, N., MacMillan, H., Shaw, A., Hester, M., Bryden, P., & Feder, G. (2016). IMPRoving Outcomes for children exposed to domestic ViolencE (IMPROVE): An evidence synthesis. Public Health Research, 4(10), 1–342. https://doi.org/10.3310/phr04100
Howarth, E., Powell, C., Woodman, J., Walker, E., Chesters, H., Szilassy, E., Gilber, R. & Feder, G. (2021). Protocol for developing core outcome sets for evaluation of psychosocial interventions for children and families with experience or at risk of child maltreatment or domestic abuse. BMJ Open, 11(8): 044431. https://doi.org/10.1136/bmjopen-2020-044431
Howell, K. H. (2011). Resilience and psychopathology in children exposed to family violence. Aggression and Violent Behavior, 16(6), 562–569. https://doi.org/10.1016/j.avb.2011.09.001
Howell, K. H., Miller-Graff, L. E., Hasselle, A. J., & Scrafford, K. E. (2017). The unique needs of pregnant, violence-exposed women: A systematic review of current interventions and directions for translational research. Aggression & Violent Behavior, 34, 128–138. https://doi.org/10.1016/j.avb.2017.01.021
Howell, K. H., Miller, L. E., Lilly, M. M., Burlaka, V., Grogan-Kaylor, A. C., & Graham-Bermann, S. A. (2015). Strengthening positive parenting through intervention: Evaluating the Moms’ Empowerment Program for women experiencing intimate partner violence. Journal of Interpersonal Violence, 30(2), 232–252. https://doi.org/10.1177/0886260514533155
Humphreys, C., Diemer, K., Bornemisza, A., Spiteri-Staines, A., Kaspiew, R., & Horsfall, B. (2018). More present than absent: Men who use domestic violence and their fathering. Child & Family Social Work, 0(0). https://doi.org/10.1111/cfs.12617
Humphreys, C. (2011). Rebuilding together: Strengthening the mother–child bond in the aftermath of violence. DVRCV Quarterly, 3, 6.
Humphreys, C., Thiara, R. K., & Skamballis, A. (2011). Readiness to change: Mother–child relationship and domestic violence intervention. British Journal of Social Work, 41(1), 166–184. https://doi.org/10.1093/bjsw/bcq046
Humphreys, C., Mullender, A., Thiara, R., & Skamballis, A. (2006). “Talking to my mum”: Developing communication between mothers and children in the aftermath of domestic violence. Journal of Social Work, 6(1), 53–63. https://doi.org/10.1177/1468017306062223
Isobe, J., Healey, L., & Humphreys, C. (2020). A critical interpretive synthesis of the intersection of domestic violence with parental issues of mental health and substance misuse. Health and Social Care in the Community, 28(5), 1394–1407. https://doi.org/10.1111/hsc.12978
Iwaoka-Scott, A. Y., & Lieberman, A. F. (2015). Moving from dyads to triads: Implementation of child–parent psychotherapy with fathers. Zero to Three, 35(5), 18–24.
Jack, S. M., Boyle, M., McKee, C., Ford-Gilboe, M., Wathen, C., Scribano, P., Davidov, D., McNaughton, D., O’Brien, R., Johnston, C., Gasbarro, M., Tanaka, M., Kimber, M., Coben, J., Olds, D. L., & MacMillan, H. L. (2019). Effect of addition of an intimate partner violence intervention to a nurse home visitation program on maternal quality of life: A randomized clinical trial. Journal of the American Medical Association, 321(16), 1576–1585. https://doi.org/10.1001/jama.2019.3211
James-Hanman, D., & Holt, S. (2021). Post-separation contact and domestic violence: Our 7-point plan for safe[r] contact for children. Journal of Family Violence. https://doi.org/10.1007/s10896-021-00256-7
Jones, S., & Bunston, W. (2012). The “original couple”: Enabling mothers and infants to think about what destroys as well as engenders love, when there has been intimate partner violence. Couple and Family Psychoanalysis, 2(2), 215–232. https://doi.org/10.33212/cfp.v2n2.2012.215
Jouriles, E. N., McDonald, R., Rosenfield, D., Stephens, N., Corbitt-Shindler, D., & Miller, P. C. (2009). Reducing conduct problems among children exposed to intimate partner violence: A randomized clinical trial examining effects of Project Support. Journal of Consulting Clinical Psychology & Psychotherapy, 77(4), 705. https://doi.org/10.1037/a0015994
Kamal, L., Strand, J., Jutengren, G., & Tidefors, I. (2017). Perceptions and experiences of an attachment-based intervention for parents troubled by intimate partner violence. Clinical Social Work Journal, 45(4), 311–319. https://doi.org/10.1007/s10615-016-0606-1
Katz, E. (2019). Coercive control, domestic violence, and a five-factor framework: Five factors that influence closeness, distance, and strain in mother–child relationships. Violence Against Women, 1077801218824998. https://doi.org/10.1177/1077801218824998
Keeshin, B. R., Oxman, A., Schindler, S., & Campbell, K. A. (2015). A domestic violence shelter parent training program for mothers with young children. Journal of Family Violence, 30(4), 461–466. https://doi.org/10.1007/s10896-015-9698-6
Kitzmann, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witnesses to domestic violence: a meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339. https://doi.org/10.1037/0022-006X.71.2.339
Kong, T. (2021) From frontline assessment to reunification: The integration of CPP into a hospital-based child protection service [Symposium Session]. World Association for Infant Mental Health World Congress, Brisbane & online, Australia.
Labarre, M., Bourassa, C., Holden, G. W., Turcotte, P., & Letourneau, N. (2016). Intervening with fathers in the context of intimate partner violence: An analysis of ten programs and suggestions for a research agenda. Journal of Child Custody, 13(1), 1–29. https://doi.org/10.1080/15379418.2016.1127793
Lamb, K., Humphreys, C., & Hegarty, K. (2018). “Your behaviour has consequences”: Children and young people’s perspectives on reparation with their fathers after domestic violence. Children and Youth Services Review, 88, 164–169. https://doi.org/10.1016/j.childyouth.2018.03.013
Lanier, P., Kohl, P. L., Benz, J., Swinger, D., Moussette, P., & Drake, B. (2011). Parent–child interaction therapy in a community setting: Examining outcomes, attrition, and treatment setting. Research on Social Work Practice, 21(6), 689–698. https://doi.org/10.1177/1049731511406551
Larrieu, J. A. (2018). Introducing evidence-based trauma treatment in preventive services: Child–Parent Psychotherapy. In V. Strand & G. Sprang (Eds.), Trauma responsive child welfare systems (pp. 147–164). Springer, Cham. https://doi.org/10.1007/978-3-319-64602-2_9
Latzman, N. E., Casanueva, C., Brinton, J., & Forman-Hoffman, V. L. (2019). The promotion of well-being among children exposed to intimate partner violence: A systematic review of interventions. Campbell Systematic Reviews, 15(e1049). https://doi.org/10.1002/cl2.1049
Lavi, I., Gard, A. M., Hagan, M., Van Horn, P., & Lieberman, A. F. (2015). Child–parent psychotherapy examined in a perinatal sample: Depression, posttraumatic stress symptoms and child-rearing attitudes. Journal of Social and Clinical Psychology, 34(1), 64–82. https://doi.org/10.1521/jscp.2015.34.1.64
Letourneau, N., Anis, L., Ntanda, H., Novick, J., Steele, M., Steele, H., & Hart, M. (2020). Attachment & Child Health (ATTACH) pilot trials: Effect of parental reflective function intervention for families affected by toxic stress. Infant Mental Health Journal. https://doi.org/10.1002/imhj.21833
Levendosky, A. A., Lannert, B., & Yalch, M. (2012). The effects of intimate partner violence on women and child survivors: An attachment perspective. Psychodyn Psychiatry, 40(3), 397–434. https://doi.org/10.1521/pdps.2012.40.3.397
Lieberman, A. F. (2004). Child–parent psychotherapy: A relationship-based approach to the treatment of mental health disorders in infancy and early childhood. In A. J. Sameroff, S. C. McDonough, & K. L. Rosenblum (Eds.), Treating parent–infant relationship problems: Strategies for intervention (pp. 97–122). Guilford Press.
Lieberman, A., Van Horn, P., & Ghosh Ippen, C. (2005). Toward evidence-based treatment: Child–parent psychotherapy with preschoolers exposed to marital violence. Journal of the American Academy of Child & Adolescent psychiatry, 44(12), 1241–1248. https://dx.doi.org/10.1097/01.chi.0000181047.59702.58
Lieberman, A., Chu, A., Van Horn, P., & Harris, W. (2011). Trauma in early childhood: Empirical evidence and clinical implications. Development and Psychopathology, 23(2), 397-410. https://doi.org/10.1017/S0954579411000137
Lieberman, A. F., Diaz, M. A., & Van Horn, P. (2011). Perinatal child–parent psychotherapy: Adaptation of an evidence-based treatment for pregnant women and babies exposed to intimate partner violence. In S. A. Graham & B. A. Levendosky (Eds.), How intimate partner violence affects children: Developmental research, case studies, and evidence-based intervention (pp. 47–66). American Psychological Association. https://doi.org/10.1037/12322-003
Lieberman, A. F., Diaz, M. A., Castro, G., & Bucio, G. O. (2020). Make room for baby: Perinatal child-parent psychotherapy to repair trauma and promote attachment. Guilford Publications.
Lieberman, A. F., Ghosh Ippen, C., & Hernandez Dimmler, M. (2019). Child–parent psychotherapy. Assessing and treating youth exposed to traumatic stress. In C. H. Zeanah (Ed.), Handbook of Infant Mental Health, Fourth Edition (pp. 485-499). Guilford Press.
Lieberman, A. F., Ghosh Ippen, C., & Van Horn, P. (2006). Child–parent psychotherapy: 6-month follow-up of a randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 45(8), 913–918. https://doi.org/10.1097/01.chi.0000222784.03735.92
Lieberman, A. F., Ghosh Ippen, C., & Van Horn, P. (2015). Don’t hit my mommy!: A manual for child–parent psychotherapy with young children exposed to violence and other trauma. ZERO TO THREE.
Lieberman, A. F., Padrón, E., Van Horn, P., Harris, W. W., Drell, M. J., Osofsky, J. D., Zuckerman, B., & Zuckerman, P. (2005). Angels in the nursery: The intergenerational transmission of benevolent parental influences [Commentary]. Infant Mental Health Journal, 26(6), 504–520. https://doi.org10.1002/imhj.20071
Luyten, P., Mayes, L., Sadler, L., Fonagy, P., Nicholls, S., Crowley, M., Vesper, A., Mobley, A., Stewart, T., & Close, N. (2009). The Parental Reflective Functioning Questionnaire-1 (PRFQ-1) [Unpublished manual]. University of Leuven, Belgium.
Lyons-Ruth, K., Todd Manly, J., Von Klitzing, K., Tamminen, T., Emde, R., Fitzgerald, H., Paul, C., Keren, M., Berg, A., Foley, M., & Watanabe, H. (2017). The worldwide burden of infant mental and emotional disorder: Report of the task force of the world association for infant mental health. Infant Mental Health Journal, 38(6), 695–705. https://doi.org/10.1002/imhj.21674
Marie-Mitchell, A., & Kostolansky, R. (2019). A systematic review of trials to improve child outcomes associated with adverse childhood experiences. American Journal of Preventive Medicine, 56(5), 756–764. https://doi.org/10.1016/j.amepre.2018.11.030
Marsden, S., Humphreys, C., & Hegarty, K. (2020). Women survivors’ accounts of seeing psychologists: Harm or benefit? Journal of Gender-Based Violence. https://doi.org/10.1332/239868020X16040863370635
Matias, C., Scott, S., & O’Connor, T. (2006). Coding of attachment-related parenting (CARP). Institute of Psychiatry, Kings College.
May, C., & Finch, T. (2009). Implementing, embedding, and integrating practices: An outline of Normalization Process Theory. Sociology, 43(3), 535–554. https://doi.org/10.1177/0038038509103208
May, C. R., Cummings, A., Girling, M., Bracher, M., Mair, F. S., May, C. M., Murray, E., Myall, M., Rapley, T., & Finch, T. (2018). Using Normalization Process Theory in feasibility studies and process evaluations of complex healthcare interventions: A systematic review. Implementation Science, 13(1), 80. https://doi.org/10.1186/s13012-018-0758-1
McLean, S. A, & McIntosh, J. E. (2021). The mental and physical health of family mental health practitioners during COVID-19: Relationships with family violence and workplace practices. Australian Journal of Psychology, 1–10. https://doi.org/10.1080/00049530.2021.1934118
McConnell, N., Barnard, M., & Taylor, J. (2017). Caring Dads Safer Children: Families’ perspectives on an intervention for maltreating fathers. Psychology of Violence, 7(3), 406–416. https://doi.org/10.1037/vio0000105
McFarlane, J., Symes, L., Binder, B. K., Maddoux, J., & Paulson, R. (2014). Maternal–child dyads of functioning: The intergenerational impact of violence against women on children. Maternal Child Health Journal, 18(9), 2236–2243. https://doi.org/10.1007/s10995-014-1473-4
McGorry, P. D. (2021). The reality of mental health care for young people, and the urgent need for solutions. Medical Journal of Australia. https://doi.org/10.5694/mja2.51327
Miller-Graff, L. E., Galano, M., & Graham-Bermann, S. (2016). Expression of re-experiencing symptoms in the therapeutic context: A mixed-method analysis of young children exposed to intimate partner violence. Child Care in Practice, 22(1), 1–2. https://doi.org/10.1080/13575279.2015.1064360
Mohaupt, H., Duckert, F., & Askeland, I. R. (2020). How do men in treatment for intimate partner violence experience parenting their young child? A descriptive phenomenological analysis. Journal of Family Violence, 35(8), 863–875. https://doi.org/10.1007/s10896-019-00083-x
Morales, Y., Lutzker, J. R., Shanley, J. R., & Guastaferro, K. M. (2015). Parent–infant interaction training with a Latino mother. International Journal of Child Health and Human Development, 8(2), 135–145.
Morris, A., Humphreys, C., & Hegarty, K. (2015). Children’s views of safety and adversity when living with domestic violence. In N. Stanley & C. Humphreys (Eds.), Domestic violence and protecting children: New thinking and approaches (pp. 18–33). Jessica Kingsley Publishers.
Mountain, G., Cahill, J., & Thorpe, H. (2017). Sensitivity and attachment interventions in early childhood: A systematic review and meta-analysis. Infant Behavior and Development, 46, 14–32. https://doi.org/10.1016/j.infbeh.2016.10.006
Narayan, A. J., Atzl, V. M., Merrick, J. S., Harris, W. W., & Lieberman, A. F. (2020). Developmental origins of ghosts and angels in the nursery: Adverse and benevolent childhood experiences. Adversity and Resilience Science, 1(2), 121–134. https://doi.org/10.1007/s42844-020-00008-4
Nardone, G., & Salvini, A. (2019). International dictionary of psychotherapy. Routledge.
National Scientific Council on the Developing Child. (2010). Persistent fear and anxiety can affect young children’s learning and development: Working paper 13. https://developingchild.harvard.edu/wp-content/uploads/2010/05/Persistent-Fear-and-Anxiety-Can-Affect-Young-Childrens-Learning-and-Development.pdf
Norlén, A., Thorén, A., & Almqvist, K. (2021). Implementing child–parent psychotherapy (CPP) in Sweden: A qualitative study exploring experiences by caregivers taking part of the intervention with their child. Journal of Infant, Child, and Adolescent Psychotherapy, 1–17. https://doi.org/10.1080/15289168.2021.1925001
Olsen, L. R., Mortensen, E. L., & Bech, P. (2006). Mental distress in the Danish general population. Acta Psychiatrica Scandinavica, 113(6), 477–484. https://doi.org/10.1111/j.1600-0447.2005.00743.x
Orr, C., Fisher, C. M., Preen, D. B., Glauert, R. A., & O’Donnell, M. (2020). Exposure to family and domestic violence is associated with increased childhood hospitalisations. PLOS ONE, 15(8), e0237251. https://doi.org/10.1371/journal.pone.0237251
Overbeek, M., Koren-Karie, N., Ben-Haim, A., De Schipper, J., Dreier Gligoor, P., & Schuengel, C. (2019). Trauma exposure in relation to the content of mother–child emotional conversations and quality of interaction. International Journal of Environmental Research and Public Health, 16(5), 805. https://doi.org/10.3390/ijerph16050805
Pernebo, K., & Almqvist, K. (2016). Young children’s experiences of participating in group treatment for children exposed to intimate partner violence: A qualitative study. Clinical Child Psychology and Psychiatry, 21(1), 119–132. https://doi.org/10.1177/1359104514558432
Pernebo, K., Fridell, M., & Almqvist, K. (2018). Outcomes of psychotherapeutic and psychoeducative group interventions for children exposed to intimate partner violence. Child Abuse & Neglect, 79, 213–223. https://doi.org/10.1016/j.chiabu.2018.02.014
Pernebo, K., Fridell, M., & Almqvist, K. (2019). Reduced psychiatric symptoms at 6 and 12 months’ follow-up of psychotherapeutic and psychoeducative group interventions for children exposed to intimate partner violence. Child Abuse & Neglect, 93, 228–238. https://doi.org/0.1016/j.chiabu.2019.05.002
Pfitzner, N., Fitz-Gibbon, K., & True, J. (2020). Responding to the “shadow pandemic”: Practitioner views on the nature of and responses to violence against women in Victoria, Australia during the COVID-19 restrictions. Monash Gender and Family Violence Prevention Centre. https://apo.org.au/node/306064
Productivity Commission. (2020). Mental health inquiry report (95). Canberra.
QSR International. (2018). NVivo qualitative data analysis software. Version 12. https://www.qsrinternational.com/
Raykar, V., Lawless, K, & Ryan, N. (2021). CPP in a rural CAMHS context [Symposium Session]. World Association for Infant Mental Health World Congress, Brisbane & online, Australia.
Rizo, C. F., Wretman, C. J., Macy, R. J., Guo, S., & Ermentrout, D. M. (2018). A novel intervention for system-involved female intimate partner violence survivors: Changes in mental health. American journal of Orthopsychiatry, 88(6), 681–690. https://doi.org/10.1037/ort0000332
Roopnarine, J. L., & Dede Yildirim, E. (2018). Influence of relationship skills education on pathways of associations between paternal depressive symptoms and IPV and childhood behaviors. Psychology of Men & Masculinity, 19(2), 223–233. https://doi.org/10.1037/men0000100
Satyanarayana, V. A., Nattala, P., Selvam, S., Pradeep, J., Hebbani, S., Hegde, S., & Srinivasan, K. (2016). Integrated cognitive behavioral intervention reduces intimate partner violence among alcohol dependent men, and improves mental health outcomes in their spouses: A clinic based randomized controlled trial from South India. Journal of Substance Abuse Treatment, 64, 29–34. https://doi.org/10.1016/j.jsat.2016.02.005
Schechter, D. S., Moser, D. A., Reliford, A., McCaw, J. E., Coates, S. W., Turner, J., Serpa, S. R., & Willheim, E. (2015). Negative and distorted attributions towards child, self, and primary attachment figure among posttraumatically stressed mothers: What changes with Clinician Assisted Videofeedback Exposure Sessions (CAVES). Child Psychiatry and Human Development, 46(1), 10–20. https://doi.org/10.1007/s10578-014-0447-5
Scheeringa, M. S., & Haslett, N. (2010). The reliability and criterion validity of the diagnostic infant and preschool assessment: A new diagnostic instrument for young children. Child Psychiatry & Human Development, 41(3), 299–312. https://doi.org/10.1007/s10578-009-0169-2
Scott, K. (2017). Cluster RCT of embedded parenting intervention to prevent recurrence and reduce impairment in young children exposed to domestic violence. ClinicalTrials.gov. https://clinicaltrials.gov/show/nct03198429
Segal, L., Guy, S., & Furber, G. (2018). What is the current level of mental health service delivery and expenditure on infants, children, adolescents, and young people in Australia? Australian & New Zealand Journal of Psychiatry, 52(2), 163–172. https://doi.org/10.1177/0004867417717796
Shafi, R., Bieber, E. D., Shekunov, J., Croarkin, P. E., & Romanowicz, M. (2019). Evidence based dyadic therapies for 0-to 5-year-old children with emotional and behavioral difficulties. Frontiers in Psychiatry, 10, 677. https://doi.org/10.3389/fpsyt.2019.00877
Smith, E. (2016). Domestic abuse, recovering together (DART): Evaluation report. NSPCC. https://library.nspcc.org.uk/HeritageScripts/Hapi.dll/search2?searchTerm0=C6566
Sousa, C. A., Siddiqi, M., & Bogue, B. (2021). What do we know after decades of research about parenting and IPV? A systematic scoping review integrating findings. Trauma, Violence, & Abuse, 152483802110160. https://doi.org/10.1177/15248380211016019
Southwell, J. (2016). Using “expressive therapies” to treat developmental trauma and attachment problems in preschool-aged children. Children Australia, 41(2), 114–125. https://doi.org/10.1017/cha.2016.7
Spangaro, J. (2017). What is the role of health systems in responding to domestic violence? An evidence review. Australian Health Review, 41(6), 639–645. https://doi.org/10.1071/AH16155
Stanley, N., Graham-Kevan, N., & Borthwick, R. (2012). Fathers and domestic violence: Building motivation for change through perpetrator programmes. Child Abuse Review, 21(4), 264–274. https://doi.org/10.1002/car.2222
State of Victoria. (2016). Royal Commission into Family Violence: Summary and recommendations. Victorian Government Printer. https://files.rcfv.com.au/Reports/RCFV_Full_Report_Interactive.pdf
State of Victoria. (2019). Victorian Government submission to the Royal Commission into Victoria’s Mental Health System. https://www2.health.vic.gov.au/mental-health/priorities-and-transformation/royal-commission
State of Victoria. (2021). Royal Commission into Victoria’s Mental Health System: Final Report. https://finalreport.rcvmhs.vic.gov.au/download-report/
Steele, H., Murphy, A., Bonuck, K., Meissner, P., & Steele, M. (2019). Randomized control trial report on the effectiveness of Group Attachment-Based Intervention (GABI©): Improvements in the parent–child relationship not seen in the control group. Development & Psychopathology, 31(1), 203–217. https://doi.org/10.1017/S0954579418001621
Stover, C. S., & Lent, K. (2014). Training and certification for domestic violence service providers: The need for a national standard curriculum and training approach. Psychology of Violence, 4(2), 117–127. https://doi.org/10.1037/a0036022
Stover, C. S. (2015). Fathers for Change for substance use and intimate partner violence: Initial community pilot. Family Process, 54(4), 600–609. https://doi.org/10.1111/famp.12136
Stover, C. S., Carlson, M., & Patel, S. (2017). Integrating intimate partner violence and parenting intervention into residential substance use disorder treatment for fathers. Journal of Substance Abuse Treatment, 81, 35–43. https://doi.org/10.1016/j.jsat.2017.07.013
Stover, C. S., Beebe, R., Clough, M., DiVietro, S., Madigan, L., & Grasso, D. J. (2020). Evaluation of a statewide implementation of Fathers for Change: A fathering intervention for families impacted by partner violence. Journal of Family Violence. https://doi.org/10.1007/s10896-020-00199-5
Stronach, E. P., Toth, S. L., Rogosch, F., & Cicchetti, D. (2013). Preventive interventions and sustained attachment security in maltreated children. Development and Psychopathology, 25(4pt1), 919–930. https://doi.org/10.1017/s0954579413000278
Toth, S. L., Maughan, A., Manly, J. T., Spagnola, M., & Cicchetti, D. (2002). The relative efficacy of two interventions in altering maltreated preschool children’s representational models: Implications for attachment theory. Development and Psychopathology, 14(04), 877–908. https://doi.org/10.1017.S095457940200411X
Toth, S. L., Rogosch, F. A., Manly, J. T., & Cicchetti, D. (2006). The efficacy of toddler–parent psychotherapy to reorganize attachment in the young offspring of mothers with major depressive disorder: A randomized preventive trial. Journal of Consulting and Clinical Psychology, 74(6), 1006–1016. https://doi.org/10.1037/0022-006X.74.6.1006
Toone, E. (2015). Appendix 1: Supplementary submission: Therapeutic responses for infants and children at escalating risk of family violence. In S. Keebaugh, J. Pocock & A. Jones(Eds.), No Place for Violence: Berry Street Submission to the Victorian Royal Commission into Family Violence (pp. 53–65). Royal Commission into Family Violence.
Toone, E. (2018). Safe with Dad. Berry Street. https://learning.berrystreet.org.au/sites/default/files/2019-02/Safe-with-dad_0.pdf
Toone, E., Hermans, D., & Hooker, L. (2021, 26–28 May). Safe connection after violent storms and togetherness droughts: Child-Parent Psychotherapy learning after family violence [Conference presentation]. Safe and Together Asia Pacific Conference, Melbourne & Online, Australia.
Trevillion, K., Oram, S., Feder, G., & Howard, L. M. (2012). Experiences of domestic violence and mental disorders: A systematic review and meta-analysis. PLOS ONE, 7(12), e51740. https://doi.org/10.1371/journal.pone.0051740
UN Women. (2020). Violence against women and girls: The shadow pandemic. https://www.unwomen.org/en/news/stories/2020/4/statement-ed-phumzile-violence-against-women-during-pandemic
Valentino. (2017). Relational interventions for maltreated children. Child Development, 88(2), 359–367. https://doi.org/10.1111/cdev.12735
Veritas Health Innovation. Covidence systematic review software. www.covidence.org
Victorian Government Department of Families, Fairness and Housing (2018). What is family violence? https://services.dffh.vic.gov.au/what-family-violence
Visser, M. M., Telman, M. D., de Schipper, J. C., Lamers-Winkelman, F., Schuengel, C., & Finkenauer, C. (2015). The effects of parental components in a trauma-focused cognitive behavioral based therapy for children exposed to interparental violence: Study protocol for a randomized controlled trial. BMC Psychiatry, 15, 131. https://doi.org/10.1186/s12888-015-0533-7
Vu, N. L., Jouriles, E. N., McDonald, R., & Rosenfield, D. (2016). Children’s exposure to intimate partner violence: A meta-analysis of longitudinal associations with child adjustment problems. Clinical Psychology Review, 46, 25–33. https://doi.org/https://doi.org/10.1016/j.cpr.2016.04.003
Waldman-Levi, A., & Weintraub, N. (2015). Efficacy of a crisis intervention in improving mother–child interaction and children’s play functioning. American Journal of Occupational Therapy, 69(1), 1–11. https://doi.org/10.5014/ajot.2015.013375
Waters, S. F., Hagan, M. J., Rivera, L., & Lieberman, A. F. (2015). Improvements in the child-rearing attitudes of Latina mothers exposed to interpersonal trauma predict greater maternal sensitivity toward their 6-month-old infants. Journal of Traumatic Stress, 28(5), 426–433. https://doi.org/10.1002/jts.22043
Wathen, C. N., Schmitt, B., & MacGregor, J. C. D. (2021). Measuring trauma- (and violence-) informed care: A scoping review. Trauma, Violence, & Abuse, 15248380211029399. https://doi.org/10.1177/15248380211029399
Weissman, M. M., Pilowsky, D. J., Wickramaratne, P. J., Talati, A., Wisniewski, S. R., Fava, M., Hughes, C. W., Garber, J., Malloy, E., King, C. A., Cerda, G., Sood, A. B., Alpert, J. E., Trivedi, M. H., & Rush, A. J. (2006). Remissions in maternal depression and child psychopathology: A STAR*D–Child Report. Journal of the American Medical Association, 295(12), 1389–1398. https://doi.org/10.1001/jama.295.12.1389
Westrupp, E., Rose, N., Nicholson, J., & Brown, S. (2015). Exposure to inter-parental conflict across 10 years of childhood: Data from the longitudinal study of Australian children. Maternal and Child Health Journal, 19(9), 1966–1973. https://doi.org/10.1007/s10995-015-1704-3
World Health Organization. (2013a). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non partner sexual violence. https://apps.who.int/iris/bitstream/10665/85239/1/9789241564625_eng.pdf
World Health Organization. (2013b). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf
World Health Organization. (2016). Ethical and safety recommendations for intervention research on violence against women: Building on lessons from the WHO publication Putting women first: Ethical and safety recommendations for intervention research on violence against women. https://apps.who.int/iris/bitstream/handle/10665/251759/9789241510189-engpdf;jsessionid=C50D3F751F53D3BADBD07BEFE6A9500B?sequence=1
World Health Organization. (2021). Violence against women prevalence estimates, 2018. Global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. https://www.who.int/publications/i/item/violence-against-women-prevalence-estimates
Zubrick, S. R., Lucas, N., Westrupp, E. M., & Nicholson, J. M. (2014). Parenting measures in the Longitudinal Study of Australian Children: Construct validity and measurement quality, Waves 1 to 4. Growing Up in Australia. https://www.growingupinaustralia.gov.au/pubs/technical/tp12.pdf
APPENDIX A:
Keyword search terms and grey
literature sites searched
Concept 1:
Population
Concept 2:
Parent–child relationships
Concept 3:
Family violence
Concept 4:
Interventions/support
- Mother*
- Father*
- Parent*
- Child*
- Infant*
- Toddler
- Pre-school*
- Kinder*
- “Child mental health”
- “Maternal mental health”
- “Child development”
- “Family relationships”
- “mother–child relation*”
- “mother–child bond”
- “mother–child connection”
- “mother–child link”
- “parent–child relation*”
- “parent–child bond”
- mothering
- dyad
- “Domestic violence”
- “Family violence”
- “Intimate partner violence”
- Batter*
- “Domestic abuse”
- “Spouse abuse”
- “Domestic assault”
- “intimate partner abuse”
- “marital abuse”
- “spouse assault”
- “partner abuse”
- “partner assault”
- “partner violence”
- “partner aggression”
- “wife abuse”
- “batter* wife”
- “batter*women”
- “batter* wives”
- “inter-parental violence”
- “inter-parental conflict”
- “couple violence”
- “family conflict”
- “parental conflict”
- Intervention
- Therapy
- Support
- Relationship support
- Child–parent psychotherapy
- Mother–child support
- Treatment
- “Dyadic work”
- “relationship therapy”
- “group support”
- “advocacy program*”
- Counsel*
- “individual therapy”
- “individual support”
- “group therapy”
- “group treatment”
- “group work”
APPENDIX B:
Ovid MEDLINE search strategy
- exp domestic violence/ or exp gender-based violence/ or exp intimate partner violence/
- exp Exposure to Violence/
- exp Family Conflict/
- domestic violence or intimate partner violence or domestic assault or domestic abuse).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating subheading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- batter*.mp.
- exposure to violence.mp.
- inter-parental conflict.mp.
- family conflict.mp.
- relational aggression.mp.
- 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9
- exp parent–child relations/ or exp father–child relations/ or exp mother–child relations/
- exp Child Development/
- (mother–child or father–child or parent–child or child–parent).mp.
- (attachment and (child* or infant*)).mp.
- (bond* and (child* or infant*)).mp.
- mental health.mp. and (*child/or infant*.mp.)
- (mental health and (maternal or paternal or parent)).mp.
- 11 or 12 or 13 or 14 or 15 or 16 or 17
- exp play therapy/ or exp psychotherapy, group/ or exp family therapy/
- exp Psychoanalytic Therapy/
- (therapy or treatment or intervention or counselling or counseling).mp.
- (group work or group psychotherapy or family therapy).mp.
- dyadic.mp.
- 19 or 20 or 21 or 22 or 23
- 10 and 18 and 24
- limit 25 to (humans and yr=“2015 -Current”)
APPENDIX C:
Grey literature search: Relevant websites
National
- Australian Institute of Family Studies https://www.aifs.gov.au/
- Australian Institute of Health and Welfare https://www.aihw.gov.au/
- Australia’s National Research Organisation for Women’s Safety https://www.anrows.org.au/
- Australian Government Department of Health https://www.health.gov.au/
- Australian Government Department of Social Services https://www.dss.gov.au/
International
- Blue Prints for Healthy Youth Development, USA https://www.blueprintsprograms.org/
- Centers for Disease Control and Prevention https://www.cdc.gov/ViolencePrevention/
- Center on the Developing Child—Harvard University https://developingchild.harvard.edu/
- Child Trends https://www.childtrends.org/
- Child Welfare Information Gateway, USA https://www.childwelfare.gov/
- Cochrane Central Register of Controlled Trials (CENTRAL) https://www.cochranelibrary.com/central/about-central
- Google Scholar using “mother–child relationship” and “domestic violence” and treatment (or variations thereof)
- New Zealand Domestic Violence Clearinghouse https://nzfvc.org.nz/
- NHS https://www.nhs.uk/
- United Kingdom Government https://www.gov.uk/crime-justice-and-law/violence-against-women-and-girls
- Yale Child Studies Centre https://medicine.yale.edu/childstudy/
- Zero to Three https://www.zerotothree.org/
APPENDIX D:
PRISMA flow chart
APPENDIX E:
Summary table of included studies
Randomised Control Trials-PROTOCOLS
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Scott, 2017
Canada
Urban
RCT
Self-completed questionnaires
Mothers
Fathers
Children
Group
200
This is an RCT examining the efficacy of embedding two different parenting interventions – Mothers in Mind (MIM) and Caring Dads – into child protection services for young children who have been exposed to IPV. Child protection case workers for families are randomly assigned to receive professional development training, supervision support and priority client access to parenting interventions.
MIM is a mother–child dyadic intervention with 10 weekly group sessions and two individual sessions. Caring Dads is a fathering intervention that aims to prevent a recurrence of child exposure to IPV with 14 group sessions and two individual sessions
Treatment as usual: workers continue to provide in-home support to children and families. This is not a placebo: families receive the full child protection service they would normally have received if this trial were not being run
Primary:
Recurrence of abuse
Secondary:
Workers’ case conceptualisation of the risks/needs of mothers & fathers
Workers’ efficacy for using embedded parenting interventions
Child social and emotional development
Study protocol available only
Visser et al., 2015
Netherlands
Unclear
RCT
2-by-2 factorial experimental design
Multicentre trial
Data collected at baseline, post-intervention and 6-mth follow up (FU)
Questionnaires and observational tasks
Children
Parents
Group & dyadic
100
HORIZON is a trauma-focused cognitive behavioural therapy (TF-CBT) group program plus preparatory parenting program plus parent–child sessions. Main aim is to test the additional parent program and parent–child sessions against TF-CBT. Consists of four conditions
Usual care is the
TF-CBT group
Primary outcomes:
Trauma symptoms
Child internalising & externalising behaviour symptoms
Secondary outcomes:
Child mental health
Testing effect of the added components of intervention on child adjustment
Study protocol available only
Randomised controlled trials
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Jack et al., 2019
United States
Unclear
Cluster RCT
Cluster-based, single blind
Measured via interview at baseline & every 6 months until 24 months
Pregnant women over 16 years
Individual
492
Nurse home visiting program with an augmented IPV intervention for socially disadvantaged pregnant women.
Intervention sites (eight), nurses were provided with intensive IPV education and delivered IPV intervention including assessment and tailored planning for safety, violence awareness, self-efficacy, and referral to social supports
Control group (eight sites) received HV usual care
Primary outcome: quality of life
Range of secondary outcomes covering physical and mental health, family violence (FV), general health, alcohol and drug use
No significant difference in primary and secondary outcomes, although several study limitations (e.g. fidelity to model) were noted which may have affected efficacy
Graham-Bermann et al., 2015
United States
Canada
Unclear
RCT
Data collected at baseline, post-intervention and 8 months FU
Mothers and children (aged 4 to6; mean 4.9 years)
Group
120
The intervention is Preschool Kids’ Club which is 10 sessions and takes a skills-based approach delivered to children. It is intended to be delivered in parallel with Moms’ Empowerment Program (MEP) (delivered to the mothers). Preschool Kids’ Club is 10 sessions and takes a skills-based approach. It covers topics like attitudes and beliefs, managing emotions and fears, safety planning and conflict resolution
Waitlist
IPV
Child adjustment
Baseline IPV prevalence results.
Only girls in intervention group showed significant improvement in internalising symptoms.
For children who adhered to the treatment protocol, there was a significant difference in both boys and girls
Miller-Graff et al., 2016
As above
As above
Mixed method
Evaluation of children’s re-experiencing symptoms in therapy described above
Data collected from therapists via a child symptom checklist and examination of clinical notes
Qualitative study examining case notes via thematic analysis
Mean age 5 years
56 notes
2016 results: 68% (38/56) developed re-experiencing symptoms during treatment. No difference in age, gender or IPV exposure.
Re-experiencing symptoms spiked in session 3 – recommend min 6 to 10 sessions
Howell et al., 2015
United States
Unclear
RCT data from earlier Graham-Bermann et al., 2006 study
Data collected at baseline and 5 weeks post
Interviews during which study measures were collected
Mothers
Group
120
MEP is a community-based intervention that aims to improve the mental health, access to resources, and parenting abilities of women exposed to IPV. 10x1hr sessions are provided over 5 weeks with five to seven participants in each group
Waitlist
Violence severity
Depression and mood
Post-traumatic stress
Parenting practices
Significant improvement in parenting behaviours in intervention group
Grogan-Kaylor et al., 2019
As above
As above
Pre/post and 6- to 8-month FU study
Mother and child pairs (4 to 6; mean 4.9 years
113
This study specifically looked at use of corporal punishment pre & post MEP
Significant reduction in use of punishment in intervention group post-intervention and at 6-mth FU
Feinberg et al., 2016
United States
Urban
RCT
Randomised via block design
Data collected at baseline and 10 months postpartum
Participant completed questionnaires
Videotaped observation of triadic family interactions which were then coded
Mothers-to-be
Fathers-to-be
Group
399
Family Foundations is a transition to parenthood universal prevention intervention. Nine sessions (five prenatal and four postnatal) are held and aim to address parent mental health, couple relationship functioning to impact children’s long-term emotional, mental health and academic outcomes
Control group families were sent written materials on child care choices and stages of child development
Co-parenting
Couple relationship quality
Parenting quality
Parent adjustment
Infant behaviour
FV
Significant positive intervention effect on many outcomes.
Significant intervention impact with large effect size for three of four violence outcomes.
Relationship satisfaction was lower among intervention couples
Roopnarine & Dede Yildirim, 2018
United States
Both
RCT
Data were collected 15 & 36 months after random assignment
Survey
Mothers
Fathers
Group
3045
Building Stronger Families is a relationship skills education intervention with low-income unmarried couples designed to improve child and parent wellbeing. Delivered in eight sites and used one of three curricula, delivered weekly over 5 to 6 months. Coordinators provided couples with emotional support and relationship building skills. Support was provided to men to access education, employment, and mental health services.
This article specifically examines father data only and the relationship between the intervention, paternal depression, IPV and childhood behaviours
Unclear
(Father only)
Depressive symptoms
IPV
Avoidance of destructive conflict behaviour
Paternal warmth
Child internalising and externalising behaviours
The intervention had a positive influence on paternal depressive symptoms and IPV at 15 months post intervention.
The intervention also seemed to improve father–child relationships and childhood development
Satyanarayana et al., 2016
India
Urban
RCT
ICBI vs treatment as usual
Spouse and child FU at 1 and 3 months post patient discharge
Male inpatients in mental health facility
Group
177
Effectiveness of an integrated cognitive–behavioural intervention (ICBI) in reducing use of IPV among alcohol dependent men and improving mental health of spouse and children.
Eight CBT sessions (45 to60 mins) on alcohol and IPV, triggers for alcohol use and IPV, consequences and prevention of IPV
Treatment as usual: pharmaco-therapy and psycho-education
Men: alcohol intake, IPV perpetration
Women’s mental health
Child mental health and behaviour
Lower IPV perp, women had less depression, anxiety and stress.
No difference in alcohol use by men or child behaviour change between groups from baseline to 3 month FU
Steele et al., 2019
United States
Urban
RCT
Questionnaires
Parent–child observation
Mothers
Children (aged 0 to 3)
Group
78
Group attachment-based 26-week intervention (GABI) for parents and their children that is trauma-informed where families (parents and/or children) have adverse childhood experiences (ACE-including domestic violence). Parents attend with their children up to three times weekly for 2hrs. It seeks to address intergenerational trauma and promote a secure attachment relationship between the mother and child
Systematic Training for Effective Parenting (STEP) intervention
ACE
Mothers’ BMI
Zero to three psychosocial & environmental stressors
Only reports on maternal behaviour (supportive presence and maternal hostility) and mother–child interaction behaviours and reciprocity differences between groups.
Improved maternal presence and dyadic reciprocity.
Declines in maternal hostility and dyadic constriction (proxy measures for risk of child abuse)
Stover, 2015
United States
Urban
RCT (pilot)
Pre, post and 3 months FU surveys
Completed by children’s father and mother
Fathers
Individual and dyadic
18
Fathers for Change includes: 1) focus on the fathering role as a motivator for change; 2) integration of strategies for reducing IPV and substance abuse (SA) in each session; 3) intergenerational transmission of IPV and SA; 4) communication skills and co-parenting; 5) the impact of IPV and SA on child development; and 6) parenting skills
Usual treatment: drug counselling sessions over 16 weeks
Severity of violence
Substance abuse
Parenting
Psychiatric issues
Father–child relationship
Fathers for Change group – more likely to complete treatment, program satisfaction.
Less parental intrusiveness on free play between father and child than controls.
Trend seen in less IPV
Mixed designs (RCT and non-RCT)
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Anis et al., 2020
Canada
Urban
2 x pilots
1 RCT and 1 non-RCT
Pre–post parent questionnaire
Mothers and children (0 to 32 months).
Co-parent in three sessions
Dyadic and triadic
Study 1 (RCT) – 20
Study 2 (non-RCT) –10
ATTACH (Attachment and Child Health)
Parental reflective function-focused intervention. Psycho-educational parenting program of 10 to 12 sessions
Usual care: Nurturing Parent Program
Parent–child interactions
Child development
Study 1 and 2: improved parent–child interaction quality and child development
Letourneau et al., 2020
Canada
Urban
3x pilots
Two RCTs and one Non RCT
Pre–post parent survey via therapist interviews and video recordings
Mothers and children (9 to 36 months). Co-parent in two to three sessions
Dyadic and
triadic
Study 1 (RCT) – 20
Study 2 (non-RCT) – 10
Study 3 (RCT) – 10
ATTACH
Parental reflective function-focused intervention. Psycho-educational parenting program of 10 to 12 sessions
Study 1: usual care: Nurturing Parent Program
Study 3: parenting program called “Theraplay”
Parental reflective function
Maternal–child attachment
Studies 1 and 3: improvement in attachment, significant improvements in child reflective functioning and trend in improved maternal reflective functioning.
Study 2: Significant improvement in maternal and overall reflective functioning. Trend towards improved attachment
Non-randomised controlled study
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Waldman-Levi & Weintraub, 2015
Israel
Unclear
Pre- & post- testing with control group
Questionnaire administered via interview
Mothers
Children
Dyadic
37
FI-OP (Family Intervention for Improving Occupational Performance)
A crisis-based intervention offered in eight domestic violence (DV) shelters – eight sessions @30 mins
Aims to improve mother–child interaction and children’s play functioning for families who have experienced DV. It is based on attachment, social learning and social-cognitive theory and the concept of a “secure space”
Playroom program
Preschool play & playfulness
Parent/infant interactive behaviour
Significant difference in intervention group for some aspects of mother–child interaction and children’s play skills.
Not significant in other areas
Schechter et al., 2015
United States
Urban
Pre- & post- with comparison groups
Clinician-administered questionnaires
Mothers
Children
Dyadic
59
CAVES, a clinician-assisted video-feedback exposure intervention with a sample of non-referred community mothers who have experienced IPV and their children aged 1 to 4. It aims to change parental state of mind and associated behaviours toward children in a relatively brief period of time
All received intervention but were grouped by post-traumatic stress disorder (PTSD) ratings.
Controls were those with no PTSD diagnosis
Depression and mood
Maternal attribution
Reduction in degree of negativity in clinically significant PTSD group towards their child but not themselves or their primary attachment figure
Pre- & post- no comparison group
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Rizo et al., 2018
United States
Unclear
Pre-3m post and 6m FU pilot study
Questionnaire – self-completed or administered
Mothers
Children 5+ (in concurrent therapeutic support group)
Group
73
Mothers Overcoming Violence Through Education and Empowerment (MOVE), a community-based, service-mandated 13-week (meet once per week for 2.5 hours) psychoeducation program to address the safety, parenting and mental health needs of mothers exposed to IPV
N/A
Safety
Parenting
Maternal mental health
Significant reductions in depression and post-traumatic stress
Southwell, 2016
Australia
Both
Pre- & post- testing
Parent assessments
Parent feedback survey (administered via interview with therapist)
Therapist reports
Children (parent–child therapy may be offered)
Individual
41
YETI (yourtown’s Expressive Therapies Intervention) intervention for traumatised and attachment-disturbed children. Therapies include art, music, drama, dance/movement, poetry and bibliotherapy, play and sand play. No set number of sessions, 30 to 60 mins. Provided at 2 sites: a child and family service centre and a DV refuge
N/A
Child behaviour
Significant improvement in all measures except somatic complaints
Bunston et al., 2016
Australia
Urban
Pre- & post- testing
Mixed methods
Parent-rated questionnaires
Clinician-rated questionnaires
Qualitative data via open-ended questions in satisfaction survey
Mothers
Children
Group
105 mothers with 133 infants
Peek-a-Boo Club, a therapeutic infant/mother group intervention used “infant led” approach to repair the relationship after DV. Based on object relations and attachment theory frameworks. 11 x 2-hour sessions held in three phases: encouraging engagement, encouraging reflection, and encouraging consolidation
N/A
Infant functioning
Mother–infant attachment
Clinician-rated carer–infant functioning
Improved scores for infant, mother and infant–mother functioning.
Authors assessed clinical significance and found that only some of the improvements were clinically significant
Pernebo et al., 2018
Sweden
Urban
Pre- & post- testing
Mixed methods
Surveys, structured interviews, self-report inventory measures
Children aged 4 to 13 (mean age 7 years) and their mothers
Group
31 in CBI and 19 in psychotherapeutic=50
Two interventions:
1) community-based psycho-educative intervention (CBI): “Children are People Too”
2) psycho-therapeutic treatment intervention: “Trauma-focused group psychotherapy for children with experience of FV” (CAMHSI)
Both interventions included parallel group sessions for children and for abused parents and entailed 12 to 15 weekly 90-minute sessions. Groups included four to eight children
N/A
IPV (CTS2)
Child mental health, emotional regulation and behaviour
Child trauma
Maternal mental health
Maternal trauma
Both interventions substantially reduced maternal post-traumatic stress.
Children’s trauma symptom reduction was larger (and more sustained at 12-month follow-up) in the psychotherapeutic intervention, and children with initially high levels of trauma symptoms benefited the most
Pernebo et al., 2019
Sweden
Urban
6- and 12-month FU study on sustainable change
As above
Children aged 4 to 13 (mean age 7 years) and their mothers
Group
31
As above
N/A
As above
Sustained treatment gains reported, no increase in symptoms or increase in IPV
McConnell et al., 2017
United Kingdom
Unclear
Pre- & post- testing with 6-mth FU
Small cohort study with unmatched comparison group also done at one centre (small numbers)
Mixed method
Note: fathers, partners and children participated in evaluation.
Partners and children: face-to-face surveys with practitioners.
Fathers: surveys, case records analysis, qualitative interviews with subgroups of partners and children
Fathers
Group
271
Caring Dads Safer Children, based on a Canadian intervention. Delivered across five centres. Fathers attended 2-hour weekly sessions for 17 weeks, with one individual session at end of program.
Goals: 1) develop trust and motivation to examine their fathering; 2) increase awareness of child-centred fathering; 3) increase awareness and responsibility for abusive and neglectful fathering; 4) consolidate learning, rebuild trust and plan for future
N/A
Fathers’ attitudes & parenting behaviours
Fathers’ controlling behaviour towards partners
Children’s and partners’ wellbeing
Significant improvements in fathers reported in parental distress, parent–child dysfunctional interaction, perceptions of child being difficult, overall parenting stress score. Only one change in parenting behaviour (reduced hostility and aggression subscale). Some significant improvements in fathers’ controlling behaviour towards partners.
Some fathers’ attitudes & behaviour did not change, or only changed partially or temporarily.
Children reported improvement in parenting behaviour but not statistically significant.
Inconclusive findings for children’s wellbeing, but improvements in partners’ wellbeing
Berry et al., 2019
United Kingdom
Urban
Pre- & post-feasibility study
Mixed methods
Surveys, semi-structured interviews and focus groups with parents, facilitators and managers
Mothers
Group
19 mothers
Family Vision, a life coaching program for single mothers with experience of FV with pre-school and school-aged children
N/A
Parent efficacy
Mental wellbeing
Child–parent relationship
Strengths and difficulties
Appears to be feasible and acceptable. Did not conduct significant tests on outcomes
Domoney et al., 2019
United Kingdom
Both
Pre- & post- testing
Data collected at baseline, 1 year and 2 years
Mixed methods
Quantitative outcome data
Qualitative interviews
Observations of child development and parent–child interactions
Data collected via interviews
Mothers
Fathers
Individual
40
For Baby’s Sake, a trauma-informed whole family, home visiting intervention for parents from pregnancy – 2 years postpartum to break DV cycle and improve child outcomes. Staff come from a variety of backgrounds & provide face-to-face therapeutic sessions to parents to assist with past behaviours and experiences, including ACEs, current DV
N/A
Domestic abuse
Mental health
Parenting
Child development
Child behaviour
Participant experience
Preliminary data only available
Waters et al., 2015
United States
Urban
Pre- & post- testing with 6-mth FU
Clinician-administered assessments
Video recording of play between mother and child made and coded
Mothers
Children
Dyadic
52
Perinatal adaptation of child–parent psychotherapy (CPP) intervention for predominately Latina, low-income pregnant women with a history of IPV. Includes psychoeducation on pregnancy, childbirth, infant development and the impact of IPV on the foetus/baby. Also some PTSD response therapy, maternal insight into negative attributions to her infant. Sessions continued 6 months after birth
N/A
PTSD
Abuse
Trauma
Parenting inventory
Maternal sensitivity
PTSD decreased and their child-rearing attitudes improved.
Greater improvements in child-rearing attitudes predicted higher levels of maternal sensitivity, however improvements in PTSD did not
Stover et al., 2017
United States
Urban
Pre- & post-
Mixed method feasibility study
Quant: written assessment at baseline. Post-assessment follow-up completed by research assistant
Therapy sessions were video recorded to assess treatment adherence
Qual: Two focus groups with sub-set of fathers (n=11)
Fathers
Individual and dyadic
44
Fathers for Change emphasises fathering role as a motivation to continue treatment. Delivered to fathers in substance use disorder treatment with a history of IPV. Delivered over 16 weeks, it addresses 14 topics in 60-minute sessions. Combines attachment, family systems & CBT. Goals are: 1) maintaining abstinence from substances; 2) cessation of violence & aggression; 3) decreased child maltreatment; 4) improved co-parenting
N/A
Addiction severity
Anger intensity
Emotional regulation difficulties
Thoughts related to jealousy and anger
Satisfaction with intervention
Significant improvement in anger, emotional regulation, co-parenting, dependency, personalisation, explicit negative affect measures.
High level of satisfaction and attendance
Lavi et al., 2015
United States
Urban
Pre- & post- pilot
Participants and clinicians completed written assessments
Mothers (to be)
Children
Dyadic (before and after birth)
64
CPP intervention with pregnant mothers continuing post-birth. Referred if reported to the social worker that they felt unsafe in their relationship.
Aims to prevent and/or ameliorate short- and long-term consequences of IPV on child and maternal wellbeing and safety.
Perinatal adaptation includes consideration of unique emotional and physical transitions that occur during this time
N/A
Attachment
Depression
PTSD
Child-rearing attitudes
Significantly low levels of depression and PTSD symptoms (PTSS) post-treatment.
Women displayed higher levels of positive child-rearing attitudes post-treatment.
Women with low levels of maternal–foetal attachment prior to treatment showed the greatest improvement in depression, PTSS and child-rearing attitudes
Hagan et al., 2017
United States
Urban
Pre- & post- testing
Parent-reported PTSS
Some were clinician-administered via interviews
Mothers
Children
Dyadic
199
CPP intervention provided to a cohort referred for outpatient mental health services at an urban public hospital. Unstructured weekly 1hr sessions were held.
Goal: to foster physical and emotional safety in the caregiver–child relationship to restore the child’s health & developmental progress
N/A
PTSS
Exposure to traumatic events
Treatment characteristics
Reduction in PTSS for parents and children.
Extent of improvement varied depending on child, parent and treatment characteristics.
Reduction greater in families who reported fewer traumatic life events for parents
Herschell et al., 2017
United States
Urban
Pre- & post- testing (pilot study)
Data collected at baseline, mid-treatment and post-treatment
Assessments were conducted by independent research assistants. Parents completed assessment questionnaires
Parents (mainly mothers)
Children
Dyadic
21 (only 9 dyads completed PCIT)
A parent–child interaction therapy (PCIT) intervention in a DV shelter, provided by community-based clinicians. Sessions were provided weekly and treatment was for 12 to 20 weeks.
First phase: child-directed interaction, which focuses on relationship enhancement. Second is parent-directed and focuses on effective discipline and limit setting
N/A
Life experiences (exposure to traumatic events)
Child behaviour
Parenting practices
Parental mental health
Treatment engagement and satisfaction
Positive significant effect on child behaviour, some parenting practices and mental health symptoms.
No significant improvement in some measures including positive parenting practices.
High dropout rate.
Small numbers due to pilot study
Other (single case study, series)
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Morales et al., 2015
United States
Unclear
Single case study
Quantitative data collected at baseline and one- and three-month FU
Self-reported measures (computer delivered)
Qualitative data
Mother
Group & individual
One
SafeCare – home visitation program
Aims to reduce risk of child maltreatment and recognises that IPV and child maltreatment frequently co-occur. SafeCare Parent–Infant Interaction module aims to reduce both.
This study examines the cultural adaptability of the model for Latino families
N/A
Parenting skills
Daily activities
Conflict
Child abuse potential
Neglectful behaviour
Brief symptom inventory
Parenting stress
Protective factors
Satisfaction
Improvements in all measures against baseline and high levels of satisfaction with intervention delivered in participants’ primary language.
Needs effectiveness study with larger group
Keeshin et al., 2015
United States
Unclear
Case series
They compared use of positive and negative comments in first 5 mins of individual sessions attended
Clinician-rated coding
Mothers
Children (2 to 5 years) in DV shelter
Dyadic & group
Eight (mother–child dyads)
The provision of PCIT at a self-contained extended stay shelter.
Between two and eight x 30 min dyadic sessions and 7x weekly 90-min group sessions were held
N/A
Clinician-rated mothers’ use of positive and negative comments.
Themes brought up at group sessions
More positive comments used as sessions continued.
Mothers increased their use of PRIDE skills and valued the opportunity to reflect on their parent–child interactions during group sessions
Qualitative studies
Author, date
Country of origin
Urban, rural or both
Study design (most dominant design)
Data collection methods
Participants
Group, dyadic or individual
Sample size
Brief description of intervention
Control group
Outcomes assessed
Evidence of effectiveness?
Broady et al., 2017
Australia
Both
Qualitative
One-on-one interviews
Thematic analysis undertaken
Fathers
Group
21
Taking Responsibility is an 18-week group course for fathers complemented by periodic individual support sessions. Program covers topics such as tactics of power and control, exploring beliefs about male and female roles, understanding the impact of violence on others (including children), developing empathy and exploring thinking processes underpinning men’s behaviour
N/A
Perceptions and personal narratives regarding experiences of the program and behavioural change.
This paper specifically focuses on participants’ children and parenting relationships
Fathers’ desire to maintain and improve relationships with their children, however, some fathers reported a belief that their children had not been impacted by their violent behaviour
Kamal et al., 2017
Sweden
Unclear
Qualitative
Focus groups
Mothers
Fathers
Group
26
Parenting and Violence, a 10-week attachment-based psycho-educational intervention for parents who are victims or perpetrators. Each group has maximum five participants, with mothers and fathers grouped separately. Sessions are 1.5 hours Aims: 1) increase parental awareness and involvement in child perception of violence; 2) minimise impact of violence on child development; 3) prevent violence from following child into adulthood & their future relationships
N/A
Experiences of intervention
How intervention influences participants’ handling of family situations
Participants perceived improved self-control, self-esteem and communication skills and these seemed to positively influence their children’s wellbeing and behaviour
Pernebo & Almqvist, 2016
Sweden
Urban
Qualitative
2016 – interviews
Nine children (4 to 6 years) post therapy.
78% had no contact with perpetrator
Group
Nine
Group trauma-informed therapy (weekly sessions with parallel group for mother) for children who have exposure to IPV against mother
N/A
Experience participating in group therapy and completed a drawing of experience
Themes using interpretive phenomenology
1. Joy
2. Security
3. Relatedness
4. To talk
5. Competence
APPENDIX F:
Summary table of interventions identified
Randomised controlled trial protocols
Author and date
Intervention title
Scott et al., 2017
Caring Dads (CD) and Mothers in Mind (MIM)
Visser et al., 2015
Trauma Focused Cognitive Behavioural Therapy (TF-CBT)
Randomised and non-randomised controlled studies
Author and date
Intervention title
Jack et al., 2019
Nurse Family Partnership Home Visiting with IPV (HV-IPV)
Graham-Berman et al., 2015; Miller-Graff et al., 2016
Preschool Kids’ Club (PKC) and Mothers’ Empowerment program (MEP)
Howell et al., 2015; Grogan-Kaylor et al., 2019
MEP
Feinberg et al., 2016
Family Foundations
Letourneau et al., 2020; Anis et al., 2020
Attachment and Child Health (ATTACH)
Roopnarine et al., 2018
Building Strong Families
Satyanarayana et al., 2016
CBT
Steele et al., 2019
Group Attachment-Based Intervention (GABI)
Stover, 2015; Stover et al., 2017
Fathers for Change
Waldman-Levi et al., 2015
Family Intervention for Improving Occupational Performance (FI-OP)
Schechter et al., 2015
Clinician Assisted Video feedback Exposure Sessions (CAVES)
Pre–post observational studies
Author and date
Intervention title
Berry et al., 2019
Family Vision
Bunston et al., 2016
Peek-a-Boo Club
Domoney et al., 2019
For Baby’s Sake
Hagan et al., 2017
Child–Parent Psychotherapy (CPP)
Herschell et al., 2017
Parent Child Interaction Therapy (PCIT)
Lavi et al., 2015; Waters et al., 2015
Perinatal CPP
McConnell et al., 2017
Caring Dads Safer Children
Pernebo et al., 2018, 2019
Community Based Intervention (CBI) and Child and Adolescent Mental Health Service Intervention (CAMHSI)
Rizo et al., 2018
Mothers Overcoming Violence Through Education and Empowerment (MOVE)
Southwell et al., 2016
yourtown’s Expressive Therapies Intervention (YETI)
Qualitative and other studies
Author and date
Intervention title
Broady et al., 2017
Taking Responsibility
Kamal et al., 2017
Parenting and Violence
Keeshin et al., 2015
PCIT
Morales et al., 2015
Safe Care
Pernebo et al., 2016
Trauma-Informed Therapy
APPENDIX G:
Intervention descriptions
Group work: Psychoeducational, psychotherapeutic
Group work can be defined as an endeavour where individuals choose to meet for the specific and mutual purpose of interacting with one another to achieve identified goals. A facilitator is responsible for organising and maintaining the agreed-upon setting and fostering group engagement. There are many group formats which may include psychoeducational groups and psychotherapy groups. Psychoeducational groups emphasise the delivery of specific educational content by the facilitator, for example a group on “parenting skills”, and may be run much like a tutorial whereby the group task is to learn the concepts and explore these in the format of group activities, discussion and reflection. These groups are often manualised, with set content and activities for each group session. Psychotherapy groups emphasise experiential learning with the “educational content” arising from within the context of the relationships in the group. For example, the psychotherapy group may be for women wishing to explore the difficulties that they encounter as mothers and agreeing to share their respective experiences with each other as a basis for learning, discussion and development. This is in distinction to psychoeducational groups where set pre-prepared educational content is introduced. The group tasks in these instances are therefore for participants to observe and reflect upon their own states and those of others. Although there is no set content for sessions, the focus for the group and other variables are often set by group participants at the onset of the group. In principle, psychoeducational groups can be delivered to larger groups of participants whereas psychotherapy groups are usually smaller to ensure that each participant has time to be heard and understood by the group as part of the treatment process (Erford & Bardhoshi, 2018).
Psychotherapies: Individual, parent, dyadic
Psychotherapy (or therapy) is a form of mental health treatment that uses communication between two or more people as treatment method. There are a range of psychotherapies or therapies that focus more or less on either the nature of the relationship/s between two people as a means of understanding and overcoming barriers clients encounter in their relationships (psychoanalytic, psychodynamic, attachment-based or family therapies), or identifying and changing clients’ specific problematic behaviour or thought processes (cognitive behavioural or cognitive analytical therapies; Nardone & Salvini, 2019).
Psychotherapy can be undertaken by an individual, adult couple, child and parent dyad or family. Individual therapy is usually focused on problems related to an individual’s functioning. For example, a woman affected by violence may seek therapeutic help with her wariness in relationships or with her capacity to relax and sleep at night after her experiences of violence. Alternatively, a woman may be more immediately concerned with her child’s recovery and her confidence in parenting, so she may seek a form of parent therapy to focus specifically on this. Both individual and parent therapies may be exclusively psychodynamic or cognitive, or a mix of both, according to need.
Children may be supported either by individual or dyadic therapies. Because children may depend less on talking for communication and more on non-verbal cues and play, these broader forms of communication are also employed by child therapists, pitched to developmental capacity. Dyadic therapy (also referred to as mother–child, parent–child, child–parent, relational, or infant–parent therapy) engages both child and parent simultaneously in the treatment to directly redress relationship tension between them, and is the treatment of choice where the child is under the age of 6 due to their level of caregiver dependence (Dowling, 2019; Nardone & Salvini, 2019).
Tailored individual and dyadic interventions are particularly appropriate for infants, young children and affected mothers after IPV, given that the trauma of family violence is known to impact not only each individually but their relationships with one another. These dyads can also be supported in bigger group work settings, however the clinician’s capacity to respond specifically to the individual needs of the dyad (which we will call small dyad work) is limited where there are bigger numbers. This may be offset for the dyad by the positive impact of knowing that they are not alone in their experience in relation to their peers and indeed in an ideal service system perhaps a suite of group work and individual and small dyad therapies would be available. However, there are many dyads who require tailored small dyad work before, during or after group-work intervention where, within the privacy and specificity of this setting, they can develop the trust with their clinician that may be needed to revisit and reset the impact of family violence trauma upon their relationship.
APPENDIX H:
Maternal interview schedule
- Introduction
- Reminder of consent and reassure confidentiality
- Explain that sometimes talking about personal experiences in a research project can be distressing and we can stop at any time if you need to. You may like to talk further about some of the issues raised, either with the researcher, therapist or with someone else afterwards. Resource material will be provided at the beginning of the interviews for referral options including phone and website options.
- Explain recording and approximate time frame
- Any questions before we begin?
We are interested to know about your general experience with the CPP treatment you have recently completed with your child.
Perceived benefits
- Thinking back to the start of treatment, can you tell me what you hoped or expected from the program? Changes/benefits for your child? For yourself? Mother-child relationship?
- What outcomes/results of treatment are most important to you? E.g. understanding the violence and its effects, communication between mother and child, reduction in behaviour problems
Acceptability/satisfaction
- Do you know how many sessions you completed?
- In general how was your experience with the therapy? Have you and your child been helped with what you wanted? If yes, how do you think this has occurred? Enablers? If no why? Barriers?
- How do you think the experience was for your child?
- Was there something that has been particularly good?
- What has been most helpful for you?
- What has been most helpful for your child?
- Was there any aspect of the treatment that you did not like?
- In the survey (completed with therapists) were there any questions you did not feel comfortable answering? General health, mental health, quality of life, child behaviour, exposure to violence, relationship with child, parenting?
- How was your experience with being video recorded during the play sessions?
- Therapy can be confronting, was there anything in the treatment that made you feel uncomfortable?
- Does the method need to be adjusted in any way to work better? Can you suggest how?
- Are there any things you would like help with now that the treatment has not addressed?
Children’s contribution
- How do you think children have experienced the intervention
- Were there child initiated moments of change or turning points in the dyad interaction you could identify? Can you give an example
- How did children respond to the questioning of mothers e.g. survey questions
- Children’s general influences/contribution of the therapy
Feasibility
- Have there been any difficulties for you to attend sessions and participate in treatment? If so what were these? (e.g. travel, costs, illness, interaction with perpetrator, the child does not want to attend etc.)
- Can you tell me what the costs have been to attend treatment each week e.g. weekly bus fare? Child care for other children, loss of wages etc.
Participation
- Have you changed since receiving treatment? If so, how?
- Has your child changed? How?
- Have you ever received any similar treatment like this for yourself and your child?
- Did you get enough information about the treatment before you decided to participate? Was there any information missing?
- Have you and/or your child received any other support while you have been in treatment?
- To what extent have you and your child had interactions with the partner who abused you during treatment e.g. daily, weekly, monthly, never?
- Do you think you will use the things you have learnt in the treatment?
- What do you think will happen now that you and your child have completed treatment?
Is there anything else you would like to discuss about your experience with receiving CPP treatment?
Check how they are feeling after the interview to ensure that any feelings of distress are supported.
Thank you
Read the PDF version of the report
This report addresses work covered in the ANROWS research project RF.19.02 “RECOVER – Reconnecting mothers and children after violence: The child-parent psychotherapy pilot”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Plan Outcome 4 – Services meet the needs of women and their children experiencing violence.
Suggested citation:
Hooker, L., Toone, E., Wendt, S., Taft, A., & Humphreys, C. (2021). RECOVER – Reconnecting mothers and children after family violence: The child–parent psychotherapy pilot (Research report, 05). ANROWS.
Judith Lumley Centre, La Trobe University
Plenty Rd & Kingsbury Dr, Bundoora VIC
La Trobe Rural Health School, La Trobe University
Edwards Rd, Flora Hill VIC
Author acknowledgement
Thank you to all children, mothers, therapists and organisations who participated in RECOVER. Thank you to our industry partner, Berry Street, and Marg Hamley for early championing of the project, and Sally Watson (South Australian Branch, Australian Association for Infant Mental Health), Julie Larrieu (Tulane University), Chandra Ghosh Ippen (University of California) and Kjerstin Almqvist (Karlstad University) for sharing their knowledge. Thank you also to Dr Jess Ison for research assistance and support, including preparation of this document. We also extend our gratitude to our steering committee: Tom Bowerman (Berry Street), Vibhay Raykar (Goulburn Valley Health), Anita Morris (Department of Families, Fairness and Housing, Victoria) and Elizabeth Westrupp (Deakin University).
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732) and Lifeline (13 11 14).
Contents
Implications and recommendations for policymakers
Implications and guidance for practitioners and service providers
Part 1: State of knowledge review
1. How acceptable and feasible is CPP to the Australian context?
2. Do CPP therapists-in-training adhere to CPP model fidelity?
3. How effective is treatment by CPP therapists-in-training during the study?
Implications and recommendations for policymakers
Implications and guidance for practitioners and service providers
APPENDIX A: Keyword search terms and grey literature sites searched
APPENDIX B: Ovid MEDLINE search strategy
APPENDIX C: Grey literature search: Relevant websites
APPENDIX E: Summary table of included studies
APPENDIX F: Summary table of interventions identified
APPENDIX G: Intervention descriptions
Group work: Psychoeducational, psychotherapeutic
Psychotherapies: Individual, parent, dyadic
APPENDIX H: Maternal interview schedule
Key definitions
| Concept | Definition |
|---|---|
| Cisgender | A person who identifies as the gender they were assigned at birth. |
| Dyad | A grouping of two participants. In this report we refer to a dyad as the caregiver and child receiving child–parent psychotherapy (CPP). |
| Dyadic interventions | Dyadic interventions (also referred to as mother–child, parent–child, child–parent, relational, infant–parent therapy) are a model of therapeutic or mental health and wellbeing care that engage both child and parent simultaneously and focus on their relationship as target for change. |
| Family violence | Family violence (FV) is defined by the Victorian Department of Families, Fairness and Housing (2018) as any violent, threatening, coercive or controlling behaviour that occurs in current or past family, domestic or intimate relationships. This includes not only physical injury but direct or indirect threats, sexual assault, emotional and psychological torment, economic control, damage to property, social isolation and any behaviour which causes a person to live in fear. |
| Intimate partner violence | Intimate partner violence (IPV) is defined as behaviour by a partner or ex-partner that includes physical, sexual and/or psychological abuse and controlling behaviours. |
| Practice champions | Leadership figures within an organisation who are skilled in a particular intervention and passionate about using evidence to inform practice. RECOVER practice champions supported the implementation of CPP in the clinical settings and reported back regularly to the research team. |
| Shadow pandemic | The increase in violence against women, especially IPV, since the outbreak of the COVID-19 pandemic. |
| Therapeutic readiness | Therapeutic readiness is a term initially coined in relation to the application of child psychiatry within community settings (Despert, 1949). It considers factors internal and external to the child and caregivers that are conducive to treatment engagement and success. CPP provides a foundational framework that equips clinicians to determine therapeutic readiness, considering child and family strengths and contextual risks (Lieberman et al., 2015, p. 265). |
| Trauma- and violence-informed care | Incorporates an understanding of the effects of trauma while accounting for intersecting impacts of systemic and interpersonal violence and structural inequalities (Wathen et al., 2021). |
Executive summary
Background
Family violence, especially intimate partner violence (IPV), is prevalent in Australia (Australian Institute of Health and Welfare [AIHW], 2019). IPV is defined as behaviour by a partner or ex-partner that includes physical, sexual and/or psychological abuse and controlling behaviours (World Health Organization [WHO], 2013a). While people of all genders and sexualities can experience IPV, the focus of the RECOVER project is on IPV perpetrated by men in cisgender heterosexual couples and the harm it causes mothers
and children.
Globally, up to one in three women have experienced IPV in their lifetime. Higher rates of IPV are noted in low- and middle-income countries compared to high-income countries like Australia (WHO, 2021). In Australia, one in six women (and one in 17 men) report an experience of partner violence since the age of 15 years (Australian Bureau of Statistics [ABS], 2017). Women’s mental health, parenting and relationships with their children can be profoundly impacted by partner violence (Hooker, Kaspiew, & Taft, 2016; Humphreys et al., 2006; Trevillion et al., 2012). Couple relationships are complex and separations stressful, particularly when there has been violence in family relationships (Jones & Bunston, 2012). Separations after IPV are particularly fraught and often complicated by ongoing patterns of coercive control, harassment and physical dangers, including fatality risks to women and children (AIHW, 2019).
Twenty per cent of young Australian children experience poor mental health (AIHW, 2020), but less than 1 per cent of under four-year-olds receive treatment (Segal et al., 2018a).
Children’s mental health, wellbeing and the relationships that they depend upon for their development and recovery are all impacted by IPV (Humphreys et al., 2018; James-Hanman & Holt, 2021; Morris et al., 2015). These harms to health and wellbeing are extensive (Fitzpatrick et al., 2020; Trevillion et al., 2012; Vu et al., 2016), hampering the recovery of the mother–child relationship (Buchanan & Humphreys, 2021; Humphreys et al., 2006). Less is known about the impact of IPV use on father–child relationships, although these relationships too may be distorted (Mohaupt et al., 2020; Stover et al., 2020). Of all age groups, very young children are disproportionately affected by traumatic events and the most developmentally vulnerable to IPV-related physical dangers and relational harms (Lieberman, Chu et al., 2011; Lyons-Ruth et al., 2017). While the harms to older children and adolescents from family violence are well known (Evans et al., 2008; Kitzmann et al., 2003; Vu et al., 2016), the extent of burden to pre-school-aged children’s mental health from family violence is less clear (Howell et al., 2011; Orr et al., 2020). Twenty per cent of young Australian children experience poor mental health (AIHW, 2020, p. 87), but less than 1 per cent of under four-year-olds receive treatment (Segal et al., 2018a). Programs that include mothers and children together (dyadic interventions) show significant benefits (Anderson & van Ee, 2018). Child–parent psychotherapy (CPP) is an evidence-based dyadic intervention initially designed for young children and their mothers affected by IPV to strengthen their relationship and positively impact on their mental health (Lieberman et al., 2015).
Across several randomised controlled trials (RCTs), CPP has been shown to reduce child behavioural problems and maternal and child trauma and mental health symptoms (Cicchetti et al., 2000; Cicchetti et al., 2011; Ghosh Ippen et al., 2011; Lieberman, Van Horn & Ghosh Ippen, 2005; Lieberman et al., 2006), and improve attachment between mothers and children (Cicchetti et al., 1999; Toth 2002, 2006). CPP improves mental health outcomes in children and mothers simultaneously and treatment effects are maintained over time (Lieberman et al., 2015).
The state of knowledge review completed for this report identified very few evidence-based preventive treatments for mothers and children affected by IPV, especially in Australia. The present report identifies the need for suitable treatment for women and children exposed to IPV and reports on a pilot evaluation of CPP for this population in Australia.
Project aims and methodology
Aims
To test the feasibility of implementing CPP into the Australian context for children and their mothers affected by IPV.
Research questions:
- How acceptable and feasible is CPP to the Australian context?
- Do therapists adhere to CPP model fidelity?
- How effective is CPP treatment at improving maternal and child health and wellbeing outcomes?
About the intervention
Child–parent psychotherapy is a relationship-focused treatment for parents and young children who have experienced trauma (Lieberman et al., 2015). CPP originated in the psychoanalytic tradition of infant–parent psychotherapy and was designed for mother–child dyads affected by IPV, integrating a lens of social justice (Cerulli et al., 2021; Lieberman, 2004; Lieberman et al., 2015). Although CPP has since found application in other trauma populations, in this project, exposure to IPV is the trauma of focus. The goal of CPP is to support and strengthen the parent–child relationship, which acts as the vehicle to restore the child’s sense of safety, attachment, and social and emotional wellbeing. CPP is a manualised, flexible intervention, where the goals of treatment are co-designed with mothers and children. Treatment is offered by qualified therapists, weekly for up to 12 months or longer if needed and includes parent-and-child play sessions and collateral, parent-only reflective sessions. Through a range of modalities such as developmental guidance, insight-oriented interpretation and advocacy, treatment aims to help children and parents make sense of, and recover from, trauma (Lieberman et al., 2015). Opportunities for change are harnessed within spontaneous child–parent interactions. Parents are helped to understand the impact of trauma on their parenting and to confidently respond to their child’s behaviour as a form of communication (Lieberman et al., 2015; Lieberman et al., 2019). A detailed explanation of the RECOVER study background and methodology has been published elsewhere (Hooker et al., 2019).
Study sites and recruitment
Eleven community-based, clinical sites including specialist family violence services (with clinical services for children), child and adolescent mental health services (CAMHS), one enhanced maternal and child health centre with a multidisciplinary team and co-located infant mental health specialist, and one private perinatal psychiatry clinic participated in RECOVER and actively recruited suitable mother–child dyads for the study. These included four urban and seven rural/regional sites. Recruitment was staggered as new sites came on board and occurred over two waves – RECOVER 1 in 2018 and RECOVER 2 in 2019–20, with the welcome addition of ANROWS funding in the form of legacy funds from the former Luke Batty Foundation.
We looked for mother–child dyads using the following inclusion criteria:
- pre-school-aged child (3 to 5 years)
- English-speaking biological mothers
- recent exposure to IPV (past 12 months) and with advocacy support already received
- clinical signs of trauma (e.g. child presenting with emotional or behavioural issues/impaired mother–child interaction based on clinical assessment)
- therapeutic readiness: post-crisis situation, or not living with the person using violence.
Mixed methods evaluation
Program evaluation involved mixed methods, including:
- semi-structured interviews with CPP therapists, service managers and eligible women. Implementation theory (May & Finch, 2009) guided interview questions and data analysis
- therapists completed fidelity logbooks and documented the dose/number of treatment sessions completed
- maternal survey data and video-recorded free play between mothers and children before (T1), during treatment (T2) and after treatment (T3).
Key findings
Eighteen dyads consented to and received treatment, 15 completed the baseline (T1) survey and 10 mothers completed at least two surveys at two time points, T1 and either T2 or T3. The average age of mothers was 34 years, with children around four years of age. Forty per cent of women who completed the baseline survey were separated from their partners, over half of all women were not working in a paid job (53%), and 60% were on a pension. No women were Aboriginal or Torres Strait Islander, and all were Australian born. Two women were from rural locations and the remaining 13 were city based.
Therapists offered 293 CPP treatment sessions to 15 dyads during the project. The median number of sessions across all dyads was 23 (range 5 to 50). Treatment time was approximately six months. Forty in-depth interviews were completed, including 28 process and impact interviews with therapists (n=15) and managers (n=13), and 12 interviews with women completed after treatment.
She’s just a different child now.
(Mother, 3)
How acceptable and feasible is CPP to the Australian context?
CPP appears feasible for this population of mothers and children affected by IPV under certain conditions, despite the implementation barriers outlined below. The intervention was highly acceptable to study participants. All therapists reported that they found the CPP training enjoyable, and that the intervention suited their clinical needs; they noted swift and satisfying changes in their clients. In line with the concept of victims’ and survivors’ stages of change or readiness (Chang et al., 2006), despite seeking help, some women required alternative supports (e.g. acute mental health treatment) before the intensive dyadic treatment commenced. Managers reported that they felt pleased to be able to offer an evidence-based intervention for this under-serviced population. Therapists reported that children were often drivers of change in the dyadic relationship. The research highlighted that a range of systemic structures and processes need to be in place to enable CPP to occur.
Implementation enablers:
- CPP leaders within services that act as practice champions (or leaders) assisting implementation processes (e.g. recruitment, collaborations)
- therapists with family violence practice knowledge
- therapists with prior clinical experience, especially with young children
- organisations with established therapeutic services within their family violence service
- clear organisational clinical governance, and supportive policy and procedures
- systems that both support therapists and identify victims and survivors.
Implementation barriers:
- coincided with a time of escalating service delivery and service reform demands
- COVID-19 pandemic and impacts on families and clinical services
- limited organisational and workforce family violence knowledge and/or practice skills
- systems and practices that prioritise older children’s mental health needs
- poor collaborative links with family violence networks/referral options (especially in rural areas)
- crisis-driven systems, no time and/or resources to offer early intervention
- restricted access to qualified CPP workforce.
Do CPP therapists-in-training adhere to CPP model fidelity?
In total, eight therapists who provided CPP in the project completed fidelity logbooks for each dyad and recorded their perceived adherence to CPP goals at the completion of each dyadic session. Greater adherence to the model was reported in conveying a sense of hope and aid in developing a relationship with the dyad. Enhancement of safety in therapy was also high. Areas lacking in focus were client care coordination, supporting the child’s relationship with others and helping the dyad put the trauma into perspective. Urban sites reported greater fidelity and adherence to all CPP objectives compared to rural and small services.
How effective is CPP treatment delivered by CPP therapists-in-training during the study?
In the original Lieberman et. al trial (2005), CPP treatment comprised an average of 32 sessions completed by therapists experienced in CPP and delivered to 75 dyads. In our RECOVER study, therapists were still learning the CPP model and provided an average of 23 sessions. Ten RECOVER cases completed T1 and either T2 or T3 surveys and were used in the statistical analysis. Four dyad video interactions with complete data were double-coded and analysed.
In this study, all women reported substantial IPV from a male perpetrator, which reduced significantly after treatment (T3; p<0.005).
Differences across many study outcomes showed no statistically significant effect of treatment, however trends in positive directions were noted across most outcomes. These results are not surprising considering the small sample which limits any conclusions of causation and the effectiveness of CPP in this study. We found no statistically significant change in maternal emotional health, reflective functioning and parenting due to CPP. In addition, no significant changes were seen across child functioning and trauma symptoms, or mother–child attachment.
Two important outcome measures did change significantly, including parental warmth, which increased after treatment (p<0.028), and improved child emotions and behaviours (p<0.005).
I think the best part is … the joy of seeing children and their primary caregiver start to heal with each other and start to feel safe to – to express things to each other that previously they hadn’t been able to – or they had been communicating to each other in a way that had left either party feeling very isolated and alone … It is such a privilege to witness that. (Therapist 6)
Summary
CPP has been shown in several previous RCTs to be an effective dyadic treatment model for mothers and children exposed to IPV (Lieberman, Van Horn & Ghosh Ippen, 2005; Lieberman et al., 2006). The RECOVER project tests the feasibility of implementing this model in an Australian service setting for mother–child dyads affected by IPV, delivered by CPP therapists-in-training. We found that CPP is acceptable and feasible for this population and can be implemented into the Australian setting, in locations with established family violence system partnerships, service capacity to prioritise mental health and wellbeing responses for very young children, and strong clinical governance structures.
Although the intervention was delivered by CPP therapists-in-training and our sample size was too small to conclude efficacy, positive changes were found in child behaviour and parental warmth and reinforced by qualitative reports from women and therapists. Findings also show that women experienced less IPV post-intervention. This may be a natural reduction in abuse over time – from crisis to a more stable environment – rather than a true treatment effect, however, further research to explore this outcome with a larger sample is required.
With the high prevalence of IPV and the contributing “shadow pandemic” arising from the public health response to COVID-19 (Pfitzner et al., 2020) there is an overwhelming demand for evidence-based, relational therapy like CPP. An improved trauma- and violence-informed child mental health workforce is needed (Wathen et al., 2021). Systems reforms facilitating better non-government organisation and public child mental health partnerships and equity of mental health service delivery across the age range are also required for CPP to be expanded in CAMHS for this population of women and children.
I think it’s quite a pragmatic approach … It’s a broad model, it encompasses lots of different therapeutic approaches. It’s not a very limited focus, I think it sees the bigger picture. CPP takes into account the child, the parent, the systems and that’s what really helps. (Manager 6)
CPP is a feasible model for expansion for this population of children and women affected by IPV in Australia. This is especially so within the current family violence and mental health service system reform contexts at state and national levels. The model is also adaptable for families from conception through to children aged five who have experienced a wide range of family stresses and trauma and is in fact already being expanded to Aboriginal and Torres Strait Islander populations (Toone et al., 2021), perinatal child protection populations (Kong, 2021), broader populations within rural CAMHS (Raykar et al., 2021) and for use via telehealth in Australia (Fogarty et al., 2021). CPP can be delivered to children in their relationships with parents or caregivers who have used violence within relationships, with clear guidelines for assessing therapeutic readiness of families (Lieberman et al., 2015). CPP for IPV-exposed dyads is acceptable to clients and organisations, can be delivered in under six months, and will be increasingly available as more Australian therapists across non-government organisations; perinatal, child and adolescent mental health services; and private practitioners are trained in CPP and gain experience in skilled delivery. The CPP model of training and model of treatment delivery can equip services to better respond to young children and their caregiving relationships after violence and trauma, for the betterment of their lives and for future generations.
Implications and recommendations for policymakers
Implications
- Very young children’s mental health and wellbeing can be particularly impacted by IPV trauma, alongside those of their affected mothers.
- The mental health care needs of very young children are often overlooked in Australian service systems, as are the needs of IPV affected mother–child dyads.
- The way to restore young children’s mental health after IPV is within their safe relationships (as a first step this is often, but not always, with their mother).
- CPP is an evidence-based model for this population that is acceptable and increasingly feasible across settings within Australia.
- The CPP model of care also provides the theory, skills training and reflective supervision framework to build and sustain a mental health and wellbeing workforce for young children and parents/caregivers impacted by IPV trauma.
Recommendations
- Promote equity of mental health service delivery for children across the age range, to ensure responsive care is available for all children from earliest life.
- Invest in and expand the trauma- and violence-informed child mental health workforce that is growing in Australia, based on the CPP training and workforce development model.
- Develop a national trauma- and violence-informed child mental health and wellbeing practice framework, to guide safe engagement for children within all important caregiving relationships after IPV. This should be inclusive of both victim and survivor and perpetrator co-parents when safe, and across caregiver genders and sexualities.
Implications and guidance for practitioners and service providers
RECOVER has made considerable service impacts across project sites that can guide future care. RECOVER has:
- reinforced the value of tailoring services for IPV-exposed mothers and very young children previously missing out on care and/or identified service gaps for this age group
- highlighted the need to identify safe windows of therapeutic readiness for change with families
- identified that rural therapists/managers with less experience need more support to implement CPP
- operationalised trauma history assessment for children and caregivers referred to the service to better inform and tailor treatment plans for children and families
- facilitated the introduction of family violence screening at triage and realisation that family violence is prevalent among the clinical population
- facilitated partnerships between child mental health and family violence services
- highlighted the need for and value of building a
trauma- and violence-informed child mental health/therapeutic workforce - facilitated the training of further cohorts of CPP-qualified clinicians who are in turn now offering CPP across Victoria and South Australia (to Aboriginal and Torres Strait Islander families, migrant and refugee families, and some parents – mothers, fathers, caregivers – who have used violence in their relationships), as well as delivering CPP via telehealth
- developed a national community of practice, practice activities and knowledge translation.
Introduction
This report outlines the findings of the RECOVER project (“Reconnecting mothers and children after family violence: The child–parent psychotherapy pilot”). The study aimed to implement and evaluate the child–parent psychotherapy (CPP) model of care (Lieberman et al., 2015) for Australian women and children (<5 years) affected by intimate partner violence (IPV).
Intimate partner violence
IPV is defined as behaviour by a partner or ex-partner that includes physical, sexual and/or psychological abuse and controlling behaviours (World Health Organization [WHO], 2013a). Up to one in three women globally have experienced IPV in their lifetime (WHO, 2021), compared to one in six women in Australia (Australian Bureau of Statistics [ABS], 2017). One in 17 Australian men report experiencing IPV since the age of 15 years (ABS, 2017).
While people of all genders and sexualities can experience IPV, the focus of the RECOVER project is on IPV perpetrated by men in cisgender heterosexual couples and the harm it causes mothers and children – and in particular, fathers or other intimate partners/ex-partners as perpetrators of the violence, and victims and survivors as mothers (protective parent/caregiver) and children. All women can be at risk of IPV, and women from marginalised backgrounds can face heightened risk – for example, women with disability, First Nations women and women from migrant and refugee backgrounds (ABS, 2017). Partner violence is more prevalent among women of childbearing age (WHO, 2021), especially those with infants and young children; consequently, the violence impacts on both mothers and children simultaneously (WHO, 2013a).
Our study cohort replicates the population targeted in the original CPP trial (Lieberman, Van Horn et al., 2005). We note that future studies could expand to include diverse genders and sexualities, male victims and survivors, and parents and caregivers who are not the biological mother to reflect the expanding breadth of CPP practice (Iwaoka-Scott et al., 2015; Larrieu, 2018; Lieberman et al., 2019).
Effects on children
Children can be impacted by IPV in a range of ways depending on their age and stage of development. The impact and resilience of children depends on the severity and chronicity of IPV experienced, other adverse experiences in the home, and the availability and responsivity of caregivers (Fogarty, Giallo et al., 2019). Child abuse, including sexual abuse, is also associated with IPV (Bidarra et al., 2016; Holt et al., 2008).
Persistent fear and anxiety in children’s lives results in activation of prolonged stress responses, with detrimental structural and physiological changes in the developing brain (Cicchetti et al., 2011; National Scientific Council on the Developing Child, 2010). There is strong evidence outlining frequent externalising behavioural problems and post-traumatic stress, depression and anxiety in children due to IPV (Vu et al., 2016). Children’s mental and physical health is impacted by exposure to violence in the home (Orr et al., 2020), with up to 20 per cent of young children suffering from poor mental health (Australian Institute of Health and Welfare [AIHW], 2020; Lyons-Ruth et al., 2017; Westrupp et al., 2015). Consequently, children exposed to IPV may suffer a range of serious and ongoing socio-behavioural, physical, academic and mental health problems, including re-victimisation and perpetration of violence in their adulthood (Chan & Yeung, 2009; Felitti et al., 1998; Holt et al., 2008; Vu et al., 2016).
Infancy and early childhood are critically important developmental periods when children’s brains are particularly vulnerable to the harms of IPV. Recent Australian longitudinal evidence (in a sample of 615 mother–child dyads) shows that any IPV exposure from infancy to 10 years was associated with poorer child health outcomes (Gartland et al., 2021). Almost half of all children with mental health and language disorders had been exposed to IPV (Conway et al., 2020; Gartland et al., 2021).
Children living in separated families are often left to navigate complex relationships with other caregivers, including with fathers or other caregivers, on their own while they are still recovering from the impacts of IPV trauma (Morris et al., 2015). Children’s experiences of IPV and their relationships are often not discussed and the consequential harms to children often go unrecognised (Humphreys et al., 2011; Lamb et al., 2018; Morris et al., 2018).
Harms to women and the mother–child relationship
The maternal morbidity and mortality associated with IPV is well documented and understood. Harmful effects include significant mental health issues, physical illness and somatoform disorders, reproductive health problems, substance abuse disorders, chronic illness and disability (WHO, 2013a).
Becoming a parent is a stressful developmental phase (Lieberman, Ghosh Ippen et al., 2015) and can be made significantly harder in the context of IPV trauma. Women’s agency and confidence as a mother may be directly undermined by her partner through tactics of coercive control, impacting her experience of motherhood and the quality of mother–child relationships (Buchanan & Humphreys, 2021; Hooker, Samaraweera, et al., 2016; Katz, 2019).
The impacts of IPV on social isolation, including the mental health impacts of stress and trauma, may mean that mothers are understandably hampered in their capacity to sensitively and consistently respond to their children at times when their children are presenting with challenging behavioural symptoms of traumatic stress (Bancroft et al., 2012; Holt et al., 2008; Isobe et al., 2020). Along with the practical insults of IPV on mother–child relationships (Hooker, Samaraweera et al., 2016), mothers and children can also begin to misunderstand each other “as the child’s traumatic expectations interact with the (traumatic) expectations of the parents” (Lieberman et al., 2015, p. 21).
Family separations after IPV are also particularly fraught for women and children and often complicated by ongoing patterns of coercive control and physical dangers, including fatality risks to women and children (AIHW, 2019). Therefore, even when protective steps are taken by mothers, ongoing psychosocial stressors from men’s use of violence may continue to undermine mother–child relational recovery (Humphreys et al., 2018).
Treatment and support for women and children
Evidence reviews exploring treatment for victims and survivors of trauma and abuse (Barlow et al., 2015; Gillies et al., 2016; Howarth et al., 2016) have identified a lack of evidence-based interventions focused on IPV and the parent–child relationship. Quality parent–child or dyadic therapies favour interventions delivered to the (non-abusive) parent and child, rather than individual treatments (Graham-Bermann et al., 2007; Howarth et al., 2016).
One such intervention is CPP, an evidence-based intervention that was initially designed for pre-school-aged children and mothers affected by IPV. The intervention is adaptable across different populations, including a range of family constellations and culturally diverse populations, and across the entire 0- to 5-year-old age range (Lieberman et al., 2019; Shafiet al., 2019). CPP has been extensively evaluated across many randomised controlled trials (RCTs), with different traumatised parent–infant populations, including children with mothers experiencing domestic violence and depression, and children with a history of maltreatment/poor attachment (Ghosh Ippen et al., 2011; Lieberman, Van Horn et al., 2005; Lieberman et al., 2006; Lieberman et al., 2015). Findings show improvements in maternal and child trauma symptoms and mental health, child behaviour and the parent–child relationship (Hagan et al., 2017; Lieberman et al., 2015). Sustained benefits of CPP include decreased child behavioural problems and maternal distress to six months (Lieberman et al., 2006), and decreased parenting stress and attachment security to one year (Cicchetti et al., 2011; Stronach et al., 2013). In recent evidence from Guild et al. (2021), CPP participation of depressed mothers and infants enhanced maternal warmth and child problem behaviour six years post-intervention.
CPP is built on a psychodynamic model, the hallmark of which is the premise that learning and relational change can only occur within the context of safe relationships (e.g. the therapist–supervisor relationship, the therapist–mother relationship and the mother–child relationship). CPP is a flexible and non-didactic relational model of learning and treatment that is therefore inherently resource and time intensive. Questions on the accessibility and scalability of CPP have therefore been raised (Alto et al., 2021). Interestingly however, rates of attrition for CPP do not vary, irrespective of study population and/or socioeconomic status. This suggests intervention length is not a barrier to participation.
Alto et al. (2021) have reviewed the literature of other parenting and attachment interventions and have found that many studies do not provide attrition information, and those that do provide comparable attrition rates whether interventions are brief or longer term. There are mixed results about whether briefer dyadic or parenting intervention models can achieve comparable outcomes (Mountain et al., 2017; Shafi et al., 2019).
What is clear is that there is an urgent need for early intervention and secondary prevention programs for mothers and young children to arrest the detrimental consequences of IPV. Maternal functioning with a reduction in trauma symptoms is currently considered one of the best predictors of child outcomes (Graham-Bermann et al., 2011; McFarlane et al., 2014). In securely attached relationships, where the emotional and physical needs of children are consistently met, fewer child behavioural, language and school readiness problems are seen, compared with insecure mother–child attachments (Carpenter & Stacks, 2009; Guild et al., 2021). Children’s resilience to the negative impacts of IPV is enhanced when mothers’ health and wellbeing are supported (Fogarty, Giallo et al., 2019; Fogarty, Woolhouse et al., 2019). Interventions that jointly address maternal and child symptoms and their relationship with each other may have added benefit and arrest intergenerational trauma and abuse (Lieberman et al., 2015).
Study rationale
Interventions for women and children living with violence in Australia
Despite the clear evidence of harm, less than 1 per cent of all Australian children under five years receive formal mental health treatment (Segal et al., 2018). Australia’s mental health system does not have a focus on prevention and early intervention, with most people treated long after the onset of their symptoms (Productivity Commission, 2020). The mental health care needs of infants and young children are poorly identified, and the treatment that is offered frequently arises in crisis situations and/or is directed to older children and youths. Recent state and national inquiries and commissions have identified substantial service gaps or the “missing middle” (McGorry, 2021) between primary care (GP) and tertiary hospital/mental health bed-based services for all clients with mental health problems. This includes a lack of focus on the early years and young children needing more mental health support (Productivity Commission, 2020; State of Victoria, 2021). Consistent and comprehensive mental health services for those living in rural and regional areas are particularly lacking (Productivity Commission, 2020; State of Victoria, 2019, 2021). Rural areas also face the additional burden of fewer experienced mental health care professionals (Productivity Commission, 2020).
Modifiable risk factors for adult mental illness (like IPV) are prevalent and occur at the earliest stages of life (Guy et al., 2016; Orr et al., 2020). Challenges include the identification of young children as victims and survivors of IPV and subsequent mental health problems (Bunston et al., 2017), and service gaps and capacity in mental health systems. In addition, very few Australian individual, group or dyadic programs have been rigorously evaluated, identifying the benefits of interventions for abused women and children (Campo, 2015; Hooker et al., 2019). Suboptimal mental health care has been reported by women seeking mental health care after IPV (Marsden et al., 2020). Australian services that deliver IPV support for non-abusive parent and child populations, such as community-based individual counselling, group work and parenting programs, are often siloed, subject to the uncertainty of poor organisational clinical governance and government funding cycles, and not evidence-based (Campo, 2015; Hooker, Kaspiew & Taft, 2016).
Therefore, the RECOVER project outlined in this report sought to pilot an established trauma- and violence-informed relational intervention with strong evidence, the CPP model of care, across rural and urban settings. Although contemporary CPP can be provided across the 0- to 5-year-old age range, to a wide range of family contexts and caregiver genders and sexualities, to address a range of traumatic experiences, the focus of this project was to test the acceptability and feasibility of CPP for pre-school-aged children and mothers affected by IPV in an Australian context, drawing on the original CPP trial (Lieberman, Van Horn et al., 2005).
Research questions
The RECOVER project addressed the following research questions on the feasibility of CPP for a population of women and children affected by IPV.
1. How acceptable and feasible is CPP to the Australian context?
- How acceptable is the intervention for women and service providers?
- What are the barriers and facilitators to the implementation of the CPP model into services?
- What (if any) are the dyad recruitment and retention issues encountered?
- Are there process and impact differences between service providers across sites?
2. Do CPP therapists-in-training adhere to CPP model fidelity?
3. How effective is treatment delivered by CPP therapists-in-training during the study?
- Do women’s and children’s trauma symptoms differ before and after treatment?
- Does treatment improve the mother–child relationship?
Intervention description
Child–parent psychotherapy
CPP is an intervention for parents and young children who have experienced some form of trauma. Integrating theories of psychoanalysis, attachment theory and developmental psychology, CPP was developed to support children and their mothers affected by family violence. In addition to considering psychodynamic and relational processes, it privileges safety and the socioeconomic and cultural context of the family. Delivered in hour-long weekly sessions by specially trained therapists, treatment time can extend to 12 months, depending on family need (Lieberman et al., 2015; Lieberman et al., 2019). A CPP intervention comprises three phases:
- foundation phase: assessment and engagement sessions (4 to 6 weeks)
- core intervention phase (length varies depending on the need; approx. 20 to 32 weeks)
- recapitulation and termination phase: promoting sustainability (<8 weeks; Lieberman et al., 2015).
Family strengths and context, trauma type and developmental impact, and the child’s age all inform the structure and length of the CPP sessions. Therapy for infants includes actively engaging them in sessions and reflecting together with mothers to understand their infants’ expressions of distress and attempts to connect. Play-based therapy facilitates communication for toddlers and pre-school-aged children with their mothers using a range of objects, toys, and stories. Child-friendly spaces are provided alongside adult-friendly collateral or parent sessions for mothers (Lieberman, 2004; Lieberman, Chu et al., 2011; Lieberman et al., 2015; Lieberman, et al., 2020).
How child–parent psychotherapy works
CPP targets the mother–child relationship as the central change agent to restore the child’s health and development (Chu et al., 2021; Lieberman et al., 2015). Relationships may be seen as a “web of jointly constructed meanings” based on each participant’s perceptions of and actions toward one another (Lieberman, 2004; Lieberman et al. 2015). When mothers and children are exposed to IPV and overwhelmed by frightening experiences, their relationship suffers (Jones & Bunston, 2012; Levendosky et al., 2012). They can misunderstand each other’s intentions and actions and find it much more difficult to connect in a safe and rewarding way (Lieberman et al. 2015; Overbeek et al., 2019). The focus of CPP is therefore to change these misunderstandings so that relationship repair can occur, and mothers and children can return to safe and more rewarding patterns of relating (Bernstein et al., 2019; Lieberman et. al., 2015).
Therapists take time to get to know mothers and children, including their family’s strengths and cultural values. During this “foundation phase”, the therapist will map the history, nature and effects of violence and trauma on the child, mother and their relationship (Lieberman et. al., 2015, p. 55). In so doing, the mother and child will get an initial sense of how the therapist will work and decide whether they feel comfortable in proceeding. Treatment goals and plans are co-created using the CPP “Triangle of Explanations” (Figure 1), which links past trauma experiences. The triangle is developed with the mother and then, with her permission, communicated in an age-appropriate manner to the child directly.
Figure 1: The CPP Triangle of Explanations
An example of a triangle of explanation communicated to the child might be:
You saw mummy and daddy fighting. Daddy hurt mummy, and then he was gone [trauma/experience]. Since then you can’t sleep at night and don’t want to leave mummy’s side [behaviour]. You’ve been missing daddy while he is getting help with his angry feelings. And worried that you and your mummy will be safe and okay. Mummy and I will meet with you each week to talk and play to help you with big feelings so you can feel better inside [treatment plan].
Explaining the triangle to children in the above way ushers in the beginning of the core phase of CPP. Toddlers and pre-school-aged children often are able to add to the triangle or ask questions about events that have been troubling them, once they see that the space is for them. Children see their mother and their therapist as examples of adults working safely together, and even though frightening feelings may come up, no one gets hurt. Moments like this are often transformative for mothers too, as they may come to see the child’s behaviour as an attempt to communicate when words are not possible (Fraiberg et al., 1975; Lieberman & Van Horn, 2011; Lieberman et al., 2015; Lieberman et al., 2019).
Collateral sessions with the parent alone consider the impact that IPV (e.g. earlier maternal childhood traumas or “ghosts in the nursery”; Fraiberg et al., 1975) may have on the mother’s ability to parent (Lieberman, Padron et al., 2005). For example, a mother may find herself becoming frightened of her toddler’s loud tantrums and unable to set a limit. This may be an understandable response if she, for instance, has had an experience of being hurt by someone in the context of raised voices. The mother’s trauma response would be normalised and psychoeducation about normal toddler development provided. Exacerbating external stressors from IPV, like housing, poverty or court demands, would be considered. The therapist and mother may develop body-based emotional regulation strategies to calm her own trauma response (e.g. breathing exercises), and workshop alternative ways of engaging with her toddler’s feelings expressed through tantrums. Risk and safety are continuously monitored throughout treatment, and referral and advocacy provided as needed (Lieberman & Van Horn, 2011; Lieberman et al., 2015; Narayan et al., 2020). A core aspect of this phase of treatment is also to honour the child’s relationship with the frightening/absent caregiver (for example, in this population, their dad), understanding that children develop their sense of themselves based upon their relationship with all parents or caregivers present or absent in their lives. CPP also has protocols for inclusion of caregivers who use violence into parallel collateral or dyadic treatment where safe (Groves et al., 2015; Lieberman et al., 2015).
During this process of dyadic and collateral work, children and mothers become more active in shaping the therapeutic narrative. As the mother–child relationship is repaired, the triangle is changed over time. The trauma story begins to recede and more benevolent and hopeful experiences or “angels in the nursery” moments are built (Lieberman, Padron et al., 2005). The therapist’s role becomes less active, and eventually redundant. The mother and child and their recovery journey are honoured and the journey is concluded in the termination phase (Lieberman et al., 2015; Lieberman et al., 2020).
While there is a large body of evidence on the effectiveness of CPP, qualitative evidence is lacking to support improved implementation and gain clarity on participant experiences (especially children’s). The complex change mechanisms that occur due to CPP continue to be explored. The attachment relationship is, however, considered to be the main driver of change.
The program logic model (Figure 2) outlines the problem statement, consequences of the IPV on victims and survivors and associated factors, the relational CPP intervention and the theory of change proposed in the dyad.
Figure 2: CPP Program Logic Modela
aAdapted from the United Kingdom’s Domestic Abuse, Recovering Together (DART) program (Smith, 2016)
Child–parent psychotherapy training in Australia
CPP training in Australia is open to allied health and medical clinicians with experience in infant–parent mental health and currently employed within a clinical setting. The CPP training is conducted by an endorsed international CPP trainer from the United States. Training in CPP is currently delivered via a “learning collaborative model” (Ebert et al., 2012), an 18-month training model that centres on providing reflective case presentations with an international trainer and the establishment of local peer/supervision group presentations for learning (Lieberman et al., 2019). Specifically, the training comprises:
- seven days of core didactics and case-based competency building
- eighteen months of case-based consultation calls
- case-based participation in smaller local reflective supervision groups
It is expected that the smaller case-based reflective supervision groups will continue post-training as structures to sustain quality CPP delivery (or trauma- and violence-informed mental health/wellbeing care).
To date, two CPP Learning Collaborative (LC) models have been completed in Australia. The first LC was convened by the South Australian branch of the Australian Association for Infant Mental Health (AAIMH) in 2016–17, and the second was convened by Berry Street Victoria in 2017–19 in partnership with the RECOVER research project. A third LC commenced in 2020 and has been run completely online, with participants also learning to deliver CPP remotely. This current training is due to conclude in mid-2022. A fourth LC is due to commence in 2022. Training is funded in a range of ways:
- non-government organisations providing mental health and wellbeing care in the community with (now) ongoing funding to provide CPP to women and children affected by IPV
- public child and adolescent mental health services, or hospital-based therapeutic child protection services with professional development budgets for their staff or within their award structures
- individual private practitioners who self-fund training as part of their commitment to their professional development.
The child–parent psychotherapy workforce in Australia
The CPP workforce resembles the broader infant and child mental health and wellbeing workforce in Australia, consisting of clinicians across social work, occupational therapy, speech pathology, maternal and child health nursing, child psychotherapy, family therapy, psychology, perinatal and child psychiatry and paediatrics. Clinicians work in non-government organisations, child and adolescent mental health services, hospitals, child protection, private practice and local government settings. Two thirds of clinicians are situated in metropolitan areas. Most clinicians are situated within (or provide consultancy to) services that work with children who have experienced multiple adverse childhood and family experiences (including but not limited to family violence) and across statutory and non-statutory systems. To date, CPP in Australia has been delivered by this workforce to children and adoptive, foster-care, kith and kin care and biological parents. This includes CPP work with parents who are victims and survivors or perpetrators of sexual and family violence, including pregnant parents and or/where there is a risk of child removal.
Report structure
This report is divided into three main sections: Part 1: A systematic state of knowledge review; Part 2: Research process and methods; and Part 3: Research findings, including discussion and implications for policy and practice.
Part 1 outlines the current state of knowledge on family violence, the impact on children and suitable interventions for families to heal from abuse.
Part 2 provides insight into the research aims, methods, CPP training and therapeutic service sites. While maternal and child health and wellbeing outcomes were measured throughout the project, the feasibility of CPP implementation in the Australian context was the focus, rather than program efficacy. Eleven clinical partners were involved in the delivery of CPP. A thriving CPP community of practice was established.
Part 3 of the report focuses on the acceptability and feasibility of implementing CPP, barriers and enablers to implementation and the impacts the intervention has had on existing services. Practice implications and future research are also outlined. Findings provide policy and practice guidance on future therapeutic intervention work with families with young children exposed to family violence.
Part 1:
State of knowledge review
Context of this review
Our previous ANROWS Landscapes state of knowledge review explored literature on parenting in the context of domestic and family violence (Hooker, Kaspiew & Taft, 2016). In addition to identifying the prevalence, impacts and dynamics of abuse in families, it reviewed clinical trial-level evidence and other promising research on interventions to strengthen and support a positive and healthy mother–child relationship, post-IPV. Since publication, these results have informed future testing of interventions to support the recovery of abused women and children (Hooker et al., 2019).
The 2016 review identified a range of programs suitable for victim and survivor mothers and children to repair relationships and improve wellbeing. Intensive home visiting trials proved inconclusive with findings showing more targeted, IPV-specific therapy is needed for families. Other empowerment (Maternal Empowerment Program; Graham-Bermann et al., 2007), advocacy (Jouriles et al., 2009), psychoeducational (Circle of Security; Hoffman et al., 2006), psychotherapeutic (CPP; Lieberman, Van Horn et al., 2005) and trauma-focused cognitive behavioural therapy interventions (Cohen et al., 2011) were identified. Some relevant, non-trial interventions showed promise, yet lacked robust, ongoing evaluation due to a lack of funding (Bunston, 2008; Bunston, Pavlidis & Cartwright, 2016).
Psychotherapeutic interventions based on trauma that combined therapy for mothers and children together showed the most benefit. We subsequently recommended further development of effective interventions (like CPP) for mother–child victims and survivors of IPV, including measures of the parent–child relationship, in more pragmatic settings with representative samples, to fully understand what works to help women and children recover from IPV.
Existing review evidence
This RECOVER state of knowledge review builds on our previous evidence review outlined above (Hooker, Kaspiew & Taft, 2016). Prior to starting this study, we broadly explored recent (since 2016) literature or systematic reviews on interventions for families experiencing IPV.
Findings include separate reviews of evidence on children exposed to violence, pregnant women and mothers experiencing IPV, and interventions for fathers using violence.
A systematic review by Marie-Mitchell & Kostolansky (2019) on children’s outcomes associated with adverse childhood experiences identified that multicomponent/disciplinary-delivered interventions addressing parenting, mental health and social support for parents can reduce the impact of adverse childhood experiences and improve the parent–child relationship for pre-school-aged children (Marie-Mitchell & Kostolansky, 2019). Treating maternal mental health reduces mental health symptoms and behavioural problems in children (Marie-Mitchell & Kostolansky, 2019; Weissman et al., 2006) and is a strong argument for treating both mothers and children together in the aftermath of IPV.
Study heterogeneity and poor study quality limit review findings, although as described in earlier studies, Latzman et al. (2019) found programs targeting the non-offending parent had the largest effect. Programs with separate individual treatments for children and mothers were the least effective. Interventions based at home had a greater effect than clinic-based services (Latzman et al., 2019). Intensive home visiting interventions may decrease child behaviour problems in children exposed to IPV but overall, it remains unclear what IPV psychosocial interventions (and in what circumstances) are best for the promotion of child health and wellbeing (Latzman et al., 2019).
Austin et al.’s (2019) systematic review of interventions for women as parents in the context of IPV found it impossible to determine what interventions were most effective in addressing mothers’ needs. Study limitations found Austin et al. drawing similar inconclusive findings to Latzman et al. (2019). Earlier, Howell and colleagues looked at the unique needs of pregnant women exposed to partner violence (Howell et al., 2017). Despite the well-known negative effects associated with violence during pregnancy, very few interventions exist and those that do are limited to crisis-level interventions. Developmentally specific, strength- and theory-based interventions (like perinatal CPP) for pregnant women (and the foetus and newborn) exposed to IPV are urgently needed.
Interventions for fathers who use violence focused on increasing men’s accountability and empathy while decreasing violence, fostering positive fathering, and the father–child relationship (Labarre et al., 2016; Toone, 2018). Aims included promoting healthy interactions between father and child, and father and the child’s mother, including supporting the mother’s parenting. Program effectiveness was unclear due to a lack of quality program evaluation. Concerns were identified with fathers’ co-parenting and the potential for causing further harm to children and mothers when comprehensive safety and ongoing risk assessment is lacking (Labarre et al., 2016; Toone, 2018). However, going beyond dyadic mother–child interventions to also include fathers in children’s relational repair after violence can potentially improve father–child relationships and children’s sense of safety and wellbeing. More workforce training/skill development and organisational support for clinicians is needed to provide safe experiences and improved outcomes for victims and survivors (Toone, 2018).
Most similar to our current state of knowledge review, Anderson & van Ee (2018) revised treatment interventions for mothers and children (up to 18 years) exposed to IPV and attempted to document the theory of change. From 17 studies, multilevel, combination sessions (joint and separate) for mothers and their children seem most effective compared to individual- or joint-only programs. Benefits were gained from enhancing dyadic interactions. Authors have called for future research to test and replicate research identified in the review (including using the same outcome measures), in order to strengthen and consolidate the evidence (Anderson & van Ee, 2018; Howarth et al., 2015; Howarth et al., 2016).
Other reviews of research on program evaluations and interventions for families experiencing IPV do exist and have been described above; however, unique in comparison to other reviews, we searched the most recent (2015 to 2021) evidence on mothers and/or fathers and focused on pre-school-aged children.
Method
The purpose of this RECOVER state of knowledge review was to explore the nature and extent of global interventions (for parents and pre-school-aged children) to restore the parent–child relationship after IPV. We adopted a systematic, narrative literature review process to identify key themes across the evidence base.
Search strategy
In view of the previous systematic reviews completed on this topic, bibliographic databases were searched for peer-reviewed literature from the time of our previous ANROWS state of knowledge literature review (April 2015) to August 2019, with an updated search completed in May 2021. Databases include Medline (1946 onwards), CINAHL, SocIndex, Informit (Health & Family), PsycINFO and ProQuest. Using a modified PICO/PEO structure and Boolean AND/OR operators, the four main concepts explored were:
- population – child/parent
- intervention – treatment intervention/support
- exposure – intimate partner violence
- outcome – parent–child relationship.
Keywords and Medline search strategy are outlined in Appendices A and B.
To capture unpublished work including practice experiences, we explored the international and national grey literature/websites (see Appendix C) including Google Scholar. In addition, we hand-searched all references and citations (“snowballing”) of identified studies and reviews.
Eligibility criteria
The above search applied the following eligibility criteria to identified titles, abstracts and full-text articles.
Inclusions
- English language studies only from April 2015 to May 2021
- interventions with an IPV focus
- evaluation studies of a therapeutic intervention
- intervention at minimum addresses IPV, but may also address multiple risk factors/traumas
- population includes at least one of either pregnant women, mothers, fathers or both parents, and children aged from birth to 5 years
- interventions: either group, dyadic or individual therapy to support the parent–child relationship
- quantitative and qualitative evaluations of any design
Exclusions
- systematic reviews
- not evaluation of a therapeutic intervention
- not empirical study (e.g. commentaries, opinion pieces)
- studies without a parenting focus or parent–child outcome measure
- studies with the majority of children >5 years.
Data analysis
Based on the above eligibility criteria, all titles and abstracts were reviewed by two authors using Covidence software (Veritas Health Innovation) and inter-rater reliability was monitored using a predetermined article review template. If all inclusion criteria were met, articles were retrieved for full-text review, with items marked as unsure also included for full-text review.
Final full-text items were charted, and relevant data were extracted from each study (see Appendix F). Abstraction included study authors and year of publication, country of origin, setting, study design, data collection methods, sample details (participants and size), type of intervention and delivery method, comparison group details, outcomes assessed and evidence of effectiveness. Identified studies were synthesised and reported according to the delivery method and research design/hierarchy of evidence. The quality of the quantitative evidence was ordered as follows: randomised/quasi-randomised controlled trials (classed as high-quality evidence); non-randomised studies with a comparison group; non-randomised without comparison (pre–post observation studies); and finally, low-level quality for studies using single case study/series designs (classed as low-quality).
Results
Search results
We identified 34 articles, representing 29 separate interventions (see Appendices E and F) from April 2015 until May 2021. The search identified 2,027 records for assessment, with 22 additional records from grey literature and reference lists or citations of included studies. We excluded 1,655 from the title and abstract review, with 215 full texts potentially relevant for inclusion. After further application of eligibility criteria, we excluded 181 records (see PRISMA diagram in Appendix D for exclusion reasons) to reach our final 34 articles.
Articles included 10 RCTs and two ongoing trials (protocols only; 35%), two non-RCTs and 13 pre–post observational studies (44%) without a comparison group. Two papers reported on multiple pilot evaluations of the Attachment and Child Health (ATTACH) intervention, using a mix of RCT and non-RCT designs. The remaining involved qualitative research and case study evaluations (15%). More than two thirds of studies (68%) were published between 2015 and 2017, with only two papers identified since 2020.
Research was reported from eight countries with no quality trial-level evidence based in Australia. Australian evidence was restricted to two pre–post studies (Bunston, Eyre et al., 2016; Southwell, 2016) and one qualitative evaluation (Broady et al., 2017). Across all records identified, most articles (n=17) were from the United States (50%), and four (12%) each from Sweden and Canada. The United Kingdom and Australia published three each. Single studies were reported from Israel, India and the Netherlands. Urban settings dominated the research with no rural-only research identified. Four of the final 34 studies were conducted in both rural and urban settings (Broady et al., 2017; Domoney et al., 2019; Roopnarine & Dede Yildirim, 2018; Southwell, 2016), yet many settings were poorly described.
Significant heterogeneity in intervention type, comparison group used, target audience, delivery method and setting were noted across identified studies, making synthesis, comparisons and conclusions on best methods challenging. Group interventions made up most of the studies (53%), followed by dyadic/triadic interventions (23%), combination approaches (15%), and individual-only programs (9%; see Appendix G for various therapy descriptions). Some studies, for example, reported on group plus individual sessions with parents (Morales et al., 2015), while others used group plus dyadic interaction sessions with parents and children (Visser et al., 2015).
In this review we report studies according to intervention type (group, dyadic, individual or combined) and by study design to highlight the level and quality of the evidence.
1. Group treatment programs
Randomised/non-randomised controlled studies
RCTs offer the strongest design for measuring effectiveness and identifying the best methods of supporting women and children healing from IPV.
Of the 12 RCTs (including two RCT protocols and two studies without randomisation but including a control group), seven described group-based therapy (Feinberg et al., 2016; Graham-Bermann et al., 2015; Howell et al., 2015; Roopnarine & Dede Yildirim, 2018; Satyanarayana et al., 2016; Scott, 2017; Steele et al., 2019).
Interventions with the protective parent (mother) and child programs were most common and included maternal empowerment programs (MEP) with a parallel intervention for pre-school-aged children (Pre Kids’ Club; Graham-Bermann et al., 2015) and a group attachment-based intervention (Steele et al., 2019). In the Graham-Bermann et al. (2015) study, which included separate psychotherapeutic and educational group treatment for mothers and children, compared to a waitlist control group, female children in the treatment group showed improvements in internalising symptoms (depression/anxiety). Further analysis of these data and case notes indicated that 68 per cent of children developed re-experiencing symptoms during treatment, which spiked around the third session, resulting in recommendations to provide a minimum of 6 to 10 sessions for children to overcome these symptoms and prevent ongoing harm (Miller-Graff et al., 2016).
Howell et al. (2015) evaluated MEP only, a psychoeducational/advocacy intervention that aims to improve maternal mental health, parenting and self-efficacy. Significant improvements were seen in parenting behaviours compared to waitlist controls, with a reduction in corporal punishment immediately post-intervention and at six months follow-up (Grogan-Kaylor et al., 2019).
Scott’s (2017) protocol describes a trial underway evaluating two group-based parenting interventions: Mothers in Mind (MIM) and Caring Dads. MIM is a program for mothers and children that focuses on increasing maternal awareness of the impact of the IPV on the child and themselves, to positively influence parenting skills and competence. Caring Dads aims to prevent reoccurring IPV exposure for children by working with fathers (Scott, 2017). Program emphasis is on ending violence towards the child’s mother and improving child-centred fathering.
The other father-only group intervention was an integrated cognitive behavioural therapy (CBT) program for 177 IPV perpetrators with a dependence on alcohol (Satyanarayana et al., 2016). Satyanarayana et al. (2016) also found significantly less IPV perpetration among fathers attending the CBT treatment than controls. Spouses (mothers) also reported fewer mental health problems, however, no changes were seen in child behaviour or fathers’ alcohol consumption from baseline to three months follow-up.
Two studies described couple (mother and father) prevention interventions (Feinberg et al., 2016; Roopnarine & Dede Yildirim, 2018). Roopnarine and Dede Yildirim (2018) reported on 3,045 fathers from the Building Stronger Families psychoeducational intervention for vulnerable families, showing positive changes in paternal depression and IPV at 15 months post-intervention. Father–child relationships and child behaviour also improved, however self-report measures – especially fathers’ reporting on self and functioning – is a serious study limitation. Data from female participants were not reported in this article.
The Family Foundations psychoeducational program evaluated by Feinberg et al. (2016) is a transition to parenthood prevention intervention held pre- and postnatally over nine sessions (n=399). Outcomes focus on couple relationships, parenting quality, IPV and infant behaviour. After 10 months postpartum, better post-test levels compared with control couples were seen on more than two thirds of measures of co-parenting/parenting, parent mental health, child adjustment and partner violence. Effects on IPV were the largest, with strong trends in many other secondary outcomes. The large sample size and positive findings that reflect those of a previous pilot are study strengths, however, the mature and well-educated sample limits generalisations to all at-risk couples.
Pre–post observational studies (no controls)
Group therapy was again the most frequently reported type of intervention delivery in the observational studies identified. Six programs are described (Berry et al., 2019; Bunston, Eyre et al., 2016; McConnell et al., 2017; Pernebo et al., 2018, 2019; Rizo et al., 2018).
From Australia, Bunston, Eyre et al. (2016) reported on 30 dyads engaged in the Peek-a-Boo Club, a relational repair/psychotherapeutic intervention for infants and mothers impacted by partner violence. Improvements were seen in infant–maternal attachment and functioning, however clinical significance was uncertain, and authors suggest more comprehensive evaluation methods when testing the program in future.
Maternal mental health outcomes were the focus of Rizo et al.’s (2018) psychoeducational empowerment pilot study (MOVE: Mothers Overcoming Violence through Education and Empowerment). Mothers exposed to IPV reported significant improvements in depression and post-traumatic stress symptoms at both three- and six-month post-intervention time points.
The evaluation of the Family Vision coaching program (Berry et al., 2019) for 19 single mothers indicates that this type of group-based program for mothers is acceptable and feasible to implement in community settings, although statistical differences in pre–post outcomes on child–parent relationship measures and other parenting measures were not reported (Berry et al., 2019).
Caring Dads Safer Families (based on the Canadian Caring Dads model) was evaluated using a predominantly pre–post design. Using the fathering role to motivate men to examine and change their behaviour, Caring Dads explores men’s anger, family cohesion, co-parenting, domestic violence, perceptions of the child as a problem, use of corporal punishment, positive and involved parent–child relationship, self-centeredness and substance use. After two-hour weekly group sessions for 17 weeks, significant improvements in (father-reported) parental distress, parent–child dysfunction and parenting stress were shown. Partners’ and children’s reports enhanced the reliability of results which show promising evidence that the program can reduce risks to children and families (McConnell et al., 2017).
Pernebo et al. (2018) tested two group interventions and assessed outcome scores pre-intervention, post-intervention, six months later and 12 months later. Community-based psychoeducation and trauma-focused psychotherapy interventions both substantially reduced maternal trauma symptoms, although children benefited more from psychotherapy than the psychoeducation program. These treatment gains were sustained to 12 months with no increase in symptoms of IPV reported (Pernebo et al., 2019). Ongoing poor maternal mental health appears to hinder child recovery and children with high levels of trauma benefit most.
Qualitative research and other designs
Of all included studies, only one article focused solely on children. Pernebo and Almqvist’s (2016) qualitative paper explored nine pre-school-aged children’s experiences participating in a group psychotherapeutic intervention. Overwhelmingly positive responses ensued with themes around joy, security, relatedness, talking and competence. All children reported wishing to attend the group and no harmful effects were identified. Authors reinforce that young children (4 to 6 years) can contribute to research with valuable viewpoints that augment existing knowledge on interventions for women and children exposed to IPV (Pernebo & Almqvist, 2016).
Fathers reported on their experiences of the 18-week Taking Responsibility group (behaviour change) program, with a specific focus on fathers’ parenting and relationships with children (Broady et al., 2017). Twenty-one fathers reported that love for their children was a motivator to stop using violence, however, several group members considered themselves good fathers and failed to acknowledge that children were affected by the violence used. Despite this, children’s wellbeing and fathering may work as key leverage points for future interventions with men and children (Lamb et al., 2018).
The Parenting and Violence psychoeducational parenting program from Sweden (Kamal et al., 2017) aimed to improve parental awareness of children’s involvement in violence and minimise effects on child development and ongoing intergenerational trauma. Group therapy is offered separately for parents who are victims and survivors or perpetrators of IPV. Qualitative findings indicated that participants developed improved self-control, self-esteem and communication skills which had positive self-perceived effects on child wellbeing and behaviour.
2. Dyadic or joint treatment programs
Randomised/non-randomised controlled studies
Two dyadic studies used non-randomised controlled designs (Schechter et al., 2015; Waldman-Levi & Weintraub, 2015). The Family Intervention for Improving Occupational Performance program from Israel (Waldman-Levi & Weintraub, 2015) involved a dyadic crisis-based intervention for mothers and children, with an emphasis on dyadic interaction and play functioning. In the intervention arm, some significant differences were seen in mother–child interactions and play skills, but not playfulness. Video feedback with traumatised mothers and children (one to four years) in the Clinician Assisted Video Feedback Exposure Sessions (CAVES; Schechter et al., 2015) showed reduced parental negativity indicators towards their children, but not themselves, compared with non-traumatised mothers.
Letourneau et al. (2020) and Anis et al. (2020) report on the mixed pilot evaluation of the ATTACH program. The authors used both randomised controlled and non-randomised controlled designs to test the intervention with mothers and young children under 36 months of age. Although mostly dyadic, three of the 10 to 12 sessions offered included a triadic approach with a co-parent (father, relative, friend or other). Aside from Feinberg et al.’s (2016) Family Foundations study, these were the only two papers to report interventions that may have included the non-abusive (mostly mother) and abusive parent (father). Arguments for co-parent inclusion were to buffer maternal stress, offer social support and nurture attachment security. No mention of risk assessment or management of participant safety/ongoing IPV during therapy was explored in the papers. This information is needed if future interventions are to safely involve fathers who continue to parent children post-separation. The ATTACH evaluation showed significant improvements in overall reflective functioning and positive trends in enhanced parent–child attachment.
Pre–post observational studies (no controls)
We identified four dyadic studies using pre–post designs to test the effectiveness of two main interventions: CPP (Hagan et al., 2017; Lavi et al., 2015; Waters et al., 2015) and parent–child interaction therapy (PCIT; Herschell et al., 2017).
CPP has been evaluated extensively in the past using RCTs (Lieberman & Van Horn, 2005). In the above studies, further adaption/testing of CPP is reported against different samples and maternal outcomes. A pilot study of weekly perinatal CPP delivered to 64 pregnant women in the third trimester until infants were six months old (Lavi et al., 2015) found reduced depression and trauma symptoms from pre- to post-assessment. Women with lower feelings of attachment to the foetus demonstrated the greatest improvements in child-rearing attitudes and mental health (Lavi et al., 2015). Similar findings were reported by Waters et al. (2015) with Latina, low-income, pregnant women (n=52), indicating that the addition of a perinatal component to CPP may be a very useful intervention to consider in maternity service settings for pregnant women experiencing IPV – especially as very few interventions exist for pregnant women experiencing partner violence (Howell et al., 2017). However, further research using perinatal CPP is required with larger randomised and representative samples using comparison groups to show real effect.
Conflicting with other findings, Hagan et al. (2017) found trauma symptoms improved more in female children, in dyads (n=199) with fewer lifetime stressors, and among those who received fewer CPP sessions. These findings are inconsistent with previous research which has found no gender differences in effects (Hagan et al., 2017), and in other studies included in this review which reported improved benefits (mental health, trauma and behaviour symptoms) for those at greatest risk (Lavi et al., 2015; Pernebo et al., 2019). These conflicts reinforce the need for replication of studies and more research on the feasibility and efficacy of CPP.
Challenges were identified in the implementation of PCIT in a shelter population evaluated by Herschell et al. (2017), with high attrition (57%) and only nine of the 21 participant dyads completing treatment. Positive effects on child behaviour were seen but there were no improvements on parenting practices.
Qualitative research and other designs
In a case series study by Keeshin et al. (2015) with shelter participants (n=8), combination PCIT with individual parent training and dyadic sessions were acceptable to mothers and children (2 to 5 years). PCIT improved women’s parenting capacity including more positive communication and praise of children (Keeshin et al., 2015). However, shelter settings may not be suitable sites for intensive therapy due to women’s and children’s ongoing stressors at this time (e.g. leaving the shelter, relocating, changing schools; Herschell et al., 2017).
3. Individual treatment programs
Randomised/non-randomised controlled studies
Intensive nurse home visiting (HV) programs have shown promise in reducing child abuse and parenting behaviours but there have been inconsistent findings on their benefits for reducing IPV and its impact on mothers and children. In the United States, Jack et al. (2019) enrolled 492 socially disadvantaged pregnant women in a 2.5-year HV program that included an augmented IPV component comprising further assessment, tailored care and social supports. Although women’s quality of life improved in both control (usual HV care) and intervention groups at 24 months post-delivery, no differences across arms were seen. Caution is needed in interpreting these results as although this was a rigorously evaluated trial, fidelity to the augmented HV intervention was challenging and these results may reflect poor implementation, rather than poor intervention effect (Hooker & Taft, 2019).
Pre–post observational studies (no controls)
In a less rigorous design, HV was again evaluated in the United Kingdom by Domoney who tested For Baby’s Sake, a trauma-informed parenting program aimed at breaking the cycle of IPV and improving child outcomes. The intervention is offered to vulnerable families from pregnancy until children are two years old. Conclusive data are yet to be published; however, early findings indicate parents value the approach. More HV research to address IPV and improve the health and wellbeing of affected mothers, fathers and children is needed.
In response to unmet demand, an Australian community service organisation developed the yourtown Expressive Therapies Intervention (YETI) program in Queensland for disadvantaged families (Southwell, 2016). Set in refuge and family support services, YETI provides individual treatment for infants and young children that draws on theoretical frameworks including expressive, child-centred play and parent–child relationship therapy. Evaluation data over two years showed 85 children under 5 years attending, with 41 parents providing outcome data on child behaviour and mental health. Significant and promising results showed improvements in child behaviour and mental health, including child social functioning, self-confidence and the parent–child relationship. Although dropout rates were high, this is not unusual in vulnerable populations (Herschell et al., 2017) and this program can be delivered by non-specialist staff who receive regular clinical and operational supervision (Southwell, 2016).
Qualitative research and other designs
No qualitative/other papers were identified that reported individual treatments.
4. Combination treatment programs
Randomised/non-randomised controlled studies
Visser and colleagues (2015) from the Netherlands describe the HORIZON trial currently underway that includes preparatory group work with parents only, parallel groups for parents and children, and dyadic parent–child sessions based on trauma-focused CBT.
Fathers for Change (Stover, 2015) uses the fathering role as a motivator for change and integrates methods to reduce paternal substance abuse. Individual sessions and dyadic treatment with partners and children are offered over four months. Compared with controls (offered group drug counselling), the Fathers for Change participants completed more treatment sessions, described greater program satisfaction and were less intrusive in father–child interactions during free-play sessions. In addition, a trend in the reduction of IPV was seen in these fathers.
Pre–post observational studies (no controls)
Fathers for Change was also evaluated in 2017 in a feasibility study testing program implementation in a residential substance use disorder treatment setting (Stover et al., 2017). Participants generally engaged and were satisfied with the program, with a reduction in anger and emotional regulation problems. Fathers for Change is a feasible treatment for fathers using violence and substances within residential drug treatment facilities. Results of these preliminary studies show promise in the context of fathers’ co-parenting; however, authors acknowledge further evaluation of Fathers for Change and other parenting programs is warranted in this setting (Stover et al., 2017). Larger samples and testing the intervention in non-drug affected, mandated populations may also be beneficial.
Qualitative research and other designs
Morales et al. (2015) used a single case study design to describe the impact and cultural adaptability of SafeCare for Latina families (parent–infant interaction module), an HV program that aims to reduce child maltreatment and the impacts of IPV on parent–child interactions. A range of parenting and maternal health and wellbeing factors improved at one and three months post-treatment, with high levels of participant satisfaction. Assessing the suitability of programs across cultures is essential for program success, with further research needed to confirm that SafeCare is appropriate for Latina families (Morales et al., 2015).
Discussion
To inform the development of Australian programs and services and improve outcomes for women and children experiencing IPV, we conducted a comprehensive state of knowledge literature review of IPV interventions addressing the parent–child relationship for families exposed to IPV. This review builds on previous ANROWS research we have completed on parenting and domestic and family violence, including a 2016 scoping literature review exploring the nature of healing interventions for victim and survivor mothers and children (Hooker, Kaspiew & Taft, 2016).
Review limitations
Our review was restricted to English-only studies from April 2015 to May 2021. While every attempt was made to identify all published and unpublished work on interventions to heal the parent–child relationship among those experiencing IPV, the significant increase in research on this topic means we may have missed some of the evidence. In addition, this is a narrative review that has not included the rigour of other types of more systematic literature reviews, including a detailed analysis of the quality of the evidence. To address this, we have reported findings according to the levels of evidence to highlight the scope of the literature. Categories used to organise and describe studies (designs and delivery type: group, dyadic etc.) may have some overlap. The following discussion reports on common review themes and identifies evidence gaps for further research.
Focus on fathers
Since 2015, there appears to have been an explosion of research published on IPV and parent–child interaction, especially related to interventions for fathers. The significant variation in study type, design, intervention delivery method, setting, sample size and outcomes measured makes it difficult to make sound conclusions about what methods are best for supporting parents and children to restore relationships post-IPV. Trial-level evidence for programs (to support abused women and children) is reasonably strong, with good sample sizes, although in-depth analysis of the risk of bias was beyond the scope of this review. We agree with other researchers that the evidence base is underdeveloped and that more rigorous studies are required (Latzman et al., 2019).
The evidence on fathering interventions did not address earlier concerns highlighted in the literature about safety and ongoing IPV risk (Labarre et al., 2016; Toone, 2018). This was possibly due to the types of interventions for fathers we identified (e.g. primary prevention, clinical treatments) but ongoing risk assessment remains a high priority in interventions with fathers. Critique of father interventions was more directed to methodological issues and potential bias, for example where abusive men are self-reporting improvement in attitudes, knowledge and behaviour change. A small amount of qualitative or mixed methods research was identified but much more is needed to inform program feasibility (especially in rural areas) and to identify the essential elements of successful program implementation, in conjunction with future trials.
Relational interventions
Psychotherapeutic and psychoeducational interventions dominate the evidence, with some suggestion that longer term psychotherapy improves child, maternal and relationship outcomes. Overall, few studies reported on the sustained benefits of programs. Treating both mothers and children together appears optimal, as there is clear evidence that improvements in maternal mental health predict enhanced child functioning and mother–child relationships (Marie-Mitchell & Kostolansky, 2019). Brief interventions, while appealing to funding bodies and providers, may not be suitable for families exposed to IPV, especially children with high trauma symptoms who were reported to benefit most from treatment (Pernebo et al., 2019). Dyadic work is resource-intensive but may be the most cost-effective considering the harm IPV has on children, families and generations (Spangaro, 2017). Dyadic psychotherapy for mothers and children exposed to IPV has been recommended since 2013 (WHO, 2013b).
New studies are now combining treatments to include group, dyadic and individual sessions for pregnant women and all family members, however, the sustained and real benefit of group therapy over dyadic treatment remains unclear. Outcome measures seem to have expanded beyond child behaviour and mental health since the earlier review (Howarth et al., 2016) and call by Howarth et al. (2015) for more consistent use of outcomes in this field. However, outcomes remain clinically focused, and a lack of consensus remains on best measures/instruments to use.
Australian research needed
Very few studies originated in Australia, indicating a lack of evidence-based treatment options and research on IPV and parenting locally. The testing and replication of interventions identified in this and previous reviews are warranted. Psychotherapy or combined psychotherapy/educational programs that are jointly delivered to abused mothers and children may be of greater benefit than educational programs alone. Identification of contextual differences and cultural adaptation (including in rural settings) is essential for many of these interventions which have been tested in the United States, often with non-representative samples.
In late 2019, our research team was successful in obtaining ANROWS funding, with legacy funds from the former Luke Batty Foundation, to test the feasibility of implementing CPP into Australian rural and urban service settings. This funding extended existing research: Reconnecting Mothers and Children after Family Violence, or RECOVER, which had begun in 2017 through the Safer Families Centre for Research Excellence at the University of Melbourne. [1]
1. See https://www.saferfamilies.org.au/
Part 2:
Research process
Research questions
1. How acceptable and feasible is CPP for IPV-affected mother–child dyads to the Australian context?
- How acceptable is the intervention for women and service providers?
- What are the barriers and facilitators to the implementation of the CPP model into services?
- What (if any) are the dyad recruitment and retention issues encountered?
- Are there process and impact differences between service providers across sites?
2. Do CPP therapists-in-training adhere to CPP model fidelity?
3. How effective is CPP treatment delivered by CPP therapists-in-training during the study?
- Do women’s and children’s trauma symptoms differ before and after treatment?
- Does treatment improve the mother–child relationship?
Design
We used a concurrent, mixed methods feasibility study design to assess acceptability, implementation processes and effectiveness of CPP for RECOVER families. In addition to qualitative process evaluation, descriptive quantitative data on recruitment and implementation were collected. In a longitudinal, repeated measure design, outcome measures were assessed via parent survey at three time points: baseline (pre-intervention; T1), 12 weeks into the core CPP phase (midpoint; T2), and at the completion of the intervention (post; T3). Clinical data of measures were collected from service records. Practice champions were embedded within two services and supported recruitment and facilitated data collection. Practice champions are leadership staff within an organisation who are passionate about using evidence to inform practice and who support the implementation of new practices within the clinical environment.
Qualitative in-depth interviews with therapists and managers occurred mid- and post-intervention. Women were interviewed post-treatment. Direct observation of dyad interactions throughout treatment were recorded and assessed.
Participants
- CPP-trained therapists from Victoria and South Australia
- service managers
- practice champions
- mother–child dyads who have experienced IPV and meet the inclusion criteria.
Practice champion role
RECOVER practice champions included clinical leaders (one in a rural CAMHS, one in an urban family violence service) who advocated for CPP implementation and development within their respective services. These two practice champions (involved in the RECOVER 1 sites) were carried over to the RECOVER 2 settings. On a part-time basis, they maintained relationships with CPP international trainers, coordinated team supervision or mentoring, monitored CPP fidelity, and ensured that CPP and young children’s needs were kept on the agenda within multidisciplinary teams delivering a range of service offerings to different age groups. Both practice champions participated in the CPP national community of practice and in a monthly supervision phone call with CPP international trainers. The roles grew to provide peer support to each other and on one occasion, when a champion from one service took extended leave, there was an arrangement whereby the other provided CPP supervision to staff to ensure training requirements were met.
Study sites and recruitment process
In addition to clinical site therapists and managers, we sought eligible parent–child dyads from clinical services via intake systems. These study sites were chosen due to the accessibility of trained or trainee CPP therapists and service providers. As there is a shortage of staff qualified in CPP, most therapists underwent CPP training during the time of the study.
Eleven community-based, clinical sites including specialist family violence services (with clinical services for children), child and adolescent mental health services (CAMHS), one enhanced maternal and child health centre with a multidisciplinary team and co-located infant mental health specialist, and one private perinatal psychiatry clinic participated in RECOVER and actively recruited suitable mother–child dyads for the study.
Five urban, three rural and three regional service sites were chosen across Victoria and South Australia (Table 1). Recruitment periods at sites were approximately six months each for RECOVER 1 and 2, depending on workforce availability and capacity.
Table 1: CPP recruitment sites, location, phase and therapist qualifications (n=11)
| Clinical site | Location | Australian state | RECOVER phase | Therapist base qualification |
|---|---|---|---|---|
| Family violence service | Urban | 1 and 2 | Child psychotherapist/psychologist | |
| Family violence service | Regional | 1 | Social worker/psychologist | |
| CAMHS | Regional | 1 and 2 | Mental health nurse/ | |
| CAMHS | South Australia | 2 | Social worker | |
| CAMHS | Rural | South Australia | 2 | Social worker |
| CAMHS | Rural | South Australia | 2 | Occupational therapist |
| CAMHS | Urban | South Australia | 2 | Social worker |
| Take Two | Regional | Victoria | 2 | Social worker |
| Hospital child protection services (CPS) | Urban | South Australia | 2 | Psychologist |
| Private perinatal | Urban | Victoria | 2 | Perinatal psychiatrist |
| Enhanced maternal and child health service (with co-located infant mental health specialist) | Urban | Victoria | 2 | Maternal and child health nurse |
Dyads were recruited and received treatment through specialist family violence and CAMHS, in metropolitan and regional areas of Victoria and South Australia. Recruitment was staggered as new sites came on board and occurred over two waves – RECOVER 1 in 2018 and RECOVER 2 in 2019–2020, with the welcome addition of ANROWS funding (with legacy funds from the former Luke Batty Foundation). Due to organisational capacity, a smaller number of dyads were recruited from other services such as hospital-based therapeutic child protection services (CPS), a private perinatal psychiatric clinic and a local government maternal and child health service. Potential mother–child dyads entering services were screened by CPP therapists to determine participant eligibility for the project, describe the study and gain informed consent. In this study, the emphasis is on exploring feasibility rather than efficacy and in fact efficacy cannot be reliably tested when therapists are still learning the model and have not met the full training requirements for delivery of CPP.
Fathers’ consent
All service sites that participated in the study had existing procedures for obtaining parental consent (from both parents) to treat children, including consideration of court orders governing parental decision-making. The specialist family violence service sites (children’s clinical service) had additional decision-making procedures directing safe engagement with fathers who were perpetrators in consent conversations about their child’s need for treatment. This included procedures for initial conversations and decision-making with victim and survivor mothers about the risks and benefits of therapists engaging or not engaging fathers in consent conversations about their child’s treatment.
All sites implemented the CPP foundation fidelity requirements that provide specific direction for “Assessing Child Safety Risks to Engaging in Trauma-Informed Treatment” (Lieberman et al., 2015. p. 262), where risks are coded. These include considering whether “child has contact with a violent caregiver who is unaware that child is participating in trauma treatment” or “child has contact with a violent caregiver who denies the child’s experience of trauma” (Lieberman et al., 2015. p. 262). It is worth noting that in contemporary CPP practice, perpetrator co-parents would at minimum be included in consent conversations about their child’s treatment and assessed for suitability to be included via collateral parenting or parallel father–child dyadic sessions (Groves et al., 2007; Lieberman et al., 2015). However, in RECOVER, while fathers’ consent for child treatment was requested, they were not provided with CPP collateral parenting or dyadic treatment at the study sites.
Therapeutic readiness
A complex range of individual, relationship and organisational or ecological factors impact on participant readiness to take up interventions (Fogarty et al., 2020; Howarth et al., 2018). “Therapeutic readiness” is a term initially coined in relation to the application of child psychiatry within community settings (Despert, 1949). It considers what factors internal to the individual child and caregivers, versus factors external to the child and caregivers, are conducive to initiation and engagement in treatment. The authors of the current study initially attempted to describe the idea of therapeutic readiness by developing an inclusion criterion based on the concepts of 1) maternal “readiness to change” within situations of IPV (Humphreys et al., 2011); and 2) a definition of sufficient mother–child safety as “post-crisis situation, or not living with the person using violence”. However, CPP itself provides a foundational framework that equips clinicians to determine therapeutic readiness considering family strengths and contextual risks (Lieberman et al., 2015, p. 265). Over the duration of study implementation and continuing to date, services participating in the study have continued at a local level to expand implementation of CPP and refine concepts of therapeutic readiness for this population. This expansion has especially considered the realities experienced by families experiencing cycles of violence, some of whom will separate, re-partner or remain together. More work however is needed to integrate and consolidate this learning as part of a national trauma- and violence-informed child mental health framework.
Recruitment criteria
Inclusion criteria:
- pre-school-aged child (3 to 5 years)
- biological mother of the child
- English-speaking mother
- recent exposure to IPV (past 12 months)
- mother has received subsequent IPV assessment and advocacy support (risk assessment and safety
plan, counselling and referral to legal, housing,
healthcare services) - therapeutic readiness: post-crisis or not living with the person using violence
- clinical signs of trauma (e.g. a child presenting with emotional or behavioural issues/impaired mother–child interaction based on clinical assessment).
Exclusion criteria:
- mother–child dyads where the person using violence continues to use violence and live in the family home or there is insufficient safety
- mothers who have been substantiated/documented abusers of the child
- mothers who are currently dependent on alcohol and other drugs
- previous diagnosis of maternal intellectual disability
- significant maternal mental illness, for example, psychosis
- children with a significant intellectual disability and/or autism which interferes with their capacity for engagement in treatment.
Process evaluation
To assess program feasibility, Bowen et al. (2009) suggest there are eight core study aspects to evaluate. These are program acceptability, demand, implementation, practicality (costs), adaption, integration, expansion and limited efficacy testing. In this study, we evaluated acceptability, implementation and costs, in addition to fidelity, reach and dose.
Acceptability
We explored whether CPP was a suitable method of treatment for therapists and families receiving treatment. Suitability criteria included satisfaction with/appropriateness of the model, intervention length, content and types of questions used in the survey, intention to continue with the treatment, and the fit of CPP within the organisational culture.
Implementation
Therapeutic interventions to support women and children need to be sustainable. The collection of process data is an important aspect in the evaluation of complex interventions like RECOVER. Assessing the feasibility of CPP in the Australian context involves having a greater understanding of the barriers and enablers to implementation and program sustainability.
Theoretical framework
In this study, factors influencing integration of the CPP model were explored using May and Finch’s (2009) implementation framework: normalisation process theory (NPT). This socio-behavioural theory proposes four essential principles or constructs that explain the type of work people need to do to implement a new practice or intervention. These include coherence (sense-making work), cognitive participation (relational work), collective action (operational work) and reflexive monitoring (appraisal work; May & Finch, 2009). These NPT constructs have been used to frame data collection tools and support the intervention and process evaluation.
Intervention fidelity, reach and dose
CPP fidelity monitoring was essential due to the potential diversity of clinical presentations and program flexibility. The CPP manual describes a six-strand fidelity framework, which includes reflective practice, emotional process, dyadic relations, trauma framework, and procedural and content fidelity (Lieberman et al., 2015). Each CPP phase has detailed fidelity tools incorporating this framework, which were completed by clinicians. Clinicians completed specially designed fidelity logbooks (based on work by Almqvist [n.d.]) after each consultation, which indicate adherence to CPP goals. Throughout official CPP training, treatment fidelity was closely monitored through a review of process notes and regular clinical supervision. Clinical data were collected on maternal, child and/or dyad assessment; fidelity measures; and the intervention reach (number of eligible dyads offered CPP) and dose (sessions attended/delivered).
Practicality including costs
Parents were asked about costs incurred in attending treatment sessions to gain some insight into the burden on parents. A cost–benefit analysis of CPP was not undertaken.
Data management
Participants and therapists were given a unique ID code for use throughout the study. A secure, purpose-built online electronic database was used to record and store all data including participant and therapist details. Dyadic interaction was recorded using tablet devices. Onsite clinical researchers regularly collated intake, fidelity and survey data. All data were uploaded as electronic files to university research drives that are securely stored.
Data collection time points
Pre-intervention
Therapists collected baseline quantitative outcome measures using a maternal survey (and parent–child interaction, free-play recording) in the foundation phase of treatment and recorded dyad free-play sessions. Survey responses also captured women’s expectations of the treatment and outcomes that most suited their needs. Therapists documented fidelity, attendance rates and dose for each dyad at each session. Table 2 provides time points and outcomes measured.
Table 2: RECOVER project outcome measures and data collection time points
Mental health and wellbeing
| Outcome measures | Pre | Mid | Post |
|---|---|---|---|
| Symptoms Checklist–90 Revised (SCL-90-R) | X | X | X |
| PTSD Symptom Scale–Interview (PSSI) | X | X | X |
| Composite Abuse Scale (CASR-SF) | X | X |
Child functioning and trauma symptoms
| Outcome measures | Pre | Mid | Post |
|---|---|---|---|
| Strengths and Difficulties Questionnaire (SDQ) | X | X | X |
| Young Child PTSD Checklist (YCPC) | X | X | X |
Parenting
| Outcome measures | Pre | Mid | Post |
|---|---|---|---|
| Parental self-efficacy, warmth, irritability and consistency | X | X | X |
Mother-child relationship
| Outcome measures | Pre | Mid | Post |
|---|---|---|---|
| Parental Reflective Functioning Questionnaire (PRFQ) | X | X | X |
| Recording of parent–child interaction assessed using | X | X | X |
Midpoint
While the true midpoint of a flexible, needs-based intervention is undetermined, findings from previous CPP studies suggest dyads require between 20 and 32 weeks of core therapy. Consequently, we defined our midpoint evaluation to be at 12 weeks. Researchers conducted process evaluation interviews with CPP therapists and managers, using NPT to explore feasibility, experiences and contextual factors related to implementation. Therapists also collected maternal reports of quantitative outcome measures and recorded direct observation of dyad free play.
Post-intervention
Researchers conducted impact evaluation interviews with mothers, therapists and managers, using NPT to explore feasibility, perceptions/experiences and contextual factors related to implementation. Quantitative outcome measures and dyad free-play recording were completed by therapists in the termination phase of treatment.
Outcome measures
The main focus of this study was on feasibility as CPP is an evidence-based intervention. However, we were interested in testing evaluation instruments with mothers and therapists and reporting any concerns and possible outcome changes. When deciding on outcome measures to use in this study, we considered 1) measures used in the original Lieberman (2015) trial and those recommended by CPP developers; 2) calls within the literature to expand assessment beyond child mental health and behaviour; 3) participant and therapist burden; 4) service provider capacity and experience (and alignment with existing measures used by services); 5) instrument and training costs; and 6) the age of children. The main outcomes of interest included maternal and child mental health and trauma (PTSD) symptoms and child behavioural problems. PTSD in 3- to 5-year-olds often manifests as behaviour problems and these were used as a basis for the description of the disorder (Table 2). Secondary outcomes measured recovery by assessing parenting (self-efficacy, warmth, irritability and consistency), reflective functioning (or the mother’s ability to hold the child’s mental states in mind), responsiveness and the mother–child relationship/interaction.
Analysis
All interviews were audio-recorded, transcribed by a professional transcription service, coded by two RECOVER researchers and analysed using an NPT lens. Process evaluation assessed the model’s feasibility and identified contextual program barriers and facilitators to inform future research. NVivo software was used to assist the analysis. Statistical analyses were completed using STATA Version 15. Proportions and means (with 95% CIs [confidence intervals]) were calculated to describe participant baseline characteristics, fidelity and feasibility measures. Paired samples t-tests compared mean scores at different time points. If data were not evenly distributed, medians, range and non-parametric tests were used. Survey responses with missing values were removed list-wise.
Dyad video recordings of free play were viewed and coded using a coding scheme specifically designed for observation of parent–child interaction called Coding of Attachment-Related Parenting (CARP; Matias et al., 2006). Domains included parental responsiveness, sensitivity and affect; child affect; and dyad mutuality. All recordings were double coded by researchers, with inter-rater reliability calculated. If parents did not consent to recording, then therapists made notes of parent–child interaction and these notes were then coded and analysed using the CARP guide.
Ethical considerations
Consent
Due to the nature of treatment, women’s consent to the project could only be obtained when it was clear that women and children required treatment. This was not evident until a thorough assessment of the dyad was made by an experienced therapist, after intake to one of the participating services. If women and children were deemed unsuitable or not ready for this specialist type of treatment, they were offered alternative support (e.g. case management, individual/group counselling). As such, therapists, rather than researchers, obtained informed consent and facilitated collection of clinical outcome data. Women were provided with a participant information statement and invited to ask questions about the research and sign the consent form for herself and her child to participate. However, all participants had clear instructions (in verbal and written form) that their participation was voluntary and that they could withdraw from the study at any stage without prejudice, disadvantage or interruption of treatment.
Vulnerable group
The clients are a vulnerable group, some of whom have potentially been traumatised by their experiences of violence. Experienced qualified clinicians delivered CPP and managed any potential distress. Researchers interviewed clients once post-treatment and adopted a distress protocol including information for referral. RECOVER researchers are trained and experienced in family violence identification and supportive debriefing in the event of participant distress.
When therapists and service managers were interviewed, they may have felt uncomfortable about discussing implementation in relation to their organisation, and concern that they could be identified. Clear information was provided to staff regarding privacy prior to consent, and all participant data were de-identified.
All ethical considerations and applications for approval of the research were guided by the WHO recommendations on ethics and safety for intervention research on violence against women (WHO, 2016).
Prior to research commencing, human research ethics committee approval was received (including all modifications) from La Trobe University (HEC17-108), Goulburn Valley Health (GVH 03/18), the Victorian Government Department of Health and Human Services (HHSD/19/234647), and South Australia’s Women’s and Children’s Health Network (HREC/19/WCHN/88).
Part 3:
Research findings
1. How acceptable and feasible is CPP to the Australian context?
Forty in-depth process and impact interviews were completed during the RECOVER project to assess program acceptability and feasibility: 28 interviews with therapists (n=15) and managers (n=13), and 12 interviews with women on the completion of treatment. Overwhelmingly, the intervention was acceptable to the majority of participants. Except for two women, all participants including therapists and managers reported CPP as a suitable treatment option for IPV-exposed families. In addition to asking women about the acceptability of the intervention, therapists were asked how acceptable CPP was for their clients and themselves.
Mothers
There are so few interventions for young children, with many being for older children, meaning CPP is quite unique. The majority of mothers found the program useful and acceptable. One mother called it “phenomenal” (Mother 3).
Those who found the program the most acceptable usually had a very good relationship with the therapist, as did their children. These dyads often received longer treatment and saw their children develop as well as their own confidence as a parent, as they learned how to manage their situation.
This experience, good has to come out of it and one of the things is connecting with her [the therapist] and having her support and my son just adores her, she’s been amazing. (Mother 6)
Therapists noted that mothers would often see the importance of CPP for their child but, through the therapeutic process, realise the impact on their own healing, as the program supports parental confidence and growth, as well as healing the dyad relationship. “It’s a lovely model to support mums and children.” (Therapist 6)
One mother described how she had previously been “covered in armour” protecting herself as a result of prolonged IPV. She attempted to shield her children from the abuse alongside her own stress and trauma. Working with the therapist helped her learn to express her inner feelings and emotions with her children and to reach out to support networks. “It helped me express who I am.” (Mother 11)
Women’s motivation to seek therapy was generally for the wellbeing of their child/ren after experiencing family violence-related trauma. They predominantly saw it as an opportunity to support their children emotionally and to improve their relationship with their children and their own parenting skills. Many mothers reported their child to be anxious and/or having attachment problems and hoped the program would help build the child’s confidence and improve communication, especially about their feelings. “I wanted to figure out how do I help her, then to help us.” (Mother 3)
The program allowed mothers to see how the therapist worked with the child, modelling a learning, reflective and relational practice, so they could learn to adopt these reflective strategies with their child.
They’re kind of getting to learn and say, “Oh, well I can try that, or the therapist did that, that didn’t work very well”, or whatever. There’s kind of a sense of teamwork like you’re trying stuff out and you might not always get it right, but sometimes it works and you know, there’s that kind of sense of us being in the struggle and sharing that struggle with mums and kids, and them not being alone and perhaps to feel that they can take some of what they learn back with them, out of the room, as well. (Manager 4)
The mothers themselves wanted to gain these skills.
For myself, it was about getting some tools and strategies to help my little girls to help them get an understanding of what their feelings were and how to help them with that when they were really struggling. (Mother 9)
However, some mothers were focused on supporting their children without fully grasping the impact CPP may have on them, as mothers. Women come into the program with their own trauma history (recent IPV and/or earlier trauma), which they often do not expect will be considered in the sessions. Some mothers may not want to share their history.
Interviews were captured with some women who disengaged early, before treatment even started. Mothers in this group (n=2) did not find the sessions acceptable, usually not connecting with the therapist and/or having an inconsistent experience with the therapist, and not finding the sessions as useful as they had expected. These reports were from one rural service which lacked established clinical governance structures and where therapists were still completing CPP training. “I didn’t get along with her – she was nice, but I didn’t feel like we were achieving anything … I just felt like my time was being wasted.” (Mother 2)
“It’s just had such an amazing impact on all three of us and I’d do it again and again just for the things that I learnt and the things my girls learnt and the things we learnt together. I feel like to a degree they got their mummy back.” (Mother 9)
Therapists recognised that women had to be “therapeutically ready” to take on an intensive intervention like CPP. Many clients had complex trauma in the family and therapists have a very short safety window at times with clients. In these cases, when
safety is not particularly well established, mums are really traumatised themselves and are quite often nominating that they don’t have the capacity to engage in long term – they can’t think about the logistics of engaging in a long-term therapeutic intervention. (Therapist 11)
Therefore, therapists learnt over the course of the pilot to assess readiness before they suggested CPP. If a mother had very recently experienced violence and was still focused on acute practicalities, she may not be ready to make a commitment. In some instances, the mother engaged briefly with the service and then after several months came back to engage in the longer service.
Several rural therapists suggested women were unable to engage in CPP for other reasons – for example, they may not understand the treatment, thinking the problem is the child, or being burdened themselves by life circumstances.
So you know the ideal of maybe seeing a family for four sessions over four weeks doesn’t happen. I think that that’s a – they want to stay involved, but they just can’t, they don’t have – what they talk about is not having the headspace to do four weeks in a row, or they’ve got big families, no car, you know poverty is a big thing. (Therapist 9)
I mean, we get a lot of parents who come in here and say “Come here and fix my child. It has nothing to do with me.” (Therapist 1)
While there were some concerns, in general the majority of therapists were very positive about CPP for dyads: “Yes they’ve been really positive. I’m not surprised, they come every week, they’ve been really engaged. I think it’s been quite acceptable to them.” (Therapist 10)
I think that the mother having to provide her own trauma history and her own attachment history was really hard for the mum that I’m working with, to understand. She’d come for therapy for her child, she really didn’t understand what it was that – why I was talking about her parents or her childhood or, you know, her past relationships with other men, who weren’t the father of this child. I had to spend a lot of time creating a shared understanding of why I needed that information and that I wasn’t just collecting information for information’s sake, or trying to snoop into her history. That was challenging and I think wouldn’t have been accepted if it was a less overt model of – I really like the overtness in this model. We’re very upfront about what it is that we’re doing and why, with clients, at all times. I think that that creates acceptability, where I think in other kinds of therapy that would be lacking. (Therapist 11)
Suitability of outcome measures
Maternal surveys captured a lot of information, including sensitive questions about women’s relationships, health and past abuse. One therapist was concerned that the survey questions might be upsetting for the client. However, she noted, “In actual fact it wasn’t a big deal at all, the women were very happy to fill out those questionnaires and it wasn’t a problem”, and further that “a lot of the mums have reported that they found doing the measures quite validating” (Therapist 6).
Women reported mixed feelings about the IPV Composite Abuse Scale questions in the survey. Some mothers reported that the survey questions about abuse and violence were not complex enough. “I think the survey or questions that you asked to do with trauma weren’t nuanced enough to pick up on complex trauma rather than sort of more situational.” (Mother 5) In contrast, in a few cases, mothers thought the questions were difficult. “It was intimidating [the questionnaire], I guess because a lot of time it’s not something you like to think about, it’s something you choose to forget.” (Mother 2) However, this was not the case for most participants.
Therapists reported that some mothers, on describing the IPV they had experienced, had concerns about being judged as poor parents within court contexts and/or being reported to child protection services. This is an issue not unique to CPP.
I think the family violence dynamic brings in something that’s a bit even hard for me to articulate. But it does … make it much harder for a mum to trust engaging with a service, and talking about their child, when they think that there’s even a remote possibility that their parenting will be judged as poor, and that that information will get back to a court environment, or that the father or violent person will be able to somehow access the information and use it to their advantage. And just what it’s like for women to live under risk, such high levels of risk all the time, makes it very hard to come to weekly appointments, and their kids are frequently sick for the same reason. So that’s what I’ve found. (Therapist 9)
Acceptability of CPP for therapists and managers
Managers found that CPP was beneficial for the individual therapist, but also for the broader organisation. The intervention was also something that created a sense of purpose and reward for therapists. “The clinicians have said to me, you know, basically it’s the highlight of their week.” (Manager 4) Further,
There’s a real sense of community in the intervention, then those little communities that you’re developing with each of the children and the mums. You know, there’s that sense that they’re finding it valuable, you know, that kind of sense that they’re feeling – these children are feeling more able to talk and mums, even amidst all the other demands they’ve got, are being able to show up. There’s something valuable that they seem to be getting out of it, which I think is very rewarding. (Manager 4)
Well, personally I think it’s an excellent model that sits very well with the work that we do. I’m a bit surprised why it has not been used more widely, maybe because of the resource-intensive nature of the work. (Manager 6)
Therapists were optimistic about CPP positively impacting children’s mental health and the impacts this would have across their lifespan. By addressing children’s mental health needs they are potentially dealing with trauma whereas if they did not access therapy, this trauma might manifest as they age.
I have trained in a lot of different therapeutic programs and to me, CPP – if I could only do one therapy with anyone and everyone, I would only do CPP because it just – it has the biggest ability, capacity, significance in changing within children … (Therapist 4)
Addressing child mental health was important to therapists and managers who were frustrated at times at the lack of early intervention work they could offer in their organisation. CPP filled this void.
… having worked in this area and in this region. There are so many children and young people that we see and come across and we go back to their files, and we look at when was the first time that they were referred or when did the difficulties start. It all points to the early years and so it’s overwhelming the evidence. The fact that we don’t do much about it when it’s needed, but when we try to intervene later on in life, the trauma that has already occurred is probably not addressed. (Manager 6)
One therapist felt CPP was a challenging intervention to offer for those who have less experience and suggested it should be a model that is only offered to experienced clinicians.
So I think it’s more probably a model that should be offered to senior clinicians especially clinicians that have had either experience or training in infant mental health or perinatal infant mental health. Or, therapy looking at reunification of parents and children that have been separated after child protection concerns. So yeah, I think it should be saved and targeted for those kinds of clinicians or therapists rather than a kind of generalist therapeutic model. (Therapist, 8)
CPP has been criticised in the past for its intensity and the time commitment and potential length of the intervention. One therapist felt this model of delivery was justified.
… the baby can’t wait and that mum – if we focus on mum’s therapeutic intervention, you know, the baby’s developmental processes are so much quicker than the mother’s that, you know, they will have developed post-traumatic stress disordered symptoms and difficulties and emotional dysregulation, so we can’t wait to treat the mother’s symptoms in order to treat the baby’s … The length is necessary and the intensity is necessary because the baby can’t wait. I actually feel quite good about that and the rationale for that, and why that length and intensity is required. I think that the families really benefit from that very close and caring relationship with someone who helps them think about their relationship and their baby and their mother in a different way. (Therapist 11)
Acceptability of CPP for children
Therapists and managers were positive about the acceptability of CPP for children. They noted that children were engaged in the program and at times they saw rapid improvements in a child’s mental health. Although a positive outcome for children, the process of healing could be difficult. One therapist noted CPP brings up issues that children have likely been encouraged to ignore or forget, and so it is a new experience to address this trauma.
I think they come and play but I think it’s hard as well because CPP speaks the unspeakable and we don’t kind of shy away from that. What I’ve noticed is a lot of those kids, people outside of the therapy room probably avoid talking about dad and so initially they’re quite surprised when we raise him and pretty quickly and when we continue that conversation. (Therapist 10)
However, others described the process as a positive experience for children, who would often drive the change required in the dyad’s relationship.
Some of them [the children] are just hanging out to have these conversations with their parents, and to be understood in a different way, like they usually come into appointments I guess and have their parents talk about them, and all their problems … (Therapist 2)
To engage with the child, therapists build a relationship with the mother. In particular, at the initial stages, the child may not be present so that the therapist is able to assess the needs of the mother and child through intensive sessions with the mother. Once that has been established, the therapist can then build a rapport with the child. “You walk into that waiting room and they’re excited to come in.” (Therapist 1)
Initially, some mothers thought their children did not need the program. Mothers regularly hoped that their children did not remember the family violence and were minimally impacted. However, “kids always remember more than what the mum would like them to or thought they were exposed to” (Therapist, 10). For some mothers, this was “confronting”, although the program allowed for a safe space where children could explore what they had experienced. For example,
I’ve been working with her [the mother] and her little boy for over a year now, and in the session just last week, he was raising this incident, and he knew that it was safe to raise, and he knew that his mum was supportive enough that he could raise it, and we could help him to talk about what he needed to talk about, which was his memory of this really frightening thing, and just how confusing this was for him … He was able to talk about this incident, in a lot of detail, that the mum and I were able to support him to slow down, to feel really safe. So he wanted to tell his story, but he knew that it was scary to talk about, so he and his little sister cuddled up on mum’s knee, and they all kind of did what they needed to feel safe and secure with each other, and to just visit this memory for a very short time, which was really upsetting; and talk about it, and then to be supported to feel safe again in the moment, and knowing that we can keep talking about it, that you know, we can do so together in a way that he’ll feel safe and supported, and not overwhelmed and re-traumatised … CPP is a beautiful intervention, in its ability to do that. (Therapist 6)
Although processing traumatic experiences may be distressing and confronting at times, CPP is a treatment that privileges hope and is led by the spontaneity of the child. CPP treatment experiences therefore can also be fun. Children reportedly enjoyed attending the intervention because of the focus on play.
The kids I see, they really love it. You know, that time of having time with their mum, where … you know, the session is that she speaks their language, in a way … through play, and also through language that’s connected to the playing. You know, it’s a time that’s for them, and so children love coming to the sessions. (Therapist 6)
In this environment, children are able to open up about their experiences. “I just find it gobsmacking how the children will respond if there’s an opportunity for them to be heard and be respected and know that their view is important.” (Therapist 7)
Mothers’ reports on children’s experiences
Activities initiated by the therapists allowed for children to express themselves via play, for example, how they felt about the violence they had seen and experienced. The mothers reported that their children’s behaviour generally improved both in public and in private, such as in behaviour and communication skills and the ability to identify and acknowledge their emotions.
… when she got comfortable and she started connecting to the dolls and she would act things out or draw pictures and say how she’d felt. I knew that was a turning point because she’s actually expressing herself instead of trying to hide it away. (Mother 4)
Those participants who managed to attend five or more sessions, especially those who attended for more than a few months, really saw the positive impact the program had on their children. “I think probably the most helpful thing for her [the child] was to express how she was feeling.” (Mother 3)
One woman spoke of her concerns with co-parenting and the impact this could have on her and her child’s recovery:
She’s very traumatised by all of this stuff and then the courts have gone and said, “Well 50/50 share with all parents, he deserves to be a dad”, even though the majority of the issues he’s caused. (Mother 8)
For those children that did not attend many sessions, mothers reported little improvement even if they thought their child enjoyed the experience with the therapist. This occurred in a rural setting without existing structures to support staff development, and mothers acknowledged it was most likely because they did not attend enough sessions for the program to have a long-term impact.
I think they were happy enough to be there. I don’t know exactly how much they took out of it. Obviously, we didn’t go enough times for them to have a great benefit from it. (Mother 7)
Implementing CPP
- What are the barriers and facilitators to the implementation of the CPP model into services?
In this study, we used NPT (May & Finch, 2009) as a guide to understand the barriers and facilitators to implementing CPP for dyads exposed to family violence across the many different clinical contexts. NPT is a behaviour-based theory that can be used to describe the actions or work required to implement and normalise new clinical practices in complex settings. The theory can be used in research design, data analysis or to support reporting (Hooker & Taft, 2016). The four core NPT principles or constructs provide a framework to understanding implementation processes, barriers and enablers and the work required to implement and sustain programs. Table 3 outlines in further detail the NPT principles and their application to the RECOVER project.
Table 3: Normalisation process theory and application to RECOVER
| NPT construct | Examples of construct in | Identified implementation |
|---|---|---|
| Coherence |
| Barriers:
Enablers:
|
| Cognitive participation (participation work) |
| Barriers:
Enablers:
|
| Collective action (operational work) |
| Barriers:
Enablers:
|
| Reflexive monitoring (appraisal work) |
| Barriers:
Enablers:
|
Understanding CPP and family violence work (coherence)
Although all RECOVER therapists needed to be CPP trained or in training, the level of clinical experience varied across provider groups. Therapists who had existing experience in psychotherapy with young children were able to implement the program with more ease than those less experienced:
I think that for those people that already had existing expertise in that area, it’s been pretty easy, implementation, compared to those that were not familiar to talking to babies or young children or working in relationships. Also, in a family violence population, which has additional kinds of sensitivities, even to working with mums that may judge themselves, but when there’s family violence in the background, there’s extra difficulty. (Manager 4)
The workforce experience of CPP training to be able to deliver the intervention was met with positivity overall: “[The training is] one of the best training [programs] I’ve ever done and I feel like I’ve got a clear understanding of the model and how to do the therapy.” (Therapist 8)
Managers noted difficulty in their role managing staff if they as managers were not trained in CPP themselves.
I don’t really have a strong understanding of CPP but I’m the person responsible for making decisions around accepting referrals and you know talking with clinicians about the decisions that we make in terms of intervention. So, I think it would be helpful for team leaders and people supervising clinicians to have had the training or some more knowledge in CPP. (Manager ٢)
Therapists’ earlier training impacted how they approached the work and their level of confidence. Regardless of whether they were new to this model or had some previous dyad therapist training, their understanding of the work evolved over the length of the training.
Some therapists, including those working in child mental health services, did not have previous family violence education or the management skills to deal with adult women and the children affected by the abuse. Supportive systems were lacking to even identify those clients entering the service who were experiencing family violence.
I guess domestic violence has always been around but it’s not necessarily something that tertiary mental health services have necessarily thought about in terms of risk before either. (Therapist 1)
Recruitment coincided with a time of significant change and restructure for some organisations, notably changes due to the Royal Commission into Family Violence. Therapists were dealing with multiple system reforms and the piloting of other therapeutic treatment programs. Some therapists were involved in the delivery of multiple interventions or styles of therapy, in addition to CPP. For some, this was positive: “I think there’s massive overlap in a good way. I think the model and the approach is really relevant for the families that we are seeing.” (Therapist ١٠) Others found that engaging in multiple interventions made it difficult to learn and apply another intervention and could create confusion.
I think they have an understanding of it but I think they would probably consistently report to me that they want more, they want more [from the trainer], they want more exposure to [CPP]. (Therapist 10)
Clinicians struggled particularly in learning the model of CPP when situated in settings without adequate clinical governance structures. One participant discussed how her understanding improved once she had weekly supervision.
I think it’s improved. So I have regular supervision now. I’m getting weekly supervision now, and I’ve only had that for probably about six weeks. Seven weeks. And prior to that, I didn’t really get supervision, so I struggled with … I think I struggled with an understanding of CPP. (Therapist 9)
The CPP work appeared to be highly valued by therapists on the ground and to some extent the management structures. However, major changes to the organisational structure at one large urban site and the uncertainty of future program funding may have impacted on therapist investment and CPP engagement.
… it is unclear to what extent CPP will be taken up by the organisation in future. There remain key individuals that encourage involvement, however, most are on contracts ending soon. (Manager 4)
CPP participation and engagement (cognitive participation)
Therapists were generally highly engaged in the intervention. However, organisations that were able to support therapists, due to being a larger organisation or having supportive systems and adequate funding, saw staff with higher levels of engagement. This was particularly so at sites with a CPP practice champion, who promoted the CPP work and provided encouragement and support with recruitment queries, risk assessments and data collection.
When therapists observed positive changes in dyads, this encouraged engagement with the CPP work and organisational support for the model.
I was already able to see this mum thinking about and making connections between the child’s behaviour and their experiences and that was in the first session. So that was really good. (Therapist 1)
Aspects of the RECOVER eligibility criteria caused problems for some sites. Needing to recruit biological mothers limited those services that worked with children within the child protection system, not infrequently in the care of an alternative family member or foster carer. Also, in some cases of family violence, the mother had been murdered. Therapists noted that they used the principles of CPP in these cases, but they were not formally included in the RECOVER study. Similarly, requirements for the mother to have left the perpetrator were at times found to be unrealistic and not reflective of cycles of couple/family separation and repartnering.
In addition, the need to include pre-school-aged children was problematic for CAMHS. Child mental health services with clinical triage systems that prioritised certain client groups hampered recruitment and engagement with the intervention. When an older child presents in crisis, with more obvious signs of trauma, they tend to be triaged over a younger child, whose trauma may not be as recognisable to those without training in this area.
So it’s definitely not just adolescents. We’re getting eight- and nine-year-olds absconding from school and refusing school, and threatening suicide and self-harm as well. (Therapist 2)
This structural barrier to the recruitment of young children resulted in very few dyads recruited from the five CAMHS clinical sites. Additional structural barriers in CAMHS included a prior lack of family violence awareness in clients referred to the service, which prevented the identification of eligible dyads for the study. This was resolved over the life of the project.
Well, I think one of the major things has been that it has made us a whole lot more aware of family violence in our referrals. So we are now flagging with every single case and asking the question with every single case about family violence. And it’s really surprised me and a number on the team just – it’s almost every referral has some form of family violence involved with it. And that’s from the project, I think we’ve all just become much more aware of making sure yeah. (Manager 1)
Some clients wanted the father to be involved, however, fathers were not active participants in the study. “Some clients that would be ideal for CPP but it’s the dad, the dad’s the safe caregiver rather than the mum. The mum is not the perpetrator, it’s mum’s new boyfriend, but yes that gender thing as well.” (Therapist, 9)
A major barrier for therapists was excess workload and the crisis-driven nature of the clinical work.
… it’s across the board with our adolescents and all sorts of kids that are needing extra support. So our crisis presentations are the most heavy coming in, so I guess the ability to address those is priority. (Therapist 2)
Therapists at some sites were involved in multiple therapeutic modalities and had heavy caseloads.
Yeah. I mean I wonder whether as a team – because we’re learning in EMDR [eye movement desensitisation and reprocessing] and CPP and we’re trying to recruit clients for both, and work out which kids would be – and mum – would be suitable for which one. Whether if we were just doing CPP, whether we might have got more referrals for CPP, and been able to recruit more in. (Therapist 9)
The intervention is intensive, involving a substantial commitment to the client as well as commitments to weekly supervision. On top of this, therapists must adhere to the model itself which can take time to master. However, while this was an issue for some therapists, others found that CPP did fit into their workload. For example, when one therapist was asked, “How easy has it been to include CPP into your workload?” she simply replied, “Easy” (Therapist ٧).
In the later stages of the study, the COVID-19 pandemic caused further demands on services and interrupted service delivery to dyads, who spoke about the limitations of CPP via telehealth modalities. One mother called the impacts of COVID-19 “disastrous” (Mother 12). She explained that her child had started to open up in the sessions before COVID-19. The change to telehealth hindered the progress they had made. Difficulties included engaging the child to use the online modality, and setting up the lounge room to mirror the therapy space. At the end of the session, after working through some difficult topics, she would then have no reprieve or ability to change scenery, out of the new therapy space. However, due to the strong bond her child had with the therapist, they did still make some progress via telehealth.
While there were some issues incorporating CPP into organisations, over the length of the pilot, many of these issues were dealt with.
I guess we’ve been able to overcome that barrier because it’s a modality [CPP] that we see really help some clients and really works and we’ve been able to utilise it, you know, in our program very easily really. (Therapist 6)
How does the CPP work get done (collective action)?
The CPP resources and CPP training were valued by therapists, enhancing the operationalisation of the clinical work. In addition, the fidelity logbooks and other research tools aided adherence to CPP objectives.
The CPP resource manual provided therapists with the confidence and skill set to offer CPP.
The manual, Don’t Hit My Mummy, is very explicit about what skills you need to bring to it and how that looks in the room and what a port of entry is and how you intervene, so I think that I’ve learnt a huge amount in a fairly short space of time. (Therapist 11)
I use the manual a bit, when I’m working out what to do next I do look at the manual and use that, and the fidelity measures are quite good because they prompt you to make sure that you’re doing particular things through the different phases. (Therapist 2)
Outcome measure assessments as part of the RECOVER project supported therapists’ learning and guided their practice.
So I personally think it’s great. It’s got those parent–child observations in there and I do find the responses in the questionnaires helpful to kind of aid my understanding of where mum’s at and their understanding of the child and the difficulties. (Therapist, 10)
There were some difficulties for therapists in the smaller rural settings to engage in the intervention. Factors included rural therapists having less psychotherapy knowledge and skills and so they were being presented with new learning challenges. Rural therapists noted that travelling to the city for training could be difficult and was time-consuming. Lack of qualified staff was an issue for recruitment, and this was particularly heightened in rural areas. Larger urban organisations had greater funding and a range of therapists, and could train more senior and experienced staff.
I would say, the main issue is those folk in rural areas, that don’t have that additional kind of level of experience in working with infants and young children, have found it harder to engage and retain their – I think they’ve found it harder to engage and hold onto some of the clients that are coming through. I think it’s been harder for them, and also to recruit the dyads needed for the study. So, I think that’s about confidence. (Manager 4)
Rural workloads prevented extensive networking and promotion of the new therapy on offer.
I think management are a bit wary about going out and talking about what we do, just because the number of referrals is already way too overwhelming, and we don’t really want to be going out and drumming up any more work, I think that’s part of it. (Therapist 2)
One organisation created a specific role to link the services for childhood with family violence workers. Due to the connection already between the two areas in the organisation, CPP integrated seamlessly. However, inter-sector collaboration was restricted in rural areas. This interrupted referral pathways and, in particular, the offering of secondary support from family violence services to CAMHS.
I kind of thought that would be really different in the country, but my experience is agencies tend to work in silos more at times. So there’s not that collaborative approach or referrals that I would have expected coming in. (Therapist 9)
As mentioned above, the education levels and skills of the CPP therapists varied, with a variety of undergraduate professional qualifications. There was some concern from both therapists and managers about staff ability to work with young children. It was noted that the CPP model had excellent training and clear guidelines, which assisted the therapists.
It has given them the confidence to work with this age group. They had no prior experience with working with the under-fives and having gone through the training, I think it has been an important exercise in building capacity in the absence of any other training available in Australia that CAMHS can do that at this stage. (Manager 6)
All RECOVER therapists were trained or completing training in CPP. The training was met with an overwhelmingly positive response. “I think CPP – as a whole the training in CPP has been fantastic.” (Manager 6) Therapists also felt that the training was something that should be taken up by other clinicians. “I’d definitely recommend it to anyone, it’s a fantastic opportunity.” (Therapist 2)
Therapists found that the training was useful not only for learning CPP but also across their practice. While some therapists enjoyed the length of training, others found that it was burdensome alongside their busy workloads. Response to the CPP training and its application appeared to reflect the individual therapist’s background, as those who had a background in psychotherapy or infant training found they could understand and apply the techniques better than those who had no prior knowledge. Therapists were also applying the model as they continued through the training. Those with a clearer understanding of the training concepts were able to apply the model and therefore became proficient much more quickly. Therefore, they gained more experience, and the divide grew between those therapists and the therapists who did not have a psychotherapy background.
While different levels of experience could make CPP training difficult for some therapists, for others this was a welcome addition to their practice. For example, one manager noted that a particular therapist did not have extensive clinical mental health experience or child mental health experience. The training thus
[gave] her that kind of framework for working with those real young ones and the training and knowledge that you don’t get normally from doing short workshops. Like it’s been quite amazing to think that she is now in this position where she’s providing amazing intervention for these families. (Manager 1).
The ongoing training was also seen as positive, as therapists could bring questions they had to the group and discuss them each month. Therapists reported that they enjoyed the face-to-face teaching days and having this interactive learning with one another. Also, the teaching videos made by the CPP international trainer practising and modelling CPP with clients were singled out as positive learning tools. This training and organisational investment is needed to maintain the delivery of CPP. In this study, most organisations were very supportive of the project and happy to be offering CPP to clients.
I haven’t got enough people trained for sustainability, and I don’t want this investment that we’ve made to fall away. I think it’s been an important, valuable investment, but we absolutely need to invest further, to make the most of what we’ve already invested. So I probably need to train double what I’ve already trained, at least. Because obviously, you lose people, as well. (Manager 8)
Ongoing appraisal of CPP (reflexive monitoring)
All therapists offering CPP were accustomed to receiving clinical supervision and reflecting on cases and their practice. The fidelity logbook enhanced reflection, providing a practical tool to learn from and to support practice.
So I think even the nature of doing the logbook after each session, it kind of does keep you quite accountable and in the fidelity core intervention for the training, those headings that are in the logbook are expanded upon. (Therapist 10)
Staff also reflected on vicarious trauma and how this affected their work. While this might be something that therapists discuss in supervision, for some this was a more personal process. “I think that has to be something that’s more personal and separate to what would be provided at work.” (Therapist, 2) Peer discussions were viewed positively. These allowed therapists to discuss implementation issues and strategies. It also allowed staff to offer support to one another. Managers noted how positive this was and that in the future they would, ideally, have larger numbers of staff trained and delivering the program so there was a network of support.
It’s such a delight and privilege to be able to spend dedicated reflective time and [have] that built into a model where you can just really do deep dives into thinking about the experiences of children and women and also how we as clinicians get in the way and can get better and to foster that environment. (Manager 4)
Summary of implementation
The introduction of new clinical practices can be challenging. As outlined in this report there were many barriers outlined in participants’ responses to embedding CPP into their routines. Factors that enabled and challenged the implementation of CPP are as follows.
2. Do CPP therapists-in-training adhere to CPP model fidelity?
For each session, therapists completed a structured fidelity logbook assessing adherence to 17 CPP objectives according to the CPP manual and training (Lieberman, Ghosh Ippen et al., 2015). Responses to the items were made on a 0- to 3-point scale, with 3 indicating the highest level of adherence or satisfaction and 0 indicating no adherence. All eight therapists who provided CPP and treated RECOVER dyads completed logbooks, with data collated as the proportion of therapists adhering to CPP goals. Over 293 sessions, CPP therapists rated their own fidelity to the intervention as described in Table 4. Their rating of fidelity to CPP goals shows strong perceived adherence to most goals, especially conveying hope, developing relationships and enhancing safety, but less focus in other areas (in bold in Table 4). This included care coordination, supporting the child’s relationship with others and helping the dyad put the trauma into perspective. Adherence was greatest in conveying a sense of hope and developing a relationship with the dyad. Enhancement of safety in therapy was also high. Urban sites reported greater fidelity and adherence to all CPP objectives compared to rural and small services.
Table 4: Rates of adherence to CPP objectives (fidelity logbooks) reported by therapists (n=293)
| CPP objectivesa | 0–1 = No or low (%) | 2 = moderate (%) | 3 = significant (%) |
|---|---|---|---|
| 1. Convey a sense of hope | 6 | 30 | 64 |
| 2. Develop empathic relationship with family members | 7 | 28 | 65 |
| 3. Enhance physical safety | 24 | 39 | 37 |
| 4. Enhance safety – stabilisation (basic needs) | 21 | 40 | 39 |
| 5. Enhance safety and consistency in therapy | 10 | 28 | 62 |
| 6. Enhance safety within dyad relationship | 11 | 35 | 54 |
| 7. Promote emotional reciprocity between mother and child | 15 | 32 | 53 |
| 8. Coordinate care | 37 | 43 | 20 |
| 9. Strengthen dyadic affect regulation capacity | 24 | 31 | 45 |
| 10. Strengthen dyadic body-based regulation | 25 | 39 | 36 |
| 11. Support child’s relationship with other important caregivers | 31 | 43 | 26 |
| 12. Enhance understanding of the meaning of behaviour | 11 | 31 | 58 |
| 13. Support child in returning to a normal developmental trajectory | 20 | 30 | 50 |
| 14. Normalise the traumatic response | 14 | 31 | 55 |
| 15. Support dyads in acknowledging the impact of trauma | 22 | 28 | 50 |
| 16. Help dyad differentiate between then and now | 25 | 29 | 46 |
| 17. Help dyad put the traumatic experience in perspective | 26 | 29 | 45 |
a For CPP objectives, see pp. 215–223, 279–283 of the CPP manual (Lieberman, Ghosh Ippen et al., 2015).
Intervention dose
The length of each CPP treatment and intervention phase is flexible and depends on clinical assessment and dyad needs. Four dyads (27%) received a brief intervention (<10 sessions), and six dyads (40%) received a moderate dose (12 to 28 sessions). The remaining five dyads (33%) received more than 30 sessions, with one of these families receiving 50 treatment episodes over 18 months. The median number of sessions across all dyads was 23 (range 5 to 50) or less than six months of treatment time.
3. How effective is treatment by CPP therapists-in-training during the study?
Dyad characteristics
In this pilot, 18 families consented to CPP treatment and participation in the RECOVER study. Three dyads disengaged from the service before treatment began. Women who completed the T1 survey (n=15) were on average 34 years old. Children (n=15) were around four years of age
(Table 5). Forty per cent of women who completed the baseline survey were separated from their partners, 53 per cent were not working in a paid job, and 60 per cent were on a pension. No women were Aboriginal and/or Torres Strait Islander, and all were Australian born. Two women were from rural Victoria and the remaining 13 were from urban settings. As expected, all women reported substantial IPV from a male perpetrator.
Table 5: Participant characteristics (T1; n=15)
Children
| Category | Characteristic | % |
|---|---|---|
| Mean age | (months; SD) | 49.5 (13.5) |
| Gender | Male | 53.0 |
| Female | 47.0 |
Mothers
| Category | Characteristic | % |
|---|---|---|
| Mean age | (years; SD) | 34.3 (6.3) |
| Birthplace | Australian born | 100.0 |
| Aboriginal and/or Torres Strait Islander | No | 100.0 |
| Marital status | Married | 13.3 |
| Living with partner | 6.7 | |
| Have a partner but do not live together | 26.7 | |
| Separated or divorced | 40.0 | |
| Single | 13.3 | |
| Highest level of education | Degree/higher degree | 26.7 |
| Diploma/apprenticeship | 26.7 | |
| Completed secondary school to Year 12 | 26.6 | |
| Did not finish secondary school | 20.0 | |
| Employment | Paid job | 46.7 |
| Not working in a paid job at the moment | 53.3 | |
| Income source | Wages or salary | 40.0 |
| Pension or benefit | 60.0 | |
| Health Care Card (low income) | Yes | 80.0 |
| Family income (AUD) before tax | <$800 per week | 60.0 |
| $800 to $1,900 per week | 33.0 | |
| >$2,000 per week | 7.0 | |
| Intimate partner violence | Definite IPV (CASR-SF ≥ 7) | 100 |
Attrition and missing data
Table 6 outlines a comparison of baseline outcome scores between complete and attrited cases. No significant differences were seen between the two groups. Fifteen families (83.3%) completed a survey at baseline (T1) and 10 of these families (56%) completed surveys with matched data at T1 and either T2 or T3 time points. Missing survey data were less than 10 per cent and so this complete case data set (n=10) was used in the final data analysis. The small sample size reduces the statistical power to make meaningful conclusions from the quantitative data and as such we do not claim or conclude study effectiveness.
The quality of dyad free-play recordings (to assess mother–child relationships) varied greatly, with 13 recordings captured by therapists at T1 but only four dyad interactions captured at T1 and either T2 or T3. The latter four were used in the pre–post analysis (Table 7). The consistency of decision-making between coders was substantial (Cohen’s kappa=0.69).
Table 6: Attrition data and study variables of completed and attrited dyads
| Phase | n | % attrition | Comment |
|---|---|---|---|
| Dyads consented to treatment | 18 | N/A | N/A |
| CPP assessment phase | 3 | 17 | Note: 2 of the 3 mothers did not complete the baseline survey |
| CPP foundation/core phase | 5 | 28 | All completed baseline survey |
Mothers
| Study outcomes at baseline | Completed (n=10) – Median (95% CI)a | Completed (n=10) – Range | Not completed (n=5) – Median (95% CI)a | Not completed (n=5) – Range | p-valueb |
|---|---|---|---|---|---|
| Global Severity Index (SCL-90-R) | 2.17 (1.82 – 2.52) | 1.30 – 2.79 | 2.13 (1.40 – 2.86) | 1.04 – 2.38 | 0.423 |
| PTSD Symptoms Scale–Interview | 23.50 (15.94 – 31.06) | 17.0 – 45.0 | 30.50 (18.95 – 42.05) | 19.0 – 36.0 | 0.327 |
| Composite Abuse Scale (CASR-SF) | 24.0 (13.26 – 34.74) | 0 – 52.0 | 28.00 (0.34 – 55.66) | 0 – 36.0 | 0.423 |
Parenting
| Study variables | Mean | SD | Mean | SD | p-valueb |
|---|---|---|---|---|---|
| Parenting self-efficacy | 3.20 (2.39 – 4.01) | 1.13 | 2.80 (2.24 – 3.56) | 0.45 | 0.474 |
| Parenting consistency | 3.40 (3.17 – 3.63) | 0.98 | 3.45 (2.78 – 4.12) | 0.54 | 0.821 |
| Parenting irritability | 4.28 (2.35 – 6.21) | 2.69 | 2.5 (1.67 – 3.33) | 0.67 | 0.176 |
| Parenting warmth | 4.35 (3.98 – 4.72) | 0.51 | 4.47 (4.13 – 4.81) | 0.27 | 0.642 |
Child
| Study variables | Mean | SD | Mean | SD | p-valueb |
|---|---|---|---|---|---|
| Total difficulties score (SDQ) | 17.7 (13.32 – 22.08) | 6.13 | 17.0 (10.61 – 23.39) | 5.15 | 0.830 |
| Young Child PTSD Checklist (YCPC) – PTSD symptoms | 51.10 (41.56 – 60.64) | 13.34 | 52.20 (29.67 – 74.73) | 18.14 | 0.895 |
| Young Child PTSD Checklist (YCPC) – Functional impairment | 13.60 (10.12 – 17.08) | 4.86 | 15.80 (7.27 – 24.33) | 6.87 | 0.482 |
Mother–child relationship
| Study variables – Parental Reflective Functioning (PRFQ) | Mean | SD | Mean | SD | p-valueb |
|---|---|---|---|---|---|
| Pre-mentalising | 1.79 (1.35 – 2.22) | 0.61 | 1.83 (1.10 – 2.64) | 0.66 | 0.893 |
| Certainty about mental states | 3.78 (3.14 – 4.43) | 0.90 | 4.00 (3.26 – 4.74) | 0.60 | 0.638 |
| Interest and curiosity | 6.27 (5.88 – 6.66) | 0.54 | 6.29 (5.82 – 6.76) | 0.38 | 0.940 |
a 95% confidence interval.
b Nonparametric (Mann-Whitney U test) used for unevenly distributed data.
Baseline or T1 scores indicate that dyads were experiencing major mental health and trauma symptoms and parenting distress (Table 7).
The Global Severity Index, an indicator of overall maternal psychological distress, has a cut-off score of >1 (Olsen et al., 2006) to indicate severe distress. All women had scores well above this clinical cut-off at baseline and post treatment (100%). The PTSD Symptoms Scale Interview cut-off for a diagnosis of maternal PTSD is >23 (Foa et al., 2016). Over half of the sample had scores above this cut-off at baseline, which reduced to 40 per cent post-treatment. Scores did improve after treatment on all maternal mental health indicators but most variables did not significantly differ on statistical analysis between data collection time points. It is unclear why these mental health and trauma symptoms failed to change, however women did continue to experience violence from partners during the treatment which may have impacted on their mental health and wellbeing.
Parenting scores improved on most indicators post treatment –significantly so for enhanced parental warmth (p<0.028), but not for other parenting items: self-efficacy, consistency or irritability. Parental affection and feelings of closeness to the child may have altered over the dyadic treatment as CPP has a focus on enhancing parent understanding of the impact of violence on the child’s emotional health and behaviour. Parental warmth has also been demonstrated as a benefit of CPP (Chu et al., 2021; Guild et al., 2021) and other relevant IPV and parenting programs (Sousa et al., 2021).
Reduced IPV exposure was reported post treatment (p<0.029) on the short-form revised CAS. The higher the CAS score, the more IPV experienced. The high CAS scores reported here are to be expected for this population, as the CAS measures partner abuse in the past 12 months. At T1, this captures the significant violence women experienced while still living with their abusive partners. Although abuse has reduced post-treatment (when families were in safer environments), some women and almost all children were still seeing the perpetrator (co-parenting at weekends, etc.). At T3, women continue to report high rates of IPV (Table 7).
Children’s SDQ total difficulties score (combined emotional, conduct, peer and hyperactivity problems) reduced from a mean of 17.7 at T1 to 11.40 at T3 (p<0.005), indicating a significant reduction in child emotional and behavioural difficulties. Up to 80 per cent of children presented with high scores on the parent report SDQ, well above the 12 cut-off score for this age group. This proportion reduced to 50 per cent post-treatment, a clinically relevant change. Probable cut-off scores for the YCPC indicated that 90 per cent of children had probable PTSD (≥ 26 for PTSD symptoms, ≥ 4 for functioning) on beginning treatment which did not change post-CPP. While planned, we were unable to assess the impact of shorter versus longer term CPP treatment due to the small number of dyads included. The small sample size in this study is a limitation and prevents any claim of treatment efficacy, however, shifts in the desired direction can be seen across most mental health/trauma, parenting and relationship outcomes (Table 7).
Table 7: Pre- and post-CPP comparison of study variables: Complete cases (n=10)
Mothers
| Study variables | Baseline CPP (T1) – Median (95% CI)a | Baseline CPP (T1) – Range | Post CPP (T3) – Median | Post CPP (T3) – Range | Diff (T3 – T1) | p-valuesb |
|---|---|---|---|---|---|---|
| Global Severity Index (SCL-90-R) | 2.17 (1.82 – 2.52) | 1.30 – 2.79 | 1.76 (1.24 – 2.28) | 1.20 – 3.14 | -0.41 | 0.307 |
| PTSD Symptoms Scale–Interview (PSSI) | 23.50 (15.94 – 31.06) | 17.0 – 45.0 | 18.00 (10.16 – 25.84) | 2.0 – 36.0 | -5.50 | 0.091 |
| Composite Abuse Scale (CASR-SF) | 24.00 (13.26 – 34.74) | 0.0 – 52.0 | 6.50 (0.42 – 12.58) | 0.0 – 28.0 | -16.1 | 0.029 |
Parenting
| Study variables | Baseline CPP (T1) – Mean (95% CI)a | Baseline CPP (T1) – SD | Post CPP (T3) – Mean | Post CPP (T3) – SD | Diff (T3 – T1) | p-valuesb |
|---|---|---|---|---|---|---|
| Parenting self-efficacy | 3.20 (2.39 – 4.01) | 1.13 | 3.60 (2.83 – 4.37) | 1.07 | 0.40 | 0.269 |
| Parenting consistency | 3.40 (3.17 – 3.63) | 0.98 | 3.10 (2.72 – 3.48) | 1.44 | -0.30 | 0.181 |
| Parenting irritability | 4.28 (2.35 – 6.21) | 2.69 | 3.32 (1.90 – 4.74) | 1.98 | -0.96 | 0.252 |
| Parenting warmth | 4.35 (3.98 – 4.72) | 0.51 | 4.67 (4.41 – 4.92) | 0.36 | 0.32 | 0.028 |
Child
| Study variables | Baseline CPP (T1) – Mean (95% CI)a | Baseline CPP (T1) – SD | Post CPP (T3) – Mean | Post CPP (T3) – SD | Diff (T3 – T1) | p-valuesb |
|---|---|---|---|---|---|---|
| Total difficulties score (SDQ) | 17.7 (13.32 – 22.08) | 6.13 | 11.40 (7.21 – 15.59) | 5.85 | -6.30 | 0.005 |
| Young Child PTSD Checklist (YCPC) – PTSD symptoms | 51.10 (41.56 – 60.64) | 13.34 | 49.4 (40.65 – 58.15) | 12.23 | -1.70 | 0.716 |
| Young Child PTSD Checklist (YCPC) – Functional impairment | 13.60 (10.12 – 17.08) | 4.86 | 12.1 (9.01 – 15.18) | 4.31 | -1.50 | 0.346 |
Mother–child relationship
| Study variables – Parental Reflective Functioning (PRFQ) | Baseline CPP (T1) – Mean (95% CI)a | Baseline CPP (T1) – SD | Post CPP (T3) – Mean | Post CPP (T3) – SD | Diff (T3 – T1) | p-valuesb |
|---|---|---|---|---|---|---|
| Pre-mentalising | 1.79 (1.35 – 2.22) | 0.61 | 1.63 (1.11 – 2.15) | 0.73 | -0.16 | 0.603 |
| Certainty about mental states | 3.78 (3.14 – 4.43) | 0.90 | 4.10 (3.32 – 4.88) | 1.08 | 0.32 | 0.147 |
| Interest and curiosity | 6.27 (5.88 – 6.66) | 0.54 | 6.16 (5.69 – 6.63) | 0.65 | -0.11 | 0.571 |
Coding of Attachment Related Parenting (CARP; n=4)
| Study variables – Parental Reflective Functioning (PRFQ) | Baseline CPP (T1) – Mean (95% CI)a | Baseline CPP (T1) – SD | Post CPP (T3) – Mean | Post CPP (T3) – SD | Diff (T3 – T1) | p-valuesb |
|---|---|---|---|---|---|---|
| Sensitivity | 6.00 (3.75 – 8.25) | 1.41 | 6.00 (2.82 – 9.18) | 2.00 | 0 | 1.0 |
| Positive parent affect | 5.50 (3.91 – 7.09) | 1.00 | 5.25 (2.53 – 7.97) | 1.71 | -0.25 | 0.634 |
| Positive child affect | 5.25 (3.73 – 6.77) | 0.96 | 6.00 (4.70 – 7.30) | 0.82 | 0.75 | 0.266 |
| Mutuality | 5.75 (3.75 – 7.75) | 1.26 | 6.00 (3.75 – 8.25) | 1.41 | 0.25 | 0.264 |
a 95% Confidence Interval.
b Nonparametric (Wilcoxon signed-rank test) used for unevenly distributed data.
Other results
At the T1 and T3 surveys, women were asked if they or their child had previously had any contact with the perpetrator (Figure 3). If so, the frequency of the contact was recorded (daily/weekly/fortnightly/monthly/greater than monthly). Mothers’ contact with perpetrators reduced over time (from 80% having contact down to 70%), however for those who did have contact, the frequency of contact increased. Children increasingly had frequent contact with the person using violence.
Figure 3: Participant contact with the person using violence by time point
| Time Point | Frequency – Mother | Frequency – Child |
|---|---|---|
| Contact T1 | 80 | 67 |
| Daily or weekly contact | 46 | 70 |
| Contact T2 | 70 | 100 |
| Daily or weekly contact | 86 | 71 |
Costs of treatment
Most women reported minimal costs to receive CPP treatment from services (Table 8). Travel, fuel and public transport costs were the most common out-of-pocket expenses. One family received CPP from a private provider who charged professional fees.
Table 8: Costs to attend treatment each week (n=15)
By Amount per week
| Amount per week (AUD) | % |
|---|---|
| Less than $50 | 64.3 |
| $50 – $100 | 21.4 |
| $101 – $200 | 14.3 |
| >$200 | 0.0 |
By Cost Description
| Cost description | % |
|---|---|
| Childcare | 23.5 |
| Travel/public transport | 41.2 |
| Loss of income | 11.8 |
| Other (e.g., parking, private treatment fees) | 23.5 |
The CPP community of practice in Australia
Through training, peer supervision and clinical practice opportunities, this project developed and promoted a national CPP community of practice that aimed to build workforce capacity, enhance practice, and provide a vehicle for ongoing education and professional networking for those working in the field.
The RECOVER project established the CPP Australia Community of Practice (CPP AUS CoP), chaired as a collaboration between Berry Street, La Trobe University and the Australian Association for Infant Mental Health (AAIMH) South Australia. Following an initial meeting in late 2019 in Adelaide alongside the AAIMH National Conference, the CPP AUS CoP was open to 32 CPP clinicians who had completed training. Participants in attendance expressed interest in participating in a biannual CoP forum to share practice experiences and resources. With the onset of the COVID-19 pandemic in early 2020, the CPP AUS CoP held the first online forum for clinicians to share experiences of telehealth practice adaptations, followed by a forum on archetypal play with Dr Chandra Ghosh Ippen and a webinar on perinatal CPP with Dr Alicia Lieberman. CPP AUS CoP participants presented a symposium together at the 2021 World Association for Infant Mental Health (WAIMH) World Congress on local implementation innovations with CPP in Victoria and South Australia. In March 2022 another 28 clinicians across Victoria and South Australia will complete the CPP training and be invited to participate in future CPP community of practice events. Future directions include the establishment of a secure online communication resource and incorporating a yearly case-based symposium on themes of interest in CPP.
Discussion
This study examined the feasibility of implementing CPP for Australian mothers and children exposed to IPV and family violence. CPP is an evidence-based psychotherapeutic intervention for families experiencing trauma (Lieberman et al., 2015). Currently, in Australia, there is an inequity of mental health service provision for very young children (Segal et al., 2018) who are disproportionately affected by traumatic events in early life (Lieberman et al., 2011). Our state of knowledge review identified a gap in effective treatments available to young children and mothers who have experienced family violence. The high prevalence of IPV and the contributing “shadow pandemic” or increase in family violence due to COVID-19 (Pfitzner et al., 2020) means there will continue to be a high demand for relational dyadic therapies such as CPP. Factors associated with the COVID-19 pandemic such as public health measures to enforce home isolation, loss of income, greater alcohol and other drug use and worsening mental health have resulted in increased rates of all forms of violence against women, with greater calls for help (UN Women, 2020).
The RECOVER pilot of CPP in Australia, specifically for mothers and children experiencing family violence, suggests that CPP is acceptable and feasible to implement in the Australian setting, in certain locations. Factors enabling the implementation of CPP into clinical services include established family violence system partnerships, service capacity to prioritise mental health and wellbeing responses for very young children, and strong clinical governance structures.
The COVID-19 pandemic impacted aspects of recruitment late in the study and impaired CPP delivery with most therapy either put on hold or offered via telehealth, which was challenging for dyads and therapists. Staff were often moved to other acute clinical areas and client intake was restricted to crisis cases only. Evaluation of CPP delivery via telehealth is needed and guidelines for CPP delivery are currently being developed by the CPP Dissemination Team at the University of California, San Francisco (Ghosh Ippen, Chu & Lieberman, 2020).
The study was conducted at a time of significant system change across non-government and public mental health service systems in Victoria and South Australia. The timing of these reforms as well as limitations in family violence system partnerships or early childhood mental health referral pathways hindered recruitment of the target population and implementation of this intervention for that target population. This was especially pronounced in rural areas and compounded by increased service demands for older children and young people, and children in statutory care. In the face of this demand, most service sites were simply unable to prioritise young children presenting with the mental health sequelae of IPV trauma. Mental health workforce shortages were also pronounced within CAMHS but were also a feature across all rural settings. These long-standing systemic barriers to service provision earlier in life and earlier in the risk trajectory of a family have been documented elsewhere (State of Victoria, 2021).
Our RECOVER findings are consistent with other countries outside the United States that have tested CPP in their contexts (David & Schiff, 2015; Norlen et al., 2020). In Israel, feasibility research showed that aspects of the intervention, the international CPP training and organisational readiness promoted CPP implementation. Consistent with our findings, Israeli therapists were highly motivated to deliver the intervention when they observed the benefits to young children and caregivers. Limited supervision and vicarious trauma were the main inhibiting factors. Like our rural therapists, isolated or solo therapists who have limited access to established supervisory structures and work with traumatised populations may struggle to provide optimal care (McLean & McIntosh, 2021). These findings suggest that future implementation and scale-up of CPP delivery in rural areas will require planning to ensure that rural therapist selection is based on the presence of a minimum level of access to supervisory structures, and building CPP virtual teams, whereby rural therapists are partnered with other CPP therapist peers. This may be a partner in the same service, or an opportunity to partner therapists across public mental health and non-government organisations within a region. Cross-service service peer partnerships may also build collaboration between, for example, family violence and mental health service systems to support workforce retentions and wellbeing, in the service of promoting women’s and children’s safety and wellbeing.
In other CPP feasibility research, Swedish caregivers receiving CPP felt their confidence and parenting improved, with greater reflection and understanding of child behaviour and the trauma they had experienced (Norlen et al., 2020). Caregivers reported children’s enthusiasm and positive responses to treatment, indicating CPP as a helpful endeavour, even during difficult discussions. The CPP therapists were highly regarded. As we have found in RECOVER, mothers noticed significant changes in their children in terms of development and self-regulatory behaviours that enabled children to manage everyday situations (Norlen et al., 2020).
In the present study, the average duration of treatment was less than six months (median number of 23 sessions). Very little is known about how to assess which IPV-affected mother–child dyads benefit from briefer models of dyadic care, versus those dyads that may require a longer treatment. Current research evaluating a six-month course of CPP will help to clarify whether a shorter treatment course by trained CPP clinicians in established services can provide comparable positive outcomes (Cerulli et al., 2021). In the period following the conclusion of the RECOVER project, some Australian services have received ongoing funding to provide CPP for IPV-affected mother–child dyads and are delivering this as part of a tiered or stepped-care model to best target delivery to those families who can most benefit from a CPP intervention (Fogarty et al., 2021). It will be important to understand how these stepped-care models, delivered by CPP clinicians (more experienced in delivering the model), can impact on recruitment, retention and outcomes of families experiencing IPV.
In the original Lieberman et al. (2005) trial, CPP was delivered by clinicians experienced in CPP, who provided an average of 32 treatment sessions per dyad. In these circumstances, the CPP model demonstrated efficacy in child behaviour, child trauma and maternal avoidance symptoms, and most maternal and child health outcomes (Lieberman, Van Horn et al., 2005), and positive outcomes were sustained (Lieberman et al., 2006) and replicated in subsequent RCTs (Cicchetti, 1999, 2006; Toth, 2002, 2006). The RECOVER study was delivered by therapists learning the CPP model who provided an average of 23 treatment sessions per dyad. Although no significant changes were seen across several treatment domains, it is interesting to note that, given the limitations in session number and CPP experience level, there were still positive trends observed across most treatment outcomes. Positive outcomes in child emotions and behaviour and parental warmth were also observed, consistent with the original Lieberman et al. trial (2015) and other CPP studies. In the present study these quantitative outcomes were reinforced by complementary qualitative reports from women and therapists.
Most children involved in this study continued to be parented by multiple parents or caregivers, including fathers who had used violence, indicating a need for fathers to be safely offered CPP treatment with their child. Although fathers were included in treatment consent conversations, they were not included in the RECOVER intervention. Fathers’ participation in their children’s treatment, where safe, could be considered to improve father and child wellbeing outcomes (Groves et al., 2007; Iwaoka-Scott et al., 2015; Mohaupt et al., 2020). Given that CPP treatment delivery offers a pragmatic and careful risk assessment and intervention approach by clinicians skilled in engaging children and caregivers together, future CPP delivery could be expanded to include fathers who have previously used violence and wish to change, if sufficient supervision, organisational partnerships and support structures were built (Groves et al., 2007; Toone, 2018).
Our finding that women reported a reduction in IPV during treatment is new and has not been measured before in RCTs or other feasibility studies. In one instance, Lieberman, Diaz et al. (2011) completed chart audits within a study of perinatal CPP which revealed no further incidence of IPV post-treatment. Our small sample limits sound conclusions and the reduction in IPV observed in the current study may have occurred naturally over time despite the intervention. However, it is possible that therapist discussions with non-participating fathers who had used violence (to engage them in consent conversations about the impact of violence on their child and their children’s need for therapy) may have influenced their use of violent behaviour and impacted on the levels of IPV women experienced. Although research with fathers who use violence is limited (Cater & Forsell, 2014; Stover, 2015), some evidence does suggest that men’s relationships with their children may be influential in changing men’s behaviour (Broady et al., 2017; Stanley et al., 2012; Stover et al., 2020). Further research is needed to explore this possible positive effect on women’s and children’s safety.
What is needed to sustain CPP within organisations?
For CPP to be sustained within organisations, young children and their mothers affected by violence need to be identified and referred, and trained therapists need to be supported in regular supervision. Strong governance and collaborative networks are needed to address the many contextual strengths and risk factors impacting on IPV-affected dyads (Groves et al., 2007; Lieberman et al., 2015). This includes more work in building organisational capacity and practice guidance in the delivery of trauma- and violence-informed child mental health care. Guidelines should also cover therapeutic readiness assessment to support relational safety for children in the care of multiple victim and survivor and perpetrator parents or caregivers and build staff confidence in providing this form of care (Bunston, 2013; Humphreys et al., 2020; Stover, 2015; Toone, 2018).
Better service collaboration between family violence and mental health services is needed to sustain CPP practice for this population of IPV-affected mother–child dyads. Within the reform context that is driving collaboration between non-government organisations and mental health services (Productivity Commission, 2020; State of Victoria, 2016, 2021), we anticipate that CPP will readily find a place as an acceptable and effective intervention for mother–child dyads. While the RECOVER project was instrumental in establishing the Australian CPP community of practice, for the intervention to be scaled up and dyads to receive intervention benefits, more CPP-trained therapists are needed. Investment in an evidence-based program like CPP early in the child’s life course may prevent intergenerational mental health problems and abuse, which could provide future cost savings for society and the wider economy.
Conclusion
CPP for IPV-exposed dyads is acceptable to clients and organisations, can be delivered in under six months and is increasingly available as more Australian therapists are trained in the model.
The strengths of this project are the mixed methods evaluation design; use of subjective and objective evidence; delivery of CPP at multiple clinical sites; and the use of implementation theory to guide project design, research analysis and interpretation of findings. The triangulation of qualitative and quantitative data, including both maternal self-report outcome data and direct observation measures (video recordings), adds credibility to our findings. Multi-site studies allow for greater participation of clients and mitigate recruitment risk. Clinical sites across varied locations enabled a deeper understanding of CPP feasibility, with comparisons between different qualified therapists, geographic locations and clinical organisations.
In this study, NPT (May & Finch, 2009) guided the design of data collection tools, analysis and reporting. Using implementation theory helps explain the key mechanisms that prevent or promote the implementation of complex interventions. This provides an additional level of rigour to process evaluation research. NPT supports the identification of individual and organisational barriers to embedding and sustaining new clinical practices (May et al., 2018). These can then be acted upon to improve policy, address the knowledge-to-practice gap and ultimately enhance clinical outcomes.
However, there were several limitations to the RECOVER project. The small survey sample significantly increases our margin for error and means we had limited power to predict the true impacts of the intervention. The limited inclusion criteria and attempt to define therapeutic readiness with reference to a post-separation and post-violence window of safety for families was not reflective of the experiences of violence-cyclical families. Therapeutic readiness requires a more nuanced and flexible approach, and training in such an approach is in fact provided by the CPP training model. This study criteria may have significantly impacted our recruitment. Addressing this and the other identified service recruitment and implementation barriers will assist with obtaining greater participant numbers in future CPP studies to further test program efficacy and impacts.
While it was disappointing that we were unable to retain some dyads, attrition in therapeutic programs with vulnerable groups like CPP is not uncommon (Herschell et al., 2017). The lowest rate of attrition in a CPP study was 14 per cent (Lieberman et al., 2005). The highest rates have been in preventative CPP interventions with non-clinical-treatment-seeking samples (Alto et al., 2021). While attrition varies across CPP studies (14 to 40%), there are similar dropout rates across treatment (intervention and control) groups, indicating challenges with study participation in general, rather than a failing of CPP overall. Similar dyadic interventions report comparable or higher attrition rates, for example attachment and biobehavioural catch-up (22%; Alto et al., 2021) and parent–child interaction therapy (25 to 69%; Lanier et al., 2011).
There may be many reasons why families disengage from services. In our study, women reported their relationship with the therapist to be a key factor influencing their ongoing engagement and experience of program acceptability. Some rural therapists lacked experience engaging young children and were more isolated from supervisory support structures, which in turn may have impacted on their capacity to build the necessary skills in parental engagement needed for CPP delivery. In addition, women and children who have experienced IPV may continue to be exposed to post-separation violence and psychosocial stressors (Humphreys et al., 2018), impacting their availability for regular sessions. Therapists in this study reported families temporarily ceasing treatment during times of maternal ill health, crisis or ongoing abuse. However, it is worth noting that the lowest attrition rate of CPP across all populations tested was with a racially diverse population of IPV-affected dyads and this lower rate was for a CPP treatment that was longer in duration than that provided in the current study. The treatment was also provided by therapists already experienced in CPP working from within an established CPP clinic (Lieberman et al., 2015). Many of the reasons families disengage do not appear to be related to treatment length or acceptability of the intervention, however further research is needed to draw any strong conclusions. Greater research is needed to understand attrition in these groups and ways of intervening during changing windows of readiness with families.
More research is needed to ensure some standardisation of outcome measures across therapeutic intervention studies allowing for greater comparisons, and more emphasis on measuring outcomes that are actually meaningful to families (Howarth et al., 2021). Existing trials of CPP have been focused on a 12-month model of CPP treatment and this is a significant investment for families and agencies (Alto et al., 2021). Longer term psychotherapy treatments require a higher level of engagement from families, as it has been recommended that CPP should be offered as part of a tiered or stepped-care model to best target delivery to those families who can most benefit (Toone, 2015; Valentino, 2017). Current research and implementation projects are evaluating briefer (six-month) courses of CPP (Cerulli et al., 2021) or brief interventions including those conducted via telehealth that draw on skills gained in CPP workforce training cohorts (Giallo et al., 2021).
Since the inception of the current study CPP has already begun to disseminate more widely in Australia within a range of service settings. CPP for the population of mothers and children affected by IPV is feasible in some settings, however this was not the case in all areas, especially with the current escalation of systemic pressures on CAMHS that limit response capacity for young children. The following key messages apply for policymakers to ensure CPP becomes part of a suite of available evidence-based treatment options for young children and their mothers or caregivers affected by violence.
Implications and recommendations for policymakers
CPP is an evidence-based treatment that is feasible to implement and is acceptable to families and services. The comprehensive CPP training package provides the skills and reflective supervision framework to equip therapists to respond to children and their mothers affected by IPV.
In Australia, many young children experiencing family violence miss out on essential mental health care. Women who have experienced IPV are also often overlooked and yet when they are their child’s primary caregiver, their relationship with their child is an essential resource for children’s recovery and resilience after trauma. Children often also need help in their relationships with their fathers (or other caregivers) who are co-parenting them after using IPV, however there are currently a lack of service parameters and policies in place to enable workforces to provide this care.
Governments need to invest in early childhood mental health and wellbeing service delivery and to expand a trauma- and violence-informed child mental health and wellbeing workforce. This should include the development of a practice guide or framework to support child victims of violence and their families to recovery. CPP training can provide the foundation for the development of this workforce development and practice framework. Future service design should emphasise assessment for therapeutic readiness, workforce supervisory structures and inter-sector collaboration between public mental health and family violence services, especially in rural areas, to ensure returns from investment in workforce training and treatment delivery are maximised.
Implications
- Very young children’s mental health and wellbeing can be particularly impacted by IPV trauma, alongside those of their affected mothers.
- The mental health care needs of very young children are often overlooked in Australian service systems, as are the needs of IPV-affected mother–child dyads.
- The way to restore young children’s mental health after IPV is within their safe relationships (and as a first step this is often, but not always, with their mother).
- CPP is an evidence-based model for this population that is acceptable and increasingly feasible across settings within Australia.
- The CPP model of care also provides the theory, skills training and reflective supervision framework to build and sustain a mental health and wellbeing workforce for young children and parents/caregivers impacted by IPV trauma.
Recommendations
- Promote equity of mental health service delivery for children across the age range, to ensure responsive care is available for all children from earliest life.
- Invest in and expand the trauma- and violence-informed child mental health workforce that is growing in Australia, based on the CPP training and workforce development model.
- Develop a national trauma- and violence-informed child mental health and wellbeing practice framework, to guide safe engagement for children within all important caregiving relationships after IPV. This should be inclusive of both victim and survivor, and perpetrator co-parents when safe, and across caregiver genders and sexualities.
Implications and guidance for practitioners and service providers
RECOVER has made considerable service impacts across several project sites that can guide future care. RECOVER has:
- reinforced the value of tailoring services for IPV-exposed mothers and very young children previously missing out on care and/or identified service gaps for this age group
- highlighted the need to identify safe windows of therapeutic readiness for change with families
- identified that rural therapists/managers with less experience need more support to implement CPP
- operationalised trauma history assessment for children and caregivers referred to the service to better inform and tailor treatment plans for children and families
- facilitated the introduction of family violence screening at triage and realisation that family violence is prevalent among the clinical population
- facilitated partnerships between child mental health and family violence services
- highlighted the need for and value of building a trauma- and violence-informed child mental health/therapeutic workforce
- facilitated the training of further cohorts of CPP-qualified clinicians who are in turn now offering CPP across Victoria and South Australia (to Aboriginal and Torres Strait Islander families, migrant and refugee families, and some parents – mothers, fathers, caregivers – who have used violence in their relationships), as well as delivering CPP via telehealth
- developed a national community of practice, practice activities and knowledge translation.
Future research
Further research is needed to identify the most effective treatments for women and children who have been impacted by IPV. This includes better understanding therapeutic readiness for violence-cyclical families to intervene with children in multiple caregiving relationships. In addition, studies in future could expand the range of caregiver and family participants to include diverse genders and sexualities.
RECOVER has outlined that CPP is feasible and acceptable to participants in this study. However, further research is required to assess intervention efficacy in an Australian context, with a larger sample and delivered by a now larger and more CPP-experienced Australian workforce.
Very little research is available on young children’s experiences of psychotherapeutic treatment (Pernebo & Almqvist, 2016) and the mechanisms for change. There is a need to explore children’s participation experiences of CPP, and to better understand how children influence their own treatment and recovery.
In metropolitan and rural Victoria and South Australia, teams are already beginning to expand CPP practice across perinatal child protection populations, culturally and linguistically diverse families and Aboriginal and Torres Strait Islander families, and via telehealth. It will be important to understand the experiences of these client populations, what adaptations therapists are making in partnership with these families, and whether these locally adapted models are effective.
Better understanding these elements will enable a more precise delivery of CPP to families that can most benefit and will maximise return on investment, ensuring that young children affected by trauma not only recover but also thrive.
References
Alto, M. E., Ross, A. J., Handley, E. D., Manly, J. T., Guild, D. J., Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2021). Longitudinal outcomes of child–parent psychotherapy: Response to commentaries. Research on Child and Adolescent Psychopathology. https://doi.org/10.1007/s10802-021-00801-4
Anderson, K., & van Ee, E. (2018). Mothers and children exposed to intimate partner violence: A review of treatment interventions. International Journal of Environmental Research & Public Health, 15(9), 07. https://doi.org/10.3390/ijerph15091955
Anis, L., Letourneau, N., Benzies, K., Ewashen, C., & Hart, M. J. (2020). Effect of the attachment and child health parent training program on parent–child interaction quality and child development. Canadian Journal of Nursing Research, 52(2), 157–168. https://doi.org/10.1177/0844562119899004
Austin, A. E., Shanaham, M. E., Barrios, Y. V., & Macy, R. J. (2019). A systematic review of interventions for women parenting in the context of intimate partner violence. Trauma Violence & Abuse, 20(4), 498–519. https://doi.org/10.1177/1524838017719233
Australian Bureau of Statistics. (2017). Personal Safety Survey, Australia (cat. no. 4906.0). ABS. https://www.abs.gov.au/ausstats/abs
Australian Institute of Health and Welfare. (2020). Australia’s children. AIHW. https://www.aihw.gov.au/reports/children-youth/australias-children
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story 2019 – In brief. AIHW. https://www.aihw.gov.au/getmedia/b0037b2d-a651-4abf-9f7b-00a85e3de528/aihw-fdv3-FDSV-in-Australia-2019.pdf.aspx?inline=true
Bancroft, L., Silverman, J. G., & Ritchie, D. (2012). The batterer as parent: Addressing the impact of domestic violence on family dynamics (2nd ed.). Sage.
Barlow, J., Bennett, C., Midgley, N., Larkin, S. K., & Wei, Y. (2015). Parent–infant psychotherapy for improving parental and infant mental health. Cochrane Database of Systematic Reviews, 1, CD010534. https://doi.org/10.1002/14651858.CD010534.pub2
Bernstein, R. E., Timmons, A. C., & Lieberman, A. F. (2019). Interpersonal Violence, maternal perception of infant emotion, and child-parent psychotherapy. Journal of Family Violence, 34(4), 309–320. https://doi.org/10.1007/s10896-019-00041-7
Berry, V., Wilkinson, K., Farr, N., & Stimson, A. (2019). Assessing the feasibility of a parent life coaching intervention to support parents and children who have experienced domestic violence and abuse. Journal of Family Violence, 34(6), 493–506. https://doi.org/10.1007/s10896-019-00042-6
Bidarra, Z. S., Lessard, G., & Dumont, A. (2016). Co-occurrence of intimate partner violence and child sexual abuse: Prevalence, risk factors and related issues. Child Abuse & Neglect, 55, 10–21. https://doi.org/10.1016/j.chiabu.2016.03.007
Bowen, D. J., Kreuter, M., Spring, B., Cofta-Woerpel, L., Linnan, L., Weiner, D., Bakken, S., Kaplan, C. P., Squiers, L., Fabrizio, C., & Fernandez, M. (2009). How we design feasibility studies. American Journal of Preventive Medicine, 36(5), 452–457. https://doi.org/https://doi.org/10.1016/j.amepre.2009.02.002
Broady, T. R., Gray, R., Gaffney, I., & Lewis, P. (2017). “I miss my little one a lot”: How father love motivates change in men who have used violence. Child Abuse Review, 26(5), 328–338. https://doi.org/10.1002/car.2381
Buchanan, F., & Humphreys, C. (2021). Coercive control during pregnancy, birthing and postpartum: Women’s experiences and perspectives on health practitioners’ responses. Journal of Family Violence, 36(3), 325–335. https://doi.org/10.1007/s10896-020-00161-5
Bunston, W. (2008). Baby lead the way: Mental health group work for infants, children and mothers affected by family violence. Journal of Family Studies, 14(2–3), 334–341. https://doi.org/10.5172/jfs.327.14.2-3.334
Bunston, W. (2013). “What about the fathers?” Bringing “Dads on Board” with their infants and toddlers following violence. Journal of Family Studies, 19(1), 70–79. https://doi.org/10.5172/jfs.2013.19.1.70
Bunston, W., Eyre, K., Carlsson, A., & Pringle, K. (2016). Evaluating relational repair work with infants and mothers impacted by family violence. Australian and New Zealand Journal of Criminology, 49(1), 113–133. https://doi.org/10.1177/0004865814559925
Bunston, W., Franich-Ray, C., & Tatlow, S. (2017). A diagnosis of denial: How mental health classification systems have struggled to recognise family violence as a serious risk factor in the development of mental health issues for infants, children, adolescents and adults. Brain Sciences, 7(10), 133. https://doi.org/10.3390/brainsci7100133
Bunston, W., Pavlidis, T., & Cartwright, P. (2016). Children, family violence and group work: Some do’s and don’ts in running therapeutic groups with children affected by family violence. Journal of Family Violence, 31(1), 85–94. https://doi.org/10.1007/s10896-015-9739-1
Campo, M. (2015). Children’s exposure to domestic and family violence: Key issues and responses. Journal of the Home Economics Institute of Australia, 22(3), 33. https://doi.org/10.13140/RG.2.1.1759.1121
Cater, Å., & Forssell, A. M. (2014). Descriptions of fathers’ care by children exposed to intimate partner violence (IPV) – Relative neglect and children’s needs. 19(2), 185–193. https://doi.org/10.1111/j.1365-2206.2012.00892.x
Carpenter, G. L., & Stacks, A. M. (2009). Developmental effects of exposure to intimate partner violence in early childhood: A review of the literature. Children and Youth Services Review, 31(8), 831–839. https://doi.org/10.1016/j.childyouth.2009.03.005
Cerulli, C., Cicchetti, D., Handley, E. D., Manly, J. T., Rogosch, F. A., & Toth, S. L. (2021). Transforming the paradigm of child welfare. Development and Psychopathology, 33(2), 377–393. https://doi.org/10.1017/S0954579420002138
Chan, Y.-C., & Yeung, J. W.-K. (2009). Children living with violence within the family and its sequel: A meta-analysis from 1995–2006. Aggression and Violent Behavior, 14(5), 313–322. https://doi.org/10.1016/j.avb.2009.04.001
Chang, J. C., Dado, D., Ashton, S., Hawker, L., Cluss, P. A., Buranosky, R., & Scholle, S. H. (2006). Understanding behavior change for women experiencing intimate partner violence: Mapping the ups and downs using the stages of change. Patient Education and Counseling, 62(3), 330–339. https://dx.doi.org/10.1016/j.pec.2006.06.009
Child–Parent Psychotherapy. (2018). Research fact sheet. https://childparentpsychotherapy.com/wp-content/uploads/2018/01/CPP-research-fact-sheet-Jan-2018.pdf
Chu, A. T., Ippen, C. G., & Lieberman, A. F. (2021). It’s all about the relationship: The role of attachment in child–parent psychotherapy. Research on Child and Adolescent Psychopathology, 49(5), 591–593. https://doi.org/10.1007/s10802-020-00741-5
Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2006). Fostering secure attachment in infants in maltreating families through preventive interventions. Development and Psychopathology, 18(03), 623-649. https://doi.org/10.1017/s0954579406060329
Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2000). The efficacy of toddler-parent psychotherapy for fostering cognitive development in offspring of depressed mothers. Journal of Abnormal Child Psychology, 28(2), 135–148. https://doi.org/10.1023/a:1005118713814
Cicchetti, D., Rogosch, F. A., Toth, S. L., & Sturge-Apple, M. L. (2011). Normalizing the development of cortisol regulation in maltreated infants through preventive interventions. Development and Psychopathology, 23(03), 789–800. https://doi.org/10.1017/S0954579411000307
Cicchetti, D., Toth, S. L., & Rogosch, F. A. (1999). The efficacy of toddler-parent psychotherapy to increase attachment security in offspring of depressed mothers. Attachment & Human Development, 1(1), 34–66. https://doi.org/10.1080/14616739900134021
Cohen, J. A., Mannarino, A. P., & Iyengar, S. (2011). Community treatment of posttraumatic stress disorder for children exposed to intimate partner violence: A randomized controlled trial. Archives of Pediatrics Adolescent Medicine, 165(1), 16–21. https://doi.org/10.1001/archpediatrics.2010.247
Conway, L. J., Cook, F., Cahir, P., Brown, S., Reilly, S., Gartland, D., Mensah, F., & Giallo, R. (2020). Children’s language abilities at age 10 and exposure to intimate partner violence in early childhood: Results of an Australian prospective pregnancy cohort study. Child Abuse & Neglect, 104794. https://doi.org/10.1016/j.chiabu.2020.104794
David, P., & Schiff, M. (2015). Learning from bottom-up dissemination: Importing an evidence-based trauma intervention for infants and young children to Israel. Evaluation and Program Planning, 53, 18–24. https://doi.org/10.1016/j.evalprogplan.2015.07.012
Despert, J. L. (1949) Therapeutic readiness in child psychiatry. Psychiatry, 12(2), 153–158. https://doi.org/10.1080/00332747.1949.11022728
Derogatis, L. R., & Unger, R. (2010). Symptom Checklist-90–Revised. In The Corsini Encyclopedia of Psychology. John Wiley & Sons, Inc. https://doi.org/10.1002/9780470479216.corpsy0970
Domoney, J., Fulton, E., Stanley, N., McIntyre, A., Heslin, M., Byford, S., Bick, D., Ramchandani, P., MacMillan, H., Howard, L. M., & Trevillion, K. (2019). For baby’s sake: Intervention development and evaluation design of a whole-family perinatal intervention to break the cycle of domestic abuse. Journal of Family Violence, 34(6), 539–551. https://doi.org/10.1007/s10896-019-00037-3
Dowling, D. (2019). An independent practitioner’s introduction to child and adolescent psychotherapy: Playing with ideas. Routledge.
Ebert, L., Amaya-Jackson, L., Markiewicz, J., & Fairbank, J. A. (2012). Development and application of the NCCTS learning collaborative model for the implementation of evidence-based child trauma treatment. In R. K. McHugh & D. H. Barlow (Eds.). Dissemination and implementation of evidence-based psychological interventions (pp. 97–123). Oxford University Press.
Erford, B., & Bardhoshi, G. (2018). Introduction to group work: Historical perspectives and functional group models. In B. Erford (Ed.). Group Work (pp. 35–64). Routledge.
Evans, S., Davies, C., & DiLillo, D. (2008). Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggression and Violent Behavior, 13(2), 131–140. https://doi.org/
Feinberg, M. E., Jones, D. E., Hostetler, M. L., Roettger, M. E., Paul, I. M., & Ehrenthal, D. B. (2016). Couple-focused prevention at the transition to parenthood, a randomized trial: Effects on coparenting, parenting, family violence, and parent and child adjustment. Prevention Science, 17(6), 751–764. https://doi.org/10.1007/s11121-016-0674-z
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Fitzpatrick, K. M., Brown, S., Hegarty, K., Mensah, F., & Gartland, D. (2020). Physical and emotional intimate partner violence and women’s health in the first year after childbirth: An Australian pregnancy cohort study. Journal of Interpersonal Violence, 088626052093442. https://doi.org/10.1177/0886260520934426
Foa, E. B., Riggs, D. S., Dancu, C. V., & Rothbaum, B. O. (1993). Reliability and validity of a brief instrument for assessing post‐traumatic stress disorder. Journal of Traumatic Stress, 6(4), 459–473. https://doi/10.1002/jts.2490060405
Foa, E., McLean, C., Zang, Y. , Zhong, J., Rauch, S., Porter, K., Knowles, K., Powers, M. & Kauffman, B. (2016). Psychometric properties of the posttraumatic stress disorder symptom scale interview for DSM-5 (PSSI-5). Psychological Assessment, 28(10), 1159–1165. https://doi.org/10.1037/pas0000259
Fogarty, A., Giallo, R., Wood, C., Kaufman, J., & Brown, S. (2019). Emotional-behavioral resilience and competence in preschool children exposed and not exposed to intimate partner violence in early life. International Journal of Behavioral Development, 44(2), 97–106. https://doi.org/10.1177/0165025419830241
Fogarty, A., Savopoulos, P., Seymour, M., Cox, A., Williams, K., Petrie, S., Herman, S., Toone, E., Schroeder, K., & Giallo, R. (2021). Providing therapeutic services to women and children who have experienced intimate partner violence during the COVID-19 pandemic: Challenges and learnings. Child Abuse & Neglect, 105365. https://doi.org/10.1016/j.chiabu.2021.105365
Fogarty, A., Treyvaud, K., Savopoulos, P., Jones, A., Cox, A., Toone, E., & Giallo, R. (2020). Facilitators to engagement in a mother–child therapeutic intervention following intimate partner violence. Journal of Interpersonal Violence, 0886260520926316. https://doi.org/10.1177/0886260520926316
Fogarty, A., Woolhouse, H., Giallo, R., Wood, C., Kaufman, J., & Brown, S. (2019). Promoting resilience and wellbeing in children exposed to intimate partner violence: A qualitative study with mothers. Child Abuse & Neglect, 95, 104039. https://doi.org/10.1016/j.chiabu.2019.104039
Ford-Gilboe, M., Wathen, C. N., Varcoe, C., MacMillan, H. L., Scott-Storey, K., Mantler, T., Hegarty, K., & Perrin, N. (2016). Development of a brief measure of intimate partner violence experiences: The Composite Abuse Scale (Revised) – Short Form (CASR-SF). BMJ Open, 6(12). https://doi.org/10.1136/bmjopen-2016-012824
Fraiberg, S., Adelson, E., & Shapiro, V. (1975). Ghosts in the nursery: A psychoanalytic approach to the problems of impaired infant-mother relationships. Journal of the American Academy of Child Psychiatry, 14(3), 387-421. https://doi.org/10.1016/S0002-7138(09)61442-4
Gartland, D., Conway, L. J., Giallo, R., Mensah, F. K., Cook, F., Hegarty, K., Herrman, H., Nicholson, J., Reilly, S., Hiscock, H., Sciberras, E., & Brown, S. J. (2021). Intimate partner violence and child outcomes at age 10: A pregnancy cohort. Archives of Disease in Childhood. https://doi.org/10.1136/archdischild-2020-320321
Ghosh Ippen, C., Chu, A., & Lieberman, A. F. (2020). CPP & Telehealth: What we know and how it guides us. CPP https://childparentpsychotherapy.com/wp-content/uploads/2020/03/CPP-and-Telehealth-module1.pdf
Ghosh Ippen, C., Harris, W. W., Van Horn, P., & Lieberman, A. F. (2011). Traumatic and stressful events in early childhood: Can treatment help those at highest risk? Child Abuse & Neglect, 35(7), 504–513. https://doi.org/http://dx.doi.org/10.1016/j.chiabu.2011.03.009
Giallo, R., Fogarty, A., Savopoulos, P., Cox, A., Toone, E., Williams, K., Jones, A. & Treyvaud, K. (2021). Capturing the experiences of clinicians implementing a new brief intervention for parents and children who have experienced family violence in Australia. Health & Social Care in the Community. https://doi.org/10.1111/hsc.13587
Gillies, D., Maiocchi, L., Bhandari, A. P., Taylor, F., Gray, C., & O’Brien, L. (2016). Psychological therapies for children and adolescents exposed to trauma. Cochrane Database of Systematic Reviews, 2016(10), Article Cd012371. https://doi.org/10.1002/14651858.CD012371
Goodman, R. (2001). Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337–1345. https://doi.org/10.1097/00004583-200111000-00015
Graham-Bermann, S. A. (2006). Early intervention for children exposed to domestic violence. Grant funded by Blue Cross and Blue Shield of Michigan Foundation.
Graham-Bermann, S. A., Howell, K. H., Lilly, M., & DeVoe, E. (2011). Mediators and moderators of change in adjustment following intervention for children exposed to intimate partner violence. Journal of Interpersonal Violence, 26(9), 1815–1833. https://doi.org/10.1177/0886260510372931
Graham-Bermann, S. A., Lynch, S., Banyard, V., DeVoe, E. R., & Halabu, H. (2007). Community-based intervention for children exposed to intimate partner violence: An efficacy trial. Journal of Consulting Clinical Psychology & Psychotherapy, 75(2), 199. https://doi.org/10.1037/0022-006X.75.2.199
Graham-Bermann, S. A., Miller-Graff, L. E., Howell, K. H., & Grogan-Kaylor, A. (2015). An efficacy trial of an intervention program for children exposed to intimate partner violence. Child Psychiatry & Human Development, 46(6), 928–939. https://doi.org/10.1007/s10578-015-0532-4
Grogan-Kaylor, A., Galano, M. M., Howell, K. H., Miller-Graff, L., & Graham-Bermann, S. A. (2019). Reductions in parental use of corporal punishment on pre-school children following participation in the Moms’ Empowerment Program. Journal of Interpersonal Violence, 34(8), 1563–1582. https://doi.org/10.1177/0886260516651627
Groves, B. M., Van Horn, P., & Lieberman, A. F. (2007). Deciding on fathers’ involvement in their children’s treatment after domestic violence. In J. L. Edleson & O. J. Williams, Parenting by men who batter: New directions for assessment and intervention (pp. 65–84). https://doi.org/10.1093/acprof:oso/9780195309034.001.0001
Guild, D. J., Alto, M. E., Handley, E. D., Rogosch, F., Cicchetti, D., & Toth, S. L. (2021). Attachment and affect between mothers with depression and their children: Longitudinal outcomes of child–parent psychotherapy. Research on Child and Adolescent Psychopathology, 49(5), 563–577. https://doi.org/10.1007/s10802-020-00681-0
Guy, S., Furber, G., Leach, M., & Segal, L. (2016). How many children in Australia are at risk of adult mental illness? Australian & New Zealand Journal of Psychiatry, 50(12), 1146–1160. https://doi.org/10.1177/0004867416640098
Hagan, M. J., Browne, D. T., Sulik, M., Ippen, C. G., Bush, N., & Lieberman, A. F. (2017). Parent and child trauma symptoms during child–parent psychotherapy: A prospective cohort study of dyadic change. Journal of Traumatic Stress, 30(6), 690–697. https://doi.org/10.1002/jts.22240
Herschell, A., Scudder, A., Schaffner, K., & Slagel, L. (2017). Feasibility and effectiveness of parent–child interaction therapy with victims of domestic violence: A pilot study. Journal of Child & Family Studies, 26(1), 271–283. https://doi.org/10.1007/s10826-016-0546-y
Hoffman, K. T., Marvin, R. S., Cooper, G., & Powell, B. (2006). Changing toddlers’ and preschoolers’ attachment classifications: The Circle of Security intervention. Journal of Consulting Clinical Psychology & Psychotherapy, 74(6), 1017. https://doi.org/10.1037/0022-006X.74.6.1017
Holt, S., Buckley, H., & Whelan, S. (2008). The impact of exposure to domestic violence on children and young people: A review of the literature. Child Abuse & Neglect, 32(8), 797–810. https://doi.org/10.1016/j.chiabu.2008.02.004
Hooker, L., Kaspiew, R., & Taft, A. (2016). Domestic and family violence and parenting: Mixed method insights into impact and support needs: State of knowledge paper (ANROWS Landscapes 01/16). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/L1.16_1.8-Parenting-2.pdf
Hooker, L., Samaraweera, N., Agius, P., & Taft, A. (2016). Intimate partner violence and the experience of motherhood: A cross-sectional analysis of factors associated with a poor experience of motherhood. Midwifery, 34, 88–94. https://doi.org/10.1016/j.midw.2015.12.011
Hooker, L., & Taft, A. (2016). Using theory to design, implement and evaluate sustained nurse domestic violence screening and supportive care. Journal of Research in Nursing, 21(5–6), 432–442. https://doi.org/10.1177/1744987116649633
Hooker, L., & Taft, A. J. (2019). Incorporating intimate partner violence interventions in nurse home visitation programs. Journal of the American Medical Association, 322(11), 1103. https://doi.org/10.1001/jama.2019.10598
Hooker, L., Toone, E., Raykar, V., Humphreys, C., Westrupp, E., Morris, A., & Taft, A. (2019). Reconnecting mothers and children after violence (RECOVER): The Australian Child–Parent Psychotherapy feasibility project – Study protocol. BMJ Open, 9:e023653. https://doi.org/10.1136/bmjopen-2018-023653
Howarth, E., Moore, T. H., Shaw, A. R., Welton, N. J., Feder, G. S., Hester, M., MacMillan, H. L., & Stanley, N. (2015). The effectiveness of targeted interventions for children exposed to domestic violence: Measuring success in ways that matter to children, parents and professionals. Child Abuse Review, 24(4), 297–310. https://doi.org/10.1002/car.2408
Howarth, E., Moore, T. H. M., Stanley, N., MacMillan, H. L., Feder, G., & Shaw, A. (2018). Towards an ecological understanding of readiness to engage with interventions for children exposed to domestic violence and abuse: Systematic review and qualitative synthesis of perspectives of children, parents and practitioners. Health & Social Care in the Community. https://doi.org/10.1111/hsc.12587
Howarth, E., Moore, T. H., Welton, N. J., Lewis, N., Stanley, N., MacMillan, H., Shaw, A., Hester, M., Bryden, P., & Feder, G. (2016). IMPRoving Outcomes for children exposed to domestic ViolencE (IMPROVE): An evidence synthesis. Public Health Research, 4(10), 1–342. https://doi.org/10.3310/phr04100
Howarth, E., Powell, C., Woodman, J., Walker, E., Chesters, H., Szilassy, E., Gilber, R. & Feder, G. (2021). Protocol for developing core outcome sets for evaluation of psychosocial interventions for children and families with experience or at risk of child maltreatment or domestic abuse. BMJ Open, 11(8): 044431. https://doi.org/10.1136/bmjopen-2020-044431
Howell, K. H. (2011). Resilience and psychopathology in children exposed to family violence. Aggression and Violent Behavior, 16(6), 562–569. https://doi.org/10.1016/j.avb.2011.09.001
Howell, K. H., Miller-Graff, L. E., Hasselle, A. J., & Scrafford, K. E. (2017). The unique needs of pregnant, violence-exposed women: A systematic review of current interventions and directions for translational research. Aggression & Violent Behavior, 34, 128–138. https://doi.org/10.1016/j.avb.2017.01.021
Howell, K. H., Miller, L. E., Lilly, M. M., Burlaka, V., Grogan-Kaylor, A. C., & Graham-Bermann, S. A. (2015). Strengthening positive parenting through intervention: Evaluating the Moms’ Empowerment Program for women experiencing intimate partner violence. Journal of Interpersonal Violence, 30(2), 232–252. https://doi.org/10.1177/0886260514533155
Humphreys, C., Diemer, K., Bornemisza, A., Spiteri-Staines, A., Kaspiew, R., & Horsfall, B. (2018). More present than absent: Men who use domestic violence and their fathering. Child & Family Social Work, 0(0). https://doi.org/10.1111/cfs.12617
Humphreys, C. (2011). Rebuilding together: Strengthening the mother–child bond in the aftermath of violence. DVRCV Quarterly, 3, 6.
Humphreys, C., Thiara, R. K., & Skamballis, A. (2011). Readiness to change: Mother–child relationship and domestic violence intervention. British Journal of Social Work, 41(1), 166–184. https://doi.org/10.1093/bjsw/bcq046
Humphreys, C., Mullender, A., Thiara, R., & Skamballis, A. (2006). “Talking to my mum”: Developing communication between mothers and children in the aftermath of domestic violence. Journal of Social Work, 6(1), 53–63. https://doi.org/10.1177/1468017306062223
Isobe, J., Healey, L., & Humphreys, C. (2020). A critical interpretive synthesis of the intersection of domestic violence with parental issues of mental health and substance misuse. Health and Social Care in the Community, 28(5), 1394–1407. https://doi.org/10.1111/hsc.12978
Iwaoka-Scott, A. Y., & Lieberman, A. F. (2015). Moving from dyads to triads: Implementation of child–parent psychotherapy with fathers. Zero to Three, 35(5), 18–24.
Jack, S. M., Boyle, M., McKee, C., Ford-Gilboe, M., Wathen, C., Scribano, P., Davidov, D., McNaughton, D., O’Brien, R., Johnston, C., Gasbarro, M., Tanaka, M., Kimber, M., Coben, J., Olds, D. L., & MacMillan, H. L. (2019). Effect of addition of an intimate partner violence intervention to a nurse home visitation program on maternal quality of life: A randomized clinical trial. Journal of the American Medical Association, 321(16), 1576–1585. https://doi.org/10.1001/jama.2019.3211
James-Hanman, D., & Holt, S. (2021). Post-separation contact and domestic violence: Our 7-point plan for safe[r] contact for children. Journal of Family Violence. https://doi.org/10.1007/s10896-021-00256-7
Jones, S., & Bunston, W. (2012). The “original couple”: Enabling mothers and infants to think about what destroys as well as engenders love, when there has been intimate partner violence. Couple and Family Psychoanalysis, 2(2), 215–232. https://doi.org/10.33212/cfp.v2n2.2012.215
Jouriles, E. N., McDonald, R., Rosenfield, D., Stephens, N., Corbitt-Shindler, D., & Miller, P. C. (2009). Reducing conduct problems among children exposed to intimate partner violence: A randomized clinical trial examining effects of Project Support. Journal of Consulting Clinical Psychology & Psychotherapy, 77(4), 705. https://doi.org/10.1037/a0015994
Kamal, L., Strand, J., Jutengren, G., & Tidefors, I. (2017). Perceptions and experiences of an attachment-based intervention for parents troubled by intimate partner violence. Clinical Social Work Journal, 45(4), 311–319. https://doi.org/10.1007/s10615-016-0606-1
Katz, E. (2019). Coercive control, domestic violence, and a five-factor framework: Five factors that influence closeness, distance, and strain in mother–child relationships. Violence Against Women, 1077801218824998. https://doi.org/10.1177/1077801218824998
Keeshin, B. R., Oxman, A., Schindler, S., & Campbell, K. A. (2015). A domestic violence shelter parent training program for mothers with young children. Journal of Family Violence, 30(4), 461–466. https://doi.org/10.1007/s10896-015-9698-6
Kitzmann, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witnesses to domestic violence: a meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339. https://doi.org/10.1037/0022-006X.71.2.339
Kong, T. (2021) From frontline assessment to reunification: The integration of CPP into a hospital-based child protection service [Symposium Session]. World Association for Infant Mental Health World Congress, Brisbane & online, Australia.
Labarre, M., Bourassa, C., Holden, G. W., Turcotte, P., & Letourneau, N. (2016). Intervening with fathers in the context of intimate partner violence: An analysis of ten programs and suggestions for a research agenda. Journal of Child Custody, 13(1), 1–29. https://doi.org/10.1080/15379418.2016.1127793
Lamb, K., Humphreys, C., & Hegarty, K. (2018). “Your behaviour has consequences”: Children and young people’s perspectives on reparation with their fathers after domestic violence. Children and Youth Services Review, 88, 164–169. https://doi.org/10.1016/j.childyouth.2018.03.013
Lanier, P., Kohl, P. L., Benz, J., Swinger, D., Moussette, P., & Drake, B. (2011). Parent–child interaction therapy in a community setting: Examining outcomes, attrition, and treatment setting. Research on Social Work Practice, 21(6), 689–698. https://doi.org/10.1177/1049731511406551
Larrieu, J. A. (2018). Introducing evidence-based trauma treatment in preventive services: Child–Parent Psychotherapy. In V. Strand & G. Sprang (Eds.), Trauma responsive child welfare systems (pp. 147–164). Springer, Cham. https://doi.org/10.1007/978-3-319-64602-2_9
Latzman, N. E., Casanueva, C., Brinton, J., & Forman-Hoffman, V. L. (2019). The promotion of well-being among children exposed to intimate partner violence: A systematic review of interventions. Campbell Systematic Reviews, 15(e1049). https://doi.org/10.1002/cl2.1049
Lavi, I., Gard, A. M., Hagan, M., Van Horn, P., & Lieberman, A. F. (2015). Child–parent psychotherapy examined in a perinatal sample: Depression, posttraumatic stress symptoms and child-rearing attitudes. Journal of Social and Clinical Psychology, 34(1), 64–82. https://doi.org/10.1521/jscp.2015.34.1.64
Letourneau, N., Anis, L., Ntanda, H., Novick, J., Steele, M., Steele, H., & Hart, M. (2020). Attachment & Child Health (ATTACH) pilot trials: Effect of parental reflective function intervention for families affected by toxic stress. Infant Mental Health Journal. https://doi.org/10.1002/imhj.21833
Levendosky, A. A., Lannert, B., & Yalch, M. (2012). The effects of intimate partner violence on women and child survivors: An attachment perspective. Psychodyn Psychiatry, 40(3), 397–434. https://doi.org/10.1521/pdps.2012.40.3.397
Lieberman, A. F. (2004). Child–parent psychotherapy: A relationship-based approach to the treatment of mental health disorders in infancy and early childhood. In A. J. Sameroff, S. C. McDonough, & K. L. Rosenblum (Eds.), Treating parent–infant relationship problems: Strategies for intervention (pp. 97–122). Guilford Press.
Lieberman, A., Van Horn, P., & Ghosh Ippen, C. (2005). Toward evidence-based treatment: Child–parent psychotherapy with preschoolers exposed to marital violence. Journal of the American Academy of Child & Adolescent psychiatry, 44(12), 1241–1248. https://dx.doi.org/10.1097/01.chi.0000181047.59702.58
Lieberman, A., Chu, A., Van Horn, P., & Harris, W. (2011). Trauma in early childhood: Empirical evidence and clinical implications. Development and Psychopathology, 23(2), 397-410. https://doi.org/10.1017/S0954579411000137
Lieberman, A. F., Diaz, M. A., & Van Horn, P. (2011). Perinatal child–parent psychotherapy: Adaptation of an evidence-based treatment for pregnant women and babies exposed to intimate partner violence. In S. A. Graham & B. A. Levendosky (Eds.), How intimate partner violence affects children: Developmental research, case studies, and evidence-based intervention (pp. 47–66). American Psychological Association. https://doi.org/10.1037/12322-003
Lieberman, A. F., Diaz, M. A., Castro, G., & Bucio, G. O. (2020). Make room for baby: Perinatal child-parent psychotherapy to repair trauma and promote attachment. Guilford Publications.
Lieberman, A. F., Ghosh Ippen, C., & Hernandez Dimmler, M. (2019). Child–parent psychotherapy. Assessing and treating youth exposed to traumatic stress. In C. H. Zeanah (Ed.), Handbook of Infant Mental Health, Fourth Edition (pp. 485-499). Guilford Press.
Lieberman, A. F., Ghosh Ippen, C., & Van Horn, P. (2006). Child–parent psychotherapy: 6-month follow-up of a randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 45(8), 913–918. https://doi.org/10.1097/01.chi.0000222784.03735.92
Lieberman, A. F., Ghosh Ippen, C., & Van Horn, P. (2015). Don’t hit my mommy!: A manual for child–parent psychotherapy with young children exposed to violence and other trauma. ZERO TO THREE.
Lieberman, A. F., Padrón, E., Van Horn, P., Harris, W. W., Drell, M. J., Osofsky, J. D., Zuckerman, B., & Zuckerman, P. (2005). Angels in the nursery: The intergenerational transmission of benevolent parental influences [Commentary]. Infant Mental Health Journal, 26(6), 504–520. https://doi.org10.1002/imhj.20071
Luyten, P., Mayes, L., Sadler, L., Fonagy, P., Nicholls, S., Crowley, M., Vesper, A., Mobley, A., Stewart, T., & Close, N. (2009). The Parental Reflective Functioning Questionnaire-1 (PRFQ-1) [Unpublished manual]. University of Leuven, Belgium.
Lyons-Ruth, K., Todd Manly, J., Von Klitzing, K., Tamminen, T., Emde, R., Fitzgerald, H., Paul, C., Keren, M., Berg, A., Foley, M., & Watanabe, H. (2017). The worldwide burden of infant mental and emotional disorder: Report of the task force of the world association for infant mental health. Infant Mental Health Journal, 38(6), 695–705. https://doi.org/10.1002/imhj.21674
Marie-Mitchell, A., & Kostolansky, R. (2019). A systematic review of trials to improve child outcomes associated with adverse childhood experiences. American Journal of Preventive Medicine, 56(5), 756–764. https://doi.org/10.1016/j.amepre.2018.11.030
Marsden, S., Humphreys, C., & Hegarty, K. (2020). Women survivors’ accounts of seeing psychologists: Harm or benefit? Journal of Gender-Based Violence. https://doi.org/10.1332/239868020X16040863370635
Matias, C., Scott, S., & O’Connor, T. (2006). Coding of attachment-related parenting (CARP). Institute of Psychiatry, Kings College.
May, C., & Finch, T. (2009). Implementing, embedding, and integrating practices: An outline of Normalization Process Theory. Sociology, 43(3), 535–554. https://doi.org/10.1177/0038038509103208
May, C. R., Cummings, A., Girling, M., Bracher, M., Mair, F. S., May, C. M., Murray, E., Myall, M., Rapley, T., & Finch, T. (2018). Using Normalization Process Theory in feasibility studies and process evaluations of complex healthcare interventions: A systematic review. Implementation Science, 13(1), 80. https://doi.org/10.1186/s13012-018-0758-1
McLean, S. A, & McIntosh, J. E. (2021). The mental and physical health of family mental health practitioners during COVID-19: Relationships with family violence and workplace practices. Australian Journal of Psychology, 1–10. https://doi.org/10.1080/00049530.2021.1934118
McConnell, N., Barnard, M., & Taylor, J. (2017). Caring Dads Safer Children: Families’ perspectives on an intervention for maltreating fathers. Psychology of Violence, 7(3), 406–416. https://doi.org/10.1037/vio0000105
McFarlane, J., Symes, L., Binder, B. K., Maddoux, J., & Paulson, R. (2014). Maternal–child dyads of functioning: The intergenerational impact of violence against women on children. Maternal Child Health Journal, 18(9), 2236–2243. https://doi.org/10.1007/s10995-014-1473-4
McGorry, P. D. (2021). The reality of mental health care for young people, and the urgent need for solutions. Medical Journal of Australia. https://doi.org/10.5694/mja2.51327
Miller-Graff, L. E., Galano, M., & Graham-Bermann, S. (2016). Expression of re-experiencing symptoms in the therapeutic context: A mixed-method analysis of young children exposed to intimate partner violence. Child Care in Practice, 22(1), 1–2. https://doi.org/10.1080/13575279.2015.1064360
Mohaupt, H., Duckert, F., & Askeland, I. R. (2020). How do men in treatment for intimate partner violence experience parenting their young child? A descriptive phenomenological analysis. Journal of Family Violence, 35(8), 863–875. https://doi.org/10.1007/s10896-019-00083-x
Morales, Y., Lutzker, J. R., Shanley, J. R., & Guastaferro, K. M. (2015). Parent–infant interaction training with a Latino mother. International Journal of Child Health and Human Development, 8(2), 135–145.
Morris, A., Humphreys, C., & Hegarty, K. (2015). Children’s views of safety and adversity when living with domestic violence. In N. Stanley & C. Humphreys (Eds.), Domestic violence and protecting children: New thinking and approaches (pp. 18–33). Jessica Kingsley Publishers.
Mountain, G., Cahill, J., & Thorpe, H. (2017). Sensitivity and attachment interventions in early childhood: A systematic review and meta-analysis. Infant Behavior and Development, 46, 14–32. https://doi.org/10.1016/j.infbeh.2016.10.006
Narayan, A. J., Atzl, V. M., Merrick, J. S., Harris, W. W., & Lieberman, A. F. (2020). Developmental origins of ghosts and angels in the nursery: Adverse and benevolent childhood experiences. Adversity and Resilience Science, 1(2), 121–134. https://doi.org/10.1007/s42844-020-00008-4
Nardone, G., & Salvini, A. (2019). International dictionary of psychotherapy. Routledge.
National Scientific Council on the Developing Child. (2010). Persistent fear and anxiety can affect young children’s learning and development: Working paper 13. https://developingchild.harvard.edu/wp-content/uploads/2010/05/Persistent-Fear-and-Anxiety-Can-Affect-Young-Childrens-Learning-and-Development.pdf
Norlén, A., Thorén, A., & Almqvist, K. (2021). Implementing child–parent psychotherapy (CPP) in Sweden: A qualitative study exploring experiences by caregivers taking part of the intervention with their child. Journal of Infant, Child, and Adolescent Psychotherapy, 1–17. https://doi.org/10.1080/15289168.2021.1925001
Olsen, L. R., Mortensen, E. L., & Bech, P. (2006). Mental distress in the Danish general population. Acta Psychiatrica Scandinavica, 113(6), 477–484. https://doi.org/10.1111/j.1600-0447.2005.00743.x
Orr, C., Fisher, C. M., Preen, D. B., Glauert, R. A., & O’Donnell, M. (2020). Exposure to family and domestic violence is associated with increased childhood hospitalisations. PLOS ONE, 15(8), e0237251. https://doi.org/10.1371/journal.pone.0237251
Overbeek, M., Koren-Karie, N., Ben-Haim, A., De Schipper, J., Dreier Gligoor, P., & Schuengel, C. (2019). Trauma exposure in relation to the content of mother–child emotional conversations and quality of interaction. International Journal of Environmental Research and Public Health, 16(5), 805. https://doi.org/10.3390/ijerph16050805
Pernebo, K., & Almqvist, K. (2016). Young children’s experiences of participating in group treatment for children exposed to intimate partner violence: A qualitative study. Clinical Child Psychology and Psychiatry, 21(1), 119–132. https://doi.org/10.1177/1359104514558432
Pernebo, K., Fridell, M., & Almqvist, K. (2018). Outcomes of psychotherapeutic and psychoeducative group interventions for children exposed to intimate partner violence. Child Abuse & Neglect, 79, 213–223. https://doi.org/10.1016/j.chiabu.2018.02.014
Pernebo, K., Fridell, M., & Almqvist, K. (2019). Reduced psychiatric symptoms at 6 and 12 months’ follow-up of psychotherapeutic and psychoeducative group interventions for children exposed to intimate partner violence. Child Abuse & Neglect, 93, 228–238. https://doi.org/0.1016/j.chiabu.2019.05.002
Pfitzner, N., Fitz-Gibbon, K., & True, J. (2020). Responding to the “shadow pandemic”: Practitioner views on the nature of and responses to violence against women in Victoria, Australia during the COVID-19 restrictions. Monash Gender and Family Violence Prevention Centre. https://apo.org.au/node/306064
Productivity Commission. (2020). Mental health inquiry report (95). Canberra.
QSR International. (2018). NVivo qualitative data analysis software. Version 12. https://www.qsrinternational.com/
Raykar, V., Lawless, K, & Ryan, N. (2021). CPP in a rural CAMHS context [Symposium Session]. World Association for Infant Mental Health World Congress, Brisbane & online, Australia.
Rizo, C. F., Wretman, C. J., Macy, R. J., Guo, S., & Ermentrout, D. M. (2018). A novel intervention for system-involved female intimate partner violence survivors: Changes in mental health. American journal of Orthopsychiatry, 88(6), 681–690. https://doi.org/10.1037/ort0000332
Roopnarine, J. L., & Dede Yildirim, E. (2018). Influence of relationship skills education on pathways of associations between paternal depressive symptoms and IPV and childhood behaviors. Psychology of Men & Masculinity, 19(2), 223–233. https://doi.org/10.1037/men0000100
Satyanarayana, V. A., Nattala, P., Selvam, S., Pradeep, J., Hebbani, S., Hegde, S., & Srinivasan, K. (2016). Integrated cognitive behavioral intervention reduces intimate partner violence among alcohol dependent men, and improves mental health outcomes in their spouses: A clinic based randomized controlled trial from South India. Journal of Substance Abuse Treatment, 64, 29–34. https://doi.org/10.1016/j.jsat.2016.02.005
Schechter, D. S., Moser, D. A., Reliford, A., McCaw, J. E., Coates, S. W., Turner, J., Serpa, S. R., & Willheim, E. (2015). Negative and distorted attributions towards child, self, and primary attachment figure among posttraumatically stressed mothers: What changes with Clinician Assisted Videofeedback Exposure Sessions (CAVES). Child Psychiatry and Human Development, 46(1), 10–20. https://doi.org/10.1007/s10578-014-0447-5
Scheeringa, M. S., & Haslett, N. (2010). The reliability and criterion validity of the diagnostic infant and preschool assessment: A new diagnostic instrument for young children. Child Psychiatry & Human Development, 41(3), 299–312. https://doi.org/10.1007/s10578-009-0169-2
Scott, K. (2017). Cluster RCT of embedded parenting intervention to prevent recurrence and reduce impairment in young children exposed to domestic violence. ClinicalTrials.gov. https://clinicaltrials.gov/show/nct03198429
Segal, L., Guy, S., & Furber, G. (2018). What is the current level of mental health service delivery and expenditure on infants, children, adolescents, and young people in Australia? Australian & New Zealand Journal of Psychiatry, 52(2), 163–172. https://doi.org/10.1177/0004867417717796
Shafi, R., Bieber, E. D., Shekunov, J., Croarkin, P. E., & Romanowicz, M. (2019). Evidence based dyadic therapies for 0-to 5-year-old children with emotional and behavioral difficulties. Frontiers in Psychiatry, 10, 677. https://doi.org/10.3389/fpsyt.2019.00877
Smith, E. (2016). Domestic abuse, recovering together (DART): Evaluation report. NSPCC. https://library.nspcc.org.uk/HeritageScripts/Hapi.dll/search2?searchTerm0=C6566
Sousa, C. A., Siddiqi, M., & Bogue, B. (2021). What do we know after decades of research about parenting and IPV? A systematic scoping review integrating findings. Trauma, Violence, & Abuse, 152483802110160. https://doi.org/10.1177/15248380211016019
Southwell, J. (2016). Using “expressive therapies” to treat developmental trauma and attachment problems in preschool-aged children. Children Australia, 41(2), 114–125. https://doi.org/10.1017/cha.2016.7
Spangaro, J. (2017). What is the role of health systems in responding to domestic violence? An evidence review. Australian Health Review, 41(6), 639–645. https://doi.org/10.1071/AH16155
Stanley, N., Graham-Kevan, N., & Borthwick, R. (2012). Fathers and domestic violence: Building motivation for change through perpetrator programmes. Child Abuse Review, 21(4), 264–274. https://doi.org/10.1002/car.2222
State of Victoria. (2016). Royal Commission into Family Violence: Summary and recommendations. Victorian Government Printer. https://files.rcfv.com.au/Reports/RCFV_Full_Report_Interactive.pdf
State of Victoria. (2019). Victorian Government submission to the Royal Commission into Victoria’s Mental Health System. https://www2.health.vic.gov.au/mental-health/priorities-and-transformation/royal-commission
State of Victoria. (2021). Royal Commission into Victoria’s Mental Health System: Final Report. https://finalreport.rcvmhs.vic.gov.au/download-report/
Steele, H., Murphy, A., Bonuck, K., Meissner, P., & Steele, M. (2019). Randomized control trial report on the effectiveness of Group Attachment-Based Intervention (GABI©): Improvements in the parent–child relationship not seen in the control group. Development & Psychopathology, 31(1), 203–217. https://doi.org/10.1017/S0954579418001621
Stover, C. S., & Lent, K. (2014). Training and certification for domestic violence service providers: The need for a national standard curriculum and training approach. Psychology of Violence, 4(2), 117–127. https://doi.org/10.1037/a0036022
Stover, C. S. (2015). Fathers for Change for substance use and intimate partner violence: Initial community pilot. Family Process, 54(4), 600–609. https://doi.org/10.1111/famp.12136
Stover, C. S., Carlson, M., & Patel, S. (2017). Integrating intimate partner violence and parenting intervention into residential substance use disorder treatment for fathers. Journal of Substance Abuse Treatment, 81, 35–43. https://doi.org/10.1016/j.jsat.2017.07.013
Stover, C. S., Beebe, R., Clough, M., DiVietro, S., Madigan, L., & Grasso, D. J. (2020). Evaluation of a statewide implementation of Fathers for Change: A fathering intervention for families impacted by partner violence. Journal of Family Violence. https://doi.org/10.1007/s10896-020-00199-5
Stronach, E. P., Toth, S. L., Rogosch, F., & Cicchetti, D. (2013). Preventive interventions and sustained attachment security in maltreated children. Development and Psychopathology, 25(4pt1), 919–930. https://doi.org/10.1017/s0954579413000278
Toth, S. L., Maughan, A., Manly, J. T., Spagnola, M., & Cicchetti, D. (2002). The relative efficacy of two interventions in altering maltreated preschool children’s representational models: Implications for attachment theory. Development and Psychopathology, 14(04), 877–908. https://doi.org/10.1017.S095457940200411X
Toth, S. L., Rogosch, F. A., Manly, J. T., & Cicchetti, D. (2006). The efficacy of toddler–parent psychotherapy to reorganize attachment in the young offspring of mothers with major depressive disorder: A randomized preventive trial. Journal of Consulting and Clinical Psychology, 74(6), 1006–1016. https://doi.org/10.1037/0022-006X.74.6.1006
Toone, E. (2015). Appendix 1: Supplementary submission: Therapeutic responses for infants and children at escalating risk of family violence. In S. Keebaugh, J. Pocock & A. Jones(Eds.), No Place for Violence: Berry Street Submission to the Victorian Royal Commission into Family Violence (pp. 53–65). Royal Commission into Family Violence.
Toone, E. (2018). Safe with Dad. Berry Street. https://learning.berrystreet.org.au/sites/default/files/2019-02/Safe-with-dad_0.pdf
Toone, E., Hermans, D., & Hooker, L. (2021, 26–28 May). Safe connection after violent storms and togetherness droughts: Child-Parent Psychotherapy learning after family violence [Conference presentation]. Safe and Together Asia Pacific Conference, Melbourne & Online, Australia.
Trevillion, K., Oram, S., Feder, G., & Howard, L. M. (2012). Experiences of domestic violence and mental disorders: A systematic review and meta-analysis. PLOS ONE, 7(12), e51740. https://doi.org/10.1371/journal.pone.0051740
UN Women. (2020). Violence against women and girls: The shadow pandemic. https://www.unwomen.org/en/news/stories/2020/4/statement-ed-phumzile-violence-against-women-during-pandemic
Valentino. (2017). Relational interventions for maltreated children. Child Development, 88(2), 359–367. https://doi.org/10.1111/cdev.12735
Veritas Health Innovation. Covidence systematic review software. www.covidence.org
Victorian Government Department of Families, Fairness and Housing (2018). What is family violence? https://services.dffh.vic.gov.au/what-family-violence
Visser, M. M., Telman, M. D., de Schipper, J. C., Lamers-Winkelman, F., Schuengel, C., & Finkenauer, C. (2015). The effects of parental components in a trauma-focused cognitive behavioral based therapy for children exposed to interparental violence: Study protocol for a randomized controlled trial. BMC Psychiatry, 15, 131. https://doi.org/10.1186/s12888-015-0533-7
Vu, N. L., Jouriles, E. N., McDonald, R., & Rosenfield, D. (2016). Children’s exposure to intimate partner violence: A meta-analysis of longitudinal associations with child adjustment problems. Clinical Psychology Review, 46, 25–33. https://doi.org/https://doi.org/10.1016/j.cpr.2016.04.003
Waldman-Levi, A., & Weintraub, N. (2015). Efficacy of a crisis intervention in improving mother–child interaction and children’s play functioning. American Journal of Occupational Therapy, 69(1), 1–11. https://doi.org/10.5014/ajot.2015.013375
Waters, S. F., Hagan, M. J., Rivera, L., & Lieberman, A. F. (2015). Improvements in the child-rearing attitudes of Latina mothers exposed to interpersonal trauma predict greater maternal sensitivity toward their 6-month-old infants. Journal of Traumatic Stress, 28(5), 426–433. https://doi.org/10.1002/jts.22043
Wathen, C. N., Schmitt, B., & MacGregor, J. C. D. (2021). Measuring trauma- (and violence-) informed care: A scoping review. Trauma, Violence, & Abuse, 15248380211029399. https://doi.org/10.1177/15248380211029399
Weissman, M. M., Pilowsky, D. J., Wickramaratne, P. J., Talati, A., Wisniewski, S. R., Fava, M., Hughes, C. W., Garber, J., Malloy, E., King, C. A., Cerda, G., Sood, A. B., Alpert, J. E., Trivedi, M. H., & Rush, A. J. (2006). Remissions in maternal depression and child psychopathology: A STAR*D–Child Report. Journal of the American Medical Association, 295(12), 1389–1398. https://doi.org/10.1001/jama.295.12.1389
Westrupp, E., Rose, N., Nicholson, J., & Brown, S. (2015). Exposure to inter-parental conflict across 10 years of childhood: Data from the longitudinal study of Australian children. Maternal and Child Health Journal, 19(9), 1966–1973. https://doi.org/10.1007/s10995-015-1704-3
World Health Organization. (2013a). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non partner sexual violence. https://apps.who.int/iris/bitstream/10665/85239/1/9789241564625_eng.pdf
World Health Organization. (2013b). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf
World Health Organization. (2016). Ethical and safety recommendations for intervention research on violence against women: Building on lessons from the WHO publication Putting women first: Ethical and safety recommendations for intervention research on violence against women. https://apps.who.int/iris/bitstream/handle/10665/251759/9789241510189-engpdf;jsessionid=C50D3F751F53D3BADBD07BEFE6A9500B?sequence=1
World Health Organization. (2021). Violence against women prevalence estimates, 2018. Global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. https://www.who.int/publications/i/item/violence-against-women-prevalence-estimates
Zubrick, S. R., Lucas, N., Westrupp, E. M., & Nicholson, J. M. (2014). Parenting measures in the Longitudinal Study of Australian Children: Construct validity and measurement quality, Waves 1 to 4. Growing Up in Australia. https://www.growingupinaustralia.gov.au/pubs/technical/tp12.pdf
APPENDIX A:
Keyword search terms and grey
literature sites searched
| Concept 1: | Concept 2: | Concept 3: | Concept 4: |
|---|---|---|---|
|
|
|
|
APPENDIX B:
Ovid MEDLINE search strategy
- exp domestic violence/ or exp gender-based violence/ or exp intimate partner violence/
- exp Exposure to Violence/
- exp Family Conflict/
- domestic violence or intimate partner violence or domestic assault or domestic abuse).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating subheading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- batter*.mp.
- exposure to violence.mp.
- inter-parental conflict.mp.
- family conflict.mp.
- relational aggression.mp.
- 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9
- exp parent–child relations/ or exp father–child relations/ or exp mother–child relations/
- exp Child Development/
- (mother–child or father–child or parent–child or child–parent).mp.
- (attachment and (child* or infant*)).mp.
- (bond* and (child* or infant*)).mp.
- mental health.mp. and (*child/or infant*.mp.)
- (mental health and (maternal or paternal or parent)).mp.
- 11 or 12 or 13 or 14 or 15 or 16 or 17
- exp play therapy/ or exp psychotherapy, group/ or exp family therapy/
- exp Psychoanalytic Therapy/
- (therapy or treatment or intervention or counselling or counseling).mp.
- (group work or group psychotherapy or family therapy).mp.
- dyadic.mp.
- 19 or 20 or 21 or 22 or 23
- 10 and 18 and 24
- limit 25 to (humans and yr=“2015 -Current”)
APPENDIX C:
Grey literature search: Relevant websites
National
- Australian Institute of Family Studies https://www.aifs.gov.au/
- Australian Institute of Health and Welfare https://www.aihw.gov.au/
- Australia’s National Research Organisation for Women’s Safety https://www.anrows.org.au/
- Australian Government Department of Health https://www.health.gov.au/
- Australian Government Department of Social Services https://www.dss.gov.au/
International
- Blue Prints for Healthy Youth Development, USA https://www.blueprintsprograms.org/
- Centers for Disease Control and Prevention https://www.cdc.gov/ViolencePrevention/
- Center on the Developing Child—Harvard University https://developingchild.harvard.edu/
- Child Trends https://www.childtrends.org/
- Child Welfare Information Gateway, USA https://www.childwelfare.gov/
- Cochrane Central Register of Controlled Trials (CENTRAL) https://www.cochranelibrary.com/central/about-central
- Google Scholar using “mother–child relationship” and “domestic violence” and treatment (or variations thereof)
- New Zealand Domestic Violence Clearinghouse https://nzfvc.org.nz/
- NHS https://www.nhs.uk/
- United Kingdom Government https://www.gov.uk/crime-justice-and-law/violence-against-women-and-girls
- Yale Child Studies Centre https://medicine.yale.edu/childstudy/
- Zero to Three https://www.zerotothree.org/
APPENDIX D:
PRISMA flow chart
APPENDIX E:
Summary table of included studies
Randomised Control Trials-PROTOCOLS
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Scott, 2017 | Canada | Urban | RCT | Self-completed questionnaires | Mothers Fathers Children | Group | 200 | This is an RCT examining the efficacy of embedding two different parenting interventions – Mothers in Mind (MIM) and Caring Dads – into child protection services for young children who have been exposed to IPV. Child protection case workers for families are randomly assigned to receive professional development training, supervision support and priority client access to parenting interventions. MIM is a mother–child dyadic intervention with 10 weekly group sessions and two individual sessions. Caring Dads is a fathering intervention that aims to prevent a recurrence of child exposure to IPV with 14 group sessions and two individual sessions | Treatment as usual: workers continue to provide in-home support to children and families. This is not a placebo: families receive the full child protection service they would normally have received if this trial were not being run | Primary: Recurrence of abuse Secondary: Workers’ case conceptualisation of the risks/needs of mothers & fathers Workers’ efficacy for using embedded parenting interventions Child social and emotional development | Study protocol available only |
| Visser et al., 2015 | Netherlands | Unclear | RCT 2-by-2 factorial experimental design Multicentre trial Data collected at baseline, post-intervention and 6-mth follow up (FU) | Questionnaires and observational tasks | Children Parents | Group & dyadic | 100 | HORIZON is a trauma-focused cognitive behavioural therapy (TF-CBT) group program plus preparatory parenting program plus parent–child sessions. Main aim is to test the additional parent program and parent–child sessions against TF-CBT. Consists of four conditions | Usual care is the TF-CBT group | Primary outcomes: Child internalising & externalising behaviour symptoms Secondary outcomes: Testing effect of the added components of intervention on child adjustment | Study protocol available only |
Randomised controlled trials
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Jack et al., 2019 | United States | Unclear | Cluster RCT | Cluster-based, single blind Measured via interview at baseline & every 6 months until 24 months | Pregnant women over 16 years | Individual | 492 | Nurse home visiting program with an augmented IPV intervention for socially disadvantaged pregnant women. Intervention sites (eight), nurses were provided with intensive IPV education and delivered IPV intervention including assessment and tailored planning for safety, violence awareness, self-efficacy, and referral to social supports | Control group (eight sites) received HV usual care | Primary outcome: quality of life Range of secondary outcomes covering physical and mental health, family violence (FV), general health, alcohol and drug use | No significant difference in primary and secondary outcomes, although several study limitations (e.g. fidelity to model) were noted which may have affected efficacy |
| Graham-Bermann et al., 2015 | United States Canada | Unclear | RCT Data collected at baseline, post-intervention and 8 months FU | Mothers and children (aged 4 to6; mean 4.9 years) | Group | 120 | The intervention is Preschool Kids’ Club which is 10 sessions and takes a skills-based approach delivered to children. It is intended to be delivered in parallel with Moms’ Empowerment Program (MEP) (delivered to the mothers). Preschool Kids’ Club is 10 sessions and takes a skills-based approach. It covers topics like attitudes and beliefs, managing emotions and fears, safety planning and conflict resolution | Waitlist | IPV Child adjustment | Baseline IPV prevalence results. Only girls in intervention group showed significant improvement in internalising symptoms. For children who adhered to the treatment protocol, there was a significant difference in both boys and girls | |
| Miller-Graff et al., 2016 | As above | As above | Mixed method Evaluation of children’s re-experiencing symptoms in therapy described above | Data collected from therapists via a child symptom checklist and examination of clinical notes Qualitative study examining case notes via thematic analysis | Mean age 5 years | 56 notes | 2016 results: 68% (38/56) developed re-experiencing symptoms during treatment. No difference in age, gender or IPV exposure. Re-experiencing symptoms spiked in session 3 – recommend min 6 to 10 sessions | ||||
| Howell et al., 2015 | United States | Unclear | RCT data from earlier Graham-Bermann et al., 2006 study Data collected at baseline and 5 weeks post | Interviews during which study measures were collected | Mothers | Group | 120 | MEP is a community-based intervention that aims to improve the mental health, access to resources, and parenting abilities of women exposed to IPV. 10x1hr sessions are provided over 5 weeks with five to seven participants in each group | Waitlist | Violence severity Depression and mood Post-traumatic stress Parenting practices | Significant improvement in parenting behaviours in intervention group |
| Grogan-Kaylor et al., 2019 | As above | As above | Pre/post and 6- to 8-month FU study | Mother and child pairs (4 to 6; mean 4.9 years | 113 | This study specifically looked at use of corporal punishment pre & post MEP | Significant reduction in use of punishment in intervention group post-intervention and at 6-mth FU | ||||
| Feinberg et al., 2016 | United States | Urban | RCT Randomised via block design Data collected at baseline and 10 months postpartum | Participant completed questionnaires Videotaped observation of triadic family interactions which were then coded | Mothers-to-be Fathers-to-be | Group | 399 | Family Foundations is a transition to parenthood universal prevention intervention. Nine sessions (five prenatal and four postnatal) are held and aim to address parent mental health, couple relationship functioning to impact children’s long-term emotional, mental health and academic outcomes | Control group families were sent written materials on child care choices and stages of child development | Co-parenting Couple relationship quality Parenting quality Parent adjustment Infant behaviour FV | Significant positive intervention effect on many outcomes. Significant intervention impact with large effect size for three of four violence outcomes. Relationship satisfaction was lower among intervention couples |
| Roopnarine & Dede Yildirim, 2018 | United States | Both | RCT Data were collected 15 & 36 months after random assignment | Survey | Mothers Fathers | Group | 3045 | Building Stronger Families is a relationship skills education intervention with low-income unmarried couples designed to improve child and parent wellbeing. Delivered in eight sites and used one of three curricula, delivered weekly over 5 to 6 months. Coordinators provided couples with emotional support and relationship building skills. Support was provided to men to access education, employment, and mental health services. This article specifically examines father data only and the relationship between the intervention, paternal depression, IPV and childhood behaviours | Unclear | (Father only) Depressive symptoms IPV Avoidance of destructive conflict behaviour Paternal warmth Child internalising and externalising behaviours | The intervention had a positive influence on paternal depressive symptoms and IPV at 15 months post intervention. The intervention also seemed to improve father–child relationships and childhood development |
| Satyanarayana et al., 2016 | India | Urban | RCT | ICBI vs treatment as usual Spouse and child FU at 1 and 3 months post patient discharge | Male inpatients in mental health facility | Group | 177 | Effectiveness of an integrated cognitive–behavioural intervention (ICBI) in reducing use of IPV among alcohol dependent men and improving mental health of spouse and children. Eight CBT sessions (45 to60 mins) on alcohol and IPV, triggers for alcohol use and IPV, consequences and prevention of IPV | Treatment as usual: pharmaco-therapy and psycho-education | Men: alcohol intake, IPV perpetration Women’s mental health Child mental health and behaviour | Lower IPV perp, women had less depression, anxiety and stress. No difference in alcohol use by men or child behaviour change between groups from baseline to 3 month FU |
| Steele et al., 2019 | United States | Urban | RCT | Questionnaires Parent–child observation | Mothers Children (aged 0 to 3) | Group | 78 | Group attachment-based 26-week intervention (GABI) for parents and their children that is trauma-informed where families (parents and/or children) have adverse childhood experiences (ACE-including domestic violence). Parents attend with their children up to three times weekly for 2hrs. It seeks to address intergenerational trauma and promote a secure attachment relationship between the mother and child | Systematic Training for Effective Parenting (STEP) intervention | ACE Mothers’ BMI Zero to three psychosocial & environmental stressors | Only reports on maternal behaviour (supportive presence and maternal hostility) and mother–child interaction behaviours and reciprocity differences between groups. Improved maternal presence and dyadic reciprocity. Declines in maternal hostility and dyadic constriction (proxy measures for risk of child abuse) |
| Stover, 2015 | United States | Urban | RCT (pilot) | Pre, post and 3 months FU surveys Completed by children’s father and mother | Fathers | Individual and dyadic | 18 | Fathers for Change includes: 1) focus on the fathering role as a motivator for change; 2) integration of strategies for reducing IPV and substance abuse (SA) in each session; 3) intergenerational transmission of IPV and SA; 4) communication skills and co-parenting; 5) the impact of IPV and SA on child development; and 6) parenting skills | Usual treatment: drug counselling sessions over 16 weeks | Severity of violence Substance abuse Parenting Psychiatric issues Father–child relationship | Fathers for Change group – more likely to complete treatment, program satisfaction. Less parental intrusiveness on free play between father and child than controls. Trend seen in less IPV |
Mixed designs (RCT and non-RCT)
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anis et al., 2020 | Canada | Urban | 2 x pilots 1 RCT and 1 non-RCT | Pre–post parent questionnaire | Mothers and children (0 to 32 months). Co-parent in three sessions | Dyadic and triadic | Study 1 (RCT) – 20 Study 2 (non-RCT) –10 | ATTACH (Attachment and Child Health) Parental reflective function-focused intervention. Psycho-educational parenting program of 10 to 12 sessions | Usual care: Nurturing Parent Program | Parent–child interactions Child development | Study 1 and 2: improved parent–child interaction quality and child development |
| Letourneau et al., 2020 | Canada | Urban | 3x pilots Two RCTs and one Non RCT | Pre–post parent survey via therapist interviews and video recordings | Mothers and children (9 to 36 months). Co-parent in two to three sessions | Dyadic and triadic | Study 1 (RCT) – 20 Study 2 (non-RCT) – 10 Study 3 (RCT) – 10 | ATTACH Parental reflective function-focused intervention. Psycho-educational parenting program of 10 to 12 sessions | Study 1: usual care: Nurturing Parent Program Study 3: parenting program called “Theraplay” | Parental reflective function Maternal–child attachment | Studies 1 and 3: improvement in attachment, significant improvements in child reflective functioning and trend in improved maternal reflective functioning. Study 2: Significant improvement in maternal and overall reflective functioning. Trend towards improved attachment |
Non-randomised controlled study
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Waldman-Levi & Weintraub, 2015 | Israel | Unclear | Pre- & post- testing with control group | Questionnaire administered via interview | Mothers Children | Dyadic | 37 | FI-OP (Family Intervention for Improving Occupational Performance) A crisis-based intervention offered in eight domestic violence (DV) shelters – eight sessions @30 mins Aims to improve mother–child interaction and children’s play functioning for families who have experienced DV. It is based on attachment, social learning and social-cognitive theory and the concept of a “secure space” | Playroom program | Preschool play & playfulness Parent/infant interactive behaviour | Significant difference in intervention group for some aspects of mother–child interaction and children’s play skills. Not significant in other areas |
| Schechter et al., 2015 | United States | Urban | Pre- & post- with comparison groups | Clinician-administered questionnaires | Mothers Children | Dyadic | 59 | CAVES, a clinician-assisted video-feedback exposure intervention with a sample of non-referred community mothers who have experienced IPV and their children aged 1 to 4. It aims to change parental state of mind and associated behaviours toward children in a relatively brief period of time | All received intervention but were grouped by post-traumatic stress disorder (PTSD) ratings. Controls were those with no PTSD diagnosis | Depression and mood Maternal attribution | Reduction in degree of negativity in clinically significant PTSD group towards their child but not themselves or their primary attachment figure |
Pre- & post- no comparison group
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rizo et al., 2018 | United States | Unclear | Pre-3m post and 6m FU pilot study | Questionnaire – self-completed or administered | Mothers Children 5+ (in concurrent therapeutic support group) | Group | 73 | Mothers Overcoming Violence Through Education and Empowerment (MOVE), a community-based, service-mandated 13-week (meet once per week for 2.5 hours) psychoeducation program to address the safety, parenting and mental health needs of mothers exposed to IPV | N/A | Safety Parenting Maternal mental health | Significant reductions in depression and post-traumatic stress | ||||||||||||
| Southwell, 2016 | Australia | Both | Pre- & post- testing | Parent assessments Parent feedback survey (administered via interview with therapist) Therapist reports | Children (parent–child therapy may be offered) | Individual | 41 | YETI (yourtown’s Expressive Therapies Intervention) intervention for traumatised and attachment-disturbed children. Therapies include art, music, drama, dance/movement, poetry and bibliotherapy, play and sand play. No set number of sessions, 30 to 60 mins. Provided at 2 sites: a child and family service centre and a DV refuge | N/A | Child behaviour | Significant improvement in all measures except somatic complaints | ||||||||||||
| Bunston et al., 2016 | Australia | Urban | Pre- & post- testing | Mixed methods Parent-rated questionnaires Clinician-rated questionnaires Qualitative data via open-ended questions in satisfaction survey | Mothers Children | Group | 105 mothers with 133 infants | Peek-a-Boo Club, a therapeutic infant/mother group intervention used “infant led” approach to repair the relationship after DV. Based on object relations and attachment theory frameworks. 11 x 2-hour sessions held in three phases: encouraging engagement, encouraging reflection, and encouraging consolidation | N/A | Infant functioning Mother–infant attachment Clinician-rated carer–infant functioning | Improved scores for infant, mother and infant–mother functioning. Authors assessed clinical significance and found that only some of the improvements were clinically significant | ||||||||||||
| Pernebo et al., 2018 | Sweden | Urban | Pre- & post- testing | Mixed methods Surveys, structured interviews, self-report inventory measures | Children aged 4 to 13 (mean age 7 years) and their mothers | Group | 31 in CBI and 19 in psychotherapeutic=50 | Two interventions: 1) community-based psycho-educative intervention (CBI): “Children are People Too” 2) psycho-therapeutic treatment intervention: “Trauma-focused group psychotherapy for children with experience of FV” (CAMHSI) Both interventions included parallel group sessions for children and for abused parents and entailed 12 to 15 weekly 90-minute sessions. Groups included four to eight children | N/A | IPV (CTS2) Child mental health, emotional regulation and behaviour Child trauma Maternal mental health Maternal trauma | Both interventions substantially reduced maternal post-traumatic stress. Children’s trauma symptom reduction was larger (and more sustained at 12-month follow-up) in the psychotherapeutic intervention, and children with initially high levels of trauma symptoms benefited the most | ||||||||||||
| Pernebo et al., 2019 | Sweden | Urban | 6- and 12-month FU study on sustainable change | As above | Children aged 4 to 13 (mean age 7 years) and their mothers | Group | 31 | As above | N/A | As above | Sustained treatment gains reported, no increase in symptoms or increase in IPV | ||||||||||||
| McConnell et al., 2017 | United Kingdom | Unclear | Pre- & post- testing with 6-mth FU Small cohort study with unmatched comparison group also done at one centre (small numbers) | Mixed method Note: fathers, partners and children participated in evaluation. Partners and children: face-to-face surveys with practitioners. Fathers: surveys, case records analysis, qualitative interviews with subgroups of partners and children | Fathers | Group | 271 | Caring Dads Safer Children, based on a Canadian intervention. Delivered across five centres. Fathers attended 2-hour weekly sessions for 17 weeks, with one individual session at end of program. Goals: 1) develop trust and motivation to examine their fathering; 2) increase awareness of child-centred fathering; 3) increase awareness and responsibility for abusive and neglectful fathering; 4) consolidate learning, rebuild trust and plan for future | N/A | Fathers’ attitudes & parenting behaviours Fathers’ controlling behaviour towards partners Children’s and partners’ wellbeing | Significant improvements in fathers reported in parental distress, parent–child dysfunctional interaction, perceptions of child being difficult, overall parenting stress score. Only one change in parenting behaviour (reduced hostility and aggression subscale). Some significant improvements in fathers’ controlling behaviour towards partners. Some fathers’ attitudes & behaviour did not change, or only changed partially or temporarily. Children reported improvement in parenting behaviour but not statistically significant. Inconclusive findings for children’s wellbeing, but improvements in partners’ wellbeing | ||||||||||||
| Berry et al., 2019 | United Kingdom | Urban | Pre- & post-feasibility study | Mixed methods Surveys, semi-structured interviews and focus groups with parents, facilitators and managers | Mothers | Group | 19 mothers | Family Vision, a life coaching program for single mothers with experience of FV with pre-school and school-aged children | N/A | Parent efficacy Mental wellbeing Child–parent relationship Strengths and difficulties | Appears to be feasible and acceptable. Did not conduct significant tests on outcomes | ||||||||||||
| Domoney et al., 2019 | United Kingdom | Both | Pre- & post- testing Data collected at baseline, 1 year and 2 years | Mixed methods Quantitative outcome data Qualitative interviews Observations of child development and parent–child interactions Data collected via interviews | Mothers Fathers | Individual | 40 | For Baby’s Sake, a trauma-informed whole family, home visiting intervention for parents from pregnancy – 2 years postpartum to break DV cycle and improve child outcomes. Staff come from a variety of backgrounds & provide face-to-face therapeutic sessions to parents to assist with past behaviours and experiences, including ACEs, current DV | N/A | Domestic abuse Mental health Parenting Child development Child behaviour Participant experience | Preliminary data only available | ||||||||||||
| Waters et al., 2015 | United States | Urban | Pre- & post- testing with 6-mth FU | Clinician-administered assessments Video recording of play between mother and child made and coded | Mothers Children | Dyadic | 52 | Perinatal adaptation of child–parent psychotherapy (CPP) intervention for predominately Latina, low-income pregnant women with a history of IPV. Includes psychoeducation on pregnancy, childbirth, infant development and the impact of IPV on the foetus/baby. Also some PTSD response therapy, maternal insight into negative attributions to her infant. Sessions continued 6 months after birth | N/A | PTSD Abuse Trauma Parenting inventory Maternal sensitivity | PTSD decreased and their child-rearing attitudes improved. Greater improvements in child-rearing attitudes predicted higher levels of maternal sensitivity, however improvements in PTSD did not | ||||||||||||
| Stover et al., 2017 | United States | Urban | Pre- & post- Mixed method feasibility study | Quant: written assessment at baseline. Post-assessment follow-up completed by research assistant Therapy sessions were video recorded to assess treatment adherence Qual: Two focus groups with sub-set of fathers (n=11) | Fathers | Individual and dyadic | 44 | Fathers for Change emphasises fathering role as a motivation to continue treatment. Delivered to fathers in substance use disorder treatment with a history of IPV. Delivered over 16 weeks, it addresses 14 topics in 60-minute sessions. Combines attachment, family systems & CBT. Goals are: 1) maintaining abstinence from substances; 2) cessation of violence & aggression; 3) decreased child maltreatment; 4) improved co-parenting | N/A | Addiction severity Anger intensity Emotional regulation difficulties Thoughts related to jealousy and anger Satisfaction with intervention | Significant improvement in anger, emotional regulation, co-parenting, dependency, personalisation, explicit negative affect measures. High level of satisfaction and attendance | ||||||||||||
| Lavi et al., 2015 | United States | Urban | Pre- & post- pilot | Participants and clinicians completed written assessments | Mothers (to be) Children | Dyadic (before and after birth) | 64 | CPP intervention with pregnant mothers continuing post-birth. Referred if reported to the social worker that they felt unsafe in their relationship. Aims to prevent and/or ameliorate short- and long-term consequences of IPV on child and maternal wellbeing and safety. Perinatal adaptation includes consideration of unique emotional and physical transitions that occur during this time | N/A | Attachment Depression PTSD Child-rearing attitudes | Significantly low levels of depression and PTSD symptoms (PTSS) post-treatment. Women displayed higher levels of positive child-rearing attitudes post-treatment. Women with low levels of maternal–foetal attachment prior to treatment showed the greatest improvement in depression, PTSS and child-rearing attitudes | ||||||||||||
| Hagan et al., 2017 | United States | Urban | Pre- & post- testing | Parent-reported PTSS Some were clinician-administered via interviews | Mothers Children | Dyadic | 199 | CPP intervention provided to a cohort referred for outpatient mental health services at an urban public hospital. Unstructured weekly 1hr sessions were held. Goal: to foster physical and emotional safety in the caregiver–child relationship to restore the child’s health & developmental progress | N/A | PTSS Exposure to traumatic events Treatment characteristics | Reduction in PTSS for parents and children. Extent of improvement varied depending on child, parent and treatment characteristics. Reduction greater in families who reported fewer traumatic life events for parents | ||||||||||||
| Herschell et al., 2017 | United States | Urban | Pre- & post- testing (pilot study) Data collected at baseline, mid-treatment and post-treatment | Assessments were conducted by independent research assistants. Parents completed assessment questionnaires | Parents (mainly mothers) Children | Dyadic | 21 (only 9 dyads completed PCIT) | A parent–child interaction therapy (PCIT) intervention in a DV shelter, provided by community-based clinicians. Sessions were provided weekly and treatment was for 12 to 20 weeks. First phase: child-directed interaction, which focuses on relationship enhancement. Second is parent-directed and focuses on effective discipline and limit setting | N/A | Life experiences (exposure to traumatic events) Child behaviour Parenting practices Parental mental health Treatment engagement and satisfaction | Positive significant effect on child behaviour, some parenting practices and mental health symptoms. No significant improvement in some measures including positive parenting practices. High dropout rate. Small numbers due to pilot study | ||||||||||||
Other (single case study, series)
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Morales et al., 2015 | United States | Unclear | Single case study Quantitative data collected at baseline and one- and three-month FU | Self-reported measures (computer delivered) Qualitative data | Mother | Group & individual | One | SafeCare – home visitation program Aims to reduce risk of child maltreatment and recognises that IPV and child maltreatment frequently co-occur. SafeCare Parent–Infant Interaction module aims to reduce both. This study examines the cultural adaptability of the model for Latino families | N/A | Parenting skills Daily activities Conflict Child abuse potential Neglectful behaviour Brief symptom inventory Parenting stress Protective factors Satisfaction | Improvements in all measures against baseline and high levels of satisfaction with intervention delivered in participants’ primary language. Needs effectiveness study with larger group |
| Keeshin et al., 2015 | United States | Unclear | Case series They compared use of positive and negative comments in first 5 mins of individual sessions attended | Clinician-rated coding | Mothers Children (2 to 5 years) in DV shelter | Dyadic & group | Eight (mother–child dyads) | The provision of PCIT at a self-contained extended stay shelter. Between two and eight x 30 min dyadic sessions and 7x weekly 90-min group sessions were held | N/A | Clinician-rated mothers’ use of positive and negative comments. Themes brought up at group sessions | More positive comments used as sessions continued. Mothers increased their use of PRIDE skills and valued the opportunity to reflect on their parent–child interactions during group sessions |
Qualitative studies
| Author, date | Country of origin | Urban, rural or both | Study design (most dominant design) | Data collection methods | Participants | Group, dyadic or individual | Sample size | Brief description of intervention | Control group | Outcomes assessed | Evidence of effectiveness? | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Broady et al., 2017 | Australia | Both | Qualitative | One-on-one interviews Thematic analysis undertaken | Fathers | Group | 21 | Taking Responsibility is an 18-week group course for fathers complemented by periodic individual support sessions. Program covers topics such as tactics of power and control, exploring beliefs about male and female roles, understanding the impact of violence on others (including children), developing empathy and exploring thinking processes underpinning men’s behaviour | N/A | Perceptions and personal narratives regarding experiences of the program and behavioural change. This paper specifically focuses on participants’ children and parenting relationships | Fathers’ desire to maintain and improve relationships with their children, however, some fathers reported a belief that their children had not been impacted by their violent behaviour | ||||||||||||
| Kamal et al., 2017 | Sweden | Unclear | Qualitative | Focus groups | Mothers Fathers | Group | 26 | Parenting and Violence, a 10-week attachment-based psycho-educational intervention for parents who are victims or perpetrators. Each group has maximum five participants, with mothers and fathers grouped separately. Sessions are 1.5 hours Aims: 1) increase parental awareness and involvement in child perception of violence; 2) minimise impact of violence on child development; 3) prevent violence from following child into adulthood & their future relationships | N/A | Experiences of intervention How intervention influences participants’ handling of family situations | Participants perceived improved self-control, self-esteem and communication skills and these seemed to positively influence their children’s wellbeing and behaviour | ||||||||||||
| Pernebo & Almqvist, 2016 | Sweden | Urban | Qualitative | 2016 – interviews | Nine children (4 to 6 years) post therapy. 78% had no contact with perpetrator | Group | Nine | Group trauma-informed therapy (weekly sessions with parallel group for mother) for children who have exposure to IPV against mother | N/A | Experience participating in group therapy and completed a drawing of experience | Themes using interpretive phenomenology 1. Joy 2. Security 3. Relatedness 4. To talk 5. Competence | ||||||||||||
APPENDIX F:
Summary table of interventions identified
Randomised controlled trial protocols
| Author and date | Intervention title |
|---|---|
| Scott et al., 2017 | Caring Dads (CD) and Mothers in Mind (MIM) |
| Visser et al., 2015 | Trauma Focused Cognitive Behavioural Therapy (TF-CBT) |
Randomised and non-randomised controlled studies
| Author and date | Intervention title |
|---|---|
| Jack et al., 2019 | Nurse Family Partnership Home Visiting with IPV (HV-IPV) |
| Graham-Berman et al., 2015; Miller-Graff et al., 2016 | Preschool Kids’ Club (PKC) and Mothers’ Empowerment program (MEP) |
| Howell et al., 2015; Grogan-Kaylor et al., 2019 | MEP |
| Feinberg et al., 2016 | Family Foundations |
| Letourneau et al., 2020; Anis et al., 2020 | Attachment and Child Health (ATTACH) |
| Roopnarine et al., 2018 | Building Strong Families |
| Satyanarayana et al., 2016 | CBT |
| Steele et al., 2019 | Group Attachment-Based Intervention (GABI) |
| Stover, 2015; Stover et al., 2017 | Fathers for Change |
| Waldman-Levi et al., 2015 | Family Intervention for Improving Occupational Performance (FI-OP) |
| Schechter et al., 2015 | Clinician Assisted Video feedback Exposure Sessions (CAVES) |
Pre–post observational studies
| Author and date | Intervention title |
|---|---|
| Berry et al., 2019 | Family Vision |
| Bunston et al., 2016 | Peek-a-Boo Club |
| Domoney et al., 2019 | For Baby’s Sake |
| Hagan et al., 2017 | Child–Parent Psychotherapy (CPP) |
| Herschell et al., 2017 | Parent Child Interaction Therapy (PCIT) |
| Lavi et al., 2015; Waters et al., 2015 | Perinatal CPP |
| McConnell et al., 2017 | Caring Dads Safer Children |
| Pernebo et al., 2018, 2019 | Community Based Intervention (CBI) and Child and Adolescent Mental Health Service Intervention (CAMHSI) |
| Rizo et al., 2018 | Mothers Overcoming Violence Through Education and Empowerment (MOVE) |
| Southwell et al., 2016 | yourtown’s Expressive Therapies Intervention (YETI) |
Qualitative and other studies
| Author and date | Intervention title |
|---|---|
| Broady et al., 2017 | Taking Responsibility |
| Kamal et al., 2017 | Parenting and Violence |
| Keeshin et al., 2015 | PCIT |
| Morales et al., 2015 | Safe Care |
| Pernebo et al., 2016 | Trauma-Informed Therapy |
APPENDIX G:
Intervention descriptions
Group work: Psychoeducational, psychotherapeutic
Group work can be defined as an endeavour where individuals choose to meet for the specific and mutual purpose of interacting with one another to achieve identified goals. A facilitator is responsible for organising and maintaining the agreed-upon setting and fostering group engagement. There are many group formats which may include psychoeducational groups and psychotherapy groups. Psychoeducational groups emphasise the delivery of specific educational content by the facilitator, for example a group on “parenting skills”, and may be run much like a tutorial whereby the group task is to learn the concepts and explore these in the format of group activities, discussion and reflection. These groups are often manualised, with set content and activities for each group session. Psychotherapy groups emphasise experiential learning with the “educational content” arising from within the context of the relationships in the group. For example, the psychotherapy group may be for women wishing to explore the difficulties that they encounter as mothers and agreeing to share their respective experiences with each other as a basis for learning, discussion and development. This is in distinction to psychoeducational groups where set pre-prepared educational content is introduced. The group tasks in these instances are therefore for participants to observe and reflect upon their own states and those of others. Although there is no set content for sessions, the focus for the group and other variables are often set by group participants at the onset of the group. In principle, psychoeducational groups can be delivered to larger groups of participants whereas psychotherapy groups are usually smaller to ensure that each participant has time to be heard and understood by the group as part of the treatment process (Erford & Bardhoshi, 2018).
Psychotherapies: Individual, parent, dyadic
Psychotherapy (or therapy) is a form of mental health treatment that uses communication between two or more people as treatment method. There are a range of psychotherapies or therapies that focus more or less on either the nature of the relationship/s between two people as a means of understanding and overcoming barriers clients encounter in their relationships (psychoanalytic, psychodynamic, attachment-based or family therapies), or identifying and changing clients’ specific problematic behaviour or thought processes (cognitive behavioural or cognitive analytical therapies; Nardone & Salvini, 2019).
Psychotherapy can be undertaken by an individual, adult couple, child and parent dyad or family. Individual therapy is usually focused on problems related to an individual’s functioning. For example, a woman affected by violence may seek therapeutic help with her wariness in relationships or with her capacity to relax and sleep at night after her experiences of violence. Alternatively, a woman may be more immediately concerned with her child’s recovery and her confidence in parenting, so she may seek a form of parent therapy to focus specifically on this. Both individual and parent therapies may be exclusively psychodynamic or cognitive, or a mix of both, according to need.
Children may be supported either by individual or dyadic therapies. Because children may depend less on talking for communication and more on non-verbal cues and play, these broader forms of communication are also employed by child therapists, pitched to developmental capacity. Dyadic therapy (also referred to as mother–child, parent–child, child–parent, relational, or infant–parent therapy) engages both child and parent simultaneously in the treatment to directly redress relationship tension between them, and is the treatment of choice where the child is under the age of 6 due to their level of caregiver dependence (Dowling, 2019; Nardone & Salvini, 2019).
Tailored individual and dyadic interventions are particularly appropriate for infants, young children and affected mothers after IPV, given that the trauma of family violence is known to impact not only each individually but their relationships with one another. These dyads can also be supported in bigger group work settings, however the clinician’s capacity to respond specifically to the individual needs of the dyad (which we will call small dyad work) is limited where there are bigger numbers. This may be offset for the dyad by the positive impact of knowing that they are not alone in their experience in relation to their peers and indeed in an ideal service system perhaps a suite of group work and individual and small dyad therapies would be available. However, there are many dyads who require tailored small dyad work before, during or after group-work intervention where, within the privacy and specificity of this setting, they can develop the trust with their clinician that may be needed to revisit and reset the impact of family violence trauma upon their relationship.
APPENDIX H:
Maternal interview schedule
- Introduction
- Reminder of consent and reassure confidentiality
- Explain that sometimes talking about personal experiences in a research project can be distressing and we can stop at any time if you need to. You may like to talk further about some of the issues raised, either with the researcher, therapist or with someone else afterwards. Resource material will be provided at the beginning of the interviews for referral options including phone and website options.
- Explain recording and approximate time frame
- Any questions before we begin?
We are interested to know about your general experience with the CPP treatment you have recently completed with your child.
Perceived benefits
- Thinking back to the start of treatment, can you tell me what you hoped or expected from the program? Changes/benefits for your child? For yourself? Mother-child relationship?
- What outcomes/results of treatment are most important to you? E.g. understanding the violence and its effects, communication between mother and child, reduction in behaviour problems
Acceptability/satisfaction
- Do you know how many sessions you completed?
- In general how was your experience with the therapy? Have you and your child been helped with what you wanted? If yes, how do you think this has occurred? Enablers? If no why? Barriers?
- How do you think the experience was for your child?
- Was there something that has been particularly good?
- What has been most helpful for you?
- What has been most helpful for your child?
- Was there any aspect of the treatment that you did not like?
- In the survey (completed with therapists) were there any questions you did not feel comfortable answering? General health, mental health, quality of life, child behaviour, exposure to violence, relationship with child, parenting?
- How was your experience with being video recorded during the play sessions?
- Therapy can be confronting, was there anything in the treatment that made you feel uncomfortable?
- Does the method need to be adjusted in any way to work better? Can you suggest how?
- Are there any things you would like help with now that the treatment has not addressed?
Children’s contribution
- How do you think children have experienced the intervention
- Were there child initiated moments of change or turning points in the dyad interaction you could identify? Can you give an example
- How did children respond to the questioning of mothers e.g. survey questions
- Children’s general influences/contribution of the therapy
Feasibility
- Have there been any difficulties for you to attend sessions and participate in treatment? If so what were these? (e.g. travel, costs, illness, interaction with perpetrator, the child does not want to attend etc.)
- Can you tell me what the costs have been to attend treatment each week e.g. weekly bus fare? Child care for other children, loss of wages etc.
Participation
- Have you changed since receiving treatment? If so, how?
- Has your child changed? How?
- Have you ever received any similar treatment like this for yourself and your child?
- Did you get enough information about the treatment before you decided to participate? Was there any information missing?
- Have you and/or your child received any other support while you have been in treatment?
- To what extent have you and your child had interactions with the partner who abused you during treatment e.g. daily, weekly, monthly, never?
- Do you think you will use the things you have learnt in the treatment?
- What do you think will happen now that you and your child have completed treatment?
Is there anything else you would like to discuss about your experience with receiving CPP treatment?
Check how they are feeling after the interview to ensure that any feelings of distress are supported.
Thank you