
RESEARCH REPORT WRAP around families experiencing AVITH: Towards a collaborative service response
ELENA CAMPBELL
Associate Director, Centre for Innovative Justice, RMIT University
RILEY ELLARD
Manager, Centre for Innovative Justice, RMIT University
ELIZA HEW
Project Officer, Centre for Innovative Justice, RMIT University
MATILDA SIMPSON
Project Officer, Centre for Innovative Justice, RMIT University
BETH McCANN
General Manager, Centre for Family Research and Evaluation, Drummond Street Services
SILKE MEYER
Chair in Child and Family Research, Griffith University and Adjunct Professor,
Monash Gender and Family Violence Prevention Centre, Monash University
RESEARCH REPORT
ISSUE 4 | APRIL 2023
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we live and work. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and emerging. We value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with First Nations Peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2023

With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au
ABN 67 162 349 171
ISBN: 978-1-922645-66-1 (paperback)
ISBN: 978-1-922645-67-8 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project “WRAP around families experiencing AVITH: Towards a collaborative service response”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Outcome 4 – Services meet the needs of women and their children experiencing violence.
Suggested citation:
Campbell, E., Ellard, R., Hew, E., Simpson, S., McCann, B. & Meyer, S. (2023). WRAP around families experiencing AVITH: Towards a collaborative service response (Research report, 04/2023). ANROWS.

Centre for Innovative Justice, RMIT University
Level 2, Building 52
147–155 Pelham Street, Carlton VIC 3053
Wurundjeri Country
Author acknowledgement
The project was led by the Centre for Innovative Justice (CIJ) at RMIT University, in partnership with the Centre for Family Research and Evaluation (CFRE) at Drummond Street Services and the Monash Gender and Family Violence Prevention Centre (MGFVPC).
The lead author wishes to acknowledge all the dedicated practitioners who gave up their time to participate in this research during Victoria’s protracted lockdowns. In particular, the author wishes to acknowledge practitioners at Drummond Street Services and staff of the CFRE who facilitated provision of data for the case file review. The team also wishes to acknowledge the contributions of the parents who participated in interviews for this research – their resilience in the face of long histories of intimate partner violence and their determination to protect their children shone through in their contributions. They confirm once again the need for better support for women and children in the wake of adult-perpetrated harm.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
ANROWS acknowledges that children and young people living in homes where domestic and family violence (DFV) is present are not simply “exposed” to DFV – they are experiencing it. There are no circumstances in which children and young people are exposed to DFV and are not also being impacted by this violence. Therefore, ANROWS will always default to using “experienced DFV” instead of “were exposed to DFV” or “witnessed DFV”. This language recognises that children experience DFV as victims in their own right, and also seeks to honour the voices of victims and survivors who have felt minimised, erased or unacknowledged as childhood survivors.
Please note that in this report, in certain contexts, the authors have chosen to use the term “exposed to DFV”.
Caution: The following report contains descriptions of domestic and family violence and adolescent violence in the home, and mention of suicide. Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76)
Definitions and concepts
Concept
Definition
AVITH
This report uses the term “adolescent violence in the home” (or “AVITH”) to describe the use of violence or harm against family members by children and young people. The majority of the evidence base indicates that this behaviour is more commonly used by young males than young females, although some recent research indicates that young females may either self-report as using violence more frequently, or be identified by the system for use of violence where use of the same behaviour by young males may be overlooked. While the gendered nature of the use of AVITH is not as distinct as the gendered nature of adult-perpetrated violence, far more pronounced is the gendered nature of victimisation. Specifically, evidence indicates that AVITH is most commonly experienced by mothers or female caregivers, particularly in the context of sole parent or separated families.[1]
The research team purposefully uses a term that is broader than “domestic and family violence” or “family violence” because, as the PIPA project (“Positive Interventions for Perpetrators of Adolescent violence in the home”) demonstrated and this research confirms, use of harm by young people can occur along a broad spectrum of behaviours (Campbell et al., 2020; see also definition below). In particular, the PIPA project found that some of this behaviour does not meet the legislative definition of family violence in Victoria; some of it is related to dysregulation or the impacts of past trauma; some of it manifests as resistance to current trauma or experiences of victimisation; and some of it is directly related to disability. This means, for example, that the behaviour is more complex, has different drivers or has a different intent than adult intimate partner violence. By using this broad definition, the authors do not suggest inany way that family members who experience this harm do not find it incredibly frightening and distressing. Rather, the use of this term is intended to recognise the complexity inherent in this phenomenon. AVITH is also the term used by the practitioners who participated in this study.
Family violence
At points during this report, the term “family violence” is used in preference to the broader term “domestic and family violence” (DFV). This is because “family violence” is the predominant term used in Victoria, the Australian jurisdiction in which this research took place. At other times, where more broadly applicable, the wider term DFV is used.
Young person
Although the title and terminology of the phenomenon used throughout this report refers to “adolescents”, as does the majority of the relevant literature, it is important to note that the preferred terminology of the practitioners participating in this report was “young people”. This reflects a wider shift in the social and human services environment which uses respectful and strengths-based terminology, as well as acknowledging neurodevelopmental trajectories beyond childhood. The term “young people” is also more inclusive of the client base of some services participating in this research that work with young people up to the age of 22. Where the term is used to refer to people over the age of 18 in the context of this research, and is therefore referring to young adults, this is identified. In general, however, the term “young people” used in this report refers to individuals aged under 18, recognising their legal status aschildren and, in the cases of younger children, their lack of access to relevant supports without the consent of their parents.
The PIPA project
The PIPA project was an ANROWS-funded study that examined legal and service responses to AVITH across three Australian jurisdictions (Victoria, Tasmania and Western Australia). The data collection for the research was conducted during 2017 and 2018 with the final report published in March 2020. The primary findings across this study concerned the harmful and counterproductive impacts of legal responses where young people are identified by the legal system as using AVITH; the significant prevalence of disability and neurodivergence among young people caught up in the legal response to AVITH in Victoria, in particular; and, specifically, the need for service responses to identify risk and needs across family structures and to wrap around each family with appropriate support. It is this final recommendation to which the current study specifically responds.
The Orange Door
The Orange Door network is a network of support and safety hubs established by the Victorian Government following recommendations by the state’s Royal Commission into Family Violence. The network is supposed to function as a shopfront with a “no wrong door” approach, operating as the intake point for police referrals in relation to victims and survivors and people using violence, as well as child safety and wellbeing concerns. Individuals can also self-refer without going through police, whether by phoning or attending in person. The Orange Door functions primarily as an intake point through which matters are then triaged and referred out to other appropriate services.
Drummond Street Services
Drummond Street Services is a large community-based organisation that has delivered support to vulnerable families and young people for over 100 years. It provides a range of services, including mental health services, family services, parenting services, support for blended and stepfamilies, specialist family violence services and supports for marginalised cohorts. These include supports for families from culturally and linguistically diverse communities; families in public housing; and LGBTQA+ and intersex young people and families, through its Queerspace programs.
Acronyms
Acronym
Definition
ACCO
Aboriginal community-controlled organisation
AOD
Alcohol and other drugs
AVITH
Adolescent violence in the home
CALD
Culturally and linguistically diverse
CFECFW
Centre for Excellence in Child and Family Welfare
CFRE
Centre for Family Research and Evaluation
DFV
Domestic and family violence
DS
Drummond Street Services
FVISS
Family Violence Information Sharing Scheme
GP
General Practitioner
LGBTQ+ and intersex
Lesbian, gay, bisexual, trans, queer and intersex
NDIS
National Disability Insurance Scheme
NVR
Non-violent resistance
PIPA
Positive Interventions for Perpetrators of AVITH
RCFV
Royal Commission into Family Violence
RYPP
Respect Young People’s Programme (United Kingdom)
VFRIM
Victorian Family Violence Implementation Monitor
WRAP
Wraparound Responses for AVITH Programming
Executive summary
Background
“WRAP around families experiencing AVITH: Towards a collaborative service response” (the “WRAP around families” project) was a targeted, mixed-methods research project with the specific aim of developing a framework for holistic, evidence-based practice in response to the complex issue of adolescent violence in the home (AVITH). The research was a direct response to a recommendation from the PIPA project (Campbell et al., 2020), which highlighted the complexity of needs across many families experiencing AVITH. The PIPA project found that appropriate service interventions require wraparound, whole-of-family responses, rather than responses directed predominantly at a young person’s behaviour.
Aims
As a “deep dive” into the service response to AVITH, the WRAP around families project aimed to identify current system barriers and to surface the enablers which may contribute to more consistent and collaborative practice. Originally the research aimed to explore what young people and their families identified about their own needs, including the impacts on siblings and the role of pre-existing trauma in parents. The ongoing impacts of COVID-19 on practitioner engagement with clients during the data collection period limited the extent to which this aim could be achieved, although rich accounts from interviews with three parents and reviews of 33 case files contributed significantly. The research also aimed to move practice and policy towards a consistent understanding of AVITH, given the uncertain position that it continues to occupy in domestic and family violence (DFV) responses.
Method
The research was informed by two data streams, the first being an exploration of current community-based service responses through focus groups with 75 practitioners in Victoria, a jurisdiction with a particular investment in this area. The majority of these focus groups were conducted from July to September 2021, while focus groups with Aboriginal community-controlled organisations (ACCOs) were conducted from June to August 2022. The second strand involved a mixed-methods case study approach to an intervention developed by a large community service organisation, Drummond Street Services (DS). The case study involved reviews of 33 case files from the service, with findings tested and validated through workshops with practitioners in this program. The case study also included interviews with three parents. Ethical approval for the research was obtained from the Victorian Department of Justice Human Research Ethics Committee (CF/21/5126).
A targeted scan of relevant peer-reviewed and grey literature was also conducted. Important to note, this was not intended to function as a systematic or even standard literature review, but rather to ensure that major relevant studies and program responses that were specifically relevant to service delivery and had been released or developed since the initial research phase of the PIPA project could inform the WRAP around families project’s design and analysis.
Findings
The research signalled that practitioners and programs were working hard to respond to young people and families experiencing AVITH in a service and system context which continues to have limitations. While there is now greater familiarity with the concept of AVITH and nuance in the practice of individual practitioners, the research found that Victoria’s response is still some way from being properly developed and bedded down at a systemic level. It should be acknowledged that this shifted to a degree between the point of data collection and publication, with growing government investment in service design, as well as the pending release of risk assessment and management tools.
Practice challenges
Naming and identifying AVITH
Findings from the focus groups were echoed to a significant extent in the parent interviews and signalled a number of substantial barriers to effective practice operating at the time of the research. These included the wider service system often having difficulty identifying AVITH or understanding its nuances, with responses to AVITH often dependent on the knowledge of individual practitioners and many services still responding within the binary framework of adult intimate partner violence. In this framework, policy and service responses are framed in terms of victims and survivors on the one hand or perpetrators on the other, rather than being able to contemplate that an individual may be using and experiencing violence at the same point or over the course of a lifetime. This binary framing in turn could impact the nature of referrals, the information that these referrals contained and the responses that were provided as a result.
Constraints on effective practice
Funding parameters impacted the capacity of services to respond in ways that families required. This included the need to work with multiple family members in a meaningful way or provide flexible and client-centred approaches, such as conducting outreach or engaging with young people through in-person activities and over the long term, as the case study component of this research indicated was required. Practitioners also described the detrimental impact of cyclical funding and limits on caseloads on the capacity to deliver effective service, although they did highlight the significant benefits of brokerage provided as part of a recent injection of additional investment.
Previous and ongoing adult-perpetrated violence and control
The predominant presenting client needs described by practitioners and apparent in the case study stemmed from pre-existing trauma from adult-perpetrated DFV, as well as the presence of ongoing coercive control. The presence of current adult-perpetrated DFV is not explored as thoroughly in the literature and in policy settings as the impacts of past DFV. The presence of current adult-perpetrated DFV across practitioner caseloads and the case study was therefore an important finding. The eligibility criteria of some programs precluded work with young people where adult-perpetrated DFV was present, while other programs were trying to conduct this work, despite not having associated supports or frameworks.
This experience of past and current trauma was clearly contributing to complex combinations of co-occurring issues in many young people and victim and survivor parents, which included, most prominently, significant mental health and sometimes alcohol and other drug (AOD) issues, as well as disability. Crucial to note, despite families presenting to DS in relation to their children, the overwhelming theme across the interviews and case files was the way in which adult-perpetrated DFV and ongoing coercive control was continuing to impact every aspect of the lives of mothers and their children. While parents were seeking support for their child’s behaviour, severe mental ill health, disability and learning needs, as well as for school disengagement, the single greatest contributing factor to these support needs – as well as to the needs of mothers – appeared to be the impacts of adult-perpetrated harm.
Impacts of other adverse experiences
In addition to adult-perpetrated DFV, the findings pointed to the impacts of other adverse experiences and the way in which these contributed either to the use of harmful behaviour by young people, or the way in which parents and siblings could manage what was occurring in their home environment. These included sub-themes that emerged from the focus groups: the relationship of bullying victimisation to use of AVITH, as well as the impacts of grief and separation on families as a whole, including separation from caregivers as a result of illness.
Impacts of COVID-19
More broadly, the findings indicated that co-occurring needs across families – including the risk of current adult-perpetrated DFV – were compounded by the impacts of COVID-19, while the challenges of engaging with and supporting clients during this time were made more acute. Practitioners voiced concerns that they had fewer “eyes” on the current risk that a young person might be experiencing, while the parents interviewed highlighted the need for face-to-face engagement that was not always available during the period covered by the research.
System challenges
Under-servicing and over-servicing
Practitioners voiced a particularly strong concern that families were either being “under-serviced”, and receiving no effective support for multiple presenting needs, or alternatively were being “over-serviced”, with multiple services involved over a long period, despite this over-servicing having no constructive effect. The case study similarly reflected the challenges of families receiving no effective service support and experiencing stop-start engagement which had limited capacity to support young people and which commenced and ceased involvement without any meaningful results.
Impact of negative service interactions
Prior negative experiences of service interactions were also apparent as a particular barrier to service engagement. The predominant examples nominated by practitioners were the damaging impact of multiple services in a young person’s or family’s life. Parents interviewed and case files all highlighted the impacts of ill-informed or misguided engagement with a private psychologist or school counsellor, including where these were manipulated by an adult perpetrator in ways which made young people refuse to engage in “talk therapy” again.
Care teams
The research identified important findings around care teams, with the research team anticipating that care teams would be a mechanism for emerging collaboration. Focus groups indicated that the purpose and composition of a care team could run counter to trauma-informed practice with young people, including where care teams focused on holding young people accountable, rather than on providing care and support.
In particular, the research found that care teams often lacked a practitioner to coordinate the activities to which care team members had committed. This was needed to ensure that practitioners followed up on their responsibilities and that one practitioner was liaising with the young person and family.
Promising practice
Evolving service recognition
Despite challenges in consistent and coherent articulation of what AVITH actually involves, the findings indicated that recognition of AVITH was growing among families, with many families in the case study having self-referred. Findings also suggested that it was a specialist area of work from which other services were grateful to receive support. A crucial consideration identified by practitioners was being aware of the context in which the intervention on offer was being described or labelled by services, with young people understandably reluctant to be labelled for behaviours which may have been repeatedly used against them.
Working with multiple family members
The research highlighted creative ways to support multiple family members. These included examples of supporting a caregiver’s wider needs and the impacts of trauma, while working with a young person around their use of harm and a sibling around their mental health needs. Participating ACCOs, in particular, emphasised that it was essential to cement any gains made with a young person through the provision of appropriate supports at home.
Capacity for flexible, client-centred responses
Findings confirmed the significant benefits where funding or organisational support allowed for work to be conducted on a longer-term basis, providing sufficient time to develop trust and rapport with young people. Emphasised as crucial by practitioners and parents alike – and evident in case files – were the benefits of outreach and shared activities, as well as brokerage to provide access to specific and tailored supports for different family members which could have a positive impact overall.
Shared positive experiences and strengths-based approaches
One of the primary findings of the research, echoed by key Australian research (Burck, 2021; Meyer et al., 2021; Burck et al., 2019), was that mothers and children who have experienced adult-perpetrated DFV, and continue to grapple with its ongoing impacts, need opportunities to build attachments and form their collective identity around positive experiences. Parent interviews and case files reflected the impacts of shared experiences of trauma on mothers’ relationships with their children and capacity to parent, while practitioners and case files provided examples of how brokerage or other mechanisms could facilitate positive experiences through which they could start to see their family in a new light. Again, ACCOs provided particularly strong examples of this, describing the benefits of supporting families proactively, rather than waiting for a crisis.
Giving voice to young people, keeping an original perpetrator in view
Corresponding with this, the research highlighted the importance of giving voice to young people where their experiences were often not coming through in referrals or in care team discussions and where the impacts of adult-perpetrated DFV – including ongoing systems abuse – remained out of view. Practitioners described nuanced examples of working with other agencies to widen the intervention lens to allow consideration of the presence of an adult perpetrator. Case files similarly demonstrated the delicate considerations involved, including where a perpetrator parent could withhold consent for a young person’s receipt of services to exercise ongoing control.
Reflective practice and emerging collaboration
Findings therefore indicated the need for a critical and reflective approach as a core foundation to AVITH-focused work. Examples of effective service intervention rested on constant interrogation of what was actually occurring in the lives of families and young people, as well as a constant interrogation of a practitioner’s own assumptions. This involved questioning the reasoning behind other service or practitioner decisions and stepping in or stepping out again as services focused on what families and young people identified as their most pressing need, rather than what services dictated.
Discussion and framework
Specialisation within a specialisation: Towards a collaborative framework
The complexity of this practice – which had been conducted for decades by one service and for years by others – signalled the need for AVITH-focused work to be recognised as a “specialisation within a specialisation”. The findings indicated that this work could be supported by services being sufficiently resourced to allow work with multiple family members; sufficiently flexible to provide for client-centred responses; and sufficiently secure to allow workforces to be developed over the long term.
To this end, the WRAP around families project proposes a Collaborative Practice Framework, through which policymakers can take responsibility for enablers, practitioners can engage with the core principles of practice, and all involved can base decisions on the foundational pillars so essential to the work. Practice examples, rather than discrete recommendations, are provided to support consideration of how the Framework might be applied in particular contexts.
Overall, therefore, what was originally expected to be a blueprint for collaboration across services became a blueprint for collaboration across practice and policy – so apparent was the need for this wider lens to be applied.
Pillars of the Framework
The Collaborative Practice Framework is based on four core pillars of understanding, workforce, coordination and evidence. As well as constituting individual components of an effective system-wide AVITH response, practitioners emphasised the mutually constitutive nature of the pillars, with each continually informing and reinforcing the others.
Shared understanding can help to challenge and unpack the binary paradigm of “victim and survivor”/”perpetrator” that underpins wider DFV work, recognising that young people using AVITH are most often victims and survivors in their own right and that the functions of their behaviour may be a signal of unmet needs. Practitioners can support this understanding in their advocacy to their own organisations, in their involvement in care teams, and in the terminology that they use with clients. Organisations and government can design, scope and resource interventions in recognition that this specialist work requires nuance, complexity and time.
An “AVITH workforce” involves a specialist workforce capable of delivering therapeutic interventions and case management, as well as baseline capability across the wider service system to identify AVITH, refer appropriately and work alongside specialist practitioners. This further involves organisations and governments scoping and resourcing interventions appropriately, integrating with other services to facilitate referrals and secondary consultations, and being supported by clinical supervision and training. Just as key, it involves identifying specialist roles in wider DFV and service contexts, as well as building the baseline capability of the broader community-based service, health, education and justice sectors.
Coordination is a building block of collaboration, involving clear structures, processes and mechanisms to support organised and seamless practice. Crucially, coordination is not about outputs but about service accountability to young people and families, fostering a shared understanding of what success might look like for a family or young person and what their readiness for service engagement might be. It involves follow-up, liaison with families and young people, and information sharing to ensure that all services working around a family have an adequate lens on risk and what is occurring for the family.
Evidence recognises the evolving nature of the service system, as well as our understanding of “what works” in response to AVITH. Valuing evidence includes allocating time for debriefing and reflective practice, as well as capacity to share practice across organisations. It also includes ensuring that AVITH responses are underpinned by effective processes for monitoring, evaluation and learning over the long term – informed by the voices of young people and their families in a way that recognises the complexity and time involved in conducting this kind of consultation safely and appropriately. Just as key is government support for a system-wide approach to building and sharing evidence, piloting responses and taking effective interventions to scale. This means focusing on evidence-informed practice rather than prescriptive approaches, and on outcomes rather than outputs.
Principles of the Framework
Trauma and family violence risk–informed emphasises that it is crucial for practitioners to make the ongoing impacts of trauma – including from adult-perpetrated harm as well as the potential presence of current adult-perpetrated DFV – as a central consideration across their work. This means maintaining a lens on all forms of risk across a family and working in ways that keep any adult perpetrator in view. At its core it involves asking “What has happened to you?”, rather than “What is wrong with you?”
Whole-of-family means keeping the needs and experiences across the family in sight and considering interventions which can help to support safer family functioning. This does not necessarily mean working with every member of the family – particularly where this is not safe. Rather, relational work is seen as crucial in supporting the young person’s recovery, working with particular family members to address particular needs in ways that can reduce risk and contribute to positive relationships and outcomes.
Addressing barriers to engagement acknowledges that families and young people experiencing AVITH may have either been under-serviced or over-serviced or had prior negative experiences of service interaction. Existing shame and stigma may have been compounded by service responses, while systemic and structural harm may play a role for some families. Keeping this principle in mind means understanding these histories and working to build trust and reduce the burden of service engagement.
Flexible and needs-based recognises that young people and families need to be supported in ways that work for them. This includes working over the longer term, and adopting outreach as a key approach to build trust and rapport; leveraging brokerage to address specific needs across the family and build positive shared experiences; and, most importantly, responding to readiness and working in partnership with clients. It includes ensuring that program responses offer a variety of service responses.
Intersectional and culturally safe requires AVITH responses to include a lens on diversity and marginalisation. Practitioners must actively consider how experiences of young people may be compounded by stigma, intergenerational trauma or discrimination. Organisations should actively seek to build capacity for working in culturally safe and sensitive ways with clients from Aboriginal and Torres Strait Islander, culturally and linguistically diverse (CALD), and LGBTQ+ and intersex communities, as well as clients with disability.
Service accountability means that the roles, responsibilities and expertise of each practitioner or service involved is understood by all. An accountable service is one that does what it says it will do and which is committed to working with the family to agree on, plan for and progress their specific identified goals. For service accountability to occur at the system level, communication between services must be proactive and transparent, with an overall focus on ensuring that dynamic risk information is shared and managed collectively.
Figure 1: High-level overview of Collaborative Practice Framework: Multidisciplinary and multi-system
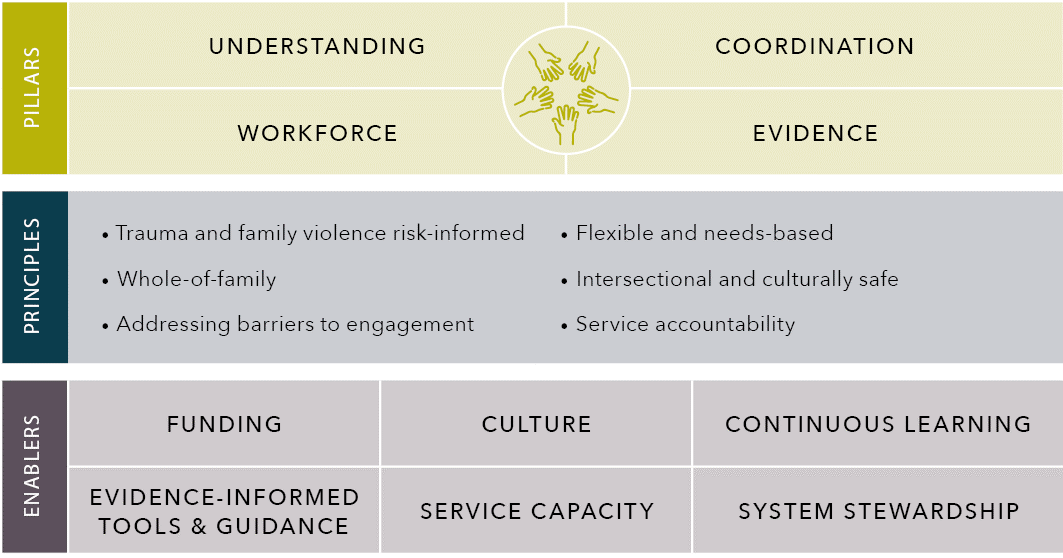
Source: Centre for Innovative Justice.
Text alternative for the figure above
Understanding
- Understanding
- Workforce
- Coordination
- Evidence
Principles
- Trauma and family violence risk-informed
- Whole-of-family
- Addressing barriers to engagement
- Flexible and needs-based
- Intersectional and culturally safe
- Service accountability
Enables
- Funding
- Evidence-Informed Tools & Guidance
- Culture
- Service Capacity
- Continuous Learning
- System Stewardship
Enablers in the Framework
Funding needs to be secure and stable, supporting workforce recruitment and retention over the longer term, as well as long-term work with clients, and supporting appropriate caseloads which account for the complexity and scope of AVITH-focused work and have a focus on outcomes rather than outputs.
Culture is crucial. Individual practitioners should see themselves as one part of a broader response to AVITH. Organisations should signal to practitioners that it is valuable to invest time and effort in collaborative work and that identifying and responding to AVITH is a shared responsibility.
Continuous learning is critical given the emerging nature of understanding around AVITH. Learning must occur at the practitioner, organisational and system levels, including creating opportunities for reflective practice and shared learning within and across programs and organisations.
Evidence-informed tools can foster a shared language and understanding, as well as supporting a structured approach to identifying and managing risk. Rather than replicating adult-focused tools, evidence-informed tools should be strengths-based, with capacity to recognise, assess and work with complex risk dynamics.
Service capacity requires the ability to work flexibly and responsibly, intensively and over the long term, with timely responses to prevent escalation of risk. Service capacity also requires resourcing to support workforce retention, including through supervision, training and reflective practice.
System stewardship involves government taking a lead in fostering an AVITH system which is founded on a shared understanding, removes barriers to collaboration within and across systems, and involves government collaborating with the sector to steer the system towards key outcomes.
Limitations of the research
The research had key limitations which should be acknowledged. The first was the impacts of COVID-19 on the case study program at DS which made engagement with clients – and associated recruitment to the interviews – a considerable challenge, as well as limiting data available on case files to a less significant extent. Associated limitations also include the absence of Child Protection input.
Arguably, the above limitations are all primarily attributable to the period during which data collection was conducted in the context of entrenched complexity in clients and increased workload at a practice and system level. That said, while this was anticipated to be a key focus of the focus group discussions, the primary concerns of participating practitioners related to system and policy settings which predated the pandemic but which they feared would be compounded by a lack of government resourcing in the future as a result of the pandemic and its impacts.
Implications for policy and practice
The concern voiced by practitioners is a key consideration for policymakers as they move towards future service design and investment. While the impacts of COVID-19 will continue to stretch public resources, the WRAP around families research points to the need for greater support for families and young people, provided at an earlier point to prevent greater economic and social impacts down the track.
Significantly, this involves support for women and children who have experienced adult-perpetrated DFV and, crucially, may still be experiencing its impacts. Equally this research echoes the PIPA project and other research which points to the substantial need for greater support for families with a young person with disability.
Investment in earlier intervention therefore represents a vital opportunity for prevention of AVITH – rather than waiting, as participants in the PIPA project described, until it is “10 years too late”. Where the system fails to intervene earlier, however, the WRAP around families project offers a blueprint to support a genuinely collaborative and consistent framework to respond. In doing so it signals that the nuance, flexibility and complexity which are required in practice may mean that current approaches to service funding should be re-examined and a genuine concerted investment brought to the fore.
Directions for future research
The project’s findings indicated that it was attempting to address a bigger research and practice gap in relation to collaboration than anticipated. Significant opportunities therefore exist for future research which can explore the adoption of resulting collaborative, wraparound approaches across the service system and the impacts of doing so, including any subsequent adoption of the proposed Framework.
More specifically, although case files provided insights into the experiences of siblings, the ultimate limitations on the research team’s capacity to engage directly with young people confirms examination of sibling experiences as a direction for future research. The research also suggests that the relationship of wider adverse childhood experiences to the use of AVITH, including bullying and familial grief, should be an area of future research attention. Given that practitioners identified challenges – and opportunities for more effective collaboration – related to Child Protection involvement in families’ lives, this is also a clear area in need of future focus. Further research could potentially be conducted in the context of broader work around improvements in Child Protection authorities’ capacity to identify and respond to adult perpetration.
Crucially, the relationship of current as well as prior experiences of adult-perpetrated DFV in the context of AVITH should be a significant focus of future research, avoiding the common default of describing the relationship of trauma to the use of AVITH as predominantly a historical one. A failure to identify current risk from adult-perpetrated DFV may result, in part, from the lack of young people’s voices contributing to research. It is therefore crucial that future research include opportunities for young people to share their experiences safely and in their own words.
Conclusion
The WRAP around families project was designed to be a targeted investigation into the service response to AVITH as a direct follow-up, or “coda”, to a recommendation from the PIPA project. As such, it had very limited resourcing and was expected to be conducted as a brief inquiry, or stocktake, into the extent to which service responses had progressed since the PIPA project, as well as to provide a Framework which could help to accelerate this progress further. The impacts of COVID-19, however, had flow-on effects for the project which expanded both its timeframes and scale on the one hand, while limiting its scope on the other.
Despite these challenges, however, the findings and Framework resulting from the research potentially come at a more salient time than would have otherwise been the case. Increased investment and practice development, as well as considerations around training, will position policymakers and practitioners well to be able to consider next steps. This is important because, as practitioners contributing to the refinement of the proposed Framework explained, “We have made some important progress, but the Framework is the ‘where to from here’.” Just as vitally, the research team hopes that the Framework offers policymakers and practitioners across multiple jurisdictions a blueprint for how they might consider reform in this area – no matter at which point along the path to more effective service responses to AVITH they may be.
Part 1:
Introduction and context
“WRAP around families experiencing AVITH: Towards a collaborative service response” (the WRAP around families project) was designed as a brief and targeted study. Its specific aim was to develop a framework for holistic, evidence-based practice in response to the complex issue of adolescent violence in the home (AVITH).
Rather than being a study exploring the wider phenomenon of AVITH and its manifestations, therefore, the WRAP around families project was designed to function as a “coda” in direct response to a recommendation of the earlier, more substantial PIPA project (Campbell et al., 2020). This recommendation was that appropriate service interventions in AVITH require wraparound, collaborative responses that address risk and needs across the whole family, rather than responses directed predominantly at a young person’s behaviour. The PIPA project highlighted the complexity of needs across many families who present to services and may be experiencing AVITH, but who have had either very little, or largely ineffective and damaging, prior service support. The PIPA project also highlighted the way in which young people’s perspectives and their experiences of service interventions – both effective and otherwise – are not frequently documented in literature (Campbellet al., 2020), as emphasised more recently by Condry and Miles (2021) in the UK context.
The WRAP around families project therefore originally aimed to address a gap in what young people and their families identify about their own needs, as well as a gap in understanding about co-occurring issues and wider service involvement which may prevent AVITH-focused interventions from being effective (Boxall, Morgan, Voce & Coughlan, 2020; Moulds et al., 2019). The research also aimed to contribute to evidence about the role of pre-existing trauma on parental capacity to address AVITH, highlighting the need for interventions which support recovery from adult-perpetrated intimate partner violence (Burck, 2021). Further, it aimed to explore the needs of children experiencing AVITH, with literature describing evidence in this area as particularly “scarce” (Perkins & Grossman, 2020; Perkins et al., 2021).
In particular, however, the WRAP around families research aimed to identify current system barriers to effective practice which can address the complex phenomenon of AVITH, as well as to surface the enablers which may contribute to more consistent and collaborative practice in the future. The research aimed to move practice and policy towards a considered and coalescing understanding of AVITH, given the uncertain position that it currently appears to occupy within the wider gamut of policy concerning violence against women and children. Specifically, therefore, the WRAP around families project was intended to function as a targeted “deep dive” into the community-based service response to AVITH, whereas the PIPA project’s predominant focus was the legal and wider system response.
With a focus on the aims described above, the research posed the following questions.
Research questions
- What are the co-occurring issues which present in young people and families experiencing AVITH, and prior experiences of service support to address these needs?
- What are the co-occurring issues or experiences specific to victims and survivors of AVITH, including mothers and siblings, which may be going unaddressed in standard AVITH interventions?
- What are the particular family needs which may prevent AVITH interventions from being effective?
- How are practitioners and services currently working together to address these issues in the context of AVITH responses?
- What are the system barriers and levers to collaborative ways of working for services and practitioners responding to AVITH?
The research was informed by two primary strands of data, the first being a qualitative exploration of community-based service responses through focus groups with practitioners in Victoria, a jurisdiction with an increasing focus on support for evidence-based service responses to AVITH. The second strand involved a mixed-methods case study approach examining a response to AVITH which was funded by the Commonwealth Department of Social Services and developed by Drummond Street Services (DS), a large community service organisation working with vulnerable families and marginalised cohorts in metropolitan Melbourne, as well as one large regional area in Victoria.
Part 2 of this report aims to address the first three questions through the practitioner focus groups, interviews with parents who were clients of the DS program, and examples of client complexity and needs evident on the case file review. A significant focus addresses the final question regarding barriers to collaboration, such was the substantial volume of challenges evident across the research.
Signs of promising practice are then explored in Part 3, which focuses primarily on the fourth question of how services and practitioners are working together to address these challenges. It does so by examining the complex and nuanced ways of working described by practitioners and services, and then through examples from the case files, signalling where conceptualisations and service design needs to be directed. Rather than including recommendations which may not be relevant in different service contexts, or which can so often become siloed in policy or funding environments, Part 4 of the report then discusses and proposes the Collaborative Practice Framework which was the primary objective of the research. This Framework is designed to be flexible and client-centred rather than prescriptive, reflecting the overarching emphasis of the research findings. It includes practice examples to guide policymakers and practitioners in applying the Framework totheir own particular context.
Methods
Literature scan
To support development of the research aims and methodology, a brief scan of relevant peer-reviewed and grey literature built on the literature explored in the PIPA project (Campbell et al., 2020). Important to note, this was not intended to function as a systematic or even standard literature review. Rather, it focused on evidence which became available in and following 2018 to explore considerations around service responses, including positive and effective interventions, such as collaborative, holistic and whole-of-family approaches. Other literature outside these parameters was referred to as appropriate, but not reviewed in depth. The scan was conducted in the first half of 2021 and then updated on a limited basis in 2022 using searches of the following databases:
- Attorney-General’s Information Service (AGIS Plus Text)
- Australian Criminology Database (CINCH)
- Australian Criminology Database – Aboriginal and Torres Strait Islander Subset (CINCH – ATSIS)
- Health Issues in Criminal Justice (CINCH-Health)
- Australian Public Affairs Full Text (APAFT)
- Australian Public Affairs Information Service – Aboriginal and Torres Strait Islander Subset (APAIS-ATSIS)
- Australian Family & Society Abstracts Database (FAMILY)
- Australian Family & Society Abstracts Database – Aboriginal and Torres Strait Islander Subset (FAMILY-ATSIS)
- Families & Society Collection
- ProQuest
- Google Scholar.
Boolean logic was used to connect and combine multiple key terms. The first search applied a data parameter for literature from 2018 onwards combining the terms “adolescent”, “adolescent-to-parent”, “child”, “child-to-parent”, “juvenile”, “youth”, “sibling”, “teen”, “teenager” and “filio” with “violence”, “family violence”, “abuse”, “conflict”, “violence in the home” and “aggression”. A second search, with a date parameter from 2010 to 2021, combined these terms with descriptors of intervention types, including “therapeutic”, “family systems”, “family-focused”, “case managed”, “interagency”, “collaborative”, “participatory”, “integrated”, “coordinated”, “holistic”, “multi-disciplinary”, “whole-of-family”, “wraparound”, “trauma-informed”, “intergenerational” and “restorative”. Non-English publications were not reviewed.
Studies that related to “parent-to-child abuse” and “child sexual abuse”, “adult intimate partner violence” and “general youth offending” were not included in this initial search, as the objective of the scan was to identify, describe and understand literature specifically regarding the use of violence at home by adolescents, as well as specific service responses to this phenomenon. This included some consideration and description of the quality of each study reviewed. Titles and abstracts were read to determine relevance and, following that, complete texts. Further research was found by reviewing the reference lists of key articles. Sources unavailable in English were not searched for or reviewed.
Relevant considerations from this literature scan feature throughout the Context and Discussions sections in this report, as well as the Findings sections where specifically relevant.
Qualitative research with practitioners
As noted above, the first component of primary data collection was intended to be a very targeted exploration of the contemporary service landscape in Victoria. The aim of this component was to provide breadth and context for the companion case study component and therefore it was designed to have a broad focus on how the service system was responding to AVITH at the time, including the extent to which services were working together to wrap around families, barriers to collaborative practice, and service gaps. Specifically, it was designed to update findings from the PIPA project in relation to service provision, given that the data collection relevant to Victoria for the PIPA project occurred in 2017.
The expectations when the research was originally designed and resourced was that up to 40 practitioners would participate. This group was anticipated to include practitioners working across the relatively limited number of AVITH-focused interventions operating at the time of the original study design, as well as practitioners in legal, court, restorative justice, mental health and alcohol and other drug (AOD) contexts.
Following the design of the research, however, the Victorian Government provided an injection of funding to increase capacity for AVITH-focused interventions. This was described as a response to a recognised increase in rates of AVITH during Victoria’s extended lockdown periods (State of Victoria, 2020). Although limited in its parameters, this additional resourcing contributed to a rapid growth in the number of practitioners working in this field in 2021, with the bulk of additional funding being provided to large community-based organisations already delivering therapeutic recovery support to women and children who had experienced domestic and family violence (DFV). As a result, the scope of service providers from which the research team could recruit expanded. Despite the limits of the study’s original design and funding, the research team saw this as an opportunity to explore and compare different service and organisational approaches. Accordingly,recruitment efforts were focused on those services which had previously been funded by the Victorian Government to deliver AVITH-focused interventions, as well as those which the government advised had received the additional funding at the start of 2021.
In addition to these specific providers, the research team approached practitioners providing legal assistance to children and young people; practitioners working in acute and community-based mental health services; and practitioners working in AOD-focused services as a way of testing the extent to which themes were being seen outside the dedicated program environments. This included practitioners participating in an informal AVITH Collaborative Network, which emerged in Victoria during 2021 and met online on a monthly basis. This network continued to function as a reference point to test findings from the current study from a practice perspective.
Participants were recruited through their employer organisations, with participant information and consent forms then distributed to practitioners. An online consent option was provided to enable an efficient opt-in to the research, given that so many practitioners were working from home during this period. Online focus groups were then conducted on an organisational basis, so that practitioners could speak freely about any challenges that they had experienced in developing and/or adapting responses to AVITH, particularly where these were emerging responses. Because indications of consent went straight to the research team, employing organisations were not aware of which individual practitioners participated.
To note, the initial project timeframes and resourcing – and associated targeted study focus – meant that the research team did not seek to involve statutory agencies in the research, given the additional ethical approval and organisational constraints. Equally – and crucial to note – Aboriginal community-controlled organisations (ACCOs) who had either previously or more recently been funded to deliver culturally specific interventions had very limited capacity to participate at the time of initial data collection, such was the significant additional demand on these services during Victoria’s extended lockdown periods, as well as the imperatives on ACCOs to deliver direct support to communities during this time. Because of this, the data collection period was “paused” to keep the window for participation open. Four practitioners from ACCOs delivering AVITH-focused interventions ultimately participated in the research in the middle of 2022.
Despite the additional demand facing all services responding to family safety during Victoria’s extended lockdowns – as well as the compounding challenges of providing support to vulnerable clients while working from home or with rolling illness once lockdowns were lifted – the research team were delighted that 75 practitioners participated in the focus groups within the extended timeframes. Important to note, as specific challenges related to collaboration between services and Child Protection authorities emerged across the findings, an invitation to test these findings was extended to senior Child Protection stakeholders. Given that this occurred during 2021 and across Victoria’s extended lockdowns, it is understandable that this invitation did not receive a response.
Case study component
Noting that there is little consensus on a single case study method (Simons, 2012), the label “case study” in the project referred to the in-depth examination of a particular collaborative response to AVITH being offered by DS. In this case study, the research team aimed to engage with a range of data to explore the area of study (e.g. Mack et al., 2005) and then test this through the knowledge and perspectives of practitioners, as well as the perspectives of people who had used the program.
Given the distinctive features of the particular program being investigated, the research team did not expect to be able to generalise the findings, as might occur in relation to other case studies (Gerring, 2004). More specifically, we anticipated that the findings would be instructive in relation to the emergence of innovative responses or promising practice, which the current study confirmed. The value of a case study method for investigating and evaluating innovative programs is observed by Simons (2014), who argues that case studies are useful to “understand and represent complexity, for puzzling through the ambiguities that exist in many contexts and programs and for presenting and negotiating different values and interests in fair and just ways”
(pp. 2–3). Flyvberg (2006) also argues that areas of inquiry are strengthened by in-depth case studies of best practice or promising examples.
Client interviews
The case study component originally aimed to include in-depth interviews with six to ten young people and eight to twelve adult family members. The interviews were designed to explore their experience of the DS program and the broader service system; the extent to which the program and the broader service system were meeting their needs; what responses or types of support may have been missing from either the program or the wider system; and what might have benefitted them individually and as a family.
Family case conferences, which occurred as part of the case study program between all practitioners working around the family, were used as a screening mechanism to assess whether it was safe and suitable to invite one or more members from a particular family to participate in the research. Where a client was assessed as eligible, the practitioner explained what the research involved and confirmed with the client at a later date, such as at their next appointment/session, if they would like to participate. The practitioner confirmed with the client whether they were able to attend the service premises for the interview, or whether a phone or video interview would be safe and appropriate. The three participating parents all preferred a phone or online interview, which practitioners deemed safe in their particular circumstances. At the time that they confirmed the interview time and location, the recruiting practitioner confirmed with the client that thepractitioner would also be available following the interview to provide support and debriefing by phone.
Because the data collection period ran from mid-2021 to mid-2022, through Victoria’s protracted sixth lockdown and the subsequent waves of the COVID-19 Omicron subvariants, there were significant limitations on the type of work that DS could conduct with clients. This was particularly the case with young people, who were generally harder to engage online or over the phone, and where practitioners had significant concerns about client privacy and safety during therapeutic work. This ultimately meant that recruitment to the interview component of the research was extremely challenging, with no young people expressing interest and only three parents ultimately participating in the research (three additional parents initially expressed interest but circumstances at the time made it too difficult or unsafe for them to participate). In particular, these three parents had not experienced much contact between DS and their children, two because of the impactsof COVID-19 on face-to-face engagement and another because of issues around parental consent, which is explored in the report.
As a result, findings from the three interviews with parents are featured throughout this report as illustrative only, where they echo other findings and themes. The interview findings predominantly relate to the limitations of the wider service response and, in particular, the ongoing impacts of adult-perpetrated DFV, as well as how these impacts interact with their experience of service systems. To an extent, however, they highlight the need for wraparound responses like the DS program, where circumstances enable a program to work with children and young people.
Case file review
The file review aimed to examine the case files of approximately 40 families engaged with the DS Family Violence and Young People program in relation to their experience of AVITH. This program purposefully takes a whole-of-family approach which enables different family members to engage with the program on a separate case file from the young person. This was described to the research team as taking a strengths-based and person-centred approach, particularly where a young person identifies that they would feel more comfortable engaging without the presence of their parents. Taking this approach allows for the consent of the young person (and of parents where the young person is under 16 years old).
The case file review aimed to examine:
- families’ demographic data, risk factors and co-occurring needs
- where and how families experiencing AVITH were presenting to services
- family structure and dynamics, including multidirectional use of violence
- the nature and extent of prior service contact and engagement, including in relation to prior experiences of trauma and violence
- how prior experiences of trauma and violence may be impacting on the family, including where mothers’ experiences of violence may be impacting parenting behaviours
- the under-examined needs of siblings experiencing AVITH and its multiple impacts across the family structure and relationships.
The research team was ultimately provided with case files in relation to 39 families engaged through the program. Six were then excluded once initial analysis indicated that they did not demonstrate sufficient engagement with the family as a result of the same COVID-19-related impacts described in relation to the client interviews, or for other reasons.
Ethical considerations
Ethical approval for all components of the research was sought and received from the Victorian Department of Justice Human Research Ethics Committee (CF/21/5126). Approval from this committee was sought because of the vulnerability of clients in the DS program and the potential for any young people participating in the case study to be a respondent to a civil protection order and therefore formally a client of the justice system.
Focus groups with practitioners
Specific to the focus groups, the research team recognised that practitioners working in this area may experience vicarious trauma as a consequence of empathetic labour. The research team also recognised the low risk that some practitioners participating in the research may have lived experience, including histories of trauma or experiences of DFV. Accordingly, the research team designed the project to minimise the potential to impact practitioners in negative ways by:
- ensuring that interview questions did not direct or encourage practitioners to recount specific incidents or histories of trauma
- redirecting the discussion in the event that a particular question or topic was resulting in distress, including by reframing the discussion to focus on client strengths and factors contributing to positive client outcomes
- using other techniques as required, including offering to take a break or to reconvene the interview at a later time.
While the research team have extensive experience in trauma-informed approaches to data collection, it is important to note that there were no indications of negative experience for participants across any of the focus groups. Rather, the overwhelming assessment of their experience of participation was expressed by practitioners as extremely positive, with regular indications of appreciation for the opportunity to share reflections and to do so in a collegiate environment. This was particularly because these opportunities had not been a common feature of their experience in recent years, such was the focus on responding to caseloads and service demand compounded by the impacts of COVID-19.
These reflections from practitioners are consistent with contemporary methodological observations about the benefits of co-production of evidence with practitioners and service providers (Breckenridge & Hamer, 2014; Coutts, 2019; Simons, 2012), also positioning the research more effectively to be translated to benefits in policy and practice (Belzile & Oberg, 2012), which was the reason for the selection of focus groups as the method for this component of the research. To note, practitioners were given the opportunity to participate in an individual interview, including as a way of ensuring that their decision to participate was not communicated either to colleagues or to their employer organisation, but all preferred to discuss their evolving practice in a group setting. Given this, the research team adopted the approach of assigning each practitioner an identifying number, rather than identifying the type of service in which they worked. Thiswas to minimise any chance of them being identified by their employing organisation or re-identified by others who had participated in that particular focus group.
Client interviews
The research team’s approach to qualitative research with vulnerable participants is to recruit through agencies which are already providing them with support.
This is because these practitioners have a sufficient understanding of clients’ needs and circumstances to determine whether it is safe and appropriate to seek to recruit a client at a particular point in time. This includes, for example, not seeking to recruit a client where they have a matter before a court at that time; they are experiencing increased family violence risk; they are at risk of re-traumatisation; or they are otherwise experiencing significant instability, such as homelessness. Risk factors were considered individually and at a whole-of-family level. These methods of recruitment ensure minimal risks of potential harm to the participant.
Benefits of recruiting this way also include practitioners being able to identify additional supports that may facilitate participation in research for people with complex needs – thereby minimising the extent to which marginalised cohorts are excluded from research. This method of recruitment also ensures that participants have a trusted practitioner from whom they can receive debriefing, rather than having to re-tell their story to a stranger. The research team has designed this methodology in consultation with practitioners over the course of multiple studies as a way of ensuring that participants who may not otherwise be included in research have the opportunity to do so, while feeling comfortable about declining the invitation where they have developed a rapport with a worker but have concluded their program engagement.
Interview questions were designed to focus on a participant’s experience of the DS program and wider service system, as well as their support needs, rather than their experiences of AVITH or sources of trauma. This reflected the research team’s trauma-informed and strengths-based approach and an emphasis on conducting research with participants as experts in the service system, rather than as passive subjects. That said, all three parents volunteered extensive histories of trauma related to adult-perpetrated DFV, a theme which had an impact on every aspect of their service interaction and the most substantial theme to emerge from the client interviews, as discussed throughout the report.
At the conclusion of the interview, the principal chief investigator (PCI) conducting the interviews inquired about further support needs, and one participant expressed an interest in debriefing with a practitioner and reconnecting with the DS program, which the PCI arranged. All participants expressed an appreciation for the way that the interviews had been conducted and for the opportunity to have a voice, with one parent explaining, “I would really love to see some change for other people going through this” (Parent 1). Participants were all provided with a voucher as a thank you for their time and will all be provided with a copy of the research upon completion. They were also reminded that they could request a copy of the transcript of their interview from the PCI at any time.
Case file review
Quantitative and qualitative information was extracted from existing case files via two case file review tools developed for the study, which related to the program’s primary and secondary clients. Information collected did not include names, dates, unique client identifiers or other information that was likely to make the person whose information was being collected identifiable. Different family members were referred to by different case numbers but were linked in the data provided to the research team. Information was only extracted from the case files of clients who had consented to their information being used for research and evaluation purposes. Data was collected by Centre for Family Research and Evaluation (CFRE) researchers who came within the scope of DS’s client consent processes while still being sufficiently independent from service provision as to mitigate the risk of reporting bias.
Only de-identified data, as captured through the case file review tools, was shared with the broader research team. To reduce the potential identifiability of qualitative data, the case file review tool included instructions to exclude information which, based on the relevant CFRE researcher’s judgement, would likely have the effect of making the client identifiable. Information was only recorded using the approved tools, with no additional information recorded. Data analysis was then tested with the CFRE researchers through formal data reflection sessions to ensure that the way in which data was analysed was consistent with DS’s informed consent processes. This process also enabled the wider research team to test wider findings and explore data gaps.
Data analysis
Focus groups
Anticipating the benefits of co-production of evidence noted above, focus groups were the preferred approach. Because of the analytical value of discussions and interactions between participants, as well as the fact that focus groups are an efficient way of accessing a significant number of participants (Peek & Fothergill, 2009), the research was designed as a genuinely collaborative endeavour to understand the current response to a policy and service challenge which is yet to receive a consistent intervention.
While the research team recognised that a single data type may be a potential limitation, they also anticipated and observed an immediate and organic process of data integrity-testing occurring in many focus groups, where participants disagreed with each other or, conversely, extended or tested a point, drawing on their particular expertise or location in the system. The research team also actively included memo-ed reflections of group dynamics as a valuable dimension of the data (Pösö et al., 2008; Warr 2005). This included noting that group dynamics were impacted by a range of organisational and systemic imperatives outside the relationships within the group.
Focus groups were recorded via Microsoft Teams, with transcripts then downloaded and checked against the audio recording for accuracy. Transcripts were analysed thematically using the qualitative analysis software NVivo, with data coded in accordance with 22 nodes. These nodes were tested against memo-ed reflections taken by different members of the research team and workshops with the PCI for reliability, as well as being checked by the PCI in a manual review of the transcripts. Emerging themes from the coding were then further tested with the AVITH collaborative network, mentioned above, for practice relevance, as well as with the focus group participants in the context of their participation in the workshops that were held to inform the development of the Collaborative Practice Framework.
Focus group participants were given an individual number during the coding to ensure that their contributions could be tracked. These numbers have not been linked to organisational identifiers to limit the extent to which participants could be re-identified, particularly as many contributions were quite critical of the funding environment that was in operation at the time.
The analysis was informed by broad feminist theory and critical theory (Fraser, 1985; Wellmer, 2014), with the research team maintaining a constant interrogation of choices of terminology and assumptions at the inception of and throughout the research, as well as the conceptualisations about AVITH to which services were attempting to respond. This critical lens extended through to the nuance incorporated and reflected in the Collaborative Practice Framework that was the ultimate product of the research.
Client interviews
As noted above, three clients participated in interviews, which lasted an average of 90 minutes each. Interviews were recorded, downloaded and transcribed before being analysed and coded, ultimately resulting in 11 nodes. The predominant nodes were the impacts of trauma from past adult-perpetrated DFV as well as ongoing systems abuse by a perpetrator parent, followed by support needs of young people and negative prior service interaction. The relatively small number of nodes and their nature resulted from the limits on these particular clients’ engagement with the DS program, despite the fact that DS had been able to engage more extensively with the 33 families whose case files were reviewed.
As a result, the majority of the data from client interviews is featured as illustrative in Part 2 of this report, which focuses on practice and system challenges, given that they relate to clients’ experiences of prior service interaction, as well as what their hopes would be for interaction in the future. This was considered to be a more appropriate and ethical use of the contributions of these participants than combining them with the findings of the case file review, which was predominantly focused on the various ways in which DS had been able to work effectively with other clients.
Although this was not the original aim of the study, the ultimate result provides a useful contrast in terms of the lived experience of those seeking to access support for their experiences of AVITH.
Case file review
DS provided the external research team with 39 case files. Of those 39 files, six were ultimately excluded once initial analysis indicated that minimal engagement by the family or other factors limited the extent of information available for full analysis and comparison. In total, the case file review included files related to 33 families – with each “file” including a mastercase and secondary cases linked together.
The breadth of data within each case file varied for several reasons, including the extent of engagement that families had with DS; the variation in record-keeping practices by individual DS practitioners; and variation in the number and nature of sessions held between a DS practitioner and a family. For example, within the 33 files reviewed, the number of sessions held between DS and the client ranged between two and forty-one, where the young person was engaged with other support (e.g. a psychologist); where DS may have been unable to make contact with the family again following intake; or, in some instances, where the violence had improved after only a few sessions and the case was closed.
A database was created, with basic descriptive statistics extracted from the quantitative component of the file review tools and recorded using Excel. This was to give context to the primary focus of the review, which was to conduct a qualitative exploration of client presenting needs and the corresponding DS approach to practice in response to these needs. Data from the qualitative component of the file review tools was analysed thematically using the qualitative analysis software NVivo, with data coded in accordance with five primary nodes or themes, and 15 sub-themes. Two further manual reviews were conducted to cross-check for error or duplication.
Additional project oversight
In addition to the collaborative approach taken by the research team across the focus groups, the research was also overseen by an advisory committee with representatives from Safe and Equal (formerly Domestic Violence Victoria), No to Violence, the Children’s Court of Victoria, the Commission for Children and Young People, Youthlaw, Victoria Legal Aid, and Djirra (a service providing family violence legal advice and prevention services to Aboriginal women and children). Djirra had limited capacity to attend meetings, however, because of the ongoing impacts of COVID-19. The research team also explored opportunities for a parent/carer or young person with lived experience to be involved in the advisory committee. Potential participants were approached through three service pathways once considerations around their safety were assessed but, ultimately, all decided that they were not yet comfortable acknowledging their experiences in a group setting. Thispotentially reflected wider challenges in this area in terms of the particular stigma that people who have experienced or used AVITH may feel and the impacts of this on their capacity to receive support.
Context: An evolving service environment
The following section provides a brief outline of the extent to which AVITH is recognised in literature. It also contains a brief discussion of wider service contexts and growing recognition in the literature that responses which address need and wrap around a whole family are required. Finally, the section outlines the evolving service and policy landscape in Victoria to provide context for the subsequent findings. The service landscape, as with the legal response, is dictated to an extent by the broad definition of family violence in Victorian legislative and consequent policy settings, which have captured use of family violence by a range of family members since 2008.
Conceptualisation and recognition in literature
The varying conceptualisations and definitions of AVITH across literature make assessing prevalence and dynamics a challenge, with researchers highlighting the importance of establishing consistency in understanding what constitutes AVITH (Peck et al., 2020).
Different jurisdictions, services and studies adopt varying age ranges when assessing and defining AVITH, generally starting at 10 or 12 years and ranging up to 17 or 25 years, with further variation in whether the context is legal, clinical or community based (Campbell, et al., 2020). Studies have also highlighted the value of maintaining visibility of the behaviour of pre-adolescent children as a predictor of behaviour in adolescence (Rutter, 2020), while a recent Australian study found that, of a sample of 435 university students aged 18 to 25, one in seven had used harm against their parents in the past 12 months (Simmons et al., 2020).
A frequently cited definition by Cottrell (2001) defines AVITH as an abuse of power perpetrated by adolescents against their parents, carers and/or other relatives including siblings, which “occurs when an adolescent attempts to physically or psychologically dominate, coerce and control others in their family” (page 3). Holt subsequently specified a requirement for a “pattern of behaviour that produces harmful outcomes [emphasis in original]” (Holt, 2016, p. 2) rather than an isolated incident.
A more recently developed definition by Pereira and colleagues builds on these definitions and signals an emerging consensus as to the circumstances and behaviours that they suggest should be within scope:
Repeated behavior of physical, psychological (verbal or non-verbal) or economic violence, directed toward the parents or the people who occupy their place. Excluded are one-off aggressions that occur in a state of diminished consciousness which disappear when upon recovery [sic] (intoxications, withdrawal syndromes, delirious states or hallucinations), those caused by (transient or stable) psychological disorders (autism and severe mental deficiency) and parricide without history of previous aggressions. (Pereira et al., 2017, p 220).
We note, in particular, the specific exclusion suggested by Pereira and colleagues of what they term “autism and severe mental deficiency”. This is particularly relevant when considering prevalence and dynamics given that young people with disability are currently captured within the rates of AVITH reported in Victoria because of the operation of the Family Violence Protection Act 2008 (Campbell et al., 2020). Accordingly, it is important to acknowledge that policy contexts and policing practices further impact prevalence estimates (Kehoe et al., 2020). For example, studies indicate that young people identified as using AVITH in legal settings appear to have more entrenched behaviour and histories of adverse childhood experiences compared to young people whose parents have the resources to opt for private clinical support (Loinaz & de Sousa, 2020).
Recent Australian research also confirms that young people in contact with criminal justice systems for use of AVITH have backgrounds of particularly entrenched disadvantage, including young parenthood, histories of child removal, mental ill health and disability. Young people from Aboriginal and Torres Strait Islander backgrounds featured to a notable extent in the data included in an important recent Australian study (Douglas & Walsh, 2022).
Legal system samples are commonly used to measure AVITH prevalence and one example – a study of police data across four Australian states – indicated that between 1 and 7 per cent of DFV matters reported to police involved AVITH (Moulds et al., 2019). An examination of justice data for the Royal Commission into Family Violence (RCFV) reported that approximately 10 per cent of DFV police reports involved AVITH (State of Victoria, 2016). Similarly, between July 2019 and June 2020, around 10 per cent of individuals recorded by Victoria Police for DFV incidents were between the ages of 10 and 19 (Crime Statistics Agency, 2020).
The PIPA project, however, found that variations contained in the legal and court files reviewed suggested that justice data did not necessarily provide useful measures, because young people who were identified as respondents through the Victorian protection order response should arguably be excluded from the definition of AVITH by Pereira and colleagues because of cognitive impairment, current victimisation or behaviours not meeting the legislative definition of DFV (Campbell et al., 2020). This complicated rather than clarified questions about prevalence, at least in the Victorian context.
Under-reporting is also a compounding factor, with AVITH described in studies as one of the most significantly under-reported forms of DFV (Campbell et al., 2020; Fitz-Gibbon et al., 2018; Kehoe et al., 2020). Kehoe and colleagues attribute this to “a lack of community acknowledgement and understanding”, as well as “parental guilt, denial, self-blame, stigma and shame, and the minimisation of the abuse as being ‘typical’ adolescent behaviour” (Kehoe et al., 2020; Meyer et al., 2021). Despite the effect of under-reporting, some international studies indicate that AVITH is a growing phenomenon (Contreras et al., 2019), resulting in associated investment in assessment instruments.
Extensive evidence across different samples and settings (Pagani et al., 2004; Routt & Anderson, 2016) describes prior experience of adult-perpetrated DFV, both indirectly and directly, as arguably the most significant contributor to a young person’s use of AVITH (Armstrong et al., 2018; Beckmann et al., 2021; Campbell et al., 2020; Contreras & del Carmen Cano, 2016; Elliott et al., 2017; Holt, 2013; Holt & Retford, 2013; Howard & Holt, 2015; Ibabe et al., 2013). The presence of victimisation features in studies across different settings, with this experience among young people who use AVITH found to be higher than in comparable cohorts of young people (Contreras & del Carmen Cano, 2016).
Evidence links to theories of intergenerational transmission of violence (Kwong et al., 2003; Meyer et al., 2021) and “social learning”, whereby young people observe behaviours used by adults in their lives and replicate them (Margolin & Baucom, 2014) – for example, once a perpetrator father has been removed or the family has separated. Other explanations include resistance (i.e. acting out towards a perpetrator) or protection (i.e. trying to protect an abused parent; Margolin & Baucom, 2014), or observation and replaying of behaviours used by older siblings (Campbell et al., 2020).
Interwoven with the impacts of social learning is evidence of the ways that adult perpetrators of DFV deliberately undermine relationships between mothers and children (Bagshaw et al., 2011; Brown, 2006; Burck, 2021; Burck, et al., 2019; Maher et al., 2021; Meyer et al., 2021; Katz, 2019; Spearman et al., 2022; Thiara & Humphreys, 2015), including post-separation. Examples involve systems abuse through the family law and Child Protection processes; using children as a vehicle for abuse tactics; and otherwise using shared parental responsibility and an ongoing, “absent” presence to undermine the mother–child bond or a child’s access to services (Campbell et al., 2020; Thiara & Humphreys, 2015). An increasing volume of literature therefore seeks to make the gender of victims and survivors far more visible (Armstrong et al., 2021; Burck, 2021; Meyer et al., 2021) and, accordingly, support women’s recovery (Burck, 2021; Paterson, et al., 2002).
This is particularly important to note when considering the gendered nature of AVITH. While research highlights that young people using AVITH are more likely to be male than female (Campbell et al., 2020; Condry & Miles, 2014; Holt, 2016; Howard, 2015; Routt & Anderson, 2011), the gendered nature of the use of AVITH is less conclusive and perhaps more complex than evidence clearly indicates in relation to the gendered nature of adult-perpetrated DFV (Australian Domestic and Family Violence Death Review Network & Australian National Research Organisation for Women’s Safety, 2022).
For example, a recent prevalence study indicated that respondents identifying as female were more likely to self-report using AVITH than young males (at 23% of females compared with 14% of males; Fitz-Gibbon et al., 2022). Here it is worth noting that young women may be more likely to self-report any kind of violence compared with males, as suggested in the context of wider evidence regarding adolescent dating violence (O’Keefe, 2005). Other research has also noted use of serious physical violence by young females in the context of histories of complex and sustained trauma, with participating practitioners in this particular study suggesting that young girls are more likely to be identified and met with punitive responses where they break with gendered norms (Campbell et al., 2020). Conversely, other studies have suggested that parents may be more likely to report the use of AVITH by young males given the perceived risk of physical harm (Miles &Condry, 2016).
Despite this complexity in terms of the demographics of who is using AVITH, it is perhaps the gendered nature of victimisation – with the vast majority of victims and survivors being mothers – that is a more relevant area of focus for service provision and policymaking alike. This is in part because, as noted above and discussed in some of the below examples, available evidence points to the value of interventions which support mothers and their children in healing from trauma and in working towards safety for all.
Examples of approaches interstate and internationally
A range of programs have been developed to respond to AVITH in both the Australian and international contexts, with the following discussion providing examples of contrasting approaches. This sample is by no means intended to be exhaustive, acknowledging the substantial literature exploring a range of interventions in a number of diverse jurisdictions, particularly the United Kingdom and Spain (Holt, 2016).
Group work with parents and young people
The Step-Up model, established in the United States in 1998, involves group work interventions with court-involved young people and their parents, and has become influential internationally (Gilman & Walker, 2020; Routt & Anderson, 2016). The Step-Up program uses a restorative approach where the young people are encouraged to take responsibility and accountability for their use of harm while also repairing damaged relationships and safety planning (Routt & Anderson, 2011, 2016).
In their evaluation of the program, Gilman and Walker (2020) looked at the outcome of general and DFV-related recidivism within 12 months of program commencement and found that participation was associated with a reduction in future court referrals overall, but not specifically for DFV-related offences, after controlling for variables. The authors observed, however, that previous evaluations – although not as methodologically rigorous – have found some evidence of reductions in ongoing use of violence in the home (Gilman & Walker, 2020). It should be noted here that eligibility criteria for the US iteration of Step-Up include that the young people have had some involvement with the criminal justice system; are not currently experiencing, or have not in the past experienced, violence from the parent towards whom they are currently using violence; and that all participants (young people and parent) do not have a current substance abuse problem or anuntreated mental health issue (Gilman & Walker, 2020).
As is evident from current literature, as well as the findings from this project, many instances of AVITH involve young people being both a victim and survivor and using violence, and many families experiencing AVITH also experience substance abuse and mental health issues (Campbell et al., 2020). This suggests that, unless modified to accommodate families experiencing multiple complexities in addition to AVITH, the US Step-Up program may not be sufficient as a response to AVITH if delivered in isolation and would need to be linked to more holistic and integrated responses.
Another well-established program working with parents and young people together is the Respect Young People’s Programme (RYPP), an intervention for families where children or young people aged between 8 and 18 use harm towards the people close to them, particularly their parents or carers. Delivered by the Respect agency in the United Kingdom, the program describes itself as working with young people and their families; encouraging everyone to take a role in stopping the abuse; and learning respectful ways of managing conflict, difficulty and intimacy.
The RYPP is currently delivered across a number of local authorities and police and crime commissioner areas in England. The RYPP involves weekly structured sessions for 18 weeks (nine sessions with the young person, seven sessions with the parents and two sessions with the family together), with the sessions lasting up to an hour. Using a multi-modal design and combining a range of theoretical models with primarily a cognitive behavioural approach, the program also aims to influence particular features of the young person’s environment which may contribute to use of harm. Prior to the group work sessions starting, Respect offers two pre-work sessions, in order to support engagement and buy-in to the program by the young people and their parents. The aim of this is also to complete a full risk assessment and ensure program suitability. Respect is also conducting work to develop appropriate interventions for young people who are neurodivergent or havecognitive impairments (Respect, 2021); while a case study of the program’s delivery during COVID found that, while young people were difficult to engage during this time, engagement by parents increased (Rutter et al., 2022)
Programs which work primarily with parents
The “non-violent resistance” (NVR) model used in the United Kingdom and the Republic of Ireland works primarily with parents and seeks to move away from blaming either parents or young people and to “take account of the challenges of parenting in the context of cultural beliefs about parenting practices, relationships between parents and children, and supports for parents and children” (Coogan, 2018, p. 170). Practitioners work with parents over the course of eight to fifteen sessions to address reversed power dynamics in the family, address the patterns of escalating violent behaviour, and focus on reducing isolation and helplessness (Coogan, 2016).
The model aims to empower parents to focus more on aspects that they can control, such as the ways that they respond to the behaviour (Coogan, 2016). Reviews and evaluations of this model, although limited in scope and sample size, have found that it generally “improves parental wellbeing, decreases parental helplessness and leads to positive improvements in the child’s behaviour” (Coogan, 2016, p. 7). Important to note, practitioners participating in these evaluations acknowledge that the use of NVR is not designed for families experiencing multiple vulnerabilities (Coogan, 2016).
The Break4Change model in the United Kingdom is partially based on the NVR model, although it incorporates interventions which directly involve young people as an additional component, teaching emotional regulation skills. Although there is no publicly available evaluation, the Centre for Justice Innovation reports that, following the program, parents feel less isolated and more confident, and have skills to address their child’s behaviour, while young people “reported having increased empathy, drastically reduced physical violence and increased satisfaction at home” (Centre for Justice Innovation, 2021).
Programs which work with mothers and sons who have experienced adult violence
The ReNew program in Queensland is a therapeutic program directed at working with mothers and their sons aged 12 to 17 who have experienced DFV from an adult perpetrator, usually a father, and are now using violence towards their mothers (Burck, 2021). The first iteration of the ReNew program was trialled in 2016, with a partnership between a family support service and specialist DFV service funded to deliver the program for a two-year pilot. The pilot used three different group work components: combined groups with mothers and young people as well as separate groups with mothers and young people, respectively (Burck, 2021).
The trial was evaluated by Griffith University, with a favourable interim report resulting in an extension of the trial. This included an external co-design process to review and build upon the existing model.
ReNew was specifically informed by evidence which shows that experiences of adult-perpetrated DFV can severely undermine the mother–child bond. The primary goal of the program has therefore been described by one of its founders as “to reduce violence in the home through strengthening the mother/son attachment after experiencing [intimate partner violence]” (Burck, 2021, p. 57). The program also recognised that mothers can feel further shamed and blamed when they are not included in any work occurring with young people (Jackson, 2003 as cited in Burck, 2021, p. 57). ReNew therefore aims to intervene at a critical juncture to rebuild respectful relationships between mothers and their sons, following experiences of DFV; to increase attachment; and to reduce the risk of young people using DFV as adults.
The research team has been informed that the current ReNew program involves two stages, as follows:
- In phase one, risk is assessed in relation to the violence used by the adult male perpetrator and the young person. The needs of the family are assessed, so that decisions can be made as to whether families should undertake a psycho-education program, either individually or in a group. Sons between the ages of 12 and 17 are eligible to participate in the psycho-education program.
- Upon completing a 10-week program, mothers and sons attend a second service for onboarding and orientation, before entering into the therapeutic element of the ReNew program, which applies an attachment and trauma focus to rebuilding relationships between mothers and sons.
- Both phases of the ReNew program can be delivered individually or via a group format. The intervention is dependent on the two services working in a collaborative partnership to deliver one cohesive intervention for mothers and sons, while providing wraparound support for other family members, such as siblings.
The implementation and delivery of the revised ReNew program is also subject to an evaluation and the research team understands that preliminary findings highlight that the program addresses an under-met service delivery need.
In particular, a strong theme from the program described by one of its designers and facilitators is enabling mothers and their sons to form positive memories and have safe interactions which can gradually rebuild their views about their relationships, as well as their views about themselves. Burck cautions against defining a young person by their use of violence, urging instead that “We, as professionals, must care for the young person while holding them accountable for the violence” (Burck, 2021, p. 66).
Programs which work with young people involved in justice settings
The KIND program was piloted in South Australia and offered a voluntary intervention to young people involved in youth justice contexts who have used AVITH or adolescent intimate partner violence. Evaluated by Moulds and colleagues (2019), the program worked with the young people and their families and partners, with a combination of group and individual sessions occurring weekly over three months and incorporating therapeutic and educational activities. It primarily focused on physical forms of abuse and incorporated cognitive behavioural therapy and some elements of acceptance and commitment therapy, as well as restorative practices, with the understanding that violence is a learned behaviour which can be unlearned through teaching new skills to manage behaviour. The program aimed to be trauma-informed, individually tailored and culturally sensitive, especially given the over-representation of Aboriginal and Torres Strait Islander people in thejustice system.
The early iteration of the KIND program only included young people aged between 15 and 18 years and who were subject to a youth justice order. It also excluded young people who had used sexual violence and who were themselves victims of DFV. The program was piloted in 2017 over seven months and received 27 referrals, although only nine young people and their families participated. Acknowledging the small sample size, the evaluation found that satisfaction, communication and coping skills within families were improved; attitudes towards violence were altered; and safety plans were able to be developed. Important to note, Moulds and colleagues (2019) also found that factors such as mental health, housing and substance use were outside the scope of the program and hampered progress in some cases. The KIND program was additionally limited, as noted above, in terms of its inclusion of participants within only a small age range and a requirement for youthjustice involvement.
The research team understands that there were significant developments made in relation to the KIND program in 2021, during which the program was revised and implemented again with broader inclusion criteria. It is now being rolled out in several sites across Queensland as well as in South Australia. An evaluation of the program is being conducted by Griffith University over the course of 2022, funded by the Australian Institute of Criminology.
Multidisciplinary or collaborative responses
Reflecting limitations to some of the programs described above, attention is increasingly being drawn to service design capable of addressing multiple needs and ensuring that barriers to engaging hard-to-reach families are addressed. This includes service design where challenges experienced by young people and/or their families who are in crisis or who are unable or unwilling to engage with services can be overcome and where basic communication and life skills can be developed to contribute to improvements in family functioning (Kehoe et al., 2020).
Given that families are likely to be experiencing multiple co-occurring issues, the literature increasingly suggests that multisystemic or “ecological” responses (Shanholtz et al., 2020), which include work with the young person, their family and their wider social environment, are most likely to be effective. As part of a community-based participatory research project in the United States, for example, Shanholtz and colleagues (2020) sought the views of court staff, as well as young people and families attending mandated DFV education classes, on helpful responses to AVITH in court settings. Participants stressed the importance of providing support across the family to help to foster more positive intra-family relationships, as well as to address wider environmental factors impacting the family (Shanholtz et al., 2020). Researchers have also emphasised the need for interdisciplinary collaboration to develop a framework for defining, measuring andaddressing AVITH across different sectors (O’Hara et al., 2017). Arguably this framework also needs to make a clear distinction between AVITH and broader DFV.
Kehoe and colleagues (2020) further advocate for AVITH to be viewed as a health, rather than a justice, issue – one that child and youth mental health services, when adequately resourced, are well placed to deliver. Drawing on findings from a 2019 study involving consultations and a co-design workshop held with key stakeholders − including a small sample of parents and young people with lived experience of AVITH − the study identified a wide range of co-occurring needs across families experiencing AVITH. In combination, these needs meant that families presented as “complex” and fell through service gaps (Kehoe et al., 2020, p. 348). By contrast, the study highlighted the need for interventions that are:
- trauma-informed, inclusive and family-focused, ensuring that all family members have access to services to address issues relating to intra-family conflict and communication, as well as other issues impacting on family health and cohesion, including school disengagement, disability, substance dependence and mental health issues
- provided under a multidisciplinary, specialist and case-managed model
- flexible and tailored, with therapeutic needs determining the nature of the response, ranging from a single session to up to 12 months.
The findings also emphasised the need for early intervention, with proactive outreach seen as essential to ensure that services are accessible for disengaged young people, or young people experiencing homelessness as a result of the violence (Kehoe et al., 2020). The establishment of a peer workforce, support groups for families and an awareness campaign to help reduce stigma and increase help-seeking were also raised as important in the design of specialist AVITH programs (Kehoe et al., 2020).
More broadly, evidence increasingly points to the importance of trauma-informed and culturally responsive interventions in contexts where young people may be using a range of challenging behaviours.
This includes therapeutic kinship care programs which can respond to and address intergenerational trauma (Kickett et al., 2019), as well as programs which can take account of the historical and interconnected nature of violence across family structures, including where sibling violence may be present (Perkins et al., 2021), where grandparents may be caring for grandchildren (Gair et al., 2019), or where relationships across generations impact on a young person’s use of violence (Shannahan, 2017).
Research continues to confirm the importance of context for young people in their families, indicating a strong connection between individual and collective experiences of marginalisation or disadvantage (Blakemore et al., 2018), in turn requiring a multisystemic response which can take account of this context in sufficiently creative, collaborative and culturally inclusive ways (Blakemore et al., 2018).
Unsurprisingly, studies increasingly suggest that positive relationships within a family offer a significant protective factor against AVITH, and that a focus on rewarding desirable and positive behaviour improves results (Beckmann, 2020; Elliott et al., 2017; Kehoe et al., 2020). The existence of certain factors, such as parental warmth, have been shown to serve a particular protective function in preventing the use of AVITH by young girls (Beckmann et al., 2021; Zhang et al., 2019).
The importance of protective factors and resources in a young person’s wider environment, such as strong attachments with teachers or peers, has also been highlighted (Beckmann, 2020; Nam et al., 2020), as has school engagement generally. In particular, evidence points to addressing external risk factors – such as reducing bullying victimisation at school – as well as supporting the development of prosocial skills in parents as significant protective factors in reducing AVITH (Espejo-Siles et al., 2020).
Factors such as these are well understood by services providing interventions in AVITH, which frequently highlight the value of working with parents to support the development of coping skills and positive ways of interacting with their child. These include seeing past the trauma of their child’s use of violence to see the strengths and positives in their child, rather than their child as just a replica of a former partner using violence.
Wraparound interventions: A research gap
Certainly, wider community-based responses are increasingly moving towards integrated responses to families experiencing marginalisation or safety concerns (McDonald et al., 2011; Robinson et al., 2011, Robinson & Miller, 2012). This focus on integrated and whole-of-family responses contrasts to an extent with the limited inclusion criteria for participants in some of the programs reviewed for this project. While several of these studies were promising in various ways, therefore, this suggests that a response which is accessible to everyone who experiences AVITH and seeks help is required, regardless of the complexity of their needs.
An example of a service which appears designed to respond to multiple issues, the YUVA (Young People using Violence and Abuse) young people’s service, operates across six local authority areas in London and provides support to young people aged 11 to 18, as well as for young people up to age 25 who have additional needs. YUVA emerged from a gap in service provision identified by services which were encountering both AVITH and adolescent intimate partner violence and which felt caught in the divide between youth-focused interventions and mainstream DFV services. Although the service does not appear to have been formally evaluated, research conducted in relation to the service notes that the majority of referrals (84%) involve young people requiring assistance with a range of issues including substance use, disability, experiences of abuse and DFV, learning difficulties, caring responsibilities, and criminal justice involvement. This is in addition tosubstantial support needs across the wider family, with a history of intra-familial violence being the most common support need (McGeeney et al., 2016, p 120).
Practitioners reflecting on the service in this particular study noted that the breadth and complexity of issues with which families were presenting demanded a flexible, holistic and joined-up approach, where services are provided in parallel across the agency and in partnership with external providers (McGeeney et al., 2016). Similarly, practitioners noted that, while the service’s location within a mainstream DFV service allowed them to draw on established ways of working with perpetrators and victims and survivors, the complexity of need in this area necessitated the development of new conceptual models and a range of skillsets across whole family structures (McGeeney et al., 2016).
One of the PIPA report’s key recommendations was for services to develop capacity to build trust and engagement over longer term periods of between six and 12 months (Campbell et al., 2020). Although this is outside the scope of many of these models, developing capability for longer term service engagement is needed to keep families and young people from falling through service gaps, particularly those who may take longer to trust a service or a practitioner when there is trauma or other complexity involved, or where system harm has compounded this harm. Outreach models were also recommended over compliance-based models to improve engagement and compliance with treatment and build trust (Campbell et al., 2020).
Further indications from the literature above point to the imperative of addressing the trauma and damaged relationships in mothers and children who have experienced adult-perpetrated DFV, including by providing opportunities to develop positive memories and an identity which is about things beyond the harm (Burck, 2021). While Shanholtz and colleagues (2020) argue that multisystemic approaches which include the whole family therefore require intensive resourcing, other researchers acknowledge the following:
Programs that do not address other issues, such as mental health, previous trauma, and family dysfunction are unlikely to have an impact on youth, with coordinated, tailored approaches targeted at the youth and their family the most effective. (Fellmeth et al., 2013 as cited in Moulds et al., 2019, p. 2)
Victorian policy and legislative landscape
AVITH has gained particular awareness in Victoria after the RCFV identified it as a growing concern. Statistics in relation to DFV police reports and highlighted by the RCFV, however, are in many ways related to the broad legislative definition of DFV in Victorian legislation. The Family Violence Protection Act 2008 (Vic) sets out that “family violence” – as it is referred to in the Victorian context – can be perpetrated in the context of a wide range of family relationships, including by young people.
Further, a proactive code of practice requires members of Victoria Police to bring an application for a civil protection order on behalf of someone who they consider may be at risk of experiencing future violence (rather than recommend that the individual bring an application themselves; Victoria Police, 2017). Combined, this broad legislative definition and proactive policing approach has led to a relatively consistent rate of police attendance at DFV callouts resulting in applications for protection orders being brought against young people in the jurisdiction of the Children’s Court of Victoria.
Concerns and challenges in relation to this trend – including the relevant legislation’s failure to require a court to consider a respondent’s capacity to understand or comply with an order – are discussed in detail in the PIPA project’s report (Campbell et al., 2020). As noted above, this earlier ANROWS study explored the combined legal and service response to AVITH in three Australian jurisdictions which, at the time of the study, had distinct legislative and policy settings. The weight of the PIPA project’s analysis focused on legal responses and, in particular, on the way in which the Victorian response may “miss the mark” because of its failure to consider young people’s prior experiences of trauma or their developmental capacity (Campbell, 2021). It also outlined the associated service landscape, which was arguably attempting to stem this harm, but not linked in consistent ways with the legal response.
Victorian service landscape
At the time of the PIPA project, the service landscape reflected the policy settings that had evolved in Victoria, with a lack of systemic responses leading to some organisations developing their own programmatic responses. These included various iterations of a family systems therapy approach delivered by Anglicare, in addition to the Breaking the Cycle program, a manualised, therapeutic, group work program for parents of young people who use AVITH. This program involves facilitated group meetings for parents, with a range of therapeutic activities, occurring once per week for eight weeks. The group work has a primary focus on safety while removing blame from parents, empowering them to strengthen intra-familial relationships, and holding the young person responsible for their behaviour and for changing their own behaviour to regain respect in the parent–child relationship. The program relies on the premise that positive changes that the parents makewill promote change through the whole family system, particularly where young people using violence are often reluctant to engage with services.
While more recent evaluations of the program are not publicly available, an early published evaluation by Wilks and Wise (2012) points to positive outcomes, while also suggesting that skills learnt in the program may take time to develop and be implemented in the home.
Step-Up in Victoria
In addition to programs specific to particular organisations, such as Breaking the Cycle (above), in 2014, the Victorian Government funded three programs described as “adolescent family violence programs” (AFVPs) in two regional locations and one metropolitan location (State of Victoria, 2014). Program design was influenced by the Step-Up model, but programs are delivered in voluntary, community-based contexts, rather than in court-based contexts. An evaluation of these programs conducted by the Australian Institute of Criminology (Boxall, Morgan, Voce & Coughlan, 2020) found that there was some evidence of reduction in severity and frequency of violence by a young person while engaged in the program.
The evaluation also found that programs helped parents experiencing AVITH by reducing associated levels of stigma and shame, thus increasing their confidence to report their experiences, and helped adolescents and families by improving skills related to reducing conflict (Boxall, Morgan, Voce & Coughlan, 2020; Campbell et al., 2020). This evaluation was conducted between 2014 and 2015 and was somewhat limited by small sample sizes and no long-term follow-up (Boxall, Morgan, Voce & Coughlan, 2020). Similar to the limitations of the US-based model, however, the evaluation reinforced the importance of addressing and breaking cycles of violence within families, as many of the participants had experienced intergenerational harm. It also highlighted the challenges inherent in adequately addressing the multiple co-occurring risk factors and complexities present in families experiencing AVITH (Boxall, Morgan, Voce & Coughlan, 2020), echoing thefindings of the KIND evaluation (Moulds et al., 2019). The authors of the AIC evaluation acknowledged that,
given the evidence that substance use and mental illness are associated with the onset, recurrence and escalation of [AVITH], young people need integrated interventions and coordinated support to address their abusive behaviours as well as psychiatric and substance use treatment. (Boxall, Morgan, Voce & Coughlan, 2020, p. 1)
Recommended expansion of the Victorian Step-Up-based programs
The RCFV recommended that the Victorian Step-Up-based programs be expanded on a statewide basis, subject to the results of the above evaluation, which were available to the Victorian Government before it was formally published. As at 2020 – when both the AIC evaluation and the PIPA research were released – this expansion had not occurred. In the interim, however, the Victorian Government had provided additional funding to the three existing programs to support individually based work and had also funded an ACCO to develop a community-led, culturally specific program (State of Victoria, 2018). More broadly, it is important to note that similar group work programs based on the Step-Up model had emerged in other locations throughout Victoria, delivered by organisations receiving broader DFV and integrated family services funding.
In the second half of 2020, the then Victorian Minister for Family Violence Prevention announced that additional funding would be directed towards responses to people using DFV, with responses to AVITH identified within that allocation (State of Victoria, 2020). This was described as a response to the increase in DFV and AVITH during Victoria’s 2020 lockdowns. Further detail about the AVITH-focused nature of the investment was forthcoming in early 2021, when organisations which already delivered therapeutic recovery programs for victims and survivors were asked to establish AVITH-focused interventions as an additional component of their work. Organisations were asked to establish programs and provide early data within six months, with funding later extended for a further 12 months.
During 2022 – a period during which government had the opportunity to review drafts of the current study while the project was paused, as well as other AVITH-related research – the Victorian Government initiated a procurement process for services to deliver programs using a model of care for adolescent family violence in the home (AFVITH). The model of care proposed that suppliers adopt a whole-of-family approach, ideally through a collaborative or service consortium arrangement. The proposed model sought to prioritise early intervention and emphasise care coordination.
Other AVITH-focused policy and investment in Victoria
More broadly, many of the other AVITH-focused RCFV recommendations had also been implemented prior to the WRAP around families research being initiated, including the appointment of specialist practitioners at the Melbourne Children’s Court to support young people and families where a young person was a respondent to a protection order application; the establishment of a legislative statewide diversion scheme; and the expanded use of Youth Resource Officers within Victoria Police, some of whom incorporate a dedicated focus on young people’s use of violence at home into their role.
A trial of “restorative family meetings” incorporated into the adolescent family violence programs, as recommended by the RCFV, was also conducted but not continued. Findings from an internal evaluation were not available at the time of writing but Victoria’s Family Violence Reform Implementation Monitor (FVRIM) noted that efforts should be made to revisit this (FVRIM, 2021a). Notably, an investment in respite via dedicated crisis accommodation linked with therapeutic support for young people using AVITH (as recommended by the RCFV) had not been forthcoming, although investment in crisis accommodation for young people experiencing DFV had occurred. This lack of progress in implementing appropriate respite options was also identified by the FVRIM (2021a).
Outside direct implementation of RCFV recommendations, the Victorian Government also established a cross-government working group in 2018 with a focus on developing a coordinated service response to AVITH. It also funded the Centre for Excellence in Child and Family Welfare (CFECFW) to build and share evidence through an open platform, hold an AVITH-focused symposium to discuss current evidence, and coordinate a community of practice for specifically funded AVITH services.
Flowing on from AVITH being recognised as a specific form of family violence in Principle 10 of Victoria’s Multi-Agency Risk Assessment and Management Framework, as well as in related victim survivor practice guides, the Victorian Government also progressed work to develop risk identification and assessment tools applicable to the use of a range of interpersonal harm by young people, as well as to consider the experience of children and young people as victims and survivors of violence in their own right.
This included a focus on considering the full spectrum of risk and where young people may have been misidentified as the predominant aggressor, a concern highlighted by FVRIM in late 2021 (FVRIM, 2021b). The lead author of the current study was part of a team engaged to contribute to the development of a practice guide to inform and accompany these tools, to be released at a later date.
Recognising the impacts of COVID-19 on opportunities to progress this broad-ranging work, it is nonetheless worth noting that, while a focus on service delivery and associated investment was clearly visible during this time, engagement with relevant challenges in the legal system was not. This includes engagement with the findings of the PIPA project around the challenges associated with the legal response – crucially, that the current legal response frequently sees young people made subject to a protection order without appearing at court or having the opportunity to engage with lawyers and disclose their own experiences. Further, Victorian legislation still does not require any consideration of a young person’s capacity to understand or comply with any order imposed, nor consideration of safety risks where a young person is excluded from the home and placed with another adult. As a result, young people are being pushed into a tertiary end response,with its associated potential for an escalation in risk, by virtue of the legal process. Funnelling of resources into this tertiary end response in turn pulls focus and investment away from early intervention and wraparound approaches.
COVID-19 in the literature
Providing further backdrop for the period during which this research was conducted was the COVID-19 pandemic and, in particular, Victoria’s extended lockdowns during 2020 and 2021. Evidence has already highlighted the impact of the COVID-19 pandemic on DFV generally, observing a significant increase in both severity and frequency (Boxall, Morgan & Brown, 2020; Pfitzner et al., 2020; Usher et al., 2020; Usher et al., 2021) quite early in the pandemic. Studies have also noted increased numbers of people seeking support from specialist DFV services; an increased complexity of needs; and escalation in controlling behaviours from adult perpetrators (Boxall & Morgan, 2020; Perkins et al., 2021; Peterman et al., 2020; Pfitzner et al., 2020), who leveraged the isolation and added barriers for victims and survivors to seek support or escape (Perkins et al., 2021; Peterman et al., 2020; Pfitzner et al., 2020; Usher et al., 2020; Usher et al., 2021).
Evidence also establishes that the COVID-19 pandemic has increased mental health issues in many people (Fisher et al., 2020; Tucci et al., 2020), including young people (Cardenas et al., 2020; Drummond Street Services, 2020; VicHealth, 2020).
In particular, a study conducted over the United Kingdom’s initial lockdown in 2020 revealed a marked increase in the incidence of AVITH, with 70 per cent of 104 parents surveyed reporting more frequent incidents, while practitioners reported an increase in referrals and a rise in severity of the violence (Condry et al., 2020). Explanations cited were spatial confinement and forced proximity within family homes; dramatic changes in structure and routine leading to disruption; increased opportunities for young people to use power and control; and general heightened fear and anxiety (Condry et al., 2020, pp. 21–27). The study concluded that, for many families, AVITH will have become more entrenched and further damaged relationships, with an increased need for additional support – or a “safeguarding surge” – predicted by the authors (Condry et al., 2020, p. 54).
A study from the United States examined the impact of the pandemic on sibling violence specifically (Perkins et al., 2021), and highlighted the effect of unsupervised and concentrated time on an increase in sibling violence during lockdowns. The study also noted that increased stress and trauma, as well as child abuse and neglect, within families is generally associated with an increase in sibling violence and will have been compounded during the pandemic (Perkins et al., 2021).
In the Victorian context, Victoria Police data suggested a 20 per cent increase in reported family violence incidents involving young people between October 2019 and September 2020 (Crime Statistics Agency, 2020). An issues paper prepared by the Centre for Innovative Justice and the CFRE at DS similarly responded to reports from practitioners that AVITH was increasing during the pandemic, particularly during the extended lockdowns and restrictions experienced in Victoria during 2020 (Campbell & McCann, 2020).
The paper drew on consultations with service and legal practitioners who described a “net-widening” of young people experiencing a legal response because of behaviour which had developed and escalated during lockdowns. Practitioners also described an escalation in mental health issues – particularly where families were required to spend more time together without “circuit breakers” such as school, work or extracurricular activities (Drummond Street Services, 2020). This was described as prompting crisis responses which in turn ruptured family relationships over the long term (Campbell & McCann, 2020).
Practitioners also reported that the lack of service responses was impacting legal outcomes for young people, as was the difficulty in engaging young people online or via phone, particularly where young people had cognitive disabilities or learning delays (Campbell & McCann, 2020). In particular, practitioners reported concerns for the safety of young people where they may not have a safe or private space to have conversations or make disclosures while confined within their home, particularly where they were living in crowded public housing (Campbell & McCann, 2020) and, for a time, subject to “hard lockdown” during July 2020 (Om, 2020; Victorian Ombudsman, 2020). One regional integrated service network reported a particular increase in sibling violence (Campbell & McCann, 2020).
Part 2:
Challenges, change and conceptualisation
Overview
This section of the report outlines some of the findings from the focus groups with practitioners across AVITH-focused mental health, legal, court-based and AOD support services. It also features the voices of parents interviewed for the research, who described significant and multiple needs that had not been met by the service system. In addition, it incorporates references to data from the case files which reflect the complexity of this area and echo many of the challenges identified throughout.
Overall, the research highlighted the ways in which practitioners were working hard to respond to clients in a service and system context which, in some ways, had become even more complex since the Victorian data collection period of the PIPA project. Despite additional government investment, the nature of this investment had not yet offered a sufficiently coherent articulation of what Victoria’s response to AVITH was intended to be, despite the effort of practitioners. Further, the additional activity required of services since the RCFV’s recommendations appeared to have constrained service capacity to share practice knowledge and developments in a way that might be expected or, arguably, had previously occurred. The findings therefore suggested that, while there was now greater familiarity with the concept of AVITH – assisted by the RCFV’s articulation of it as a standalone issue, and subsequent research – Victoria’s response was still in the processof being appropriately and fully developed.
The findings and analysis in this section are set out in relation to two overarching areas. The first is practice challenges, including naming and identifying AVITH as a concept, funding, referrals, program design and presenting needs of families. Within the latter theme, the support needs of mothers and children associated with their experiences of prior and ongoing adult-perpetrated DFV was the most substantial sub-theme. The second area relates to systemic barriers and challenges which practitioners were experiencing at the point of data collection and continue to experience at the time of publication.
Practice challenges: Naming and identifying AVITH as a concept
Across the focus groups, practitioners suggested that a greater awareness of DFV overall was enabling families to identify and name what they were experiencing in relation to their young person’s behaviour. This included families starting to self-refer into AVITH programs or being more inclined to call the police for assistance with safety, even where they did not want their child to experience a justice response. Parents participating in interviews and families recorded in case files also self-referred in many instances. “Parents are definitely coming out and naming it … so they’re looking for a specific response. And Googling it … So it’s definitely kind of named and talked about” (Practitioner 2).
That said, a consistent theme across the research was the reluctance of young people or families to be linked with a service which was identified as specific to DFV. Kehoe and colleagues (2020) suggest that intervention efforts are further stymied by parental reticence to engage in services which may escalate feelings of shame and stigma (Kehoe et al., 2021). Parents may also feel that their child’s behaviour is normal; that they have failed in being a good parent; or that they are alone in their experience of AVITH and therefore feel disempowered to seek help (Kehoe et al., 2020).
Literature notes that mothers, in particular, often blame themselves for their child’s use of violence and seek to hide it (Fitz-Gibbon et al., 2018; Meyer et al., 2021), while young people feel guilt and embarrassment (Burck et al., 2019; Burck, 2021; Condry & Miles, 2021; Papamichail & Bates, 2020). Practitioners in this research similarly described these feelings of shame as sometimes contributing to escalated risk, with young people acting out further as a direct response to their feelings of guilt: “We know how shameful it can be accessing services … often the risk levels are quite high because of the shame associated with that” (Practitioner 22).
Parents similarly described the shame that their child felt when they had used harm against their family.
[Young person and older brother] have done things where they … have either punched me or physically done something … and the verbal stuff that used to come out [to me and their sister] and … then would go into these huge depressions afterwards because of the guilt. (Parent 1)
Practitioners also described young people feeling resentful about involvement in a program when they have been a victim and survivor themselves but were now being labelled as the person causing harm. Practitioners working in ACCOs which had been funded through the recent Victorian Government investment reflected on this and explained that language and terminology were particularly crucial in community-based contexts.
Talking to other colleagues … who work as adolescent family violence workers from other organisations and from other areas at [our organisation] and stuff as well, like, it’s been challenging, I think with the language around what the program’s called … not to downplay any of the actions of the young people, but there’s a big scale of violence as well. And so sometimes we might work with someone where there’s quite serious kind of family, physical violence and things like that happening. Other times that might be something that is, that’s one aspect … But it’s really difficult often for us to kind of get the young person to recognise if they’ve experienced family violence or other kind of trauma as well, to recognise what their behaviours are in relation to the things they’ve experienced as well, because often the things that they’ve experienced are … much worse than what they’re doing. So, it’s hard for them to say, well, you know, “Dad isn’thasn’t [sic] faced any consequences for his actions or whatever. So why am I?” (Practitioner 73)
In relation to the system’s capacity to name and identify AVITH, practitioners described persistent service confusion about the behaviours that might constitute AVITH. Practitioners also described a system that had worked very hard to identify patterns of adult-perpetrated DFV, but could not yet identify AVITH or, more specifically, understand considerations required to deliver effective responses.
The system is catching up with all this … language around [risk assessment] that is still filtering through policing and the courts … we’re asking police and courts to believe victims, survivors and to identify when women are experiencing family violence. And then we’re adding, you know when it comes to young people using violence … police are seeing a 16-, 17-year-old using violence and they view him as an adult perpetrator, we’re not responding to him as a child. So it’s like asking for another shift, another complexity, another nuance that the system isn’t really ready for. (Practitioner 50)
What I notice as a shift is a deeper understanding around adolescent brain development. But where I don’t see the dots joining is then where it connects with perpetration of adolescent family violence. There’s still this kind of like “they’re going to be monsters when they’re men”. (Practitioner 35)
Practitioners across the research volunteered that the concept of AVITH did not fit well within the victim and survivor/perpetrator dichotomy on which wider DFV responses were based. This poor fit then shaped recognition of the issue as one warranting a safety response; the nature of this response; and referrals on to other services. This could function as a barrier to support for family members experiencing AVITH or, alternatively, mean that young people received a punitive – and therefore unconstructive – response.
We had a really disappointing experience with a family that got bounced around all over the place trying to get a referral into our program which included [an intake service] responding to them and saying “Oh no, you’re talking about a teenager, we’re not going to help you” and just kind of ending the conversation because it wasn’t an adult perpetrator. (Participant 22)
There’s just something about working with the perpetrator that [means that specialist DFV services] just don’t go there, like, “That’s not the work we do. We work with victim survivors” … It’s so binary and it doesn’t help anyone to view families in this really binary way. (Practitioner 27)
We’re dealing with children and young people – and sometimes they are children, they are little kids … You get these very perverse outcomes where a child might make a move towards reconciling with the family and [where there’s a protection order in place] that move towards reconciliation is a criminal action … It’s kind of adult perpetrator frameworks expressed in a way that is not developmentally attuned at all. (Practitioner 54)
Practice challenges: Referrals into AVITH-focused support
Practitioners explained that the ambiguity or uncertainty described above could impact the type, as well as the flow, of referrals into services. The research team heard that, upon establishment, some new programs had received a rush of referrals from local schools, mental health supports or disability services that were not appropriate for an intervention focused on AVITH.
This reflected what practitioners described as a lack of services available to respond to challenging behaviours or expressions of trauma or disability in young people in their area.
Some of them were really inappropriate referrals. So like we’ve got kids that are like, you know, incredibly low IQ, with specialist school history … sexual abuse, who’ve ended up in the program. Like that young person had no capacity to even understand why the behaviour was not okay. Our team leader does admit that, at the start, it was like, you know, grab for whoever was coming through but then towards the end, we refined the process down. (Practitioner 17)
We’ve had [the intake point] make referrals for whole-of-family case management … that sat well outside the scope of what the program was all about … and really required an intensive Integrated Family Services kind of approach. (Practitioner 43)
Importantly – and as explored in more detail in Part 3 of this report – focus groups suggested that, where referrals were working most effectively for the newly funded services, these services were leveraging the integrated referral pathways that already existed within their own organisations.
That said, practitioners who worked in well-established services – including youth substance abuse services, as well as AVITH-specific services – also described referrals coming through once behaviour was entrenched but had not initially been identified through a DFV or trauma lens.
These young people are hitting wrong doors all the time … they will hit different parts of the service system, particularly the tertiary system … and then the referral comes after they’ve done six or 12 months of intervening and case work and there’s been, you know, hectic substance use and then there’s like “too hard” or it will bump it back to us. (Practitioner 52)
When trauma or the presence of adult-perpetrated DFV had potentially been identified, practitioners also expressed frustration that appropriate supports had not been provided to young people or families where earlier support could have made a difference.
… the number of referrals that we get from Child Protection when there’s been so many prior reports, sometimes with an intervention, sometimes with nothing, and then we still get it with the same criteria and the problems will be entrenched. And if we read the referral, we can quickly surmise that there’s been something really complex and why hasn’t it been picked up? Why hasn’t something been offered to the family? (Practitioner 1)
Interviews with parents certainly reflected this pattern of a lack of support in relation to adult-perpetrated harm experienced earlier in childhood.
[Young person] has only really ever known conflict … [and] the kids have never really spoken about any of that [adult-perpetrated violence]… there’s never been any formal sort of support putting in place to help them debrief or grieve through all of that. Yeah, ’cause grief is a really big factor there. Yep. For that relationship. (Parent 1)
In some cases, AVITH-focused interventions that had previously received referrals directly from Victoria Police were no longer directly linked into this process because of wider change across the Victorian family violence system. This was primarily because referrals were now going from police to the Orange Door network (see “Definitions”). Demonstrating a need for either multiple referral pathways or sufficient resourcing and staffing to allow for follow-up and expediting of referrals once made, practitioners therefore spoke about challenges that arose when they did not have the direct visibility of a young person’s or family’s circumstances to which they had previously had access. This included where a specialist DFV response was put around a mother, but no referral, or a referral which only contained limited information, was forthcoming for the young person. These practitioners described the need to push for more information, particularly when areferral signalled that the situation was “at breaking point” (Practitioner 5).
… in relation to the referrals that come from [the intake point] … was the lack of information … I have so many questions that came up in the referral … and [the practitioner has to] chase back down with the family or other services that are involved … I’ve had questions about sexual assault and [the referrer] just can’t answer them. They can’t answer what medication a young person is on. (Practitioner 8)
Practice challenges: Funding parameters
Funding parameters
Directly related to the number and type of referrals that services could accept were the funding parameters constraining operation at the time of data collection. This was particularly the case in relation to the services funded in early 2021, which in many cases were working primarily with allocations of between 40 and 110 case hours, with the upper limit being dependent on the complexity of the young person’s behaviour and the needs of the family. Practitioners noted that a limited timeframe such as 40 hours “is just not enough, like adolescents just don’t engage in 40 hours, especially in the middle of a bloody pandemic” (Practitioner 17).
Practitioners explained that this allocation could quickly be exhausted and result in very limited face-to-face contact with a young person once outreach, service coordination and file work was also completed. The research team notes, however, differing understanding and practice across programs where some practitioners described the 40 hours as a floor, rather than a ceiling. This appeared to be where practitioners worked in organisations which provided programs with wider support and integration with other services.
Just as importantly, practitioners noted that constraints on their funding did not allow them to engage with other family members in addition to the working with the young person: “… [where families are] from a CALD community, like you can’t work with a young person if you can’t work with their family” (Practitioner 55).
Funding parameters at the time also limited program capacity to respond to young people in ways that were appropriate for them, including through a workforce of sufficient size which could support a young person if they were likely to respond more positively to a practitioner of a particular age or gender.
I … reality is that I’m just another middle-aged lady who’s coming into [his] life telling him what to do and they’ve got that at school already and they’ve got that at home already. (Practitioner 18)
Importantly, it also limited the period over which they could engage with young people.
I’ve had a couple of clients when really short, sharp interventions have worked … One of them I instantly spotted this kid had a communication issue and we got the speech therapist and it was a quick, “This is what it is” and that was fine but, overall, most of them need really consistent, long-term interventions … So, the advice in the PIPA report was like, “Don’t do short-term, short-term interventions bad” and then the government was like “only do short term interventions, please”. (Practitioner 17)
Parents also reflected on the need for longer term engagement being available: “Kids naturally test boundaries … So, you know, the offer has to be unconditional and without an end point” (Parent 1).
More broadly, the research highlighted the impact of the short-term nature of the relevant program funding in terms of referral pathways. Practitioners explained that some referrers had indicated that they did not want to refer young people if they could not be certain that the engagement and support were going to be available over the longer term (Practitioner 18). This was in part because the cessation of the support would only seek to entrench young people’s sense of being let down by the system overall.
Practitioners also explained that the short-term nature of the current funding – extended for a further six months just after the completion of the focus groups and then again later in 2021 – was limiting their capacity in a range of other ways. This included the ability to recruit, train and then retain a workforce. In fact, some practitioners volunteered that they were looking to move on to other roles, despite their commitment to and belief in the work, simply because of the uncertainty of their current position.
What we’re doing takes skilled and dedicated practitioners and they’re so hard to get when you keep stuffing people around … so we’re just constantly putting families on the back foot and saying they’re not important. (Practitioner 27)
Focus groups featured regular discussions about the uncertainty created by the short-term nature of community-based service funding arrangements, in which a substantial amount of practitioner time was allocated to seeking and reapplying for funding.
It’s just this weird funding cycle that makes everyone really anxious and not be able to do any actual work. (Practitioner 27)
People are just getting their hands on money. And then trying to figure it out from there, rather than any thought going into the work. (Practitioner 10)
Funding challenges, however, were not limited to the recently funded programs. Practitioners working in established AVITH-focused interventions, as well as in wider services which regularly came into contact with AVITH, described the way in which particular funding limits or parameters constrained the nature of the support that they could deliver.
[The funding organisation is] saying “How does this person make criteria? Prove it.” And we’re saying “they will” but shit, they don’t. (Practitioner 55)
We still get this expectation that we work with families for this specific period and it’s all about referring on … whereas we’re all therapeutically trained and we have the capacity to do the deeper work. (Practitioner 2)
A common theme across the focus groups, in fact, was the challenge created by the wider approach to human and social services funding which continued to impact the organisations in which practitioners worked, as well as the capacity to deliver AVITH-specific interventions.
One of the major challenges that we’ve had from year to year is essentially where you would get a program and it would start and you would build momentum … and then it became unfunded and we spent … months looking for funding … So we essentially started from scratch and had to build that momentum again. (Practitioner 62)
Practitioners noted the way in which wider approaches to competitive tendering in community-based service contexts impeded collaboration (Practitioner 44) and made it hard to establish consistency in design, as well as outcomes for families.
… I think that’s pretty disheartening. But also just operationally makes it really challenging … if you’re going to make a change you’ve actually got to change the hierarchy and competitiveness in the setup. (Practitioner 12)
Systems … are increasingly about hierarchy and actually about transactional, you know, kind of high-volume, low-touch services that ultimately can only exist if you deny the impact of trauma. (Practitioner 2)
Importantly, a practitioner from one participating ACCO observed that funding was a perennial challenge in terms of the wide-ranging work that they did – work that was not adequately captured through the target- and output-based nature of the way in which most community-based services were funded.
We certainly report on the hours we work but, if we do over, we just don’t report that and there’s no way to report it really … I think [government] want[s] to support you to a certain degree, but [it’s] so target-driven and hour-driven that we can’t get past that … What we do on the side is what we do on the side … And you’ve got to because the targets and the hours … don’t meet what our need is really. They help support a funded position. That’s really what it amounts to, you know … So it’s a catch 22 in the end, it’s really difficult, but … we’re here to serve a community and the need is there, so that’s what we’ve got to do. (Practitioner 72)
Practice challenges: Lack of consistent frameworks
To an extent, the research found that funding models dictated the framework through which programs were delivered. Although there is a broad understanding at a policy level that interventions will have a whole-of-family focus, practitioners revealed a wide range of approaches being adopted by programs across Victoria. These included a combination of group work and an increasing emphasis on individualised case management being delivered by the established programs which had originally been based on the Step-Up model. They also included the primary focus on young people dictated by the reality of the funding parameters in the more recently funded services.
Group work
Program design included funding attached to certain expectations about the activities that would occur, despite the fact that some practitioners did not always see these activities as being of sufficient value: “Groups for young people aren’t overly successful … if it’s not managed right, a group can be really detrimental to a young person” (Practitioner 5).
These particular practitioners explained that they were required to report a certain component of group work in order to retain their funding, but that they were finding this additionally difficult in the context of significant need across the families with whom they worked, particularly during COVID-19.
We’ve got all of these targets … and we’ve got to try and run group as well as part of our funding … but in these current times, we’re lucky to be able to respond to these families’ current needs without even trying to run a group as well. And I don’t know if we can respond, to be honest. You know, if we want to do each family justice. (Practitioner 5)
Another program appeared to focus its group work on parents, with case management and outreach then directed towards young people. A further program retained concurrent group work with young people and parents, including meeting with parents and young people on an individual basis and bringing in local services and Victoria Police to give talks and foster connections. Some programs that were not funded directly by the Victorian Government ran a group work component, along with intensive family therapy and dyadic work, while others focused on group work with young people at an earlier stage of concerning behaviours. Overall, practitioners described the need for flexibility and the capacity to offer different approaches to engagement within different families: “There’s a place for all of us and every model. Not everyone is going to fit into group work. Not everyone is going to fit into one-on-one” (Practitioner 44).
Limitations in support for families
Practitioners from programs that had received the more recent injection of funding at the beginning of 2021 frequently described themselves as only being funded sufficiently to work with young people, rather than to work with other family members. Where practitioners could draw on other programs and practitioners within their organisation, they could complement the work of their funded role. Where some practitioners were working in isolation, however, this meant that they were simply not able to provide sufficient support to parents or siblings, or alternatively they opted to give their allocated hours to a parent where this was more effective.
Sometimes it’s just Mum who will engage. We need to have flexible models where we can just engage whoever is willing to work with us at that particular time. (Practitioner 9)
It would be bloody nice if we were always engaged alongside family services so that there was a practitioner for their family … so we’re engaged explicitly for the young person but a lot of the time we know the work has to be done with the family, like a 12-year-old doesn’t have the capacity to make those changes for themselves, it’s gotta be a family approach. (Practitioner 17)
A further challenge arose, however, because AVITH-focused interventions were voluntary. Where young people over 16 were unwilling to engage or did not consent to their parents being involved, therefore, practitioners could not work with the parents.
There needs to be consent from the young person and … then [we’re] telling parents, “Well we can’t work with you because, yeah, we haven’t got the consent from your child” … It’s certainly something that I think, in terms of … how we fund adolescent violence services in the future … it’s something that is a bit of an issue and needs a bit of thought (Practitioner 10).
Capacity for flexible, client-centred approaches
Program parameters also dictated the types of activities which were able to be conducted through AVITH-focused interventions, with capacity for flexible and client-centred approaches emphasised by practitioners as being particularly crucial. Interviews with parents also signalled that young people needed flexible and very pragmatic approaches, such as outreach, rather than “talk therapy” (Practitioner 57) as one practitioner described it.
I haven’t had any support from anyone, pretty much for four years because my son refuses to talk to anyone … So, I’ve really, really, really struggled with actually getting any physical support. (Parent 1)
The interviews also echoed what practitioners highlighted about the need for longer engagements over which young people could develop rapport, especially if trust had previously been damaged.
It makes me feel really like I’m not doing the right thing … where I’ve tried so many organisations, but no one’s willing to actually step out, push the boundaries a little bit and go, “Okay, you know what? That’s fine. You don’t wanna talk to us … But I’m gonna ring in and check on you every week. And I would like you to answer the phone call and let me know you’re okay. That’s it. You don’t have to talk. But just say yes, I’m fine this week” … Because you know what? In four or five weeks, something might actually click … (Parent 1)
[The psychologist] tried … to make [my daughter] talk to her dad when she wasn’t ready … “Have you spoken to your dad?” “Have you spoken to your father?” … So [my daughter] refused to talk to [the psychologist] for 21 months, and the psychologist kept pushing her. And I’m like, “when she’s ready, she will talk to him. She’s not currently ready”. (Parent 3)
We had a case worker about six or seven years ago and initially … my children would refuse to have any conversations with this person and over the course of, I think it was four or five visits, they actually started to open up and by the last visit, they actually started talking to him … and then he says, “Oh, this is my last visit ’cause I’ve done my time here”, and I’m like “Oh my God!” … Why do you have to have a case manager just for X amount of time or X amount of visits? … Especially when there’s kids who have had huge traumas and have had abuse … or have been led down the wrong path by a counsellor … and they don’t have that trust there initially … they’ve gotta build the trust before they’ll start speaking. (Parent 1)
One participant from an ACCO explained that flexibility was a central and inevitable part of their practice because of the fact that practitioners were often working within the context of, and had obligations to, their own communities. This practitioner noted that this was not always understood or recognised within funding parameters or in government policy settings.
Our community workers certainly have that feeling of never been able to clock off. I’m pretty strict on trying to make sure that they do clock off and, you know, like work phones don’t go home with them and stuff like that because you have to have that time. But community workers – people know you and know how to contact you and all the rest of it, so it’s not as simple as that. (Practitioner 72)
Practice challenges: Presenting needs of families and young people
An adult perpetrator – and systems abuse – out of view
The ongoing impacts of adult-perpetrated DFV was a recurrent theme across the research, as it was across the PIPA project (Campbell et al., 2020). In 88 per cent of case files, for example, the young person had experienced and/or witnessed DFV or DFV-supportive behaviours. In only three cases the file data did not appear to indicate prior experiences, although this was inconclusive given that prior experiences of adult-perpetrated DFV may simply not have been recorded in these files. More broadly, it was one of many presenting needs to which practitioners across the focus groups were required to respond – or at least to take into account – in the context of their practice.
A big sort of intersection that we see … is where there’s been some sort of extensive Child Protection involvement for a child in their early years. Usually because there’s been intimate partner violence and then down the track when the time the child is in their teens, they’re using violence and they’ve got this significant history of trauma and possibly still family violence going on for them. (Practitioner 68)
… where there’s a significant history of them being exposed to family violence in the home and you kind of just hold your hands up like this and go, “Well what did we expect is gonna happen?” (Practitioner 61)
It is crucial to note that the ongoing impacts of adult perpetration were ultimately the most substantial theme across the client interviews as well as being apparent in the case file review. Parents who participated in the interviews – all of whom were sole parent mothers – described extensive histories of violence which had included very serious physical and verbal abuse against them and their children, and in one case multiple subsequent relationships involving violence.
Before we split up, it was like … shouting a lot and throwing things around and breaking things and, not hitting me, but verbally very aggressive and controlling and if something didn’t go his way “I’ll just break something, punch something”. He punched holes in the wall. And that’s when I got an intervention order against him … it was like he was jealous … it’s almost like he feels like [young person] was born and then everything changed, I guess because … my focus wasn’t on making him happy anymore. It was looking after a child. (Parent 2)
[The children saw] when I was physically backed up against the wall [with a knife in my face] … every time I had tried to walk away from him in like, say an argument or whatever, every time I tried to leave, he would grab me and then physically start hitting me … From my experience I felt like I had no way to get away. (Parent 3)
The nature of the violence experienced by young people and mothers engaged with the DS program and evident across the case files was, in some cases, incredibly stark and multi-directional.
Young people’s experiences of prior adult-perpetrated DFV
- In file DS021: “The mother reports that her ex-partner (recently separated) and the young person have always clashed” and there was an incident “when the young person was in Grade 4 and her ex-partner strangled the young person, who was very scared”.
- A young person was exposed to her father’s DFV from a young age (DS008): “When [young person] was very young, their biological dad smacked [her] on her bare bottom in public. He made his dog growl at her when she was two because she told a lie. They also witnessed him choker her and punch her in the face.”
- Case notes from file DS250 involve a young person’s mother describing the father’s violence towards the young person, explaining that he would hit her with so much force that she would report to the mother that her whole body would vibrate. While the parents were still married, the father would control all the finances, preventing the mother from working and “refusing to care” for the children. The mother also describes violence and controlling behaviour used by the children’s father towards her, including calling her a “cunt” and “slut” in front of the children.
- Information on file DS032 describes a young person’s father holding the mother by the throat up against the fridge until her face turned blue, resulting in the young person stepping in and begging him not to kill the mother.
As well as acknowledging the prevalence of prior experiences of adult-perpetrated harm, however, practitioners expressed concerns that limited capacity to work with different members of the family did not give them a lens on the adult DFV risk that might be present in that home or in the young person’s life on an ongoing basis. The challenge of a lack of visibility of an adult (usually male) perpetrator continuing to use abuse was a prominent theme across all of the focus group discussions.
Practitioners working within the newly funded programs explained that it was often not until well into engagement with a young person (including when a caseload allocation was winding up) that the presence of adult-perpetrated DFV became apparent.
I think the awkward thing is that like we don’t actually know … Like, one of my families, I didn’t know there was family violence present there till I was actually in the house [conducting outreach] and by that stage it was too late. (Practitioner 17)
I’ve got a family at the moment where I’ve been holding a question about intimate partner violence, as well as the adolescent family violence … My sense is that it’s going on but no one’s admitting to it and Child Protection has been involved and the school’s got concerns and so it’s quite complex. And I’m there trying to engage with the adolescent but also trying to assess risk and what’s really going on in the home. (Practitioner 9)
I think that risk is perhaps missed, even with Child Protection, so that the stepfather has got a criminal history of family violence. But … the young person … is the focus and makes disclosures of family violence in the home and then retracts them … Child Protection is gone and said “we can’t find any evidence” so close the file. (Practitioner 9)
Challenges were compounded when the parameters of some services precluded work with young people where an adult was continuing to use DFV. These limitations were designed to prevent scenarios of young people being “held accountable” for behaviours towards people who have used harm against them, but legal practitioners in particular were concerned about the exclusion of young people from support.
Where can we actually get the right support for these young people? That’s safe for them to have their own person to speak to? A lot of the services are ruled out because they can’t work with a young person when there’s an adult perpetrator in the home. (Practitioner 46)
When we do get the referrals or the intakes … the young person is often not a part of that process … [their] voice is often not there. It’s other people’s interpretation of the young person’s experience or their own experience of the young person … it’s almost like distancing of an adult perpetrator as well, and then holding the young person as the perpetrator. (Practitioner 33)
A lot of our families have had family violence and Dad of course is potentially … perpetrating family violence from outside the home. But we’re actually not having any collaboration with any men’s behaviour change services or any male services … we don’t know what the male perpetrator is doing. Despite all this supposed collaboration, we have no idea. (Practitioner 5)
The capacity to understand the risk posed by adult perpetrators – and to keep an adult perpetrator in view – was highlighted as a significant challenge beyond specific program capabilities and capacity, with the impact of post-separation systems abuse a particular concern raised by participants: “The family court is a massive problem … it impacts our ability in this space” (Practitioner 27).
Ongoing family law struggles – as well as serious adult-perpetrated DFV and coercive control – were very apparent in the case files. These included young people continuing to live in very unsafe situations, either with a separated biological father or in new family structures where they are experiencing adult-perpetrated DFV. In particular, some of the files echoed practitioner observations that separated fathers may “coach” young people from the sidelines in relation to their use of violence or aggression towards their mother or, alternatively, that young people may only “act out” once they return from contact visits to the safety of their mother’s residence.
Ongoing abuse
- File DS838 describes the influence of the father over the young person, with the mother reporting that the father reinforces the young person’s aggressive behaviour towards the mother and states that the mother must be the problem given that the young person does not use the same behaviour at the father’s house.
- In file DS021, case notes discuss a young person’s relationship with his separated father undermining the bond he had with his mother. Case notes also describe that the young person could nonetheless feel overwhelmed and confused and, when this occurred, elected not to go to his father’s house, at which point he felt guilty and experienced retaliation from his father.
- In file DS311, case notes describe the young person and his older brother returning from their father’s to accuse their mother of “making their father suffer”. Case notes also describe the young person becoming increasingly aggressive on these occasions and undermining the mother and her parenting strategies.
- In file DS789, the young person and two siblings were living with their father, despite a current protection order in place to protect the mother and all children from the father. This was because the mother did not have a fixed address and was experiencing secondary homelessness. Child Protection was involved while the children were in their father’s care.
- Multiple files describe violence where a stepfather had recently taken on a parenting role. In file DS043, the young person received a mobile phone from a friend, which his mother said to conceal from his stepfather. Upon discovering the phone, the stepfather was described as “destroy[ing] it by throwing it across the room”, “screaming and shouting”.
- In another file (DS456), the dynamic between a young person, her mother, her mother’s current partner and the mother and current partner’s two sons led to a situation where the adult male used violence towards the young person. Case notes reflect concerns that the mother may be under the influence of her partner, who is known to other services as controlling. Case notes record that the partner makes threats to take the children away and exhibits controlling behaviour and verbal abuse.
- In file DS311, case notes state that the young person and their older brother have seen and heard a lot of fighting, including different types of physical and emotional abuse as well as gaslighting. Case notes indicate that the ex-partner has spent a lot of time trying to make the children believe that the mother deserves everything he was doing.
- Case notes from another family (DS021) refer to the young person’s father instilling distrust in the young person regarding the school welfare worker and encouraging the young person not to talk to them, leaving the young person without any external support.
Similarly, parent interviews suggested that prolonged co-parenting abuse and coercive control stood out as potentially having an impact equal to or greater than earlier physical and emotional violence.
God knows how much hatred he says over the phone to my daughter about me. (Parent 3)
I’ve had so many bouts of depression over the last 10 or 15 years because I haven’t coped with what’s going on … And it completely hasn’t been spoken about because I’ve been too ashamed or too scared … and then later on when I when my [physical health deteriorated] … we couldn’t say anything because he could turn up at any time and take the kids and I couldn’t do anything about it. And when I [went into hospital] … I said to [the kids], “Look, this is another option, instead of you getting separated and going into care, you could go to your Dad’s” and it was like “No way, no way” and they weren’t mentioning or saying anything to anyone where it might get back to him … I don’t know how he would go if he found out about [young person]. (Parent 1)
I picked [young person] up one day and he said that [ex-partner] had strangled him, so I reported that to the police … and [ex-partner] made a whole lot of allegations about me … Child Protection turned up and I thought they were coming because I’d [reported], but actually they were coming because he’d been reporting me … and [ex-partner] actually ended up getting extra time with the kids instead of less … Basically, I wasn’t believed … You know, it was so expensive … and in the end I just, I basically ran out of money. (Parent 2)
The ongoing impact of adult-perpetrated DFV included separated fathers using coercive and controlling tactics to limit young people’s access to a range of positive extracurricular activities. Examples of controlling behaviour included a refusal to pay child support, with one parent stating that her daughter had two jobs to pay for her activities which she sought to give her a positive outlet outside the environment at home (Parent 1).
When the kids joined [extracurricular activity], [ex-partner] initially agreed but then changed his mind … and because … they weren’t at home for pick up on that Saturday morning even though [he] knew about this weeks in advance, we ended up having the police turn up … to come and collect the kids … and [he]’s on the other side going “I want these kids now” and like they were so embarrassed and hurt. And there’s been other sporting events where he would do exactly the same … So the kids didn’t wanna play sport anymore because they don’t want this happening in front of their friends … (Parent 1)
Other examples included perpetrator fathers manipulating the contact that young people had with support practitioners – particularly psychologists or school counsellors – in an effort to perpetuate control.
There was a counsellor at the school that [young person] was talking to a little bit, but then [ex-partner] went and saw her and apparently cried. And she told [young person] that he really should go start going to see his dad because his dad’s so upset. And I … met with her and the principal and I said, “Look, I don’t think that’s appropriate, [young person] is the child and the victim here. [Ex-partner] is not the victim. Even though he thinks he’s the victim.” (Parent 2)
Because it was quite an abusive situation and they were all going through lots of different things, the counsellor they were all seeing decided to, with my consent … reach out to my ex-husband to say “Hey, you need to back off because this is what’s happening at the moment with the kids and this is what they’re experiencing” … and then he’s taken it upon himself to send each child an individual letter letting them know that “I’ve spoken to your counsellor. They’ve told me everything that you’re going through and they’re gonna help us get together.” And my kids were ropeable because they felt like she had told them everything that they had told her. Yeah, and she hadn’t … and ever since then they won’t speak to anybody … because they don’t have that trust there. I get where she was coming from. Somebody had to tell him to back up because [he] wasn’t listening to anyone … but then he turned around and has just thrown it all back in our faces andit was just so wrong for everybody. (Parent 1)
The interviews with parents and case file review signalled a particular challenge in relation to perpetrator fathers withholding consent for their young person to be involved in support services, especially if language around “DFV” is invoked.
[Practitioner] was really supporting me … suggesting all these great things and talking about things we could do, but when it was time for when we needed [ex-partner’s] consent for anything, [ex-partner] wouldn’t … once he saw [the reference to DFV] he wouldn’t buy it … I feel like, you know, that [program] could have done good things for us if the consent hadn’t been quashed. (Parent 2)
Having encountered this challenge, practitioners in the case study program reported that they often now presented themselves as providing more universal support for a young person, whether it be for behaviour at school or for their wider mental health, to facilitate consent from perpetrator parents. Similarly, the mother quoted above described a contrasting experience where she had been able to obtain her former partner’s consent for her child to receive general counselling from a psychologist, noting that her younger child nonetheless missed out on this type of support as he did not want it to be brought to his father’s attention.
… so he was comfortable about that because she wasn’t a domestic violence practitioner and he had arranged that. So, you know, if he feels like he’s in control [it’s okay but] if he feels like he’s not in control he makes things really difficult … [Younger sibling] did say that he wanted to talk to someone one day and I said “Well okay, you know, your dad would have to actually agree to doing that, but do you want me to, you know, organise something?” And he kind of went “No, no, don’t worry about it.” (Parent 2)
Services attuned to these patterns of behaviour described the importance of maintaining a lens on adult-perpetrated harm as a central consideration to their work.
It’s generally us that are identifying the violence [that a young person is experiencing] … It’s after asking those questions about their safety and their side of the story. Because often they haven’t been asked or they haven’t been believed. (Practitioner 46)
Practitioners described needing to account for potential interference in the benefits of their program by the presence of ongoing adult-perpetrated DFV, highlighting that a young person often moved between their primary place of residence and the home of a separated father.
You know the challenge for us is that we’re trying to, you know, how do we not let that work that we’re potentially doing with the young people not be undermined in the family home and at dad’s place as well? (Practitioner 23)
Noting that specialist DFV services had conventionally “shied away” from clinical work with families where children were still having contact with an adult perpetrator, some practitioners insisted that this should not be a reason for young people missing out on services: “The only reason we won’t work with the families is if it’s going to increase family violence, risk and safety factors” (Practitioner 22).
This insistence was significant, given that practitioners from this program noted that “all but two” referrals had involved an adult male perpetrator who was actually still residing in the home, rather than just being involved in a young person’s life in the context of shared parenting arrangements (Practitioner 26). Practitioners from another program described the ongoing presence of an adult male on a full exclusion protection order while a mother faced violence from her child as well.
I had [one case where] police attended for an [AVITH] call and the [adult] male perpetrator of DFV who has a full exclusion intervention order was within 100 metres of the house and the police officer responded to the mum … “He’s [adult perpetrator] probably 101 metres, so we’re not going to charge him.” So, she’s … experiencing [AVITH] as well and she gets that response. (Practitioner 21)
Experiences of ongoing adult-perpetrated DFV therefore remain crucial to highlight. This is because, while evidence continues to acknowledge exposure to prior adult-perpetrated DFV as a major contributor to the use of AVITH (Contreras et al., 2020; Fagan, 2020; Fitz-Gibbon et al., 2021; Gallego et al., 2019; Meyer et al., 2021; Nowakowski-Sims, 2019; Perkins et al., 2021; Tucker et al., 2020; Walker & Woerner, 2018), studies give less emphasis to the ongoing presence of DFV, either in the home or in the context of separated families. Studies highlight the high prevalence of sole parent mothers as victims and survivors of AVITH (Armstrong et al., 2018; Fitz-Gibbon et al., 2018), including one study that suggests that AVITH exists in 20 per cent of sole parent homes (Armstrong et al., 2018; noting here that 57% of case files reviewed for this research involved a young person living with a sole parent mother).
The lack of emphasis on current adult-perpetrated DFV, however, may result from assumptions that where parents are separated the violence has ceased. This assumption stands in stark contrast with significant recognition of separation as one of the highest risk periods for the escalation of violence, as well as the ongoing impact of protracted family law proceedings (Bagshaw et al., 2011; Brown, 2006; Katz, 2019; Maher et al., 2021; Spearman et al., 2022; Thiara & Humphreys, 2015). The lack of emphasis on current, or ongoing, adult-perpetrated violence may also result from an acknowledged lack of young people’s voices. Evidence certainly indicates that young people and family members impacted by AVITH rarely have the opportunity to tell their story (Campbell et al., 2020; Condry & Miles, 2021; Papamichail & Bates, 2020). This is particularly the case with young people who – often having experienced violence as well as using it – can feelthat their own experience is ignored or that it is considered worthless (Campbell et al., 2020; Condry & Miles, 2021).
Research also suggests that young people may blame themselves for their own adverse childhood experiences and sense of emotional rejection from parents (Burck, 2021; Papamichail & Bates, 2020), with feelings of parental rejection recognised as a core contributor to AVITH in the literature (Contreras & del Carmen Cano, 2019). This is echoed in feelings of guilt and rejection in the descriptions of young people’s experiences in parent interviews. Also evident in the case files was the sense of responsibility and fear shouldered by siblings, with many taking on a protective role for the mother, seeking out help, or living in fear at home.
Sibling experiences
- In file DS631, the young person reported to the DS practitioner that, during conflict between the young person and his father, the young person’s brother gets scared and hides under his bed. The young person questioned why his younger brother was not engaged with the service and felt that his brother should be contacted because he often gets forgotten about.
- In another instance where a sibling was engaged with DS due to a young person’s use of violence (DS076), the sibling identified his role in the family as being to look out for his mother and two sisters and always being available to help his mother. This sibling reported that, when he thinks about the significant physical violence used by his elder brother against his mother, he feels upset and gets a stomach-ache. This sibling also witnessed a history of violence perpetrated by his father against his mother. DS identified the sibling as also being at risk of using violence, with case notes indicating that the sibling had been fighting with his eldest brother and the rest of the family.
Barriers to service engagement: The link between trauma and shame
Whether related to previous or ongoing adult-perpetrated DFV, a strong theme in the current study was the shame that many mothers experienced in relation to the presence of AVITH and the links of this shame to their own experiences of wider trauma. This included the way in which their relationship with their child had been undermined by their current or former partner.
There’s almost always trauma. Significant trauma in a family or from impact of family violence on the family, or childhood abuse with the mother … which makes it really hard for mothers to hold on to their parenting strategies to stay regulated. They freeze or they disappear. (Practitioner 1)
Parent interviews reflected the impacts of prior adult-perpetrated DFV on their capacity to manage their response to a young person’s use of harm.
I can see him crashing and burning and it’s heartbreaking … because he’s also quite abusive … which then sets off triggers. So, it’s sort of “I wanna give you the love, but shit!” … When you’ve got someone screaming verbal abuse at you, it’s just really difficult to try to do that. (Parent 1)
I just feel like, I sometimes wonder if I’m being manipulated … Sometimes it’s worse than others. Like, you know, it’ll be months at a time where things are relatively okay and I’ll go, “Oh, you know, thank God I can, you know, breathe a bit.” (Parent 2)
Certainly, noting the evidence referred to in Part 1, experiences of adult-perpetrated DFV can not only impact on mothers’ feelings of shame but also on their capacity to parent effectively (Hernández et al., 2020), and on their feelings of psychological distress when responding to their children’s own use of harm (Burck, 2021; Jouriles et al., 2021). Evidence similarly suggests that children exposed to adult-perpetrated DFV frequently do not access appropriate services or treatment to assist them to recover (Stylianou & Elbright, 2021). This was apparent in the case file reviews (explored in Part 3 in the context of supports provided by the DS program) as well as in interviews with parents.
The thing is their anger, their sadness, their grief, their fear … being rejected because their father doesn’t want anything to do with them or treated them so horribly … has never been discussed with my kids … I’ve never brought it up … I’m too scared with the ramifications that would come if we started having those discussions … We’re still mending. (Parent 1)
Linked to experiences of shame in the current study was the way in which different sector conceptualisations sat in tension with one another, and the phenomenon of AVITH – as well as its drivers – not being well understood. Practitioners described how parents who sought help could be left feeling blamed for the young person’s use of violence at home if the young person’s behaviour was not apparent in another context, such as at school.
They feel stigmatised that it’s their fault, that they’re not able to control their naughty child. (Practitioner 62)
I think there’s a lot of fear in other services about being able to hold risk as well and, like, unpack it a bit more … because it’s still very mother-blaming as well, like this young person has these behaviours, but obviously this is Mum’s fault because she stayed in that relationship, like we are still in that narrative a bit sometimes … (Practitioner 25).
… you see the same submissions made by [Child Protection] that were made 10 years ago … (Practitioner 67)
Parents participating in the research described experiencing blame and minimisation of their family’s needs when contacting specialist DFV services or intake points.
… places like Orange Door … they gave me such a hard time that [young person] had no support or I haven’t done enough for him … I spoke to one person on the phone. And then somebody else has been trying to ring [young person] … “Why hasn’t he answered the phone?”… He finally answered the phone to some person who wasn’t the person I initially spoke to and they had a bit of a conversation with him. They left me a message on my answering machine saying “We’ve checked in with [young person]. He’s all good. We’re closing our books on you.” … He’s talk[ed] suicide twice. There’s self-harm. Who disengages? This is a kid that doesn’t go to school, doesn’t get out of bed. And you’re telling me he’s all okay? Like my God, that was it? And I rang up, I was so frustrated. And I’m like, “You told me this time you’re gonna come in and help.” [And they said] “But he said he’s fine. He’s going to school.” I’m like, “He went to school for one day” … (Parent 1)
Parents also described feeling that they were not imposing enough boundaries. This included having the behaviour minimised by extended family and suggestions that it was the parent’s fault.
… when [my son] was really struggling [during a difficult time] … and he would throw … trash cans and huge tantrums … And my father turned around and said, “He just needs a firm hand” … [My son] was just really struggling with the whole dynamics of everything … Now if they ask me how I’m going I say … how easy it’s going … I don’t say anything. (Parent 1)
[My mother] will say to me, “You’ve gone out, you know, on Friday night” and “Your kids need you. They need you to be home” … That’s part of where the anxiety comes from. (Parent 3)
Just as relevantly, parents described feeling exhausted and drained by their experiences, or limited in their options across their wider lives.
I’ve been in the same job a long time. I’d like to look for a different job … but I don’t have the mental energy to do that … because I’ve got all this stuff in the background that I have to deal with all the time. (Parent 2)
I felt like as a single parent, as a young mother … I felt like if I wasn’t there, you know, that I was completely detrimentally affecting them and completely failing (Parent 3).
If I’m mentally healthier, happier, I cope with it a little bit better and when I’m not, I don’t. And there’s been a couple of times I’ve walked out and I’ve just driven a couple of streets away down a back road and sat there and cried in my car. I’ve had a couple of times …where I didn’t think I was gonna make it through … It’s really overwhelming when you don’t get to replenish yourself … Somebody once described it as you’ve got a cup full of tea and … the tea leaves in your cup need to be rehydrated. Like they’re just totally dry. (Parent 1)
Echoing crucial existing research (Burck, 2021; Condry & Miles, 2021), practitioners volunteered that stigma and shame were a significant factor for young people as well.
… the trajectory of trauma into the adolescent phase of development with these young people piecing together their identity … at a time when their brains are expanding, they’re putting all this together, sitting with the grief and loss around their histories. (Practitioner 26)
Parents participating in interviews for the research also described their young people being shamed by their interactions with support professionals.
The psychologist said, “You realise you look older than you are, you will become prey for older men” … That’s why [my daughter] didn’t wanna see her again. And I don’t blame her … she didn’t want to do it [counselling through DS] because she already had that experience. (Parent 3)
Practitioner observations also included the way in which shame could sometimes be deployed by parents who did not have the skills, were not ready, or were still too traumatised themselves to take other approaches, contributing to one program’s reluctance to use group work combining young people and parents.
If the caregiver isn’t ready and they’re not in that right space and they want to shame that child, I’ve seen it done and to shut it down sometimes is really, really hard. (Practitioner 5)
Disability, mental health issues, wider trauma and complex needs
Disability
A significant number of presenting needs apparent across the research were related to disability. This is highlighted as a feature in other recent Australian studies (Fitz-Gibbon et al., 2018; Kehoe et al., 2020; Meyer et al., 2021) and is echoed in the findings of the PIPA project, which explored in detail the co-occurrence of disability in young people identified as using AVITH in the context of Victoria’s DFV response (Campbell et al., 2020). The PIPA project found that approximately 50 per cent of young people in a wider legal sample had some kind of disability (including psychosocial disability), while nearly 25 per cent of young people in a court file sample had been diagnosed with autism spectrum disorder (ASD) (Campbell et al., 2020).
Similarly, of the 33 files reviewed for the case study, 39 per cent involved at least one member of the family disclosing a disability or disorder. Echoing the rates in the PIPA project, the most common diagnoses were ASD (24%), attention deficit hyperactivity disorder (ADHD; 21%) and oppositional defiant disorder (6%). Seven young people were diagnosed with more than one disability. In one case, the young person and younger sibling both had diagnoses of ASD, ADHD and anxiety issues (DS 170). In another, the young person had been diagnosed with ASD, anxiety, obsessive compulsive disorder, ADHD and learning difficulties (DS 043), with this family involved with multiple additional services.
It is important to recognise that families experiencing harmful behaviours from young people with disability may be able to access supports through the NDIS and community-based disability providers, although this research highlighted substantial challenges in that regard. The question, however, is whether this behaviour is appropriate to be included in the category of AVITH, particularly where the definition by Pereira and colleagues (2017) specifically excludes it.
By contrast, Victoria’s legislative imperatives mean that young people with disability are being caught up in a highly proactive and often punitive response (Campbell, 2021; Campbell et al., 2020). It is therefore vital to emphasise that the PIPA project’s finding about the significant rate of disability among young people identified as using AVITH in Victoria was a reflection of the way that the Victorian legislative and policy landscape works, rather than an indication that disability and AVITH are inextricably linked (see also Sutherland et al., 2022).
In the context of this particular research, the presence of disability, sometimes involving diagnoses of multiple conditions, in young people identified as using AVITH also suggested that an ongoing lack of appropriate supports for young people with disability was contributing to families experiencing harmful behaviours from their child. This was reflected by one parent in the description of her child’s experience.
[My child] wasn’t very great at regulating his emotions … he would lash out a lot when he’s [at school and] being treated differently to others. He would think something was unfair because he wasn’t treated the same as the next child or he would hurt somebody because they hurt him … He was diagnosed [with ASD and ADHD] when he was eight and we’d been on a waitlist since he was four. We completely missed out on funding until then … (Parent 3)
Practitioners observed that while the needs of families were acute, the supports they received were often inadequate or too difficult to navigate, given that so few young people with disability were able to access the NDIS. This points to the need for greater policy attention and resourcing in this regard, both in terms of access to the NDIS and access to community-based disability services, with resourcing of these services significantly impacted upon the introduction of the NDIS. It also points to the need for wider community-based services to be resourced and family and child services workforces to be trained to respond to clients with disability.
The amount of referrals we’re getting for young people who either have an NDIS plan, or who have a diagnosis and/or disability, that has skyrocketed as well. (Practitioner 19)
A fair few of my kids have got NDIS plans, but the plan doesn’t necessarily always assist the family and what they need … the family don’t always know how to get more support, who to talk to about changing the plan reviews or anything. (Practitioner 8)
Other learning difficulties were also described as compounding distress for young clients: “With dyslexia, we have three to four in one group of ten” (Practitioner 64).
Practitioners described the way in which children with language delays or cognitive impairments could be at additional risk of experiencing violence, as well as at risk of using it: “Kids with speech language problems can’t find the words … they just don’t have the internalised scripts … the brain shuts off and the body takes over” (Practitioner 42).
Certainly, learning difficulties and associated school disengagement were presenting needs for young people in 40 per cent of the case files. The research team heard that language delays and behaviours of concern were being seen more frequently as the eligibility for AVITH services was expanded to include children of an increasingly young age.
For example, the expansion of the existing Step-Up programs in Victoria included the expansion of program eligibility to incorporate children as young as 10, while the eligibility criteria for the newly funded programs also incorporated this age group. One practitioner considered this inappropriate, however, given that 10-year-olds rarely had the capacity to engage with services and, more broadly, had no capacity to change the wider dynamics in a household (Practitioner 17).
They opened it up to … to see how many we would get … services are actually getting those young children … and they don’t know what to do with the behaviour. (Practitioner 5)
Particular learning needs were highlighted by parents as having a serious impact on young people when not appropriately recognised, either by schools or by adult perpetrators in their lives.
Because [they said] he was a danger to himself and other children … the teacher wouldn’t understand … they would just remove him. (Parent 3)
[Young person] … had a few different things going on with his [vision] … we went and got him tested, we’ve had all these procedures … and because [ex-partner] wasn’t involved at all, it was like, “That doesn’t exist”, “You’re all speaking crap” … And he wouldn’t let [young person] … wear his glasses, he was taking them off him and putting them away while he was in his care and he would let him ride bikes and stuff, so he was forever going to … hospital. (Parent 1)
Echoing the intersection of learning or support needs with the impacts of adult perpetration, focus group participants also suggested that many young people’s needs, including those identified as stemming from disability, were inextricably linked with trauma.
Often when children have been acting out or perpetrating, inverted commas, family violence they have also been at the receiving end of it … and in many cases [this is] complicated by the fact that they’re often children with complex other needs, trauma or autistic children, children with intellectual disabilities. (Practitioner 68)
I think it’s really hard to distinguish for a lot of our clients whether it is a behaviour that’s coming from a diagnosis or disability, or whether it actually is AVITH. (Practitioner 19)
When they’re using violence, that’s telling us something. That’s giving us information about what their experience has been like and their development. (Practitioner 29)
Mental health
Also very apparent across the research was the prevalence of mental health issues. Emotional, behavioural or mental health symptoms were identified in 78 per cent of cases, while parental mental health was identified as a risk factor present in 60 per cent. Anxiety was a co-occurring presenting need for 48.5 per cent of families and depression for 24 per cent. Instances of self-harm, including suicidal ideation, were identified in 33.3 per cent of the files.
Literature confirms that young people and families impacted by AVITH experience a range of co-occurring issues which both contribute to and compound the effects of their behaviour (Malti et al., 2018). These include severe mental health issues, such as acute psychological distress, suicidal ideation and self-harming behaviours (Kehoe et al., 2020; Martinez-Ferrer et al., 2020), as well as low levels of “family and social self-concept” (Martinez-Ferrer et al., 2020).
Practitioners working in acute mental health contexts, including hospital emergency departments, also described the relationship of experiences of trauma to serious mental health presentations in young people who were using violence. This reflected what was described anecdotally by practitioners working in these contexts as a significant increase in presentations of young people using AVITH to emergency departments during Victoria’s extended lockdowns throughout 2020 and 2021, including as a result of being brought there by police in lieu of a protection order response.
… so those young people that present often to our emergency department, it’s probably one of the most predictable experiences that they have in their day or in their week … it’s almost like a … co-regulation … but it’s occurring in the emergency department because it’s the safest place and most predictable space. (Practitioner 41)
The research team heard about parents seeking help from emergency departments for their child’s behaviour while presenting with their own mental health issues as well.
It’s all also overlaid with parents, who more than likely have their own neurodevelopmental problems and mental health problems, shame around feeling like they’re failures as parents … [We have to assess] what’s the adult’s capacity and resilience around their own self-regulation, their own mental health … (Practitioner 42)
The biggest thing I think, for a lot of our families, or a lot of our young people, is that they literally do not have the tools to do this by themselves. (Practitioner 18)
The response that young people and families receive in these settings, however, may be somewhat dependent on the experience of the staff in each hospital, as suggested by this reflection from a parent.
So there was a lot of support around for that, but with headspace [National Youth Mental Health Foundation] saying “Get your child to a hospital”, it took me three hours to get [young person] to the hospital and when we got there, there was no paediatric person on call at all. And so we had to wait three hours and after 15, 20 minutes, [he] was already going “Get me out of here.” And [by the time they got somebody in there] he goes “I’m not interested, I’m just gonna tell ’em what they wanna hear.” And when we got in there, he said to the guy, “Yeah, no, I’m fine.” The … doctor [said to me.] “You’re just exaggerating it. Go home.” I will never be able to get him to hospital again. I’ll never be able to go down that path. (Parent 1)
Case files also highlighted the ways in which mental health was a factor for families experiencing AVITH – for parents and siblings, as well as for young people using harm.
Mental health presentations, including self-harm and suicidal ideation
- One family (DS170) had been in and out of the Royal Children’s Hospital for support around a young person’s eating disorder.
- In another family (DS532; DS236), mental health concerns arose upon the discovery of homicidal material (towards children and animals) in the young person’s room. Following assessment, the young person was diagnosed with psychosis and schizophrenia and held involuntarily in hospital under relevant mental health legislation.
- In case DS126, the 11-year-old sibling of a young person using violence reported that her mother was often “not well”, staying in bed and being absent from the young person and her brother’s lives for days and nights at a time.
- In one case (DS098), the young person had been in an inpatient mental health unit and moved into unstable housing (homelessness and then in emergency accommodation) before eventually moving in with his father, who had been abusive to the young person in the past.
- In one file (DS043), the loss of a close friend resulted in the young person self-harming and threatening to suicide.
- In DS456, the young person was severely self-harming and the DS practitioner advised the young person’s mother to call an ambulance and a suicide hotline.
The case files also indicated how experiences of adult-perpetrated DFV could intersect with mental ill health in parents and intergenerational harm to compound trauma for young people, including files indicating histories of intergenerational drug use and adult-perpetrated DFV as well as severe mental health issues, including suicide of young people’s parents.
Bullying
Also emerging as a sub-theme across the research – related to young people’s mental health as well as to their use of harm – were experiences of bullying. Emerging studies show the relationship of bullying victimisation with the use of violence at home (Espejo-Siles et al., 2020), and practitioners similarly volunteered that young people’s experiences of bullying were common in their client base, potentially related to attempts to act out after their experiences or to regain a sense of control.
If bullying is present, you can see that come into the home. (Practitioner 3)
We would probably get well around 80 per cent [who have] experienced bullying or are the bully themselves or are a mixture of both. (Practitioner 64)
Practitioners explained that experiences of bullying could further isolate young people who were already facing additional challenges, including violence at home or cognitive or other learning delays.
… one young man who, when we talk about different strategies of, you know, how does he cope with [being bullied] he just talks about, like, positioning himself in certain places in the school yard and … his strategy has just been to basically not interact with anyone. (Practitioner 63)
Of note, experiences of bullying victimisation were also volunteered in a parent interview as a contributing factor to the use of coercive controlling tactics by perpetrator fathers: “[Ex-partner] said that he was the youngest and his older brothers bullied him, and so he’s not gonna allow [young person] to bully [younger sibling]” (Parent 2).
The case file review also demonstrated that bullying was a presenting need in 24 per cent of files as either perpetrated against, or by, the young person using violence, although victimisation appeared to be a greater factor, leading to disengagement from school.
Bullying and school disengagement
- In one case (DS631), the young person refused to eat at school because this was the reason for being bullied previously. His experience of bullying included an incident of physical violence from a large group of other children which resulted in his hospitalisation.
- In another file (DS932), case information reveals that the young person was being bullied and had been acting out at school as the result of an inability to regulate his emotions. Case notes state that the young person was becoming physically violent and attacked other students after being bullied for an extended period of months. The young person’s mother did not know about his experiences of bullying until this attack on other students.
Wider trauma and complex needs
It is important to highlight that the research indicated wider forms of trauma and marginalisation were also presenting needs in families and young people experiencing AVITH. Certainly, a wider evidence base establishes a link between adverse childhood experiences and a range of behavioural or developmental problems in adolescence (Docherty et al., 2018; Malvaso et al., 2019), as well as a correlation between individual, familial and social experiences of disadvantage and disconnection and use of harm in close relationships by young people (Blakemore et al., 2018).
Adverse childhood experiences can include traumatic refugee experiences which shape children’s neurodevelopment and can lead to associated hypervigilance and behaviours (Campbell et al., 2020; Lamb, 2018), as well as structural barriers and systemic racism (Fagan, 2020), including over-policing and differential legal responses (Armstrong et al., 2021).
Emerging studies have also begun to highlight the relationship between intergenerational trauma and the significant impacts of AVITH in the context of kinship care placements (Breman et al., 2018; Gair et al., 2019; Holt & Birchall, 2020), as well as the relationship of pre-existing trauma and child removal to the prevalence of AVITH in adoptive families (Selwyn & Meakings, 2016). Researchers have therefore called for a greater focus on intersectionality and experiences over the life cycle in the context of use of AVITH (Holt & Shan, 2018), rather than a focus primarily on adolescence.
Recognition of intersectionality and trauma experiences over the life cycle were a feature of the case file review. For example, trauma was a co-occurring presenting need for 91 per cent of families, with qualitative data describing families fleeing persecution; families living in a refugee camp; young people witnessing a parental suicide attempt; the loss of a parent or loved one (in one case to COVID-19), combined with lockdown; child removal and adoption; and the bullying and adult-perpetrated DFV described above.
The case file review indicated that 24 per cent of cases involved at least one family member born outside of Australia and 12 per cent speaking a language other than English at home. Some case files highlighted that experiences of marginalisation can intersect with use of harmful behaviour by young people, while experiences of adult-perpetrated DFV can further marginalise families and young people.
Exclusion from services and marginalisation
- Two families explicitly reported experiencing exclusion from services as a result of their CALD background (DS236; DS098).
- Another young person reported that, when her family migrated to Australia, she felt that she had to be the “strong one for the family … I had to be okay and make my parents not worry” (DS482).
- One family of six (DS098) were born in the Horn of Africa and were once in a refugee camp, with case notes indicating the impact of racism on a younger sibling, including verbal taunts at school. In this case, the father had a history of using violence within the family, but because he was the only family member who could speak English, he was the main contact person for engagement.
One young person across the files identified as Aboriginal (noting that two case files did not report the young person’s Aboriginal and/or Torres Strait Islander status) and their file involved experiences of child removal and complex mental health and learning difficulties, for which the young person was linked in with a range of different supports.
More broadly, as well as trauma from adult-perpetrated DFV as the predominant experience, the experiences of the parent sample included separation from children; a lack of emotional and/or pragmatic support from extended family; early parenthood in one case; and experiences of childhood sexual abuse, including the abuse not being believed by the other parent. Siblings, as described by parents, had also experienced wider trauma, including sexual assault external to the family and stigma associated with that experience.
A particular sub-theme to emerge from the research findings was the impact of prior periods of separation as a result of mothers’ physical ill health, leading to disrupted attachments between mothers and children. Experiences of grief, separation and wider trauma appeared to play a significant role in the contexts described by two out of the three parents interviewed. This included the experience of one parent who, post separation from her abusive partner, had required hospitalisation for a long-term injury and, lacking other appropriate supports, felt she had no other choice but to have her children separated and placed in temporary out-of-home care.
A lot of people were saying, “They’ll be right. They’re only young, they’ll be right” … [but the kids were saying,] “What happens if you die? What happens if you can never walk again? What happens to us?” … And that was a real fear for them all … [Older child] had a huge amount of trauma … He really, really struggled and left home early because he was the adult in the family for so many years, he really struggled to give me back that power of being the adult and him being a kid … It’s taken us huge amounts of work for us to mend our relationship, which that itself has also had damage on [adolescent child]. (Parent 1)
This was also a theme in two of the case files.
Maternal guilt and separation
- A mother in one family disclosed falling ill and being in a coma a few years prior to the young person’s use of violence began and believed that, during this time, the young person became “angry at her for something outside of her control” (DS838).
- In another file (DS098), a mother revealed that she had a long-term illness for which she had twice been hospitalised for a significant time, and which she feels has impacted her children’s development and childhood.
Practice challenges: COVID-19 compounding risk and needs
Echoing the literature referenced in Part 1 of this report, practice reflections emerging across the research indicated particular challenges in supporting and engaging with young people during COVID-19. In particular, practitioners described the challenges encountered when face-to-face engagement with young people was suspended in the context of Victoria’s first lockdowns.
What we’ve learned from that is that we lost a lot of engagement from young people and that the most effective way to try and engage them is face to face. (Practitioner 21)
This was a challenge reflected in some of the case files.
Need for face-to-face engagement with young people
- In one case (DS678), after multiple attempts from DS to engage the young person’s grandmother (with whom two young people using violence were living), the grandmother stated that she did not wish to continue to receive support through DS as ongoing lockdowns prevented them from continuing face-to-face.
- In another file (DS169), case notes indicate that during lockdown the young person completely disengaged from school because of the online learning environment and refused to attend other appointments, either online or by phone. Instead, the young person’s mother suggested a face-to-face visit as the young person was comfortable engaging in “small talk” with adults in a face-to-face context while also having the option to choose to leave the physical environment.
This was also a very real challenge for two of the three parents interviewed. Although all three mothers described benefits from the support that they had been able to receive themselves from DS, in two cases, DS had not been able to engage with their children, primarily because of COVID-19-related restrictions.
I needed physical help … but COVID happened at the same time … which of course just crashed and burned everything. I needed somebody … to come in who can physically help support [young person] with getting him over the line with anxiety, depression, getting him out of bed, maybe having some sort of “let’s go kick the ball” to build some sort of rapport with him … But while things are only over the phone … that’s not helping. (Parent 1)
The children had practitioners assigned to them but because of COVID we weren’t able to see them. (Parent 3)
One parent also described the impacts of COVID-19 escalating risk and conflict between her and her ex-partner, who was still involved in the children’s lives (and who had denied consent for his children to be supported by the DS program).
When [changeover] is on the school day, he picks him up from school and he takes him to school the next day. So, I don’t see him … [but] one of the things with the whole lockdowns [during COVID-19] was, because they weren’t doing the changeovers at school, we were seeing each other all the time (Parent 2).
Even where practitioners were able to maintain contact and engagement with young people, focus groups also highlighted the challenges for their practice and the support which they could facilitate where other services were not available during the lockdown periods.
Some of these young people have absolutely no supports in place at that point … If we’ve received a referral during lockdown, there’s absolutely nothing in place … (Practitioner 64)
Practitioners also described challenges related to service uptake, where other service networks and practitioners were either not aware that the service was available or were not necessarily confident that they could offer a young client or family the requisite support during lockdown.
We will sort of put out like a big generic email and I’ll get a few calls and do a few consults and we’ll have a boom time … then it’s because we keep opening and closing with lockdowns and it’s like that they forget that the program’s there again. (Practitioner 62)
Impacts of technology
Intertwined with the impacts of COVID-19 were the particular challenges associated with young people’s increasing use of technology. Although this was not a significant theme raised by practitioners across the research or by parents in interviews, use of violence related to technology was a significant feature on 21.2 per cent of case files, contributing to a stressful home environment and placing additional pressure on parents, as well as contributing to young people’s anxiety, isolation and lack of sleep.
Use of technology in the context of COVID-19
- In one file (DS043), a young person physically assaulted his mother when his stepfather took the TV remote away. The stepfather’s frustration stemmed from the fact that the young person was watching TV rather than helping with chores around the house.
- Similarly, a mother raised concerns about a young person’s device usage and time spent alone in his room (DS169), and worried about managing this over the school holidays. The mother informed DS that the situation “blew up” after she turned the internet off at 10:00 pm.
- In one file (DS237), a mother reported that the young person had ceased attending school, hardly came out of his room and stayed up all night watching TV. Case file notes indicate that the DS practitioner asked what it would look like if the mother removed the TV, to which the mother reportedly responded, “I wouldn’t even try … I don’t want to know.” The mother added that the young person communicates in an aggressive manner, harasses her and blocks her access to exits when she attempts to set boundaries.
- In another example (DS578), a young person’s mother described an incident where she confiscated the young person’s Xbox remote as it was late at night. The mother went to return to bed and the young person “attacked” her from behind, hit her and pushed her against the wall.
System challenges: Under-serviced and over-serviced families
As well as the practice challenges described above, substantial systemic barriers also emerged across the research which, in turn, limited effective practice. Particular systemic challenges included the extent to which families who experienced AVITH were either significantly under-serviced, as the PIPA project described, or – conversely – over-serviced and immersed in service intervention. Sometimes the experience of multiple services in a family or young person’s life could ultimately result in them having received no useful intervention at all – leaving them under-serviced, despite constant service system activity.
Focus groups highlighted the ways in which some families had been identified by the system for the first time. In particular, practitioners highlighted the lack of service support for children who had been exposed to adult-perpetrated DFV, as reflected in the literature (Stylianou & Ebright, 2021), and in the parent interviews.
One I have now is quite young, 13, and has had no issues in the past. Just been diagnosed with ASD. A lot of family issues, a lot of family violence witnessed in the past. Still sort of witnessing it from Dad as well … He’s started showing symptoms of the gaslighting and things like that as well … They’ve sort of never had any services before (Practitioner 14).
Practitioners described families or young people who had opted not to engage and felt that they could address their situation themselves.
We get people who it’s their first entry point, really tried to manage everything themselves their whole life and it’s just got to the point where they can’t anymore. (Practitioner 6)
Not everyone wants services. Lots of times they’re calling, they just want support. They just want to understand the situation. (Practitioner 61)
Practitioners also described families experiencing significant needs who had not had these needs addressed and were presenting to an AVITH-focused intervention having exhausted all other options.
Either there’s just too many services involved, like NDIS shoved a lot onto them, or you’re waiting for those services to become involved and we’re holding that. (Practitioner 19)
We get other people who have been engaging in services since the kids were in kindergarten and they’ve been to different psychologists, different psychiatrists, different paediatricians and we’re really at the end of the line. (Practitioner 6)
We’re creating distrust in services because we’re achieving nothing or only achieving tiny things. (Practitioner 17)
Parents participating in interviews echoed this experience.
I couldn’t tell you who referred me to [DS] because it wasn’t my first organisation. I’ve been trying to sort some support for both my son and us as a family for quite a while. (Parent 1)
A predominant theme across the research, therefore, was the involvement of multiple services in families’ lives without these services having been of any help. This was described as having a detrimental impact on young people and families alike, with legal practitioners commenting that “system fatigue is really big for our kids” (Practitioner 69).
We’re often very mindful about the pressure on young people, particularly in the sense of not being over-serviced and because that can often have quite detrimental impacts on them too that they just have so many people trying to support them. (Practitioner 13)
And sometimes, you know, [mothers] will be getting multiple calls from services after an incident saying, “Hey, what’s happened?” and you’ve got an adult who has been … in a really traumatic experience with their child and having to relive it four times in one day after it’s happened … (Practitioner 26)
This was echoed in parents’ descriptions of their interactions with services as well.
I’m just tired of getting my hopes up with, “Maybe someone can come in and help” and then they don’t … I’m so over having to repeat all of this because when I repeat it, I just realise how sad it sounds … And I feel so sorry because [young person has] had no real support to help get through any aspect … (Parent 1)
Within this context, practitioners described the damaging impacts that could arise from the involvement of multiple services or systems in families’ lives, particularly when this was experienced as punitive in terms of criminalisation of the young person, child removal, or criminalisation of other family members.
I guess when we’re doing safety planning, it’s certainly not the first thing that we would recommend is to contact the police … We don’t want them to be in a situation where they’re too scared to call the police and they get injured themselves but … they don’t know what’s going to happen to their young person … There’s a lot of things that I guess police miss – like in judging who the person using violence is as well … the mum or whoever is calling might be upset and so then police think that it’s that person [who has] been using violence as well. And obviously police reactions and police violence towards Aboriginal people is a big concern … That’s part of something that we work within safety planning with the adults. (Practitioner 73)
I’m a six-month service and it took six months for that family to go “Okay, [practitioner’s name] is okay” …We’re fighting against historical service [exposure with families] who don’t get along with workers … workers that are trying to remove the children and are constantly disciplining the adults. (Practitioner 55)
I think some of the complexities about working in this space is that we’re almost trying to undo a lot of the harmful responses that have occurred … (Practitioner 25)
Just as relevantly, interviews with parents described the way in which negative experiences of service system interaction could mean that young people refused to engage in further referrals, including because of a distrust in “talk therapy” as noted above, as well as the delay between when help was sought and a response from the service system was initiated.
… the fact that you’ve gotta go through such a long process to be triaged and sometimes by the time someone speaks to me and then by the time they try to get to talk to one of the kids, it can be like a couple of weeks. And they will put you on our waiting list and then, “We’ll get someone to get back to you.” But then we don’t hear from anyone for three or four weeks. It sort of defeats the purpose of it all. It’s like [my children] are not important enough for it to be acted on there and then. (Parent 1)
The involvement of multiple services in families’ lives was similarly apparent across the case files. At the time of their referral to DS, families were engaged with a broad range of services, including multiple services at one time. In particular, 48 per cent were involved with mental health services, with primary health (21%) and NDIS (12%) the next most prominent services in families’ lives. While some positive examples of multiple service involvement were evident and are featured in the next part of this report, also evident was the ineffective or damaging impacts of service engagement for some families.
Over-servicing or negative service experiences
- One family (DS-567) specifically identified that, despite the young person and the family having “lots of services involved”, including participation in the Step-Up program, this did not lead to positive improvement in the young person’s behaviour and use of violence. Within this family, the mother had a counsellor and had been in contact with the Orange Door but did not feel that the support offered by these services led to meaningful change in the family.
- One young person who chose not to engage with any of her long-term supports told DS that she “had too many supports already” (DS456).
- For one family (DS169), engagement with a counsellor prior to referral to DS “has left a huge trail of distrust” and impacted the young person and their sibling’s desire to be connected with services in the future. Case notes reveal that the young person attended a mental health service as a result of concerns around suicidality but refused to attend again after the first session, after this was seen as a negative experience by the young person.
Wider literature acknowledges that experiencing multiple co-occurring issues can mean that the needs of these families often do not fit within the remit of any single service (Condry & Miles, 2021). Because of the way in which services are designed and funded, disability or mental health services struggle to respond to DFV, while specialist DFV services – designed to work with victims and survivors – struggle to support young people who are experiencing, but also using, violence (Campbell et al., 2020).
As a result, families are often passed from one service to another, leading to increasing distress (Burck, 2021; Campbell et al., 2020; Fitz-Gibbon et al., 2021) and disillusionment. Having moved between multiple referrals, these families and young people often drop out of service engagement and have little reason to engage with any newly introduced service or practitioner – either because they have no hope that it will help, or they do not want to get their hopes up, as one parent described above.
Evidence further suggests that many families impacted by AVITH have not experienced respectful responses from relevant services (Burck, 2021; Campbell et al., 2020; Condry & Miles, 2021), often compounding this sense of shame or blame. In particular, evidence also suggests that adoptive families may feel a particular sense of blame and parenting failure (Selwyn & Meakings, 2016).
In the context of the current research, parents participating in interviews all shared stories of how they had attempted to engage their children in services (usually private psychologists) in response to their children’s experiences of adult-perpetrated DFV, with this generally being the only service pathway that they had felt was available at the time. A misguided breach of confidentiality, manipulation by an adult perpetrator or a judgemental comment from a professional, however, had made their children permanently reluctant to engage or to make themselves vulnerable by describing their experiences to yet another stranger.
Negative experiences of service intervention therefore left their children under-serviced in their recovery from adult-perpetrated DFV, and suspicious of engagement with any further services. These children’s experiences highlight that the challenge involved in supporting families and young people appropriately involves more than ensuring that they are not under-serviced, on the one hand, or over-serviced on the other. Rather, experiences of service interaction also need to be positive and trauma-informed to ensure that young people and families do not ultimately end up without any meaningful support at all.
System challenges: Siloes not collaboration
Where there was involvement of multiple services in a family’s or young person’s life, the research found that this was not necessarily having a beneficial effect, with families passed from one service to another in what one participant described as an “assess and refer on” model (Practitioner 2), rather than services wrapping around the family or working in a coordinated fashion.
Sometimes it feels like they’ve been ping-ponged around, like they’ve been sent to headspace and … to Step-Up … then to somewhere else … (Practitioner 5)
We’re like little Lone Rangers getting in there trying to move mountains, it’s quite challenging … It’s really not a wraparound approach … It’s just an isolated, “We’ve referred, good enough” kind of approach. (Practitioner 17)
It seems to exist as this kind of relay almost … in that we’re passing the idea or the problem of the family from one person to another instead of coming together … because then there’s also that fear of oversaturation of services as well. (Practitioner 7)
As the above comment suggests, practitioners explained that the lack of a wraparound service model was partly a result of reluctance to have too many services involved at once, as well as services not responding to or providing the type of support that a family was requesting.
They’ve just been bounced around and around and around different services because they’re never quite the right one [and] nobody is listening to what the family is seeking because what we think might be beneficial isn’t necessarily what the family’s needing right now. (Practitioner 22).
I think one of the issues is that the system response is linear. So you’re like either a respondent or you’re a victim, right? And young people, they’re both. (Practitioner 61)
Just as relevantly, participants described a “siloing”, in which services were not prepared to stay “open” if another service was able to “hold the risk”, particularly where they did not consider themselves as the most appropriate service to respond to AVITH, as was noted at the outset of this part of the report.
I’ve got one client who came from Family Services as a referral, and [they were] working with Mum and she’d achieved the majority of her goals in a 12-month period and then these behaviours from her son were worsening and so she’s referred to us and then she’s closed because Mum’s achieved their goals [and now] … that’s another client that I can’t engage. (Practitioner 17)
It’s literally a siloed kind of work … like the way that models are funded, the way that service systems are funded. It can affect the experience of families on the ground in that they just don’t have a destination that’s obvious. (Practitioner 52)
The focus groups highlighted that the “linear” nature of the service system could mean that, while families or young people were passed forward from one service to another, they could not necessarily be passed back the other way if the risk profile was perceived to have changed.
One of the barriers is that the system is not there to back you up when you need it. So, you sort of assume that if it gets to a certain threshold, you’ll be able to contact Child Protection and send it back there. But they’re not interested. I had a family during the lockdown, Mum was really drug affected, really mentally unwell, she broke every window in the house and … [Child Protection] closed before they even spoke to the family. (Practitioner 3)
When we make a report [to Child Protection], it goes to intake. If they don’t do anything about it, we’re still left with the same situation that we’ve got. If it goes to investigation, we have to close, because part of our criteria is that we can’t work with any clients who have investigation with Child Protection, so it’s a bit of a catch 22 for our … clients. The situation either isn’t bad enough for it to go to investigation or it is, and then we’re going to withdraw anyway. (Practitioner 20)
If we see that there’s a high-risk situation with a family [then] we’re going to the Department [i.e. Child Protection] to explore around “How we can keep that family safe?” And our challenge to the Department is, “What are you going to do about it?” And sometimes we don’t get our way, even though we’ve placed all this evidence and notes and everything, you know, facts on the table. (Practitioner 74)
Practitioners from one of the programs explained that the siloed and linear nature of the service response could mean that there was “nobody in between” (Practitioner 57) a crisis response and a community-based model, with young people exited from a crisis service and put onto waiting lists for months. It could also mean that, where a crisis response was engaged, the framework in which this operated could run counter to the understanding of risk from the AVITH-focused intervention and override significant concerns around safety.
You might work with a family and it gets to a threshold where you really need [acute mental health] involved for the young person because the risk of suicide’s huge … but then they are directing the parents to do things that are counter to the principles that we would want to hold on to which are, you know, safety first … [Mental health] is saying to the parent, “You need to use your authority” and I’m like, “Oh my god, Mum’s going to get stabbed if she does that.” (Practitioner 2)
The research team also heard that the siloed nature of the service response impacted the types of information that each service had available. This was because services could pass the baton of families to each other without ensuring that information relevant to risk was also part of this “relay”. It was also because services could “close” their involvement with families without properly engaging or advising that they would no longer be involved.
[The] mum could never remember engaging with the service … she just remembers that they stopped contacting her … She was filling in services on information that they should have been aware of. (Practitioner 8)
We are really siloed in our capacity because we don’t have access to that information sharing. (Practitioner 51)
Noting that “young people are not siloed beings” (Practitioner 57), practitioners suggested that considerably more work needed to occur in order to improve responses and support for young people and families experiencing AVITH – work that should not rely on individual practitioners or programs making connections.
It’s the way that we speak to each other as services as well. It’s like “You do mental health, you do AOD, you do this” … when working with young people, none of that should be particularly siloed. We should all be a little bit aware of each other. (Practitioner 57)
There hasn’t really been consistent practice … services have adapted to meet their own local needs … It’s so dependent on the practitioners that you’ve got and the ability that you’ve got to adapt your own program. (Practitioner 13)
Overall, these findings about a siloed and linear service response echo repeated concerns across research related to DFV responses and point to the need for sufficient resourcing which allows for coordination, integration and follow-up, rather than just a “refer on” or throughput approach. They also point to the need for funding and program models which measure outcomes, rather than outputs – creating time and opportunity for slowed-down service interactions which are more likely to “land”, as practitioners in the research described it, and “get the intervention right the first time”.
System challenges: Care teams
Associated with practitioner concerns around siloed service responses were challenges in relation to care teams. While the use of care teams has become a well-established feature of the Victorian service landscape – in which practitioners from multiple services involved in a young person’s or family’s life meet to discuss their support needs – the research found that these mechanisms were not always providing useful support in the AVITH context in the way that the research team had expected.
In fact, while notable exceptions are highlighted in Part 3 of this report, including in the context of the case study, practitioners participating in the focus groups generally struggled to nominate more than a handful of examples in which a care team had operated for the benefit of a young person. This appeared to be for a number of reasons, outlined below.
Care team purpose
A strong theme in the discussions regarding care teams was practitioner concerns around their perceived purpose. AVITH-focused practitioners – including those working in mental health or AOD service contexts – felt that the purpose of a care team was for services to ensure that a young person was receiving the support that they required to improve their wellbeing, as well as to improve their behaviour. This was not always the way in which a care team’s purpose was perceived by other practitioners, however, with focus groups suggesting that this was a direct result of the binary frameworks in which some other services worked.
When there’s presence of Child Protection in that care team, it defaults back to “Okay now we’ve got to prevent this, we gotta stop this contact happening” and “That could be a breach” … There’s perpetrator language and frameworks creeping into care teams. (Practitioner 52)
These meetings are just about, you know, passing judgement … just making really unnecessary comments about what the young person’s been doing, rather than actually working together to identify what’s not working and … what in our interventions or our support is not helpful? … I think care teams can really lack accountability when the young person isn’t present … we’re providing the service, we’re the ones that need to be accountable. (Practitioner 29)
Care team composition
Directly related to the perceived purpose of a care team was practitioners’ suggestion that the composition of services within the care team was important. Practitioners suggested that the infrequent involvement of the specialist DFV sector in these settings inhibited the capacity of that particular sector to engage with the far less binary and more nuanced nature of AVITH-focused work.
This is not a criticism of the family violence sector, because I know they are doing heroic work with caseloads at double and triple hours and people die on their caseloads and so that’s not the point I’m making. The point I’m making is that they’re not a strong presence in care teams … I cannot think of a time when I’ve had a family violence practitioner in a youth care team or child care team … there is not a presence in that long-term care planning for a child or young person and it’s centred around the caregiver’s experience … I’m not even confident that the family violence sector would have a framework around adolescent family violence … (Practitioner 52)
Where specialist DFV practitioners were not involved in care teams, this also limited that care team’s capacity to acknowledge and respond to the presence of ongoing adult-perpetrated DFV, a practice challenge highlighted in the discussion above.
Intimate partner violence is a huge thing … but it’s not often addressed or spoken about and I find that some workers in care teams have a reluctance in trying to address any of these issues … “I’m AOD, I’m mental health, I’m Child Protection, I’m justice, I’m not a family violence worker.” (Practitioner 53)
Demand and service fatigue
Intertwined with service reluctance to venture into unfamiliar territory, practitioners explained the impact of system “overwhelm”, or pressures from the constant demand across human service systems.
I’ve been part of care teams where I’ve been the new worker or the new addition … and have been able to come in with, you know, fresh eyes, and can just see how fatigued the care team is. (Practitioner 29)
They also described how this fatigue could translate into highly insensitive discussions in front of a young person where they were present in the care team.
[I’ve heard] really extraordinary things said to young people during care teams. A real clanger I saw was a 15-year-old girl where a Child Protection worker with a clipboard said “Okay next, sexual exploitation, what are we doing about that?” to the 15-year-old who was a victim [and] survivor of sexual assault … It says something about systems replicating the damage. (Practitioner 57)
These system pressures could mean that there were often practitioners in a care team who had little visibility of the issues impacting the young person, or who did not feel a sense of connection with – and therefore a sense of accountability to – them. Participants commented that they could often feel “as if they were the only person in that care team advocating for the young person” (Practitioner 29).
A complex care team … [were] phenomenal to talk to and had they had really good ideas about who to bring together and they had the authority to make stuff happen … So I had this, you know, great consultation and plan, but actually that worker never did anything because she’s so swamped and overwhelmed in that role that she actually wasn’t able to action anything at all for the family I worked with, and … the things that I was trying to coordinate around, lots of complex things, you know … We were trying to work across hospitals and mental health and schools. And, you know, a wide variety of things. But over four months, I think, of engaging that complex care team, nothing actually happened. And I think that’s a real shame, because I know that the intention was there to support me in my work, but the capacity, she was just flooded … I needed her authority and she just didn’t have time. (Practitioner 1)
Often, I’m in that care team and I look around and count – how many people have actually met the young person face to face? (Practitioner 44)
Lack of coordination
Practitioners explained that, because of the involvement of too many services in a care team, at times they opted to provide a “secondary consult” role. At other times, they tried to provide much needed coordination, particularly given that there could be a lack of follow-up about the different tasks for which services were supposed to take responsibility. One participant noted that this coordination role was a function missing from AVITH work, but was often present in other service contexts (Practitioner 26).
- There’s been other times when there has been lots of people in the care team meeting but that young person has felt less supported than just having one or two workers because it’s just “Oh no, that’s what this person will be doing” or “Oh no, that’s what that person will be doing” – that assumption that “they’ll be following up” but nothing is actually happening. (Practitioner 30)
- I think that most of the service systems are so defensive it really is dump and run. “We just need to get throughput”, you know? So, actually, in the last five years there’s been no collaboration. You’re better off actually doing it yourself because it’s easier on some levels. (Practitioner 2)
Where there was no one providing a coordination function, practitioners noted that this role often fell back on the victim and survivor parent – usually a sole parent mother – in terms of ensuring that young people accessed the services with which they were supposed to engage. Practitioners further explained that multi-service involvement in a care team could increase the burden on families and young people.
We have quite a lot of young people and they have care team meetings and some of the services that are linked in are not that supportive. It seems that there are a lot of things that they express that the young person isn’t achieving when we’re looking at strengths-based approaches and what the person is achieving … especially when young people have got like six people that they have to attend appointments within a week. And then they have to work full-time and then there’s other commitments and study … I’ve witnessed that in care team meetings I’m thinking, well, “How will they be effectively supporting this young person to move forward and reach their goals when they’re in a very negative space in that environment?” (Practitioner 58)
The bigger the care team, the more control we’re putting onto families … We end up just doing a whole bunch of prescribing … and particularly young people, often their behaviour escalates in those situations because they’re like, “Stuff this, why am I talking to three different workers? I don’t even know what all of you do.” (Practitioner 10)
System challenges: Barriers in knowledge sharing and engagement
Despite the lack of consistent frameworks within AVITH-focused interventions, the challenges in relation to care teams appeared to be a consequence of a lack of wider system conceptualisations and capacity to share knowledge.
The collaboration is often actually around having a coherent conceptualisation. We hold the direction of the work and we’re trying to get everyone on the same page and sometimes that might actually be in opposition to what [other] services are saying. (Practitioner 2)
[There’s] a lot of defining the program to make it understood to different stakeholders … the lack of knowledge and understanding around adolescent family violence is palpable. (Practitioner 35)
When we first started … we did a lot of drive back then in terms of community awareness and all those sorts of things. I don’t think that much has shifted to be honest. I think there is a little bit more awareness of AVITH … like there’s a few, there’s a handful of people that I could say, yeah, I remember working with those people but … in terms of staff turnover, I think that’s where our issue is … that knowledge is not sustained. (Practitioner 5)
Practitioners explained that the challenges that they encountered were not limited to the wider service sector, including having to advocate to their own organisations or funders about why they tried to work with young people or families for longer, and that “one of the key barriers, I guess, is that we’re always explaining ourselves” (Practitioner 1).
Practitioners suggested that the lack of consistent conceptualisation identified above could, in part, be addressed through co-location in different service contexts. As well as the involvement of DFV practitioners in care teams, practitioners also pointed to the potential benefits of a dedicated AVITH practice lead in each Orange Door, as distinct from the dedicated role focusing on the experience of children and young people as victims and survivors. Practitioners in this research made it very clear that this existing role was not sufficient in terms of incorporating a specific and dedicated “AVITH lens” into this increasingly prominent Victorian point of intake.
More broadly, focus group participants suggested that collaboration and consistent conceptualisation needed to be led at a government level.
There’s been a little bit of engagement, but it didn’t really manifest itself in the way that I think that [government] had advocated that it would or hoped that it would in that it would be a sharing of practice. (Practitioner 2)
As noted in Part 1, at the time that the focus groups were conducted, the CFECFW had been commissioned to establish a community of practice specifically for AVITH-focused interventions. An AVITH-focused practice guide to support risk assessment and management was also being developed as part of the Multi-Agency Risk Assessment and Management framework (MARAM), which is now driving the Victorian response to DFV and was recommended by the RCFV.
More broadly, participants across the focus groups – especially those in established programs – observed the lost opportunities to harness their experiences and practice expertise before the 2021 injection of funding was rolled out. Practitioners from newly funded programs noted that they had not been provided with any design parameters.
I read a lot of textbooks. Actually, I’ve read two textbooks and I read some things like the PIPA project and there was one from Monash [University] and there was a bit of literature from a similar program … about 10 years ago. (Practitioner 17)
Practitioners working in established programs similarly noted the challenges for their own practice, given the lack of specialised training around AVITH or resources. Some had been involved in one-off training, including in 2017 when the PIPA project funded a visit to Australia by one of the founders of Step-Up, Lily Anderson, but this training or similar opportunities were not recurrent.
I found it in the [organisation’s wider] training manual. There was this little piece [about AVITH]. There’s so much emphasis on perpetrators … and it can kind of get lost in that and then the whole community doesn’t even understand that this is a very different issue. (Practitioner 6)
While recognising the absence of training, focus group participants noted that the system demands were such at present that they no longer had the opportunity to share practice experience with each other.
There’s a few of us that have been doing this for a long time, so we’ve probably got some really valuable things where they don’t need to reinvent the wheel … I think about even the collaboration with other [AVITH programs]. We don’t really collaborate that much either. We don’t have capacity … (Practitioner 5)
Overall, practitioners called for significant workforce development, as well as capacity and capability building that included opportunities for clinical supervision and reflective practice to mitigate the impacts of vicarious trauma and the stress of working in this environment. They also called for capability building to ensure that all work “was occurring through a trauma lens” (Practitioner 10) and incorporating understanding of DFV, young people, mental health, disability and neurodevelopment as part of what one practitioner described and others in their focus group agreed was a “specialisation upon specialisation” (Practitioner 16).
Part 3:
Signs of promising practice
Introduction
Having explored the many challenges that the research identified in relation to delivering effective service responses to young people and families experiencing AVITH, this report now turns to an exploration of promising practice demonstrated by practitioners and programs in Victoria. In some examples, the promising practice discussed is subtle and focuses on employing a reflective and critical way of working, signalling the way in which work in this area is continuing to evolve. In other examples, the steps that some programs or services have been able to take have been more concrete.
It is crucial to recognise that the extent to which all programs were able to realise their potential was hampered to a considerable degree by the impacts of the COVID-19 pandemic. The findings in this part of the report should therefore be read with this consideration in mind.
Naming and identifying AVITH as a concept
As discussed in Part 2, practitioners highlighted the engagement challenges involved when a program was clearly identified as being designed to address a young person’s use of harm, or as associated with DFV more broadly. At the time of the focus groups, practitioners from one program which had previously been specifically titled “Adolescent Family Violence” were therefore involved in a process to develop a less alienating name and underpinning concept for their program.
We’ve been quite closely supported by … lived experience consultants who have been providing us with guidance and reflective practice around co-designing this program to really look at what is it that young people are actually wanting in this space? How do we actually design this program in a way that is meeting their needs as an adolescent as well as the broader family system? (Practitioner 27)
Similarly, practitioners from programs that had not initially had references to DFV in their title were nonetheless pushing for a shift in language when interacting with clients or referring to their behaviour.
When the program started, it was designed as a “family violence” program and at the time we were using the term “perpetrator” for people under the age of 18, which never sat really comfortably with me … Very quickly we ascertained that, hang on a minute, [we’ve] actually got a whole bunch of young people here [who] have experienced significant trauma, whether that be from family, violence, neglect, abuse, whatever, that looks like for them [and] while it is still a family violence–based program and it is still about adolescents who use violence in the home, we have a very strong trauma-informed process around what has been their experience of trauma and how do we do this in the best, most trauma informed way? …
[Now] … any opportunity we have, we continually make sure … that we do not use the word “perpetrator”, and we consistently try and shift other people’s thinking and language around that, when the opportunity arises in the most respectful way possible. So if we’re dealing with the school and they’re like “Little Johnny has done whatever, and he’s perpetrating violence against others”, it’s like, “He’s using violence” … trying to do that through that education and that gentle move across … (Practitioner 62)
Practitioners from across the research nonetheless observed that, perhaps in tandem with a shift in language, they had noticed a shift in parental receptiveness to offers of assistance. They similarly described a noticeable difference in the way that families were recognising behaviour as “family violence” and identifying a corresponding need for support.
A lot of the families are coming in through our centralised intake, so calling in for family support, calling in because they’re saying they’re struggling with the young person’s behaviour … the word “violence” is used, “young people using violence”. (Practitioner 32)
Those working in a particular program had also noticed an increase in self-referrals that appeared to correspond with the publicity around the newly opened Orange Door as well as associated community-wide discussion about family violence overall.
Similarly, two parents interviewed for the research had self-identified that they needed support in relation to their young person’s behaviour and wellbeing and had contacted DS for this reason, aware of the different kind of support that the organisation specifically provided. The case file review also contained examples of family members – young people, siblings and parents – self-referring for support.
Echoing this growing awareness of certain concepts and use of specific terminology, some practitioners working in the newly funded services – many of which were specifically labelled an “adolescent family violence program” – noted that there appeared to be benefits in being identified in this way as far as collaboration and referrals were concerned. This was because other services were relieved that a practitioner or agency possessed clear specialisation around an issue that they may be finding too difficult or complex to manage within their own practice remit.
The difference here is that we’re an “adolescent family violence” service … If a referral comes to me, now there’s an expectation that you are there for this kind of role, where I think when you haven’t got that title … you almost have to carve it out for yourself. (Practitioner 10)
That said, practitioners had still encountered resistance to this description in different settings, or an overreach in terms of what was expected in others, resulting in inappropriate referrals as described in Part 2. This meant that they needed to adapt their descriptions and work continuously with referring agencies to break down stigma or manage expectations.
We had to work a little bit with our language because the language that we were using is quite strong around family violence and what that looks like. And you know, the term “abusive or controlling behaviour”. And so we had a lot of pushback from the partnership schools and the parents and guardians of the young people, because it was, I guess, quite heavy language and quite strong. So we needed to work more in that prevention, early intervention space and soften that language a little bit for those who had not been exposed to the service system before … On the other side of that, we’ve had … referrals for a whole-of-family case management approach that, for me, sat well outside the scope of what [our] program was all about. (Practitioner 62)
Overall practitioners reflected that they needed to be flexible and give careful consideration to how they referred to their service offering, depending on the context in which they were operating. This included practitioners who conducted youth-focused work (not specifically designed to address AVITH but often incorporating it) identifying broad variation in the way that they described their roles when engaging with family members, schools or a young person’s peers.
I work with families where if I pick [the young person] up from school, they say “Well what are you gonna tell the school? What are you going to tell my friends?” And I say, “Well, that’s up to [you], it’s whatever [you] tell [your] friends, school, whatever, that’s who I am.” I have one kid who says that “she’s my auntie”. I have another kid who says “she’s a family friend of mine”. And I just go with it. I just literally smile. For me, it’s not my role to tell other people why I’m involved … Keep in mind I have young people that are like “she’s my worker” … I have to tell these kids, you gotta tell me this before I come into the home … (Practitioner 55)
While the above reflection is from a practitioner seeking to reduce stigma for the young person and to engage families in the young person’s wider support, the research found that flexibility and consideration of the context are especially important where the presence of current adult perpetration or continuing coercive control may be a factor. This was because use of terminology associated with DFV in any program title can also present a significant barrier to consent being granted by a perpetrator parent (where consent is relevant because a young person is aged under 16), as noted above in Part 2.
Shared conceptualisation and evolving service recognition
Across the research, practitioners described growing awareness of and evolution in the conceptualisation of AVITH that was translating into increased referrals in some settings, while also signalling a need for more support in how to make referrals in others.
It [AVITH] should be identified at intake. Most referrers are usually pretty good at identifying that. I’d say that schools are probably the one that, you know, we get very limited information on the referral form from schools. They’re probably not as used to filling out detailed referral forms as community services agencies are for the rest of our referrals. (Practitioner 22)
Many of the referrals were described as eventuating from existing networks, such as Integrated Family Violence Networks; from relationships that were being developed through promotion and outreach; or from “piggybacking” on existing programs. The research team heard that referrals were increasing from Victoria Police, Child Protection, schools, Parentline, GPs and other primary health settings, as well as through a significant number of self-referrals – including from families from other parts of Australia who had turned to the internet in search of support that was specific to their experiences (Practitioner 2).
As indicated above, practitioners noted that referrals needed to capture relevant information – something that was not only achieved by an awareness on the part of the referrers, but by the referral form’s design: “We need to adapt our referral form, to reflect that families are coming through because … [the form is] very much focused on adult perpetrators of violence” (Practitioner 22).
Having specific programs known and identifiable through the intake process was also described as key so that the “relay” process described in Part 2 of this report could be avoided, or at least minimised. This included where families self-referred for broader parenting or family support and where the centralised intake point could identify that intervention in relation to the young person’s use of harm was warranted and could gather relevant information at intake as a result.
Developing program responses also included identifying the approach that was most appropriate for particular young people and their families, including in the context of diverse communities. This included practitioners drawing on wider resources and programs within their organisation.
So, whether we’re working with a family from a particular cultural background or we’re working with, like a queer family, or we’re working with a young person in care … the families that we’re working with around the young person are very diverse and we’re lucky to have those resources and that knowledge here. (Practitioner 31)
Our organisation] has quite a lot of men’s programs … So I reached out to a few of the workers there and had a few yarns with them about some of the work that they do and I guess sort of took that and looked at how could I implement that into the program we were doing and it was sort of like “We can’t just mirror that because we can’t talk to those young people the same way that, you know, these workers might talk to the men there” … We’re planting the seeds for change … Trauma pathways … are really difficult to heal and to you know, move forward over. And that can’t necessarily always be done in 40 hours or 110 hours that might be allocated to work with the young person. (Practitioner 73)
Crucially, practitioners working across different specialised contexts explained that their approach was led to an extent by the young person themselves.
… you know, asking “What do you do when you get angry … what do you do when you get sad?” Their reaction to that question will then inform what happens next, so I’ve had young people who have just said, “I don’t like emotions, we’re not going there” and I’ve gone “Okay, let’s come back to that and we’ll move over to who is safe in your life.” And there are other people who are happy to talk to that stuff. And we unpack that. But yeah, it’s really dependent on the young person. (Practitioner 33)
Working with multiple family members
While being led by the needs and responses of the young person was central to their work, practitioners also described the importance of identifying opportunities to work with multiple family members, albeit in different ways.
Sometimes it’s safe to do it as a whole family, other times we do need to do sort of separate pieces of work in there. Depending on the level of risk … but we’re definitely not just looking at what’s going on for the primary young person that’s referred but actually looking at what’s going on in the whole family system. (Practitioner 44)
I sort of make one or two goals for the adolescent, but then a lot of the times because, you know, we’re working with young people that are like 12 or 13 – it’s hard for them to make that change by themselves – so you have to include the family. (Practitioner 17)
Practitioners described working across organisations or across programs within their own organisation to provide support to different family members, including siblings.
The referral came from another organisation and the other worker was working with the sibling and we’ve been able to really build that relationship … and get all these other services back involved. (Practitioner 5)
If we received siblings and one was listed as the victim [and] survivor and one … as using violence, we would coordinate within our own team about how we’re responding. (Practitioner 29)
The beauty of this program is that we are able to … highlight the other children in the family who may be being missed … like really checking in with them as well, because often we know that they are overlooked. (Practitioner 26)
This was particularly evident on the case files, with siblings regularly supported in addition to the young person or other family members or even as a pathway to engagement with other family members.
Promising practice:
Supporting siblings
- In file DS126, an 11-year-old female was engaged with DS as a sibling of a young person using AVITH. The relationship between the mother and children involved frequent conflict ever since the father used violence in the home and left four years ago. The mother was often absent from sessions, as she was unwell and in bed, and the young person would attend the sessions on her own. DS worked with the young person to provide mental health support, including counselling and strategies to manage her anxiety. The young person now stays in her room, locks the door and uses breathing techniques to manage her anxiety when conflict arises in the home.
Promising practice:
Siblings as the doorway to support for the whole family
- A sibling of a young person using AVITH was referred to DS after reaching out to a youth mental health/family violence service for help regarding his brother’s use of AVITH against him and their mother (DS532). Through the brother’s engagement, DS contacted the young person’s mother and began working with her across 29 sessions (DS236). During this engagement, the mother reported a history of DFV from her ex-husband and disclosed having to lock her bedroom door to keep safe from her son who was using violence that mimicked his father’s behaviour.
- While the young person using violence declined engagement with the program, DS were able to support the mother and sibling, including through collaboration with the youth mental health service engaged with the family. DS also provided information and strategies to support the relationship between the mother and sibling, as well as how to manage conflict in the sibling relationship
As well as bringing other members of the family into the work, parents, siblings or grandparents could be the focus where the young person themselves would not engage.
Work in the AVITH space doesn’t necessarily mean that the work has to be with the young person in terms of changing that system and, you know, particularly if a young person is refusing to engage in therapy or in a case management program, what are other ways we can support the system to reduce the stress in the family home and seek change? (Practitioner 44)
If the young person is not wanting to connect but actually we can do some work with the parent, we can target our clinical work on what’s going on for Mum. It might be that we’re looking at younger siblings, how can we support the younger siblings instead? Because if that stress is reduced in terms of that trauma history in relation to healing from family violence, then maybe [Mum’s] got more space to think … (Participant 27)
Some programs that could draw on a well-established funding pool or wider resources had a specific focus on supporting parents through providing opportunities to share their experiences and developing new skills and resources. This in large part draws on the Step-Up model of intervention, while noting considerable variation in the way that it is applied across different programs.
When I first started here … there was a really strong focus on the young person being the client. And over the last 12 months, I think we’re now – not so much at the clinician’s point of workload – but more so from a consult and allocations component, we’re seeing probably 50/50 split of referrals coming through that are for young people or for parents. So initially we were getting a few cases coming through where the young people weren’t giving consent and we were just sort of doing a little bit of work with parents and carers to the point now where I do think it’s about a 50/50 split where we’ve formalised it and said, “If we don’t get consent from the young person, we have a six- to eight-week window where we will work with the parents or the carers or the family.” (Practitioner 19)
Practitioners also explained that it could be a key part of their role to identify not only how family members were experiencing their young person’s behaviour but the response of the service system.
I’ve got an example of a young person working with [mental health service] and the family feeling very much left out, discounted, unacknowledged and also that their experience of violence was being minimised … so the young person is saying “This is just my anxiety”, but really sort of minimising that, actually, this is really hurtful, harmful behaviour that is causing a lot of distress. So, in those instances we’ve found it really worthwhile to try and bridge that gap between family and the [other] service supporting that young person. (Practitioner 35)
Although practitioners across the research emphasised the value of providing parents with support and ensuring that their feelings of stigma and isolation were addressed, practitioners also emphasised that it was not just a matter of focusing primarily on the young person’s behaviour.
At times we might spend a lot more time with the parent or the carer, chatting with them about their needs and kind of working through things with them … Because if the mum or the carer is not having their needs met, then they’re not going to be able to implement the strategies of things that we’re talking about for the young person either. (Practitioner 73)
We do often find that a parent’s phoning in distress, typically they’re asking somebody to see their kids straight away to kind of tell them to pull their head in. And so we work really hard around actually naming the importance that we need to slow things down, that actually it starts with talking to the parents first, getting a sense of who’s in the family and we will be asking about … like for example, their attempts to try to engage the young person in services and what’s happened and typically they’ll say … that’s been a failure or it’s escalated violence in their attempts to try to force the young person to engage in support. (Practitioner 2)
Equally crucial to delivering appropriate responses was developing an understanding of parents’ own experiences of trauma and other adverse experiences in their own childhood.
A lot of the time, it’s the parents that are pushing the buttons or don’t know when to let the young person cool their jets and have another go a bit later on so it’s a good thing to sort of teach the parents as well and a lot of the time the parents … pick up some strategies to regulate their emotions as well. (Practitioner 45)
In that session a lot of that parent’s behaviours were talked about … just because of the nature of me coming in with an argument happening. And that’s when we really noticed the youngest sibling’s role in it and how they were reacting. And so I saw a need for support to be offered to the younger sibling and the young person agreed that I should bring that up in a case discussion as well, which was fantastic. (Practitioner 33)
One other thing I’m realising is … the parents have grown up in family violence or, you know, they never had their needs met … so they just don’t have the skills … so [the young person] is getting bullied and presenting with these behaviours, but Mum doesn’t know anything other than, you know, “I’ll give you something to cry about” … (Practitioner 17)
This latter reflection was echoed by one of the parents interviewed for the research. She explained that DS had provided her with crucial support around learning how to parent in a way that was more constructive than her own experience of childhood, which was marked by emotional neglect and experiences of sexual abuse, before further trauma through severe adult-perpetrated DFV in adulthood.
I perpetuated how my father raised me and my sister, which was authoritarian and disciplinarian … [program] helped me out with my emotional regulation and things and not letting it get that far that it affects the children. (Parent 3)
Practitioners described the extensive impacts of adult-perpetrated DFV on mothers who needed substantial support to recover – and, sometimes, simply to be heard by the systems.
A large cohort of the mums, for example, are single parenting and they’re dealing with the ongoing impact of co-parenting with, typically, a father who remains abusive and controlling and coercive and gaslighting and undermining Mum’s authority in many ways. So, a big part of what you have to hold in mind is that the mum is often doubly victimised so they’re experiencing ongoing abuse from an ex-partner, as well as the abuse that’s happening from the young person. So, they’re blamed in all directions … How can you address the trauma in a parent unless you actually see them as a person? (Practitioner 2)
Parents certainly emphasised the support that they had received from DS as very helpful in managing their own experiences, despite the barriers to service engagement with their children posed by COVID-19 in two cases and the withholding of consent by a controlling father in another.
Looking [at it] from another perspective often gave me a different way of handling it – because you get so caught up with your scenario that you forget to step back and breathe … When you’ve had someone screaming verbal or physical abuse at you, it’s definitely very hard to kind of step back and see them in a slightly detached light … because you’re triggered the whole time. (Parent 1)
Even though [DS practitioner] couldn’t work directly with the kids, it really helped for me because, you know, in lockdown, it’s sort of very isolating … So it was still good for me to have that support and it definitely gave me …. not just someone to talk to about it, but you know, support with handling some things. (Parent 2)
… I didn’t know that they had a family violence unit themselves that they could coach me on, I suppose the remnants of family violence from previous partners or years etc. so it doesn’t build up on the children … you know, it could be like an ex-partner of, you know, 10 years ago, but then you still got some PTSD … [practitioner said] write in the journal and reflect on some things … reflect on what this is supposed to mean or what a safe environment would look like for me and the children or what … being happy and comfortable would look like … It was quite cathartic … because it did help me get some goals … like to get a proper job where I could function with my children as a family unit … And that it wasn’t a bad thing that … if I’m going to work …
[DS practitioner] was wonderful. She really helped us connect to be better and, you know … provided me information and coaching … which have been really helpful to get [my] children in touch with their emotions. And letting me know their needs and behaviours they’re exhibiting because of said needs and can’t voice. (Parent 3)
The benefits of support focused on the mother to build protective factors and safety were particularly apparent across the case files.
Promising practice:
Strengthening parenting, supporting mothers
- In file DS789, DS had 35 sessions with the family, principally involving one-on-one counselling/parenting support and case management with the mother. During the engagement with DS, the mother obtained a secure job and housing, and regained access to her children on a regular basis. DS assisted the mother to redirect bills to the father, to receive a utility relief grant and to have a large amount of debt cancelled, and supported her to report any acts by the father that breached the protection order that was in place.
- In file DS954, care team meetings were held with the mother to coordinate supports for the family and to discuss goals. The mother received counselling, parenting support and help to develop assertive communication skills. She also received help with coordination of current protection orders, safety planning and support as the young person moved out of the family home. With the help of DS, the mother “is working on her own mental health and increasing her connections with others outside of the household” and how to enact her safety plan when needed.
- Case file DS043 described support for the mother around regulating her own emotions so that she could “help the young person regulate himself”. A family action plan was also created to improve relationships. The young person started seeing an occupational therapist and psychologist regularly to strengthen his emotional response and has a paediatrician to monitor medication, as well as receiving NDIS support.
Some of the DS work involved raising awareness and supporting mothers to understand the nature of what they were experiencing from their young person, or the likely impacts of past experiences on their children which could enable them to support their children and manage their behaviours in ways which more effectively de-escalated and reduced risk.
Promising practice:
Seeing the young person’s behaviour through a new lens
- In file DS250, DS worked with a mother on parenting strategies, resulting in greater insight into the impact of trauma (DFV from ex-partner) on current family functioning and relationships. During the engagement, the mother adopted a harm minimisation approach to the young person’s risky behaviour, which led to a reduction of conflict in the home and the young person engaging more in school and engaging with DS. Based on risk assessment notes, the young person “has a safe home to go to, she knows this and will go home”. With the assistance of DS, the family concluded that mental health support was the best approach to ceasing the young person’s conflict in the home. It was also reported in the case notes that, following another young person’s court matter regarding an assault in which the young person was involved, her mother had a “new awareness and reading of family violence and its impact”. Notes show that the mother wasdistressed to learn how much it had impacted her and her children and was taking the practitioner’s advice and had a better understanding of the trauma that the young person had been experiencing.
Promising practice:
Understanding family violence
- In file DS932, DS was able to fill a gap relating to the impact of DFV and a death in the family, providing family counselling/therapy around family relationships, as well as individual counselling for the young person and siblings around grief and loss. Targeted individual counselling was provided specifically for the young person around emotional regulation and navigating peer relationships.
Promising practice:
Providing connection
- The positive impact of DS on a parent is reflected in case notes on file DS098, which describe a parent thanking a practitioner for helping her and understanding her feelings after a settlement experience through which this parent felt that she had lost everything.
In some cases, DS supported the victim and survivor mother to do more than understand the nature of her current or past experiences – assisting her to leave a violent adult partner and to ensure that Child Protection were aware of relevant risks.
Promising practice:
Supporting the mother to leave a violent relationship
- During engagement with DS, one family (DS180) experienced positive changes across several elements of the family’s life. The mother received counselling support to gain employment and improve her parenting skills and mental health. She also received support to recognise DFV behaviours coming from her partner and the way that these behaviours impact the children at home. The mother was supported to leave the violent relationship and seek a protection order, resulting in reports of improved wellbeing and family relationships. As a result of the support provided by DS, the young person’s mother reported a decrease in anxiety and depression and greater confidence in parenting, with an associated decrease in problematic behaviour from the children. The DS practitioner kept Child Protection and the children’s school abreast of the new protection order.
Promising practice:
Supporting safety planning
- In file DS054, a safety plan was put in place with police and the mother was supported to speak to police about what needs to happen if they are called. The mother and DS worked together to book in short-term accommodation respite and the mother described beginning to connect with the family violence team at the police station to create a point of contact in making reports where needed.
As noted in Part 2, the ongoing impacts of adult-perpetrated DFV were an overarching theme in the interviews with parents. The impacts of this violence were influencing every aspect of the mothers’ and children’s lives. In all three cases, the mothers’ focus was on obtaining support for their young person and siblings, all of whom had been impacted by their shared trauma in different ways. It was clear in each case that assisting the young person would therefore be a way of assisting the mother, despite her own experiences of harmful behaviour from the young person.
Reflecting this, some practitioners working in court or legal contexts explained that the support they were providing to the young person was also a way of supporting the protective parent, despite the fact that they were likely to be experiencing the violence as well.
Oftentimes the young person is the respondent [to a protection order], but it’s actually Mum … who I work with … because both have the same goals and … they want the young person to get help … obviously it’s [Mum] who drives the young person to the appointments and all that kind of stuff anyway when the young person’s in school and young people don’t answer their phones … so I think it’s usually works [sic] with going through the parent. Obviously, you make judgement calls around what’s safe … (Practitioner 61)
… seeing young people feeding back information from their lawyer back to their worried mum … I think sometimes there is a bit of relief … that the young person has either a lawyer or at least a service that’s checking in regularly … even though sometimes that’s unsafe and inappropriate, but other times … even if you’re not working with [the protective parent], you still kind of are working with [the protective parent] because at the end of the day these young people, they are dependent on someone for care as well … (Practitioner 51)
By contrast to circumstances in which a single practitioner was working with the young person while keeping other family members in view as above, some programs – including the DS program – were purposefully drawing on multiple practitioners across the agency.
It starts right from when we get the referrals … When we’re doing the allocations, if it’s for one of the parents, first to start to see what their support might look like … and we read in the allocations note around who could potentially be the practice lead based on the support needs of the family and who the practitioners … will be as well. So, we start that discussion right from the beginning and … then we set up regular … “case discussions” with the practice lead and the practitioners working with the family. (Practitioner 31)
Practitioners explained that this approach included identifying which practitioner was most appropriate to contact each family member, or where consent from parents was required. Conversely, information sharing was vital where it may be useful to bring in another family member but where a young person was the presenting client. In these cases, this contact with the other family members was discussed with the young person and not initiated unless endorsed by them.
Practitioners, including those from DS, described how they might start to engage with a young person while keeping the whole family in view.
I find a family tree, just making that kind of genogram, that is the best place to start … they often really easily engage with the family tree and unpacking the different family members and usually pets is a really, really positive place to start and will tell a lot about them and what they deem as important and their connection, which is often overlooked by other family members or on the referral … What it has also done is it has allowed a breadth for actual safety planning, because … how it’s constructed is different … So how are we safety planning? How are we talking about that? What does that risk mean? For whom? When does it change? At what times, and what are we noticing? (Practitioner 33)
Work by DS with young people evident in the case files on occasion had an emphasis on early intervention. The research team heard that this was possible given that a significant number of referrals were coming from schools or through self-referrals in which young people or families identified the DS suite of programs as a possible source of support. In certain cases, being able to engage the young person was a particular achievement for the reasons that the research has explored around young people’s distrust of services and the impact of prior negative service engagement.
Promising practice:
Strengths-based approaches and exploring positive experiences
- In one case file (DS432), the young person spoke about a range of hobbies and activities, as well as casual employment, which were used as part of safety planning and building rapport with the young person. Safety planning included the young person retreating to his room to play video games, as his family respects that boundary and leaves him alone; going for a walk; or talking to a friend. After only three sessions with the DS practitioner, the young person reported no longer feeling fear to return home or fear that the yelling would turn into physical violence. The young person reported being able to leave the situation and return to his bedroom when the yelling erupts within the family unit, which is a strategy discussed with DS to diffuse the arguments.
Consistent with broader practice experience and evidence, practitioners working in Aboriginal community-led organisations placed particular emphasis on ensuring that the whole family was supported, even where a young person’s behaviour and the factors contributing to it were the service entry point. This focus was situated within a broader emphasis on connection to community and whole-of-family responses because, as one participant explained, community-led programs were “not prepared to shut anybody off” (Practitioner 72).
We do our [risk assessment and management] assessments keeping in mind what is impacting on our community members, physically, mentally, emotionally and spiritually. A lot of the time it’s disconnection from their community, so that’s part of the spiritual realm and our role is to get them back connected into the community … Why I push for these groups to happen is to get them connected with other young people … So, [other practitioners are] working with the family while [youth-focused practitioner] focuses on the young person. And so we can provide case management support, whether that’s through our family services stream, out-of-home care stream, kinship stream, family violence support, NDIS support, playgroup supports, we’ve got all of those services here at our fingertips that we can refer into those different areas and strengthen that family. (Practitioner 74)
Practitioners from the program above explained that a young person’s progress needed “to be supported at home as well, not just in the couple of hours that we see them” (Practitioner 73). One noted that a careful balance was required to ensure that unconstructive messages were not being delivered.
One thing that kind of sat a little bit uneasy with me was if … the young person that’s been using violence at home is being taken out to … do all these fun things together that it doesn’t necessarily send like a good message to the other young people. So, I kind of would start to also take some of the siblings out as well – not each time, because we want to have those conversations with the client that we are working with but, you know, if we’re going to a movie every now and then or do something fun … I’ll bring those other siblings along as well. And so, it’s … not setting that sort of strange dynamic of the person being rewarded and it’s really nice, I think, that some of the families that have not had that experience before of, like, going to a movie and doing those kinds of things and it kind of brings the siblings closer together as well. (Practitioner 73)
… I know it’s a word that’s thrown around all the time. But it’s “community”, we aren’t just working with one person in the family, you have to include all of them. If you’re going to take one of your kids to the movies, same with my kids, you don’t just take one of the kids you take all of the kids. And you’ve got to keep that balance in the home as well. (Practitioner 74)
Capacity for flexible, client-centred approaches
To a significant extent, funding and design parameters dictated the types of activities which were able to be conducted through AVITH-focused interventions, with capacity for flexible and client-centred approaches emphasised as being particularly crucial. The research also indicated a critical interrogation of service interventions as the more well-established programs were learning about what was effective.
I think [well-established program] just keeps evolving and I mean, as practitioners, we have the scope to respond to our clients and meet them where they’re at, so nothing’s really off the table. So when I have worked with an 11-year-old, you know, like high functioning autism … the program is supportive of that … [That child] had, you know been in so many services and he was in the care of his grandma and they were at … breaking point. (Practitioner 5)
We try to very much meet the young people and their families sort of where they’re at, we have a very significant focus on improving safety and really understanding, kind of where the adolescent sits within their sort of own internal family systems, but also within this sort of wider community. (Practitioner 16)
For instance some of the ones at school, they might be using gender shaming, sort of behaviour to other students, and they would be, you know, using a racial slurs [sic] and things like that. So they’re sort of indicators to us that, you know, it’s possibly a learned behaviour and then we sort of ask a few more questions and establish if this is ongoing or whether they might just be having a bad day to help direct our support a little bit more. Then it can be, you know, to the other sort of spectrum of they might have had a suicide attempt, which we tend to get a lot more of those in the community referrals. (Practitioner 62)
This included, as noted in Part 2, varying approaches to the use of group work, with one program moving away from it, one focusing on parents, and one running concurrent groups, as described below.
We’ll start it off … with both the young person and parents to get a clear understanding of the goals. And then normally what I will do is separate it just because of their adolescent age and stage of development, they take a little bit longer to pick up on some topics compared to the parents … Say, for example, I might meet with the parent and young person every week separately and then that parent work might drop off for a time, so the young person can pick up on a particular concept … it might take a little bit longer for the young person to pick up on their warning signs and their triggers and a timeout plan is not really super effective unless they can really start to identify their warning signs. (Practitioner 19)
Practitioners across other programs offering group work to young people (resourced through different funding streams) also described the need to consider the composition of any group and its potential dynamic across age, as well as types of behaviours exhibited and risk indicated.
If you have a whole bunch of 13-year-olds who are [engaged in] gender shaming and verbal abuse of their siblings and family at home, they … sit within that family violence range but, on the continuum … they’re at one end. And then you have a young person who’s exhibiting significant physical violence within the home. We would consider putting that person in a group that’s a little bit older with more high-risk behaviours … (Practitioner 64)
Practitioners explained that interventions needed to be sufficiently resourced to work in a flexible, client-centred way, highlighting that working with a culturally diverse range of young people could sometimes mean that young males may not want to engage with female workers (Practitioner 57). The research team also heard that some young people would respond more effectively to a practitioner from a certain age group than to others (Practitioner 18). Practitioners similarly explained that a considerable amount of sector and workforce development was required around working with young people from CALD communities, with referrals often directed in a siloed way towards dedicated services because mainstream services were not able to respond appropriately (Practitioner 10).
To note, practitioners from different ACCOs had varying views about group work involving young people. A participant from one organisation explained that it was important to understand how a young person was going to respond to being around peers, reflecting below on the needs of a particular client.
Our men’s group, there’s all sort of walks of life there. And we’ve got Elders there, we’ve got people that are in their 30s … So we do art pottery, woodcarving … they go on trips together to see various things … We’ve specifically done it that way because our Elders need somewhere to go and they’ve got some wisdom. They’ve perhaps been there and done that … and they’ve changed and got through life and come out the other end and become a respected Elder … and it’s teaching this young fella to be respectful … We’re not all pointing the finger and telling you off, these are people that care and want to look after you.
Yeah, I think if it was a group of young people, young boys, different story, you’d just be asking for issues then. But because I’ve got such a mix of ages, it doesn’t come to that ever. I think what we’ve gotta do is teach these young people how to speak to people properly and how to respect their Elders, but also how to respect their parents and their mums … There’s a place for a young group, but … where this kid is at the moment, an older group is better for him because he’s wanting to learn respect. (Practitioner 72)
Practitioners from another ACCO, however, saw particular value in their groups for the young people with whom they were working.
The group is really great because the young people get to connect with each other in terms [of] where they are on their journey, not just on their journey of, like, who they are as an Aboriginal person but, you know, as teenagers. So, who they are trying to become or who do they want to become? They’re trying all those things out to kind of see what they want to do, what works for them and all of that … For some of the young people that we work with, it’s the first time that they kind of really identify as being Aboriginal …
And I think having that kind of space like at the youth group and at the men’s cultural camp that we went to, having those yarning circles and introducing the idea where [you] can go around and talk about who you are, who your mob is or where you come from – all those kinds of things are a great way to kind of introduce the idea of that. (Practitioner 73)
It’s important to recognise that their peers are a huge part of their life … because it gives them more confidence to be able to be who they are … And that’s what we’re striving for, aren’t we? You know, we are wanting these young adolescents to grow up knowing who they are, to be strong and who they are and be able to be out in the community and society. That’s … hopefully our goal. (Practitioner 75)
Sequencing and readiness
Across the research, practitioners highlighted the need for interventions to be guided by what clients identified as their own needs and preferences, rather than what a service might assess. A feature of this involved assessing the extent to which clients were ready for particular interventions or had the capacity to engage, staggering or sequencing support depending on what else was happening in their lives.
Generally, we’ll have an initial meeting to work out, “Well, who’s doing what?” So then everyone’s pretty clear … working out who does what and whether we stagger things … so that we can maintain a good engagement and the families aren’t feeling overwhelmed either with different service responses and different information all at the same time. (Practitioner 1)
One of the exciting components that we have in our program is working in partnership with case management and a clinical role, so there’s kind of that capacity for young people if they’re not kind of therapy ready, you know [for] the case managers to kind of walk alongside them and develop that therapeutic relationship that can potentially … then articulate into the … integration of a more clinical intervention later on. (Practitioner 26)
Importantly, an example offered by an Aboriginal community-led service involved significant thought put into supporting a young person who had an extensive history of trauma, including child removal. The service described consideration about sequencing over the long term, prioritising secure housing, and work to obtain identification documents, given that these did not exist, which could allow him to access Centrelink benefits.
During this time the young person was also linked with cultural programs and was volunteering to help with the service’s NAIDOC event. He was also linked with assessments for relevant language and developmental delays. Eventually the plan with the young person was to work towards securing employment,
’cause if we don’t capture him before 18, 19, and it keeps going down the path of stupid petty rubbish, he’s gonna be in big boys’ jail and then we’ve lost him. (Practitioner 72)
Case files similarly indicated that effective intervention required considerations around sequencing. The following promising practice example illustrates some of the complexity involved in considering how and when work should occur – and with which service.
Promising practice:
Flexible and client-centred approaches – sequencing
- In file DS054, care team meetings took place for the family on a monthly basis for one year and, through these, long-term work was done between the Children’s Court worker, behavioural specialist, [children’s hospital] worker, social worker, DS and the mother. The case file shows collaborative work and collective decision-making through care team meetings with a diverse range of supports offered. In particular, detailed conversations occurred between the young person and the Children’s Court worker around the diversion process and the importance of taking responsibility, as well as ensuring that the young person understood their legal matters and obligations.
Collaboration occurred between care team meeting practitioners (occupational therapist, Children’s Court worker) to teach the young person about family violence, while the mother was supported around safety planning and how to make reports of breaches of the order.
Plans were also made for DS to work on an NDIS application with an NDIS coordinator to coordinate respite and safety planning with police, and to arrange a referral for a specialist with expertise relevant to the young person’s complex needs.
Outreach and activities
The research team heard that being led by a client’s preferences included recognising that working with young people requires adaptability. Practitioners explained that the value of many of their programs was that they were voluntary, so that young people who had a history of negative service engagement – such as the young people described by parents interviewed for the research – would not feel that they were compelled to engage but could gradually form a “therapeutic alliance” (Practitioner 55) with a worker. They also emphasised that outreach and flexible working practices were an increasingly well-utilised part of their approach.
The day-to-day would be, either clients coming into the office, but some clients don’t really like doing that, so a lot of it is outreach. (Practitioner 13)
If you’re not doing outreach, you’re not seeing their family home or their family situation as a whole, you’re only seeing what the [referral] provides you with, I think we pick up on a lot more of what’s impacting on the clients. (Practitioner 20)
Participants described their insistence on maintaining the capacity for outreach during COVID-19 lockdowns, finding flexible ways to “maintain eyes” on young people and families and get a sense of what was occurring in their lives, even if practitioners could not attend a young person’s home and get the fuller picture about risk and support needs which could not be obtained over the phone.
I did an outreach walk today for 15 minutes, during COVID, just to keep them engaged, ’cause if we do not keep sort of speaking with them and meeting them, they do fall off quickly. (Practitioner 14)
This was particularly the case for ACCOs
Our expectation was that our workers still got out there to … make sure the families were okay. (Practitioner 74)
We do home visits a lot, the petrol bill tells me that we do a lot in the cars! (Practitioner 72)
The research indicated, however, that capacity to conduct outreach varied across services and systems, with many programs relying on other services where they did not have outreach counted in their caseloads or where they could not access vehicles to facilitate the outreach.
Services love to lean back on [our program] because we’ve got cars, and we go and see young people, and we do all this wonderful organic work with them so they go, “Will you do it?” And you have to be really kind of boundaried in saying, “We don’t have that capacity.” (Practitioner 52)
Practitioners also discussed the potential benefits of outreach approaches being adopted in contexts beyond community-based programs.
Outreach is the most critical component working with young people … I think that courts need to start stepping up and having some component of outreach capacity …You know, there’s something about needing to be able to go to where people are at … to conduct these assessments around what’s really going on … Every case is an iceberg … but half the information that’s reflected to us about what’s going on for the young person, if you’re just getting it over the phone, I mean it ends up being the least important information you could get, than what you get in the home. (Practitioner 35)
Case files similarly indicate that outreach was considered vital where possible, so that practitioners could increase their understanding of risk present across the family structure and develop rapport.
Promising practice:
Flexible and client-centred approaches – outreach
- In case DS169, DS and a mother spent considerable time and effort unpacking different ways to offer the young person support, including via outreach sessions, providing flexibility for the young person to elect the day and time that would suit him best, and giving the young person full autonomy to decide how he would like to “meet and greet” the DS practitioner.
Promising practice:
Flexible and client-led approaches – working with schools
- In file DS233, where a young person had been refusing to engage with school online, DS supported the mother to approach the school and facilitated a flexible arrangement where the young person could attend school during the COVID-19 lockdowns. Supports were coordinated for the family through meetings with the school, an occupational therapist and NDIS workers to arrange allocations of support that was better suited to the family’s specific needs.
Just as important as outreach was an approach that responded to a young person’s interests or involved shared activities. This could include, as one practitioner described, connecting young people with older mentors who shared an interest, such as skateboarding, and generally “thinking about what a kid actually wants to do and therefore how they will engage” (Practitioner 67).
Practitioners across the research similarly noted that young people were more likely to engage during shared activities or be particularly likely to engage in conversations while driving together, rather than sitting face-to-face with a worker. As noted in Part 2, practitioners explained that young people were usually disinterested in what services described as “talk therapy” (Practitioner 52). This was especially the case where previous negative experiences with wellbeing coordinators at schools or psychologists – such as those of the young people described by parents interviewed for the research – had not made a difference and had potentially contributed to a young person’s mistrust of services instead. “A lot of young people don’t want counsellors. They don’t want to see a therapist, so we talk about support workers, so just use different language” (Practitioner 61).
These observations from practitioners were also echoed very strongly by one parent, who emphasised the importance of practical, physical support and outreach-based activities.
I wish organisations would see that, for kids, especially when there’s a lot of trauma … playing into it, sometimes they need someone not to speak to, like a counsellor, but, “Hey let’s play [a] game of footy”, or “Let’s go for an ice cream”, or “Here, let’s bake a cake together” or something like that so that they can build that friendship, that rapport, just connecting with them … [and] can feel comfortable enough to talk. (Parent 1)
Practitioners also highlighted that the hours that they worked needed to be examined when developing more appropriate and “user friendly” responses for young people.
Working with young people … you don’t put meetings on of a morning with young people because they’re not out of bed yet. So thinking about, you know, when is the best time to work with young people? Is it 9 to 5? Is it 12 to 8? I don’t know but thinking about the end result being about how the user accesses us, rather than how we access a client. (Practitioner 19)
Length of engagement
Also highlighted as particularly crucial across the research was the capacity to work with young people and families over a longer duration, as referred to earlier in this report.
Practitioners working in the more well-established programs had greater capacity to work with clients over the longer term.
A real asset and value-add to the program is we’re not time limited. So, as with other interventions, there’s you know your 40 hours or 110 hours or whatever they all are, we have three to six months to work with the client and we can go either side of that and we do go other side of that, so I think that’s a real strength … at the end of interventions with young people who had spent a significant amount of time, like, you know six to nine months within the program and the biggest reflection that [one young person] had was, “I was able to build a relationship with you” and “You were able to understand what was going on” and “I had the time and it wasn’t that I had to then go on to another service” … And there was significant behaviour change within that family, so I think that that is a really, really big strength of the program. (Practitioner 20)
Another long-running program insisted on the capacity to work with clients over one to two years where necessary, but noted that meaningful benefits could usually be realised within a shorter period of time.
… actually 75 per cent of the families we work with have significant change in less than 12 months of intervention. And when it comes to those that need the longer term support – and we’re talking years, kind of stuff – that’s not a huge proportion, it might be 25 per cent of our client group. (Practitioner 2)
A practitioner from one participating ACCO also emphasised the importance of giving families and individuals time to engage and, perhaps most importantly, re-engage.
We don’t have time limits on people … It can be hard for the workers because they do a lot of work with them at one time and then it’s all wasted and then, you know, they come back six months later … Eventually, though, somebody wants to change and then that’s when you grab a hold and don’t let go really … It’s about when that person’s ready to make the changes they need to make, we’ve gotta have the door open for that time. (Practitioner 72)
Practitioners from DS emphasised the value of their organisation “allowing them to take time with people and move at whatever pace feels right for the person” (Practitioner 33), tailoring the support uniquely to the family and individual. In particular, they noted that working towards engagement of young people requires that the provision of support is not time-limited, so that young people can see that engagement with the DS service does not hang on certain conditions.
Promising practice:
Steps towards building attachments
- Although DS originally engaged with the young person’s mother (DS233) for mental health and parenting support, months after initial engagement, the young person consented to being on a separate case and was engaging with face-to-face sessions. Through these individual sessions, DS and the young person discussed the young person’s self-harm and suicide risk, anger and family connection issues. DS worked with the young person to build a degree of positive engagement with his parents. A parent whose child had not been able to be engaged through the program because of COVID-19 nonetheless noted the potential of longer-term engagement. “There has to be some continuity for kids like, whether it be the same person, that’s always all the same. Maybe two people for safety reasons …” (Parent 1).
Brokerage
A further theme which emerged spontaneously from the research was the value of brokerage which had been made available through the newly funded programs. Practitioners described examples of ways in which they had used brokerage, such as putting funding towards a young person’s braces because their need for them was impacting their self-esteem (Practitioner 22); purchasing equipment which could provide an outlet for a young person’s energy, such as gym equipment or trampolines (Practitioner 27); funding NDIS assessments; or even providing specific supports, such as counselling, for siblings.
One of the nice things about the way that this program has been funded is that we had so much brokerage attached so that each sort of individual response that we’re providing with families we’ve been able to purchase in some really specific interventions … that make a really tailored response and not like one-size-fits-all. (Practitioner 26)
So we’ve used brokerage to support some respite for the young person to actually spend time away from their family to just break that cycle of the … relational intensity and build-up. And it seems to be a really big gap in service provision, being able to access respite, because at the moment we’re using brokerage for that but … that ends up being the young person going and staying at in an Airbnb … yeah, it seems to be a really big gap. (Practitioner 22)
Importantly, practitioners working in Aboriginal community-led contexts were using brokerage in a range of ways. This included to access specialist assessments; providing families with vouchers to assist with shopping or petrol; funding activities such as taking young people out to buy lunch or go to a movie; providing them with sports equipment, such as footballs, where the young people may not have these themselves; and even providing backpacks with clothes and accessories from Clothing the Gap.
Early last year we purchased some really good bikes for a lot of clients. So, you know, that was a really helpful thing, not just for the kids to have fun after school, but it meant that some of the kids are riding their bike to school and then Mum is, you know, has a couple of less kids or maybe no kids to take to school first thing in the morning. And so that’s like a bit of a burden off the family for that … We’ve bought a few kids music equipment and something that, you know, working with them, they’ve identified that that’s a therapeutic thing for them. They can go into their room, they can play keyboard, headphones on or listen to music or they’re writing music. (Practitioner 73)
As well as describing ways in which brokerage could help to alleviate pressure on families or give young people an outlet or respite, practitioners also explained that what they purchased for young people could often be directly related to safety or any needs for immediate assistance.
We’ve bought some phones and computers and things like that so that we can provide those for young people. And I think the phones, particularly, are really important because it’s a safety sort of planning mechanism for young people as well. [For example] with Beyond Blue they have that app where you can kind of put in all of your safety plan … into the app and like headspace do have an app where you can kind of text as well instead of calling the helpline or whatever … And so, I think the phones make up the important component of that. … we pre-purchased a bunch of those so that we’ve got them ready to give to clients … (Practitioner 73)
A practitioner from another Aboriginal community-led program similarly talked about the value of using brokerage to provide whole families or young people with positive experiences and ways that they could see themselves in a positive light, a theme further explored in the section below.
And you know it’s giving them that experience, they go down to Scienceworks and those sorts of things … We were able to get a lot of tickets for the Dreamtime game, so we got a lot of families into that … It’s sort of stuff that some people just think of as normal but, for our families that are in low socioeconomic situations, they can’t afford to do things like that. So it’s just about being a bit proactive … being involved with the community … and not just waiting for a crisis. (Practitioner 72)
Strengths-based approaches and shared positive experiences
Across the research more broadly, practitioners volunteered the importance of helping families – who had often lived for a long time as if they were “walking on eggshells”, as the wider research describes (McKenna & O’Connor, 2012) – to have shared experiences which enabled them to see their family in a different light and therefore signal the possibility for further change. As noted in Part 1, wider studies increasingly suggest that positive relationships offer a significant protective factor against AVITH (Elliott et al., 2017; Kehoe et al., 2020), with findings from the ReNew program emphasising the importance of mothers and sons building attachment and positive memories (Burck, 2021).
Particularly striking across the parent interviews was the extraordinary resilience and strength of all the mothers and children involved, with mothers continually looking for positive experiences and connections for their children, while young people and siblings were often doing the same. That said, two of the three service user interviewees suggested that there was such extensive and varied trauma in the lives of the mothers and their children that relationships remained incredibly fragile, with their collective identity formed around their shared experiences of harm. One mother had recently started working and studying, encouraged by DS, contributing to a shift in the way that she saw herself which was having a positive impact on her relationship with her children.
Certainly, the focus groups suggested that creation of positive experiences and development of positive attachments were particularly important in the context of families’ exposure to adult-perpetrated DFV or wider intergenerational harm: “We’ve funded lots of vouchers and that sort of thing so that families can spend time together sort of forming positive memories” (Practitioner 25).
Creating opportunities for positive experiences was particularly important in terms of supporting young people. The research team heard that this was because young people were forming their identity during adolescence and should not be forming their identity around negative views of themselves.
I’m often really mindful and careful about the way that we present ourselves … during an identity-forming time of a young person’s development … we often get them at the age where they’re really starting to put their heads up and choose from the world who and what they might like to move towards being. (Practitioner 52)
That’s what I do find the hardest is when you’re working with the [17- and 18-year-olds], like some of the ones I do in the one-on-one stuff. They’re like, “I already know I’m the problem, I know I’m shit, I know I’m not going to change and I’m going to grow up and be like Dad” and it’s just like, “Who has told you that?” and it’s like every system, every adult, every teacher that kicked you outta class. Every footy coach that didn’t put you on. And that is hard. (Practitioner 44)
Stigma and shame played different roles for the young people described in service user interviews. One child was using harm in the context of his disability and experienced significant shame after each incident. Another was being manipulated by a separated father to control a younger sibling. A further young person who was using harmful behaviour at home – while experiencing very acute mental health distress – appeared to feel additional shame that he had not “coped” with their family’s experiences like his siblings. Long periods of school disengagement related to a mother’s illness also contributed to low self-esteem.
One of the parents participating in interviews described that the only thing that seemed to make a difference for her child was the informal support and interest from an older sibling.
I really need someone who can physically get in here and help me with that aspect of things. I’m so lost on what and how to do that. And like, [older brother] has gotten in there and he goes right “You’re coming to the gym with me” …. and you can actually hear [adolescent’s] conversation change because someone is physically taking an interest in him … (Parent 1)
Practitioners in the focus groups spoke correspondingly about the importance of avoiding a deficit-based approach and, in some cases, not continuing to focus on what young people were doing “wrong”.
I think young people … notice a difference that we don’t get the big sort of problem saturated story … and just go in and take that deficit approach, like “This is going wrong, you’re not going to school, you’re doing this” … (Practitioner 45)
I guess you know when someone is saying over and over again that they’re not going to school … sometimes you have to go, “Okay, well are we just going to continue to have only that conversation with them … or do we look at other alternatives?” (Practitioner 73)
Clearly, we’re responding to family violence. But … when I speak to young people, I mention that I’m … just wanting to check in, if you’re feeling safe, ask if there’s anything that you need support with but, really, wanting to start with where the young person’s at in terms of what they identify is most … pressing for them … I’m trying to have that opportunity to connect with a young person, you know, affirm their experience and explore “What supports do you need?” And just be able to recognise … it’s hard to know how to contain yourself when you’ve had all of these experiences that have meant that relationships are difficult … I do really understand the limits and constraints of the system … but I still think that’s not an excuse for … not striving for best practice and not striving for upholding the dignity of young people. (Practitioner 29)
Building positive engagement between protective parents and young people – as well as leveraging the strengths and protective factors in a young person’s life – was deemed to be key. In many case files, the DS practitioner discussed protective factors for the young person and asked the young person about their interests, hobbies, employment or any other positive features in their life, particularly those that divert from the situation of violence within the home.
Promising practice:
Building rituals and recognising developmental stages
- In case DS021, DS worked collaboratively with a parenting practitioner who supported the young person’s mother by providing resources and strategies including videos about children’s developmental stages, tip sheets, redirection and distraction for children when conflict occurs, and ways to build rituals into the week. Notes recorded a discussion with the mother about using a communication book or app for all communication between the parents as well as considering Child Protection notifications, where appropriate, in relation to a perpetrator father’s ongoing systems abuse.
Practitioners from Aboriginal community-led programs described connections with culture as a particularly valuable way of strengthening young people’s views of themselves and their place within family and community. These included developing cultural support plans in collaboration with young people where they did not yet have strong connections with culture or community.
We really try and keep kids engaged in our youth program and that’s, you know, it’s once again embedding culture in their lives. Our youth team, both junior and senior, are learning to dance. And yes, so it’s just doing things on that they make damper and they do, you know like it’s active things. So it’s not just sort of sitting there and doing lessons … (Participant 72)
So, for some young people that might be playing music or joining the footy team or connecting further to culture … that might not immediately look like something that is a response to the family violence incident but … we’re looking at people that are still developing their skills and being able to make decisions … We’ve also recently had a cultural boys’ camp … I think the boys came out of that a lot stronger in themselves … learning some cultural knowledge that is pretty hard to find out in the streets of Melbourne … that can give them a stronger sense of identity and to make … decisions that are not just shaped by them as young teenage boys but shaped by thousands of years of history. (Practitioner 73)
What happened with working with the Elders at the camp was that they got to build or create their own didgeridoo and they got to use it … and a week or two later, we had a community event for NAIDOC Day and the person that we had asked to come in to do the didgeridoo couldn’t make it. This is the impact from what happened at the camp – those boys that had just learnt the didgeridoo and they played at this event! So, what I’m trying to say is that the impact of culture, these young people building their self-esteem, their confidence, their identity, as a fundamental part of their wellbeing, as well as their family and community … (Practitioner 74)
Importantly, practitioners from ACCOs also highlighted that cultural identity was “broad and complex”.
We have so many Aboriginal and Torres Strait Islander people coming either interstate or who are coming within different regions of Victoria who live in this area. So, it’s about being sensitive as well because they’re from different mobs … but what [it] provides is like a – I don’t know if I can say it in this way – like a blanket, a comfort blanket because we provide Elders that are here to talk to our … adolescents … which provides that support for Aboriginal identity because, although they’ve coming from different areas, they still get that connectedness and that way of linking themselves back to who they are. (Practitioner 75)
Giving voice to young people and their experiences
As well as the value of working with family members and, as one practitioner above described it, seeing the parent “as a person” (Practitioner 2), the research indicated that a crucial component of effective AVITH-focused interventions is giving voice to young people and how they have experienced their world.
This work is really, really trying to centre young peoples’ experience and really trying to, you know, affirm that young people are primary victims [and] survivors in their own right, and when they’re using violence, that’s telling us something that’s giving us information about what their experience has been [and] their development so, you know, I think it’s such a missed opportunity if we can’t connect with young people early … having a positive experience where they’re not feeling judged and not feeling like they’re the problem … (Practitioner 29)
… knowing your rights in terms of like your legal rights. Also just your human rights in terms of privacy, respect … freedom of mobility … (Practitioner 28)
Some practitioners suggested that this could have benefits in both directions, noting young people’s limitations to have full choice and agency over their own lives.
I do think giving a voice to children, particularly adolescents, is really important, because … if you give adolescents a voice, you can also address accountability. It’s a two-way street. If they have a voice, you can also demand responsibility. (Practitioner 69)
A dedicated legal service working with young people as respondents to protection orders explained that they had a unique opportunity to give voice to young people because they could establish rapport and trust once young people understood that the service was working exclusively for them, as explored in detail in the PIPA project (Campbell et al., 2020; see also Centre for Innovative Justice, 2022).
We do prioritise their own safety and will always ask questions around how safe they feel at home and often that leads to disclosures … Generally, we may be one of the first people they’ve disclosed to … The young person’s often fearful of telling anyone else, particularly fearful of [Child Protection]’s involvement or getting moved into a resi[dential] care or they’re fearful of repercussions from their parents, of anyone finding out … Our conversations have that legal privilege, so they’ve finally found a safe way to tell someone. (Practitioner 49)
Giving voice to young people was not limited to facilitating disclosures of harm or wider traumatic experiences but was also about a practitioner being an advocate for the young person where they were not present or able to tell their story themselves.
There’s been a real focus on diagnosis like mental health diagnoses as “This is the issue, this is why this is happening”, “There’s ADHD” or “There’s this or there’s that” and I’ve noticed a big shift recently … around not just services looking for diagnoses but parents looking for diagnoses too. So them actually not seeing themselves as part of a solution, it’s like “I need to get my kid diagnosed because that will then explain everything” … I had the same experience even this morning discussing a young person in a care team meeting and, yeah, the first response was “We need to get them to a paediatrician and get them assessed for all these things”. And I’m sitting there saying “Well, there’s been about 15 years of trauma here” … (Practitioner 10)
Actively leaving room and time for identification of experiences of harm in the context of assessments was therefore crucial.
We have improved our assessments and sometimes it doesn’t show up until the course of treatment that you see that Mum or Dad are using aggression in terms of their inability to manage their own distress, so it’s typically co-dysregulation[2] in that context. (Practitioner 38)
We do risk assessments for each adolescent we work with in our initial assessments, but like you know it can take several engagements before the young person even discloses … The [young person] with the speech [disorder], it was like six sessions and Mum eventually said to me or
“You know, last time Dad got on the beers, the kids were pulled out the window by the police.” (Practitioner 17)
Violence doesn’t just come out of nowhere for these young people … these young people are generally survivors of experiences of violence, either past or current. So that’s something that we’re always keeping in mind … that’s my priority when going into these assessments, finding out about the safety of the young person and what’s going on at home … (Practitioner 49)
Keeping an original perpetrator – and potential systems abuse – in view
The research showed clearly that assessments for young people’s exposure to adult-perpetrated violence need to include assessments for current experiences. Where an adult is separated from the family, this should include mapping and understanding the impacts of ongoing systems abuse or, as one practitioner called it, “the shadow of the perpetrator” (Practitioner 27) in the young person’s life. A crucial part includes understanding the impacts of this on an adult victim and survivor.
I definitely take the strong family violence lens of kids’ behaviours are definitely triggering and re-traumatising Mum and her responses are in the [context] of that but also that the adolescent family violence is not Mum’s fault and … re-framing that with her and just working with her to strengthen that …
I’m thinking of one particular client at the moment where the children’s behaviours have just escalated beyond belief, you know strangling Mum, phone-stealing, stealing car keys on purpose and locking her out and things like that and Mum just doesn’t have the capacity to respond to that because it’s re-triggering her from the family violence perpetrated by the father and the father is continuing to kind of perpetrate that family violence through that kind of coercive control. (Practitioner 20)
We do have kind of a cohort where you’ve got … your persistent, very toxic partners that [are] misusing the family law courts, misusing breaches … and continue to make the woman’s life hell and well until … the youngest child is 18 … it’s also the presentation of the mum, because often they do have quite a typical post-traumatic stress disorder kind of symptoms and you can’t make head or tail of it and they come across as quite crazy or mad or enraged and resentful … and it would be really easy to, you know, kind of blame her or disregard her or disengage … when actually underneath it … you’ve got a really tricky and toxic ex-partner … that presentation will just send her to a GP for medication, or you know she’s been seeing a psychologist for 15 years, but there’s no change . … [those] symptoms and behaviours are in the context of the world that she’s living in, so you have to kind of ask around it. And, also, you have to slow things downenough and be respectful enough to hear that story to not rush into solutions and be yet another person telling them that they’re wrong … [and] paralleling an authoritarian power over response. (Practitioner 2)
DS practitioners explained that a whole-of-family approach can also offer an opportunity to obtain crucial contextual information about DFV behaviours present, with the below examples demonstrating some of the complexities and challenges involved in engaging with adults using harm or keeping an original perpetrator in view and suggesting considerations for emerging practice.
Promising practice:
Surfacing adult-perpetrated DFV
- The young person’s father and sibling (who was identified as at risk of using violence) were all on separate files (DS170, DS621, DS631). While the parents accessed support from DS to explore the young person’s aggressive behaviour and support him to change that behaviour, the father’s own use of violence – where he “rages”, breaks the young person’s property and is in conflict with the mother – also required attention. Having separate engagement with these family members enabled the father’s pervasive use of violence and the impact of this violence on the young person and their sibling to be surfaced.
Promising practice:
Needing to keep potential control in view
- In case DS021, DS was engaged with a 13-year-old’s mother, while the father (mother’s ex-partner) requested to be involved with the program separately. Intake case notes indicate that the young mother had applied for a protection order against her ex-partner in the past (not current) as a result of DFV perpetrated against her and the young person. The father’s willingness to engage with the program may have represented an opportunity for positive change within the family structure (though the research team noted that it could also be a tactic for controlling the engagement by other family members). Case notes from the file indicate that risks were discussed between the DS co-workers within the program to facilitate engagement with each parent. Case notes also refer to DS practitioners consulting with parenting practitioners to establish appropriate supports for the family.
More broadly, practitioners across the research described constantly advocating to Child Protection and other services around fathers’ behaviours and the fact that this should be the priority.
… the complexities with the families coming in … with family law court orders and [protection] orders … we do consults with them at the beginning to get an understanding, but what those support periods could look like and what the risks would be if we were providing supports. For example, if you were providing support to a young person, what that might mean for them, but also what that might mean systemically … so within the justice system, as well as within the family law system and Child Protection as well … It’s challenging because you have to think really broadly about the implications of systems abuses … by people who have perpetrated violence … holding the knowledge around what that could be as well. (Practitioner 32)
… if Mum’s still in a relationship with a perpetrator and there’s an adolescent and Mum’s afraid of stepdad – it’s often stepdad – and adolescent both, so she’s dealing with both. It really just becomes … a black-and-white kind of description. Is it stepdad or is it the child? And often children can really feel ganged up on in those situations, whereas there is a complexity where … it might more often than not actually [involve] dealing with both and that’s really, really important to empower Mum as much as possible rather than going down this really, really simplistic kind of you know “Who’s to blame?” way of doing things. (Practitioner 65)
An equally crucial part of this work includes identifying where young people have been misidentified as the predominant aggressor or inappropriate target of the system’s intervention, and advocating for a different approach.
I’m thinking of [a] family in Child Protection, there were male perpetrators within the home, but everybody was blaming this young person … and wanted … us to “fix them” … And we kept saying, “But you’ve got this adult perpetrator in the home, like, who’s holding him accountable?” So, we’re really bringing that lens and safety framework together to that care team … we actually had really good outcomes. The Child Protection worker did a bit more work on that and then ended up removing [the father] from the home. (Practitioner 27)
There’s times … where we’ve attended a joint care team meeting after reading through the referral and realising that the current [adult] family violence risk in the family home was actually what the priority was, not the young person’s use of violence. That young person had actually been moved into a residential unit and was very much being blamed for what was going on in the family, when [we] could really see that there were so many other things going on that were concerning and so we are providing, I guess, that systemic lens at times. (Practitioner 22)
I know everyone wants a quick tick-a-box answer, but actually we really need the essence of … what’s happening and the recent referral when I met Mum and Dad, it’s like, “Whoa, you know, Dad just took over the session” and … so already I’m going “Whoa, there’s a lot of control issues happening here.” So … we’re in trouble if we only tick a box and don’t get the essence because the control is always hidden underneath. (Practitioner 2)
Probably what’s been the biggest eye-opener for me … is the misidentification … around young people being the ones who are committing the violence. However, when you kind of unpack stuff … parents are so much better speakers, I guess, and can advocate for themselves. And so yeah, so we would probably see a lot of this firsthand … (Practitioner 52)
The potential for misidentification of young people – or at, the very least, a failure to identify an adult perpetrator who remains out of the system’s view – has therefore become a subject of system and practice advocacy for many of the practitioners participating in the research.
The complexity of dealing with an unidentified adult perpetrator and the practitioners’ lack of awareness of that or challenges around that, or just acknowledging the general challenges of working with adult perpetrators and how manipulative they can be, also charming or how pressuring they could be on a sole worker which can then overflow into our workspace. And I think then for the worker not actually putting two and two together and considering the safety impacts of that on the young person in this approach … (Practitioner 27)
I’ve been in court where there’s a very clear rhetoric that a present parent is a good parent. If a parent has showed up … then they couldn’t possibly be perpetrating violence against a young person and you are pushing a big rock up a big hill if you’re going to allege otherwise and it just it baffles me a bit because we all of a sudden change our thought processes around these young people and that … they have become people who use violence and there’s nothing more to be seen … It’s like this unique little element of the world where we … think parents are doing a fantastic job because they’re there and they’ve showed up. And it might not be physical violence … but recently we’ve had [from parents] withholding food … we’ve had all sorts of manipulation. (Practitioner 49)
… the way in which we tend to be raising AVITH … at the moment, it’s through some of our existing kind of campaigns or advocacy pieces, so it’s a part of our mis-ID work. It’s a part of our … work which is about kids in residential care who cross over from Child Protection to come to youth crime and … it’s an issue that’s raised there … and usually we are drawing on the same recommendations as the PIPA report. (Practitioner 65)
Crucially, practitioners also described the way in which keeping adult-perpetrated DFV in view could contribute to appropriate sequencing of interventions and collaboration as a way of ensuring that safety was prioritised and that the most immediate needs of the family were addressed.
If a parent is experiencing ongoing and current intimate partner violence, then … change within that family system approach is very, very hard … So we would usually encourage the mother … to engage [in an appropriate specialist service] and … look at trying to support her with the intimate partner violence situation first … And so you wouldn’t just drop out in that situation, we would continue to work closely with other … specialist services. And in those cases … I think that’s probably been the best kind of collaboration that we’ve had because, I mean … when risk is very high, everybody is really sort of on their game maybe a bit more and so it’s a bit more tightly managed. (Practitioner 12)
Reflective practice and emerging collaboration
Reflective practice and curiosity
Echoing the advocacy and collaboration in the example above, AVITH-focused practitioners told the research team that they were trying to encourage more reflective and critical approaches.
A lot of the other services or people around the young person are … not necessarily taking a step back … and being like “Hang on a second … let’s just think about this. What’s going on here? What’s behind that? Let’s … spend a period of time in this care team being reflective, [that] can be a really powerful way of being a point of difference.” (Practitioner 22)
We tried to take much more of an analytical view of multiservice involvement … often driving that care team process. I think that the more pressured that services feel, the more siloed they tend to work within … It’s quite helpful that we tried to often try and … drive that process in coordinating, really understanding, who’s doing it and reviewing that. (Practitioner 13)
This also went the other way, with specialist youth workers very keen for specialist DFV knowledge and a lens on adult perpetration to be included.
When specialist family violence services are there [in care teams] it can be super helpful around understanding orders, understanding the justice system, navigating legal advice, even navigating like things like trauma, support and stuff for parents, which is fabulous. (Practitioner 57)
Reflective practice and inquiry could include querying how other practitioners might speak about the young person or protective parent in care team meetings, as well as encouraging other practitioners to reflect critically on whether there was adult-perpetrated violence still occurring in the young person’s life.
Just as importantly, where practitioners do not necessarily bring a shared conceptualisation to the work, AVITH-focused practitioners explained that they would attempt to develop that shared conceptualisation as part of an ongoing conversation.
… so just the level of advocacy that needs to take place, like in any and almost all spaces, like wider care team spaces, for not just the young person that we’re working with, but also the ongoing exploration of practice from other practitioners in the sector. There’s also the amount of work in the time that it takes to sit in a care team meeting, which involves constantly kind of questioning back: “Oh can you tell me a little bit more about what you mean when you’re asking that question?” and “When you refer to the young person in this particular way, can you just talk a little bit more about what your understanding is of their experience prior to your involvement?” And so yeah, just a lot of work across the sector in those care team meetings … (Practitioner 33)
… the collaboration often is around actually having a coherent conceptualisation, we hold the direction of the work and we’re trying to get everybody on the same page and sometimes … that might be in opposition to what other services are saying or focusing on … we’re holding the case direction and conceptualisation and kind of the assessment and what then needs to happen and trying to get people to … be working together. Another key one which people don’t think about is … that the parenting [is occurring] under abnormal circumstances and so normal parenting strategies which do seem good actually work counter. So sometimes we are actually advising to do the opposite of what might be good sort of parenting. (Practitioner 2)
… there’s been some really good collaboration … with services when you can start to do that advocacy around the young person’s experiences so that – again, with consent from that young person – can be shared with other services that are engaged with the young person or the family so that their side of the story is also known to those other services as well, an independent, well-resourced family violence service that can do whole-of-family assessments on an urgent basis … in the same way that there is urgent need for [Child Protection] reports or whatever else, that there is an urgent point of escalation for these families … And the other side of that is that there’s someone independent assessing what is actually going on? But trauma-informed too … Walk the walk and talk the talk, or at least listen to the people who have tried to walk the walk and tried to talk the talk and are trying to guide you on that path … Even if you don’t knowyourself, have open ears to the people who are trying to explain it to you. (Practitioner 49)
Reflective practice and collaboration also included capacity-building in wider services by providing secondary consults. This was particularly valuable where other practitioners are working in very different practice settings or disciplinary frameworks.
[I’m thinking of one example] … we were kind of like polar opposites, like, we’re youth work sitting in family violence and she was a family violence worker sitting in a youth team … We kind of partnered up and she … sent us this really lovely email just appreciating the connection because it was … isolating for her to be sitting alone with … people not sharing the same framework. So we were trying to have a, like a bimonthly reflective practice where we could get together and just have the space to … talk about practice and talk about frameworks. (Practitioner 29)
I’ve opened conversations with Child Protection workers around [Aboriginal and Torres Strait Islander families’ experiences] because … there’s definitely been times where just a lack of understanding around those kinds of things has meant that some workers from the Department have acted in a certain way … and we’ve been able to talk to them before they’ve been able to kind of have that conversation with the family themselves. (Practitioner 73)
Practitioners participating in the research spoke about the value of opportunities for shared discussions and reflective practice within their organisations, as well as cross-organisationally.
… it’s translating into changing me as a practitioner, I know that I’m just one person and this is what I need to be able to sustain myself in the work and to sustain my drive and commitment to being so person-centred in my work. And I can’t do that if I don’t have the space to have, you know, other people reflecting all this stuff with. (Practitioner 28)
We talk so much at the moment in the sector around having an intersectional framework, but then what does that actually mean for the people that we’re working with and identifying through these labels? … What does that mean when they’re also talking about, like not being able to read and write and then, like going to specialist classes and you know having ADHD and you know then talking about the medication … But it’s like “How do we draw all of those bits together as a support team?” If you have particular practitioners that may work in similar ways, then that support team can feel very different and very like their support is driven by the young person in the family rather than the ideologies of the particular organisations or teams. (Practitioner 32)
… with all of us needing to be skilled up across the whole sector, with [risk assessment and management approaches], with understanding around mandatory reporting and information sharing … it feels like the last two years now, we’ve been really skilling up … so I think from what it used to be to what it is now, people are really good at identifying … where might be red flags or even just to be curious around some of the descriptions that young people might present with around their own family relationships so the assessments have shifted as well, like those documentations have all been amended too. You know it’s those kinds of simple ways of kind of trying to understand and then be curious further. (Practitioner 35)
This was echoed in the experiences of DS practitioners who were able to benefit from the practice lead overseeing their program.
Promising practice:
Internal collaboration
- The case files indicated collaborative work occurring within DS itself, including supervision between DS colleagues to discuss the progress of case files (e.g. DS321). In one case file (DS054), the DS practitioner’s supervisor provided secondary consultation regarding the frequency of meetings between the family and the DS practitioner, including increasing frequency following an upcoming court hearing date. A secondary consult via supervision appeared to be particularly helpful where DS was engaged with the family via multiple programs, reflective of increased complexity within the family case.
Collaboration
Across the research, practitioners were regularly collaborating with each other in support of a young person or family, although to varying extents in different contexts. This included highlighting the welcome advent of care team meetings online in the context of the COVID-19 pandemic, a practice which was continuing past lockdown periods and was saving practitioners a lot of time.
… because we’ve been going out there and kind of forming these connections, [services] … just call us and go, kind of just do a bit of a consult, “Is this a family that’s appropriate for your service?” and then we kind of have a bit of a chat … or we’re part of a bigger care team that’s already there … I’ve got one where there’s Child Protection, then [sexual assault service] are involved and there’s a whole bunch of different services for the family, as these things usually work … I can’t think of a case where I’m working just with the family. (Practitioner 10)
When asked to describe their experiences of collaboration, practitioners gave varying examples.
I can think of examples … just where I’ve worked with a young person at the school and then two weeks ago I got … an email from the school saying “I’ve got a parent talking to me about the young person using violence, how do they refer into your program?” So she wasn’t clear about the process, but she obviously recognised that’s what we do … So I’m like, oh well, “tick”, that’s good … It’s small, but it’s still, you know, you just don’t know how that ripples … (Practitioner 5)
[Across specific] services there has been quite a bit curation of “Who can see this one, this one’s an urgent one, who has any time now?” And some of that … we’ve sort of stepped in because our other systems weren’t working … We will get some families who aren’t engaging with [other services] very well, so they kind of do that referral for us as a last ditch … So then we’ve managed to actually build up a bit of a rapport with some of the families to then get them to that next step. So … that collaborative space is really vital. (Practitioner 62)
The RAMP [Risk Assessment and Management Program] coordinator called me saying there’s a real lack of somebody with adolescent violence, kind of experience. And “Can you please consult with some of the families that were there that are coming to us?” You know that kind of thing, so I think there is a bit of action going around people thinking about this in a different way. (Practitioner 9)
Practitioners in ACCOs also emphasised that often their wraparound work was about the young person’s wider needs which may or may not be contributing to use of violence at home.
This young person … was going through self-harm and suicidal thoughts and already escalated to the suicidal plan. So … it was a wraparound service that came on board to look after this young person and then we went to the steps of, you know, who would be doing what, coordinating to their roles. [We communicated] … that we had put in measures of safety plans within our family violence case manager and our adolescent youth worker … and our therapeutic family violence counsellor. We also hit the schools that were monitored and contacted around that youth to ensure they have a safety plan there and we yeah, we installed a safe to put in, you know items that may harm that young person. So, it was a lot of emails, a lot of follow-up, a lot of steps to have that safety around that young person. And on Monday she had verbally said to the counsellor that she felt safe and supported by this group. So, I think that was an excellent example of wraparoundfocus for families. (Participant 75)
Practitioners also described varying levels of success with different forms of collaboration – across organisations, as well as within them.
When you’re working across different organisations it becomes a very complex dynamic trying to sort of co-work with families when that level of handover isn’t there, they’d have different policies, different procedures, different responses, and you would think that all organisations work in the same way, but they really don’t and I’ve been in that space … where I was trying to run a joint triage across two organisations and it was very problematic. There was lots of double handling and … it didn’t work and they’ve actually brought it back to now to being held within one organisation because it’s actually quicker, more streamlined, faster, and can provide a better service to families. (Practitioner 25)
In the last few months, within our organisation, there’s been some good changes to allow for more collaboration within that sort of larger team. And … so people within the team can consult with us to if they want to, if they’re working with Family Services and they identify that there’s an issue, then they can just have a consult without necessarily doing a referral. And then even that helps build knowledge within the organisation of what [AVITH program] is, which then goes out to the broader community, and they remember you, they’ve got all your contact details and so that’s how it works. (Practitioner 5)
Examples of collaboration and communication with different services were clearly apparent across the case files. Sometimes this included informal liaison, sometimes it included care team meetings and sometimes it included decisions to withdraw from service engagement to avoid over-servicing. Data indicates that 10 families (30.3%) had formal care team meetings/consults during their engagement with DS. The number of care team meetings held for families across the case files ranged from none to as many as eight.
Promising practice:
Working with multiple services to facilitate practical support and safety
- In one example (DS098), DS extensively liaised with other services involved with the young person and their family. DS contacted the Men’s Referral Service to find housing and case management for the young person as a (young adult) male excluded from the home as a result of protection order conditions. The practitioner liaised with the social worker at the mental health unit from which the young person was discharged and organised housing support. DS also liaised with [specialist DFV service] regarding housing support for the mother and other children and liaised with the Asylum Seeker Resource Centre. DS also organised ongoing financial and food support for the mother and the family and provided assistance with getting onto Centrelink payments.
Promising practice:
Safety planning in care teams
- For the family which had eight care team meetings during engagement with DS (DS456), services/practitioners that were regularly involved included a school wellbeing officer, child and adolescent mental health services, Child Protection, DS and community primary health services. During these care team meetings, a safety plan was put in place for the family, as well as plans to support the young person’s transition into residential care and to coordinate the young person’s move from that facility to another residential care facility, while balancing the young person’s distance education.
Promising practice:
Flexible and client-led approaches – mitigating over-servicing
- In one file (DS443), case notes indicate that the DS practitioner eventually ceased working with the family because it was determined that the young person and mother were well supported by the care team. Case notes indicate that the DS practitioner undertook the following work with the family: supporting the young person and mother to navigate the criminal justice system; linking the young person into services; safety planning, risk management and liaising with workers; and family functioning support and advice. On case closure the family was engaged with a NDIS worker and a psychologist.
Examples of promising practice across the research also included collaboration with police or joint attendance at DFV police callouts by a specialist youth team, which echoed other collaborative responses by police, such as those conducted in the mental health context.
Basically, we would attend [the callout] with police, but then … we would facilitate that referral to [wider youth service], but we would also go to the house and have that conversation with the family, with the young person … Is that what they want? … explaining you know that it is voluntary, that it is going to support them. (Practitioner 54)
So, I had … the Youth Engagement police officers … reach out to me around a young person that I was working with and they wanted to have a conversation with the care team about what was the most appropriate emergency response for them to have. And we had a fantastic conversation with the police officers, different members of the care team and the parents as well. We wrote down a story for the young person around that and the way that they could understand when police got involved and the police were just fantastic. They were really creative, really open in what they could do in their response for the young person. (Practitioner 22)
We’ve got a really lovely example of where it worked really well using multiple services bringing people together for this family. This boy had been using violence for four years daily and throwing, you know, [things] off balconies, smashing windows. He was 12. And every car panel was smashed in. Urinating in front of his dad if his dad said no to something. I didn’t know what to do … and we couldn’t have done it on our own, I think. But … coming in with different services, we were lucky that … in the area that they live in, there’s a great community police officer. So we were able to focus on … getting this boy assessed and understood and helping the parents build their capacity and … [the police officer] went out and actually had a chat with the boy. He provided the external motivator in some ways of, you know, “Mate if this continues, then there’s a good chance you’re gonna end up not living with Mum and Dad” and he’s like, “Well I don’twant that” … And we continued doing the work with the parents and we assessed him and you know, ADHD, ASD, people understood his social communication approach needed to be very different and just the combination of it all for this family … Dad realised he’s got ADHD as well so he went off and got himself diagnosed and ended up medicated and less reactive, less impulsive and he was actually being physical, you know, with his son as well and using his frame to protect his daughter and his wife. But he was being aggressive with his 12-year-old as well. So, lots of shifting needed to happen [but] it’s a good news story. (Practitioner 41)
AVITH-focused practitioners were regularly creating or instigating care team meetings to get a sense of the services involved in a young person’s life and then coordinating how each role would function.
I work with young people who initially don’t have anyone, so there’s lots of care team creation – I think one of the things that I have tried initially to do when connecting is getting a really clear picture of what their parameters are, what they look like they need to do within their role and what they’ve got the capacity to do within that role and then trying to really pin down what each person’s doing … That’s the really tricky thing, young people are not siloed beings, so it’s about us sort of working out the parameters of each role. (Practitioner 55)
When I start to work with someone, I find it really helpful just to have a care team meeting [to ask what’s] your scope and what are other people doing so that 1) there’s no overlap and 2) there’s no underlap and … so we’re all aware of what’s happening specifically with that young person … It’s been really helpful to get little bits of information around risk, say the perpetrator’s family calling or passing by, like little bits that add up to be a lot more serious … And having that constant dialogue … I feel like we’re pretty lucky in that within our team … you know, we sit and we talk about risk and strength and safety and family violence constantly. (Practitioner 30)
Practitioners from a service which worked extensively with Aboriginal communities in a particular regional area pointed out the importance of maintaining a constant dialogue around the intersection of other forms of violence and structural harm, including racism and intergenerational trauma.
I think that’s where I’m finding … some of the really good work to be done and because it allows it as well – probably like buzzword – but to be intersectional because it’s not saying, this is just family violence. It’s like this is intertwined with every other form of violence and community. Every other form of racism, discrimination, like all these ideas, are all intermingled – and what these kids are hearing on the street and in school every day. (Practitioner 45)
Advocacy around the best approach to engagement was also crucial in situations of complex trauma or multiple needs across a family.
[Practitioner] had one of her cases where … she did meet with the parents, but … the young person by that point was in the residential unit. You know, we could have intervened 12 months ago, that was probably the right time, but at that point, the focus actually needed to be on the young person without the context of the family. And so, you know, doing systemic work with the care team, [identifying] the most appropriate service and why we’re recommending that service … as to why it wasn’t safe, you know, and the outcome of that, for example, was that Child Protection were able to prioritise it for an intensive therapeutic service … because that was what was required … (Practitioner 22)
The case I’m thinking of, I mean it was … horrific violence, just day-to-day, nonstop … and Dad had a disability, you know. So, everything was just long-term trauma and cultural diversity … so many issues. And yeah, and the Child Protection worker finally listens to me …. And it’s like oh that’s like a breath of fresh air, thank you, because I want to tell you not to force the young person to come in because we’re about to escalate a situation of violence. (Practitioner 1)
Collaborative work on the case files also included working with Child Protection in several cases.
Promising practice:
Working with Child Protection
- In one case (DS147), Child Protection and DS discussed concerns about the father’s ongoing behaviour towards the young person and his “unwillingness to do the work in relation to his behaviour and motivation for change”. In this case, Child Protection informed DS about other reports in relation to the young person’s behaviour and that the mother recently self-referred to the Orange Door. At the conclusion of the discussion, case notes indicate that “CP was going to do information sharing and explore a [protection order] and reconnect with DS”. In this case, evidence of DFV behaviours resulted in the young person being reallocated to a separate case as the sole client to work with DS because of risks brought up during the risk assessment.
Also crucial in terms of emerging forms of collaboration was growing awareness on the part of Victoria Police in terms of young people being linked with legal advice, as well as linking the parent or young person with other supports prior to a court hearing through specialist court practitioners or a specialist legal service (Practitioner 61). This included growing awareness in the magistracy about the availability of services, where magistrates could encourage families to speak with relevant practitioners about connecting with services (Practitioner 60).
Just as importantly, the research team heard that pre-court referrals and discussions between lawyers and police could result in more constructive court outcomes, including the withdrawal of an application for a protection order or an agreement to an undertaking so that young people were not at risk of criminal charges upon breach (Practitioner 73). As well as removing the risk of criminalisation for the young person, recent research has also discussed the way in which application for protection orders and involvement in the legal process can actually increase risk for victims and survivors of AVITH by further undermining the mother–child bond and also by placing protective parents (usually mothers) in the role of helping young people to comply with the orders and avoid breach (Campbell, 2021; Campbell et al., 2020; Centre for Innovative Justice, 2022). The research team also heard about strong relationships andworking groups across the Children’s Court, Victoria Legal Aid, Youthlaw and the RESTORE Program at the Children’s Court (Campbell et al., 2020), as well as increasing advocacy by the Children’s Court specialist practitioner in the context of other specialist networks across the wider Magistrates’ Court. These working groups could allow stakeholders to share case examples and “ventilate an issue” (Practitioner 65) in a way that ensured that practice or system barriers could be overcome. Important to note here, practitioners observed that relevant government departments needed to be more engaged with legal and court stakeholders.
Case files indicated that collaboration was also occurring between DS and services working in the context of the legal system. An emphasis here appeared to be on clear communication about roles so that families felt adequately supported but not overwhelmed by service involvement.
Promising practice:
Collaboration in the context of the criminal justice system
- A young person in one case file (DS443) was referred to DS by the Melbourne Children’s Court due to their criminal activity, as well as being the respondent to a protection order related to a matter outside the family context. Care team meeting notes indicate that the young person had been associating with a group of friends who identified as a gang. The young person’s mother reported that the young person was using drugs, becoming increasingly unpredictable and aggressive, and stealing money to pay for the drugs. The young person had also recently received threats from other students at his school who alleged that the young person owed them money. The care team included a youth specialist from Victoria Police, an outreach worker and a Youth Justice worker. The files indicate that these responses assisted the young person to access support needs; supported the young person in understanding risks, decision-making and strategies;and supported the young person to navigate court orders and legal matters.
As one practitioner working in the legal context observed:
While it feels cumbersome, there is collaboration, and there are positive outcomes … We do achieve really good outcomes on a very basic level that young people aren’t left with full court orders against them and potentially impacting their future … It’s not necessarily that it doesn’t happen, it’s just that it’s not very streamlined, would be my view and there are exceptions to that, where it’s an uphill battle, but for the most part I think we do get there. (Practitioner 49)
Improving collaboration
While practitioners regularly worked in care teams, as discussed in Part 2, they also highlighted what could be prioritised in the development of future responses.
I think there’s one thing I’d like to see in a AVITH care model … is that built into that assessment is a really genuine asking of the parents of, in some way, of “Where are you up to? What is your capacity to respond at this moment?”, because we can throw all the ideas at you in the world, but if we’re not genuinely attending to both parties saying “Where are you up to right now?” it won’t work. And have some way of kind of almost scaling, on a scale of 1 to 10, you know, “What’s tolerance for your child today?” Most parents will tell you a different scale every day and I don’t think we ask that … (Practitioner 38)
If I had, you know, a pipe dream, it would be that we think about who’s supported … You know this care team is not just around how do we sort of identify who else is tending to the young person, it’s “Who[’s] tending to Mum? Who’s tending to Grandma? What do we know about them?” (Practitioner 29)
… if Child Protection would work more collaboratively to take us more seriously … we do need some things at times and one of those is just the authority to kind of pull people together. (Practitioner 2)
When [government] sort of first … had the program as a trial program, it wasn’t clear necessarily what the role was going to be and what we were going to do. And so, you know, [we] kind of spent time sort of a little bit of trial and error and trying things out, brainstorming what it should look like … particularly for the community that we’re working with … we’re still continuing to make those connections. (Participant 73)
Considerations around information sharing and consent
Of particular consideration for practitioners in terms of how interventions could work in the future were issues around information sharing and consent.
I think there’s been some really great collaboration, mainly with the youth services that are already engaged with that young person specifically. We’re really open – again, with consent of that young person – for as much information to be shared with us prior to us engaging with them so that we can come at it with all that information already. And then we can work in a collaborative way (again with consent of the young person) to work together on their needs, which is really, really great. (Practitioner 51)
Practitioners were not suggesting that the young person’s consent was not required – rather, that the nuanced way in which practitioners may need to navigate these issues should be acknowledged in the design of the service and in guidance given to practitioners. This was to maximise opportunities for supporting different family members while also ensuring that confidential information was not inappropriately shared.
I always check with the family member if they want that particular thing shared at the [internal case study team] case discussion and I feel like that is really, really important … And to always remember that this is just information sharing, this isn’t to then shift the focus of the next session or the intervention and not to disclose exactly what has been shared in that discussion, because that can have huge impacts on the family. (Practitioner 33)
As flagged earlier in the report, the need for parental consent where a young person was under 16 could often function as a barrier to service engagement or even increase risk where a perpetrator parent was seeking to gatekeep or exercise control. This signals a particularly important consideration for AVITH-focused service design and highlights the importance of nuance in the practice, as well as future policy considerations around considering ways for children and young people to access relevant supports without parental permission, such as having a safe and trusted adult professional who the young person nominates to provide consent on the young person’s behalf.
Recognition of AVITH work as specialisation
Recognition of the weight and severity of work in relation to young people’s use of AVITH and the context in which this was occurring was a theme which emerged spontaneously from the focus groups.
I think that [this organisation] they have amazing supervision and they have really amazing reflective practice … and just that space to have ongoing learning to be aware of what’s happening outside of the organisation and be updated … Your window of tolerance is definitely bigger when you feel safe and supported by your team and … that can increase your capacity to stay regulated … so that we can go into thinking about these cases flexibly and creatively. Whereas I think if people aren’t afforded that safety and the support, they’re responding to things in a really heightened state and you can’t think flexibly in those states and that’s where you get, you know, the blame, the shame, the judgement, the fear and the anxiety. (Practitioner 28)
We try to make sure they’re supported in supervision and clinical supervision because some of the stuff is really pretty hairy and it’s pretty scary. (Participant 72)
As an [AVITH worker], you have to be pretty confident that you’re bringing something that they don’t have … I feel pretty confident in articulating that … and I think that’s probably because of where I worked. I wonder if I didn’t have that experience at [specialist sexual assault and family violence intake] and if I purely came from Child Protection into [this program], whether or not I would still be working the way that I am. (Practitioner 20)
Multiple practitioners spoke of the need for recognition of their work as a specialisation – something which involved the development and provision of training for existing practitioners, as well as investment in the development and embedding of an associated workforce. Here practitioners recognised that the CFECFW was in the process of developing training, although at the time of writing in 2022 it was still not certain when this training would be released or delivered.
We need more staff, we need more specialist practitioners in this space. Because of holding such complexity and risk and the amount of work it can potentially be with a family … that’s a barrier for us to being able to like take on more and more clients. (Practitioner 31)
What we’re doing takes skilled and dedicated practitioners and they’re so hard to get when you keep stuffing people around … because they wanna work in a long-term and secure environment and so, you know, we are just constantly putting families on the back foot all the time and saying they’re not important by doing that. (Practitioner 22)
Working with young people who use [AVITH] is a very specialised space with a mix of family violence, knowledge and youth knowledge predominantly and in the group delivery space, a bit of education skill wouldn’t go astray either. But there’s not many people that hold all of those things that come to the space and want to come to your program for 12 months or whatever that looks like. When we go to look for training to be able to support our practitioners to be able to deliver this program or work in a youth family violence space, there actually isn’t any. There was one person that used to deliver it … and that was a few years ago now. So, instead we are looking at, “Here’s some youth training”, “Here’s some family violence training” and “Let’s kind of just mash that together” … So, some absolutely focused training … would be amazing. (Practitioner 62)
The research team also heard that a specialist workforce was not going to be properly utilised without wider services being able to identify AVITH and refer young people and families into specialist support. This included in the context of Victoria’s family violence intake points via the Orange Door network, where a number of practitioners volunteered that a specialist AVITH role was required. This was distinct from existing child and young person–focused roles, as discussed in Part 2.
I also think it has to be … greater training or greater information at that base intake level, so those points of intake, those points of entry, more information for those workers to actually be able to know, through the assessment, identify the actual needs and then share that funnelling it through ’cause that seems to be those, those moments of loss … It has to be about what questions are getting asked or what training or capability those workers have to be able to see these programs for what they need to be … (Practitioner 6)
We just keep getting like all of these announcements for the new appointments to the [region] Orange Door and there were all these practice lead roles and it just occurred to me, why isn’t there one for young people? Like why isn’t the intersection of being a young person [and using violence] counted as, you know, a specific vulnerability – not because young people are vulnerable but because the system makes young people vulnerable. (Practitioner 29)
In addition to specialist AVITH-focused training, practitioners also spoke about the value of training which enabled workforces to understand the impact of adult-perpetrated DFV on children and young people, such as the Safe & Together Model, as well as training such as “Tracking Better”, which focused on emotional and behavioural regulation. Practitioners also identified a need for practice guidance, which they acknowledged would be produced by the Victorian Government in the future in relation to risk assessment and management.
I think having something that would ensure that we actually collaborate and that there’s some clear guidelines … I mean, we’ve got our own individual plans and our own individual program guidelines and what’s expected … We’ve got that as a service, but … I don’t think as a service system that we have that. (Practitioner 29)
I’m looking forward to the AVITH [multi-agency risk assessment and management tool] and all that sort of work that’s building on our capacity to deliver strongly in that space. So I think there’s still a long way to go [but] … there’s been some really good steps. (Practitioner 19)
A regular theme to emerge spontaneously from the focus groups was the need to “slow down” the risk assessment and management response and examine what was occurring across the family system.
… being more proactive in that space so, you know, police and ambulance are actually coming out to meet the young person when they are regulated and do some of that planning with them, I think is really key … It’s about slowing down thinking “What information do we have that can help educate the people who will be carers every night, every day, to understand how this young person functions?” and … really in terms of that wraparound and trauma-informed care – that’s the bit that we need to slow down on and work together across those systems. (Practitioner 38)
Imagine in an ideal world where we could engage with young people either experiencing or using family violence in this kind of slow, measured, safer way … The fact that a police officer at sergeant level can make that decision, they may have no experience in dealing with young people. And that there’s a more rigorous inspection of ex parte interim applications against children because it’s made ex parte against a child and then you are in the fight of your life to get a court to consider other issues around that. (Practitioner 49)
A further theme to emerge was the need for continued opportunities to share practice and learn from each other as their practice evolved.
Having more opportunities to kind of come together like, you know, to conference or things like that, where professionals can kind of network with each other and share those ideas and things more would be great. (Practitioner 73)
There’s a number of networks that we’ve got management engaged in/coordinated in. We meet weekly for allocations, so there’s a whole process around the agencies coming together. Reading through all the referrals that are sitting for the different agencies and, you know, an agreement around who’s going [to] pick them up. How do we disseminate those referrals? Who’s got capacity? Who hasn’t? Who’s the best service? So there is a lot of work that’s done at that overarching level, but, you know, there’s always room for improvement. (Practitioner 19)
Wider system support and imperatives
A number of gains and opportunities for further systemic improvement were volunteered by practitioners across the focus groups. A theme that emerged from the focus groups, for example, was the valuable assistance – as well as sometimes the lost opportunities – that collaboration with schools presented.
Many practitioners spoke about the difference that committed staff, whether classroom teachers or wellbeing coordinators, could make if they were aware of an AVITH-focused program or were otherwise capable of identifying AVITH and understanding its complexities.
I have seen schools and teachers who have just worked absolutely tirelessly and have for so long not had access to appropriate services to respond to a lot of these issues, schools that just go absolutely above and beyond. I think given the current lockdown and you know the [previous] five lockdowns before this, just when young people are not going to school, how much the situation does escalate, so it really highlights how important the role of schools are and the role of teachers having their eyes on families and thinking about how, moving forward, we can capitalise on those relationships … in recognition that, you know, a lot of therapy doesn’t happen in the room. It can happen in those spaces as well … I think that’s such an important opportunity. (Practitioner 44)
Another theme included recognition of the value of Victoria’s Family Violence Information Sharing Scheme (FVISS). Practitioners noted concerns that young people’s information may be shared without their consent where they are identified by the system as “perpetrators”, a label which may not be accurate in the context of misidentification and which also carries significant implications for their subsequent access to services. That said, practitioners across the focus groups more frequently nominated the creative and collaborative ways in which they had been able to use the FVISS to complete comprehensive risk assessments, including about the risk that young people may face from an adult in their lives, contributing to more effective safety planning.
I think that the information-sharing scheme has been really good in terms of completing risk assessments. I recently had a phone call with a young person who is being supported by one of the other Orange Doors and wanting further support. So I explained that we needed a risk assessment and she mentioned that she had already completed one, so we applied for a copy of that. So at least she doesn’t have to go through all of those questions again and then we could just fill in whatever she feels like adding and just reducing that retelling … So that has been really, really helpful. (Practitioner 28)
I think that’s where you utilise the care teams and the frequency of that information sharing … because sometimes people need a gentle reminder that they care and … I have found a few of my referrals have actually come over from the women’s team once … the adult family violence has been – for want of a better word – safety planned (and is no longer occurring) and then jumping over to us to work with their adolescent family violence. So I do think there is an increased understanding and the information sharing is actually occurring pretty well. (Practitioner 20)
Despite the value of the FVISS, however, practitioners spoke about the potential value of receiving wider system-focused information. This included providing information to courts about the support services that existed; leveraging other systems to provide police and other agencies with relevant information; and collecting and sharing aggregate data about the scale of the challenge. They pointed to the value of resourcing a centralised database of available services for families experiencing DFV.
Something that I see is missing … is sort of a centralised tool, so to speak, of what’s out there. So, if someone comes to court and you know and they’re linked in with [the specialist practitioner] and she says, “Okay, you live in [an area of Melbourne]”, to be able to jump on that and say, “Okay, well, in [this area of Melbourne] there’s x, y, z”, you know … “You appear to fit the criteria and I can try and link you in today while you’re with me” … Without that, you’re sort of fumbling in the dark. It’s a bit like, there’s stuff there, but no one’s turned the light on. (Practitioner 61)
… to have an officer who searches LEAP [Law Enforcement Assistance Program] and looks at the amount of times that the young person has experienced family violence in the home before they then go ahead and apply for a [protection order]. I know that they have access to that information, but they don’t necessarily go ahead and use it and so then, as a practitioner, you’re having to get signed authority from that young person to request … copies of all previous [protection] orders … because we don’t have access to all that information-sharing capacity. (Practitioner 51)
Practitioners spoke about the variability of the information they received about a young person or family, often influenced by their prior service involvement.
You get sort of like a cut and paste in Child Protection history which comes straight out of the Child Protection files … I think it really depends on the information that is kind of held on the Orange Door database when the referral comes in. (Practitioner 12)
[A concern is] that lack of data around what is actually happening to the kids … So, you know, where are the referrals being sent, where do they go at the end of the incident? Like do we have any idea of what the stats are in terms of who’s actually ending up with family or in some kind of crisis housing, and then … what is the percentage of incidents where there’s a repeat call out to the house? We don’t actually have all that information necessarily collected systematically across the state … we’re just still putting together the pieces of the puzzle. (Practitioner 35)
Given the complexity that is so apparent in their practice, practitioners spoke about the need for greater resourcing and thought being put into program design to support different aspects of the work, including design which draws on expertise from practitioners and people with lived experience.
Having people to help us with intake will then relieve us of things that we could be doing to kind of connect with community … And then there needs to be another level where we’re doing, whether there’s enough space, enough funding, and enough resources to be able to actually go out and do that sector development stuff, and also to be able to do some community development around this area too. So sector development, community development, and then also on the ground working with families … (Practitioner 5)
At the systems level, co-design of these programs with the frontline and also perhaps with families themselves, we’ve got peer workers in our team who are victim[s and] survivors of family violence and their input is just so valuable … (Practitioner 27)
Practitioners also spoke about opportunities to consider how supports that are currently available to victims and survivors of adult DFV could be made available to people experiencing AVITH as well.
What is safety planning with [AVITH] versus intimate partner violence? How is that different? And yeah, what options and resources are there and even things like, you know, flexible support packages, stuff like that – they’re not set up for [AVITH], they have specific criteria around, for instance, that the victim [and] survivor needs to leave or be planning to leave the relationship and … that’s not appropriate for the majority of those cases. (Practitioner 9)
Just as importantly – and echoing the findings of the PIPA project, which suggested that interventions in AVITH were coming “ten years too late” (Campbell et al., 2020) – practitioners spoke about the need for them to be brought into the picture earlier, a challenge when additional layers of intake and referral had been incorporated into the Victorian response.
We see so much work that you know, had we been involved a year earlier, we could have been able to do such beautiful work. So, we really would love to do a bit more work in the prevention space. (Practitioner 27)
Once a parent has decided to call the police, that’s at the pointy end already and we’re five L17s [police referrals] down the track. We need to be there now. (Practitioner 5)
Overall, practitioners who had developed a “specialisation within a specialisation” – whether over a long period of time or more recently – saw a need for ongoing practice development, research and interrogation.
The whole of Australia is only beginning to develop stuff for adolescent family violence … I mean PIPA is not that old. (Practitioner 65)
It’s so exciting to be doing this work but, at times … you look at the literature and there’s just really, really not much there, so kind of just getting those beacons and direction from researchers is really valuable – so, thanks. (Practitioner 24)
Part 4:
Towards a collaborative practice framework
As described in the Introduction and Methods sections, the Collaborative Practice Framework was developed through iterative engagement with practitioners who participated in the focus groups during July to September 2021. Findings from the focus groups were analysed and presented, together with a draft proposed Framework, to practitioners in a series of workshops in February 2022. Feedback from workshop participants was then incorporated and a further draft of the Framework tested and refined with practitioners in June 2022.
Aims of the Framework
Practitioners across the research indicated a need for a clearly articulated framework to underpin collaborative practice and emphasised the need for any response to be based on shared understanding of AVITH; the factors which often underpin families’ experiences of violence and harm; and what a genuinely collaborative service response involves. Practitioners also highlighted the need for any framework to be broad and inclusive, recognising that meaningful responses to AVITH can require the involvement of system actors outside of what we traditionally conceptualise as the “service system”.
Practitioners therefore described the key aims of any framework as follows:
- Supporting shared knowledge and consistency of practice: Despite considerable progress, the system’s capacity to deliver effective responses to AVITH continues to be stymied by service confusion regarding the behaviours that constitute AVITH, as well as the considerations central to any AVITH intervention. Practitioners identified that a key function of a collaborative practice framework is to underpin shared understanding among practitioners and across systems, as a necessary precondition for achieving practice consistency. Crucially, this includes enabling practitioners to maintain a shared focus on issues for the family and providing the scaffolding for understanding and responding to the function of young people’s behaviours, rather than the behaviours themselves.
- Improving recognition at the organisational and system levels: Poor understanding of AVITH across the system often means that AVITH services are insufficiently resourced and scoped in ways which fail to account for the complex considerations required in any meaningful service response. Practitioners described the benefits of a tool which articulates the complexity of working with families experiencing AVITH, as well as the benefits of ensuring that this work is properly recognised and supported, both within organisations and at a system-level. This includes recognising AVITH as an emerging specialisation, with program resourcing to include consideration of professional and practice development; supervision and reflective practice; and capacity to participate in relevant forums, networks and governance structures at the local and system levels.
- Ensuring role clarity across the system: Practitioners described one of the benefits of a framework as improving coordination with those services and agencies that may be harder to draw into a collaborative system response, including police, Child Protection, schools and the legal system. This requires supporting different parts of the system to understand the scope of their role in responding to AVITH, whether that involves referring to a specialist program or working alongside those programs to meet the needs of families. For practitioners working within more traditional service settings, the Framework was seen as having the potential to deepen practitioners’ existing understanding of the scope and expectations of their role, as well as to recognise where it might be necessary to draw on practitioners with different skills and specialisations.
- Bridging knowledge gaps between systems and sectors: Where services and agencies within the wider system are drawn into AVITH service responses, practitioners described the ways in which a clear framework for collaborative practice can build understanding across different sectors of key considerations when responding to AVITH. Improved understanding of the factors which can underpin AVITH, particularly the prevalence of trauma experiences for young people using violence in the home, can, for example, contribute to more informed decision-making where a young person comes to the attention of the legal system due to being identified as using violence. Informed decision-making can include linking a young person or family with appropriate services and supports which can address the functions of a young person’s behaviour, rather than delivering a punitive response which is likely to compound harm and systemdistrust.
Figure 1: High-level overview of Collaborative Practice Framework: Multidisciplinary and multi-system
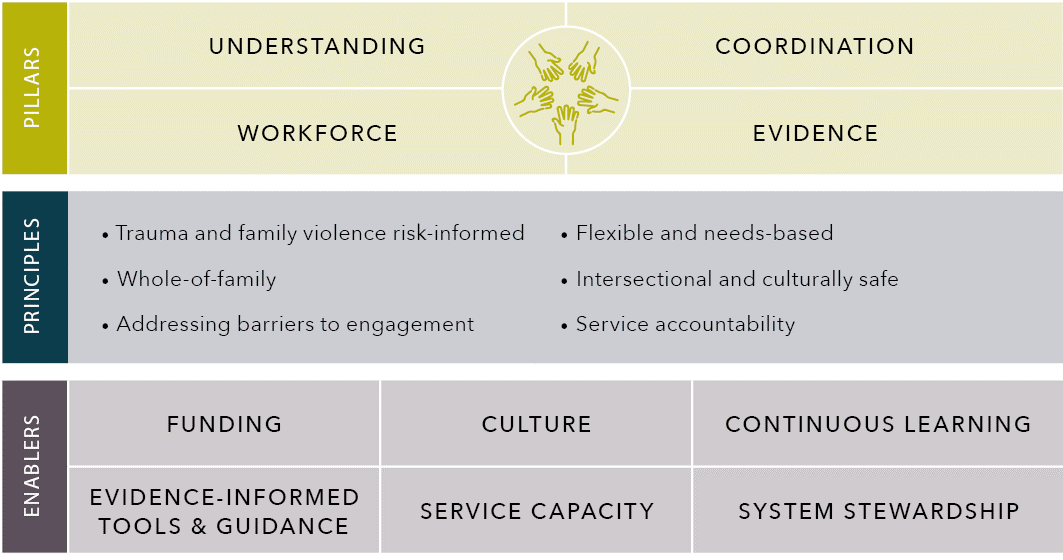
Source: Centre for Innovative Justice.
Text alternative to the figure above
Understanding
- Understanding
- Workforce
- Coordination
- Evidence
Principles
- Trauma and family violence risk-informed
- Whole-of-family
- Addressing barriers to engagement
- Flexible and needs-based
- Intersectional and culturally safe
- Service accountability
Enables
- Funding
- Evidence-Informed Tools & Guidance
- Culture
- Service Capacity
- Continuous Learning
- System Stewardship
illars of collaborative practice
The proposed Collaborative Practice Framework is based on the four core pillars of understanding, workforce, coordination and evidence. As well as constituting individual components of an effective, system-wide AVITH response, practitioners emphasised the mutually constitutive nature of the pillars, with each continually informing and reinforcing the others.
Understanding
This pillar involves development of a shared understanding – across specialist practitioners as well as the wider service sector – of AVITH. This includes conceptualisation of AVITH as distinct from adult-perpetrated DFV, and in ways which account for trauma (including, most prevalently, from adult-perpetrated DFV), developmental stage and the function of used behaviours in AVITH presentations. Shared understanding can help to challenge and unpack binary paradigms. Understanding also involves establishing a shared language – across the multiple services and agencies involved in responding to AVITH – of key terms and practice approaches, such as “collaboration”, “whole-of-family”, “family violence/DFV risk” and “family safety”. Finally, understanding relates to the need to establish a clear understanding of roles and responsibilities at the system-level and individual practice level. This improved role clarity can, in turn, improve practitionerconfidence and reduce the sense of simply “holding risk” rather than responding meaningfully to address it.\
Understanding in practice:
Role of practitioners
- Adopt language which emphasises a young person’s and/or family’s strengths and which reduces shame and stigma. Be mindful in how the service is presented to young people and protective parents to avoid stigma, as well as to non-protective parents where consent may be withheld as a further means of control.
- When working alongside non-specialist services, use interactions (such as care team meetings) to build capacity and understanding, including by sharing information which can aid wider services in maintaining visibility of the family context and challenging views and approaches which do not adequately distinguish AVITH from adult-perpetrated DFV.
- Centre the young person’s achievements; a caregiver parent’s strengths and resilience; and the need to bring any adult perpetrator into view. Advocate for the intervention of certain services and recognition that imperatives that operate in some contexts – such as the imposition of parental boundaries – may be counterproductive or harmful in the context of AVITH.
Understanding in practice:
Role of organisations
- Design and scope AVITH-focused programs appropriately and in ways which allow for highly flexible and responsive ways of working, including working across the family unit; working intensively where required; working on an outreach basis (supported through provision of vehicles); and working with young people and families over the longer term. Design referral forms to assist adequate capture of whole-of-family information.
- Recognise specialisation and complexity of the work through appropriate caseloads, opportunities for community and sector engagement – such as sharing of evidence across different disciplines – and collaborative practice, as well as through the provision of clinical supervision and ongoing professional development.
- In naming programs, consider the impacts of language on young people’s and families’ willingness to engage, as well as the risk of stigmatising young people or non-protective parents withholding consent.
Understanding in practice:
Role of government
- Resource AVITH-focused interventions in ways which reflect the complexity and specialisation of the work and the need to work flexibly, on an outreach basis, over the long term and in client-led ways, factoring in appropriate caseloads and capacity for practitioner development. Brokerage will remain key, as will consideration around an equivalent to flexible support packages, albeit with appropriate eligibility criteria. Resourcing for dedicated AVITH respite options requires urgent attention.
- Support shared understanding and conceptualisations through development of sector guidance not only for risk assessment and management but for service delivery, as well as ongoing training and regular opportunities for sharing practice and evidence.
- Embed shared understanding across government and systems, including health and legal systems as well as community service sectors. Identify and advocate in areas where the operation of one system – such as the legal response – may be working against effective responses to AVITH. Develop and build on existing resources in other sectors – such as the “White Book” in primary health settings – to emphasise the need for all professionals supporting young people to keep the potential for an adult perpetrator and ongoing systems abuse in view.
Workforce
This pillar highlights the importance of a skilled and well-supported workforce to respond to families experiencing AVITH. This includes a recognition across the system that – due to the breadth of presenting needs of families experiencing AVITH – an “AVITH workforce” must comprise a specialist workforce capable of delivering targeted interventions and case management, as well as baseline capability across the wider service system to identify AVITH, refer appropriately, and work alongside specialist practitioners to support families and young people as required.
In thinking about a specialist workforce, practitioners participating in workshops consistently emphasised the breadth and complexity of work and the need for “specialisation within specialisation”. For example, practitioners described the significant differences in approach required to respond to children and young people in ways that are developmentally appropriate, as well as the layers of specialisation and capacity required to work with young people and families where specific needs such as complex disability, mental ill health, grief, intergenerational trauma or migration trauma featured. Given widely acknowledged workforce challenges in the specialist and wider community service sectors, this points to the need for governments at state and federal levels to invest in long-term workforce development strategies which can provide the foundation on which this highly specialised workforce can be built. This includes identifying relevant training andqualifications pathways, as well as fixing more appropriate remuneration levels and ongoing professional development opportunities.
Beyond working directly with young people, the research identified multiple examples of practitioners working with a protective parent (either as the primary client, or alongside direct work with the young person) in relation to their own recovery, as well as supporting their understanding of the impacts of their trauma experiences on parenting. The research also identified examples of highly sensitive work where adult perpetration of DFV continues to occur, including being attuned to the risk of systems abuse and ensuring that any engagement with an adult perpetrator is non-collusive.
Given the breadth and complexity of this work, practitioners emphasised the need for the specialist AVITH workforce to be empowered to work flexibly, including in relation to the nature, intensity and duration of support, all of which should be informed by family readiness and level of need. Program resourcing should also incorporate ample time for reflective practice and practice development.
Workforce in practice:
Role of practitioners
- Centre individual client needs and service readiness, identifying where secondary consultation with other services is sufficient or appropriate and where an AVITH specialist needs to take the lead in client engagement.
- Participate in collaborative practice networks and available training, advocating to employer organisations for appropriate clinical supervision and support. Draw on available practice guidance, service manuals and risk assessment and management tools. Ensure that referral forms and information about the service reflect family complexity and need.
- Identify opportunities for early intervention and shared positive experiences to stem the escalation of risk and need for crisis responses.
Workforce in practice:
Role of organisations
- Scope and resource AVITH programs to enable flexible and family-led ways of working, affording practitioners autonomy regarding the nature, intensity and duration of support delivered to young people and families. This includes resourcing outreach as a core function of practice and allocating caseloads that can mitigate vicarious trauma for staff.
- Ensure that AVITH-specific programs are well integrated with wider service offerings, with a view to facilitating secondary consultations and referrals, joint servicing of families (where appropriate), and opportunities for mutual capacity-building across programs.
- Put in place appropriate supervision and professional development arrangements which reflect the complexity and breadth of work being undertaken by specialist AVITH practitioners, including the need for AVITH practitioners to respond to multiple and often intersecting needs (both at the individual level and collectively across the family).
Workforce in practice:
Role of government
- When funding AVITH programs, ensure that resourcing includes consideration of non-client-facing work, including time for reflective practice and debriefing; coordination and engagement with other services working around the family; clinical supervision; and participation in key forums and practice networks. Resource programs over the longer term – with five years as the standard – to enable a sufficient and specialist workforce to be recruited, developed and retained.
- Identify the need for specialist roles across key components of the system – such as, for example, establishing dedicated AVITH Practice Leads across the Orange Door network in the Victorian context. Resource and recognise AVITH-focused roles as senior and highly specialised roles that provide a leadership function across the sector.
- Establish clear requirements relating to baseline capacity to identify and respond to AVITH across the wider family violence/DFV sector and related sectors, such as through the development of an AVITH-focused workforce development framework.
Coordination
This refers to the need for a network of services which can work in a coordinated way to respond to a family’s breadth of needs. Importantly, it positions “coordination” as a building block of “collaboration”, requiring clear structures, processes and mechanisms. Practitioners cautioned against an output-based understanding of coordination – such as the occurrence of a care team meeting – and emphasised the need to focus on the effectiveness and appropriateness of such mechanisms. This included by working towards models of care in which practice leads could support individual practitioners working with particular family members to hold the risk across the whole family in view.
Effective coordination requires (but is not limited to) ensuring that a care team meeting involves the right services, agencies and practitioners; that the role and expertise of each practitioner is well understood across the care team; and that there is a shared understanding across the care team of what success looks like (both individually and collectively) for the family unit. This includes a shared understanding of family readiness, with practitioners working together to sequence interventions appropriately and in a way that can maximise the benefits of engagement.
Coordination needs to be led by an appropriate service, with that service identified based on the family’s needs and existing service relationships, rather than adopting a one-size-fits-all approach to the structure and leadership of care team meetings or a similar mechanism. This may include consideration of which services have capacity to remain engaged over the longer term and undertaking a robust coordination risk management function, streamlining services interactions and reducing service overwhelm.
Where certain practitioners are not able to participate in care team meetings due to the nature of their roles (for example, legal practitioners and/or private practitioners who engage with family members on a sessional basis), strategies to support appropriate coordination and information sharing with these wider supports around the family should be adopted to ensure that all services working around a family have an adequate lens on risk and what is occurring for the family.
Coordination in practice:
Role of practitioners
- Support and empower families to co-chair care team meetings or other collaborative service forums with a trusted service, ensuring that the process is genuinely family-led and provides the family with an opportunity to articulate their goals; holds services accountable; and ensures that planning reflects family readiness.
- In establishing a care team or other collaborative mechanism around a family, identify the most appropriate service or agency to lead coordination, with consideration to be given to factors such as whether services have capacity to stay involved with the family over the longer term and what existing relationships of trust exist around the family. Invite additional agencies that may bring a missing lens.
- Work towards a “practice lead” approach in which a senior practitioner with a lens on the risk across the whole family can support and coordinate the work of individual practitioners, an approach which is distinct from individual clinical supervision.
- Where assuming the coordination role, follow up regularly with services about the tasks that they were set; facilitate information sharing where appropriate; and provide a liaison point for the family and/or young person. Lead by example, adopting a strengths-based approach in meetings where a family’s and/or young person’s achievements can be recognised, regardless of nature or scale, and where a young person’s wellbeing, as well as their behaviour, is the focus of collaborative effort. Share information, where appropriate, with other agencies, such as legal practitioners or private practitioners, who may not have care team participation as part of their practice remit.
Coordination in practice:
Role of organisations
- Ensure that program scope and resourcing accounts for work beyond direct therapeutic or case work interventions, including participation in care team meetings and other collaborative service forums. This includes, where relevant, resourcing programs to adopt a leadership and coordination role within care teams and other forums where appropriate.
- Actively build awareness of AVITH-specific programs across the organisation to facilitate appropriate referrals, secondary consultations, co-case management and other coordinated ways of working.
- Support opportunities to foster relationships with external organisations and agencies that can contribute to effective collaboration and information sharing, including at a management and leadership level.
Coordination in practice:
Role of government
- Resource AVITH-focused interventions in ways which acknowledge participation in collaborative mechanisms, including coordination activities such as information sharing, follow-up and liaison with clients.
- Develop guidance across the community sector workforce to articulate the obligations of practitioners working in collaborative forums and the opportunities for reducing risk that these provide. This may also include formal identification of opportunities for AVITH-focused roles to participate in other coordinated risk management mechanisms, such as Risk Assessment and Management Panels in the Victorian context.
- Resource associated collaborative mechanisms, such as Complex Care Teams in the Child Protection context, in ways that allow for service follow-through and leveraging of legislative imperatives.
Evidence
This pillar is concerned with the evolving nature of service system understanding of AVITH (and related service responses) and the need for this to be underpinned and informed by emerging evidence. This includes evidence relating to the needs, risk and experiences of young people and families, as well as emerging evidence of “what works” when responding to AVITH.
The research emphasised the need for practice roles to be resourced and supported to incorporate evidence and learning into daily practice. This includes through formal and informal opportunities for debriefing and reflective practice, as well as capacity to participate in collaborative practice networks so that learnings can be shared across sectoral and organisational boundaries.
Organisations similarly need to ensure that emerging AVITH responses are underpinned by effective processes for monitoring, evaluation and learning. This includes consideration of processes through which the voices of young people and families can inform service design, planning and continuous improvement. It also requires an agile approach to program design, implementation and delivery, with emerging evidence able to be progressively incorporated to strengthen program delivery over time.
This pillar also highlights the role of government in leading a system-wide approach to building and sharing evidence, piloting responses and taking effective interventions to scale. This includes resourcing for AVITH services to operate over a longer period of time (with five years as the standard); and investing in evaluations which can incorporate continuous learning and adopt an outcomes-focused (rather than output-focused) approach to evaluating effectiveness. Importantly, this pillar focuses on fostering continuous, critical interrogation, rather than simply the expansion of existing programs.
Evidence in practice:
Role of practitioners
- Engaging with evidence in the context of AVITH practice requires focus on evidence about the needs of young people and families, including the impacts of past or ongoing adult-perpetrated DFV and other forms of trauma (including intergenerational or migration trauma); evidence concerning child and adolescent brain development; evidence concerning disability and mental health; evidence concerning bullying and school disengagement; evidence around experiences of LGBTQA+ and intersex young people; evidence around non-collusive practice with adult perpetrators; and evidence about “what works” when supporting and connecting with young people, such as outreach and strengths-based activities.
- Participation in formal and informal opportunities for reflective practice is crucial, as is participation in clinical supervision and training, as well as wider community-of-practice forums.
- Opportunities for co-location with, or secondment to, other teams across an organisation may provide further learning and engagement with evidence in other areas or disciplines.
Evidence in practice:
Role of organisations
- Evidence-based service design and practice includes the provision of appropriate training and information across the multiple areas of practice relevant to AVITH responses, as noted above, and acknowledgement that reflective practice and clinical supervision are core to the work.
- Across organisations, including local or regional DFV networks, organisations can contribute to evidence development by sharing knowledge across different agencies and disciplines.
- Service evaluation, participation in research and provision of opportunities for client voices to inform service design are crucial to organisational roles in building and maintaining evidence. This may incorporate clear client feedback mechanisms, participation in research and/or the co-design of interventions with people with lived experience.
Evidence in practice:
Role of government
- Continuous improvement and critical interrogation of practice is key not only to ensure evidence-informed responses but to guard against “program drift”. Investment in an evidence base includes resourcing interventions over several years – with five years as the proposed standard – so that practice can be bedded down and comprehensive evaluation undertaken, including with a focus on outcomes and follow-up over time.
- Continuing to build the evidence base involves resourcing independent research and evaluation, while also acknowledging that participating in or facilitating these activities impacts service delivery/practitioner time. This should be recognised in program funding and associated caseloads, either through default inclusion in program funding or through allocated backfill resourcing for service participation when research or evaluations are commissioned.
- Government also plays a role in promoting and sharing evidence across the system and with other senior stakeholders. Senior departmental leaders working in areas focused on AVITH and DFV should seek opportunities to share evidence and exchange learnings with senior stakeholders in health, justice and other relevant settings.
Principles of collaborative practice
Alongside the four core pillars of collaborative practice, the research identified a set of principles which necessarily underpin all AVITH work, including collaborative responses, and which further emphasise the significant complexity and nuance of AVITH-focused work. Crucially, a principles-based approach to responding to AVITH can accommodate genuinely flexible and family-led work, as compared with more prescriptive approaches to defining AVITH responses, which may exclude some young people and families or fail to account for their breadth of needs.
Trauma and family violence risk–informed
This principle aims to ensure that practitioners and services working with young people and families experiencing AVITH adopt a holistic view of risk and use of violence. This involves maintaining a lens on the impacts of prior and current adult-perpetrated DFV on the young person, as well as wider family members in the home, including caregivers and siblings. This principle aims to flag to practitioners the need to consider the extent to which current and ongoing violence may be influencing behaviours and support needs in the home, as well as impacting the way in which young people present to the service system.
Crucially, this principle does not exclusively refer to trauma in a DFV context, but includes other forms of trauma, such as migration trauma, intergenerational trauma experienced by Aboriginal and Torres Strait Islander people, and trauma experienced at the hands of the system itself. Trauma of systems may include harm perpetrated by a legacy of colonisation, punitive government policies, and the intervention of statutory agencies such as Child Protection in the lives of people already experiencing multiple layers of disadvantage. In a different context, trauma of systems may result from negative service interactions, including histories of over-serviced and under-serviced families.
Principle in practice:
- Lead a practice shift away from blaming or deficit-based discourse towards a framework of understanding each young person and family as presenting with their own story and own unique set of experiences and challenges. Consider the starting point of “What has happened to you?” rather than “What is wrong with you?” Highlight factors of strengths and resilience to support recovery.
- Provide time and opportunity for caregivers who may be impacted by trauma to relate their experiences and validate their efforts to protect their children and support their family unit. Recognise that they may have reduced tolerance for their young people at different times.
- Maintain a lens on all relationships of violence in the home or in a young person’s wider life, including demonstrating commitment to keeping adult perpetrators in view. Failure to do so may exacerbate shame and confusion for young people where they are being held accountable for behaviours that have been used against them. Maintaining a lens on systems abuse also includes recognising potential levers of control attempting to be used by an adult perpetrator, including where they may withhold consent for a young person to engage with a service or undermine service engagement in other ways, or where an adult perpetrator may seek to dominate service engagement or leverage it for information. Consider how requests for consent are framed and avoid opportunities for collusion.
- Recognise that young people are at a development stage of identity formation which involves testing and negotiating how they interact with the world. Recognise that caregivers who have experienced adult-perpetrated DFV may present as traumatised, erratic, unable to regulate emotions, or unable to manage a young person’s behaviour constructively because of the ongoing impacts of trauma. Provide time and opportunity for their experiences to be heard and for them to be “seen as a person”.
Whole-of-family
This principle refers to a requirement for practitioners and services to consider needs and histories across the entire family structure when assessing and managing risk. Importantly, this principle does not refer to family therapy or interventions that require all members of the family to be present in the same room but, rather, refers to practitioners maintaining consideration of issues and needs as they exist across all members of the family, including grandparents, non-traditional caregivers and siblings. This is particularly important where there is systems abuse occurring in the young person’s life or multidirectional harm occurring within the home, but where the young person has been identified (or misidentified) by the system as the person using harm.
Across the framework development workshops, practitioners described the whole-of-family principle as speaking to the key role that relational work plays in any AVITH intervention. Relational work is particularly crucial when working with adolescents, who are in the process of identity formation, self-actualisation and, more broadly, navigating how they choose to function in relation to their wider world. Relational work is seen as crucial in supporting the young person’s recovery, including their recovery from negative experiences of the system itself.
Principle in practice
- Where it is safe (and the family is ready) to do so, working with multiple members of the family may include, for example, working with the young person in the context of their use of harm; working with a caregiver in relation to experiences of adult-perpetrated DFV, which may be impacting parenting skills and capabilities; and working with a sibling in relation to disability or mental health. Practical supports which can improve overall safety and family functioning should be remembered as a crucial component. Genograms (being a graphic representation of a family tree which includes detail about relationships and dynamics) can help to support understanding and identify what is important to young people, including pets and individual interests.
- Widening the service lens to incorporate each member of the family may result in an adult using violence, such as a father or stepfather, being brought into view. Using a whole-of-family lens may allow a practitioner to understand the function of the young person’s behaviour as motivated by fear, anxiety or confusion. Maintaining a lens on systems abuse or the way in which coercive control is still a presence across the family – whether or not in the home – can help to identify creative ways of helping a young person to engage with supports. Widening the service lens also includes consideration of broader experiences of family members, such as grief, loss, discrimination or intergenerational trauma, and how this may impact engagement or capacity to support a young person.
- Adopting a whole-of-family approach may involve only working with one or two members of a family while maintaining visibility of the ways in which the family’s experiences impact on those individuals. Considering family readiness is crucial, including maintaining opportunities for family members to exercise autonomy in how interventions are sequenced so as to maximise benefit from any service contact.
Addressing barriers to engagement
Particular challenges to engagement may exist for practitioners working with young people and families experiencing AVITH. These may stem from a family’s history of being significantly under-serviced or, conversely, over-serviced and immersed in service interaction, but without any constructive effect. Other barriers to engagement highlighted throughout the research include young people’s mistrust in a system that has not addressed their own experiences of harm, or which has compounded it through perceived breaches of confidentiality; which blame or minimise; or which inadvertently collude with an adult perpetrator. Further barriers include those at a systems and structural level, including the ongoing impacts of colonisation and various forms of discrimination, as well as the over-involvement of statutory authorities in the lives of some communities. In these instances, extensive reparation is required before any meaningful engagement can occur.
Principle in practice:
- Work flexibly and in a coordinated way while leveraging existing therapeutic relationships across the family. Service contact should be streamlined and appropriately scaffolded to reduce burden on the family and young person and allow them to be active participants in a process being conducted “with” them, rather than one that is happening “to” them.
- Creative approaches which mitigate service disengagement include outreach and engagement over the long term to build trust and rapport on a gradual basis. Examples may include attending a young person’s home each week for a cup of tea and a chat (either with the protective parent or the young person if they are willing); exploring a young person’s interests or hobbies and participating in these with them (without any associated expectation of “talk therapy”); or assisting the family or young person by driving the young person to an appointment or generally being a physical and practical form of support in a family’s life.
- Advocacy to other systems and authorities on behalf of the young person also plays a role, including providing the young person and family with information about their rights and how they can advocate constructively for themselves. Particular consideration of a young person’s or family member’s capacity to engage is also crucial given the prevalence of trauma, disability and neurodivergence among this cohort. For example, practitioners may incorporate considerations around light and sound sensitivity for young people with ASD, or the use of communication aids or greater reliance on visual methods of communication.
Flexible and needs-based
This principle centres the importance of practitioners providing a service response that is tailored to the individual needs and goals of young people and their families. Different AVITH presentations include where the function of the young person’s behaviour is connected with their disability and/or mental health, as well as where the young person’s behaviour should be more appropriately characterised as resistance to harm perpetrated by another member of the family. Responses must be flexible and ultimately adapted to the needs which the family identifies as most pressing at that time. Flexibility also enables practitioners to provide a response at times that reflect the individual readiness of each family member. Implicit in this principle is understanding that, in order for practitioners to provide flexible and needs-based responses, they must be appropriately skilled and appropriately supported by both the system and their organisation.
Principle in practice:
- Programs must be resourced to provide a variety of service offerings in order to respond to what works best for the individual family and young person. This includes practitioners providing outreach to attend the family home or to meet the young person in a setting in which they feel most comfortable, such as a skatepark, library or community hub, school, or café. Resourcing and programming needs to allow for multiple attempts through different modes of engagement, including outreach and virtual or in-office catch-ups, as well as the use of various creative tools to generate engagement.
- Program resourcing and design needs to allow for engagement with multiple family members where relevant, including by different practitioners in the team, or the provision of specific supports to address particular needs in the family which are not directly related to AVITH, but which can improve family functioning and reduce household stress overall. Crucially, this may include brokerage to support family members to access brief periods of respite, specialist assessments or particular equipment which may improve their general wellbeing (such as music or sporting equipment). It may also involve using brokerage to facilitate opportunities for shared positive experiences, such as family outings. The research found that this was particularly crucial in the context of family histories which had formed collective or individual identity around trauma and shame and require support to start to rebuild and repair attachments.
- “Follow-through”, “open-ended” and “sequencing” are crucial concepts, so that clients have time to develop confidence that a practitioner will act on their commitments, be led by a client’s preferences, and be available when that client is ready to engage.
Intersectional and culturally safe
This principle involves ensuring that practitioners and services are equipped to respond to the specific cultural considerations of families and the intersecting identities of young people experiencing AVITH. This principle centres the experiences of Aboriginal and Torres Strait Islander families, families from CALD backgrounds, and LGBTQA+ and intersex young people and families, as well as families with young people with disability. To ensure that AVITH services are culturally responsive and safe, services must develop relationships with and across organisations working with specific communities – not to silo the work but to foster collaboration, support continuous learning and, most importantly, provide clients with agency and choice in the services with which they interact. Services must also recognise that individual family members will have different experiences of marginalisation – and that sources of common experience may also be sources ofconflict in the family dynamic.
Principle in practice:
- Program design and practice require active consideration of the ways in which wider experiences and community context intersect with young people’s use of AVITH. The research found that this requires consideration of how a young person’s experience or background may mean that they live with intergenerational trauma or have been exposed to particular stigma and marginalisation – including exclusion from services, homophobia, biphobia or transphobia (whether internal or external to their family home), as well as profiling and discrimination by police. Experiences of discrimination may intersect with co-occurring mental health and/or disability needs which, together, place young people in an increased position of vulnerability. Marginalised status may also be a source of conflict or tension between family members who feel disempowered or have a lack of access to wider supports. It may also be leveraged by other family members inthe context of broader DFV.
- Culturally safe and responsive ways of working include an awareness of, and active engagement with, a client’s identity and the ways in which culture and community may impact their needs and experiences. Supporting a young person and their family from a CALD background, for example, may involve assisting the family to heal from trauma in relation to their experiences as asylum seekers or refugees. Assistance might involve supporting the family around visa status needs or assisting them to navigate the complex service system where English is their second language, as well as providing them with pragmatic supports.
- Working with an Aboriginal and/or Torres Strait Islander family might involve identifying appropriate community-led services with which to collaborate or which can lead the response, as well as bringing in the young person’s wider family and kinship networks, including by involving respected Elders and community members.
- Work with a sexuality, sex or gender diverse young person, meanwhile, may include considerations around their experiences of coming out or transitioning, how these have been supported in the family or school, and their access to wider social and community networks that can build a sense of inclusion and belonging.
- Most importantly, intersectional and culturally safe responses demand strengths-based approaches that affirm and celebrate a young person’s identity in all its forms at a time during which they are exploring and taking their place in their community and the wider world.
Service accountability
This principle seeks to highlight the importance of keeping the service sector accountable in the support being provided to the young person and family, rather than maintaining a focus purely on holding the young person accountable to the system. To do this, the roles, responsibilities and expertise of each practitioner or service involved must be well understood by all.
Principle in practice:
- Program resourcing, design and practice must be sufficient to allow for follow-through and follow-up. An accountable service is one that does what it says it will do. Services which are committed to working with the family should agree, plan for and progress their specific goals, as determined by the family. At the system level this includes proactive and transparent communication between services, with an overall focus on ensuring that dynamic risk information is shared and managed collectively.
- Service accountability is also about undoing the harm caused by previous service interactions. Necessary ingredients include role clarity, proactive communication and coordinated ways of working to assume shared responsibility across the system for identifying and managing risk. This includes where there exists current risk from adult-perpetrated DFV which may be identified by some – but not all – of the services involved with the family and advocating to these services about widening their gaze to where the most urgent source of risk really lies.
- Practitioners can commit to accountability as a means of minimising the exhaustion and overwhelm so often experienced by parents engaged with the AVITH service sector. When an incident occurs within the family, for example, practitioners may choose to engage proactively with another practitioner who is also involved with the family to obtain relevant information. This is to avoid a situation where their parents are retelling the story multiple times to multiple services.
Enablers of collaborative practice
Critical enablers of collaborative practice were consistently identified throughout the research. Where these enablers were not recognised or present within the system, practitioners observed that this functioned as a barrier and stymied efforts to work collaboratively. Practitioners similarly observed that, where these enablers have been established, they can provide an important foundation for collaborative practice moving forward. Dialogue between the pillars and enablers are where the responsibilities of government and organisations lie, supporting the principle-informed practice that lies in between. Engagement with multiple levels of the Framework is also how genuine collaboration across the system, rather than just across practice, can occur.
Enabler:
Funding
- Adequate and appropriate funding was identified throughout the research as a critical enabler of effective and collaborative practice. Governments should resource programs over longer periods, such as over five years, to enable development and retention of a suitably skilled workforce and to allow for programs to be properly embedded and evaluated. Funding for individual programs should reflect appropriate caseloads, accounting for the complexity and scope of AVITH-focused work, as well as the time required to engage in genuinely collaborative work across service boundaries – including, for example, where multiple services are working around a family to respond to individual and collective needs. They should also provide for outreach as a core function, for clinical supervision and sector engagement and provision of brokerage and pragmatic support. Funding structures should be outcome-focused, rather than being focused onthrough-put, and should allow for long-term and intensive work where this is required.
Enabler:
Culture
- While the research highlighted the need for clear structures and processes to support coordinated and collaborative responses, a culture of collaboration emerged as equally crucial. Where practitioners or services have a narrow view of their role and accountabilities – rather than seeing themselves as simply one part of a broader response – this can undermine the potential for meaningful collaboration around the family.
Organisations should actively foster a culture of collaboration within and across organisational boundaries. This includes signalling to practitioners that it is valuable to invest time and effort in establishing and maintaining collaborative ways of working. Equally, organisations must embed recognition that identifying and responding to AVITH is a shared responsibility and that families may present to (or require support from) a range of programs, not simply those with an explicit AVITH focus. Government at local, state and federal levels has an opportunity to foster a culture of collaboration to support development of AVITH practice, recognising and valuing it as a specialisation and communicating its values to other sectors and systems. It can also support this by facilitating the provision of service information across sectors.
Enabler:
Continuous learning
- Given the emerging nature of understandings of AVITH (and related service responses), a commitment to continuous learning at the practitioner, organisational and system levels is critical. This includes creating opportunities for and valuing reflective practice, as well as opportunities for shared learning within and across programs and organisations – such as providing presentations around different areas of expertise and engaging in collaborative practice discussions around case studies.
Opportunities for continuous learning also interact with the principle of intersectional and culturally safe responses, with an imperative on all AVITH-focused services (and the governments and organisations which resource them) to develop relationships with organisations which work with specific cohorts and communities, fostering windows for ongoing practice development, secondary consultations and safer and more supported responses for young people and families.
Enabler:
Evidence-informed tools
- The requirement to use tools, practice guidance and frameworks that do not account for the complexity and breadth of AVITH presentations can function as a barrier to collaborative responses to AVITH. Conversely, the availability of relevant and appropriate tools can foster a shared language and understanding among practitioners, as well as supporting a structured approach to identifying and managing risk within families experiencing AVITH.
Tools which seek to adopt language and frames which reflect understandings of adult-perpetrated DFV were universally seen by AVITH practitioners participating in the research as being unsuitable and potentially harmful when working with families experiencing AVITH. Tools developed to support AVITH-focused work should instead be strengths-based and avoid stigmatisation of young people, siblings and protective parents, with capacity to recognise, assess and work with complex risk dynamics within families. This includes families in which there have been (or continue to be) experiences of adult-perpetrated violence, as well as the presence of multidirectional violence.
Enabler:
Service capacity
- The ability to work flexibly and responsively, including the capacity to work with families long-term and intensively where required, is contingent on appropriate caseloads within AVITH-specific services. At the same time, it is important that all families experiencing AVITH (or identified as being at risk of experiencing AVITH) are able to access a timely service response to prevent the escalation of risk.
It is therefore crucial for government to maintain a lens on the capacity of AVITH-specific services, as well as wider services which can provide early intervention where AVITH risk is identified, in order to meet demand. This includes monitoring where specific crises, such as the COVID-19 pandemic, contribute to increased risk, as well as monitoring longer term trends in demand. Importantly, government should work closely with those organisations with specific expertise in delivering AVITH interventions to ensure that additional resourcing and scaling up of service capacity is implemented in a way which is supported and sustainable for the sector, and leverages program infrastructure and existing expertise.
Enabler:
System stewardship
- A clear role exists for government in fostering an AVITH system response which is founded on a shared understanding of the nature and dynamics of AVITH; appropriate ways of responding; and the outcomes which a meaningful AVITH system response should be working to achieve. In particular, the multi-system nature of the “AVITH system” – which draws on the community-based service system, as well as legal, education, Child Protection and welfare systems – requires government to remove barriers to collaboration within and across systems and to facilitate opportunities for shared learning and reflection. This includes identifying where responses within one component of the AVITH system (such as the legal process) can act to undermine or counteract wider system responses aimed at family resilience, safety and (where appropriate) repair.
System stewardship also includes the accumulation and provision of information across different sectors which can support more effective practice. This includes, for example, the provision of information about AVITH-focused services to the legal system or working with legal system players to support information provision across areas to support more informed decision-making. It also includes placing greater emphasis on gathering information about what happens to young people when the tertiary end of the system intervenes, such as when they are removed from the home or present to emergency departments.
Importantly, system stewardship approaches involve government working alongside organisations and agencies, leveraging their expertise and working to steer the system towards key outcomes. This can occur at the system level, as well as through the adoption of place-based approaches and local service networks which can deliver holistic, tailored responses to families experiencing AVITH within their communities.
The discussion included above is also reflected in a more detailed representation of the Collaborative Practice Framework (Appendix A).
Discussion
The WRAP around families project was designed to be a targeted investigation into the service response to AVITH as a direct follow-up, or “coda”, to a recommendation from the PIPA project. As such, it had limited resourcing and was expected to be conducted as a brief inquiry, or stocktake, into the extent to which service responses had progressed since the PIPA project, as well as to provide support through a practice framework which could help to accelerate this progress further.
The impacts of COVID-19, however, had flow-on effects for the project which expanded both its timeframes and scale on the one hand, while limiting its scope on the other. The swift injection of funding from the Victorian Government in early 2021 – which came after the study’s initial design and in response to a recognised increase in AVITH during COVID-19-related lockdowns in 2020 – resulted in more practitioners working in the field, but with far less guidance than the pre-existing workforce. These practitioners were also in the position of establishing and running new programs while working primarily from home as Victoria returned to extended lockdown through the second half of 2021. This extended lockdown period, the increasing vulnerability of clients without service visibility, and an emphasis on responding to clients’ material needs ultimately meant that some services were simply not able to engage in the research, while also finding it difficultto build rapport with young clients.
Combined, these impacts meant that a project which was originally designed to be short, sharp and completed by the end of 2021 extended well into 2022 as sufficient time was allowed for practitioners from ACCOs to participate and for the DS program to continue to attempt client recruitment for the case study component. Ultimately, this meant that the research data involved contributions from a far greater number of practitioners than originally anticipated, but a smaller number of clients.
Despite these challenges, however, the findings and Framework resulting from the research potentially come at a more salient time than would have otherwise been the case. While policymakers and practitioners in Victoria were focused on surviving the state’s lockdowns and the ongoing impacts of multiple Omicron-variant waves throughout 2022, investment in a service model of care, the pending release of a practice guide to support risk assessment and management, and the development of training by the CFECFW will position policymakers and practitioners well to be able to consider next steps. This is important because, as practitioners contributing to the refinement of the Collaborative Practice Framework proposed above explained, “We have made some important progress, but the Framework is the ‘where to from here’.”
The Framework proposed by the research team is offered in lieu of a list of specific research recommendations around service provision for a number of reasons. The first is that the service landscape in jurisdictions around Australia (and internationally) differs so greatly that recommendations around specific service reform would not necessarily be useful beyond Victoria. The second is the clear indication from practitioner descriptions of their practice for the need to avoid prescriptive approaches, with the Framework designed to be adopted and applied in different contexts.
The third is that practice in this area involves such nuance and complexity that the Framework pushes policymakers towards considering this practice as a whole, rather than defaulting to acquittal of one recommendation in isolation from another, as the FVRIM has rightly identified too often occurs (FVRIM, 2021). That said, the practice examples nominated as part of the Framework are included to encourage practitioners and policymakers alike to consider how it can support reform in their particular environment. Practitioners, organisations and policymakers are therefore urged to engage with the Framework; to identify where their particular responsibilities lie within it; and how it could help them to move towards evidence-informed and genuinely collaborative responses, wherever they are on the service reform journey.
Assumptions challenged by the research
Several assumptions underpinned the project’s original design, which are important to identify here. This includes an assumption that longer term interventions – and interventions which worked with multiple family members – were increasingly viewed as the service standard. The research design was also driven by an assumption that collaboration was relatively achievable where sufficient practitioner will and interest existed. In particular, the research team were aware of the wider use of care teams and similar structures which bring together different disciplines around a young person or a family. Accordingly, the research team anticipated that these would be a potential source of support. The expectation of the research was also that collaboration could be just as easily achieved across a wider service network as it could within an organisation. While all the participants involved in the focus groups agreed with these imperatives and the basis ofthese assumptions, the research indicated that system recognition, capacity and, perhaps most relevantly, maturity were somewhat further behind.
Finally – and perhaps most importantly – the research was designed on the assumption that trauma in caregivers and young people from adult-perpetrated DFV was a significant driving factor in the use of AVITH, as well as in reduced capacity of caregivers to manage the impacts of this behaviour and address their own support needs while responding to their child’s. This was a strong finding from the PIPA project and is also increasingly emphasised in literature which highlights the gendered nature of AVITH victimisation and the importance of repairing ruptured relationships between mothers and children (Burck, 2021).
While the research team was well aware that this trauma can include current adult-perpetrated DFV, including through leveraging the legal system response as identified by the PIPA project (Campbell et al., 2020), what was perhaps underestimated was the sheer extent to which this ongoing coercive control and systems abuse were such a significant feature of practice contexts and, arguably, the predominant factor in many clients’ lives. Certainly, while only illustrative given the small sample size, the overwhelming narrative of the three interviews with mothers, as well as on the case files, was the way in which DFV from a former partner was continuing to impact almost every aspect of the mothers’ and children’s lives, including more than a decade after separation. This echoed the suggestion in the PIPA project that a system focus on young people using harm was often missing the “original perpetrator,” who remainedout of view of the system (Campbell et al., 2020, p. 132) but who continued to be the source of real harm across the family.
Some practitioners across the research suggest that this limited lens on the impacts of adult-perpetrated DFV on children and young people – and the extraordinary lengths to which some perpetrator parents, predominantly fathers in the context of these research findings, will go to control their children’s lives – may have something to do with the community’s wider discomfort with its collective failure to protect children and young people in the first place.
Where it becomes dangerous is [practitioners not] … noticing what’s going on, actually leaning into that rather than avoiding it like the plague … As a community we don’t want to know about trauma, we don’t wanna know that kids are treated this way. I think fundamentally what sits under a lot of it is “Why is our system so crap at looking after these kids?” Because, you know, we are a fairly affluent society that doesn’t want to believe that kids get kicked and cigarette burned and, you know, everything else that happens. (Practitioner 38)
Listen to the people who are working with this child. That’s what gets me in the heart about all this … We can talk about practice issues, policy issues, whatever, but there is a child that is telling you that they’re unsafe and you’re not giving them the benefit of the doubt … (Practitioner 49)
This finding around the dominating presence of current adult-perpetrated DFV is important because it further confirms where practice and service attention in this area should be directed – whether at the point of:
- early intervention in terms of an emphasis on supporting recovery for women and children escaping violence
- therapeutic responses for young people who use violence at home, rather than punitive responses which push them by default onto a criminal justice trajectory
- statutory authority involvement, which maintains a lens on where the real source of risk to children may lie.
Just as crucially, it suggests a genuine prevention opportunity with respect to AVITH, where service systems can intervene early to support mothers and children to recover and to form new, positive family identities, rather than “waiting until there’s a crisis” (Practitioner 72) or when it’s simply “ten years too late” (Campbell et al., 2020, p. 154).
Limitations of the research
The research had other key limitations which should be acknowledged. The first was the substantial and ongoing impacts of COVID-19 on the DS program, which made engagement with clients – and associated recruitment to the interviews, in particular – a considerable challenge. Accordingly, the interviews with parents highlighted more about the limitations of prior service engagement and the ongoing impacts of adult-perpetrated DFV than they did about engagement with the DS program to an extent. That said, parents did identify what they saw as being beneficial in terms of the support that they had received from the program, as well as what they think that young people require from a service under more stable service delivery circumstances.
Other limitations include the absence of Child Protection practitioner or Victoria Police contributions (although Victoria Police contributed significantly to the PIPA project), also largely attributable to the demands of the pandemic, as well as to the targeted scope of the project itself. A further potential limitation is the lack of contribution from private practitioners, such as psychologists, which was similarly acknowledged as a gap by the practitioners across the focus groups in terms of the effectiveness of care teams. To note, psychologists and other practitioners providing services on a fee-for-service basis may be less likely to see clients who have been immersed in service system involvement or “over-serviced” and, in turn, clients who are less likely to report – or at least disclose – histories of trauma (Gallagher, 2016). As the PIPA project found, however, this does not prevent these families from presenting to the legal system (asopposed to the community-based service system), including in the context of young people who are identified as using AVITH while being victims and survivors of adult-perpetrated emotional and psychological abuse (Campbell et al., 2020).
Additionally important to acknowledge is the extent to which the circumstances of COVID-19 lockdowns may have been contributing to an escalation in the challenges that practitioners were experiencing, given the recognised associated increase in AVITH during this time. This potentially means that practitioners were seeing a “net widening” in the types of matters to which they were responding, or an entrenched complexity in clients which contributed to increased demand.
This increased demand was actually anticipated by the research team to be emphasised in practitioner contributions to the focus group discussions, given that the rise in the number of families experiencing AVITH – co-occurring with young people’s and parents’ deteriorating mental health during repeated lockdowns – had been a finding of earlier work by members of the research team (Campbell & McCann, 2020; Drummond Street Services, 2020). Important to note, however, is that the primary concerns of participating practitioners related to system and policy settings which pre-dated the pandemic, but which they feared would be compounded by a lack of government resourcing in human services sectors in the future as a result of the pandemic and its impacts.
Implications for policy and practice
Practitioners in the focus group discussions were concerned that pre-existing system challenges had not only been compounded by the pandemic but would also be less likely to be addressed given the pandemic’s drain on public resources. This practitioner concern is therefore a key consideration for policymakers as they move towards future service design and investment –whether it is fiscally responsible to constrain service funding in the short term when client needs and complexity are likely to have been further entrenched, as international research suggests (Condry et al., 2020), and an exhausted workforce is depleted. Rather, the WRAP around families research points to the need for, as Condry and colleagues (2020) described it, a “safeguarding surge”, including greater support for families and young people at an earlier point. Most significantly, this involves providing support for women and children as soon as they are identified as experiencing, oras having experienced, adult-perpetrated DFV. This includes recognising children and young people as victims and survivors in their own right, including in early childhood. Crucially, this also includes avoiding any assumptions that a child or young person is no longer at risk or experiencing ongoing impacts of the harm, despite the original perpetrator remaining out of view. Equally this research echoes the PIPA project and other research which points to the substantial need for greater support for families with a young person with disability and who may become vulnerable to a family violence system response as a result of associated behaviour.
Investment in earlier intervention also represents an opportunity for prevention of AVITH and escalation of any risk for families, as noted above. This requires a commitment from government at both state and federal levels to resource services sufficiently to allocate time and attention to families who have not yet reached crisis. It also requires a commitment from government at these levels to invest in the long-term development of an appropriate workforce, as noted above.
Where the system fails to intervene earlier, however, the WRAP around families project offers a blueprint to support a genuinely collaborative and consistent framework for service responses to AVITH. In doing so it signals that the nuance, flexibility and complexity which are so clearly required in the practice may mean that current approaches to service funding should be re-examined and a genuine investment in longer term and meaningful results instead brought to the fore.
… commitment to a kind of long-standing program that could be evaluated over a five-year period rather than just, you know, 12 months … so it can really be evaluated and developed …. It’s a very specialist area and I think it worthy of a really specialist, nuanced approach to the work. It’s still sort of in its infancy to a large extent. (Practitioner 16)
Directions for future research
The findings from the WRAP around families project highlight significant scope for future research in the area of collaborative service responses to AVITH. Rather than being able to describe different versions of embedded collaboration as anticipated, the research team concluded that the study was attempting to address a bigger research and practice gap than anticipated. Significant opportunities therefore exist for future research which can explore the potential adoption of resulting collaborative approaches, including the Framework proposed by this research, across the service system. This includes at an organisational as well as a multi-agency level.
More specifically, although the research team was not ultimately able to speak to young people, the findings overall suggested that the needs of children and young people grappling with the wider impacts of a sibling using violence confirms this as a direction for future research. In addition, the research suggested that the relationship of wider adverse childhood experiences to the use of AVITH – including, in particular, bullying victimisation and familial grief – should be an area of future research attention.
Given that challenges – and opportunities for more effective collaboration – were volunteered by practitioners across the research regarding Child Protection involvement in families’ lives, this is also a clear area of need for future research focus. The PIPA project recommended the development of a specific AVITH focus and framework within Child Protection authorities and, accordingly, relevant senior stakeholders were also invited to test the findings from practitioner focus groups but did not take up the invitation. Dedicated research exploring how Child Protection practitioners can engage with their statutory obligations in the context of AVITH – including collaborating effectively and consistently with other services – should therefore be explored, potentially in the context of broader work around improvements in Child Protection authorities’ capacity to identify and respond to adult perpetration.
Crucially, the relationship of current, as well as prior, experiences of adult-perpetrated DFV in the context of AVITH should be a significant focus of future research. This requires pushing the focus of research attention beyond the default in literature and policy environments alike to describe the relationship of trauma to the use of AVITH as predominantly a historical one. Given that a failure to identify current risk from adult-perpetrated violence may result, in part, from the lack of young people’s voices contributing to research, directions for future research must include, most importantly of all, opportunities for young people to share their experiences safely and in their own words.
I hope that we can get to the point where the work that we do with young people and their families is resourced in a manner that removes the stigma and the shame and the guilt that sits alongside it … For me, that’s the key to having real change. (Practitioner 19)
Let’s all just come together and know that if we don’t get it right with them, they’re not going to turn into well-rounded, high-achieving adults, we’re further damaging them. And it’s only going to come back on us as a community. (Practitioner 49)
As one practitioner remarked, developing appropriate and effective responses to AVITH – and, ideally, preventing it in the first place – “is a forever journey” (Practitioner 24), something in which all systems will continue to be engaged and challenged as they learn, respond and evolve.
References
Armstrong, G., Cain, C., Wylie, L., Muftić, L., & Bouffard, L. (2018). Risk factor profile of youth incarcerated for child to parent violence: A nationally representative sample. Journal of Criminal Justice, 58, 1–9. https://doi.org/10.1016/j.jcrimjus.2018.06.002
Armstrong, G. S., Muftic, L. R., & Bouffard, L. A. (2021). Factors influencing law enforcement responses to child to parent violence. Journal of Interpersonal Violence, 36(9–10), 4979–4997.
https://doi.org/10.1177/0886260518794510
Australian Domestic and Family Violence Death Review Network, & Australia’s National Research Organisation for Women’s Safety. (2022). Australian Domestic and Family Violence Death Review Network Data Report: Intimate partner violence homicides 2010–2018 (2nd ed.; Research report, 03/2022). ANROWS. https://www.anrows.org.au/publication/australian-domestic-and-family-violence-death-review-network-data-report-intimate-partner-violence-homicides-2010-2018/read/
Bagshaw, D., Brown, T., Wendt, S., Campbell, A., McInnes, E., Tinning, B., Batagol, B., Sifris, A., Tyson, D., Baker, J., & Fernandez Arias, P. (2011). The effect of family violence on post-separation parenting arrangements: The experiences of children and adults from families who separated post 1995 and post 2006. Family Matters, 86, 49–61.
Beckmann, L. (2020). Exposure to family violence and adolescent aggression in multiple social contexts: Classroom social resources as moderators. Journal of Family Violence, 35(5), 471–484.
Beckmann, L., Bergmann, M., Fischer, F., & Mößle, T. (2021). Risk and Protective Factors of Child-to-Parent Violence: A Comparison Between Physical and Verbal Aggression. Journal of Interpersonal Violence, 36(3–4), NP1309–1334NP. https://doi.org/10.1177/088626051774612
Belzile, J. A., & Öberg, G. (2012). Where to begin? Grappling with how to use participant interaction in focus group design. Qualitative Research, 12(4), 459–472.
Blakemore, T., Rak, L., Agllias, K., Mallett, X., & McCarthy S. (2018) ‘Understandings of youth perpetrated interpersonal violence among service providers in regional Australia’ Journal of Applied Youth Studies, 2(5), 53–69.
Boxall, H., & Morgan, A. (2020). Repeat domestic and family violence among young people (Trends and Issues in Crime and Criminal justice no. 591). Australian Institute of Criminology https://www.aic.gov.au/sites/default/files/2020-05/ti591_repeat_domestic_and_family_violence_among_young_people.pdf
Boxall, H., Morgan, A., & Brown, R. (2020). The prevalence of domestic violence among women during the COVID-19 pandemic (Statistical Bulletin no. 28). Australian Institute of Criminology.
https://www.aic.gov.au/sites/default/files/2020-07/sb28_prevalence_of_domestic_violence_among_women_during_covid-19_pandemic.pdf
Boxall, H., Morgan, A., Voce, I., & Coughlan, M. (2020). Responding to adolescent family violence: Findings from an impact evaluation (Trends and Issues in Crime and Criminal Justice no. 601). Australian Institute of Criminology. https://www.aic.gov.au/sites/default/files/2020-09/ti601_responding_to_adolescent_family_violence.pdf
Breckenridge, J., & Hamer, J. (2014). Traversing the maze of “evidence” and “best practice” in domestic and family violence service provision in Australia (Issues paper no. 26). Australian Domestic and Family Violence Clearinghouse.
Breman, R., MacRae, A., & Vicary, D. (2018). Child-perpetrated family violence in kinship care in Victoria. Children Australia, 43(3), 2018, 192–197. https://doi.org/10.3316/agispt.20181107003585
Brown, T. C. (2006). Child abuse and domestic violence in the context of parental separation and divorce: New models of intervention. In C. Humphreys & N. Stanley (eds.), Domestic violence and child protection (pp. 155–168). Jessica Kingsley Publishers.
Burck, D. (2021) Adolescent-to-parent violence and the promise of attachment-based interventions. In K. Fitz-Gibbon, H. Douglas & J. Maher (eds.), Young people using family violence: International perspectives on research, responses and reforms (pp. 55–68). Springer.
Burck, D., Walsh, D., & Lynch, D. (2019). Silenced mothers: Exploring definitions of adolescent-to-parent violence and implications for practice. Advances in Social Work and Welfare Education, 21(1), 7–18.
https://doi.org/10.1177/15248380211053618
Campbell, E. (2021) Missing the mark: The problem of applying a “one size fits all” standard legal response to adolescent family violence perpetration. In K. Fitz-Gibbon, H. Douglas & J. Maher (eds.), Young people using family violence: international perspectives on research, responses and reforms (pp. 87–106). Springer.
Campbell, E., & McCann, B. (2020). Behind closed doors: Adolescent violence in the home (AVITH) during COVID & challenges to come. Centre for Innovative Justice, RMIT University, Centre for Family Research & Evaluation, & Drummond Street Services.
Campbell, E., Richter, J., Howard, J., & Cockburn, H. (2020). The PIPA project: Positive interventions for perpetrators of adolescent violence in the home (AVITH) (Research report, 04/2020). ANROWS.
https://www.anrows.org.au/publication/the-pipa-project-positive-interventions-for-perpetrators-of-adolescent-violence-in-the-home-avith/
Cardenas, M. C., Bustos, S. S., & Chakraborty, R. (2020). A “parallel pandemic”: The psychosocial burden of COVID-19 in children and adolescents. Acta Paediatrica, 109(11), 2187–2188.
https://doi.org/10.1111/apa.15536
Centre for Innovative Justice. (2022). Evaluation of the pre-court support for adolescents using violence in the home (AVITH) pilot: Final evaluation report. RMIT University.
Centre for Justice Innovation. (2021). Break4Change. Retrieved June 9, 2021, from
https://justiceinnovation.org/project/break4change
Condry, R., & Miles, C. (2021). Children who perpetrate family violence are still children: Understanding and responding to adolescent to parent violence. In K. Fitz-Gibbon, H. Douglas & J. Maher (eds.), Young people using family violence: international perspectives on research, responses and reforms (pp. 1–18). Springer.
Condry, R., Miles, C., Brunton-Douglas, T., & Oladapo, A. (2020). Experiences of child and adolescent to parent violence in the Covid-19 pandemic. University of Oxford.
https://www.law.ox.ac.uk/sites/files/oxlaw/final_report_capv_in_covid-19_aug20.pdf
Contreras, L., Bustos-Navarrete, C., & Cano-Lozano, M. (2019). Child-to-parent violence questionnaire (CPV-Q): Validation among Spanish adolescents. International Journal of Clinical and Health Psychology, 19, 67–74. https://doi.org/10.1016/j.ijchp.2018.09.001
Contreras, L., & del Carmen Cano, M. (2016). Child-to-parent violence: The role of exposure to violence and its relationship to social-cognitive processing. European Journal of Psychology Applied to Legal Context, 8(2), 43. https://doi.org/10.1016/j.ejpal.2016.03.003
Contreras, L., León, S., & Cano-Lozano, M. (٢٠٢٠). Assessing child-to-parent violence with the child-to-parent violence questionnaire, parents’ version (CPV-Q-P): Factor structure, prevalence, and reasons. Frontiers in Psychology, 11, 604956. https://doi.org/10.3389/fpsyg.2020.604956
Coogan, D. (2016). Listening to the voices of practitioners who encounter child to parent violence and abuse: Some findings from an action research project. Irish Social Worker Journal (Winter), 41–48.
Coogan, D. (2018). Child to parent violence and abuse: Family interventions with non-violent resistance. Jessica Kingsley Publishers.
Cottrell, B. (2001). Parent abuse: The abuse of parents by their teenage children. Health Canada, Population and Public Health Branch, National Clearinghouse on Family Violence.
Coutts, P. (2019). The many shades of co-produced evidence. Carnegie UK Trust.
Crime Statistics Agency. (2020). Victoria Police July 2015–June 2020. Retrieved May 5, 2021, from
https://www.crimestatistics.vic.gov.au/family-violence-data-portal/download-data-tables
Docherty, M., Kubik, J., Herrera, C., & Boxer, P. (2018). Early maltreatment is associated with greater risk of conduct problems and lack of guilt in adolescence. Child Abuse & Neglect, 79, 173–182.
Douglas, H., & Walsh, T. (2022). Adolescent family and dating violence and the criminal law response. Journal of Family Violence, 38, 287–299. https://doi.org/10.1007/s10896-022-00373-x
Drummond Street Services. (2020). Evaluating the impacts of COVID-19 and drummond street’s response (COVID-19 Response Edition 1). https://ds.org.au/wp-content/uploads/2020/10/COVID-19-Staff-report-Edition-1-public.pdf
Elliott, K., McGowan, J., Benier, K., Maher, J., & Fitz-Gibbon, K. (2017). Investigating adolescent family violence: Background, research and directions: Context report. Monash University.
https://www.monash.edu/__data/assets/pdf_file/0007/1532275/investigating-adolescent-family-violence-background-research-and-directions.pdf
Espejo-Siles, R., Zych, I., Farrington, D. P., & Llorent, V. J. (2020). Moral disengagement, victimization, empathy, social and emotional competencies as predictors of violence in children and adolescents. Children and Youth Services Review, 118, 105337.
https://psycnet.apa.org/doi/10.1016/j.childyouth.2020.105337
Fagan, A. A. (2020). Child maltreatment and aggressive behaviors in early adolescence: Evidence of moderation by parent/child relationship quality. Child Maltreatment, 25(2), 182–191.
Family Violence Protection Act 2008 (Vic).
http:// www5.austlii.edu.au/au/legis/vic/consol_act/fvpa2008283/
Family Violence Reform Implementation Monitor. (2021a). Report of the Family Violence Reform Implementation Monitor. Victorian Government. https://www.fvrim.vic.gov.au/report-family-violence-reform-implementation-monitor-1-november-2020
Family Violence Reform Implementation Monitor. (2021b). Accurate identification of the predominant aggressor. Victorian Government. https://www.fvrim.vic.gov.au/monitoring-victorias-family-violence-reforms-accurate-identification-predominant-aggressor
Fisher, J. R., Tran, T. D., Hammargerg, K., Sastry, J., Nguyen, H., Rowe, H., Popplestone, S., Stocker, R., Stubber, C., & Kirkman, M. (2020). Mental health of people in Australia in the first month of COVID-19 restrictions: A national survey. Medical Journal of Australia, 213(10), 458–464.
https://doi.org/10.5694/mja2.50831
Fitz-Gibbon, K., Elliott, K., & Maher, J. (2018). Investigating adolescent family violence in Victoria: Understanding experiences and practitioner perspectives. Monash University.
https://researchmgt.monash.edu/ws/portalfiles/portal/250376810/Adolescent_Family_Violence_in_Victoria_Final_Report.pdf
Fitz-Gibbon, K., Maher, J., & Elliott, K. (2021). Barriers to help seeking for women victims of adolescent family violence: A Victorian (Australian) case study. In K. Fitz-Gibbon, H. Douglas, & J. Maher (eds.), Young people using family violence: international perspectives on research, responses and reforms (pp. 39–54). Springer.
Fitz-Gibbon, K., Meyer, S., Maher, J., & Roberts, S. (2022). Adolescent family violence in Australia: A national study of prevalence, history of childhood victimisation and impacts (Research report, 15/2022). ANROWS. https://www.anrows.org.au/publication/adolescent-family-violence-in-australia-a-national-study-of-prevalence-history-of-childhood-victimisation-and-impacts/
Flyvberg, B. (2006). Five misunderstandings about case study research. Qualitative Inquiry, 12(2), 219–245. https://doi.org/10.1177/1077800405284363
Fraser, N. (1985). What’s critical about critical theory? The case of Habermas and gender. New German Critique, 35, 97–131. https://doi.org/10.2307/488202
Gair, S., Zuchowski, I., Thorpe, R., Henderson, D., & Munns, L. (2019). “In the firing line”: Grandparent carers at risk of family violence. Journal of Family Violence, 34(4), 321–329.
Gallagher, E. (2016) The “Who’s in Charge” program. In A. Holt (ed.), Working with adolescent violence towards parents: Approaches and contexts for intervention (pp. 34–46). Routledge.
Gallego, R., Novo, M., Farina, F., & Arce, R. (2019). Child-to-parent violence and parent-to-child violence: A meta-analytic review. European Journal of Psychology Applied to Legal Context, 11(2), 51–59. https://doi.org/10.5093/ejpalc2019a4
Gerring, John. (2004). What is a case study and what is it good for? American Political Science Review, 98(2), 341–354.
Gilman, A. B., & Walker, S. C. (2020). Evaluating the effects of an adolescent family violence intervention program on recidivism among court-involved youth. Journal of Family Violence, 35(2), 95–106. https://doi.org/10.1007/s10896-019-00070-2
Hernández, A., Martín, A., Hess-Medler, S., & García-García, J. (2020). What goes on in this house does not stay in this house: Family variables related to adolescent-to-parent offenses. Frontiers in Psychology, 11, 581761.
Holt, A. (2013). Adolescent-to-parent-abuse: Current understandings in research, policy and practice. Policy Press. https://doi.org/10.2307/j.ctt1t6p748
Holt, A. (ed.). (2016). Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention. Routledge.
Holt, A., & Birchall, J. (2020). Investigating experiences of violence towards grandparents in a kinship care context: Project summary. University of Roehampton, London.
https://helenbonnick.files.wordpress.com/2020/05/violenceagainstgrandparents_projectsummary_may2020.pdf
Holt, A., & Retford, S. (2013). Practitioner accounts of responding to parent abuse: A case study in ad hoc delivery, perverse outcomes and a policy silence. Child and Family Social Work, 18, 365,
https://doi.org/10.1111/j.1365-2206.2012.00860.x .
Holt, A., & Shan, P. C. (2018). Exploring fatal and non-fatal violence against parents: Challenging the orthodoxy of abused adolescent perpetrators. Journal of Offender Therapy and Comparative Criminology, 62(4), 915–934. https://doi.org/10.1177/0306624X16672444
Howard, J., & Holt, A. (2015). Special considerations when working with adolescent family violence. In A. Holt (ed.), Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention. Taylor & Francis Group.
Ibabe, I,. Jaureguizar, J., & Bentler, P. (2013). Risk factors for child-to-parent violence. Journal of Family Violence, 28, 523. http://dx.doi.org/10.1007/s10896-013-9512-2
Jouriles, E. N., Gower, T., Rancher, C., Johnson, E., Jackson, M. L., & McDonald, R. (2021). Families seeking services for sexual abuse: Intimate partner violence, mothers’ psychological distress, and mother–adolescent conflict. Journal of Family Psychology, 35(1), 103.
https://psycnet.apa.org/doi/10.1037/fam0000798
Katz, E. (2019). Coercive control, domestic violence and a five-factor framework: Five factors that influence closeness, distance and strain in mother–child relationships. Violence Against Women, 25(15), 1829–1853. https://doi.org/10.1177/1077801218824998
Kehoe, M., Ott, N., & Hopkins, L. (2020). Responding to adolescent violence in the home: A community mental health approach. Australian and New Zealand Journal of Family Therapy, 41, 342–354.
https://doi.org/10.1002/anzf.1432
Kickett, G., Chandran, S., & Mitchell, J. (2019). Woon-yah Ngullah Goorlanggass – Caring for our children: A culturally strong, therapeutic kinship care for Aboriginal children, young people and their families. Developing Practice: The Child, Youth and Family Work Journal, 52, 25–39.
https://doi.org/10.3316/informit.852240543758477
Kwong, M., Bartholomew, K., Henderson, A., & Trinke, S. (2003). The intergenerational transmission of relationship violence. Journal of Family Psychology, 17(3), 288. https://doi.org/10.1037/0893-3200.17.3.288
Lamb, C. (2018). Breaking the cycle of violence for child refugees who display aggressive behaviour. Educating Young Children: Learning and Teaching in the Early Childhood Years, 24(3), 21–23. https://search.informit.org/doi/10.3316/aeipt.221755
Loinaz, I., & de Sousa, A. (2020). Assessing risk and protective factors in clinical and judicial child-to-parent violence cases. European Journal of Psychology Applied to Legal Context, 12(1), 43.
https://doi.org/10.5093/ejpalc2020a5
Mack, N., Woodsong, C., MacQueen, K., Guest, G., & Namey, E. (2005). Qualitative research methods: A data collector’s field guide. Family Health International.
Maher, J. M., Fitz-Gibbon, K., Meyer, S., Roberts, S., & Pftizner, N. (2021). Mothering through and in violence: Discourses of the “good mother”. Sociology, 55(4), 659–676.
https://doi.org/10.1177/0038038520967262
Malvaso, C. G., Delfabbro, P. H., & Day, A. (2019). Adverse childhood experiences in a South Australian sample of young people in detention. Australian and New Zealand Journal of Criminology, 52(3), 411–431. https://doi.org/10.1177/0004865818810069
Margolin, G., & Baucom, B. (2014). Adolescents’ aggression to parents: Longitudinal links with parents’ physical aggression. Journal of Adolescent Health, 55(5), 645.
https://doi.org/10.1016%2Fj.jadohealth.2014.05.008
Martínez-Ferrer, B., Romero-Abrio, A., León-Moreno, C., Villarreal-González, M., & Musitu-Ferrer, D. (2020). Suicidal ideation, psychological distress and child-to-parent violence: A gender analysis. Frontiers in Psychology, 11, 575388. https://doi.org/10.3389/fpsyg.2020.575388
McDonald, C., Wiebe, D., Guerra, T., Thomas, N., & Richmond, T. (2011). The importance of family to youth living in violent communities. Journal of Psychiatric and Mental Health Nursing, 653.
https://doi.org/10.1111/j.1365-2850.2011.01774.x
McGeeney, E., Barakat, F., Langeland, G., & Williams, S. (2016). The Yuva young people’s service: A holistic approach to addressing child-to-parent violence in London. In A. Holt (ed.), Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention (pp. 117–133). Routledge.
McKenna, M., & O’Connor, R. (2012). Walking on eggshells: Child and adolescent violence in the family. Relationships Australia (SA), Flinders University & Southern Junction Community Services.
Meyer, S., Reeves, E., & Fitz-Gibbon, K. (2021), The intergenerational transmission of family violence: Mothers’ perceptions of children’s experiences and use of violence in the home. Child & Family Social Work, 26, 476–484. https://doi.org/10.1111/cfs.12830
Meyer, S., & Stambie, R. M. (2020). Mothering in the context of violence: Indigenous and non-Indigenous mothers’ experiences in regional settings in Australia. Journal of Interpersonal Violence.
https://doi.org/10.1177/0886260520975818
Moulds, L. G., Malvaso, C., Hackett, L., & Francis, L. (2019). The KIND program for adolescent family and dating violence. Australian and New Zealand Journal of Family Therapy.
https://doi.org/10.1002/anzf.1364
Nam, B., Kim, J.Y., Bright, C. L., & Jang, D. (2020). Exposure to family violence, peer attachment, and adolescent-to-parent violence. Journal of Interpersonal Violence, 37(7–8), 1–22.
https://doi.org/10.1177/0886260520960109
Nowakowski-Sims, E. (2019). An exploratory study of childhood adversity and delinquency among youth in the context of child-to-parent and sibling-to-sibling violence. Journal of Family Social Work, 22(2), 126–145. https://doi.org/10.1080/10522158.2018.1496510
O’Hara, K. L., Duchschere, J. E., Beck, C. J. A., & Lawrence, E. (2017). Adolescent-to-parent violence: Translating research into effective practice. Adolescent Research Review, 2(3), 181–198.
https://doi.org/10.1007/s40894-016-0051-y
O’Keefe, M. (2005) Teen dating violence: A review of risk factors and prevention efforts. National Online Resource Center on Violence Against Women. https://vawnet.org/material/teen-dating-violence-review-risk-factors-and-prevention-efforts
Om, J. (2020, August 25). Coronavirus hard lockdown of Melbourne public housing towers left residents feeling like “criminals”, inquiry hears. ABC News. https://www.abc.net.au/news/2020-08-25/coronavirus-melbourne-public-housing-tower-shutdown-inquiry/12589372
Pagani, L., Tremblay, R., Nagin, D., Zoccolillo, M., Vitaro, F., & McDuff, P. (2004). Risk factor models for adolescent verbal and physical aggression toward mothers. International Journal of Behavioural Development, 28(6), 528. https://doi.org/10.1080/01650250444000243
Papamichail, A., & Bates, E. (2020). “I want my mum to know that I am a good guy …”: A thematic analysis of the accounts of adolescents who exhibit child-to-parent violence in the United Kingdom. Journal of Interpersonal Violence, 37(9-10), 5849–5856.
https://doi.org/10.1177/0886260520926317
Paterson, R., Luntz, H., Perlesz, A., & Cotton, S. (2002). Adolescent violence towards parents: Maintaining family connections when the going gets tough. Australian and New Zealand Journal of Family Therapy, 23, 90. https://doi.org/10.1002/j.1467-8438.2002.tb00493.x
Peck, A., Hutchinson, M., & Provost, S. (2020). Young person-to-mother violence: An integrative review of evidence from Australia and New Zealand. Australian Social Work, 1. https:// doi.org/10.1080/0312407X.2021.188730
Peek, L., & Fothergill, A. (2009). Using focus groups: Lessons from studying daycare centers, 9/11, and Hurricane Katrina. Qualitative Research, 9, 31–59. https://doi.org/10.1177/1468794108098029
Pereira, R., Loinaz, I., del Hoyo-Bilbao, J., Arrospide, J., Bertino, L., Calvo, A., Montes, Y., & Gutiérrez, M. M. (2017). Proposal for a definition of filio-parental violence: Consensus of the Spanish Society for the Study of Filio-Parental Violence (SEVIFIP). Psychologist Papers, 38(3), 216–223.
https://doi.org/10.23923/pap.psicol2017.2839
Perkins, N., & Grossman, S. F. (2020). Sibling violence: The missing piece in family violence policy. Advances in Social Work, 19(1), 138–156. https://doi.org/10.18060/22611
Perkins, N. H., Rai, A., & Grossman, S. F. (2021). Physical and emotional sibling violence in the time of COVID-19. Journal of Family Violence, 1–8. https://doi.org/10.1007/s10896-021-00249-6
Peterman, A., Potts, A., O’Donnell, M., Thompson, K., Shah, N., Oertelt-Prigione, S., & van Gelder, N. (2020). Pandemics and violence against women and children (Working paper no. 528). Center for Global Development. https://www.cgdev.org/sites/default/files/pandemics-and-vawg-april2.pdf
Pfitzner, N., Fitz-Gibbon, K., Meyer, S., & True, J. (2020). Responding to Queensland’s “shadow pandemic” during the period of COVID-19 restrictions: Practitioner views on the nature of and responses to violence against women. Monash Gender and Family Violence Prevention Centre, Monash University. https://apo.org.au/sites/default/files/resource-files/2020-06/apo-nid306064.pdf
Pösö, T., Honkatukia, P., & Nyqvist, L. (2008). Focus groups and the study of violence. Qualitative Research, 8(1), 73–89. https://doi.org/10.1177/1468794107085297
Reed R. G., Barnard, K., & Butler, E. A. (2015). Distinguishing emotional coregulation from codysregulation: An investigation of emotional dynamics and body weight in romantic couples. Emotion, 15(1), 45–60. https://doi.org/10.1037/a0038561
Respect. (2021). Respect Young People’s Programme.
https://www.respect.uk.net/pages/115-rypp
Robinson, E., Power, L., & Allan, D. (2011). What works with adolescents? Family connections and involvement in interventions for adolescents with problem behaviours. Family Matters, 88, 57–64.
Robinson, E., & Miller, R. (2012). Adolescents and their families: Best interest case practice model specialist practice resource. Victorian Government, Department of Human Services.
Routt, G., & Anderson, L. (2011). Adolescent violence towards parents. Journal of Aggression, Maltreatment & Trauma, 20(1), 1. https:// doi.org/10.1080/10926771.2011.537595
Routt, G., & Anderson, L. (2016). Building respectful family relationships: Partnering restorative practice with cognitive-behavioural skill learning. In A. Holt (ed.), Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention (pp. 15–33). Routledge.
Rutter, N. (2020). “I’m meant to be his comfort blanket, not a punching bag”: Ethnomimesis as an exploration of maternal child to parent violence in pre-adolescents. Qualitative Social Work: Research and Practice, 20(1), 1317–1338. https://doi.org/10.1177/1473325020940774
Rutter, N., Hall, K., & Westmarland, N. (2022) Responding to child and adolescent-to-parent violence and abuse from a distance: Remote delivery of interventions during Covid-19. Children & Society, 1–7.
https://doi.org/10.1111/chso.12622
Selwyn, J., & Meakings, S. (2016). Adolescent-to-parent violence in adoptive families. British Journal of Social Work, 46(5), 1224–1240. https://doi.org/10.1093/bjsw/bcv072
Shanholtz, C. E., O’Hara, K. L., Duchschere, J. E., Beck, C. J., & Lawrence, E. (2020). Understanding the perception of stakeholders in reducing adolescent-to-parent violence/aggression. Journal of Adolescence, 80, 264–274. https://doi.org/10.1016/j.adolescence.2020.02.015
Shannahan, B. (2017). We don’t give up: Developing family and community responses to adolescent-to-parent violence. International Journal of Narrative Therapy and Community Work, 2, 13–27.
https://search.informit.org/doi/10.3316/informit.959969122982399
Simons, H. (2012). Case study research in practice. SAGE Publications Ltd.
Simmons, M., McEwan, T. E., & Purcell, R. (2020). A social-cognitive investigation of young adults who abuse their parents. Journal of Interpersonal Violence, 37(1–2), 327–349. https://doi.org/10/1177/0886260520915553
Simons, H. (2014). Case study research: In-depth understanding in context. In P. Leavy (ed.), The Oxford Handbook of Qualitative Research (pp. 1–29). Oxford University Press.
Spearman, K., Hardesty, J., & Campbell, J. (2022). Post-separation abuse: A concept analysis. Journal of Advanced Nursing. https://doi.org/10.1111/jan.15310
State of Victoria. (2014). Adolescent family violence program service model (Draft, February 2014).
https:// providers.dhhs.vic.gov.au/adolescent-family-violence-program-service-model-word
State of Victoria. (2016). Royal Commission into Family Violence: Full report.
https://www.rcfv.com.au/MediaLibraries/RCFamilyViolence/Reports/RCFV_Full_Report_Interactive.pdf
State of Victoria. (2018, January 24). Putting kids first: Evidence-based trials to improve safety [Media release]. https://www.premier.vic.gov.au/putting-kids-first-evidence-based-trials-to-improve-safety
State of Victoria. (2020, August 17). Keeping family violence in sight during coronavirus.
https://www.premier.vic.gov.au/keeping-family-violence-sight-during-coronavirus
Stylianou, A., & Ebright, E. (2021). Providing coordinated, immediate, trauma-focused, and interdisciplinary responses to children exposed to severe intimate partner violence: Assessing feasibility of a collaborative model. Journal of Interpersonal Violence, 36(5–6), 2773–2799.
https://doi.org/10.1177/0886260518769359
Sutherland, G., Rangi, M., King, T., Llewellyn, G., Kavanagh, A., & Vaughan, C. (2022). A socio-ecological exploration of adolescent violence in the home and young people with disability: The perceptions of mothers and practitioners (Research report, 19/2022). ANROWS.
https://www.anrows.org.au/publication/a-socio-ecological-exploration-of-adolescent-violence-in-the-home-and-young-people-with-disability-the-perceptions-of-mothers-and-practitioners
Thiara, R., & Humphreys, C. (2015). Absent presence: The ongoing impact of men’s violence on the mother–child relationship. Child & Family Social Work, 22(1), 137–145.
https://doi.org/10.1111/cfs.12210
Tucci, J., Mitchell, J., & Thomas, L. (2020). A lasting legacy: The impact of COVID-19 on children and parents. Australian Childhood Foundation.
Tucker, C. J., Finkelhor, D., & Turner, H. (2020). Family predictors of sibling versus peer victimization. Journal of Family Psychology, 34(2), 186–195. https:// doi.org/10.1037/fam0000592
Usher, K., Bhullar, N., Durkin, J., Gyamfi, N., & Jackson, D. (2020). Family violence and COVID‐19: Increased vulnerability and reduced options for support. International Journal of Mental Health Nursing, 29(4), 549–552. https://doi.org/10.1111/inm.12735
Usher, K., Bradbury-Jones, C., Bhullar, N., Durkin, J., Gyamfi, N., Fatema, S., & Jackson, D. (2021). COVID-19 and family violence: Is this a perfect storm? International Journal of Mental Health Nursing. https://doi.org/10.1111/inm.12876
VicHealth. (2020). Young people coping with coronavirus: Interim report.
https://www.vichealth.vic.gov.au/-/media/ResearchandEvidence/Young-people-coping-with-coronavirus.pdf
Victoria Police. (2017). Code of practice for the investigation of family violence (3rd ed.).
https://content.police.vic.gov.au/sites/default/files/2019-01/Code-of-Practice-for-the-Investigation-of-Family-Violence-Edition-3-V3-FINAL.pdf
Victorian Ombudsman. (2020). Investigation into the detention and treatment of public housing residents arising from a COVID-19 “hard lockdown” in July 2020. Victorian Ombudsman. https://www.ombudsman.vic.gov.au/our-impact/investigation-reports/investigation-into-the-detention-and-treatment-of-public-housing-residents-arising-from-a-covid-19-hard-lockdown-in-july-2020/
Walker, S., & Woerner, J. (2018). Adolescent sibling violence in Victoria. Melbourne, Australia. Crime Statistics Agency.
https://www.crimestatistics.vic.gov.au/sites/default/files/embridge_cache/emshare/original/public/2020/07/b8/3047e4ed5/Crime%20Statistics%20Agency%20-%20In%20Fact%208%20-%20Adolescent%20sibling%20violence.pdf
Warr, D. J. (2005). “It was fun … but we don’t usually talk about these things”: Analyzing sociable interaction in focus groups. Qualitative Inquiry, 11(2), 200–225.
https://doi.org/10.1177/1077800404273412
Wellmer, A. (2014). On critical theory. Social Research: An International Quarterly, 81(3), 705–733.
https://doi.org/10.1353/sor.2014.0045
Wilks, S., & Wise, S. (2012). Stopping adolescent violence in the home: An outcome evaluation of Breaking the Cycle. Anglicare Victoria.
Zhang, L., Cai, C., Wang, Z., Tao, M., Liu, X., & Craig, W. (2019). Adolescent-to-mother psychological aggression: The role of father violence and maternal parenting style. Child Abuse and Neglect, 98.
https://doi.org/10.1016/j.chiabu.2019.104229
APPENDIX A:
AVITH Collaborative Practice Framework: Multidisciplinary and
multi-system
Pillars
Understanding
- A shared recognition of AVITH as distinct from adult-perpetrated violence and which accounts for trauma, developmental stage and the function of used behaviours
- A shared understanding of key terms, such as “collaboration”, “whole-of-family”, “family violence risk” and “family safety” established across the system
- Clear understanding of roles and responsibilities at both a system level and individual
practice level
Coordination
- Processes and mechanisms are in place to support a coordinated risk approach, with clear accountability around the role of each service and practitioner, ideally with a practice lead holding the whole family in view. Coordination is led by a service with capacity to provide continuity, streamline service interactions and reduce overwhelm
- Services work together to sequence interventions appropriately and in a way that reflects family readiness and maximises the benefits of engagement
Workforce
- A highly specialised workforce which is supported to work flexibly (and intensively where
required) to meet the specific needs of families experiencing AVITH - System and organisational recognition that program resourcing must incorporate ample time for reflective practice and continuous learning
- Baseline capacity across the wider system to identify and support the management of AVITH-related risk, including through appropriate referrals and early intervention work
Evidence
- Practitioners incorporate evidence and learning into their daily practice, including through debriefing, reflective practice and collaborative practice networks
- AVITH responses draw on evidence and data – including the voices of young people and their families
– to inform service design, planning and continuous improvement - Government supports a system-wide approach to building and sharing evidence, piloting responses and taking effective interventions to scale
Principles
- Trauma- and family violence risk–informed: All practitioners and services involved adopt a holistic view of family violence risk and use of harm, recognising the impacts of prior and current adult-perpetrated violence and how these may be influencing current behaviours and relational dynamics, including trauma in caregivers. Practitioners maintain a lens on the impacts of trauma on child brain development, including language, meaning, emotional regulation and impulse control.
- Whole-of-family: Practitioners and services give full consideration to needs and histories across
- the family in assessing and managing risk. Opportunities to reduce AVITH-related risk may
- involve interventions with multiple family members where appropriate and safe, including where multidirectional use of violence is present or misidentification has occurred. Relational work is recognised as crucial to recovery, as well as playing a key role in adolescent identity formation and self-actualisation.
- Addressing barriers to engagement: Recognising the particular engagement challenges when working with young people and families experiencing AVITH, including prior experiences of under-servicing or over-servicing, services work flexibly and in a coordinated way, adopting relational approaches which leverage existing supports and therapeutic relationships around the family. Service contact is streamlined and scaffolded to reduce the burden on the family and young person.
- Flexible and needs-based: Young people and families receive a response which is tailored to their individual needs and goals. Practitioners and services are skilled, supported and flexible enough to respond to different AVITH presentations, including where the function of a young person’s behaviour is connected with disability and/or mental health needs. Responses take account of what a family identifies as their most immediate needs and reflects their readiness to engage at a given point in time.
- Intersectional and culturally safe: Services are equipped to respond to the intersecting and layered identities of families experiencing AVITH. This includes Aboriginal and Torres Strait Islander families, families from CALD backgrounds, LGBTQ+ families and young people, and families with a child with a disability. Cultural responsiveness is central to continuous learning and development, underpinned by strong relationships and consultation with culturally specific services. Services recognise and understand that individual family members will have different experiences, including where shared marginalisation may be a source of conflict.
- Service accountability: The roles, responsibilities and expertise of each practitioner or service involved in a family’s support are well understood, with the involvement of services determined by the family’s needs, preferences and readiness. Services are accountable and committed to working with the family to agree, plan for and progress their specific goals. Communication between services is proactive and transparent, with a particular focus on ensuring that dynamic risk information is shared and managed collectively.
Enables
Funding
- Program funding is adequate, consistent and flexible to enable long-term, whole-of-family work
Evidence-Informed Tools
- Robust and shared tools which are tailored to AVITH contexts are used to assess and plan
Culture
- Organisations foster a culture of collaboration, including within and across organisational boundaries
Service Capacity
- Capacity to meet demand and complexity across the system is actively monitored and adjusted as required
Continuous Learning
- Services are supported to adopt a structured approach to continuous learning and practice development
System Stewardship
- Government functions as an interface between systems, removing barriers to collaboration and responsive practice
Endnotes
- For a more detailed discussion about the literature regarding prevalence of AVITH, see “Context: An evolving service environment” Back to reference ↑
- Co-dysregulation” refers to a process in which the emotions of people in a close relationship are “bi-directionally linked and mutually amplifying, away from emotional stability” (Reed et al., 2015, p. 46). Back to reference ↑
ELENA CAMPBELL
Associate Director, Centre for Innovative Justice, RMIT University
RILEY ELLARD
Manager, Centre for Innovative Justice, RMIT University
ELIZA HEW
Project Officer, Centre for Innovative Justice, RMIT University
MATILDA SIMPSON
Project Officer, Centre for Innovative Justice, RMIT University
BETH McCANN
General Manager, Centre for Family Research and Evaluation, Drummond Street Services
SILKE MEYER
Chair in Child and Family Research, Griffith University and Adjunct Professor,
Monash Gender and Family Violence Prevention Centre, Monash University
RESEARCH REPORT
ISSUE 4 | APRIL 2023
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we live and work. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and emerging. We value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with First Nations Peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2023
![]()
With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au
ABN 67 162 349 171
ISBN: 978-1-922645-66-1 (paperback)
ISBN: 978-1-922645-67-8 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project “WRAP around families experiencing AVITH: Towards a collaborative service response”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Outcome 4 – Services meet the needs of women and their children experiencing violence.
Suggested citation:
Campbell, E., Ellard, R., Hew, E., Simpson, S., McCann, B. & Meyer, S. (2023). WRAP around families experiencing AVITH: Towards a collaborative service response (Research report, 04/2023). ANROWS.
![]()
Centre for Innovative Justice, RMIT University
Level 2, Building 52
147–155 Pelham Street, Carlton VIC 3053
Wurundjeri Country
Author acknowledgement
The project was led by the Centre for Innovative Justice (CIJ) at RMIT University, in partnership with the Centre for Family Research and Evaluation (CFRE) at Drummond Street Services and the Monash Gender and Family Violence Prevention Centre (MGFVPC).
The lead author wishes to acknowledge all the dedicated practitioners who gave up their time to participate in this research during Victoria’s protracted lockdowns. In particular, the author wishes to acknowledge practitioners at Drummond Street Services and staff of the CFRE who facilitated provision of data for the case file review. The team also wishes to acknowledge the contributions of the parents who participated in interviews for this research – their resilience in the face of long histories of intimate partner violence and their determination to protect their children shone through in their contributions. They confirm once again the need for better support for women and children in the wake of adult-perpetrated harm.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
ANROWS acknowledges that children and young people living in homes where domestic and family violence (DFV) is present are not simply “exposed” to DFV – they are experiencing it. There are no circumstances in which children and young people are exposed to DFV and are not also being impacted by this violence. Therefore, ANROWS will always default to using “experienced DFV” instead of “were exposed to DFV” or “witnessed DFV”. This language recognises that children experience DFV as victims in their own right, and also seeks to honour the voices of victims and survivors who have felt minimised, erased or unacknowledged as childhood survivors.
Please note that in this report, in certain contexts, the authors have chosen to use the term “exposed to DFV”.
Caution: The following report contains descriptions of domestic and family violence and adolescent violence in the home, and mention of suicide. Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76)
Definitions and concepts
| Concept | Definition |
|---|---|
| AVITH | This report uses the term “adolescent violence in the home” (or “AVITH”) to describe the use of violence or harm against family members by children and young people. The majority of the evidence base indicates that this behaviour is more commonly used by young males than young females, although some recent research indicates that young females may either self-report as using violence more frequently, or be identified by the system for use of violence where use of the same behaviour by young males may be overlooked. While the gendered nature of the use of AVITH is not as distinct as the gendered nature of adult-perpetrated violence, far more pronounced is the gendered nature of victimisation. Specifically, evidence indicates that AVITH is most commonly experienced by mothers or female caregivers, particularly in the context of sole parent or separated families.[1] The research team purposefully uses a term that is broader than “domestic and family violence” or “family violence” because, as the PIPA project (“Positive Interventions for Perpetrators of Adolescent violence in the home”) demonstrated and this research confirms, use of harm by young people can occur along a broad spectrum of behaviours (Campbell et al., 2020; see also definition below). In particular, the PIPA project found that some of this behaviour does not meet the legislative definition of family violence in Victoria; some of it is related to dysregulation or the impacts of past trauma; some of it manifests as resistance to current trauma or experiences of victimisation; and some of it is directly related to disability. This means, for example, that the behaviour is more complex, has different drivers or has a different intent than adult intimate partner violence. By using this broad definition, the authors do not suggest inany way that family members who experience this harm do not find it incredibly frightening and distressing. Rather, the use of this term is intended to recognise the complexity inherent in this phenomenon. AVITH is also the term used by the practitioners who participated in this study. |
| Family violence | At points during this report, the term “family violence” is used in preference to the broader term “domestic and family violence” (DFV). This is because “family violence” is the predominant term used in Victoria, the Australian jurisdiction in which this research took place. At other times, where more broadly applicable, the wider term DFV is used. |
| Young person | Although the title and terminology of the phenomenon used throughout this report refers to “adolescents”, as does the majority of the relevant literature, it is important to note that the preferred terminology of the practitioners participating in this report was “young people”. This reflects a wider shift in the social and human services environment which uses respectful and strengths-based terminology, as well as acknowledging neurodevelopmental trajectories beyond childhood. The term “young people” is also more inclusive of the client base of some services participating in this research that work with young people up to the age of 22. Where the term is used to refer to people over the age of 18 in the context of this research, and is therefore referring to young adults, this is identified. In general, however, the term “young people” used in this report refers to individuals aged under 18, recognising their legal status aschildren and, in the cases of younger children, their lack of access to relevant supports without the consent of their parents. |
| The PIPA project | The PIPA project was an ANROWS-funded study that examined legal and service responses to AVITH across three Australian jurisdictions (Victoria, Tasmania and Western Australia). The data collection for the research was conducted during 2017 and 2018 with the final report published in March 2020. The primary findings across this study concerned the harmful and counterproductive impacts of legal responses where young people are identified by the legal system as using AVITH; the significant prevalence of disability and neurodivergence among young people caught up in the legal response to AVITH in Victoria, in particular; and, specifically, the need for service responses to identify risk and needs across family structures and to wrap around each family with appropriate support. It is this final recommendation to which the current study specifically responds. |
| The Orange Door | The Orange Door network is a network of support and safety hubs established by the Victorian Government following recommendations by the state’s Royal Commission into Family Violence. The network is supposed to function as a shopfront with a “no wrong door” approach, operating as the intake point for police referrals in relation to victims and survivors and people using violence, as well as child safety and wellbeing concerns. Individuals can also self-refer without going through police, whether by phoning or attending in person. The Orange Door functions primarily as an intake point through which matters are then triaged and referred out to other appropriate services. |
| Drummond Street Services | Drummond Street Services is a large community-based organisation that has delivered support to vulnerable families and young people for over 100 years. It provides a range of services, including mental health services, family services, parenting services, support for blended and stepfamilies, specialist family violence services and supports for marginalised cohorts. These include supports for families from culturally and linguistically diverse communities; families in public housing; and LGBTQA+ and intersex young people and families, through its Queerspace programs. |
Acronyms
| Acronym | Definition |
|---|---|
| ACCO | Aboriginal community-controlled organisation |
| AOD | Alcohol and other drugs |
| AVITH | Adolescent violence in the home |
| CALD | Culturally and linguistically diverse |
| CFECFW | Centre for Excellence in Child and Family Welfare |
| CFRE | Centre for Family Research and Evaluation |
| DFV | Domestic and family violence |
| DS | Drummond Street Services |
| FVISS | Family Violence Information Sharing Scheme |
| GP | General Practitioner |
| LGBTQ+ and intersex | Lesbian, gay, bisexual, trans, queer and intersex |
| NDIS | National Disability Insurance Scheme |
| NVR | Non-violent resistance |
| PIPA | Positive Interventions for Perpetrators of AVITH |
| RCFV | Royal Commission into Family Violence |
| RYPP | Respect Young People’s Programme (United Kingdom) |
| VFRIM | Victorian Family Violence Implementation Monitor |
| WRAP | Wraparound Responses for AVITH Programming |
Executive summary
Background
“WRAP around families experiencing AVITH: Towards a collaborative service response” (the “WRAP around families” project) was a targeted, mixed-methods research project with the specific aim of developing a framework for holistic, evidence-based practice in response to the complex issue of adolescent violence in the home (AVITH). The research was a direct response to a recommendation from the PIPA project (Campbell et al., 2020), which highlighted the complexity of needs across many families experiencing AVITH. The PIPA project found that appropriate service interventions require wraparound, whole-of-family responses, rather than responses directed predominantly at a young person’s behaviour.
Aims
As a “deep dive” into the service response to AVITH, the WRAP around families project aimed to identify current system barriers and to surface the enablers which may contribute to more consistent and collaborative practice. Originally the research aimed to explore what young people and their families identified about their own needs, including the impacts on siblings and the role of pre-existing trauma in parents. The ongoing impacts of COVID-19 on practitioner engagement with clients during the data collection period limited the extent to which this aim could be achieved, although rich accounts from interviews with three parents and reviews of 33 case files contributed significantly. The research also aimed to move practice and policy towards a consistent understanding of AVITH, given the uncertain position that it continues to occupy in domestic and family violence (DFV) responses.
Method
The research was informed by two data streams, the first being an exploration of current community-based service responses through focus groups with 75 practitioners in Victoria, a jurisdiction with a particular investment in this area. The majority of these focus groups were conducted from July to September 2021, while focus groups with Aboriginal community-controlled organisations (ACCOs) were conducted from June to August 2022. The second strand involved a mixed-methods case study approach to an intervention developed by a large community service organisation, Drummond Street Services (DS). The case study involved reviews of 33 case files from the service, with findings tested and validated through workshops with practitioners in this program. The case study also included interviews with three parents. Ethical approval for the research was obtained from the Victorian Department of Justice Human Research Ethics Committee (CF/21/5126).
A targeted scan of relevant peer-reviewed and grey literature was also conducted. Important to note, this was not intended to function as a systematic or even standard literature review, but rather to ensure that major relevant studies and program responses that were specifically relevant to service delivery and had been released or developed since the initial research phase of the PIPA project could inform the WRAP around families project’s design and analysis.
Findings
The research signalled that practitioners and programs were working hard to respond to young people and families experiencing AVITH in a service and system context which continues to have limitations. While there is now greater familiarity with the concept of AVITH and nuance in the practice of individual practitioners, the research found that Victoria’s response is still some way from being properly developed and bedded down at a systemic level. It should be acknowledged that this shifted to a degree between the point of data collection and publication, with growing government investment in service design, as well as the pending release of risk assessment and management tools.
Practice challenges
Naming and identifying AVITH
Findings from the focus groups were echoed to a significant extent in the parent interviews and signalled a number of substantial barriers to effective practice operating at the time of the research. These included the wider service system often having difficulty identifying AVITH or understanding its nuances, with responses to AVITH often dependent on the knowledge of individual practitioners and many services still responding within the binary framework of adult intimate partner violence. In this framework, policy and service responses are framed in terms of victims and survivors on the one hand or perpetrators on the other, rather than being able to contemplate that an individual may be using and experiencing violence at the same point or over the course of a lifetime. This binary framing in turn could impact the nature of referrals, the information that these referrals contained and the responses that were provided as a result.
Constraints on effective practice
Funding parameters impacted the capacity of services to respond in ways that families required. This included the need to work with multiple family members in a meaningful way or provide flexible and client-centred approaches, such as conducting outreach or engaging with young people through in-person activities and over the long term, as the case study component of this research indicated was required. Practitioners also described the detrimental impact of cyclical funding and limits on caseloads on the capacity to deliver effective service, although they did highlight the significant benefits of brokerage provided as part of a recent injection of additional investment.
Previous and ongoing adult-perpetrated violence and control
The predominant presenting client needs described by practitioners and apparent in the case study stemmed from pre-existing trauma from adult-perpetrated DFV, as well as the presence of ongoing coercive control. The presence of current adult-perpetrated DFV is not explored as thoroughly in the literature and in policy settings as the impacts of past DFV. The presence of current adult-perpetrated DFV across practitioner caseloads and the case study was therefore an important finding. The eligibility criteria of some programs precluded work with young people where adult-perpetrated DFV was present, while other programs were trying to conduct this work, despite not having associated supports or frameworks.
This experience of past and current trauma was clearly contributing to complex combinations of co-occurring issues in many young people and victim and survivor parents, which included, most prominently, significant mental health and sometimes alcohol and other drug (AOD) issues, as well as disability. Crucial to note, despite families presenting to DS in relation to their children, the overwhelming theme across the interviews and case files was the way in which adult-perpetrated DFV and ongoing coercive control was continuing to impact every aspect of the lives of mothers and their children. While parents were seeking support for their child’s behaviour, severe mental ill health, disability and learning needs, as well as for school disengagement, the single greatest contributing factor to these support needs – as well as to the needs of mothers – appeared to be the impacts of adult-perpetrated harm.
Impacts of other adverse experiences
In addition to adult-perpetrated DFV, the findings pointed to the impacts of other adverse experiences and the way in which these contributed either to the use of harmful behaviour by young people, or the way in which parents and siblings could manage what was occurring in their home environment. These included sub-themes that emerged from the focus groups: the relationship of bullying victimisation to use of AVITH, as well as the impacts of grief and separation on families as a whole, including separation from caregivers as a result of illness.
Impacts of COVID-19
More broadly, the findings indicated that co-occurring needs across families – including the risk of current adult-perpetrated DFV – were compounded by the impacts of COVID-19, while the challenges of engaging with and supporting clients during this time were made more acute. Practitioners voiced concerns that they had fewer “eyes” on the current risk that a young person might be experiencing, while the parents interviewed highlighted the need for face-to-face engagement that was not always available during the period covered by the research.
System challenges
Under-servicing and over-servicing
Practitioners voiced a particularly strong concern that families were either being “under-serviced”, and receiving no effective support for multiple presenting needs, or alternatively were being “over-serviced”, with multiple services involved over a long period, despite this over-servicing having no constructive effect. The case study similarly reflected the challenges of families receiving no effective service support and experiencing stop-start engagement which had limited capacity to support young people and which commenced and ceased involvement without any meaningful results.
Impact of negative service interactions
Prior negative experiences of service interactions were also apparent as a particular barrier to service engagement. The predominant examples nominated by practitioners were the damaging impact of multiple services in a young person’s or family’s life. Parents interviewed and case files all highlighted the impacts of ill-informed or misguided engagement with a private psychologist or school counsellor, including where these were manipulated by an adult perpetrator in ways which made young people refuse to engage in “talk therapy” again.
Care teams
The research identified important findings around care teams, with the research team anticipating that care teams would be a mechanism for emerging collaboration. Focus groups indicated that the purpose and composition of a care team could run counter to trauma-informed practice with young people, including where care teams focused on holding young people accountable, rather than on providing care and support.
In particular, the research found that care teams often lacked a practitioner to coordinate the activities to which care team members had committed. This was needed to ensure that practitioners followed up on their responsibilities and that one practitioner was liaising with the young person and family.
Promising practice
Evolving service recognition
Despite challenges in consistent and coherent articulation of what AVITH actually involves, the findings indicated that recognition of AVITH was growing among families, with many families in the case study having self-referred. Findings also suggested that it was a specialist area of work from which other services were grateful to receive support. A crucial consideration identified by practitioners was being aware of the context in which the intervention on offer was being described or labelled by services, with young people understandably reluctant to be labelled for behaviours which may have been repeatedly used against them.
Working with multiple family members
The research highlighted creative ways to support multiple family members. These included examples of supporting a caregiver’s wider needs and the impacts of trauma, while working with a young person around their use of harm and a sibling around their mental health needs. Participating ACCOs, in particular, emphasised that it was essential to cement any gains made with a young person through the provision of appropriate supports at home.
Capacity for flexible, client-centred responses
Findings confirmed the significant benefits where funding or organisational support allowed for work to be conducted on a longer-term basis, providing sufficient time to develop trust and rapport with young people. Emphasised as crucial by practitioners and parents alike – and evident in case files – were the benefits of outreach and shared activities, as well as brokerage to provide access to specific and tailored supports for different family members which could have a positive impact overall.
Shared positive experiences and strengths-based approaches
One of the primary findings of the research, echoed by key Australian research (Burck, 2021; Meyer et al., 2021; Burck et al., 2019), was that mothers and children who have experienced adult-perpetrated DFV, and continue to grapple with its ongoing impacts, need opportunities to build attachments and form their collective identity around positive experiences. Parent interviews and case files reflected the impacts of shared experiences of trauma on mothers’ relationships with their children and capacity to parent, while practitioners and case files provided examples of how brokerage or other mechanisms could facilitate positive experiences through which they could start to see their family in a new light. Again, ACCOs provided particularly strong examples of this, describing the benefits of supporting families proactively, rather than waiting for a crisis.
Giving voice to young people, keeping an original perpetrator in view
Corresponding with this, the research highlighted the importance of giving voice to young people where their experiences were often not coming through in referrals or in care team discussions and where the impacts of adult-perpetrated DFV – including ongoing systems abuse – remained out of view. Practitioners described nuanced examples of working with other agencies to widen the intervention lens to allow consideration of the presence of an adult perpetrator. Case files similarly demonstrated the delicate considerations involved, including where a perpetrator parent could withhold consent for a young person’s receipt of services to exercise ongoing control.
Reflective practice and emerging collaboration
Findings therefore indicated the need for a critical and reflective approach as a core foundation to AVITH-focused work. Examples of effective service intervention rested on constant interrogation of what was actually occurring in the lives of families and young people, as well as a constant interrogation of a practitioner’s own assumptions. This involved questioning the reasoning behind other service or practitioner decisions and stepping in or stepping out again as services focused on what families and young people identified as their most pressing need, rather than what services dictated.
Discussion and framework
Specialisation within a specialisation: Towards a collaborative framework
The complexity of this practice – which had been conducted for decades by one service and for years by others – signalled the need for AVITH-focused work to be recognised as a “specialisation within a specialisation”. The findings indicated that this work could be supported by services being sufficiently resourced to allow work with multiple family members; sufficiently flexible to provide for client-centred responses; and sufficiently secure to allow workforces to be developed over the long term.
To this end, the WRAP around families project proposes a Collaborative Practice Framework, through which policymakers can take responsibility for enablers, practitioners can engage with the core principles of practice, and all involved can base decisions on the foundational pillars so essential to the work. Practice examples, rather than discrete recommendations, are provided to support consideration of how the Framework might be applied in particular contexts.
Overall, therefore, what was originally expected to be a blueprint for collaboration across services became a blueprint for collaboration across practice and policy – so apparent was the need for this wider lens to be applied.
Pillars of the Framework
The Collaborative Practice Framework is based on four core pillars of understanding, workforce, coordination and evidence. As well as constituting individual components of an effective system-wide AVITH response, practitioners emphasised the mutually constitutive nature of the pillars, with each continually informing and reinforcing the others.
Shared understanding can help to challenge and unpack the binary paradigm of “victim and survivor”/”perpetrator” that underpins wider DFV work, recognising that young people using AVITH are most often victims and survivors in their own right and that the functions of their behaviour may be a signal of unmet needs. Practitioners can support this understanding in their advocacy to their own organisations, in their involvement in care teams, and in the terminology that they use with clients. Organisations and government can design, scope and resource interventions in recognition that this specialist work requires nuance, complexity and time.
An “AVITH workforce” involves a specialist workforce capable of delivering therapeutic interventions and case management, as well as baseline capability across the wider service system to identify AVITH, refer appropriately and work alongside specialist practitioners. This further involves organisations and governments scoping and resourcing interventions appropriately, integrating with other services to facilitate referrals and secondary consultations, and being supported by clinical supervision and training. Just as key, it involves identifying specialist roles in wider DFV and service contexts, as well as building the baseline capability of the broader community-based service, health, education and justice sectors.
Coordination is a building block of collaboration, involving clear structures, processes and mechanisms to support organised and seamless practice. Crucially, coordination is not about outputs but about service accountability to young people and families, fostering a shared understanding of what success might look like for a family or young person and what their readiness for service engagement might be. It involves follow-up, liaison with families and young people, and information sharing to ensure that all services working around a family have an adequate lens on risk and what is occurring for the family.
Evidence recognises the evolving nature of the service system, as well as our understanding of “what works” in response to AVITH. Valuing evidence includes allocating time for debriefing and reflective practice, as well as capacity to share practice across organisations. It also includes ensuring that AVITH responses are underpinned by effective processes for monitoring, evaluation and learning over the long term – informed by the voices of young people and their families in a way that recognises the complexity and time involved in conducting this kind of consultation safely and appropriately. Just as key is government support for a system-wide approach to building and sharing evidence, piloting responses and taking effective interventions to scale. This means focusing on evidence-informed practice rather than prescriptive approaches, and on outcomes rather than outputs.
Principles of the Framework
Trauma and family violence risk–informed emphasises that it is crucial for practitioners to make the ongoing impacts of trauma – including from adult-perpetrated harm as well as the potential presence of current adult-perpetrated DFV – as a central consideration across their work. This means maintaining a lens on all forms of risk across a family and working in ways that keep any adult perpetrator in view. At its core it involves asking “What has happened to you?”, rather than “What is wrong with you?”
Whole-of-family means keeping the needs and experiences across the family in sight and considering interventions which can help to support safer family functioning. This does not necessarily mean working with every member of the family – particularly where this is not safe. Rather, relational work is seen as crucial in supporting the young person’s recovery, working with particular family members to address particular needs in ways that can reduce risk and contribute to positive relationships and outcomes.
Addressing barriers to engagement acknowledges that families and young people experiencing AVITH may have either been under-serviced or over-serviced or had prior negative experiences of service interaction. Existing shame and stigma may have been compounded by service responses, while systemic and structural harm may play a role for some families. Keeping this principle in mind means understanding these histories and working to build trust and reduce the burden of service engagement.
Flexible and needs-based recognises that young people and families need to be supported in ways that work for them. This includes working over the longer term, and adopting outreach as a key approach to build trust and rapport; leveraging brokerage to address specific needs across the family and build positive shared experiences; and, most importantly, responding to readiness and working in partnership with clients. It includes ensuring that program responses offer a variety of service responses.
Intersectional and culturally safe requires AVITH responses to include a lens on diversity and marginalisation. Practitioners must actively consider how experiences of young people may be compounded by stigma, intergenerational trauma or discrimination. Organisations should actively seek to build capacity for working in culturally safe and sensitive ways with clients from Aboriginal and Torres Strait Islander, culturally and linguistically diverse (CALD), and LGBTQ+ and intersex communities, as well as clients with disability.
Service accountability means that the roles, responsibilities and expertise of each practitioner or service involved is understood by all. An accountable service is one that does what it says it will do and which is committed to working with the family to agree on, plan for and progress their specific identified goals. For service accountability to occur at the system level, communication between services must be proactive and transparent, with an overall focus on ensuring that dynamic risk information is shared and managed collectively.
Figure 1: High-level overview of Collaborative Practice Framework: Multidisciplinary and multi-system
Source: Centre for Innovative Justice.
Text alternative for the figure above
Understanding
- Understanding
- Workforce
- Coordination
- Evidence
Principles
- Trauma and family violence risk-informed
- Whole-of-family
- Addressing barriers to engagement
- Flexible and needs-based
- Intersectional and culturally safe
- Service accountability
Enables
- Funding
- Evidence-Informed Tools & Guidance
- Culture
- Service Capacity
- Continuous Learning
- System Stewardship
Enablers in the Framework
Funding needs to be secure and stable, supporting workforce recruitment and retention over the longer term, as well as long-term work with clients, and supporting appropriate caseloads which account for the complexity and scope of AVITH-focused work and have a focus on outcomes rather than outputs.
Culture is crucial. Individual practitioners should see themselves as one part of a broader response to AVITH. Organisations should signal to practitioners that it is valuable to invest time and effort in collaborative work and that identifying and responding to AVITH is a shared responsibility.
Continuous learning is critical given the emerging nature of understanding around AVITH. Learning must occur at the practitioner, organisational and system levels, including creating opportunities for reflective practice and shared learning within and across programs and organisations.
Evidence-informed tools can foster a shared language and understanding, as well as supporting a structured approach to identifying and managing risk. Rather than replicating adult-focused tools, evidence-informed tools should be strengths-based, with capacity to recognise, assess and work with complex risk dynamics.
Service capacity requires the ability to work flexibly and responsibly, intensively and over the long term, with timely responses to prevent escalation of risk. Service capacity also requires resourcing to support workforce retention, including through supervision, training and reflective practice.
System stewardship involves government taking a lead in fostering an AVITH system which is founded on a shared understanding, removes barriers to collaboration within and across systems, and involves government collaborating with the sector to steer the system towards key outcomes.
Limitations of the research
The research had key limitations which should be acknowledged. The first was the impacts of COVID-19 on the case study program at DS which made engagement with clients – and associated recruitment to the interviews – a considerable challenge, as well as limiting data available on case files to a less significant extent. Associated limitations also include the absence of Child Protection input.
Arguably, the above limitations are all primarily attributable to the period during which data collection was conducted in the context of entrenched complexity in clients and increased workload at a practice and system level. That said, while this was anticipated to be a key focus of the focus group discussions, the primary concerns of participating practitioners related to system and policy settings which predated the pandemic but which they feared would be compounded by a lack of government resourcing in the future as a result of the pandemic and its impacts.
Implications for policy and practice
The concern voiced by practitioners is a key consideration for policymakers as they move towards future service design and investment. While the impacts of COVID-19 will continue to stretch public resources, the WRAP around families research points to the need for greater support for families and young people, provided at an earlier point to prevent greater economic and social impacts down the track.
Significantly, this involves support for women and children who have experienced adult-perpetrated DFV and, crucially, may still be experiencing its impacts. Equally this research echoes the PIPA project and other research which points to the substantial need for greater support for families with a young person with disability.
Investment in earlier intervention therefore represents a vital opportunity for prevention of AVITH – rather than waiting, as participants in the PIPA project described, until it is “10 years too late”. Where the system fails to intervene earlier, however, the WRAP around families project offers a blueprint to support a genuinely collaborative and consistent framework to respond. In doing so it signals that the nuance, flexibility and complexity which are required in practice may mean that current approaches to service funding should be re-examined and a genuine concerted investment brought to the fore.
Directions for future research
The project’s findings indicated that it was attempting to address a bigger research and practice gap in relation to collaboration than anticipated. Significant opportunities therefore exist for future research which can explore the adoption of resulting collaborative, wraparound approaches across the service system and the impacts of doing so, including any subsequent adoption of the proposed Framework.
More specifically, although case files provided insights into the experiences of siblings, the ultimate limitations on the research team’s capacity to engage directly with young people confirms examination of sibling experiences as a direction for future research. The research also suggests that the relationship of wider adverse childhood experiences to the use of AVITH, including bullying and familial grief, should be an area of future research attention. Given that practitioners identified challenges – and opportunities for more effective collaboration – related to Child Protection involvement in families’ lives, this is also a clear area in need of future focus. Further research could potentially be conducted in the context of broader work around improvements in Child Protection authorities’ capacity to identify and respond to adult perpetration.
Crucially, the relationship of current as well as prior experiences of adult-perpetrated DFV in the context of AVITH should be a significant focus of future research, avoiding the common default of describing the relationship of trauma to the use of AVITH as predominantly a historical one. A failure to identify current risk from adult-perpetrated DFV may result, in part, from the lack of young people’s voices contributing to research. It is therefore crucial that future research include opportunities for young people to share their experiences safely and in their own words.
Conclusion
The WRAP around families project was designed to be a targeted investigation into the service response to AVITH as a direct follow-up, or “coda”, to a recommendation from the PIPA project. As such, it had very limited resourcing and was expected to be conducted as a brief inquiry, or stocktake, into the extent to which service responses had progressed since the PIPA project, as well as to provide a Framework which could help to accelerate this progress further. The impacts of COVID-19, however, had flow-on effects for the project which expanded both its timeframes and scale on the one hand, while limiting its scope on the other.
Despite these challenges, however, the findings and Framework resulting from the research potentially come at a more salient time than would have otherwise been the case. Increased investment and practice development, as well as considerations around training, will position policymakers and practitioners well to be able to consider next steps. This is important because, as practitioners contributing to the refinement of the proposed Framework explained, “We have made some important progress, but the Framework is the ‘where to from here’.” Just as vitally, the research team hopes that the Framework offers policymakers and practitioners across multiple jurisdictions a blueprint for how they might consider reform in this area – no matter at which point along the path to more effective service responses to AVITH they may be.
Part 1:
Introduction and context
“WRAP around families experiencing AVITH: Towards a collaborative service response” (the WRAP around families project) was designed as a brief and targeted study. Its specific aim was to develop a framework for holistic, evidence-based practice in response to the complex issue of adolescent violence in the home (AVITH).
Rather than being a study exploring the wider phenomenon of AVITH and its manifestations, therefore, the WRAP around families project was designed to function as a “coda” in direct response to a recommendation of the earlier, more substantial PIPA project (Campbell et al., 2020). This recommendation was that appropriate service interventions in AVITH require wraparound, collaborative responses that address risk and needs across the whole family, rather than responses directed predominantly at a young person’s behaviour. The PIPA project highlighted the complexity of needs across many families who present to services and may be experiencing AVITH, but who have had either very little, or largely ineffective and damaging, prior service support. The PIPA project also highlighted the way in which young people’s perspectives and their experiences of service interventions – both effective and otherwise – are not frequently documented in literature (Campbellet al., 2020), as emphasised more recently by Condry and Miles (2021) in the UK context.
The WRAP around families project therefore originally aimed to address a gap in what young people and their families identify about their own needs, as well as a gap in understanding about co-occurring issues and wider service involvement which may prevent AVITH-focused interventions from being effective (Boxall, Morgan, Voce & Coughlan, 2020; Moulds et al., 2019). The research also aimed to contribute to evidence about the role of pre-existing trauma on parental capacity to address AVITH, highlighting the need for interventions which support recovery from adult-perpetrated intimate partner violence (Burck, 2021). Further, it aimed to explore the needs of children experiencing AVITH, with literature describing evidence in this area as particularly “scarce” (Perkins & Grossman, 2020; Perkins et al., 2021).
In particular, however, the WRAP around families research aimed to identify current system barriers to effective practice which can address the complex phenomenon of AVITH, as well as to surface the enablers which may contribute to more consistent and collaborative practice in the future. The research aimed to move practice and policy towards a considered and coalescing understanding of AVITH, given the uncertain position that it currently appears to occupy within the wider gamut of policy concerning violence against women and children. Specifically, therefore, the WRAP around families project was intended to function as a targeted “deep dive” into the community-based service response to AVITH, whereas the PIPA project’s predominant focus was the legal and wider system response.
With a focus on the aims described above, the research posed the following questions.
Research questions
- What are the co-occurring issues which present in young people and families experiencing AVITH, and prior experiences of service support to address these needs?
- What are the co-occurring issues or experiences specific to victims and survivors of AVITH, including mothers and siblings, which may be going unaddressed in standard AVITH interventions?
- What are the particular family needs which may prevent AVITH interventions from being effective?
- How are practitioners and services currently working together to address these issues in the context of AVITH responses?
- What are the system barriers and levers to collaborative ways of working for services and practitioners responding to AVITH?
The research was informed by two primary strands of data, the first being a qualitative exploration of community-based service responses through focus groups with practitioners in Victoria, a jurisdiction with an increasing focus on support for evidence-based service responses to AVITH. The second strand involved a mixed-methods case study approach examining a response to AVITH which was funded by the Commonwealth Department of Social Services and developed by Drummond Street Services (DS), a large community service organisation working with vulnerable families and marginalised cohorts in metropolitan Melbourne, as well as one large regional area in Victoria.
Part 2 of this report aims to address the first three questions through the practitioner focus groups, interviews with parents who were clients of the DS program, and examples of client complexity and needs evident on the case file review. A significant focus addresses the final question regarding barriers to collaboration, such was the substantial volume of challenges evident across the research.
Signs of promising practice are then explored in Part 3, which focuses primarily on the fourth question of how services and practitioners are working together to address these challenges. It does so by examining the complex and nuanced ways of working described by practitioners and services, and then through examples from the case files, signalling where conceptualisations and service design needs to be directed. Rather than including recommendations which may not be relevant in different service contexts, or which can so often become siloed in policy or funding environments, Part 4 of the report then discusses and proposes the Collaborative Practice Framework which was the primary objective of the research. This Framework is designed to be flexible and client-centred rather than prescriptive, reflecting the overarching emphasis of the research findings. It includes practice examples to guide policymakers and practitioners in applying the Framework totheir own particular context.
Methods
Literature scan
To support development of the research aims and methodology, a brief scan of relevant peer-reviewed and grey literature built on the literature explored in the PIPA project (Campbell et al., 2020). Important to note, this was not intended to function as a systematic or even standard literature review. Rather, it focused on evidence which became available in and following 2018 to explore considerations around service responses, including positive and effective interventions, such as collaborative, holistic and whole-of-family approaches. Other literature outside these parameters was referred to as appropriate, but not reviewed in depth. The scan was conducted in the first half of 2021 and then updated on a limited basis in 2022 using searches of the following databases:
- Attorney-General’s Information Service (AGIS Plus Text)
- Australian Criminology Database (CINCH)
- Australian Criminology Database – Aboriginal and Torres Strait Islander Subset (CINCH – ATSIS)
- Health Issues in Criminal Justice (CINCH-Health)
- Australian Public Affairs Full Text (APAFT)
- Australian Public Affairs Information Service – Aboriginal and Torres Strait Islander Subset (APAIS-ATSIS)
- Australian Family & Society Abstracts Database (FAMILY)
- Australian Family & Society Abstracts Database – Aboriginal and Torres Strait Islander Subset (FAMILY-ATSIS)
- Families & Society Collection
- ProQuest
- Google Scholar.
Boolean logic was used to connect and combine multiple key terms. The first search applied a data parameter for literature from 2018 onwards combining the terms “adolescent”, “adolescent-to-parent”, “child”, “child-to-parent”, “juvenile”, “youth”, “sibling”, “teen”, “teenager” and “filio” with “violence”, “family violence”, “abuse”, “conflict”, “violence in the home” and “aggression”. A second search, with a date parameter from 2010 to 2021, combined these terms with descriptors of intervention types, including “therapeutic”, “family systems”, “family-focused”, “case managed”, “interagency”, “collaborative”, “participatory”, “integrated”, “coordinated”, “holistic”, “multi-disciplinary”, “whole-of-family”, “wraparound”, “trauma-informed”, “intergenerational” and “restorative”. Non-English publications were not reviewed.
Studies that related to “parent-to-child abuse” and “child sexual abuse”, “adult intimate partner violence” and “general youth offending” were not included in this initial search, as the objective of the scan was to identify, describe and understand literature specifically regarding the use of violence at home by adolescents, as well as specific service responses to this phenomenon. This included some consideration and description of the quality of each study reviewed. Titles and abstracts were read to determine relevance and, following that, complete texts. Further research was found by reviewing the reference lists of key articles. Sources unavailable in English were not searched for or reviewed.
Relevant considerations from this literature scan feature throughout the Context and Discussions sections in this report, as well as the Findings sections where specifically relevant.
Qualitative research with practitioners
As noted above, the first component of primary data collection was intended to be a very targeted exploration of the contemporary service landscape in Victoria. The aim of this component was to provide breadth and context for the companion case study component and therefore it was designed to have a broad focus on how the service system was responding to AVITH at the time, including the extent to which services were working together to wrap around families, barriers to collaborative practice, and service gaps. Specifically, it was designed to update findings from the PIPA project in relation to service provision, given that the data collection relevant to Victoria for the PIPA project occurred in 2017.
The expectations when the research was originally designed and resourced was that up to 40 practitioners would participate. This group was anticipated to include practitioners working across the relatively limited number of AVITH-focused interventions operating at the time of the original study design, as well as practitioners in legal, court, restorative justice, mental health and alcohol and other drug (AOD) contexts.
Following the design of the research, however, the Victorian Government provided an injection of funding to increase capacity for AVITH-focused interventions. This was described as a response to a recognised increase in rates of AVITH during Victoria’s extended lockdown periods (State of Victoria, 2020). Although limited in its parameters, this additional resourcing contributed to a rapid growth in the number of practitioners working in this field in 2021, with the bulk of additional funding being provided to large community-based organisations already delivering therapeutic recovery support to women and children who had experienced domestic and family violence (DFV). As a result, the scope of service providers from which the research team could recruit expanded. Despite the limits of the study’s original design and funding, the research team saw this as an opportunity to explore and compare different service and organisational approaches. Accordingly,recruitment efforts were focused on those services which had previously been funded by the Victorian Government to deliver AVITH-focused interventions, as well as those which the government advised had received the additional funding at the start of 2021.
In addition to these specific providers, the research team approached practitioners providing legal assistance to children and young people; practitioners working in acute and community-based mental health services; and practitioners working in AOD-focused services as a way of testing the extent to which themes were being seen outside the dedicated program environments. This included practitioners participating in an informal AVITH Collaborative Network, which emerged in Victoria during 2021 and met online on a monthly basis. This network continued to function as a reference point to test findings from the current study from a practice perspective.
Participants were recruited through their employer organisations, with participant information and consent forms then distributed to practitioners. An online consent option was provided to enable an efficient opt-in to the research, given that so many practitioners were working from home during this period. Online focus groups were then conducted on an organisational basis, so that practitioners could speak freely about any challenges that they had experienced in developing and/or adapting responses to AVITH, particularly where these were emerging responses. Because indications of consent went straight to the research team, employing organisations were not aware of which individual practitioners participated.
To note, the initial project timeframes and resourcing – and associated targeted study focus – meant that the research team did not seek to involve statutory agencies in the research, given the additional ethical approval and organisational constraints. Equally – and crucial to note – Aboriginal community-controlled organisations (ACCOs) who had either previously or more recently been funded to deliver culturally specific interventions had very limited capacity to participate at the time of initial data collection, such was the significant additional demand on these services during Victoria’s extended lockdown periods, as well as the imperatives on ACCOs to deliver direct support to communities during this time. Because of this, the data collection period was “paused” to keep the window for participation open. Four practitioners from ACCOs delivering AVITH-focused interventions ultimately participated in the research in the middle of 2022.
Despite the additional demand facing all services responding to family safety during Victoria’s extended lockdowns – as well as the compounding challenges of providing support to vulnerable clients while working from home or with rolling illness once lockdowns were lifted – the research team were delighted that 75 practitioners participated in the focus groups within the extended timeframes. Important to note, as specific challenges related to collaboration between services and Child Protection authorities emerged across the findings, an invitation to test these findings was extended to senior Child Protection stakeholders. Given that this occurred during 2021 and across Victoria’s extended lockdowns, it is understandable that this invitation did not receive a response.
Case study component
Noting that there is little consensus on a single case study method (Simons, 2012), the label “case study” in the project referred to the in-depth examination of a particular collaborative response to AVITH being offered by DS. In this case study, the research team aimed to engage with a range of data to explore the area of study (e.g. Mack et al., 2005) and then test this through the knowledge and perspectives of practitioners, as well as the perspectives of people who had used the program.
Given the distinctive features of the particular program being investigated, the research team did not expect to be able to generalise the findings, as might occur in relation to other case studies (Gerring, 2004). More specifically, we anticipated that the findings would be instructive in relation to the emergence of innovative responses or promising practice, which the current study confirmed. The value of a case study method for investigating and evaluating innovative programs is observed by Simons (2014), who argues that case studies are useful to “understand and represent complexity, for puzzling through the ambiguities that exist in many contexts and programs and for presenting and negotiating different values and interests in fair and just ways”
(pp. 2–3). Flyvberg (2006) also argues that areas of inquiry are strengthened by in-depth case studies of best practice or promising examples.
Client interviews
The case study component originally aimed to include in-depth interviews with six to ten young people and eight to twelve adult family members. The interviews were designed to explore their experience of the DS program and the broader service system; the extent to which the program and the broader service system were meeting their needs; what responses or types of support may have been missing from either the program or the wider system; and what might have benefitted them individually and as a family.
Family case conferences, which occurred as part of the case study program between all practitioners working around the family, were used as a screening mechanism to assess whether it was safe and suitable to invite one or more members from a particular family to participate in the research. Where a client was assessed as eligible, the practitioner explained what the research involved and confirmed with the client at a later date, such as at their next appointment/session, if they would like to participate. The practitioner confirmed with the client whether they were able to attend the service premises for the interview, or whether a phone or video interview would be safe and appropriate. The three participating parents all preferred a phone or online interview, which practitioners deemed safe in their particular circumstances. At the time that they confirmed the interview time and location, the recruiting practitioner confirmed with the client that thepractitioner would also be available following the interview to provide support and debriefing by phone.
Because the data collection period ran from mid-2021 to mid-2022, through Victoria’s protracted sixth lockdown and the subsequent waves of the COVID-19 Omicron subvariants, there were significant limitations on the type of work that DS could conduct with clients. This was particularly the case with young people, who were generally harder to engage online or over the phone, and where practitioners had significant concerns about client privacy and safety during therapeutic work. This ultimately meant that recruitment to the interview component of the research was extremely challenging, with no young people expressing interest and only three parents ultimately participating in the research (three additional parents initially expressed interest but circumstances at the time made it too difficult or unsafe for them to participate). In particular, these three parents had not experienced much contact between DS and their children, two because of the impactsof COVID-19 on face-to-face engagement and another because of issues around parental consent, which is explored in the report.
As a result, findings from the three interviews with parents are featured throughout this report as illustrative only, where they echo other findings and themes. The interview findings predominantly relate to the limitations of the wider service response and, in particular, the ongoing impacts of adult-perpetrated DFV, as well as how these impacts interact with their experience of service systems. To an extent, however, they highlight the need for wraparound responses like the DS program, where circumstances enable a program to work with children and young people.
Case file review
The file review aimed to examine the case files of approximately 40 families engaged with the DS Family Violence and Young People program in relation to their experience of AVITH. This program purposefully takes a whole-of-family approach which enables different family members to engage with the program on a separate case file from the young person. This was described to the research team as taking a strengths-based and person-centred approach, particularly where a young person identifies that they would feel more comfortable engaging without the presence of their parents. Taking this approach allows for the consent of the young person (and of parents where the young person is under 16 years old).
The case file review aimed to examine:
- families’ demographic data, risk factors and co-occurring needs
- where and how families experiencing AVITH were presenting to services
- family structure and dynamics, including multidirectional use of violence
- the nature and extent of prior service contact and engagement, including in relation to prior experiences of trauma and violence
- how prior experiences of trauma and violence may be impacting on the family, including where mothers’ experiences of violence may be impacting parenting behaviours
- the under-examined needs of siblings experiencing AVITH and its multiple impacts across the family structure and relationships.
The research team was ultimately provided with case files in relation to 39 families engaged through the program. Six were then excluded once initial analysis indicated that they did not demonstrate sufficient engagement with the family as a result of the same COVID-19-related impacts described in relation to the client interviews, or for other reasons.
Ethical considerations
Ethical approval for all components of the research was sought and received from the Victorian Department of Justice Human Research Ethics Committee (CF/21/5126). Approval from this committee was sought because of the vulnerability of clients in the DS program and the potential for any young people participating in the case study to be a respondent to a civil protection order and therefore formally a client of the justice system.
Focus groups with practitioners
Specific to the focus groups, the research team recognised that practitioners working in this area may experience vicarious trauma as a consequence of empathetic labour. The research team also recognised the low risk that some practitioners participating in the research may have lived experience, including histories of trauma or experiences of DFV. Accordingly, the research team designed the project to minimise the potential to impact practitioners in negative ways by:
- ensuring that interview questions did not direct or encourage practitioners to recount specific incidents or histories of trauma
- redirecting the discussion in the event that a particular question or topic was resulting in distress, including by reframing the discussion to focus on client strengths and factors contributing to positive client outcomes
- using other techniques as required, including offering to take a break or to reconvene the interview at a later time.
While the research team have extensive experience in trauma-informed approaches to data collection, it is important to note that there were no indications of negative experience for participants across any of the focus groups. Rather, the overwhelming assessment of their experience of participation was expressed by practitioners as extremely positive, with regular indications of appreciation for the opportunity to share reflections and to do so in a collegiate environment. This was particularly because these opportunities had not been a common feature of their experience in recent years, such was the focus on responding to caseloads and service demand compounded by the impacts of COVID-19.
These reflections from practitioners are consistent with contemporary methodological observations about the benefits of co-production of evidence with practitioners and service providers (Breckenridge & Hamer, 2014; Coutts, 2019; Simons, 2012), also positioning the research more effectively to be translated to benefits in policy and practice (Belzile & Oberg, 2012), which was the reason for the selection of focus groups as the method for this component of the research. To note, practitioners were given the opportunity to participate in an individual interview, including as a way of ensuring that their decision to participate was not communicated either to colleagues or to their employer organisation, but all preferred to discuss their evolving practice in a group setting. Given this, the research team adopted the approach of assigning each practitioner an identifying number, rather than identifying the type of service in which they worked. Thiswas to minimise any chance of them being identified by their employing organisation or re-identified by others who had participated in that particular focus group.
Client interviews
The research team’s approach to qualitative research with vulnerable participants is to recruit through agencies which are already providing them with support.
This is because these practitioners have a sufficient understanding of clients’ needs and circumstances to determine whether it is safe and appropriate to seek to recruit a client at a particular point in time. This includes, for example, not seeking to recruit a client where they have a matter before a court at that time; they are experiencing increased family violence risk; they are at risk of re-traumatisation; or they are otherwise experiencing significant instability, such as homelessness. Risk factors were considered individually and at a whole-of-family level. These methods of recruitment ensure minimal risks of potential harm to the participant.
Benefits of recruiting this way also include practitioners being able to identify additional supports that may facilitate participation in research for people with complex needs – thereby minimising the extent to which marginalised cohorts are excluded from research. This method of recruitment also ensures that participants have a trusted practitioner from whom they can receive debriefing, rather than having to re-tell their story to a stranger. The research team has designed this methodology in consultation with practitioners over the course of multiple studies as a way of ensuring that participants who may not otherwise be included in research have the opportunity to do so, while feeling comfortable about declining the invitation where they have developed a rapport with a worker but have concluded their program engagement.
Interview questions were designed to focus on a participant’s experience of the DS program and wider service system, as well as their support needs, rather than their experiences of AVITH or sources of trauma. This reflected the research team’s trauma-informed and strengths-based approach and an emphasis on conducting research with participants as experts in the service system, rather than as passive subjects. That said, all three parents volunteered extensive histories of trauma related to adult-perpetrated DFV, a theme which had an impact on every aspect of their service interaction and the most substantial theme to emerge from the client interviews, as discussed throughout the report.
At the conclusion of the interview, the principal chief investigator (PCI) conducting the interviews inquired about further support needs, and one participant expressed an interest in debriefing with a practitioner and reconnecting with the DS program, which the PCI arranged. All participants expressed an appreciation for the way that the interviews had been conducted and for the opportunity to have a voice, with one parent explaining, “I would really love to see some change for other people going through this” (Parent 1). Participants were all provided with a voucher as a thank you for their time and will all be provided with a copy of the research upon completion. They were also reminded that they could request a copy of the transcript of their interview from the PCI at any time.
Case file review
Quantitative and qualitative information was extracted from existing case files via two case file review tools developed for the study, which related to the program’s primary and secondary clients. Information collected did not include names, dates, unique client identifiers or other information that was likely to make the person whose information was being collected identifiable. Different family members were referred to by different case numbers but were linked in the data provided to the research team. Information was only extracted from the case files of clients who had consented to their information being used for research and evaluation purposes. Data was collected by Centre for Family Research and Evaluation (CFRE) researchers who came within the scope of DS’s client consent processes while still being sufficiently independent from service provision as to mitigate the risk of reporting bias.
Only de-identified data, as captured through the case file review tools, was shared with the broader research team. To reduce the potential identifiability of qualitative data, the case file review tool included instructions to exclude information which, based on the relevant CFRE researcher’s judgement, would likely have the effect of making the client identifiable. Information was only recorded using the approved tools, with no additional information recorded. Data analysis was then tested with the CFRE researchers through formal data reflection sessions to ensure that the way in which data was analysed was consistent with DS’s informed consent processes. This process also enabled the wider research team to test wider findings and explore data gaps.
Data analysis
Focus groups
Anticipating the benefits of co-production of evidence noted above, focus groups were the preferred approach. Because of the analytical value of discussions and interactions between participants, as well as the fact that focus groups are an efficient way of accessing a significant number of participants (Peek & Fothergill, 2009), the research was designed as a genuinely collaborative endeavour to understand the current response to a policy and service challenge which is yet to receive a consistent intervention.
While the research team recognised that a single data type may be a potential limitation, they also anticipated and observed an immediate and organic process of data integrity-testing occurring in many focus groups, where participants disagreed with each other or, conversely, extended or tested a point, drawing on their particular expertise or location in the system. The research team also actively included memo-ed reflections of group dynamics as a valuable dimension of the data (Pösö et al., 2008; Warr 2005). This included noting that group dynamics were impacted by a range of organisational and systemic imperatives outside the relationships within the group.
Focus groups were recorded via Microsoft Teams, with transcripts then downloaded and checked against the audio recording for accuracy. Transcripts were analysed thematically using the qualitative analysis software NVivo, with data coded in accordance with 22 nodes. These nodes were tested against memo-ed reflections taken by different members of the research team and workshops with the PCI for reliability, as well as being checked by the PCI in a manual review of the transcripts. Emerging themes from the coding were then further tested with the AVITH collaborative network, mentioned above, for practice relevance, as well as with the focus group participants in the context of their participation in the workshops that were held to inform the development of the Collaborative Practice Framework.
Focus group participants were given an individual number during the coding to ensure that their contributions could be tracked. These numbers have not been linked to organisational identifiers to limit the extent to which participants could be re-identified, particularly as many contributions were quite critical of the funding environment that was in operation at the time.
The analysis was informed by broad feminist theory and critical theory (Fraser, 1985; Wellmer, 2014), with the research team maintaining a constant interrogation of choices of terminology and assumptions at the inception of and throughout the research, as well as the conceptualisations about AVITH to which services were attempting to respond. This critical lens extended through to the nuance incorporated and reflected in the Collaborative Practice Framework that was the ultimate product of the research.
Client interviews
As noted above, three clients participated in interviews, which lasted an average of 90 minutes each. Interviews were recorded, downloaded and transcribed before being analysed and coded, ultimately resulting in 11 nodes. The predominant nodes were the impacts of trauma from past adult-perpetrated DFV as well as ongoing systems abuse by a perpetrator parent, followed by support needs of young people and negative prior service interaction. The relatively small number of nodes and their nature resulted from the limits on these particular clients’ engagement with the DS program, despite the fact that DS had been able to engage more extensively with the 33 families whose case files were reviewed.
As a result, the majority of the data from client interviews is featured as illustrative in Part 2 of this report, which focuses on practice and system challenges, given that they relate to clients’ experiences of prior service interaction, as well as what their hopes would be for interaction in the future. This was considered to be a more appropriate and ethical use of the contributions of these participants than combining them with the findings of the case file review, which was predominantly focused on the various ways in which DS had been able to work effectively with other clients.
Although this was not the original aim of the study, the ultimate result provides a useful contrast in terms of the lived experience of those seeking to access support for their experiences of AVITH.
Case file review
DS provided the external research team with 39 case files. Of those 39 files, six were ultimately excluded once initial analysis indicated that minimal engagement by the family or other factors limited the extent of information available for full analysis and comparison. In total, the case file review included files related to 33 families – with each “file” including a mastercase and secondary cases linked together.
The breadth of data within each case file varied for several reasons, including the extent of engagement that families had with DS; the variation in record-keeping practices by individual DS practitioners; and variation in the number and nature of sessions held between a DS practitioner and a family. For example, within the 33 files reviewed, the number of sessions held between DS and the client ranged between two and forty-one, where the young person was engaged with other support (e.g. a psychologist); where DS may have been unable to make contact with the family again following intake; or, in some instances, where the violence had improved after only a few sessions and the case was closed.
A database was created, with basic descriptive statistics extracted from the quantitative component of the file review tools and recorded using Excel. This was to give context to the primary focus of the review, which was to conduct a qualitative exploration of client presenting needs and the corresponding DS approach to practice in response to these needs. Data from the qualitative component of the file review tools was analysed thematically using the qualitative analysis software NVivo, with data coded in accordance with five primary nodes or themes, and 15 sub-themes. Two further manual reviews were conducted to cross-check for error or duplication.
Additional project oversight
In addition to the collaborative approach taken by the research team across the focus groups, the research was also overseen by an advisory committee with representatives from Safe and Equal (formerly Domestic Violence Victoria), No to Violence, the Children’s Court of Victoria, the Commission for Children and Young People, Youthlaw, Victoria Legal Aid, and Djirra (a service providing family violence legal advice and prevention services to Aboriginal women and children). Djirra had limited capacity to attend meetings, however, because of the ongoing impacts of COVID-19. The research team also explored opportunities for a parent/carer or young person with lived experience to be involved in the advisory committee. Potential participants were approached through three service pathways once considerations around their safety were assessed but, ultimately, all decided that they were not yet comfortable acknowledging their experiences in a group setting. Thispotentially reflected wider challenges in this area in terms of the particular stigma that people who have experienced or used AVITH may feel and the impacts of this on their capacity to receive support.
Context: An evolving service environment
The following section provides a brief outline of the extent to which AVITH is recognised in literature. It also contains a brief discussion of wider service contexts and growing recognition in the literature that responses which address need and wrap around a whole family are required. Finally, the section outlines the evolving service and policy landscape in Victoria to provide context for the subsequent findings. The service landscape, as with the legal response, is dictated to an extent by the broad definition of family violence in Victorian legislative and consequent policy settings, which have captured use of family violence by a range of family members since 2008.
Conceptualisation and recognition in literature
The varying conceptualisations and definitions of AVITH across literature make assessing prevalence and dynamics a challenge, with researchers highlighting the importance of establishing consistency in understanding what constitutes AVITH (Peck et al., 2020).
Different jurisdictions, services and studies adopt varying age ranges when assessing and defining AVITH, generally starting at 10 or 12 years and ranging up to 17 or 25 years, with further variation in whether the context is legal, clinical or community based (Campbell, et al., 2020). Studies have also highlighted the value of maintaining visibility of the behaviour of pre-adolescent children as a predictor of behaviour in adolescence (Rutter, 2020), while a recent Australian study found that, of a sample of 435 university students aged 18 to 25, one in seven had used harm against their parents in the past 12 months (Simmons et al., 2020).
A frequently cited definition by Cottrell (2001) defines AVITH as an abuse of power perpetrated by adolescents against their parents, carers and/or other relatives including siblings, which “occurs when an adolescent attempts to physically or psychologically dominate, coerce and control others in their family” (page 3). Holt subsequently specified a requirement for a “pattern of behaviour that produces harmful outcomes [emphasis in original]” (Holt, 2016, p. 2) rather than an isolated incident.
A more recently developed definition by Pereira and colleagues builds on these definitions and signals an emerging consensus as to the circumstances and behaviours that they suggest should be within scope:
Repeated behavior of physical, psychological (verbal or non-verbal) or economic violence, directed toward the parents or the people who occupy their place. Excluded are one-off aggressions that occur in a state of diminished consciousness which disappear when upon recovery [sic] (intoxications, withdrawal syndromes, delirious states or hallucinations), those caused by (transient or stable) psychological disorders (autism and severe mental deficiency) and parricide without history of previous aggressions. (Pereira et al., 2017, p 220).
We note, in particular, the specific exclusion suggested by Pereira and colleagues of what they term “autism and severe mental deficiency”. This is particularly relevant when considering prevalence and dynamics given that young people with disability are currently captured within the rates of AVITH reported in Victoria because of the operation of the Family Violence Protection Act 2008 (Campbell et al., 2020). Accordingly, it is important to acknowledge that policy contexts and policing practices further impact prevalence estimates (Kehoe et al., 2020). For example, studies indicate that young people identified as using AVITH in legal settings appear to have more entrenched behaviour and histories of adverse childhood experiences compared to young people whose parents have the resources to opt for private clinical support (Loinaz & de Sousa, 2020).
Recent Australian research also confirms that young people in contact with criminal justice systems for use of AVITH have backgrounds of particularly entrenched disadvantage, including young parenthood, histories of child removal, mental ill health and disability. Young people from Aboriginal and Torres Strait Islander backgrounds featured to a notable extent in the data included in an important recent Australian study (Douglas & Walsh, 2022).
Legal system samples are commonly used to measure AVITH prevalence and one example – a study of police data across four Australian states – indicated that between 1 and 7 per cent of DFV matters reported to police involved AVITH (Moulds et al., 2019). An examination of justice data for the Royal Commission into Family Violence (RCFV) reported that approximately 10 per cent of DFV police reports involved AVITH (State of Victoria, 2016). Similarly, between July 2019 and June 2020, around 10 per cent of individuals recorded by Victoria Police for DFV incidents were between the ages of 10 and 19 (Crime Statistics Agency, 2020).
The PIPA project, however, found that variations contained in the legal and court files reviewed suggested that justice data did not necessarily provide useful measures, because young people who were identified as respondents through the Victorian protection order response should arguably be excluded from the definition of AVITH by Pereira and colleagues because of cognitive impairment, current victimisation or behaviours not meeting the legislative definition of DFV (Campbell et al., 2020). This complicated rather than clarified questions about prevalence, at least in the Victorian context.
Under-reporting is also a compounding factor, with AVITH described in studies as one of the most significantly under-reported forms of DFV (Campbell et al., 2020; Fitz-Gibbon et al., 2018; Kehoe et al., 2020). Kehoe and colleagues attribute this to “a lack of community acknowledgement and understanding”, as well as “parental guilt, denial, self-blame, stigma and shame, and the minimisation of the abuse as being ‘typical’ adolescent behaviour” (Kehoe et al., 2020; Meyer et al., 2021). Despite the effect of under-reporting, some international studies indicate that AVITH is a growing phenomenon (Contreras et al., 2019), resulting in associated investment in assessment instruments.
Extensive evidence across different samples and settings (Pagani et al., 2004; Routt & Anderson, 2016) describes prior experience of adult-perpetrated DFV, both indirectly and directly, as arguably the most significant contributor to a young person’s use of AVITH (Armstrong et al., 2018; Beckmann et al., 2021; Campbell et al., 2020; Contreras & del Carmen Cano, 2016; Elliott et al., 2017; Holt, 2013; Holt & Retford, 2013; Howard & Holt, 2015; Ibabe et al., 2013). The presence of victimisation features in studies across different settings, with this experience among young people who use AVITH found to be higher than in comparable cohorts of young people (Contreras & del Carmen Cano, 2016).
Evidence links to theories of intergenerational transmission of violence (Kwong et al., 2003; Meyer et al., 2021) and “social learning”, whereby young people observe behaviours used by adults in their lives and replicate them (Margolin & Baucom, 2014) – for example, once a perpetrator father has been removed or the family has separated. Other explanations include resistance (i.e. acting out towards a perpetrator) or protection (i.e. trying to protect an abused parent; Margolin & Baucom, 2014), or observation and replaying of behaviours used by older siblings (Campbell et al., 2020).
Interwoven with the impacts of social learning is evidence of the ways that adult perpetrators of DFV deliberately undermine relationships between mothers and children (Bagshaw et al., 2011; Brown, 2006; Burck, 2021; Burck, et al., 2019; Maher et al., 2021; Meyer et al., 2021; Katz, 2019; Spearman et al., 2022; Thiara & Humphreys, 2015), including post-separation. Examples involve systems abuse through the family law and Child Protection processes; using children as a vehicle for abuse tactics; and otherwise using shared parental responsibility and an ongoing, “absent” presence to undermine the mother–child bond or a child’s access to services (Campbell et al., 2020; Thiara & Humphreys, 2015). An increasing volume of literature therefore seeks to make the gender of victims and survivors far more visible (Armstrong et al., 2021; Burck, 2021; Meyer et al., 2021) and, accordingly, support women’s recovery (Burck, 2021; Paterson, et al., 2002).
This is particularly important to note when considering the gendered nature of AVITH. While research highlights that young people using AVITH are more likely to be male than female (Campbell et al., 2020; Condry & Miles, 2014; Holt, 2016; Howard, 2015; Routt & Anderson, 2011), the gendered nature of the use of AVITH is less conclusive and perhaps more complex than evidence clearly indicates in relation to the gendered nature of adult-perpetrated DFV (Australian Domestic and Family Violence Death Review Network & Australian National Research Organisation for Women’s Safety, 2022).
For example, a recent prevalence study indicated that respondents identifying as female were more likely to self-report using AVITH than young males (at 23% of females compared with 14% of males; Fitz-Gibbon et al., 2022). Here it is worth noting that young women may be more likely to self-report any kind of violence compared with males, as suggested in the context of wider evidence regarding adolescent dating violence (O’Keefe, 2005). Other research has also noted use of serious physical violence by young females in the context of histories of complex and sustained trauma, with participating practitioners in this particular study suggesting that young girls are more likely to be identified and met with punitive responses where they break with gendered norms (Campbell et al., 2020). Conversely, other studies have suggested that parents may be more likely to report the use of AVITH by young males given the perceived risk of physical harm (Miles &Condry, 2016).
Despite this complexity in terms of the demographics of who is using AVITH, it is perhaps the gendered nature of victimisation – with the vast majority of victims and survivors being mothers – that is a more relevant area of focus for service provision and policymaking alike. This is in part because, as noted above and discussed in some of the below examples, available evidence points to the value of interventions which support mothers and their children in healing from trauma and in working towards safety for all.
Examples of approaches interstate and internationally
A range of programs have been developed to respond to AVITH in both the Australian and international contexts, with the following discussion providing examples of contrasting approaches. This sample is by no means intended to be exhaustive, acknowledging the substantial literature exploring a range of interventions in a number of diverse jurisdictions, particularly the United Kingdom and Spain (Holt, 2016).
Group work with parents and young people
The Step-Up model, established in the United States in 1998, involves group work interventions with court-involved young people and their parents, and has become influential internationally (Gilman & Walker, 2020; Routt & Anderson, 2016). The Step-Up program uses a restorative approach where the young people are encouraged to take responsibility and accountability for their use of harm while also repairing damaged relationships and safety planning (Routt & Anderson, 2011, 2016).
In their evaluation of the program, Gilman and Walker (2020) looked at the outcome of general and DFV-related recidivism within 12 months of program commencement and found that participation was associated with a reduction in future court referrals overall, but not specifically for DFV-related offences, after controlling for variables. The authors observed, however, that previous evaluations – although not as methodologically rigorous – have found some evidence of reductions in ongoing use of violence in the home (Gilman & Walker, 2020). It should be noted here that eligibility criteria for the US iteration of Step-Up include that the young people have had some involvement with the criminal justice system; are not currently experiencing, or have not in the past experienced, violence from the parent towards whom they are currently using violence; and that all participants (young people and parent) do not have a current substance abuse problem or anuntreated mental health issue (Gilman & Walker, 2020).
As is evident from current literature, as well as the findings from this project, many instances of AVITH involve young people being both a victim and survivor and using violence, and many families experiencing AVITH also experience substance abuse and mental health issues (Campbell et al., 2020). This suggests that, unless modified to accommodate families experiencing multiple complexities in addition to AVITH, the US Step-Up program may not be sufficient as a response to AVITH if delivered in isolation and would need to be linked to more holistic and integrated responses.
Another well-established program working with parents and young people together is the Respect Young People’s Programme (RYPP), an intervention for families where children or young people aged between 8 and 18 use harm towards the people close to them, particularly their parents or carers. Delivered by the Respect agency in the United Kingdom, the program describes itself as working with young people and their families; encouraging everyone to take a role in stopping the abuse; and learning respectful ways of managing conflict, difficulty and intimacy.
The RYPP is currently delivered across a number of local authorities and police and crime commissioner areas in England. The RYPP involves weekly structured sessions for 18 weeks (nine sessions with the young person, seven sessions with the parents and two sessions with the family together), with the sessions lasting up to an hour. Using a multi-modal design and combining a range of theoretical models with primarily a cognitive behavioural approach, the program also aims to influence particular features of the young person’s environment which may contribute to use of harm. Prior to the group work sessions starting, Respect offers two pre-work sessions, in order to support engagement and buy-in to the program by the young people and their parents. The aim of this is also to complete a full risk assessment and ensure program suitability. Respect is also conducting work to develop appropriate interventions for young people who are neurodivergent or havecognitive impairments (Respect, 2021); while a case study of the program’s delivery during COVID found that, while young people were difficult to engage during this time, engagement by parents increased (Rutter et al., 2022)
Programs which work primarily with parents
The “non-violent resistance” (NVR) model used in the United Kingdom and the Republic of Ireland works primarily with parents and seeks to move away from blaming either parents or young people and to “take account of the challenges of parenting in the context of cultural beliefs about parenting practices, relationships between parents and children, and supports for parents and children” (Coogan, 2018, p. 170). Practitioners work with parents over the course of eight to fifteen sessions to address reversed power dynamics in the family, address the patterns of escalating violent behaviour, and focus on reducing isolation and helplessness (Coogan, 2016).
The model aims to empower parents to focus more on aspects that they can control, such as the ways that they respond to the behaviour (Coogan, 2016). Reviews and evaluations of this model, although limited in scope and sample size, have found that it generally “improves parental wellbeing, decreases parental helplessness and leads to positive improvements in the child’s behaviour” (Coogan, 2016, p. 7). Important to note, practitioners participating in these evaluations acknowledge that the use of NVR is not designed for families experiencing multiple vulnerabilities (Coogan, 2016).
The Break4Change model in the United Kingdom is partially based on the NVR model, although it incorporates interventions which directly involve young people as an additional component, teaching emotional regulation skills. Although there is no publicly available evaluation, the Centre for Justice Innovation reports that, following the program, parents feel less isolated and more confident, and have skills to address their child’s behaviour, while young people “reported having increased empathy, drastically reduced physical violence and increased satisfaction at home” (Centre for Justice Innovation, 2021).
Programs which work with mothers and sons who have experienced adult violence
The ReNew program in Queensland is a therapeutic program directed at working with mothers and their sons aged 12 to 17 who have experienced DFV from an adult perpetrator, usually a father, and are now using violence towards their mothers (Burck, 2021). The first iteration of the ReNew program was trialled in 2016, with a partnership between a family support service and specialist DFV service funded to deliver the program for a two-year pilot. The pilot used three different group work components: combined groups with mothers and young people as well as separate groups with mothers and young people, respectively (Burck, 2021).
The trial was evaluated by Griffith University, with a favourable interim report resulting in an extension of the trial. This included an external co-design process to review and build upon the existing model.
ReNew was specifically informed by evidence which shows that experiences of adult-perpetrated DFV can severely undermine the mother–child bond. The primary goal of the program has therefore been described by one of its founders as “to reduce violence in the home through strengthening the mother/son attachment after experiencing [intimate partner violence]” (Burck, 2021, p. 57). The program also recognised that mothers can feel further shamed and blamed when they are not included in any work occurring with young people (Jackson, 2003 as cited in Burck, 2021, p. 57). ReNew therefore aims to intervene at a critical juncture to rebuild respectful relationships between mothers and their sons, following experiences of DFV; to increase attachment; and to reduce the risk of young people using DFV as adults.
The research team has been informed that the current ReNew program involves two stages, as follows:
- In phase one, risk is assessed in relation to the violence used by the adult male perpetrator and the young person. The needs of the family are assessed, so that decisions can be made as to whether families should undertake a psycho-education program, either individually or in a group. Sons between the ages of 12 and 17 are eligible to participate in the psycho-education program.
- Upon completing a 10-week program, mothers and sons attend a second service for onboarding and orientation, before entering into the therapeutic element of the ReNew program, which applies an attachment and trauma focus to rebuilding relationships between mothers and sons.
- Both phases of the ReNew program can be delivered individually or via a group format. The intervention is dependent on the two services working in a collaborative partnership to deliver one cohesive intervention for mothers and sons, while providing wraparound support for other family members, such as siblings.
The implementation and delivery of the revised ReNew program is also subject to an evaluation and the research team understands that preliminary findings highlight that the program addresses an under-met service delivery need.
In particular, a strong theme from the program described by one of its designers and facilitators is enabling mothers and their sons to form positive memories and have safe interactions which can gradually rebuild their views about their relationships, as well as their views about themselves. Burck cautions against defining a young person by their use of violence, urging instead that “We, as professionals, must care for the young person while holding them accountable for the violence” (Burck, 2021, p. 66).
Programs which work with young people involved in justice settings
The KIND program was piloted in South Australia and offered a voluntary intervention to young people involved in youth justice contexts who have used AVITH or adolescent intimate partner violence. Evaluated by Moulds and colleagues (2019), the program worked with the young people and their families and partners, with a combination of group and individual sessions occurring weekly over three months and incorporating therapeutic and educational activities. It primarily focused on physical forms of abuse and incorporated cognitive behavioural therapy and some elements of acceptance and commitment therapy, as well as restorative practices, with the understanding that violence is a learned behaviour which can be unlearned through teaching new skills to manage behaviour. The program aimed to be trauma-informed, individually tailored and culturally sensitive, especially given the over-representation of Aboriginal and Torres Strait Islander people in thejustice system.
The early iteration of the KIND program only included young people aged between 15 and 18 years and who were subject to a youth justice order. It also excluded young people who had used sexual violence and who were themselves victims of DFV. The program was piloted in 2017 over seven months and received 27 referrals, although only nine young people and their families participated. Acknowledging the small sample size, the evaluation found that satisfaction, communication and coping skills within families were improved; attitudes towards violence were altered; and safety plans were able to be developed. Important to note, Moulds and colleagues (2019) also found that factors such as mental health, housing and substance use were outside the scope of the program and hampered progress in some cases. The KIND program was additionally limited, as noted above, in terms of its inclusion of participants within only a small age range and a requirement for youthjustice involvement.
The research team understands that there were significant developments made in relation to the KIND program in 2021, during which the program was revised and implemented again with broader inclusion criteria. It is now being rolled out in several sites across Queensland as well as in South Australia. An evaluation of the program is being conducted by Griffith University over the course of 2022, funded by the Australian Institute of Criminology.
Multidisciplinary or collaborative responses
Reflecting limitations to some of the programs described above, attention is increasingly being drawn to service design capable of addressing multiple needs and ensuring that barriers to engaging hard-to-reach families are addressed. This includes service design where challenges experienced by young people and/or their families who are in crisis or who are unable or unwilling to engage with services can be overcome and where basic communication and life skills can be developed to contribute to improvements in family functioning (Kehoe et al., 2020).
Given that families are likely to be experiencing multiple co-occurring issues, the literature increasingly suggests that multisystemic or “ecological” responses (Shanholtz et al., 2020), which include work with the young person, their family and their wider social environment, are most likely to be effective. As part of a community-based participatory research project in the United States, for example, Shanholtz and colleagues (2020) sought the views of court staff, as well as young people and families attending mandated DFV education classes, on helpful responses to AVITH in court settings. Participants stressed the importance of providing support across the family to help to foster more positive intra-family relationships, as well as to address wider environmental factors impacting the family (Shanholtz et al., 2020). Researchers have also emphasised the need for interdisciplinary collaboration to develop a framework for defining, measuring andaddressing AVITH across different sectors (O’Hara et al., 2017). Arguably this framework also needs to make a clear distinction between AVITH and broader DFV.
Kehoe and colleagues (2020) further advocate for AVITH to be viewed as a health, rather than a justice, issue – one that child and youth mental health services, when adequately resourced, are well placed to deliver. Drawing on findings from a 2019 study involving consultations and a co-design workshop held with key stakeholders − including a small sample of parents and young people with lived experience of AVITH − the study identified a wide range of co-occurring needs across families experiencing AVITH. In combination, these needs meant that families presented as “complex” and fell through service gaps (Kehoe et al., 2020, p. 348). By contrast, the study highlighted the need for interventions that are:
- trauma-informed, inclusive and family-focused, ensuring that all family members have access to services to address issues relating to intra-family conflict and communication, as well as other issues impacting on family health and cohesion, including school disengagement, disability, substance dependence and mental health issues
- provided under a multidisciplinary, specialist and case-managed model
- flexible and tailored, with therapeutic needs determining the nature of the response, ranging from a single session to up to 12 months.
The findings also emphasised the need for early intervention, with proactive outreach seen as essential to ensure that services are accessible for disengaged young people, or young people experiencing homelessness as a result of the violence (Kehoe et al., 2020). The establishment of a peer workforce, support groups for families and an awareness campaign to help reduce stigma and increase help-seeking were also raised as important in the design of specialist AVITH programs (Kehoe et al., 2020).
More broadly, evidence increasingly points to the importance of trauma-informed and culturally responsive interventions in contexts where young people may be using a range of challenging behaviours.
This includes therapeutic kinship care programs which can respond to and address intergenerational trauma (Kickett et al., 2019), as well as programs which can take account of the historical and interconnected nature of violence across family structures, including where sibling violence may be present (Perkins et al., 2021), where grandparents may be caring for grandchildren (Gair et al., 2019), or where relationships across generations impact on a young person’s use of violence (Shannahan, 2017).
Research continues to confirm the importance of context for young people in their families, indicating a strong connection between individual and collective experiences of marginalisation or disadvantage (Blakemore et al., 2018), in turn requiring a multisystemic response which can take account of this context in sufficiently creative, collaborative and culturally inclusive ways (Blakemore et al., 2018).
Unsurprisingly, studies increasingly suggest that positive relationships within a family offer a significant protective factor against AVITH, and that a focus on rewarding desirable and positive behaviour improves results (Beckmann, 2020; Elliott et al., 2017; Kehoe et al., 2020). The existence of certain factors, such as parental warmth, have been shown to serve a particular protective function in preventing the use of AVITH by young girls (Beckmann et al., 2021; Zhang et al., 2019).
The importance of protective factors and resources in a young person’s wider environment, such as strong attachments with teachers or peers, has also been highlighted (Beckmann, 2020; Nam et al., 2020), as has school engagement generally. In particular, evidence points to addressing external risk factors – such as reducing bullying victimisation at school – as well as supporting the development of prosocial skills in parents as significant protective factors in reducing AVITH (Espejo-Siles et al., 2020).
Factors such as these are well understood by services providing interventions in AVITH, which frequently highlight the value of working with parents to support the development of coping skills and positive ways of interacting with their child. These include seeing past the trauma of their child’s use of violence to see the strengths and positives in their child, rather than their child as just a replica of a former partner using violence.
Wraparound interventions: A research gap
Certainly, wider community-based responses are increasingly moving towards integrated responses to families experiencing marginalisation or safety concerns (McDonald et al., 2011; Robinson et al., 2011, Robinson & Miller, 2012). This focus on integrated and whole-of-family responses contrasts to an extent with the limited inclusion criteria for participants in some of the programs reviewed for this project. While several of these studies were promising in various ways, therefore, this suggests that a response which is accessible to everyone who experiences AVITH and seeks help is required, regardless of the complexity of their needs.
An example of a service which appears designed to respond to multiple issues, the YUVA (Young People using Violence and Abuse) young people’s service, operates across six local authority areas in London and provides support to young people aged 11 to 18, as well as for young people up to age 25 who have additional needs. YUVA emerged from a gap in service provision identified by services which were encountering both AVITH and adolescent intimate partner violence and which felt caught in the divide between youth-focused interventions and mainstream DFV services. Although the service does not appear to have been formally evaluated, research conducted in relation to the service notes that the majority of referrals (84%) involve young people requiring assistance with a range of issues including substance use, disability, experiences of abuse and DFV, learning difficulties, caring responsibilities, and criminal justice involvement. This is in addition tosubstantial support needs across the wider family, with a history of intra-familial violence being the most common support need (McGeeney et al., 2016, p 120).
Practitioners reflecting on the service in this particular study noted that the breadth and complexity of issues with which families were presenting demanded a flexible, holistic and joined-up approach, where services are provided in parallel across the agency and in partnership with external providers (McGeeney et al., 2016). Similarly, practitioners noted that, while the service’s location within a mainstream DFV service allowed them to draw on established ways of working with perpetrators and victims and survivors, the complexity of need in this area necessitated the development of new conceptual models and a range of skillsets across whole family structures (McGeeney et al., 2016).
One of the PIPA report’s key recommendations was for services to develop capacity to build trust and engagement over longer term periods of between six and 12 months (Campbell et al., 2020). Although this is outside the scope of many of these models, developing capability for longer term service engagement is needed to keep families and young people from falling through service gaps, particularly those who may take longer to trust a service or a practitioner when there is trauma or other complexity involved, or where system harm has compounded this harm. Outreach models were also recommended over compliance-based models to improve engagement and compliance with treatment and build trust (Campbell et al., 2020).
Further indications from the literature above point to the imperative of addressing the trauma and damaged relationships in mothers and children who have experienced adult-perpetrated DFV, including by providing opportunities to develop positive memories and an identity which is about things beyond the harm (Burck, 2021). While Shanholtz and colleagues (2020) argue that multisystemic approaches which include the whole family therefore require intensive resourcing, other researchers acknowledge the following:
Programs that do not address other issues, such as mental health, previous trauma, and family dysfunction are unlikely to have an impact on youth, with coordinated, tailored approaches targeted at the youth and their family the most effective. (Fellmeth et al., 2013 as cited in Moulds et al., 2019, p. 2)
Victorian policy and legislative landscape
AVITH has gained particular awareness in Victoria after the RCFV identified it as a growing concern. Statistics in relation to DFV police reports and highlighted by the RCFV, however, are in many ways related to the broad legislative definition of DFV in Victorian legislation. The Family Violence Protection Act 2008 (Vic) sets out that “family violence” – as it is referred to in the Victorian context – can be perpetrated in the context of a wide range of family relationships, including by young people.
Further, a proactive code of practice requires members of Victoria Police to bring an application for a civil protection order on behalf of someone who they consider may be at risk of experiencing future violence (rather than recommend that the individual bring an application themselves; Victoria Police, 2017). Combined, this broad legislative definition and proactive policing approach has led to a relatively consistent rate of police attendance at DFV callouts resulting in applications for protection orders being brought against young people in the jurisdiction of the Children’s Court of Victoria.
Concerns and challenges in relation to this trend – including the relevant legislation’s failure to require a court to consider a respondent’s capacity to understand or comply with an order – are discussed in detail in the PIPA project’s report (Campbell et al., 2020). As noted above, this earlier ANROWS study explored the combined legal and service response to AVITH in three Australian jurisdictions which, at the time of the study, had distinct legislative and policy settings. The weight of the PIPA project’s analysis focused on legal responses and, in particular, on the way in which the Victorian response may “miss the mark” because of its failure to consider young people’s prior experiences of trauma or their developmental capacity (Campbell, 2021). It also outlined the associated service landscape, which was arguably attempting to stem this harm, but not linked in consistent ways with the legal response.
Victorian service landscape
At the time of the PIPA project, the service landscape reflected the policy settings that had evolved in Victoria, with a lack of systemic responses leading to some organisations developing their own programmatic responses. These included various iterations of a family systems therapy approach delivered by Anglicare, in addition to the Breaking the Cycle program, a manualised, therapeutic, group work program for parents of young people who use AVITH. This program involves facilitated group meetings for parents, with a range of therapeutic activities, occurring once per week for eight weeks. The group work has a primary focus on safety while removing blame from parents, empowering them to strengthen intra-familial relationships, and holding the young person responsible for their behaviour and for changing their own behaviour to regain respect in the parent–child relationship. The program relies on the premise that positive changes that the parents makewill promote change through the whole family system, particularly where young people using violence are often reluctant to engage with services.
While more recent evaluations of the program are not publicly available, an early published evaluation by Wilks and Wise (2012) points to positive outcomes, while also suggesting that skills learnt in the program may take time to develop and be implemented in the home.
Step-Up in Victoria
In addition to programs specific to particular organisations, such as Breaking the Cycle (above), in 2014, the Victorian Government funded three programs described as “adolescent family violence programs” (AFVPs) in two regional locations and one metropolitan location (State of Victoria, 2014). Program design was influenced by the Step-Up model, but programs are delivered in voluntary, community-based contexts, rather than in court-based contexts. An evaluation of these programs conducted by the Australian Institute of Criminology (Boxall, Morgan, Voce & Coughlan, 2020) found that there was some evidence of reduction in severity and frequency of violence by a young person while engaged in the program.
The evaluation also found that programs helped parents experiencing AVITH by reducing associated levels of stigma and shame, thus increasing their confidence to report their experiences, and helped adolescents and families by improving skills related to reducing conflict (Boxall, Morgan, Voce & Coughlan, 2020; Campbell et al., 2020). This evaluation was conducted between 2014 and 2015 and was somewhat limited by small sample sizes and no long-term follow-up (Boxall, Morgan, Voce & Coughlan, 2020). Similar to the limitations of the US-based model, however, the evaluation reinforced the importance of addressing and breaking cycles of violence within families, as many of the participants had experienced intergenerational harm. It also highlighted the challenges inherent in adequately addressing the multiple co-occurring risk factors and complexities present in families experiencing AVITH (Boxall, Morgan, Voce & Coughlan, 2020), echoing thefindings of the KIND evaluation (Moulds et al., 2019). The authors of the AIC evaluation acknowledged that,
given the evidence that substance use and mental illness are associated with the onset, recurrence and escalation of [AVITH], young people need integrated interventions and coordinated support to address their abusive behaviours as well as psychiatric and substance use treatment. (Boxall, Morgan, Voce & Coughlan, 2020, p. 1)
Recommended expansion of the Victorian Step-Up-based programs
The RCFV recommended that the Victorian Step-Up-based programs be expanded on a statewide basis, subject to the results of the above evaluation, which were available to the Victorian Government before it was formally published. As at 2020 – when both the AIC evaluation and the PIPA research were released – this expansion had not occurred. In the interim, however, the Victorian Government had provided additional funding to the three existing programs to support individually based work and had also funded an ACCO to develop a community-led, culturally specific program (State of Victoria, 2018). More broadly, it is important to note that similar group work programs based on the Step-Up model had emerged in other locations throughout Victoria, delivered by organisations receiving broader DFV and integrated family services funding.
In the second half of 2020, the then Victorian Minister for Family Violence Prevention announced that additional funding would be directed towards responses to people using DFV, with responses to AVITH identified within that allocation (State of Victoria, 2020). This was described as a response to the increase in DFV and AVITH during Victoria’s 2020 lockdowns. Further detail about the AVITH-focused nature of the investment was forthcoming in early 2021, when organisations which already delivered therapeutic recovery programs for victims and survivors were asked to establish AVITH-focused interventions as an additional component of their work. Organisations were asked to establish programs and provide early data within six months, with funding later extended for a further 12 months.
During 2022 – a period during which government had the opportunity to review drafts of the current study while the project was paused, as well as other AVITH-related research – the Victorian Government initiated a procurement process for services to deliver programs using a model of care for adolescent family violence in the home (AFVITH). The model of care proposed that suppliers adopt a whole-of-family approach, ideally through a collaborative or service consortium arrangement. The proposed model sought to prioritise early intervention and emphasise care coordination.
Other AVITH-focused policy and investment in Victoria
More broadly, many of the other AVITH-focused RCFV recommendations had also been implemented prior to the WRAP around families research being initiated, including the appointment of specialist practitioners at the Melbourne Children’s Court to support young people and families where a young person was a respondent to a protection order application; the establishment of a legislative statewide diversion scheme; and the expanded use of Youth Resource Officers within Victoria Police, some of whom incorporate a dedicated focus on young people’s use of violence at home into their role.
A trial of “restorative family meetings” incorporated into the adolescent family violence programs, as recommended by the RCFV, was also conducted but not continued. Findings from an internal evaluation were not available at the time of writing but Victoria’s Family Violence Reform Implementation Monitor (FVRIM) noted that efforts should be made to revisit this (FVRIM, 2021a). Notably, an investment in respite via dedicated crisis accommodation linked with therapeutic support for young people using AVITH (as recommended by the RCFV) had not been forthcoming, although investment in crisis accommodation for young people experiencing DFV had occurred. This lack of progress in implementing appropriate respite options was also identified by the FVRIM (2021a).
Outside direct implementation of RCFV recommendations, the Victorian Government also established a cross-government working group in 2018 with a focus on developing a coordinated service response to AVITH. It also funded the Centre for Excellence in Child and Family Welfare (CFECFW) to build and share evidence through an open platform, hold an AVITH-focused symposium to discuss current evidence, and coordinate a community of practice for specifically funded AVITH services.
Flowing on from AVITH being recognised as a specific form of family violence in Principle 10 of Victoria’s Multi-Agency Risk Assessment and Management Framework, as well as in related victim survivor practice guides, the Victorian Government also progressed work to develop risk identification and assessment tools applicable to the use of a range of interpersonal harm by young people, as well as to consider the experience of children and young people as victims and survivors of violence in their own right.
This included a focus on considering the full spectrum of risk and where young people may have been misidentified as the predominant aggressor, a concern highlighted by FVRIM in late 2021 (FVRIM, 2021b). The lead author of the current study was part of a team engaged to contribute to the development of a practice guide to inform and accompany these tools, to be released at a later date.
Recognising the impacts of COVID-19 on opportunities to progress this broad-ranging work, it is nonetheless worth noting that, while a focus on service delivery and associated investment was clearly visible during this time, engagement with relevant challenges in the legal system was not. This includes engagement with the findings of the PIPA project around the challenges associated with the legal response – crucially, that the current legal response frequently sees young people made subject to a protection order without appearing at court or having the opportunity to engage with lawyers and disclose their own experiences. Further, Victorian legislation still does not require any consideration of a young person’s capacity to understand or comply with any order imposed, nor consideration of safety risks where a young person is excluded from the home and placed with another adult. As a result, young people are being pushed into a tertiary end response,with its associated potential for an escalation in risk, by virtue of the legal process. Funnelling of resources into this tertiary end response in turn pulls focus and investment away from early intervention and wraparound approaches.
COVID-19 in the literature
Providing further backdrop for the period during which this research was conducted was the COVID-19 pandemic and, in particular, Victoria’s extended lockdowns during 2020 and 2021. Evidence has already highlighted the impact of the COVID-19 pandemic on DFV generally, observing a significant increase in both severity and frequency (Boxall, Morgan & Brown, 2020; Pfitzner et al., 2020; Usher et al., 2020; Usher et al., 2021) quite early in the pandemic. Studies have also noted increased numbers of people seeking support from specialist DFV services; an increased complexity of needs; and escalation in controlling behaviours from adult perpetrators (Boxall & Morgan, 2020; Perkins et al., 2021; Peterman et al., 2020; Pfitzner et al., 2020), who leveraged the isolation and added barriers for victims and survivors to seek support or escape (Perkins et al., 2021; Peterman et al., 2020; Pfitzner et al., 2020; Usher et al., 2020; Usher et al., 2021).
Evidence also establishes that the COVID-19 pandemic has increased mental health issues in many people (Fisher et al., 2020; Tucci et al., 2020), including young people (Cardenas et al., 2020; Drummond Street Services, 2020; VicHealth, 2020).
In particular, a study conducted over the United Kingdom’s initial lockdown in 2020 revealed a marked increase in the incidence of AVITH, with 70 per cent of 104 parents surveyed reporting more frequent incidents, while practitioners reported an increase in referrals and a rise in severity of the violence (Condry et al., 2020). Explanations cited were spatial confinement and forced proximity within family homes; dramatic changes in structure and routine leading to disruption; increased opportunities for young people to use power and control; and general heightened fear and anxiety (Condry et al., 2020, pp. 21–27). The study concluded that, for many families, AVITH will have become more entrenched and further damaged relationships, with an increased need for additional support – or a “safeguarding surge” – predicted by the authors (Condry et al., 2020, p. 54).
A study from the United States examined the impact of the pandemic on sibling violence specifically (Perkins et al., 2021), and highlighted the effect of unsupervised and concentrated time on an increase in sibling violence during lockdowns. The study also noted that increased stress and trauma, as well as child abuse and neglect, within families is generally associated with an increase in sibling violence and will have been compounded during the pandemic (Perkins et al., 2021).
In the Victorian context, Victoria Police data suggested a 20 per cent increase in reported family violence incidents involving young people between October 2019 and September 2020 (Crime Statistics Agency, 2020). An issues paper prepared by the Centre for Innovative Justice and the CFRE at DS similarly responded to reports from practitioners that AVITH was increasing during the pandemic, particularly during the extended lockdowns and restrictions experienced in Victoria during 2020 (Campbell & McCann, 2020).
The paper drew on consultations with service and legal practitioners who described a “net-widening” of young people experiencing a legal response because of behaviour which had developed and escalated during lockdowns. Practitioners also described an escalation in mental health issues – particularly where families were required to spend more time together without “circuit breakers” such as school, work or extracurricular activities (Drummond Street Services, 2020). This was described as prompting crisis responses which in turn ruptured family relationships over the long term (Campbell & McCann, 2020).
Practitioners also reported that the lack of service responses was impacting legal outcomes for young people, as was the difficulty in engaging young people online or via phone, particularly where young people had cognitive disabilities or learning delays (Campbell & McCann, 2020). In particular, practitioners reported concerns for the safety of young people where they may not have a safe or private space to have conversations or make disclosures while confined within their home, particularly where they were living in crowded public housing (Campbell & McCann, 2020) and, for a time, subject to “hard lockdown” during July 2020 (Om, 2020; Victorian Ombudsman, 2020). One regional integrated service network reported a particular increase in sibling violence (Campbell & McCann, 2020).
Part 2:
Challenges, change and conceptualisation
Overview
This section of the report outlines some of the findings from the focus groups with practitioners across AVITH-focused mental health, legal, court-based and AOD support services. It also features the voices of parents interviewed for the research, who described significant and multiple needs that had not been met by the service system. In addition, it incorporates references to data from the case files which reflect the complexity of this area and echo many of the challenges identified throughout.
Overall, the research highlighted the ways in which practitioners were working hard to respond to clients in a service and system context which, in some ways, had become even more complex since the Victorian data collection period of the PIPA project. Despite additional government investment, the nature of this investment had not yet offered a sufficiently coherent articulation of what Victoria’s response to AVITH was intended to be, despite the effort of practitioners. Further, the additional activity required of services since the RCFV’s recommendations appeared to have constrained service capacity to share practice knowledge and developments in a way that might be expected or, arguably, had previously occurred. The findings therefore suggested that, while there was now greater familiarity with the concept of AVITH – assisted by the RCFV’s articulation of it as a standalone issue, and subsequent research – Victoria’s response was still in the processof being appropriately and fully developed.
The findings and analysis in this section are set out in relation to two overarching areas. The first is practice challenges, including naming and identifying AVITH as a concept, funding, referrals, program design and presenting needs of families. Within the latter theme, the support needs of mothers and children associated with their experiences of prior and ongoing adult-perpetrated DFV was the most substantial sub-theme. The second area relates to systemic barriers and challenges which practitioners were experiencing at the point of data collection and continue to experience at the time of publication.
Practice challenges: Naming and identifying AVITH as a concept
Across the focus groups, practitioners suggested that a greater awareness of DFV overall was enabling families to identify and name what they were experiencing in relation to their young person’s behaviour. This included families starting to self-refer into AVITH programs or being more inclined to call the police for assistance with safety, even where they did not want their child to experience a justice response. Parents participating in interviews and families recorded in case files also self-referred in many instances. “Parents are definitely coming out and naming it … so they’re looking for a specific response. And Googling it … So it’s definitely kind of named and talked about” (Practitioner 2).
That said, a consistent theme across the research was the reluctance of young people or families to be linked with a service which was identified as specific to DFV. Kehoe and colleagues (2020) suggest that intervention efforts are further stymied by parental reticence to engage in services which may escalate feelings of shame and stigma (Kehoe et al., 2021). Parents may also feel that their child’s behaviour is normal; that they have failed in being a good parent; or that they are alone in their experience of AVITH and therefore feel disempowered to seek help (Kehoe et al., 2020).
Literature notes that mothers, in particular, often blame themselves for their child’s use of violence and seek to hide it (Fitz-Gibbon et al., 2018; Meyer et al., 2021), while young people feel guilt and embarrassment (Burck et al., 2019; Burck, 2021; Condry & Miles, 2021; Papamichail & Bates, 2020). Practitioners in this research similarly described these feelings of shame as sometimes contributing to escalated risk, with young people acting out further as a direct response to their feelings of guilt: “We know how shameful it can be accessing services … often the risk levels are quite high because of the shame associated with that” (Practitioner 22).
Parents similarly described the shame that their child felt when they had used harm against their family.
[Young person and older brother] have done things where they … have either punched me or physically done something … and the verbal stuff that used to come out [to me and their sister] and … then would go into these huge depressions afterwards because of the guilt. (Parent 1)
Practitioners also described young people feeling resentful about involvement in a program when they have been a victim and survivor themselves but were now being labelled as the person causing harm. Practitioners working in ACCOs which had been funded through the recent Victorian Government investment reflected on this and explained that language and terminology were particularly crucial in community-based contexts.
Talking to other colleagues … who work as adolescent family violence workers from other organisations and from other areas at [our organisation] and stuff as well, like, it’s been challenging, I think with the language around what the program’s called … not to downplay any of the actions of the young people, but there’s a big scale of violence as well. And so sometimes we might work with someone where there’s quite serious kind of family, physical violence and things like that happening. Other times that might be something that is, that’s one aspect … But it’s really difficult often for us to kind of get the young person to recognise if they’ve experienced family violence or other kind of trauma as well, to recognise what their behaviours are in relation to the things they’ve experienced as well, because often the things that they’ve experienced are … much worse than what they’re doing. So, it’s hard for them to say, well, you know, “Dad isn’thasn’t [sic] faced any consequences for his actions or whatever. So why am I?” (Practitioner 73)
In relation to the system’s capacity to name and identify AVITH, practitioners described persistent service confusion about the behaviours that might constitute AVITH. Practitioners also described a system that had worked very hard to identify patterns of adult-perpetrated DFV, but could not yet identify AVITH or, more specifically, understand considerations required to deliver effective responses.
The system is catching up with all this … language around [risk assessment] that is still filtering through policing and the courts … we’re asking police and courts to believe victims, survivors and to identify when women are experiencing family violence. And then we’re adding, you know when it comes to young people using violence … police are seeing a 16-, 17-year-old using violence and they view him as an adult perpetrator, we’re not responding to him as a child. So it’s like asking for another shift, another complexity, another nuance that the system isn’t really ready for. (Practitioner 50)
What I notice as a shift is a deeper understanding around adolescent brain development. But where I don’t see the dots joining is then where it connects with perpetration of adolescent family violence. There’s still this kind of like “they’re going to be monsters when they’re men”. (Practitioner 35)
Practitioners across the research volunteered that the concept of AVITH did not fit well within the victim and survivor/perpetrator dichotomy on which wider DFV responses were based. This poor fit then shaped recognition of the issue as one warranting a safety response; the nature of this response; and referrals on to other services. This could function as a barrier to support for family members experiencing AVITH or, alternatively, mean that young people received a punitive – and therefore unconstructive – response.
We had a really disappointing experience with a family that got bounced around all over the place trying to get a referral into our program which included [an intake service] responding to them and saying “Oh no, you’re talking about a teenager, we’re not going to help you” and just kind of ending the conversation because it wasn’t an adult perpetrator. (Participant 22)
There’s just something about working with the perpetrator that [means that specialist DFV services] just don’t go there, like, “That’s not the work we do. We work with victim survivors” … It’s so binary and it doesn’t help anyone to view families in this really binary way. (Practitioner 27)
We’re dealing with children and young people – and sometimes they are children, they are little kids … You get these very perverse outcomes where a child might make a move towards reconciling with the family and [where there’s a protection order in place] that move towards reconciliation is a criminal action … It’s kind of adult perpetrator frameworks expressed in a way that is not developmentally attuned at all. (Practitioner 54)
Practice challenges: Referrals into AVITH-focused support
Practitioners explained that the ambiguity or uncertainty described above could impact the type, as well as the flow, of referrals into services. The research team heard that, upon establishment, some new programs had received a rush of referrals from local schools, mental health supports or disability services that were not appropriate for an intervention focused on AVITH.
This reflected what practitioners described as a lack of services available to respond to challenging behaviours or expressions of trauma or disability in young people in their area.
Some of them were really inappropriate referrals. So like we’ve got kids that are like, you know, incredibly low IQ, with specialist school history … sexual abuse, who’ve ended up in the program. Like that young person had no capacity to even understand why the behaviour was not okay. Our team leader does admit that, at the start, it was like, you know, grab for whoever was coming through but then towards the end, we refined the process down. (Practitioner 17)
We’ve had [the intake point] make referrals for whole-of-family case management … that sat well outside the scope of what the program was all about … and really required an intensive Integrated Family Services kind of approach. (Practitioner 43)
Importantly – and as explored in more detail in Part 3 of this report – focus groups suggested that, where referrals were working most effectively for the newly funded services, these services were leveraging the integrated referral pathways that already existed within their own organisations.
That said, practitioners who worked in well-established services – including youth substance abuse services, as well as AVITH-specific services – also described referrals coming through once behaviour was entrenched but had not initially been identified through a DFV or trauma lens.
These young people are hitting wrong doors all the time … they will hit different parts of the service system, particularly the tertiary system … and then the referral comes after they’ve done six or 12 months of intervening and case work and there’s been, you know, hectic substance use and then there’s like “too hard” or it will bump it back to us. (Practitioner 52)
When trauma or the presence of adult-perpetrated DFV had potentially been identified, practitioners also expressed frustration that appropriate supports had not been provided to young people or families where earlier support could have made a difference.
… the number of referrals that we get from Child Protection when there’s been so many prior reports, sometimes with an intervention, sometimes with nothing, and then we still get it with the same criteria and the problems will be entrenched. And if we read the referral, we can quickly surmise that there’s been something really complex and why hasn’t it been picked up? Why hasn’t something been offered to the family? (Practitioner 1)
Interviews with parents certainly reflected this pattern of a lack of support in relation to adult-perpetrated harm experienced earlier in childhood.
[Young person] has only really ever known conflict … [and] the kids have never really spoken about any of that [adult-perpetrated violence]… there’s never been any formal sort of support putting in place to help them debrief or grieve through all of that. Yeah, ’cause grief is a really big factor there. Yep. For that relationship. (Parent 1)
In some cases, AVITH-focused interventions that had previously received referrals directly from Victoria Police were no longer directly linked into this process because of wider change across the Victorian family violence system. This was primarily because referrals were now going from police to the Orange Door network (see “Definitions”). Demonstrating a need for either multiple referral pathways or sufficient resourcing and staffing to allow for follow-up and expediting of referrals once made, practitioners therefore spoke about challenges that arose when they did not have the direct visibility of a young person’s or family’s circumstances to which they had previously had access. This included where a specialist DFV response was put around a mother, but no referral, or a referral which only contained limited information, was forthcoming for the young person. These practitioners described the need to push for more information, particularly when areferral signalled that the situation was “at breaking point” (Practitioner 5).
… in relation to the referrals that come from [the intake point] … was the lack of information … I have so many questions that came up in the referral … and [the practitioner has to] chase back down with the family or other services that are involved … I’ve had questions about sexual assault and [the referrer] just can’t answer them. They can’t answer what medication a young person is on. (Practitioner 8)
Practice challenges: Funding parameters
Funding parameters
Directly related to the number and type of referrals that services could accept were the funding parameters constraining operation at the time of data collection. This was particularly the case in relation to the services funded in early 2021, which in many cases were working primarily with allocations of between 40 and 110 case hours, with the upper limit being dependent on the complexity of the young person’s behaviour and the needs of the family. Practitioners noted that a limited timeframe such as 40 hours “is just not enough, like adolescents just don’t engage in 40 hours, especially in the middle of a bloody pandemic” (Practitioner 17).
Practitioners explained that this allocation could quickly be exhausted and result in very limited face-to-face contact with a young person once outreach, service coordination and file work was also completed. The research team notes, however, differing understanding and practice across programs where some practitioners described the 40 hours as a floor, rather than a ceiling. This appeared to be where practitioners worked in organisations which provided programs with wider support and integration with other services.
Just as importantly, practitioners noted that constraints on their funding did not allow them to engage with other family members in addition to the working with the young person: “… [where families are] from a CALD community, like you can’t work with a young person if you can’t work with their family” (Practitioner 55).
Funding parameters at the time also limited program capacity to respond to young people in ways that were appropriate for them, including through a workforce of sufficient size which could support a young person if they were likely to respond more positively to a practitioner of a particular age or gender.
I … reality is that I’m just another middle-aged lady who’s coming into [his] life telling him what to do and they’ve got that at school already and they’ve got that at home already. (Practitioner 18)
Importantly, it also limited the period over which they could engage with young people.
I’ve had a couple of clients when really short, sharp interventions have worked … One of them I instantly spotted this kid had a communication issue and we got the speech therapist and it was a quick, “This is what it is” and that was fine but, overall, most of them need really consistent, long-term interventions … So, the advice in the PIPA report was like, “Don’t do short-term, short-term interventions bad” and then the government was like “only do short term interventions, please”. (Practitioner 17)
Parents also reflected on the need for longer term engagement being available: “Kids naturally test boundaries … So, you know, the offer has to be unconditional and without an end point” (Parent 1).
More broadly, the research highlighted the impact of the short-term nature of the relevant program funding in terms of referral pathways. Practitioners explained that some referrers had indicated that they did not want to refer young people if they could not be certain that the engagement and support were going to be available over the longer term (Practitioner 18). This was in part because the cessation of the support would only seek to entrench young people’s sense of being let down by the system overall.
Practitioners also explained that the short-term nature of the current funding – extended for a further six months just after the completion of the focus groups and then again later in 2021 – was limiting their capacity in a range of other ways. This included the ability to recruit, train and then retain a workforce. In fact, some practitioners volunteered that they were looking to move on to other roles, despite their commitment to and belief in the work, simply because of the uncertainty of their current position.
What we’re doing takes skilled and dedicated practitioners and they’re so hard to get when you keep stuffing people around … so we’re just constantly putting families on the back foot and saying they’re not important. (Practitioner 27)
Focus groups featured regular discussions about the uncertainty created by the short-term nature of community-based service funding arrangements, in which a substantial amount of practitioner time was allocated to seeking and reapplying for funding.
It’s just this weird funding cycle that makes everyone really anxious and not be able to do any actual work. (Practitioner 27)
People are just getting their hands on money. And then trying to figure it out from there, rather than any thought going into the work. (Practitioner 10)
Funding challenges, however, were not limited to the recently funded programs. Practitioners working in established AVITH-focused interventions, as well as in wider services which regularly came into contact with AVITH, described the way in which particular funding limits or parameters constrained the nature of the support that they could deliver.
[The funding organisation is] saying “How does this person make criteria? Prove it.” And we’re saying “they will” but shit, they don’t. (Practitioner 55)
We still get this expectation that we work with families for this specific period and it’s all about referring on … whereas we’re all therapeutically trained and we have the capacity to do the deeper work. (Practitioner 2)
A common theme across the focus groups, in fact, was the challenge created by the wider approach to human and social services funding which continued to impact the organisations in which practitioners worked, as well as the capacity to deliver AVITH-specific interventions.
One of the major challenges that we’ve had from year to year is essentially where you would get a program and it would start and you would build momentum … and then it became unfunded and we spent … months looking for funding … So we essentially started from scratch and had to build that momentum again. (Practitioner 62)
Practitioners noted the way in which wider approaches to competitive tendering in community-based service contexts impeded collaboration (Practitioner 44) and made it hard to establish consistency in design, as well as outcomes for families.
… I think that’s pretty disheartening. But also just operationally makes it really challenging … if you’re going to make a change you’ve actually got to change the hierarchy and competitiveness in the setup. (Practitioner 12)
Systems … are increasingly about hierarchy and actually about transactional, you know, kind of high-volume, low-touch services that ultimately can only exist if you deny the impact of trauma. (Practitioner 2)
Importantly, a practitioner from one participating ACCO observed that funding was a perennial challenge in terms of the wide-ranging work that they did – work that was not adequately captured through the target- and output-based nature of the way in which most community-based services were funded.
We certainly report on the hours we work but, if we do over, we just don’t report that and there’s no way to report it really … I think [government] want[s] to support you to a certain degree, but [it’s] so target-driven and hour-driven that we can’t get past that … What we do on the side is what we do on the side … And you’ve got to because the targets and the hours … don’t meet what our need is really. They help support a funded position. That’s really what it amounts to, you know … So it’s a catch 22 in the end, it’s really difficult, but … we’re here to serve a community and the need is there, so that’s what we’ve got to do. (Practitioner 72)
Practice challenges: Lack of consistent frameworks
To an extent, the research found that funding models dictated the framework through which programs were delivered. Although there is a broad understanding at a policy level that interventions will have a whole-of-family focus, practitioners revealed a wide range of approaches being adopted by programs across Victoria. These included a combination of group work and an increasing emphasis on individualised case management being delivered by the established programs which had originally been based on the Step-Up model. They also included the primary focus on young people dictated by the reality of the funding parameters in the more recently funded services.
Group work
Program design included funding attached to certain expectations about the activities that would occur, despite the fact that some practitioners did not always see these activities as being of sufficient value: “Groups for young people aren’t overly successful … if it’s not managed right, a group can be really detrimental to a young person” (Practitioner 5).
These particular practitioners explained that they were required to report a certain component of group work in order to retain their funding, but that they were finding this additionally difficult in the context of significant need across the families with whom they worked, particularly during COVID-19.
We’ve got all of these targets … and we’ve got to try and run group as well as part of our funding … but in these current times, we’re lucky to be able to respond to these families’ current needs without even trying to run a group as well. And I don’t know if we can respond, to be honest. You know, if we want to do each family justice. (Practitioner 5)
Another program appeared to focus its group work on parents, with case management and outreach then directed towards young people. A further program retained concurrent group work with young people and parents, including meeting with parents and young people on an individual basis and bringing in local services and Victoria Police to give talks and foster connections. Some programs that were not funded directly by the Victorian Government ran a group work component, along with intensive family therapy and dyadic work, while others focused on group work with young people at an earlier stage of concerning behaviours. Overall, practitioners described the need for flexibility and the capacity to offer different approaches to engagement within different families: “There’s a place for all of us and every model. Not everyone is going to fit into group work. Not everyone is going to fit into one-on-one” (Practitioner 44).
Limitations in support for families
Practitioners from programs that had received the more recent injection of funding at the beginning of 2021 frequently described themselves as only being funded sufficiently to work with young people, rather than to work with other family members. Where practitioners could draw on other programs and practitioners within their organisation, they could complement the work of their funded role. Where some practitioners were working in isolation, however, this meant that they were simply not able to provide sufficient support to parents or siblings, or alternatively they opted to give their allocated hours to a parent where this was more effective.
Sometimes it’s just Mum who will engage. We need to have flexible models where we can just engage whoever is willing to work with us at that particular time. (Practitioner 9)
It would be bloody nice if we were always engaged alongside family services so that there was a practitioner for their family … so we’re engaged explicitly for the young person but a lot of the time we know the work has to be done with the family, like a 12-year-old doesn’t have the capacity to make those changes for themselves, it’s gotta be a family approach. (Practitioner 17)
A further challenge arose, however, because AVITH-focused interventions were voluntary. Where young people over 16 were unwilling to engage or did not consent to their parents being involved, therefore, practitioners could not work with the parents.
There needs to be consent from the young person and … then [we’re] telling parents, “Well we can’t work with you because, yeah, we haven’t got the consent from your child” … It’s certainly something that I think, in terms of … how we fund adolescent violence services in the future … it’s something that is a bit of an issue and needs a bit of thought (Practitioner 10).
Capacity for flexible, client-centred approaches
Program parameters also dictated the types of activities which were able to be conducted through AVITH-focused interventions, with capacity for flexible and client-centred approaches emphasised by practitioners as being particularly crucial. Interviews with parents also signalled that young people needed flexible and very pragmatic approaches, such as outreach, rather than “talk therapy” (Practitioner 57) as one practitioner described it.
I haven’t had any support from anyone, pretty much for four years because my son refuses to talk to anyone … So, I’ve really, really, really struggled with actually getting any physical support. (Parent 1)
The interviews also echoed what practitioners highlighted about the need for longer engagements over which young people could develop rapport, especially if trust had previously been damaged.
It makes me feel really like I’m not doing the right thing … where I’ve tried so many organisations, but no one’s willing to actually step out, push the boundaries a little bit and go, “Okay, you know what? That’s fine. You don’t wanna talk to us … But I’m gonna ring in and check on you every week. And I would like you to answer the phone call and let me know you’re okay. That’s it. You don’t have to talk. But just say yes, I’m fine this week” … Because you know what? In four or five weeks, something might actually click … (Parent 1)
[The psychologist] tried … to make [my daughter] talk to her dad when she wasn’t ready … “Have you spoken to your dad?” “Have you spoken to your father?” … So [my daughter] refused to talk to [the psychologist] for 21 months, and the psychologist kept pushing her. And I’m like, “when she’s ready, she will talk to him. She’s not currently ready”. (Parent 3)
We had a case worker about six or seven years ago and initially … my children would refuse to have any conversations with this person and over the course of, I think it was four or five visits, they actually started to open up and by the last visit, they actually started talking to him … and then he says, “Oh, this is my last visit ’cause I’ve done my time here”, and I’m like “Oh my God!” … Why do you have to have a case manager just for X amount of time or X amount of visits? … Especially when there’s kids who have had huge traumas and have had abuse … or have been led down the wrong path by a counsellor … and they don’t have that trust there initially … they’ve gotta build the trust before they’ll start speaking. (Parent 1)
One participant from an ACCO explained that flexibility was a central and inevitable part of their practice because of the fact that practitioners were often working within the context of, and had obligations to, their own communities. This practitioner noted that this was not always understood or recognised within funding parameters or in government policy settings.
Our community workers certainly have that feeling of never been able to clock off. I’m pretty strict on trying to make sure that they do clock off and, you know, like work phones don’t go home with them and stuff like that because you have to have that time. But community workers – people know you and know how to contact you and all the rest of it, so it’s not as simple as that. (Practitioner 72)
Practice challenges: Presenting needs of families and young people
An adult perpetrator – and systems abuse – out of view
The ongoing impacts of adult-perpetrated DFV was a recurrent theme across the research, as it was across the PIPA project (Campbell et al., 2020). In 88 per cent of case files, for example, the young person had experienced and/or witnessed DFV or DFV-supportive behaviours. In only three cases the file data did not appear to indicate prior experiences, although this was inconclusive given that prior experiences of adult-perpetrated DFV may simply not have been recorded in these files. More broadly, it was one of many presenting needs to which practitioners across the focus groups were required to respond – or at least to take into account – in the context of their practice.
A big sort of intersection that we see … is where there’s been some sort of extensive Child Protection involvement for a child in their early years. Usually because there’s been intimate partner violence and then down the track when the time the child is in their teens, they’re using violence and they’ve got this significant history of trauma and possibly still family violence going on for them. (Practitioner 68)
… where there’s a significant history of them being exposed to family violence in the home and you kind of just hold your hands up like this and go, “Well what did we expect is gonna happen?” (Practitioner 61)
It is crucial to note that the ongoing impacts of adult perpetration were ultimately the most substantial theme across the client interviews as well as being apparent in the case file review. Parents who participated in the interviews – all of whom were sole parent mothers – described extensive histories of violence which had included very serious physical and verbal abuse against them and their children, and in one case multiple subsequent relationships involving violence.
Before we split up, it was like … shouting a lot and throwing things around and breaking things and, not hitting me, but verbally very aggressive and controlling and if something didn’t go his way “I’ll just break something, punch something”. He punched holes in the wall. And that’s when I got an intervention order against him … it was like he was jealous … it’s almost like he feels like [young person] was born and then everything changed, I guess because … my focus wasn’t on making him happy anymore. It was looking after a child. (Parent 2)
[The children saw] when I was physically backed up against the wall [with a knife in my face] … every time I had tried to walk away from him in like, say an argument or whatever, every time I tried to leave, he would grab me and then physically start hitting me … From my experience I felt like I had no way to get away. (Parent 3)
The nature of the violence experienced by young people and mothers engaged with the DS program and evident across the case files was, in some cases, incredibly stark and multi-directional.
Young people’s experiences of prior adult-perpetrated DFV
- In file DS021: “The mother reports that her ex-partner (recently separated) and the young person have always clashed” and there was an incident “when the young person was in Grade 4 and her ex-partner strangled the young person, who was very scared”.
- A young person was exposed to her father’s DFV from a young age (DS008): “When [young person] was very young, their biological dad smacked [her] on her bare bottom in public. He made his dog growl at her when she was two because she told a lie. They also witnessed him choker her and punch her in the face.”
- Case notes from file DS250 involve a young person’s mother describing the father’s violence towards the young person, explaining that he would hit her with so much force that she would report to the mother that her whole body would vibrate. While the parents were still married, the father would control all the finances, preventing the mother from working and “refusing to care” for the children. The mother also describes violence and controlling behaviour used by the children’s father towards her, including calling her a “cunt” and “slut” in front of the children.
- Information on file DS032 describes a young person’s father holding the mother by the throat up against the fridge until her face turned blue, resulting in the young person stepping in and begging him not to kill the mother.
As well as acknowledging the prevalence of prior experiences of adult-perpetrated harm, however, practitioners expressed concerns that limited capacity to work with different members of the family did not give them a lens on the adult DFV risk that might be present in that home or in the young person’s life on an ongoing basis. The challenge of a lack of visibility of an adult (usually male) perpetrator continuing to use abuse was a prominent theme across all of the focus group discussions.
Practitioners working within the newly funded programs explained that it was often not until well into engagement with a young person (including when a caseload allocation was winding up) that the presence of adult-perpetrated DFV became apparent.
I think the awkward thing is that like we don’t actually know … Like, one of my families, I didn’t know there was family violence present there till I was actually in the house [conducting outreach] and by that stage it was too late. (Practitioner 17)
I’ve got a family at the moment where I’ve been holding a question about intimate partner violence, as well as the adolescent family violence … My sense is that it’s going on but no one’s admitting to it and Child Protection has been involved and the school’s got concerns and so it’s quite complex. And I’m there trying to engage with the adolescent but also trying to assess risk and what’s really going on in the home. (Practitioner 9)
I think that risk is perhaps missed, even with Child Protection, so that the stepfather has got a criminal history of family violence. But … the young person … is the focus and makes disclosures of family violence in the home and then retracts them … Child Protection is gone and said “we can’t find any evidence” so close the file. (Practitioner 9)
Challenges were compounded when the parameters of some services precluded work with young people where an adult was continuing to use DFV. These limitations were designed to prevent scenarios of young people being “held accountable” for behaviours towards people who have used harm against them, but legal practitioners in particular were concerned about the exclusion of young people from support.
Where can we actually get the right support for these young people? That’s safe for them to have their own person to speak to? A lot of the services are ruled out because they can’t work with a young person when there’s an adult perpetrator in the home. (Practitioner 46)
When we do get the referrals or the intakes … the young person is often not a part of that process … [their] voice is often not there. It’s other people’s interpretation of the young person’s experience or their own experience of the young person … it’s almost like distancing of an adult perpetrator as well, and then holding the young person as the perpetrator. (Practitioner 33)
A lot of our families have had family violence and Dad of course is potentially … perpetrating family violence from outside the home. But we’re actually not having any collaboration with any men’s behaviour change services or any male services … we don’t know what the male perpetrator is doing. Despite all this supposed collaboration, we have no idea. (Practitioner 5)
The capacity to understand the risk posed by adult perpetrators – and to keep an adult perpetrator in view – was highlighted as a significant challenge beyond specific program capabilities and capacity, with the impact of post-separation systems abuse a particular concern raised by participants: “The family court is a massive problem … it impacts our ability in this space” (Practitioner 27).
Ongoing family law struggles – as well as serious adult-perpetrated DFV and coercive control – were very apparent in the case files. These included young people continuing to live in very unsafe situations, either with a separated biological father or in new family structures where they are experiencing adult-perpetrated DFV. In particular, some of the files echoed practitioner observations that separated fathers may “coach” young people from the sidelines in relation to their use of violence or aggression towards their mother or, alternatively, that young people may only “act out” once they return from contact visits to the safety of their mother’s residence.
Ongoing abuse
- File DS838 describes the influence of the father over the young person, with the mother reporting that the father reinforces the young person’s aggressive behaviour towards the mother and states that the mother must be the problem given that the young person does not use the same behaviour at the father’s house.
- In file DS021, case notes discuss a young person’s relationship with his separated father undermining the bond he had with his mother. Case notes also describe that the young person could nonetheless feel overwhelmed and confused and, when this occurred, elected not to go to his father’s house, at which point he felt guilty and experienced retaliation from his father.
- In file DS311, case notes describe the young person and his older brother returning from their father’s to accuse their mother of “making their father suffer”. Case notes also describe the young person becoming increasingly aggressive on these occasions and undermining the mother and her parenting strategies.
- In file DS789, the young person and two siblings were living with their father, despite a current protection order in place to protect the mother and all children from the father. This was because the mother did not have a fixed address and was experiencing secondary homelessness. Child Protection was involved while the children were in their father’s care.
- Multiple files describe violence where a stepfather had recently taken on a parenting role. In file DS043, the young person received a mobile phone from a friend, which his mother said to conceal from his stepfather. Upon discovering the phone, the stepfather was described as “destroy[ing] it by throwing it across the room”, “screaming and shouting”.
- In another file (DS456), the dynamic between a young person, her mother, her mother’s current partner and the mother and current partner’s two sons led to a situation where the adult male used violence towards the young person. Case notes reflect concerns that the mother may be under the influence of her partner, who is known to other services as controlling. Case notes record that the partner makes threats to take the children away and exhibits controlling behaviour and verbal abuse.
- In file DS311, case notes state that the young person and their older brother have seen and heard a lot of fighting, including different types of physical and emotional abuse as well as gaslighting. Case notes indicate that the ex-partner has spent a lot of time trying to make the children believe that the mother deserves everything he was doing.
- Case notes from another family (DS021) refer to the young person’s father instilling distrust in the young person regarding the school welfare worker and encouraging the young person not to talk to them, leaving the young person without any external support.
Similarly, parent interviews suggested that prolonged co-parenting abuse and coercive control stood out as potentially having an impact equal to or greater than earlier physical and emotional violence.
God knows how much hatred he says over the phone to my daughter about me. (Parent 3)
I’ve had so many bouts of depression over the last 10 or 15 years because I haven’t coped with what’s going on … And it completely hasn’t been spoken about because I’ve been too ashamed or too scared … and then later on when I when my [physical health deteriorated] … we couldn’t say anything because he could turn up at any time and take the kids and I couldn’t do anything about it. And when I [went into hospital] … I said to [the kids], “Look, this is another option, instead of you getting separated and going into care, you could go to your Dad’s” and it was like “No way, no way” and they weren’t mentioning or saying anything to anyone where it might get back to him … I don’t know how he would go if he found out about [young person]. (Parent 1)
I picked [young person] up one day and he said that [ex-partner] had strangled him, so I reported that to the police … and [ex-partner] made a whole lot of allegations about me … Child Protection turned up and I thought they were coming because I’d [reported], but actually they were coming because he’d been reporting me … and [ex-partner] actually ended up getting extra time with the kids instead of less … Basically, I wasn’t believed … You know, it was so expensive … and in the end I just, I basically ran out of money. (Parent 2)
The ongoing impact of adult-perpetrated DFV included separated fathers using coercive and controlling tactics to limit young people’s access to a range of positive extracurricular activities. Examples of controlling behaviour included a refusal to pay child support, with one parent stating that her daughter had two jobs to pay for her activities which she sought to give her a positive outlet outside the environment at home (Parent 1).
When the kids joined [extracurricular activity], [ex-partner] initially agreed but then changed his mind … and because … they weren’t at home for pick up on that Saturday morning even though [he] knew about this weeks in advance, we ended up having the police turn up … to come and collect the kids … and [he]’s on the other side going “I want these kids now” and like they were so embarrassed and hurt. And there’s been other sporting events where he would do exactly the same … So the kids didn’t wanna play sport anymore because they don’t want this happening in front of their friends … (Parent 1)
Other examples included perpetrator fathers manipulating the contact that young people had with support practitioners – particularly psychologists or school counsellors – in an effort to perpetuate control.
There was a counsellor at the school that [young person] was talking to a little bit, but then [ex-partner] went and saw her and apparently cried. And she told [young person] that he really should go start going to see his dad because his dad’s so upset. And I … met with her and the principal and I said, “Look, I don’t think that’s appropriate, [young person] is the child and the victim here. [Ex-partner] is not the victim. Even though he thinks he’s the victim.” (Parent 2)
Because it was quite an abusive situation and they were all going through lots of different things, the counsellor they were all seeing decided to, with my consent … reach out to my ex-husband to say “Hey, you need to back off because this is what’s happening at the moment with the kids and this is what they’re experiencing” … and then he’s taken it upon himself to send each child an individual letter letting them know that “I’ve spoken to your counsellor. They’ve told me everything that you’re going through and they’re gonna help us get together.” And my kids were ropeable because they felt like she had told them everything that they had told her. Yeah, and she hadn’t … and ever since then they won’t speak to anybody … because they don’t have that trust there. I get where she was coming from. Somebody had to tell him to back up because [he] wasn’t listening to anyone … but then he turned around and has just thrown it all back in our faces andit was just so wrong for everybody. (Parent 1)
The interviews with parents and case file review signalled a particular challenge in relation to perpetrator fathers withholding consent for their young person to be involved in support services, especially if language around “DFV” is invoked.
[Practitioner] was really supporting me … suggesting all these great things and talking about things we could do, but when it was time for when we needed [ex-partner’s] consent for anything, [ex-partner] wouldn’t … once he saw [the reference to DFV] he wouldn’t buy it … I feel like, you know, that [program] could have done good things for us if the consent hadn’t been quashed. (Parent 2)
Having encountered this challenge, practitioners in the case study program reported that they often now presented themselves as providing more universal support for a young person, whether it be for behaviour at school or for their wider mental health, to facilitate consent from perpetrator parents. Similarly, the mother quoted above described a contrasting experience where she had been able to obtain her former partner’s consent for her child to receive general counselling from a psychologist, noting that her younger child nonetheless missed out on this type of support as he did not want it to be brought to his father’s attention.
… so he was comfortable about that because she wasn’t a domestic violence practitioner and he had arranged that. So, you know, if he feels like he’s in control [it’s okay but] if he feels like he’s not in control he makes things really difficult … [Younger sibling] did say that he wanted to talk to someone one day and I said “Well okay, you know, your dad would have to actually agree to doing that, but do you want me to, you know, organise something?” And he kind of went “No, no, don’t worry about it.” (Parent 2)
Services attuned to these patterns of behaviour described the importance of maintaining a lens on adult-perpetrated harm as a central consideration to their work.
It’s generally us that are identifying the violence [that a young person is experiencing] … It’s after asking those questions about their safety and their side of the story. Because often they haven’t been asked or they haven’t been believed. (Practitioner 46)
Practitioners described needing to account for potential interference in the benefits of their program by the presence of ongoing adult-perpetrated DFV, highlighting that a young person often moved between their primary place of residence and the home of a separated father.
You know the challenge for us is that we’re trying to, you know, how do we not let that work that we’re potentially doing with the young people not be undermined in the family home and at dad’s place as well? (Practitioner 23)
Noting that specialist DFV services had conventionally “shied away” from clinical work with families where children were still having contact with an adult perpetrator, some practitioners insisted that this should not be a reason for young people missing out on services: “The only reason we won’t work with the families is if it’s going to increase family violence, risk and safety factors” (Practitioner 22).
This insistence was significant, given that practitioners from this program noted that “all but two” referrals had involved an adult male perpetrator who was actually still residing in the home, rather than just being involved in a young person’s life in the context of shared parenting arrangements (Practitioner 26). Practitioners from another program described the ongoing presence of an adult male on a full exclusion protection order while a mother faced violence from her child as well.
I had [one case where] police attended for an [AVITH] call and the [adult] male perpetrator of DFV who has a full exclusion intervention order was within 100 metres of the house and the police officer responded to the mum … “He’s [adult perpetrator] probably 101 metres, so we’re not going to charge him.” So, she’s … experiencing [AVITH] as well and she gets that response. (Practitioner 21)
Experiences of ongoing adult-perpetrated DFV therefore remain crucial to highlight. This is because, while evidence continues to acknowledge exposure to prior adult-perpetrated DFV as a major contributor to the use of AVITH (Contreras et al., 2020; Fagan, 2020; Fitz-Gibbon et al., 2021; Gallego et al., 2019; Meyer et al., 2021; Nowakowski-Sims, 2019; Perkins et al., 2021; Tucker et al., 2020; Walker & Woerner, 2018), studies give less emphasis to the ongoing presence of DFV, either in the home or in the context of separated families. Studies highlight the high prevalence of sole parent mothers as victims and survivors of AVITH (Armstrong et al., 2018; Fitz-Gibbon et al., 2018), including one study that suggests that AVITH exists in 20 per cent of sole parent homes (Armstrong et al., 2018; noting here that 57% of case files reviewed for this research involved a young person living with a sole parent mother).
The lack of emphasis on current adult-perpetrated DFV, however, may result from assumptions that where parents are separated the violence has ceased. This assumption stands in stark contrast with significant recognition of separation as one of the highest risk periods for the escalation of violence, as well as the ongoing impact of protracted family law proceedings (Bagshaw et al., 2011; Brown, 2006; Katz, 2019; Maher et al., 2021; Spearman et al., 2022; Thiara & Humphreys, 2015). The lack of emphasis on current, or ongoing, adult-perpetrated violence may also result from an acknowledged lack of young people’s voices. Evidence certainly indicates that young people and family members impacted by AVITH rarely have the opportunity to tell their story (Campbell et al., 2020; Condry & Miles, 2021; Papamichail & Bates, 2020). This is particularly the case with young people who – often having experienced violence as well as using it – can feelthat their own experience is ignored or that it is considered worthless (Campbell et al., 2020; Condry & Miles, 2021).
Research also suggests that young people may blame themselves for their own adverse childhood experiences and sense of emotional rejection from parents (Burck, 2021; Papamichail & Bates, 2020), with feelings of parental rejection recognised as a core contributor to AVITH in the literature (Contreras & del Carmen Cano, 2019). This is echoed in feelings of guilt and rejection in the descriptions of young people’s experiences in parent interviews. Also evident in the case files was the sense of responsibility and fear shouldered by siblings, with many taking on a protective role for the mother, seeking out help, or living in fear at home.
Sibling experiences
- In file DS631, the young person reported to the DS practitioner that, during conflict between the young person and his father, the young person’s brother gets scared and hides under his bed. The young person questioned why his younger brother was not engaged with the service and felt that his brother should be contacted because he often gets forgotten about.
- In another instance where a sibling was engaged with DS due to a young person’s use of violence (DS076), the sibling identified his role in the family as being to look out for his mother and two sisters and always being available to help his mother. This sibling reported that, when he thinks about the significant physical violence used by his elder brother against his mother, he feels upset and gets a stomach-ache. This sibling also witnessed a history of violence perpetrated by his father against his mother. DS identified the sibling as also being at risk of using violence, with case notes indicating that the sibling had been fighting with his eldest brother and the rest of the family.
Barriers to service engagement: The link between trauma and shame
Whether related to previous or ongoing adult-perpetrated DFV, a strong theme in the current study was the shame that many mothers experienced in relation to the presence of AVITH and the links of this shame to their own experiences of wider trauma. This included the way in which their relationship with their child had been undermined by their current or former partner.
There’s almost always trauma. Significant trauma in a family or from impact of family violence on the family, or childhood abuse with the mother … which makes it really hard for mothers to hold on to their parenting strategies to stay regulated. They freeze or they disappear. (Practitioner 1)
Parent interviews reflected the impacts of prior adult-perpetrated DFV on their capacity to manage their response to a young person’s use of harm.
I can see him crashing and burning and it’s heartbreaking … because he’s also quite abusive … which then sets off triggers. So, it’s sort of “I wanna give you the love, but shit!” … When you’ve got someone screaming verbal abuse at you, it’s just really difficult to try to do that. (Parent 1)
I just feel like, I sometimes wonder if I’m being manipulated … Sometimes it’s worse than others. Like, you know, it’ll be months at a time where things are relatively okay and I’ll go, “Oh, you know, thank God I can, you know, breathe a bit.” (Parent 2)
Certainly, noting the evidence referred to in Part 1, experiences of adult-perpetrated DFV can not only impact on mothers’ feelings of shame but also on their capacity to parent effectively (Hernández et al., 2020), and on their feelings of psychological distress when responding to their children’s own use of harm (Burck, 2021; Jouriles et al., 2021). Evidence similarly suggests that children exposed to adult-perpetrated DFV frequently do not access appropriate services or treatment to assist them to recover (Stylianou & Elbright, 2021). This was apparent in the case file reviews (explored in Part 3 in the context of supports provided by the DS program) as well as in interviews with parents.
The thing is their anger, their sadness, their grief, their fear … being rejected because their father doesn’t want anything to do with them or treated them so horribly … has never been discussed with my kids … I’ve never brought it up … I’m too scared with the ramifications that would come if we started having those discussions … We’re still mending. (Parent 1)
Linked to experiences of shame in the current study was the way in which different sector conceptualisations sat in tension with one another, and the phenomenon of AVITH – as well as its drivers – not being well understood. Practitioners described how parents who sought help could be left feeling blamed for the young person’s use of violence at home if the young person’s behaviour was not apparent in another context, such as at school.
They feel stigmatised that it’s their fault, that they’re not able to control their naughty child. (Practitioner 62)
I think there’s a lot of fear in other services about being able to hold risk as well and, like, unpack it a bit more … because it’s still very mother-blaming as well, like this young person has these behaviours, but obviously this is Mum’s fault because she stayed in that relationship, like we are still in that narrative a bit sometimes … (Practitioner 25).
… you see the same submissions made by [Child Protection] that were made 10 years ago … (Practitioner 67)
Parents participating in the research described experiencing blame and minimisation of their family’s needs when contacting specialist DFV services or intake points.
… places like Orange Door … they gave me such a hard time that [young person] had no support or I haven’t done enough for him … I spoke to one person on the phone. And then somebody else has been trying to ring [young person] … “Why hasn’t he answered the phone?”… He finally answered the phone to some person who wasn’t the person I initially spoke to and they had a bit of a conversation with him. They left me a message on my answering machine saying “We’ve checked in with [young person]. He’s all good. We’re closing our books on you.” … He’s talk[ed] suicide twice. There’s self-harm. Who disengages? This is a kid that doesn’t go to school, doesn’t get out of bed. And you’re telling me he’s all okay? Like my God, that was it? And I rang up, I was so frustrated. And I’m like, “You told me this time you’re gonna come in and help.” [And they said] “But he said he’s fine. He’s going to school.” I’m like, “He went to school for one day” … (Parent 1)
Parents also described feeling that they were not imposing enough boundaries. This included having the behaviour minimised by extended family and suggestions that it was the parent’s fault.
… when [my son] was really struggling [during a difficult time] … and he would throw … trash cans and huge tantrums … And my father turned around and said, “He just needs a firm hand” … [My son] was just really struggling with the whole dynamics of everything … Now if they ask me how I’m going I say … how easy it’s going … I don’t say anything. (Parent 1)
[My mother] will say to me, “You’ve gone out, you know, on Friday night” and “Your kids need you. They need you to be home” … That’s part of where the anxiety comes from. (Parent 3)
Just as relevantly, parents described feeling exhausted and drained by their experiences, or limited in their options across their wider lives.
I’ve been in the same job a long time. I’d like to look for a different job … but I don’t have the mental energy to do that … because I’ve got all this stuff in the background that I have to deal with all the time. (Parent 2)
I felt like as a single parent, as a young mother … I felt like if I wasn’t there, you know, that I was completely detrimentally affecting them and completely failing (Parent 3).
If I’m mentally healthier, happier, I cope with it a little bit better and when I’m not, I don’t. And there’s been a couple of times I’ve walked out and I’ve just driven a couple of streets away down a back road and sat there and cried in my car. I’ve had a couple of times …where I didn’t think I was gonna make it through … It’s really overwhelming when you don’t get to replenish yourself … Somebody once described it as you’ve got a cup full of tea and … the tea leaves in your cup need to be rehydrated. Like they’re just totally dry. (Parent 1)
Echoing crucial existing research (Burck, 2021; Condry & Miles, 2021), practitioners volunteered that stigma and shame were a significant factor for young people as well.
… the trajectory of trauma into the adolescent phase of development with these young people piecing together their identity … at a time when their brains are expanding, they’re putting all this together, sitting with the grief and loss around their histories. (Practitioner 26)
Parents participating in interviews for the research also described their young people being shamed by their interactions with support professionals.
The psychologist said, “You realise you look older than you are, you will become prey for older men” … That’s why [my daughter] didn’t wanna see her again. And I don’t blame her … she didn’t want to do it [counselling through DS] because she already had that experience. (Parent 3)
Practitioner observations also included the way in which shame could sometimes be deployed by parents who did not have the skills, were not ready, or were still too traumatised themselves to take other approaches, contributing to one program’s reluctance to use group work combining young people and parents.
If the caregiver isn’t ready and they’re not in that right space and they want to shame that child, I’ve seen it done and to shut it down sometimes is really, really hard. (Practitioner 5)
Disability, mental health issues, wider trauma and complex needs
Disability
A significant number of presenting needs apparent across the research were related to disability. This is highlighted as a feature in other recent Australian studies (Fitz-Gibbon et al., 2018; Kehoe et al., 2020; Meyer et al., 2021) and is echoed in the findings of the PIPA project, which explored in detail the co-occurrence of disability in young people identified as using AVITH in the context of Victoria’s DFV response (Campbell et al., 2020). The PIPA project found that approximately 50 per cent of young people in a wider legal sample had some kind of disability (including psychosocial disability), while nearly 25 per cent of young people in a court file sample had been diagnosed with autism spectrum disorder (ASD) (Campbell et al., 2020).
Similarly, of the 33 files reviewed for the case study, 39 per cent involved at least one member of the family disclosing a disability or disorder. Echoing the rates in the PIPA project, the most common diagnoses were ASD (24%), attention deficit hyperactivity disorder (ADHD; 21%) and oppositional defiant disorder (6%). Seven young people were diagnosed with more than one disability. In one case, the young person and younger sibling both had diagnoses of ASD, ADHD and anxiety issues (DS 170). In another, the young person had been diagnosed with ASD, anxiety, obsessive compulsive disorder, ADHD and learning difficulties (DS 043), with this family involved with multiple additional services.
It is important to recognise that families experiencing harmful behaviours from young people with disability may be able to access supports through the NDIS and community-based disability providers, although this research highlighted substantial challenges in that regard. The question, however, is whether this behaviour is appropriate to be included in the category of AVITH, particularly where the definition by Pereira and colleagues (2017) specifically excludes it.
By contrast, Victoria’s legislative imperatives mean that young people with disability are being caught up in a highly proactive and often punitive response (Campbell, 2021; Campbell et al., 2020). It is therefore vital to emphasise that the PIPA project’s finding about the significant rate of disability among young people identified as using AVITH in Victoria was a reflection of the way that the Victorian legislative and policy landscape works, rather than an indication that disability and AVITH are inextricably linked (see also Sutherland et al., 2022).
In the context of this particular research, the presence of disability, sometimes involving diagnoses of multiple conditions, in young people identified as using AVITH also suggested that an ongoing lack of appropriate supports for young people with disability was contributing to families experiencing harmful behaviours from their child. This was reflected by one parent in the description of her child’s experience.
[My child] wasn’t very great at regulating his emotions … he would lash out a lot when he’s [at school and] being treated differently to others. He would think something was unfair because he wasn’t treated the same as the next child or he would hurt somebody because they hurt him … He was diagnosed [with ASD and ADHD] when he was eight and we’d been on a waitlist since he was four. We completely missed out on funding until then … (Parent 3)
Practitioners observed that while the needs of families were acute, the supports they received were often inadequate or too difficult to navigate, given that so few young people with disability were able to access the NDIS. This points to the need for greater policy attention and resourcing in this regard, both in terms of access to the NDIS and access to community-based disability services, with resourcing of these services significantly impacted upon the introduction of the NDIS. It also points to the need for wider community-based services to be resourced and family and child services workforces to be trained to respond to clients with disability.
The amount of referrals we’re getting for young people who either have an NDIS plan, or who have a diagnosis and/or disability, that has skyrocketed as well. (Practitioner 19)
A fair few of my kids have got NDIS plans, but the plan doesn’t necessarily always assist the family and what they need … the family don’t always know how to get more support, who to talk to about changing the plan reviews or anything. (Practitioner 8)
Other learning difficulties were also described as compounding distress for young clients: “With dyslexia, we have three to four in one group of ten” (Practitioner 64).
Practitioners described the way in which children with language delays or cognitive impairments could be at additional risk of experiencing violence, as well as at risk of using it: “Kids with speech language problems can’t find the words … they just don’t have the internalised scripts … the brain shuts off and the body takes over” (Practitioner 42).
Certainly, learning difficulties and associated school disengagement were presenting needs for young people in 40 per cent of the case files. The research team heard that language delays and behaviours of concern were being seen more frequently as the eligibility for AVITH services was expanded to include children of an increasingly young age.
For example, the expansion of the existing Step-Up programs in Victoria included the expansion of program eligibility to incorporate children as young as 10, while the eligibility criteria for the newly funded programs also incorporated this age group. One practitioner considered this inappropriate, however, given that 10-year-olds rarely had the capacity to engage with services and, more broadly, had no capacity to change the wider dynamics in a household (Practitioner 17).
They opened it up to … to see how many we would get … services are actually getting those young children … and they don’t know what to do with the behaviour. (Practitioner 5)
Particular learning needs were highlighted by parents as having a serious impact on young people when not appropriately recognised, either by schools or by adult perpetrators in their lives.
Because [they said] he was a danger to himself and other children … the teacher wouldn’t understand … they would just remove him. (Parent 3)
[Young person] … had a few different things going on with his [vision] … we went and got him tested, we’ve had all these procedures … and because [ex-partner] wasn’t involved at all, it was like, “That doesn’t exist”, “You’re all speaking crap” … And he wouldn’t let [young person] … wear his glasses, he was taking them off him and putting them away while he was in his care and he would let him ride bikes and stuff, so he was forever going to … hospital. (Parent 1)
Echoing the intersection of learning or support needs with the impacts of adult perpetration, focus group participants also suggested that many young people’s needs, including those identified as stemming from disability, were inextricably linked with trauma.
Often when children have been acting out or perpetrating, inverted commas, family violence they have also been at the receiving end of it … and in many cases [this is] complicated by the fact that they’re often children with complex other needs, trauma or autistic children, children with intellectual disabilities. (Practitioner 68)
I think it’s really hard to distinguish for a lot of our clients whether it is a behaviour that’s coming from a diagnosis or disability, or whether it actually is AVITH. (Practitioner 19)
When they’re using violence, that’s telling us something. That’s giving us information about what their experience has been like and their development. (Practitioner 29)
Mental health
Also very apparent across the research was the prevalence of mental health issues. Emotional, behavioural or mental health symptoms were identified in 78 per cent of cases, while parental mental health was identified as a risk factor present in 60 per cent. Anxiety was a co-occurring presenting need for 48.5 per cent of families and depression for 24 per cent. Instances of self-harm, including suicidal ideation, were identified in 33.3 per cent of the files.
Literature confirms that young people and families impacted by AVITH experience a range of co-occurring issues which both contribute to and compound the effects of their behaviour (Malti et al., 2018). These include severe mental health issues, such as acute psychological distress, suicidal ideation and self-harming behaviours (Kehoe et al., 2020; Martinez-Ferrer et al., 2020), as well as low levels of “family and social self-concept” (Martinez-Ferrer et al., 2020).
Practitioners working in acute mental health contexts, including hospital emergency departments, also described the relationship of experiences of trauma to serious mental health presentations in young people who were using violence. This reflected what was described anecdotally by practitioners working in these contexts as a significant increase in presentations of young people using AVITH to emergency departments during Victoria’s extended lockdowns throughout 2020 and 2021, including as a result of being brought there by police in lieu of a protection order response.
… so those young people that present often to our emergency department, it’s probably one of the most predictable experiences that they have in their day or in their week … it’s almost like a … co-regulation … but it’s occurring in the emergency department because it’s the safest place and most predictable space. (Practitioner 41)
The research team heard about parents seeking help from emergency departments for their child’s behaviour while presenting with their own mental health issues as well.
It’s all also overlaid with parents, who more than likely have their own neurodevelopmental problems and mental health problems, shame around feeling like they’re failures as parents … [We have to assess] what’s the adult’s capacity and resilience around their own self-regulation, their own mental health … (Practitioner 42)
The biggest thing I think, for a lot of our families, or a lot of our young people, is that they literally do not have the tools to do this by themselves. (Practitioner 18)
The response that young people and families receive in these settings, however, may be somewhat dependent on the experience of the staff in each hospital, as suggested by this reflection from a parent.
So there was a lot of support around for that, but with headspace [National Youth Mental Health Foundation] saying “Get your child to a hospital”, it took me three hours to get [young person] to the hospital and when we got there, there was no paediatric person on call at all. And so we had to wait three hours and after 15, 20 minutes, [he] was already going “Get me out of here.” And [by the time they got somebody in there] he goes “I’m not interested, I’m just gonna tell ’em what they wanna hear.” And when we got in there, he said to the guy, “Yeah, no, I’m fine.” The … doctor [said to me.] “You’re just exaggerating it. Go home.” I will never be able to get him to hospital again. I’ll never be able to go down that path. (Parent 1)
Case files also highlighted the ways in which mental health was a factor for families experiencing AVITH – for parents and siblings, as well as for young people using harm.
Mental health presentations, including self-harm and suicidal ideation
- One family (DS170) had been in and out of the Royal Children’s Hospital for support around a young person’s eating disorder.
- In another family (DS532; DS236), mental health concerns arose upon the discovery of homicidal material (towards children and animals) in the young person’s room. Following assessment, the young person was diagnosed with psychosis and schizophrenia and held involuntarily in hospital under relevant mental health legislation.
- In case DS126, the 11-year-old sibling of a young person using violence reported that her mother was often “not well”, staying in bed and being absent from the young person and her brother’s lives for days and nights at a time.
- In one case (DS098), the young person had been in an inpatient mental health unit and moved into unstable housing (homelessness and then in emergency accommodation) before eventually moving in with his father, who had been abusive to the young person in the past.
- In one file (DS043), the loss of a close friend resulted in the young person self-harming and threatening to suicide.
- In DS456, the young person was severely self-harming and the DS practitioner advised the young person’s mother to call an ambulance and a suicide hotline.
The case files also indicated how experiences of adult-perpetrated DFV could intersect with mental ill health in parents and intergenerational harm to compound trauma for young people, including files indicating histories of intergenerational drug use and adult-perpetrated DFV as well as severe mental health issues, including suicide of young people’s parents.
Bullying
Also emerging as a sub-theme across the research – related to young people’s mental health as well as to their use of harm – were experiences of bullying. Emerging studies show the relationship of bullying victimisation with the use of violence at home (Espejo-Siles et al., 2020), and practitioners similarly volunteered that young people’s experiences of bullying were common in their client base, potentially related to attempts to act out after their experiences or to regain a sense of control.
If bullying is present, you can see that come into the home. (Practitioner 3)
We would probably get well around 80 per cent [who have] experienced bullying or are the bully themselves or are a mixture of both. (Practitioner 64)
Practitioners explained that experiences of bullying could further isolate young people who were already facing additional challenges, including violence at home or cognitive or other learning delays.
… one young man who, when we talk about different strategies of, you know, how does he cope with [being bullied] he just talks about, like, positioning himself in certain places in the school yard and … his strategy has just been to basically not interact with anyone. (Practitioner 63)
Of note, experiences of bullying victimisation were also volunteered in a parent interview as a contributing factor to the use of coercive controlling tactics by perpetrator fathers: “[Ex-partner] said that he was the youngest and his older brothers bullied him, and so he’s not gonna allow [young person] to bully [younger sibling]” (Parent 2).
The case file review also demonstrated that bullying was a presenting need in 24 per cent of files as either perpetrated against, or by, the young person using violence, although victimisation appeared to be a greater factor, leading to disengagement from school.
Bullying and school disengagement
- In one case (DS631), the young person refused to eat at school because this was the reason for being bullied previously. His experience of bullying included an incident of physical violence from a large group of other children which resulted in his hospitalisation.
- In another file (DS932), case information reveals that the young person was being bullied and had been acting out at school as the result of an inability to regulate his emotions. Case notes state that the young person was becoming physically violent and attacked other students after being bullied for an extended period of months. The young person’s mother did not know about his experiences of bullying until this attack on other students.
Wider trauma and complex needs
It is important to highlight that the research indicated wider forms of trauma and marginalisation were also presenting needs in families and young people experiencing AVITH. Certainly, a wider evidence base establishes a link between adverse childhood experiences and a range of behavioural or developmental problems in adolescence (Docherty et al., 2018; Malvaso et al., 2019), as well as a correlation between individual, familial and social experiences of disadvantage and disconnection and use of harm in close relationships by young people (Blakemore et al., 2018).
Adverse childhood experiences can include traumatic refugee experiences which shape children’s neurodevelopment and can lead to associated hypervigilance and behaviours (Campbell et al., 2020; Lamb, 2018), as well as structural barriers and systemic racism (Fagan, 2020), including over-policing and differential legal responses (Armstrong et al., 2021).
Emerging studies have also begun to highlight the relationship between intergenerational trauma and the significant impacts of AVITH in the context of kinship care placements (Breman et al., 2018; Gair et al., 2019; Holt & Birchall, 2020), as well as the relationship of pre-existing trauma and child removal to the prevalence of AVITH in adoptive families (Selwyn & Meakings, 2016). Researchers have therefore called for a greater focus on intersectionality and experiences over the life cycle in the context of use of AVITH (Holt & Shan, 2018), rather than a focus primarily on adolescence.
Recognition of intersectionality and trauma experiences over the life cycle were a feature of the case file review. For example, trauma was a co-occurring presenting need for 91 per cent of families, with qualitative data describing families fleeing persecution; families living in a refugee camp; young people witnessing a parental suicide attempt; the loss of a parent or loved one (in one case to COVID-19), combined with lockdown; child removal and adoption; and the bullying and adult-perpetrated DFV described above.
The case file review indicated that 24 per cent of cases involved at least one family member born outside of Australia and 12 per cent speaking a language other than English at home. Some case files highlighted that experiences of marginalisation can intersect with use of harmful behaviour by young people, while experiences of adult-perpetrated DFV can further marginalise families and young people.
Exclusion from services and marginalisation
- Two families explicitly reported experiencing exclusion from services as a result of their CALD background (DS236; DS098).
- Another young person reported that, when her family migrated to Australia, she felt that she had to be the “strong one for the family … I had to be okay and make my parents not worry” (DS482).
- One family of six (DS098) were born in the Horn of Africa and were once in a refugee camp, with case notes indicating the impact of racism on a younger sibling, including verbal taunts at school. In this case, the father had a history of using violence within the family, but because he was the only family member who could speak English, he was the main contact person for engagement.
One young person across the files identified as Aboriginal (noting that two case files did not report the young person’s Aboriginal and/or Torres Strait Islander status) and their file involved experiences of child removal and complex mental health and learning difficulties, for which the young person was linked in with a range of different supports.
More broadly, as well as trauma from adult-perpetrated DFV as the predominant experience, the experiences of the parent sample included separation from children; a lack of emotional and/or pragmatic support from extended family; early parenthood in one case; and experiences of childhood sexual abuse, including the abuse not being believed by the other parent. Siblings, as described by parents, had also experienced wider trauma, including sexual assault external to the family and stigma associated with that experience.
A particular sub-theme to emerge from the research findings was the impact of prior periods of separation as a result of mothers’ physical ill health, leading to disrupted attachments between mothers and children. Experiences of grief, separation and wider trauma appeared to play a significant role in the contexts described by two out of the three parents interviewed. This included the experience of one parent who, post separation from her abusive partner, had required hospitalisation for a long-term injury and, lacking other appropriate supports, felt she had no other choice but to have her children separated and placed in temporary out-of-home care.
A lot of people were saying, “They’ll be right. They’re only young, they’ll be right” … [but the kids were saying,] “What happens if you die? What happens if you can never walk again? What happens to us?” … And that was a real fear for them all … [Older child] had a huge amount of trauma … He really, really struggled and left home early because he was the adult in the family for so many years, he really struggled to give me back that power of being the adult and him being a kid … It’s taken us huge amounts of work for us to mend our relationship, which that itself has also had damage on [adolescent child]. (Parent 1)
This was also a theme in two of the case files.
Maternal guilt and separation
- A mother in one family disclosed falling ill and being in a coma a few years prior to the young person’s use of violence began and believed that, during this time, the young person became “angry at her for something outside of her control” (DS838).
- In another file (DS098), a mother revealed that she had a long-term illness for which she had twice been hospitalised for a significant time, and which she feels has impacted her children’s development and childhood.
Practice challenges: COVID-19 compounding risk and needs
Echoing the literature referenced in Part 1 of this report, practice reflections emerging across the research indicated particular challenges in supporting and engaging with young people during COVID-19. In particular, practitioners described the challenges encountered when face-to-face engagement with young people was suspended in the context of Victoria’s first lockdowns.
What we’ve learned from that is that we lost a lot of engagement from young people and that the most effective way to try and engage them is face to face. (Practitioner 21)
This was a challenge reflected in some of the case files.
Need for face-to-face engagement with young people
- In one case (DS678), after multiple attempts from DS to engage the young person’s grandmother (with whom two young people using violence were living), the grandmother stated that she did not wish to continue to receive support through DS as ongoing lockdowns prevented them from continuing face-to-face.
- In another file (DS169), case notes indicate that during lockdown the young person completely disengaged from school because of the online learning environment and refused to attend other appointments, either online or by phone. Instead, the young person’s mother suggested a face-to-face visit as the young person was comfortable engaging in “small talk” with adults in a face-to-face context while also having the option to choose to leave the physical environment.
This was also a very real challenge for two of the three parents interviewed. Although all three mothers described benefits from the support that they had been able to receive themselves from DS, in two cases, DS had not been able to engage with their children, primarily because of COVID-19-related restrictions.
I needed physical help … but COVID happened at the same time … which of course just crashed and burned everything. I needed somebody … to come in who can physically help support [young person] with getting him over the line with anxiety, depression, getting him out of bed, maybe having some sort of “let’s go kick the ball” to build some sort of rapport with him … But while things are only over the phone … that’s not helping. (Parent 1)
The children had practitioners assigned to them but because of COVID we weren’t able to see them. (Parent 3)
One parent also described the impacts of COVID-19 escalating risk and conflict between her and her ex-partner, who was still involved in the children’s lives (and who had denied consent for his children to be supported by the DS program).
When [changeover] is on the school day, he picks him up from school and he takes him to school the next day. So, I don’t see him … [but] one of the things with the whole lockdowns [during COVID-19] was, because they weren’t doing the changeovers at school, we were seeing each other all the time (Parent 2).
Even where practitioners were able to maintain contact and engagement with young people, focus groups also highlighted the challenges for their practice and the support which they could facilitate where other services were not available during the lockdown periods.
Some of these young people have absolutely no supports in place at that point … If we’ve received a referral during lockdown, there’s absolutely nothing in place … (Practitioner 64)
Practitioners also described challenges related to service uptake, where other service networks and practitioners were either not aware that the service was available or were not necessarily confident that they could offer a young client or family the requisite support during lockdown.
We will sort of put out like a big generic email and I’ll get a few calls and do a few consults and we’ll have a boom time … then it’s because we keep opening and closing with lockdowns and it’s like that they forget that the program’s there again. (Practitioner 62)
Impacts of technology
Intertwined with the impacts of COVID-19 were the particular challenges associated with young people’s increasing use of technology. Although this was not a significant theme raised by practitioners across the research or by parents in interviews, use of violence related to technology was a significant feature on 21.2 per cent of case files, contributing to a stressful home environment and placing additional pressure on parents, as well as contributing to young people’s anxiety, isolation and lack of sleep.
Use of technology in the context of COVID-19
- In one file (DS043), a young person physically assaulted his mother when his stepfather took the TV remote away. The stepfather’s frustration stemmed from the fact that the young person was watching TV rather than helping with chores around the house.
- Similarly, a mother raised concerns about a young person’s device usage and time spent alone in his room (DS169), and worried about managing this over the school holidays. The mother informed DS that the situation “blew up” after she turned the internet off at 10:00 pm.
- In one file (DS237), a mother reported that the young person had ceased attending school, hardly came out of his room and stayed up all night watching TV. Case file notes indicate that the DS practitioner asked what it would look like if the mother removed the TV, to which the mother reportedly responded, “I wouldn’t even try … I don’t want to know.” The mother added that the young person communicates in an aggressive manner, harasses her and blocks her access to exits when she attempts to set boundaries.
- In another example (DS578), a young person’s mother described an incident where she confiscated the young person’s Xbox remote as it was late at night. The mother went to return to bed and the young person “attacked” her from behind, hit her and pushed her against the wall.
System challenges: Under-serviced and over-serviced families
As well as the practice challenges described above, substantial systemic barriers also emerged across the research which, in turn, limited effective practice. Particular systemic challenges included the extent to which families who experienced AVITH were either significantly under-serviced, as the PIPA project described, or – conversely – over-serviced and immersed in service intervention. Sometimes the experience of multiple services in a family or young person’s life could ultimately result in them having received no useful intervention at all – leaving them under-serviced, despite constant service system activity.
Focus groups highlighted the ways in which some families had been identified by the system for the first time. In particular, practitioners highlighted the lack of service support for children who had been exposed to adult-perpetrated DFV, as reflected in the literature (Stylianou & Ebright, 2021), and in the parent interviews.
One I have now is quite young, 13, and has had no issues in the past. Just been diagnosed with ASD. A lot of family issues, a lot of family violence witnessed in the past. Still sort of witnessing it from Dad as well … He’s started showing symptoms of the gaslighting and things like that as well … They’ve sort of never had any services before (Practitioner 14).
Practitioners described families or young people who had opted not to engage and felt that they could address their situation themselves.
We get people who it’s their first entry point, really tried to manage everything themselves their whole life and it’s just got to the point where they can’t anymore. (Practitioner 6)
Not everyone wants services. Lots of times they’re calling, they just want support. They just want to understand the situation. (Practitioner 61)
Practitioners also described families experiencing significant needs who had not had these needs addressed and were presenting to an AVITH-focused intervention having exhausted all other options.
Either there’s just too many services involved, like NDIS shoved a lot onto them, or you’re waiting for those services to become involved and we’re holding that. (Practitioner 19)
We get other people who have been engaging in services since the kids were in kindergarten and they’ve been to different psychologists, different psychiatrists, different paediatricians and we’re really at the end of the line. (Practitioner 6)
We’re creating distrust in services because we’re achieving nothing or only achieving tiny things. (Practitioner 17)
Parents participating in interviews echoed this experience.
I couldn’t tell you who referred me to [DS] because it wasn’t my first organisation. I’ve been trying to sort some support for both my son and us as a family for quite a while. (Parent 1)
A predominant theme across the research, therefore, was the involvement of multiple services in families’ lives without these services having been of any help. This was described as having a detrimental impact on young people and families alike, with legal practitioners commenting that “system fatigue is really big for our kids” (Practitioner 69).
We’re often very mindful about the pressure on young people, particularly in the sense of not being over-serviced and because that can often have quite detrimental impacts on them too that they just have so many people trying to support them. (Practitioner 13)
And sometimes, you know, [mothers] will be getting multiple calls from services after an incident saying, “Hey, what’s happened?” and you’ve got an adult who has been … in a really traumatic experience with their child and having to relive it four times in one day after it’s happened … (Practitioner 26)
This was echoed in parents’ descriptions of their interactions with services as well.
I’m just tired of getting my hopes up with, “Maybe someone can come in and help” and then they don’t … I’m so over having to repeat all of this because when I repeat it, I just realise how sad it sounds … And I feel so sorry because [young person has] had no real support to help get through any aspect … (Parent 1)
Within this context, practitioners described the damaging impacts that could arise from the involvement of multiple services or systems in families’ lives, particularly when this was experienced as punitive in terms of criminalisation of the young person, child removal, or criminalisation of other family members.
I guess when we’re doing safety planning, it’s certainly not the first thing that we would recommend is to contact the police … We don’t want them to be in a situation where they’re too scared to call the police and they get injured themselves but … they don’t know what’s going to happen to their young person … There’s a lot of things that I guess police miss – like in judging who the person using violence is as well … the mum or whoever is calling might be upset and so then police think that it’s that person [who has] been using violence as well. And obviously police reactions and police violence towards Aboriginal people is a big concern … That’s part of something that we work within safety planning with the adults. (Practitioner 73)
I’m a six-month service and it took six months for that family to go “Okay, [practitioner’s name] is okay” …We’re fighting against historical service [exposure with families] who don’t get along with workers … workers that are trying to remove the children and are constantly disciplining the adults. (Practitioner 55)
I think some of the complexities about working in this space is that we’re almost trying to undo a lot of the harmful responses that have occurred … (Practitioner 25)
Just as relevantly, interviews with parents described the way in which negative experiences of service system interaction could mean that young people refused to engage in further referrals, including because of a distrust in “talk therapy” as noted above, as well as the delay between when help was sought and a response from the service system was initiated.
… the fact that you’ve gotta go through such a long process to be triaged and sometimes by the time someone speaks to me and then by the time they try to get to talk to one of the kids, it can be like a couple of weeks. And they will put you on our waiting list and then, “We’ll get someone to get back to you.” But then we don’t hear from anyone for three or four weeks. It sort of defeats the purpose of it all. It’s like [my children] are not important enough for it to be acted on there and then. (Parent 1)
The involvement of multiple services in families’ lives was similarly apparent across the case files. At the time of their referral to DS, families were engaged with a broad range of services, including multiple services at one time. In particular, 48 per cent were involved with mental health services, with primary health (21%) and NDIS (12%) the next most prominent services in families’ lives. While some positive examples of multiple service involvement were evident and are featured in the next part of this report, also evident was the ineffective or damaging impacts of service engagement for some families.
Over-servicing or negative service experiences
- One family (DS-567) specifically identified that, despite the young person and the family having “lots of services involved”, including participation in the Step-Up program, this did not lead to positive improvement in the young person’s behaviour and use of violence. Within this family, the mother had a counsellor and had been in contact with the Orange Door but did not feel that the support offered by these services led to meaningful change in the family.
- One young person who chose not to engage with any of her long-term supports told DS that she “had too many supports already” (DS456).
- For one family (DS169), engagement with a counsellor prior to referral to DS “has left a huge trail of distrust” and impacted the young person and their sibling’s desire to be connected with services in the future. Case notes reveal that the young person attended a mental health service as a result of concerns around suicidality but refused to attend again after the first session, after this was seen as a negative experience by the young person.
Wider literature acknowledges that experiencing multiple co-occurring issues can mean that the needs of these families often do not fit within the remit of any single service (Condry & Miles, 2021). Because of the way in which services are designed and funded, disability or mental health services struggle to respond to DFV, while specialist DFV services – designed to work with victims and survivors – struggle to support young people who are experiencing, but also using, violence (Campbell et al., 2020).
As a result, families are often passed from one service to another, leading to increasing distress (Burck, 2021; Campbell et al., 2020; Fitz-Gibbon et al., 2021) and disillusionment. Having moved between multiple referrals, these families and young people often drop out of service engagement and have little reason to engage with any newly introduced service or practitioner – either because they have no hope that it will help, or they do not want to get their hopes up, as one parent described above.
Evidence further suggests that many families impacted by AVITH have not experienced respectful responses from relevant services (Burck, 2021; Campbell et al., 2020; Condry & Miles, 2021), often compounding this sense of shame or blame. In particular, evidence also suggests that adoptive families may feel a particular sense of blame and parenting failure (Selwyn & Meakings, 2016).
In the context of the current research, parents participating in interviews all shared stories of how they had attempted to engage their children in services (usually private psychologists) in response to their children’s experiences of adult-perpetrated DFV, with this generally being the only service pathway that they had felt was available at the time. A misguided breach of confidentiality, manipulation by an adult perpetrator or a judgemental comment from a professional, however, had made their children permanently reluctant to engage or to make themselves vulnerable by describing their experiences to yet another stranger.
Negative experiences of service intervention therefore left their children under-serviced in their recovery from adult-perpetrated DFV, and suspicious of engagement with any further services. These children’s experiences highlight that the challenge involved in supporting families and young people appropriately involves more than ensuring that they are not under-serviced, on the one hand, or over-serviced on the other. Rather, experiences of service interaction also need to be positive and trauma-informed to ensure that young people and families do not ultimately end up without any meaningful support at all.
System challenges: Siloes not collaboration
Where there was involvement of multiple services in a family’s or young person’s life, the research found that this was not necessarily having a beneficial effect, with families passed from one service to another in what one participant described as an “assess and refer on” model (Practitioner 2), rather than services wrapping around the family or working in a coordinated fashion.
Sometimes it feels like they’ve been ping-ponged around, like they’ve been sent to headspace and … to Step-Up … then to somewhere else … (Practitioner 5)
We’re like little Lone Rangers getting in there trying to move mountains, it’s quite challenging … It’s really not a wraparound approach … It’s just an isolated, “We’ve referred, good enough” kind of approach. (Practitioner 17)
It seems to exist as this kind of relay almost … in that we’re passing the idea or the problem of the family from one person to another instead of coming together … because then there’s also that fear of oversaturation of services as well. (Practitioner 7)
As the above comment suggests, practitioners explained that the lack of a wraparound service model was partly a result of reluctance to have too many services involved at once, as well as services not responding to or providing the type of support that a family was requesting.
They’ve just been bounced around and around and around different services because they’re never quite the right one [and] nobody is listening to what the family is seeking because what we think might be beneficial isn’t necessarily what the family’s needing right now. (Practitioner 22).
I think one of the issues is that the system response is linear. So you’re like either a respondent or you’re a victim, right? And young people, they’re both. (Practitioner 61)
Just as relevantly, participants described a “siloing”, in which services were not prepared to stay “open” if another service was able to “hold the risk”, particularly where they did not consider themselves as the most appropriate service to respond to AVITH, as was noted at the outset of this part of the report.
I’ve got one client who came from Family Services as a referral, and [they were] working with Mum and she’d achieved the majority of her goals in a 12-month period and then these behaviours from her son were worsening and so she’s referred to us and then she’s closed because Mum’s achieved their goals [and now] … that’s another client that I can’t engage. (Practitioner 17)
It’s literally a siloed kind of work … like the way that models are funded, the way that service systems are funded. It can affect the experience of families on the ground in that they just don’t have a destination that’s obvious. (Practitioner 52)
The focus groups highlighted that the “linear” nature of the service system could mean that, while families or young people were passed forward from one service to another, they could not necessarily be passed back the other way if the risk profile was perceived to have changed.
One of the barriers is that the system is not there to back you up when you need it. So, you sort of assume that if it gets to a certain threshold, you’ll be able to contact Child Protection and send it back there. But they’re not interested. I had a family during the lockdown, Mum was really drug affected, really mentally unwell, she broke every window in the house and … [Child Protection] closed before they even spoke to the family. (Practitioner 3)
When we make a report [to Child Protection], it goes to intake. If they don’t do anything about it, we’re still left with the same situation that we’ve got. If it goes to investigation, we have to close, because part of our criteria is that we can’t work with any clients who have investigation with Child Protection, so it’s a bit of a catch 22 for our … clients. The situation either isn’t bad enough for it to go to investigation or it is, and then we’re going to withdraw anyway. (Practitioner 20)
If we see that there’s a high-risk situation with a family [then] we’re going to the Department [i.e. Child Protection] to explore around “How we can keep that family safe?” And our challenge to the Department is, “What are you going to do about it?” And sometimes we don’t get our way, even though we’ve placed all this evidence and notes and everything, you know, facts on the table. (Practitioner 74)
Practitioners from one of the programs explained that the siloed and linear nature of the service response could mean that there was “nobody in between” (Practitioner 57) a crisis response and a community-based model, with young people exited from a crisis service and put onto waiting lists for months. It could also mean that, where a crisis response was engaged, the framework in which this operated could run counter to the understanding of risk from the AVITH-focused intervention and override significant concerns around safety.
You might work with a family and it gets to a threshold where you really need [acute mental health] involved for the young person because the risk of suicide’s huge … but then they are directing the parents to do things that are counter to the principles that we would want to hold on to which are, you know, safety first … [Mental health] is saying to the parent, “You need to use your authority” and I’m like, “Oh my god, Mum’s going to get stabbed if she does that.” (Practitioner 2)
The research team also heard that the siloed nature of the service response impacted the types of information that each service had available. This was because services could pass the baton of families to each other without ensuring that information relevant to risk was also part of this “relay”. It was also because services could “close” their involvement with families without properly engaging or advising that they would no longer be involved.
[The] mum could never remember engaging with the service … she just remembers that they stopped contacting her … She was filling in services on information that they should have been aware of. (Practitioner 8)
We are really siloed in our capacity because we don’t have access to that information sharing. (Practitioner 51)
Noting that “young people are not siloed beings” (Practitioner 57), practitioners suggested that considerably more work needed to occur in order to improve responses and support for young people and families experiencing AVITH – work that should not rely on individual practitioners or programs making connections.
It’s the way that we speak to each other as services as well. It’s like “You do mental health, you do AOD, you do this” … when working with young people, none of that should be particularly siloed. We should all be a little bit aware of each other. (Practitioner 57)
There hasn’t really been consistent practice … services have adapted to meet their own local needs … It’s so dependent on the practitioners that you’ve got and the ability that you’ve got to adapt your own program. (Practitioner 13)
Overall, these findings about a siloed and linear service response echo repeated concerns across research related to DFV responses and point to the need for sufficient resourcing which allows for coordination, integration and follow-up, rather than just a “refer on” or throughput approach. They also point to the need for funding and program models which measure outcomes, rather than outputs – creating time and opportunity for slowed-down service interactions which are more likely to “land”, as practitioners in the research described it, and “get the intervention right the first time”.
System challenges: Care teams
Associated with practitioner concerns around siloed service responses were challenges in relation to care teams. While the use of care teams has become a well-established feature of the Victorian service landscape – in which practitioners from multiple services involved in a young person’s or family’s life meet to discuss their support needs – the research found that these mechanisms were not always providing useful support in the AVITH context in the way that the research team had expected.
In fact, while notable exceptions are highlighted in Part 3 of this report, including in the context of the case study, practitioners participating in the focus groups generally struggled to nominate more than a handful of examples in which a care team had operated for the benefit of a young person. This appeared to be for a number of reasons, outlined below.
Care team purpose
A strong theme in the discussions regarding care teams was practitioner concerns around their perceived purpose. AVITH-focused practitioners – including those working in mental health or AOD service contexts – felt that the purpose of a care team was for services to ensure that a young person was receiving the support that they required to improve their wellbeing, as well as to improve their behaviour. This was not always the way in which a care team’s purpose was perceived by other practitioners, however, with focus groups suggesting that this was a direct result of the binary frameworks in which some other services worked.
When there’s presence of Child Protection in that care team, it defaults back to “Okay now we’ve got to prevent this, we gotta stop this contact happening” and “That could be a breach” … There’s perpetrator language and frameworks creeping into care teams. (Practitioner 52)
These meetings are just about, you know, passing judgement … just making really unnecessary comments about what the young person’s been doing, rather than actually working together to identify what’s not working and … what in our interventions or our support is not helpful? … I think care teams can really lack accountability when the young person isn’t present … we’re providing the service, we’re the ones that need to be accountable. (Practitioner 29)
Care team composition
Directly related to the perceived purpose of a care team was practitioners’ suggestion that the composition of services within the care team was important. Practitioners suggested that the infrequent involvement of the specialist DFV sector in these settings inhibited the capacity of that particular sector to engage with the far less binary and more nuanced nature of AVITH-focused work.
This is not a criticism of the family violence sector, because I know they are doing heroic work with caseloads at double and triple hours and people die on their caseloads and so that’s not the point I’m making. The point I’m making is that they’re not a strong presence in care teams … I cannot think of a time when I’ve had a family violence practitioner in a youth care team or child care team … there is not a presence in that long-term care planning for a child or young person and it’s centred around the caregiver’s experience … I’m not even confident that the family violence sector would have a framework around adolescent family violence … (Practitioner 52)
Where specialist DFV practitioners were not involved in care teams, this also limited that care team’s capacity to acknowledge and respond to the presence of ongoing adult-perpetrated DFV, a practice challenge highlighted in the discussion above.
Intimate partner violence is a huge thing … but it’s not often addressed or spoken about and I find that some workers in care teams have a reluctance in trying to address any of these issues … “I’m AOD, I’m mental health, I’m Child Protection, I’m justice, I’m not a family violence worker.” (Practitioner 53)
Demand and service fatigue
Intertwined with service reluctance to venture into unfamiliar territory, practitioners explained the impact of system “overwhelm”, or pressures from the constant demand across human service systems.
I’ve been part of care teams where I’ve been the new worker or the new addition … and have been able to come in with, you know, fresh eyes, and can just see how fatigued the care team is. (Practitioner 29)
They also described how this fatigue could translate into highly insensitive discussions in front of a young person where they were present in the care team.
[I’ve heard] really extraordinary things said to young people during care teams. A real clanger I saw was a 15-year-old girl where a Child Protection worker with a clipboard said “Okay next, sexual exploitation, what are we doing about that?” to the 15-year-old who was a victim [and] survivor of sexual assault … It says something about systems replicating the damage. (Practitioner 57)
These system pressures could mean that there were often practitioners in a care team who had little visibility of the issues impacting the young person, or who did not feel a sense of connection with – and therefore a sense of accountability to – them. Participants commented that they could often feel “as if they were the only person in that care team advocating for the young person” (Practitioner 29).
A complex care team … [were] phenomenal to talk to and had they had really good ideas about who to bring together and they had the authority to make stuff happen … So I had this, you know, great consultation and plan, but actually that worker never did anything because she’s so swamped and overwhelmed in that role that she actually wasn’t able to action anything at all for the family I worked with, and … the things that I was trying to coordinate around, lots of complex things, you know … We were trying to work across hospitals and mental health and schools. And, you know, a wide variety of things. But over four months, I think, of engaging that complex care team, nothing actually happened. And I think that’s a real shame, because I know that the intention was there to support me in my work, but the capacity, she was just flooded … I needed her authority and she just didn’t have time. (Practitioner 1)
Often, I’m in that care team and I look around and count – how many people have actually met the young person face to face? (Practitioner 44)
Lack of coordination
Practitioners explained that, because of the involvement of too many services in a care team, at times they opted to provide a “secondary consult” role. At other times, they tried to provide much needed coordination, particularly given that there could be a lack of follow-up about the different tasks for which services were supposed to take responsibility. One participant noted that this coordination role was a function missing from AVITH work, but was often present in other service contexts (Practitioner 26).
- There’s been other times when there has been lots of people in the care team meeting but that young person has felt less supported than just having one or two workers because it’s just “Oh no, that’s what this person will be doing” or “Oh no, that’s what that person will be doing” – that assumption that “they’ll be following up” but nothing is actually happening. (Practitioner 30)
- I think that most of the service systems are so defensive it really is dump and run. “We just need to get throughput”, you know? So, actually, in the last five years there’s been no collaboration. You’re better off actually doing it yourself because it’s easier on some levels. (Practitioner 2)
Where there was no one providing a coordination function, practitioners noted that this role often fell back on the victim and survivor parent – usually a sole parent mother – in terms of ensuring that young people accessed the services with which they were supposed to engage. Practitioners further explained that multi-service involvement in a care team could increase the burden on families and young people.
We have quite a lot of young people and they have care team meetings and some of the services that are linked in are not that supportive. It seems that there are a lot of things that they express that the young person isn’t achieving when we’re looking at strengths-based approaches and what the person is achieving … especially when young people have got like six people that they have to attend appointments within a week. And then they have to work full-time and then there’s other commitments and study … I’ve witnessed that in care team meetings I’m thinking, well, “How will they be effectively supporting this young person to move forward and reach their goals when they’re in a very negative space in that environment?” (Practitioner 58)
The bigger the care team, the more control we’re putting onto families … We end up just doing a whole bunch of prescribing … and particularly young people, often their behaviour escalates in those situations because they’re like, “Stuff this, why am I talking to three different workers? I don’t even know what all of you do.” (Practitioner 10)
System challenges: Barriers in knowledge sharing and engagement
Despite the lack of consistent frameworks within AVITH-focused interventions, the challenges in relation to care teams appeared to be a consequence of a lack of wider system conceptualisations and capacity to share knowledge.
The collaboration is often actually around having a coherent conceptualisation. We hold the direction of the work and we’re trying to get everyone on the same page and sometimes that might actually be in opposition to what [other] services are saying. (Practitioner 2)
[There’s] a lot of defining the program to make it understood to different stakeholders … the lack of knowledge and understanding around adolescent family violence is palpable. (Practitioner 35)
When we first started … we did a lot of drive back then in terms of community awareness and all those sorts of things. I don’t think that much has shifted to be honest. I think there is a little bit more awareness of AVITH … like there’s a few, there’s a handful of people that I could say, yeah, I remember working with those people but … in terms of staff turnover, I think that’s where our issue is … that knowledge is not sustained. (Practitioner 5)
Practitioners explained that the challenges that they encountered were not limited to the wider service sector, including having to advocate to their own organisations or funders about why they tried to work with young people or families for longer, and that “one of the key barriers, I guess, is that we’re always explaining ourselves” (Practitioner 1).
Practitioners suggested that the lack of consistent conceptualisation identified above could, in part, be addressed through co-location in different service contexts. As well as the involvement of DFV practitioners in care teams, practitioners also pointed to the potential benefits of a dedicated AVITH practice lead in each Orange Door, as distinct from the dedicated role focusing on the experience of children and young people as victims and survivors. Practitioners in this research made it very clear that this existing role was not sufficient in terms of incorporating a specific and dedicated “AVITH lens” into this increasingly prominent Victorian point of intake.
More broadly, focus group participants suggested that collaboration and consistent conceptualisation needed to be led at a government level.
There’s been a little bit of engagement, but it didn’t really manifest itself in the way that I think that [government] had advocated that it would or hoped that it would in that it would be a sharing of practice. (Practitioner 2)
As noted in Part 1, at the time that the focus groups were conducted, the CFECFW had been commissioned to establish a community of practice specifically for AVITH-focused interventions. An AVITH-focused practice guide to support risk assessment and management was also being developed as part of the Multi-Agency Risk Assessment and Management framework (MARAM), which is now driving the Victorian response to DFV and was recommended by the RCFV.
More broadly, participants across the focus groups – especially those in established programs – observed the lost opportunities to harness their experiences and practice expertise before the 2021 injection of funding was rolled out. Practitioners from newly funded programs noted that they had not been provided with any design parameters.
I read a lot of textbooks. Actually, I’ve read two textbooks and I read some things like the PIPA project and there was one from Monash [University] and there was a bit of literature from a similar program … about 10 years ago. (Practitioner 17)
Practitioners working in established programs similarly noted the challenges for their own practice, given the lack of specialised training around AVITH or resources. Some had been involved in one-off training, including in 2017 when the PIPA project funded a visit to Australia by one of the founders of Step-Up, Lily Anderson, but this training or similar opportunities were not recurrent.
I found it in the [organisation’s wider] training manual. There was this little piece [about AVITH]. There’s so much emphasis on perpetrators … and it can kind of get lost in that and then the whole community doesn’t even understand that this is a very different issue. (Practitioner 6)
While recognising the absence of training, focus group participants noted that the system demands were such at present that they no longer had the opportunity to share practice experience with each other.
There’s a few of us that have been doing this for a long time, so we’ve probably got some really valuable things where they don’t need to reinvent the wheel … I think about even the collaboration with other [AVITH programs]. We don’t really collaborate that much either. We don’t have capacity … (Practitioner 5)
Overall, practitioners called for significant workforce development, as well as capacity and capability building that included opportunities for clinical supervision and reflective practice to mitigate the impacts of vicarious trauma and the stress of working in this environment. They also called for capability building to ensure that all work “was occurring through a trauma lens” (Practitioner 10) and incorporating understanding of DFV, young people, mental health, disability and neurodevelopment as part of what one practitioner described and others in their focus group agreed was a “specialisation upon specialisation” (Practitioner 16).
Part 3:
Signs of promising practice
Introduction
Having explored the many challenges that the research identified in relation to delivering effective service responses to young people and families experiencing AVITH, this report now turns to an exploration of promising practice demonstrated by practitioners and programs in Victoria. In some examples, the promising practice discussed is subtle and focuses on employing a reflective and critical way of working, signalling the way in which work in this area is continuing to evolve. In other examples, the steps that some programs or services have been able to take have been more concrete.
It is crucial to recognise that the extent to which all programs were able to realise their potential was hampered to a considerable degree by the impacts of the COVID-19 pandemic. The findings in this part of the report should therefore be read with this consideration in mind.
Naming and identifying AVITH as a concept
As discussed in Part 2, practitioners highlighted the engagement challenges involved when a program was clearly identified as being designed to address a young person’s use of harm, or as associated with DFV more broadly. At the time of the focus groups, practitioners from one program which had previously been specifically titled “Adolescent Family Violence” were therefore involved in a process to develop a less alienating name and underpinning concept for their program.
We’ve been quite closely supported by … lived experience consultants who have been providing us with guidance and reflective practice around co-designing this program to really look at what is it that young people are actually wanting in this space? How do we actually design this program in a way that is meeting their needs as an adolescent as well as the broader family system? (Practitioner 27)
Similarly, practitioners from programs that had not initially had references to DFV in their title were nonetheless pushing for a shift in language when interacting with clients or referring to their behaviour.
When the program started, it was designed as a “family violence” program and at the time we were using the term “perpetrator” for people under the age of 18, which never sat really comfortably with me … Very quickly we ascertained that, hang on a minute, [we’ve] actually got a whole bunch of young people here [who] have experienced significant trauma, whether that be from family, violence, neglect, abuse, whatever, that looks like for them [and] while it is still a family violence–based program and it is still about adolescents who use violence in the home, we have a very strong trauma-informed process around what has been their experience of trauma and how do we do this in the best, most trauma informed way? …
[Now] … any opportunity we have, we continually make sure … that we do not use the word “perpetrator”, and we consistently try and shift other people’s thinking and language around that, when the opportunity arises in the most respectful way possible. So if we’re dealing with the school and they’re like “Little Johnny has done whatever, and he’s perpetrating violence against others”, it’s like, “He’s using violence” … trying to do that through that education and that gentle move across … (Practitioner 62)
Practitioners from across the research nonetheless observed that, perhaps in tandem with a shift in language, they had noticed a shift in parental receptiveness to offers of assistance. They similarly described a noticeable difference in the way that families were recognising behaviour as “family violence” and identifying a corresponding need for support.
A lot of the families are coming in through our centralised intake, so calling in for family support, calling in because they’re saying they’re struggling with the young person’s behaviour … the word “violence” is used, “young people using violence”. (Practitioner 32)
Those working in a particular program had also noticed an increase in self-referrals that appeared to correspond with the publicity around the newly opened Orange Door as well as associated community-wide discussion about family violence overall.
Similarly, two parents interviewed for the research had self-identified that they needed support in relation to their young person’s behaviour and wellbeing and had contacted DS for this reason, aware of the different kind of support that the organisation specifically provided. The case file review also contained examples of family members – young people, siblings and parents – self-referring for support.
Echoing this growing awareness of certain concepts and use of specific terminology, some practitioners working in the newly funded services – many of which were specifically labelled an “adolescent family violence program” – noted that there appeared to be benefits in being identified in this way as far as collaboration and referrals were concerned. This was because other services were relieved that a practitioner or agency possessed clear specialisation around an issue that they may be finding too difficult or complex to manage within their own practice remit.
The difference here is that we’re an “adolescent family violence” service … If a referral comes to me, now there’s an expectation that you are there for this kind of role, where I think when you haven’t got that title … you almost have to carve it out for yourself. (Practitioner 10)
That said, practitioners had still encountered resistance to this description in different settings, or an overreach in terms of what was expected in others, resulting in inappropriate referrals as described in Part 2. This meant that they needed to adapt their descriptions and work continuously with referring agencies to break down stigma or manage expectations.
We had to work a little bit with our language because the language that we were using is quite strong around family violence and what that looks like. And you know, the term “abusive or controlling behaviour”. And so we had a lot of pushback from the partnership schools and the parents and guardians of the young people, because it was, I guess, quite heavy language and quite strong. So we needed to work more in that prevention, early intervention space and soften that language a little bit for those who had not been exposed to the service system before … On the other side of that, we’ve had … referrals for a whole-of-family case management approach that, for me, sat well outside the scope of what [our] program was all about. (Practitioner 62)
Overall practitioners reflected that they needed to be flexible and give careful consideration to how they referred to their service offering, depending on the context in which they were operating. This included practitioners who conducted youth-focused work (not specifically designed to address AVITH but often incorporating it) identifying broad variation in the way that they described their roles when engaging with family members, schools or a young person’s peers.
I work with families where if I pick [the young person] up from school, they say “Well what are you gonna tell the school? What are you going to tell my friends?” And I say, “Well, that’s up to [you], it’s whatever [you] tell [your] friends, school, whatever, that’s who I am.” I have one kid who says that “she’s my auntie”. I have another kid who says “she’s a family friend of mine”. And I just go with it. I just literally smile. For me, it’s not my role to tell other people why I’m involved … Keep in mind I have young people that are like “she’s my worker” … I have to tell these kids, you gotta tell me this before I come into the home … (Practitioner 55)
While the above reflection is from a practitioner seeking to reduce stigma for the young person and to engage families in the young person’s wider support, the research found that flexibility and consideration of the context are especially important where the presence of current adult perpetration or continuing coercive control may be a factor. This was because use of terminology associated with DFV in any program title can also present a significant barrier to consent being granted by a perpetrator parent (where consent is relevant because a young person is aged under 16), as noted above in Part 2.
Shared conceptualisation and evolving service recognition
Across the research, practitioners described growing awareness of and evolution in the conceptualisation of AVITH that was translating into increased referrals in some settings, while also signalling a need for more support in how to make referrals in others.
It [AVITH] should be identified at intake. Most referrers are usually pretty good at identifying that. I’d say that schools are probably the one that, you know, we get very limited information on the referral form from schools. They’re probably not as used to filling out detailed referral forms as community services agencies are for the rest of our referrals. (Practitioner 22)
Many of the referrals were described as eventuating from existing networks, such as Integrated Family Violence Networks; from relationships that were being developed through promotion and outreach; or from “piggybacking” on existing programs. The research team heard that referrals were increasing from Victoria Police, Child Protection, schools, Parentline, GPs and other primary health settings, as well as through a significant number of self-referrals – including from families from other parts of Australia who had turned to the internet in search of support that was specific to their experiences (Practitioner 2).
As indicated above, practitioners noted that referrals needed to capture relevant information – something that was not only achieved by an awareness on the part of the referrers, but by the referral form’s design: “We need to adapt our referral form, to reflect that families are coming through because … [the form is] very much focused on adult perpetrators of violence” (Practitioner 22).
Having specific programs known and identifiable through the intake process was also described as key so that the “relay” process described in Part 2 of this report could be avoided, or at least minimised. This included where families self-referred for broader parenting or family support and where the centralised intake point could identify that intervention in relation to the young person’s use of harm was warranted and could gather relevant information at intake as a result.
Developing program responses also included identifying the approach that was most appropriate for particular young people and their families, including in the context of diverse communities. This included practitioners drawing on wider resources and programs within their organisation.
So, whether we’re working with a family from a particular cultural background or we’re working with, like a queer family, or we’re working with a young person in care … the families that we’re working with around the young person are very diverse and we’re lucky to have those resources and that knowledge here. (Practitioner 31)
Our organisation] has quite a lot of men’s programs … So I reached out to a few of the workers there and had a few yarns with them about some of the work that they do and I guess sort of took that and looked at how could I implement that into the program we were doing and it was sort of like “We can’t just mirror that because we can’t talk to those young people the same way that, you know, these workers might talk to the men there” … We’re planting the seeds for change … Trauma pathways … are really difficult to heal and to you know, move forward over. And that can’t necessarily always be done in 40 hours or 110 hours that might be allocated to work with the young person. (Practitioner 73)
Crucially, practitioners working across different specialised contexts explained that their approach was led to an extent by the young person themselves.
… you know, asking “What do you do when you get angry … what do you do when you get sad?” Their reaction to that question will then inform what happens next, so I’ve had young people who have just said, “I don’t like emotions, we’re not going there” and I’ve gone “Okay, let’s come back to that and we’ll move over to who is safe in your life.” And there are other people who are happy to talk to that stuff. And we unpack that. But yeah, it’s really dependent on the young person. (Practitioner 33)
Working with multiple family members
While being led by the needs and responses of the young person was central to their work, practitioners also described the importance of identifying opportunities to work with multiple family members, albeit in different ways.
Sometimes it’s safe to do it as a whole family, other times we do need to do sort of separate pieces of work in there. Depending on the level of risk … but we’re definitely not just looking at what’s going on for the primary young person that’s referred but actually looking at what’s going on in the whole family system. (Practitioner 44)
I sort of make one or two goals for the adolescent, but then a lot of the times because, you know, we’re working with young people that are like 12 or 13 – it’s hard for them to make that change by themselves – so you have to include the family. (Practitioner 17)
Practitioners described working across organisations or across programs within their own organisation to provide support to different family members, including siblings.
The referral came from another organisation and the other worker was working with the sibling and we’ve been able to really build that relationship … and get all these other services back involved. (Practitioner 5)
If we received siblings and one was listed as the victim [and] survivor and one … as using violence, we would coordinate within our own team about how we’re responding. (Practitioner 29)
The beauty of this program is that we are able to … highlight the other children in the family who may be being missed … like really checking in with them as well, because often we know that they are overlooked. (Practitioner 26)
This was particularly evident on the case files, with siblings regularly supported in addition to the young person or other family members or even as a pathway to engagement with other family members.
Promising practice:
Supporting siblings
- In file DS126, an 11-year-old female was engaged with DS as a sibling of a young person using AVITH. The relationship between the mother and children involved frequent conflict ever since the father used violence in the home and left four years ago. The mother was often absent from sessions, as she was unwell and in bed, and the young person would attend the sessions on her own. DS worked with the young person to provide mental health support, including counselling and strategies to manage her anxiety. The young person now stays in her room, locks the door and uses breathing techniques to manage her anxiety when conflict arises in the home.
Promising practice:
Siblings as the doorway to support for the whole family
- A sibling of a young person using AVITH was referred to DS after reaching out to a youth mental health/family violence service for help regarding his brother’s use of AVITH against him and their mother (DS532). Through the brother’s engagement, DS contacted the young person’s mother and began working with her across 29 sessions (DS236). During this engagement, the mother reported a history of DFV from her ex-husband and disclosed having to lock her bedroom door to keep safe from her son who was using violence that mimicked his father’s behaviour.
- While the young person using violence declined engagement with the program, DS were able to support the mother and sibling, including through collaboration with the youth mental health service engaged with the family. DS also provided information and strategies to support the relationship between the mother and sibling, as well as how to manage conflict in the sibling relationship
As well as bringing other members of the family into the work, parents, siblings or grandparents could be the focus where the young person themselves would not engage.
Work in the AVITH space doesn’t necessarily mean that the work has to be with the young person in terms of changing that system and, you know, particularly if a young person is refusing to engage in therapy or in a case management program, what are other ways we can support the system to reduce the stress in the family home and seek change? (Practitioner 44)
If the young person is not wanting to connect but actually we can do some work with the parent, we can target our clinical work on what’s going on for Mum. It might be that we’re looking at younger siblings, how can we support the younger siblings instead? Because if that stress is reduced in terms of that trauma history in relation to healing from family violence, then maybe [Mum’s] got more space to think … (Participant 27)
Some programs that could draw on a well-established funding pool or wider resources had a specific focus on supporting parents through providing opportunities to share their experiences and developing new skills and resources. This in large part draws on the Step-Up model of intervention, while noting considerable variation in the way that it is applied across different programs.
When I first started here … there was a really strong focus on the young person being the client. And over the last 12 months, I think we’re now – not so much at the clinician’s point of workload – but more so from a consult and allocations component, we’re seeing probably 50/50 split of referrals coming through that are for young people or for parents. So initially we were getting a few cases coming through where the young people weren’t giving consent and we were just sort of doing a little bit of work with parents and carers to the point now where I do think it’s about a 50/50 split where we’ve formalised it and said, “If we don’t get consent from the young person, we have a six- to eight-week window where we will work with the parents or the carers or the family.” (Practitioner 19)
Practitioners also explained that it could be a key part of their role to identify not only how family members were experiencing their young person’s behaviour but the response of the service system.
I’ve got an example of a young person working with [mental health service] and the family feeling very much left out, discounted, unacknowledged and also that their experience of violence was being minimised … so the young person is saying “This is just my anxiety”, but really sort of minimising that, actually, this is really hurtful, harmful behaviour that is causing a lot of distress. So, in those instances we’ve found it really worthwhile to try and bridge that gap between family and the [other] service supporting that young person. (Practitioner 35)
Although practitioners across the research emphasised the value of providing parents with support and ensuring that their feelings of stigma and isolation were addressed, practitioners also emphasised that it was not just a matter of focusing primarily on the young person’s behaviour.
At times we might spend a lot more time with the parent or the carer, chatting with them about their needs and kind of working through things with them … Because if the mum or the carer is not having their needs met, then they’re not going to be able to implement the strategies of things that we’re talking about for the young person either. (Practitioner 73)
We do often find that a parent’s phoning in distress, typically they’re asking somebody to see their kids straight away to kind of tell them to pull their head in. And so we work really hard around actually naming the importance that we need to slow things down, that actually it starts with talking to the parents first, getting a sense of who’s in the family and we will be asking about … like for example, their attempts to try to engage the young person in services and what’s happened and typically they’ll say … that’s been a failure or it’s escalated violence in their attempts to try to force the young person to engage in support. (Practitioner 2)
Equally crucial to delivering appropriate responses was developing an understanding of parents’ own experiences of trauma and other adverse experiences in their own childhood.
A lot of the time, it’s the parents that are pushing the buttons or don’t know when to let the young person cool their jets and have another go a bit later on so it’s a good thing to sort of teach the parents as well and a lot of the time the parents … pick up some strategies to regulate their emotions as well. (Practitioner 45)
In that session a lot of that parent’s behaviours were talked about … just because of the nature of me coming in with an argument happening. And that’s when we really noticed the youngest sibling’s role in it and how they were reacting. And so I saw a need for support to be offered to the younger sibling and the young person agreed that I should bring that up in a case discussion as well, which was fantastic. (Practitioner 33)
One other thing I’m realising is … the parents have grown up in family violence or, you know, they never had their needs met … so they just don’t have the skills … so [the young person] is getting bullied and presenting with these behaviours, but Mum doesn’t know anything other than, you know, “I’ll give you something to cry about” … (Practitioner 17)
This latter reflection was echoed by one of the parents interviewed for the research. She explained that DS had provided her with crucial support around learning how to parent in a way that was more constructive than her own experience of childhood, which was marked by emotional neglect and experiences of sexual abuse, before further trauma through severe adult-perpetrated DFV in adulthood.
I perpetuated how my father raised me and my sister, which was authoritarian and disciplinarian … [program] helped me out with my emotional regulation and things and not letting it get that far that it affects the children. (Parent 3)
Practitioners described the extensive impacts of adult-perpetrated DFV on mothers who needed substantial support to recover – and, sometimes, simply to be heard by the systems.
A large cohort of the mums, for example, are single parenting and they’re dealing with the ongoing impact of co-parenting with, typically, a father who remains abusive and controlling and coercive and gaslighting and undermining Mum’s authority in many ways. So, a big part of what you have to hold in mind is that the mum is often doubly victimised so they’re experiencing ongoing abuse from an ex-partner, as well as the abuse that’s happening from the young person. So, they’re blamed in all directions … How can you address the trauma in a parent unless you actually see them as a person? (Practitioner 2)
Parents certainly emphasised the support that they had received from DS as very helpful in managing their own experiences, despite the barriers to service engagement with their children posed by COVID-19 in two cases and the withholding of consent by a controlling father in another.
Looking [at it] from another perspective often gave me a different way of handling it – because you get so caught up with your scenario that you forget to step back and breathe … When you’ve had someone screaming verbal or physical abuse at you, it’s definitely very hard to kind of step back and see them in a slightly detached light … because you’re triggered the whole time. (Parent 1)
Even though [DS practitioner] couldn’t work directly with the kids, it really helped for me because, you know, in lockdown, it’s sort of very isolating … So it was still good for me to have that support and it definitely gave me …. not just someone to talk to about it, but you know, support with handling some things. (Parent 2)
… I didn’t know that they had a family violence unit themselves that they could coach me on, I suppose the remnants of family violence from previous partners or years etc. so it doesn’t build up on the children … you know, it could be like an ex-partner of, you know, 10 years ago, but then you still got some PTSD … [practitioner said] write in the journal and reflect on some things … reflect on what this is supposed to mean or what a safe environment would look like for me and the children or what … being happy and comfortable would look like … It was quite cathartic … because it did help me get some goals … like to get a proper job where I could function with my children as a family unit … And that it wasn’t a bad thing that … if I’m going to work …
[DS practitioner] was wonderful. She really helped us connect to be better and, you know … provided me information and coaching … which have been really helpful to get [my] children in touch with their emotions. And letting me know their needs and behaviours they’re exhibiting because of said needs and can’t voice. (Parent 3)
The benefits of support focused on the mother to build protective factors and safety were particularly apparent across the case files.
Promising practice:
Strengthening parenting, supporting mothers
- In file DS789, DS had 35 sessions with the family, principally involving one-on-one counselling/parenting support and case management with the mother. During the engagement with DS, the mother obtained a secure job and housing, and regained access to her children on a regular basis. DS assisted the mother to redirect bills to the father, to receive a utility relief grant and to have a large amount of debt cancelled, and supported her to report any acts by the father that breached the protection order that was in place.
- In file DS954, care team meetings were held with the mother to coordinate supports for the family and to discuss goals. The mother received counselling, parenting support and help to develop assertive communication skills. She also received help with coordination of current protection orders, safety planning and support as the young person moved out of the family home. With the help of DS, the mother “is working on her own mental health and increasing her connections with others outside of the household” and how to enact her safety plan when needed.
- Case file DS043 described support for the mother around regulating her own emotions so that she could “help the young person regulate himself”. A family action plan was also created to improve relationships. The young person started seeing an occupational therapist and psychologist regularly to strengthen his emotional response and has a paediatrician to monitor medication, as well as receiving NDIS support.
Some of the DS work involved raising awareness and supporting mothers to understand the nature of what they were experiencing from their young person, or the likely impacts of past experiences on their children which could enable them to support their children and manage their behaviours in ways which more effectively de-escalated and reduced risk.
Promising practice:
Seeing the young person’s behaviour through a new lens
- In file DS250, DS worked with a mother on parenting strategies, resulting in greater insight into the impact of trauma (DFV from ex-partner) on current family functioning and relationships. During the engagement, the mother adopted a harm minimisation approach to the young person’s risky behaviour, which led to a reduction of conflict in the home and the young person engaging more in school and engaging with DS. Based on risk assessment notes, the young person “has a safe home to go to, she knows this and will go home”. With the assistance of DS, the family concluded that mental health support was the best approach to ceasing the young person’s conflict in the home. It was also reported in the case notes that, following another young person’s court matter regarding an assault in which the young person was involved, her mother had a “new awareness and reading of family violence and its impact”. Notes show that the mother wasdistressed to learn how much it had impacted her and her children and was taking the practitioner’s advice and had a better understanding of the trauma that the young person had been experiencing.
Promising practice:
Understanding family violence
- In file DS932, DS was able to fill a gap relating to the impact of DFV and a death in the family, providing family counselling/therapy around family relationships, as well as individual counselling for the young person and siblings around grief and loss. Targeted individual counselling was provided specifically for the young person around emotional regulation and navigating peer relationships.
Promising practice:
Providing connection
- The positive impact of DS on a parent is reflected in case notes on file DS098, which describe a parent thanking a practitioner for helping her and understanding her feelings after a settlement experience through which this parent felt that she had lost everything.
In some cases, DS supported the victim and survivor mother to do more than understand the nature of her current or past experiences – assisting her to leave a violent adult partner and to ensure that Child Protection were aware of relevant risks.
Promising practice:
Supporting the mother to leave a violent relationship
- During engagement with DS, one family (DS180) experienced positive changes across several elements of the family’s life. The mother received counselling support to gain employment and improve her parenting skills and mental health. She also received support to recognise DFV behaviours coming from her partner and the way that these behaviours impact the children at home. The mother was supported to leave the violent relationship and seek a protection order, resulting in reports of improved wellbeing and family relationships. As a result of the support provided by DS, the young person’s mother reported a decrease in anxiety and depression and greater confidence in parenting, with an associated decrease in problematic behaviour from the children. The DS practitioner kept Child Protection and the children’s school abreast of the new protection order.
Promising practice:
Supporting safety planning
- In file DS054, a safety plan was put in place with police and the mother was supported to speak to police about what needs to happen if they are called. The mother and DS worked together to book in short-term accommodation respite and the mother described beginning to connect with the family violence team at the police station to create a point of contact in making reports where needed.
As noted in Part 2, the ongoing impacts of adult-perpetrated DFV were an overarching theme in the interviews with parents. The impacts of this violence were influencing every aspect of the mothers’ and children’s lives. In all three cases, the mothers’ focus was on obtaining support for their young person and siblings, all of whom had been impacted by their shared trauma in different ways. It was clear in each case that assisting the young person would therefore be a way of assisting the mother, despite her own experiences of harmful behaviour from the young person.
Reflecting this, some practitioners working in court or legal contexts explained that the support they were providing to the young person was also a way of supporting the protective parent, despite the fact that they were likely to be experiencing the violence as well.
Oftentimes the young person is the respondent [to a protection order], but it’s actually Mum … who I work with … because both have the same goals and … they want the young person to get help … obviously it’s [Mum] who drives the young person to the appointments and all that kind of stuff anyway when the young person’s in school and young people don’t answer their phones … so I think it’s usually works [sic] with going through the parent. Obviously, you make judgement calls around what’s safe … (Practitioner 61)
… seeing young people feeding back information from their lawyer back to their worried mum … I think sometimes there is a bit of relief … that the young person has either a lawyer or at least a service that’s checking in regularly … even though sometimes that’s unsafe and inappropriate, but other times … even if you’re not working with [the protective parent], you still kind of are working with [the protective parent] because at the end of the day these young people, they are dependent on someone for care as well … (Practitioner 51)
By contrast to circumstances in which a single practitioner was working with the young person while keeping other family members in view as above, some programs – including the DS program – were purposefully drawing on multiple practitioners across the agency.
It starts right from when we get the referrals … When we’re doing the allocations, if it’s for one of the parents, first to start to see what their support might look like … and we read in the allocations note around who could potentially be the practice lead based on the support needs of the family and who the practitioners … will be as well. So, we start that discussion right from the beginning and … then we set up regular … “case discussions” with the practice lead and the practitioners working with the family. (Practitioner 31)
Practitioners explained that this approach included identifying which practitioner was most appropriate to contact each family member, or where consent from parents was required. Conversely, information sharing was vital where it may be useful to bring in another family member but where a young person was the presenting client. In these cases, this contact with the other family members was discussed with the young person and not initiated unless endorsed by them.
Practitioners, including those from DS, described how they might start to engage with a young person while keeping the whole family in view.
I find a family tree, just making that kind of genogram, that is the best place to start … they often really easily engage with the family tree and unpacking the different family members and usually pets is a really, really positive place to start and will tell a lot about them and what they deem as important and their connection, which is often overlooked by other family members or on the referral … What it has also done is it has allowed a breadth for actual safety planning, because … how it’s constructed is different … So how are we safety planning? How are we talking about that? What does that risk mean? For whom? When does it change? At what times, and what are we noticing? (Practitioner 33)
Work by DS with young people evident in the case files on occasion had an emphasis on early intervention. The research team heard that this was possible given that a significant number of referrals were coming from schools or through self-referrals in which young people or families identified the DS suite of programs as a possible source of support. In certain cases, being able to engage the young person was a particular achievement for the reasons that the research has explored around young people’s distrust of services and the impact of prior negative service engagement.
Promising practice:
Strengths-based approaches and exploring positive experiences
- In one case file (DS432), the young person spoke about a range of hobbies and activities, as well as casual employment, which were used as part of safety planning and building rapport with the young person. Safety planning included the young person retreating to his room to play video games, as his family respects that boundary and leaves him alone; going for a walk; or talking to a friend. After only three sessions with the DS practitioner, the young person reported no longer feeling fear to return home or fear that the yelling would turn into physical violence. The young person reported being able to leave the situation and return to his bedroom when the yelling erupts within the family unit, which is a strategy discussed with DS to diffuse the arguments.
Consistent with broader practice experience and evidence, practitioners working in Aboriginal community-led organisations placed particular emphasis on ensuring that the whole family was supported, even where a young person’s behaviour and the factors contributing to it were the service entry point. This focus was situated within a broader emphasis on connection to community and whole-of-family responses because, as one participant explained, community-led programs were “not prepared to shut anybody off” (Practitioner 72).
We do our [risk assessment and management] assessments keeping in mind what is impacting on our community members, physically, mentally, emotionally and spiritually. A lot of the time it’s disconnection from their community, so that’s part of the spiritual realm and our role is to get them back connected into the community … Why I push for these groups to happen is to get them connected with other young people … So, [other practitioners are] working with the family while [youth-focused practitioner] focuses on the young person. And so we can provide case management support, whether that’s through our family services stream, out-of-home care stream, kinship stream, family violence support, NDIS support, playgroup supports, we’ve got all of those services here at our fingertips that we can refer into those different areas and strengthen that family. (Practitioner 74)
Practitioners from the program above explained that a young person’s progress needed “to be supported at home as well, not just in the couple of hours that we see them” (Practitioner 73). One noted that a careful balance was required to ensure that unconstructive messages were not being delivered.
One thing that kind of sat a little bit uneasy with me was if … the young person that’s been using violence at home is being taken out to … do all these fun things together that it doesn’t necessarily send like a good message to the other young people. So, I kind of would start to also take some of the siblings out as well – not each time, because we want to have those conversations with the client that we are working with but, you know, if we’re going to a movie every now and then or do something fun … I’ll bring those other siblings along as well. And so, it’s … not setting that sort of strange dynamic of the person being rewarded and it’s really nice, I think, that some of the families that have not had that experience before of, like, going to a movie and doing those kinds of things and it kind of brings the siblings closer together as well. (Practitioner 73)
… I know it’s a word that’s thrown around all the time. But it’s “community”, we aren’t just working with one person in the family, you have to include all of them. If you’re going to take one of your kids to the movies, same with my kids, you don’t just take one of the kids you take all of the kids. And you’ve got to keep that balance in the home as well. (Practitioner 74)
Capacity for flexible, client-centred approaches
To a significant extent, funding and design parameters dictated the types of activities which were able to be conducted through AVITH-focused interventions, with capacity for flexible and client-centred approaches emphasised as being particularly crucial. The research also indicated a critical interrogation of service interventions as the more well-established programs were learning about what was effective.
I think [well-established program] just keeps evolving and I mean, as practitioners, we have the scope to respond to our clients and meet them where they’re at, so nothing’s really off the table. So when I have worked with an 11-year-old, you know, like high functioning autism … the program is supportive of that … [That child] had, you know been in so many services and he was in the care of his grandma and they were at … breaking point. (Practitioner 5)
We try to very much meet the young people and their families sort of where they’re at, we have a very significant focus on improving safety and really understanding, kind of where the adolescent sits within their sort of own internal family systems, but also within this sort of wider community. (Practitioner 16)
For instance some of the ones at school, they might be using gender shaming, sort of behaviour to other students, and they would be, you know, using a racial slurs [sic] and things like that. So they’re sort of indicators to us that, you know, it’s possibly a learned behaviour and then we sort of ask a few more questions and establish if this is ongoing or whether they might just be having a bad day to help direct our support a little bit more. Then it can be, you know, to the other sort of spectrum of they might have had a suicide attempt, which we tend to get a lot more of those in the community referrals. (Practitioner 62)
This included, as noted in Part 2, varying approaches to the use of group work, with one program moving away from it, one focusing on parents, and one running concurrent groups, as described below.
We’ll start it off … with both the young person and parents to get a clear understanding of the goals. And then normally what I will do is separate it just because of their adolescent age and stage of development, they take a little bit longer to pick up on some topics compared to the parents … Say, for example, I might meet with the parent and young person every week separately and then that parent work might drop off for a time, so the young person can pick up on a particular concept … it might take a little bit longer for the young person to pick up on their warning signs and their triggers and a timeout plan is not really super effective unless they can really start to identify their warning signs. (Practitioner 19)
Practitioners across other programs offering group work to young people (resourced through different funding streams) also described the need to consider the composition of any group and its potential dynamic across age, as well as types of behaviours exhibited and risk indicated.
If you have a whole bunch of 13-year-olds who are [engaged in] gender shaming and verbal abuse of their siblings and family at home, they … sit within that family violence range but, on the continuum … they’re at one end. And then you have a young person who’s exhibiting significant physical violence within the home. We would consider putting that person in a group that’s a little bit older with more high-risk behaviours … (Practitioner 64)
Practitioners explained that interventions needed to be sufficiently resourced to work in a flexible, client-centred way, highlighting that working with a culturally diverse range of young people could sometimes mean that young males may not want to engage with female workers (Practitioner 57). The research team also heard that some young people would respond more effectively to a practitioner from a certain age group than to others (Practitioner 18). Practitioners similarly explained that a considerable amount of sector and workforce development was required around working with young people from CALD communities, with referrals often directed in a siloed way towards dedicated services because mainstream services were not able to respond appropriately (Practitioner 10).
To note, practitioners from different ACCOs had varying views about group work involving young people. A participant from one organisation explained that it was important to understand how a young person was going to respond to being around peers, reflecting below on the needs of a particular client.
Our men’s group, there’s all sort of walks of life there. And we’ve got Elders there, we’ve got people that are in their 30s … So we do art pottery, woodcarving … they go on trips together to see various things … We’ve specifically done it that way because our Elders need somewhere to go and they’ve got some wisdom. They’ve perhaps been there and done that … and they’ve changed and got through life and come out the other end and become a respected Elder … and it’s teaching this young fella to be respectful … We’re not all pointing the finger and telling you off, these are people that care and want to look after you.
Yeah, I think if it was a group of young people, young boys, different story, you’d just be asking for issues then. But because I’ve got such a mix of ages, it doesn’t come to that ever. I think what we’ve gotta do is teach these young people how to speak to people properly and how to respect their Elders, but also how to respect their parents and their mums … There’s a place for a young group, but … where this kid is at the moment, an older group is better for him because he’s wanting to learn respect. (Practitioner 72)
Practitioners from another ACCO, however, saw particular value in their groups for the young people with whom they were working.
The group is really great because the young people get to connect with each other in terms [of] where they are on their journey, not just on their journey of, like, who they are as an Aboriginal person but, you know, as teenagers. So, who they are trying to become or who do they want to become? They’re trying all those things out to kind of see what they want to do, what works for them and all of that … For some of the young people that we work with, it’s the first time that they kind of really identify as being Aboriginal …
And I think having that kind of space like at the youth group and at the men’s cultural camp that we went to, having those yarning circles and introducing the idea where [you] can go around and talk about who you are, who your mob is or where you come from – all those kinds of things are a great way to kind of introduce the idea of that. (Practitioner 73)
It’s important to recognise that their peers are a huge part of their life … because it gives them more confidence to be able to be who they are … And that’s what we’re striving for, aren’t we? You know, we are wanting these young adolescents to grow up knowing who they are, to be strong and who they are and be able to be out in the community and society. That’s … hopefully our goal. (Practitioner 75)
Sequencing and readiness
Across the research, practitioners highlighted the need for interventions to be guided by what clients identified as their own needs and preferences, rather than what a service might assess. A feature of this involved assessing the extent to which clients were ready for particular interventions or had the capacity to engage, staggering or sequencing support depending on what else was happening in their lives.
Generally, we’ll have an initial meeting to work out, “Well, who’s doing what?” So then everyone’s pretty clear … working out who does what and whether we stagger things … so that we can maintain a good engagement and the families aren’t feeling overwhelmed either with different service responses and different information all at the same time. (Practitioner 1)
One of the exciting components that we have in our program is working in partnership with case management and a clinical role, so there’s kind of that capacity for young people if they’re not kind of therapy ready, you know [for] the case managers to kind of walk alongside them and develop that therapeutic relationship that can potentially … then articulate into the … integration of a more clinical intervention later on. (Practitioner 26)
Importantly, an example offered by an Aboriginal community-led service involved significant thought put into supporting a young person who had an extensive history of trauma, including child removal. The service described consideration about sequencing over the long term, prioritising secure housing, and work to obtain identification documents, given that these did not exist, which could allow him to access Centrelink benefits.
During this time the young person was also linked with cultural programs and was volunteering to help with the service’s NAIDOC event. He was also linked with assessments for relevant language and developmental delays. Eventually the plan with the young person was to work towards securing employment,
’cause if we don’t capture him before 18, 19, and it keeps going down the path of stupid petty rubbish, he’s gonna be in big boys’ jail and then we’ve lost him. (Practitioner 72)
Case files similarly indicated that effective intervention required considerations around sequencing. The following promising practice example illustrates some of the complexity involved in considering how and when work should occur – and with which service.
Promising practice:
Flexible and client-centred approaches – sequencing
- In file DS054, care team meetings took place for the family on a monthly basis for one year and, through these, long-term work was done between the Children’s Court worker, behavioural specialist, [children’s hospital] worker, social worker, DS and the mother. The case file shows collaborative work and collective decision-making through care team meetings with a diverse range of supports offered. In particular, detailed conversations occurred between the young person and the Children’s Court worker around the diversion process and the importance of taking responsibility, as well as ensuring that the young person understood their legal matters and obligations.
Collaboration occurred between care team meeting practitioners (occupational therapist, Children’s Court worker) to teach the young person about family violence, while the mother was supported around safety planning and how to make reports of breaches of the order.
Plans were also made for DS to work on an NDIS application with an NDIS coordinator to coordinate respite and safety planning with police, and to arrange a referral for a specialist with expertise relevant to the young person’s complex needs.
Outreach and activities
The research team heard that being led by a client’s preferences included recognising that working with young people requires adaptability. Practitioners explained that the value of many of their programs was that they were voluntary, so that young people who had a history of negative service engagement – such as the young people described by parents interviewed for the research – would not feel that they were compelled to engage but could gradually form a “therapeutic alliance” (Practitioner 55) with a worker. They also emphasised that outreach and flexible working practices were an increasingly well-utilised part of their approach.
The day-to-day would be, either clients coming into the office, but some clients don’t really like doing that, so a lot of it is outreach. (Practitioner 13)
If you’re not doing outreach, you’re not seeing their family home or their family situation as a whole, you’re only seeing what the [referral] provides you with, I think we pick up on a lot more of what’s impacting on the clients. (Practitioner 20)
Participants described their insistence on maintaining the capacity for outreach during COVID-19 lockdowns, finding flexible ways to “maintain eyes” on young people and families and get a sense of what was occurring in their lives, even if practitioners could not attend a young person’s home and get the fuller picture about risk and support needs which could not be obtained over the phone.
I did an outreach walk today for 15 minutes, during COVID, just to keep them engaged, ’cause if we do not keep sort of speaking with them and meeting them, they do fall off quickly. (Practitioner 14)
This was particularly the case for ACCOs
Our expectation was that our workers still got out there to … make sure the families were okay. (Practitioner 74)
We do home visits a lot, the petrol bill tells me that we do a lot in the cars! (Practitioner 72)
The research indicated, however, that capacity to conduct outreach varied across services and systems, with many programs relying on other services where they did not have outreach counted in their caseloads or where they could not access vehicles to facilitate the outreach.
Services love to lean back on [our program] because we’ve got cars, and we go and see young people, and we do all this wonderful organic work with them so they go, “Will you do it?” And you have to be really kind of boundaried in saying, “We don’t have that capacity.” (Practitioner 52)
Practitioners also discussed the potential benefits of outreach approaches being adopted in contexts beyond community-based programs.
Outreach is the most critical component working with young people … I think that courts need to start stepping up and having some component of outreach capacity …You know, there’s something about needing to be able to go to where people are at … to conduct these assessments around what’s really going on … Every case is an iceberg … but half the information that’s reflected to us about what’s going on for the young person, if you’re just getting it over the phone, I mean it ends up being the least important information you could get, than what you get in the home. (Practitioner 35)
Case files similarly indicate that outreach was considered vital where possible, so that practitioners could increase their understanding of risk present across the family structure and develop rapport.
Promising practice:
Flexible and client-centred approaches – outreach
- In case DS169, DS and a mother spent considerable time and effort unpacking different ways to offer the young person support, including via outreach sessions, providing flexibility for the young person to elect the day and time that would suit him best, and giving the young person full autonomy to decide how he would like to “meet and greet” the DS practitioner.
Promising practice:
Flexible and client-led approaches – working with schools
- In file DS233, where a young person had been refusing to engage with school online, DS supported the mother to approach the school and facilitated a flexible arrangement where the young person could attend school during the COVID-19 lockdowns. Supports were coordinated for the family through meetings with the school, an occupational therapist and NDIS workers to arrange allocations of support that was better suited to the family’s specific needs.
Just as important as outreach was an approach that responded to a young person’s interests or involved shared activities. This could include, as one practitioner described, connecting young people with older mentors who shared an interest, such as skateboarding, and generally “thinking about what a kid actually wants to do and therefore how they will engage” (Practitioner 67).
Practitioners across the research similarly noted that young people were more likely to engage during shared activities or be particularly likely to engage in conversations while driving together, rather than sitting face-to-face with a worker. As noted in Part 2, practitioners explained that young people were usually disinterested in what services described as “talk therapy” (Practitioner 52). This was especially the case where previous negative experiences with wellbeing coordinators at schools or psychologists – such as those of the young people described by parents interviewed for the research – had not made a difference and had potentially contributed to a young person’s mistrust of services instead. “A lot of young people don’t want counsellors. They don’t want to see a therapist, so we talk about support workers, so just use different language” (Practitioner 61).
These observations from practitioners were also echoed very strongly by one parent, who emphasised the importance of practical, physical support and outreach-based activities.
I wish organisations would see that, for kids, especially when there’s a lot of trauma … playing into it, sometimes they need someone not to speak to, like a counsellor, but, “Hey let’s play [a] game of footy”, or “Let’s go for an ice cream”, or “Here, let’s bake a cake together” or something like that so that they can build that friendship, that rapport, just connecting with them … [and] can feel comfortable enough to talk. (Parent 1)
Practitioners also highlighted that the hours that they worked needed to be examined when developing more appropriate and “user friendly” responses for young people.
Working with young people … you don’t put meetings on of a morning with young people because they’re not out of bed yet. So thinking about, you know, when is the best time to work with young people? Is it 9 to 5? Is it 12 to 8? I don’t know but thinking about the end result being about how the user accesses us, rather than how we access a client. (Practitioner 19)
Length of engagement
Also highlighted as particularly crucial across the research was the capacity to work with young people and families over a longer duration, as referred to earlier in this report.
Practitioners working in the more well-established programs had greater capacity to work with clients over the longer term.
A real asset and value-add to the program is we’re not time limited. So, as with other interventions, there’s you know your 40 hours or 110 hours or whatever they all are, we have three to six months to work with the client and we can go either side of that and we do go other side of that, so I think that’s a real strength … at the end of interventions with young people who had spent a significant amount of time, like, you know six to nine months within the program and the biggest reflection that [one young person] had was, “I was able to build a relationship with you” and “You were able to understand what was going on” and “I had the time and it wasn’t that I had to then go on to another service” … And there was significant behaviour change within that family, so I think that that is a really, really big strength of the program. (Practitioner 20)
Another long-running program insisted on the capacity to work with clients over one to two years where necessary, but noted that meaningful benefits could usually be realised within a shorter period of time.
… actually 75 per cent of the families we work with have significant change in less than 12 months of intervention. And when it comes to those that need the longer term support – and we’re talking years, kind of stuff – that’s not a huge proportion, it might be 25 per cent of our client group. (Practitioner 2)
A practitioner from one participating ACCO also emphasised the importance of giving families and individuals time to engage and, perhaps most importantly, re-engage.
We don’t have time limits on people … It can be hard for the workers because they do a lot of work with them at one time and then it’s all wasted and then, you know, they come back six months later … Eventually, though, somebody wants to change and then that’s when you grab a hold and don’t let go really … It’s about when that person’s ready to make the changes they need to make, we’ve gotta have the door open for that time. (Practitioner 72)
Practitioners from DS emphasised the value of their organisation “allowing them to take time with people and move at whatever pace feels right for the person” (Practitioner 33), tailoring the support uniquely to the family and individual. In particular, they noted that working towards engagement of young people requires that the provision of support is not time-limited, so that young people can see that engagement with the DS service does not hang on certain conditions.
Promising practice:
Steps towards building attachments
- Although DS originally engaged with the young person’s mother (DS233) for mental health and parenting support, months after initial engagement, the young person consented to being on a separate case and was engaging with face-to-face sessions. Through these individual sessions, DS and the young person discussed the young person’s self-harm and suicide risk, anger and family connection issues. DS worked with the young person to build a degree of positive engagement with his parents. A parent whose child had not been able to be engaged through the program because of COVID-19 nonetheless noted the potential of longer-term engagement. “There has to be some continuity for kids like, whether it be the same person, that’s always all the same. Maybe two people for safety reasons …” (Parent 1).
Brokerage
A further theme which emerged spontaneously from the research was the value of brokerage which had been made available through the newly funded programs. Practitioners described examples of ways in which they had used brokerage, such as putting funding towards a young person’s braces because their need for them was impacting their self-esteem (Practitioner 22); purchasing equipment which could provide an outlet for a young person’s energy, such as gym equipment or trampolines (Practitioner 27); funding NDIS assessments; or even providing specific supports, such as counselling, for siblings.
One of the nice things about the way that this program has been funded is that we had so much brokerage attached so that each sort of individual response that we’re providing with families we’ve been able to purchase in some really specific interventions … that make a really tailored response and not like one-size-fits-all. (Practitioner 26)
So we’ve used brokerage to support some respite for the young person to actually spend time away from their family to just break that cycle of the … relational intensity and build-up. And it seems to be a really big gap in service provision, being able to access respite, because at the moment we’re using brokerage for that but … that ends up being the young person going and staying at in an Airbnb … yeah, it seems to be a really big gap. (Practitioner 22)
Importantly, practitioners working in Aboriginal community-led contexts were using brokerage in a range of ways. This included to access specialist assessments; providing families with vouchers to assist with shopping or petrol; funding activities such as taking young people out to buy lunch or go to a movie; providing them with sports equipment, such as footballs, where the young people may not have these themselves; and even providing backpacks with clothes and accessories from Clothing the Gap.
Early last year we purchased some really good bikes for a lot of clients. So, you know, that was a really helpful thing, not just for the kids to have fun after school, but it meant that some of the kids are riding their bike to school and then Mum is, you know, has a couple of less kids or maybe no kids to take to school first thing in the morning. And so that’s like a bit of a burden off the family for that … We’ve bought a few kids music equipment and something that, you know, working with them, they’ve identified that that’s a therapeutic thing for them. They can go into their room, they can play keyboard, headphones on or listen to music or they’re writing music. (Practitioner 73)
As well as describing ways in which brokerage could help to alleviate pressure on families or give young people an outlet or respite, practitioners also explained that what they purchased for young people could often be directly related to safety or any needs for immediate assistance.
We’ve bought some phones and computers and things like that so that we can provide those for young people. And I think the phones, particularly, are really important because it’s a safety sort of planning mechanism for young people as well. [For example] with Beyond Blue they have that app where you can kind of put in all of your safety plan … into the app and like headspace do have an app where you can kind of text as well instead of calling the helpline or whatever … And so, I think the phones make up the important component of that. … we pre-purchased a bunch of those so that we’ve got them ready to give to clients … (Practitioner 73)
A practitioner from another Aboriginal community-led program similarly talked about the value of using brokerage to provide whole families or young people with positive experiences and ways that they could see themselves in a positive light, a theme further explored in the section below.
And you know it’s giving them that experience, they go down to Scienceworks and those sorts of things … We were able to get a lot of tickets for the Dreamtime game, so we got a lot of families into that … It’s sort of stuff that some people just think of as normal but, for our families that are in low socioeconomic situations, they can’t afford to do things like that. So it’s just about being a bit proactive … being involved with the community … and not just waiting for a crisis. (Practitioner 72)
Strengths-based approaches and shared positive experiences
Across the research more broadly, practitioners volunteered the importance of helping families – who had often lived for a long time as if they were “walking on eggshells”, as the wider research describes (McKenna & O’Connor, 2012) – to have shared experiences which enabled them to see their family in a different light and therefore signal the possibility for further change. As noted in Part 1, wider studies increasingly suggest that positive relationships offer a significant protective factor against AVITH (Elliott et al., 2017; Kehoe et al., 2020), with findings from the ReNew program emphasising the importance of mothers and sons building attachment and positive memories (Burck, 2021).
Particularly striking across the parent interviews was the extraordinary resilience and strength of all the mothers and children involved, with mothers continually looking for positive experiences and connections for their children, while young people and siblings were often doing the same. That said, two of the three service user interviewees suggested that there was such extensive and varied trauma in the lives of the mothers and their children that relationships remained incredibly fragile, with their collective identity formed around their shared experiences of harm. One mother had recently started working and studying, encouraged by DS, contributing to a shift in the way that she saw herself which was having a positive impact on her relationship with her children.
Certainly, the focus groups suggested that creation of positive experiences and development of positive attachments were particularly important in the context of families’ exposure to adult-perpetrated DFV or wider intergenerational harm: “We’ve funded lots of vouchers and that sort of thing so that families can spend time together sort of forming positive memories” (Practitioner 25).
Creating opportunities for positive experiences was particularly important in terms of supporting young people. The research team heard that this was because young people were forming their identity during adolescence and should not be forming their identity around negative views of themselves.
I’m often really mindful and careful about the way that we present ourselves … during an identity-forming time of a young person’s development … we often get them at the age where they’re really starting to put their heads up and choose from the world who and what they might like to move towards being. (Practitioner 52)
That’s what I do find the hardest is when you’re working with the [17- and 18-year-olds], like some of the ones I do in the one-on-one stuff. They’re like, “I already know I’m the problem, I know I’m shit, I know I’m not going to change and I’m going to grow up and be like Dad” and it’s just like, “Who has told you that?” and it’s like every system, every adult, every teacher that kicked you outta class. Every footy coach that didn’t put you on. And that is hard. (Practitioner 44)
Stigma and shame played different roles for the young people described in service user interviews. One child was using harm in the context of his disability and experienced significant shame after each incident. Another was being manipulated by a separated father to control a younger sibling. A further young person who was using harmful behaviour at home – while experiencing very acute mental health distress – appeared to feel additional shame that he had not “coped” with their family’s experiences like his siblings. Long periods of school disengagement related to a mother’s illness also contributed to low self-esteem.
One of the parents participating in interviews described that the only thing that seemed to make a difference for her child was the informal support and interest from an older sibling.
I really need someone who can physically get in here and help me with that aspect of things. I’m so lost on what and how to do that. And like, [older brother] has gotten in there and he goes right “You’re coming to the gym with me” …. and you can actually hear [adolescent’s] conversation change because someone is physically taking an interest in him … (Parent 1)
Practitioners in the focus groups spoke correspondingly about the importance of avoiding a deficit-based approach and, in some cases, not continuing to focus on what young people were doing “wrong”.
I think young people … notice a difference that we don’t get the big sort of problem saturated story … and just go in and take that deficit approach, like “This is going wrong, you’re not going to school, you’re doing this” … (Practitioner 45)
I guess you know when someone is saying over and over again that they’re not going to school … sometimes you have to go, “Okay, well are we just going to continue to have only that conversation with them … or do we look at other alternatives?” (Practitioner 73)
Clearly, we’re responding to family violence. But … when I speak to young people, I mention that I’m … just wanting to check in, if you’re feeling safe, ask if there’s anything that you need support with but, really, wanting to start with where the young person’s at in terms of what they identify is most … pressing for them … I’m trying to have that opportunity to connect with a young person, you know, affirm their experience and explore “What supports do you need?” And just be able to recognise … it’s hard to know how to contain yourself when you’ve had all of these experiences that have meant that relationships are difficult … I do really understand the limits and constraints of the system … but I still think that’s not an excuse for … not striving for best practice and not striving for upholding the dignity of young people. (Practitioner 29)
Building positive engagement between protective parents and young people – as well as leveraging the strengths and protective factors in a young person’s life – was deemed to be key. In many case files, the DS practitioner discussed protective factors for the young person and asked the young person about their interests, hobbies, employment or any other positive features in their life, particularly those that divert from the situation of violence within the home.
Promising practice:
Building rituals and recognising developmental stages
- In case DS021, DS worked collaboratively with a parenting practitioner who supported the young person’s mother by providing resources and strategies including videos about children’s developmental stages, tip sheets, redirection and distraction for children when conflict occurs, and ways to build rituals into the week. Notes recorded a discussion with the mother about using a communication book or app for all communication between the parents as well as considering Child Protection notifications, where appropriate, in relation to a perpetrator father’s ongoing systems abuse.
Practitioners from Aboriginal community-led programs described connections with culture as a particularly valuable way of strengthening young people’s views of themselves and their place within family and community. These included developing cultural support plans in collaboration with young people where they did not yet have strong connections with culture or community.
We really try and keep kids engaged in our youth program and that’s, you know, it’s once again embedding culture in their lives. Our youth team, both junior and senior, are learning to dance. And yes, so it’s just doing things on that they make damper and they do, you know like it’s active things. So it’s not just sort of sitting there and doing lessons … (Participant 72)
So, for some young people that might be playing music or joining the footy team or connecting further to culture … that might not immediately look like something that is a response to the family violence incident but … we’re looking at people that are still developing their skills and being able to make decisions … We’ve also recently had a cultural boys’ camp … I think the boys came out of that a lot stronger in themselves … learning some cultural knowledge that is pretty hard to find out in the streets of Melbourne … that can give them a stronger sense of identity and to make … decisions that are not just shaped by them as young teenage boys but shaped by thousands of years of history. (Practitioner 73)
What happened with working with the Elders at the camp was that they got to build or create their own didgeridoo and they got to use it … and a week or two later, we had a community event for NAIDOC Day and the person that we had asked to come in to do the didgeridoo couldn’t make it. This is the impact from what happened at the camp – those boys that had just learnt the didgeridoo and they played at this event! So, what I’m trying to say is that the impact of culture, these young people building their self-esteem, their confidence, their identity, as a fundamental part of their wellbeing, as well as their family and community … (Practitioner 74)
Importantly, practitioners from ACCOs also highlighted that cultural identity was “broad and complex”.
We have so many Aboriginal and Torres Strait Islander people coming either interstate or who are coming within different regions of Victoria who live in this area. So, it’s about being sensitive as well because they’re from different mobs … but what [it] provides is like a – I don’t know if I can say it in this way – like a blanket, a comfort blanket because we provide Elders that are here to talk to our … adolescents … which provides that support for Aboriginal identity because, although they’ve coming from different areas, they still get that connectedness and that way of linking themselves back to who they are. (Practitioner 75)
Giving voice to young people and their experiences
As well as the value of working with family members and, as one practitioner above described it, seeing the parent “as a person” (Practitioner 2), the research indicated that a crucial component of effective AVITH-focused interventions is giving voice to young people and how they have experienced their world.
This work is really, really trying to centre young peoples’ experience and really trying to, you know, affirm that young people are primary victims [and] survivors in their own right, and when they’re using violence, that’s telling us something that’s giving us information about what their experience has been [and] their development so, you know, I think it’s such a missed opportunity if we can’t connect with young people early … having a positive experience where they’re not feeling judged and not feeling like they’re the problem … (Practitioner 29)
… knowing your rights in terms of like your legal rights. Also just your human rights in terms of privacy, respect … freedom of mobility … (Practitioner 28)
Some practitioners suggested that this could have benefits in both directions, noting young people’s limitations to have full choice and agency over their own lives.
I do think giving a voice to children, particularly adolescents, is really important, because … if you give adolescents a voice, you can also address accountability. It’s a two-way street. If they have a voice, you can also demand responsibility. (Practitioner 69)
A dedicated legal service working with young people as respondents to protection orders explained that they had a unique opportunity to give voice to young people because they could establish rapport and trust once young people understood that the service was working exclusively for them, as explored in detail in the PIPA project (Campbell et al., 2020; see also Centre for Innovative Justice, 2022).
We do prioritise their own safety and will always ask questions around how safe they feel at home and often that leads to disclosures … Generally, we may be one of the first people they’ve disclosed to … The young person’s often fearful of telling anyone else, particularly fearful of [Child Protection]’s involvement or getting moved into a resi[dential] care or they’re fearful of repercussions from their parents, of anyone finding out … Our conversations have that legal privilege, so they’ve finally found a safe way to tell someone. (Practitioner 49)
Giving voice to young people was not limited to facilitating disclosures of harm or wider traumatic experiences but was also about a practitioner being an advocate for the young person where they were not present or able to tell their story themselves.
There’s been a real focus on diagnosis like mental health diagnoses as “This is the issue, this is why this is happening”, “There’s ADHD” or “There’s this or there’s that” and I’ve noticed a big shift recently … around not just services looking for diagnoses but parents looking for diagnoses too. So them actually not seeing themselves as part of a solution, it’s like “I need to get my kid diagnosed because that will then explain everything” … I had the same experience even this morning discussing a young person in a care team meeting and, yeah, the first response was “We need to get them to a paediatrician and get them assessed for all these things”. And I’m sitting there saying “Well, there’s been about 15 years of trauma here” … (Practitioner 10)
Actively leaving room and time for identification of experiences of harm in the context of assessments was therefore crucial.
We have improved our assessments and sometimes it doesn’t show up until the course of treatment that you see that Mum or Dad are using aggression in terms of their inability to manage their own distress, so it’s typically co-dysregulation[2] in that context. (Practitioner 38)
We do risk assessments for each adolescent we work with in our initial assessments, but like you know it can take several engagements before the young person even discloses … The [young person] with the speech [disorder], it was like six sessions and Mum eventually said to me or
“You know, last time Dad got on the beers, the kids were pulled out the window by the police.” (Practitioner 17)
Violence doesn’t just come out of nowhere for these young people … these young people are generally survivors of experiences of violence, either past or current. So that’s something that we’re always keeping in mind … that’s my priority when going into these assessments, finding out about the safety of the young person and what’s going on at home … (Practitioner 49)
Keeping an original perpetrator – and potential systems abuse – in view
The research showed clearly that assessments for young people’s exposure to adult-perpetrated violence need to include assessments for current experiences. Where an adult is separated from the family, this should include mapping and understanding the impacts of ongoing systems abuse or, as one practitioner called it, “the shadow of the perpetrator” (Practitioner 27) in the young person’s life. A crucial part includes understanding the impacts of this on an adult victim and survivor.
I definitely take the strong family violence lens of kids’ behaviours are definitely triggering and re-traumatising Mum and her responses are in the [context] of that but also that the adolescent family violence is not Mum’s fault and … re-framing that with her and just working with her to strengthen that …
I’m thinking of one particular client at the moment where the children’s behaviours have just escalated beyond belief, you know strangling Mum, phone-stealing, stealing car keys on purpose and locking her out and things like that and Mum just doesn’t have the capacity to respond to that because it’s re-triggering her from the family violence perpetrated by the father and the father is continuing to kind of perpetrate that family violence through that kind of coercive control. (Practitioner 20)
We do have kind of a cohort where you’ve got … your persistent, very toxic partners that [are] misusing the family law courts, misusing breaches … and continue to make the woman’s life hell and well until … the youngest child is 18 … it’s also the presentation of the mum, because often they do have quite a typical post-traumatic stress disorder kind of symptoms and you can’t make head or tail of it and they come across as quite crazy or mad or enraged and resentful … and it would be really easy to, you know, kind of blame her or disregard her or disengage … when actually underneath it … you’ve got a really tricky and toxic ex-partner … that presentation will just send her to a GP for medication, or you know she’s been seeing a psychologist for 15 years, but there’s no change . … [those] symptoms and behaviours are in the context of the world that she’s living in, so you have to kind of ask around it. And, also, you have to slow things downenough and be respectful enough to hear that story to not rush into solutions and be yet another person telling them that they’re wrong … [and] paralleling an authoritarian power over response. (Practitioner 2)
DS practitioners explained that a whole-of-family approach can also offer an opportunity to obtain crucial contextual information about DFV behaviours present, with the below examples demonstrating some of the complexities and challenges involved in engaging with adults using harm or keeping an original perpetrator in view and suggesting considerations for emerging practice.
Promising practice:
Surfacing adult-perpetrated DFV
- The young person’s father and sibling (who was identified as at risk of using violence) were all on separate files (DS170, DS621, DS631). While the parents accessed support from DS to explore the young person’s aggressive behaviour and support him to change that behaviour, the father’s own use of violence – where he “rages”, breaks the young person’s property and is in conflict with the mother – also required attention. Having separate engagement with these family members enabled the father’s pervasive use of violence and the impact of this violence on the young person and their sibling to be surfaced.
Promising practice:
Needing to keep potential control in view
- In case DS021, DS was engaged with a 13-year-old’s mother, while the father (mother’s ex-partner) requested to be involved with the program separately. Intake case notes indicate that the young mother had applied for a protection order against her ex-partner in the past (not current) as a result of DFV perpetrated against her and the young person. The father’s willingness to engage with the program may have represented an opportunity for positive change within the family structure (though the research team noted that it could also be a tactic for controlling the engagement by other family members). Case notes from the file indicate that risks were discussed between the DS co-workers within the program to facilitate engagement with each parent. Case notes also refer to DS practitioners consulting with parenting practitioners to establish appropriate supports for the family.
More broadly, practitioners across the research described constantly advocating to Child Protection and other services around fathers’ behaviours and the fact that this should be the priority.
… the complexities with the families coming in … with family law court orders and [protection] orders … we do consults with them at the beginning to get an understanding, but what those support periods could look like and what the risks would be if we were providing supports. For example, if you were providing support to a young person, what that might mean for them, but also what that might mean systemically … so within the justice system, as well as within the family law system and Child Protection as well … It’s challenging because you have to think really broadly about the implications of systems abuses … by people who have perpetrated violence … holding the knowledge around what that could be as well. (Practitioner 32)
… if Mum’s still in a relationship with a perpetrator and there’s an adolescent and Mum’s afraid of stepdad – it’s often stepdad – and adolescent both, so she’s dealing with both. It really just becomes … a black-and-white kind of description. Is it stepdad or is it the child? And often children can really feel ganged up on in those situations, whereas there is a complexity where … it might more often than not actually [involve] dealing with both and that’s really, really important to empower Mum as much as possible rather than going down this really, really simplistic kind of you know “Who’s to blame?” way of doing things. (Practitioner 65)
An equally crucial part of this work includes identifying where young people have been misidentified as the predominant aggressor or inappropriate target of the system’s intervention, and advocating for a different approach.
I’m thinking of [a] family in Child Protection, there were male perpetrators within the home, but everybody was blaming this young person … and wanted … us to “fix them” … And we kept saying, “But you’ve got this adult perpetrator in the home, like, who’s holding him accountable?” So, we’re really bringing that lens and safety framework together to that care team … we actually had really good outcomes. The Child Protection worker did a bit more work on that and then ended up removing [the father] from the home. (Practitioner 27)
There’s times … where we’ve attended a joint care team meeting after reading through the referral and realising that the current [adult] family violence risk in the family home was actually what the priority was, not the young person’s use of violence. That young person had actually been moved into a residential unit and was very much being blamed for what was going on in the family, when [we] could really see that there were so many other things going on that were concerning and so we are providing, I guess, that systemic lens at times. (Practitioner 22)
I know everyone wants a quick tick-a-box answer, but actually we really need the essence of … what’s happening and the recent referral when I met Mum and Dad, it’s like, “Whoa, you know, Dad just took over the session” and … so already I’m going “Whoa, there’s a lot of control issues happening here.” So … we’re in trouble if we only tick a box and don’t get the essence because the control is always hidden underneath. (Practitioner 2)
Probably what’s been the biggest eye-opener for me … is the misidentification … around young people being the ones who are committing the violence. However, when you kind of unpack stuff … parents are so much better speakers, I guess, and can advocate for themselves. And so yeah, so we would probably see a lot of this firsthand … (Practitioner 52)
The potential for misidentification of young people – or at, the very least, a failure to identify an adult perpetrator who remains out of the system’s view – has therefore become a subject of system and practice advocacy for many of the practitioners participating in the research.
The complexity of dealing with an unidentified adult perpetrator and the practitioners’ lack of awareness of that or challenges around that, or just acknowledging the general challenges of working with adult perpetrators and how manipulative they can be, also charming or how pressuring they could be on a sole worker which can then overflow into our workspace. And I think then for the worker not actually putting two and two together and considering the safety impacts of that on the young person in this approach … (Practitioner 27)
I’ve been in court where there’s a very clear rhetoric that a present parent is a good parent. If a parent has showed up … then they couldn’t possibly be perpetrating violence against a young person and you are pushing a big rock up a big hill if you’re going to allege otherwise and it just it baffles me a bit because we all of a sudden change our thought processes around these young people and that … they have become people who use violence and there’s nothing more to be seen … It’s like this unique little element of the world where we … think parents are doing a fantastic job because they’re there and they’ve showed up. And it might not be physical violence … but recently we’ve had [from parents] withholding food … we’ve had all sorts of manipulation. (Practitioner 49)
… the way in which we tend to be raising AVITH … at the moment, it’s through some of our existing kind of campaigns or advocacy pieces, so it’s a part of our mis-ID work. It’s a part of our … work which is about kids in residential care who cross over from Child Protection to come to youth crime and … it’s an issue that’s raised there … and usually we are drawing on the same recommendations as the PIPA report. (Practitioner 65)
Crucially, practitioners also described the way in which keeping adult-perpetrated DFV in view could contribute to appropriate sequencing of interventions and collaboration as a way of ensuring that safety was prioritised and that the most immediate needs of the family were addressed.
If a parent is experiencing ongoing and current intimate partner violence, then … change within that family system approach is very, very hard … So we would usually encourage the mother … to engage [in an appropriate specialist service] and … look at trying to support her with the intimate partner violence situation first … And so you wouldn’t just drop out in that situation, we would continue to work closely with other … specialist services. And in those cases … I think that’s probably been the best kind of collaboration that we’ve had because, I mean … when risk is very high, everybody is really sort of on their game maybe a bit more and so it’s a bit more tightly managed. (Practitioner 12)
Reflective practice and emerging collaboration
Reflective practice and curiosity
Echoing the advocacy and collaboration in the example above, AVITH-focused practitioners told the research team that they were trying to encourage more reflective and critical approaches.
A lot of the other services or people around the young person are … not necessarily taking a step back … and being like “Hang on a second … let’s just think about this. What’s going on here? What’s behind that? Let’s … spend a period of time in this care team being reflective, [that] can be a really powerful way of being a point of difference.” (Practitioner 22)
We tried to take much more of an analytical view of multiservice involvement … often driving that care team process. I think that the more pressured that services feel, the more siloed they tend to work within … It’s quite helpful that we tried to often try and … drive that process in coordinating, really understanding, who’s doing it and reviewing that. (Practitioner 13)
This also went the other way, with specialist youth workers very keen for specialist DFV knowledge and a lens on adult perpetration to be included.
When specialist family violence services are there [in care teams] it can be super helpful around understanding orders, understanding the justice system, navigating legal advice, even navigating like things like trauma, support and stuff for parents, which is fabulous. (Practitioner 57)
Reflective practice and inquiry could include querying how other practitioners might speak about the young person or protective parent in care team meetings, as well as encouraging other practitioners to reflect critically on whether there was adult-perpetrated violence still occurring in the young person’s life.
Just as importantly, where practitioners do not necessarily bring a shared conceptualisation to the work, AVITH-focused practitioners explained that they would attempt to develop that shared conceptualisation as part of an ongoing conversation.
… so just the level of advocacy that needs to take place, like in any and almost all spaces, like wider care team spaces, for not just the young person that we’re working with, but also the ongoing exploration of practice from other practitioners in the sector. There’s also the amount of work in the time that it takes to sit in a care team meeting, which involves constantly kind of questioning back: “Oh can you tell me a little bit more about what you mean when you’re asking that question?” and “When you refer to the young person in this particular way, can you just talk a little bit more about what your understanding is of their experience prior to your involvement?” And so yeah, just a lot of work across the sector in those care team meetings … (Practitioner 33)
… the collaboration often is around actually having a coherent conceptualisation, we hold the direction of the work and we’re trying to get everybody on the same page and sometimes … that might be in opposition to what other services are saying or focusing on … we’re holding the case direction and conceptualisation and kind of the assessment and what then needs to happen and trying to get people to … be working together. Another key one which people don’t think about is … that the parenting [is occurring] under abnormal circumstances and so normal parenting strategies which do seem good actually work counter. So sometimes we are actually advising to do the opposite of what might be good sort of parenting. (Practitioner 2)
… there’s been some really good collaboration … with services when you can start to do that advocacy around the young person’s experiences so that – again, with consent from that young person – can be shared with other services that are engaged with the young person or the family so that their side of the story is also known to those other services as well, an independent, well-resourced family violence service that can do whole-of-family assessments on an urgent basis … in the same way that there is urgent need for [Child Protection] reports or whatever else, that there is an urgent point of escalation for these families … And the other side of that is that there’s someone independent assessing what is actually going on? But trauma-informed too … Walk the walk and talk the talk, or at least listen to the people who have tried to walk the walk and tried to talk the talk and are trying to guide you on that path … Even if you don’t knowyourself, have open ears to the people who are trying to explain it to you. (Practitioner 49)
Reflective practice and collaboration also included capacity-building in wider services by providing secondary consults. This was particularly valuable where other practitioners are working in very different practice settings or disciplinary frameworks.
[I’m thinking of one example] … we were kind of like polar opposites, like, we’re youth work sitting in family violence and she was a family violence worker sitting in a youth team … We kind of partnered up and she … sent us this really lovely email just appreciating the connection because it was … isolating for her to be sitting alone with … people not sharing the same framework. So we were trying to have a, like a bimonthly reflective practice where we could get together and just have the space to … talk about practice and talk about frameworks. (Practitioner 29)
I’ve opened conversations with Child Protection workers around [Aboriginal and Torres Strait Islander families’ experiences] because … there’s definitely been times where just a lack of understanding around those kinds of things has meant that some workers from the Department have acted in a certain way … and we’ve been able to talk to them before they’ve been able to kind of have that conversation with the family themselves. (Practitioner 73)
Practitioners participating in the research spoke about the value of opportunities for shared discussions and reflective practice within their organisations, as well as cross-organisationally.
… it’s translating into changing me as a practitioner, I know that I’m just one person and this is what I need to be able to sustain myself in the work and to sustain my drive and commitment to being so person-centred in my work. And I can’t do that if I don’t have the space to have, you know, other people reflecting all this stuff with. (Practitioner 28)
We talk so much at the moment in the sector around having an intersectional framework, but then what does that actually mean for the people that we’re working with and identifying through these labels? … What does that mean when they’re also talking about, like not being able to read and write and then, like going to specialist classes and you know having ADHD and you know then talking about the medication … But it’s like “How do we draw all of those bits together as a support team?” If you have particular practitioners that may work in similar ways, then that support team can feel very different and very like their support is driven by the young person in the family rather than the ideologies of the particular organisations or teams. (Practitioner 32)
… with all of us needing to be skilled up across the whole sector, with [risk assessment and management approaches], with understanding around mandatory reporting and information sharing … it feels like the last two years now, we’ve been really skilling up … so I think from what it used to be to what it is now, people are really good at identifying … where might be red flags or even just to be curious around some of the descriptions that young people might present with around their own family relationships so the assessments have shifted as well, like those documentations have all been amended too. You know it’s those kinds of simple ways of kind of trying to understand and then be curious further. (Practitioner 35)
This was echoed in the experiences of DS practitioners who were able to benefit from the practice lead overseeing their program.
Promising practice:
Internal collaboration
- The case files indicated collaborative work occurring within DS itself, including supervision between DS colleagues to discuss the progress of case files (e.g. DS321). In one case file (DS054), the DS practitioner’s supervisor provided secondary consultation regarding the frequency of meetings between the family and the DS practitioner, including increasing frequency following an upcoming court hearing date. A secondary consult via supervision appeared to be particularly helpful where DS was engaged with the family via multiple programs, reflective of increased complexity within the family case.
Collaboration
Across the research, practitioners were regularly collaborating with each other in support of a young person or family, although to varying extents in different contexts. This included highlighting the welcome advent of care team meetings online in the context of the COVID-19 pandemic, a practice which was continuing past lockdown periods and was saving practitioners a lot of time.
… because we’ve been going out there and kind of forming these connections, [services] … just call us and go, kind of just do a bit of a consult, “Is this a family that’s appropriate for your service?” and then we kind of have a bit of a chat … or we’re part of a bigger care team that’s already there … I’ve got one where there’s Child Protection, then [sexual assault service] are involved and there’s a whole bunch of different services for the family, as these things usually work … I can’t think of a case where I’m working just with the family. (Practitioner 10)
When asked to describe their experiences of collaboration, practitioners gave varying examples.
I can think of examples … just where I’ve worked with a young person at the school and then two weeks ago I got … an email from the school saying “I’ve got a parent talking to me about the young person using violence, how do they refer into your program?” So she wasn’t clear about the process, but she obviously recognised that’s what we do … So I’m like, oh well, “tick”, that’s good … It’s small, but it’s still, you know, you just don’t know how that ripples … (Practitioner 5)
[Across specific] services there has been quite a bit curation of “Who can see this one, this one’s an urgent one, who has any time now?” And some of that … we’ve sort of stepped in because our other systems weren’t working … We will get some families who aren’t engaging with [other services] very well, so they kind of do that referral for us as a last ditch … So then we’ve managed to actually build up a bit of a rapport with some of the families to then get them to that next step. So … that collaborative space is really vital. (Practitioner 62)
The RAMP [Risk Assessment and Management Program] coordinator called me saying there’s a real lack of somebody with adolescent violence, kind of experience. And “Can you please consult with some of the families that were there that are coming to us?” You know that kind of thing, so I think there is a bit of action going around people thinking about this in a different way. (Practitioner 9)
Practitioners in ACCOs also emphasised that often their wraparound work was about the young person’s wider needs which may or may not be contributing to use of violence at home.
This young person … was going through self-harm and suicidal thoughts and already escalated to the suicidal plan. So … it was a wraparound service that came on board to look after this young person and then we went to the steps of, you know, who would be doing what, coordinating to their roles. [We communicated] … that we had put in measures of safety plans within our family violence case manager and our adolescent youth worker … and our therapeutic family violence counsellor. We also hit the schools that were monitored and contacted around that youth to ensure they have a safety plan there and we yeah, we installed a safe to put in, you know items that may harm that young person. So, it was a lot of emails, a lot of follow-up, a lot of steps to have that safety around that young person. And on Monday she had verbally said to the counsellor that she felt safe and supported by this group. So, I think that was an excellent example of wraparoundfocus for families. (Participant 75)
Practitioners also described varying levels of success with different forms of collaboration – across organisations, as well as within them.
When you’re working across different organisations it becomes a very complex dynamic trying to sort of co-work with families when that level of handover isn’t there, they’d have different policies, different procedures, different responses, and you would think that all organisations work in the same way, but they really don’t and I’ve been in that space … where I was trying to run a joint triage across two organisations and it was very problematic. There was lots of double handling and … it didn’t work and they’ve actually brought it back to now to being held within one organisation because it’s actually quicker, more streamlined, faster, and can provide a better service to families. (Practitioner 25)
In the last few months, within our organisation, there’s been some good changes to allow for more collaboration within that sort of larger team. And … so people within the team can consult with us to if they want to, if they’re working with Family Services and they identify that there’s an issue, then they can just have a consult without necessarily doing a referral. And then even that helps build knowledge within the organisation of what [AVITH program] is, which then goes out to the broader community, and they remember you, they’ve got all your contact details and so that’s how it works. (Practitioner 5)
Examples of collaboration and communication with different services were clearly apparent across the case files. Sometimes this included informal liaison, sometimes it included care team meetings and sometimes it included decisions to withdraw from service engagement to avoid over-servicing. Data indicates that 10 families (30.3%) had formal care team meetings/consults during their engagement with DS. The number of care team meetings held for families across the case files ranged from none to as many as eight.
Promising practice:
Working with multiple services to facilitate practical support and safety
- In one example (DS098), DS extensively liaised with other services involved with the young person and their family. DS contacted the Men’s Referral Service to find housing and case management for the young person as a (young adult) male excluded from the home as a result of protection order conditions. The practitioner liaised with the social worker at the mental health unit from which the young person was discharged and organised housing support. DS also liaised with [specialist DFV service] regarding housing support for the mother and other children and liaised with the Asylum Seeker Resource Centre. DS also organised ongoing financial and food support for the mother and the family and provided assistance with getting onto Centrelink payments.
Promising practice:
Safety planning in care teams
- For the family which had eight care team meetings during engagement with DS (DS456), services/practitioners that were regularly involved included a school wellbeing officer, child and adolescent mental health services, Child Protection, DS and community primary health services. During these care team meetings, a safety plan was put in place for the family, as well as plans to support the young person’s transition into residential care and to coordinate the young person’s move from that facility to another residential care facility, while balancing the young person’s distance education.
Promising practice:
Flexible and client-led approaches – mitigating over-servicing
- In one file (DS443), case notes indicate that the DS practitioner eventually ceased working with the family because it was determined that the young person and mother were well supported by the care team. Case notes indicate that the DS practitioner undertook the following work with the family: supporting the young person and mother to navigate the criminal justice system; linking the young person into services; safety planning, risk management and liaising with workers; and family functioning support and advice. On case closure the family was engaged with a NDIS worker and a psychologist.
Examples of promising practice across the research also included collaboration with police or joint attendance at DFV police callouts by a specialist youth team, which echoed other collaborative responses by police, such as those conducted in the mental health context.
Basically, we would attend [the callout] with police, but then … we would facilitate that referral to [wider youth service], but we would also go to the house and have that conversation with the family, with the young person … Is that what they want? … explaining you know that it is voluntary, that it is going to support them. (Practitioner 54)
So, I had … the Youth Engagement police officers … reach out to me around a young person that I was working with and they wanted to have a conversation with the care team about what was the most appropriate emergency response for them to have. And we had a fantastic conversation with the police officers, different members of the care team and the parents as well. We wrote down a story for the young person around that and the way that they could understand when police got involved and the police were just fantastic. They were really creative, really open in what they could do in their response for the young person. (Practitioner 22)
We’ve got a really lovely example of where it worked really well using multiple services bringing people together for this family. This boy had been using violence for four years daily and throwing, you know, [things] off balconies, smashing windows. He was 12. And every car panel was smashed in. Urinating in front of his dad if his dad said no to something. I didn’t know what to do … and we couldn’t have done it on our own, I think. But … coming in with different services, we were lucky that … in the area that they live in, there’s a great community police officer. So we were able to focus on … getting this boy assessed and understood and helping the parents build their capacity and … [the police officer] went out and actually had a chat with the boy. He provided the external motivator in some ways of, you know, “Mate if this continues, then there’s a good chance you’re gonna end up not living with Mum and Dad” and he’s like, “Well I don’twant that” … And we continued doing the work with the parents and we assessed him and you know, ADHD, ASD, people understood his social communication approach needed to be very different and just the combination of it all for this family … Dad realised he’s got ADHD as well so he went off and got himself diagnosed and ended up medicated and less reactive, less impulsive and he was actually being physical, you know, with his son as well and using his frame to protect his daughter and his wife. But he was being aggressive with his 12-year-old as well. So, lots of shifting needed to happen [but] it’s a good news story. (Practitioner 41)
AVITH-focused practitioners were regularly creating or instigating care team meetings to get a sense of the services involved in a young person’s life and then coordinating how each role would function.
I work with young people who initially don’t have anyone, so there’s lots of care team creation – I think one of the things that I have tried initially to do when connecting is getting a really clear picture of what their parameters are, what they look like they need to do within their role and what they’ve got the capacity to do within that role and then trying to really pin down what each person’s doing … That’s the really tricky thing, young people are not siloed beings, so it’s about us sort of working out the parameters of each role. (Practitioner 55)
When I start to work with someone, I find it really helpful just to have a care team meeting [to ask what’s] your scope and what are other people doing so that 1) there’s no overlap and 2) there’s no underlap and … so we’re all aware of what’s happening specifically with that young person … It’s been really helpful to get little bits of information around risk, say the perpetrator’s family calling or passing by, like little bits that add up to be a lot more serious … And having that constant dialogue … I feel like we’re pretty lucky in that within our team … you know, we sit and we talk about risk and strength and safety and family violence constantly. (Practitioner 30)
Practitioners from a service which worked extensively with Aboriginal communities in a particular regional area pointed out the importance of maintaining a constant dialogue around the intersection of other forms of violence and structural harm, including racism and intergenerational trauma.
I think that’s where I’m finding … some of the really good work to be done and because it allows it as well – probably like buzzword – but to be intersectional because it’s not saying, this is just family violence. It’s like this is intertwined with every other form of violence and community. Every other form of racism, discrimination, like all these ideas, are all intermingled – and what these kids are hearing on the street and in school every day. (Practitioner 45)
Advocacy around the best approach to engagement was also crucial in situations of complex trauma or multiple needs across a family.
[Practitioner] had one of her cases where … she did meet with the parents, but … the young person by that point was in the residential unit. You know, we could have intervened 12 months ago, that was probably the right time, but at that point, the focus actually needed to be on the young person without the context of the family. And so, you know, doing systemic work with the care team, [identifying] the most appropriate service and why we’re recommending that service … as to why it wasn’t safe, you know, and the outcome of that, for example, was that Child Protection were able to prioritise it for an intensive therapeutic service … because that was what was required … (Practitioner 22)
The case I’m thinking of, I mean it was … horrific violence, just day-to-day, nonstop … and Dad had a disability, you know. So, everything was just long-term trauma and cultural diversity … so many issues. And yeah, and the Child Protection worker finally listens to me …. And it’s like oh that’s like a breath of fresh air, thank you, because I want to tell you not to force the young person to come in because we’re about to escalate a situation of violence. (Practitioner 1)
Collaborative work on the case files also included working with Child Protection in several cases.
Promising practice:
Working with Child Protection
- In one case (DS147), Child Protection and DS discussed concerns about the father’s ongoing behaviour towards the young person and his “unwillingness to do the work in relation to his behaviour and motivation for change”. In this case, Child Protection informed DS about other reports in relation to the young person’s behaviour and that the mother recently self-referred to the Orange Door. At the conclusion of the discussion, case notes indicate that “CP was going to do information sharing and explore a [protection order] and reconnect with DS”. In this case, evidence of DFV behaviours resulted in the young person being reallocated to a separate case as the sole client to work with DS because of risks brought up during the risk assessment.
Also crucial in terms of emerging forms of collaboration was growing awareness on the part of Victoria Police in terms of young people being linked with legal advice, as well as linking the parent or young person with other supports prior to a court hearing through specialist court practitioners or a specialist legal service (Practitioner 61). This included growing awareness in the magistracy about the availability of services, where magistrates could encourage families to speak with relevant practitioners about connecting with services (Practitioner 60).
Just as importantly, the research team heard that pre-court referrals and discussions between lawyers and police could result in more constructive court outcomes, including the withdrawal of an application for a protection order or an agreement to an undertaking so that young people were not at risk of criminal charges upon breach (Practitioner 73). As well as removing the risk of criminalisation for the young person, recent research has also discussed the way in which application for protection orders and involvement in the legal process can actually increase risk for victims and survivors of AVITH by further undermining the mother–child bond and also by placing protective parents (usually mothers) in the role of helping young people to comply with the orders and avoid breach (Campbell, 2021; Campbell et al., 2020; Centre for Innovative Justice, 2022). The research team also heard about strong relationships andworking groups across the Children’s Court, Victoria Legal Aid, Youthlaw and the RESTORE Program at the Children’s Court (Campbell et al., 2020), as well as increasing advocacy by the Children’s Court specialist practitioner in the context of other specialist networks across the wider Magistrates’ Court. These working groups could allow stakeholders to share case examples and “ventilate an issue” (Practitioner 65) in a way that ensured that practice or system barriers could be overcome. Important to note here, practitioners observed that relevant government departments needed to be more engaged with legal and court stakeholders.
Case files indicated that collaboration was also occurring between DS and services working in the context of the legal system. An emphasis here appeared to be on clear communication about roles so that families felt adequately supported but not overwhelmed by service involvement.
Promising practice:
Collaboration in the context of the criminal justice system
- A young person in one case file (DS443) was referred to DS by the Melbourne Children’s Court due to their criminal activity, as well as being the respondent to a protection order related to a matter outside the family context. Care team meeting notes indicate that the young person had been associating with a group of friends who identified as a gang. The young person’s mother reported that the young person was using drugs, becoming increasingly unpredictable and aggressive, and stealing money to pay for the drugs. The young person had also recently received threats from other students at his school who alleged that the young person owed them money. The care team included a youth specialist from Victoria Police, an outreach worker and a Youth Justice worker. The files indicate that these responses assisted the young person to access support needs; supported the young person in understanding risks, decision-making and strategies;and supported the young person to navigate court orders and legal matters.
As one practitioner working in the legal context observed:
While it feels cumbersome, there is collaboration, and there are positive outcomes … We do achieve really good outcomes on a very basic level that young people aren’t left with full court orders against them and potentially impacting their future … It’s not necessarily that it doesn’t happen, it’s just that it’s not very streamlined, would be my view and there are exceptions to that, where it’s an uphill battle, but for the most part I think we do get there. (Practitioner 49)
Improving collaboration
While practitioners regularly worked in care teams, as discussed in Part 2, they also highlighted what could be prioritised in the development of future responses.
I think there’s one thing I’d like to see in a AVITH care model … is that built into that assessment is a really genuine asking of the parents of, in some way, of “Where are you up to? What is your capacity to respond at this moment?”, because we can throw all the ideas at you in the world, but if we’re not genuinely attending to both parties saying “Where are you up to right now?” it won’t work. And have some way of kind of almost scaling, on a scale of 1 to 10, you know, “What’s tolerance for your child today?” Most parents will tell you a different scale every day and I don’t think we ask that … (Practitioner 38)
If I had, you know, a pipe dream, it would be that we think about who’s supported … You know this care team is not just around how do we sort of identify who else is tending to the young person, it’s “Who[’s] tending to Mum? Who’s tending to Grandma? What do we know about them?” (Practitioner 29)
… if Child Protection would work more collaboratively to take us more seriously … we do need some things at times and one of those is just the authority to kind of pull people together. (Practitioner 2)
When [government] sort of first … had the program as a trial program, it wasn’t clear necessarily what the role was going to be and what we were going to do. And so, you know, [we] kind of spent time sort of a little bit of trial and error and trying things out, brainstorming what it should look like … particularly for the community that we’re working with … we’re still continuing to make those connections. (Participant 73)
Considerations around information sharing and consent
Of particular consideration for practitioners in terms of how interventions could work in the future were issues around information sharing and consent.
I think there’s been some really great collaboration, mainly with the youth services that are already engaged with that young person specifically. We’re really open – again, with consent of that young person – for as much information to be shared with us prior to us engaging with them so that we can come at it with all that information already. And then we can work in a collaborative way (again with consent of the young person) to work together on their needs, which is really, really great. (Practitioner 51)
Practitioners were not suggesting that the young person’s consent was not required – rather, that the nuanced way in which practitioners may need to navigate these issues should be acknowledged in the design of the service and in guidance given to practitioners. This was to maximise opportunities for supporting different family members while also ensuring that confidential information was not inappropriately shared.
I always check with the family member if they want that particular thing shared at the [internal case study team] case discussion and I feel like that is really, really important … And to always remember that this is just information sharing, this isn’t to then shift the focus of the next session or the intervention and not to disclose exactly what has been shared in that discussion, because that can have huge impacts on the family. (Practitioner 33)
As flagged earlier in the report, the need for parental consent where a young person was under 16 could often function as a barrier to service engagement or even increase risk where a perpetrator parent was seeking to gatekeep or exercise control. This signals a particularly important consideration for AVITH-focused service design and highlights the importance of nuance in the practice, as well as future policy considerations around considering ways for children and young people to access relevant supports without parental permission, such as having a safe and trusted adult professional who the young person nominates to provide consent on the young person’s behalf.
Recognition of AVITH work as specialisation
Recognition of the weight and severity of work in relation to young people’s use of AVITH and the context in which this was occurring was a theme which emerged spontaneously from the focus groups.
I think that [this organisation] they have amazing supervision and they have really amazing reflective practice … and just that space to have ongoing learning to be aware of what’s happening outside of the organisation and be updated … Your window of tolerance is definitely bigger when you feel safe and supported by your team and … that can increase your capacity to stay regulated … so that we can go into thinking about these cases flexibly and creatively. Whereas I think if people aren’t afforded that safety and the support, they’re responding to things in a really heightened state and you can’t think flexibly in those states and that’s where you get, you know, the blame, the shame, the judgement, the fear and the anxiety. (Practitioner 28)
We try to make sure they’re supported in supervision and clinical supervision because some of the stuff is really pretty hairy and it’s pretty scary. (Participant 72)
As an [AVITH worker], you have to be pretty confident that you’re bringing something that they don’t have … I feel pretty confident in articulating that … and I think that’s probably because of where I worked. I wonder if I didn’t have that experience at [specialist sexual assault and family violence intake] and if I purely came from Child Protection into [this program], whether or not I would still be working the way that I am. (Practitioner 20)
Multiple practitioners spoke of the need for recognition of their work as a specialisation – something which involved the development and provision of training for existing practitioners, as well as investment in the development and embedding of an associated workforce. Here practitioners recognised that the CFECFW was in the process of developing training, although at the time of writing in 2022 it was still not certain when this training would be released or delivered.
We need more staff, we need more specialist practitioners in this space. Because of holding such complexity and risk and the amount of work it can potentially be with a family … that’s a barrier for us to being able to like take on more and more clients. (Practitioner 31)
What we’re doing takes skilled and dedicated practitioners and they’re so hard to get when you keep stuffing people around … because they wanna work in a long-term and secure environment and so, you know, we are just constantly putting families on the back foot all the time and saying they’re not important by doing that. (Practitioner 22)
Working with young people who use [AVITH] is a very specialised space with a mix of family violence, knowledge and youth knowledge predominantly and in the group delivery space, a bit of education skill wouldn’t go astray either. But there’s not many people that hold all of those things that come to the space and want to come to your program for 12 months or whatever that looks like. When we go to look for training to be able to support our practitioners to be able to deliver this program or work in a youth family violence space, there actually isn’t any. There was one person that used to deliver it … and that was a few years ago now. So, instead we are looking at, “Here’s some youth training”, “Here’s some family violence training” and “Let’s kind of just mash that together” … So, some absolutely focused training … would be amazing. (Practitioner 62)
The research team also heard that a specialist workforce was not going to be properly utilised without wider services being able to identify AVITH and refer young people and families into specialist support. This included in the context of Victoria’s family violence intake points via the Orange Door network, where a number of practitioners volunteered that a specialist AVITH role was required. This was distinct from existing child and young person–focused roles, as discussed in Part 2.
I also think it has to be … greater training or greater information at that base intake level, so those points of intake, those points of entry, more information for those workers to actually be able to know, through the assessment, identify the actual needs and then share that funnelling it through ’cause that seems to be those, those moments of loss … It has to be about what questions are getting asked or what training or capability those workers have to be able to see these programs for what they need to be … (Practitioner 6)
We just keep getting like all of these announcements for the new appointments to the [region] Orange Door and there were all these practice lead roles and it just occurred to me, why isn’t there one for young people? Like why isn’t the intersection of being a young person [and using violence] counted as, you know, a specific vulnerability – not because young people are vulnerable but because the system makes young people vulnerable. (Practitioner 29)
In addition to specialist AVITH-focused training, practitioners also spoke about the value of training which enabled workforces to understand the impact of adult-perpetrated DFV on children and young people, such as the Safe & Together Model, as well as training such as “Tracking Better”, which focused on emotional and behavioural regulation. Practitioners also identified a need for practice guidance, which they acknowledged would be produced by the Victorian Government in the future in relation to risk assessment and management.
I think having something that would ensure that we actually collaborate and that there’s some clear guidelines … I mean, we’ve got our own individual plans and our own individual program guidelines and what’s expected … We’ve got that as a service, but … I don’t think as a service system that we have that. (Practitioner 29)
I’m looking forward to the AVITH [multi-agency risk assessment and management tool] and all that sort of work that’s building on our capacity to deliver strongly in that space. So I think there’s still a long way to go [but] … there’s been some really good steps. (Practitioner 19)
A regular theme to emerge spontaneously from the focus groups was the need to “slow down” the risk assessment and management response and examine what was occurring across the family system.
… being more proactive in that space so, you know, police and ambulance are actually coming out to meet the young person when they are regulated and do some of that planning with them, I think is really key … It’s about slowing down thinking “What information do we have that can help educate the people who will be carers every night, every day, to understand how this young person functions?” and … really in terms of that wraparound and trauma-informed care – that’s the bit that we need to slow down on and work together across those systems. (Practitioner 38)
Imagine in an ideal world where we could engage with young people either experiencing or using family violence in this kind of slow, measured, safer way … The fact that a police officer at sergeant level can make that decision, they may have no experience in dealing with young people. And that there’s a more rigorous inspection of ex parte interim applications against children because it’s made ex parte against a child and then you are in the fight of your life to get a court to consider other issues around that. (Practitioner 49)
A further theme to emerge was the need for continued opportunities to share practice and learn from each other as their practice evolved.
Having more opportunities to kind of come together like, you know, to conference or things like that, where professionals can kind of network with each other and share those ideas and things more would be great. (Practitioner 73)
There’s a number of networks that we’ve got management engaged in/coordinated in. We meet weekly for allocations, so there’s a whole process around the agencies coming together. Reading through all the referrals that are sitting for the different agencies and, you know, an agreement around who’s going [to] pick them up. How do we disseminate those referrals? Who’s got capacity? Who hasn’t? Who’s the best service? So there is a lot of work that’s done at that overarching level, but, you know, there’s always room for improvement. (Practitioner 19)
Wider system support and imperatives
A number of gains and opportunities for further systemic improvement were volunteered by practitioners across the focus groups. A theme that emerged from the focus groups, for example, was the valuable assistance – as well as sometimes the lost opportunities – that collaboration with schools presented.
Many practitioners spoke about the difference that committed staff, whether classroom teachers or wellbeing coordinators, could make if they were aware of an AVITH-focused program or were otherwise capable of identifying AVITH and understanding its complexities.
I have seen schools and teachers who have just worked absolutely tirelessly and have for so long not had access to appropriate services to respond to a lot of these issues, schools that just go absolutely above and beyond. I think given the current lockdown and you know the [previous] five lockdowns before this, just when young people are not going to school, how much the situation does escalate, so it really highlights how important the role of schools are and the role of teachers having their eyes on families and thinking about how, moving forward, we can capitalise on those relationships … in recognition that, you know, a lot of therapy doesn’t happen in the room. It can happen in those spaces as well … I think that’s such an important opportunity. (Practitioner 44)
Another theme included recognition of the value of Victoria’s Family Violence Information Sharing Scheme (FVISS). Practitioners noted concerns that young people’s information may be shared without their consent where they are identified by the system as “perpetrators”, a label which may not be accurate in the context of misidentification and which also carries significant implications for their subsequent access to services. That said, practitioners across the focus groups more frequently nominated the creative and collaborative ways in which they had been able to use the FVISS to complete comprehensive risk assessments, including about the risk that young people may face from an adult in their lives, contributing to more effective safety planning.
I think that the information-sharing scheme has been really good in terms of completing risk assessments. I recently had a phone call with a young person who is being supported by one of the other Orange Doors and wanting further support. So I explained that we needed a risk assessment and she mentioned that she had already completed one, so we applied for a copy of that. So at least she doesn’t have to go through all of those questions again and then we could just fill in whatever she feels like adding and just reducing that retelling … So that has been really, really helpful. (Practitioner 28)
I think that’s where you utilise the care teams and the frequency of that information sharing … because sometimes people need a gentle reminder that they care and … I have found a few of my referrals have actually come over from the women’s team once … the adult family violence has been – for want of a better word – safety planned (and is no longer occurring) and then jumping over to us to work with their adolescent family violence. So I do think there is an increased understanding and the information sharing is actually occurring pretty well. (Practitioner 20)
Despite the value of the FVISS, however, practitioners spoke about the potential value of receiving wider system-focused information. This included providing information to courts about the support services that existed; leveraging other systems to provide police and other agencies with relevant information; and collecting and sharing aggregate data about the scale of the challenge. They pointed to the value of resourcing a centralised database of available services for families experiencing DFV.
Something that I see is missing … is sort of a centralised tool, so to speak, of what’s out there. So, if someone comes to court and you know and they’re linked in with [the specialist practitioner] and she says, “Okay, you live in [an area of Melbourne]”, to be able to jump on that and say, “Okay, well, in [this area of Melbourne] there’s x, y, z”, you know … “You appear to fit the criteria and I can try and link you in today while you’re with me” … Without that, you’re sort of fumbling in the dark. It’s a bit like, there’s stuff there, but no one’s turned the light on. (Practitioner 61)
… to have an officer who searches LEAP [Law Enforcement Assistance Program] and looks at the amount of times that the young person has experienced family violence in the home before they then go ahead and apply for a [protection order]. I know that they have access to that information, but they don’t necessarily go ahead and use it and so then, as a practitioner, you’re having to get signed authority from that young person to request … copies of all previous [protection] orders … because we don’t have access to all that information-sharing capacity. (Practitioner 51)
Practitioners spoke about the variability of the information they received about a young person or family, often influenced by their prior service involvement.
You get sort of like a cut and paste in Child Protection history which comes straight out of the Child Protection files … I think it really depends on the information that is kind of held on the Orange Door database when the referral comes in. (Practitioner 12)
[A concern is] that lack of data around what is actually happening to the kids … So, you know, where are the referrals being sent, where do they go at the end of the incident? Like do we have any idea of what the stats are in terms of who’s actually ending up with family or in some kind of crisis housing, and then … what is the percentage of incidents where there’s a repeat call out to the house? We don’t actually have all that information necessarily collected systematically across the state … we’re just still putting together the pieces of the puzzle. (Practitioner 35)
Given the complexity that is so apparent in their practice, practitioners spoke about the need for greater resourcing and thought being put into program design to support different aspects of the work, including design which draws on expertise from practitioners and people with lived experience.
Having people to help us with intake will then relieve us of things that we could be doing to kind of connect with community … And then there needs to be another level where we’re doing, whether there’s enough space, enough funding, and enough resources to be able to actually go out and do that sector development stuff, and also to be able to do some community development around this area too. So sector development, community development, and then also on the ground working with families … (Practitioner 5)
At the systems level, co-design of these programs with the frontline and also perhaps with families themselves, we’ve got peer workers in our team who are victim[s and] survivors of family violence and their input is just so valuable … (Practitioner 27)
Practitioners also spoke about opportunities to consider how supports that are currently available to victims and survivors of adult DFV could be made available to people experiencing AVITH as well.
What is safety planning with [AVITH] versus intimate partner violence? How is that different? And yeah, what options and resources are there and even things like, you know, flexible support packages, stuff like that – they’re not set up for [AVITH], they have specific criteria around, for instance, that the victim [and] survivor needs to leave or be planning to leave the relationship and … that’s not appropriate for the majority of those cases. (Practitioner 9)
Just as importantly – and echoing the findings of the PIPA project, which suggested that interventions in AVITH were coming “ten years too late” (Campbell et al., 2020) – practitioners spoke about the need for them to be brought into the picture earlier, a challenge when additional layers of intake and referral had been incorporated into the Victorian response.
We see so much work that you know, had we been involved a year earlier, we could have been able to do such beautiful work. So, we really would love to do a bit more work in the prevention space. (Practitioner 27)
Once a parent has decided to call the police, that’s at the pointy end already and we’re five L17s [police referrals] down the track. We need to be there now. (Practitioner 5)
Overall, practitioners who had developed a “specialisation within a specialisation” – whether over a long period of time or more recently – saw a need for ongoing practice development, research and interrogation.
The whole of Australia is only beginning to develop stuff for adolescent family violence … I mean PIPA is not that old. (Practitioner 65)
It’s so exciting to be doing this work but, at times … you look at the literature and there’s just really, really not much there, so kind of just getting those beacons and direction from researchers is really valuable – so, thanks. (Practitioner 24)
Part 4:
Towards a collaborative practice framework
As described in the Introduction and Methods sections, the Collaborative Practice Framework was developed through iterative engagement with practitioners who participated in the focus groups during July to September 2021. Findings from the focus groups were analysed and presented, together with a draft proposed Framework, to practitioners in a series of workshops in February 2022. Feedback from workshop participants was then incorporated and a further draft of the Framework tested and refined with practitioners in June 2022.
Aims of the Framework
Practitioners across the research indicated a need for a clearly articulated framework to underpin collaborative practice and emphasised the need for any response to be based on shared understanding of AVITH; the factors which often underpin families’ experiences of violence and harm; and what a genuinely collaborative service response involves. Practitioners also highlighted the need for any framework to be broad and inclusive, recognising that meaningful responses to AVITH can require the involvement of system actors outside of what we traditionally conceptualise as the “service system”.
Practitioners therefore described the key aims of any framework as follows:
- Supporting shared knowledge and consistency of practice: Despite considerable progress, the system’s capacity to deliver effective responses to AVITH continues to be stymied by service confusion regarding the behaviours that constitute AVITH, as well as the considerations central to any AVITH intervention. Practitioners identified that a key function of a collaborative practice framework is to underpin shared understanding among practitioners and across systems, as a necessary precondition for achieving practice consistency. Crucially, this includes enabling practitioners to maintain a shared focus on issues for the family and providing the scaffolding for understanding and responding to the function of young people’s behaviours, rather than the behaviours themselves.
- Improving recognition at the organisational and system levels: Poor understanding of AVITH across the system often means that AVITH services are insufficiently resourced and scoped in ways which fail to account for the complex considerations required in any meaningful service response. Practitioners described the benefits of a tool which articulates the complexity of working with families experiencing AVITH, as well as the benefits of ensuring that this work is properly recognised and supported, both within organisations and at a system-level. This includes recognising AVITH as an emerging specialisation, with program resourcing to include consideration of professional and practice development; supervision and reflective practice; and capacity to participate in relevant forums, networks and governance structures at the local and system levels.
- Ensuring role clarity across the system: Practitioners described one of the benefits of a framework as improving coordination with those services and agencies that may be harder to draw into a collaborative system response, including police, Child Protection, schools and the legal system. This requires supporting different parts of the system to understand the scope of their role in responding to AVITH, whether that involves referring to a specialist program or working alongside those programs to meet the needs of families. For practitioners working within more traditional service settings, the Framework was seen as having the potential to deepen practitioners’ existing understanding of the scope and expectations of their role, as well as to recognise where it might be necessary to draw on practitioners with different skills and specialisations.
- Bridging knowledge gaps between systems and sectors: Where services and agencies within the wider system are drawn into AVITH service responses, practitioners described the ways in which a clear framework for collaborative practice can build understanding across different sectors of key considerations when responding to AVITH. Improved understanding of the factors which can underpin AVITH, particularly the prevalence of trauma experiences for young people using violence in the home, can, for example, contribute to more informed decision-making where a young person comes to the attention of the legal system due to being identified as using violence. Informed decision-making can include linking a young person or family with appropriate services and supports which can address the functions of a young person’s behaviour, rather than delivering a punitive response which is likely to compound harm and systemdistrust.
Figure 1: High-level overview of Collaborative Practice Framework: Multidisciplinary and multi-system
Source: Centre for Innovative Justice.
Text alternative to the figure above
Understanding
- Understanding
- Workforce
- Coordination
- Evidence
Principles
- Trauma and family violence risk-informed
- Whole-of-family
- Addressing barriers to engagement
- Flexible and needs-based
- Intersectional and culturally safe
- Service accountability
Enables
- Funding
- Evidence-Informed Tools & Guidance
- Culture
- Service Capacity
- Continuous Learning
- System Stewardship
illars of collaborative practice
The proposed Collaborative Practice Framework is based on the four core pillars of understanding, workforce, coordination and evidence. As well as constituting individual components of an effective, system-wide AVITH response, practitioners emphasised the mutually constitutive nature of the pillars, with each continually informing and reinforcing the others.
Understanding
This pillar involves development of a shared understanding – across specialist practitioners as well as the wider service sector – of AVITH. This includes conceptualisation of AVITH as distinct from adult-perpetrated DFV, and in ways which account for trauma (including, most prevalently, from adult-perpetrated DFV), developmental stage and the function of used behaviours in AVITH presentations. Shared understanding can help to challenge and unpack binary paradigms. Understanding also involves establishing a shared language – across the multiple services and agencies involved in responding to AVITH – of key terms and practice approaches, such as “collaboration”, “whole-of-family”, “family violence/DFV risk” and “family safety”. Finally, understanding relates to the need to establish a clear understanding of roles and responsibilities at the system-level and individual practice level. This improved role clarity can, in turn, improve practitionerconfidence and reduce the sense of simply “holding risk” rather than responding meaningfully to address it.\
Understanding in practice:
Role of practitioners
- Adopt language which emphasises a young person’s and/or family’s strengths and which reduces shame and stigma. Be mindful in how the service is presented to young people and protective parents to avoid stigma, as well as to non-protective parents where consent may be withheld as a further means of control.
- When working alongside non-specialist services, use interactions (such as care team meetings) to build capacity and understanding, including by sharing information which can aid wider services in maintaining visibility of the family context and challenging views and approaches which do not adequately distinguish AVITH from adult-perpetrated DFV.
- Centre the young person’s achievements; a caregiver parent’s strengths and resilience; and the need to bring any adult perpetrator into view. Advocate for the intervention of certain services and recognition that imperatives that operate in some contexts – such as the imposition of parental boundaries – may be counterproductive or harmful in the context of AVITH.
Understanding in practice:
Role of organisations
- Design and scope AVITH-focused programs appropriately and in ways which allow for highly flexible and responsive ways of working, including working across the family unit; working intensively where required; working on an outreach basis (supported through provision of vehicles); and working with young people and families over the longer term. Design referral forms to assist adequate capture of whole-of-family information.
- Recognise specialisation and complexity of the work through appropriate caseloads, opportunities for community and sector engagement – such as sharing of evidence across different disciplines – and collaborative practice, as well as through the provision of clinical supervision and ongoing professional development.
- In naming programs, consider the impacts of language on young people’s and families’ willingness to engage, as well as the risk of stigmatising young people or non-protective parents withholding consent.
Understanding in practice:
Role of government
- Resource AVITH-focused interventions in ways which reflect the complexity and specialisation of the work and the need to work flexibly, on an outreach basis, over the long term and in client-led ways, factoring in appropriate caseloads and capacity for practitioner development. Brokerage will remain key, as will consideration around an equivalent to flexible support packages, albeit with appropriate eligibility criteria. Resourcing for dedicated AVITH respite options requires urgent attention.
- Support shared understanding and conceptualisations through development of sector guidance not only for risk assessment and management but for service delivery, as well as ongoing training and regular opportunities for sharing practice and evidence.
- Embed shared understanding across government and systems, including health and legal systems as well as community service sectors. Identify and advocate in areas where the operation of one system – such as the legal response – may be working against effective responses to AVITH. Develop and build on existing resources in other sectors – such as the “White Book” in primary health settings – to emphasise the need for all professionals supporting young people to keep the potential for an adult perpetrator and ongoing systems abuse in view.
Workforce
This pillar highlights the importance of a skilled and well-supported workforce to respond to families experiencing AVITH. This includes a recognition across the system that – due to the breadth of presenting needs of families experiencing AVITH – an “AVITH workforce” must comprise a specialist workforce capable of delivering targeted interventions and case management, as well as baseline capability across the wider service system to identify AVITH, refer appropriately, and work alongside specialist practitioners to support families and young people as required.
In thinking about a specialist workforce, practitioners participating in workshops consistently emphasised the breadth and complexity of work and the need for “specialisation within specialisation”. For example, practitioners described the significant differences in approach required to respond to children and young people in ways that are developmentally appropriate, as well as the layers of specialisation and capacity required to work with young people and families where specific needs such as complex disability, mental ill health, grief, intergenerational trauma or migration trauma featured. Given widely acknowledged workforce challenges in the specialist and wider community service sectors, this points to the need for governments at state and federal levels to invest in long-term workforce development strategies which can provide the foundation on which this highly specialised workforce can be built. This includes identifying relevant training andqualifications pathways, as well as fixing more appropriate remuneration levels and ongoing professional development opportunities.
Beyond working directly with young people, the research identified multiple examples of practitioners working with a protective parent (either as the primary client, or alongside direct work with the young person) in relation to their own recovery, as well as supporting their understanding of the impacts of their trauma experiences on parenting. The research also identified examples of highly sensitive work where adult perpetration of DFV continues to occur, including being attuned to the risk of systems abuse and ensuring that any engagement with an adult perpetrator is non-collusive.
Given the breadth and complexity of this work, practitioners emphasised the need for the specialist AVITH workforce to be empowered to work flexibly, including in relation to the nature, intensity and duration of support, all of which should be informed by family readiness and level of need. Program resourcing should also incorporate ample time for reflective practice and practice development.
Workforce in practice:
Role of practitioners
- Centre individual client needs and service readiness, identifying where secondary consultation with other services is sufficient or appropriate and where an AVITH specialist needs to take the lead in client engagement.
- Participate in collaborative practice networks and available training, advocating to employer organisations for appropriate clinical supervision and support. Draw on available practice guidance, service manuals and risk assessment and management tools. Ensure that referral forms and information about the service reflect family complexity and need.
- Identify opportunities for early intervention and shared positive experiences to stem the escalation of risk and need for crisis responses.
Workforce in practice:
Role of organisations
- Scope and resource AVITH programs to enable flexible and family-led ways of working, affording practitioners autonomy regarding the nature, intensity and duration of support delivered to young people and families. This includes resourcing outreach as a core function of practice and allocating caseloads that can mitigate vicarious trauma for staff.
- Ensure that AVITH-specific programs are well integrated with wider service offerings, with a view to facilitating secondary consultations and referrals, joint servicing of families (where appropriate), and opportunities for mutual capacity-building across programs.
- Put in place appropriate supervision and professional development arrangements which reflect the complexity and breadth of work being undertaken by specialist AVITH practitioners, including the need for AVITH practitioners to respond to multiple and often intersecting needs (both at the individual level and collectively across the family).
Workforce in practice:
Role of government
- When funding AVITH programs, ensure that resourcing includes consideration of non-client-facing work, including time for reflective practice and debriefing; coordination and engagement with other services working around the family; clinical supervision; and participation in key forums and practice networks. Resource programs over the longer term – with five years as the standard – to enable a sufficient and specialist workforce to be recruited, developed and retained.
- Identify the need for specialist roles across key components of the system – such as, for example, establishing dedicated AVITH Practice Leads across the Orange Door network in the Victorian context. Resource and recognise AVITH-focused roles as senior and highly specialised roles that provide a leadership function across the sector.
- Establish clear requirements relating to baseline capacity to identify and respond to AVITH across the wider family violence/DFV sector and related sectors, such as through the development of an AVITH-focused workforce development framework.
Coordination
This refers to the need for a network of services which can work in a coordinated way to respond to a family’s breadth of needs. Importantly, it positions “coordination” as a building block of “collaboration”, requiring clear structures, processes and mechanisms. Practitioners cautioned against an output-based understanding of coordination – such as the occurrence of a care team meeting – and emphasised the need to focus on the effectiveness and appropriateness of such mechanisms. This included by working towards models of care in which practice leads could support individual practitioners working with particular family members to hold the risk across the whole family in view.
Effective coordination requires (but is not limited to) ensuring that a care team meeting involves the right services, agencies and practitioners; that the role and expertise of each practitioner is well understood across the care team; and that there is a shared understanding across the care team of what success looks like (both individually and collectively) for the family unit. This includes a shared understanding of family readiness, with practitioners working together to sequence interventions appropriately and in a way that can maximise the benefits of engagement.
Coordination needs to be led by an appropriate service, with that service identified based on the family’s needs and existing service relationships, rather than adopting a one-size-fits-all approach to the structure and leadership of care team meetings or a similar mechanism. This may include consideration of which services have capacity to remain engaged over the longer term and undertaking a robust coordination risk management function, streamlining services interactions and reducing service overwhelm.
Where certain practitioners are not able to participate in care team meetings due to the nature of their roles (for example, legal practitioners and/or private practitioners who engage with family members on a sessional basis), strategies to support appropriate coordination and information sharing with these wider supports around the family should be adopted to ensure that all services working around a family have an adequate lens on risk and what is occurring for the family.
Coordination in practice:
Role of practitioners
- Support and empower families to co-chair care team meetings or other collaborative service forums with a trusted service, ensuring that the process is genuinely family-led and provides the family with an opportunity to articulate their goals; holds services accountable; and ensures that planning reflects family readiness.
- In establishing a care team or other collaborative mechanism around a family, identify the most appropriate service or agency to lead coordination, with consideration to be given to factors such as whether services have capacity to stay involved with the family over the longer term and what existing relationships of trust exist around the family. Invite additional agencies that may bring a missing lens.
- Work towards a “practice lead” approach in which a senior practitioner with a lens on the risk across the whole family can support and coordinate the work of individual practitioners, an approach which is distinct from individual clinical supervision.
- Where assuming the coordination role, follow up regularly with services about the tasks that they were set; facilitate information sharing where appropriate; and provide a liaison point for the family and/or young person. Lead by example, adopting a strengths-based approach in meetings where a family’s and/or young person’s achievements can be recognised, regardless of nature or scale, and where a young person’s wellbeing, as well as their behaviour, is the focus of collaborative effort. Share information, where appropriate, with other agencies, such as legal practitioners or private practitioners, who may not have care team participation as part of their practice remit.
Coordination in practice:
Role of organisations
- Ensure that program scope and resourcing accounts for work beyond direct therapeutic or case work interventions, including participation in care team meetings and other collaborative service forums. This includes, where relevant, resourcing programs to adopt a leadership and coordination role within care teams and other forums where appropriate.
- Actively build awareness of AVITH-specific programs across the organisation to facilitate appropriate referrals, secondary consultations, co-case management and other coordinated ways of working.
- Support opportunities to foster relationships with external organisations and agencies that can contribute to effective collaboration and information sharing, including at a management and leadership level.
Coordination in practice:
Role of government
- Resource AVITH-focused interventions in ways which acknowledge participation in collaborative mechanisms, including coordination activities such as information sharing, follow-up and liaison with clients.
- Develop guidance across the community sector workforce to articulate the obligations of practitioners working in collaborative forums and the opportunities for reducing risk that these provide. This may also include formal identification of opportunities for AVITH-focused roles to participate in other coordinated risk management mechanisms, such as Risk Assessment and Management Panels in the Victorian context.
- Resource associated collaborative mechanisms, such as Complex Care Teams in the Child Protection context, in ways that allow for service follow-through and leveraging of legislative imperatives.
Evidence
This pillar is concerned with the evolving nature of service system understanding of AVITH (and related service responses) and the need for this to be underpinned and informed by emerging evidence. This includes evidence relating to the needs, risk and experiences of young people and families, as well as emerging evidence of “what works” when responding to AVITH.
The research emphasised the need for practice roles to be resourced and supported to incorporate evidence and learning into daily practice. This includes through formal and informal opportunities for debriefing and reflective practice, as well as capacity to participate in collaborative practice networks so that learnings can be shared across sectoral and organisational boundaries.
Organisations similarly need to ensure that emerging AVITH responses are underpinned by effective processes for monitoring, evaluation and learning. This includes consideration of processes through which the voices of young people and families can inform service design, planning and continuous improvement. It also requires an agile approach to program design, implementation and delivery, with emerging evidence able to be progressively incorporated to strengthen program delivery over time.
This pillar also highlights the role of government in leading a system-wide approach to building and sharing evidence, piloting responses and taking effective interventions to scale. This includes resourcing for AVITH services to operate over a longer period of time (with five years as the standard); and investing in evaluations which can incorporate continuous learning and adopt an outcomes-focused (rather than output-focused) approach to evaluating effectiveness. Importantly, this pillar focuses on fostering continuous, critical interrogation, rather than simply the expansion of existing programs.
Evidence in practice:
Role of practitioners
- Engaging with evidence in the context of AVITH practice requires focus on evidence about the needs of young people and families, including the impacts of past or ongoing adult-perpetrated DFV and other forms of trauma (including intergenerational or migration trauma); evidence concerning child and adolescent brain development; evidence concerning disability and mental health; evidence concerning bullying and school disengagement; evidence around experiences of LGBTQA+ and intersex young people; evidence around non-collusive practice with adult perpetrators; and evidence about “what works” when supporting and connecting with young people, such as outreach and strengths-based activities.
- Participation in formal and informal opportunities for reflective practice is crucial, as is participation in clinical supervision and training, as well as wider community-of-practice forums.
- Opportunities for co-location with, or secondment to, other teams across an organisation may provide further learning and engagement with evidence in other areas or disciplines.
Evidence in practice:
Role of organisations
- Evidence-based service design and practice includes the provision of appropriate training and information across the multiple areas of practice relevant to AVITH responses, as noted above, and acknowledgement that reflective practice and clinical supervision are core to the work.
- Across organisations, including local or regional DFV networks, organisations can contribute to evidence development by sharing knowledge across different agencies and disciplines.
- Service evaluation, participation in research and provision of opportunities for client voices to inform service design are crucial to organisational roles in building and maintaining evidence. This may incorporate clear client feedback mechanisms, participation in research and/or the co-design of interventions with people with lived experience.
Evidence in practice:
Role of government
- Continuous improvement and critical interrogation of practice is key not only to ensure evidence-informed responses but to guard against “program drift”. Investment in an evidence base includes resourcing interventions over several years – with five years as the proposed standard – so that practice can be bedded down and comprehensive evaluation undertaken, including with a focus on outcomes and follow-up over time.
- Continuing to build the evidence base involves resourcing independent research and evaluation, while also acknowledging that participating in or facilitating these activities impacts service delivery/practitioner time. This should be recognised in program funding and associated caseloads, either through default inclusion in program funding or through allocated backfill resourcing for service participation when research or evaluations are commissioned.
- Government also plays a role in promoting and sharing evidence across the system and with other senior stakeholders. Senior departmental leaders working in areas focused on AVITH and DFV should seek opportunities to share evidence and exchange learnings with senior stakeholders in health, justice and other relevant settings.
Principles of collaborative practice
Alongside the four core pillars of collaborative practice, the research identified a set of principles which necessarily underpin all AVITH work, including collaborative responses, and which further emphasise the significant complexity and nuance of AVITH-focused work. Crucially, a principles-based approach to responding to AVITH can accommodate genuinely flexible and family-led work, as compared with more prescriptive approaches to defining AVITH responses, which may exclude some young people and families or fail to account for their breadth of needs.
Trauma and family violence risk–informed
This principle aims to ensure that practitioners and services working with young people and families experiencing AVITH adopt a holistic view of risk and use of violence. This involves maintaining a lens on the impacts of prior and current adult-perpetrated DFV on the young person, as well as wider family members in the home, including caregivers and siblings. This principle aims to flag to practitioners the need to consider the extent to which current and ongoing violence may be influencing behaviours and support needs in the home, as well as impacting the way in which young people present to the service system.
Crucially, this principle does not exclusively refer to trauma in a DFV context, but includes other forms of trauma, such as migration trauma, intergenerational trauma experienced by Aboriginal and Torres Strait Islander people, and trauma experienced at the hands of the system itself. Trauma of systems may include harm perpetrated by a legacy of colonisation, punitive government policies, and the intervention of statutory agencies such as Child Protection in the lives of people already experiencing multiple layers of disadvantage. In a different context, trauma of systems may result from negative service interactions, including histories of over-serviced and under-serviced families.
Principle in practice:
- Lead a practice shift away from blaming or deficit-based discourse towards a framework of understanding each young person and family as presenting with their own story and own unique set of experiences and challenges. Consider the starting point of “What has happened to you?” rather than “What is wrong with you?” Highlight factors of strengths and resilience to support recovery.
- Provide time and opportunity for caregivers who may be impacted by trauma to relate their experiences and validate their efforts to protect their children and support their family unit. Recognise that they may have reduced tolerance for their young people at different times.
- Maintain a lens on all relationships of violence in the home or in a young person’s wider life, including demonstrating commitment to keeping adult perpetrators in view. Failure to do so may exacerbate shame and confusion for young people where they are being held accountable for behaviours that have been used against them. Maintaining a lens on systems abuse also includes recognising potential levers of control attempting to be used by an adult perpetrator, including where they may withhold consent for a young person to engage with a service or undermine service engagement in other ways, or where an adult perpetrator may seek to dominate service engagement or leverage it for information. Consider how requests for consent are framed and avoid opportunities for collusion.
- Recognise that young people are at a development stage of identity formation which involves testing and negotiating how they interact with the world. Recognise that caregivers who have experienced adult-perpetrated DFV may present as traumatised, erratic, unable to regulate emotions, or unable to manage a young person’s behaviour constructively because of the ongoing impacts of trauma. Provide time and opportunity for their experiences to be heard and for them to be “seen as a person”.
Whole-of-family
This principle refers to a requirement for practitioners and services to consider needs and histories across the entire family structure when assessing and managing risk. Importantly, this principle does not refer to family therapy or interventions that require all members of the family to be present in the same room but, rather, refers to practitioners maintaining consideration of issues and needs as they exist across all members of the family, including grandparents, non-traditional caregivers and siblings. This is particularly important where there is systems abuse occurring in the young person’s life or multidirectional harm occurring within the home, but where the young person has been identified (or misidentified) by the system as the person using harm.
Across the framework development workshops, practitioners described the whole-of-family principle as speaking to the key role that relational work plays in any AVITH intervention. Relational work is particularly crucial when working with adolescents, who are in the process of identity formation, self-actualisation and, more broadly, navigating how they choose to function in relation to their wider world. Relational work is seen as crucial in supporting the young person’s recovery, including their recovery from negative experiences of the system itself.
Principle in practice
- Where it is safe (and the family is ready) to do so, working with multiple members of the family may include, for example, working with the young person in the context of their use of harm; working with a caregiver in relation to experiences of adult-perpetrated DFV, which may be impacting parenting skills and capabilities; and working with a sibling in relation to disability or mental health. Practical supports which can improve overall safety and family functioning should be remembered as a crucial component. Genograms (being a graphic representation of a family tree which includes detail about relationships and dynamics) can help to support understanding and identify what is important to young people, including pets and individual interests.
- Widening the service lens to incorporate each member of the family may result in an adult using violence, such as a father or stepfather, being brought into view. Using a whole-of-family lens may allow a practitioner to understand the function of the young person’s behaviour as motivated by fear, anxiety or confusion. Maintaining a lens on systems abuse or the way in which coercive control is still a presence across the family – whether or not in the home – can help to identify creative ways of helping a young person to engage with supports. Widening the service lens also includes consideration of broader experiences of family members, such as grief, loss, discrimination or intergenerational trauma, and how this may impact engagement or capacity to support a young person.
- Adopting a whole-of-family approach may involve only working with one or two members of a family while maintaining visibility of the ways in which the family’s experiences impact on those individuals. Considering family readiness is crucial, including maintaining opportunities for family members to exercise autonomy in how interventions are sequenced so as to maximise benefit from any service contact.
Addressing barriers to engagement
Particular challenges to engagement may exist for practitioners working with young people and families experiencing AVITH. These may stem from a family’s history of being significantly under-serviced or, conversely, over-serviced and immersed in service interaction, but without any constructive effect. Other barriers to engagement highlighted throughout the research include young people’s mistrust in a system that has not addressed their own experiences of harm, or which has compounded it through perceived breaches of confidentiality; which blame or minimise; or which inadvertently collude with an adult perpetrator. Further barriers include those at a systems and structural level, including the ongoing impacts of colonisation and various forms of discrimination, as well as the over-involvement of statutory authorities in the lives of some communities. In these instances, extensive reparation is required before any meaningful engagement can occur.
Principle in practice:
- Work flexibly and in a coordinated way while leveraging existing therapeutic relationships across the family. Service contact should be streamlined and appropriately scaffolded to reduce burden on the family and young person and allow them to be active participants in a process being conducted “with” them, rather than one that is happening “to” them.
- Creative approaches which mitigate service disengagement include outreach and engagement over the long term to build trust and rapport on a gradual basis. Examples may include attending a young person’s home each week for a cup of tea and a chat (either with the protective parent or the young person if they are willing); exploring a young person’s interests or hobbies and participating in these with them (without any associated expectation of “talk therapy”); or assisting the family or young person by driving the young person to an appointment or generally being a physical and practical form of support in a family’s life.
- Advocacy to other systems and authorities on behalf of the young person also plays a role, including providing the young person and family with information about their rights and how they can advocate constructively for themselves. Particular consideration of a young person’s or family member’s capacity to engage is also crucial given the prevalence of trauma, disability and neurodivergence among this cohort. For example, practitioners may incorporate considerations around light and sound sensitivity for young people with ASD, or the use of communication aids or greater reliance on visual methods of communication.
Flexible and needs-based
This principle centres the importance of practitioners providing a service response that is tailored to the individual needs and goals of young people and their families. Different AVITH presentations include where the function of the young person’s behaviour is connected with their disability and/or mental health, as well as where the young person’s behaviour should be more appropriately characterised as resistance to harm perpetrated by another member of the family. Responses must be flexible and ultimately adapted to the needs which the family identifies as most pressing at that time. Flexibility also enables practitioners to provide a response at times that reflect the individual readiness of each family member. Implicit in this principle is understanding that, in order for practitioners to provide flexible and needs-based responses, they must be appropriately skilled and appropriately supported by both the system and their organisation.
Principle in practice:
- Programs must be resourced to provide a variety of service offerings in order to respond to what works best for the individual family and young person. This includes practitioners providing outreach to attend the family home or to meet the young person in a setting in which they feel most comfortable, such as a skatepark, library or community hub, school, or café. Resourcing and programming needs to allow for multiple attempts through different modes of engagement, including outreach and virtual or in-office catch-ups, as well as the use of various creative tools to generate engagement.
- Program resourcing and design needs to allow for engagement with multiple family members where relevant, including by different practitioners in the team, or the provision of specific supports to address particular needs in the family which are not directly related to AVITH, but which can improve family functioning and reduce household stress overall. Crucially, this may include brokerage to support family members to access brief periods of respite, specialist assessments or particular equipment which may improve their general wellbeing (such as music or sporting equipment). It may also involve using brokerage to facilitate opportunities for shared positive experiences, such as family outings. The research found that this was particularly crucial in the context of family histories which had formed collective or individual identity around trauma and shame and require support to start to rebuild and repair attachments.
- “Follow-through”, “open-ended” and “sequencing” are crucial concepts, so that clients have time to develop confidence that a practitioner will act on their commitments, be led by a client’s preferences, and be available when that client is ready to engage.
Intersectional and culturally safe
This principle involves ensuring that practitioners and services are equipped to respond to the specific cultural considerations of families and the intersecting identities of young people experiencing AVITH. This principle centres the experiences of Aboriginal and Torres Strait Islander families, families from CALD backgrounds, and LGBTQA+ and intersex young people and families, as well as families with young people with disability. To ensure that AVITH services are culturally responsive and safe, services must develop relationships with and across organisations working with specific communities – not to silo the work but to foster collaboration, support continuous learning and, most importantly, provide clients with agency and choice in the services with which they interact. Services must also recognise that individual family members will have different experiences of marginalisation – and that sources of common experience may also be sources ofconflict in the family dynamic.
Principle in practice:
- Program design and practice require active consideration of the ways in which wider experiences and community context intersect with young people’s use of AVITH. The research found that this requires consideration of how a young person’s experience or background may mean that they live with intergenerational trauma or have been exposed to particular stigma and marginalisation – including exclusion from services, homophobia, biphobia or transphobia (whether internal or external to their family home), as well as profiling and discrimination by police. Experiences of discrimination may intersect with co-occurring mental health and/or disability needs which, together, place young people in an increased position of vulnerability. Marginalised status may also be a source of conflict or tension between family members who feel disempowered or have a lack of access to wider supports. It may also be leveraged by other family members inthe context of broader DFV.
- Culturally safe and responsive ways of working include an awareness of, and active engagement with, a client’s identity and the ways in which culture and community may impact their needs and experiences. Supporting a young person and their family from a CALD background, for example, may involve assisting the family to heal from trauma in relation to their experiences as asylum seekers or refugees. Assistance might involve supporting the family around visa status needs or assisting them to navigate the complex service system where English is their second language, as well as providing them with pragmatic supports.
- Working with an Aboriginal and/or Torres Strait Islander family might involve identifying appropriate community-led services with which to collaborate or which can lead the response, as well as bringing in the young person’s wider family and kinship networks, including by involving respected Elders and community members.
- Work with a sexuality, sex or gender diverse young person, meanwhile, may include considerations around their experiences of coming out or transitioning, how these have been supported in the family or school, and their access to wider social and community networks that can build a sense of inclusion and belonging.
- Most importantly, intersectional and culturally safe responses demand strengths-based approaches that affirm and celebrate a young person’s identity in all its forms at a time during which they are exploring and taking their place in their community and the wider world.
Service accountability
This principle seeks to highlight the importance of keeping the service sector accountable in the support being provided to the young person and family, rather than maintaining a focus purely on holding the young person accountable to the system. To do this, the roles, responsibilities and expertise of each practitioner or service involved must be well understood by all.
Principle in practice:
- Program resourcing, design and practice must be sufficient to allow for follow-through and follow-up. An accountable service is one that does what it says it will do. Services which are committed to working with the family should agree, plan for and progress their specific goals, as determined by the family. At the system level this includes proactive and transparent communication between services, with an overall focus on ensuring that dynamic risk information is shared and managed collectively.
- Service accountability is also about undoing the harm caused by previous service interactions. Necessary ingredients include role clarity, proactive communication and coordinated ways of working to assume shared responsibility across the system for identifying and managing risk. This includes where there exists current risk from adult-perpetrated DFV which may be identified by some – but not all – of the services involved with the family and advocating to these services about widening their gaze to where the most urgent source of risk really lies.
- Practitioners can commit to accountability as a means of minimising the exhaustion and overwhelm so often experienced by parents engaged with the AVITH service sector. When an incident occurs within the family, for example, practitioners may choose to engage proactively with another practitioner who is also involved with the family to obtain relevant information. This is to avoid a situation where their parents are retelling the story multiple times to multiple services.
Enablers of collaborative practice
Critical enablers of collaborative practice were consistently identified throughout the research. Where these enablers were not recognised or present within the system, practitioners observed that this functioned as a barrier and stymied efforts to work collaboratively. Practitioners similarly observed that, where these enablers have been established, they can provide an important foundation for collaborative practice moving forward. Dialogue between the pillars and enablers are where the responsibilities of government and organisations lie, supporting the principle-informed practice that lies in between. Engagement with multiple levels of the Framework is also how genuine collaboration across the system, rather than just across practice, can occur.
Enabler:
Funding
- Adequate and appropriate funding was identified throughout the research as a critical enabler of effective and collaborative practice. Governments should resource programs over longer periods, such as over five years, to enable development and retention of a suitably skilled workforce and to allow for programs to be properly embedded and evaluated. Funding for individual programs should reflect appropriate caseloads, accounting for the complexity and scope of AVITH-focused work, as well as the time required to engage in genuinely collaborative work across service boundaries – including, for example, where multiple services are working around a family to respond to individual and collective needs. They should also provide for outreach as a core function, for clinical supervision and sector engagement and provision of brokerage and pragmatic support. Funding structures should be outcome-focused, rather than being focused onthrough-put, and should allow for long-term and intensive work where this is required.
Enabler:
Culture
- While the research highlighted the need for clear structures and processes to support coordinated and collaborative responses, a culture of collaboration emerged as equally crucial. Where practitioners or services have a narrow view of their role and accountabilities – rather than seeing themselves as simply one part of a broader response – this can undermine the potential for meaningful collaboration around the family.
Organisations should actively foster a culture of collaboration within and across organisational boundaries. This includes signalling to practitioners that it is valuable to invest time and effort in establishing and maintaining collaborative ways of working. Equally, organisations must embed recognition that identifying and responding to AVITH is a shared responsibility and that families may present to (or require support from) a range of programs, not simply those with an explicit AVITH focus. Government at local, state and federal levels has an opportunity to foster a culture of collaboration to support development of AVITH practice, recognising and valuing it as a specialisation and communicating its values to other sectors and systems. It can also support this by facilitating the provision of service information across sectors.
Enabler:
Continuous learning
- Given the emerging nature of understandings of AVITH (and related service responses), a commitment to continuous learning at the practitioner, organisational and system levels is critical. This includes creating opportunities for and valuing reflective practice, as well as opportunities for shared learning within and across programs and organisations – such as providing presentations around different areas of expertise and engaging in collaborative practice discussions around case studies.
Opportunities for continuous learning also interact with the principle of intersectional and culturally safe responses, with an imperative on all AVITH-focused services (and the governments and organisations which resource them) to develop relationships with organisations which work with specific cohorts and communities, fostering windows for ongoing practice development, secondary consultations and safer and more supported responses for young people and families.
Enabler:
Evidence-informed tools
- The requirement to use tools, practice guidance and frameworks that do not account for the complexity and breadth of AVITH presentations can function as a barrier to collaborative responses to AVITH. Conversely, the availability of relevant and appropriate tools can foster a shared language and understanding among practitioners, as well as supporting a structured approach to identifying and managing risk within families experiencing AVITH.
Tools which seek to adopt language and frames which reflect understandings of adult-perpetrated DFV were universally seen by AVITH practitioners participating in the research as being unsuitable and potentially harmful when working with families experiencing AVITH. Tools developed to support AVITH-focused work should instead be strengths-based and avoid stigmatisation of young people, siblings and protective parents, with capacity to recognise, assess and work with complex risk dynamics within families. This includes families in which there have been (or continue to be) experiences of adult-perpetrated violence, as well as the presence of multidirectional violence.
Enabler:
Service capacity
- The ability to work flexibly and responsively, including the capacity to work with families long-term and intensively where required, is contingent on appropriate caseloads within AVITH-specific services. At the same time, it is important that all families experiencing AVITH (or identified as being at risk of experiencing AVITH) are able to access a timely service response to prevent the escalation of risk.
It is therefore crucial for government to maintain a lens on the capacity of AVITH-specific services, as well as wider services which can provide early intervention where AVITH risk is identified, in order to meet demand. This includes monitoring where specific crises, such as the COVID-19 pandemic, contribute to increased risk, as well as monitoring longer term trends in demand. Importantly, government should work closely with those organisations with specific expertise in delivering AVITH interventions to ensure that additional resourcing and scaling up of service capacity is implemented in a way which is supported and sustainable for the sector, and leverages program infrastructure and existing expertise.
Enabler:
System stewardship
- A clear role exists for government in fostering an AVITH system response which is founded on a shared understanding of the nature and dynamics of AVITH; appropriate ways of responding; and the outcomes which a meaningful AVITH system response should be working to achieve. In particular, the multi-system nature of the “AVITH system” – which draws on the community-based service system, as well as legal, education, Child Protection and welfare systems – requires government to remove barriers to collaboration within and across systems and to facilitate opportunities for shared learning and reflection. This includes identifying where responses within one component of the AVITH system (such as the legal process) can act to undermine or counteract wider system responses aimed at family resilience, safety and (where appropriate) repair.
System stewardship also includes the accumulation and provision of information across different sectors which can support more effective practice. This includes, for example, the provision of information about AVITH-focused services to the legal system or working with legal system players to support information provision across areas to support more informed decision-making. It also includes placing greater emphasis on gathering information about what happens to young people when the tertiary end of the system intervenes, such as when they are removed from the home or present to emergency departments.
Importantly, system stewardship approaches involve government working alongside organisations and agencies, leveraging their expertise and working to steer the system towards key outcomes. This can occur at the system level, as well as through the adoption of place-based approaches and local service networks which can deliver holistic, tailored responses to families experiencing AVITH within their communities.
The discussion included above is also reflected in a more detailed representation of the Collaborative Practice Framework (Appendix A).
Discussion
The WRAP around families project was designed to be a targeted investigation into the service response to AVITH as a direct follow-up, or “coda”, to a recommendation from the PIPA project. As such, it had limited resourcing and was expected to be conducted as a brief inquiry, or stocktake, into the extent to which service responses had progressed since the PIPA project, as well as to provide support through a practice framework which could help to accelerate this progress further.
The impacts of COVID-19, however, had flow-on effects for the project which expanded both its timeframes and scale on the one hand, while limiting its scope on the other. The swift injection of funding from the Victorian Government in early 2021 – which came after the study’s initial design and in response to a recognised increase in AVITH during COVID-19-related lockdowns in 2020 – resulted in more practitioners working in the field, but with far less guidance than the pre-existing workforce. These practitioners were also in the position of establishing and running new programs while working primarily from home as Victoria returned to extended lockdown through the second half of 2021. This extended lockdown period, the increasing vulnerability of clients without service visibility, and an emphasis on responding to clients’ material needs ultimately meant that some services were simply not able to engage in the research, while also finding it difficultto build rapport with young clients.
Combined, these impacts meant that a project which was originally designed to be short, sharp and completed by the end of 2021 extended well into 2022 as sufficient time was allowed for practitioners from ACCOs to participate and for the DS program to continue to attempt client recruitment for the case study component. Ultimately, this meant that the research data involved contributions from a far greater number of practitioners than originally anticipated, but a smaller number of clients.
Despite these challenges, however, the findings and Framework resulting from the research potentially come at a more salient time than would have otherwise been the case. While policymakers and practitioners in Victoria were focused on surviving the state’s lockdowns and the ongoing impacts of multiple Omicron-variant waves throughout 2022, investment in a service model of care, the pending release of a practice guide to support risk assessment and management, and the development of training by the CFECFW will position policymakers and practitioners well to be able to consider next steps. This is important because, as practitioners contributing to the refinement of the Collaborative Practice Framework proposed above explained, “We have made some important progress, but the Framework is the ‘where to from here’.”
The Framework proposed by the research team is offered in lieu of a list of specific research recommendations around service provision for a number of reasons. The first is that the service landscape in jurisdictions around Australia (and internationally) differs so greatly that recommendations around specific service reform would not necessarily be useful beyond Victoria. The second is the clear indication from practitioner descriptions of their practice for the need to avoid prescriptive approaches, with the Framework designed to be adopted and applied in different contexts.
The third is that practice in this area involves such nuance and complexity that the Framework pushes policymakers towards considering this practice as a whole, rather than defaulting to acquittal of one recommendation in isolation from another, as the FVRIM has rightly identified too often occurs (FVRIM, 2021). That said, the practice examples nominated as part of the Framework are included to encourage practitioners and policymakers alike to consider how it can support reform in their particular environment. Practitioners, organisations and policymakers are therefore urged to engage with the Framework; to identify where their particular responsibilities lie within it; and how it could help them to move towards evidence-informed and genuinely collaborative responses, wherever they are on the service reform journey.
Assumptions challenged by the research
Several assumptions underpinned the project’s original design, which are important to identify here. This includes an assumption that longer term interventions – and interventions which worked with multiple family members – were increasingly viewed as the service standard. The research design was also driven by an assumption that collaboration was relatively achievable where sufficient practitioner will and interest existed. In particular, the research team were aware of the wider use of care teams and similar structures which bring together different disciplines around a young person or a family. Accordingly, the research team anticipated that these would be a potential source of support. The expectation of the research was also that collaboration could be just as easily achieved across a wider service network as it could within an organisation. While all the participants involved in the focus groups agreed with these imperatives and the basis ofthese assumptions, the research indicated that system recognition, capacity and, perhaps most relevantly, maturity were somewhat further behind.
Finally – and perhaps most importantly – the research was designed on the assumption that trauma in caregivers and young people from adult-perpetrated DFV was a significant driving factor in the use of AVITH, as well as in reduced capacity of caregivers to manage the impacts of this behaviour and address their own support needs while responding to their child’s. This was a strong finding from the PIPA project and is also increasingly emphasised in literature which highlights the gendered nature of AVITH victimisation and the importance of repairing ruptured relationships between mothers and children (Burck, 2021).
While the research team was well aware that this trauma can include current adult-perpetrated DFV, including through leveraging the legal system response as identified by the PIPA project (Campbell et al., 2020), what was perhaps underestimated was the sheer extent to which this ongoing coercive control and systems abuse were such a significant feature of practice contexts and, arguably, the predominant factor in many clients’ lives. Certainly, while only illustrative given the small sample size, the overwhelming narrative of the three interviews with mothers, as well as on the case files, was the way in which DFV from a former partner was continuing to impact almost every aspect of the mothers’ and children’s lives, including more than a decade after separation. This echoed the suggestion in the PIPA project that a system focus on young people using harm was often missing the “original perpetrator,” who remainedout of view of the system (Campbell et al., 2020, p. 132) but who continued to be the source of real harm across the family.
Some practitioners across the research suggest that this limited lens on the impacts of adult-perpetrated DFV on children and young people – and the extraordinary lengths to which some perpetrator parents, predominantly fathers in the context of these research findings, will go to control their children’s lives – may have something to do with the community’s wider discomfort with its collective failure to protect children and young people in the first place.
Where it becomes dangerous is [practitioners not] … noticing what’s going on, actually leaning into that rather than avoiding it like the plague … As a community we don’t want to know about trauma, we don’t wanna know that kids are treated this way. I think fundamentally what sits under a lot of it is “Why is our system so crap at looking after these kids?” Because, you know, we are a fairly affluent society that doesn’t want to believe that kids get kicked and cigarette burned and, you know, everything else that happens. (Practitioner 38)
Listen to the people who are working with this child. That’s what gets me in the heart about all this … We can talk about practice issues, policy issues, whatever, but there is a child that is telling you that they’re unsafe and you’re not giving them the benefit of the doubt … (Practitioner 49)
This finding around the dominating presence of current adult-perpetrated DFV is important because it further confirms where practice and service attention in this area should be directed – whether at the point of:
- early intervention in terms of an emphasis on supporting recovery for women and children escaping violence
- therapeutic responses for young people who use violence at home, rather than punitive responses which push them by default onto a criminal justice trajectory
- statutory authority involvement, which maintains a lens on where the real source of risk to children may lie.
Just as crucially, it suggests a genuine prevention opportunity with respect to AVITH, where service systems can intervene early to support mothers and children to recover and to form new, positive family identities, rather than “waiting until there’s a crisis” (Practitioner 72) or when it’s simply “ten years too late” (Campbell et al., 2020, p. 154).
Limitations of the research
The research had other key limitations which should be acknowledged. The first was the substantial and ongoing impacts of COVID-19 on the DS program, which made engagement with clients – and associated recruitment to the interviews, in particular – a considerable challenge. Accordingly, the interviews with parents highlighted more about the limitations of prior service engagement and the ongoing impacts of adult-perpetrated DFV than they did about engagement with the DS program to an extent. That said, parents did identify what they saw as being beneficial in terms of the support that they had received from the program, as well as what they think that young people require from a service under more stable service delivery circumstances.
Other limitations include the absence of Child Protection practitioner or Victoria Police contributions (although Victoria Police contributed significantly to the PIPA project), also largely attributable to the demands of the pandemic, as well as to the targeted scope of the project itself. A further potential limitation is the lack of contribution from private practitioners, such as psychologists, which was similarly acknowledged as a gap by the practitioners across the focus groups in terms of the effectiveness of care teams. To note, psychologists and other practitioners providing services on a fee-for-service basis may be less likely to see clients who have been immersed in service system involvement or “over-serviced” and, in turn, clients who are less likely to report – or at least disclose – histories of trauma (Gallagher, 2016). As the PIPA project found, however, this does not prevent these families from presenting to the legal system (asopposed to the community-based service system), including in the context of young people who are identified as using AVITH while being victims and survivors of adult-perpetrated emotional and psychological abuse (Campbell et al., 2020).
Additionally important to acknowledge is the extent to which the circumstances of COVID-19 lockdowns may have been contributing to an escalation in the challenges that practitioners were experiencing, given the recognised associated increase in AVITH during this time. This potentially means that practitioners were seeing a “net widening” in the types of matters to which they were responding, or an entrenched complexity in clients which contributed to increased demand.
This increased demand was actually anticipated by the research team to be emphasised in practitioner contributions to the focus group discussions, given that the rise in the number of families experiencing AVITH – co-occurring with young people’s and parents’ deteriorating mental health during repeated lockdowns – had been a finding of earlier work by members of the research team (Campbell & McCann, 2020; Drummond Street Services, 2020). Important to note, however, is that the primary concerns of participating practitioners related to system and policy settings which pre-dated the pandemic, but which they feared would be compounded by a lack of government resourcing in human services sectors in the future as a result of the pandemic and its impacts.
Implications for policy and practice
Practitioners in the focus group discussions were concerned that pre-existing system challenges had not only been compounded by the pandemic but would also be less likely to be addressed given the pandemic’s drain on public resources. This practitioner concern is therefore a key consideration for policymakers as they move towards future service design and investment –whether it is fiscally responsible to constrain service funding in the short term when client needs and complexity are likely to have been further entrenched, as international research suggests (Condry et al., 2020), and an exhausted workforce is depleted. Rather, the WRAP around families research points to the need for, as Condry and colleagues (2020) described it, a “safeguarding surge”, including greater support for families and young people at an earlier point. Most significantly, this involves providing support for women and children as soon as they are identified as experiencing, oras having experienced, adult-perpetrated DFV. This includes recognising children and young people as victims and survivors in their own right, including in early childhood. Crucially, this also includes avoiding any assumptions that a child or young person is no longer at risk or experiencing ongoing impacts of the harm, despite the original perpetrator remaining out of view. Equally this research echoes the PIPA project and other research which points to the substantial need for greater support for families with a young person with disability and who may become vulnerable to a family violence system response as a result of associated behaviour.
Investment in earlier intervention also represents an opportunity for prevention of AVITH and escalation of any risk for families, as noted above. This requires a commitment from government at both state and federal levels to resource services sufficiently to allocate time and attention to families who have not yet reached crisis. It also requires a commitment from government at these levels to invest in the long-term development of an appropriate workforce, as noted above.
Where the system fails to intervene earlier, however, the WRAP around families project offers a blueprint to support a genuinely collaborative and consistent framework for service responses to AVITH. In doing so it signals that the nuance, flexibility and complexity which are so clearly required in the practice may mean that current approaches to service funding should be re-examined and a genuine investment in longer term and meaningful results instead brought to the fore.
… commitment to a kind of long-standing program that could be evaluated over a five-year period rather than just, you know, 12 months … so it can really be evaluated and developed …. It’s a very specialist area and I think it worthy of a really specialist, nuanced approach to the work. It’s still sort of in its infancy to a large extent. (Practitioner 16)
Directions for future research
The findings from the WRAP around families project highlight significant scope for future research in the area of collaborative service responses to AVITH. Rather than being able to describe different versions of embedded collaboration as anticipated, the research team concluded that the study was attempting to address a bigger research and practice gap than anticipated. Significant opportunities therefore exist for future research which can explore the potential adoption of resulting collaborative approaches, including the Framework proposed by this research, across the service system. This includes at an organisational as well as a multi-agency level.
More specifically, although the research team was not ultimately able to speak to young people, the findings overall suggested that the needs of children and young people grappling with the wider impacts of a sibling using violence confirms this as a direction for future research. In addition, the research suggested that the relationship of wider adverse childhood experiences to the use of AVITH – including, in particular, bullying victimisation and familial grief – should be an area of future research attention.
Given that challenges – and opportunities for more effective collaboration – were volunteered by practitioners across the research regarding Child Protection involvement in families’ lives, this is also a clear area of need for future research focus. The PIPA project recommended the development of a specific AVITH focus and framework within Child Protection authorities and, accordingly, relevant senior stakeholders were also invited to test the findings from practitioner focus groups but did not take up the invitation. Dedicated research exploring how Child Protection practitioners can engage with their statutory obligations in the context of AVITH – including collaborating effectively and consistently with other services – should therefore be explored, potentially in the context of broader work around improvements in Child Protection authorities’ capacity to identify and respond to adult perpetration.
Crucially, the relationship of current, as well as prior, experiences of adult-perpetrated DFV in the context of AVITH should be a significant focus of future research. This requires pushing the focus of research attention beyond the default in literature and policy environments alike to describe the relationship of trauma to the use of AVITH as predominantly a historical one. Given that a failure to identify current risk from adult-perpetrated violence may result, in part, from the lack of young people’s voices contributing to research, directions for future research must include, most importantly of all, opportunities for young people to share their experiences safely and in their own words.
I hope that we can get to the point where the work that we do with young people and their families is resourced in a manner that removes the stigma and the shame and the guilt that sits alongside it … For me, that’s the key to having real change. (Practitioner 19)
Let’s all just come together and know that if we don’t get it right with them, they’re not going to turn into well-rounded, high-achieving adults, we’re further damaging them. And it’s only going to come back on us as a community. (Practitioner 49)
As one practitioner remarked, developing appropriate and effective responses to AVITH – and, ideally, preventing it in the first place – “is a forever journey” (Practitioner 24), something in which all systems will continue to be engaged and challenged as they learn, respond and evolve.
References
Armstrong, G., Cain, C., Wylie, L., Muftić, L., & Bouffard, L. (2018). Risk factor profile of youth incarcerated for child to parent violence: A nationally representative sample. Journal of Criminal Justice, 58, 1–9. https://doi.org/10.1016/j.jcrimjus.2018.06.002
Armstrong, G. S., Muftic, L. R., & Bouffard, L. A. (2021). Factors influencing law enforcement responses to child to parent violence. Journal of Interpersonal Violence, 36(9–10), 4979–4997.
https://doi.org/10.1177/0886260518794510
Australian Domestic and Family Violence Death Review Network, & Australia’s National Research Organisation for Women’s Safety. (2022). Australian Domestic and Family Violence Death Review Network Data Report: Intimate partner violence homicides 2010–2018 (2nd ed.; Research report, 03/2022). ANROWS. https://www.anrows.org.au/publication/australian-domestic-and-family-violence-death-review-network-data-report-intimate-partner-violence-homicides-2010-2018/read/
Bagshaw, D., Brown, T., Wendt, S., Campbell, A., McInnes, E., Tinning, B., Batagol, B., Sifris, A., Tyson, D., Baker, J., & Fernandez Arias, P. (2011). The effect of family violence on post-separation parenting arrangements: The experiences of children and adults from families who separated post 1995 and post 2006. Family Matters, 86, 49–61.
Beckmann, L. (2020). Exposure to family violence and adolescent aggression in multiple social contexts: Classroom social resources as moderators. Journal of Family Violence, 35(5), 471–484.
Beckmann, L., Bergmann, M., Fischer, F., & Mößle, T. (2021). Risk and Protective Factors of Child-to-Parent Violence: A Comparison Between Physical and Verbal Aggression. Journal of Interpersonal Violence, 36(3–4), NP1309–1334NP. https://doi.org/10.1177/088626051774612
Belzile, J. A., & Öberg, G. (2012). Where to begin? Grappling with how to use participant interaction in focus group design. Qualitative Research, 12(4), 459–472.
Blakemore, T., Rak, L., Agllias, K., Mallett, X., & McCarthy S. (2018) ‘Understandings of youth perpetrated interpersonal violence among service providers in regional Australia’ Journal of Applied Youth Studies, 2(5), 53–69.
Boxall, H., & Morgan, A. (2020). Repeat domestic and family violence among young people (Trends and Issues in Crime and Criminal justice no. 591). Australian Institute of Criminology https://www.aic.gov.au/sites/default/files/2020-05/ti591_repeat_domestic_and_family_violence_among_young_people.pdf
Boxall, H., Morgan, A., & Brown, R. (2020). The prevalence of domestic violence among women during the COVID-19 pandemic (Statistical Bulletin no. 28). Australian Institute of Criminology.
https://www.aic.gov.au/sites/default/files/2020-07/sb28_prevalence_of_domestic_violence_among_women_during_covid-19_pandemic.pdf
Boxall, H., Morgan, A., Voce, I., & Coughlan, M. (2020). Responding to adolescent family violence: Findings from an impact evaluation (Trends and Issues in Crime and Criminal Justice no. 601). Australian Institute of Criminology. https://www.aic.gov.au/sites/default/files/2020-09/ti601_responding_to_adolescent_family_violence.pdf
Breckenridge, J., & Hamer, J. (2014). Traversing the maze of “evidence” and “best practice” in domestic and family violence service provision in Australia (Issues paper no. 26). Australian Domestic and Family Violence Clearinghouse.
Breman, R., MacRae, A., & Vicary, D. (2018). Child-perpetrated family violence in kinship care in Victoria. Children Australia, 43(3), 2018, 192–197. https://doi.org/10.3316/agispt.20181107003585
Brown, T. C. (2006). Child abuse and domestic violence in the context of parental separation and divorce: New models of intervention. In C. Humphreys & N. Stanley (eds.), Domestic violence and child protection (pp. 155–168). Jessica Kingsley Publishers.
Burck, D. (2021) Adolescent-to-parent violence and the promise of attachment-based interventions. In K. Fitz-Gibbon, H. Douglas & J. Maher (eds.), Young people using family violence: International perspectives on research, responses and reforms (pp. 55–68). Springer.
Burck, D., Walsh, D., & Lynch, D. (2019). Silenced mothers: Exploring definitions of adolescent-to-parent violence and implications for practice. Advances in Social Work and Welfare Education, 21(1), 7–18.
https://doi.org/10.1177/15248380211053618
Campbell, E. (2021) Missing the mark: The problem of applying a “one size fits all” standard legal response to adolescent family violence perpetration. In K. Fitz-Gibbon, H. Douglas & J. Maher (eds.), Young people using family violence: international perspectives on research, responses and reforms (pp. 87–106). Springer.
Campbell, E., & McCann, B. (2020). Behind closed doors: Adolescent violence in the home (AVITH) during COVID & challenges to come. Centre for Innovative Justice, RMIT University, Centre for Family Research & Evaluation, & Drummond Street Services.
Campbell, E., Richter, J., Howard, J., & Cockburn, H. (2020). The PIPA project: Positive interventions for perpetrators of adolescent violence in the home (AVITH) (Research report, 04/2020). ANROWS.
https://www.anrows.org.au/publication/the-pipa-project-positive-interventions-for-perpetrators-of-adolescent-violence-in-the-home-avith/
Cardenas, M. C., Bustos, S. S., & Chakraborty, R. (2020). A “parallel pandemic”: The psychosocial burden of COVID-19 in children and adolescents. Acta Paediatrica, 109(11), 2187–2188.
https://doi.org/10.1111/apa.15536
Centre for Innovative Justice. (2022). Evaluation of the pre-court support for adolescents using violence in the home (AVITH) pilot: Final evaluation report. RMIT University.
Centre for Justice Innovation. (2021). Break4Change. Retrieved June 9, 2021, from
https://justiceinnovation.org/project/break4change
Condry, R., & Miles, C. (2021). Children who perpetrate family violence are still children: Understanding and responding to adolescent to parent violence. In K. Fitz-Gibbon, H. Douglas & J. Maher (eds.), Young people using family violence: international perspectives on research, responses and reforms (pp. 1–18). Springer.
Condry, R., Miles, C., Brunton-Douglas, T., & Oladapo, A. (2020). Experiences of child and adolescent to parent violence in the Covid-19 pandemic. University of Oxford.
https://www.law.ox.ac.uk/sites/files/oxlaw/final_report_capv_in_covid-19_aug20.pdf
Contreras, L., Bustos-Navarrete, C., & Cano-Lozano, M. (2019). Child-to-parent violence questionnaire (CPV-Q): Validation among Spanish adolescents. International Journal of Clinical and Health Psychology, 19, 67–74. https://doi.org/10.1016/j.ijchp.2018.09.001
Contreras, L., & del Carmen Cano, M. (2016). Child-to-parent violence: The role of exposure to violence and its relationship to social-cognitive processing. European Journal of Psychology Applied to Legal Context, 8(2), 43. https://doi.org/10.1016/j.ejpal.2016.03.003
Contreras, L., León, S., & Cano-Lozano, M. (٢٠٢٠). Assessing child-to-parent violence with the child-to-parent violence questionnaire, parents’ version (CPV-Q-P): Factor structure, prevalence, and reasons. Frontiers in Psychology, 11, 604956. https://doi.org/10.3389/fpsyg.2020.604956
Coogan, D. (2016). Listening to the voices of practitioners who encounter child to parent violence and abuse: Some findings from an action research project. Irish Social Worker Journal (Winter), 41–48.
Coogan, D. (2018). Child to parent violence and abuse: Family interventions with non-violent resistance. Jessica Kingsley Publishers.
Cottrell, B. (2001). Parent abuse: The abuse of parents by their teenage children. Health Canada, Population and Public Health Branch, National Clearinghouse on Family Violence.
Coutts, P. (2019). The many shades of co-produced evidence. Carnegie UK Trust.
Crime Statistics Agency. (2020). Victoria Police July 2015–June 2020. Retrieved May 5, 2021, from
https://www.crimestatistics.vic.gov.au/family-violence-data-portal/download-data-tables
Docherty, M., Kubik, J., Herrera, C., & Boxer, P. (2018). Early maltreatment is associated with greater risk of conduct problems and lack of guilt in adolescence. Child Abuse & Neglect, 79, 173–182.
Douglas, H., & Walsh, T. (2022). Adolescent family and dating violence and the criminal law response. Journal of Family Violence, 38, 287–299. https://doi.org/10.1007/s10896-022-00373-x
Drummond Street Services. (2020). Evaluating the impacts of COVID-19 and drummond street’s response (COVID-19 Response Edition 1). https://ds.org.au/wp-content/uploads/2020/10/COVID-19-Staff-report-Edition-1-public.pdf
Elliott, K., McGowan, J., Benier, K., Maher, J., & Fitz-Gibbon, K. (2017). Investigating adolescent family violence: Background, research and directions: Context report. Monash University.
https://www.monash.edu/__data/assets/pdf_file/0007/1532275/investigating-adolescent-family-violence-background-research-and-directions.pdf
Espejo-Siles, R., Zych, I., Farrington, D. P., & Llorent, V. J. (2020). Moral disengagement, victimization, empathy, social and emotional competencies as predictors of violence in children and adolescents. Children and Youth Services Review, 118, 105337.
https://psycnet.apa.org/doi/10.1016/j.childyouth.2020.105337
Fagan, A. A. (2020). Child maltreatment and aggressive behaviors in early adolescence: Evidence of moderation by parent/child relationship quality. Child Maltreatment, 25(2), 182–191.
Family Violence Protection Act 2008 (Vic).
http:// www5.austlii.edu.au/au/legis/vic/consol_act/fvpa2008283/
Family Violence Reform Implementation Monitor. (2021a). Report of the Family Violence Reform Implementation Monitor. Victorian Government. https://www.fvrim.vic.gov.au/report-family-violence-reform-implementation-monitor-1-november-2020
Family Violence Reform Implementation Monitor. (2021b). Accurate identification of the predominant aggressor. Victorian Government. https://www.fvrim.vic.gov.au/monitoring-victorias-family-violence-reforms-accurate-identification-predominant-aggressor
Fisher, J. R., Tran, T. D., Hammargerg, K., Sastry, J., Nguyen, H., Rowe, H., Popplestone, S., Stocker, R., Stubber, C., & Kirkman, M. (2020). Mental health of people in Australia in the first month of COVID-19 restrictions: A national survey. Medical Journal of Australia, 213(10), 458–464.
https://doi.org/10.5694/mja2.50831
Fitz-Gibbon, K., Elliott, K., & Maher, J. (2018). Investigating adolescent family violence in Victoria: Understanding experiences and practitioner perspectives. Monash University.
https://researchmgt.monash.edu/ws/portalfiles/portal/250376810/Adolescent_Family_Violence_in_Victoria_Final_Report.pdf
Fitz-Gibbon, K., Maher, J., & Elliott, K. (2021). Barriers to help seeking for women victims of adolescent family violence: A Victorian (Australian) case study. In K. Fitz-Gibbon, H. Douglas, & J. Maher (eds.), Young people using family violence: international perspectives on research, responses and reforms (pp. 39–54). Springer.
Fitz-Gibbon, K., Meyer, S., Maher, J., & Roberts, S. (2022). Adolescent family violence in Australia: A national study of prevalence, history of childhood victimisation and impacts (Research report, 15/2022). ANROWS. https://www.anrows.org.au/publication/adolescent-family-violence-in-australia-a-national-study-of-prevalence-history-of-childhood-victimisation-and-impacts/
Flyvberg, B. (2006). Five misunderstandings about case study research. Qualitative Inquiry, 12(2), 219–245. https://doi.org/10.1177/1077800405284363
Fraser, N. (1985). What’s critical about critical theory? The case of Habermas and gender. New German Critique, 35, 97–131. https://doi.org/10.2307/488202
Gair, S., Zuchowski, I., Thorpe, R., Henderson, D., & Munns, L. (2019). “In the firing line”: Grandparent carers at risk of family violence. Journal of Family Violence, 34(4), 321–329.
Gallagher, E. (2016) The “Who’s in Charge” program. In A. Holt (ed.), Working with adolescent violence towards parents: Approaches and contexts for intervention (pp. 34–46). Routledge.
Gallego, R., Novo, M., Farina, F., & Arce, R. (2019). Child-to-parent violence and parent-to-child violence: A meta-analytic review. European Journal of Psychology Applied to Legal Context, 11(2), 51–59. https://doi.org/10.5093/ejpalc2019a4
Gerring, John. (2004). What is a case study and what is it good for? American Political Science Review, 98(2), 341–354.
Gilman, A. B., & Walker, S. C. (2020). Evaluating the effects of an adolescent family violence intervention program on recidivism among court-involved youth. Journal of Family Violence, 35(2), 95–106. https://doi.org/10.1007/s10896-019-00070-2
Hernández, A., Martín, A., Hess-Medler, S., & García-García, J. (2020). What goes on in this house does not stay in this house: Family variables related to adolescent-to-parent offenses. Frontiers in Psychology, 11, 581761.
Holt, A. (2013). Adolescent-to-parent-abuse: Current understandings in research, policy and practice. Policy Press. https://doi.org/10.2307/j.ctt1t6p748
Holt, A. (ed.). (2016). Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention. Routledge.
Holt, A., & Birchall, J. (2020). Investigating experiences of violence towards grandparents in a kinship care context: Project summary. University of Roehampton, London.
https://helenbonnick.files.wordpress.com/2020/05/violenceagainstgrandparents_projectsummary_may2020.pdf
Holt, A., & Retford, S. (2013). Practitioner accounts of responding to parent abuse: A case study in ad hoc delivery, perverse outcomes and a policy silence. Child and Family Social Work, 18, 365,
https://doi.org/10.1111/j.1365-2206.2012.00860.x .
Holt, A., & Shan, P. C. (2018). Exploring fatal and non-fatal violence against parents: Challenging the orthodoxy of abused adolescent perpetrators. Journal of Offender Therapy and Comparative Criminology, 62(4), 915–934. https://doi.org/10.1177/0306624X16672444
Howard, J., & Holt, A. (2015). Special considerations when working with adolescent family violence. In A. Holt (ed.), Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention. Taylor & Francis Group.
Ibabe, I,. Jaureguizar, J., & Bentler, P. (2013). Risk factors for child-to-parent violence. Journal of Family Violence, 28, 523. http://dx.doi.org/10.1007/s10896-013-9512-2
Jouriles, E. N., Gower, T., Rancher, C., Johnson, E., Jackson, M. L., & McDonald, R. (2021). Families seeking services for sexual abuse: Intimate partner violence, mothers’ psychological distress, and mother–adolescent conflict. Journal of Family Psychology, 35(1), 103.
https://psycnet.apa.org/doi/10.1037/fam0000798
Katz, E. (2019). Coercive control, domestic violence and a five-factor framework: Five factors that influence closeness, distance and strain in mother–child relationships. Violence Against Women, 25(15), 1829–1853. https://doi.org/10.1177/1077801218824998
Kehoe, M., Ott, N., & Hopkins, L. (2020). Responding to adolescent violence in the home: A community mental health approach. Australian and New Zealand Journal of Family Therapy, 41, 342–354.
https://doi.org/10.1002/anzf.1432
Kickett, G., Chandran, S., & Mitchell, J. (2019). Woon-yah Ngullah Goorlanggass – Caring for our children: A culturally strong, therapeutic kinship care for Aboriginal children, young people and their families. Developing Practice: The Child, Youth and Family Work Journal, 52, 25–39.
https://doi.org/10.3316/informit.852240543758477
Kwong, M., Bartholomew, K., Henderson, A., & Trinke, S. (2003). The intergenerational transmission of relationship violence. Journal of Family Psychology, 17(3), 288. https://doi.org/10.1037/0893-3200.17.3.288
Lamb, C. (2018). Breaking the cycle of violence for child refugees who display aggressive behaviour. Educating Young Children: Learning and Teaching in the Early Childhood Years, 24(3), 21–23. https://search.informit.org/doi/10.3316/aeipt.221755
Loinaz, I., & de Sousa, A. (2020). Assessing risk and protective factors in clinical and judicial child-to-parent violence cases. European Journal of Psychology Applied to Legal Context, 12(1), 43.
https://doi.org/10.5093/ejpalc2020a5
Mack, N., Woodsong, C., MacQueen, K., Guest, G., & Namey, E. (2005). Qualitative research methods: A data collector’s field guide. Family Health International.
Maher, J. M., Fitz-Gibbon, K., Meyer, S., Roberts, S., & Pftizner, N. (2021). Mothering through and in violence: Discourses of the “good mother”. Sociology, 55(4), 659–676.
https://doi.org/10.1177/0038038520967262
Malvaso, C. G., Delfabbro, P. H., & Day, A. (2019). Adverse childhood experiences in a South Australian sample of young people in detention. Australian and New Zealand Journal of Criminology, 52(3), 411–431. https://doi.org/10.1177/0004865818810069
Margolin, G., & Baucom, B. (2014). Adolescents’ aggression to parents: Longitudinal links with parents’ physical aggression. Journal of Adolescent Health, 55(5), 645.
https://doi.org/10.1016%2Fj.jadohealth.2014.05.008
Martínez-Ferrer, B., Romero-Abrio, A., León-Moreno, C., Villarreal-González, M., & Musitu-Ferrer, D. (2020). Suicidal ideation, psychological distress and child-to-parent violence: A gender analysis. Frontiers in Psychology, 11, 575388. https://doi.org/10.3389/fpsyg.2020.575388
McDonald, C., Wiebe, D., Guerra, T., Thomas, N., & Richmond, T. (2011). The importance of family to youth living in violent communities. Journal of Psychiatric and Mental Health Nursing, 653.
https://doi.org/10.1111/j.1365-2850.2011.01774.x
McGeeney, E., Barakat, F., Langeland, G., & Williams, S. (2016). The Yuva young people’s service: A holistic approach to addressing child-to-parent violence in London. In A. Holt (ed.), Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention (pp. 117–133). Routledge.
McKenna, M., & O’Connor, R. (2012). Walking on eggshells: Child and adolescent violence in the family. Relationships Australia (SA), Flinders University & Southern Junction Community Services.
Meyer, S., Reeves, E., & Fitz-Gibbon, K. (2021), The intergenerational transmission of family violence: Mothers’ perceptions of children’s experiences and use of violence in the home. Child & Family Social Work, 26, 476–484. https://doi.org/10.1111/cfs.12830
Meyer, S., & Stambie, R. M. (2020). Mothering in the context of violence: Indigenous and non-Indigenous mothers’ experiences in regional settings in Australia. Journal of Interpersonal Violence.
https://doi.org/10.1177/0886260520975818
Moulds, L. G., Malvaso, C., Hackett, L., & Francis, L. (2019). The KIND program for adolescent family and dating violence. Australian and New Zealand Journal of Family Therapy.
https://doi.org/10.1002/anzf.1364
Nam, B., Kim, J.Y., Bright, C. L., & Jang, D. (2020). Exposure to family violence, peer attachment, and adolescent-to-parent violence. Journal of Interpersonal Violence, 37(7–8), 1–22.
https://doi.org/10.1177/0886260520960109
Nowakowski-Sims, E. (2019). An exploratory study of childhood adversity and delinquency among youth in the context of child-to-parent and sibling-to-sibling violence. Journal of Family Social Work, 22(2), 126–145. https://doi.org/10.1080/10522158.2018.1496510
O’Hara, K. L., Duchschere, J. E., Beck, C. J. A., & Lawrence, E. (2017). Adolescent-to-parent violence: Translating research into effective practice. Adolescent Research Review, 2(3), 181–198.
https://doi.org/10.1007/s40894-016-0051-y
O’Keefe, M. (2005) Teen dating violence: A review of risk factors and prevention efforts. National Online Resource Center on Violence Against Women. https://vawnet.org/material/teen-dating-violence-review-risk-factors-and-prevention-efforts
Om, J. (2020, August 25). Coronavirus hard lockdown of Melbourne public housing towers left residents feeling like “criminals”, inquiry hears. ABC News. https://www.abc.net.au/news/2020-08-25/coronavirus-melbourne-public-housing-tower-shutdown-inquiry/12589372
Pagani, L., Tremblay, R., Nagin, D., Zoccolillo, M., Vitaro, F., & McDuff, P. (2004). Risk factor models for adolescent verbal and physical aggression toward mothers. International Journal of Behavioural Development, 28(6), 528. https://doi.org/10.1080/01650250444000243
Papamichail, A., & Bates, E. (2020). “I want my mum to know that I am a good guy …”: A thematic analysis of the accounts of adolescents who exhibit child-to-parent violence in the United Kingdom. Journal of Interpersonal Violence, 37(9-10), 5849–5856.
https://doi.org/10.1177/0886260520926317
Paterson, R., Luntz, H., Perlesz, A., & Cotton, S. (2002). Adolescent violence towards parents: Maintaining family connections when the going gets tough. Australian and New Zealand Journal of Family Therapy, 23, 90. https://doi.org/10.1002/j.1467-8438.2002.tb00493.x
Peck, A., Hutchinson, M., & Provost, S. (2020). Young person-to-mother violence: An integrative review of evidence from Australia and New Zealand. Australian Social Work, 1. https:// doi.org/10.1080/0312407X.2021.188730
Peek, L., & Fothergill, A. (2009). Using focus groups: Lessons from studying daycare centers, 9/11, and Hurricane Katrina. Qualitative Research, 9, 31–59. https://doi.org/10.1177/1468794108098029
Pereira, R., Loinaz, I., del Hoyo-Bilbao, J., Arrospide, J., Bertino, L., Calvo, A., Montes, Y., & Gutiérrez, M. M. (2017). Proposal for a definition of filio-parental violence: Consensus of the Spanish Society for the Study of Filio-Parental Violence (SEVIFIP). Psychologist Papers, 38(3), 216–223.
https://doi.org/10.23923/pap.psicol2017.2839
Perkins, N., & Grossman, S. F. (2020). Sibling violence: The missing piece in family violence policy. Advances in Social Work, 19(1), 138–156. https://doi.org/10.18060/22611
Perkins, N. H., Rai, A., & Grossman, S. F. (2021). Physical and emotional sibling violence in the time of COVID-19. Journal of Family Violence, 1–8. https://doi.org/10.1007/s10896-021-00249-6
Peterman, A., Potts, A., O’Donnell, M., Thompson, K., Shah, N., Oertelt-Prigione, S., & van Gelder, N. (2020). Pandemics and violence against women and children (Working paper no. 528). Center for Global Development. https://www.cgdev.org/sites/default/files/pandemics-and-vawg-april2.pdf
Pfitzner, N., Fitz-Gibbon, K., Meyer, S., & True, J. (2020). Responding to Queensland’s “shadow pandemic” during the period of COVID-19 restrictions: Practitioner views on the nature of and responses to violence against women. Monash Gender and Family Violence Prevention Centre, Monash University. https://apo.org.au/sites/default/files/resource-files/2020-06/apo-nid306064.pdf
Pösö, T., Honkatukia, P., & Nyqvist, L. (2008). Focus groups and the study of violence. Qualitative Research, 8(1), 73–89. https://doi.org/10.1177/1468794107085297
Reed R. G., Barnard, K., & Butler, E. A. (2015). Distinguishing emotional coregulation from codysregulation: An investigation of emotional dynamics and body weight in romantic couples. Emotion, 15(1), 45–60. https://doi.org/10.1037/a0038561
Respect. (2021). Respect Young People’s Programme.
https://www.respect.uk.net/pages/115-rypp
Robinson, E., Power, L., & Allan, D. (2011). What works with adolescents? Family connections and involvement in interventions for adolescents with problem behaviours. Family Matters, 88, 57–64.
Robinson, E., & Miller, R. (2012). Adolescents and their families: Best interest case practice model specialist practice resource. Victorian Government, Department of Human Services.
Routt, G., & Anderson, L. (2011). Adolescent violence towards parents. Journal of Aggression, Maltreatment & Trauma, 20(1), 1. https:// doi.org/10.1080/10926771.2011.537595
Routt, G., & Anderson, L. (2016). Building respectful family relationships: Partnering restorative practice with cognitive-behavioural skill learning. In A. Holt (ed.), Working with adolescent violence and abuse towards parents: Approaches and contexts for intervention (pp. 15–33). Routledge.
Rutter, N. (2020). “I’m meant to be his comfort blanket, not a punching bag”: Ethnomimesis as an exploration of maternal child to parent violence in pre-adolescents. Qualitative Social Work: Research and Practice, 20(1), 1317–1338. https://doi.org/10.1177/1473325020940774
Rutter, N., Hall, K., & Westmarland, N. (2022) Responding to child and adolescent-to-parent violence and abuse from a distance: Remote delivery of interventions during Covid-19. Children & Society, 1–7.
https://doi.org/10.1111/chso.12622
Selwyn, J., & Meakings, S. (2016). Adolescent-to-parent violence in adoptive families. British Journal of Social Work, 46(5), 1224–1240. https://doi.org/10.1093/bjsw/bcv072
Shanholtz, C. E., O’Hara, K. L., Duchschere, J. E., Beck, C. J., & Lawrence, E. (2020). Understanding the perception of stakeholders in reducing adolescent-to-parent violence/aggression. Journal of Adolescence, 80, 264–274. https://doi.org/10.1016/j.adolescence.2020.02.015
Shannahan, B. (2017). We don’t give up: Developing family and community responses to adolescent-to-parent violence. International Journal of Narrative Therapy and Community Work, 2, 13–27.
https://search.informit.org/doi/10.3316/informit.959969122982399
Simons, H. (2012). Case study research in practice. SAGE Publications Ltd.
Simmons, M., McEwan, T. E., & Purcell, R. (2020). A social-cognitive investigation of young adults who abuse their parents. Journal of Interpersonal Violence, 37(1–2), 327–349. https://doi.org/10/1177/0886260520915553
Simons, H. (2014). Case study research: In-depth understanding in context. In P. Leavy (ed.), The Oxford Handbook of Qualitative Research (pp. 1–29). Oxford University Press.
Spearman, K., Hardesty, J., & Campbell, J. (2022). Post-separation abuse: A concept analysis. Journal of Advanced Nursing. https://doi.org/10.1111/jan.15310
State of Victoria. (2014). Adolescent family violence program service model (Draft, February 2014).
https:// providers.dhhs.vic.gov.au/adolescent-family-violence-program-service-model-word
State of Victoria. (2016). Royal Commission into Family Violence: Full report.
https://www.rcfv.com.au/MediaLibraries/RCFamilyViolence/Reports/RCFV_Full_Report_Interactive.pdf
State of Victoria. (2018, January 24). Putting kids first: Evidence-based trials to improve safety [Media release]. https://www.premier.vic.gov.au/putting-kids-first-evidence-based-trials-to-improve-safety
State of Victoria. (2020, August 17). Keeping family violence in sight during coronavirus.
https://www.premier.vic.gov.au/keeping-family-violence-sight-during-coronavirus
Stylianou, A., & Ebright, E. (2021). Providing coordinated, immediate, trauma-focused, and interdisciplinary responses to children exposed to severe intimate partner violence: Assessing feasibility of a collaborative model. Journal of Interpersonal Violence, 36(5–6), 2773–2799.
https://doi.org/10.1177/0886260518769359
Sutherland, G., Rangi, M., King, T., Llewellyn, G., Kavanagh, A., & Vaughan, C. (2022). A socio-ecological exploration of adolescent violence in the home and young people with disability: The perceptions of mothers and practitioners (Research report, 19/2022). ANROWS.
https://www.anrows.org.au/publication/a-socio-ecological-exploration-of-adolescent-violence-in-the-home-and-young-people-with-disability-the-perceptions-of-mothers-and-practitioners
Thiara, R., & Humphreys, C. (2015). Absent presence: The ongoing impact of men’s violence on the mother–child relationship. Child & Family Social Work, 22(1), 137–145.
https://doi.org/10.1111/cfs.12210
Tucci, J., Mitchell, J., & Thomas, L. (2020). A lasting legacy: The impact of COVID-19 on children and parents. Australian Childhood Foundation.
Tucker, C. J., Finkelhor, D., & Turner, H. (2020). Family predictors of sibling versus peer victimization. Journal of Family Psychology, 34(2), 186–195. https:// doi.org/10.1037/fam0000592
Usher, K., Bhullar, N., Durkin, J., Gyamfi, N., & Jackson, D. (2020). Family violence and COVID‐19: Increased vulnerability and reduced options for support. International Journal of Mental Health Nursing, 29(4), 549–552. https://doi.org/10.1111/inm.12735
Usher, K., Bradbury-Jones, C., Bhullar, N., Durkin, J., Gyamfi, N., Fatema, S., & Jackson, D. (2021). COVID-19 and family violence: Is this a perfect storm? International Journal of Mental Health Nursing. https://doi.org/10.1111/inm.12876
VicHealth. (2020). Young people coping with coronavirus: Interim report.
https://www.vichealth.vic.gov.au/-/media/ResearchandEvidence/Young-people-coping-with-coronavirus.pdf
Victoria Police. (2017). Code of practice for the investigation of family violence (3rd ed.).
https://content.police.vic.gov.au/sites/default/files/2019-01/Code-of-Practice-for-the-Investigation-of-Family-Violence-Edition-3-V3-FINAL.pdf
Victorian Ombudsman. (2020). Investigation into the detention and treatment of public housing residents arising from a COVID-19 “hard lockdown” in July 2020. Victorian Ombudsman. https://www.ombudsman.vic.gov.au/our-impact/investigation-reports/investigation-into-the-detention-and-treatment-of-public-housing-residents-arising-from-a-covid-19-hard-lockdown-in-july-2020/
Walker, S., & Woerner, J. (2018). Adolescent sibling violence in Victoria. Melbourne, Australia. Crime Statistics Agency.
https://www.crimestatistics.vic.gov.au/sites/default/files/embridge_cache/emshare/original/public/2020/07/b8/3047e4ed5/Crime%20Statistics%20Agency%20-%20In%20Fact%208%20-%20Adolescent%20sibling%20violence.pdf
Warr, D. J. (2005). “It was fun … but we don’t usually talk about these things”: Analyzing sociable interaction in focus groups. Qualitative Inquiry, 11(2), 200–225.
https://doi.org/10.1177/1077800404273412
Wellmer, A. (2014). On critical theory. Social Research: An International Quarterly, 81(3), 705–733.
https://doi.org/10.1353/sor.2014.0045
Wilks, S., & Wise, S. (2012). Stopping adolescent violence in the home: An outcome evaluation of Breaking the Cycle. Anglicare Victoria.
Zhang, L., Cai, C., Wang, Z., Tao, M., Liu, X., & Craig, W. (2019). Adolescent-to-mother psychological aggression: The role of father violence and maternal parenting style. Child Abuse and Neglect, 98.
https://doi.org/10.1016/j.chiabu.2019.104229
APPENDIX A:
AVITH Collaborative Practice Framework: Multidisciplinary and
multi-system
Pillars
Understanding
- A shared recognition of AVITH as distinct from adult-perpetrated violence and which accounts for trauma, developmental stage and the function of used behaviours
- A shared understanding of key terms, such as “collaboration”, “whole-of-family”, “family violence risk” and “family safety” established across the system
- Clear understanding of roles and responsibilities at both a system level and individual
practice level
Coordination
- Processes and mechanisms are in place to support a coordinated risk approach, with clear accountability around the role of each service and practitioner, ideally with a practice lead holding the whole family in view. Coordination is led by a service with capacity to provide continuity, streamline service interactions and reduce overwhelm
- Services work together to sequence interventions appropriately and in a way that reflects family readiness and maximises the benefits of engagement
Workforce
- A highly specialised workforce which is supported to work flexibly (and intensively where
required) to meet the specific needs of families experiencing AVITH - System and organisational recognition that program resourcing must incorporate ample time for reflective practice and continuous learning
- Baseline capacity across the wider system to identify and support the management of AVITH-related risk, including through appropriate referrals and early intervention work
Evidence
- Practitioners incorporate evidence and learning into their daily practice, including through debriefing, reflective practice and collaborative practice networks
- AVITH responses draw on evidence and data – including the voices of young people and their families
– to inform service design, planning and continuous improvement - Government supports a system-wide approach to building and sharing evidence, piloting responses and taking effective interventions to scale
Principles
- Trauma- and family violence risk–informed: All practitioners and services involved adopt a holistic view of family violence risk and use of harm, recognising the impacts of prior and current adult-perpetrated violence and how these may be influencing current behaviours and relational dynamics, including trauma in caregivers. Practitioners maintain a lens on the impacts of trauma on child brain development, including language, meaning, emotional regulation and impulse control.
- Whole-of-family: Practitioners and services give full consideration to needs and histories across
- the family in assessing and managing risk. Opportunities to reduce AVITH-related risk may
- involve interventions with multiple family members where appropriate and safe, including where multidirectional use of violence is present or misidentification has occurred. Relational work is recognised as crucial to recovery, as well as playing a key role in adolescent identity formation and self-actualisation.
- Addressing barriers to engagement: Recognising the particular engagement challenges when working with young people and families experiencing AVITH, including prior experiences of under-servicing or over-servicing, services work flexibly and in a coordinated way, adopting relational approaches which leverage existing supports and therapeutic relationships around the family. Service contact is streamlined and scaffolded to reduce the burden on the family and young person.
- Flexible and needs-based: Young people and families receive a response which is tailored to their individual needs and goals. Practitioners and services are skilled, supported and flexible enough to respond to different AVITH presentations, including where the function of a young person’s behaviour is connected with disability and/or mental health needs. Responses take account of what a family identifies as their most immediate needs and reflects their readiness to engage at a given point in time.
- Intersectional and culturally safe: Services are equipped to respond to the intersecting and layered identities of families experiencing AVITH. This includes Aboriginal and Torres Strait Islander families, families from CALD backgrounds, LGBTQ+ families and young people, and families with a child with a disability. Cultural responsiveness is central to continuous learning and development, underpinned by strong relationships and consultation with culturally specific services. Services recognise and understand that individual family members will have different experiences, including where shared marginalisation may be a source of conflict.
- Service accountability: The roles, responsibilities and expertise of each practitioner or service involved in a family’s support are well understood, with the involvement of services determined by the family’s needs, preferences and readiness. Services are accountable and committed to working with the family to agree, plan for and progress their specific goals. Communication between services is proactive and transparent, with a particular focus on ensuring that dynamic risk information is shared and managed collectively.
Enables
Funding
- Program funding is adequate, consistent and flexible to enable long-term, whole-of-family work
Evidence-Informed Tools
- Robust and shared tools which are tailored to AVITH contexts are used to assess and plan
Culture
- Organisations foster a culture of collaboration, including within and across organisational boundaries
Service Capacity
- Capacity to meet demand and complexity across the system is actively monitored and adjusted as required
Continuous Learning
- Services are supported to adopt a structured approach to continuous learning and practice development
System Stewardship
- Government functions as an interface between systems, removing barriers to collaboration and responsive practice
Endnotes
- For a more detailed discussion about the literature regarding prevalence of AVITH, see “Context: An evolving service environment” Back to reference ↑
- Co-dysregulation” refers to a process in which the emotions of people in a close relationship are “bi-directionally linked and mutually amplifying, away from emotional stability” (Reed et al., 2015, p. 46). Back to reference ↑