
Research Report “Whatever it takes”: Access for women with disabilities to domestic and family violence services: Final report
Research report | July 2017
Issue 05 | 2017
Read the PDF version of the report
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
Acknowledgement of Country
ANROWS acknowledges the traditional owners of the land across Australia on which we work and live. We pay our respects to Aboriginal and Torres Strait Islander elders past, present and future; and we value Aboriginal and Torres Strait Islander history, culture and knowledge.
© ANROWS 2017
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW, 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
Whatever it takes? Access for women with disabilities to domestic and family violence services: Final report / Patsie Frawley, Sue Dyson, and Sally Robinson.
Sydney: ANROWS, c2017.
Pages ; 30 cm. (ANROWS Horizons, Issue 05/2017)
I. Victims of family violence – Australia. II. Women with disabilities – Services for – Australia. III. Domestic violence – Australia. IV. Abused women – Services for.
I. Dyson, Sue. II. Frawley, Patsie. III. Robinson, Sally.
ISSN: 2205-8907 (print) 2205-8923 (online)
ISBN: 978-1-925372-56-4 (print) 978-1-925372-57-1 (online)
Creative Commons Licence
Attribution Non-Commercial

CC BY-NC
This licence lets others distribute, remix and build upon the work, but only if it is for non-commercial purposes and they credit the original creator/s (and any other nominated parties). They do not have to license their Derivative Works on the same terms.
Version 3.0 (CC Australia ported licence): View CC BY-NC Australia Licence Deed | View CC BY-NC 3.0 Australia Legal Code
Version 4.0 (international licence): View CC BY-NC 4.0 Licence Deed | View CC BY-NC 4.0 Legal Code

Deakin University Australia
Geelong Waterfront, 1 Gheringhap Street, Geelong, Victoria 3220 Australia
“Whatever it takes”: Access for women with disabilities to domestic and family violence services: Final report
Prepared by:
Adjunct Associate Professor Sue Dyson, Principal Research Fellow, Australian Research Centre in Sex, Health, and Society, La Trobe University
Dr Patsie Frawley, Senior Lecturer in Disability and Inclusion, Deakin University
Dr Sally Robinson, Senior Research Fellow, Southern Cross University
The authors would like to acknowledge the work of Amie O’Shea, who was employed as a research assistant for the program. They would also like to acknowledge the work of the Consultative Research Group, advisory group, and research partners for their participation in the program and for their timely and important input. The authors would also like to acknowledge the women with disabilities who participated in the research in focus groups and interviews. Thank you for sharing your stories and experiences.
This work is part of the ANROWS Horizons series. ANROWS Horizons (research reports) are in-depth reports on empirical research produced under ANROWS’s research program.
This report addresses work covered in the ANROWS research project 3.4 “What does it take? Developing informed and effective tertiary responses to violence and abuse for women and girls with disabilities in Australia”. Please consult the ANROWS website for more information on this project. In addition to this report, ANROWS Landscapes and ANROWS Compass papers are available as part of this project.
Suggested citation:
Dyson, S., Frawley, P., & Robinson, S. (2017). “Whatever it takes”: Access for women with disabilities to domestic and domestic violence services: Research report (ANROWS Horizons, 05/2017). Sydney: ANROWS.
Contents
Tertiary responses to violence against women with disabilities
Effectiveness of tertiary response services for women with disabilities
Principles of good practice in tertiary response services for women with disabilities
Research and advisory structure
Women’s experiences using services
Specialist crisis response services
Improving response services for women with disabilities
Conclusions and recommendations
Project limitations and strengths
Appendix A: participant information and recruitment
Plain language statement: women with disabilities
Executive summary
Project aim
This research aimed to inform the development of guidelines for tertiary response services to respond effectively to the needs of women with disabilities.
Method
The mixed methods project surveyed tertiary women’s services in Australia to understand the models and approaches that are currently used to provide support to women with disabilities. Following this, five sites were recruited for qualitative research to develop a more nuanced picture of how the services work. Two of these were identified because they are specialist service models working specifically with women with disabilities and demonstrate promising practice. Case studies were developed to understand what could be learned from their approach. Three more sites were selected as case studies. A two-step process was used to select sites: (a) expression of interest by services in survey response, and (b) follow up discussions with these sites and short listing by researchers. Interviews were conducted with managers and staff; interviews and focus groups were conducted with women with disabilities; and two sites undertook a more comprehensive action research process to learn from the research and plan service improvement.
Data analysis
One hundred and thirty-eight valid responses were received to the survey. Data were analysed using SPSS Statistics V21 for basic statistical analysis, including frequencies of responses, cross tabulations, and descriptive statistics. An inductive approach was taken to analysis of the qualitative data, including interview, focus group, and action research data, which were analysed using QSR NVivo 10. Transcripts were closely read by each of the researchers. Initial themes and interpretations were reviewed by the research team (consisting of the three lead researchers from Deakin University, La Trobe University, and Southern Cross University) in telephone meetings and in a full-day workshop.
Findings
Accessibility requires more than physically modified accommodation or providing interpreters for people with sensory impairments. Access must be understood to include: how services think about disability (described as attitudinal factors), how information about services is made available, and going beyond the development of procedural access plans as required by the Disability Discrimination Act 1992 (Cth). Women with disabilities who participated in the research provided insights drawn from their experiences that suggest a need to extend the definition of “access” to include appropriateness, approachability, and acceptability as core components. By addressing broader issues of access in addition to disability-specific needs (such as the way information is provided to meet broad information access needs), the interface between what services offer and what women with disabilities need can be better aligned.
Many women who come to tertiary response services for support have disabilities. However, their disabilities may not be “officially” recognised for a variety of reasons: some have disabilities as a direct result of living with sustained violence and some are not easily identified because they are compounded by other life experiences. Tertiary response services are not experts in disability and meeting some women’s specific access needs can be challenging. A “clash of cultures” between tertiary response services and other services that support women with disabilities was identified that hampered collaboration. High-quality collaboration between tertiary response services and disability services can overcome some of the challenges identified.
At times, agencies providing services to women with disabilities who have experienced violence tended to act in ways that sought to “protect them” from further re-traumatising, which led to less rather than more access to supports and services. From the perspective of some of these women, the result was that they had been denied information, had not had their experience acknowledged, or had missed out on having contact with other women in similar positions to share experiences and get support. In the effort to protect women with disabilities, often their ideas and opinions about service improvements were not sought or heard.
Work undertaken in the case study sites in the action research phase demonstrated how service improvements and cross-sector collaboration could be incorporated into practice through reflection and facilitated planning processes. Rather than simply referring women with disabilities to disability services for support, a process of collaborating and engaging with disability services (rather than handing over to them) was developed. This established continuous improvement and cross-sector collaboration as underpinning principles for working with women with disabilities. Other key findings included that a one-size-fits-all approach does not meet all access needs; adequate time for counselling, case management, and consultation must be permitted to meet individual needs; and that women value relationships with workers that involve trust and taking as much time as is needed. Finally, many women seek social support from others who have had similar experiences.
Recommendations
At the time of completing this report, the Third Action Plan 2016-2019 of the National Plan to Reduce Violence against Women and their Children 2010-2022 (“Third Action Plan”) was released by the Commonwealth, state, and territory Governments (Department of Social Services, 2016). Women with disabilities are identified as a priority group in the Third Action Plan. This research supports the key national actions for women with disabilities identified in the Third Action Plan and contributes evidence to inform its implementation. A number of promising practices were identified from this research which can be articulated as underpinning principles for effective practice. These include:
- “Accessibility” is more than providing physical access: services must be approachable, acceptable, appropriate, affordable, and available to women with disabilities.
- Women with disabilities, like all people, experience complexity in their lives and are multi-dimensional; disability is in play with other personal and social factors. Service planning and delivery must be enhanced by the use of an intersectional lens.
- Women with disabilities need more than a focus on personal safety skills; they need social and relational support in a safe and inclusive environment.
- Service and practice planning, development, and improvement must be informed by high-quality data collection and qualitative and quantitative research. This must also be informed by the ideas and opinions of women with disabilities who have used the service.
- All aspects of tertiary response services for women with disabilities must be informed and enhanced by cross-sector collaboration.
Recommendation 1: promoting access and accessibility
Services should review their understanding of “disability” and “access” and draw on the evidence from this research and the work of Levesque et al. (2013) to ensure that they provide services that are:
- Approachable: women with disabilities know they exist and feel comfortable with approaching them.
- Acceptable and appropriate:barriers ton communication, housing, and understanding what is offered are removed.
- Affordable and available.
Recommendation 2: building cross-sector collaboration
In order to support initiatives for cross-sector collaboration, the emerging models of promising practice identified in this research should be further developed and informed using a facilitated process of reflection, consultation and engagement with other tertiary response services.
This process should aim to ensure positive outcomes for women with disabilities in all parts of the tertiary response sector through collaboration. It should not be in the form of didactic training, but use a facilitated process that involves and is informed by women with disabilities.
Recommendation 3: involving women with disabilities
Domestic and family violence (DFV) services should consider establishing peer support groups for women who survived or are escaping from violent and abusive relationships.
Service improvement and cross-sector collaboration must be informed by women with disabilities who have used tertiary response services. Women with disabilities should be consulted about their experiences using tertiary response services and their advice incorporated into planning and practice development.
The Consultative Research Group model, which ensured that the voices of women with disabilities informed this research, should be used in work with future sites to contribute to both service and sector-wide reform.
Recommendation 4: high-quality data collection
DFV services should collect data on the disability experiences of clients. Qualitative and quantitative data measures across all programs offered in DFV services should be developed and implemented, and tied to the same measurement and reporting metrics for other demographic characteristics (e.g. age, Indigenous status, and so on). Women with disabilities should be involved in providing qualitative data and be engaged to co-produce information from it that can be used in service improvement and wider sectoral reform at local, state or territory, and national levels.
Introduction
Gender-based violence is a problem of global proportions. Internationally, 30 percent of women have experienced physical or sexual intimate partner violence and 7 percent have been sexually assaulted by someone other than a partner (García-Moreno et al., 2013).[1] In Australia, the issue has been identified as a public health problem that is prevalent, serious, and preventable (Ayre, Lum On, Webster, Gourley, & Moon, 2016) and considerable work has been undertaken in recent decades to respond to and prevent intimate partner violence and sexual assault. Australian data demonstrates that “nearly one in three women over the age of 15 years have been subjected to physical violence and one in five report having experienced sexual violence at some time in their lives” (Australian Bureau of Statistics, 2012). What is less well understood is how women with disabilities fare in tertiary response services funded to provide safety and support for women escaping family violence.
Women with disabilities who have experienced violence seek help and support from tertiary response services for similar reasons that other women (or non-disabled women) do, including family and intimate partner abuse, sexual harassment and assault, coercive control, and stalking. However, women with disabilities also experience abuse related to their disabilities, including institutional violence, such as forced or coerced contraception, sterilisation, and psychiatric interventions; withholding of or forced medication; violations of privacy; deprivation of liberty; and denial of provision of essential care (Chenoweth, 1996; Dowse, Soldatic, Didi, van Toorn, & Frohmader, 2013; Frohmader, 2010).
Gender inequality is at the root of gender-based violence. However, violence against women is not limited to any particular group or class in society. Gender intersects with other forms of difference to compound discrimination, which in turn affects experiences of violence and abuse for individuals. The complexity of lived experience is very much dependent on factors such as age, class, culture, Indigenous status, intersex status, race, religion, sexuality, and so on, in addition to gender and disabilities. These factors also differ across time, according to geographic location, and are not the same for everyone. Taking account of these differences has been theorised as “intersectionality” (McCall, 2005). Understanding how these intersecting forms of difference affect access is particularly relevant for tertiary response services (Ortoleva & Lewis, 2012).
Between 2015 and 2016, the What does it take? research project was carried out to understand the ways in which services responding to the safety needs of women who have experienced family violence or sexual assault are accessible to women with disabilities. The project aimed to develop new knowledge to inform the development of guidelines for tertiary response services to respond effectively to the needs of women with disabilities in Australia. These guidelines aimed to be:
- based on a thorough and critical review of evidence concerning world best practice;
- informed by the experiences of Australian women with disabilities;
- developed in collaboration with locally based cross-sector communities of practice; and
- designed to inform a gendered understanding about violence in the disability sector.
This report details the findings of that research. It starts with a summary of international and Australian literature published in 2015 as an ANROWS state of knowledge report (Frawley, Dyson, Robinson, & Dixon, 2015). Following the summary literature review, this report details the project methodology, the qualitative and quantitative research findings, and concludes with discussion about the implications of this research for practice and for future research.
A note on language
This project sought to identify how women with disabilities who have experienced violence fare in tertiary response services. “Tertiary response services” is a broad term that encompasses a wide range of services aimed at ensuring safety and support after violence has occurred, including first responders, such as emergency and crisis services, as well as legal, health, and medical services. The scope of tertiary response services is detailed below in the literature review. The focus of the research has been on crisis response services, sometimes called domestic violence, sexual assault, or family violence services or women’s refuges. The Commonwealth funds these services under the National Partnership Agreement on Homelessness and they are administered by the states and territories.[2] There are some differences between states in terms of approaches and language used. For clarity, crisis response services responsible for ensuring women’s safe housing are referred to as “domestic or family violence response services” (shortened to DFV services). When the wider tertiary response system is implicated, the term “tertiary response services” is used.
Literature review
A literature review was carried out to establish the current state of knowledge concerning models of tertiary response services for women with disabilities who have experienced family or domestic violence or sexual abuse. Although literature reviews commonly focus on published, peer reviewed literature reported in high-quality academic journals, a comprehensive search of such databases revealed limited results to answer the following literature search questions:
- What models and approaches have been used in Australia and internationally for tertiary responses to violence and abuse for women with disabilities?
- What does the evidence say about effective models?
Although academic research was limited, many community, advocacy, and activist reports and monographs were found. As a result, this “grey literature” was included in the review, as it offered a rich source of evidence concerning the literature search questions. Therefore, in this review we have drawn on both academic and grey literature from sources we judged to be reliable.[3]
Disability research
Around one in five people in Australia report having a disability (Australian Bureau of Statistics, 2011). Of these, almost 6 percent have a severe or profound level of disability. Definitions of “disability” differ, although increasingly the World Health Organization’s (WHO) International classification of functioning, disability, and health’s (ICF) “bio-psycho-social” definitions are used (World Health Organization, 2011a).[4] Drawing on the ICF, disability can be understood as complex, dynamic, multi-dimensional, and contested (WHO, 2011a). The ICF asserts that the experience of disability should be mainstreamed and that it should be recognised as a universal human experience, as all humans can experience “a decrement in health and thereby experience some disability” (WHO, 2011a, p. 3). This multi-dimensional, “mainstreamed” definition of disability is informed by critical theorising about disability and the grassroots advocacy of people with disabilities over at least the past three decades.
Despite the high rates of violence and abuse reported in the international peer-reviewed and local grey literature, research about effective prevention and response is lacking (Lund, 2011; Mikton, Maguire, & Shakespeare, 2014). The WHO advocates an approach to violence against women that is based on a public health model of disease prevention. This model has been adopted by the Commonwealth of Australia and underpins its responses to the prevention of violence against women.
In this three level model, primary prevention aims to prevent violence from occurring through attitude and behaviour change; secondary responses provide early intervention (e.g. with perpetrators), and tertiary responses ensure safety and support for women after violence has occurred. In addition to responding to the immediate safety and support needs of women who have been affected by violence, tertiary responses also aim to minimise the impact of violence and prevent ongoing negative consequences and repeat events (Flood, 2011; Martin et al., 2009; World Health Organization, 2002). Each of these approaches is more complex than this explanation,; however the focus of this review is on tertiary responses and thus we go into no further detail about primary prevention or secondary responses.
The public health model of prevention is central to the Australian Government’s National Plan to Reduce Violence against Women and their Children 2010-2022 (National Council to Reduce Violence against Women and their Children, 2009; Council of Australian Governments, 2012). A significant body of primary prevention, and evidence-based knowledge and practice has been developed as a result of this plan (COAG, 2012). However, there is less evidence available concerning the most effective and appropriate immediate tertiary responses needed for women who have experienced violence, for both the general population and minority groups, including women with disabilities (Healey, Humphreys, & Howe, 2013).
To be effective, immediate tertiary interventions require a rapid, coordinated response that ideally encompasses the range of services needed by victims/survivors. In the immediate term, this may include policing, medical care for physical injuries, safety planning, advocacy, legal services, and family or domestic violence response services. In the medium to longer term, this includes services such as trauma counselling, support groups, employment assistance, transitional housing, children’s services, and specialist support and advocacy services.
Women with disabilities experience issues with accessing sexual assault and domestic violence services (Dowse et al., 2013; Healey et al., 2013; Healey, Howe, Humphreys, Jennings, & Julian, 2008; Woodlock et al., 2014). In the disability sector, lack of awareness about family violence and other forms of violence against women compounds the problem of access to safety and support for women with disabilities (Mikton & Shakespeare, 2014). It has been argued that despite the public health approach to understanding disability and a rights-based approach to promoting equality to prevent violence against women, to date, there has been little attention paid to the intersection of the two fields of disability and domestic and family violence (Mikton et al., 2014).
Tertiary responses to violence against women with disabilities
International and domestic anti-discrimination legislation requires all community services and facilities to be “accessible”, with standards and guidelines that articulate what this means in given situations (Australian Human Rights Commission, n.d.). People with disabilities should not experience discrimination or exclusion due to their experience of disability. Australia’s disability discrimination legislation provides the legal framework for equality for people with disabilities and for addressing discrimination. It also includes provisions for providers to argue that they cannot meet these legislative responsibilities because of “unjustifiable hardship”. This means that while the expectation is one of “universal access”, the reality is that access is frequently limited or non-existent as a result of weighing up the costs and barriers to providing access (Frawley et al., 2015).
Access for people with different experiences of disability is complex and multidimensional. To understand access requires an understanding of how disability is experienced and how the experience of disability is impacted by intersecting forms of difference. Despite this, there is an ideal of universal access that has been developed, particularly in relation to the built environment. Guidelines for physical access in building standards have been established and, in some countries, anti-discrimination legislation dictates the legal framework for determining what “access” means. In the United States, research has been undertaken on the extent to which domestic violence and sexual assault services comply with access legislation and has found considerable variability in physical accessibility (Chang et al., 2003; Frantz, Carey, & Bryen, 2006). Frantz et al. (2006) reported that while 87 percent of services in their survey said that they were able to provide services to all clients with disabilities who requested them, all fell short of actually doing so. Similarly, a study in the United Kingdom found that 76 percent of domestic violence services surveyed did not comply with the Equality Act 2010 (UK) (Hague, Thiara, & Mullender, 2011). Those researchers noted that disability access had been narrowly defined as “wheelchair access” in some services.
Tertiary response services are always under pressure from the sheer numbers of women requiring services and from limited (and diminishing) funding. Research with service managers found that (a lack of) funding and the need to prioritise budget expenditure to support physical access were key barriers to developing fully accessible services (Chang et al., 2003; Frantz et al., 2006; Healey et al., 2013; McClain, 2011).
Access and inclusion
In Australia, the disability advocacy sector and the domestic violence sector collaborated to develop a resource for tertiary response services to facilitate access for women with disabilities (People with Disabilities Australia & Domestic Violence NSW, 2015). This resource calls for existing services to go beyond the procedural requirements of the Disability Discrimination Act 1992 (Cth). The authors argue that no single change will make services more accessible and that specialist accommodation, programs, and supports targeted at women with disabilities need to be developed. The report has a significant focus on organisational change and readiness, highlighting the need for organisation-wide training that is underpinned by inclusive policies, and further argues that services must look broadly at what “access” means. Practical guidance on addressing physical access, information access, attitudinal access, and procedural access is incorporated in the resource. Similarly, Women with Disabilities Australia (WWDA) call for a broader human rights approach to recognising and responding to violence and abuse (WWDA, 2013). A human rights approach, they argue, acknowledges the need to address social structures that create barriers to equality and therefore have an impact on the incidence, prevalence, and severity of abuse and on approaches to preventing and responding to violence and abuse for women with disabilities in Australia.
The term “programmatic access” has been used in research and policy to cover all aspects of service responses that relate to working with women with disabilities. This covers approaches used from intake through to counselling and outreach, and includes service policies and staff training (Frantz et al., 2006). Frohmader, Dowse, and Didi (2015) argue that programmatic access should incorporate both procedural and attitudinal components. Frantz et al. (2006) tested programmatic access in their research and reported that only 57 percent of services asked at intake if people required accessible accommodation or adaptations to the way services were provided.
Chang et al. (2003) found that while the vast majority of organisations reported that they provided services for women with disabilities, many had difficulty providing “full services” (meaning all aspects of the service that other women could use). Notably, only partial access to outreach and counselling was reported. In a UK study by Hague et al. (2011), only 38 percent of domestic violence organisations were able to provide an accessible service (with physical access being used as the measure of access). Provision of accessible transport and accommodation was the focus of these services.
Staff training and organisational policy to address skills and attitudes to access and inclusion were reported in the literature as key factors in addressing programmatic access, yet not all services provided such training or had these policies. In one study, staff members’ lack of knowledge and understanding about the needs of women with disabilities led to feelings of trepidation, anxiety, and concern when faced with providing services to women with disabilities (Hague et al., 2011). Frantz et al. (2006) found that while over a third of services reported having training for staff and volunteers, only 9 percent had training for board members. Despite the call for staff training, no studies were found that assessed the outcomes of training or policy on practice. In Australia, Healey et al. (2013; Healey, 2015) argued that services lack a focus on inclusion policies for women with disabilities.
Recognising and responding to the breadth of needs and experiences of women with disabilities who experience violence and abuse can present challenges for service providers. Research in the United States that investigated the experiences of women with disabilities who accessed tertiary response services found that women with an intellectual disability and those with mental illness were the most represented groups (Chang et al., 2003; Frantz et al., 2006). Both of these studies reported that women with significant communication disabilities (including those with hearing impairments), women who used augmented communication devices, and women with other communication needs associated with speech and learning represented a small number of overall clients. For these women, barriers included lack of access to staff with specialist skills to support effective communication, or staff members’ lack of knowledge about how to engage with women with significant communication disabilities. Cost was cited as a barrier to accessing specialist communication supports and services for these women (Chang et al., 2003).
The reported incidence of violence and abuse of women with disabilities is likely to be lower than the actual incidence as a result of a number of complex factors to do with reporting and data collection (Dowse, Soldatic, Spangaro, & van Toorn, 2016; Dowse et al., 2013; Hughes, Lund, Gabrielli, Powers, & Curry, 2011; Jones et al., 2012; Lund, 2011; Mikton et al., 2014). In Australia, Healey et al. (2013) found a lack of policies and standards concerning data collection about disabilities by family violence services. This lack of data collection keeps disability invisible in services, hiding the need for services to address physical and programmatic access for women with disabilities.
The evaluation of the Safer and Stronger Program violence prevention program in the United States reported that women with disabilities were more likely to first reach out to someone they know and trust, such as a friend or a family member, rather than a domestic violence service (Powers et al., 2009). This is consistent with reports by women more broadly, as reported, for example, in the ABS Personal Safety Survey (ABS, 2012). Participants that faced multiple types of abuse, such as physical, sexual, and emotional abuse, were more likely to have sought education and knowledge about abuse compared to those with little or no experiences of abuse.
Collaborations and partnerships
Cross-sector collaborations between the disability and domestic violence sectors were highlighted as an important factor for more effective outcomes for women with disabilities in much of the literature (Chang et al., 2003; Healey et al., 2008; McClain, 2011). Despite this, cross-sector collaboration is reported to be low. A survey of UK disability and domestic violence services found that only 6 percent of the disability services surveyed had attended locally provided, multi-agency, domestic violence training (Hague et al., 2011). Similarly, research in the United States that studied interagency collaboration in the provision of domestic violence services to women with disabilities found that, despite agencies believing they collaborated well, women with disabilities reported frustration and anger at what they saw as a total lack of collaboration (McClain, 2011).
Effective service delivery for women with disabilities requires that both the disability and the DFV response sectors should focus on and prioritise responses to violence against women with disabilities. In Canada, a survey of 579 disability centres found that very few provided staff training about domestic violence or advocated for improved access to these services (Ballan & Freyer, 2012). In the United Kingdom, a study of interagency collaboration found that while agencies had strategies in place that included cross-training and cross-referral systems, as well as policies and funded activities to bring the sectors together, where interagency collaboration existed, it was difficult to sustain (McClain, 2011).
In the United States, collaborative efforts to improve services for women with disabilities have helped to change the ways in which services interact both with women with disabilities and with each other (Smith & Harrell, 2011). The key factors for effectiveness were identified as: the environment in which the collaboration exists, its purpose, the characteristics of the organisations and people involved, the process and structure of the collaborators’ work, the quality and frequency of their communication, and the resources available. Similarly, in Australia, Women with Disabilities Australia, through the Stop the Violence project, developed a resource compendium that recommended adopting a human rights approach that consists of the following principles: empowerment through participation, removing barriers, working in partnership, building capacity, building and using an evidence base, preventing violence before it occurs, and promoting leadership and advocacy. (WWDA, n.d.). These are supported by a number of strategies, such as providing appropriate accessibility, ensuring transferable and open communication, creating inclusivity and equality for all stakeholders, and guaranteeing that clear accountabilities are agreed upon before program development and implementation (Dowse et al., 2013).
Sexual assault services in Victoria have focused on providing services for people with disabilities who are victims or survivors of sexual violence for almost 2 decades, with cross-sector collaboration including staff training in both sectors being a key component (Frawley, 1997, 2000). One service, South Eastern Centre Against Sexual Assault (SECASA), developed the Making Rights Reality program, with support from the Federation of Community Legal Services, the Office of the Public Advocate, Victoria Police, Springvale Monash Legal Service, and Women with Disabilities Victoria (Frawley, 2014). This program provides enhanced legal advocacy and counselling services to victims/survivors with cognitive impairments.
Making Rights Reality addresses cross-sector collaboration in a number of ways: through disability training for sexual assault service staff, by engaging with the disability sector to develop Easy English resources about sexual assault, and through involvement of the disability project worker on advisory groups for projects involving women with disabilities. Evaluation of the program indicated that 40 percent of referrals to the program came from disability organisations and the police (Frawley, 2014). The number of people with disabilities using SECASA increased over the 2-year period of the pilot project, and clients received access to Victims of Crime Compensation through the legal advocacy component of the program (Frawley, 2014).
Effectiveness of tertiary response services for women with disabilities
“Effectiveness” can be defined as the degree to which something is successful in producing a desired result. To provide effective tertiary response services for women with disabilities who have experienced violence, first clarity is needed about which results are desired. A search of the academic literature reveals that very little is known about how effective tertiary response services are for women with disabilities. A systematic review of effective interventions to prevent and respond to violence against persons with disabilities reported that there remains a dearth of literature on the effectiveness of interventions and that most evaluations are not rigorously executed (Mikton, Maguire, & Shakespeare, 2014). According to these authors, this makes it difficult for policy-makers and practitioners to make informed decisions about which model and approach would be the most effective.
One of the key themes of the literature review was that women with disabilities who had experienced high levels of abuse across a number of different areas dealt with safety-promoting behaviours very differently to those who had experienced little or no abuse. What became apparent is that just as experiences of violence and abuse are different for each person, so too are the personal responses and needs for each person. Some women require more integrated levels of support and service provision, while others require more preventative levels of support (Powers et al., 2009).
Evaluation of an Australian program called A Safety Awareness Program for Women with Disabilities (ASAP) found that overall the program was effective on a number of qualitative measures (Hughes et al., 2011), including:
- ASAP was effective in educating women with disabilities at risk of abuse, as well as those who had already experienced abuse.
- The program engaged women who had previously experienced abuse and violence and found that those who had experienced the most abuse were more likely to have greater gains in safety self-efficacy after completing ASAP.
- Participation in the program greatly improved the protective factors for women with disabilities.
- Participants responded positively to the classes and found the learning materials to be engaging and effective at helping them learn safety-promoting behaviours.
- The program was regarded as being easily accessible, relevant to, and feasible for participants (Robinson-Whelen et al., 2014).
ASAP is an education program rather than an immediate support service. There are, however, some lessons that can be learned from such a program for the development of guidelines for tertiary response services for women with disabilities, in particular the approach used to make information accessible.
A key factor that is noted in the broader literature is the importance of interagency collaboration. The literature that addresses the question of effectiveness also notes the importance of interagency collaboration and highlights the importance of this collaboration being supported by a broader authorising environment for prevention and intervention (such as support from the national and state governments). This can be accomplished by improving responses to services for women with disabilities in abusive and violent situations, such as enhancing crisis response services that are specifically designed for women with disabilities and for their children if required (Woodlock et al., 2014). One of the most crucial aspects of a successful program is the expertise of staff (Babic, 2009; Hague et al., 2011; Hughes et al., 2011).
A study of service collaboration in the United States reported that little research had focused on how effectiveness is understood or measured in tertiary response services (McClain, 2011). This suggests there is a gap in the research about what characterises and determines effectiveness of tertiary response services from the perspective of women with disabilities (McClain, 2011). The following actions were recommended to ensure effective interagency collaboration:
- Employ an outside facilitator who can broker communication and agreement between service providers and women with disabilities. This can be achieved by laying down the foundations of what the collaboration is trying to achieve; sharing philosophies; building common definitions of “abuse”, “domestic violence”, “disability”, and “accessibility”; and clarifying expectations of women with disabilities.
- Develop awareness in the community and train staff in DFV services and disability services on the intersections of gender, violence, and disability.
- Develop policies, procedures, and budgets that specifically include the provision of services to women with disabilities who are victims/survivors of domestic violence/sexual assault.
- Create welcoming environments for victims/survivors with disabilities (McClain, 2011).
Principles of good practice in tertiary response services for women with disabilities
The literature review sought to identify tertiary response approaches for providing services to women with disabilities, and gain an understanding of how these approaches have been implemented (process) and the extent to which they are effective (outcomes). While the review resulted in some insights about factors that need to be considered in developing services that are responsive to the needs of women with disabilities, very few actual models of tertiary responses were identified. As a result, the review was better able to identify principles of good practice rather than complete models. Three key factors stand out as important for effective tertiary response services: physical and programmatic accessibility, cross-sector collaboration, and evidence-based practices. Two reports in the literature provided key approaches to addressing these factors.
Healey et al. (2013) developed guidelines to assess the inclusiveness of domestic violence standards that are based on current understandings about best practice, which include:
- Use the voices of women with disabilities to inform policy and practice.
- Collect disability data.
- Provide evidence that the service meets physical access standards (of all disabilities), as well as programmatic access though use of accessible information and approaches, in order to be eligible for funding.
- Provide evidence-based and rigorously-reviewed therapeutic and educational services.
- Engage in cross-sector collaborations.
- Be based on an intersectional, human rights framework.
- Underpin the services’ programs, approaches, and workforce development with these principles.
The Stop the Violence project in Australia proposed the following principles that need to underpin practice to prevent violence in the broader community, in disability services, and to inform DFV service responses:
- Adopt a human rights approach.
- Promote empowerment through participation.
- Remove barriers.
- Work in partnership.
- Build capacity.
- Build and use the evidence base.
- Prevent violence before it occurs.
- Promote leadership and advocacy.
- Provide appropriate accessibility.
- Ensure transferable and open communication.
- Create inclusivity and equality for all stakeholders.
- Guarantee that clear accountabilities are agreed upon before program development and implementation (Dowse et al., 2013)
Discussion
A key finding of this review is that effective, accessible services for women with disabilities must be built on multi-agency collaborations. Research in the United States suggests that collaboration must be based on having a clear purpose understood by all parties and developed within an environment conducive to the active and productive engagement of all parties. Other factors include the quality and frequency of communication and the existence of supportive resources (Smith & Harrell, 2011). Added to this, tertiary response services must engage women with disabilities as partners in the planning and strategic stages of service development, as they are the experts in their own lives and contribute a crucial perspective on appropriate services and support needs for women with disabilities (Healey et al., 2013). Effective collaborations must also be well-managed, and this requires substantial efforts from affiliated agencies and stakeholders that are not driven by financial gain or funding obligations but by a genuine desire to challenge existing barriers and make firm cultural and community change. Well-functioning collaborations must address access issues relating to multiple disabilities and intersectional characteristics (Dowse et al., 2013).
Some researchers advocate that educating women with disabilities on the behaviours that constitute gender-based violence and how to escape if it happens will increase their access to tertiary response services (e.g., Powers et al., 2009). However, current research is unable to identify whether there is a link between increased knowledge and an increase in reporting abuse.
High-quality data collection processes must be based on a well-developed understanding of disability, intersectionality, and accessibility so that women with disabilities using the service can shape responses. These data must in turn be analysed and used in the development of policies and practices that take account of the needs and experiences of women with disabilities, as well as informing systemic and individual advocacy processes.
A central tenet of effective tertiary response services for women with disabilities concerns empowerment and the need for those who use services to exercise agency in all aspects of the service experience. The perspectives of women with disabilities must increasingly inform both disability and tertiary response service delivery (Frawley, Barrett, & Dyson, 2012; Powers, Curry, Oschwald, & Maley, 2002; Robinson, 2013).
Research questions
Based on the findings of the state of knowledge report summarised above (Frawley et al., 2015), this project was designed to answer the following research questions:
- How do women with disabilities in Australia experience tertiary responses to violence and abuse? What can these experiences tell us about good practice in mainstream and specialist services?
- In what ways can tertiary responses be improved to deliver effective services for women with disabilities based on the knowledge developed from this research?
Methodology
This mixed methods project was underpinned by the principle of social inclusion for people with disabilities, as well as an understanding of intersectionality (discussed on page 6). To ensure the voices of women with disabilities were at the forefront of informing the findings, principles of participatory, inclusive research were drawn on. These methods are somewhat conventional in participatory feminist and disability research and are based on acknowledging power differentials between the researchers and research participants. Two key approaches were used to ensure the research was able to draw on and privilege the experiential knowledge of women with disabilities. The first was the development of a research advisory role for women with disabilities whose voices we perceived to be “harder to hear” — the Consultative Research Group. The second was maintaining a commitment to conducting interviews and focus groups with women with disabilities rather than their proxies, despite this being difficult as a result of “gatekeeping”.[5]
The methodological approach aimed to eliminate barriers to participation in the research by women with disabilities as far as possible and ensure the participants’ experiences of seeking and receiving responses to violence and abuse were heard. The research project aimed to capture inclusive and intersectional data based on the principle of “nothing about us without us”, which is the foundation of inclusive research with people with disabilities.
Research and advisory structure
A multi-level research and advisory structure and a range of communication processes were created and implemented to complement and enrich the project as it developed and to ensure a reflexive approach was built into the study. These included:
- Early in the life of the project, the research team recognised the potential for women with intellectual disabilities, dual disabilities, and complex communication needs to be marginalised. A Consultative Research Group made up of women with these disabilities was formed to provide advice to the research team. Their advice and input was used to shape the research approach, support recruitment, and gain insight to support analysis. This group will also assist with disseminating the research findings. Membership and participation in this group was negotiated with individual members as part of the research ethics of this project. The group met six times between October 2015 and September 2016 with two members of the research team and a counsellor with expertise in working with women with disabilities who have experienced sexual assault, who attended in a support role.
- Regular fortnightly telephone conferences between the research team, as well as biannual face-to-face meetings. The aim of these meetings was to share information, solve problems, and reflect on the research process as it developed.
- Quarterly face-to-face meetings between the research team and the research partners (representatives from Women with Disabilities Victoria and the Centres Against Sexual Assault [CASA] forum). The aim of these meetings was to strengthen the research focus of the study by drawing on the expertise of the research partners in research, policy advocacy, and practice. A partnership agreement was developed between the research team and the research partners early in the life of the project.
- Quarterly meetings (face-to-face or teleconference, depending on the location of the participants) between the research team, the research partners and a research advisory group (representatives from advocacy, policy, and practice organisations with a stake in this research, including PWDA, DVNSW, Australian Women Against Violence Alliance, and Advocacy for Inclusion [ACT]). The role of the research advisory group was to advise the researchers on access to and engagement with the sector, provide advice and information on key policy and practice issues that could impact the study, and to support the dissemination of information about the project and its findings. A terms of reference agreement underpinned the relationship between the research team, the research partners, and the research advisory group.
Research methods
A mixed-methods approach was used to capture the complexity of the field and ensure the voices of women with disabilities were heard in the research. This involved:
- A survey of DFV services in Australia
- Selection of three case study sites for qualitative research and inclusion of two specialist service case studies.
- Interviews and focus groups with the managers and staff in the three selected case study sites.
- Interviews and focus groups with women with disabilities who had used DFV services.
- Action research cycles within the case study sites (n = 2). The action research groups included representatives from the case study sites, women with disabilities, and broader representation from disability and DFV services in the geographic areas of the case study sites. The aim of the action research group meetings was to: present research findings, contribute to analysis of the data collected, and plan and implement locally based approaches to address identified gaps in services.
Recruitment, sampling, and the research process for each aspect of the research is detailed below. Ethics approval for the conduct of this research was granted by the Deakin University Human Ethics Committee. Although the identity of the services surveyed and the case study sites was known to the research team, all participating services were guaranteed anonymity and are therefore not named in any part of this report, other than to identify the state-location of the service. All individual research participants were informed about their rights and guaranteed anonymity. An example of a participant information statement (approved by the Deakin University Human Ethics Committee) is included in Appendix A.
Figure 1 Summary of research participation from all sources.
Data Source Number Survey of DFV services 138 Women with disabilities: interviews and focus groups 34 Managers in DFV and disability services 5 Staff members and associates in DFV services 31
Survey
The main purpose of the survey was to identify and recruit three case study sites for the qualitative phase of the research. In addition, the survey sought to understand ways in which DFV services in Australia respond to the needs of women with disabilities and how they address access and inclusion. An online survey was developed by the research team and piloted with the service representatives of the research advisory group prior to its distribution. The survey included a number of open-ended questions, as well as multiple choice and multiple response questions. The survey asked questions about:
- the kinds of access (if any) that services provided for women with disabilities;
- how services established whether a woman had disability or support needs;
- barriers to providing accessible services;
- modifications made to improve accessibility;
- policies that addressed disability;
- disability awareness training for workers; and,
- cross-sector tertiary response and disability services collaboration.
Over 300 sexual assault and DFV services were invited via email to participate in the survey. Email addresses were identified through an online search that included several databases, such as the 1800RESPECT service and Australian Government–funded service lists. All members of the ANROWS Practitioner Engagement Group were also emailed a link to the survey with a request to distribute it within their networks.
A total of 165 service representatives started the survey After incomplete or ineligible data were cleaned, 138 completed surveys were returned. The valid response rate was approximately 33 percent. Services in Victoria were most likely to participate, followed by New South Wales Services in the Northern Territory were least likely to participate in the survey. There was a good representation of services from regional, rural, suburban, and urban areas.
Although the main purpose of the survey was to identify case study sites, the survey findings included both qualitative (responses to open-ended questions) and quantitative findings that contributed to answering the research questions. As a result, the survey findings are integrated into the findings from the case studies and action research cycles throughout this report, and identified as such when this occurs. Descriptive statistical analysis of the quantitative data from the survey was completed using SPSS Statistics V21 and a thematic analysis of the qualitative data was completed using NVivo 10.
Case study sites
As discussed above, the main purpose of the survey was to identify potential sites for the case study research. Respondents were asked at the end of the survey to indicate their interest in participating as a case study site in the next stage of the project. Interest was indicated by 40 survey respondents, who were asked to identify the name and contact details of their agency. A shortlist of potential case study sites was developed by reviewing the nominated agencies’ websites. Criteria for selection was then identified based on responses to some of the survey questions and the research team reviewed the possible sites based on the extent to which they met the criteria for promising practice. These included that services had:
- adapted their services for physical and programmatic access;
- identified women with disabilities as a target group in their practice; and
- described their engagement with cross-sector collaboration.
A priority list of 12 services that met the criteria was identified. The first three services (in Northern Territory, Queensland, and Victoria) were approached and invited to participate; however, each of these declined the invitation, so approaches were made to the next three preferred services on the shortlist. The final site selection resulted in the participation of three services, one in a major city in South Australia, one in a regional city in Victoria, and one in a regional city in New South Wales. The aim of this qualitative phase of the research was threefold:
- to understand how services respond to the needs of women with disabilities from the perspectives of staff and managers;
- to understand how women with disabilities experience the services provided to them; and
- to bring together local, cross-sector agencies to promote and support the research locally, develop local action plans, and contribute to knowledge exchange.
Case study sites agreed to participate in interviews and focus groups with managers and staff, to assist with recruiting women with disabilities who had used the services for focus groups and interviews, and to participate in the action research phase of the project. Each of these are described below. Despite the expressed desire to participate in the research, from the outset there were some challenges to data collection in the sites due in part to workload demands.
Interviews and focus groups
Managers and staff
A condition of acceptance of the invitation to become a case study site was that service managers would make themselves available for interviews and would recruit staff to participate in a focus group. Women’s DFV services are busy places dealing with complex problems, and even after accepting our invitation to be a case study site, negotiating access that did not add unnecessarily to staff members’ workloads proved challenging. The researchers made every effort to fit in with the needs and timelines of the services, but, in some cases, this meant data collection was delayed.
Women with disabilities
At each case study site, the researchers aimed to recruit up to ten women with different experiences of disability to participate in interviews, focus groups, or both. To be included, participants had to be: women with disabilities who had used the service, able to communicate with the researchers, and able to give consent for participation in the study.
The case study sites agreed to assist with recruitment of women with disabilities for this phase of the research, which presented another challenge. Often women who are current users of DFV services have recently experienced violence and abuse and many live in fear. Services are protective of the women in their care and fear re-traumatising them. Women who are out of danger and living in secure accommodation may no longer be engaged with the service; indeed, they may want nothing to do with a service that reminds them of trauma. Additionally, services may not have follow-up information about women who have left the service, and the ongoing pressure of new referrals militates against follow-up. These factors meant that not all case study sites were able to put the research team in touch with the number of women with disabilities originally anticipated.
This meant that the researchers had to be resourceful in order to recruit women who were willing to participate and who would not be harmed in the process. Some women who met the inclusion criteria were recruited through disability services to participate in interviews and focus groups. In one case, a group of women in a disability service who had not used DFV services but who had concerns about their own safety in relationships agreed to participate in a focus group.
At one site, only one woman with a disability was recruited through the case study site (three others who were invited refused to participate). In the interviews with managers and staff, it became clear that they had an important partnership with a local disability support service, so permission was sought from the case study site manager to approach the disability service to recruit women. With their agreement the disability support service was approached and agreed to recruit women who met the inclusion criteria for interviews.
Women from the Consultative Research Group (discussed on page 16) also agreed to participate in a focus group. This group consisted of five women with intellectual disabilities and complex communication needs, the majority of whom had used DFV services in the past. They were also experienced self-advocates, knowledgeable about issues concerning violence against women with disabilities.
Across the three case study sites, two disability support services, one specialist service, and the Consultative Research Group, 28 women with disabilities participated in interviews or focus groups.
Action research cycles
After the qualitative data collection and analysis phase, the project planned to bring together representatives from each case study site and its local community, including women with disabilities, to present the research findings and to facilitate a process in which gaps between the services’ and women’s perspectives could be discussed. The aim of this process was to assist services to collaborate with other local stakeholders to modify existing approaches or develop new models based on the findings from the research. The outcome would be action plans based on the learnings from the project.
This plan also met with challenges and the approach had to be flexible to fit in with the participants. At one site, no action research cycle occurred because changes in staff and workload pressures prevented the service from participating after the qualitative data collection phase was completed. To address this, and with the permission of the case study site manager, a local disability service to which the case study site referred women with disabilities was recruited. The manager of the disability service was interviewed and assisted with the recruitment of women with disabilities who had used a DFV service for interviews. We will arrange further meetings with the case study site and disability service to report on the study findings and, if desired, facilitate further work if and when they are ready to re-engage.
Profiles of each of the case study sites at the time they were recruited are detailed next. Further details about the process and outcomes of the action research cycles are detailed on page 38.
Case study site profiles
In this section, we provide profiles of the three case study sites where data were collected. Case study sites were promised anonymity, so, for ethical reasons, other than the state where the service is located, identifying information is not included. All three of these services were DFV crisis response services with some adaptations for women with disabilities.
New South Wales
The New South Wales site is a large, multi-program service located in a small regional city. The service provides a range of family support services to the town and surrounding local area. Its stated aim is to “help people in need”. In addition to DFV responses, the service also provides children’s and homelessness services and financial counselling. The women’s and children’s services have operated for some decades and have purpose-built facilities. These include secure, crisis accommodation, and transitional properties that can be used by women, women with children, men, men with children, and larger families. The service provides limited services to women with disabilities, responding to women who are referred to them or who incidentally come to the service, but not actively promoting the service to them. It does not have a specific focus on supporting women with disabilities or families that include women with disabilities.
Building from a social justice foundation, the service has a history of increasingly professionalised services that focus on the support of families. The current focus on family support is evident in the underpinning service principles, which focus on capacity building and empowerment of families.
South Australia
The South Australian site is a medium-sized, geographically defined, urban service located in a metropolitan region, which has operated for some decades. It is an independent, domestic violence service run by a board of management. It incorporates two sites, with one that specifically works with Aboriginal women and children. Both sites offer secure accommodation and outreach services. These sites offer crisis accommodation, case management, and a range of counselling and support for women to be safe in the short-term and to achieve long-term stability free from violence. The service belongs to a number of community networks in the region that link community organisations working to prevent violence through community education, service collaboration, and innovative approaches to support women and children who have experienced violence.
The service describes itself as woman-centred using a feminist approach. The Aboriginal service also incorporates an in-depth understanding and respect for Indigenous cultures. These principles incorporate respect, empowerment, equity, inclusiveness, and belief in women and children’s stories. They include that:
- violence against women is a crime that denies their human rights;
- all women and children should live in a safe and secure place; and
- Aboriginal and Torres Strait Islanders are the First People of Australia and have a special connection to country that needs to be supported.
Women with disabilities access the full range of services, and physical access has been addressed in the secure accommodation services. One unit in the mainstream service has been developed to be accessible for women with physical disabilities, and all units at the Aboriginal service address physical access needs. The organisation has engaged a woman with a disability as a consultant at different times to advise on access for women with disabilities.
Victoria
The Victorian site is part of a large, statewide, independent child and family welfare service that has been in existence for over 100 years. The branch where the research was carried out is in a large, regional city. This multi-service agency covers family violence, child and youth services, residential care, education, and employment, and does not have a disability support component. The agency identifies people with a disability as an element of their service-user population and although the youth area has specialist disability services, the family violence service does not. They do, however, have a strong focus on partnership with relevant external organisations and refer women with disabilities who have particular support needs to local disability services for assistance. The focus of the family violence service is immediate response to “high risk women and their children”.
Specialist response services
In addition to the three case study sites discussed above, two specialist services were included as case studies. In the original project proposal, these two services were identified as case study sites because they were the only specialist violence and abuse response services in Australia for people with disabilities. After consultation on the project proposal, it was decided that it was more feasible to recruit generic services as one group of case studies and deal with these specialist service models separately, as their service approaches were very different to the generic services. One of these organisations provides a specialist service to people with disabilities who have experienced sexual assault alongside their generic service; the other is a specialist women-with-disabilities service. Descriptions of these two sites are included in the section that discusses the findings from the case study site action research cycles on page 44.
Findings
The findings of this research are reported against the aims that have driven the project and the research questions. The aims were to develop promising practice guidelines for effective tertiary responses to gendered violence for women and girls with disabilities in Australia that are:
- Informed by the experiences of women with disabilities.
- Based on a thorough and critical review of existing models.
- Developed in collaboration with locally based, cross-sector communities of practice.
- Based on an understanding about gendered violence in the disability sector.
Throughout this report the findings are informed by quantitative and qualitative data from the survey and qualitative data from the three case study sites. This project was not an evaluation of each site but an attempt to understand the ways in which models and approaches have been used in Australia and to identify principles for good practice. In the findings section, the data from the survey, interviews, and focus groups are integrated and data courses are clearly identified.
Understanding disability
In the survey, participants were asked how they identified or defined whether a “woman has a disability”. Many services rely on women to “self-identify as prompted by questions on intake form”. Others reported that they identify disabilities “through exploration and questions asked to the woman and one-on-one counselling”. One participant responded:
…ask as part of our assessment if the person has any disabilities. The client or their carer will usually let us know that the person has a disability and the nature of the disability. They define it for us. (Survey participant)
From interviews and focus groups in the case study sites, a more complex picture of “disability” emerged. Women who seek help from DFV services may have officially recognised disabilities (e.g. through “diagnosis”, receiving a disability pension, or having a carer). They may also have “observable disabilities” that require support or assistive equipment. Women in this latter category may or may not self-identify as disabled. Disabilities may be related to the violence experienced and may or may not be permanent.
While the research participants identified a range of understandings of disability, the understanding used by the researchers draws on the following definition:
Disabilities is an umbrella term, covering impairments, activity limitations, and participation restrictions. An impairment is a problem in body function or structure; an activity limitation is a difficulty encountered by an individual in executing a task or action; while a participation restriction is a problem experienced by an individual in involvement in life situations. Disability is thus not just a health problem. It is a complex phenomenon, reflecting the interaction between features of a person’s body and features of the society in which he or she lives. Overcoming the difficulties faced by people with disabilities requires interventions to remove environmental and social barriers…Evidence suggests that people with disabilities face barriers in accessing the services they need in many settings. (World Health Organization, 2011b)
For workers in DFV services, the experience of identifying and responding to functional disability is an everyday experience; women they see may have experienced sustained violence and have acquired brain injuries (ABI), mental health issues, or be self-medicating with alcohol or other drugs as a result of living with violence. When a woman first arrives at a DFV service, this can make the task of providing appropriate access a complex task. A worker in a focus group in Victoria explained:
…it’s hard to know—is this a disability that she has, or is it a mental health issue, or trauma—and often there’s no formal diagnosis one way or another. So it’s hard to know what you’re dealing with.
Staff in the New South Wales site described the challenges they face when working with women who appear to have cognitive impairments:
Worker 1: It’s when that falls on that borderline…
Worker 2: [Someone] who’s already suffering trauma from domestic violence, it’s really hard to gauge…
Worker 1: Yep. So I feel, you know, that’s where it becomes really grey and really tricky. And I think the other thing in my experience is with women particularly that have a mild intellectual disability; it’s obvious to me, but it’s not obvious to them, so they don’t see themselves with an intellectual disability. They just see themselves as…with domestic violence it affects them a lot.
When meeting a woman who is escaping violence, the priority is to help her obtain safe, secure accommodation. Disability is only one of a complex set of needs that the intake worker must attend to in the process of meeting these needs. To understand the ways that this plays out, the research team investigated how workers established whether a woman has a disability.
Identifying disability
The most common approach to identifying disabilities was a reliance on the woman to self-define whether or not she has disabilities, usually during intake procedures. Some services had specific questions on intake forms to establish disability status; others decided for themselves based on intake interviews or counselling. If a woman presents with support or mobility equipment, with a carer, self-identifies as disabled, or is referred by another agency that identifies her as having a disability, then her disability status is determined and acknowledged by the service. In these cases, services understand their duty of care is to ensure access needs are catered for. Some services approached disability from the perspective of potential “barriers”, for example:
[We] ask the person at initial contact if there are any barriers…there [are] a range of specific assessment questions in regards to mental health, physical disabilities, or difficulties in communicating. (Survey)
Others explained that this information can come from a variety of sources:
Often someone in the person’s life has identified that the person has an intellectual disability, or someone self-identifies. Otherwise, we have discussion with people about whether they have difficulty with certain things or ask about whether they are on a DSP [Disability Support Pension]. (Survey)
Another explained:
[We see people with] mental health disabilities, spina bifida, deaf, brain injuries, women who are assaulted about the head would be likely to sustain a brain injury, but many would go unrecognised or assessed. However, we would identify that this is a “hidden” disability for many of our clients. (Survey)
The case study sites had similar approaches to defining whether or not a woman (or her children) has support needs related to disability. Once it is known (through self-disclosure or referral) that a woman has been “officially” identified as having a disability, the service is able to make arrangements to meet her needs.
Identifying whether a woman has a disability is complicated by the fear many women have about disclosing their disabilities. This fear emerged from interviews with women in each site, with one woman noting that she had never disclosed her disability in the past. It was also recognised by the workers:
Women with disabilities are often very frightened to talk about their disabilities because they think it’s going to reflect on her parenting capacity, and they worry about how they will be perceived by Child Protection and Family Law. So that’s another conflict area. And for us, I suppose it puts more pressure on us to then be—as well as doing family violence, trying to advocate on her parenting capacity, even though we might not see her all the time, or know the full extent of how she’s disabled (Workers focus group, Vic).
Women who are not connected with disability services and do not have established disability supports in place present a challenge for services to make effective referrals and get adequate additional support in place for them. Workers at the South Australian site explained:
[A] lot of women that come here haven’t connected with any disability service before…when they come, often they haven’t even got a Medicare card or a key card, let alone, like, filled in a great big application for Disability SA or [disability assistance] so yeah, it’s not very often they come connected to those services already. (Workers focus group, SA)
This was also reported as an issue for children who workers suspected may have disabilities:
There’s been children that—and not that I’m making the [disability] assessment, you know, we cannot assess, but there’s definitely been some—it’s been later discovered or the assessments have happened but families haven’t been connected to kindergartens or childcare or schools, and so assessments haven’t occurred but there is clearly some issues. (Workers focus group, SA)
In each of the case study sites, workers faced similar challenges. Women with diagnosed disabilities who are registered with disability services are eligible for a range of disability supports through disability support services. When they meet a woman whose disability is not officially identified, she generally does not have easy access to disability supports and services. This is compounded by the bureaucracy involved in getting official recognition. The South Australian site noted that this was particularly the case for Aboriginal women at their service, and related to the transient lifestyles of many women escaping violence.
The case study sites were clear that they wanted to improve their services for women with disabilities. This was particularly related to an understanding about the high incidence of violence against women with disabilities that was not reflected in their services:
Because it isn’t our area of expertise. And not that we want to become the experts. We just want to improve…how we reach those women that aren’t being serviced that we know are out there. I guess that’s my million-dollar question: how do we get to those women that we know are being abused? (NSW manager)
Similar sentiments came up at the South Australian site:
So when you’ve got all these women out there—they’re suffering DV—that don’t have a third party service or a disability service. They’re probably never getting to us. We wouldn’t…they won’t pick up the phone because they can’t. He’s probably sitting next to them. So there’d be all these women out there that probably aren’t even getting to us. (SA manager)
For DFV services, these two groups of women with disabilities (those who are officially identified as having disabilities and those who are identified by the service but do not self-identify as disabled) present different challenges. Most services have some adaptations to accommodate women with physical disabilities: most frequently adapting one unit with wide doors, accessible bathrooms, ramps, and emergency call buttons. Far less frequent were adaptations to support women with cognition, sensory, or memory impairments.
DFV services described taking a “whatever it takes” approach to ensuring the safety of women escaping violence, and the flexibility of this approach helps women with disability in many instances. However, for services, the most challenging and difficult-to-resolve cases are those where a woman’s disabilities are not officially recognised. This is where high-quality collaboration between disability support services and DFV services is critical. DFV services did not, for the most part, demonstrate knowledge about disability supports that disability services can provide and relied on disability services to assist women to access disability supports, services, and benefits. In cases where women are not connected with disability services, when they access a DFV service will not always be a priority for DFV services to seek out support from disability services. Addressing this issue in particular presents an opportunity for substantial improvement in the lives of women with disabilities who have experienced violence and abuse.
Models and approaches
In the survey, four options for types of service responses for women with disabilities were included: “limited services”, “generic services with adaptations”, “both special and generic services with adaptations”, and “no specialist services”. As depicted in Figure 2, 18 percent of the total number of participants that answered the question (n = 138) chose the fourth option. 37 percent offered generic services with adaptations, 20 percent offered limited special services, and 24 percent offered specialist and generic services with adaptations.
Service adaptations
Survey respondents were asked to describe the ways in which their services had been adapted to ensure they were inclusive for women with disabilities. The most generic services they identified were: changes to processes and procedures, making buildings accessible, adapting resources (including using large print or pictures or both), developing disability action plans, providing interpreter services, and employing workers who are skilled in disability services.
Some indicated that they had purpose-built facilities, for example, “crisis accommodation [that is] wheelchair friendly”. Many others provided support and training for women with disabilities, some with specially trained workers:
…we have worker[s] that are trained in specific specialist fields so that we can cover all areas of speciality like, such as—youth—dv—disability—mental health—families—prison.
Some offered disability employment services or healthy relationship education for people with intellectual disabilities. One service responded that they provided:
Intensive case management to assist women and their children with a disability to remain safely in their own home, including comprehensive risk assessment and safety plan, needs assessment, and case plan.
Survey respondents were asked to describe the ways in which their services had been adapted for women with disabilities. Responses related changes to processes and procedures, making buildings accessible, adapting resources (including using large print or pictures or both), developing disability action plans, providing interpreter services, and employing workers who are skilled in disability services. Reponses included the following:
Adapted rooms and more space if in wheelchairs or on crutches. If disability is mentally based, then access to a carer on site.
Family Violence counselling and group work service provided with adaptations as required e.g. phone counselling or support people engaged.
Medical and counselling services for people who have been sexually assaulted and have a disability—disability access, disability beds, staff trained in the area of disability, intervention models that include therapeutic care teams (so working with other key carers etc.).
Outreach services, adapted transitional housing properties to assist women with disabilities, partnership with a local disability service to respond together.
In response to an open-ended question about barriers to inclusive service provision, respondents distinguished between physical access and appropriate services, such as specialist workers, communication aides, and carers. It is clear that services want to be accessible, but still see it as an add-on rather than a set of principles upon which the service operates on a day-to-day basis. One service drew attention to the lack of appropriate physical access:
Our high security women’s refuge has no access for full-size wheel chairs. We are able to accommodate children with wheelchairs when accompanying their mother…Our office/counselling room facility has a wheelchair ramp but no full chair accessible toilet. We endeavour to bring in supports for women regarding other types of disabilities such as hearing or intellectual.
Other services indicated that stairs and multi-level buildings limited access or that they were inadequately funded to respond to the needs of women with disabilities. For example, one noted “[our] website is not accessible (i.e. no audio format info)”. Others also explained:
In refuge we do not have disability access due to funding not provided to create the necessary alterations to the units.
Housing is a huge barrier, as often these women live with their carers, so, in a time of crisis, if there are no disability units available, it is difficult to get accommodation which is disability friendly.
Women with communication disabilities were poorly serviced, as one respondent noted: “No resources for a hearing-impaired client in a face-to-face interview…or reading material for the visually impaired”. This service also noted that they had “no current disability action plan/disability audit”. These limitations and barriers were noted repeatedly by survey respondents. No survey respondents noted any contact with women with communication boards or speech technologies.
Figure 2 Service types
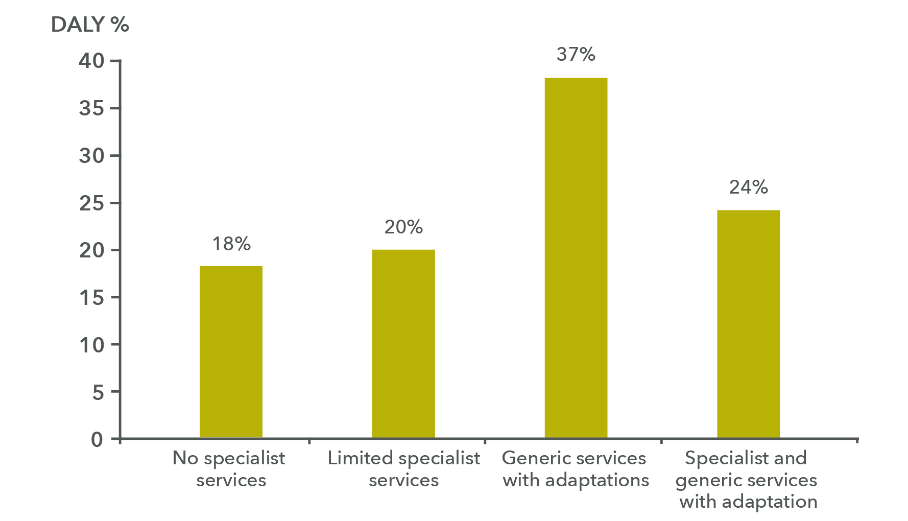
Data table for Figure 2
Service type DALY % No specialist services 18% Limited specialist services 20% Generic services with adaptations 37% Specialist and generic advices with adaptation 24%
Another issue identified was a lack of workers with specialist skills to support women with disabilities, including workers who were trained to support women with disabilities, and training for all refuge and housing support workers in working with women with intellectual disabilities or mental health disabilities.
Each of the three case study site’s response to access was “generic with adaptations”. For the most part, these adaptations concerned adjusting the service to meet the specific needs of each person by collaborating with disability services. In some cases, this collaboration was limited to referral; in others it also involved ongoing engagement.
Collaboration and referral
For DFV workers, referral or collaboration with disability services is important to ensuring the needs of women with disabilities are met. Sixteen survey respondents indicated that they referred women with disabilities to other agencies. Only two respondents identified the importance of the relationship between their service and the disability service to which they referred women with disabilities. One explained: “We speak directly to the service and try to go along with [the] person to support [clients] to connect with the new service (if appropriate)”.
In the case study sites, the most common form of service adaptation was collaboration with, and referral to, disability support services. For example, a disability consultant engaged with the South Australian site explained: “We identify our limitations: think, reflect, and ask who else we need at the table.” This site reported that they had recognised the need to respond to disability as a result of two key factors. First, seeing women with disabilities and thinking about their access needs in relation to the accommodation services. Second, awareness that there was a disconnect between the number of women with disabilities in the population and the numbers they were seeing in their service:
I think we recognised in conversations with others in the disability sector…how can we be more responsive? Because if we look at the number of women that experience disability of one form or another, be it identified or non-identified, we wouldn’t be getting a lot of those women into our service. (SA manager)
When collaboration with disability services does not function well, DFV workers needed to take on the role of advocate for women with disabilities:
I’ve worked with disability clients before, but you know, that’s—it’s not something that comes formally with family violence…we sort of just find ourselves advocating and falling into that role as part of it. Because no one else will. (SA manager)
Like the South Australian site, the Victorian site relied on collaboration with a local disability support service, as the service manager described. “They will actually come on board. You know, if we need some carers or what have you, we don’t have the capacity to do that” (Vic. manager).
A feature of the “whatever it takes” approach used in each of the three sites is an individualised, creative approach to ensuring that women receive appropriate support. A worker at the Victorian site explained how this worked with the disability support service with which they collaborate:
…there’s no after-hours support for women who have disabilities, and who need accommodation, need safety stuff. There’s no one out there, no after-hours disability number. So we’ve worked out our own system with [the local disability service] now through [our manager] meeting with them. If we accommodate someone who has a disability who needs a worker, they’ll organise the worker. (Workers focus group, Vic)
The South Australian site’s work is also underpinned by a community partnership approach. The manager described how a collaborative approach with a local disability service helped to deal with a challenging situation:
We had…a young woman came in, was in a wheelchair, had slight intellectual disability…[Her partner] was extremely abusive and there’d been some serious incidents. So we were able to work with [the disability service] and they were able to get her out. (SA manager)
The manager explained that the woman’s disabilities prevented her from being able to reach her alarm button when she was in bed and went on to explain how their collaboration with the disability service had worked:
We were able to get a different type of [mobile] alarm system in. [The disability service] were fantastic in putting carers in place because they had those links so we had around-the-clock carers because of course he’s out of the picture…she needs that support, meals, all of that. That co-working together, that belief in each other and that learning…we’ve built those relationships with one service. (SA manager)
The manager qualified this comment about building a relationship with a specific disability service: “We’ve had some real challenges with other disability services”.
In the past, the Victorian service had the assistance of a disability advocate. They emphasised that this was not a regular occurrence, but had been very helpful:
…having a disability advocate who can help navigate through the system. Joint case management with specialist disability services, where we can come in and help with the family violence side, and they can help the holistic other aspects. (Workers focus group, Vic.)
The Victorian workers focus group drew attention to a $7000 fund that is available for disability crisis support. The disability advocate knew how to access these funds:
That worker…was a sort of conduit. She understood the disability service system, so she could help us find the right way. The problem was that they had a quite narrow definition of disability. So we had to have disability as according to DHS criteria. (Workers focus group, Vic.)
While this was useful, they also noted that the cost would only cover some women with complex needs for a short period:
What didn’t work is, as a crisis service, you might spend the seven grand in two or three nights. Then you’re moving her to the case work, and DHS going, “You spent the money already”, so that’s difficult. (Workers focus group, Vic.)
DFV workers need to be creative and “think outside the box” to ensure women with disabilities receive appropriate supports. They are not resourced specifically to address the disability support needs of women and it is only collaboration that ensures women’s safety. For disability support, DFV services are dependent on “outside support which sometimes isn’t always available” (workers focus group, Vic.).
For women whose lives are transient, which is often the case for many who experience family violence, particularly Aboriginal women, making and keeping links with disability services can be challenging:
The transient nature of a lot of the women’s lives and the crisis that’s happening in communities and whatever means it’s really important to try and link in, so you’re hoping that, even if they do move on, you may have been able to establish some link with another service, [particularly] for the children. (SA manager)
This was described as a “culture clash” between the domestic violence services’ “woman-centred practice” and disability services’ “protective approach” (SA manager). A woman-centred approach acknowledges women as experts in their own lives with the capacity to make choices. This was discussed in a staff focus group:
Our difference is our focus is on empowering women to be independent. It doesn’t matter who you are, where you come from, what’s your language, [they have a right] to be independent, to feel safe, secure…you know, they’re adults; they have a right to choose. Especially…being a victim, normally they never had a voice to choose or to speak out or to have, you know, input in any decision-making. We don’t want to take them here as well. We want them to feel like, I’m a free woman; I’m an independent person. (Aboriginal service worker, SA)
The workers went on to explain how this position conflicted with that of a disability service:
There was a girl here for a long time…and our team leader, she just fought and fought and advocated constantly for this client…around housing…you know, finding her appropriate housing…supported housing, you know? And there were real clashes with other services about, you know, with negotiations about her needs being met kind of thing…Supported independence…in a property on her own, a little flat, but, you know, with support. (Workers focus group, SA)
The conflict continued, with the disability services arguing that the client could not take care of herself even as she started to develop her own sense of independence:
They’re saying to her [what you’re doing] is not enough…and when she started to make her own lists they’d say, what do you mean you want? We will tell you what you can have…They wouldn’t even let her…she wanted a Coke, she couldn’t have a Coke…then they controlled her. (Workers focus group, SA)
They went on:
There were a number of clashes with the woman, they were insensitive, you know, dominating…judgemental…yeah, very, judgemental and looking down upon…It’s very problematic for people dealing with Aboriginal people because they’re over—they’re sick of people telling them what to do. (Workers focus group, SA)
The staff responsible continued to advocate for the woman:
Our team leader kept saying, “Hey come on, she can do this stuff; engage with her”. You know, it’s about showing her how to do stuff, encouraging her to do stuff, engaging, but, you know, unfortunately the workers that were coming in weren’t interested in engaging with her. They wanted to…clock their 2 hours, get in, get out, you know, and that wasn’t meeting her needs. (Workers focus group, SA)
The staff in the Aboriginal service related other similarly disturbing conflicts between their service encouraging women to be agents of their own destiny and disability services controlling and limiting Aboriginal women’s agency. They also described how, when cross-sector collaboration did not work, this added to their workload: “it’s ten calls to make one thing happen…To and fro just to get one thing done”.
At the Victorian site, workers identified similar problems where their service and disability service cultures clashed to the detriment of women with disabilities. In one case, although a client lived in the regional city where she sought help, her disability case management was handled in Melbourne.
We had a lady and her daughter, who had multiple disabilities. Huge issues. And they were case-managed in Melbourne, and it took us what, at least 2, 3 weeks to work out how it all worked. And who to ring and who to contact. (Workers focus group, Vic)
In many cases it is the complexity of the life of the woman with disabilities (which might include alcohol or other drug issues, mental health, physical health, intellectual disabilities, and the disability pension and support service systems) that is most challenging:
It can be quite confusing at times about what services do this, different packages. It depends on the disability levels, depending on what disability help they get. I find that very hard to navigate for myself, let alone the lady that’s in the situation or the child that’s in the situation. (Vic. manager)
Some women supported by the case study services were facing serious problems, such as having children removed from their care. Supporting these women included negotiating with a range of different government departments and within the judicial system. Family violence workers needed to take on a range of issues because of their commitment to ensuring women’s safety:
Quite often we’re drug and alcohol workers, quite often we’re mental health workers. I don’t have skills in those areas. But—but often when there’s one with the lot, as we call it—one with multiple complex issues—we find that drug and alcohol won’t get involved because she hasn’t dealt with her family violence issues. Or you find that mental health won’t get involved because she hasn’t dealt with her drug and alcohol and her family violence issues. (Workers focus group, Vic.)
The findings in the section highlight the importance of resourced, high-quality, cross-sector collaboration to ensure true access for women with disabilities to the range of services and supports they need to live in secure accommodation free from violence and abuse. It also shows that there is a great deal of room for improvement across sectors if this is to be achieved.
Access and accessibility
Fundamental to this research is the concept of access for women with disabilities and, conversely, what makes services accessible. The literature review (see page 8) found recommendations for services to be made as accessible as possible: for access to go beyond the physical to include information, attitudinal and procedural access, and to go beyond what is required by the Disability Discrimination Act 1992 (Cth). Programmatic access is called for from intake through to counselling and outreach that should incorporate both procedural and attitudinal components. These recommendations expressly identify the things that are needed to make a service accessible for people with disabilities. However, the literature does not make clear what it is that makes a service accessible to all in the first place. Here, we do not argue that the modifications and adaptations recommended in the literature are incorrect, rather that there are some fundamental structural and philosophical issues that lie at the core of accessibility that precede modification and adaptation of existing programs.
According to Levesque, Harris, and Russell (2013), access is central to the performance of services. Whilst Levesque et al.’s work focuses mainly on health care services, it is equally relevant to tertiary response services; accordingly, here we adapt Levesque’s model to focus on tertiary response services.
Dictionary definitions of “access” address it as “the means or opportunity to approach or enter a place” (Oxford Dictionaries, n.d.). Access to a service refers to opportunity or ease with which people in need of a service are able to obtain and use those parts of the service that are appropriate to meet their needs. For Levesque et al. (2013), access is the interface between an individual or household’s social and physical environment and the characteristics of the service. They draw a distinction between “access” and “accessibility” as follows:
- “Access” is being able to enter or obtain services: for example, “I have access to…”
- “Accessibility” describes the nature of services, how they are designed, and what opportunities are provided for people who need the service to obtain them: “It is useable to me”.
Where there is a mismatch between what is available and what is needed, there is a barrier to access. Levesque (et al.(2013) identify five dimensions of accessibility. To be accessible, services must be:
- approachable;
- acceptable;
- available;
- affordable; and
- appropriate.
If all of these features are not in place, then a service is not accessible. Thus, adapting or adding disability modifications to a service that is not fundamentally accessible is unlikely to create access. Each of the five dimensions mentioned above must be in place before minor modifications are made.
Most of the services participating in this research only had wheelchair access and usually only in one unit. If a woman with complex disabilities wants to access a tertiary response service and the service does not understand the range of her needs, or if it is not acceptable or affordable to her, then adding communication aids does not necessarily make the service accessible. It may address one of her needs, but not all of her needs.
Women with disabilities’ insights about access
In focus groups and interviews, women with disabilities expressed a number of ideas about how services could be made more accessible to them. Although many of the women have complex social, physical, and mental health issues that are challenging for many services, their ideas for improving service access were straightforward and match the model presented by Levesque et al.(2013) discussed above. Following Levesque, the women’s ideas about access will be discussed under these sub-headings: approachable access, acceptable access, and appropriate access. Affordability and availability of services were not strong themes in the women’s interviews and focus groups so are not covered here. The main issue relating to affordability and availability access is housing, which is an important issue to address in future research.
Approachable access
In the Levesque et al. (2013) model, the starting point for approachability is that those in need of a particular service know that it exists, how it can be reached, and that it can help them. Knowing that a service exists and what it offers is thus the first step to accessibility. Elements such as transparency, information about available services, and outreach can make services more approachable. In interviews and focus groups, women had ideas about matters that made it difficult for them to engage with tertiary response services. For some, the idea of asking for help from the police was frightening:
They’d be shaking…because the police, they’re all tough and they’ve got guns and walkie-talkies and so they’d be scared. But when they’re in the room, like one-on-one, like, they’re not scary, but it’s getting in there. (Women’s focus group, NSW)
When asked about how approaching the police could be made less scary, a woman explained:
Just have a smiling face, like, when they walk in, like, say “hello” back, and then they’re alright…and be happy… they can have a cup of tea, and sit there and talk to them and explain it to them. (Women’s focus group, NSW)
Women also mentioned the importance of being able to speak to other women about experiences of violence, rather than having to tell their stories to men.
Speaking about tertiary response services in the broader sense, another woman made a plea for patience and understanding:
You have to be nice to those customers, or, umm, you have to be able to deal with, you know, what comes out…they have to have the right words to tell, like they have to say it properly. (Women’s focus group, SA)
To be approachable, services need to address matters of quality, adequacy, co-ordination, and continuity (Levesque et al., 2013).
Acceptable access
Acceptable access is about the professional culture in organisations that facilitates or impedes the ability of women with disabilities to seek help. The “culture clashes” between services (discussed above) affect access, as do clashes between women’s personal and social values, culture, and sense of autonomy and that of the service from which she is seeking help.
When a service expects a woman with disabilities who has experienced violence to fit into its culture and has expectations that are in direct conflict with her own needs, this can have major implications for access. For example, one woman explained how her needs were not met by the disability service she sought help from:
People with disabilities are each individual; I think people think they are all the same but they are not. And they need to do higher supports; if that means someone needs more support or a different way or whatever. At the start I just wanted to go away. I didn’t want to be here, to have people know where I was. But there was no funding or support for that. And that’s what I needed, just time to get my own head into [a] place where I could cope with what was going on. And he had people going past my house, and things like that so I just needed to be out of my house. Time out and time away but they wouldn’t do that…but it’s about helping me with the budget to try and get time out, to do time away, if that’s what I needed. (Interview, Vic).
In disability services, women want to feel safe. If services remain silent about the possibilities of violence and fail to provide appropriate information and education on the matter, women with disabilities’ access to acceptable support is limited. One woman explained:
…get a better place for girls with disabilities where they can go if they don’t feel safe or something like that…with lounges, umm, people to talk to…(Women’s focus group, NSW)
This draws attention to the ways in which services limit choices by “protecting” women with disabilities from information and from each other. The women identified protectionism as a problem.
In other tertiary response services, confidentiality and privacy were matters of concern. Two women spoke about how unacceptable it was for them to have to speak about their private business in the foyer. For them, it was more reassuring to discuss their business in spaces that were private and comfortable. For others it was knowing their rights:
I think the client needs to know their rights, and a lot of the time they’re not told of their rights. When you go in there [DV service/refuge], you’re not told what your rights are or what services are available, like [advocacy] and all your different things. If you have an appeal process. (Women’s focus group, SA)
Acceptable access to tertiary response services for women with disabilities who have experienced violence can be achieved when services are flexible in the way they respond to women, understand the challenges women face when they seek help, and value their rights to information, knowledge, and autonomy. To be acceptably accessible, all tertiary response services must start from this position.
Appropriate access
Appropriate access is about the fit between the service and the client’s need. It is about the time spent on understanding what the individual needs and planning appropriate responses. It is also about the technical and interpersonal qualities of the service (Levesque et al., 2013). For the service-user, it is about their ability to engage with the service. This includes women feeling empowered and in control of their own future. This is enshrined in a woman-centred approach, but may not always be achieved for women with disabilities.
In this research, women with disabilities showed a great desire for services to provide accessible information in digestible forms, such as easy-read booklets placed strategically where women could pick them up and read them at leisure: “like a booklet, with all of it, then she can go for a walk and go through it with the girls [workers]”. Central to this provision of more information was having enough time to take in the information gradually without feeling rushed, overwhelmed, or confused. Effective communication skills were also seen as important in services: “meeting in person, not on the phone” was mentioned as something that would help them and others to feel more comfortable.
For women with disabilities, appropriate access can also be addressed through having workers who are knowledgeable about disability. In a focus group, the following exchange took place:
Woman 1: Well, shouldn’t they have workers that have training in disability?…There should be.
Woman 2: Yeah, there definitely should be [suggestion by interviewer that women with disabilities be involved in this]…Yes, definitely. (Women’s focus group, SA).
For women with disabilities, the lack of knowledge and understanding about tertiary response services for those not in the system was also mentioned as a way of providing appropriate access:
I think by getting out there and promoting themselves in organisations. I think there needs more awareness for women with disabilities themselves. That these services are…exist for them. They are not only for people, women, without disabilities. And I think that’s part of the problem. (Women’s focus group, SA)
The Consultative Research Group had a range of suggestions about how to improve accessibility. Importantly, they called for services to recognise that “every woman with a disability is different—[there is] no one thing that will work for everyone”. They argued that “It’s about communication and support and advocacy”. For these women, independence and autonomy are vital; they talked about “hard won independence” and wanting to have the right to learn from their own mistakes without people saying “I told you so”.
The findings in this section on access suggest that to ensure tertiary response services are as accessible as possible for women with disabilities, services can make relatively minor changes by taking into account women’s needs and hearing from the women about their experience of using the service. Through addressing broader issues of access in addition to disability-specific needs, the interface between what the service offers and what women with disabilities need can be better aligned.
Women’s experiences using services
In this section we turn to the findings concerning women’s experiences using DFV services. As discussed in the methodology section, because of the difficulty experienced in recruiting women with disabilities who had used the case study services to participate in interviews or focus groups, women were recruited from a wider range of sites. As a result, this section includes data from women who had used the case study sites; women from disability services who had experienced sexual assault, domestic violence, and other experiences of violence and had used some support services to address the violence; and women from disability services who had not experienced abuse but had concerns about their personal safety. Two distinct groups emerged: women who knew about and had used a range of services (n = 18) and women who had no knowledge about DFV services or what to do if they were a victim of abuse (n = 5).
Women’s knowledge about family violence services
In this section, we first discuss women with disabilities’ knowledge (and lack of knowledge) about DFV services. We then turn to the women’s positive and negative experiences with DFV, disability, and other services to identify features of effective services and service systems, which includes relationships, practical support, service co-ordination, and collaboration.
Established family violence service–users
Participants in the case study sites were asked in interviews about their experiences with DFV services. Women who were established family violence service–users (n = 18) often had multiple, complex problems related to their disabilities and the social, mental, and physical effects of experiencing family violence. The DFV service was part of the fabric of their lives, and when the relationship with their worker or the service in general worked well they were full of praise. When asked what was the best thing about the service, one woman referred to her worker:
She was great; she took me to appointments, made sure I was safe in the house, spoke with my estate agents. Followed up to make sure everything went well. Does that frequently; she’s great. Everything they’ve done has been top notch. (Interview, Vic.)
Many of the women who were established service-users were embedded in a web of systems in addition to the case study site and did not necessarily separate these, providing insight into the complexity of their lives. When services worked well together or when one worker emerged as a strong advocate for a woman across systems, women were grateful and felt empowered. When the system did not work well, it could be disastrous. A woman who had used a family violence service and was recruited through a disability service told the interviewer:
They wanted me to get an intervention order, but I wasn’t ready. So instead of spending the time to get me ready, they just said “We’re going to close your case,” and it took probably another 2 months maybe to get to the point where I was OK to do the first order. Nervous as hell because he was living with me, so it was nerve-racking trying to do that and not for him to know that that’s what I was in the process of doing. So I got the first order, went to court and they pretty much didn’t stay with me or anything. (Interview, Vic.)
When they had no knowledge about how to get help prior to being referred to the DFV service, many of the women had lived with violence for sustained periods of time. One woman had found help through Lifeline:
I didn’t know, and I was too scared to open my mouth, because I didn’t want no one to get into trouble the one who was abusing me. So it took me over 30 years to open my mouth. And I actually rang up Lifeline. So I got a number from Lifeline and they were starting a loss and grief [program for people with disabilities]. And I rang up, and I spoke to this nice man, he was a social worker. And he—he was the one suggested—when I first seen him…And it—it took me months to agree for him to bring me here [to the case study service. (Women’s focus group, SA)
The theme about a prior lack of knowledge about DFV services was common. Women came to services as a result of a sense of desperation or through a referral from the police, other counselling services, doctors, or disability services. In another group, responding to the question, “How do women with disabilities find out about DV services?”, one woman said, “You don’t…but if you are at a disability service and you have the courage to tell someone they might help”. An Aboriginal woman at the South Australian site described her life of violence at the hands of her father and partners. Even though she had tried to get help, she had been unsuccessful until:
I finally got a phone call from [an Aboriginal women’s shelter in another town]. And they said that they had a vacancy there. So when I came back down, after all that, then I finally got my house, and I moved in. I’m starting to get things… (Women’s focus group, SA)
She went on to explain that later, she had returned to her family and the violence had started again:
Then my dad almost married me off to about a busload of blokes, ’cause they were all my right skin. So I took off from there too…And then after everything happened and everything started building up, and I didn’t have anybody to talk to, then I had a bit of whatsaname [a breakdown], so I left my kids with my mum, and I took off up to my step-mum up in [a remote town]. And I ended up with a traditional man, and then he bashed me every day. (Women’s focus group, SA)
After a series of violent relationships, she tried again to get help:
Well, I just ended up ringing up Crisis Care. So when I got down here, that’s when I rang up; [they said] “we need to call the DV mob, we can get you help now”. But these mob [Aboriginal refuge service] lately—these mob have been a lot more helpful. (Women’s focus group, SA)
The theme of lacking knowledge about how to get help highlights the lack of information sources and education available to women with disabilities. Constrained by fear and a lack of information, they often live with abuse until the situation reaches breaking point and the police become involved.
Women who have not used DFV services
Women who were recruited through disability services and had not used DFV services (n = 5) were part of a disability support service but had no knowledge about how to get help if they were in an abusive relationship. All of these were younger women (aged 18-24 years) who had experienced bullying (mostly at school) and were currently employed in a program for people with intellectual disabilities. They recalled learning about places where they could get help when they were at school. The police were most commonly named as where to go if they needed help. Headspace was named by three of the five women and described as a place where:
Lots of girls go there when they have problems and then they cut themselves and they go there. That’s the one at the skate park. Then if they’re going to kill themselves they go there, that’s where, that’s a really good one, I know heaps of girls that go there. (Women’s focus group, NSW)
Hospitals, counsellors, and a helpline were also discussed as places where they felt they would go if they were concerned about their safety. The woman who nominated the helpline was not able to name it, or relate the number or where to locate the number to call it. She did recall:
It was on my school laptop I can’t remember…it was like a green or red phone and it said “get help”. (Women’s focus group, NSW)
The women in this group remembered how to get help from school but had no access to information in their current workplace or support service. While they could speak easily about work-related occupational health and safety concepts (e.g. wearing safety boots, watching out for cords), handling animals, and physical safety in the general community (e.g. “watch where you’re going”, “look around; make sure no-one’s acting strange”), in terms of safety within relationships, they were less knowledgeable. One woman talked about looking out for her friends and another about communicating with everyone so that “everyone gets along together”. A third woman talked about a system at work that she connected with safety:
We get a red flag. If you get three red flags if you’re playing up or something, your parents come in, it’s like a—a behaviour thing? If you’re playing up or swearing or something they get a red flag. (Women’s focus group, NSW)
From this woman’s comment it is possible to suggest that safety within relationships for the women in this group was not addressed within a DFV framework: their self-determination was not paramount in addressing concerns about safety.
Women in the Consultative Research Group discussed how they might access information about where to get help. One woman said: “you have to go looking for it”. The researcher suggested the internet might be a source of information, to which someone else replied “they might not have or know how to use a computer or have access to the internet”. Another participant mentioned helplines:
The 1800 number will take you to the nearest service that helps with violence. But sometimes people don’t know about this number until they need it—you learn how to access the services by using them. (Consultative Research Group focus group)
Regardless of whether they have had contact with DFV services or not, the findings in this section reveal that women with disabilities lack knowledge about how and where to get help if living with or in fear of violence in relationships. The raises the importance of prevention education about domestic or family violence for women with disabilities. Rather than shielding women from information about violence, they have a right to know that that it is never acceptable and how to get help if they are in fear or it happens.
Although it was not the focus of this research, disability services are notoriously protective of the women in their care, a phenomenon called “gatekeeping” (Frawley et al., 2012). This was particularly apparent with the group of women who had only had contact with a disability service.
Another kind of gatekeeping for women with disabilities may also take place in some DFV services. Although each of the case study sites presented their work as “woman-centred”, not all of the women experienced the assistance they received as such. An Aboriginal woman from the South Australian site explained:
They need to let the client make—I don’t know how to word it. Not make the decision for us. We know what we need better than anybody…But they also need to find out why we have that disability, and then understand the disability, then get into where they can sit down with us and understand what we know, what we need. (Women’s focus group, SA)
Although it is not clear whether this passage is a criticism of the South Australian site, it is clear that self-determination is very important to this woman. Well-meaning efforts to shield women with disabilities from information or making decisions that can help them gain control over their lives are unacceptable. It is important that a “woman-centred approach” be central to day-to-day practice by DFV workers and not just service rhetoric. This approach is also important for the other services that support the needs of women with disabilities who have experienced abusive relationships. Critical reflection on the implications of this approach and continuous improvement should be an ongoing part of DFV service practice, with a particular focus on intersectionality. We expand on this in the action research section below.
Given the high incidence of family violence and sexual abuse experienced by women with disabilities, ongoing health promotion, social marketing, and prevention education is essential to ensure women can determine what constitutes violence and how to get help if it is needed.
Features of effective DFV services
Relationships
Women at all the case study sites told stories about relationships with workers or services that were positive, in which they were treated respectfully as individuals. They also told stories about poor-quality relationships. Women with disabilities who have experienced violence and abuse in relationships are dependent on a web of services that often do not function together to adequately meet their needs. Fundamentally, they value a worker who is friendly, supportive, and helps them to find safety. In many cases these women have been isolated and, although it is not the role of DFV workers, at times they just need a supportive friend to help them navigate the system. At times the worker fulfils this role because they do home visits. One disabled woman explained:
I think [workers] just need to think about, that service is for women who are at their most vulnerable and most of the time that they are in need. Because I don’t drive, it was about going to their offices and things like that and a lot of the time it might be that they need to come out and do some things at home once the order is in place, or just try and find ways around. (Interview, Vic.)
Sometimes the kind of support women with disabilities need is companionship to alleviate the stress and fear associated with being in a violent relationship. A participant from the Victorian site explained:
Probably the biggest support I need is someone to come in and maybe just take me out and do something. Or just come to my house and just chill out with me for a while and do de-stress stuff. I was in my house pretty much housebound for the first 2 or 3 weeks after the full order. I wouldn’t go out and I was scared, even now I’m thinking that and making sure he’s not near me. (Interview, Vic.)
For women at the New South Wales site, it was important that workers noticed and told them when they were doing well. They needed both acceptance and positive feedback even on the trivia of their lives:
Woman 1: You can be yourself around them, like, if I’m having a really shitty day and I’m swearing and stuff, my worker is just like, “Oh you”.
Woman 2: It makes you feel really good because sometimes they come to your house real bubbly and they go, “Oh, your house looks really lovely today”, and stuff like that. (Women’s focus group, NSW)
Trust and confidentiality were particularly important. One woman explained: “Yeah, they don’t go and talk about your business behind your back, like, after they’ve spoke to you about it” (Women’s focus group, NSW).
The women also valued consistency in their relationship with workers. Having to relate stories of abuse repeatedly to different workers can be painful or re-traumatising for some women:
I first had [a DFV worker] and she got promoted or something, so she left; then I got another worker. So it’s been three different people and that doesn’t have to make it helpful because then you have to explain yourself all over again. (Interview, Vic.)
Women at all sites were particularly positive about the consistency of support they experienced over time and felt it was important to be able to build a relationship with their caseworker. At the New South Wales site, the relationship with the DFV worker was appreciated for the sense it gave women of feeling valued and respected. It also generated a sense of purpose for each woman. They described a range of roles that were fulfilled by their caseworkers, from the intake process to the ways they were supported to attend appointments, find secure housing, get medical check-ups, enrol in parenting and other courses, and get practical help with “the little things and the big things” (e.g. dropping bread off once a week and helping with getting a new fridge).
The combination of disabilities and living with or recovering from violence or the threat of violence can be draining and even overwhelming. Trying to navigate multiple systems while attempting to live independently can seem insurmountable. Having a trusting relationship can be key, as one woman explained:
It really helps you get things done. Because if you’re sitting around home by yourself and, you know, you’re too worried about cleaning the house or doing—or dinner, that’s all you think about, oh, what am I going to have for dinner? What—I’ve got to clean this, I’ll do that. So when they’re on your back about things, like the important things that you don’t like [to] think about, it’s really good and then you can actually go to sleep at the end of the night and think, well, that’s done, I don’t have to worry about that any more. (Interview, Vic)
While it is not the role of DFV workers to befriend their clients, for the women in this study, a warm, supportive relationship was a critical part of the journey to recovery and independence. Knowing there is someone to fall back on in a crisis is also seen as an important part of the worker’s role:
The worker I had back in January 2015 wasn’t very good. Then I got my own home, um, but then I got involved with my partner, and I had to move, yep, because he was abusive. And the police contacted the agency and I got my current worker [sighs]. She organised the removalist and all the help I needed, she was great, she was brilliant. (Interview, Vic)
This raises the importance of practical support to manage day-to-day life. The ways in which workers related to women through small acts, such as recognising when women and their children were doing well, in addition to providing practical and emotional parenting support and taking as much time as needed for individuals to gain confidence, were all mentioned in interviews and focus groups by participants. The women who had lived in shared crisis accommodation also appreciated sharing cooking and child care tasks as ways of supporting others and gaining support themselves. There is evidence that being linked into group activities empowers women and enables them to both learn new skills and teach others (Mejias, Gill, & Shpigelman, 2014).
For many women with disabilities who have children, the threat of losing custody is constant. It therefore is not so surprising that providing support for the whole family is an important issue. As one woman put it: “It helps the kids when you help me too” (Women’s focus group, NSW).
Another theme from the research relates to the importance of group social support that brings together women with similar experiences. This aspect of social support is seldom provided and this leaves women with disabilities isolated, ashamed, and fearful, even after they have escaped from violence. In the Consultative Research Group, one woman suggested “a drop-in place that people can pop into to have a chat and a coffee”. Another woman, who was herself a self-advocate, mentioned greater self-advocacy would help women to break down the isolation.
In one of the specialist sites, women with disabilities met together in an ongoing social support group. In a focus group, they talked about how they liked the ongoing nature of their group and that they didn’t meet just to talk about violence, but rather chatted about all kinds of other things. The safe place philosophy that underpinned the group, as well as the relationships of trust with workers that they knew, was very important to these women.
Service co-ordination and collaboration
Many of the women with disabilities at the case study sites had experienced disruption to support services. In part, this was because they had moved around to escape violent relationships, and “When you move around…you can’t get services”. However, it was also due to a lack of co-ordination and collaboration between the various services on which they depended to live independently without violence. A key challenge identified by the participants was losing one service because another service was involved (e.g. “When disability services stop because you are using a DV service”). As one woman commented, “Youou are not getting help from either DV or disability and need ongoing counselling and case management, but nobody is giving you this.”
Another woman with multiple challenges outlined the ways in which services had failed her:
I’ve always had bad experiences of the psych services, and when I was in the refuge I was ODing pretty much every day, at least; the minimum was two to three times a week and psych services were like, “You’ve got a disability; you don’t fit into our category, so go away. Because our category is alcohol and mental health, or drugs and alcohol and mental health.” So disability wasn’t a big perception of what they wanted in their little group. So it made it really hard. (Interview, Vic.)
These experiences had occurred in the past when this woman was living in a different area. Having moved to a new location, the services were better coordinated and things had improved:
But now they are good and they are doing crisis care for me if I need it. I have a really good psychiatrist; I can call him any time. I’ve got a really good psychologist and a good mental health together. (Interview, Vic.)
Some women fear disclosing that they have multiple problems. As one Aboriginal woman noted:
I was too afraid to tell them [the refuges] that I had a disability. I went from shelter to shelter to shelter in different places and back to abusive relationships because I didn’t tell them I had a disability…didn’t get the help I needed. (Action research workshop, SA)
The women’s stories about their experiences in DFV services show that, when it is working well, there is a strong relational connection between the service or worker and women with disabilities. The women value consistency in their contact with workers and trust that they will be treated with respect and dignity. They also value being supported to take as much time as needed to manage their lives and get back on track. A whole-of-family approach to care is essential to ensure women are able to keep and care for their children. Above all, access to group support from other women who have had similar experiences was identified as imperative and lacking.
Action research cycles
As discussed in the methodology section, this stage of the research was grounded in an action research methodology in order to put into practice the collaborative principles that underpin the project and build new knowledge. This strategy responds to the experiences and perspectives of participants in the interview and focus group stages of the research process. Action research is a participatory, democratic process concerned with developing practical knowledge. It brings together action and reflection, theory and practice, with the aim of solving community problems (Bradbury, 2015).
The action research cycle brought together key DFV and disability stakeholders in two of the case study sites to collaborate on identifying, planning, and starting to implement service improvements. In this section, we start with the findings from the action research cycles, then draw together overall findings to suggest some ways in which the tertiary response sector can deliver more effective services for women with disabilities.
South Australia: action research process and outcomes
At the South Australian site, the researcher and site manager together developed the service’s action research aims after the initial data collection phase. Two key aims were identified:
- to have more meaningful and ongoing contact with women with disabilities; and
- to revisit the development of a collaborative and cross-sectoral working group that would focus on access for women with disabilities.
Over 7 months in 2015-16, the site manager worked on these two aims and reflected on the approach and outcomes with the researcher via emails and phone calls. One proposed action to achieve these aims was bringing together a group that would form the local action research group. Membership comprised a disability consultant (a woman with a disability), other disability activists, and community and government organisations. The researcher provided consultation to the manager on the ongoing development of this group.
In September 2016, the action research group was brought together for a workshop, facilitated by the researcher, at which the research findings from the project were presented. Discussion then focused on the group’s action research aims and the development of an action plan.
The researcher conducted a 2-hour reflection meeting with the manager 2 weeks after the initial workshop, where further analysis of the local aims and progress was discussed. Reflections from this meeting also fed into the final analysis of the site data and the key themes emerging from this site.
The action research approach enabled the service manager to reflect on the place of women with disabilities in the service and conclude that the service did not really engage with women in roles other than that of service-users. This raised questions about increasing the participation of women with disabilities and ways to draw on their expertise in what works best for them and others like them. The service manager identified two influential learnings from the research process. First is the importance of hearing the views of women with disabilities:
Women with disabilities bring their experiences to the service; the service responds but needs to see and reflect on what the women teach us in the process…We need to hear from women with disabilities…woman with a disability says “X” we critically reflect and use this for change. (SA manager)
Second is the importance of cultural change within the service and across the sectors that impact on the lives of women with disabilities. Some of these changes were already underway; for example, workers now recognise that they know little about what happens for women with disabilities after they leave the service. As a result, the service is now following-up with women with disabilities to check in and see how they are managing. In many cases, this has resulted in a celebration of how far the women have come. This is particularly important for Aboriginal women service-users, as they often lose important community networks and contacts when they escape from abusive relationships. The staff also noticed that women with disabilities wanted to remain involved because it was a “way of helping other women with disabilities”. The service is working out how best to incorporate this learning into their practice.
Figure 3 South Australian action research cycle process.

Text alternative for Figure 3
Feedback to local group
- Research in sites
- Analysis
Locally developed and implemented approaches
- Local group workshops
Local approaches fed into research-informed practice model
- Feedback to researcher
One of the issues raised in the research is the tendency for services to “protect” women with disabilities, which can lead to limiting their agency and autonomy. The manager reflected that their “misguided desire to not re-traumatise” women with disabilities by recontacting them may have overshadowed ongoing opportunities to positively engage with them on further developing access and inclusion.
Another insight that emerged from the action research cycle was that some women with disabilities who experience violence in relationships may not recognise their experience as “domestic violence”. In particular, this may be the case for women with severe or complex disabilities who are reliant on a carer. The women with disabilities who participated in the action research emphasised that they had not known that there were places where they could get the kind of help available through DFV services until they had started using the service.
The work undertaken by the South Australian site to improve accessibility for women with disabilities led to new relationships with a number of other agencies and, perhaps as a result, they have also experienced an increase in referrals. Engagement with the research provided this site with opportunities to critically reflect on services for women with disabilities, and to identify gaps in existing services and strategies for addressing these gaps. This has provided opportunities to formalise an advocacy model that is depicted in Figure 4. This model highlights the importance of collaboration with women with disabilities and other services as part of the “respond and refer” cycle.
Figure 4 South Australian advocacy model
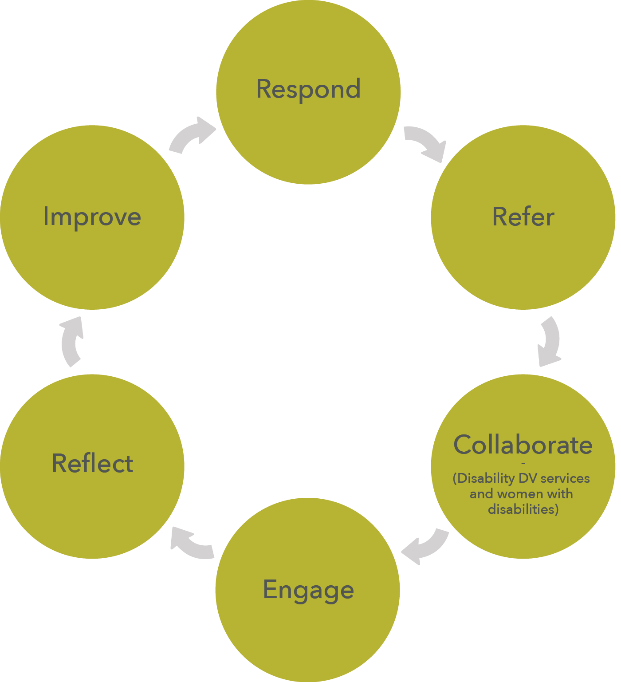
New South Wales: action research process and outcomes
The New South Wales case study site took an incremental approach to work more effectively with women with disabilities by building awareness, skills, and collaboration. Over the course of the research, four action research cycles took place, led by the service, supported by the researchers, and steadily involving an increasing number of collaborative relationships. The action research cycles in the New South Wales site involved three phases: identifying action goals, inviting cross-sector collaborators, and cross-sector training.
Phase one: identify action goals
Following the initial research contact with staff of the service, the manager and researcher derived four action goals, which arose directly from the priorities identified in the focus groups and interviews. The manager was enthusiastic about embedding these goals in the work of the service and proposed taking them to management to link them into the service draft strategic plan. This gave the goals organisational weight and connected them into work flows (such as preparing for an upcoming audit). The four goals identified were:
- To work with the quality assurance system to make sure that all policies and procedures were current and inclusive of women with disabilities.
- To review the service strategic plan to make people with disabilities a focus. The strategic plan was under review and the research prompted thinking about how the service could prioritise women with disabilities across a number of elements of the plan. Results are to be measured using the Results Based Accountability framework the service applies across multiple programs.
- To feed into the Regional Action Group. A regional domestic violence awareness forum held shortly before the research commenced produced an action plan for the organisation, which focuses on four core areas: community education, increasing community involvement in awareness campaigns, involvement of sporting clubs, and linking services together.
- To develop a small group for women with disabilities to learn from their experiences and provide support. This responded to the expressed desires of women with disabilities participating in the focus groups to provide peer support to one other.
Involvement in the research prompted the manager to reflect on the extent to which women with disabilities were included in the strategic development currently underway in the service. This led to prioritising women with disabilities and building in processes to measure the impact of the changes over time.
Phase two: invite cross-sector collaborators
The increased focus of the service on women with disabilities was conveyed to the regional domestic violence committee with the aim of stimulating interest and collaboration across services and sectors. A short presentation was prepared by the manager, with help from the researchers, that covered information about violence against women with disabilities and the key research findings. Fifteen members of the regional domestic violence committee committed to further action. The committee added women with disabilities as a priority group to the regional action plan.
The focus of the discussions was disability; however, in addition, the group discussed the impact of poverty, Aboriginality, and cultural and linguistic diversity (CALD) on the experience of violence in regional women’s lives. For example, women from CALD backgrounds living in regional areas who experience language barriers often have to rely on family members to interpret for them. The group observed that this frequently resulted in arguments between family members and were concerned that family-member interpreters managed multiple concerns of the whole family, rather than representing the woman.
Phase three: cross-sector training
The engagement of the regional domestic violence committee raised the profile of women with disabilities in some new initiatives in the region. In recognition of the siloed approach to different services, agencies have started to come together in one location on a monthly basis to ensure cross-sector collaboration and access for women with disabilities.
A remaining area of concern in the service is workers’ skills to respond to the complex needs of women with disabilities. The manager reflected that referral between DFV and disability services remained rare, despite some improvement in on-the-ground working relationships.
A series of meetings were held with key people in the disability support sector to explore the possibility of jointly hosting training for DFV and disability support services. Due to the approaching rollout of the National Disability Insurance Scheme (NDIS), disability services felt under pressure and unable to contribute to planning at this stage; however, they remained supportive of the idea. After some consideration, the NSW site decided to host and fund the training and to offer it across sectors. A specialist trainer was sourced (with support from the researchers) to provide the training and 14 workers from DFV services, disability support services, and the state government participated. Satisfaction ratings were high and indications were that participants found accessible safety planning, the opportunity to network with people in other sectors, and learning about each other’s complementary skill sets to be of particular value. A second training session is planned with women with disabilities.
Phase four: consolidate cross-sector collaboration and internal action goals
At the time of writing, the fourth action research cycle is ongoing, with goals of consolidating the cross-sector collaboration and:
- working internally on the service quality assurance system to make sure that all policies and procedures are up to date, current, and inclusive of women with disabilities;
- reviewing the strategic plan to make women with disabilities a focus;
- feeding into the regional action group;
- developing a small support group for women with disabilities; and
- developing promotional material in Easy English language.
A constant tension at this site was balancing the agreed actions with competing priorities. Setting meetings to plan the training was helpful in progressing the action research, as each person involved had clear goals. Transformative change in the service is yet to be achieved. However, signs of change are apparent. For example, there is a desire to establish a peer support group in response to the expressed wishes of service-users and training for women with disabilities will be forthcoming. The service is also interested in investing in a “train-the-trainer” model to embed this skilled support.
Figure 5 NSW action research process
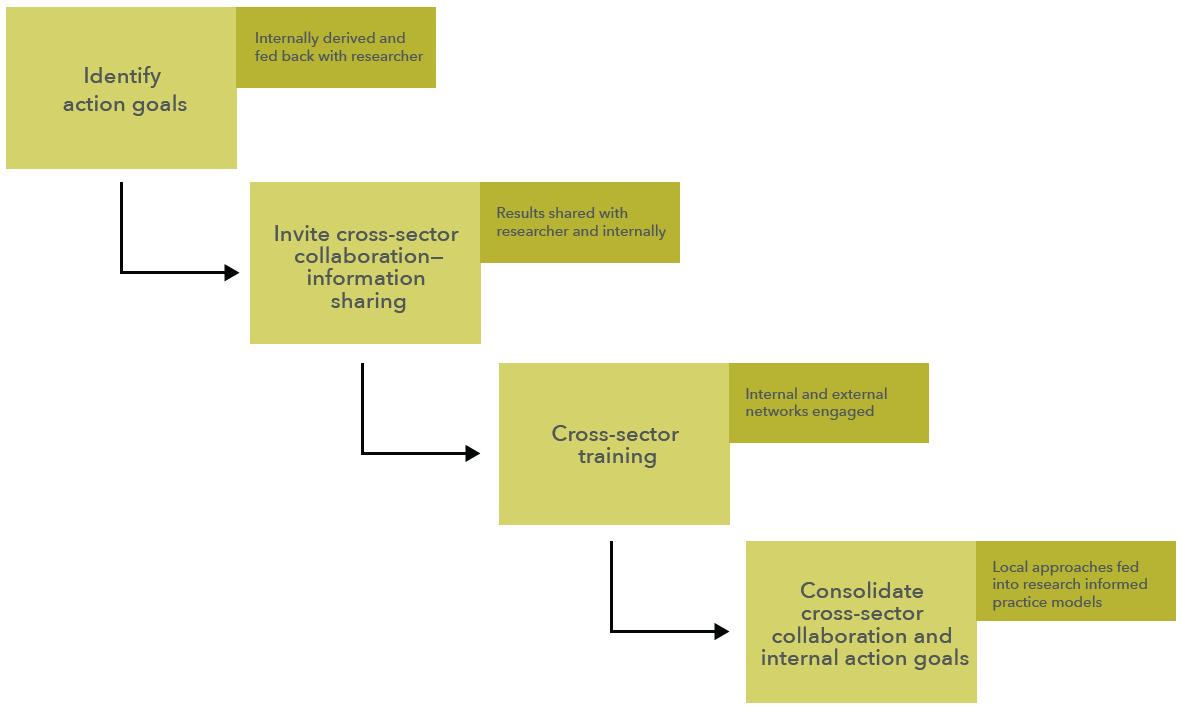
Text alternative for Figure 5:
- Identify action goals: Internally derived and fed back with researcher
- Invite cross-sector collaboration– information sharing: Results shared with researcher and internally
- Cross-sector training: Internal and external networks engaged
- Consolidate cross-sector collaboration and internal action goals: Local approaches fed into research informed practice models
Specialist crisis response services
Profiles of two additional sites that demonstrate promising practice are included here. These agencies provide specialist services to people with disabilities who have experienced sexual assault. The purpose of including these services is to identify components of the specialist models that contribute to answering the third research question concerning how services can be improved to deliver effective services for women with disabilities. The sites agreed to be profiled as part of this research; however no qualitative evaluation was done in these sites.
Queensland specialist service for people with intellectual disabilities
This specialist service works with people with intellectual or learning disabilities who have been victims/survivors of sexual violence, other crimes, or exploitation. The service provides counselling, groups, support, information and referral, community education, and training for people with intellectual disabilities. It is jointly funded for its work by state government community services and justice agencies. The service grew from the collaborative endeavours of a disability support organisation and a women’s resource centre and continues to collaborate with both of these organisations. The approach of the service is grounded in the social model of disability, which leads to a strong focus on access and building capacity in individuals, supporters, and organisations to respond effectively to violence in the lives of people with intellectual disabilities.
The model
People with intellectual disabilities who use this service engage with it in ways that they find useful. They can access individual counselling, participate in a group, and access and have input into the development of information, resources, and training. Through accessing this service, they also have the opportunity to participate in community events that engage them with violence prevention activities in the community. The service describes this as “blended support” where women (and men) come in, often through individual counselling, and then move into a group and might also participate in some one-off community events.
The second stream of service is the provision of training; there is a clear education focus for disability sector workers that includes people with disabilities as trainers. Training is provided for support workers and case managers of disability services and mainstream violence response professionals, including police, generalist counsellors, sexuality and violence counsellors, and case managers.
A third area of work of the organisations is systemic advocacy. Issues that are raised through the two streams of service provision are collated and used to lobby government and to inform government and service policies and practice. The focus is on capacity building for individuals, supporters, and organisations to respond more effectively to the needs of people with intellectual disabilities who have experienced sexual assault.
What makes the model work?
Including women and being informed by women’s experience: Women with disabilities inform the service delivery in a number of ways: through contributing ideas in regular peer support groups, via complaints and feedback systems, and in contributing to the development of training programs.
Accessibility and flexibility: The service prioritises access above all else and takes a flexible and open approach to welcoming people into the service before they are asked to consent to receiving support. The manager explained that people often cannot imagine what the service might be able to offer and may be very apprehensive, so gently introducing them to the service and what is available is critical. Prioritising access and being flexible about how people access available services (on-site, off-site, as an individual, with a partner or supporters, in groups, and at different times) means they get to “see what it’s like, what it’s all about” and then make a decision. This includes not excluding people who may, for instance, miss three scheduled sessions in a row, but instead being willing to look again at how the service can be flexible to meet their needs. Taking a flexible approach was also at times about having a gendered understanding about the experience of violence and ensuring individual’s emotional and physical safety in groups. This means, for example, ensuring that male clients are not seen when a women’s group is running.
Victorian specialist sexual assault program for people with disabilities
This specialist program provides counselling and advocacy for people with cognitive disabilities or complex communication needs who have experienced sexual assault. The model was developed as part of a decade-long campaign in Victoria to address the justice inequities experienced by people with cognitive impairments who have experienced sexual assault (Goodfellow & Camilleri, 2003). A range of legislative reforms were enacted over the same period of time in Victoria to address identified issues in the Sexual Crimes Act 2006 (Vic.) for all victims/survivors, with some specific changes recommended and implemented that referred to people with cognitive impairments (Victorian Law Reform Commission, 2004). The Federation of Community Legal Services noted, however, that significant non-legislative reforms were required to meet the needs of people with cognitive impairments (Federation of Community Legal Centres, 2011). Improved advocacy was a key issue identified in the research that informed the development of the program. Camilleri (2010) noted that advocacy for victims/survivors of sexual assault with cognitive impairments was vital and played a central role in progression of sexual assault reports by victims/survivors with cognitive impairments throughout the justice process.
The model
The program directly addresses advocacy for people with cognitive impairments or complex communication needs in three ways:
- It enhances the capacity of all counsellors and advocates in the service to work more effectively.
- It increases access to legal advocacy for victims/survivors of crime compensation.
- It addresses systemic barriers to achieving justice for clients by acting as a platform to increase sexual assault services’ involvement in research and policy advice on sexual assault of people with disabilities.
The service employs a dedicated counsellor or advocate to manage the program. This role includes:
- providing secondary consultation to other counsellors or advocates when they are working with a client with cognitive impairments or complex communication needs.
- maintaining a comprehensive resource database and providing training internally and throughout sexual assault service networks in Victoria on working effectively with clients with cognitive impairments or complex communication needs;
- providing information access for people with disabilities through the comprehensive collection of Easy English resources that were developed during the pilot program and are available online;
- funding clients to pay for additional support when they have appointments with the service the police, or to attend court dates;
- liaising with the Office of the Public Advocate to provide trained Independent Third Persons for interviews with people with disabilities who are victims/survivors of sexual assault; and
- liaising with legal service workers to enhance their practice in working with people with disabilities wishing to access crimes compensation.
What makes the model work?
For almost 2 decades the service has actively sought to improve access for victims/survivors of sexual assault with disabilities through externally funded projects. This includes the development of Easy English resources on sexual assault and in-house training on disability. They have provided leadership within the sexual assault sector on issues of access to counselling, advocacy, and justice for victim/survivors with disabilities by providing their expert input to research and a variety of community and government groups. They have also trained counsellors from a range of agencies to support women with disabilities
The program was evaluated in 2014 and a number of positive factors that influenced the program outcomes were identified:
- It provides a focus in the wider service on access for people with disabilities, thereby engaging the service not only in continual improvement to their approach but also in giving them a platform to engage more broadly in systemic advocacy about sexual assault and disability, thereby ensuring disability is considered within the broader sexual assault sector.
- The staff’s expertise as sexual assault counsellors or advocates with or without experience in disability underpins the capacity of the service to provide a very high level of service and informed practice.
- The multi-faceted approach, based on “enhancement” to counselling and legal advocacy practice, rather than “different” approaches (Frawley, 2014).
A key finding from the evaluation was that when the service focused its attention on the specific needs of people with intellectual disabilities or complex communication needs, referrals increased, as did understanding about their experiences of sexual violence. This was enhanced by the program’s collection of data and the anecdotal reflections of workers, which strengthened the service’s systemic advocacy within the sector.
Improving response services for women with disabilities
The research aimed to develop new knowledge to inform the development of guidelines for good practice in tertiary DFV services for women with disabilities in Australia. These guidelines aim to be:
- based on a thorough and critical review of evidence concerning world best practice;
- informed by the experiences of Australian women with disabilities;
- developed in collaboration with locally-based, cross-sector communities of practice; and
- designed to inform a gendered understanding about violence in the disability sector.
The review of literature that preceded this research demonstrated that a great deal of work has been carried out in the past to identify good practice principles for working with women with disabilities who have experienced violence. Three key factors stood out in the review as important for accessible, effective tertiary response services. These are physical and programmatic accessibility, cross-sector collaboration, and evidence-based practices. This research confirms the importance of these principles and expands on them.
Good practice principles
Broadly defined, “good practice” is practice that has been proven to work well and produce good results. In this section, we draw together the findings from the previous sections and discuss the findings to the third research question: in what ways can tertiary responses be improved to deliver effective services for women with disabilities based on the knowledge developed from this research?
Models and approaches
The findings of this research indicate that although they are committed to providing safety and support for women with disabilities, for the most part, DFV services do not demonstrate high levels of knowledge about support services available for women with disabilities. They rely on referral to disability services to assist women to access disability supports and benefits and only limited cross-sector collaboration was found. This is not to suggest that DFV services fail women coming to them for help. Rather, a complex “whatever it takes” approach is used to ensure the safety of women escaping violence. The flexibility of this approach helps women with disabilities in many instances, and many disability services are responsive to requests. However, simple referral without effective collaboration may leave women without appropriate support.
Both DFV and disability services may be overly protective of women with disabilities. For DFV services, this can be to avoid re-traumatising women after they have been resettled. As a result, women may not be consulted about the extent to which the service was accessible and appropriate to their needs. Furthermore, women with disabilities in this research called for opportunities to meet with other women who have experienced violence for social support and understanding. Services have not yet heard these calls and in their attempts to “protect” women, they may be denying them this important, ongoing form of support. This was recognised by services that participated in the action research phase of the project. Offering opportunities for women with disabilities to come together through the DFV services was identified as a promising approach and one that the Queensland specialist service identified as important for women with disabilities.
Two clear “categories” of women with disabilities were found within DFV services. The first group are women whose disabilities are officially recognised and who, as a result, are eligible for a range of disability support services. These women often self-identify as having disabilities or have a friend or carer who will identify her support needs when she comes into the DFV service. The second group are women who are observed by intake or caseworkers to have disabilities (such as acquired brain injuries, mental health issues, or alcohol or other drug problems), often as a result of living with violence. These women may not be immediately eligible for disability support services, even though they are needed. It is more difficult for workers to access appropriate accommodation and support for women in this second group. This difficulty is compounded by the bureaucracy involved in getting official recognition for disabilities. It is further exacerbated by a lack of cross-sector collaboration: DFV workers are not experts in the disability sector and lack knowledge and information about disability services.
A further challenge for DFV services is that women with disabilities may avoid disclosing their disabilities when they do come to a service, which has implications for what the service can provide. Women may not disclose their disability because they do not understand or trust the service or because they do not identify strongly as a woman with a disability. In some cases, women do not disclose for fear of losing custody of their children or connections with family and culture, which was particularly an issue for Aboriginal women who participated in the study. Although greater diversity was not achieved in the sample of women who participated in this study, it is possible to project that this is probably also an issue for women from CALD backgrounds. Many women with intellectual disabilities lack knowledge about domestic violence and sexual assault, so it is possible that some may not seek help until the violence becomes intolerable or is reported by a third party.
The Disability Discrimination Act 1992 (Cth) makes it unlawful to discriminate against people on the basis of their disability or perceived disability and emphasises equality of access to information and physical premises (PWDA & DVNSW, 2015). Our research suggests that for women with disabilities in need of support from DFV services, “access” is more than adapting buildings to meet physical needs of people with disabilities. Some tertiary response services have a limited understanding about disability and accessibility beyond physical access. To be truly accessible, services must be approachable, acceptable, available, affordable, and appropriate. Unless these criteria for access are met in the first place, programmatic and physical access is unlikely to be possible.
Women’s voices
Not all of the women who participated in this study found DFV services approachable, acceptable, or appropriate to their needs. Women who had not used DFV services had little knowledge that such services existed or how to get help other than going to the police if they were in a violent relationship. The police were not seen as approachable (and even seen as scary). Some women who were service /users had continued to live with violence in the past because they lacked knowledge about where to get help or that it was available.
Many of the women with disabilities interviewed for this project had long-term relationships with DFV services and disability services. These women were, for the most part, poor and living on the margins. For them, the relational nature of the support the service provided was important, as was the consistency of the support and the safety they had found. The women with disabilities who participated in this research valued above all:
- A consistent relationship with one worker rather than seeing a range of different workers.
- Being able to trust the service and their worker to maintain confidentiality and to be there for them when they are needed.
- Being treated with respect.
- Being seen as experts in their own lives and having access to the information and support they need to make their own decisions. For these women, independence and autonomy are vital; they talked about “hard-won independence”.
- Being trusted to make their own mistakes rather than being told what is best for them.
- Having access to social support, both from their workers and in groups with other women who have experienced violence in relationships.
Service improvements
Later in the research, the case study sites recognised that they had at times not acknowledged women’s experiences or trusted them as experts in their own lives. This was an important shift that creates openings to incorporate their ideas into service improvements and planning. Although not easy, given the high-pressure environments in which DFV services work, many services that participated in this research recognised that they could improve their ways of working with women with disabilities and, in particular, this could come from taking (or having) the time to reflect on the experiences and perspectives of women with disabilities. Work undertaken at the sites as part of the action research cycle demonstrates how service improvements that are informed by reflections on practice can be incorporated into practice. Through the action research cycles, services had some opportunities to stop and reflect on what women with disabilities had to say about their complex experiences seeking support after violence and abuse. DFV services are high-pressure environments that are often under time and resource pressures that limit their opportunities to stop and reflect. Through this research, this opportunity was afforded to them and, for some, the insights gained will inform future service improvements.
A “clash of cultures” was identified between DFV services and other services that support women with disabilities. Women with disabilities highlighted that there are other ways in which clashes of culture occur in relation to women’s personal and social values, their culture and sense of autonomy, and those of the service from which she seeks help. These clashes of culture can be barriers to accessibility of services but understanding and reflecting on these can also be opportunities for improvement.
Prior to the action research, the sites used a simple model of referring to disability services to address the access and support needs of women with disabilities. With support and facilitation from the researchers, services started to identify where cross-sector collaboration could contribute to improved services, and they began to develop stronger links with other stakeholders. As these relationships developed, a model emerged that involved the DFV service responding to the safety and accommodation needs of women with disabilities and referring them to disability support services, but added further steps. These involved: continuing to collaborate and engage with the service (rather than handing over to them), reflecting on the process and outcomes, and building new knowledge into the process in future. This established continuous improvement and cross-sector collaboration as underpinning principles for working with women with disabilities.
This confirms the learnings from the specialist crisis response services as models of good practice, which included:
- Working with women with disabilities who have experienced violence and abuse should not use a one-size-fits-all approach. As a woman who participated in this research put it, there is no one thing that will work for everyone”.
- The voices of women with disabilities must inform practice.
- Adequate time and flexibility must be allowed for to meet the needs of individuals.
- Stakeholders across the tertiary response sector must be brought together to deliver consistent, appropriate services to meet the needs of individuals.
- High-quality training about working with women with disabilities is essential for all workers across-sectors.
To provide effective, accessible support and safety for women with disabilities requires a coordinated service system, which is greater than standalone DFV tertiary response services. The literature review for this project draws attention to the three-level public health model for preventing violence against women, in which tertiary responses ensue after violence had already occurred. A learning from this project is that while DFV services work with women who have already experienced violence, they also play a role in preventing violence from occurring again. Disability services can assist women who have experienced violence in getting appropriate access, but they also play an important role in prevention. Rather than creating rigid distinctions between levels of prevention in the public health model, prevention and response may be better conceived of together.
Conclusions and recommendations
At the time of completing this report, the Third Action Plan 2016-2019 of the National Plan to Reduce Violence against Women and their Children 2010-2022 (Third Action Plan) was released by the Commonwealth, state, and territory governments (DSS, 2016). Women with disabilities are recognised as a priority group in the Third Action Plan and the following key national actions have been identified:
- Support the development of integrated, responsive, and more accessible services for women with disabilities.
- Explore how technologies can be better used to provide women with disabilities with safe, relevant services.
- Develop free, accredited training on domestic violence for the disability sector.
- Build evidence about the types of violence women with disabilities experience to inform future responses.
- Work with women with disabilities and disability stakeholders to explore opportunities for collaboration and identify policy priorities.
This research supports the key national actions for women with disabilities. It also contributes evidence to inform the implementation of the Third Action Plan in terms of access for women with disabilities and accessible services, cross-sector collaboration, the inclusion of women with disabilities in service development, and the collection of high-quality data to better understand how tertiary response services respond to and collaborate to prevent violence against women with disabilities.
This research aimed to inform the development of guidelines for DFV tertiary response services to respond effectively to the needs of women with disabilities. A number of promising practices were identified from this research that can be articulated as underpinning principles for effective practice. These include:
- “Accessibility” is more than providing physical access: services must be approachable, acceptable, appropriate, affordable, and available to women with disabilities.
- Women with disabilities, like all people, are complex and multi-dimensional; disability is in play with other personal and social factors. Service planning and delivery must be enhanced by the use of an intersectional lens.
- Women with disabilities need more than safety; they need social and relational support in a safe and inclusive environment.
- Service and practice planning, development, and improvement must be informed by high-quality qualitative and quantitative research. This must also be informed by the ideas and opinions of women with disabilities who have used the service.
- All aspects of tertiary response services for women with disabilities must be informed and enhanced by cross-sector collaboration.
Recommendations
To make services accessible, women with disabilities must be at the centre. Services must understand and respond to what women need and want. This research shows that what women with disabilities need and want is practical, supportive, respectful, trusting relationships with workers in services that understand them, their experiences, and their needs.
1. Promoting access and accessibility
This research finds that access for women with disabilities is about much more than simply removing barriers. Ensuring physical access is important, but service accessibility needs to be understood and promoted, so that women with disabilities know services exist that can help them, and that they will be received, acknowledged, and heard by tertiary response services. Good practice principles for accessibility suggest that services must be approachable, acceptable, affordable, available, and appropriate. Through addressing broader issues of access for disability-specific needs, the interface between what the service offers and what women with disabilities need can be better aligned. This requires a shift in how “disability”, “access”, and “accessibility” are understood.
We therefore recommend:
Services review their understanding of “disability” and “access” and draw on the evidence from this research and the work of Levesque et al. (2013) to ensure that they provide services that are:
- approachable: women with disabilities know they exist and feel comfortable to approach them;
- acceptable and appropriate: barriers to communication, housing, and understanding what is offered are removed;
- affordable and available.
2. Building cross-sector collaboration
The findings of this research indicate that DFV services are committed to providing safety and support for women with disabilities. They employ a responsive “whatever it takes” approach to ensuring their safety, which is complex, intersectional, and situational. However, DFV services may lack the time and knowledge to ensure women with disabilities have appropriate disability supports and benefits. To achieve this, they often refer women to disability services, yet only limited cross-sector collaboration was found.
Although disability services were not the subject of this research, the DFV services noted that many are responsive to requests for assistance. Nonetheless, simple referral to another service without effective collaboration may leave women without appropriate support or follow-up. There is an urgent need for the development of cross-sector collaboration that brings together all services that engage in tertiary response, including: DFV services and disability services in relation to immediate supports, and police, judicial services, housing services, and the range of other health and community services involved in supporting women with disabilities to escape from violence and access ongoing supports.
DFV services that participated in this research recognised that they could improve the way they worked with women with disabilities and began this process in the action research stage of the project. A key learning that emerged was the importance of flexibility, time, patience, persistence, and the development of trusting, respectful relationships. Those services that did embark on change processes benefited from an initial process of reflection and planning, developing relationships and then bringing all parties together for a facilitated, goal-oriented, practical process to draw on the expertise of all parties concerned to plan for high-quality, cross-sector collaboration.
Different parts of the tertiary response sector have much to learn from each other about working with women with disabilities. Cross sector collaboration will be enhanced by bringing all parties together to learn from each other and develop ways of working together. This process must be informed by the experiences of women with disabilities.
We therefore recommend:
In order to support initiatives for cross-sector collaboration, the emerging models of good practice identified in this research should be further developed and informed using a facilitated process of reflection, consultation, and engagement with other tertiary response services.
This process should aim to ensure positive outcomes for women with disabilities in all parts of the tertiary response sector through collaboration. It should not be in the form of didactic training, but should use a facilitated process that involves and is informed by women with disabilities.
3. Involving women with disabilities
For a range of reasons discussed earlier in this report, women with disabilities’ ideas and opinions do not appear to inform service improvement. In part, this is due to well-meaning efforts to protect or not re-traumatise women by re-engaging with them once their case is resolved. However, that approach results in a lack of follow-up and ongoing engagement with women.
Women in this research valued the positive and trusting relationships they developed with workers and the opportunity this gave them in some cases to have ongoing involvement with the service. They also valued practical support and opportunities for social contact with others who have shared similar experiences.
There was little evidence of women with disabilities being involved in services beyond their role of client, although when this opportunity was made available through the research in the focus groups and action research groups, women and the service staff saw value in this.
We therefore recommend:
DFV services consider establishing peer support groups for women who survived or are escaping from violent and abusive relationships.
We further recommend:
Service improvement and cross-sector collaboration must be informed by women with disabilities who have used tertiary response services. Women with disabilities should be consulted about their experiences using tertiary response services and their advice incorporated into planning and practice development.
The model of the Consultative Research Group (a group of women with disabilities engaged as research advisors in this study), which ensured that the voices of women with disabilities informed this research, could be used with future sites to contribute to both service and sector-wide reform.
4. High-quality data collection
It was clear in both the survey and case study data that measures to understand and monitor the effectiveness and outcomes of tertiary response services’ responses to women with disabilities are needed. Improving data collection will assist significantly in sustaining good practice in terms of access, inclusion, and cross-sector collaboration.
We therefore recommend:
DFV services should collect data on the disability experiences of clients. Qualitative and quantitative data measures across all programs offered in DFV services should be developed and implemented, and tied to the same measurement and reporting metrics as for other comparative data measures (e.g. age, Indigenous status, and so on). Women with disabilities should be involved in providing qualitative data and be engaged to co-produce information from it that can be used in service improvement and wider sectoral reform at local, state or territory, and national levels.
Project limitations and strengths
Disability is a complex, dynamic, and multi-dimensional lived experience and a contested phenomenon. This is highlighted in the literature review, which discussed the importance of understanding the ways that characteristics such as age, class, culture, gender, race, sexuality, and disability intersect. These aspects of identity are also affected by being a parent, partner, or lover, and connected or disconnected to family or a community.
This research was limited in a number of ways in relation to achieving diversity of research participants and diversity of geographical locality of case study sites. The scope of the project and the time frame for the project contract limited the capacity of the research to have a larger number of case study sites and therefore more geographical diversity, and the research methods used limited the gathering of demographic data. One of the case study sites has an Aboriginal program and provides services in a culturally specific site, and although there was some diversity in terms of race, culture, and experience of disabilities among the women who participated in the study, this demographic data was not collected, as discussed in the methods section. The project could also have been strengthened by working with an additional case study site, in particular a remote site.
The strengths of this project have been discussed at length in the methodology section above and throughout the report. The approach was underpinned by the principle of social inclusion for women with disabilities, as well as an understanding of intersectionality. The Consultative Research Group contributed to the planning, implementation, and analysis of all aspects of this research, as did women with disabilities from the case study sites, making it truly inclusive, participatory research.
References
Australia. Department of Social Services. (2016). Third action plan 2016-2019 of the national plan to reduce violence against women and their children 2010-2022. Canberra: DSS. Retrieved September 12, 2016 from https://www.dss.gov.au/women/programs-services/reducing-violence/third-action-plan
Australian Bureau of Statistics. (2011). Disability prevalence. Retrieved October 22, 2016 from https://www.abs.gov.au/AUSSTATS/abs@.nsf/Latestproducts/4446.0Main%20tures42009?opendocument&tabname=Summary&prodno=4446.0&issue=2009&num=&view=features42009?opendocument&tabname=Summary&prodno=4446.0&issue=2009&num=&view=
Australian Bureau of Statistics. (2012). Personal safety survey. Retrieved October 22 from https://www.abs.gov.au/ausstats/abs@.nsf/mf/4906.0
Australian Human Rights Commission. (n.d.). A quick guide to Australian discrimination laws. Retrieved October 22, 2016 from https://www.humanrights.gov.au/sites/default/files/GPGB_quick_guide_to_discrimination_laws_0.pdf
Ayre, J., Lum On, M., Webster, K., Gourley, M., & Moon, L. (2016). Examination of the burden of disease of intimate partner violence against women: Final report (ANROWS Horizons, 06/2016). Sydney: ANROWS.
Babic, M. M. (2009). Violence and persons with disability. Ljetopis socijalnog rada/Annual of Social Work, 16(3), 595-614.
Ballan, M. S., & Freyer, M. B. (2012). Self-defense among women with disabilities: An unexplored domain in domestic violence cases. Violence Against Women, 18(9), 1083-1107.
Bradbury, H. (2015). The SAGE Handbook of Action Research: Third edition. Thousand Oaks, CA: SAGE.
Camilleri, M. (2010). [Dis]abled justice: Why reports of sexual assault made by adults with a cognitive impairment fail to proceed through justice. (Doctoral dissertation). University of Ballarat, Ballarat
Chang, J., Martin, S., Moracco, K., Dulli, L., Scandlin, D., Loucks-Sorrell, M., & Bou-Saada, I. (2003). Helping women with disabilities and domestic violence: Strategies, limitations, and challenges of domestic violence programs and services. Journal of Women’s Health & Gender-Based Medicine, 12(7), 699-708.
Chenoweth, L. (1996). Violence and women with disabilities. In S. Cook & J. Bessant (Eds.), Women’s encounters with violence: Australian experiences. Thousand Oaks, CA: SAGE.
Council of Australian Governments. (2012). National implementation plan for the first action plan 2010-2013: Building a strong foundation. Canberra: FAHCSIA.
Disability Discrimination Act 1992 (Cth). Retrieved July 18, 2016 from https://www.legislation.gov.au/Series/C2004A04426
Dowse, L., Soldatic, K., Didi, A., van Toorn., & Frohmader, C. (2013). Stop the violence: Addressing violence against women and girls with disabilities in Australia: Discussion paper. Hobart: Women with Disabilities Australia.
Dowse, L., Soldatic, K., Spangaro, J., and van Toorn, G. (2016) Mind the gap: The extent of violence against women with disabilities in Australia. Australian Journal of Social Issues, 51(3), 341-359.
Equality Act 2010 (UK). Retrieved July 18, 2016 from https://www.legislation.gov.uk/ukpga/2010/15/contents
Federation of Community Legal Centres. (2011). Making rights a reality for sexual assault survivors with cognitive impairments. Melbourne: FCLC.
Flood, M. (2011). Involving men in efforts to end violence against women. Men and Masculinities, 14(3), 358-377. doi:10.1177/1097184×10363995
Frantz, B., Carey, A., & Bryen, D. (2006). Accessibility of Pennsylvania’s victim assistance programs. Journal of Disability Policy Studies, 16(4), 209-219.
Frawley, P. (1997). Training manual for Centres Against Sexual Assault: Working with victim/survivors with an intellectual disability. Melbourne: South East CASA.
Frawley, P. (2000). Sexual assault project report: Working with victim/survivors with an intellectual disability. Melbourne: Family Planning Victoria.
Frawley, P. (2014). Making rights reality: Final evaluation report 2014. Melbourne: La Trobe University.
Frawley, P., Barrett, C., & Dyson, S. (2012). Real people, core business: Living safer sexual lives: Respectful relationships. Report on the development and implementation of a peer-led violence and abuse prevention program for people with an intellectual disability. Melbourne: La Trobe University.
Frawley, P., Dyson, S., Robinson, S., & Dixon, J. (2015) What does it take? Developing informed and effective tertiary responses to violence and abuse of women with disabilities in Australia (ANROWS Landscapes, 03/2015). Sydney: ANROWS.
Frohmader, C. (2010). Women with disabilities & the human right to health: A policy paper. Melbourne: WWDA.
Frohmader, C., Dowse, L., & Didi, A. (2015). Preventing violence against women and girls with disabilities: Integrating a human rights approach. Hobart: WWDA.
García-Moreno, C., Pallitto, C., Devries, K., Stöckl, H., Watts, C., & Abrahams, N. (2013). Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and nonpartner sexual violence. Geneva: WHO.
Goodfellow, J., & Camilleri, M. (2003). Beyond belief, beyond justice. Melbourne: Disability Discrimination Legal Centre.
Hague, G., Thiara, R., & Mullender, A. (2011). Disabled women and domestic violence: Making the links: A national UK study. Psychiatry, Psychology, and Law, 18(1), 117-136. doi: 10.1080/13218719.2010.509040
Healey, L. (2015). Violence against women with disabilities: Key findings from the Voices Against Violence research project. Paper presented at the Inaugural Asia-Pacific Conference on Gendered Violence & Violations. University of New South Wales, Sydney.
Healey, L., Howe, K., Humphreys, C., Jennings, C., & Julian, F. (2008). Building the evidence: A report on the status of policy and practice in responding to violence against women with disabilities in Victoria. Melbourne: Victorian Women with Disabilities Network Advocacy Information Service.
Healey, L., Humphreys, C., & Howe, K. (2013) Inclusive domestic violence standards. Strategies to improve interventions for women with disabilities? Violence and victims, 28(1), 50-68.
Houtenville, A.J. (2009). Counting working-age people with disabilities: What current data tells us and options for improvement. Kalamazoo: Upjohn Institute.
Hughes, R. B., Lund, E. M., Gabrielli, J., Powers, L. E., & Curry, M. A. (2011). Prevalence of interpersonal violence against community-living adults with disabilities: A literature review. Rehabilitation Psychology 56(4), 302-319. doi:10.1037/a0025620
Jones, L., Bellis, M. A., Wood, S., Hughes, K., McCoy, E., Eckley, L., Officer, A. (2012). Prevalence and risk of violence against children with disabilities: A systematic review and meta-analysis of observational studies. The Lancet, 380(9845), 899-907.
Levesque, J., Harris, M. F., & Russell, G. (2013). Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. International Journal for Equity in Health, 12(1), pp 171-182. doi:10.1186/1475-9276-12-18
Lund, E. M. (2011). Community-based services and interventions for adults with disabilities who have experienced interpersonal violence: A review of the literature. Trauma, Violence & Abuse, 12(4), 171-182. doi:10.1177/1524838011416377
Martin, S. L., Coyne-Beasley, T., Hoehn, M., Mathew, M., Runyan, C. W., Orton, S., & Royster, L.-A. (2009). Primary prevention of violence against women: Training needs of violence practitioners. Violence Against Women, 15(1), 44-56. doi:10.1177/1077801208327483
McCall, L. (2005). The complexity of intersectionality. Signs, 30(3), 1771-1800
McClain, L. (2011). Women, disability and violence: Strategies to increase physical and programmatic access to victim’s services for women with disabilities. Boise, Idaho: Center for Women’s Policy Studies, Boise State University
Mejias, N. J., Gill, C. J., & Shpigelman, C.-N. (2014). Influence of a support group for young women with disabilities on sense of belonging. Journal of Counseling Psychology, 6(2), 208-220. doi:10.1037/a0035462
Mikton, C., Maguire, H., & Shakespeare, T. (2014). A systematic review of the effectiveness of interventions to prevent and respond to violence against persons with disabilities. Journal of Interpersonal Violence, 29(17), 3207-3226. doi:10.1177/0886260514534530
Mikton, C., & Shakespeare, T. (2014). Introduction to special issue on violence against people with disability. Journal of Interpersonal Violence, 29(17), 3055-3062. doi:10.1177/088626051453453
National Council to Reduce Violence against Women and their Children. (2009). Background paper to time for action: The National Council’s plan for Australia to reduce violence against women and their children, 2009-2021. Canberra: FAHCSIA.
Ortoleva, S., & Lewis, A. (2012). Forgotten sisters—A report on violence against women with disabilities: An overview of its nature, scope, causes, and consequences. North Eastern University School of Law research paper No. 104-2012. Retrieved from https://papers.ssrn.com/sol3/Papers.cfm?abstract_id=2133332
Oxford Dictionaries. (n.d.) Access—definition of access in English. Retrieved from https://en.oxforddictionaries.com/definition/access
People with Disability Australia & Domestic Violence NSW. (2015). Women with disability and domestic and family violence: A guide for policy and procedure. Sydney PWDA & DVNSW.
Powers, L. E., Curry, M. A., Oschwald, M., Maley, S. (2002). Barriers and strategies in addressing abuse: A survey of disabled women’s experiences. Journal of Rehabilitation, 68(1), 4-13.
Powers, L. E., Renker, P., Robinson-Whelen, S., Oschwald, M., Hughes, R., Swank, P., & Curry, M. A. (2009). Interpersonal violence and women with disabilities: Analysis of safety promoting behaviors. Violence Against Women, 15(9), 1040-1069. doi:10.1177/1077801209340309
Robinson, S. (2013). Preventing emotional abuse and neglect of people with intellectual disability: Stopping insult and injury. London: Jessica Kingsley.
Robinson-Whelen, S., Hughes, R. B., Gabrielli, J., Lund, E. M., Abramson, W., & Swank, P. R. (2014). A safety awareness program for women with diverse disabilities: A randomized controlled trial. Violence Against Women, 20(7), 846-868. doi:10.1177/1077801214543387
Sexual Crimes Act 2006 (Vic). Retrieved from https://www.austlii.edu.au/au/legis/vic/num_act/coa20062o2006269/
Smith, N., & Harrell, S. (2011). Forging new collaborations: A guide for rape crisis, domestic violence, and disability organizations. New York: Vera Institute of Justice.
Victorian Law Reform Commission. (2004). Sexual offences final report. Retrieved May 16, 2016 from https://www.lawreform.vic.gov.au/sites/default/files/FinalReport_0.pdf
Women With Disabilities Australia. (n.d.) Stop the violence resource compendium. Retrieved January 10, 2017 from https://www.stvp.org.au/Resource-Compendium.html
Women With Disabilities Australia. (2013) Background paper. National symposium on violence against women and girls with disabilities. Hobart: WWDA
Woodlock, D., Healey, L., Howe, K., McGuire, M., Geddes, V., & Granek, S. (2014). Voices against violence: Paper one: Summary report and recommendations. Melbourne: WWDV.
World Health Organization. (2002). World report on violence and health. Geneva: WHO.
World Health Organization. (2011a). International classification of functioning, disability, and health. Retrieved from https://www.who.int/classifications/icf/en/
World Health Organization. (2011b). Summary: World report on disability. Malta: WHO. Retrieved October 12, 2016 from https://apps.who.int/iris/bitstream/10665/70670/1/WHO_NMH_VIP_11.01_eng.pdf
Appendix A: participant information and recruitment
Plain language statement: women with disabilities
What does it take? Making services accessible to women and girls with disability who experience sexual assault and/or domestic violence
Hello,
[Insert photo]
My name is [name]. I am a researcher at [university].
I am doing a project about improving violence and abuse services for women with disability in Australia. I am working with [authors].
We want to know about what services women with disability who have experienced violence and abuse get. We want to learn what works and what needs to be improved. We hope this will help us to improve violence and abuse services for women with disability in Australia.
We are inviting women with disabilities to talk to us in either an interview or a focus group. We are talking to women with disabilities who have used services like counselling, accommodation and other services to talk about and get help after the violence has happened.
You can choose to have an individual interview with me or you can talk in a group with other women with disabilities. This is called a focus group. The interviews and focus groups will take about the same amount of time, around one hour.
If you do an interview or participate in a focus group what we talk about will be recorded using a digital recorder. Only the researchers and a person employed by the University to write the notes from these recordings will hear what we talk about.
Some of the questions might be:
How did you find out about the service? Did you know why you were going there? How did they explain this to you?
Was it easy to get to?
What was it like there? Can you describe what it was like when you got there and while you were there?
Describe the way the service worked with you. What did you do? How often did you go? Did you see the same person each time?
What is the best thing about the service?
Were there any things that weren’t so good?
What are some ways this service could be better for women with disabilities?
How could the service be improved?
There are other parts to this research. There will be some groups formed of people who work in services, women and girls with disabilities and people from other organisations who are interested in improving these services. If one of these is in your area you might be invited to join that group too.
When all of the research has been done there will be two reports written: one short report and one longer report. We will also be writing some articles for journals and presenting at conferences. Your name or any way of recognising you will not be in the reports, the presentations or anything else we say about the research.
The only time we would tell someone else about what you tell us is if we are worried that a child might be hurt in the past or the future, or if we are worried that you might hurt yourself or someone else.
Participating in this project is up to you, and if you do but then you change your mind about it later, that is ok too. You just have to tell the researchers and you don’t have to explain why. We will take the things you said out of the information we gather.
This research has been approved by the Human Research and Ethics Committee of Deakin University. If you have any complaints about the research or how we are doing it, or if you want to ask questions about your rights in the research, the person to contact is: The Manager, Office of Research Integrity, Deakin University, 221 Burwood Highway, Burwood Victoria, 3125, Telephone 9251 7129, Facsimile: 9244 6581; research-ethics@deakin.edu.au.
We know that talking about the way you got support and help after you experienced sexual assault or other abuse will be hard for you and might bring up bad memories. We will be giving you the support you need to manage this if it happens while we are talking to you or after you have talked to us.
Thank you for thinking about being involved. If you want to take part, you can say yes on the form attached to this letter. Or, you can talk it over with someone who might help you make up your mind. If you need some more information you can contact me these ways:
Contact Details
Phone
Email
Endnotes
- Sections of the introduction also appear in the publication Frawley, P., Dyson, S., Robinson, S., & Dixon J. (2015). What does it take? Developing informed and effective tertiary responses to violence and abuse of women with disabilities in Australia. (Landscapes, 03/2017). Sydney: ANROWS ↑
- Under the National Affordable Housing Agreement. https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/BudgetReview201516/DV ↑
- This section includes material published in Frawley, P., Dyson, S., Robinson, S., & Dixon J. (2015) What does it take? Developing informed and effective tertiary responses to violence and abuse of women with disabilities in Australia (ANROWS Landscapes, 03/2015). Sydney: ANROWS. ↑
- The “bio-psycho-social” model suggests that disability or illness is due to an interaction of biological, psychological, and social factors. ↑
- “Gatekeeping” is a term used to describe the phenomenon of services excluding women with disabilities or denying them information in order to “protect them” (Frawley et al., 2012). In disability research, proxies are sometimes used to speak on behalf of people with disabilities, a process that has been labelled biased (e.g., see Houtenville, 2009). ↑
Research report | July 2017
Issue 05 | 2017
Read the PDF version of the report
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
Acknowledgement of Country
ANROWS acknowledges the traditional owners of the land across Australia on which we work and live. We pay our respects to Aboriginal and Torres Strait Islander elders past, present and future; and we value Aboriginal and Torres Strait Islander history, culture and knowledge.
© ANROWS 2017
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW, 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
Whatever it takes? Access for women with disabilities to domestic and family violence services: Final report / Patsie Frawley, Sue Dyson, and Sally Robinson.
Sydney: ANROWS, c2017.
Pages ; 30 cm. (ANROWS Horizons, Issue 05/2017)
I. Victims of family violence – Australia. II. Women with disabilities – Services for – Australia. III. Domestic violence – Australia. IV. Abused women – Services for.
I. Dyson, Sue. II. Frawley, Patsie. III. Robinson, Sally.
ISSN: 2205-8907 (print) 2205-8923 (online)
ISBN: 978-1-925372-56-4 (print) 978-1-925372-57-1 (online)
Creative Commons Licence
Attribution Non-Commercial
CC BY-NC
This licence lets others distribute, remix and build upon the work, but only if it is for non-commercial purposes and they credit the original creator/s (and any other nominated parties). They do not have to license their Derivative Works on the same terms.
Version 3.0 (CC Australia ported licence): View CC BY-NC Australia Licence Deed | View CC BY-NC 3.0 Australia Legal Code
Version 4.0 (international licence): View CC BY-NC 4.0 Licence Deed | View CC BY-NC 4.0 Legal Code
Deakin University Australia
Geelong Waterfront, 1 Gheringhap Street, Geelong, Victoria 3220 Australia
“Whatever it takes”: Access for women with disabilities to domestic and family violence services: Final report
Prepared by:
Adjunct Associate Professor Sue Dyson, Principal Research Fellow, Australian Research Centre in Sex, Health, and Society, La Trobe University
Dr Patsie Frawley, Senior Lecturer in Disability and Inclusion, Deakin University
Dr Sally Robinson, Senior Research Fellow, Southern Cross University
The authors would like to acknowledge the work of Amie O’Shea, who was employed as a research assistant for the program. They would also like to acknowledge the work of the Consultative Research Group, advisory group, and research partners for their participation in the program and for their timely and important input. The authors would also like to acknowledge the women with disabilities who participated in the research in focus groups and interviews. Thank you for sharing your stories and experiences.
This work is part of the ANROWS Horizons series. ANROWS Horizons (research reports) are in-depth reports on empirical research produced under ANROWS’s research program.
This report addresses work covered in the ANROWS research project 3.4 “What does it take? Developing informed and effective tertiary responses to violence and abuse for women and girls with disabilities in Australia”. Please consult the ANROWS website for more information on this project. In addition to this report, ANROWS Landscapes and ANROWS Compass papers are available as part of this project.
Suggested citation:
Dyson, S., Frawley, P., & Robinson, S. (2017). “Whatever it takes”: Access for women with disabilities to domestic and domestic violence services: Research report (ANROWS Horizons, 05/2017). Sydney: ANROWS.
Contents
Tertiary responses to violence against women with disabilities
Effectiveness of tertiary response services for women with disabilities
Principles of good practice in tertiary response services for women with disabilities
Research and advisory structure
Women’s experiences using services
Specialist crisis response services
Improving response services for women with disabilities
Conclusions and recommendations
Project limitations and strengths
Appendix A: participant information and recruitment
Plain language statement: women with disabilities
Executive summary
Project aim
This research aimed to inform the development of guidelines for tertiary response services to respond effectively to the needs of women with disabilities.
Method
The mixed methods project surveyed tertiary women’s services in Australia to understand the models and approaches that are currently used to provide support to women with disabilities. Following this, five sites were recruited for qualitative research to develop a more nuanced picture of how the services work. Two of these were identified because they are specialist service models working specifically with women with disabilities and demonstrate promising practice. Case studies were developed to understand what could be learned from their approach. Three more sites were selected as case studies. A two-step process was used to select sites: (a) expression of interest by services in survey response, and (b) follow up discussions with these sites and short listing by researchers. Interviews were conducted with managers and staff; interviews and focus groups were conducted with women with disabilities; and two sites undertook a more comprehensive action research process to learn from the research and plan service improvement.
Data analysis
One hundred and thirty-eight valid responses were received to the survey. Data were analysed using SPSS Statistics V21 for basic statistical analysis, including frequencies of responses, cross tabulations, and descriptive statistics. An inductive approach was taken to analysis of the qualitative data, including interview, focus group, and action research data, which were analysed using QSR NVivo 10. Transcripts were closely read by each of the researchers. Initial themes and interpretations were reviewed by the research team (consisting of the three lead researchers from Deakin University, La Trobe University, and Southern Cross University) in telephone meetings and in a full-day workshop.
Findings
Accessibility requires more than physically modified accommodation or providing interpreters for people with sensory impairments. Access must be understood to include: how services think about disability (described as attitudinal factors), how information about services is made available, and going beyond the development of procedural access plans as required by the Disability Discrimination Act 1992 (Cth). Women with disabilities who participated in the research provided insights drawn from their experiences that suggest a need to extend the definition of “access” to include appropriateness, approachability, and acceptability as core components. By addressing broader issues of access in addition to disability-specific needs (such as the way information is provided to meet broad information access needs), the interface between what services offer and what women with disabilities need can be better aligned.
Many women who come to tertiary response services for support have disabilities. However, their disabilities may not be “officially” recognised for a variety of reasons: some have disabilities as a direct result of living with sustained violence and some are not easily identified because they are compounded by other life experiences. Tertiary response services are not experts in disability and meeting some women’s specific access needs can be challenging. A “clash of cultures” between tertiary response services and other services that support women with disabilities was identified that hampered collaboration. High-quality collaboration between tertiary response services and disability services can overcome some of the challenges identified.
At times, agencies providing services to women with disabilities who have experienced violence tended to act in ways that sought to “protect them” from further re-traumatising, which led to less rather than more access to supports and services. From the perspective of some of these women, the result was that they had been denied information, had not had their experience acknowledged, or had missed out on having contact with other women in similar positions to share experiences and get support. In the effort to protect women with disabilities, often their ideas and opinions about service improvements were not sought or heard.
Work undertaken in the case study sites in the action research phase demonstrated how service improvements and cross-sector collaboration could be incorporated into practice through reflection and facilitated planning processes. Rather than simply referring women with disabilities to disability services for support, a process of collaborating and engaging with disability services (rather than handing over to them) was developed. This established continuous improvement and cross-sector collaboration as underpinning principles for working with women with disabilities. Other key findings included that a one-size-fits-all approach does not meet all access needs; adequate time for counselling, case management, and consultation must be permitted to meet individual needs; and that women value relationships with workers that involve trust and taking as much time as is needed. Finally, many women seek social support from others who have had similar experiences.
Recommendations
At the time of completing this report, the Third Action Plan 2016-2019 of the National Plan to Reduce Violence against Women and their Children 2010-2022 (“Third Action Plan”) was released by the Commonwealth, state, and territory Governments (Department of Social Services, 2016). Women with disabilities are identified as a priority group in the Third Action Plan. This research supports the key national actions for women with disabilities identified in the Third Action Plan and contributes evidence to inform its implementation. A number of promising practices were identified from this research which can be articulated as underpinning principles for effective practice. These include:
- “Accessibility” is more than providing physical access: services must be approachable, acceptable, appropriate, affordable, and available to women with disabilities.
- Women with disabilities, like all people, experience complexity in their lives and are multi-dimensional; disability is in play with other personal and social factors. Service planning and delivery must be enhanced by the use of an intersectional lens.
- Women with disabilities need more than a focus on personal safety skills; they need social and relational support in a safe and inclusive environment.
- Service and practice planning, development, and improvement must be informed by high-quality data collection and qualitative and quantitative research. This must also be informed by the ideas and opinions of women with disabilities who have used the service.
- All aspects of tertiary response services for women with disabilities must be informed and enhanced by cross-sector collaboration.
Recommendation 1: promoting access and accessibility
Services should review their understanding of “disability” and “access” and draw on the evidence from this research and the work of Levesque et al. (2013) to ensure that they provide services that are:
- Approachable: women with disabilities know they exist and feel comfortable with approaching them.
- Acceptable and appropriate:barriers ton communication, housing, and understanding what is offered are removed.
- Affordable and available.
Recommendation 2: building cross-sector collaboration
In order to support initiatives for cross-sector collaboration, the emerging models of promising practice identified in this research should be further developed and informed using a facilitated process of reflection, consultation and engagement with other tertiary response services.
This process should aim to ensure positive outcomes for women with disabilities in all parts of the tertiary response sector through collaboration. It should not be in the form of didactic training, but use a facilitated process that involves and is informed by women with disabilities.
Recommendation 3: involving women with disabilities
Domestic and family violence (DFV) services should consider establishing peer support groups for women who survived or are escaping from violent and abusive relationships.
Service improvement and cross-sector collaboration must be informed by women with disabilities who have used tertiary response services. Women with disabilities should be consulted about their experiences using tertiary response services and their advice incorporated into planning and practice development.
The Consultative Research Group model, which ensured that the voices of women with disabilities informed this research, should be used in work with future sites to contribute to both service and sector-wide reform.
Recommendation 4: high-quality data collection
DFV services should collect data on the disability experiences of clients. Qualitative and quantitative data measures across all programs offered in DFV services should be developed and implemented, and tied to the same measurement and reporting metrics for other demographic characteristics (e.g. age, Indigenous status, and so on). Women with disabilities should be involved in providing qualitative data and be engaged to co-produce information from it that can be used in service improvement and wider sectoral reform at local, state or territory, and national levels.
Introduction
Gender-based violence is a problem of global proportions. Internationally, 30 percent of women have experienced physical or sexual intimate partner violence and 7 percent have been sexually assaulted by someone other than a partner (García-Moreno et al., 2013).[1] In Australia, the issue has been identified as a public health problem that is prevalent, serious, and preventable (Ayre, Lum On, Webster, Gourley, & Moon, 2016) and considerable work has been undertaken in recent decades to respond to and prevent intimate partner violence and sexual assault. Australian data demonstrates that “nearly one in three women over the age of 15 years have been subjected to physical violence and one in five report having experienced sexual violence at some time in their lives” (Australian Bureau of Statistics, 2012). What is less well understood is how women with disabilities fare in tertiary response services funded to provide safety and support for women escaping family violence.
Women with disabilities who have experienced violence seek help and support from tertiary response services for similar reasons that other women (or non-disabled women) do, including family and intimate partner abuse, sexual harassment and assault, coercive control, and stalking. However, women with disabilities also experience abuse related to their disabilities, including institutional violence, such as forced or coerced contraception, sterilisation, and psychiatric interventions; withholding of or forced medication; violations of privacy; deprivation of liberty; and denial of provision of essential care (Chenoweth, 1996; Dowse, Soldatic, Didi, van Toorn, & Frohmader, 2013; Frohmader, 2010).
Gender inequality is at the root of gender-based violence. However, violence against women is not limited to any particular group or class in society. Gender intersects with other forms of difference to compound discrimination, which in turn affects experiences of violence and abuse for individuals. The complexity of lived experience is very much dependent on factors such as age, class, culture, Indigenous status, intersex status, race, religion, sexuality, and so on, in addition to gender and disabilities. These factors also differ across time, according to geographic location, and are not the same for everyone. Taking account of these differences has been theorised as “intersectionality” (McCall, 2005). Understanding how these intersecting forms of difference affect access is particularly relevant for tertiary response services (Ortoleva & Lewis, 2012).
Between 2015 and 2016, the What does it take? research project was carried out to understand the ways in which services responding to the safety needs of women who have experienced family violence or sexual assault are accessible to women with disabilities. The project aimed to develop new knowledge to inform the development of guidelines for tertiary response services to respond effectively to the needs of women with disabilities in Australia. These guidelines aimed to be:
- based on a thorough and critical review of evidence concerning world best practice;
- informed by the experiences of Australian women with disabilities;
- developed in collaboration with locally based cross-sector communities of practice; and
- designed to inform a gendered understanding about violence in the disability sector.
This report details the findings of that research. It starts with a summary of international and Australian literature published in 2015 as an ANROWS state of knowledge report (Frawley, Dyson, Robinson, & Dixon, 2015). Following the summary literature review, this report details the project methodology, the qualitative and quantitative research findings, and concludes with discussion about the implications of this research for practice and for future research.
A note on language
This project sought to identify how women with disabilities who have experienced violence fare in tertiary response services. “Tertiary response services” is a broad term that encompasses a wide range of services aimed at ensuring safety and support after violence has occurred, including first responders, such as emergency and crisis services, as well as legal, health, and medical services. The scope of tertiary response services is detailed below in the literature review. The focus of the research has been on crisis response services, sometimes called domestic violence, sexual assault, or family violence services or women’s refuges. The Commonwealth funds these services under the National Partnership Agreement on Homelessness and they are administered by the states and territories.[2] There are some differences between states in terms of approaches and language used. For clarity, crisis response services responsible for ensuring women’s safe housing are referred to as “domestic or family violence response services” (shortened to DFV services). When the wider tertiary response system is implicated, the term “tertiary response services” is used.
Literature review
A literature review was carried out to establish the current state of knowledge concerning models of tertiary response services for women with disabilities who have experienced family or domestic violence or sexual abuse. Although literature reviews commonly focus on published, peer reviewed literature reported in high-quality academic journals, a comprehensive search of such databases revealed limited results to answer the following literature search questions:
- What models and approaches have been used in Australia and internationally for tertiary responses to violence and abuse for women with disabilities?
- What does the evidence say about effective models?
Although academic research was limited, many community, advocacy, and activist reports and monographs were found. As a result, this “grey literature” was included in the review, as it offered a rich source of evidence concerning the literature search questions. Therefore, in this review we have drawn on both academic and grey literature from sources we judged to be reliable.[3]
Disability research
Around one in five people in Australia report having a disability (Australian Bureau of Statistics, 2011). Of these, almost 6 percent have a severe or profound level of disability. Definitions of “disability” differ, although increasingly the World Health Organization’s (WHO) International classification of functioning, disability, and health’s (ICF) “bio-psycho-social” definitions are used (World Health Organization, 2011a).[4] Drawing on the ICF, disability can be understood as complex, dynamic, multi-dimensional, and contested (WHO, 2011a). The ICF asserts that the experience of disability should be mainstreamed and that it should be recognised as a universal human experience, as all humans can experience “a decrement in health and thereby experience some disability” (WHO, 2011a, p. 3). This multi-dimensional, “mainstreamed” definition of disability is informed by critical theorising about disability and the grassroots advocacy of people with disabilities over at least the past three decades.
Despite the high rates of violence and abuse reported in the international peer-reviewed and local grey literature, research about effective prevention and response is lacking (Lund, 2011; Mikton, Maguire, & Shakespeare, 2014). The WHO advocates an approach to violence against women that is based on a public health model of disease prevention. This model has been adopted by the Commonwealth of Australia and underpins its responses to the prevention of violence against women.
In this three level model, primary prevention aims to prevent violence from occurring through attitude and behaviour change; secondary responses provide early intervention (e.g. with perpetrators), and tertiary responses ensure safety and support for women after violence has occurred. In addition to responding to the immediate safety and support needs of women who have been affected by violence, tertiary responses also aim to minimise the impact of violence and prevent ongoing negative consequences and repeat events (Flood, 2011; Martin et al., 2009; World Health Organization, 2002). Each of these approaches is more complex than this explanation,; however the focus of this review is on tertiary responses and thus we go into no further detail about primary prevention or secondary responses.
The public health model of prevention is central to the Australian Government’s National Plan to Reduce Violence against Women and their Children 2010-2022 (National Council to Reduce Violence against Women and their Children, 2009; Council of Australian Governments, 2012). A significant body of primary prevention, and evidence-based knowledge and practice has been developed as a result of this plan (COAG, 2012). However, there is less evidence available concerning the most effective and appropriate immediate tertiary responses needed for women who have experienced violence, for both the general population and minority groups, including women with disabilities (Healey, Humphreys, & Howe, 2013).
To be effective, immediate tertiary interventions require a rapid, coordinated response that ideally encompasses the range of services needed by victims/survivors. In the immediate term, this may include policing, medical care for physical injuries, safety planning, advocacy, legal services, and family or domestic violence response services. In the medium to longer term, this includes services such as trauma counselling, support groups, employment assistance, transitional housing, children’s services, and specialist support and advocacy services.
Women with disabilities experience issues with accessing sexual assault and domestic violence services (Dowse et al., 2013; Healey et al., 2013; Healey, Howe, Humphreys, Jennings, & Julian, 2008; Woodlock et al., 2014). In the disability sector, lack of awareness about family violence and other forms of violence against women compounds the problem of access to safety and support for women with disabilities (Mikton & Shakespeare, 2014). It has been argued that despite the public health approach to understanding disability and a rights-based approach to promoting equality to prevent violence against women, to date, there has been little attention paid to the intersection of the two fields of disability and domestic and family violence (Mikton et al., 2014).
Tertiary responses to violence against women with disabilities
International and domestic anti-discrimination legislation requires all community services and facilities to be “accessible”, with standards and guidelines that articulate what this means in given situations (Australian Human Rights Commission, n.d.). People with disabilities should not experience discrimination or exclusion due to their experience of disability. Australia’s disability discrimination legislation provides the legal framework for equality for people with disabilities and for addressing discrimination. It also includes provisions for providers to argue that they cannot meet these legislative responsibilities because of “unjustifiable hardship”. This means that while the expectation is one of “universal access”, the reality is that access is frequently limited or non-existent as a result of weighing up the costs and barriers to providing access (Frawley et al., 2015).
Access for people with different experiences of disability is complex and multidimensional. To understand access requires an understanding of how disability is experienced and how the experience of disability is impacted by intersecting forms of difference. Despite this, there is an ideal of universal access that has been developed, particularly in relation to the built environment. Guidelines for physical access in building standards have been established and, in some countries, anti-discrimination legislation dictates the legal framework for determining what “access” means. In the United States, research has been undertaken on the extent to which domestic violence and sexual assault services comply with access legislation and has found considerable variability in physical accessibility (Chang et al., 2003; Frantz, Carey, & Bryen, 2006). Frantz et al. (2006) reported that while 87 percent of services in their survey said that they were able to provide services to all clients with disabilities who requested them, all fell short of actually doing so. Similarly, a study in the United Kingdom found that 76 percent of domestic violence services surveyed did not comply with the Equality Act 2010 (UK) (Hague, Thiara, & Mullender, 2011). Those researchers noted that disability access had been narrowly defined as “wheelchair access” in some services.
Tertiary response services are always under pressure from the sheer numbers of women requiring services and from limited (and diminishing) funding. Research with service managers found that (a lack of) funding and the need to prioritise budget expenditure to support physical access were key barriers to developing fully accessible services (Chang et al., 2003; Frantz et al., 2006; Healey et al., 2013; McClain, 2011).
Access and inclusion
In Australia, the disability advocacy sector and the domestic violence sector collaborated to develop a resource for tertiary response services to facilitate access for women with disabilities (People with Disabilities Australia & Domestic Violence NSW, 2015). This resource calls for existing services to go beyond the procedural requirements of the Disability Discrimination Act 1992 (Cth). The authors argue that no single change will make services more accessible and that specialist accommodation, programs, and supports targeted at women with disabilities need to be developed. The report has a significant focus on organisational change and readiness, highlighting the need for organisation-wide training that is underpinned by inclusive policies, and further argues that services must look broadly at what “access” means. Practical guidance on addressing physical access, information access, attitudinal access, and procedural access is incorporated in the resource. Similarly, Women with Disabilities Australia (WWDA) call for a broader human rights approach to recognising and responding to violence and abuse (WWDA, 2013). A human rights approach, they argue, acknowledges the need to address social structures that create barriers to equality and therefore have an impact on the incidence, prevalence, and severity of abuse and on approaches to preventing and responding to violence and abuse for women with disabilities in Australia.
The term “programmatic access” has been used in research and policy to cover all aspects of service responses that relate to working with women with disabilities. This covers approaches used from intake through to counselling and outreach, and includes service policies and staff training (Frantz et al., 2006). Frohmader, Dowse, and Didi (2015) argue that programmatic access should incorporate both procedural and attitudinal components. Frantz et al. (2006) tested programmatic access in their research and reported that only 57 percent of services asked at intake if people required accessible accommodation or adaptations to the way services were provided.
Chang et al. (2003) found that while the vast majority of organisations reported that they provided services for women with disabilities, many had difficulty providing “full services” (meaning all aspects of the service that other women could use). Notably, only partial access to outreach and counselling was reported. In a UK study by Hague et al. (2011), only 38 percent of domestic violence organisations were able to provide an accessible service (with physical access being used as the measure of access). Provision of accessible transport and accommodation was the focus of these services.
Staff training and organisational policy to address skills and attitudes to access and inclusion were reported in the literature as key factors in addressing programmatic access, yet not all services provided such training or had these policies. In one study, staff members’ lack of knowledge and understanding about the needs of women with disabilities led to feelings of trepidation, anxiety, and concern when faced with providing services to women with disabilities (Hague et al., 2011). Frantz et al. (2006) found that while over a third of services reported having training for staff and volunteers, only 9 percent had training for board members. Despite the call for staff training, no studies were found that assessed the outcomes of training or policy on practice. In Australia, Healey et al. (2013; Healey, 2015) argued that services lack a focus on inclusion policies for women with disabilities.
Recognising and responding to the breadth of needs and experiences of women with disabilities who experience violence and abuse can present challenges for service providers. Research in the United States that investigated the experiences of women with disabilities who accessed tertiary response services found that women with an intellectual disability and those with mental illness were the most represented groups (Chang et al., 2003; Frantz et al., 2006). Both of these studies reported that women with significant communication disabilities (including those with hearing impairments), women who used augmented communication devices, and women with other communication needs associated with speech and learning represented a small number of overall clients. For these women, barriers included lack of access to staff with specialist skills to support effective communication, or staff members’ lack of knowledge about how to engage with women with significant communication disabilities. Cost was cited as a barrier to accessing specialist communication supports and services for these women (Chang et al., 2003).
The reported incidence of violence and abuse of women with disabilities is likely to be lower than the actual incidence as a result of a number of complex factors to do with reporting and data collection (Dowse, Soldatic, Spangaro, & van Toorn, 2016; Dowse et al., 2013; Hughes, Lund, Gabrielli, Powers, & Curry, 2011; Jones et al., 2012; Lund, 2011; Mikton et al., 2014). In Australia, Healey et al. (2013) found a lack of policies and standards concerning data collection about disabilities by family violence services. This lack of data collection keeps disability invisible in services, hiding the need for services to address physical and programmatic access for women with disabilities.
The evaluation of the Safer and Stronger Program violence prevention program in the United States reported that women with disabilities were more likely to first reach out to someone they know and trust, such as a friend or a family member, rather than a domestic violence service (Powers et al., 2009). This is consistent with reports by women more broadly, as reported, for example, in the ABS Personal Safety Survey (ABS, 2012). Participants that faced multiple types of abuse, such as physical, sexual, and emotional abuse, were more likely to have sought education and knowledge about abuse compared to those with little or no experiences of abuse.
Collaborations and partnerships
Cross-sector collaborations between the disability and domestic violence sectors were highlighted as an important factor for more effective outcomes for women with disabilities in much of the literature (Chang et al., 2003; Healey et al., 2008; McClain, 2011). Despite this, cross-sector collaboration is reported to be low. A survey of UK disability and domestic violence services found that only 6 percent of the disability services surveyed had attended locally provided, multi-agency, domestic violence training (Hague et al., 2011). Similarly, research in the United States that studied interagency collaboration in the provision of domestic violence services to women with disabilities found that, despite agencies believing they collaborated well, women with disabilities reported frustration and anger at what they saw as a total lack of collaboration (McClain, 2011).
Effective service delivery for women with disabilities requires that both the disability and the DFV response sectors should focus on and prioritise responses to violence against women with disabilities. In Canada, a survey of 579 disability centres found that very few provided staff training about domestic violence or advocated for improved access to these services (Ballan & Freyer, 2012). In the United Kingdom, a study of interagency collaboration found that while agencies had strategies in place that included cross-training and cross-referral systems, as well as policies and funded activities to bring the sectors together, where interagency collaboration existed, it was difficult to sustain (McClain, 2011).
In the United States, collaborative efforts to improve services for women with disabilities have helped to change the ways in which services interact both with women with disabilities and with each other (Smith & Harrell, 2011). The key factors for effectiveness were identified as: the environment in which the collaboration exists, its purpose, the characteristics of the organisations and people involved, the process and structure of the collaborators’ work, the quality and frequency of their communication, and the resources available. Similarly, in Australia, Women with Disabilities Australia, through the Stop the Violence project, developed a resource compendium that recommended adopting a human rights approach that consists of the following principles: empowerment through participation, removing barriers, working in partnership, building capacity, building and using an evidence base, preventing violence before it occurs, and promoting leadership and advocacy. (WWDA, n.d.). These are supported by a number of strategies, such as providing appropriate accessibility, ensuring transferable and open communication, creating inclusivity and equality for all stakeholders, and guaranteeing that clear accountabilities are agreed upon before program development and implementation (Dowse et al., 2013).
Sexual assault services in Victoria have focused on providing services for people with disabilities who are victims or survivors of sexual violence for almost 2 decades, with cross-sector collaboration including staff training in both sectors being a key component (Frawley, 1997, 2000). One service, South Eastern Centre Against Sexual Assault (SECASA), developed the Making Rights Reality program, with support from the Federation of Community Legal Services, the Office of the Public Advocate, Victoria Police, Springvale Monash Legal Service, and Women with Disabilities Victoria (Frawley, 2014). This program provides enhanced legal advocacy and counselling services to victims/survivors with cognitive impairments.
Making Rights Reality addresses cross-sector collaboration in a number of ways: through disability training for sexual assault service staff, by engaging with the disability sector to develop Easy English resources about sexual assault, and through involvement of the disability project worker on advisory groups for projects involving women with disabilities. Evaluation of the program indicated that 40 percent of referrals to the program came from disability organisations and the police (Frawley, 2014). The number of people with disabilities using SECASA increased over the 2-year period of the pilot project, and clients received access to Victims of Crime Compensation through the legal advocacy component of the program (Frawley, 2014).
Effectiveness of tertiary response services for women with disabilities
“Effectiveness” can be defined as the degree to which something is successful in producing a desired result. To provide effective tertiary response services for women with disabilities who have experienced violence, first clarity is needed about which results are desired. A search of the academic literature reveals that very little is known about how effective tertiary response services are for women with disabilities. A systematic review of effective interventions to prevent and respond to violence against persons with disabilities reported that there remains a dearth of literature on the effectiveness of interventions and that most evaluations are not rigorously executed (Mikton, Maguire, & Shakespeare, 2014). According to these authors, this makes it difficult for policy-makers and practitioners to make informed decisions about which model and approach would be the most effective.
One of the key themes of the literature review was that women with disabilities who had experienced high levels of abuse across a number of different areas dealt with safety-promoting behaviours very differently to those who had experienced little or no abuse. What became apparent is that just as experiences of violence and abuse are different for each person, so too are the personal responses and needs for each person. Some women require more integrated levels of support and service provision, while others require more preventative levels of support (Powers et al., 2009).
Evaluation of an Australian program called A Safety Awareness Program for Women with Disabilities (ASAP) found that overall the program was effective on a number of qualitative measures (Hughes et al., 2011), including:
- ASAP was effective in educating women with disabilities at risk of abuse, as well as those who had already experienced abuse.
- The program engaged women who had previously experienced abuse and violence and found that those who had experienced the most abuse were more likely to have greater gains in safety self-efficacy after completing ASAP.
- Participation in the program greatly improved the protective factors for women with disabilities.
- Participants responded positively to the classes and found the learning materials to be engaging and effective at helping them learn safety-promoting behaviours.
- The program was regarded as being easily accessible, relevant to, and feasible for participants (Robinson-Whelen et al., 2014).
ASAP is an education program rather than an immediate support service. There are, however, some lessons that can be learned from such a program for the development of guidelines for tertiary response services for women with disabilities, in particular the approach used to make information accessible.
A key factor that is noted in the broader literature is the importance of interagency collaboration. The literature that addresses the question of effectiveness also notes the importance of interagency collaboration and highlights the importance of this collaboration being supported by a broader authorising environment for prevention and intervention (such as support from the national and state governments). This can be accomplished by improving responses to services for women with disabilities in abusive and violent situations, such as enhancing crisis response services that are specifically designed for women with disabilities and for their children if required (Woodlock et al., 2014). One of the most crucial aspects of a successful program is the expertise of staff (Babic, 2009; Hague et al., 2011; Hughes et al., 2011).
A study of service collaboration in the United States reported that little research had focused on how effectiveness is understood or measured in tertiary response services (McClain, 2011). This suggests there is a gap in the research about what characterises and determines effectiveness of tertiary response services from the perspective of women with disabilities (McClain, 2011). The following actions were recommended to ensure effective interagency collaboration:
- Employ an outside facilitator who can broker communication and agreement between service providers and women with disabilities. This can be achieved by laying down the foundations of what the collaboration is trying to achieve; sharing philosophies; building common definitions of “abuse”, “domestic violence”, “disability”, and “accessibility”; and clarifying expectations of women with disabilities.
- Develop awareness in the community and train staff in DFV services and disability services on the intersections of gender, violence, and disability.
- Develop policies, procedures, and budgets that specifically include the provision of services to women with disabilities who are victims/survivors of domestic violence/sexual assault.
- Create welcoming environments for victims/survivors with disabilities (McClain, 2011).
Principles of good practice in tertiary response services for women with disabilities
The literature review sought to identify tertiary response approaches for providing services to women with disabilities, and gain an understanding of how these approaches have been implemented (process) and the extent to which they are effective (outcomes). While the review resulted in some insights about factors that need to be considered in developing services that are responsive to the needs of women with disabilities, very few actual models of tertiary responses were identified. As a result, the review was better able to identify principles of good practice rather than complete models. Three key factors stand out as important for effective tertiary response services: physical and programmatic accessibility, cross-sector collaboration, and evidence-based practices. Two reports in the literature provided key approaches to addressing these factors.
Healey et al. (2013) developed guidelines to assess the inclusiveness of domestic violence standards that are based on current understandings about best practice, which include:
- Use the voices of women with disabilities to inform policy and practice.
- Collect disability data.
- Provide evidence that the service meets physical access standards (of all disabilities), as well as programmatic access though use of accessible information and approaches, in order to be eligible for funding.
- Provide evidence-based and rigorously-reviewed therapeutic and educational services.
- Engage in cross-sector collaborations.
- Be based on an intersectional, human rights framework.
- Underpin the services’ programs, approaches, and workforce development with these principles.
The Stop the Violence project in Australia proposed the following principles that need to underpin practice to prevent violence in the broader community, in disability services, and to inform DFV service responses:
- Adopt a human rights approach.
- Promote empowerment through participation.
- Remove barriers.
- Work in partnership.
- Build capacity.
- Build and use the evidence base.
- Prevent violence before it occurs.
- Promote leadership and advocacy.
- Provide appropriate accessibility.
- Ensure transferable and open communication.
- Create inclusivity and equality for all stakeholders.
- Guarantee that clear accountabilities are agreed upon before program development and implementation (Dowse et al., 2013)
Discussion
A key finding of this review is that effective, accessible services for women with disabilities must be built on multi-agency collaborations. Research in the United States suggests that collaboration must be based on having a clear purpose understood by all parties and developed within an environment conducive to the active and productive engagement of all parties. Other factors include the quality and frequency of communication and the existence of supportive resources (Smith & Harrell, 2011). Added to this, tertiary response services must engage women with disabilities as partners in the planning and strategic stages of service development, as they are the experts in their own lives and contribute a crucial perspective on appropriate services and support needs for women with disabilities (Healey et al., 2013). Effective collaborations must also be well-managed, and this requires substantial efforts from affiliated agencies and stakeholders that are not driven by financial gain or funding obligations but by a genuine desire to challenge existing barriers and make firm cultural and community change. Well-functioning collaborations must address access issues relating to multiple disabilities and intersectional characteristics (Dowse et al., 2013).
Some researchers advocate that educating women with disabilities on the behaviours that constitute gender-based violence and how to escape if it happens will increase their access to tertiary response services (e.g., Powers et al., 2009). However, current research is unable to identify whether there is a link between increased knowledge and an increase in reporting abuse.
High-quality data collection processes must be based on a well-developed understanding of disability, intersectionality, and accessibility so that women with disabilities using the service can shape responses. These data must in turn be analysed and used in the development of policies and practices that take account of the needs and experiences of women with disabilities, as well as informing systemic and individual advocacy processes.
A central tenet of effective tertiary response services for women with disabilities concerns empowerment and the need for those who use services to exercise agency in all aspects of the service experience. The perspectives of women with disabilities must increasingly inform both disability and tertiary response service delivery (Frawley, Barrett, & Dyson, 2012; Powers, Curry, Oschwald, & Maley, 2002; Robinson, 2013).
Research questions
Based on the findings of the state of knowledge report summarised above (Frawley et al., 2015), this project was designed to answer the following research questions:
- How do women with disabilities in Australia experience tertiary responses to violence and abuse? What can these experiences tell us about good practice in mainstream and specialist services?
- In what ways can tertiary responses be improved to deliver effective services for women with disabilities based on the knowledge developed from this research?
Methodology
This mixed methods project was underpinned by the principle of social inclusion for people with disabilities, as well as an understanding of intersectionality (discussed on page 6). To ensure the voices of women with disabilities were at the forefront of informing the findings, principles of participatory, inclusive research were drawn on. These methods are somewhat conventional in participatory feminist and disability research and are based on acknowledging power differentials between the researchers and research participants. Two key approaches were used to ensure the research was able to draw on and privilege the experiential knowledge of women with disabilities. The first was the development of a research advisory role for women with disabilities whose voices we perceived to be “harder to hear” — the Consultative Research Group. The second was maintaining a commitment to conducting interviews and focus groups with women with disabilities rather than their proxies, despite this being difficult as a result of “gatekeeping”.[5]
The methodological approach aimed to eliminate barriers to participation in the research by women with disabilities as far as possible and ensure the participants’ experiences of seeking and receiving responses to violence and abuse were heard. The research project aimed to capture inclusive and intersectional data based on the principle of “nothing about us without us”, which is the foundation of inclusive research with people with disabilities.
Research and advisory structure
A multi-level research and advisory structure and a range of communication processes were created and implemented to complement and enrich the project as it developed and to ensure a reflexive approach was built into the study. These included:
- Early in the life of the project, the research team recognised the potential for women with intellectual disabilities, dual disabilities, and complex communication needs to be marginalised. A Consultative Research Group made up of women with these disabilities was formed to provide advice to the research team. Their advice and input was used to shape the research approach, support recruitment, and gain insight to support analysis. This group will also assist with disseminating the research findings. Membership and participation in this group was negotiated with individual members as part of the research ethics of this project. The group met six times between October 2015 and September 2016 with two members of the research team and a counsellor with expertise in working with women with disabilities who have experienced sexual assault, who attended in a support role.
- Regular fortnightly telephone conferences between the research team, as well as biannual face-to-face meetings. The aim of these meetings was to share information, solve problems, and reflect on the research process as it developed.
- Quarterly face-to-face meetings between the research team and the research partners (representatives from Women with Disabilities Victoria and the Centres Against Sexual Assault [CASA] forum). The aim of these meetings was to strengthen the research focus of the study by drawing on the expertise of the research partners in research, policy advocacy, and practice. A partnership agreement was developed between the research team and the research partners early in the life of the project.
- Quarterly meetings (face-to-face or teleconference, depending on the location of the participants) between the research team, the research partners and a research advisory group (representatives from advocacy, policy, and practice organisations with a stake in this research, including PWDA, DVNSW, Australian Women Against Violence Alliance, and Advocacy for Inclusion [ACT]). The role of the research advisory group was to advise the researchers on access to and engagement with the sector, provide advice and information on key policy and practice issues that could impact the study, and to support the dissemination of information about the project and its findings. A terms of reference agreement underpinned the relationship between the research team, the research partners, and the research advisory group.
Research methods
A mixed-methods approach was used to capture the complexity of the field and ensure the voices of women with disabilities were heard in the research. This involved:
- A survey of DFV services in Australia
- Selection of three case study sites for qualitative research and inclusion of two specialist service case studies.
- Interviews and focus groups with the managers and staff in the three selected case study sites.
- Interviews and focus groups with women with disabilities who had used DFV services.
- Action research cycles within the case study sites (n = 2). The action research groups included representatives from the case study sites, women with disabilities, and broader representation from disability and DFV services in the geographic areas of the case study sites. The aim of the action research group meetings was to: present research findings, contribute to analysis of the data collected, and plan and implement locally based approaches to address identified gaps in services.
Recruitment, sampling, and the research process for each aspect of the research is detailed below. Ethics approval for the conduct of this research was granted by the Deakin University Human Ethics Committee. Although the identity of the services surveyed and the case study sites was known to the research team, all participating services were guaranteed anonymity and are therefore not named in any part of this report, other than to identify the state-location of the service. All individual research participants were informed about their rights and guaranteed anonymity. An example of a participant information statement (approved by the Deakin University Human Ethics Committee) is included in Appendix A.
Figure 1 Summary of research participation from all sources.
| Data Source | Number |
|---|---|
| Survey of DFV services | 138 |
| Women with disabilities: interviews and focus groups | 34 |
| Managers in DFV and disability services | 5 |
| Staff members and associates in DFV services | 31 |
Survey
The main purpose of the survey was to identify and recruit three case study sites for the qualitative phase of the research. In addition, the survey sought to understand ways in which DFV services in Australia respond to the needs of women with disabilities and how they address access and inclusion. An online survey was developed by the research team and piloted with the service representatives of the research advisory group prior to its distribution. The survey included a number of open-ended questions, as well as multiple choice and multiple response questions. The survey asked questions about:
- the kinds of access (if any) that services provided for women with disabilities;
- how services established whether a woman had disability or support needs;
- barriers to providing accessible services;
- modifications made to improve accessibility;
- policies that addressed disability;
- disability awareness training for workers; and,
- cross-sector tertiary response and disability services collaboration.
Over 300 sexual assault and DFV services were invited via email to participate in the survey. Email addresses were identified through an online search that included several databases, such as the 1800RESPECT service and Australian Government–funded service lists. All members of the ANROWS Practitioner Engagement Group were also emailed a link to the survey with a request to distribute it within their networks.
A total of 165 service representatives started the survey After incomplete or ineligible data were cleaned, 138 completed surveys were returned. The valid response rate was approximately 33 percent. Services in Victoria were most likely to participate, followed by New South Wales Services in the Northern Territory were least likely to participate in the survey. There was a good representation of services from regional, rural, suburban, and urban areas.
Although the main purpose of the survey was to identify case study sites, the survey findings included both qualitative (responses to open-ended questions) and quantitative findings that contributed to answering the research questions. As a result, the survey findings are integrated into the findings from the case studies and action research cycles throughout this report, and identified as such when this occurs. Descriptive statistical analysis of the quantitative data from the survey was completed using SPSS Statistics V21 and a thematic analysis of the qualitative data was completed using NVivo 10.
Case study sites
As discussed above, the main purpose of the survey was to identify potential sites for the case study research. Respondents were asked at the end of the survey to indicate their interest in participating as a case study site in the next stage of the project. Interest was indicated by 40 survey respondents, who were asked to identify the name and contact details of their agency. A shortlist of potential case study sites was developed by reviewing the nominated agencies’ websites. Criteria for selection was then identified based on responses to some of the survey questions and the research team reviewed the possible sites based on the extent to which they met the criteria for promising practice. These included that services had:
- adapted their services for physical and programmatic access;
- identified women with disabilities as a target group in their practice; and
- described their engagement with cross-sector collaboration.
A priority list of 12 services that met the criteria was identified. The first three services (in Northern Territory, Queensland, and Victoria) were approached and invited to participate; however, each of these declined the invitation, so approaches were made to the next three preferred services on the shortlist. The final site selection resulted in the participation of three services, one in a major city in South Australia, one in a regional city in Victoria, and one in a regional city in New South Wales. The aim of this qualitative phase of the research was threefold:
- to understand how services respond to the needs of women with disabilities from the perspectives of staff and managers;
- to understand how women with disabilities experience the services provided to them; and
- to bring together local, cross-sector agencies to promote and support the research locally, develop local action plans, and contribute to knowledge exchange.
Case study sites agreed to participate in interviews and focus groups with managers and staff, to assist with recruiting women with disabilities who had used the services for focus groups and interviews, and to participate in the action research phase of the project. Each of these are described below. Despite the expressed desire to participate in the research, from the outset there were some challenges to data collection in the sites due in part to workload demands.
Interviews and focus groups
Managers and staff
A condition of acceptance of the invitation to become a case study site was that service managers would make themselves available for interviews and would recruit staff to participate in a focus group. Women’s DFV services are busy places dealing with complex problems, and even after accepting our invitation to be a case study site, negotiating access that did not add unnecessarily to staff members’ workloads proved challenging. The researchers made every effort to fit in with the needs and timelines of the services, but, in some cases, this meant data collection was delayed.
Women with disabilities
At each case study site, the researchers aimed to recruit up to ten women with different experiences of disability to participate in interviews, focus groups, or both. To be included, participants had to be: women with disabilities who had used the service, able to communicate with the researchers, and able to give consent for participation in the study.
The case study sites agreed to assist with recruitment of women with disabilities for this phase of the research, which presented another challenge. Often women who are current users of DFV services have recently experienced violence and abuse and many live in fear. Services are protective of the women in their care and fear re-traumatising them. Women who are out of danger and living in secure accommodation may no longer be engaged with the service; indeed, they may want nothing to do with a service that reminds them of trauma. Additionally, services may not have follow-up information about women who have left the service, and the ongoing pressure of new referrals militates against follow-up. These factors meant that not all case study sites were able to put the research team in touch with the number of women with disabilities originally anticipated.
This meant that the researchers had to be resourceful in order to recruit women who were willing to participate and who would not be harmed in the process. Some women who met the inclusion criteria were recruited through disability services to participate in interviews and focus groups. In one case, a group of women in a disability service who had not used DFV services but who had concerns about their own safety in relationships agreed to participate in a focus group.
At one site, only one woman with a disability was recruited through the case study site (three others who were invited refused to participate). In the interviews with managers and staff, it became clear that they had an important partnership with a local disability support service, so permission was sought from the case study site manager to approach the disability service to recruit women. With their agreement the disability support service was approached and agreed to recruit women who met the inclusion criteria for interviews.
Women from the Consultative Research Group (discussed on page 16) also agreed to participate in a focus group. This group consisted of five women with intellectual disabilities and complex communication needs, the majority of whom had used DFV services in the past. They were also experienced self-advocates, knowledgeable about issues concerning violence against women with disabilities.
Across the three case study sites, two disability support services, one specialist service, and the Consultative Research Group, 28 women with disabilities participated in interviews or focus groups.
Action research cycles
After the qualitative data collection and analysis phase, the project planned to bring together representatives from each case study site and its local community, including women with disabilities, to present the research findings and to facilitate a process in which gaps between the services’ and women’s perspectives could be discussed. The aim of this process was to assist services to collaborate with other local stakeholders to modify existing approaches or develop new models based on the findings from the research. The outcome would be action plans based on the learnings from the project.
This plan also met with challenges and the approach had to be flexible to fit in with the participants. At one site, no action research cycle occurred because changes in staff and workload pressures prevented the service from participating after the qualitative data collection phase was completed. To address this, and with the permission of the case study site manager, a local disability service to which the case study site referred women with disabilities was recruited. The manager of the disability service was interviewed and assisted with the recruitment of women with disabilities who had used a DFV service for interviews. We will arrange further meetings with the case study site and disability service to report on the study findings and, if desired, facilitate further work if and when they are ready to re-engage.
Profiles of each of the case study sites at the time they were recruited are detailed next. Further details about the process and outcomes of the action research cycles are detailed on page 38.
Case study site profiles
In this section, we provide profiles of the three case study sites where data were collected. Case study sites were promised anonymity, so, for ethical reasons, other than the state where the service is located, identifying information is not included. All three of these services were DFV crisis response services with some adaptations for women with disabilities.
New South Wales
The New South Wales site is a large, multi-program service located in a small regional city. The service provides a range of family support services to the town and surrounding local area. Its stated aim is to “help people in need”. In addition to DFV responses, the service also provides children’s and homelessness services and financial counselling. The women’s and children’s services have operated for some decades and have purpose-built facilities. These include secure, crisis accommodation, and transitional properties that can be used by women, women with children, men, men with children, and larger families. The service provides limited services to women with disabilities, responding to women who are referred to them or who incidentally come to the service, but not actively promoting the service to them. It does not have a specific focus on supporting women with disabilities or families that include women with disabilities.
Building from a social justice foundation, the service has a history of increasingly professionalised services that focus on the support of families. The current focus on family support is evident in the underpinning service principles, which focus on capacity building and empowerment of families.
South Australia
The South Australian site is a medium-sized, geographically defined, urban service located in a metropolitan region, which has operated for some decades. It is an independent, domestic violence service run by a board of management. It incorporates two sites, with one that specifically works with Aboriginal women and children. Both sites offer secure accommodation and outreach services. These sites offer crisis accommodation, case management, and a range of counselling and support for women to be safe in the short-term and to achieve long-term stability free from violence. The service belongs to a number of community networks in the region that link community organisations working to prevent violence through community education, service collaboration, and innovative approaches to support women and children who have experienced violence.
The service describes itself as woman-centred using a feminist approach. The Aboriginal service also incorporates an in-depth understanding and respect for Indigenous cultures. These principles incorporate respect, empowerment, equity, inclusiveness, and belief in women and children’s stories. They include that:
- violence against women is a crime that denies their human rights;
- all women and children should live in a safe and secure place; and
- Aboriginal and Torres Strait Islanders are the First People of Australia and have a special connection to country that needs to be supported.
Women with disabilities access the full range of services, and physical access has been addressed in the secure accommodation services. One unit in the mainstream service has been developed to be accessible for women with physical disabilities, and all units at the Aboriginal service address physical access needs. The organisation has engaged a woman with a disability as a consultant at different times to advise on access for women with disabilities.
Victoria
The Victorian site is part of a large, statewide, independent child and family welfare service that has been in existence for over 100 years. The branch where the research was carried out is in a large, regional city. This multi-service agency covers family violence, child and youth services, residential care, education, and employment, and does not have a disability support component. The agency identifies people with a disability as an element of their service-user population and although the youth area has specialist disability services, the family violence service does not. They do, however, have a strong focus on partnership with relevant external organisations and refer women with disabilities who have particular support needs to local disability services for assistance. The focus of the family violence service is immediate response to “high risk women and their children”.
Specialist response services
In addition to the three case study sites discussed above, two specialist services were included as case studies. In the original project proposal, these two services were identified as case study sites because they were the only specialist violence and abuse response services in Australia for people with disabilities. After consultation on the project proposal, it was decided that it was more feasible to recruit generic services as one group of case studies and deal with these specialist service models separately, as their service approaches were very different to the generic services. One of these organisations provides a specialist service to people with disabilities who have experienced sexual assault alongside their generic service; the other is a specialist women-with-disabilities service. Descriptions of these two sites are included in the section that discusses the findings from the case study site action research cycles on page 44.
Findings
The findings of this research are reported against the aims that have driven the project and the research questions. The aims were to develop promising practice guidelines for effective tertiary responses to gendered violence for women and girls with disabilities in Australia that are:
- Informed by the experiences of women with disabilities.
- Based on a thorough and critical review of existing models.
- Developed in collaboration with locally based, cross-sector communities of practice.
- Based on an understanding about gendered violence in the disability sector.
Throughout this report the findings are informed by quantitative and qualitative data from the survey and qualitative data from the three case study sites. This project was not an evaluation of each site but an attempt to understand the ways in which models and approaches have been used in Australia and to identify principles for good practice. In the findings section, the data from the survey, interviews, and focus groups are integrated and data courses are clearly identified.
Understanding disability
In the survey, participants were asked how they identified or defined whether a “woman has a disability”. Many services rely on women to “self-identify as prompted by questions on intake form”. Others reported that they identify disabilities “through exploration and questions asked to the woman and one-on-one counselling”. One participant responded:
…ask as part of our assessment if the person has any disabilities. The client or their carer will usually let us know that the person has a disability and the nature of the disability. They define it for us. (Survey participant)
From interviews and focus groups in the case study sites, a more complex picture of “disability” emerged. Women who seek help from DFV services may have officially recognised disabilities (e.g. through “diagnosis”, receiving a disability pension, or having a carer). They may also have “observable disabilities” that require support or assistive equipment. Women in this latter category may or may not self-identify as disabled. Disabilities may be related to the violence experienced and may or may not be permanent.
While the research participants identified a range of understandings of disability, the understanding used by the researchers draws on the following definition:
Disabilities is an umbrella term, covering impairments, activity limitations, and participation restrictions. An impairment is a problem in body function or structure; an activity limitation is a difficulty encountered by an individual in executing a task or action; while a participation restriction is a problem experienced by an individual in involvement in life situations. Disability is thus not just a health problem. It is a complex phenomenon, reflecting the interaction between features of a person’s body and features of the society in which he or she lives. Overcoming the difficulties faced by people with disabilities requires interventions to remove environmental and social barriers…Evidence suggests that people with disabilities face barriers in accessing the services they need in many settings. (World Health Organization, 2011b)
For workers in DFV services, the experience of identifying and responding to functional disability is an everyday experience; women they see may have experienced sustained violence and have acquired brain injuries (ABI), mental health issues, or be self-medicating with alcohol or other drugs as a result of living with violence. When a woman first arrives at a DFV service, this can make the task of providing appropriate access a complex task. A worker in a focus group in Victoria explained:
…it’s hard to know—is this a disability that she has, or is it a mental health issue, or trauma—and often there’s no formal diagnosis one way or another. So it’s hard to know what you’re dealing with.
Staff in the New South Wales site described the challenges they face when working with women who appear to have cognitive impairments:
Worker 1: It’s when that falls on that borderline…
Worker 2: [Someone] who’s already suffering trauma from domestic violence, it’s really hard to gauge…
Worker 1: Yep. So I feel, you know, that’s where it becomes really grey and really tricky. And I think the other thing in my experience is with women particularly that have a mild intellectual disability; it’s obvious to me, but it’s not obvious to them, so they don’t see themselves with an intellectual disability. They just see themselves as…with domestic violence it affects them a lot.
When meeting a woman who is escaping violence, the priority is to help her obtain safe, secure accommodation. Disability is only one of a complex set of needs that the intake worker must attend to in the process of meeting these needs. To understand the ways that this plays out, the research team investigated how workers established whether a woman has a disability.
Identifying disability
The most common approach to identifying disabilities was a reliance on the woman to self-define whether or not she has disabilities, usually during intake procedures. Some services had specific questions on intake forms to establish disability status; others decided for themselves based on intake interviews or counselling. If a woman presents with support or mobility equipment, with a carer, self-identifies as disabled, or is referred by another agency that identifies her as having a disability, then her disability status is determined and acknowledged by the service. In these cases, services understand their duty of care is to ensure access needs are catered for. Some services approached disability from the perspective of potential “barriers”, for example:
[We] ask the person at initial contact if there are any barriers…there [are] a range of specific assessment questions in regards to mental health, physical disabilities, or difficulties in communicating. (Survey)
Others explained that this information can come from a variety of sources:
Often someone in the person’s life has identified that the person has an intellectual disability, or someone self-identifies. Otherwise, we have discussion with people about whether they have difficulty with certain things or ask about whether they are on a DSP [Disability Support Pension]. (Survey)
Another explained:
[We see people with] mental health disabilities, spina bifida, deaf, brain injuries, women who are assaulted about the head would be likely to sustain a brain injury, but many would go unrecognised or assessed. However, we would identify that this is a “hidden” disability for many of our clients. (Survey)
The case study sites had similar approaches to defining whether or not a woman (or her children) has support needs related to disability. Once it is known (through self-disclosure or referral) that a woman has been “officially” identified as having a disability, the service is able to make arrangements to meet her needs.
Identifying whether a woman has a disability is complicated by the fear many women have about disclosing their disabilities. This fear emerged from interviews with women in each site, with one woman noting that she had never disclosed her disability in the past. It was also recognised by the workers:
Women with disabilities are often very frightened to talk about their disabilities because they think it’s going to reflect on her parenting capacity, and they worry about how they will be perceived by Child Protection and Family Law. So that’s another conflict area. And for us, I suppose it puts more pressure on us to then be—as well as doing family violence, trying to advocate on her parenting capacity, even though we might not see her all the time, or know the full extent of how she’s disabled (Workers focus group, Vic).
Women who are not connected with disability services and do not have established disability supports in place present a challenge for services to make effective referrals and get adequate additional support in place for them. Workers at the South Australian site explained:
[A] lot of women that come here haven’t connected with any disability service before…when they come, often they haven’t even got a Medicare card or a key card, let alone, like, filled in a great big application for Disability SA or [disability assistance] so yeah, it’s not very often they come connected to those services already. (Workers focus group, SA)
This was also reported as an issue for children who workers suspected may have disabilities:
There’s been children that—and not that I’m making the [disability] assessment, you know, we cannot assess, but there’s definitely been some—it’s been later discovered or the assessments have happened but families haven’t been connected to kindergartens or childcare or schools, and so assessments haven’t occurred but there is clearly some issues. (Workers focus group, SA)
In each of the case study sites, workers faced similar challenges. Women with diagnosed disabilities who are registered with disability services are eligible for a range of disability supports through disability support services. When they meet a woman whose disability is not officially identified, she generally does not have easy access to disability supports and services. This is compounded by the bureaucracy involved in getting official recognition. The South Australian site noted that this was particularly the case for Aboriginal women at their service, and related to the transient lifestyles of many women escaping violence.
The case study sites were clear that they wanted to improve their services for women with disabilities. This was particularly related to an understanding about the high incidence of violence against women with disabilities that was not reflected in their services:
Because it isn’t our area of expertise. And not that we want to become the experts. We just want to improve…how we reach those women that aren’t being serviced that we know are out there. I guess that’s my million-dollar question: how do we get to those women that we know are being abused? (NSW manager)
Similar sentiments came up at the South Australian site:
So when you’ve got all these women out there—they’re suffering DV—that don’t have a third party service or a disability service. They’re probably never getting to us. We wouldn’t…they won’t pick up the phone because they can’t. He’s probably sitting next to them. So there’d be all these women out there that probably aren’t even getting to us. (SA manager)
For DFV services, these two groups of women with disabilities (those who are officially identified as having disabilities and those who are identified by the service but do not self-identify as disabled) present different challenges. Most services have some adaptations to accommodate women with physical disabilities: most frequently adapting one unit with wide doors, accessible bathrooms, ramps, and emergency call buttons. Far less frequent were adaptations to support women with cognition, sensory, or memory impairments.
DFV services described taking a “whatever it takes” approach to ensuring the safety of women escaping violence, and the flexibility of this approach helps women with disability in many instances. However, for services, the most challenging and difficult-to-resolve cases are those where a woman’s disabilities are not officially recognised. This is where high-quality collaboration between disability support services and DFV services is critical. DFV services did not, for the most part, demonstrate knowledge about disability supports that disability services can provide and relied on disability services to assist women to access disability supports, services, and benefits. In cases where women are not connected with disability services, when they access a DFV service will not always be a priority for DFV services to seek out support from disability services. Addressing this issue in particular presents an opportunity for substantial improvement in the lives of women with disabilities who have experienced violence and abuse.
Models and approaches
In the survey, four options for types of service responses for women with disabilities were included: “limited services”, “generic services with adaptations”, “both special and generic services with adaptations”, and “no specialist services”. As depicted in Figure 2, 18 percent of the total number of participants that answered the question (n = 138) chose the fourth option. 37 percent offered generic services with adaptations, 20 percent offered limited special services, and 24 percent offered specialist and generic services with adaptations.
Service adaptations
Survey respondents were asked to describe the ways in which their services had been adapted to ensure they were inclusive for women with disabilities. The most generic services they identified were: changes to processes and procedures, making buildings accessible, adapting resources (including using large print or pictures or both), developing disability action plans, providing interpreter services, and employing workers who are skilled in disability services.
Some indicated that they had purpose-built facilities, for example, “crisis accommodation [that is] wheelchair friendly”. Many others provided support and training for women with disabilities, some with specially trained workers:
…we have worker[s] that are trained in specific specialist fields so that we can cover all areas of speciality like, such as—youth—dv—disability—mental health—families—prison.
Some offered disability employment services or healthy relationship education for people with intellectual disabilities. One service responded that they provided:
Intensive case management to assist women and their children with a disability to remain safely in their own home, including comprehensive risk assessment and safety plan, needs assessment, and case plan.
Survey respondents were asked to describe the ways in which their services had been adapted for women with disabilities. Responses related changes to processes and procedures, making buildings accessible, adapting resources (including using large print or pictures or both), developing disability action plans, providing interpreter services, and employing workers who are skilled in disability services. Reponses included the following:
Adapted rooms and more space if in wheelchairs or on crutches. If disability is mentally based, then access to a carer on site.
Family Violence counselling and group work service provided with adaptations as required e.g. phone counselling or support people engaged.
Medical and counselling services for people who have been sexually assaulted and have a disability—disability access, disability beds, staff trained in the area of disability, intervention models that include therapeutic care teams (so working with other key carers etc.).
Outreach services, adapted transitional housing properties to assist women with disabilities, partnership with a local disability service to respond together.
In response to an open-ended question about barriers to inclusive service provision, respondents distinguished between physical access and appropriate services, such as specialist workers, communication aides, and carers. It is clear that services want to be accessible, but still see it as an add-on rather than a set of principles upon which the service operates on a day-to-day basis. One service drew attention to the lack of appropriate physical access:
Our high security women’s refuge has no access for full-size wheel chairs. We are able to accommodate children with wheelchairs when accompanying their mother…Our office/counselling room facility has a wheelchair ramp but no full chair accessible toilet. We endeavour to bring in supports for women regarding other types of disabilities such as hearing or intellectual.
Other services indicated that stairs and multi-level buildings limited access or that they were inadequately funded to respond to the needs of women with disabilities. For example, one noted “[our] website is not accessible (i.e. no audio format info)”. Others also explained:
In refuge we do not have disability access due to funding not provided to create the necessary alterations to the units.
Housing is a huge barrier, as often these women live with their carers, so, in a time of crisis, if there are no disability units available, it is difficult to get accommodation which is disability friendly.
Women with communication disabilities were poorly serviced, as one respondent noted: “No resources for a hearing-impaired client in a face-to-face interview…or reading material for the visually impaired”. This service also noted that they had “no current disability action plan/disability audit”. These limitations and barriers were noted repeatedly by survey respondents. No survey respondents noted any contact with women with communication boards or speech technologies.
Figure 2 Service types
Data table for Figure 2
| Service type | DALY % |
|---|---|
| No specialist services | 18% |
| Limited specialist services | 20% |
| Generic services with adaptations | 37% |
| Specialist and generic advices with adaptation | 24% |
Another issue identified was a lack of workers with specialist skills to support women with disabilities, including workers who were trained to support women with disabilities, and training for all refuge and housing support workers in working with women with intellectual disabilities or mental health disabilities.
Each of the three case study site’s response to access was “generic with adaptations”. For the most part, these adaptations concerned adjusting the service to meet the specific needs of each person by collaborating with disability services. In some cases, this collaboration was limited to referral; in others it also involved ongoing engagement.
Collaboration and referral
For DFV workers, referral or collaboration with disability services is important to ensuring the needs of women with disabilities are met. Sixteen survey respondents indicated that they referred women with disabilities to other agencies. Only two respondents identified the importance of the relationship between their service and the disability service to which they referred women with disabilities. One explained: “We speak directly to the service and try to go along with [the] person to support [clients] to connect with the new service (if appropriate)”.
In the case study sites, the most common form of service adaptation was collaboration with, and referral to, disability support services. For example, a disability consultant engaged with the South Australian site explained: “We identify our limitations: think, reflect, and ask who else we need at the table.” This site reported that they had recognised the need to respond to disability as a result of two key factors. First, seeing women with disabilities and thinking about their access needs in relation to the accommodation services. Second, awareness that there was a disconnect between the number of women with disabilities in the population and the numbers they were seeing in their service:
I think we recognised in conversations with others in the disability sector…how can we be more responsive? Because if we look at the number of women that experience disability of one form or another, be it identified or non-identified, we wouldn’t be getting a lot of those women into our service. (SA manager)
When collaboration with disability services does not function well, DFV workers needed to take on the role of advocate for women with disabilities:
I’ve worked with disability clients before, but you know, that’s—it’s not something that comes formally with family violence…we sort of just find ourselves advocating and falling into that role as part of it. Because no one else will. (SA manager)
Like the South Australian site, the Victorian site relied on collaboration with a local disability support service, as the service manager described. “They will actually come on board. You know, if we need some carers or what have you, we don’t have the capacity to do that” (Vic. manager).
A feature of the “whatever it takes” approach used in each of the three sites is an individualised, creative approach to ensuring that women receive appropriate support. A worker at the Victorian site explained how this worked with the disability support service with which they collaborate:
…there’s no after-hours support for women who have disabilities, and who need accommodation, need safety stuff. There’s no one out there, no after-hours disability number. So we’ve worked out our own system with [the local disability service] now through [our manager] meeting with them. If we accommodate someone who has a disability who needs a worker, they’ll organise the worker. (Workers focus group, Vic)
The South Australian site’s work is also underpinned by a community partnership approach. The manager described how a collaborative approach with a local disability service helped to deal with a challenging situation:
We had…a young woman came in, was in a wheelchair, had slight intellectual disability…[Her partner] was extremely abusive and there’d been some serious incidents. So we were able to work with [the disability service] and they were able to get her out. (SA manager)
The manager explained that the woman’s disabilities prevented her from being able to reach her alarm button when she was in bed and went on to explain how their collaboration with the disability service had worked:
We were able to get a different type of [mobile] alarm system in. [The disability service] were fantastic in putting carers in place because they had those links so we had around-the-clock carers because of course he’s out of the picture…she needs that support, meals, all of that. That co-working together, that belief in each other and that learning…we’ve built those relationships with one service. (SA manager)
The manager qualified this comment about building a relationship with a specific disability service: “We’ve had some real challenges with other disability services”.
In the past, the Victorian service had the assistance of a disability advocate. They emphasised that this was not a regular occurrence, but had been very helpful:
…having a disability advocate who can help navigate through the system. Joint case management with specialist disability services, where we can come in and help with the family violence side, and they can help the holistic other aspects. (Workers focus group, Vic.)
The Victorian workers focus group drew attention to a $7000 fund that is available for disability crisis support. The disability advocate knew how to access these funds:
That worker…was a sort of conduit. She understood the disability service system, so she could help us find the right way. The problem was that they had a quite narrow definition of disability. So we had to have disability as according to DHS criteria. (Workers focus group, Vic.)
While this was useful, they also noted that the cost would only cover some women with complex needs for a short period:
What didn’t work is, as a crisis service, you might spend the seven grand in two or three nights. Then you’re moving her to the case work, and DHS going, “You spent the money already”, so that’s difficult. (Workers focus group, Vic.)
DFV workers need to be creative and “think outside the box” to ensure women with disabilities receive appropriate supports. They are not resourced specifically to address the disability support needs of women and it is only collaboration that ensures women’s safety. For disability support, DFV services are dependent on “outside support which sometimes isn’t always available” (workers focus group, Vic.).
For women whose lives are transient, which is often the case for many who experience family violence, particularly Aboriginal women, making and keeping links with disability services can be challenging:
The transient nature of a lot of the women’s lives and the crisis that’s happening in communities and whatever means it’s really important to try and link in, so you’re hoping that, even if they do move on, you may have been able to establish some link with another service, [particularly] for the children. (SA manager)
This was described as a “culture clash” between the domestic violence services’ “woman-centred practice” and disability services’ “protective approach” (SA manager). A woman-centred approach acknowledges women as experts in their own lives with the capacity to make choices. This was discussed in a staff focus group:
Our difference is our focus is on empowering women to be independent. It doesn’t matter who you are, where you come from, what’s your language, [they have a right] to be independent, to feel safe, secure…you know, they’re adults; they have a right to choose. Especially…being a victim, normally they never had a voice to choose or to speak out or to have, you know, input in any decision-making. We don’t want to take them here as well. We want them to feel like, I’m a free woman; I’m an independent person. (Aboriginal service worker, SA)
The workers went on to explain how this position conflicted with that of a disability service:
There was a girl here for a long time…and our team leader, she just fought and fought and advocated constantly for this client…around housing…you know, finding her appropriate housing…supported housing, you know? And there were real clashes with other services about, you know, with negotiations about her needs being met kind of thing…Supported independence…in a property on her own, a little flat, but, you know, with support. (Workers focus group, SA)
The conflict continued, with the disability services arguing that the client could not take care of herself even as she started to develop her own sense of independence:
They’re saying to her [what you’re doing] is not enough…and when she started to make her own lists they’d say, what do you mean you want? We will tell you what you can have…They wouldn’t even let her…she wanted a Coke, she couldn’t have a Coke…then they controlled her. (Workers focus group, SA)
They went on:
There were a number of clashes with the woman, they were insensitive, you know, dominating…judgemental…yeah, very, judgemental and looking down upon…It’s very problematic for people dealing with Aboriginal people because they’re over—they’re sick of people telling them what to do. (Workers focus group, SA)
The staff responsible continued to advocate for the woman:
Our team leader kept saying, “Hey come on, she can do this stuff; engage with her”. You know, it’s about showing her how to do stuff, encouraging her to do stuff, engaging, but, you know, unfortunately the workers that were coming in weren’t interested in engaging with her. They wanted to…clock their 2 hours, get in, get out, you know, and that wasn’t meeting her needs. (Workers focus group, SA)
The staff in the Aboriginal service related other similarly disturbing conflicts between their service encouraging women to be agents of their own destiny and disability services controlling and limiting Aboriginal women’s agency. They also described how, when cross-sector collaboration did not work, this added to their workload: “it’s ten calls to make one thing happen…To and fro just to get one thing done”.
At the Victorian site, workers identified similar problems where their service and disability service cultures clashed to the detriment of women with disabilities. In one case, although a client lived in the regional city where she sought help, her disability case management was handled in Melbourne.
We had a lady and her daughter, who had multiple disabilities. Huge issues. And they were case-managed in Melbourne, and it took us what, at least 2, 3 weeks to work out how it all worked. And who to ring and who to contact. (Workers focus group, Vic)
In many cases it is the complexity of the life of the woman with disabilities (which might include alcohol or other drug issues, mental health, physical health, intellectual disabilities, and the disability pension and support service systems) that is most challenging:
It can be quite confusing at times about what services do this, different packages. It depends on the disability levels, depending on what disability help they get. I find that very hard to navigate for myself, let alone the lady that’s in the situation or the child that’s in the situation. (Vic. manager)
Some women supported by the case study services were facing serious problems, such as having children removed from their care. Supporting these women included negotiating with a range of different government departments and within the judicial system. Family violence workers needed to take on a range of issues because of their commitment to ensuring women’s safety:
Quite often we’re drug and alcohol workers, quite often we’re mental health workers. I don’t have skills in those areas. But—but often when there’s one with the lot, as we call it—one with multiple complex issues—we find that drug and alcohol won’t get involved because she hasn’t dealt with her family violence issues. Or you find that mental health won’t get involved because she hasn’t dealt with her drug and alcohol and her family violence issues. (Workers focus group, Vic.)
The findings in the section highlight the importance of resourced, high-quality, cross-sector collaboration to ensure true access for women with disabilities to the range of services and supports they need to live in secure accommodation free from violence and abuse. It also shows that there is a great deal of room for improvement across sectors if this is to be achieved.
Access and accessibility
Fundamental to this research is the concept of access for women with disabilities and, conversely, what makes services accessible. The literature review (see page 8) found recommendations for services to be made as accessible as possible: for access to go beyond the physical to include information, attitudinal and procedural access, and to go beyond what is required by the Disability Discrimination Act 1992 (Cth). Programmatic access is called for from intake through to counselling and outreach that should incorporate both procedural and attitudinal components. These recommendations expressly identify the things that are needed to make a service accessible for people with disabilities. However, the literature does not make clear what it is that makes a service accessible to all in the first place. Here, we do not argue that the modifications and adaptations recommended in the literature are incorrect, rather that there are some fundamental structural and philosophical issues that lie at the core of accessibility that precede modification and adaptation of existing programs.
According to Levesque, Harris, and Russell (2013), access is central to the performance of services. Whilst Levesque et al.’s work focuses mainly on health care services, it is equally relevant to tertiary response services; accordingly, here we adapt Levesque’s model to focus on tertiary response services.
Dictionary definitions of “access” address it as “the means or opportunity to approach or enter a place” (Oxford Dictionaries, n.d.). Access to a service refers to opportunity or ease with which people in need of a service are able to obtain and use those parts of the service that are appropriate to meet their needs. For Levesque et al. (2013), access is the interface between an individual or household’s social and physical environment and the characteristics of the service. They draw a distinction between “access” and “accessibility” as follows:
- “Access” is being able to enter or obtain services: for example, “I have access to…”
- “Accessibility” describes the nature of services, how they are designed, and what opportunities are provided for people who need the service to obtain them: “It is useable to me”.
Where there is a mismatch between what is available and what is needed, there is a barrier to access. Levesque (et al.(2013) identify five dimensions of accessibility. To be accessible, services must be:
- approachable;
- acceptable;
- available;
- affordable; and
- appropriate.
If all of these features are not in place, then a service is not accessible. Thus, adapting or adding disability modifications to a service that is not fundamentally accessible is unlikely to create access. Each of the five dimensions mentioned above must be in place before minor modifications are made.
Most of the services participating in this research only had wheelchair access and usually only in one unit. If a woman with complex disabilities wants to access a tertiary response service and the service does not understand the range of her needs, or if it is not acceptable or affordable to her, then adding communication aids does not necessarily make the service accessible. It may address one of her needs, but not all of her needs.
Women with disabilities’ insights about access
In focus groups and interviews, women with disabilities expressed a number of ideas about how services could be made more accessible to them. Although many of the women have complex social, physical, and mental health issues that are challenging for many services, their ideas for improving service access were straightforward and match the model presented by Levesque et al.(2013) discussed above. Following Levesque, the women’s ideas about access will be discussed under these sub-headings: approachable access, acceptable access, and appropriate access. Affordability and availability of services were not strong themes in the women’s interviews and focus groups so are not covered here. The main issue relating to affordability and availability access is housing, which is an important issue to address in future research.
Approachable access
In the Levesque et al. (2013) model, the starting point for approachability is that those in need of a particular service know that it exists, how it can be reached, and that it can help them. Knowing that a service exists and what it offers is thus the first step to accessibility. Elements such as transparency, information about available services, and outreach can make services more approachable. In interviews and focus groups, women had ideas about matters that made it difficult for them to engage with tertiary response services. For some, the idea of asking for help from the police was frightening:
They’d be shaking…because the police, they’re all tough and they’ve got guns and walkie-talkies and so they’d be scared. But when they’re in the room, like one-on-one, like, they’re not scary, but it’s getting in there. (Women’s focus group, NSW)
When asked about how approaching the police could be made less scary, a woman explained:
Just have a smiling face, like, when they walk in, like, say “hello” back, and then they’re alright…and be happy… they can have a cup of tea, and sit there and talk to them and explain it to them. (Women’s focus group, NSW)
Women also mentioned the importance of being able to speak to other women about experiences of violence, rather than having to tell their stories to men.
Speaking about tertiary response services in the broader sense, another woman made a plea for patience and understanding:
You have to be nice to those customers, or, umm, you have to be able to deal with, you know, what comes out…they have to have the right words to tell, like they have to say it properly. (Women’s focus group, SA)
To be approachable, services need to address matters of quality, adequacy, co-ordination, and continuity (Levesque et al., 2013).
Acceptable access
Acceptable access is about the professional culture in organisations that facilitates or impedes the ability of women with disabilities to seek help. The “culture clashes” between services (discussed above) affect access, as do clashes between women’s personal and social values, culture, and sense of autonomy and that of the service from which she is seeking help.
When a service expects a woman with disabilities who has experienced violence to fit into its culture and has expectations that are in direct conflict with her own needs, this can have major implications for access. For example, one woman explained how her needs were not met by the disability service she sought help from:
People with disabilities are each individual; I think people think they are all the same but they are not. And they need to do higher supports; if that means someone needs more support or a different way or whatever. At the start I just wanted to go away. I didn’t want to be here, to have people know where I was. But there was no funding or support for that. And that’s what I needed, just time to get my own head into [a] place where I could cope with what was going on. And he had people going past my house, and things like that so I just needed to be out of my house. Time out and time away but they wouldn’t do that…but it’s about helping me with the budget to try and get time out, to do time away, if that’s what I needed. (Interview, Vic).
In disability services, women want to feel safe. If services remain silent about the possibilities of violence and fail to provide appropriate information and education on the matter, women with disabilities’ access to acceptable support is limited. One woman explained:
…get a better place for girls with disabilities where they can go if they don’t feel safe or something like that…with lounges, umm, people to talk to…(Women’s focus group, NSW)
This draws attention to the ways in which services limit choices by “protecting” women with disabilities from information and from each other. The women identified protectionism as a problem.
In other tertiary response services, confidentiality and privacy were matters of concern. Two women spoke about how unacceptable it was for them to have to speak about their private business in the foyer. For them, it was more reassuring to discuss their business in spaces that were private and comfortable. For others it was knowing their rights:
I think the client needs to know their rights, and a lot of the time they’re not told of their rights. When you go in there [DV service/refuge], you’re not told what your rights are or what services are available, like [advocacy] and all your different things. If you have an appeal process. (Women’s focus group, SA)
Acceptable access to tertiary response services for women with disabilities who have experienced violence can be achieved when services are flexible in the way they respond to women, understand the challenges women face when they seek help, and value their rights to information, knowledge, and autonomy. To be acceptably accessible, all tertiary response services must start from this position.
Appropriate access
Appropriate access is about the fit between the service and the client’s need. It is about the time spent on understanding what the individual needs and planning appropriate responses. It is also about the technical and interpersonal qualities of the service (Levesque et al., 2013). For the service-user, it is about their ability to engage with the service. This includes women feeling empowered and in control of their own future. This is enshrined in a woman-centred approach, but may not always be achieved for women with disabilities.
In this research, women with disabilities showed a great desire for services to provide accessible information in digestible forms, such as easy-read booklets placed strategically where women could pick them up and read them at leisure: “like a booklet, with all of it, then she can go for a walk and go through it with the girls [workers]”. Central to this provision of more information was having enough time to take in the information gradually without feeling rushed, overwhelmed, or confused. Effective communication skills were also seen as important in services: “meeting in person, not on the phone” was mentioned as something that would help them and others to feel more comfortable.
For women with disabilities, appropriate access can also be addressed through having workers who are knowledgeable about disability. In a focus group, the following exchange took place:
Woman 1: Well, shouldn’t they have workers that have training in disability?…There should be.
Woman 2: Yeah, there definitely should be [suggestion by interviewer that women with disabilities be involved in this]…Yes, definitely. (Women’s focus group, SA).
For women with disabilities, the lack of knowledge and understanding about tertiary response services for those not in the system was also mentioned as a way of providing appropriate access:
I think by getting out there and promoting themselves in organisations. I think there needs more awareness for women with disabilities themselves. That these services are…exist for them. They are not only for people, women, without disabilities. And I think that’s part of the problem. (Women’s focus group, SA)
The Consultative Research Group had a range of suggestions about how to improve accessibility. Importantly, they called for services to recognise that “every woman with a disability is different—[there is] no one thing that will work for everyone”. They argued that “It’s about communication and support and advocacy”. For these women, independence and autonomy are vital; they talked about “hard won independence” and wanting to have the right to learn from their own mistakes without people saying “I told you so”.
The findings in this section on access suggest that to ensure tertiary response services are as accessible as possible for women with disabilities, services can make relatively minor changes by taking into account women’s needs and hearing from the women about their experience of using the service. Through addressing broader issues of access in addition to disability-specific needs, the interface between what the service offers and what women with disabilities need can be better aligned.
Women’s experiences using services
In this section we turn to the findings concerning women’s experiences using DFV services. As discussed in the methodology section, because of the difficulty experienced in recruiting women with disabilities who had used the case study services to participate in interviews or focus groups, women were recruited from a wider range of sites. As a result, this section includes data from women who had used the case study sites; women from disability services who had experienced sexual assault, domestic violence, and other experiences of violence and had used some support services to address the violence; and women from disability services who had not experienced abuse but had concerns about their personal safety. Two distinct groups emerged: women who knew about and had used a range of services (n = 18) and women who had no knowledge about DFV services or what to do if they were a victim of abuse (n = 5).
Women’s knowledge about family violence services
In this section, we first discuss women with disabilities’ knowledge (and lack of knowledge) about DFV services. We then turn to the women’s positive and negative experiences with DFV, disability, and other services to identify features of effective services and service systems, which includes relationships, practical support, service co-ordination, and collaboration.
Established family violence service–users
Participants in the case study sites were asked in interviews about their experiences with DFV services. Women who were established family violence service–users (n = 18) often had multiple, complex problems related to their disabilities and the social, mental, and physical effects of experiencing family violence. The DFV service was part of the fabric of their lives, and when the relationship with their worker or the service in general worked well they were full of praise. When asked what was the best thing about the service, one woman referred to her worker:
She was great; she took me to appointments, made sure I was safe in the house, spoke with my estate agents. Followed up to make sure everything went well. Does that frequently; she’s great. Everything they’ve done has been top notch. (Interview, Vic.)
Many of the women who were established service-users were embedded in a web of systems in addition to the case study site and did not necessarily separate these, providing insight into the complexity of their lives. When services worked well together or when one worker emerged as a strong advocate for a woman across systems, women were grateful and felt empowered. When the system did not work well, it could be disastrous. A woman who had used a family violence service and was recruited through a disability service told the interviewer:
They wanted me to get an intervention order, but I wasn’t ready. So instead of spending the time to get me ready, they just said “We’re going to close your case,” and it took probably another 2 months maybe to get to the point where I was OK to do the first order. Nervous as hell because he was living with me, so it was nerve-racking trying to do that and not for him to know that that’s what I was in the process of doing. So I got the first order, went to court and they pretty much didn’t stay with me or anything. (Interview, Vic.)
When they had no knowledge about how to get help prior to being referred to the DFV service, many of the women had lived with violence for sustained periods of time. One woman had found help through Lifeline:
I didn’t know, and I was too scared to open my mouth, because I didn’t want no one to get into trouble the one who was abusing me. So it took me over 30 years to open my mouth. And I actually rang up Lifeline. So I got a number from Lifeline and they were starting a loss and grief [program for people with disabilities]. And I rang up, and I spoke to this nice man, he was a social worker. And he—he was the one suggested—when I first seen him…And it—it took me months to agree for him to bring me here [to the case study service. (Women’s focus group, SA)
The theme about a prior lack of knowledge about DFV services was common. Women came to services as a result of a sense of desperation or through a referral from the police, other counselling services, doctors, or disability services. In another group, responding to the question, “How do women with disabilities find out about DV services?”, one woman said, “You don’t…but if you are at a disability service and you have the courage to tell someone they might help”. An Aboriginal woman at the South Australian site described her life of violence at the hands of her father and partners. Even though she had tried to get help, she had been unsuccessful until:
I finally got a phone call from [an Aboriginal women’s shelter in another town]. And they said that they had a vacancy there. So when I came back down, after all that, then I finally got my house, and I moved in. I’m starting to get things… (Women’s focus group, SA)
She went on to explain that later, she had returned to her family and the violence had started again:
Then my dad almost married me off to about a busload of blokes, ’cause they were all my right skin. So I took off from there too…And then after everything happened and everything started building up, and I didn’t have anybody to talk to, then I had a bit of whatsaname [a breakdown], so I left my kids with my mum, and I took off up to my step-mum up in [a remote town]. And I ended up with a traditional man, and then he bashed me every day. (Women’s focus group, SA)
After a series of violent relationships, she tried again to get help:
Well, I just ended up ringing up Crisis Care. So when I got down here, that’s when I rang up; [they said] “we need to call the DV mob, we can get you help now”. But these mob [Aboriginal refuge service] lately—these mob have been a lot more helpful. (Women’s focus group, SA)
The theme of lacking knowledge about how to get help highlights the lack of information sources and education available to women with disabilities. Constrained by fear and a lack of information, they often live with abuse until the situation reaches breaking point and the police become involved.
Women who have not used DFV services
Women who were recruited through disability services and had not used DFV services (n = 5) were part of a disability support service but had no knowledge about how to get help if they were in an abusive relationship. All of these were younger women (aged 18-24 years) who had experienced bullying (mostly at school) and were currently employed in a program for people with intellectual disabilities. They recalled learning about places where they could get help when they were at school. The police were most commonly named as where to go if they needed help. Headspace was named by three of the five women and described as a place where:
Lots of girls go there when they have problems and then they cut themselves and they go there. That’s the one at the skate park. Then if they’re going to kill themselves they go there, that’s where, that’s a really good one, I know heaps of girls that go there. (Women’s focus group, NSW)
Hospitals, counsellors, and a helpline were also discussed as places where they felt they would go if they were concerned about their safety. The woman who nominated the helpline was not able to name it, or relate the number or where to locate the number to call it. She did recall:
It was on my school laptop I can’t remember…it was like a green or red phone and it said “get help”. (Women’s focus group, NSW)
The women in this group remembered how to get help from school but had no access to information in their current workplace or support service. While they could speak easily about work-related occupational health and safety concepts (e.g. wearing safety boots, watching out for cords), handling animals, and physical safety in the general community (e.g. “watch where you’re going”, “look around; make sure no-one’s acting strange”), in terms of safety within relationships, they were less knowledgeable. One woman talked about looking out for her friends and another about communicating with everyone so that “everyone gets along together”. A third woman talked about a system at work that she connected with safety:
We get a red flag. If you get three red flags if you’re playing up or something, your parents come in, it’s like a—a behaviour thing? If you’re playing up or swearing or something they get a red flag. (Women’s focus group, NSW)
From this woman’s comment it is possible to suggest that safety within relationships for the women in this group was not addressed within a DFV framework: their self-determination was not paramount in addressing concerns about safety.
Women in the Consultative Research Group discussed how they might access information about where to get help. One woman said: “you have to go looking for it”. The researcher suggested the internet might be a source of information, to which someone else replied “they might not have or know how to use a computer or have access to the internet”. Another participant mentioned helplines:
The 1800 number will take you to the nearest service that helps with violence. But sometimes people don’t know about this number until they need it—you learn how to access the services by using them. (Consultative Research Group focus group)
Regardless of whether they have had contact with DFV services or not, the findings in this section reveal that women with disabilities lack knowledge about how and where to get help if living with or in fear of violence in relationships. The raises the importance of prevention education about domestic or family violence for women with disabilities. Rather than shielding women from information about violence, they have a right to know that that it is never acceptable and how to get help if they are in fear or it happens.
Although it was not the focus of this research, disability services are notoriously protective of the women in their care, a phenomenon called “gatekeeping” (Frawley et al., 2012). This was particularly apparent with the group of women who had only had contact with a disability service.
Another kind of gatekeeping for women with disabilities may also take place in some DFV services. Although each of the case study sites presented their work as “woman-centred”, not all of the women experienced the assistance they received as such. An Aboriginal woman from the South Australian site explained:
They need to let the client make—I don’t know how to word it. Not make the decision for us. We know what we need better than anybody…But they also need to find out why we have that disability, and then understand the disability, then get into where they can sit down with us and understand what we know, what we need. (Women’s focus group, SA)
Although it is not clear whether this passage is a criticism of the South Australian site, it is clear that self-determination is very important to this woman. Well-meaning efforts to shield women with disabilities from information or making decisions that can help them gain control over their lives are unacceptable. It is important that a “woman-centred approach” be central to day-to-day practice by DFV workers and not just service rhetoric. This approach is also important for the other services that support the needs of women with disabilities who have experienced abusive relationships. Critical reflection on the implications of this approach and continuous improvement should be an ongoing part of DFV service practice, with a particular focus on intersectionality. We expand on this in the action research section below.
Given the high incidence of family violence and sexual abuse experienced by women with disabilities, ongoing health promotion, social marketing, and prevention education is essential to ensure women can determine what constitutes violence and how to get help if it is needed.
Features of effective DFV services
Relationships
Women at all the case study sites told stories about relationships with workers or services that were positive, in which they were treated respectfully as individuals. They also told stories about poor-quality relationships. Women with disabilities who have experienced violence and abuse in relationships are dependent on a web of services that often do not function together to adequately meet their needs. Fundamentally, they value a worker who is friendly, supportive, and helps them to find safety. In many cases these women have been isolated and, although it is not the role of DFV workers, at times they just need a supportive friend to help them navigate the system. At times the worker fulfils this role because they do home visits. One disabled woman explained:
I think [workers] just need to think about, that service is for women who are at their most vulnerable and most of the time that they are in need. Because I don’t drive, it was about going to their offices and things like that and a lot of the time it might be that they need to come out and do some things at home once the order is in place, or just try and find ways around. (Interview, Vic.)
Sometimes the kind of support women with disabilities need is companionship to alleviate the stress and fear associated with being in a violent relationship. A participant from the Victorian site explained:
Probably the biggest support I need is someone to come in and maybe just take me out and do something. Or just come to my house and just chill out with me for a while and do de-stress stuff. I was in my house pretty much housebound for the first 2 or 3 weeks after the full order. I wouldn’t go out and I was scared, even now I’m thinking that and making sure he’s not near me. (Interview, Vic.)
For women at the New South Wales site, it was important that workers noticed and told them when they were doing well. They needed both acceptance and positive feedback even on the trivia of their lives:
Woman 1: You can be yourself around them, like, if I’m having a really shitty day and I’m swearing and stuff, my worker is just like, “Oh you”.
Woman 2: It makes you feel really good because sometimes they come to your house real bubbly and they go, “Oh, your house looks really lovely today”, and stuff like that. (Women’s focus group, NSW)
Trust and confidentiality were particularly important. One woman explained: “Yeah, they don’t go and talk about your business behind your back, like, after they’ve spoke to you about it” (Women’s focus group, NSW).
The women also valued consistency in their relationship with workers. Having to relate stories of abuse repeatedly to different workers can be painful or re-traumatising for some women:
I first had [a DFV worker] and she got promoted or something, so she left; then I got another worker. So it’s been three different people and that doesn’t have to make it helpful because then you have to explain yourself all over again. (Interview, Vic.)
Women at all sites were particularly positive about the consistency of support they experienced over time and felt it was important to be able to build a relationship with their caseworker. At the New South Wales site, the relationship with the DFV worker was appreciated for the sense it gave women of feeling valued and respected. It also generated a sense of purpose for each woman. They described a range of roles that were fulfilled by their caseworkers, from the intake process to the ways they were supported to attend appointments, find secure housing, get medical check-ups, enrol in parenting and other courses, and get practical help with “the little things and the big things” (e.g. dropping bread off once a week and helping with getting a new fridge).
The combination of disabilities and living with or recovering from violence or the threat of violence can be draining and even overwhelming. Trying to navigate multiple systems while attempting to live independently can seem insurmountable. Having a trusting relationship can be key, as one woman explained:
It really helps you get things done. Because if you’re sitting around home by yourself and, you know, you’re too worried about cleaning the house or doing—or dinner, that’s all you think about, oh, what am I going to have for dinner? What—I’ve got to clean this, I’ll do that. So when they’re on your back about things, like the important things that you don’t like [to] think about, it’s really good and then you can actually go to sleep at the end of the night and think, well, that’s done, I don’t have to worry about that any more. (Interview, Vic)
While it is not the role of DFV workers to befriend their clients, for the women in this study, a warm, supportive relationship was a critical part of the journey to recovery and independence. Knowing there is someone to fall back on in a crisis is also seen as an important part of the worker’s role:
The worker I had back in January 2015 wasn’t very good. Then I got my own home, um, but then I got involved with my partner, and I had to move, yep, because he was abusive. And the police contacted the agency and I got my current worker [sighs]. She organised the removalist and all the help I needed, she was great, she was brilliant. (Interview, Vic)
This raises the importance of practical support to manage day-to-day life. The ways in which workers related to women through small acts, such as recognising when women and their children were doing well, in addition to providing practical and emotional parenting support and taking as much time as needed for individuals to gain confidence, were all mentioned in interviews and focus groups by participants. The women who had lived in shared crisis accommodation also appreciated sharing cooking and child care tasks as ways of supporting others and gaining support themselves. There is evidence that being linked into group activities empowers women and enables them to both learn new skills and teach others (Mejias, Gill, & Shpigelman, 2014).
For many women with disabilities who have children, the threat of losing custody is constant. It therefore is not so surprising that providing support for the whole family is an important issue. As one woman put it: “It helps the kids when you help me too” (Women’s focus group, NSW).
Another theme from the research relates to the importance of group social support that brings together women with similar experiences. This aspect of social support is seldom provided and this leaves women with disabilities isolated, ashamed, and fearful, even after they have escaped from violence. In the Consultative Research Group, one woman suggested “a drop-in place that people can pop into to have a chat and a coffee”. Another woman, who was herself a self-advocate, mentioned greater self-advocacy would help women to break down the isolation.
In one of the specialist sites, women with disabilities met together in an ongoing social support group. In a focus group, they talked about how they liked the ongoing nature of their group and that they didn’t meet just to talk about violence, but rather chatted about all kinds of other things. The safe place philosophy that underpinned the group, as well as the relationships of trust with workers that they knew, was very important to these women.
Service co-ordination and collaboration
Many of the women with disabilities at the case study sites had experienced disruption to support services. In part, this was because they had moved around to escape violent relationships, and “When you move around…you can’t get services”. However, it was also due to a lack of co-ordination and collaboration between the various services on which they depended to live independently without violence. A key challenge identified by the participants was losing one service because another service was involved (e.g. “When disability services stop because you are using a DV service”). As one woman commented, “Youou are not getting help from either DV or disability and need ongoing counselling and case management, but nobody is giving you this.”
Another woman with multiple challenges outlined the ways in which services had failed her:
I’ve always had bad experiences of the psych services, and when I was in the refuge I was ODing pretty much every day, at least; the minimum was two to three times a week and psych services were like, “You’ve got a disability; you don’t fit into our category, so go away. Because our category is alcohol and mental health, or drugs and alcohol and mental health.” So disability wasn’t a big perception of what they wanted in their little group. So it made it really hard. (Interview, Vic.)
These experiences had occurred in the past when this woman was living in a different area. Having moved to a new location, the services were better coordinated and things had improved:
But now they are good and they are doing crisis care for me if I need it. I have a really good psychiatrist; I can call him any time. I’ve got a really good psychologist and a good mental health together. (Interview, Vic.)
Some women fear disclosing that they have multiple problems. As one Aboriginal woman noted:
I was too afraid to tell them [the refuges] that I had a disability. I went from shelter to shelter to shelter in different places and back to abusive relationships because I didn’t tell them I had a disability…didn’t get the help I needed. (Action research workshop, SA)
The women’s stories about their experiences in DFV services show that, when it is working well, there is a strong relational connection between the service or worker and women with disabilities. The women value consistency in their contact with workers and trust that they will be treated with respect and dignity. They also value being supported to take as much time as needed to manage their lives and get back on track. A whole-of-family approach to care is essential to ensure women are able to keep and care for their children. Above all, access to group support from other women who have had similar experiences was identified as imperative and lacking.
Action research cycles
As discussed in the methodology section, this stage of the research was grounded in an action research methodology in order to put into practice the collaborative principles that underpin the project and build new knowledge. This strategy responds to the experiences and perspectives of participants in the interview and focus group stages of the research process. Action research is a participatory, democratic process concerned with developing practical knowledge. It brings together action and reflection, theory and practice, with the aim of solving community problems (Bradbury, 2015).
The action research cycle brought together key DFV and disability stakeholders in two of the case study sites to collaborate on identifying, planning, and starting to implement service improvements. In this section, we start with the findings from the action research cycles, then draw together overall findings to suggest some ways in which the tertiary response sector can deliver more effective services for women with disabilities.
South Australia: action research process and outcomes
At the South Australian site, the researcher and site manager together developed the service’s action research aims after the initial data collection phase. Two key aims were identified:
- to have more meaningful and ongoing contact with women with disabilities; and
- to revisit the development of a collaborative and cross-sectoral working group that would focus on access for women with disabilities.
Over 7 months in 2015-16, the site manager worked on these two aims and reflected on the approach and outcomes with the researcher via emails and phone calls. One proposed action to achieve these aims was bringing together a group that would form the local action research group. Membership comprised a disability consultant (a woman with a disability), other disability activists, and community and government organisations. The researcher provided consultation to the manager on the ongoing development of this group.
In September 2016, the action research group was brought together for a workshop, facilitated by the researcher, at which the research findings from the project were presented. Discussion then focused on the group’s action research aims and the development of an action plan.
The researcher conducted a 2-hour reflection meeting with the manager 2 weeks after the initial workshop, where further analysis of the local aims and progress was discussed. Reflections from this meeting also fed into the final analysis of the site data and the key themes emerging from this site.
The action research approach enabled the service manager to reflect on the place of women with disabilities in the service and conclude that the service did not really engage with women in roles other than that of service-users. This raised questions about increasing the participation of women with disabilities and ways to draw on their expertise in what works best for them and others like them. The service manager identified two influential learnings from the research process. First is the importance of hearing the views of women with disabilities:
Women with disabilities bring their experiences to the service; the service responds but needs to see and reflect on what the women teach us in the process…We need to hear from women with disabilities…woman with a disability says “X” we critically reflect and use this for change. (SA manager)
Second is the importance of cultural change within the service and across the sectors that impact on the lives of women with disabilities. Some of these changes were already underway; for example, workers now recognise that they know little about what happens for women with disabilities after they leave the service. As a result, the service is now following-up with women with disabilities to check in and see how they are managing. In many cases, this has resulted in a celebration of how far the women have come. This is particularly important for Aboriginal women service-users, as they often lose important community networks and contacts when they escape from abusive relationships. The staff also noticed that women with disabilities wanted to remain involved because it was a “way of helping other women with disabilities”. The service is working out how best to incorporate this learning into their practice.
Figure 3 South Australian action research cycle process.
Text alternative for Figure 3
Feedback to local group
- Research in sites
- Analysis
Locally developed and implemented approaches
- Local group workshops
Local approaches fed into research-informed practice model
- Feedback to researcher
One of the issues raised in the research is the tendency for services to “protect” women with disabilities, which can lead to limiting their agency and autonomy. The manager reflected that their “misguided desire to not re-traumatise” women with disabilities by recontacting them may have overshadowed ongoing opportunities to positively engage with them on further developing access and inclusion.
Another insight that emerged from the action research cycle was that some women with disabilities who experience violence in relationships may not recognise their experience as “domestic violence”. In particular, this may be the case for women with severe or complex disabilities who are reliant on a carer. The women with disabilities who participated in the action research emphasised that they had not known that there were places where they could get the kind of help available through DFV services until they had started using the service.
The work undertaken by the South Australian site to improve accessibility for women with disabilities led to new relationships with a number of other agencies and, perhaps as a result, they have also experienced an increase in referrals. Engagement with the research provided this site with opportunities to critically reflect on services for women with disabilities, and to identify gaps in existing services and strategies for addressing these gaps. This has provided opportunities to formalise an advocacy model that is depicted in Figure 4. This model highlights the importance of collaboration with women with disabilities and other services as part of the “respond and refer” cycle.
Figure 4 South Australian advocacy model
New South Wales: action research process and outcomes
The New South Wales case study site took an incremental approach to work more effectively with women with disabilities by building awareness, skills, and collaboration. Over the course of the research, four action research cycles took place, led by the service, supported by the researchers, and steadily involving an increasing number of collaborative relationships. The action research cycles in the New South Wales site involved three phases: identifying action goals, inviting cross-sector collaborators, and cross-sector training.
Phase one: identify action goals
Following the initial research contact with staff of the service, the manager and researcher derived four action goals, which arose directly from the priorities identified in the focus groups and interviews. The manager was enthusiastic about embedding these goals in the work of the service and proposed taking them to management to link them into the service draft strategic plan. This gave the goals organisational weight and connected them into work flows (such as preparing for an upcoming audit). The four goals identified were:
- To work with the quality assurance system to make sure that all policies and procedures were current and inclusive of women with disabilities.
- To review the service strategic plan to make people with disabilities a focus. The strategic plan was under review and the research prompted thinking about how the service could prioritise women with disabilities across a number of elements of the plan. Results are to be measured using the Results Based Accountability framework the service applies across multiple programs.
- To feed into the Regional Action Group. A regional domestic violence awareness forum held shortly before the research commenced produced an action plan for the organisation, which focuses on four core areas: community education, increasing community involvement in awareness campaigns, involvement of sporting clubs, and linking services together.
- To develop a small group for women with disabilities to learn from their experiences and provide support. This responded to the expressed desires of women with disabilities participating in the focus groups to provide peer support to one other.
Involvement in the research prompted the manager to reflect on the extent to which women with disabilities were included in the strategic development currently underway in the service. This led to prioritising women with disabilities and building in processes to measure the impact of the changes over time.
Phase two: invite cross-sector collaborators
The increased focus of the service on women with disabilities was conveyed to the regional domestic violence committee with the aim of stimulating interest and collaboration across services and sectors. A short presentation was prepared by the manager, with help from the researchers, that covered information about violence against women with disabilities and the key research findings. Fifteen members of the regional domestic violence committee committed to further action. The committee added women with disabilities as a priority group to the regional action plan.
The focus of the discussions was disability; however, in addition, the group discussed the impact of poverty, Aboriginality, and cultural and linguistic diversity (CALD) on the experience of violence in regional women’s lives. For example, women from CALD backgrounds living in regional areas who experience language barriers often have to rely on family members to interpret for them. The group observed that this frequently resulted in arguments between family members and were concerned that family-member interpreters managed multiple concerns of the whole family, rather than representing the woman.
Phase three: cross-sector training
The engagement of the regional domestic violence committee raised the profile of women with disabilities in some new initiatives in the region. In recognition of the siloed approach to different services, agencies have started to come together in one location on a monthly basis to ensure cross-sector collaboration and access for women with disabilities.
A remaining area of concern in the service is workers’ skills to respond to the complex needs of women with disabilities. The manager reflected that referral between DFV and disability services remained rare, despite some improvement in on-the-ground working relationships.
A series of meetings were held with key people in the disability support sector to explore the possibility of jointly hosting training for DFV and disability support services. Due to the approaching rollout of the National Disability Insurance Scheme (NDIS), disability services felt under pressure and unable to contribute to planning at this stage; however, they remained supportive of the idea. After some consideration, the NSW site decided to host and fund the training and to offer it across sectors. A specialist trainer was sourced (with support from the researchers) to provide the training and 14 workers from DFV services, disability support services, and the state government participated. Satisfaction ratings were high and indications were that participants found accessible safety planning, the opportunity to network with people in other sectors, and learning about each other’s complementary skill sets to be of particular value. A second training session is planned with women with disabilities.
Phase four: consolidate cross-sector collaboration and internal action goals
At the time of writing, the fourth action research cycle is ongoing, with goals of consolidating the cross-sector collaboration and:
- working internally on the service quality assurance system to make sure that all policies and procedures are up to date, current, and inclusive of women with disabilities;
- reviewing the strategic plan to make women with disabilities a focus;
- feeding into the regional action group;
- developing a small support group for women with disabilities; and
- developing promotional material in Easy English language.
A constant tension at this site was balancing the agreed actions with competing priorities. Setting meetings to plan the training was helpful in progressing the action research, as each person involved had clear goals. Transformative change in the service is yet to be achieved. However, signs of change are apparent. For example, there is a desire to establish a peer support group in response to the expressed wishes of service-users and training for women with disabilities will be forthcoming. The service is also interested in investing in a “train-the-trainer” model to embed this skilled support.
Figure 5 NSW action research process
Text alternative for Figure 5:
- Identify action goals: Internally derived and fed back with researcher
- Invite cross-sector collaboration– information sharing: Results shared with researcher and internally
- Cross-sector training: Internal and external networks engaged
- Consolidate cross-sector collaboration and internal action goals: Local approaches fed into research informed practice models
Specialist crisis response services
Profiles of two additional sites that demonstrate promising practice are included here. These agencies provide specialist services to people with disabilities who have experienced sexual assault. The purpose of including these services is to identify components of the specialist models that contribute to answering the third research question concerning how services can be improved to deliver effective services for women with disabilities. The sites agreed to be profiled as part of this research; however no qualitative evaluation was done in these sites.
Queensland specialist service for people with intellectual disabilities
This specialist service works with people with intellectual or learning disabilities who have been victims/survivors of sexual violence, other crimes, or exploitation. The service provides counselling, groups, support, information and referral, community education, and training for people with intellectual disabilities. It is jointly funded for its work by state government community services and justice agencies. The service grew from the collaborative endeavours of a disability support organisation and a women’s resource centre and continues to collaborate with both of these organisations. The approach of the service is grounded in the social model of disability, which leads to a strong focus on access and building capacity in individuals, supporters, and organisations to respond effectively to violence in the lives of people with intellectual disabilities.
The model
People with intellectual disabilities who use this service engage with it in ways that they find useful. They can access individual counselling, participate in a group, and access and have input into the development of information, resources, and training. Through accessing this service, they also have the opportunity to participate in community events that engage them with violence prevention activities in the community. The service describes this as “blended support” where women (and men) come in, often through individual counselling, and then move into a group and might also participate in some one-off community events.
The second stream of service is the provision of training; there is a clear education focus for disability sector workers that includes people with disabilities as trainers. Training is provided for support workers and case managers of disability services and mainstream violence response professionals, including police, generalist counsellors, sexuality and violence counsellors, and case managers.
A third area of work of the organisations is systemic advocacy. Issues that are raised through the two streams of service provision are collated and used to lobby government and to inform government and service policies and practice. The focus is on capacity building for individuals, supporters, and organisations to respond more effectively to the needs of people with intellectual disabilities who have experienced sexual assault.
What makes the model work?
Including women and being informed by women’s experience: Women with disabilities inform the service delivery in a number of ways: through contributing ideas in regular peer support groups, via complaints and feedback systems, and in contributing to the development of training programs.
Accessibility and flexibility: The service prioritises access above all else and takes a flexible and open approach to welcoming people into the service before they are asked to consent to receiving support. The manager explained that people often cannot imagine what the service might be able to offer and may be very apprehensive, so gently introducing them to the service and what is available is critical. Prioritising access and being flexible about how people access available services (on-site, off-site, as an individual, with a partner or supporters, in groups, and at different times) means they get to “see what it’s like, what it’s all about” and then make a decision. This includes not excluding people who may, for instance, miss three scheduled sessions in a row, but instead being willing to look again at how the service can be flexible to meet their needs. Taking a flexible approach was also at times about having a gendered understanding about the experience of violence and ensuring individual’s emotional and physical safety in groups. This means, for example, ensuring that male clients are not seen when a women’s group is running.
Victorian specialist sexual assault program for people with disabilities
This specialist program provides counselling and advocacy for people with cognitive disabilities or complex communication needs who have experienced sexual assault. The model was developed as part of a decade-long campaign in Victoria to address the justice inequities experienced by people with cognitive impairments who have experienced sexual assault (Goodfellow & Camilleri, 2003). A range of legislative reforms were enacted over the same period of time in Victoria to address identified issues in the Sexual Crimes Act 2006 (Vic.) for all victims/survivors, with some specific changes recommended and implemented that referred to people with cognitive impairments (Victorian Law Reform Commission, 2004). The Federation of Community Legal Services noted, however, that significant non-legislative reforms were required to meet the needs of people with cognitive impairments (Federation of Community Legal Centres, 2011). Improved advocacy was a key issue identified in the research that informed the development of the program. Camilleri (2010) noted that advocacy for victims/survivors of sexual assault with cognitive impairments was vital and played a central role in progression of sexual assault reports by victims/survivors with cognitive impairments throughout the justice process.
The model
The program directly addresses advocacy for people with cognitive impairments or complex communication needs in three ways:
- It enhances the capacity of all counsellors and advocates in the service to work more effectively.
- It increases access to legal advocacy for victims/survivors of crime compensation.
- It addresses systemic barriers to achieving justice for clients by acting as a platform to increase sexual assault services’ involvement in research and policy advice on sexual assault of people with disabilities.
The service employs a dedicated counsellor or advocate to manage the program. This role includes:
- providing secondary consultation to other counsellors or advocates when they are working with a client with cognitive impairments or complex communication needs.
- maintaining a comprehensive resource database and providing training internally and throughout sexual assault service networks in Victoria on working effectively with clients with cognitive impairments or complex communication needs;
- providing information access for people with disabilities through the comprehensive collection of Easy English resources that were developed during the pilot program and are available online;
- funding clients to pay for additional support when they have appointments with the service the police, or to attend court dates;
- liaising with the Office of the Public Advocate to provide trained Independent Third Persons for interviews with people with disabilities who are victims/survivors of sexual assault; and
- liaising with legal service workers to enhance their practice in working with people with disabilities wishing to access crimes compensation.
What makes the model work?
For almost 2 decades the service has actively sought to improve access for victims/survivors of sexual assault with disabilities through externally funded projects. This includes the development of Easy English resources on sexual assault and in-house training on disability. They have provided leadership within the sexual assault sector on issues of access to counselling, advocacy, and justice for victim/survivors with disabilities by providing their expert input to research and a variety of community and government groups. They have also trained counsellors from a range of agencies to support women with disabilities
The program was evaluated in 2014 and a number of positive factors that influenced the program outcomes were identified:
- It provides a focus in the wider service on access for people with disabilities, thereby engaging the service not only in continual improvement to their approach but also in giving them a platform to engage more broadly in systemic advocacy about sexual assault and disability, thereby ensuring disability is considered within the broader sexual assault sector.
- The staff’s expertise as sexual assault counsellors or advocates with or without experience in disability underpins the capacity of the service to provide a very high level of service and informed practice.
- The multi-faceted approach, based on “enhancement” to counselling and legal advocacy practice, rather than “different” approaches (Frawley, 2014).
A key finding from the evaluation was that when the service focused its attention on the specific needs of people with intellectual disabilities or complex communication needs, referrals increased, as did understanding about their experiences of sexual violence. This was enhanced by the program’s collection of data and the anecdotal reflections of workers, which strengthened the service’s systemic advocacy within the sector.
Improving response services for women with disabilities
The research aimed to develop new knowledge to inform the development of guidelines for good practice in tertiary DFV services for women with disabilities in Australia. These guidelines aim to be:
- based on a thorough and critical review of evidence concerning world best practice;
- informed by the experiences of Australian women with disabilities;
- developed in collaboration with locally-based, cross-sector communities of practice; and
- designed to inform a gendered understanding about violence in the disability sector.
The review of literature that preceded this research demonstrated that a great deal of work has been carried out in the past to identify good practice principles for working with women with disabilities who have experienced violence. Three key factors stood out in the review as important for accessible, effective tertiary response services. These are physical and programmatic accessibility, cross-sector collaboration, and evidence-based practices. This research confirms the importance of these principles and expands on them.
Good practice principles
Broadly defined, “good practice” is practice that has been proven to work well and produce good results. In this section, we draw together the findings from the previous sections and discuss the findings to the third research question: in what ways can tertiary responses be improved to deliver effective services for women with disabilities based on the knowledge developed from this research?
Models and approaches
The findings of this research indicate that although they are committed to providing safety and support for women with disabilities, for the most part, DFV services do not demonstrate high levels of knowledge about support services available for women with disabilities. They rely on referral to disability services to assist women to access disability supports and benefits and only limited cross-sector collaboration was found. This is not to suggest that DFV services fail women coming to them for help. Rather, a complex “whatever it takes” approach is used to ensure the safety of women escaping violence. The flexibility of this approach helps women with disabilities in many instances, and many disability services are responsive to requests. However, simple referral without effective collaboration may leave women without appropriate support.
Both DFV and disability services may be overly protective of women with disabilities. For DFV services, this can be to avoid re-traumatising women after they have been resettled. As a result, women may not be consulted about the extent to which the service was accessible and appropriate to their needs. Furthermore, women with disabilities in this research called for opportunities to meet with other women who have experienced violence for social support and understanding. Services have not yet heard these calls and in their attempts to “protect” women, they may be denying them this important, ongoing form of support. This was recognised by services that participated in the action research phase of the project. Offering opportunities for women with disabilities to come together through the DFV services was identified as a promising approach and one that the Queensland specialist service identified as important for women with disabilities.
Two clear “categories” of women with disabilities were found within DFV services. The first group are women whose disabilities are officially recognised and who, as a result, are eligible for a range of disability support services. These women often self-identify as having disabilities or have a friend or carer who will identify her support needs when she comes into the DFV service. The second group are women who are observed by intake or caseworkers to have disabilities (such as acquired brain injuries, mental health issues, or alcohol or other drug problems), often as a result of living with violence. These women may not be immediately eligible for disability support services, even though they are needed. It is more difficult for workers to access appropriate accommodation and support for women in this second group. This difficulty is compounded by the bureaucracy involved in getting official recognition for disabilities. It is further exacerbated by a lack of cross-sector collaboration: DFV workers are not experts in the disability sector and lack knowledge and information about disability services.
A further challenge for DFV services is that women with disabilities may avoid disclosing their disabilities when they do come to a service, which has implications for what the service can provide. Women may not disclose their disability because they do not understand or trust the service or because they do not identify strongly as a woman with a disability. In some cases, women do not disclose for fear of losing custody of their children or connections with family and culture, which was particularly an issue for Aboriginal women who participated in the study. Although greater diversity was not achieved in the sample of women who participated in this study, it is possible to project that this is probably also an issue for women from CALD backgrounds. Many women with intellectual disabilities lack knowledge about domestic violence and sexual assault, so it is possible that some may not seek help until the violence becomes intolerable or is reported by a third party.
The Disability Discrimination Act 1992 (Cth) makes it unlawful to discriminate against people on the basis of their disability or perceived disability and emphasises equality of access to information and physical premises (PWDA & DVNSW, 2015). Our research suggests that for women with disabilities in need of support from DFV services, “access” is more than adapting buildings to meet physical needs of people with disabilities. Some tertiary response services have a limited understanding about disability and accessibility beyond physical access. To be truly accessible, services must be approachable, acceptable, available, affordable, and appropriate. Unless these criteria for access are met in the first place, programmatic and physical access is unlikely to be possible.
Women’s voices
Not all of the women who participated in this study found DFV services approachable, acceptable, or appropriate to their needs. Women who had not used DFV services had little knowledge that such services existed or how to get help other than going to the police if they were in a violent relationship. The police were not seen as approachable (and even seen as scary). Some women who were service /users had continued to live with violence in the past because they lacked knowledge about where to get help or that it was available.
Many of the women with disabilities interviewed for this project had long-term relationships with DFV services and disability services. These women were, for the most part, poor and living on the margins. For them, the relational nature of the support the service provided was important, as was the consistency of the support and the safety they had found. The women with disabilities who participated in this research valued above all:
- A consistent relationship with one worker rather than seeing a range of different workers.
- Being able to trust the service and their worker to maintain confidentiality and to be there for them when they are needed.
- Being treated with respect.
- Being seen as experts in their own lives and having access to the information and support they need to make their own decisions. For these women, independence and autonomy are vital; they talked about “hard-won independence”.
- Being trusted to make their own mistakes rather than being told what is best for them.
- Having access to social support, both from their workers and in groups with other women who have experienced violence in relationships.
Service improvements
Later in the research, the case study sites recognised that they had at times not acknowledged women’s experiences or trusted them as experts in their own lives. This was an important shift that creates openings to incorporate their ideas into service improvements and planning. Although not easy, given the high-pressure environments in which DFV services work, many services that participated in this research recognised that they could improve their ways of working with women with disabilities and, in particular, this could come from taking (or having) the time to reflect on the experiences and perspectives of women with disabilities. Work undertaken at the sites as part of the action research cycle demonstrates how service improvements that are informed by reflections on practice can be incorporated into practice. Through the action research cycles, services had some opportunities to stop and reflect on what women with disabilities had to say about their complex experiences seeking support after violence and abuse. DFV services are high-pressure environments that are often under time and resource pressures that limit their opportunities to stop and reflect. Through this research, this opportunity was afforded to them and, for some, the insights gained will inform future service improvements.
A “clash of cultures” was identified between DFV services and other services that support women with disabilities. Women with disabilities highlighted that there are other ways in which clashes of culture occur in relation to women’s personal and social values, their culture and sense of autonomy, and those of the service from which she seeks help. These clashes of culture can be barriers to accessibility of services but understanding and reflecting on these can also be opportunities for improvement.
Prior to the action research, the sites used a simple model of referring to disability services to address the access and support needs of women with disabilities. With support and facilitation from the researchers, services started to identify where cross-sector collaboration could contribute to improved services, and they began to develop stronger links with other stakeholders. As these relationships developed, a model emerged that involved the DFV service responding to the safety and accommodation needs of women with disabilities and referring them to disability support services, but added further steps. These involved: continuing to collaborate and engage with the service (rather than handing over to them), reflecting on the process and outcomes, and building new knowledge into the process in future. This established continuous improvement and cross-sector collaboration as underpinning principles for working with women with disabilities.
This confirms the learnings from the specialist crisis response services as models of good practice, which included:
- Working with women with disabilities who have experienced violence and abuse should not use a one-size-fits-all approach. As a woman who participated in this research put it, there is no one thing that will work for everyone”.
- The voices of women with disabilities must inform practice.
- Adequate time and flexibility must be allowed for to meet the needs of individuals.
- Stakeholders across the tertiary response sector must be brought together to deliver consistent, appropriate services to meet the needs of individuals.
- High-quality training about working with women with disabilities is essential for all workers across-sectors.
To provide effective, accessible support and safety for women with disabilities requires a coordinated service system, which is greater than standalone DFV tertiary response services. The literature review for this project draws attention to the three-level public health model for preventing violence against women, in which tertiary responses ensue after violence had already occurred. A learning from this project is that while DFV services work with women who have already experienced violence, they also play a role in preventing violence from occurring again. Disability services can assist women who have experienced violence in getting appropriate access, but they also play an important role in prevention. Rather than creating rigid distinctions between levels of prevention in the public health model, prevention and response may be better conceived of together.
Conclusions and recommendations
At the time of completing this report, the Third Action Plan 2016-2019 of the National Plan to Reduce Violence against Women and their Children 2010-2022 (Third Action Plan) was released by the Commonwealth, state, and territory governments (DSS, 2016). Women with disabilities are recognised as a priority group in the Third Action Plan and the following key national actions have been identified:
- Support the development of integrated, responsive, and more accessible services for women with disabilities.
- Explore how technologies can be better used to provide women with disabilities with safe, relevant services.
- Develop free, accredited training on domestic violence for the disability sector.
- Build evidence about the types of violence women with disabilities experience to inform future responses.
- Work with women with disabilities and disability stakeholders to explore opportunities for collaboration and identify policy priorities.
This research supports the key national actions for women with disabilities. It also contributes evidence to inform the implementation of the Third Action Plan in terms of access for women with disabilities and accessible services, cross-sector collaboration, the inclusion of women with disabilities in service development, and the collection of high-quality data to better understand how tertiary response services respond to and collaborate to prevent violence against women with disabilities.
This research aimed to inform the development of guidelines for DFV tertiary response services to respond effectively to the needs of women with disabilities. A number of promising practices were identified from this research that can be articulated as underpinning principles for effective practice. These include:
- “Accessibility” is more than providing physical access: services must be approachable, acceptable, appropriate, affordable, and available to women with disabilities.
- Women with disabilities, like all people, are complex and multi-dimensional; disability is in play with other personal and social factors. Service planning and delivery must be enhanced by the use of an intersectional lens.
- Women with disabilities need more than safety; they need social and relational support in a safe and inclusive environment.
- Service and practice planning, development, and improvement must be informed by high-quality qualitative and quantitative research. This must also be informed by the ideas and opinions of women with disabilities who have used the service.
- All aspects of tertiary response services for women with disabilities must be informed and enhanced by cross-sector collaboration.
Recommendations
To make services accessible, women with disabilities must be at the centre. Services must understand and respond to what women need and want. This research shows that what women with disabilities need and want is practical, supportive, respectful, trusting relationships with workers in services that understand them, their experiences, and their needs.
1. Promoting access and accessibility
This research finds that access for women with disabilities is about much more than simply removing barriers. Ensuring physical access is important, but service accessibility needs to be understood and promoted, so that women with disabilities know services exist that can help them, and that they will be received, acknowledged, and heard by tertiary response services. Good practice principles for accessibility suggest that services must be approachable, acceptable, affordable, available, and appropriate. Through addressing broader issues of access for disability-specific needs, the interface between what the service offers and what women with disabilities need can be better aligned. This requires a shift in how “disability”, “access”, and “accessibility” are understood.
We therefore recommend:
Services review their understanding of “disability” and “access” and draw on the evidence from this research and the work of Levesque et al. (2013) to ensure that they provide services that are:
- approachable: women with disabilities know they exist and feel comfortable to approach them;
- acceptable and appropriate: barriers to communication, housing, and understanding what is offered are removed;
- affordable and available.
2. Building cross-sector collaboration
The findings of this research indicate that DFV services are committed to providing safety and support for women with disabilities. They employ a responsive “whatever it takes” approach to ensuring their safety, which is complex, intersectional, and situational. However, DFV services may lack the time and knowledge to ensure women with disabilities have appropriate disability supports and benefits. To achieve this, they often refer women to disability services, yet only limited cross-sector collaboration was found.
Although disability services were not the subject of this research, the DFV services noted that many are responsive to requests for assistance. Nonetheless, simple referral to another service without effective collaboration may leave women without appropriate support or follow-up. There is an urgent need for the development of cross-sector collaboration that brings together all services that engage in tertiary response, including: DFV services and disability services in relation to immediate supports, and police, judicial services, housing services, and the range of other health and community services involved in supporting women with disabilities to escape from violence and access ongoing supports.
DFV services that participated in this research recognised that they could improve the way they worked with women with disabilities and began this process in the action research stage of the project. A key learning that emerged was the importance of flexibility, time, patience, persistence, and the development of trusting, respectful relationships. Those services that did embark on change processes benefited from an initial process of reflection and planning, developing relationships and then bringing all parties together for a facilitated, goal-oriented, practical process to draw on the expertise of all parties concerned to plan for high-quality, cross-sector collaboration.
Different parts of the tertiary response sector have much to learn from each other about working with women with disabilities. Cross sector collaboration will be enhanced by bringing all parties together to learn from each other and develop ways of working together. This process must be informed by the experiences of women with disabilities.
We therefore recommend:
In order to support initiatives for cross-sector collaboration, the emerging models of good practice identified in this research should be further developed and informed using a facilitated process of reflection, consultation, and engagement with other tertiary response services.
This process should aim to ensure positive outcomes for women with disabilities in all parts of the tertiary response sector through collaboration. It should not be in the form of didactic training, but should use a facilitated process that involves and is informed by women with disabilities.
3. Involving women with disabilities
For a range of reasons discussed earlier in this report, women with disabilities’ ideas and opinions do not appear to inform service improvement. In part, this is due to well-meaning efforts to protect or not re-traumatise women by re-engaging with them once their case is resolved. However, that approach results in a lack of follow-up and ongoing engagement with women.
Women in this research valued the positive and trusting relationships they developed with workers and the opportunity this gave them in some cases to have ongoing involvement with the service. They also valued practical support and opportunities for social contact with others who have shared similar experiences.
There was little evidence of women with disabilities being involved in services beyond their role of client, although when this opportunity was made available through the research in the focus groups and action research groups, women and the service staff saw value in this.
We therefore recommend:
DFV services consider establishing peer support groups for women who survived or are escaping from violent and abusive relationships.
We further recommend:
Service improvement and cross-sector collaboration must be informed by women with disabilities who have used tertiary response services. Women with disabilities should be consulted about their experiences using tertiary response services and their advice incorporated into planning and practice development.
The model of the Consultative Research Group (a group of women with disabilities engaged as research advisors in this study), which ensured that the voices of women with disabilities informed this research, could be used with future sites to contribute to both service and sector-wide reform.
4. High-quality data collection
It was clear in both the survey and case study data that measures to understand and monitor the effectiveness and outcomes of tertiary response services’ responses to women with disabilities are needed. Improving data collection will assist significantly in sustaining good practice in terms of access, inclusion, and cross-sector collaboration.
We therefore recommend:
DFV services should collect data on the disability experiences of clients. Qualitative and quantitative data measures across all programs offered in DFV services should be developed and implemented, and tied to the same measurement and reporting metrics as for other comparative data measures (e.g. age, Indigenous status, and so on). Women with disabilities should be involved in providing qualitative data and be engaged to co-produce information from it that can be used in service improvement and wider sectoral reform at local, state or territory, and national levels.
Project limitations and strengths
Disability is a complex, dynamic, and multi-dimensional lived experience and a contested phenomenon. This is highlighted in the literature review, which discussed the importance of understanding the ways that characteristics such as age, class, culture, gender, race, sexuality, and disability intersect. These aspects of identity are also affected by being a parent, partner, or lover, and connected or disconnected to family or a community.
This research was limited in a number of ways in relation to achieving diversity of research participants and diversity of geographical locality of case study sites. The scope of the project and the time frame for the project contract limited the capacity of the research to have a larger number of case study sites and therefore more geographical diversity, and the research methods used limited the gathering of demographic data. One of the case study sites has an Aboriginal program and provides services in a culturally specific site, and although there was some diversity in terms of race, culture, and experience of disabilities among the women who participated in the study, this demographic data was not collected, as discussed in the methods section. The project could also have been strengthened by working with an additional case study site, in particular a remote site.
The strengths of this project have been discussed at length in the methodology section above and throughout the report. The approach was underpinned by the principle of social inclusion for women with disabilities, as well as an understanding of intersectionality. The Consultative Research Group contributed to the planning, implementation, and analysis of all aspects of this research, as did women with disabilities from the case study sites, making it truly inclusive, participatory research.
References
Australia. Department of Social Services. (2016). Third action plan 2016-2019 of the national plan to reduce violence against women and their children 2010-2022. Canberra: DSS. Retrieved September 12, 2016 from https://www.dss.gov.au/women/programs-services/reducing-violence/third-action-plan
Australian Bureau of Statistics. (2011). Disability prevalence. Retrieved October 22, 2016 from https://www.abs.gov.au/AUSSTATS/abs@.nsf/Latestproducts/4446.0Main%20tures42009?opendocument&tabname=Summary&prodno=4446.0&issue=2009&num=&view=features42009?opendocument&tabname=Summary&prodno=4446.0&issue=2009&num=&view=
Australian Bureau of Statistics. (2012). Personal safety survey. Retrieved October 22 from https://www.abs.gov.au/ausstats/abs@.nsf/mf/4906.0
Australian Human Rights Commission. (n.d.). A quick guide to Australian discrimination laws. Retrieved October 22, 2016 from https://www.humanrights.gov.au/sites/default/files/GPGB_quick_guide_to_discrimination_laws_0.pdf
Ayre, J., Lum On, M., Webster, K., Gourley, M., & Moon, L. (2016). Examination of the burden of disease of intimate partner violence against women: Final report (ANROWS Horizons, 06/2016). Sydney: ANROWS.
Babic, M. M. (2009). Violence and persons with disability. Ljetopis socijalnog rada/Annual of Social Work, 16(3), 595-614.
Ballan, M. S., & Freyer, M. B. (2012). Self-defense among women with disabilities: An unexplored domain in domestic violence cases. Violence Against Women, 18(9), 1083-1107.
Bradbury, H. (2015). The SAGE Handbook of Action Research: Third edition. Thousand Oaks, CA: SAGE.
Camilleri, M. (2010). [Dis]abled justice: Why reports of sexual assault made by adults with a cognitive impairment fail to proceed through justice. (Doctoral dissertation). University of Ballarat, Ballarat
Chang, J., Martin, S., Moracco, K., Dulli, L., Scandlin, D., Loucks-Sorrell, M., & Bou-Saada, I. (2003). Helping women with disabilities and domestic violence: Strategies, limitations, and challenges of domestic violence programs and services. Journal of Women’s Health & Gender-Based Medicine, 12(7), 699-708.
Chenoweth, L. (1996). Violence and women with disabilities. In S. Cook & J. Bessant (Eds.), Women’s encounters with violence: Australian experiences. Thousand Oaks, CA: SAGE.
Council of Australian Governments. (2012). National implementation plan for the first action plan 2010-2013: Building a strong foundation. Canberra: FAHCSIA.
Disability Discrimination Act 1992 (Cth). Retrieved July 18, 2016 from https://www.legislation.gov.au/Series/C2004A04426
Dowse, L., Soldatic, K., Didi, A., van Toorn., & Frohmader, C. (2013). Stop the violence: Addressing violence against women and girls with disabilities in Australia: Discussion paper. Hobart: Women with Disabilities Australia.
Dowse, L., Soldatic, K., Spangaro, J., and van Toorn, G. (2016) Mind the gap: The extent of violence against women with disabilities in Australia. Australian Journal of Social Issues, 51(3), 341-359.
Equality Act 2010 (UK). Retrieved July 18, 2016 from https://www.legislation.gov.uk/ukpga/2010/15/contents
Federation of Community Legal Centres. (2011). Making rights a reality for sexual assault survivors with cognitive impairments. Melbourne: FCLC.
Flood, M. (2011). Involving men in efforts to end violence against women. Men and Masculinities, 14(3), 358-377. doi:10.1177/1097184×10363995
Frantz, B., Carey, A., & Bryen, D. (2006). Accessibility of Pennsylvania’s victim assistance programs. Journal of Disability Policy Studies, 16(4), 209-219.
Frawley, P. (1997). Training manual for Centres Against Sexual Assault: Working with victim/survivors with an intellectual disability. Melbourne: South East CASA.
Frawley, P. (2000). Sexual assault project report: Working with victim/survivors with an intellectual disability. Melbourne: Family Planning Victoria.
Frawley, P. (2014). Making rights reality: Final evaluation report 2014. Melbourne: La Trobe University.
Frawley, P., Barrett, C., & Dyson, S. (2012). Real people, core business: Living safer sexual lives: Respectful relationships. Report on the development and implementation of a peer-led violence and abuse prevention program for people with an intellectual disability. Melbourne: La Trobe University.
Frawley, P., Dyson, S., Robinson, S., & Dixon, J. (2015) What does it take? Developing informed and effective tertiary responses to violence and abuse of women with disabilities in Australia (ANROWS Landscapes, 03/2015). Sydney: ANROWS.
Frohmader, C. (2010). Women with disabilities & the human right to health: A policy paper. Melbourne: WWDA.
Frohmader, C., Dowse, L., & Didi, A. (2015). Preventing violence against women and girls with disabilities: Integrating a human rights approach. Hobart: WWDA.
García-Moreno, C., Pallitto, C., Devries, K., Stöckl, H., Watts, C., & Abrahams, N. (2013). Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and nonpartner sexual violence. Geneva: WHO.
Goodfellow, J., & Camilleri, M. (2003). Beyond belief, beyond justice. Melbourne: Disability Discrimination Legal Centre.
Hague, G., Thiara, R., & Mullender, A. (2011). Disabled women and domestic violence: Making the links: A national UK study. Psychiatry, Psychology, and Law, 18(1), 117-136. doi: 10.1080/13218719.2010.509040
Healey, L. (2015). Violence against women with disabilities: Key findings from the Voices Against Violence research project. Paper presented at the Inaugural Asia-Pacific Conference on Gendered Violence & Violations. University of New South Wales, Sydney.
Healey, L., Howe, K., Humphreys, C., Jennings, C., & Julian, F. (2008). Building the evidence: A report on the status of policy and practice in responding to violence against women with disabilities in Victoria. Melbourne: Victorian Women with Disabilities Network Advocacy Information Service.
Healey, L., Humphreys, C., & Howe, K. (2013) Inclusive domestic violence standards. Strategies to improve interventions for women with disabilities? Violence and victims, 28(1), 50-68.
Houtenville, A.J. (2009). Counting working-age people with disabilities: What current data tells us and options for improvement. Kalamazoo: Upjohn Institute.
Hughes, R. B., Lund, E. M., Gabrielli, J., Powers, L. E., & Curry, M. A. (2011). Prevalence of interpersonal violence against community-living adults with disabilities: A literature review. Rehabilitation Psychology 56(4), 302-319. doi:10.1037/a0025620
Jones, L., Bellis, M. A., Wood, S., Hughes, K., McCoy, E., Eckley, L., Officer, A. (2012). Prevalence and risk of violence against children with disabilities: A systematic review and meta-analysis of observational studies. The Lancet, 380(9845), 899-907.
Levesque, J., Harris, M. F., & Russell, G. (2013). Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. International Journal for Equity in Health, 12(1), pp 171-182. doi:10.1186/1475-9276-12-18
Lund, E. M. (2011). Community-based services and interventions for adults with disabilities who have experienced interpersonal violence: A review of the literature. Trauma, Violence & Abuse, 12(4), 171-182. doi:10.1177/1524838011416377
Martin, S. L., Coyne-Beasley, T., Hoehn, M., Mathew, M., Runyan, C. W., Orton, S., & Royster, L.-A. (2009). Primary prevention of violence against women: Training needs of violence practitioners. Violence Against Women, 15(1), 44-56. doi:10.1177/1077801208327483
McCall, L. (2005). The complexity of intersectionality. Signs, 30(3), 1771-1800
McClain, L. (2011). Women, disability and violence: Strategies to increase physical and programmatic access to victim’s services for women with disabilities. Boise, Idaho: Center for Women’s Policy Studies, Boise State University
Mejias, N. J., Gill, C. J., & Shpigelman, C.-N. (2014). Influence of a support group for young women with disabilities on sense of belonging. Journal of Counseling Psychology, 6(2), 208-220. doi:10.1037/a0035462
Mikton, C., Maguire, H., & Shakespeare, T. (2014). A systematic review of the effectiveness of interventions to prevent and respond to violence against persons with disabilities. Journal of Interpersonal Violence, 29(17), 3207-3226. doi:10.1177/0886260514534530
Mikton, C., & Shakespeare, T. (2014). Introduction to special issue on violence against people with disability. Journal of Interpersonal Violence, 29(17), 3055-3062. doi:10.1177/088626051453453
National Council to Reduce Violence against Women and their Children. (2009). Background paper to time for action: The National Council’s plan for Australia to reduce violence against women and their children, 2009-2021. Canberra: FAHCSIA.
Ortoleva, S., & Lewis, A. (2012). Forgotten sisters—A report on violence against women with disabilities: An overview of its nature, scope, causes, and consequences. North Eastern University School of Law research paper No. 104-2012. Retrieved from https://papers.ssrn.com/sol3/Papers.cfm?abstract_id=2133332
Oxford Dictionaries. (n.d.) Access—definition of access in English. Retrieved from https://en.oxforddictionaries.com/definition/access
People with Disability Australia & Domestic Violence NSW. (2015). Women with disability and domestic and family violence: A guide for policy and procedure. Sydney PWDA & DVNSW.
Powers, L. E., Curry, M. A., Oschwald, M., Maley, S. (2002). Barriers and strategies in addressing abuse: A survey of disabled women’s experiences. Journal of Rehabilitation, 68(1), 4-13.
Powers, L. E., Renker, P., Robinson-Whelen, S., Oschwald, M., Hughes, R., Swank, P., & Curry, M. A. (2009). Interpersonal violence and women with disabilities: Analysis of safety promoting behaviors. Violence Against Women, 15(9), 1040-1069. doi:10.1177/1077801209340309
Robinson, S. (2013). Preventing emotional abuse and neglect of people with intellectual disability: Stopping insult and injury. London: Jessica Kingsley.
Robinson-Whelen, S., Hughes, R. B., Gabrielli, J., Lund, E. M., Abramson, W., & Swank, P. R. (2014). A safety awareness program for women with diverse disabilities: A randomized controlled trial. Violence Against Women, 20(7), 846-868. doi:10.1177/1077801214543387
Sexual Crimes Act 2006 (Vic). Retrieved from https://www.austlii.edu.au/au/legis/vic/num_act/coa20062o2006269/
Smith, N., & Harrell, S. (2011). Forging new collaborations: A guide for rape crisis, domestic violence, and disability organizations. New York: Vera Institute of Justice.
Victorian Law Reform Commission. (2004). Sexual offences final report. Retrieved May 16, 2016 from https://www.lawreform.vic.gov.au/sites/default/files/FinalReport_0.pdf
Women With Disabilities Australia. (n.d.) Stop the violence resource compendium. Retrieved January 10, 2017 from https://www.stvp.org.au/Resource-Compendium.html
Women With Disabilities Australia. (2013) Background paper. National symposium on violence against women and girls with disabilities. Hobart: WWDA
Woodlock, D., Healey, L., Howe, K., McGuire, M., Geddes, V., & Granek, S. (2014). Voices against violence: Paper one: Summary report and recommendations. Melbourne: WWDV.
World Health Organization. (2002). World report on violence and health. Geneva: WHO.
World Health Organization. (2011a). International classification of functioning, disability, and health. Retrieved from https://www.who.int/classifications/icf/en/
World Health Organization. (2011b). Summary: World report on disability. Malta: WHO. Retrieved October 12, 2016 from https://apps.who.int/iris/bitstream/10665/70670/1/WHO_NMH_VIP_11.01_eng.pdf
Appendix A: participant information and recruitment
Plain language statement: women with disabilities
What does it take? Making services accessible to women and girls with disability who experience sexual assault and/or domestic violence
Hello,
[Insert photo]
My name is [name]. I am a researcher at [university].
I am doing a project about improving violence and abuse services for women with disability in Australia. I am working with [authors].
We want to know about what services women with disability who have experienced violence and abuse get. We want to learn what works and what needs to be improved. We hope this will help us to improve violence and abuse services for women with disability in Australia.
We are inviting women with disabilities to talk to us in either an interview or a focus group. We are talking to women with disabilities who have used services like counselling, accommodation and other services to talk about and get help after the violence has happened.
You can choose to have an individual interview with me or you can talk in a group with other women with disabilities. This is called a focus group. The interviews and focus groups will take about the same amount of time, around one hour.
If you do an interview or participate in a focus group what we talk about will be recorded using a digital recorder. Only the researchers and a person employed by the University to write the notes from these recordings will hear what we talk about.
Some of the questions might be:
How did you find out about the service? Did you know why you were going there? How did they explain this to you?
Was it easy to get to?
What was it like there? Can you describe what it was like when you got there and while you were there?
Describe the way the service worked with you. What did you do? How often did you go? Did you see the same person each time?
What is the best thing about the service?
Were there any things that weren’t so good?
What are some ways this service could be better for women with disabilities?
How could the service be improved?
There are other parts to this research. There will be some groups formed of people who work in services, women and girls with disabilities and people from other organisations who are interested in improving these services. If one of these is in your area you might be invited to join that group too.
When all of the research has been done there will be two reports written: one short report and one longer report. We will also be writing some articles for journals and presenting at conferences. Your name or any way of recognising you will not be in the reports, the presentations or anything else we say about the research.
The only time we would tell someone else about what you tell us is if we are worried that a child might be hurt in the past or the future, or if we are worried that you might hurt yourself or someone else.
Participating in this project is up to you, and if you do but then you change your mind about it later, that is ok too. You just have to tell the researchers and you don’t have to explain why. We will take the things you said out of the information we gather.
This research has been approved by the Human Research and Ethics Committee of Deakin University. If you have any complaints about the research or how we are doing it, or if you want to ask questions about your rights in the research, the person to contact is: The Manager, Office of Research Integrity, Deakin University, 221 Burwood Highway, Burwood Victoria, 3125, Telephone 9251 7129, Facsimile: 9244 6581; research-ethics@deakin.edu.au.
We know that talking about the way you got support and help after you experienced sexual assault or other abuse will be hard for you and might bring up bad memories. We will be giving you the support you need to manage this if it happens while we are talking to you or after you have talked to us.
Thank you for thinking about being involved. If you want to take part, you can say yes on the form attached to this letter. Or, you can talk it over with someone who might help you make up your mind. If you need some more information you can contact me these ways:
Contact Details
Phone
Endnotes
- Sections of the introduction also appear in the publication Frawley, P., Dyson, S., Robinson, S., & Dixon J. (2015). What does it take? Developing informed and effective tertiary responses to violence and abuse of women with disabilities in Australia. (Landscapes, 03/2017). Sydney: ANROWS ↑
- Under the National Affordable Housing Agreement. https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/BudgetReview201516/DV ↑
- This section includes material published in Frawley, P., Dyson, S., Robinson, S., & Dixon J. (2015) What does it take? Developing informed and effective tertiary responses to violence and abuse of women with disabilities in Australia (ANROWS Landscapes, 03/2015). Sydney: ANROWS. ↑
- The “bio-psycho-social” model suggests that disability or illness is due to an interaction of biological, psychological, and social factors. ↑
- “Gatekeeping” is a term used to describe the phenomenon of services excluding women with disabilities or denying them information in order to “protect them” (Frawley et al., 2012). In disability research, proxies are sometimes used to speak on behalf of people with disabilities, a process that has been labelled biased (e.g., see Houtenville, 2009). ↑