
Research report Voices from the frontline: Qualitative perspectives of the workforce on transforming responses to domestic, family and sexual violence
Dr Patricia Cullen
Research Fellow, University of New South Wales
Natasha Walker
Research Associate, University of New South Wales
Dr Maria Koleth
ANROWS
Associate Professor Dominiek Coates
ANROWS
RESEARCH REPORT
ISSUE 21 | DECEMBER 2022
ANROWS acknowledgement
This material was produced with funding from the Australian Government Department of Social Services. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from the government, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government Department of Social Services.
Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we live and work. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and emerging. We value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with First Nations peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2022

With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
ISBN: 978-1-922645-58-6 (paperback)
ISBN: 978-1-922645-57-9 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project 4AP.8 “Transforming responses to intimate partner and sexual violence: Listening to the voices of victims, perpetrators and services”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Outcome 4 – Services meet the needs of women and their children experiencing violence, and National Outcome 6 – Perpetrators stop their violence and are held to account.
Suggested citation:
Cullen, P., Walker, N., Koleth, M., & Coates, D. (2022). Voices from the frontline: Qualitative perspectives of the workforce on transforming responses to domestic, family and sexual violence (Research report, 21/2022). ANROWS.

UNSW Sydney
High St
Kensington NSW 2052
Author acknowledgement
We acknowledge the Gadigal and Bedegal people of the Eora nation on which ANROWS and UNSW stand. We sincerely thank the workforce for sharing their thoughtful and detailed perspectives. We are grateful to the “Voices” advisory committee for their generous support and insights. We recognise the contributions of the “Voices” project team, with immense thanks to Kelsey Hegarty, Laura Tarzia, Matt Addison and Mandy McKenzie for their support and collegiality, and to Lauren Hamilton and Cassandra Dawes for guidance and leadership. We also thank Sally Nathan for her advice on qualitative methodology. We wish to acknowledge everyone impacted by domestic, family and sexual violence and hope that this report contributes to better outcomes for us all.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76
Definitions and concepts
Concept
Definition
Coercive control
Coercive control is characterised by ongoing patterns of behaviours enacted with the intention of gaining control and power over victims and survivors of violence and abuse, including physical, sexual, psychological, emotional and/or financial abuse (Myhill & Hohl, 2016; Stark, 2007). It is nuanced and evolves and/or escalates over time (Stark & Hester, 2019), such that it is cumulative, insidious and sometimes hard to recognise as abuse (Stark, 2007). A classic feature of coercive control is a loss of sense of self, perception of reality and freedom for victims and survivors (Stark, 2007). A key tactic of perpetrators of coercive control is using aspects of victims’ and survivors’ identities that are discriminated against or oppressed, such as their cultural identity or ethnicity, to assert power and control (Sharp-Jeffs et al., 2018; Smyth et al., 2021). Whether coercive control should be criminalised is debated (Stark
& Hester, 2019). In Australia at the time of publishing, Tasmania is the only state or territory to have criminalised patterns of coercive controlling behaviours (Tasmania Government, 2004). New South Wales (Joint Select Committee on Coercive Control, 2021), Queensland (Women’s Safety and Justice Taskforce, 2021) and South Australia (Government of South Australia, 2022) are in the process of criminalising coercive control.
Person with disability and disabled person
When referring to people with disability or disabled people in Australia, identity-first or person-first language can be used (People with Disability of Australia, 2019). Ultimately the choice of language should be led by the person with disability or disabled person, and respected and affirmed (People with Disability of Australia, 2019). Using person-first language is seen by some as way of ensuring disability is not unnecessarily focused on or used to dehumanise and justify violence (People with Disability of Australia, 2019). However, identity-first language is preferred by some who view their disability as an inherent part of their identity (People with Disability of Australia, 2019). In the Deaf and Autistic communities, identity-first language is preferred because it also represents a connection to a wider cultural group (Brown, 2022; People with Disability of Australia, 2019). Terms that are not supported by disability
advocacy organisations include “handicapable”, “differently-abled”, “special needs” and “living with disability” (People with Disability of Australia, 2019). In this report “person with disability” and “disabled person” will both be used to acknowledge and respect individual choice.
Domestic violence
Domestic violence is violence perpetrated against a person by their current or former intimate partner. A key feature of domestic violence is establishing power and control over a partner through ongoing patterns of behaviour that create fear (Council of Australian Governments Advisory Panel, 2010). Behaviour can be criminal or non-criminal and includes physical and sexual violence as well as emotional and psychological abuse, which can include controlling finances, isolating from friends and family, humiliation, threatening children or pets, and threatening injury or death (Council of Australian Governments Advisory Panel, 2010).
Family violence
Family violence is a broad term that includes multiple forms of violence perpetrated by family members (Council of Australian Governments Advisory Panel, 2010). The wider scope of family violence includes violence perpetrated by extended family, communities and kinship networks, and as such can be the preferred terminology for violence experienced by Aboriginal and Torres Strait Islander women or within Aboriginal and Torres Strait Islander communities (Council of Australian Governments Advisory Panel, 2010; Victorian Indigenous Taskforce, 2003).
Gender inequality
Gender inequality is a social construct that describes unequal power dynamics, distribution of resources and access to opportunities between men and women (Our Watch, 2022a). As a result of gender inequality, men’s and women’s voices, ideas and work are not given equal value by society (Our Watch, 2022a). Gender inequality is a key driver of domestic, family and sexual violence in terms of reinforcing hierarchical gender stereotypes, excusing violence, justifying controlling male behaviour, and celebrating aggression and dominance as expressions of masculinity (Our Watch, 2022a).
Gender pay gap
The gender pay gap represents the difference between the average earnings of men and women (Workplace Gender Equality Agency, 2022b). It reflects the disadvantaged position of women in the workforce compared to men. This is distinct from unequal pay for the same or comparable work, which is a criminal offence. In 2020–21 in Australia, women earned $25,800 less than men and the pay gap widened for 37 per cent of employers (Workplace Gender Equality Agency, 2022a). Over a lifetime, compared to men, women will earn less and accumulate less superannuation, are less likely to be hired in senior roles and are ultimately more likely to live in poverty (Workplace Gender Equality Agency, 2022b). Despite women making up 50 per cent of the workforce, they are less than 20 per cent of CEOs (Workplace Gender Equality Agency, 2022a). Driving the gender pay gap are social and economic factors such as hiring and pay discrimination and bias, lower
wages in female-dominated industries, higher rates of women in part-time work, and lack of workforce flexibility for and gendered burden of caring responsibilities, including more time out of the workforce and domestic work (Workplace Gender Equality Agency, 2022b). In 2020–21, 12 per cent of people who took paid parental leave were male and only 51 per cent of employers offered it (Workplace Gender Equality Agency, 2022a). Additionally, 41 per cent of the female workforce is full-time compared to 67 per cent of the male workforce (Workplace Gender Equality Agency, 2022a). Gender inequality is a main driver of violence against women and addressing the gender pay gap is an important step towards ending violence against women (Ferrer-Perez et al., 2020; Heise & Kotsadam, 2015; Herrero et al., 2017).
Intersectionality
Intersectionality represents the additional burden of discrimination faced by people because of their intersecting social identities, such as age, sexuality, gender, ethnicity and cultural background, disability, religion, and migration and refugee status (Crenshaw, 1991; Victoria Department of Premier and Cabinent, 2019). The term was originally defined by Kimberlé Crenshaw in her discussion of the intersecting burdens of racism and sexism faced by Black women and violence as a manifestation of this burden (Crenshaw, 1991). Viewed through the lens of intersectionality, people who experience intersecting axes of social oppression are at increased risk of experiencing violence and/or more severe or frequent violence, as well as being at increased risk of experiencing discrimination and disregard from services and systems of support (The Equality Institute, 2017). Thereby, service responses and interventions for domestic, family and
sexual violence must have an understanding of intersectionality in terms of the impacts of additional layers of oppression, and how these may manifest for people experiencing violence, as well as work to reduce the disproportionate burdens experienced (Victoria Department of Premier and Cabinent, 2019). This means offering supports and interventions that are accessible, inclusive, non-discriminatory and responsive to the unique needs of people (Victoria Department of Premier and Cabinent, 2019).
Reproductive coercion
Reproductive coercion is the deliberate abuse of power to remove an individual’s autonomy over their reproductive health (Grace & Anderson, 2018; Marie Stopes, 2020). It can be perpetrated at an interpersonal level – directed specifically at an individual – or at a structural level where social, cultural, economic, legal and political systems enable it (Marie Stopes, 2020). Examples of interpersonal reproductive coercion include sabotaging contraception, pressuring someone into or controlling the outcome of a pregnancy, and/or non-consensual sterilisation. Examples of structural reproductive coercion include government policies and legislation, workplace policies and/or practices, and access to healthcare.
Sex and gender
Sex and gender are often used interchangeably (Canadian Institutes of Health Research, 2018). This is despite sex referring to biological attributes and gender referring to socially constructed roles, behaviours, expressions and identities (Canadian Institutes of Health Research, 2018). Sex can be characterised as female, male or intersex and is determined at birth. Comparably, gender is diverse and fluid and can change multiple times in a lifetime (Canadian Institutes of Health Research, 2018). Gender reflects the identity an individual chooses but also societal pressures and norms (Canadian Institutes of Health Research, 2018). It is important that the impact of sex and gender in experiences of violence are better understood as violence is highly gendered (Day et al., 2016). It has been established that cisgender women are more likely to experience violence than cisgender men and that transgender women are at greater risk of
violence when compared to cisgender women (Langenderfer-Magruder et al., 2016). However, in Australia, violence prevalence data is only available by sex, as gender is not captured by national data collection surveys (Australian Bureau of Statistics, 2017a, 2017b).
Sexual violence
Sexual violence is the use of coercion to obtain or attempt to obtain any sexual act or act that is directed against an individual’s sexuality (World Health Organization, 2021). It can be perpetrated by a stranger or someone known to the victim and survivor (World Health Organization, 2021). It includes rape as well as other forms of assault, such as unwanted sexual touching, sexual assault, sexual assault with implements, being forced to engage in pornography or prostitution, and being forced to watch pornography or have sex with friends of the perpetrator (Council of Australian Governments Advisory Panel, 2010).
Acronyms
Acronym
Definition
ABS
Australian Bureau of Statistics
ACCO
Aboriginal community-controlled organisation
ACCHO
Aboriginal community-controlled health organisation
AVO
Apprehended violence order
ANROWS
Australia’s National Research Organisation for Women’s Safety
AUSLAN
Australian sign language
CASA
Centres Against Sexual Assault
CBT
Cognitive behavioural therapy
COAG
Council of Australian Governments
CPI
Consumer price index
GP
General practitioner
LGBTQ+
Lesbian, gay, bisexual, transgender, queer and questioning
MBCP
Men’s behaviour change program
MARAM
Multi-Agency Risk Assessment and Management framework
NCAS
National Community Attitudes towards Violence against Women Survey
NDIS
National Disability Insurance Scheme
NFP
Not-for-profit
NGO
Non-government organisation
PSS
Personal Safety Survey
WDVCAS
Women’s Domestic Violence Court Advocacy Service
Executive summary
Background
This report presents the findings from a national survey of the workforce (service providers, managers and researchers) in the domestic, family and sexual violence sector. The survey is part of a larger national project investigating the perspectives of people with lived experience and expertise on responses to domestic, family and sexual violence in Australia, investigating “what works, what might work and what doesn’t work”. It aligns with the intended outcomes of the Commonwealth Government’s National Plan to Reduce Violence Against Women and their Children 2010–2022 (Council of Australian Governments Advisory Panel, 2010).
Aim and objectives
The overarching aim of the larger project is to develop recommendations for service and system improvements to better respond to victims and survivors, including children and young people, and perpetrators of domestic, family and sexual violence. The focus of this report is to provide insight into the workforce’s perspectives on the effectiveness and appropriateness of existing interventions and responses – in particular, what is required for successful implementation and sustainability of responses and interventions.
Method
The online survey was developed in consultation with the project’s advisory committee (see Appendix A). The survey consisted of two sections: respondent demographics and career information, and existing responses or interventions for victims and survivors, children and young people and/or perpetrators of domestic, family and sexual violence. It was distributed among expert stakeholders and their networks via email, social media and newsletter advertising and was open from November 2020 to January 2021. The survey received 199 responses, which is a response rate of 30 per cent based on direct email invitations. One hundred and four were excluded because they did not provide substantive responses beyond demographics. A total of 95 respondents were included for analysis.
The majority of respondents identified as female (n=86, 91%). Respondents were drawn from all states and territories, however most worked in Victoria (n=31, 33%), Western Australia (n=16, 17%) and New South Wales (n=15, 16%). The majority were practitioners (n=60, 63%), while fewer were service designers or managers (n=21, 22%) and researchers (n=14, 15%).
Ethics approval was granted by the University of Melbourne Human Research Ethics Committee.
Key findings
The key findings are first presented in accordance with the six outcomes from the National Plan (Council of Australian Governments Advisory Panel, 2010), namely:
- Communities are safe and free from violence
- Relationships are respectful
- Aboriginal and Torres Strait Islander communities are strengthened
- Services meet the needs of women and children experiencing violence
- Justice responses are effective
- Perpetrators stop their violence and are held to account.
Across these outcomes, we describe workforce perceptions of contextual factors that inform the perceived effectiveness and appropriateness of interventions and responses. We also present priorities and opportunities identified by the workforce as important for future directions.
To encapsulate workforce perceptions on what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators, we generated five themes:
- addressing upstream determinants of domestic, family and sexual violence
- reactivity and inequity in responses harms victims and survivors
- changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
- enabling choice and the right to self-determination
- power of connection, collective healing and compassion.
Addressing upstream determinants of domestic, family and sexual violence
This theme speaks to the need for greater investment in addressing upstream determinants of domestic, family and sexual violence. This means addressing structural barriers that create and sustain multiple and intersecting forms of inequality, which are root causes of violence in our relationships, families, schools, workplaces and communities. The workforce identified key social determinants that require an upstream approach, with the primary ones being poverty, safe and affordable housing, and equal participation in the workforce.
Much consideration was given to gender inequality and the intersections with other forms of discrimination and oppression. Issues related to gender inequality and intersectionality permeated the data, along with concern more broadly for how considerations of intersectionality have not been embedded within policy and assertions that this must change as we shape future directions. Given the complex intersections, it is imperative that we respond using a public health approach, through implementation of health promotion strategies to address upstream determinants and provide equitable and enabling authorising environments.
Reactivity and inequity in responses harms victims and survivors
This theme reflects respondents’ views that systemic changes across the full spectrum of prevention, early intervention, response and recovery are needed. The system is set up to be reactive to incidents of violence, with less resourcing and capability for early intervention and prevention. Respondents identified issues of traumatisation, re-traumatisation and ineffective responses that can harm victims and survivors. These systemic issues also reflect inadequate responses and lack of services for perpetrators, which ultimately increase harm and risk for victims and survivors. These systemic issues are closely related to inadequate resourcing of services, with narrow eligibility criteria and rigid key performance indicators that are determined by funders and do not reflect community need.
Respondents indicated the need for a trauma- and violence-informed system that considers the intersecting experiences of oppression, power and privilege. Within trauma- and violence-informed care, a decolonisation approach is integral to ensuring that across the workforce there is a shared language and understanding of colonisation and the ways in which this continues to impact our society and social care systems. Despite cultural competency training being delivered in almost all workplaces, respondents indicated that this has had limited structural impact on the capability of the workforce to deliver culturally safe services for and with Aboriginal and Torres Strait Islander peoples. To address this shortcoming, we must recognise that current frameworks and approaches are embedded within colonising structures that continue to perpetrate harm for Aboriginal and Torres Strait Islander peoples and communities. Promising approaches have been developed and
implemented by Aboriginal community-controlled organisations (ACCOs), which are typically informed by and relevant to the local context.
Changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
This theme amalgamates respondents’ views that knowledge and cultural shifts are required to better conceptualise domestic, family and sexual violence, so that our understandings consider the intersection of violence within the broader context of structural and social determinants. Deeply entrenched systemic biases are underpinned by victim blaming, which results in responses and outcomes that do not adequately hold perpetrators to account and can further victimise and traumatise victims and survivors. Respondents considered these issues in light of debates around coercive control, as well as in the contexts of young people who use violence and child protection frameworks.
An alternative model proposed by respondents was the “social entrapment” model, which avoids victim blaming and has potential to promote holistic responses that better meet the needs of victims and survivors.[1] In terms of service responses that redress misconceptions and misattribution of blame, several respondents identified a child-focused model, such as the Safe & Together model, as promising.[2]
Enabling choice and the right to self-determination
This theme draws on assertions within the previous three themes that systemic biases, inequities and victim blaming constrain choice and resourcefulness that are essential for victims and survivors. Indeed, respondents assert that the systems that are intended to enable safety and agency can entrench victims’ and survivors’ isolation, mistrust and helplessness.
Respondents emphasised how critical choice and self-determination are for victims and survivors. Importantly, respondents asserted that these can be further constrained for those for whom mainstream services do not adequately meet needs for cultural safety, inclusion and accessibility. While resourcing is an issue that constrains choice, respondents also pointed to widespread inconsistencies in access to supports that stem from limited and inconsistent access to appropriate information about rights and options. Respondents attributed this to shortcomings in workforce capability and knowledge, and this also reflects the need for broader systemic shifts toward trauma- and violence-informed responses to promote choice, dignity and agency.
Power of connection, collective healing and compassion
Respondents emphasised that while there are systemic issues that can be powerful in enacting and compounding victims’ and survivors’ experiences of trauma, there are also systemic strengths that are powerful in generating healing and recovery. Fundamental to recovery and healing are our shared experiences, which bring opportunities for connection and compassion. Building therapeutic relationships is a key aspect of healing from violence, and one of the workforce’s main strengths lies in its relational capacity, with many members highly skilled in compassionate and trauma- and violence-informed responses.
The workforce pointed to innovative and promising solutions, particularly in terms of moving beyond crisis interventions to embrace the full spectrum of prevention, early intervention and recovery. Supporting the healing and recovery of victims and survivors, children and young people and people who use violence was also identified as a key component of violence prevention and important for averting intergenerational trauma.
Conclusion
This report presents findings from a national survey of 95 service providers and researchers across the domestic, family and sexual violence workforce. Respondents identified key systemic issues around resourcing, capability and inequitable policy. These shortcomings drive ineffective responses, constrain interventions and contribute to harm for victims and survivors and children and young people. Many of these effects were attributed to inherent reactivity across the system and dominant understandings of domestic, family and sexual violence, which entrench victim blaming and coalesce with social determinants of health, structural inequities and colonialism. This manifests in responses and interventions that do not adequately hold perpetrators to account and do not effectively recognise and respond to victims’ and survivors’ needs, strengths and resistance.
By contrast, responses that embrace complexity and enable choice and self-determination are highly regarded. With adequate resourcing and workforce strengthening, systemic strengths in collaboration, connection, collective healing and compassion can be further harnessed to create powerful shifts in addressing the full spectrum of prevention, early intervention, response and recovery.
The workforce called for a public health approach to address the social determinants of health that intersect and impact victims and survivors, children and young people and perpetrators. Key to redressing systemic inequities and gaps is implementing strengths-based approaches that are trauma- and violence-informed and decolonising across health, justice and social services. Enabling policy and substantial investment is critical to address inadequate resourcing, strengthen workforce capability and bring forth innovative responses.
Key recommendations
Our findings point to important opportunities and priorities for service and system improvement, with recommendations across four key areas:
- Promote safer communities, workplaces, schools and homes.
- Enhance workforce competency, capability and collaboration across sectors.
- Break intergenerational cycles of violence and trauma by better supporting children and young people.
- Bring forth innovative solutions.
Promote safer communities, workplaces, schools and homes
Recommendations to promote safer communities, workplaces, schools and homes are underpinned by the recognition of domestic, family and sexual violence as a social determinant of health. Accordingly, these recommendations seek to ensure that domestic, family and sexual violence is addressed within the context of its intersection with other social determinants, such as safe housing and communities; income equality; workforce participation; social inclusion and non-discrimination; and equitable access to justice, healthcare and social services.
Recommendation 1
Prioritise safe and affordable housing solutions by governments to address critical shortages and bottlenecks in emergency housing, as well as shortages in other short- and long-term housing. Universal design principles are essential to ensuring that housing solutions are appropriate and accessible for all.
Recommendation 2
Provide federally funded and accredited community bystander training to mobilise and equip individuals to recognise and respond to domestic, family and sexual violence.
Training should be free and co-produced with lived expertise advocates.
Recommendation 3
Recognise the importance of workplaces and educational settings for generating community change in knowledge, attitudes and behaviours. In educational settings, implementation of nationally consistent curricula on consent, healthy relationships and domestic, family and sexual violence must be supported, for example by funding local violence prevention practitioners to deliver additional training and support to schools.
In workplaces, violence prevention and anti-violence initiatives are important to enable a safe work environment for all, as is implementation of specific policies that have been developed to support victims and survivors, such as paid domestic violence leave policy. The implementation of such initiatives requires ongoing monitoring and evaluation to determine uptake and effectiveness.
Enhance workforce competency, capability and collaboration across sectors
Recommendation 4
Increase core funding for frontline services, with built-in mechanisms to account for consumer price index (CPI) and award wage increases, as well as flexible support packages and emergency funds, which can be mobilised rapidly to frontline services following disasters. Funding cycles should be a minimum of three to five years to ensure frontline services are sustained. Funding packages must allow for flexibility and tailoring to local contexts, with resourcing to introduce responses that have been shown to be effective in similar contexts as well as capacity to implement new and context-specific responses.
Recommendation 5
Develop nationally accredited workforce training that can be tailored to health, police, magistrates and child welfare, which draws on the social entrapment model of violence and principles of trauma- and violence-informed care. This training should be co-designed by those with professional and lived experience and expertise.
Recommendation 6
Mandate training in the Safe & Together model for those working in child protection and related services including police, magistrates, judicial registrars and expert witnesses. Expand Safe & Together training to be accessible to those working with families across health, education, legal and related services.
Recommendation 7
Fund targeted research, that is led by Aboriginal and Torres Strait Islander peoples and communities, to investigate and implement decolonising approaches to enhance workforce competency and capability.
Break intergenerational cycles of violence and trauma by better supporting children and young people
Recommendations to address intergenerational cycles of violence and trauma by better supporting children and young people are underpinned by recognition of children and young people as victims and survivors in their own right. This recognition should be embedded in policy and practice guidelines and must be accompanied by greater investment in child-specific interventions.
Recommendation 8
Fund targeted research to establish evidence of effectiveness of therapeutic interventions for young people who are victims and survivors and those who use violence.
Recommendation 9
Fund targeted research to establish evidence of effectiveness of promising whole-of-family approaches which use a child-focused lens, with a view to supporting expanded implementation.
Recommendation 10
Re-evaluate the roles, responsibilities and training needs of Independent Children’s Lawyers, family report writers and other child court experts to ensure that there are independent and robust assessments of a child’s best interests in circumstances of family violence and other safety concerns. This will help to inform decision-makers and provide an effective voice for children as victims and survivors in their own right.
Bring forth innovative solutions
Recommendation 11
Build on promising digital and telehealth solutions that emerged as innovations during the COVID-19 pandemic to improve equitable access to services, including use of interpreters. Consider hybrid and hub models for digitally enabled service delivery to regional and remote locations to enable outreach options and strengthen collaboration with local services.
Recommendation 12
Invest in implementation of secure platforms for operational information sharing that were advanced during the pandemic. This must be accompanied by legislation, guidelines, training and practice resources to support information sharing.
Recommendation 13
Invest in therapeutic interventions that are focused on long-term health, healing and recovery, such as trauma-specific services. This requires adequate resourcing of therapeutic interventions delivered by health services including Aboriginal community-controlled organisations. An important component of this is alternatives to criminal justice responses, such as therapeutic court interventions, as well as prison throughcare programs and family restoration programs.
Introduction
In Australia, domestic, family and sexual violence is disproportionately experienced by women. In its 2016 Personal Safety Survey (PSS), the Australian Bureau of Statistics (ABS) reported that, since the age of 15, women were three times more likely to experience partner violence compared to men (one in six women and one in 16 men; Australian Bureau of Statistics, 2017a). This included physical and sexual violence by a current or former partner. Additionally, one in four women experienced emotional violence from a partner, compared to one in six men, and one in five women experienced sexual violence compared to one in 20 men (Australian Bureau of Statistics, 2017a). Between 2005 and 2016, the rate of partner violence against women has remained stable; between 2012 and 2016, the rate of sexual violence against women has increased (Australian Bureau of Statistics, 2017a). This is despite the rate of
total violence in Australia decreasing, which largely reflects rates of physical violence perpetrated against men decreasing (Australian Bureau of Statistics, 2017a).
The risk and complexity of experiencing domestic, family and sexual violence is higher for some women and communities in Australia (Australian Bureau of Statistics, 2017a; Australian Institute of Health and Welfare, 2019). Viewed through the framework of intersectionality (see “Definitions and concepts”), social identities intersect along axes of power. For victims and survivors who experience intersecting axes of oppression and discrimination, the experiences and impacts of violence can be more complex and severe, and they occur in the context of greater barriers to reporting and accessing effective support and service responses.
Children and young people who have experienced domestic, family and sexual violence are victims and survivors in their own right. When there is violence occurring in the home, children and young people experience this by seeing, hearing and/or being involved (Australian Bureau of Statistics, 2017a; Kulkarni et al., 2011; Richards, 2011). Not only do experiences of violence in the home have negative health, social and developmental consequences for children and young people, they are also associated with physical and sexual child abuse (Gracia et al., 2017; Hamby & Grych, 2013; Richards, 2011). Children who experience violence are also at higher risk of using violence in adolescence or adulthood (Child Family Community Australia, 2014; Roberts et al., 2010).
It is well recognised that current service system responses to domestic, family and sexual violence are complex and difficult to navigate (Council of Australian Governments, 2019). Often victims and survivors require access to multiple services across different sectors, including health, justice and specialist domestic, family and sexual violence services. Across and within sectors, services are frequently fragmented and siloed (Neave et al., 2016; NSW Ministry of Health, 2019). This results in victims and survivors needing to repeat their story multiple times, which can lead to re-traumatisation (Salter et al., 2020). At a systems level, the impact of service fragmentation is limited knowledge translation and coordination (Government of Western Australia, 2020; Neave et al., 2016; NSW Government, 2019).
Services are generally funded for crisis intervention and are not resourced to provide comprehensive responses to the intersecting and long-term health, economic and social consequences of abuse (Neave et al., 2016; Salter et al., 2020; Trevillion et al., 2014). This is compounded by a lack of consistent responses within sectors and the time-limited requirements of service delivery models (Neave et al., 2016). As a result, there is little focus on medium- and long-term recovery, especially for women with multiple, long-term or complex needs (Neave et al., 2016; Salter et al., 2020; Trevillion et al., 2014). To address these shortcomings, a greater understanding of the service experiences and support needs of victims and survivors, children and young people and perpetrators is needed – in particular, the unique and diverse needs of specific groups of people who are at higher risk of experiencing violence.
Since 2013, national and state-based surveys and censuses have attempted to capture the gaps and challenges faced by workers who engage with individuals impacted by violence (Cortis et al., 2018; Department for Victorian Communities, 2021; NSW Health, 2014). They provide an important perspective on who is responding to domestic, family and sexual violence and workforce issues such as confidence, collaboration, training and resourcing. However, they have not investigated what workers find effective and ineffective in responding to victims and survivors, children and young people and perpetrators.
This report forms part of a larger national project on the responses to domestic, family and sexual violence in Australia that is focused on amplifying the voices of victims and survivors, perpetrators and the domestic, family and sexual violence workforce. This report presents findings from a survey of the workforce including service providers, managers and researchers who are experts through their experience working in the sector.
Aims of the study
This study uses an online qualitative survey to explore the lived experience of service providers, managers and researchers who are experts across health, justice and specialist family, domestic and sexual violence services in order to understand, from their perspectives, “what works, what might work and what doesn’t work” in response to domestic, family and sexual violence.
Background
National policy context
In Australia, addressing violence against women and children is a national priority. The National Plan to Reduce Violence against Women and their Children 2010–2022 (the National Plan), established in 2010, represents a national framework for action to reduce domestic, family and sexual violence. A new National Plan is under development and expected to commence in late 2022 when the current plan ends.
Implemented over 12 years in four phases, the first National Plan was framed by six outcome areas that are focused on achieving reduced prevalence of and deaths related to violence, a reduced proportion of children experiencing family violence, and an increased proportion of women who feel safe in their communities (Council of Australian Governments Advisory Panel, 2010). The findings of this report will be framed under these six outcomes:
- The first outcome of the National Plan is that communities are safe and free from violence, demonstrated by community attitudinal changes.
- The second outcome is that relationships are respectful, demonstrated by young people’s improved attitudes towards, and skills and behaviour in, respectful relationships.
- The third outcome is that Aboriginal and Torres Strait Islander communities are strengthened, demonstrated by a reduced perception that violence is an issue in these communities and an increase in prevention efforts.
- The fourth outcome is that services meet the needs of women and children experiencing violence, demonstrated by improved access to and responsiveness of services for victims and survivors.
- The fifth outcome is that justice responses are effective, demonstrated by an increase in reported domestic violence and sexual assault.
- The sixth outcome is that perpetrators stop offending and are held to account, demonstrated by a reduction in perpetration.
In 2015, the Council of Australian Governments (COAG) endorsed the National Outcome Standards for Perpetrator Interventions (Council of Australian Governments, 2015), which is a set of principles to measure and assess the effectiveness of perpetrator interventions. In the same year the Advisory Panel on Reducing Violence against Women and their Children was established to advise COAG on violence against women. On 1 April 2016 they submitted a report to COAG that identified six areas for action and 28 recommendations that COAG considered in the development of the Third Action Plan of the National Plan (Council of Australian Governments, 2016).
The Fourth Action Plan, building on the progress of the previous three action plans, sets out five national priorities to guide responses to violence against women and children between 2019 and 2022 (Council of Australian Governments, 2019). The priorities are:
- Primary prevention is key:
-
- Implement coordinated and targeted interventions.
- Promote gender equality, respect for women and healthy and safe relationships.
- Address intergenerational trauma for Aboriginal and Torres Strait Islander peoples.
- Support Aboriginal and Torres Strait Islander women and their children:
-
- Engage Aboriginal and Torres Strait Islander expertise.
- Innovate on alternative models of support.
- Build workforce capacity to respond in a culturally safe way.
- Address immediate impacts and underlying drivers of violence.
- Respect, listen and respond to the diverse lived experience and knowledge of women and their children affected by violence:
-
- Implement community-led and tailored initiatives.
- Address complex forms of violence and the disproportionate impact of violence on particular groups.
- Respond to sexual violence and sexual harassment:
-
- Promote informed consent, bodily autonomy and respectful relationships.
- Strengthen capacity of sectors to respond.
- Deliver client-centred, trauma-informed, specialised and consistent support.
- Improve support and service system responses:
-
- Focus on safety and recovery for victims and survivors and trauma-informed support for perpetrators.
- Collaborate across services, sectors and workforces.
- Build the evidence base.
- Improve access to accommodation for victims and survivors.
In 2019, the National Women’s Health Strategy 2020–2030 (Commonwealth of Australia, 2019) outlined the national approach to improving health outcomes for women and girls in Australia. The health impacts of violence against women and girls are included as a priority area to raise awareness, and address the health and related impacts, of domestic, family and sexual violence, and co-design and deliver safe and accessible services for women experiencing violence (Department of Health, 2018).The Strategy includes five key priority areas that inter-relate and overlap such that improvements in one priority area positively influence other priority areas. The other priority areas are maternal, sexual and reproductive health; healthy ageing; chronic conditions and preventive health; and mental health.
In order to raise awareness of the health impacts of violence, the Strategy has committed to promoting peer education of children, young people and adults, as well as developing an awareness campaign on the physical and mental health impacts of violence. In terms of addressing health and related impacts of violence, the Strategy has committed to developing innovative models of care that provide access for women who disproportionately experience violence, as well as increasing the capacity of the health workforce to respond to violence. The Strategy also emphasises the importance of co-designing and delivering safe and accessible services by improving access to and investment in crisis intervention support, pathways to recovery, and freely accessible information and support services.
The key measures of success for the priority area addressing the health impacts of violence include:
- an increase in the number of services available and women accessing services
- a decrease in deaths from physical violence
- a reduction in the proportion of women who have experienced abuse or trauma
- a reduction in the rate of reproductive coercion
- a reduction in the gap in mental and physical health trajectories between women who have and have not experienced violence.
In 2021, the House of Representatives Standing Committee on Social Policy and Legal Affairs published a report on their Inquiry into family, domestic and sexual violence (Commonwealth of Australia, 2021). A key recommendation was the development of national data collection for service systems and improved understanding of the experiences of Aboriginal and Torres Strait Islander victims and survivors and communities impacted by violence.
Also in 2021, the National Association of Services Against Sexual Violence was commissioned by the Commonwealth Government to publish the third edition of the Standards of Practice Manual for Services Against Sexual Violence (National Association of Services Against Sexual Violence, 2021). The Standards are intended to act as a guideline to ensure services provide accessible, quality and consistent care.[3]
The Commonwealth Government is currently in the process of developing the National Plan to End Violence against Women and Children 2022–2032 (Department of Social Services, 2022). This will replace the current National Plan, which ends mid-2022. It will be underpinned by two five-year action plans, including separate action plans dedicated to Aboriginal and Torres Strait Islander peoples.
All state and territory governments have separate policies on addressing violence in line with their commitment to the National Plan and accompanying action plans.
Victims and survivors of violence in Australia
The health, economic and social consequences of domestic, family and sexual violence are extensive and impact victims and survivors, children and young people, perpetrators, and communities (World Health Organization, 2014). For victims and survivors, experiences of violence and the accompanying trauma contribute to the burden of disease and can have acute and chronic health consequences (Dillon et al., 2013; Walker, Beek, et al., 2020; Webster, 2016). For women aged 18 to 44, in 2016 it was estimated that 5.1 per cent of the burden of disease was due to intimate partner violence (Webster, 2016). Poor mental health outcomes are the most reported health consequence of intimate partner violence (Ayre et al., 2016; Dillon et al., 2013; Oram et al., 2022; Szalacha et al., 2017; Webster, 2016). Experiences of violence can also impact victims’ and survivors’ employment and housing security (Webster, 2016). The yearly economic cost of
violence against women and children is estimated to be $22 billion (KPMG, 2016). This cost is borne by victims and survivors, children, perpetrators, families, friends, communities, employers and the Australian Government (KPMG, 2016).
In Australia, the following peoples and communities experience a disproportionate burden of domestic, family and sexual violence, along with greater barriers to accessing appropriate and effective justice, safety and support. However, as aforementioned, experiences of domestic, family and sexual violence coalesce with other intersecting axes of oppression, disadvantage and stigmatisation. Accordingly, peoples’ and communities’ experiences must be viewed through an intersectional lens, to understand how experiences of violence can be compounded by other inequities and experiences of trauma.
Aboriginal and Torres Strait Islander women experience a disproportionate burden of violence. This reflects the ongoing impact of colonisation, racism and intergenerational trauma that maintains interpersonal and structural violence and compounds the consequences of violence (Blagg et al., 2015; Blagg et al., 2018; Nancarrow, 2010). For example, as a result of intergenerational trauma related to the Stolen Generation, Aboriginal and Torres Strait Islander women are reluctant to report violence and seek support for fear of losing custody of their children or of their children being placed in the out-of-home care system (Langton et al., 2020). This contributes to the under-reporting of domestic, family and sexual violence in Aboriginal and Torres Strait Islander communities (Willis, 2011). Additionally, there is an assumption that violence experienced by Aboriginal and Torres Strait Islander
women is mainly perpetrated within communities and by Aboriginal and Torres Strait Islander men. However, this is a narrow conception of violence with a colonial legacy (Clark, 2014; Walker, Mackean, et al., 2020). There is anecdotal evidence that non-Indigenous men perpetrate a significant proportion of the violence experienced by Aboriginal and Torres Strait Islander women (Our Watch, 2018).
Adults who experienced violence as children have a higher risk of experiencing violence in adulthood (Australian Institute of Health and Welfare, 2019). A recent meta-analysis found the average prevalence of recurrent sexual violence in adulthood was almost 50 per cent (Walker et al., 2019).
Culturally and linguistically diverse women, including refugee women and migrant women, experience unique forms of violence including forced marriage, female genital mutilation and dowry-related violence (Neave et al., 2016), as well as more severe and prolonged violence compared to women who are not from culturally and linguistically diverse backgrounds (Ayre et al., 2016). For example, women who are from culturally and linguistically diverse backgrounds are more likely to experience multi-perpetrator family violence compared to women who are not (Salter, 2013; Vaughan et al., 2016). For women in a relationship with Anglo-Australian men, violence can include race- or religion-based discrimination (Vaughan et al., 2016). For many culturally and linguistically diverse women, these experiences are compounded by experiences of trauma and violence that relate to their refugee or immigrant experience (Vaughan et al., 2016).
LGBTQ+ communities disproportionately experience violence, with lesbian and bisexual women and trans women experiencing the biggest burden of violence compared to cisgender, exclusively heterosexual people and men in same-sex relationships (Edwards et al., 2015; Gebicki et al., 2018; Hill et al., 2020; Langenderfer-Magruder et al., 2016; Szalacha et al., 2017). However, in Australia there are no national estimates of the prevalence of violence against women who identify as gender diverse and/or in a sexual minority group because the PSS does not collect data on LGBTQ+ identity. In 2022 the Australian Research Centre in Sex, Health and Society (ARCSHS) published a national survey of the health and wellbeing of 6,835 LGTQ+ people (Hill et al., 2020). Forty-two per cent of participants reported having ever been in an intimate relationship where they were abused by their partner and 39 per cent reported
ever being abused by a family member (Hill et al., 2020). This echoed a 2021 ARCSHS report on the experiences of 6,418 LGBTQA+ people aged 14 to 21, in which 43 per cent of participants experienced one or more forms of homelessness because of family violence, often related to family rejection (Hill et al., 2021).
Older women (> 65 years) are at risk of experiencing elder abuse, defined as violence that occurs in a relationship with an expectation of trust, such as an intimate partner relationship (WHO, 2018). For Aboriginal and Torres Strait Islander women, there is an increased risk of elder abuse from the age of 50. Older women are more likely to experience emotional and sexual violence than physical violence (Meyer et al., 2020; Pathak et al., 2019).
Women who are or have been incarcerated have high rates (>70%) of domestic, family or sexual violence histories (Justice Health & Forensic Mental Health Network, 2017). In many cases, offending is associated with experiences of violence, for example driving without a license to flee, or self-defence (Bevis et al., 2020). Being incarcerated can also mimic experiences of abuse and lead to re-traumatisation and complex trauma (Day et al., 2018; Stathopoulos et al., 2012). Additionally, a Queensland study found women who have a history of incarceration are 16 times more likely to die from violence (Willoughby et al., 2020).
Pregnant women often experience violence for the first time during pregnancy, or the severity of existing violence increases (James et al., 2013). In the PSS, during pregnancy, one in five women experienced violence from a current partner and almost half experienced violence from a previous partner (Australian Bureau of Statistics, 2017a). The risk of violence during pregnancy is more pronounced for young women (Brownridge et al., 2011). Women who experience violence during pregnancy are also three times more likely to experience depression (Brown et al., 2015).
Sex workers experience a high burden of domestic, family and sexual violence in their lifetime (Decker et al., 2013; Muldoon et al., 2015). In a Queensland study of female sex workers’ health there was a high prevalence of child sexual abuse history among participants (Seib et al., 2009). However, the literature is limited on the prevalence of domestic, family and sexual violence among sex workers in Australia and the majority of evidence focuses on violence that occurs within the context of sex work (Decker et al., 2010; Shannon et al., 2008; Shannon et al., 2009).
Socio-economically disadvantaged women are 1.5 times more likely to experience violence compared to women living in areas of least disadvantage (Australian Bureau of Statistics, 2017a). Additionally, prolonged experiences of violence can compound and/or produce financial stress and precarity, which can be related to financial abuse and impacts on employment (Cortis & Bullen, 2016).
Women living in rural and regional communities are 1.4 times more likely to experience violence than women living in major cities (Australian Bureau of Statistics, 2017a). In 2018, women living in remote and very remote areas were 24 times more likely to be hospitalised for violence compared to people living in major cities (Australian Institute of Health and Welfare, 2019). These experiences of violence are compounded by small, tight-knit communities with cultures of silencing and denying violence, as well as limited support services (Blagg et al., 2015; Owen & Carrington, 2015).
Women with disability and disabled women experience more prolonged and severe violence that leads to serious injuries compared to women without disability (Australian Bureau of Statistics, 2017a; Didi et al., 2016). In the 2016 PSS, women with disability or disabled women were 1.8 times more likely to experience intimate partner violence in the previous year and 1.7 times more likely to have experienced sexual violence since the age of 15 compared to women without disability (Australian Bureau of Statistics, 2017a). Additionally, one third of adults who have experienced sexual harassment have a disability or are disabled (Australian Bureau of Statistics, 2017a). Re-occurrence is common for women with disability or disabled women, as violence is more likely to be perpetrated by multiple male perpetrators throughout a lifespan (Australian Bureau of Statistics, 2017a). People with psychological or
intellectual disability are more likely to experience domestic, family and sexual violence compared with other disabilities (Australian Bureau of Statistics, 2017a).
Women who have separated from their partner can experience violence for the first time or an escalation in violence perpetrated by their partner (Bruton & Tyson, 2017). In the PSS, one in seven women reported violence for the first time during a separation and 14 per cent reported an increase in violence (Australian Bureau of Statistics, 2017a). Of women who separated from a partner who used violence, two in five continued to experience violence by this partner post-separation (Australian Bureau of Statistics, 2017a).
Young women (aged 15 to 34) are more likely to experience domestic, family and sexual violence compared to all other age groups. In the PSS, young women were 2.7 times more likely to experience intimate partner violence compared to women over 35 years old (Australian Bureau of Statistics, 2017a), and in 2017 women aged 15 to 34 made up more than half (53%) of female sexual assault victims and survivors recorded by the police (Australian Bureau of Statistics, 2017a). Since the start of COVID-19, young women (18 to 24) have experienced the highest rates of all types of violence compared to other age groups (Australian Institute of Health and Welfare, 2021a).
Children and young people
Frequently, children and young people’s experiences of family and domestic violence are described as “witnessing” violence, however this description is limited as it does not capture the various ways children can experience and be exposed to violence (Humphreys, 2007). Experiences of domestic and family violence can also include being used as a hostage, being asked to spy on a parent, being blamed for violence or attempting to intervene to stop the violence (Richards, 2011). Emotional abuse can also include former partners lying to children with the intention of turning them against their parent, or threatening to take the children away (Australian Bureau of Statistics, 2017a).
In the PSS, 50 to 68 per cent of children had seen/heard violence perpetrated by a parent or a parent’s current or former partner, and before the age of 15 one in eight women witnessed violence towards their mother by a partner and one in 20 witnessed violence towards their father by a partner (Australian Bureau of Statistics, 2017a). In 2019 to 2020, the most common primary type of child abuse recorded by child protection services was emotional abuse, which included children’s “exposure” to family violence (Australian Institute of Health and Welfare, 2021b).
The Family Law Act 1975 (Cth) explicitly states that exposure to violence is child abuse in s 4(1). However, whether it is classified as abuse is usually dependent on the frequency and nature of the violence the child or young person experiences (Richards, 2011). Additionally, the application of the legislation has been criticised for placing an unfair burden on victims and survivors to prevent children’s experiences of violence (Flood & Fergus, 2008; Kaufman & Little, 2003). For Aboriginal and Torres Strait Islander women this can intersect with historical and intergenerational trauma related to the state-sanctioned removal of Aboriginal and Torres Strait Islander children, and also the contemporary over-representation of Aboriginal and Torres Strait Islander children in out-of-home care (Humphreys, 2007, 2008).
Experiences of domestic and family violence are often associated with physical and sexual child abuse (Bedi & Goddard, 2007; Gracia et al., 2017; Hamby & Grych, 2013; Richards, 2011). When children directly experience physical violence in the family context, it is usually perpetrated by an adult in a position of trust such as a parent, guardian or partner of a parent/guardian (Australian Bureau of Statistics, 2017a; Campo, 2015). Co-occurrent experiences of child abuse are more likely to occur when violence is more severe and frequent (Kaufman & Little, 2003). However, the prevalence of children’s co-occurring experience of domestic and family violence and experience of sexual abuse is not clear because it is under-reported and/or reported as emotional or physical abuse (Australian Institute of Health and Welfare, 2021b; Richards, 2011).
For children who experience violence there can be ongoing health, social and developmental issues that extend beyond childhood, into adolescence and adulthood (Campo et al., 2014; Webster, 2016). These include mental health difficulties, unemployment, homelessness and impaired cognitive functioning (Campo et al., 2014; Ellonen et al., 2013; Oram et al., 2022; Richards, 2011). Additionally, experiencing violence in childhood is associated with intergenerational transmission of domestic, family and sexual violence perpetration or victimisation (Ehrensaft et al., 2003; Oram et al., 2022; Richards, 2011).
Perpetrators
Perpetrators of domestic, family and sexual violence are more likely to be male (Australian Bureau of Statistics, 2017a; Australian Institute of Health and Welfare, 2018). In the PSS, three in four instances of intimate partner violence were perpetrated by a male former or current partner and 99 per cent of intimate partner violence perpetrated against female victims and survivors was perpetrated by a current or former male partner (Australian Bureau of Statistics, 2017a). This is also true for femicide, the killing of women. In Australia between 2010 and 2018, 77 per cent of intimate partner homicide was perpetrated by male offenders (Australian Domestic and Family Violence Death Review Network & Australia’s National Research Organisation for Women’s Safety, 2022).
The perpetration of domestic, family and sexual violence is associated with a history of experiencing violence, including experiencing violence as a child or young person, and a history of trauma (Australian Institute of Health and Welfare, 2019; Neave et al., 2016). In a recent report on male-perpetrated intimate partner homicide, 54 per cent of offenders reported a history of trauma (Boxall et al., 2022).
Who is responding to domestic, family and sexual violence?
Services within the sector in Australia that directly respond to domestic, family and sexual violence include health, justice, welfare and specialist domestic, family and sexual violence services.
Specialist domestic, family and sexual violence service providers in Australia include but are not limited to:
- shelters, refuges or homelessness services
- domestic and family violence courts and court support services
- family violence and women’s legal services
- specialist domestic and sexual violence counselling services (telephone, online, in person)
- sexual assault services
- violence, abuse and neglect services
- men’s behaviour change programs
- crisis support, including helplines and emergency payments
- outreach services
- community organisations.
Mainstream services provide a range of services that are not specific to domestic, family and sexual violence but are accessed by people who experience and perpetrate domestic, family and sexual violence. The mainstream services responding in the justice, health and welfare sectors include but are not limited to:
- police
- legal aid
- community legal centres
- court advocacy programs for victims and perpetrators
- courts and tribunals
- child protection
- Aboriginal community-controlled organisations (ACCOs)
- Aboriginal and Torres Strait Islander legal services
- Aboriginal community-controlled health organisations (ACCHOs)
- women’s health centres
- primary healthcare
- social work
- community health
- allied health
- maternal and child health
- mental health
- alcohol and other drugs
- housing services
- ambulance and emergency department
- aged care
- public health programs and health promotion organisations
- disability support
- dental.
In recent years, surveys and censuses of the workforce responding to domestic, family and sexual violence have attempted to capture the characteristics of the workforce, as well as the gaps and challenges from workers’ perspectives (Cortis et al., 2018; Department for Victorian Communities, 2021). In 2017 a national survey was conducted of workers in services used by people affected by domestic, family and sexual violence (Cortis et al., 2018). In 2019 to 2020 a similar survey was conducted in Victoria of specialist and primary prevention workforces and the broader workforces that intersect with family violence (Department for Victorian Communities, 2021). Both surveys considered issues related to confidence, collaboration, training and resourcing.
Three in five specialist workers in the Victorian survey reported they were extremely or very confident to respond to family violence, while only 28 per cent of workers felt confident in the broader workforce that responds to family violence, including health, justice and social services (Department for Victorian Communities, 2021). In the national survey, workers felt more confident recognising and responding to physical and emotional abuse, compared to financial and sexual abuse, and considered collaboration and sharing information as the most important additional support to increase confidence (Cortis et al., 2018). Respondents identified that the main barriers to collaboration were limited knowledge of services and systems available, lack of specific protocols facilitating collaboration and a lack of time to build networks (Cortis et al., 2018).
In the national survey, the top five areas workers wanted more training in were risk assessment, therapeutic approaches, legal training, general counselling and screening (Cortis et al., 2018). Additionally, the majority of participants wanted more training on how violence impacts, and is experienced by, specific groups including people with disability or disabled people, Aboriginal and Torres Strait Islander people, LGBTQ+ communities, people from refugee backgrounds and people with experiences of homelessness (Cortis et al., 2018). A similar result was seen in the Victorian study: participants wanted more training on working with people with disability or disabled people (Department for Victorian Communities, 2021).
In the national survey, the majority of participants (61%) worked full-time (Cortis et al., 2018). Among part-time workers the reasons for part-time work included caring, personal or family responsibilities; limited full-time positions available or resources to support a full-time position; and reducing stress, burnout, vicarious trauma or compassion fatigue. Retention issues were attributed to poor pay, challenging work, limited organisational support and career pathways. These issues were more pronounced in early career workers or positions that worked closely with perpetrators. While these surveys and censuses establish a picture of the gaps and challenges faced by the workforce, they do not establish what the workforce perceives to be effective, ineffective and promising in addressing domestic, family and sexual violence.
Methodology
This study used a qualitative online survey to gather the perspectives of the domestic, family and sexual violence workforce in Australia. Drawing on contextualism, we carried out a reflexive thematic inquiry to understand how the workforce perceives interventions and approaches to be effective, as well as barriers, enablers and opportunities in preventing and responding to domestic, family and sexual violence. Contextualism emphasises that knowledge is context-specific and sensitive, and as such, the way that people ascribe meaning to their experiences is deeply connected to the context of their experiences (Braun & Clarke, 2006, 2019; Braun et al., 2018; Jaeger & Rosnow, 1988). This perspective was appropriate as we sought to understand how the workforce’s views are context-bound. Therefore, implementation and perceived effectiveness of interventions and approaches need to be seen in the context within which they are delivered.
Just as workforce views are contextually bound, so too are meanings and interpretations ascribed by the research team. Members of the research team come from diverse professional backgrounds that combine academic and clinical experiences, working in public health, law, policy, medicine, psychology and allied health. We also bring personal, family and community lived experience that shapes our understandings of domestic, family and sexual violence. Our learned experience as clinicians and researchers is primarily through a public health lens, and we are conscious of how this context has shaped the design, data collection and analysis. We have sought to reflect on our own assumptions, biases and perspectives using regular debriefing and journal notes to inform our reflexive process.
Advisory committee
For the larger study, an advisory committee was formed comprising representatives from government, service and advocacy organisations in the domestic, family and sexual violence sector in Australia (see Appendix A). The Voices Advisory Committee provided guidance and advice at meetings and via email to inform the research at various stages. Specifically, its input shaped the study design, development of the survey instrument, recruitment processes, and analysis and interpretation of findings and implications for policy, practice and further research.
Research questions
To address the aim of the study, we were guided by the following research questions:
- What contextual factors inform the perceived effectiveness and appropriateness of interventions and responses and the way they are understood to work?
- What outcomes are different interventions and responses designed to achieve?
- What are the recommendations for service and system improvement to better respond to victims and survivors, children and young people and perpetrators?
Survey instruments
The survey was developed in consultation with the advisory committee through an iterative process of compiling and testing survey questions. The design of the survey was informed by the literature and feedback received during the pilot process by the experts on the advisory committee, who initially reviewed the survey to confirm it measured the constructs of interest (Bolarinwa, 2015). The survey was then piloted with the advisory committee and ANROWS staff, who provided feedback prior to finalisation and delivery.
The survey contained two sections. Respondents were first asked to provide their demographics and career information, including gender; professional role; primary discipline; primary sectors; experience (years) in the domestic, family and sexual violence sector; and their current organisation’s area of operation/jurisdiction or geographical scope of research. They were also asked to nominate specific groups of people that they felt able to comment on. The options included young people (16 to 24 years), older people (50 years and older), Aboriginal and Torres Strait Islander peoples, culturally and linguistically diverse communities, people with disability or disabled people, LGBTQ+ communities, people living in rural or remote areas, women who are or have been incarcerated, and sex workers.
Respondents were asked to identify up to three existing responses or interventions that were promising or effective, and up to three that were ineffective, for each of the following:
- victims and survivors of domestic or sexual violence
- children and young people who have experienced domestic or family violence (<18 years)
- perpetrators of domestic or sexual violence
- adolescent perpetrators of violence in intimate relationships or sexual violence
- any specific group that they had nominated in the previous section.
Questions asked respondents to describe each nominated response or intervention, including who provides it, in what setting and the group it is designed for, as well as the outcomes it achieves and how they are achieved. Respondents were also asked about the existing gaps in policy, legislation and/or appropriate service provision for the group of people the intervention is designed for, as well as recommendations for future directions in responding to the group.
Recruitment strategy and data collection
In order to capture the range of responses and interventions, a purposive sampling approach was used with potential respondents invited from a range of backgrounds and organisations. The research team emailed potential respondents to introduce the project. Potential respondents were included based on their occupation (practitioner, service designer/manager, researcher in academic or non-academic organisation) or experience in addressing domestic, family and sexual violence in Australia.
Invitations to the first survey were emailed to 650 stakeholders on ANROWS’s expert stakeholder list. Potential respondents were emailed three times (including the initial email). The survey was also promoted via Twitter to 14 relevant professional associations. Two adverts were placed in ANROWS’s fortnightly online newsletter, Notepad.
A modified snowball strategy was also used to recruit respondents, where respondents were asked to share the survey link with other experts in their network (Bryman, 2001; Crabtree & Miller, 1992). Participation was voluntary and no incentive was provided for completing the survey.
The survey was developed and distributed via weblink using the secure SurveyMonkey software platform. The survey was estimated to take 20 to 30 minutes to complete, however may have taken more or less time, depending on the number of areas of expertise selected. Respondents were able to complete the survey anonymously and could discontinue the survey at any point.
Between 17 November 2020 and 29 January 2021, the survey received 199 responses, which is a response rate of 30 per cent based on direct email invitations. However, it must be acknowledged that as a result of the COVID-19 pandemic, between November 2020 and January 2021 there was increased demand on the domestic, family and sexual violence workforce, which may have impacted response rates (Australian Institute of Health and Welfare, 2021c). Additionally, while 199 responses were received, 104 were excluded because they did not provide substantive responses beyond demographics. Thereby, respondents who did not complete any of the qualitative questions but limited responses to the quantitative demographical questions were excluded. A total of 95 respondents were included for analysis.
Data analysis
Data was exported from SurveyMonkey into a Microsoft Excel document. Microsoft Word and NVivo software were used to manage and store the data. Descriptive analysis to report on frequency (count and percentages) of responses, such as respondent demographics, was undertaken using Microsoft Excel. Qualitative data were analysed using reflexive thematic analysis (Braun & Clarke, 2019; Braun et al., 2018).
Reflexive thematic analysis occurred in six phases. First, we familiarised ourselves with the data by reading through and sorting responses into categories according to the cohort (victims and survivors, children and young people and perpetrators). Second, we generated codes to organise the data. Third, we began to generate initial themes, drawing together codes and identifying patterns and meaning across the data. Next, these themes were iteratively revised and their meaning clarified through collaborative discussion. This included sharing the preliminary themes with the wider Voices project team and then with the advisory committee. In the final two phases, the themes were defined and then further refined and tested during the report-writing process in the context of existing literature. Respondents were assigned a non-identifying number for data extracts and potentially identifying information from illustrative quotes was removed.
The findings were shared with key stakeholders from state and national government departments through a presentation in January 2022 and via a brief report that was emailed in April 2022. The draft report was shared with key stakeholders from state and national government departments during peer review, and the recommendations were shared with the advisory committee through a presentation in July 2022. Feedback at each stage was incorporated into the final report.
Ethics
Ethics approval was granted by the University of Melbourne Human Research Ethics Committee (HREC reference number: 2057459.1).
Survey respondents were provided with the contact details of several support services and had the option to suspend the survey and return at a later time. A contact number of a member of the research team was provided if respondents had any questions.
Findings and discussion
Who participated in the Voices survey?
The majority of respondents identified as female (n=86, 91%; males: n=7, 7%). Two respondents identified as non-binary. Respondents were drawn from all states and territories, however most worked in Victoria (n=31, 33%), Western Australia (n=16, 17%) and New South Wales (n=15, 16%; Figure 1).
Figure 1: Distribution of respondents (N=95) by statea (%)
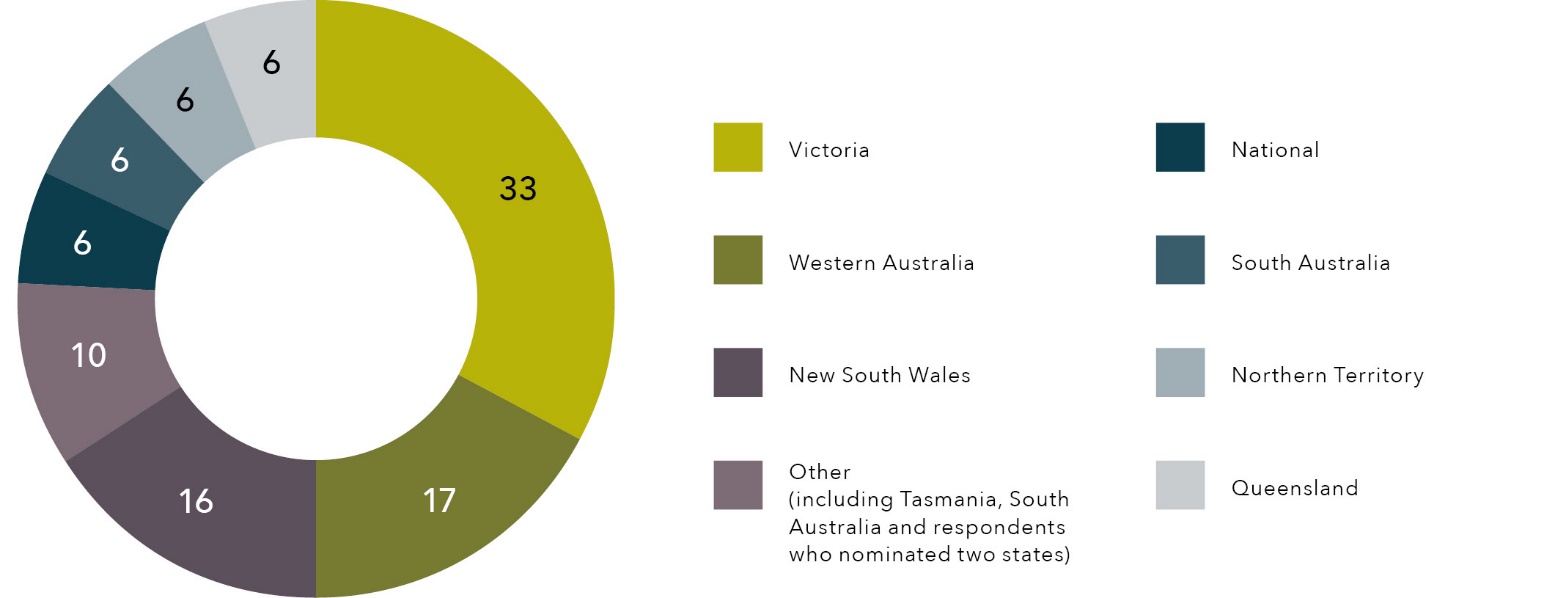
Note: a “Other” indicates states with a small cell size, which includes Tasmania and South Australia, as well as respondents nominating two states.
The majority were practitioners (n=60, 63%), while fewer were service designers or managers (n=21, 22%) and researchers (n=14, 15%). A small number of respondents who were categorised as practitioners also identified as researchers (n<5). Those working as practitioners, service designers or managers (n=81) were drawn from the following services:
- women’s specialist domestic and family violence services (including shelters, advocacy and casework services; n=23, 28%)
- sexual violence services (n=14, 17%)
- health services (including mental health services; n=10, 12%)
- men’s behaviour change services (n=7, 9%)
- primary prevention organisations (n=6, 7%)
- other services (including policing, Aboriginal and Torres Strait Islander organisations, legal services, disability services, multicultural services, education services, family services, financial counselling, aged care; n=21, 26%).
Among all respondents, two thirds had six or more years of experience, with most of these having 10 or more years (Figure 2).
Figure 2: Professional experience (years) of respondents (%)
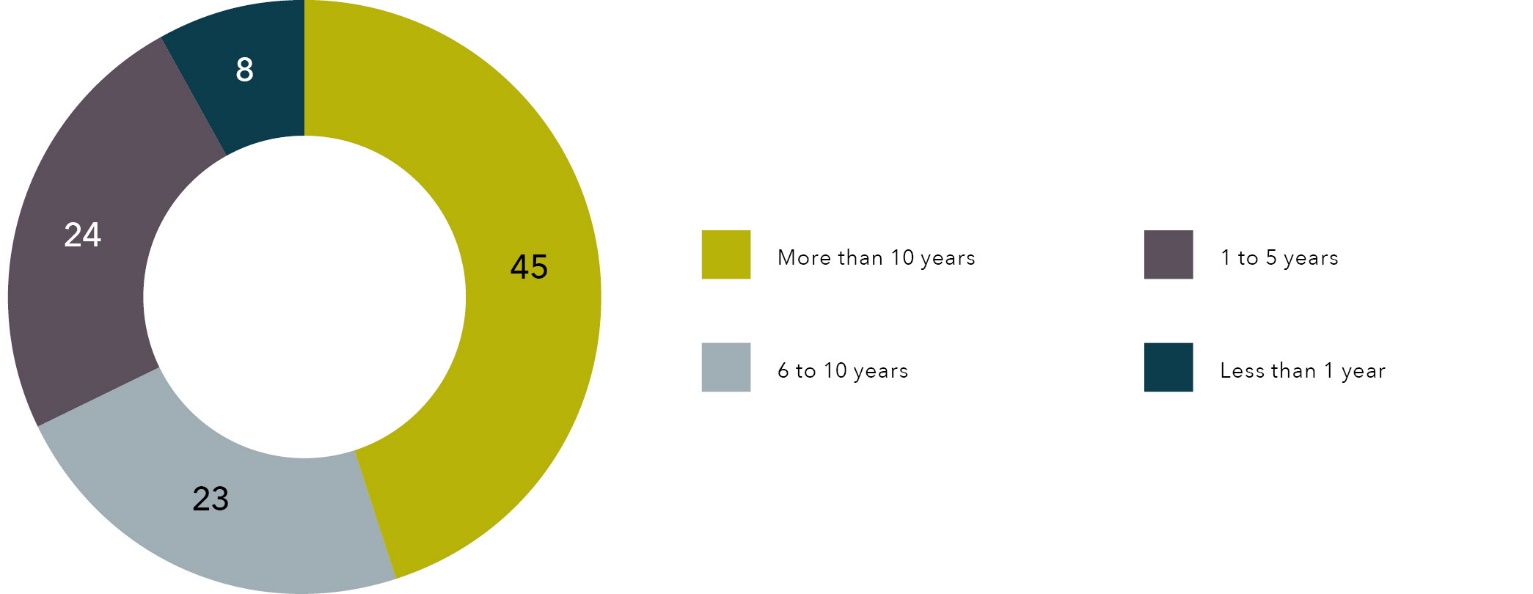
Key findings
The key findings are first presented in accordance with the six outcomes from the National Plan, namely:
- Communities are safe and free from violence
- Relationships are respectful
- Aboriginal and Torres Strait Islander communities are strengthened
- Services meet the needs of women and children experiencing violence
- Justice responses are effective
- Perpetrators stop their violence and are held to account.
Across these outcomes, we describe workforce perceptions of contextual factors that inform the perceived effectiveness and appropriateness of interventions and responses. We also present priorities and opportunities identified by the workforce as important for future directions.
Following this we present the five key themes that we constructed to encapsulate workforce perceptions on what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators (Figure 3).
Figure 3: Summary of workforce perspectives on what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators.
Addressing upstream determinants of domestic, family and sexual violence
Reactivity and inequity in responses harms victims and survivors
Changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
Enabling choice and the right to self-determination
Power of connection, collective healing and compassion
National Outcome 1 – Communities are safe and free from violence
Where are we now?
There was consensus among respondents that addressing gender inequality was critical in shifting the unequal status of women in society, since gender inequality is a key driver of domestic, family violence and sexual violence:
Gender inequality is understood to be the underlying phenomenon for [domestic, family and sexual violence]. By addressing gender inequality, we assist to address the power and control dynamics present in [domestic, family and sexual violence]. (Respondent 40, Service designer/manager)
The primary gaps in keeping communities safe and free from violence identified by respondents centred on the multilayered aspects of gender inequality that structure society as well as our workplaces, families and relationships. Primarily, respondents perceived that women’s unequal participation in the workforce is a key contributor to the unequal status of women. Workplace harassment and discrimination was identified as a substantial barrier to women’s fair and equal participation in the workforce.
In particular, some respondents identified the greater burden of unpaid caring among women and the “gender pay gap” as detrimental to progress toward gender inequality. The gender pay gap in Australia derives from the lower proportion of women in senior positions and lower wages for women compared to men. Lower wages for women also compound isolation and abuse by perpetrators who seek to restrict victims’ and survivors’ financial resources: “Social isolation as well as reducing the resources of the women is an active perpetrator tactic.” (Respondent 40, Service designer/manager)
Future directions
Respondents identified advancing gender inequality in the workplace as well as primary prevention and promoting community involvement and awareness (Table 1).
Table 1: Future directions for keeping communities safe and free from violence identified by respondents with exemplar quotes
Addressing gender inequality in the workplace
Future direction
Respondent
The workplace is an important setting in which there is unrealised potential to make significant change to policy that is discriminatory, as well as to shape community knowledge, attitudes and behaviours. For example, it was suggested that all workplaces implement anti-violence policies. Further, respondents identified the need for more comprehensive policy measures, such as adequate paid parental leave for both parents
“The duty of child rearing rests largely with women. This can be misused by perpetrators to control the women and also remove them from employment as well as other resources and support.”
Respondent 40, Service designer/manager
Mass media in primary prevention
Future direction
Respondent
There was consensus that primary prevention requires cultural and attitudinal change in order to change behaviours. Central to this is raising awareness of gender stereotypes and inequalities. A key area of agreement was on the role of media in shaping social and gender norms, particularly through depictions of relationships. Respondents identified that the media can be harnessed to challenge gender norms, particularly those that underlie inequalities
“Outcomes achieved by educating adults and children of the subliminal messages in advertising … the unchallenged attitudes in society that perpetuate the gender inequalities.”
Respondent 16, Researcher
Respondents suggested that mass media and social marketing approaches can be a powerful tool in shifting community attitudes, citing successes by anti-smoking campaigns, which are long-term, well-resourced, multilevel campaigns. This would require buy-in from all levels of government and community
“Fully funded, long-term campaign which is creative and involves all levels of society.”
Respondent 37, Service designer/manager
Promoting community involvement and awareness
Future direction
Respondent
Two potential approaches to promoting community involvement and awareness were identified: bystander training though workshops or online modules, and lived expertise advocates, who were considered powerful in generating community awareness and change
“Encouraging young people to support their mates and stand up for mates, including when the young person is in the wrong.”
Respondent 47, Practitioner
“Improve gender equity at all facets of society. Media and societal advocates have a huge role to play in this.”
Respondent 40, Service designer/manager
National Outcome 2 – Relationships are respectful
Where are we now?
There was minimal data relating to what works in promoting respectful relationships. However, there was consensus that schools are an appropriate and important setting for consent and healthy relationships education for young people. Respondents asserted that in their current delivery, such programs are not adequately resourced and are not consistent in terms of the curriculum.
Respondents identified Love Bites as a promising intervention. Love Bites is a school-based relationships education program that provides young people with a safe environment to discuss and explore respectful relationships. Love Bites consists of two interactive workshops, “Relationship violence” and “Sex and relationships”, followed by creative workshops and community campaigns: “LOVE BITES education is focused on three critical areas for learning: knowledge: youth-led collaborative learning; attitudes: critical thinking and decision-making; and behaviours: problem solving and communication skills.” (Respondent 78, Practitioner and researcher)
The program was highly regarded by respondents as it “views young people as active participants who are able to make choices for themselves and their relationships when supported with information and opportunity for skill development” (Respondent 78, Practitioner and researcher).
Respondents also identified a lack of interventions to address young people who demonstrate abusive behaviours that have been modelled by caregivers, which can manifest as bullying behaviours with peers, at home with their family and/or in their intimate relationships.
Future directions
There were three possible areas identified as important future directions to promote respectful relationships, which again centred on young people: changes to the curriculum, better resourcing for consent and healthy relationships education, and interventions for young people to support building healthy relationships (Table 2).
Table 2: Future directions for promoting respectful relationships identified by respondents with exemplar quotes
Changes to curriculum
Future direction
Respondent
Respondents identified embedding respectful relationships education in curriculums, including within early education, through a consistent national curriculum for primary, secondary and tertiary students
“More youth need to be exposed to the healthy relationships training called ‘Love Bites’ it’s very informative and really defines what a healthy relationship should look like. Often [domestic and family violence] is a repeated act that the perpetrator has seen happen as a form of getting things done, so they identify that this is normalized behaviour, if we can educate the youth before they are in relationships, they have a better understanding of how to be treated and what to expect.”
Respondent 88, Service designer/manager
Better resourcing for consent education
Future direction
Respondent
Changes to curriculum must be accompanied by adequate resourcing to implement consent education effectively. In terms of adequate resourcing, one suggestion was to fund “violence prevention” practitioner positions in each region who could provide oversight and coordination for such initiatives
“Schools have now been formed into regional clusters to support them to carry out this initiative – each cluster needs a Violence Prevention Practitioner to provide a meaningful level of resourcing.”
Respondent 50, Service designer/manager
Interventions for children and young people to support building healthy relationships
Future direction
Respondent
Respondents called for sufficient resourcing for interventions that provide therapy and other support for children and young people who engage in abusive behaviours that have been modelled by caregivers. Respondents indicated that this may include mentoring and other approaches that aim to provide role-modelling and build community connections for children and young people
“Get them into building relationships in the community to help with transition to adulthood.”
Respondent 88, Service designer/manager
National Outcome 3 – Aboriginal and Torres Strait Islander communities are strengthened
Where are we now?
Primarily respondents raised concerns about systemic issues that intersect with ongoing racism and discrimination experienced by Aboriginal and Torres Strait Islander peoples in Australia. Much of this centred on the criminal justice and child protection systems, particularly with regard to responses that are considered punitive and not trauma-informed or culturally safe.
Respondents cited concerns about high rates of Aboriginal and Torres Strait Islander children removed from families. Specifically, concerns centred on lack of collaboration with families and capability among the child protection workforce in terms of understanding how to work effectively with Aboriginal and Torres Strait Islander families. This also related to concerns around workforce understanding of the dynamics of family violence, as well as how this intersects with other forms of violence and trauma, including racism, intergenerational trauma and the ongoing legacy of colonisation:
Despite policy emphasising whole of family support, in practice there are often examples of interventions that are high-handed, do not involve collaboration with the family or explore alternatives to a punitive approach. Victim- and mother-blaming are still prevalent. There is little understanding of the patterns of behaviour that are involved with abuse and neglect and there continues to be a lack of awareness of issues and alternative approaches within the Aboriginal community. (Respondent 49, Practitioner)
Respondents also acknowledged the challenges for the child protection workforce, in terms of training, high rates of staff turnover and the need for ongoing support to manage burnout and vicarious trauma:
Child protection on its own as an intervention scheme is not helpful. Child protection is often involved after incidents of [family violence] where children are present. There is a lot of mistrust of the system, and it can seem punitive, which can make clients resistant to engagement. There is such a high workload within these agencies that it is nearly impossible for staff to spend any real time with clients. (Respondent 78, Practitioner and researcher)
By contrast, respondents reported that there are effective and culturally safe practices that have been developed and implemented through ACCOs and ACCHOs. These approaches are typically led by community, embedded with local contextual knowledge and leadership and delivery by Aboriginal and Torres Strait Islander staff: “There are good practices among ACCHOs or Aboriginal-led community responses to [family violence].” (Respondent 40, Service designer/manager)
Future directions
Respondents identified a number of promising approaches emphasising the need to prioritise self-determination and have solutions be led by Aboriginal and Torres Strait Islander communities and organisations (Table 3). Key to enabling this is adequate resourcing for sustainable, community-led and culturally safe responses:
Any future directions for supporting Aboriginal women should be culturally appropriate and safe, community-led and run by Aboriginal organisations and communities and should allow for Aboriginal decision making and self-determination. (Respondent 27, Practitioner)
Table 3: Future directions to better support Aboriginal and Torres Strait Islander communities identified by respondents with exemplar quotes
Workforce is key
Future direction
Respondent
Respondents suggested ensuring cultural competence of mainstream staff as well as increasing the proportion of Aboriginal and Torres Strait Islander peoples through identified positions and training. Strengthening workforce capability will also support improved referral pathways between ACCHOs and mainstream services
“Comprehensive cultural awareness and safety training provided by local people for every new staff member. With refreshers provided every 12 months. Or even better develop a cultural safety framework. Utilise their Aboriginal staff in a more productive and meaningful way, not just consultation.”
Respondent 78, Practitioner and researcher
Increasing competency and capability of all staff to enhance culturally safe responses. Importantly, respondents pointed out that this should not involve overburdening or delegating this responsibility to Aboriginal and Torres Strait Islander staff in mainstream services. It is the responsibility of mainstream services and non-Aboriginal staff to ensure their cultural competency
“Cultural competence of staff is not the responsibility of Aboriginal staff.”
Respondent 59, Practitioner
Better practice models and risk assessment tools
Future direction
Respondent
Respondents indicated that models that work with Aboriginal and Torres Strait Islander families must consider biases and harm related to risk assessment tools that are not culturally responsive or valid
“Better risk assessment to assess … families who will benefit from additional support.”
Respondent 40, Service designer/manager
Whole-of-family approaches
Future direction
Respondent
Respondents identified that whole-of-family approaches, in collaboration with multisectoral supports such as schools and health services, can be an effective way to support families to make holistic and lasting change
“Families need to be empowered in these process[es] to ensure there will be sustainable change that is realistic and achievable.”
Respondent 78, Practitioner and researcher
Whole-of-family approaches must also be preventative, rather than reactive and/or punitive. This can also involve broader community work to address inequity, such as poverty, unemployment and housing
“Work harder at kinship care, keeping the child in the home with the parents … do preventative work in the community. The biggest issues [are] poverty, so reduce poverty.”
Respondent 48, Practitioner
Engage rather than marginalise men
Future direction
Respondent
In addition to whole-of-family approaches, respondents valued working in a way that engages men and may include specific programs or supports that are aimed at reconnecting with culture and community through strengths-based approaches
“Aboriginal women say ‘we need something for our men, they are hurting too.”
Respondent 35, Researcher
Respondents called for approaches that focus not just on reducing offending but also emphasise healing and connection to Country and culture. For example, an effective way to engage men is to support other men to be role models and leaders in their community
“Reductions in contact with the criminal justice system, reductions in alcohol and drug use, reduction in violence against partners and children, men standing up against violence in the community, men taking control of their lives and being strong role models, participating in on-country programs where they learn about being a good Aboriginal man and father.”
Respondent 35, Researcher
National Outcome 4 – Services meet the needs of women and children experiencing violence
Where are we now?
Respondents identified multiple systemic issues that contribute to service gaps and harm for victims and survivors. An overarching issue expressed by respondents was that the system is focused on single incidents and we need better understanding of and responses to patterns of abuse, including coercive control.
The most substantial gaps centred on resourcing insufficiencies, which drive and contribute to the reactivity in the system. There was consensus that resourcing is largely directed toward crisis responses and interventions, rather than early intervention or recovery. Further, there was criticism that resource constraints frequently manifested in interventions that are limited by eligibility criteria and duration, without sufficient follow-up measures in place.
Underlying these service gaps are issues of insecure, inflexible and insufficient funding, which respondents identified as a major issue in delivering services, as well as ensuring workforce capability and sustainability through longer-term funding and employment contracts. These issues are compounded in rural and remote areas, where there is a stark lack of services, especially for children and young people. Likewise, resourcing constraints are evident in the lack of culturally appropriate and accessible services for women who may experience intersecting forms of discrimination and oppression.
Respondents cited the health workforce capability as a strength, particularly in routine screening in health settings (e.g. maternal, early childhood, drug and alcohol, mental health and emergency), as well as risk screening in general practice. However, the effectiveness of this is constrained by a number of systemic factors such as clinicians’ knowledge of, or access to, clear referral pathways. Consequently, respondents identified that the health workforce requires ongoing support and education for staff to safely screen patients in these settings:
Better education for all staff who work in emergency on what is helpful and not helpful. It is really hard to change judgemental attitudes but protocols on what not to say or do in certain circumstances might be helpful. (Respondent 15, Practitioner)
Further, in health settings, the biomedical model is dominant. As such, respondents felt that the focus on physical incidents of violence without consideration or understanding of the psychosocial context can be problematic.
Respondents elaborated substantially on issues within the housing and child protection sectors. It was clear that respondents perceive that longstanding insufficiencies and deeply entrenched inequities in these systems cause harm and trauma for victims and survivors.
Housing
Multiple issues that centred on housing were described by respondents. These issues contribute to people remaining in, or returning to, unsafe circumstances, as well as traumatisation and re-traumatisation as a result of engaging with services and being unable to access appropriate housing support: “The horrendous housing situation in Australia is deterring women from leaving abusive relationships.” (Respondent 37, Service designer/manager)
There was acknowledgement that housing is a social determinant of health and that systemic issues preventing access to safe and affordable long-term housing greatly contribute to risk and harm for people experiencing violence: “Decades-long waiting list for community housing coupled with high rents and demand outstripping supply of rental properties means that finding sustainable long-term housing is becoming more difficult.” (Respondent 27, Practitioner)
Alongside widespread housing shortages, there are also substantial insufficiencies and bottlenecks in emergency accommodation.
After the 8-week tenancy, our women and children find it very difficult to find housing and at times, extend their lease. This prevents other women and children at serious threat from accessing safe crisis accommodation. It also means that women in transitional properties who are looking for long-term tenancies are finding it more difficult to move, again placing a bottleneck as some women move from crisis accommodation to transitional housing for three months before securing a tenancy. (Respondent 27, Practitioner)
Respondents elaborated on issues with emergency accommodation:
- Some accommodation has high levels of violence, which can be “scary and retraumatising and likely to prolong their suffering and delay recovery” (Respondent 15, Practitioner).
- Victims and survivors use hotels and motels for emergency accommodation, which are not universally accessible and are not suitable for children and families.
- There is a lack of options beyond emergency accommodation.
Conversely, some respondents argued there were no options for women after emergency accommodation:
- There seems to be a good amount of support with immediate crisis housing, but a lack of options for the next step, many women are left in hotels for months and months with no hope for finding safe and sustainable longer-term housing. (Respondent 52, Practitioner)
Respondents identified that these issues, which limit the safety, supply and suitability of housing, are forms of systems abuse that perpetuate trauma, increase risk, and constrain agency and choice. These issues are compounded by lack of supply and suitable housing options for LGBTQ+ communities, older persons, persons with disability or disabled persons, women without children and women with older children.
When placed in hotel cheap accommodation that is not safe and overcrowded for the family, this can place the family in a different type of harm [systems abuse] and they will return to the perpetrator. (Respondent 10, Practitioner)
The refuge I manage was not able to accommodate boys over the age of 14 for many years due to bathrooms being shared, recent refurbishment ensured all family rooms have private bathrooms enabling us to accommodate older boys … prior to being able to accept [older] aged boys we were experiencing women declining safe accommodation as they had to source other accommodation for their boys or leave them with the perpetrator. (Respondent 72, Service designer/manager)
Child protection
Respondents drew together a number of intersecting issues that centred on the child protection system. There was a sense that the system is unfairly punitive toward non-offending parents and that this drives mistrust and adverse outcomes. Respondents indicated that in practice, this frequently means that mothers are unfairly held to account for violence perpetrated by their partner and/or the children’s father: “The bulk of the pressure to act has been directed at victims of family violence. It’s the women’s parenting that has been pulled apart, not the man.” (Respondent 48, Practitioner)
One respondent framed this in the context of systems abuse, which not only harms victims and survivors and children, but ultimately discourages seeking help and support:
Removing children from women who are the non-offending parent is a collusion with the perpetrator and can be perceived [as] an extension of the violence inflicted by the perpetrator … A re-traumatising system does not encourage help-seeking behaviour. (Respondent 40, Service designer/manager)
To counter this, respondents emphasised the need for experienced workers who understand dynamics of domestic and family violence in the child protection workforce. Specifically, they outlined the need for more training for child protection workers in working with both perpetrators and non-offending parents:
… supporting the non-offending parent to keep her children safe through provision of safe housing, financial and practical resources as required, acknowledging the work the safe parent is doing to keep children safe, acknowledging and placing responsibility for the abuse with the offending parent. (Respondent 59, Practitioner)
Furthermore, workforce capability is impacted by high workloads and turnover of staff, which also contributes to issues around cultural competency and cultural safety for Aboriginal and Torres Strait Islander families:
Burnout is frequent and so there is a high turnover. This means new workers all the time, often not local. These workers often put themselves in culturally unsafe positions due to their lack of local knowledge. (Respondent 78, Practitioner and researcher)
Who is being left behind?
Respondents outlined broad systemic issues that have widespread impact. However, they also detailed more nuanced issues that disproportionately impact those who are likely to also be experiencing other forms of discrimination, oppression and barriers to accessing support.
Rather than viewing people in terms of discrete identities, respondents took an intersectional approach and identified specific systemic and service issues that must be considered in order to improve future responses for those experiencing ageism, racism, colonialism, ableism, religious prejudice, heteronormativity, homophobia, cis-sexism, transphobia and classism. Respondents elaborated on these systemic issues and described the nuanced and often less visible ways that these contribute to service gaps and harm for the following people, families and communities.
Children and young people
There was a strong sense that children and young people are not adequately considered in the context of their own rights, experiences and needs: “Children are often invisible in service delivery.” (Respondent 48, Practitioner)
Instead, children and young people seem to be treated as an adjunct to the situation or as bystanders, with one respondent noting that unless services “are specific to children and a child’s trauma, [they] do not focus on the impact on the child” (Respondent 89, Practitioner).
For example, children are often not named on intervention orders. Likewise, family law matters and arrangements for the care of children of separated families rarely centre the “voice of the child or [provide] instruction for children on how to remain safe when in custody of perpetrator” (Respondent 4, Researcher).
Often, children and young people are considered in relation to their parents or caregivers, which respondents related to traditional case management models that consider the “women to be the client and feel that they are not funded to provide services to children, or do not treat children as victim survivors in their own right” (Respondent 48, Practitioner).
Respondents also identified lack of services that specifically meet the needs of younger women who are victims and survivors: “Young women tend not to attend these general groups and are underrepresented as clients of specialist [domestic, family and sexual violence] services.” (Respondent 59, Practitioner)
For young people who use violence, respondents felt there needs to be greater recognition that they are likely also victims and survivors, which needs to inform service responses:
Violence is learnt, it can be unlearnt, but if you constantly label a young person as violent without understanding why or how the violence was used, then that [young person] will grow up into an adult who has learnt they are violent … We must acknowledge [a young person’s] vulnerability as a victim while simultaneously working with their use of violence. (Respondent 14, Practitioner)
Women who are incarcerated
Respondents pointed out that women are criminalised for offending in the context of violence, abuse and trauma, including for resisting violence:
[We] continue to punish women for behaviours in the context of [domestic and family violence] where men are “driving” the women’s behaviour, such as sex work, theft, drug possession [and] dealing … Also convicting victims of murder [or] assault when this may be a survival tactic in the face of overwhelming male-perpetrated [violence]. (Respondent 41, Practitioner)
Respondents also related this to the incompatibility of prison with addressing underlying trauma and providing the necessary conditions for women to be able to move forward in their lives:
… addressing the “anger” behaviours rather than the traumas which often underpin the “anger response”. Band-aiding the bigger and more complex issues, also blame[s] women for their trauma responses. (Respondent 41, Practitioner)
The majority of incarcerated women are there because of drug offences. In order to stay out of prison they need to avoid drugs and drug dealers, which is very difficult to do living amongst them. (Respondent 15, Practitioner)
Post-release, there are issues of inadequate housing and a need for more comprehensive throughcare support. Again, the restriction of agency and choice for women who are or have been incarcerated was identified as a key violation of rights and a barrier to women accessing effective support. For example, mandated counselling will not be effective if the woman has not been given a choice in how or if to engage: “Parole officer insisting on counselling when woman not wanting [to] or not ready.” (Respondent 15, Practitioner)
Women living in rural and remote communities
Some of the issues identified for rural and remote communities reflect broader systemic issues around resourcing and workforce capability. However, these issues are amplified in regions where there are insufficient services to meet the needs of rural and remote communities, which also constrains choice and accessibility for groups with specific needs.
1800RESPECT is a service available to people in remote or rural localities and can direct users to local services. It cannot replace or provide services in regions where they are inadequate or absent. (Respondent 88, Service designer/manager)
… services that can meet the needs of all people who need to use services in particular services that understand and respond to disability, [LGBTQ+] and cultural needs. (Respondent 39, Researcher)
Respondents also described the unique needs of rural and remote communities, the importance of the health sector in meeting these needs, and the need for more specialist services and emergency accommodation:
[Domestic and family violence] is more prevalent and has specific effects in rural and remote localities. These specific effects include access because of transport and distances, a lack of perpetrator accountability and other issues that discourage help-seeking such as privacy concerns and shame. (Respondent 49, Practitioner)
LGBTQ+ communities
Workforce capability was a major concern, with respondents citing lack of training for staff in mainstream and specialist domestic, family and sexual violence services regarding LGBTQ+ communities. This lack of capability in supporting LGBTQ+ communities also reflects a lack of societal knowledge and awareness more broadly, as well as the pervasive stereotypes and misunderstandings within society about domestic, family and sexual violence experienced by individuals in these communities. While training is important for the workforce, there is also a need for more LBGTQ+ specific services in mainstream healthcare services as well as specialist services, particularly in regional areas: “Currently support in regional New South Wales is limited to telesupports.” (Respondent 59, Practitioner)
Culturally and linguistically diverse women and communities
Respondents acknowledged that resourcing and workforce capability were key issues for culturally and linguistically diverse communities, with one saying that “mainstream service models are underfunded and resourced to respond appropriately to [culturally and linguistically diverse women]” (Respondent 23, Service designer/manager).
Respondents also identified that there is a lack of policy frameworks supporting women and perpetrators from culturally and linguistically diverse communities, as well as a lack of specialised support services: “There is not a clear policy on how to address specific cultural factors that mediate violence against women, especially against women from refugee and migrant background[s].” (Respondent 65, Researcher)
Respondents also pointed to policy issues that impact women on temporary visas and notably prevent access to social support such as emergency payments, income support and healthcare (e.g. through Medicare). This is a substantial barrier to women leaving their relationships as the services are inadequately resourced to support their needs, as described by the following:
As a refuge we are required to pay for everything and forgo rent, for sometimes 2+ years while the visa and court processes are taking place … [We] pay for everything and we are required to find support services (e.g. migration lawyers) that work pro bono. (Respondent 86, Service designer/manager)
Women with disability and disabled women
Respondents identified the lack of accessible services for women with disability and disabled women as a key issue:
… improved access to services, meeting the needs of all clients, ensuring equitable access, removing barriers to support … [For example], using Auslan interpreters for people with hearing impairments, making sure the service meets the requirements of people with disabilities and is accessible. (Respondent 59, Practitioner)
They also pointed to how limited service options constrain choice. This can be particularly harmful for victims and survivors who engage with multiple systems such as health, housing and employment. The National Disability Insurance Scheme (NDIS) was considered to be particularly problematic, as women face multiple barriers to accessing support through the scheme, as described by this respondent:
It is exhausting/emotionally draining and very worrying. People put in a lot of effort to be frustrated several times before they are finally accepted … I’ve had so many people say, “I can’t try again. It’s too hard.” I persuade them and they usually do. (Respondent 15, Practitioner)
It also places strain on services to provide resources and supports when clients have not been able to access them through the NDIS: “Our NGO service paid $200 to access an interpreter for a client with a hearing impairment as no funding was available.” (Respondent 59, Practitioner)
What is working?
There were four main approaches that respondents perceived to be working effectively:
- advocacy and coordination of support
- multi-agency responses
- therapeutic interventions
- interventions that are specifically for children and
young people.
Advocacy and coordination
Specific advocacy and coordinated care assists women to navigate options across sectors, which enables access to support but also minimises risk of “secondary systems abuse” (Respondent 23, Service designer/manager).
Respondents identified benefits of advocacy and coordinated care, for victims and survivors but also for workers who can face burnout brought about by systems failures. Advocacy and coordinated care are most effective when delivered by workers who hold a specific advocacy role, for example case management staff, with such roles embedded in organisational structures and policies.
In some settings, specific child advocacy can be effective for supporting older children, such that they are treated as clients in their own right and additional safety planning is tailored to their developmental needs: “The boys are linked into programs such as the police and citizens youth clubs and other support groups specific to young men and boys for positive male mentoring.” (Respondent 72, Service designer/manager)
One practitioner identified Legal Aid NSW’s Women’s Domestic Violence Court Advocacy Service (WDVCAS) as an example of an effective advocacy program. The WDVCAS is delivered through locally based, non-government service providers. The program provides information, advocacy and referrals to assist women and their children with their legal, social and welfare needs, including obtaining legal protection through applications for apprehended violence orders (AVOs) and providing referrals for services such as housing, counselling, financial assistance or health services.
Multi-agency responses
Respondents held multi-agency responses in high regard and identified current approaches that are considered to be promising, including co-location of services (e.g. Health Justice Partnerships) and the NSW Department of Communities and Justice Safer Pathways program. Such programs enable collaboration between services, with efficient information sharing to enhance safety and reduce re-traumatisation: “Safer Pathway provides a way for what I consider to be effective collaboration to happen but is more effective for cases rated as at serious threat.” (Respondent 49, Practitioner)
Therapeutic interventions
Trauma-informed therapeutic interventions were considered effective in promoting healing and recovery. Again, choice is vital, and the therapeutic relationship rather than therapeutic modality was considered by respondents to be particularly important. Respondents pointed to individual, family and group therapeutic interventions, as well as broader approaches to trauma recovery that address the embodied aspects of trauma, for example through yoga or similar.
… evidence-based therapies for trauma including complex trauma, developing secure attachments between non-offending parent and their child/ren … practices that recognise the complexity of each woman’s situation and assist them to identify their strengths, resources and coping skills while supporting them to make their own informed choices. (Respondent 30, Practitioner)
In addition to trauma-informed approaches, response-based practice was identified as an effective therapeutic way of working that frames victims’ and survivors’ responses within the context of violence and abuse, with one respondent noting: “Response-based practice has made a substantial difference to upholding dignity, locating responsibility for the person using violence and highlighting women’s resistance to violence.” (Respondent 27, Practitioner)
Likewise, therapeutic approaches that integrate trauma psychoeducation are destigmatising, and depathologise responses to trauma. This was considered to be effective in reducing victims’ and survivors’ sense of self-blame and shame.
By contrast, therapies that use exposure, requiring victims and survivors to revisit the details of the trauma, were considered potentially harmful if not undertaken appropriately and in conjunction with other therapeutic approaches: “Many clients have reported that they have found exposure therapy highly re-traumatising because it required them to repeatedly revisit the details of the trauma they experience.” (Respondent 50, Service designer/manager)
Respondents also cautioned that couples counselling and relationship services can be harmful if domestic, family and sexual violence is not recognised and understood, particularly in relationships where perpetrators use coercive control: “Couples and/or marriage counselling is meant to be for couples who are having relationship issues that do not involve using power and control behaviours over the other person.” (Respondent 28, Service designer/manager)
Family interventions described were those that work with parent(s) only or those that work with the whole family. Whole-of-family approaches were considered a promising model particularly to address reactivity, biases and harm in risk assessment and child protective services. In particular, there was support for therapeutic interventions that work with the non-offending parent to maintain a safe and stable home environment and to enable them “to continue being a capable primary carer for children, to overcome trauma and abuse” (Respondent 4, Researcher).
Family therapy brings a systemic approach whereby change created in one part of the system enables further change to take place. This approach takes into account the impact of early relational trauma, intergenerational trauma and disruption in attachment between family members: “In working with children, the system must also be considered i.e. family, school.” (Respondent 87, Service designer/manager)
One respondent described a narrative family therapy framework, in which change is made to the sense of meaning that the family brings to their experience: “The whole family is strengthened … to create new meaning and potentially a new narrative around the family, who they are and where they are heading.” (Respondent 89, Practitioner)
This respondent contrasted this framework with the dominant individual therapy paradigm, cognitive behavioural therapy (CBT), which focuses on the relationship between the thoughts, feelings and behaviours that someone has about themselves as an individual and their experience:
While [CBT] can have good effect with symptom management, it does not address deeper levels of meaning and experience. Furthermore, even though there is a trauma-focused CBT framework, it’s [sic] focus tends to be limited to the individual and their specific experience as opposed to their broader relational world. (Respondent 89, Practitioner)
Therapeutic interventions that are delivered in groups were considered effective in building connection and compassion through shared experiences. Furthermore, validation and support derived from group experiences can be helpful in rebuilding a sense of trust and increasing understanding of the complexity of domestic, family and sexual violence.
Typically, such interventions are delivered in a weekly format for a defined time period and consist of facilitated group discussion and education modules developed by specialist staff using evidence-based strategies. The interventions are delivered by trained facilitators “who have understanding on how coercive control behaviours influence women’s options and choices, [and] how women’s strengths and resistance are a way to reclaim back human rights.” (Respondent 27, Practitioner)
Access to group interventions is enabled by reducing barriers, such as providing them for free or at low cost for participants and providing onsite childcare. In some group interventions, additional individual counselling sessions and the support of a case worker are also offered.
Children and young people–specific interventions
For children and young people who are victims and survivors, respondents emphasised that effective interventions must overcome barriers to engagement by using innovative approaches that are responsive to their needs, such as art, music, play therapy and other somatic therapies (e.g. animal-assisted therapy). These interventions should address relational trauma and attachment, emotional regulation and awareness, and incorporate psychoeducation aimed at understanding “abusive behaviour [and] safety planning to know how to respond when unsafe situations occur” (Respondent 4, Researcher).
Additionally, “responses need to be developmentally appropriate, relational, trauma informed and cognisant of attachment processes [and] disruptions” (Respondent 89, Practitioner).
Brief interventions that can be delivered during periods of crisis were considered promising and can be useful in overcome lengthy wait times, in that they can be delivered to those on wait lists for long-term counselling. For example, the Bouverie Centre model offers free counselling services to children who have experienced family violence. The model includes child-centred single sessions as well as access to therapeutic group sessions. The single sessions are tailored to families in crisis who are unable to commit to or are on a waitlist for longer-term counselling:
The model has one children’s counsell[or] working with the child and another children’s counsellor working with the mother. Then they come together to engage in a facilitated conversation between mother (caregiver) and child … developing a safe space for the child to express their feelings and concerns. The process may be over a few sessions rather than one session depending on the individual’s circumstances including safety. (Respondent 37, Service designer/manager)
The purpose of the session is to provide an interim response for children who require longer-term counselling, in order to provide the caregiver and child some tools to support them in the short term until the immediate crisis is resolved. These types of approaches require therapists skilled in a number of different therapeutic models, including art therapy and play therapy. The therapist’s knowledge of family violence is critical to the success of the model and the whole of the organisation focuses on children not just as a model of practice but also in terms of creating an environment where children feel safe and “have a sense of ownership of the space” (Respondent 37, Service designer/manager).
Respondents identified examples of promising interventions for working with young people who use violence. For example, interventions for young people who engage in harmful sexual behaviour include Turning Corners and the Good Way Model, which was designed for young people with intellectual disability and a history of engaging in harmful sexual behaviour, but is also applicable to other young people who engage in sexual and other forms of violence. This model uses narrative therapy principles to assist young people to “develop a new sense of meaning as to who they are, their place in their world, their future options, their relationships with others” (Respondent 89, Practitioner).
Future directions
A number of promising approaches and interventions were identified by respondents to inform future directions (Table 4). There was acknowledgement that resourcing, workforce capability and enabling policy frameworks are key factors to be addressed across sectors and critical to this is adequate funding for services, with longer funding cycles and employment contracts to ensure workforce consistency and sustainability.
Table 4: Future directions to better support victims and survivors and children and young people experiencing violence identified by respondents with exemplar quotes
Adequate resourcing that is sustained, flexible and tailored to local contexts
Future direction
Respondent
Respondents identified the need for:
- Increasing resources for advocacy and coordination using holistic wrap-around support that is not time limited and includes ongoing support for legal, health, housing and financial needs
“Long-term assistance to live [a] healthy life – everything is crisis related and focused on legal outcomes, not health and wellbeing.”
Respondent 4, Researcher
- Better resourcing of healing and therapeutic interventions to ensure that these are not time limited and do not exclude people on the basis of historical incidents or lack of documentation to support histories of abuse and trauma
“Longer-term interventions need to be available to people who have experienced family violence.”
Respondent 30, Practitioner
- Providing flexible support packages and emergency funds
“Access to income suqpport, especially for those who are on temporary visas.”
Respondent 73, Practitioner
- Effectively and appropriately using interpreters and ensuring they are available for all clients who identify they would like an interpreter. This may also include using registered interstate interpreters, particularly in smaller communities where there may be privacy concerns
“Provision of appropriate and accredited interpreters.”
Respondent 38, Service designer/manager
In custodial settings, there are multiple resourcing issues that need to be addressed to ensure better throughcare support, particularly for housing and employment
In recognition that most women in prison have trauma histories, there is a duty of care to provide a trauma-informed environment that is conducive to recovery and healing
“A support worker who spends time with the client/prepares a resume/finds out what sort of work [the] woman would be comfortable doing and goes out to find opportunities. Offers support in the early days, perhaps negotiating short days to start with.”
Respondent 15, Practitioner
“Programs that allow animals in prisons, birds, dogs etc. Humanise the prison environment and encourage connectedness and care.”
Respondent 41, Practitioner
“Intensive support where desired for women leaving prison who have experienced and/or are at risk of domestic and family violence.”
Respondent 59, Practitioner
Enhanced workforce competency, capability and collaboration across sectors
Future direction
Respondent
The health sector is an important resource, particularly in rural and remote regions. Respondents suggested increasing training for general practitioners (GPs), hospital staff and the allied health workforce – for example, expanding Multi-Agency Risk Assessment and Management Framework (MARAM) and/or Safe & Together training for these clinicians
A promising Victorian example that may be appropriate for other states is the Strengthening Hospital Response to Family Violence, which educates healthcare workers to identify and care for women experiencing family violence
“Whole-of-hospital approach to educate staff in how to sensitively enquire about family violence and in what to do when a woman discloses. Led by the Royal Women’s Hospital, it is a program that builds capacity across all hospitals in Victoria.”
Respondent 83, Service designer/manager
Respondents identified the need for:
- ensuring staff have training to sensitively support LGBTQ+ communities
Further funding and training in this space to support same-sex perpetrators of [domestic and family violence] would be beneficial.”
Respondent 2, Practitioner
“Displaying signage that shows support for all community members, including rainbow flag, using pronouns on email signature.”
Respondent 59, Practitioner
- providing specific training for service providers and the broader community around violence and abuse of older women
“Community education about sexual assault of older women. Ensuring older women and their advocates know they can speak out and be supported.”
Respondent 94, Practitioner
Address housing shortages, bottlenecks and accessibility issues
Future direction
Respondent
Respondents identified the need for:
- more options for accessible housing, including emergency housing that is accessible for all
“Build more crisis accommodation that uses universal design principles, so these services are fully accessible for all women including women with a range of disabilities.”
Respondent 39, Researcher
- providing better access to public housing and private rentals and not just short-term or emergency accommodation
“More social housing, better funding for refuges, consideration of housing for perpetrators are some of the issues that remain unaddressed.”
Respondent 49, Practitioner
- offering workforce training beyond frontline services that will raise awareness and enable greater collaboration with the private housing sector
“Education for real estate agents with property management services to reduce bias against women experiencing [domestic and family violence] and Start Safely packages, to sustain tenancies.”
Respondent 27, Practitioner
Addressing punitive approaches in child protection through early intervention and collaboration
Future direction
Respondent
Respondents identified the need for:
- greater investment in early intervention and prevention programs that empower and work collaboratively with families, in particular the non-offending parent
“Best Beginnings is a home visiting service for families of new infants. It involves regular visits to your home by caring, trained professionals who provide support, advice, information, connections and practical help. The program is structured according to your needs. The aim is to improve child health and wellbeing, parent and family functioning and social support networks. Support can come from a range of professionals including nurses, teachers, social workers and psychologists.”
Respondent 92, Service designer/manager
- alternative frameworks to child protection casework, such as the “Signs of Safety” approach, which was developed in Western Australia. The approach is strengths based, focusing on family and individual strengths as well as safety and good care as a foundation for future stability
“Communication as basis for identifying capacity for change … through continual assessment and centring the child/ren’s voice … What I loved about this model was how it uses really user-friendly language, worries and concerns, hopes and dreams, what’s working well, what needs to change. It looks at the perspective of the parents, the perspective of the child and the perspective of the worker. As a risk assessment framework, it enables not only workers but parents too (once shown) how they can consider risks to their family and in particular the needs of their children.”
Respondent 33, Researcher
Better responses that meet the specific needs of children and young people
Future direction
Respondent
Schools are an important setting to provide trauma-informed support for children and young people. School counsellors and psychologists are a central resource, however they are vastly underfunded such that children with more serious behavioural issues are prioritised for counselling support. Respondents suggested there is scope to provide enhanced training for all school staff to embed principles of trauma-informed practice in schools
“Children need to have escalated behavioural issues to receive counselling and then the focus is on their behaviour at the time (present) and not the behaviour they have been exposed to.”
Respondent 4, Researcher
“Trauma-informed training for teachers at schools.”
Respondent 76, Practitioner
Respondents identified the need for:
- employing evidence-based responses that are trauma-informed and child-focused, and address relational and attachment disruptions
“Bringing a child-focused lens to family violence crisis care work.”
Respondent 79, Practitioner
“Different programs have different motivations and praxis, but those relevant to the [domestic and family violence] field focus on family relationships and issues such as values, attachment and connections to family members and community.”
Respondent 49, Practitioner
- using interventions that promote emotional regulation, rather than narrowly focusing on behaviour management or behaviour change programs that are deficit-focused and blame young people for their behaviour(s)
“It labels young people as broken and that’s wrong, it’s just they need to learn how to appropriately and safely channel their expression.”
Respondent 14, Practitioner
- implementing a nationally recognised trauma-informed framework for working with young people who use violence, which would support services to deliver developmentally appropriate responses. Such a framework would explain how and why young people engage in violent behaviour as a means of communicating and meeting their needs for safety and relationships
“A framework that understands that relationships can be triggering/frightening and that for some young people the only way to find safety is to use violence as a protective measure … that this is not an excuse for violence, but a context in which we can understand it.”
Respondent 89, Practitioner
- embedding specialist domestic, family and sexual violence services in youth services so that they are provided in settings that are youth-friendly and accessible for young people. Scope to build young people’s capacity to deliver peer support and mentoring, and co-facilitate group therapeutic support
“Easier to access, break down the stigma and make them more ‘youth friendly.”
Respondent 52, Practitioner
“In places young people already access, as well as specialist domestic and family violence settings.”
Respondent 59, Practitioner
Mobilise telehealth and digitally enabled services
Future direction
Respondent
Respondents believed that telehealth and digital services could overcome barriers faced by rural and remote communities, such as distance or lack of services. There is the potential to establish telehealth hubs to enhance accessibility, safety and privacy for clients
“Improving opportunities for women in rural or remote areas to access counselling e.g. if there are barriers to travel such as distance, work demands or childcare concerns.”
Respondent 30, Practitioner
Enabling policy frameworks
Future direction
Respondent
Policy was consistently identified as an area that urgently needs attention and could incorporate principles of intersectionality
“Policy needs to be framed from an intersectional perspective to identify and respond to these complexities and funding, for example, for women with disabilities in rural and remote areas needs to be flexible so additional supports and services can be accessed without compromising safety.”
Respondent 39, Researcher
National Outcome 5 – Justice responses are effective
Where are we now?
Respondents identified several key issues that impact the effectiveness of justice responses. They centred on policing, prosecution and the family law courts.
Policing and prosecution
Respondents described shortcomings in policing that result in domestic, family and sexual violence not being responded to appropriately and being under-prosecuted. Respondents acknowledged that under-resourcing is a barrier to effective policing, for example in terms of delays in police response times. However, they also identified systemic issues around information sharing, victim blaming and workforce capability that thwart justice responses and harm victims and survivors. In particular, respondents described that policing responses can be traumatising for victims and survivors when police do not have the requisite knowledge and capability in responding to reports of domestic, family and sexual violence. This includes a lack of trauma-informed approaches, including inadequate and harmful responses reported by survey respondents, such as dismissive verbal and non-verbal responses, as well as not providing the appropriate physical environment and not
providing access to specialised policing units and staff:
Police responses to disclosures of [domestic, family and sexual violence] can be problematic when they are not [trauma and violence–]informed. We hear reports of police siding with perpetrators because they seem rational and calm when interviewed in response to an incident of [domestic, family and sexual violence] (in contrast to the victim/survivor who may be heightened and distressed). (Respondent 59, Practitioner)
Eyes were rolled, blame was implied for not making reports sooner, confidentiality was not established, safety was not ensured. (Respondent 74, Practitioner)
Victim/survivors are required to tell details of their stories in a physical space that is not supportive. (Respondent 7, Practitioner)
Reports of [domestic, family and sexual violence] are not necessarily taken seriously by the police and access to the specialised units is denied or the front desk officer demands to know the full story. (Respondent 15, Practitioner)
Many victim survivors are met with an abrupt and unkind manner by the police. Are sometimes made to feel like they are not believed or are victim blamed by the police. (Respondent 52, Practitioner)
Respondents specifically highlighted that those reporting sexual violence are frequently met with disbelief and victim-blaming attitudes when first reporting to police. One respondent felt that these re-traumatising experiences are evident across the journey that victims and survivors take through “the process of reporting, police statements, forensic examinations, investigating process and court process” (Respondent 52, Practitioner).
As respondents describe it, these initial adverse experiences are then followed with lengthy trial wait times, inadequate bail thresholds, low conviction rates and sentencing outcomes that respondents perceive to be “lenient”. These issues not only increase risks to victims and survivors but also deter people from making reports: “Women or children will do the right thing by going to the police and then the perpetrator is walking free again.” (Respondent 90, Practitioner)
These issues were partially attributed to under-resourcing and high workloads, particularly in relation to length of time taken for cases to be finalised. However, there was also a sense that, in some cases, delays can be an intentional strategy by defence lawyers:
It takes far too long for cases to come to court. This is partly because police are so under-resourced and the courts are very busy, but some thought needs to be given. Defence lawyers should not be allowed to get away with endless adjournments. (Respondent 15, Practitioner)
Court process to get to these outcomes takes a substantial amount of time. This amount of time often leads to victims reconciling with offender or no longer wishing to assist judicial process. (Respondent 57, Practitioner)
These issues with reporting and prosecution can also have adverse implications for victims and survivors seeking compensation. Furthermore, respondents considered that the evidentiary requirements of applications to New South Wales’s Victims Services for compensation are onerous and lead to significant delays in processing applications:
Changes to assessment process now requires victims to take the onus [in] providing medical and reporting evidence of [domestic, family and sexual violence] incidents (previously Victims Services gathered evidence on behalf of the victim, with consent). Evidentiary requirements are also cumbersome, as the requirement for medical evidence may in some instances not allow [victims and survivors] to apply for victims’ compensation because they have not reported incidents of violence, or they did not seek medical attention. (Respondent 27, Practitioner)
Family law courts
Much of the data relating to legal and court processes was concerned with systemic issues in the family law courts in Australia. Again, some of the issues identified related to resourcing, which contributes to lengthy wait times for cases to be heard by the courts. However, respondents also noted delays due to multiple adjournments, as well as the prohibitive costs of legal representation and the challenges for self-represented litigants:
Families may have to self-represent so experience poor outcomes as can’t afford a lawyer. Often violent men are given shared care when they should not [be] due to their violent behaviour. (Respondent 48, Practitioner)
Respondents described how, in their view, perpetrators weaponise court processes, such as adjournments and concealing assets, to enact abuse and coercive control:
[The family law courts are] used as an instrument to inflict maximum disruption and harm to women and children. (Respondent 54, Practitioner)
Perpetrators using violence often block therapeutic interventions [for children] as a way of maintaining power and control over mothers. (Respondent 59, Practitioner)
While respondents asserted that family law court proceedings and/or processes are frequently a source of re-traumatisation and systems abuse for victims and survivors, they also expressed how this system specifically harms children and disregards their voices. While Independent Children’s Lawyers should enable children’s voices to be heard, respondents lamented that in practice, Independent Children’s Lawyers, along with child and family assessors in family law court proceedings, frequently do not have sufficient capability or resources to make assessments in families where dynamics of abuse and violence are complex. A primary concern was that perpetrators are frequently granted access to children at the expense of their safety and wellbeing: “Courts give violent perpetrators chance after chance – and all too often award access to men who are terrorising their children.” (Respondent 15, Practitioner)
Following the commencement of the Australian Government’s court reform legislation, the Federal Circuit and Family Court of Australia commenced operation on 1 September 2021. The Court operates in all Australian states and territories, with the exception of Western Australia. The Australian Government’s reforms are intended to address many of the inefficiencies identified by respondents and to prevent adverse outcomes and harm for families. When first proposed by the Australian Government, the reforms faced opposition and criticism from key legal stakeholder groups centring on how adequately suited the proposed reforms were to addressing many of the factors that contribute to harm and poor outcomes, particularly around resourcing and training. The impact of these reforms on addressing these deeply entrenched systemic issues, particularly for those impacted by domestic, family and sexual violence, remains to be seen given the relatively recent
establishment of the Court:
The Family Court can and should do more to hold people using violence responsible and accountable instead of punishing victims [and] survivors for reporting violence and abuse and accusing them of “alienating” children from their fathers. (Respondent 59, Practitioner)
Future directions
Respondents identified a number of specialised approaches that have been implemented in some jurisdictions in Australia and elsewhere as promising future directions (Table 5). However, systemic issues of resourcing, workforce capability and multidisciplinary responses remain and are critical to addressing harm and poor outcomes in justice responses.
Table 5: Future directions to ensure justice responses are effective identified by respondents with exemplar quotes
Trauma- and violence-informed workforce training to improve outcomes at every stage of the justice process
Future direction
Respondent
Respondents identified the need for:
- implementing and/or funding more comprehensive training of court staff, magistrates, legal professionals and police to increase their awareness and understanding of the behavioural patterns underlying domestic, family and sexual violence. This should include quality improvement processes to monitor outcomes
“Increased training and monitoring of police responses. Following up with [domestic, family and sexual violence] victims and survivors to check in on the response received.”
Respondent 59, Practitioner
“Magistrates are making life-changing decisions about who children will live with and/or have visitation with based on reports written by professionals with little to no understanding of [domestic, family and sexual violence].”
Respondent 59, Practitioner
- centring children’s voices and needs through a child-centred approach along with trauma- and violence-informed workforce capability in court assessments, reporting and communication of outcomes
“Children are sometimes consulted and may be represented in legal decisions however often are not communicated with after on outcomes of decisions and why their views and wishes may not have been the ultimate decision.”
Respondent 4, Researcher
Increased resourcing for specialised multidisciplinary responses within and across sectors of the justice system
Future direction
Respondent
In policing, greater resourcing relates to increasing domestic, family and sexual violence liaison officers and specialised sexual violence support workers within stations to reduce risk of re-traumatisation and improve outcomes for victims and survivors
“Sexual assault teams, counselling and mental health support workers should be available at all police stations made available for victims [and] survivors making reports.”
Respondent 74, Practitioner
Respondents called for guidelines and legislation for implementation of information-sharing platforms to reduce re-traumatisation and enhance efficiencies
“Information-sharing imperatives (legislation and guidelines) which lack any implementation platforms [are not useful].”
Respondent 20, Service designer/manager
Increased regulation and monitoring for Independent Children’s Lawyers, report writers and other child court experts
Future direction
Respondent
Respondents proposed introducing minimum standards for Independent Children’s Lawyers, which include annual auditing of cases through an independent review process. This should include mechanisms for ongoing monitoring and evaluation to increase transparency and consistency of Independent Children’s Lawyers’ processes, assessments and outcomes
“Should be mandatory for them to speak to all professionals and services involved with the family and to see their client at least once.”
Respondent 15, Practitioner
Likewise, respondents suggested training, regulation and monitoring of Court Child Experts and other family report writers (independent social workers or psychologists that conduct family assessments)
“An assessment should be carried out by a highly skilled social worker or psychologist and their recommendations listened to.”
Respondent 15, Practitioner
Specialised responses to better support victims and survivors, and children and young people
Future direction
Respondent
Respondents identified the need for:
- enhancing existing mechanisms for family court-ordered supervised contact visits with parents who use violence. This would take the burden off the non-offending parent and enable a neutral observer to report on behaviours and hold perpetrators accountable
“Increasing children’s safety, holding people using violence accountable, lifting the burden off mother’s shoulders (currently they are required to manage their children’s safety, this causes a great deal of emotional stress and worry for many mothers and as their ex-partner’s behaviour is out of their control, it is actually an impossible, unmanageable task).”
Respondent 59, Practitioner
- ensuring that legal support is free, or affordable and accessible for all victims and survivors in relation to parenting arrangements
“Ensuring fair and equitable access to legal advice and representation.”
Respondent 59, Practitioner
- increasing availability of restorative justice processes that address the lack of legal outcomes and may better meet some victims’ and survivors’ needs than other legal responses
“Many victim survivors either choose not to go through legal process or do make a police report but does not make it to court, or perpetrator found not guilty. By witnessing and/or restorative justice process, victims and survivors have an opportunity to have their voice heard and perpetrator to take responsibility.”
Respondent 52, Practitioner
Respondents indicated that establishment of specialist family violence courts in Victoria, which adopt a victim-centred approach, could be promising for other jurisdictions. These are an outcome of Victoria’s Royal Commission into Family Violence
“As time goes on the knowledge and expertise of the magistrates should increase and better inform their decisions. They [courts] are intended to be a place where victims can feel secure that they will be understood and action taken to keep them safe. At this stage outcomes are still patchy, but one hopes they will improve.”
Respondent 15, Practitioner)
National Outcome 6 – Perpetrators stop their violence and are held to account
Where are we now
Similar to service responses for victims and survivors, respondents identified shortcomings in perpetrator responses that centre on insufficient services to meet demand, inadequate trauma-informed support for perpetrators and a lack of housing. These issues contribute to recidivism and also increase risks for victims and survivors: “Not providing any service to perpetrators is not effective.” (Respondent 15, Practitioner)
Moreover, responses are typically focused on averting immediate risk. There is a lack of long-term supports for perpetrators, which means there is little being done to generate lasting change:
The woman might be safe for now, but the male will perpetrate the same violence against his next partner and traumatise her children. (Respondent 15, Practitioner)
Little to no support … perpetrators are often victims first. (Respondent 88, Service designer/manager)
More specifically, respondents identified that initiatives addressing perpetrator accountability are variable across jurisdictions and that inadequate responses to breaches of court orders are highly problematic. One of the issues with intervention orders is that they typically only name the main victims and survivors. Respondents indicated that it would be beneficial to also include the victim’s and survivor’s wider support network, for example other family members or new partners who may be at risk from the perpetrator. Respondents also expressed the view that there need to be more stringent conditions on intervention orders and that breaches should be addressed with stronger penalties:
Messages are sent where this sort of contact is not allowed, sometimes threatening or abusive and the police note it, maybe have a talk to the perpetrator but do not breach, or if they do, the magistrate tells the perpetrator that if it happens again, the consequences will be severe – and the perpetrator gets the message that he can get away with anything. (Respondent 15, Practitioner)
The main interventions identified by respondents were therapeutic responses, where perpetrators are mandated to attend treatment, and group-based men’s behaviour change programs (MBCPs) to reduce recidivism. Various models of MBCPs were described, including MBCPs with case management, MBCPs with support for partners and MBCPs delivered in prison settings. Respondents identified that one of the strengths across various models of MBCPs was the approach taken by facilitators. They are mindful to maintain non-judgemental, non-coercive language and to work constructively with resistance:
Accredited behaviour change programs operate from a framework of gender disparity and hope to effect change by understanding the background of individuals and raising awareness of societal elements that contribute to men’s power and control leading to abuse. (Respondent 49, Practitioner)
MBCPs that combine varied approaches, such as motivational interviewing and case management, were considered to be sufficiently flexible in their approach to enable and engage participants with varied needs:
A combination of approaches [has] worked well to support change within the program – including narrative and strength-based approaches (to relate ethical choices back into men’s life experiences and to identify positive values that can be built upon). Motivational interviewing techniques are also used by facilitators, understanding that participants may be at different stages of change. A risk–needs–responsivity approach also underpins the program delivery – identifying clients[’] varied needs and dynamic risks and responding with appropriate interventions and responses including additional supports and referrals. The flexibility of case management assists participants with varied needs to remain engaged. (Respondent 2, Practitioner)
Further, case management can overcome barriers to accessing groups that have long waitlists or for men who need specific supports to enable them to be ready for group MBCP interventions:
Case-managed interventions allow increased flexibility to engage with men who may not be suitable for group (whether this is due to parental/employment responsibilities or other reasons such as mental health or substance misuse issues). (Respondent 2, Practitioner)
Groups like MBCPs are not always suitable, or the men need a lot of one-to-one group readiness work before attending the MBCP group. There are big wait lists for MBCPs, so case management could hold the men while they wait and reduce risk factors that may be contributing. (Respondent 48, Practitioner)
One respondent commented that there is a lack of understanding of MBCPs among magistrates, which leads to inappropriate sentencing:
There have been cases following a breach of [intervention orders] where magistrates have directed men [to MBCP]who have been assessed as either ineligible/unsuitable for [MBCP] interventions (e.g. clients being aggressive towards workers or demonstrating no interest in engaging/making any changes). (Respondent 2, Practitioner)
While respondents indicated that MBCPs can be effective, there were also concerns that they are not always culturally appropriate for Aboriginal and Torres Strait Islander men and men from culturally and linguistically diverse backgrounds: “MBCPs are not accessible to many men as their first language is not English.” (Respondent 48, Practitioner) Insufficient programs are available for LGBTQ+ communities.
Additionally, there can be variability in the accountability that is required of men who attend programs. This is key, both in terms of committing to attending the sessions and being held to account for their attitudes and behaviours: “Groups where they are not challenged on their ideas and behaviours … They can put in an appearance a couple of times and get away with saying they have attended.” (Respondent 15, Practitioner)
One respondent reflected on MBCPs delivered in prisons. They indicated that these can be ineffective at reducing recidivism as they need more psychoeducation, skill-building and focus on post-release supports: “Higher focus on emotional regulation … skills workshops, increased and extended supports upon release … Incarceration without rehabilitation is punitive and does not address the problem.” (Respondent 78, Practitioner and researcher)
Likewise, another respondent reflected that such programs need to be longer and more intensive, and include mentoring or peer support: “longer-term, group therapeutic program with a peer support element” (Respondent 87, Service designer/manager).
Some MBCPs have advocacy and other support for the men’s partners, which respondents indicated was a holistic and promising model:
Support and advocate with women their basic needs including safety planning, referral to others [sic] services and supports for themselves and their children. Case support aims to provide a framework where women are in control of decision-making, identify and direct what support they require. The outcome being that women will have an opportunity to be in control of their lives and become confident in seeking support and making decisions. (Respondent 28, Service designer/manager)
A whole-of-family response is vital to achieving safe outcomes – [MBCP with partner support] working closely throughout client engagement to assess and manage risk. (Respondent 2, Practitioner)
Likewise, for Aboriginal and Torres Strait Islander men, programs that are holistic and community led were considered to be most effective: “Interventions do not rely on the cognitive behaviour change approach but in men re-connecting with culture and community.” (Respondent 35, Researcher)
In contrast to MBCPs, respondents identified that many alternatives, such as moral reconation therapy groups and anger management groups, are ineffective. Respondents indicated such interventions can increase risk in some cases, particularly as they do not use a gender lens:
Sometimes courts accept an anger management group, but it is about power and control and male privilege, not anger management … it assumes the men can’t control their behaviour. (Respondent 48, Practitioner)
It is widely accepted in the men’s behaviour change field that men do not have an innate tendency to anger and its poor management is not what drives violence against women. It does not address power and control or the fact that men can be violent or controlling when not angry and that such behaviour is selectively deployed. (Respondent 49, Practitioner)
Likewise, respondents indicated that couples counselling can be ineffective and harmful, particularly when therapists do not have capability in recognising abusive and coercive behaviours:
Relationship counselling can be ineffective in cases where a power imbalance in the relationship is not addressed. An understanding of power and control and patterns of behaviour is necessary to promote a context where each partner has equity. Failure to account for this can lead to entrenched conduct and justification and further risk to vulnerable partners. (Respondent 49, Practitioner)
It is a space where abusers can use it to further abuse the victim. (Respondent 48, Practitioner)
In terms of early intervention, respondents identified gaps in responses to young people who use violence or are at risk of using violence. As respondents described it, there needs to be greater recognition that young people who use violence are frequently also victims and survivors who have had early adverse experiences and complex family dynamics. While diversionary interventions are promising, there also needs to be early intervention that focuses on promoting safety and wellbeing for these young people as opposed to focusing only on averting risk: “Diversion systems that expect young people to complete a three-month treatment program, or 10 sessions funded by Medicare, is [sic] simply inadequate.” (Respondent 14, Practitioner)
Future directions
Respondents identified promising future directions that expand the focus from averting risk to generating lasting behavioural change. While respondents felt it was important that justice responses are consistent and hold perpetrators to account, they also identified the need for more alternatives to criminal justice responses, including deterrence measures and strengthening therapeutic responses so that these better meet the diverse needs of perpetrators and families (Table 6).
Table 6: Future directions to stop perpetrators using violence and hold them to account identified by respondents with exemplar quotes
Address inconsistencies in holding perpetrators accountable
Future direction
Respondent
Respondents identified the need for:
- more stringent conditions on intervention orders with stronger penalties for breaches
“Enforcing harsher penalties for those convicted of breaching [intervention orders].”
Respondent 57, Practitioner
“Police prosecuting any breach plus magistrates taking it seriously and imposing suitable consequences.”
Respondent 15, Practitioner
- enhancing collaboration between MBCPs and magistrates to ensure appropriate sentencing and identification of men who are and are not suitable for court-mandated MBCPs
“Close working relationship between [MBCP] providers and the criminal justice system (in progress at present) to increase understanding of program objectives and scope.”
Respondent 2, Practitioner
Investigation and implementation of promising deterrence measures to reduce risk of recidivism
Future direction
Respondent
Respondents noted that deterrence devices, such as personal safety alarms, have shown promise in reducing recidivism and breaches of intervention orders
“Implementing as originally intended as a perpetrator deterrence device in conjunction with police, based on a pilot study … had a 98 per cent success rate in preventing AVO breaches for high-risk women.”
Respondent 8, Practitioner
Strengthen therapeutic interventions for perpetrators
Future direction
Respondent
Respondents identified the need for:
- enhancing cultural appropriateness of domestic, family and sexual violence interventions for perpetrators. This includes cultural competency workforce training but also development of more responsive approaches to working with men from culturally and linguistically diverse backgrounds
“Culturally sensitive family violence services for men (perpetrators) from a [culturally and linguistically diverse] background.”
Respondent 48, Practitioner
- addressing inequity in access to MBCPs for men in regional and remote locations, which may include online delivery of groups and/or case management
“As with group work and case managed (face to face) meetings, remote working would support men who want to engage to address their choice to use abusive and violent behaviours – most likely via an online platform.”
Respondent 2, Practitioner
- increasing availability of and access to specialised training for therapists and counsellors to identify abusive and/or coercive perpetrator behaviour
“Counsellors have to be vigilant and call out the perpetrators when [they] try to normalise or trivialise their behaviour.”
Respondent 16, Researcher
“All psychologists and counsellors need to have raised awareness of the dangers of family violence and counselling with couples. They need raised awareness of how to identify signs/red flags of family violence.”
Respondent 48, Practitioner
- increasing resourcing of psychoeducation programs for perpetrators other than MBCPs, such as parenting programs with a focus on understanding trauma and managing emotions
“It is co-facilitated by a male and a female to model effective and equal communication between males and females … Sometimes there is a corresponding female group which acts as a control group reporting on how and if change is occurring in the home.”
Respondent 15, Practitioner
- investment in early intervention and therapeutic programs, such as therapeutic treatment orders for young people who have engaged in problem sexual or sexually abusive behaviours
“Look to what works in other countries. Therapeutic court interventions work.”
Respondent 14, Practitioner
“In Victoria there is already a system including specific legislation [therapeutic treatment orders] and treatment services [Sexually Abusive Behaviours Treatment Service] that works in hand with the justice response.”
Respondent 89, Practitioner
Key themes
We generated five key themes that reflect workforce perceptions of what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators. These are contextualised and expanded with reference to literature that examines system and service responses to domestic, family and sexual violence.
Addressing upstream determinants of domestic, family and sexual violence
This theme points to the need for greater investment in addressing upstream determinants of violence and abuse. Enacting an upstream approach means addressing structural barriers that create and sustain multiple and intersecting forms of inequality, which are root causes of violence and abuse in our relationships, families, schools, workplaces and communities. In practical terms, respondents identified key social determinants that require an upstream approach, with the primary ones being poverty, equal participation in the workforce, and safe and affordable housing: “A public health approach is required”, including “a stronger focus and resources on prevention” (Respondent 46, Researcher).
Equal and fair participation in the workforce in Australia has the power to change structures, norms and practices that ultimately drive violence (Our Watch, 2022b). The gender pay gap in Australia is the result of gender inequality and perpetuates the devaluing, exclusion and marginalisation of women (Our Watch, 2022b). To address this, the social and economic factors facilitating the gender pay gap need to be addressed, as do attitudes towards women in the workplace. In 2017, the National Community Attitudes towards Violence against Women Survey (NCAS) found that 14 per cent of respondents did not believe women were as capable as men in politics, 14 per cent believed men were more capable bosses, 24 per cent did not see an issue with sexist jokes, 40 per cent felt women exaggerated inequality between men and women, and 10 per cent did not think discrimination against women in the workplace was an
issue (Webster et al., 2018).
Women are more likely than men to experience direct and indirect discrimination in the workplace because of pregnancy, breastfeeding, carer responsibilities or relationship status. Discrimination contributes to the factors facilitating the gender pay gap and sexual harassment in the workplace (Our Watch, 2022c). Sexual harassment includes any unwanted or unwelcome sexual behaviour that it is reasonable to assume will offend, humiliate or intimidate (Australian Human Rights Commission, 2022). Workplace sexual harassment is highly gendered. Between 2017 and 2018, 23 per cent of women were sexually harassed at work compared to 16 per cent of men, and the majority of perpetrators (four in five) were male (Gebicki et al., 2018). Some women are more vulnerable to sexual harassment in the workplace, including Aboriginal and Torres Strait Islander women, women with disability or disabled women, LGBTQ+ people and young women (18 to 24
years; Gebicki et al., 2018). Women are more likely to experience sexual harassment in workplaces that are
male -dominated (Gruber, 1998; Saunders & Easteal Am, 2013). This was demonstrated in a review of the treatment of women in the Australian Defence Force Academy, which found that 71 per cent of female cadets experienced sexual harassment, compared to 30 per cent of male cadets (Australian Human Rights Commission, 2011).
In addition to workplace harassment and discrimination, experiencing violence outside the workplace can directly or indirectly be a barrier to victims’ and survivors’ full and equal participation in the workforce (Moe & Bell, 2004). For some victims and survivors, experiencing violence is associated with unstable employment (Adams et al., 2012; Crowne et al., 2011; Moe & Bell, 2004; Staggs & Riger, 2005). This can be the result of abusive tactics that directly interfere with employment, such as harassing victims and survivors at their place of work, or interfering with the process of upskilling for or finding a job (Adams et al., 2012). Indirectly, the physical and mental health consequences of violence can lead to time off, frequent job changes and decreased job satisfaction (Crowne et al., 2011; Moe & Bell, 2004; Riger et al., 2004; Tolman & Wang, 2005). The impact of violence on job stability can persist long
after the abuse has ended (Crowne et al., 2011). Additionally, without a stable income, victims and survivors are less likely to have the economic resources required to leave a perpetrator (Adams et al., 2012; Cortis & Bullen, 2016). In Australia in 2020–21, 51 per cent of employers offered paid domestic violence leave, a fourfold increase from 2015 (Workplace Gender Equality Agency, 2022a). Not only does this type of leave provide victims and survivors with some financial stability when leaving a perpetrator, but when organisations adopt it, it represents their commitment to staff wellbeing and raises awareness of the impacts of violence on employment (Breckenridge et al., 2015).
Respondents’ views on housing are in line with literature that argues it is a key determinant in addressing domestic and family violence (Braaf & Meyering, 2011; Cortis & Bullen, 2015; Webster, 2016): “Housing is one of the biggest barriers to resolving the effects of [domestic and family violence] on victims.” (Respondent 49, Practitioner)
In 2020–21, 42 per cent of specialist homelessness service clients had experienced family or domestic violence (Australian Institute of Health and Welfare, 2021d). Since 2011–12, this number has increased annually (Australian Institute of Health and Welfare, 2021d). The majority of these clients were returning clients, and domestic and family violence was the main reason they were seeking support (Australian Institute of Health and Welfare, 2021d). Following domestic and family violence, loss of housing ownership, limited access to affordable social and private rental housing, and discrimination in the private rental market make it difficult for victims and survivors to access safe and affordable housing (Cortis & Bullen, 2015). Some victims and survivors do not have rental history or have poor rental history because of continued abuse or threats that require them to break leases and/or regularly relocate (Braaf & Meyering,
2011).
In line with the National Plan and the Fourth Action Plan, the Commonwealth Government introduced a “Keeping Women Safe in their Homes” initiative to enable women and children to remain in their home or a home of their choosing (Department of Social Services, 2021). The programs implemented as part of this initiative offer long-term and wrap-around support, case management and ongoing safety planning (Breckenridge et al., 2016). This departure from traditional crisis interventions is seen as a strength because victims and survivors are impacted by violence long after they leave the perpetrator (Breckenridge et al., 2016; Diemer et al., 2017). However, this initiative is only suitable for victims and survivors who will not be at risk of further violence by remaining in their home, and is not successful without proactive action from police and courts to monitor perpetrators and enforce protection orders (Breckenridge et al., 2016;
Diemer et al., 2017).
Reactivity and inequity in responses harms victims and survivors
This theme speaks to the need for systemic changes that address the full spectrum of prevention, early intervention, response, and recovery. Respondents emphasised that the system is set up to be reactive to incidents of violence, with less resourcing and capability for early intervention and prevention. This reactivity impacts, in particular, Aboriginal and Torres Strait Islander peoples and communities, with one respondent noting: “We have another stolen generation through Child Protection. We need to strengthen families, do more prevention community work … less reactive responses.” (Respondent 48, Practitioner)
Further, beyond crisis intervention responses that focus on immediate safety, respondents identified that there are gaps and bottlenecks in responses that focus more on long-term recovery and transitions. This largely relates to a lack of services and referral pathways, which is compounded in regional and remote areas and for people who face additional structural barriers to accessing support, including racism, ableism and ageism. The effect of this is that many perpetrators and victims and survivors are not able to effectively move forward from violence and abuse – the cycle repeats, with continued strain on crisis intervention services as well as the criminal justice, health and child protection systems. “[We need] a system that believes the [victim and survivor] has right to and provides safety and recovery.” (Respondent 10, Practitioner)
This theme also relates to issues of traumatisation, re-traumatisation and ineffective responses that harm victims and survivors. These systemic issues can also manifest in inadequate responses and lack of services for perpetrators, which ultimately increase harm and risk for victims and survivors.
Respondents acknowledged systemic issues are closely related to inadequate resourcing and limited funding, which results in narrow eligibility criteria for accessing services and rigid key performance indicators that are determined by funders and do not reflect community need. The implications of this in practice are long wait times and lack of choice, which are not only harmful but can also perpetuate trauma and deprive victims and survivors of agency:
As a worker I struggle sometimes getting in touch with [domestic, family and sexual violence] services, often nobody answers, needing to leave messages, sometimes days go by without a response. I can only imagine what this experience would be like for women calling for support … Also, the wait lists can be very long, I’ve had clients wait over one year for case management support. (Respondent 52, Practitioner)
It is vital that contact is made quite quickly and the [victim and survivor] does not have to wait. (Respondent 15, Practitioner)
Importantly, respondents linked these systemic issues around resourcing and workforce capability with poor coordination and inadequate responses that contribute to victims’ and survivors’ resource deprivation, isolation and traumatisation. This is consistent with workforce perspectives in the 2017 National Survey of Workers in the Domestic, Family and Sexual Violence Sectors (Cortis et al., 2018). Only 38 per cent of respondents felt their service was adequately staffed and four in five felt their services were inaccessible (Cortis et al., 2018). In particular, respondents felt there were limited service options for perpetrators, Aboriginal and Torres Strait Islander communities, young people, rural communities and people seeking housing support (Cortis et al., 2018).
Further, these reports of limited service options align with victim and survivor accounts (Evans & Feder, 2016; Kiamanesh & Hauge, 2019; Peckover, 2003; Robinson & Spilsbury, 2008). Victims and survivors who accessed specialist services reported access to support was difficult unless experiencing a crisis or homelessness (Evans & Feder, 2016). Resources such as shelter or informal support were rarely offered to victims and survivors despite disclosure and histories of mental health issues related to violence (Evans & Feder, 2016). Culturally and linguistically diverse women in a shelter reported that support services did not improve their situation because they were not tailored to their specific needs (Kiamanesh & Hauge, 2019). They described the help offered as a burden (Kiamanesh & Hauge, 2019). Similar results were seen in qualitative studies of victims and survivors accessing mainstream health
services (Peckover, 2003; Robinson & Spilsbury, 2008).
The traumatisation and re-traumatisation of victims and survivors and simultaneous deprivation of resources can lead to “loss spirals” (Schmidt, 2014). These can be considered in the context of conservation of resource theory, which is based on the idea that psychological reactions to stress such as trauma are related to accompanying social, economic and interpersonal resource loss or the threat of loss (Hobfoll, 2001; Hobfoll & Lilly, 1993; Schmidt, 2014). Trauma then exacerbates further loss, leading to these loss spirals (Hobfoll & Lilly, 1993; Schmidt, 2014). As such, individuals with fewer resources when they experience a stressor are more vulnerable to a greater and faster loss spiral (Hobfoll & Lilly, 1993; Schmidt, 2014). When services reinforce a stressor or deprive victims and survivors of resources, it replicates the context of violence and abuse and exacerbates loss spirals (Adams et al., 2008; Bybee &
Sullivan, 2002; Sullivan & Bybee, 1999; Sullivan et al., 2002). Equally, services that do support victims and survivors to access resources lessen the mental health impacts of violence and/or support recovery (Beeble et al., 2010; Coker et al., 2003; Schmidt, 2014).
There was much consideration of gender inequality by respondents, and how the impacts of gender inequality are not felt equally by all. Furthermore, binary notions of gender that are the foundations of gender inequality discourse are problematic and can disregard or marginalise the experiences of non-binary, gender-diverse or non-cisgender individuals. Moreover, respondents detailed systemic biases that impact those who experience multiple forms of discrimination and advocated that an intersectional lens must be applied to address systems abuse. While there is awareness that systems abuse disproportionately impacts those who experience intersecting axes of oppression, and intersectional approaches are referenced in policy and practice guidelines, this is largely still a poorly understood framework. As respondents identified, it is also not well operationalised in practice: “[We need] intersectional approaches to intervention – each survivor is
understood and what unique challenges they have because of systems that are, for example, racist or homophobic.” (Respondent 73, Practitioner)
This is indicative of the need for a trauma- and violence-informed system that considers the intersecting experiences of oppression, power and privilege. Trauma- and violence-informed care acknowledges that people who experience systemic inequities and structural violence will have experienced multiple and intersecting forms of trauma that extend beyond traumatic events or interpersonal trauma (Browne et al., 2017; Browne et al., 2012).
Critical to embedding trauma- and violence-informed approaches is recognition of the historical and contemporary violence of colonisation. This requires understanding trauma as intergenerational and influenced by systemic inequities and structural violence. As such, the focus is on validating and recognising strengths in the context of trauma and establishing lifelong healing as well as preventing re-traumatisation (Browne et al., 2017; Browne et al., 2012). Key to embedding trauma- and violence-informed care across the system is workforce capability, coordination and collaboration (Carlson et al., 2021; Cullen, Mackean, et al., 2021; Cullen et al., 2020). This can include strengthening partnerships, multisectoral responses and coordination, for example through streamlined information sharing between services and sectors or advocacy to influence policies or available services in a community (Browne et al., 2012).
Changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
This theme amalgamates respondents’ views that knowledge and cultural shifts are required to better conceptualise domestic, family and sexual violence, so that our understandings consider the intersection of violence within the broader context of structural and social determinants. Respondents asserted that harmful understandings of domestic, family and sexual violence contribute to victim blaming. In practice, this results in responses and outcomes that do not hold perpetrators to account for their use of violence and can further victimise and traumatise victims and survivors. In particular, respondents identified welfare and child protection frameworks that pathologise and harm victims and survivors:
Traditional welfare models often pathologise the victim and do not emphasise a rights-based approach. They may also collude with offenders. The criminal justice system has a significant role to play but these systems offer work counter to the needs of victim survivors. (Respondent 23, Service designer/manager)
There were concerns that such frameworks frequently blame non-offending parents, typically mothers, for not keeping children safe rather than focusing on the person using violence in the home:
When women come into the refuge space, they are supported with child protection services, amongst other services. But the perpetrator soon becomes invisible and it all becomes about her and her behaviour. Was she a protective mother? Does she have [mental health] issues that impact her parenting and is her [alcohol and drug] use damaging to the children. We should be pivoting back to the perpetrator. That is, how did his actions impact on her functioning and family ecology? (Respondent 86, Service designer/manager)
There was a nuanced relationship between perpetration and victim blaming when it comes to young people who use violence. Respondents indicated that young people’s actions are often not sufficiently conceptualised in the context of their history of experiencing violence and abuse. As one respondent put it, when young people are charged and prosecuted for their behaviour:
It is shaming and blaming and as a result feeds into the dynamics that have likely led that young person to engage in the violent behaviour … it is punitive and pays little mind to a young person’s developmental status or history of trauma. It does not in and of itself offer a young person a different way of being, the potential to develop a new way of relating. (Respondent 14, Practitioner)
Victim blaming and narrow conceptions of violence and abuse were also considered in the context of coercive control. Recent debates around the criminalisation of coercive control have shed much light on the challenges around understanding, identifying and responding to perpetrators and victims and survivors (Fitz-Gibbon et al., 2020; Smyth et al., 2021; Wangmann, 2020). One of the challenges with widespread community understanding of coercive control is the commonly held incident-based understanding of domestic, family and sexual violence that fails to consider the evolving, cumulative and individualised nature of coercive control (Joint Select Committee on Coercive Control, 2021; Smyth et al., 2021; Women’s Safety and Justice Taskforce, 2021). Another related challenge is the issue of misidentification of the primary victim and the risk of systems abuse by the perpetrator (Joint Select Committee on Coercive Control, 2021; Smyth et al.,
2021; Women’s Safety and Justice Taskforce, 2021): “The lack of recognition/prosecution for coercive control and an ability to evidence it often means women’s statements aren’t proceeded with and police/judicial practices don’t support women.” (Respondent 27, Practitioner)
In order to overcome these challenges, states that are criminalising coercive control have committed to ensuring public education on coercive control is a central element of the legislative process (Joint Select Committee on Coercive Control, 2021; Smyth et al., 2021; Women’s Safety and Justice Taskforce, 2021). However, there needs to be sufficient time, training and resourcing, and despite assurances to the contrary there are community concerns that legislation to criminalise coercive control has the potential to harm rather than protect victims and survivors. This relates to the known intersections between coercive control and other societal systems of oppression and violence, and in particular the disregard for, discrimination against and criminalisation of Aboriginal and Torres Strait Islander women.
An alternative model proposed by respondents to overcome systemic biases and misconceptions was the “social entrapment” model. The social entrapment model avoids victim blaming by recognising intersecting structural and social determinants that underpin the perpetrator’s ability to enact violence and the safety responses available to the victim (Douglas et al., 2021; Ptacek, 1999). Applying the social entrapment model as a framework to conceptualise experiences of violence has potential to promote holistic responses that better meet the needs of victims and survivors (Douglas et al., 2021; Ptacek, 1999; Tolmie et al., 2018). One respondent outlined key considerations in this model:
Understanding the pattern of harm over time, with an emphasis on coercive control … Realistically looking at what safety options exist, rather than assuming them … Seeing structural inequities as essential to understanding not only the victim’s circumstances and the perpetrator’s behaviour, but also the social response (the service system, options for safety, community attitudes, practitioner responses) as a whole. (Respondent 48, Practitioner)
In terms of service responses that address misconceptions and misattribution of blame, several respondents identified the Safe & Together model. A child-focused model, Safe & Together is based on three principles that prioritise the safety and wellbeing of children: keep children safe and together with non-offending parents; partner with the perpetrator and hold them accountable; intervene with the perpetrator to reduce risk and harm to children (Safe & Together Institute, 2020).
The critical components of the model involve gaining a deeper understanding of the patterns of coercive control and the harmful actions of the perpetrator; adverse impacts on the child; the role of substance use, mental health, culture and other socio-economic factors; and the protective role of the non-offending parent (Safe & Together Institute, 2020). This model originated in the United States and has been implemented in the United Kingdom, Scotland and Australia. The model (originally designed for child protection settings) has recently been adapted to the context of Australia’s family law system and the roles performed by those court officials and judicial officers with training delivered to judges, registrars and Court Child Experts within the Federal Circuit and Family Court of Australia. Safe & Together was highly regarded by respondents as it creates a shared language, understanding and collaborative practice aimed at supporting
the non-offending parent:
This child-centred model derives its name from the concept that children are best served when we can work toward keeping them safe and together with the non-offending parent (the adult domestic violence survivor). The model provides a framework for partnering with domestic violence survivors and intervening with domestic violence perpetrators in order to enhance the safety and wellbeing of children. (Respondent 48, Practitioner)
… recognised in Australia and internationally as a way to address siloing of information between services. It creates a common language and focus for all stakeholders including police, magistrates, family court, counsellors, [domestic violence] services, legal services and child protection. The perpetrator mapping tool shifts focus to the perpetrator. (Respondent 8, Practitioner)
Underpinned by the social entrapment model, Safe & Together averts victim blaming through a strengths-based approach that focuses on recognising and strengthening “the protective behaviours of the mother” (Respondent 52, Practitioner). Additionally, accountability for perpetrators is key and this is accompanied by practical supports to make meaningful change toward being a safe and capable parent: “Holding them accountable towards every step towards change, recognising unhealthy patterns.” (Respondent 33, Researcher)
Enabling choice and the right to self-determination
This theme draws on approaches that counter assertions within the previous three themes that systemic biases, inequities and victim blaming constrain choice and resourcefulness that are essential for victims and survivors. Indeed, respondents assert that the systems that are intended to enable safety and agency can entrench victims’ and survivors’ isolation, mistrust and helplessness.
[Victims and survivors] need to be treated with respect and made aware of their rights in order to help them recover. When this does not happen, they are mired in their sense of worthlessness. (Respondent 15, Practitioner)
While resourcing is an issue that constrains choice, respondents also pointed to widespread inconsistencies in access to supports that stem from limited and inconsistent access to appropriate information about rights and options. Respondents attributed this to shortcomings in workforce capability and knowledge, and this also reflects the need for broader systemic shifts toward trauma- and violence-informed responses, which promote choice, dignity and agency.
[We need] clearer information given to [victims and survivors] about the whole process so people can make informed choice[s]. (Respondent 52, Practitioner)
This perpetuates feeling of helplessness and just being someone things are done to rather than [an] adult with agency. (Respondent 15, Practitioner)
In order to enable choice for victims and survivors, gender sensitive and trauma- and violence-informed service models are essential (Oram et al., 2022). Respondents identified that the Victorian Centres Against Sexual Assault (CASA) is such a model, which seeks to enable victims’ and survivors’ choice and self-determination. Since 1990, 15 CASA have been established in Victoria to ensure victims and survivors of sexual assault and family violence have access to responsive, comprehensive and safe support and interventions. The services offered by CASA include 24-hour crisis care, advocacy, counselling, referrals and therapeutic treatment services for young people with sexually abusive behaviours. CASA are also involved in workforce development training, school safety programs and research projects.
The CASA model is underpinned by the victims’ rights model of justice, which acknowledges the link between rights, empowerment and long-term healing for victims and survivors of sexual assault. This model is non-punitive and focused on crime prevention and restorative justice (Roach, 1999). It is based on the idea that, when successful, it helps to foster stronger communities through a process of healing, compensation and restorative justice (Roach, 1999). Underpinned by this model, CASA work to centre and empower victims and survivors with rights and choices (Centres Against Sexual Assault Forum, 2014). They are also committed to collaborative decision-making and long-term healing (Centres Against Sexual Assault Forum, 2014). As one respondent describes it:
Knowledge and understanding of the individual, cultural, social and universal context of the lives of women and children is fundamental. The framework therefore acknowledges that CASAs respond to the presenting issues of sexual assault and to the victim[s’] and survivors[’] individual experience of it. This includes the emotional, psychological, developmental, economic and social consequences relating to the sexual assault. The CASA model places importance on the valuing of clients’ experience, strengths and skills. (Respondent 50, Service designer/manager)
Key to the CASA model is providing timely treatment and choice. The counselling and therapeutic models are centred around principles of feminist practice (Centres Against Sexual Assault Forum, 2014). These principles include empowering through choice and options, believing and validating experiences, reframing and reinterpreting abuse, and non-judgemental language. Equally, a central goal of the crisis care is facilitating victims’ and survivors’ choice and control over outcomes (Centres Against Sexual Assault Forum, 2014):
Regaining of control via informed decision making. Management of health issues that may arise as a consequence of being raped. Personal advocacy which diminishes the risk of secondary systems abuse … provided with information and is supported to implement decisions that she makes. (Respondent 23, Service designer/manager)
Through immediate delivery of services subsequent to a [sexual assault] the victim’s sense of control can start to be rebuilt. (Respondent 23, Service designer/manager)
Indeed, respondents emphasised how critical choice and self-determination are for victims and survivors. Importantly, respondents asserted that these can be further constrained for those for whom mainstream services do not adequately meet needs for cultural safety, inclusion and accessibility:
Ideally the service is trained in accessibility, cultural competency and inclusion. It is also important that referral pathways are in place for community-controlled services so groups such as Indigenous women or LGBTQI+ people have a choice which service to engage. (Respondent 49, Practitioner)
For Aboriginal and Torres Strait Islander communities, self-determination draws on decolonising approaches, which are critical to enabling community-owned and -led solutions. Respondents identified highly regarded approaches that take a decolonising approach and as such are grounded in self-determination. One respondent described how this is embedded within Marninwarntikura Women’s Resource Centre in Fitzroy Crossing, Kimberley, Western Australia:
Marnin is based on Bunuba country and works from within law and culture. It covers the spectrum of women’s needs, it has a legal service and a refuge, but places emphasis on community-led initiatives and strengthening culture. It engages Elders in a leadership role and focuses on intergenerational trauma rather than simply male power. It takes an explicitly decolonising approach … It ensures that cultural knowledge leads in the creation of interventions, there is a belief that culture must lead interventions. For example, decision-making often takes place on country, where Aboriginal knowledge takes precedence over mainstream knowledge. The various clan and language groups are all represented, often with women Elders in a leadership role. (Respondent 35, Researcher)
The importance of self-determination is seen in Aboriginal and Torres Strait Islander–led policy and reviews on what works in response to family violence (Carlson et al., 2021; VACCA et al., 2019; Victoria Department of Health and Human Services, 2018). State-based family violence policies such as Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families (Victoria Department of Health and Human Services, 2018) and the Nargneit Birrang framework (VACCA et al., 2019) centre self-determination as a guiding principle. The Nargneit Birrang framework is a Victorian holistic healing framework for family violence. Other key principles in
the Nargneit Birrang framework include safety as a priority; embedding culture, Country and community in healing; the past impacts on the present; trauma-informed healing; and resilience and hope (VACCA et al., 2019).
The importance of community-based and culturally safe services has been emphasised in policy, research and advocacy by Aboriginal and Torres Strait Islander scholars (Longbottom, 2019; Porter et al., 2021). A review of Aboriginal and Torres Strait Islander family violence programs found that self-determination is a key factor in healing (Carlson et al., 2021). A review examining what works in responses to family violence from the perspectives of Aboriginal and Torres Strait Islander women and communities similarly emphasised that Aboriginal and Torres Strait Islander peoples play a significant role in the development of effective and culturally safe responses (Olsen & Lovett, 2016). This was echoed in a qualitative study on the experiences of Aboriginal and Torres Strait Islander women’s engagement with legal and social family violence services (Langton et al., 2020). This study found that culturally safe care, that was appropriate and accessible,
was in most cases provided by Aboriginal and Torres Strait Islander–specific services (Langton et al., 2020).
Power of connection, collective healing and compassion
This theme emphasises that experiences of violence, abuse and trauma are unfortunately common, and our shared experiences bring opportunities for connection and compassion, which are fundamental to healing for individuals but also for collective healing. Respondents were clear that while there are systemic issues that can be powerful in enacting and compounding victims’ and survivors’ experiences of trauma, there are also systemic strengths that are powerful in generating healing and recovery.
For services and practitioners working with victims and survivors, creating a sense of safety through hearing and believing their experiences is imperative. This is especially true for those working with children and young people.
… to enhance personal safety and control, to enable people to process their trauma effectively … without further violence and without the economic and social disadvantage that can inhibit their recovery. (Respondent 87, Service designer/manager)
In terms of healing and recovery, one of the workforce’s main strengths lies in its relational capacity, with many members highly skilled in compassionate and trauma-informed responses. Building therapeutic relationships is a key aspect of healing from violence (Flasch et al., 2015; Sinko et al., 2021). This enables victims and survivors to feel safe, build support networks and cultivate a feeling of belonging (Sinko et al., 2021). Additionally, such relationships are akin to “walking beside” victims and survivors, which is important in not only preventing systems trauma and responding to crisis, but also in supporting healing in the longer term (Cullen, Stevenson, et al., 2021). This is echoed in a qualitative study of women with a history of sexual violence and mental health difficulties, in which women identified that their healing journey was enhanced by supportive counselling within holistic models of care that fostered a sense of
connection (Hegarty et al., 2017). As one respondent affirmed, the therapeutic relationship and providing the right support at the right time are critical in recovery and healing:
Rapport between therapist and client is vital. To go at client’s pace. Allow the client control – don’t try to force client to tell story too early … To introduce formal therapy when client ready, ideally graded exposure but it is important to recognise that many clients never reach this stage. (Respondent 15, Practitioner)
Respondents emphasised that therapeutic interventions focusing on embodied, relational and attachment approaches were important, as were narrative therapy approaches that enable victims and survivors to make sense of their experiences and integrate these within the narrative of their life experiences:
Trauma-focused CBT is better than traditional CBT. I’m not convinced it’s really the best way to go in the family violence/harmful sexual behaviour realm, as it does not take into account the impact of early relational trauma, intergenerational trauma, attachment disruption. (Respondent 89, Practitioner)
Current evidence supports a much broader approach to supporting trauma recovery, including yoga etc. (Respondent 8, Practitioner)
Further, respondents identified that psychoeducation is important in validating victims’ and survivors’ experiences of violence, abuse and trauma, as well as facilitating understanding of responses to trauma. This aligns with evidence that psychoeducation is a key point of best practice for complex trauma as it allows victims and survivors to understand how trauma has impacted their lives (Salter et al., 2020). Helpful psychoeducation topics include normalising responses to trauma, identifying and responding to triggers, naming and understanding abusive relationships and tactics, healthy relationships, and safety planning (Salter et al., 2020). “To provide psychoeducation on trauma – absolutely vital. To teach strategies to deal with intrusive thoughts and memories and to self-regulate.” (Respondent 15, Practitioner)
Respondents felt psychoeducation was particularly effective when delivered in a group format, as this enables collective healing that accompanies sharing of experiences. This is consistent with evidence that sharing stories can lead to feelings of validation and mutuality, especially when shared in a non-judgemental environment facilitated by peer workers and/or counsellors (Heywood et al., 2019). Indeed, advocates and peer workers who bring lived expertise are an important part of the workforce in promoting connection and healing through shared experiences.
The aims of the group were to support self-expression, relationship buildings to reduce isolation, increase feelings of empowerment and mastery through artmaking and stimulating different senses and curiosity. A strengths-based approach was deliberately adopted to broaden positive experiences without re-traumatisation. (Respondent 50, Service designer/manager)
The importance of collective healing is also emphasised in responses to Aboriginal and Torres Strait Islander peoples’ experiences of violence (Carlson et al., 2021; Olsen & Lovett, 2016). The focus in this context is on collective and family healing, with the aim of strengthening family relationships, community cohesion and connectedness to culture and Country (Carlson et al., 2021).
Promoting healing and recovery was viewed as a priority area for further research and service development. Respondents asserted that supporting the healing and recovery of victims and survivors, children and young people and people who use violence is important in averting intergenerational trauma, and is a key component of response and prevention.
Strengths and limitations
The findings from this study should be considered in light of its strengths and limitations. Firstly, the sample of 95 is a small representation of the workforce responding to domestic, family and sexual violence and under-represents key sectors and jurisdictions. Geographically, the majority of respondents are drawn from Victoria, Western Australia and New South Wales, with more than one third of respondents working in Victoria. This means that there was an emphasis on models of care and responses in these jurisdictions and limited insight into effective responses and contextual factors specific to other jurisdictions.
There were few respondents drawn from key sectors such as policing, clinical health services, legal services, disability services and Aboriginal and Torres Strait Islander organisations. Further, there were no respondents who identified as working in child protection, housing or LGBTQ+ specialist services. There were also few respondents whose work focused on primary prevention. This relates to the recruitment strategy, which, though purposive, relied on existing networks. Accordingly, more than half of respondents were drawn from services whose core business is addressing domestic, family and sexual violence. This has given substantial insight into the challenges and successes in these settings, and the perspectives of this workforce are rich with highly specialised expertise and knowledge of domestic, family and sexual violence. However, there was less insight into what works and is needed in more mainstream settings that are not specialised in
responding to domestic, family and sexual violence, or what works in primary prevention. Perhaps this partially reflects the siloing of services in Australia, and a broader recruitment strategy is certainly a consideration for future studies that wish to capture more diverse perspectives.
We sought to privilege the perspectives of the respondents, however reflexive thematic analysis is inherently linked to the experiences and interpretations of the research team. As such, the research team were mindful of our world views and how they are context-bound and may be reflected in the analysis. To enable a breadth of perspectives to shape the findings, the research team sought insight and guidance from key stakeholders and experts in domestic, family and sexual violence – firstly, from the Voices Advisory Committee, who provided valuable input into the study design, methods and interpretation of the findings; and secondly, from key stakeholders across state and territory jurisdictions as well as the Australian Government, who provided feedback on the findings and recommendations.
The online survey used an iterative qualitative approach with open-ended questions that enabled respondents some flexibility in how they responded. Unlike a fully qualitative approach, the online survey contained fixed, structured questions presented in standard order, which obviously differs from a flexible, semi-structured interview or focus group. A limitation of this is that it does not allow for conversation, observation, clarification or probing for more details. Despite this, there are several benefits to this approach. Online qualitative surveys are a cost-effective and efficient method for gathering perspectives from a large population. They are convenient for respondents, who can participate on their own terms, and the anonymity of the online format may have supported respondents to be candid and considered in their responses.
While respondents were able to choose the sections of the survey they responded to according to their expertise, some respondents indicated that the survey was unduly long and repetitive. Additionally, there were a large number of respondents not included in the analysis as they did not provide substantive responses to the qualitative questions, which may suggest that the requirements of the survey were perceived to be onerous, the time of year being a busy period, or the increased workload due to the impact of the COVID-19 pandemic on the sector. These factors are important considerations for further studies using this approach and additional piloting with the workforce is recommended.
Nonetheless, this dataset is richly detailed and gives unique perspectives and insights from a highly experienced workforce. Most respondents had worked in the sector for six or more years, with almost half having 10 or more years of experience. As a result, there is a depth of experience that provides important insights into the challenges of working in this complex sector. This is also reflected in the opportunities and priorities identified by the workforce, which comprehensively address intersecting issues of equity, accessibility and justice.
Conclusion and recommendations
This study explored the perspectives of the domestic, family and sexual violence workforce in Australia using an online qualitative survey. Richly imbued with lived expertise from those on the frontlines, the findings identify important priorities and opportunities for innovative responses that embrace complexity and enable choice and self-determination. Underpinned by sustainable resourcing, enabling policy and workforce strengthening, systemic strengths can generate powerful shifts toward addressing the full spectrum of prevention, early intervention, response and recovery. This study demonstrates the depth of insight and expertise in the Australian domestic, family and sexual violence workforce, whose knowledge of the complexities, strengths and challenges faced by the sector are invaluable in creating meaningful change. Their voices are a powerful call to action and signal the importance of centring lived experience and expertise in policy and
practice solutions.
A primary concern for the workforce was inadequate and short-term funding cycles, which prevent services from meeting demand and constrain capacity for collaboration and sustaining the workforce. Issues with resourcing also impact workforce competency and capability, which was identified by respondents as a barrier to effective collaboration and outcomes. Respondents indicated that there is a high degree of variability in the workforce capability and thereby recognised that responding to victims and survivors and holding perpetrators to account is highly variable in practice.
A number of areas of competency were identified for different sectors, indicating a need for comprehensive trauma- and violence-informed care training across health, justice and social services. As a framework, trauma- and violence-informed care provides a foundation for understanding domestic, family and sexual violence as well as the intersections with other forms of power, privilege and oppression. In particular, there is a need for greater capability in understanding and responding to the dynamics of abuse, the ways these intersect with other experiences of violence and trauma, and how this can manifest in different contexts.
Key recommendations
Our findings point to important opportunities and priorities for service and system improvement with recommendations across four key areas:
- Promote safer communities, workplaces, schools and homes.
- Enhance workforce competency, capability and collaboration across sectors.
- Break intergenerational cycles of violence and trauma by better supporting children and young people.
- Bring forth innovative solutions.
Promote safer communities, workplaces, schools and homes
Recommendations to promote safer communities, workplaces, schools and homes are underpinned by the recognition of domestic, family and sexual violence as a social determinant of health. Accordingly, these recommendations seek to ensure that domestic, family and sexual violence is addressed within the context of intersection with other social determinants, such as safe housing and communities; income equality; workforce participation; social inclusion and non-discrimination; and equitable access to justice, healthcare and social services.
Recommendation 1
Prioritise safe and affordable housing solutions by governments to address critical shortages and bottlenecks in emergency housing, as well as shortages in other short- and long-term housing. Universal design principles are essential to ensuring that housing solutions are appropriate and accessible for all.
Recommendation 2
Provide federally funded and accredited community bystander training to mobilise and equip individuals to recognise and respond to domestic, family and sexual violence. Training should be free and co-produced with lived expertise advocates.
Recommendation 3
Recognise the importance of workplaces and education settings for generating community change in knowledge, attitudes and behaviours. In educational settings, implementation of nationally consistent curricula on consent, healthy relationships and domestic, family and sexual violence must be supported, for example by funding local violence prevention practitioners to deliver additional training and support to schools.
In workplaces, violence prevention and anti-violence initiatives are important to enable a safe work environment for all, as is implementation of specific policies that have been developed to support victims and survivors, such as paid domestic violence leave policy. The implementation of such initiatives requires ongoing monitoring and evaluation to determine uptake and effectiveness.
Enhance workforce competency, capability and collaboration across sectors
Recommendation 4
Increase core funding for frontline services, with built-in mechanisms to account for consumer price index (CPI) and award wage increases, as well as flexible support packages and emergency funds, which can be mobilised rapidly to frontline services following disasters. Funding cycles should be a minimum of three to five years to ensure frontline services are sustained. Funding packages must allow for flexibility and tailoring to local contexts, with resourcing to introduce responses that have been shown to be effective in similar contexts as well as capacity to implement new and context-specific responses.
Recommendation 5
Develop nationally accredited workforce training that can be tailored to health, police, magistrates and child welfare, which draws on the social entrapment model of violence, and trauma- and violence-informed care. This training should be co-designed by those with professional and lived experience and expertise.
Recommendation 6
Mandate Safe & Together training for those working in child protection and related services including police, magistrates, judicial registrars and expert witnesses. Expand Safe & Together training to be accessible to those working with families across health, education, legal and related services.
Recommendation 7
Fund targeted research, that is led by Aboriginal and Torres Strait Islander peoples and communities, to investigate and implement decolonising approaches to enhance workforce competency and capability.
Break intergenerational cycles of violence and trauma by better supporting children and young people
Recommendations to address intergenerational cycles of violence and trauma by better supporting children and young people are underpinned by recognition of children and young people as victims and survivors in their own right. This should be embedded in policy and practice guidelines and must be accompanied by greater investment in child-specific interventions.
Recommendation 8
Fund targeted research to establish evidence of effectiveness of therapeutic interventions for young people who are victims and survivors and those who use violence.
Recommendation 9
Fund targeted research to establish evidence of effectiveness of promising whole-of-family approaches, which bring a child-focused lens, with a view to supporting expanded implementation.
Recommendation 10
Re-evaluate the roles, responsibilities and training needs of Independent Children’s Lawyers, family report writers and other child court experts to ensure that there are independent and robust assessments of a child’s best interests in circumstances of family violence and other safety concerns. This will help to inform decision-makers and provide an effective voice for children as victims and survivors in their own right.
Bring forth innovative solutions
Recommendation 11
Build on innovative and promising digital and telehealth solutions that emerged as innovations during the pandemic to improve equitable access to services, including use of interpreters. Consider hybrid and hub models for digitally enabled service delivery to regional and remote locations to enable outreach options and strengthen collaboration with local services.
Recommendation 12
Invest in implementation of secure platforms for operational information sharing that were advanced during the pandemic. This must be accompanied by legislation, guidelines, training and practice resources to support information sharing.
Recommendation 13
Invest in therapeutic interventions that are focused on long-term health, healing and recovery, such as trauma-specific services. This requires adequate resourcing of therapeutic interventions delivered by health services including ACCOs. An important component of this are alternatives to criminal justice responses, such as therapeutic court interventions, as well as prison throughcare programs and family restoration programs.
Author contributions
In collaboration with the Voices project team, Dominiek Coates and Maria Koleth designed the survey and managed the ethics, recruitment and data collection.
Dominiek Coates had principal oversight for the Voices project and provided detailed feedback for the initial data coding and thematic analysis.
Maria Koleth processed the resulting survey data and undertook the descriptive analyses of respondent demographics and initial coding of the qualitative data.
Natasha Walker drafted the background literature review section of the report and contributed to drafting the methods and discussion of findings, under the supervision of Patricia Cullen. Natasha further assisted in formatting, proofreading and adding references to the report.
Patricia Cullen led the thematic analysis with input from the Voices project team and the project’s advisory committee. Patricia led the drafting of the report and contributed to all sections of the report.
References
Adams, A. E., Sullivan, C. M., Bybee, D., & Greeson, M. R. (2008). Development of the Scale of Economic Abuse. Violence Against Women, 14(5), 563–588. https://doi.org/10.1177/1077801208315529
Adams, A. E., Tolman, R. M., Bybee, D., Sullivan, C. M., & Kennedy, A. C. (2012). The impact of intimate partner violence on low-income women’s economic well-being: The mediating role of job stability. Violence Against Women, 18(12), 1345–1367. https://doi.org/10.1177/1077801212474294
Australian Bureau of Statistics. (2017a). Personal Safety Survey 2016 (ABS cat. no. 4906.0.). ABS.
Australian Bureau of Statistics. (2017b). Personal Safety Survey, Australia: User Guide, 2016. https://www.abs.gov.au/ausstats/[email protected]/Lookup/4906.0.55.003main+features42016#Persondemo
Australian Domestic and Family Violence Death Review Network, & Australia’s National Research Organisation for Women’s Safety. (2022). Australian Domestic and Family Violence Death Review Network data report: Intimate partner violence homicides 2010–2018 (2nd ed.; Research report 03/2022). ANROWS.
Australian Human Rights Commission. (2011). Report on the Review into the Treatment of Women at the Australian Defence Force Academy: Phase 1 of the Review into the Treatment of Women in the Australian Defence Force. AHRC.
Australian Human Rights Commission. (2022). Sexual harassment. https://humanrights.gov.au/quick-guide/12096
Australian Institute of Health and Welfare. (2018). Family, domestic and sexual violence in Australia 2018 (Cat. no. FDV 2.). AIHW.
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story 2019 (Cat. no. FDV 3.). AIHW.
Australian Institute of Health and Welfare. (2021a). Australia’s youth: COVID-19 and the impact on young people. https://www.aihw.gov.au/reports/children-youth/covid-19-and-young-people
Australian Institute of Health and Welfare. (2021b). Child protection in Australia 2019–20 (Cat. no. CWS 78.). AIHW.
Australian Institute of Health and Welfare. (2021c). Family, domestic and sexual violence service responses in the time of COVID-19 (Cat no FDV 8.). https://www.aihw.gov.au/reports/domestic-violence/family-domestic-and-sexual-violence-service-respon/summary
Australian Institute of Health and Welfare. (2021d). Specialist homelessness services annual report 2020–21. https://www.aihw.gov.au/reports/homelessness-services/specialist-homelessness-services-annual-report/contents/summary
Ayre, J., Lum On, M., Webster, K., Gourley, M., & Moon, L. (2016). Examination of the burden of disease of intimate partner violence against women in 2011: Final report (ANROWS Horizons, Issue 06/2016). ANROWS.
Bedi, G., & Goddard, C. (2007). Intimate partner violence: What are the impacts on children? Australian Psychologist, 42(1), 66–77.
Beeble, M. L., Bybee, D., & Sullivan, C. M. (2010). The impact of resource constraints on the psychological well-being of survivors of intimate partner violence over time. Journal of Community Psychology, 38(8), 943–959. https://doi.org/10.1002/jcop.20407
Bevis, M., Atkinson, J., McCarthy, L., & Sweet, M. (2020). Kungas’ trauma experiences and effects on behaviour in Central Australia (Research report, 03/2020). ANROWS.
Blagg, H., Bluett-Boyd, N., & Williams, E. (2015). Innovative models in addressing violence against Indigenous women: State of knowledge paper (ANROWS Horizons, Issue 08). ANROWS.
Blagg, H., Williams, E., Cummings, E., Hovane, V., Torres-Carne, M., & Karen, N. W. (2018). Innovative models in addressing violence against Indigenous women: Final report (ANROWS Horizons, Issue 01). ANROWS.
Bolarinwa, O. (2015). Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger Postgrad Med J, 22(4), 195–201. https://doi.org/10.4103/1117-1936.173959
Boxall, H., Doherty, L., Lawler, S., Franks, C., & Bricknell, S. (2022). The “Pathways to intimate partner homicide” project: Key stages and events in male-perpetrated intimate partner homicide in Australia (Research report, 04/2022). ANROWS.
Braaf, R., & Meyering, I. (2011). Seeking security: Promoting women’s economic wellbeing following domestic violence. Australian Domestic and Family Violence Clearinghouse.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
Braun, V., Clarke, V., Hayfield, N., & Terry, G. (2018). Thematic analysis. In P. Liamputtong (Ed.), Handbook of research methods in health social sciences (pp. 1–18). Springer Singapore.
Breckenridge, J., Cale, J., Hameed, S., McCaskie, L., & Tzoumakis, S. (2015). Implementation of domestic violence clauses: An employer’s perspective. Gendered Violence Research Network, UNSW.
Breckenridge, J., Chung, D., Spinney, A., & Zufferey, C. (2016). National mapping and meta-evaluation outlining key features of effective “safe at home” programs that enhance safety and prevent homelessness for women and their children who have experienced domestic and family violence: State of knowledge (ANROWS Landscape, Issue 05/2015). ANROWS.
Brown, L. (2022). Identity-first language. Autistic Self Advocacy Network. https://autisticadvocacy.org/about-asan/identity-first-language/
Brown, S., Gartland, D., Woolhouse, H., & Giallo, R. (2015). Translating evidence from the maternal health study to inform policy and practice (Policy Brief 2). Murdoch Children’s Research Institute.
Browne, A. J., Varcoe, C., Lavoie, J., Smye, V., Wong, S. T., Krause, M., Tu, D., Godwin, O., Khan, K., & Fridkin, A. (2017). Enhancing health care equity with Indigenous populations: Evidence-based strategies from an ethnographic study. BMC Health Services Research, 16(1), 544. https://doi.org/10.1186/s12913-016-1707-9
Browne, A. J., Varcoe, C. M., Wong, S. T., Smye, V. L., Lavoie, J., Littlejohn, D., Tu, D., Godwin, O., Krause, M., Khan, K. B., Fridkin, A., Rodney, P., O’Neil, J., & Lennox, S. (2012). Closing the health equity gap: Evidence-based strategies for primary health care organizations. International Journal for Equity in Health, 11(1), 59. https://doi.org/10.1186/1475-9276-11-59
Brownridge, D., Taillieu, T., Tyler, K., Tiwari, A., Ko Ling, C., & Santos, S. (2011). Pregnancy and intimate partner violence: Risk factors, severity, and health effects. Violence Against Women, 17(7), 858–881. https://doi.org/10.1177/1077801211412547
Bruton, C., & Tyson, D. (2017). Leaving violent men: A study of women’s experiences of separation in Victoria, Australia. Australian & New Zealand Journal of Criminology, 51(3), 339–354. https://doi.org/10.1177/0004865817746711
Bryman, A. (2001). Social research methods. Oxford University Press.
Bybee, D. I., & Sullivan, C. M. (2002). The process through which an advocacy intervention resulted in positive change for battered women over time. American Journal of Community Psychology, 30(1), 103–132. https://doi.org/10.1023/A:1014376202459
Campo, M. (2015). Children’s exposure to domestic and family violence: Key issues and responses (Paper no. 36). Australian Institute of Family Studies.
Campo, M., Kaspiew, R., Moore, S., & Tayton, S. (2014). Children affected by domestic and family violence: A review of domestic and family violence prevention, early intervention and response services. Australian Institute of Family Studies.
Canadian Institutes of Health Research. (2018). Science is better with sex and gender: Strategic plan 2018–2023. https://publications.gc.ca/collections/collection_2019/irsc-cihr/MR4-32-2018-eng.pdf
Carlson, B., Day, M., & Farrelly, T. (2021). What works? Exploring the literature on Aboriginal and Torres Strait Islander healing programs that respond to family violence (Research report, 01/2021). ANROWS.
Centres Against Sexual Assault Forum. (2014). Victorian Centres Against Sexual Assault standards of practice (2nd ed.). https://static1.squarespace.com/static/5fa0db2b7ce66d7cda3bbe00/t/5fb757dcd5e88918f42e32e0/1605851103790/NASASV_Standards_2nd_Edition_2015.pdf
Child Family Community Australia. (2014). Effects of child abuse and neglect for adult survivors [CFCA resource sheet]. Australian Institute of Family Studies. https://aifs.gov.au/cfca/publications/effects-child-abuse-and-neglect-adult-survivors
Clark, N. (2014). Perseverance, determination and resistance: An Indigenous intersectional-based policy analysis of violence in the lives of Indigenous girls. In H. O (Ed.), An intersectionality-based policy analysis framework (pp. 26). Institute for Intersectionality Research and Policy, Simon Fraser University.
Coker, A. L., Watkins, K. W., Smith, P. H., & Brandt, H. M. (2003). Social support reduces the impact of partner violence on health: Application of structural equation models. Preventive Medicine, 37(3), 259–267. https://doi.org/10.1016/S0091-7435(03)00122-1
Commonwealth of Australia. (2019). National Women’s Health Strategy 2020–2030. Department of Health.
Commonwealth of Australia. (2021). Inquiry into family, domestic and sexual violence: Report. House of Representatives Standing Committee on Social Policy and Legal Affairs.
Cortis, N., Blaxland, M., Breckenridge, J., valentine, k., Mahoney, N., Chung, D., Cordier, R., Chen, Y.-w., & Green, D. (2018). National survey of workers in the domestic, family and sexual violence sectors: Final report. Social Policy Research Centre (UNSW).
Cortis, N., & Bullen, J. (2015). Building effective policies and services to promote women’s economic security following domestic violence: State of knowledge (ANROWS Landscapes, Issue 11/2015). ANROWS.
Cortis, N., & Bullen, J. (2016). Domestic violence and women’s economic security: Building Australia’s capacity for prevention and redress: Key findings and future directions (ANROWS Compass, Issue 06/2016). ANROWS.
Council of Australian Governments. (2015). National Outcome Standards for Perpetrator Interventions. COAG.
Council of Australian Governments. (2016). Third Action Plan 2016–2019 of the National Plan to Reduce Violence against Women and their Children 2010–2022. Department of Social Services.
Council of Australian Governments. (2019). Fourth Action Plan: National Plan to Reduce Violence against Women and their Children 2010–2022. COAG.
Council of Australian Governments Advisory Panel. (2010). National Plan to Reduce Violence Against Women and their Children 2010-2022. Council of Australian Governments.
Crabtree, B. F., & Miller, W. L. (1992). Doing qualitative research: Research methods for primary care (Vol. 3). Sage Publications.
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241–1299. https://doi.org/10.2307/1229039
Crowne, S. S., Juon, H. S., Ensminger, M., Burrell, L., McFarlane, E., & Duggan, A. (2011). Concurrent and long-term impact of intimate partner violence on employment stability. Journel of Interpersonal Violence, 26(6), 1282–1304. https://doi.org/10.1177/0886260510368160
Cullen, P., Mackean, T., Walker, N., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., Worner, F., & Longbottom, M. (2021). Integrating trauma and violence informed care in primary health care settings for First Nations women experiencing violence: a systematic review. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838020985571
Cullen, P., Mackean, T., Worner, F., Wellington, C., Longbottom, H., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., & Longbottom, M. (2020). Trauma and violence informed care through decolonising interagency partnerships: A complexity case study of Waminda’s model of systemic decolonisation. International Journal of Environmental Research and Public Health, 17(20), 7363. https://doi.org/10.3390/ijerph17207363
Cullen, P., Stevenson, S., Baffsky, R., & Walker, N. (2021). A new model of care for women experiencing trauma from domestic, family and sexual violence: Co-design report. University of New South Wales. https://womenshealthcentre.com.au/wp-content/uploads/2021/11/WTRC-Report_F-digital.pdf
Day, A., Casey, S., Gerace, A., Oster, C., & O’Kane, D. (2018). The forgotten victims: Prisoner experience of victimisation and engagement with the criminal justice system (Issue 01/2018). ANROWS.
Day, S., Mason, R., Lagosky, S., & Rochon, P. A. (2016). Integrating and evaluating sex and gender in health research. Health Research Policy and Systems, 14(1), 75. https://doi.org/10.1186/s12961-016-0147-7
Decker, M., McCauley, H. L., Phuengsamran, D., Janyam, S., Seage, G. R. 3rd, & Silverman, J. G. (2010). Violence victimisation, sexual risk and sexually transmitted infection symptoms among female sex workers in Thailand. Sexually Transmitted Infections, 86(3), 236–240. http://dx.doi.org/10.1136/sti.2009.037846
Decker, M. R., Pearson, E., Illangasekare, S. L., Clark, E., & Sherman, S. G. (2013). Violence against women in sex work and hiv risk implications differ qualitatively by perpetrator. BMC Public Health, 13(1), 876. https://doi.org/10.1186/1471-2458-13-876
Department for Victorian Communities. (2021). Family violence workforce census. Victorian Government. https://www.vic.gov.au/family-violence-workforce-census
Department of Health. (2018). National Women’s Health Strategy 2020–2030. Australian Government.
Department of Social Services. (2021). Keeping women safe in their homes. https://www.dss.gov.au/women-programs-services-reducing-violence/keeping-women-safe-in-their-homes
Department of Social Services. (2022). Draft National Plan to End Violence against Women and Children 2022–2032. https://engage.dss.gov.au/draft-national-plan-to-end-violence-against-women-and-children-2022-2032/
Didi, A., Soldatic, K., Frohmader, C., & Dowse, L. (2016). Violence against women with disabilities: Is Australia meeting its human rights obligations? Australian Journal of Human Rights, 22(1), 159–177. https://doi.org/10.1080/1323-238X.2016.11882162
Diemer, K., Humphreys, C., & Crinall, K. (2017). Safe at home? Housing decisions for women leaving family violence. Australian Journal of Social Issues, 52(1), 32–47. https://doi.org/10.1002/ajs4.5
Dillon, G., Hussain, R., Loxton, D., & Rahman, S. (2013). Mental and physical health and intimate partner violence against women: A review of the literature. International Journal of Family Medicine, 2013, 1–15. https://doi.org/10.1155/2013/313909
Douglas, H., Tarrant, S., & Tolmie, J. (2021). Social entrapment evidence: Understanding its role in self-defence cases involving intimate partner violence. University of New South Wales Law Journal, 44(1).
https://doi.org/10.53637/VJII7190
Edwards, K. M., Sylaska, K. M., & Neal, A. M. (2015). Intimate partner violence among sexual minority populations: A critical review of the literature and agenda for future research. Psychology of Violence, 5(2), 112–121. https://doi.org/10.1037/a0038656
Ehrensaft, M., Cohen, P., Brown, J., Smailes, E., Chen, H., & Johnson, J. G. (2003). Intergenerational transmission of partner violence: A 20-year prospective study. J Consult Clin Psychol, 71(4), 741–753. https://doi.org/10.1037/0022-006X.71.4.741
Ellonen, N., Piispa, M., Peltonen, K., & Oranen, M. (2013). Exposure to parental violence and outcomes of child psychosocial adjustment. Violence Vict(1), 3–15. https://doi.org/10.1891/0886-6708.28.1.3
Evans, M., & Feder, G. (2016). Help-seeking amongst women survivors of domestic violence: A qualitative study of pathways towards formal and informal support. Health Expectations, 19(1), 62–73. https://doi.org/10.1111/hex.12330
Family Violence Act 2004 (Cth).
Ferrer-Perez, V. A., Bosch-Fiol, E., Ferreiro-Basurto, V., Delgado-Alvarez, C., & Sánchez-Prada, A. (2020). Comparing implicit and explicit attitudes toward intimate partner violence against women. Front Psychol, 11, 2147. https://doi.org/10.3389/fpsyg.2020
Fitz-Gibbon, K., Walklate, S., & Meyer, S. (2020). Criminalisation of coercive control: Research brief. Monash Gender and Family Violence Prevention Centre. https://arts.monash.edu/__data/assets/pdf_file/0019/1530343/rb-coercive-control.pdf
Flasch, P., Murray, C. E., & Crowe, A. (2015). Overcoming abuse: A phenomenological investigation of the journey to recovery from past intimate partner violence. Journal of Interpersonal Violence, 32(22), 3373–3401. https://doi.org/10.1177/0886260515599161
Flood, M., & Fergus, L. (2008). An assault on our future: The impact of violence on young people and their relationships. White Ribbon Foundation. http://www.ncdsv.org/images/WhiteRibbon_AssaultOnOurFutureImpactOfViolence
OnYoungPeopleAndTheirRelationships_ExecSumm.pdf
Gebicki, C., Meagher, A., & Flax, G. (2018). Everyone’s business: Fourth national survey on sexual harassment in Australian workplaces. Australian Human Rights Commission. https://humanrights.gov.au/our-work/sex-discrimination/publications/everyones-business-fourth-national-survey-sexual
Government of South Australia. (2022). Discussion paper: Implementation considerations should coercive control be criminalised in South Australia. Attorney-General’s Department, SA Government.
Government of Western Australia. (2020). Path to safety: Western Australia’s Strategy to Reduce Family and Domestic Violence 2020–2030. Government of Western Australia, Department of Communities.
Grace, K. T., & Anderson, J. C. (2018). Reproductive coercion: A systematic review. Trauma, Violence & Abuse, 19(4), 371–390. https://doi.org/10.1177/1524838016663935
Gracia, E., Rodriguez, C. M., Martín-Fernández, M., & Lila, M. (2017). Acceptability of family violence: Underlying ties between intimate partner violence and child abuse. Journal of Interpersonal Violence, 35(17–18), 3217–3236. https://doi.org/10.1177/0886260517707310
Gruber, J. E. (1998). The impact of male work environments and organizational policies on women’s experiences of sexual harassment. Gender & Society, 12(3), 301–320. https://doi.org/10.1177/0891243298012003004
Hamby, S., & Grych, J. (2013). The web of violence: Exploring connections among different forms of interpersonal violence and abuse (13th ed.). Springer.
Hegarty, K., Tarzia, L., Rees, S., Fooks, A., Forsdike, K., Woodlock, D., Simpson, L., McCormack, C., & Amanatidis, S. (2017). Women’s Input into a Trauma-informed systems model of care in Health settings (The WITH study): Final report (ANROWS Horizons 02/2017). ANROWS.
Heise, L. L., & Kotsadam, A. (2015). Cross-national and multilevel correlates of partner violence: An analysis of data from population-based surveys. Lancet Global Health, 3(6), e332–e340. https://doi.org/10.1016/S2214-109X(15)00013-3
Herrero, J., Rodríguez, F. J., & Torres, A. (2017). Acceptability of partner violence in 51 societies: The role of sexism and attitudes toward violence in social relationships. Violence Against Women, 23(3), 351–367. https://doi.org/10.1177/1077801216642870
Heywood, I., Sammut, D., & Bradbury-Jones, C. (2019). A qualitative exploration of “thrivership” among women who have experienced domestic violence and abuse: Development of a new model. BMC women’s health, 19(1), 106. https://doi.org/10.1186/s12905-019-0789-z
Hill, A., Bourne, A., McNair, R., Carman, M., & Lyons, A. (2020). Private Lives 3: The health and wellbeing of LGBTIQ people in Australia (ARCSHS Monograph Series No. 122). Australian Research Centre in Sex, Health and Society, La Trobe University. https://www.latrobe.edu.au/__data/assets/pdf_file/0009/1185885/Private-Lives-3.pdf
Hill, A. O., Lyons, A., Jones, J., McGowan, I., Carman, M., Parsons, M., Power, J., & Bourne, A. (2021). Writing Themselves In 4: The health and wellbeing of LGBTQA+ young people in Australia (Monograph Series Number 124). Australian Research Centre in Sex, Health and Society, La Trobe University. https://www.latrobe.edu.au/__data/assets/pdf_file/0010/1198945/Writing-Themselves-In-4-National-report.pdf
Hobfoll, S. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing conservation of resources theory. Applied Psychology, 50(3), 337–421. https://doi.org/10.1111/1464-0597.00062
Hobfoll, S., & Lilly, R. (1993). Resource conservation as a strategy for community psychology. Journal of Community Psychology, 21(2), 128–148. https://doi.org/10.1002/1520-6629(199304)21:2<128::AID-JCOP2290210206>3.0.CO;2-5
Humphreys, C. (2007). Domestic violence and child protection: challenging directions for practice (Issues paper 13). Australian Domestic & Family Violence Clearinghouse.
Humphreys, C. (2008). Problems in the system of mandatory reporting of children living with domestic violence. Journal of Family Studies, 14(2–3), 228–239. https://doi.org/10.5172/jfs.327.14.2-3.228
Jaeger, M. E., & Rosnow, R. L. (1988). Contextualism and its implications for psychological inquiry. British Journal of Psychology, 79(1), 63–75.
James, L., Brody, D., & Hamilton, Z. (2013). Risk factors for domestic violence during pregnancy: A meta-analytic review. Violence Vict, 28(3), 359–380. https://doi.org/10.1891/0886-6708.VV-D-12-00034
Joint Select Committee on Coercive Control. (2021). Coercive control in domestic relationships (Report 1/57). Parliament of NSW. https://nla.gov.au/nla.obj-2969950536/view
Justice Health & Forensic Mental Health Network. (2017). Network patient health survey report 2015. Justice Health & Forensic Mental Health Network. https://www.justicehealth.nsw.gov.au/publications/2015_NHPS_FINALREPORT.pdf
Kaufman, K., & Little, L. (2003). Defining the boundaries of child neglect: When does domestic violence equate with parental failure to protect? Journal of Interpersonal Violence, 18(4), 338–355. https://doi.org/10.1177/0886260502250834
Kiamanesh, P., & Hauge, M.-I. (2019). “We are not weak, we just experience domestic violence”—Immigrant women’s experiences of encounters with service providers as a result of domestic violence. Child & Family Social Work, 24(2), 301–308. https://doi.org/10.1111/cfs.12615
KPMG. (2016). The cost of violence against women and their children in Australia. Department of Social Services.
Kulkarni, M., Graham-Bermann, S., Rauch, S., & Seng, J. (2011). Witnessing versus experiencing direct violence in childhood as correlates of adulthood PTSD. Journal of Interpersonal Violence, 26(6), 1264–1281. https://doi.org/10.1177/0886260510368159
Langenderfer-Magruder, L., Whitfield, D. L., Walls, N. E., Kattari, S. K., & Ramos, D. (2016). Experiences of intimate partner violence and subsequent police reporting among lesbian, gay, bisexual, transgender, and queer adults in Colorado: Comparing rates of cisgender and transgender victimization. J Interpers Violence, 31(5), 855–871. https://doi.org/10.1177/0886260514556767
Langton, M., Smith, K., Eastman, T., O’Neill, L., Cheesman, E., & Rose, M. (2020). Improving family violence legal and support services for Aboriginal and Torres Strait Islander women (Issue 25). ANROWS.
Longbottom, M. A. (2019). Balwalwanga Bhulungs: We are strong women [Unpublished thesis]. Wollotuka Institute, University of Newcastle.
Marie Stopes. (2020). Hidden forces: A white paper on reproductive coercion in contexts of family and domestic violence (2nd ed.). https://www.mariestopes.org.au/wp-content/uploads/Hidden-Forces-Second-Edition-.pdf
Meyer, S. R., Lasater, M. E., & García-Moreno, C. (2020). Violence against older women: A systematic review of qualitative literature. PLOS One, 15(9), e0239560. https://doi.org/10.1371/journal.pone.0239560
Moe, A. M., & Bell, M. P. (2004). Abject economics: The effects of battering and violence on women’s work and employability. Violence Against Women, 10(1), 29–55. https://doi.org/10.1177/1077801203256016
Muldoon, K. A., Deering, K. N., Feng, C. X., Shoveller, J. A., & Shannon, K. (2015). Sexual relationship power and intimate partner violence among sex workers with non-commercial intimate partners in a Canadian setting. AIDS Care, 27(4), 512–519. https://doi.org/10.1080/09540121.2014.978732
Myhill, A., & Hohl, K. (2016). The golden thread: Coercive control and risk assessment for domestic violence. Journal of Interpersonal Violence, 34, 4477–4497. https://doi.org/10.1177/0886260516675464
Nancarrow, H. (2010). Restorative justice for domestic family violence: hopes and fears of Indigenous and Non-Indigenous Australian women. In J. Ptacek (Ed.), Restorative justice and violence against women (pp. 123–149). Oxford University Press.
National Association of Services Against Sexual Violence. (2021). The standards of practice manual for services against sexual violence (3rd edition). https://static1.squarespace.com/static/5fa0db2b7ce66d7cda3bbe00/t/613583e1573d0042b238fd9b/1630897132183/Standards+of+Practice+Manual+for+Services+Against+
Sexual+Violence+3rd+Edition.PDF
Neave, M., Faulkner, P., & Nicholson, T. (2016). Royal Commission into Family Violence: Summary and recommendations (Parl Paper No 132). Victorian Government.
NSW Government. (2019). The case for change: Integrated prevention and response to violence, abuse and neglect in NSW Health. NSW Ministry of Health. https://www.health.nsw.gov.au/parvan/Publications/case-for-change.pdf
NSW Health. (2014). NSW Health workforce domestic violence survey. NSW Government. https://www.health.nsw.gov.au/parvan/DV/Documents/dv-workforce-survey-report.pdf
NSW Ministry of Health. (2019). The case for change: Integrated prevention and response to violence, abuse and neglect in NSW Health. NSW Government. https://www.health.nsw.gov.au/parvan/Publications/case-for-change.pdf
Olsen, A., & Lovett, R. (2016). Existing knowledge, practice and responses to violence against women in Australian Indigenous communities: State of knowledge paper (Issue 2/2016). ANROWS.
Oram, S., Fisher, H. L., Minnis, H., Seedat, S., Walby, S., Hegarty, K., Rouf, K., Angénieux, C., Callard, F., Chandra, P. S., Fazel, S., Garcia-Moreno, C., Henderson, M., Howarth, E., MacMillan, H. L., Murray, L. K., Othman, S., Robotham, D., Rondon, M. B., Sweeney, A., Taggart, D., & Howard, L. M. (2022). The Lancet Psychiatry Commission on Intimate Partner Violence and Mental Health: Advancing mental health services, research, and policy. Lancet Psychiatry, 9(6), 487–524. https://doi.org/10.1016/S2215-0366(22)00008-6
Our Watch. (2018). Changing the picture: A national resource to support the prevention of violence against Aboriginal and Torres Strait Islander women and their children. https://apo.org.au/sites/default/files/resource-files/2018-07/apo-nid182621.pdf
Our Watch. (2022a). The issue. https://www.ourwatch.org.au/the-issue/
Our Watch. (2022b). The power of the workplace. https://workplace.ourwatch.org.au/why-do-this-work/the-power-of-the-workplace/
Our Watch. (2022c). Understanding sexual harassment in workplaces. https://workplace.ourwatch.org.au/why-do-this-work/understanding-sexual-harassment-in-workplaces/#the-gendered-drivers-of-violence
Owen, S., & Carrington, K. (2015). Domestic violence service provision and the architecture of rural life: An Australian case study. Journal of Rural Studies, 39, 229–238. https://doi.org/10.1016/j.jrurstud.2014.11.004
Pathak, N., Dhairyawan, R., & Tariq, S. (2019). The experience of intimate partner violence among older women: A narrative review. Maturitas, 121, 63–75. https://doi.org/10.1016/j.maturitas.2018.12.011
Peckover, S. (2003). “I could have just done with a little more help”: An analysis of women’s help-seeking from health visitors in the context of domestic violence. Health & Social Care in the Community, 11(3), 275–282. https://doi.org/10.1046/j.1365-2524.2003.00423.x
People with Disability of Australia. (2019). What do I say? A guide to language about disability. https://pwd.org.au/wp-content/uploads/2019/08/PWDA_LanguageGuide_A5_WEB.pdf
Porter, A., Deslandes, A. L., McKinnon, C., & Longbottom, M. (2021). Women’s police stations in Australia: Would they work for “all” women? The Conversation. https://theconversation.com/womens-police-stations-in-australia-would-they-work-for-all-women-165873
Ptacek, J. (1999). Battered women in the courtroom: The power of judicial responses. Northeastern University Press.
Richards, K. (2011). Children’s exposure to domestic violence in Australia (no. 419). Australian Institute of Criminology.
Riger, S., Staggs, S. L., & Schewe, P. (2004). Intimate partner violence as an obstacle to employment among mothers affected by welfare reform. Journal of Social Issues, 60(4), 801–818. https://doi.org/10.1111/j.0022-4537.2004.00387.x
Roach, K. (1999). Four models of the criminal process. Journal of Criminal Law and Criminology, 89(671). https://doi.org/10.2307/1144140
Roberts, A. L., Gilman, S. E., Fitzmaurice, G., Decker, M. R., & Koenen, K. C. (2010). Witness of intimate partner violence in childhood and perpetration of intimate partner violence in adulthood. Epidemiology (Cambridge, Mass.), 21(6), 809–818. https://doi.org/10.1097/EDE.0b013e3181f39f03
Robinson, L., & Spilsbury, K. (2008). Systematic review of the perceptions and experiences of accessing health services by adult victims of domestic violence. Health & Social Care in the Community, 16(1), 16–30. https://doi.org/10.1111/j.1365-2524.2007.00721.x
Safe & Together Institute. (2020). Safe & Together model principles & critical components. https://safeandtogetherinstitute.com/safe-together/safe-together-overview/assumptions-principles-critical-components/
Salter, M. (2013). Multi-perpetrator domestic violence. Trauma, Violence, & Abuse, 15(2), 102–112. https://doi.org/10.1177/1524838013511542
Salter, M., Conroy, E., Dragiewicz, M., Burke, J., Ussher, J., Middleton, W., Vilenica, S., Martin Monzon, B., & Noack-Lundberg, K. (2020). “A deep wound under my heart”: Constructions of complex trauma and implications for women’s wellbeing and safety from violence (Research report, 12/2020). ANROWS. https://www.anrows.org.au/publication/a-deep-wound-under-my-heart-constructions-of-complex-trauma-and-implications-for-womens-wellbeing-and-safety-from-violence/
Saunders, S., & Easteal Am, P. (2013). The nature, pervasiveness and manifestations of sexual harassment in rural Australia: Does “masculinity” of workplace make a difference? Women’s Studies International Forum, 40, 121–131. https://doi.org/10.1016/j.wsif.2013.05.013
Schmidt, I. D. (2014). Addressing PTSD in low-income victims of intimate partner violence: Moving toward a comprehensive intervention. Soc Work, 59(3), 253–260.
Seib, C., Fischer, J., & Najman, J. M. (2009). The health of female sex workers from three industry sectors in Queensland, Australia. Social Science & Medicine, 68(3), 473–478. https://doi.org/10.1016/j.socscimed.2008.10.024
Shannon, K., Kerr, T., Bright, V., Gibson, K., & Tyndall, M. W. (2008). Drug sharing with clients as a risk marker for increased violence and sexual and drug-related harms among survival sex workers. AIDS Care, 20(2), 228–234. https://doi.org/10.1080/09540120701561270
Shannon, K., Kerr, T., Strathdee, S. A., Shoveller, J., Montaner, J. S., & Tyndall, M. W. (2009). Prevalence and structural correlates of gender based violence among a prospective cohort of female sex workers. BMJ, 339, b2939. https://doi.org/10.1136/bmj.b2939
Sharp-Jeffs, N., Kelly, L., & Klein, R. (2018). Long journeys toward freedom: The relationship between coercive control and space for action-measurement and emerging evidence. Violence Against Women, 24(2), 163–185. https://doi.org/10.1177/107780121668619
Sinko, L., James, R., & Hughesdon, K. (2021). Healing after gender-based violence: A qualitative metasynthesis using meta-ethnography. Trauma, Violence, & Abuse, 1524838021991305. https://doi.org/10.1177/1524838021991305
Smyth, C., Cullen, P., Breckenridge, J., Cortis, N., & valentine, k. (2021). COVID-19 lockdowns, intimate partner violence and coercive control. The Australian Journal of Social Issues. https://doi.org/10.1002/ajs4.162
Staggs, S. L., & Riger, S. (2005). Effects of intimate partner violence on low-income women’s health and employment. American Journal of Community Psychology, 36(1), 133–145. https://doi.org/10.1007/s10464-005-6238-1
Stark, E. (2007). Coercive control: How men entrap women in personal life. Oxford University Press.
Stark, E., & Hester, M. (2019). Coercive control: Update and review. Violence Against Women, 25(1), 81–104. https://doi.org/10.1177/1077801218816191
Stathopoulos, M., Quadara, A., Fileborn, B., & Clark, H. (2012). Addressing women’s victimisation histories in custodial settings (Issue no. 13). Australian Institute of Family Studies. https://aifs.gov.au/sites/default/files/publication-documents/i13_0.pdf
Sullivan, C. M., & Bybee, D. I. (1999). Reducing violence using community-based advocacy for women with abusive partners. Journal of Consulting and Clinical Psychology, 67(1), 43–53. https://doi.org/10.1037/0022-006X.67.1.43
Sullivan, C. M., Bybee, D. I., & Allen, N. E. (2002). Findings from a community-based program for battered women and their children. Journal of Interpersonal Violence, 17(9), 915–936. https://doi.org/10.1177/0886260502017009001
Szalacha, L. A., Hughes, T. L., McNair, R., & Loxton, D. (2017). Mental health, sexual identity, and interpersonal violence: Findings from the Australian Longitudinal Women’s Health Study. BMC Women’s Health, 17(1), 94. https://doi.org/10.1186/s12905-017-0452-5
The Equality Institute. (2017). Preventing and responding to family violence: Taking an intersectional approach to address violence in Australian communities. https://apo.org.au/sites/default/files/resource-files/2017-10/apo-nid185301.pdf
Tolman, R. M., & Wang, H. C. (2005). Domestic violence and women’s employment: Fixed effects models of three waves of women’s employment study data. Am J Community Psychol, 36(1–2), 147–158. https://doi.org/10.1007/s10464-005-6239-0
Tolmie, J., Smith, R., Short, J., Wilson, D., & Sach, J. (2018). Social entrapment: A realistic understanding of the criminal offending of primary victims of intimate partner violence. New Zealand Law Review, 2018, 181.
Trevillion, K., Hughes, B., Feder, G., Borschmann, R., Oram, S., & Howard, L. M. (2014). Disclosure of domestic violence in mental health settings: A qualitative meta-synthesis. International Review of Psychiatry, 26(4), 430–444. https://doi.org/10.3109/09540261.2014.924095
VACCA, ThinkPlace, & Family Safety Victoria. (2019). Nargneit Birrang: Aboriginal holistic healing framework for family violence. State of Victoria.
Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Quiazon, R., Block, K., & Warr, D. (2016). Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: The ASPIRE project (ANROWS Landscapes, Issue 12/2015). ANROWS.
Victoria Department of Health and Human Services. (2018). Dhelk Dja: Safe our way – Strong culture, strong peoples, strong families. Department of Health and Human Services.
Victoria Department of Premier and Cabinent. (2019). Victorian family violence data collection framework. State Government of Victoria.
Victorian Indigenous Taskforce. (2003). Victorian Indigenous Family Violence Task Force: Final report. Aboriginal Affairs Department for Victorian Communities. https://www.vgls.vic.gov.au/client/en_AU/search/asset/1162179/0
Walker, H., Freud, J., Ellis, R., Fraine, S., & Wilson, L. (2019). The prevalence of sexual revictimization: A meta-analytic review. Trauma, Violence, & Abuse, 20(1), 67–80. https://doi.org/10.1177/1524838017692364
Walker, N., Beek, K., Chen, H., Shang, J., Stevenson, S., Williams, K., Herzog, H., Ahmed, J., & Cullen, P. (2020). The experiences of persistent pain among women with a history of intimate partner violence: A systematic review. Trauma, Violence, & Abuse, 1524838020957989. https://doi.org/10.1177/1524838020957989
Walker, N., Mackean, T., Longbottom, M., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., Redfern, J., & Cullen, P. (2020). Responses to the primary health care needs of Aboriginal and Torres Strait Islander women experiencing violence: A scoping review of policy and practice guidelines. Health Promotion Journal of Australia. https://doi.org/10.1002/hpja.417
Wangmann, J. (2020). Coercive control as the context for intimate partner violence: The challenge for the legal system. In M. McMahon & P. McGorrery (Eds.), Criminalising coercive control (pp. 219–242). Springer.
Webster, K. (2016). A preventable burden: Measuring and addressing the prevalence and health impacts of intimate partner violence in Australian women: Key findings and future directions (ANROWS Compass, 07/2016). ANROWS.
Webster, K., Diemer, K., Honey, N., Mannix, S., Mickle, J., Morgan, J., Parkes, A., Politoff, V., Powell, A., Stubbs, J., & Ward, A. (2018). Australians’ attitudes to violence against women and gender equality: Findings from the 2017 National Community Attitudes towards Violence against Women Survey (NCAS) (Research report, 03/2018). ANROWS.
Willis, M. (2011). Non-disclosure of violence in Indigenous communities (Trends & Issues in Crime and Criminal Justice, no. 405). Australian Institute of Criminology.
Willoughby, M., Spittal, M. J., Borschmann, R., Tibble, H., & Kinner, S. A. (2020). Violence-related deaths among people released from prison: A data linkage study. Journal of Interpersonal Violence, 36(23–24), NP13229–NP13253. https://doi.org/10.1177/0886260520905546
Women’s Safety and Justice Taskforce. (2021). Options for legislating against coercive control and the creation of a standalone domestic violence offence: Discussion paper 1. https://www.womenstaskforce.qld.gov.au/__data/assets/pdf_file/0004/684913/WSJT-Discussion-paper-1-Options-for-legislating-against-coercive-control-and-the-creation-of-a-standaone-domestic-violence-offence.pdf
Workplace Gender Equality Agency. (2022a). Australia’s gender equality scorecard. https://www.wgea.gov.au/publications/australias-gender-equality-scorecard
Workplace Gender Equality Agency. (2022b). The gender pay gap. https://www.wgea.gov.au/the-gender-pay-gap
World Health Organization. (2014). Global status report on violence prevention. https://www.who.int/publications/i/item/9789241564793
World Health Organization. (2018). Elder abuse: Fact sheet. http://www.who.int/news-room/fact-sheets/detail/elder-abuse
World Health Organization. (2021). Violence against women. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
Appendix A:
Voices project advisory committee members
Dr Hayley Boxall (Australian Institute of Criminology)
The Healing Foundation
Heather Clarke (National Association of Services against Sexual Violence)
On the Line Australia
Louise Gottardo (Queensland Department of Justice and Attorney-General)
Emily Grant (WEAVERs panel)
Angela Hampton (Central Australian Aboriginal Congress)
ACON’s Sexual, Domestic and Family Violence Team
Sally Mills (Australian Institute of Health and Welfare)
Dr Astrid Perry (Settlement Services International)
Safiyah Salim (WA Health)
Officers from the Attorney-General’s Department
WA Department of Communities, Office for Prevention of Family and Domestic Violence
Amanda Wallace (WEAVERs panel)
Jacqui Watt (No to Violence)
Endnotes
- The social entrapment model avoids victim blaming by recognising intersecting structural and social determinants that underpin the perpetrator’s ability to enact violence and the safety responses available to the victim (Douglas et al., 2021; Ptacek, 1999). Back to reference ↑
- Safe & Together is based on three principles that prioritise the safety and wellbeing of children: keep children safe and together with non-offending parents; partner with the perpetrator and hold them accountable; intervene with the perpetrator to reduce risk and harm to children (Safe & Together Institute, 2020). Back to reference ↑
- Acknowledging the importance of preventing and responding to child sexual violence, the Australian Government has also established the National Office for Children’s Safety and provided initial funding for the National Centre for Action on Child Sexual Abuse. Back to reference ↑
Dr Patricia Cullen
Research Fellow, University of New South Wales
Natasha Walker
Research Associate, University of New South Wales
Dr Maria Koleth
ANROWS
Associate Professor Dominiek Coates
ANROWS
RESEARCH REPORT
ISSUE 21 | DECEMBER 2022
ANROWS acknowledgement
This material was produced with funding from the Australian Government Department of Social Services. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from the government, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government Department of Social Services.
Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we live and work. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and emerging. We value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with First Nations peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2022
![]()
With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
ISBN: 978-1-922645-58-6 (paperback)
ISBN: 978-1-922645-57-9 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project 4AP.8 “Transforming responses to intimate partner and sexual violence: Listening to the voices of victims, perpetrators and services”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Outcome 4 – Services meet the needs of women and their children experiencing violence, and National Outcome 6 – Perpetrators stop their violence and are held to account.
Suggested citation:
Cullen, P., Walker, N., Koleth, M., & Coates, D. (2022). Voices from the frontline: Qualitative perspectives of the workforce on transforming responses to domestic, family and sexual violence (Research report, 21/2022). ANROWS.
UNSW Sydney
High St
Kensington NSW 2052
Author acknowledgement
We acknowledge the Gadigal and Bedegal people of the Eora nation on which ANROWS and UNSW stand. We sincerely thank the workforce for sharing their thoughtful and detailed perspectives. We are grateful to the “Voices” advisory committee for their generous support and insights. We recognise the contributions of the “Voices” project team, with immense thanks to Kelsey Hegarty, Laura Tarzia, Matt Addison and Mandy McKenzie for their support and collegiality, and to Lauren Hamilton and Cassandra Dawes for guidance and leadership. We also thank Sally Nathan for her advice on qualitative methodology. We wish to acknowledge everyone impacted by domestic, family and sexual violence and hope that this report contributes to better outcomes for us all.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76
Definitions and concepts
| Concept | Definition |
|---|---|
| Coercive control | Coercive control is characterised by ongoing patterns of behaviours enacted with the intention of gaining control and power over victims and survivors of violence and abuse, including physical, sexual, psychological, emotional and/or financial abuse (Myhill & Hohl, 2016; Stark, 2007). It is nuanced and evolves and/or escalates over time (Stark & Hester, 2019), such that it is cumulative, insidious and sometimes hard to recognise as abuse (Stark, 2007). A classic feature of coercive control is a loss of sense of self, perception of reality and freedom for victims and survivors (Stark, 2007). A key tactic of perpetrators of coercive control is using aspects of victims’ and survivors’ identities that are discriminated against or oppressed, such as their cultural identity or ethnicity, to assert power and control (Sharp-Jeffs et al., 2018; Smyth et al., 2021). Whether coercive control should be criminalised is debated (Stark |
| Person with disability and disabled person | When referring to people with disability or disabled people in Australia, identity-first or person-first language can be used (People with Disability of Australia, 2019). Ultimately the choice of language should be led by the person with disability or disabled person, and respected and affirmed (People with Disability of Australia, 2019). Using person-first language is seen by some as way of ensuring disability is not unnecessarily focused on or used to dehumanise and justify violence (People with Disability of Australia, 2019). However, identity-first language is preferred by some who view their disability as an inherent part of their identity (People with Disability of Australia, 2019). In the Deaf and Autistic communities, identity-first language is preferred because it also represents a connection to a wider cultural group (Brown, 2022; People with Disability of Australia, 2019). Terms that are not supported by disability |
| Domestic violence | Domestic violence is violence perpetrated against a person by their current or former intimate partner. A key feature of domestic violence is establishing power and control over a partner through ongoing patterns of behaviour that create fear (Council of Australian Governments Advisory Panel, 2010). Behaviour can be criminal or non-criminal and includes physical and sexual violence as well as emotional and psychological abuse, which can include controlling finances, isolating from friends and family, humiliation, threatening children or pets, and threatening injury or death (Council of Australian Governments Advisory Panel, 2010). |
| Family violence | Family violence is a broad term that includes multiple forms of violence perpetrated by family members (Council of Australian Governments Advisory Panel, 2010). The wider scope of family violence includes violence perpetrated by extended family, communities and kinship networks, and as such can be the preferred terminology for violence experienced by Aboriginal and Torres Strait Islander women or within Aboriginal and Torres Strait Islander communities (Council of Australian Governments Advisory Panel, 2010; Victorian Indigenous Taskforce, 2003). |
| Gender inequality | Gender inequality is a social construct that describes unequal power dynamics, distribution of resources and access to opportunities between men and women (Our Watch, 2022a). As a result of gender inequality, men’s and women’s voices, ideas and work are not given equal value by society (Our Watch, 2022a). Gender inequality is a key driver of domestic, family and sexual violence in terms of reinforcing hierarchical gender stereotypes, excusing violence, justifying controlling male behaviour, and celebrating aggression and dominance as expressions of masculinity (Our Watch, 2022a). |
| Gender pay gap | The gender pay gap represents the difference between the average earnings of men and women (Workplace Gender Equality Agency, 2022b). It reflects the disadvantaged position of women in the workforce compared to men. This is distinct from unequal pay for the same or comparable work, which is a criminal offence. In 2020–21 in Australia, women earned $25,800 less than men and the pay gap widened for 37 per cent of employers (Workplace Gender Equality Agency, 2022a). Over a lifetime, compared to men, women will earn less and accumulate less superannuation, are less likely to be hired in senior roles and are ultimately more likely to live in poverty (Workplace Gender Equality Agency, 2022b). Despite women making up 50 per cent of the workforce, they are less than 20 per cent of CEOs (Workplace Gender Equality Agency, 2022a). Driving the gender pay gap are social and economic factors such as hiring and pay discrimination and bias, lower |
| Intersectionality | Intersectionality represents the additional burden of discrimination faced by people because of their intersecting social identities, such as age, sexuality, gender, ethnicity and cultural background, disability, religion, and migration and refugee status (Crenshaw, 1991; Victoria Department of Premier and Cabinent, 2019). The term was originally defined by Kimberlé Crenshaw in her discussion of the intersecting burdens of racism and sexism faced by Black women and violence as a manifestation of this burden (Crenshaw, 1991). Viewed through the lens of intersectionality, people who experience intersecting axes of social oppression are at increased risk of experiencing violence and/or more severe or frequent violence, as well as being at increased risk of experiencing discrimination and disregard from services and systems of support (The Equality Institute, 2017). Thereby, service responses and interventions for domestic, family and |
| Reproductive coercion | Reproductive coercion is the deliberate abuse of power to remove an individual’s autonomy over their reproductive health (Grace & Anderson, 2018; Marie Stopes, 2020). It can be perpetrated at an interpersonal level – directed specifically at an individual – or at a structural level where social, cultural, economic, legal and political systems enable it (Marie Stopes, 2020). Examples of interpersonal reproductive coercion include sabotaging contraception, pressuring someone into or controlling the outcome of a pregnancy, and/or non-consensual sterilisation. Examples of structural reproductive coercion include government policies and legislation, workplace policies and/or practices, and access to healthcare. |
| Sex and gender | Sex and gender are often used interchangeably (Canadian Institutes of Health Research, 2018). This is despite sex referring to biological attributes and gender referring to socially constructed roles, behaviours, expressions and identities (Canadian Institutes of Health Research, 2018). Sex can be characterised as female, male or intersex and is determined at birth. Comparably, gender is diverse and fluid and can change multiple times in a lifetime (Canadian Institutes of Health Research, 2018). Gender reflects the identity an individual chooses but also societal pressures and norms (Canadian Institutes of Health Research, 2018). It is important that the impact of sex and gender in experiences of violence are better understood as violence is highly gendered (Day et al., 2016). It has been established that cisgender women are more likely to experience violence than cisgender men and that transgender women are at greater risk of |
| Sexual violence | Sexual violence is the use of coercion to obtain or attempt to obtain any sexual act or act that is directed against an individual’s sexuality (World Health Organization, 2021). It can be perpetrated by a stranger or someone known to the victim and survivor (World Health Organization, 2021). It includes rape as well as other forms of assault, such as unwanted sexual touching, sexual assault, sexual assault with implements, being forced to engage in pornography or prostitution, and being forced to watch pornography or have sex with friends of the perpetrator (Council of Australian Governments Advisory Panel, 2010). |
Acronyms
| Acronym | Definition |
|---|---|
| ABS | Australian Bureau of Statistics |
| ACCO | Aboriginal community-controlled organisation |
| ACCHO | Aboriginal community-controlled health organisation |
| AVO | Apprehended violence order |
| ANROWS | Australia’s National Research Organisation for Women’s Safety |
| AUSLAN | Australian sign language |
| CASA | Centres Against Sexual Assault |
| CBT | Cognitive behavioural therapy |
| COAG | Council of Australian Governments |
| CPI | Consumer price index |
| GP | General practitioner |
| LGBTQ+ | Lesbian, gay, bisexual, transgender, queer and questioning |
| MBCP | Men’s behaviour change program |
| MARAM | Multi-Agency Risk Assessment and Management framework |
| NCAS | National Community Attitudes towards Violence against Women Survey |
| NDIS | National Disability Insurance Scheme |
| NFP | Not-for-profit |
| NGO | Non-government organisation |
| PSS | Personal Safety Survey |
| WDVCAS | Women’s Domestic Violence Court Advocacy Service |
Executive summary
Background
This report presents the findings from a national survey of the workforce (service providers, managers and researchers) in the domestic, family and sexual violence sector. The survey is part of a larger national project investigating the perspectives of people with lived experience and expertise on responses to domestic, family and sexual violence in Australia, investigating “what works, what might work and what doesn’t work”. It aligns with the intended outcomes of the Commonwealth Government’s National Plan to Reduce Violence Against Women and their Children 2010–2022 (Council of Australian Governments Advisory Panel, 2010).
Aim and objectives
The overarching aim of the larger project is to develop recommendations for service and system improvements to better respond to victims and survivors, including children and young people, and perpetrators of domestic, family and sexual violence. The focus of this report is to provide insight into the workforce’s perspectives on the effectiveness and appropriateness of existing interventions and responses – in particular, what is required for successful implementation and sustainability of responses and interventions.
Method
The online survey was developed in consultation with the project’s advisory committee (see Appendix A). The survey consisted of two sections: respondent demographics and career information, and existing responses or interventions for victims and survivors, children and young people and/or perpetrators of domestic, family and sexual violence. It was distributed among expert stakeholders and their networks via email, social media and newsletter advertising and was open from November 2020 to January 2021. The survey received 199 responses, which is a response rate of 30 per cent based on direct email invitations. One hundred and four were excluded because they did not provide substantive responses beyond demographics. A total of 95 respondents were included for analysis.
The majority of respondents identified as female (n=86, 91%). Respondents were drawn from all states and territories, however most worked in Victoria (n=31, 33%), Western Australia (n=16, 17%) and New South Wales (n=15, 16%). The majority were practitioners (n=60, 63%), while fewer were service designers or managers (n=21, 22%) and researchers (n=14, 15%).
Ethics approval was granted by the University of Melbourne Human Research Ethics Committee.
Key findings
The key findings are first presented in accordance with the six outcomes from the National Plan (Council of Australian Governments Advisory Panel, 2010), namely:
- Communities are safe and free from violence
- Relationships are respectful
- Aboriginal and Torres Strait Islander communities are strengthened
- Services meet the needs of women and children experiencing violence
- Justice responses are effective
- Perpetrators stop their violence and are held to account.
Across these outcomes, we describe workforce perceptions of contextual factors that inform the perceived effectiveness and appropriateness of interventions and responses. We also present priorities and opportunities identified by the workforce as important for future directions.
To encapsulate workforce perceptions on what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators, we generated five themes:
- addressing upstream determinants of domestic, family and sexual violence
- reactivity and inequity in responses harms victims and survivors
- changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
- enabling choice and the right to self-determination
- power of connection, collective healing and compassion.
Addressing upstream determinants of domestic, family and sexual violence
This theme speaks to the need for greater investment in addressing upstream determinants of domestic, family and sexual violence. This means addressing structural barriers that create and sustain multiple and intersecting forms of inequality, which are root causes of violence in our relationships, families, schools, workplaces and communities. The workforce identified key social determinants that require an upstream approach, with the primary ones being poverty, safe and affordable housing, and equal participation in the workforce.
Much consideration was given to gender inequality and the intersections with other forms of discrimination and oppression. Issues related to gender inequality and intersectionality permeated the data, along with concern more broadly for how considerations of intersectionality have not been embedded within policy and assertions that this must change as we shape future directions. Given the complex intersections, it is imperative that we respond using a public health approach, through implementation of health promotion strategies to address upstream determinants and provide equitable and enabling authorising environments.
Reactivity and inequity in responses harms victims and survivors
This theme reflects respondents’ views that systemic changes across the full spectrum of prevention, early intervention, response and recovery are needed. The system is set up to be reactive to incidents of violence, with less resourcing and capability for early intervention and prevention. Respondents identified issues of traumatisation, re-traumatisation and ineffective responses that can harm victims and survivors. These systemic issues also reflect inadequate responses and lack of services for perpetrators, which ultimately increase harm and risk for victims and survivors. These systemic issues are closely related to inadequate resourcing of services, with narrow eligibility criteria and rigid key performance indicators that are determined by funders and do not reflect community need.
Respondents indicated the need for a trauma- and violence-informed system that considers the intersecting experiences of oppression, power and privilege. Within trauma- and violence-informed care, a decolonisation approach is integral to ensuring that across the workforce there is a shared language and understanding of colonisation and the ways in which this continues to impact our society and social care systems. Despite cultural competency training being delivered in almost all workplaces, respondents indicated that this has had limited structural impact on the capability of the workforce to deliver culturally safe services for and with Aboriginal and Torres Strait Islander peoples. To address this shortcoming, we must recognise that current frameworks and approaches are embedded within colonising structures that continue to perpetrate harm for Aboriginal and Torres Strait Islander peoples and communities. Promising approaches have been developed and
implemented by Aboriginal community-controlled organisations (ACCOs), which are typically informed by and relevant to the local context.
Changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
This theme amalgamates respondents’ views that knowledge and cultural shifts are required to better conceptualise domestic, family and sexual violence, so that our understandings consider the intersection of violence within the broader context of structural and social determinants. Deeply entrenched systemic biases are underpinned by victim blaming, which results in responses and outcomes that do not adequately hold perpetrators to account and can further victimise and traumatise victims and survivors. Respondents considered these issues in light of debates around coercive control, as well as in the contexts of young people who use violence and child protection frameworks.
An alternative model proposed by respondents was the “social entrapment” model, which avoids victim blaming and has potential to promote holistic responses that better meet the needs of victims and survivors.[1] In terms of service responses that redress misconceptions and misattribution of blame, several respondents identified a child-focused model, such as the Safe & Together model, as promising.[2]
Enabling choice and the right to self-determination
This theme draws on assertions within the previous three themes that systemic biases, inequities and victim blaming constrain choice and resourcefulness that are essential for victims and survivors. Indeed, respondents assert that the systems that are intended to enable safety and agency can entrench victims’ and survivors’ isolation, mistrust and helplessness.
Respondents emphasised how critical choice and self-determination are for victims and survivors. Importantly, respondents asserted that these can be further constrained for those for whom mainstream services do not adequately meet needs for cultural safety, inclusion and accessibility. While resourcing is an issue that constrains choice, respondents also pointed to widespread inconsistencies in access to supports that stem from limited and inconsistent access to appropriate information about rights and options. Respondents attributed this to shortcomings in workforce capability and knowledge, and this also reflects the need for broader systemic shifts toward trauma- and violence-informed responses to promote choice, dignity and agency.
Power of connection, collective healing and compassion
Respondents emphasised that while there are systemic issues that can be powerful in enacting and compounding victims’ and survivors’ experiences of trauma, there are also systemic strengths that are powerful in generating healing and recovery. Fundamental to recovery and healing are our shared experiences, which bring opportunities for connection and compassion. Building therapeutic relationships is a key aspect of healing from violence, and one of the workforce’s main strengths lies in its relational capacity, with many members highly skilled in compassionate and trauma- and violence-informed responses.
The workforce pointed to innovative and promising solutions, particularly in terms of moving beyond crisis interventions to embrace the full spectrum of prevention, early intervention and recovery. Supporting the healing and recovery of victims and survivors, children and young people and people who use violence was also identified as a key component of violence prevention and important for averting intergenerational trauma.
Conclusion
This report presents findings from a national survey of 95 service providers and researchers across the domestic, family and sexual violence workforce. Respondents identified key systemic issues around resourcing, capability and inequitable policy. These shortcomings drive ineffective responses, constrain interventions and contribute to harm for victims and survivors and children and young people. Many of these effects were attributed to inherent reactivity across the system and dominant understandings of domestic, family and sexual violence, which entrench victim blaming and coalesce with social determinants of health, structural inequities and colonialism. This manifests in responses and interventions that do not adequately hold perpetrators to account and do not effectively recognise and respond to victims’ and survivors’ needs, strengths and resistance.
By contrast, responses that embrace complexity and enable choice and self-determination are highly regarded. With adequate resourcing and workforce strengthening, systemic strengths in collaboration, connection, collective healing and compassion can be further harnessed to create powerful shifts in addressing the full spectrum of prevention, early intervention, response and recovery.
The workforce called for a public health approach to address the social determinants of health that intersect and impact victims and survivors, children and young people and perpetrators. Key to redressing systemic inequities and gaps is implementing strengths-based approaches that are trauma- and violence-informed and decolonising across health, justice and social services. Enabling policy and substantial investment is critical to address inadequate resourcing, strengthen workforce capability and bring forth innovative responses.
Key recommendations
Our findings point to important opportunities and priorities for service and system improvement, with recommendations across four key areas:
- Promote safer communities, workplaces, schools and homes.
- Enhance workforce competency, capability and collaboration across sectors.
- Break intergenerational cycles of violence and trauma by better supporting children and young people.
- Bring forth innovative solutions.
Promote safer communities, workplaces, schools and homes
Recommendations to promote safer communities, workplaces, schools and homes are underpinned by the recognition of domestic, family and sexual violence as a social determinant of health. Accordingly, these recommendations seek to ensure that domestic, family and sexual violence is addressed within the context of its intersection with other social determinants, such as safe housing and communities; income equality; workforce participation; social inclusion and non-discrimination; and equitable access to justice, healthcare and social services.
Recommendation 1
Prioritise safe and affordable housing solutions by governments to address critical shortages and bottlenecks in emergency housing, as well as shortages in other short- and long-term housing. Universal design principles are essential to ensuring that housing solutions are appropriate and accessible for all.
Recommendation 2
Provide federally funded and accredited community bystander training to mobilise and equip individuals to recognise and respond to domestic, family and sexual violence.
Training should be free and co-produced with lived expertise advocates.
Recommendation 3
Recognise the importance of workplaces and educational settings for generating community change in knowledge, attitudes and behaviours. In educational settings, implementation of nationally consistent curricula on consent, healthy relationships and domestic, family and sexual violence must be supported, for example by funding local violence prevention practitioners to deliver additional training and support to schools.
In workplaces, violence prevention and anti-violence initiatives are important to enable a safe work environment for all, as is implementation of specific policies that have been developed to support victims and survivors, such as paid domestic violence leave policy. The implementation of such initiatives requires ongoing monitoring and evaluation to determine uptake and effectiveness.
Enhance workforce competency, capability and collaboration across sectors
Recommendation 4
Increase core funding for frontline services, with built-in mechanisms to account for consumer price index (CPI) and award wage increases, as well as flexible support packages and emergency funds, which can be mobilised rapidly to frontline services following disasters. Funding cycles should be a minimum of three to five years to ensure frontline services are sustained. Funding packages must allow for flexibility and tailoring to local contexts, with resourcing to introduce responses that have been shown to be effective in similar contexts as well as capacity to implement new and context-specific responses.
Recommendation 5
Develop nationally accredited workforce training that can be tailored to health, police, magistrates and child welfare, which draws on the social entrapment model of violence and principles of trauma- and violence-informed care. This training should be co-designed by those with professional and lived experience and expertise.
Recommendation 6
Mandate training in the Safe & Together model for those working in child protection and related services including police, magistrates, judicial registrars and expert witnesses. Expand Safe & Together training to be accessible to those working with families across health, education, legal and related services.
Recommendation 7
Fund targeted research, that is led by Aboriginal and Torres Strait Islander peoples and communities, to investigate and implement decolonising approaches to enhance workforce competency and capability.
Break intergenerational cycles of violence and trauma by better supporting children and young people
Recommendations to address intergenerational cycles of violence and trauma by better supporting children and young people are underpinned by recognition of children and young people as victims and survivors in their own right. This recognition should be embedded in policy and practice guidelines and must be accompanied by greater investment in child-specific interventions.
Recommendation 8
Fund targeted research to establish evidence of effectiveness of therapeutic interventions for young people who are victims and survivors and those who use violence.
Recommendation 9
Fund targeted research to establish evidence of effectiveness of promising whole-of-family approaches which use a child-focused lens, with a view to supporting expanded implementation.
Recommendation 10
Re-evaluate the roles, responsibilities and training needs of Independent Children’s Lawyers, family report writers and other child court experts to ensure that there are independent and robust assessments of a child’s best interests in circumstances of family violence and other safety concerns. This will help to inform decision-makers and provide an effective voice for children as victims and survivors in their own right.
Bring forth innovative solutions
Recommendation 11
Build on promising digital and telehealth solutions that emerged as innovations during the COVID-19 pandemic to improve equitable access to services, including use of interpreters. Consider hybrid and hub models for digitally enabled service delivery to regional and remote locations to enable outreach options and strengthen collaboration with local services.
Recommendation 12
Invest in implementation of secure platforms for operational information sharing that were advanced during the pandemic. This must be accompanied by legislation, guidelines, training and practice resources to support information sharing.
Recommendation 13
Invest in therapeutic interventions that are focused on long-term health, healing and recovery, such as trauma-specific services. This requires adequate resourcing of therapeutic interventions delivered by health services including Aboriginal community-controlled organisations. An important component of this is alternatives to criminal justice responses, such as therapeutic court interventions, as well as prison throughcare programs and family restoration programs.
Introduction
In Australia, domestic, family and sexual violence is disproportionately experienced by women. In its 2016 Personal Safety Survey (PSS), the Australian Bureau of Statistics (ABS) reported that, since the age of 15, women were three times more likely to experience partner violence compared to men (one in six women and one in 16 men; Australian Bureau of Statistics, 2017a). This included physical and sexual violence by a current or former partner. Additionally, one in four women experienced emotional violence from a partner, compared to one in six men, and one in five women experienced sexual violence compared to one in 20 men (Australian Bureau of Statistics, 2017a). Between 2005 and 2016, the rate of partner violence against women has remained stable; between 2012 and 2016, the rate of sexual violence against women has increased (Australian Bureau of Statistics, 2017a). This is despite the rate of
total violence in Australia decreasing, which largely reflects rates of physical violence perpetrated against men decreasing (Australian Bureau of Statistics, 2017a).
The risk and complexity of experiencing domestic, family and sexual violence is higher for some women and communities in Australia (Australian Bureau of Statistics, 2017a; Australian Institute of Health and Welfare, 2019). Viewed through the framework of intersectionality (see “Definitions and concepts”), social identities intersect along axes of power. For victims and survivors who experience intersecting axes of oppression and discrimination, the experiences and impacts of violence can be more complex and severe, and they occur in the context of greater barriers to reporting and accessing effective support and service responses.
Children and young people who have experienced domestic, family and sexual violence are victims and survivors in their own right. When there is violence occurring in the home, children and young people experience this by seeing, hearing and/or being involved (Australian Bureau of Statistics, 2017a; Kulkarni et al., 2011; Richards, 2011). Not only do experiences of violence in the home have negative health, social and developmental consequences for children and young people, they are also associated with physical and sexual child abuse (Gracia et al., 2017; Hamby & Grych, 2013; Richards, 2011). Children who experience violence are also at higher risk of using violence in adolescence or adulthood (Child Family Community Australia, 2014; Roberts et al., 2010).
It is well recognised that current service system responses to domestic, family and sexual violence are complex and difficult to navigate (Council of Australian Governments, 2019). Often victims and survivors require access to multiple services across different sectors, including health, justice and specialist domestic, family and sexual violence services. Across and within sectors, services are frequently fragmented and siloed (Neave et al., 2016; NSW Ministry of Health, 2019). This results in victims and survivors needing to repeat their story multiple times, which can lead to re-traumatisation (Salter et al., 2020). At a systems level, the impact of service fragmentation is limited knowledge translation and coordination (Government of Western Australia, 2020; Neave et al., 2016; NSW Government, 2019).
Services are generally funded for crisis intervention and are not resourced to provide comprehensive responses to the intersecting and long-term health, economic and social consequences of abuse (Neave et al., 2016; Salter et al., 2020; Trevillion et al., 2014). This is compounded by a lack of consistent responses within sectors and the time-limited requirements of service delivery models (Neave et al., 2016). As a result, there is little focus on medium- and long-term recovery, especially for women with multiple, long-term or complex needs (Neave et al., 2016; Salter et al., 2020; Trevillion et al., 2014). To address these shortcomings, a greater understanding of the service experiences and support needs of victims and survivors, children and young people and perpetrators is needed – in particular, the unique and diverse needs of specific groups of people who are at higher risk of experiencing violence.
Since 2013, national and state-based surveys and censuses have attempted to capture the gaps and challenges faced by workers who engage with individuals impacted by violence (Cortis et al., 2018; Department for Victorian Communities, 2021; NSW Health, 2014). They provide an important perspective on who is responding to domestic, family and sexual violence and workforce issues such as confidence, collaboration, training and resourcing. However, they have not investigated what workers find effective and ineffective in responding to victims and survivors, children and young people and perpetrators.
This report forms part of a larger national project on the responses to domestic, family and sexual violence in Australia that is focused on amplifying the voices of victims and survivors, perpetrators and the domestic, family and sexual violence workforce. This report presents findings from a survey of the workforce including service providers, managers and researchers who are experts through their experience working in the sector.
Aims of the study
This study uses an online qualitative survey to explore the lived experience of service providers, managers and researchers who are experts across health, justice and specialist family, domestic and sexual violence services in order to understand, from their perspectives, “what works, what might work and what doesn’t work” in response to domestic, family and sexual violence.
Background
National policy context
In Australia, addressing violence against women and children is a national priority. The National Plan to Reduce Violence against Women and their Children 2010–2022 (the National Plan), established in 2010, represents a national framework for action to reduce domestic, family and sexual violence. A new National Plan is under development and expected to commence in late 2022 when the current plan ends.
Implemented over 12 years in four phases, the first National Plan was framed by six outcome areas that are focused on achieving reduced prevalence of and deaths related to violence, a reduced proportion of children experiencing family violence, and an increased proportion of women who feel safe in their communities (Council of Australian Governments Advisory Panel, 2010). The findings of this report will be framed under these six outcomes:
- The first outcome of the National Plan is that communities are safe and free from violence, demonstrated by community attitudinal changes.
- The second outcome is that relationships are respectful, demonstrated by young people’s improved attitudes towards, and skills and behaviour in, respectful relationships.
- The third outcome is that Aboriginal and Torres Strait Islander communities are strengthened, demonstrated by a reduced perception that violence is an issue in these communities and an increase in prevention efforts.
- The fourth outcome is that services meet the needs of women and children experiencing violence, demonstrated by improved access to and responsiveness of services for victims and survivors.
- The fifth outcome is that justice responses are effective, demonstrated by an increase in reported domestic violence and sexual assault.
- The sixth outcome is that perpetrators stop offending and are held to account, demonstrated by a reduction in perpetration.
In 2015, the Council of Australian Governments (COAG) endorsed the National Outcome Standards for Perpetrator Interventions (Council of Australian Governments, 2015), which is a set of principles to measure and assess the effectiveness of perpetrator interventions. In the same year the Advisory Panel on Reducing Violence against Women and their Children was established to advise COAG on violence against women. On 1 April 2016 they submitted a report to COAG that identified six areas for action and 28 recommendations that COAG considered in the development of the Third Action Plan of the National Plan (Council of Australian Governments, 2016).
The Fourth Action Plan, building on the progress of the previous three action plans, sets out five national priorities to guide responses to violence against women and children between 2019 and 2022 (Council of Australian Governments, 2019). The priorities are:
- Primary prevention is key:
-
- Implement coordinated and targeted interventions.
- Promote gender equality, respect for women and healthy and safe relationships.
- Address intergenerational trauma for Aboriginal and Torres Strait Islander peoples.
- Support Aboriginal and Torres Strait Islander women and their children:
-
- Engage Aboriginal and Torres Strait Islander expertise.
- Innovate on alternative models of support.
- Build workforce capacity to respond in a culturally safe way.
- Address immediate impacts and underlying drivers of violence.
- Respect, listen and respond to the diverse lived experience and knowledge of women and their children affected by violence:
-
- Implement community-led and tailored initiatives.
- Address complex forms of violence and the disproportionate impact of violence on particular groups.
- Respond to sexual violence and sexual harassment:
-
- Promote informed consent, bodily autonomy and respectful relationships.
- Strengthen capacity of sectors to respond.
- Deliver client-centred, trauma-informed, specialised and consistent support.
- Improve support and service system responses:
-
- Focus on safety and recovery for victims and survivors and trauma-informed support for perpetrators.
- Collaborate across services, sectors and workforces.
- Build the evidence base.
- Improve access to accommodation for victims and survivors.
In 2019, the National Women’s Health Strategy 2020–2030 (Commonwealth of Australia, 2019) outlined the national approach to improving health outcomes for women and girls in Australia. The health impacts of violence against women and girls are included as a priority area to raise awareness, and address the health and related impacts, of domestic, family and sexual violence, and co-design and deliver safe and accessible services for women experiencing violence (Department of Health, 2018).The Strategy includes five key priority areas that inter-relate and overlap such that improvements in one priority area positively influence other priority areas. The other priority areas are maternal, sexual and reproductive health; healthy ageing; chronic conditions and preventive health; and mental health.
In order to raise awareness of the health impacts of violence, the Strategy has committed to promoting peer education of children, young people and adults, as well as developing an awareness campaign on the physical and mental health impacts of violence. In terms of addressing health and related impacts of violence, the Strategy has committed to developing innovative models of care that provide access for women who disproportionately experience violence, as well as increasing the capacity of the health workforce to respond to violence. The Strategy also emphasises the importance of co-designing and delivering safe and accessible services by improving access to and investment in crisis intervention support, pathways to recovery, and freely accessible information and support services.
The key measures of success for the priority area addressing the health impacts of violence include:
- an increase in the number of services available and women accessing services
- a decrease in deaths from physical violence
- a reduction in the proportion of women who have experienced abuse or trauma
- a reduction in the rate of reproductive coercion
- a reduction in the gap in mental and physical health trajectories between women who have and have not experienced violence.
In 2021, the House of Representatives Standing Committee on Social Policy and Legal Affairs published a report on their Inquiry into family, domestic and sexual violence (Commonwealth of Australia, 2021). A key recommendation was the development of national data collection for service systems and improved understanding of the experiences of Aboriginal and Torres Strait Islander victims and survivors and communities impacted by violence.
Also in 2021, the National Association of Services Against Sexual Violence was commissioned by the Commonwealth Government to publish the third edition of the Standards of Practice Manual for Services Against Sexual Violence (National Association of Services Against Sexual Violence, 2021). The Standards are intended to act as a guideline to ensure services provide accessible, quality and consistent care.[3]
The Commonwealth Government is currently in the process of developing the National Plan to End Violence against Women and Children 2022–2032 (Department of Social Services, 2022). This will replace the current National Plan, which ends mid-2022. It will be underpinned by two five-year action plans, including separate action plans dedicated to Aboriginal and Torres Strait Islander peoples.
All state and territory governments have separate policies on addressing violence in line with their commitment to the National Plan and accompanying action plans.
Victims and survivors of violence in Australia
The health, economic and social consequences of domestic, family and sexual violence are extensive and impact victims and survivors, children and young people, perpetrators, and communities (World Health Organization, 2014). For victims and survivors, experiences of violence and the accompanying trauma contribute to the burden of disease and can have acute and chronic health consequences (Dillon et al., 2013; Walker, Beek, et al., 2020; Webster, 2016). For women aged 18 to 44, in 2016 it was estimated that 5.1 per cent of the burden of disease was due to intimate partner violence (Webster, 2016). Poor mental health outcomes are the most reported health consequence of intimate partner violence (Ayre et al., 2016; Dillon et al., 2013; Oram et al., 2022; Szalacha et al., 2017; Webster, 2016). Experiences of violence can also impact victims’ and survivors’ employment and housing security (Webster, 2016). The yearly economic cost of
violence against women and children is estimated to be $22 billion (KPMG, 2016). This cost is borne by victims and survivors, children, perpetrators, families, friends, communities, employers and the Australian Government (KPMG, 2016).
In Australia, the following peoples and communities experience a disproportionate burden of domestic, family and sexual violence, along with greater barriers to accessing appropriate and effective justice, safety and support. However, as aforementioned, experiences of domestic, family and sexual violence coalesce with other intersecting axes of oppression, disadvantage and stigmatisation. Accordingly, peoples’ and communities’ experiences must be viewed through an intersectional lens, to understand how experiences of violence can be compounded by other inequities and experiences of trauma.
Aboriginal and Torres Strait Islander women experience a disproportionate burden of violence. This reflects the ongoing impact of colonisation, racism and intergenerational trauma that maintains interpersonal and structural violence and compounds the consequences of violence (Blagg et al., 2015; Blagg et al., 2018; Nancarrow, 2010). For example, as a result of intergenerational trauma related to the Stolen Generation, Aboriginal and Torres Strait Islander women are reluctant to report violence and seek support for fear of losing custody of their children or of their children being placed in the out-of-home care system (Langton et al., 2020). This contributes to the under-reporting of domestic, family and sexual violence in Aboriginal and Torres Strait Islander communities (Willis, 2011). Additionally, there is an assumption that violence experienced by Aboriginal and Torres Strait Islander
women is mainly perpetrated within communities and by Aboriginal and Torres Strait Islander men. However, this is a narrow conception of violence with a colonial legacy (Clark, 2014; Walker, Mackean, et al., 2020). There is anecdotal evidence that non-Indigenous men perpetrate a significant proportion of the violence experienced by Aboriginal and Torres Strait Islander women (Our Watch, 2018).
Adults who experienced violence as children have a higher risk of experiencing violence in adulthood (Australian Institute of Health and Welfare, 2019). A recent meta-analysis found the average prevalence of recurrent sexual violence in adulthood was almost 50 per cent (Walker et al., 2019).
Culturally and linguistically diverse women, including refugee women and migrant women, experience unique forms of violence including forced marriage, female genital mutilation and dowry-related violence (Neave et al., 2016), as well as more severe and prolonged violence compared to women who are not from culturally and linguistically diverse backgrounds (Ayre et al., 2016). For example, women who are from culturally and linguistically diverse backgrounds are more likely to experience multi-perpetrator family violence compared to women who are not (Salter, 2013; Vaughan et al., 2016). For women in a relationship with Anglo-Australian men, violence can include race- or religion-based discrimination (Vaughan et al., 2016). For many culturally and linguistically diverse women, these experiences are compounded by experiences of trauma and violence that relate to their refugee or immigrant experience (Vaughan et al., 2016).
LGBTQ+ communities disproportionately experience violence, with lesbian and bisexual women and trans women experiencing the biggest burden of violence compared to cisgender, exclusively heterosexual people and men in same-sex relationships (Edwards et al., 2015; Gebicki et al., 2018; Hill et al., 2020; Langenderfer-Magruder et al., 2016; Szalacha et al., 2017). However, in Australia there are no national estimates of the prevalence of violence against women who identify as gender diverse and/or in a sexual minority group because the PSS does not collect data on LGBTQ+ identity. In 2022 the Australian Research Centre in Sex, Health and Society (ARCSHS) published a national survey of the health and wellbeing of 6,835 LGTQ+ people (Hill et al., 2020). Forty-two per cent of participants reported having ever been in an intimate relationship where they were abused by their partner and 39 per cent reported
ever being abused by a family member (Hill et al., 2020). This echoed a 2021 ARCSHS report on the experiences of 6,418 LGBTQA+ people aged 14 to 21, in which 43 per cent of participants experienced one or more forms of homelessness because of family violence, often related to family rejection (Hill et al., 2021).
Older women (> 65 years) are at risk of experiencing elder abuse, defined as violence that occurs in a relationship with an expectation of trust, such as an intimate partner relationship (WHO, 2018). For Aboriginal and Torres Strait Islander women, there is an increased risk of elder abuse from the age of 50. Older women are more likely to experience emotional and sexual violence than physical violence (Meyer et al., 2020; Pathak et al., 2019).
Women who are or have been incarcerated have high rates (>70%) of domestic, family or sexual violence histories (Justice Health & Forensic Mental Health Network, 2017). In many cases, offending is associated with experiences of violence, for example driving without a license to flee, or self-defence (Bevis et al., 2020). Being incarcerated can also mimic experiences of abuse and lead to re-traumatisation and complex trauma (Day et al., 2018; Stathopoulos et al., 2012). Additionally, a Queensland study found women who have a history of incarceration are 16 times more likely to die from violence (Willoughby et al., 2020).
Pregnant women often experience violence for the first time during pregnancy, or the severity of existing violence increases (James et al., 2013). In the PSS, during pregnancy, one in five women experienced violence from a current partner and almost half experienced violence from a previous partner (Australian Bureau of Statistics, 2017a). The risk of violence during pregnancy is more pronounced for young women (Brownridge et al., 2011). Women who experience violence during pregnancy are also three times more likely to experience depression (Brown et al., 2015).
Sex workers experience a high burden of domestic, family and sexual violence in their lifetime (Decker et al., 2013; Muldoon et al., 2015). In a Queensland study of female sex workers’ health there was a high prevalence of child sexual abuse history among participants (Seib et al., 2009). However, the literature is limited on the prevalence of domestic, family and sexual violence among sex workers in Australia and the majority of evidence focuses on violence that occurs within the context of sex work (Decker et al., 2010; Shannon et al., 2008; Shannon et al., 2009).
Socio-economically disadvantaged women are 1.5 times more likely to experience violence compared to women living in areas of least disadvantage (Australian Bureau of Statistics, 2017a). Additionally, prolonged experiences of violence can compound and/or produce financial stress and precarity, which can be related to financial abuse and impacts on employment (Cortis & Bullen, 2016).
Women living in rural and regional communities are 1.4 times more likely to experience violence than women living in major cities (Australian Bureau of Statistics, 2017a). In 2018, women living in remote and very remote areas were 24 times more likely to be hospitalised for violence compared to people living in major cities (Australian Institute of Health and Welfare, 2019). These experiences of violence are compounded by small, tight-knit communities with cultures of silencing and denying violence, as well as limited support services (Blagg et al., 2015; Owen & Carrington, 2015).
Women with disability and disabled women experience more prolonged and severe violence that leads to serious injuries compared to women without disability (Australian Bureau of Statistics, 2017a; Didi et al., 2016). In the 2016 PSS, women with disability or disabled women were 1.8 times more likely to experience intimate partner violence in the previous year and 1.7 times more likely to have experienced sexual violence since the age of 15 compared to women without disability (Australian Bureau of Statistics, 2017a). Additionally, one third of adults who have experienced sexual harassment have a disability or are disabled (Australian Bureau of Statistics, 2017a). Re-occurrence is common for women with disability or disabled women, as violence is more likely to be perpetrated by multiple male perpetrators throughout a lifespan (Australian Bureau of Statistics, 2017a). People with psychological or
intellectual disability are more likely to experience domestic, family and sexual violence compared with other disabilities (Australian Bureau of Statistics, 2017a).
Women who have separated from their partner can experience violence for the first time or an escalation in violence perpetrated by their partner (Bruton & Tyson, 2017). In the PSS, one in seven women reported violence for the first time during a separation and 14 per cent reported an increase in violence (Australian Bureau of Statistics, 2017a). Of women who separated from a partner who used violence, two in five continued to experience violence by this partner post-separation (Australian Bureau of Statistics, 2017a).
Young women (aged 15 to 34) are more likely to experience domestic, family and sexual violence compared to all other age groups. In the PSS, young women were 2.7 times more likely to experience intimate partner violence compared to women over 35 years old (Australian Bureau of Statistics, 2017a), and in 2017 women aged 15 to 34 made up more than half (53%) of female sexual assault victims and survivors recorded by the police (Australian Bureau of Statistics, 2017a). Since the start of COVID-19, young women (18 to 24) have experienced the highest rates of all types of violence compared to other age groups (Australian Institute of Health and Welfare, 2021a).
Children and young people
Frequently, children and young people’s experiences of family and domestic violence are described as “witnessing” violence, however this description is limited as it does not capture the various ways children can experience and be exposed to violence (Humphreys, 2007). Experiences of domestic and family violence can also include being used as a hostage, being asked to spy on a parent, being blamed for violence or attempting to intervene to stop the violence (Richards, 2011). Emotional abuse can also include former partners lying to children with the intention of turning them against their parent, or threatening to take the children away (Australian Bureau of Statistics, 2017a).
In the PSS, 50 to 68 per cent of children had seen/heard violence perpetrated by a parent or a parent’s current or former partner, and before the age of 15 one in eight women witnessed violence towards their mother by a partner and one in 20 witnessed violence towards their father by a partner (Australian Bureau of Statistics, 2017a). In 2019 to 2020, the most common primary type of child abuse recorded by child protection services was emotional abuse, which included children’s “exposure” to family violence (Australian Institute of Health and Welfare, 2021b).
The Family Law Act 1975 (Cth) explicitly states that exposure to violence is child abuse in s 4(1). However, whether it is classified as abuse is usually dependent on the frequency and nature of the violence the child or young person experiences (Richards, 2011). Additionally, the application of the legislation has been criticised for placing an unfair burden on victims and survivors to prevent children’s experiences of violence (Flood & Fergus, 2008; Kaufman & Little, 2003). For Aboriginal and Torres Strait Islander women this can intersect with historical and intergenerational trauma related to the state-sanctioned removal of Aboriginal and Torres Strait Islander children, and also the contemporary over-representation of Aboriginal and Torres Strait Islander children in out-of-home care (Humphreys, 2007, 2008).
Experiences of domestic and family violence are often associated with physical and sexual child abuse (Bedi & Goddard, 2007; Gracia et al., 2017; Hamby & Grych, 2013; Richards, 2011). When children directly experience physical violence in the family context, it is usually perpetrated by an adult in a position of trust such as a parent, guardian or partner of a parent/guardian (Australian Bureau of Statistics, 2017a; Campo, 2015). Co-occurrent experiences of child abuse are more likely to occur when violence is more severe and frequent (Kaufman & Little, 2003). However, the prevalence of children’s co-occurring experience of domestic and family violence and experience of sexual abuse is not clear because it is under-reported and/or reported as emotional or physical abuse (Australian Institute of Health and Welfare, 2021b; Richards, 2011).
For children who experience violence there can be ongoing health, social and developmental issues that extend beyond childhood, into adolescence and adulthood (Campo et al., 2014; Webster, 2016). These include mental health difficulties, unemployment, homelessness and impaired cognitive functioning (Campo et al., 2014; Ellonen et al., 2013; Oram et al., 2022; Richards, 2011). Additionally, experiencing violence in childhood is associated with intergenerational transmission of domestic, family and sexual violence perpetration or victimisation (Ehrensaft et al., 2003; Oram et al., 2022; Richards, 2011).
Perpetrators
Perpetrators of domestic, family and sexual violence are more likely to be male (Australian Bureau of Statistics, 2017a; Australian Institute of Health and Welfare, 2018). In the PSS, three in four instances of intimate partner violence were perpetrated by a male former or current partner and 99 per cent of intimate partner violence perpetrated against female victims and survivors was perpetrated by a current or former male partner (Australian Bureau of Statistics, 2017a). This is also true for femicide, the killing of women. In Australia between 2010 and 2018, 77 per cent of intimate partner homicide was perpetrated by male offenders (Australian Domestic and Family Violence Death Review Network & Australia’s National Research Organisation for Women’s Safety, 2022).
The perpetration of domestic, family and sexual violence is associated with a history of experiencing violence, including experiencing violence as a child or young person, and a history of trauma (Australian Institute of Health and Welfare, 2019; Neave et al., 2016). In a recent report on male-perpetrated intimate partner homicide, 54 per cent of offenders reported a history of trauma (Boxall et al., 2022).
Who is responding to domestic, family and sexual violence?
Services within the sector in Australia that directly respond to domestic, family and sexual violence include health, justice, welfare and specialist domestic, family and sexual violence services.
Specialist domestic, family and sexual violence service providers in Australia include but are not limited to:
- shelters, refuges or homelessness services
- domestic and family violence courts and court support services
- family violence and women’s legal services
- specialist domestic and sexual violence counselling services (telephone, online, in person)
- sexual assault services
- violence, abuse and neglect services
- men’s behaviour change programs
- crisis support, including helplines and emergency payments
- outreach services
- community organisations.
Mainstream services provide a range of services that are not specific to domestic, family and sexual violence but are accessed by people who experience and perpetrate domestic, family and sexual violence. The mainstream services responding in the justice, health and welfare sectors include but are not limited to:
- police
- legal aid
- community legal centres
- court advocacy programs for victims and perpetrators
- courts and tribunals
- child protection
- Aboriginal community-controlled organisations (ACCOs)
- Aboriginal and Torres Strait Islander legal services
- Aboriginal community-controlled health organisations (ACCHOs)
- women’s health centres
- primary healthcare
- social work
- community health
- allied health
- maternal and child health
- mental health
- alcohol and other drugs
- housing services
- ambulance and emergency department
- aged care
- public health programs and health promotion organisations
- disability support
- dental.
In recent years, surveys and censuses of the workforce responding to domestic, family and sexual violence have attempted to capture the characteristics of the workforce, as well as the gaps and challenges from workers’ perspectives (Cortis et al., 2018; Department for Victorian Communities, 2021). In 2017 a national survey was conducted of workers in services used by people affected by domestic, family and sexual violence (Cortis et al., 2018). In 2019 to 2020 a similar survey was conducted in Victoria of specialist and primary prevention workforces and the broader workforces that intersect with family violence (Department for Victorian Communities, 2021). Both surveys considered issues related to confidence, collaboration, training and resourcing.
Three in five specialist workers in the Victorian survey reported they were extremely or very confident to respond to family violence, while only 28 per cent of workers felt confident in the broader workforce that responds to family violence, including health, justice and social services (Department for Victorian Communities, 2021). In the national survey, workers felt more confident recognising and responding to physical and emotional abuse, compared to financial and sexual abuse, and considered collaboration and sharing information as the most important additional support to increase confidence (Cortis et al., 2018). Respondents identified that the main barriers to collaboration were limited knowledge of services and systems available, lack of specific protocols facilitating collaboration and a lack of time to build networks (Cortis et al., 2018).
In the national survey, the top five areas workers wanted more training in were risk assessment, therapeutic approaches, legal training, general counselling and screening (Cortis et al., 2018). Additionally, the majority of participants wanted more training on how violence impacts, and is experienced by, specific groups including people with disability or disabled people, Aboriginal and Torres Strait Islander people, LGBTQ+ communities, people from refugee backgrounds and people with experiences of homelessness (Cortis et al., 2018). A similar result was seen in the Victorian study: participants wanted more training on working with people with disability or disabled people (Department for Victorian Communities, 2021).
In the national survey, the majority of participants (61%) worked full-time (Cortis et al., 2018). Among part-time workers the reasons for part-time work included caring, personal or family responsibilities; limited full-time positions available or resources to support a full-time position; and reducing stress, burnout, vicarious trauma or compassion fatigue. Retention issues were attributed to poor pay, challenging work, limited organisational support and career pathways. These issues were more pronounced in early career workers or positions that worked closely with perpetrators. While these surveys and censuses establish a picture of the gaps and challenges faced by the workforce, they do not establish what the workforce perceives to be effective, ineffective and promising in addressing domestic, family and sexual violence.
Methodology
This study used a qualitative online survey to gather the perspectives of the domestic, family and sexual violence workforce in Australia. Drawing on contextualism, we carried out a reflexive thematic inquiry to understand how the workforce perceives interventions and approaches to be effective, as well as barriers, enablers and opportunities in preventing and responding to domestic, family and sexual violence. Contextualism emphasises that knowledge is context-specific and sensitive, and as such, the way that people ascribe meaning to their experiences is deeply connected to the context of their experiences (Braun & Clarke, 2006, 2019; Braun et al., 2018; Jaeger & Rosnow, 1988). This perspective was appropriate as we sought to understand how the workforce’s views are context-bound. Therefore, implementation and perceived effectiveness of interventions and approaches need to be seen in the context within which they are delivered.
Just as workforce views are contextually bound, so too are meanings and interpretations ascribed by the research team. Members of the research team come from diverse professional backgrounds that combine academic and clinical experiences, working in public health, law, policy, medicine, psychology and allied health. We also bring personal, family and community lived experience that shapes our understandings of domestic, family and sexual violence. Our learned experience as clinicians and researchers is primarily through a public health lens, and we are conscious of how this context has shaped the design, data collection and analysis. We have sought to reflect on our own assumptions, biases and perspectives using regular debriefing and journal notes to inform our reflexive process.
Advisory committee
For the larger study, an advisory committee was formed comprising representatives from government, service and advocacy organisations in the domestic, family and sexual violence sector in Australia (see Appendix A). The Voices Advisory Committee provided guidance and advice at meetings and via email to inform the research at various stages. Specifically, its input shaped the study design, development of the survey instrument, recruitment processes, and analysis and interpretation of findings and implications for policy, practice and further research.
Research questions
To address the aim of the study, we were guided by the following research questions:
- What contextual factors inform the perceived effectiveness and appropriateness of interventions and responses and the way they are understood to work?
- What outcomes are different interventions and responses designed to achieve?
- What are the recommendations for service and system improvement to better respond to victims and survivors, children and young people and perpetrators?
Survey instruments
The survey was developed in consultation with the advisory committee through an iterative process of compiling and testing survey questions. The design of the survey was informed by the literature and feedback received during the pilot process by the experts on the advisory committee, who initially reviewed the survey to confirm it measured the constructs of interest (Bolarinwa, 2015). The survey was then piloted with the advisory committee and ANROWS staff, who provided feedback prior to finalisation and delivery.
The survey contained two sections. Respondents were first asked to provide their demographics and career information, including gender; professional role; primary discipline; primary sectors; experience (years) in the domestic, family and sexual violence sector; and their current organisation’s area of operation/jurisdiction or geographical scope of research. They were also asked to nominate specific groups of people that they felt able to comment on. The options included young people (16 to 24 years), older people (50 years and older), Aboriginal and Torres Strait Islander peoples, culturally and linguistically diverse communities, people with disability or disabled people, LGBTQ+ communities, people living in rural or remote areas, women who are or have been incarcerated, and sex workers.
Respondents were asked to identify up to three existing responses or interventions that were promising or effective, and up to three that were ineffective, for each of the following:
- victims and survivors of domestic or sexual violence
- children and young people who have experienced domestic or family violence (<18 years)
- perpetrators of domestic or sexual violence
- adolescent perpetrators of violence in intimate relationships or sexual violence
- any specific group that they had nominated in the previous section.
Questions asked respondents to describe each nominated response or intervention, including who provides it, in what setting and the group it is designed for, as well as the outcomes it achieves and how they are achieved. Respondents were also asked about the existing gaps in policy, legislation and/or appropriate service provision for the group of people the intervention is designed for, as well as recommendations for future directions in responding to the group.
Recruitment strategy and data collection
In order to capture the range of responses and interventions, a purposive sampling approach was used with potential respondents invited from a range of backgrounds and organisations. The research team emailed potential respondents to introduce the project. Potential respondents were included based on their occupation (practitioner, service designer/manager, researcher in academic or non-academic organisation) or experience in addressing domestic, family and sexual violence in Australia.
Invitations to the first survey were emailed to 650 stakeholders on ANROWS’s expert stakeholder list. Potential respondents were emailed three times (including the initial email). The survey was also promoted via Twitter to 14 relevant professional associations. Two adverts were placed in ANROWS’s fortnightly online newsletter, Notepad.
A modified snowball strategy was also used to recruit respondents, where respondents were asked to share the survey link with other experts in their network (Bryman, 2001; Crabtree & Miller, 1992). Participation was voluntary and no incentive was provided for completing the survey.
The survey was developed and distributed via weblink using the secure SurveyMonkey software platform. The survey was estimated to take 20 to 30 minutes to complete, however may have taken more or less time, depending on the number of areas of expertise selected. Respondents were able to complete the survey anonymously and could discontinue the survey at any point.
Between 17 November 2020 and 29 January 2021, the survey received 199 responses, which is a response rate of 30 per cent based on direct email invitations. However, it must be acknowledged that as a result of the COVID-19 pandemic, between November 2020 and January 2021 there was increased demand on the domestic, family and sexual violence workforce, which may have impacted response rates (Australian Institute of Health and Welfare, 2021c). Additionally, while 199 responses were received, 104 were excluded because they did not provide substantive responses beyond demographics. Thereby, respondents who did not complete any of the qualitative questions but limited responses to the quantitative demographical questions were excluded. A total of 95 respondents were included for analysis.
Data analysis
Data was exported from SurveyMonkey into a Microsoft Excel document. Microsoft Word and NVivo software were used to manage and store the data. Descriptive analysis to report on frequency (count and percentages) of responses, such as respondent demographics, was undertaken using Microsoft Excel. Qualitative data were analysed using reflexive thematic analysis (Braun & Clarke, 2019; Braun et al., 2018).
Reflexive thematic analysis occurred in six phases. First, we familiarised ourselves with the data by reading through and sorting responses into categories according to the cohort (victims and survivors, children and young people and perpetrators). Second, we generated codes to organise the data. Third, we began to generate initial themes, drawing together codes and identifying patterns and meaning across the data. Next, these themes were iteratively revised and their meaning clarified through collaborative discussion. This included sharing the preliminary themes with the wider Voices project team and then with the advisory committee. In the final two phases, the themes were defined and then further refined and tested during the report-writing process in the context of existing literature. Respondents were assigned a non-identifying number for data extracts and potentially identifying information from illustrative quotes was removed.
The findings were shared with key stakeholders from state and national government departments through a presentation in January 2022 and via a brief report that was emailed in April 2022. The draft report was shared with key stakeholders from state and national government departments during peer review, and the recommendations were shared with the advisory committee through a presentation in July 2022. Feedback at each stage was incorporated into the final report.
Ethics
Ethics approval was granted by the University of Melbourne Human Research Ethics Committee (HREC reference number: 2057459.1).
Survey respondents were provided with the contact details of several support services and had the option to suspend the survey and return at a later time. A contact number of a member of the research team was provided if respondents had any questions.
Findings and discussion
Who participated in the Voices survey?
The majority of respondents identified as female (n=86, 91%; males: n=7, 7%). Two respondents identified as non-binary. Respondents were drawn from all states and territories, however most worked in Victoria (n=31, 33%), Western Australia (n=16, 17%) and New South Wales (n=15, 16%; Figure 1).
Figure 1: Distribution of respondents (N=95) by statea (%)
Note: a “Other” indicates states with a small cell size, which includes Tasmania and South Australia, as well as respondents nominating two states.
The majority were practitioners (n=60, 63%), while fewer were service designers or managers (n=21, 22%) and researchers (n=14, 15%). A small number of respondents who were categorised as practitioners also identified as researchers (n<5). Those working as practitioners, service designers or managers (n=81) were drawn from the following services:
- women’s specialist domestic and family violence services (including shelters, advocacy and casework services; n=23, 28%)
- sexual violence services (n=14, 17%)
- health services (including mental health services; n=10, 12%)
- men’s behaviour change services (n=7, 9%)
- primary prevention organisations (n=6, 7%)
- other services (including policing, Aboriginal and Torres Strait Islander organisations, legal services, disability services, multicultural services, education services, family services, financial counselling, aged care; n=21, 26%).
Among all respondents, two thirds had six or more years of experience, with most of these having 10 or more years (Figure 2).
Figure 2: Professional experience (years) of respondents (%)
Key findings
The key findings are first presented in accordance with the six outcomes from the National Plan, namely:
- Communities are safe and free from violence
- Relationships are respectful
- Aboriginal and Torres Strait Islander communities are strengthened
- Services meet the needs of women and children experiencing violence
- Justice responses are effective
- Perpetrators stop their violence and are held to account.
Across these outcomes, we describe workforce perceptions of contextual factors that inform the perceived effectiveness and appropriateness of interventions and responses. We also present priorities and opportunities identified by the workforce as important for future directions.
Following this we present the five key themes that we constructed to encapsulate workforce perceptions on what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators (Figure 3).
Figure 3: Summary of workforce perspectives on what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators.
Addressing upstream determinants of domestic, family and sexual violence
Reactivity and inequity in responses harms victims and survivors
Changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
Enabling choice and the right to self-determination
Power of connection, collective healing and compassion
National Outcome 1 – Communities are safe and free from violence
Where are we now?
There was consensus among respondents that addressing gender inequality was critical in shifting the unequal status of women in society, since gender inequality is a key driver of domestic, family violence and sexual violence:
Gender inequality is understood to be the underlying phenomenon for [domestic, family and sexual violence]. By addressing gender inequality, we assist to address the power and control dynamics present in [domestic, family and sexual violence]. (Respondent 40, Service designer/manager)
The primary gaps in keeping communities safe and free from violence identified by respondents centred on the multilayered aspects of gender inequality that structure society as well as our workplaces, families and relationships. Primarily, respondents perceived that women’s unequal participation in the workforce is a key contributor to the unequal status of women. Workplace harassment and discrimination was identified as a substantial barrier to women’s fair and equal participation in the workforce.
In particular, some respondents identified the greater burden of unpaid caring among women and the “gender pay gap” as detrimental to progress toward gender inequality. The gender pay gap in Australia derives from the lower proportion of women in senior positions and lower wages for women compared to men. Lower wages for women also compound isolation and abuse by perpetrators who seek to restrict victims’ and survivors’ financial resources: “Social isolation as well as reducing the resources of the women is an active perpetrator tactic.” (Respondent 40, Service designer/manager)
Future directions
Respondents identified advancing gender inequality in the workplace as well as primary prevention and promoting community involvement and awareness (Table 1).
Table 1: Future directions for keeping communities safe and free from violence identified by respondents with exemplar quotes
Addressing gender inequality in the workplace
| Future direction | Respondent |
|---|---|
| The workplace is an important setting in which there is unrealised potential to make significant change to policy that is discriminatory, as well as to shape community knowledge, attitudes and behaviours. For example, it was suggested that all workplaces implement anti-violence policies. Further, respondents identified the need for more comprehensive policy measures, such as adequate paid parental leave for both parents | “The duty of child rearing rests largely with women. This can be misused by perpetrators to control the women and also remove them from employment as well as other resources and support.” Respondent 40, Service designer/manager |
Mass media in primary prevention
| Future direction | Respondent |
|---|---|
| There was consensus that primary prevention requires cultural and attitudinal change in order to change behaviours. Central to this is raising awareness of gender stereotypes and inequalities. A key area of agreement was on the role of media in shaping social and gender norms, particularly through depictions of relationships. Respondents identified that the media can be harnessed to challenge gender norms, particularly those that underlie inequalities | “Outcomes achieved by educating adults and children of the subliminal messages in advertising … the unchallenged attitudes in society that perpetuate the gender inequalities.” Respondent 16, Researcher |
| Respondents suggested that mass media and social marketing approaches can be a powerful tool in shifting community attitudes, citing successes by anti-smoking campaigns, which are long-term, well-resourced, multilevel campaigns. This would require buy-in from all levels of government and community | “Fully funded, long-term campaign which is creative and involves all levels of society.” Respondent 37, Service designer/manager |
Promoting community involvement and awareness
| Future direction | Respondent |
|---|---|
| Two potential approaches to promoting community involvement and awareness were identified: bystander training though workshops or online modules, and lived expertise advocates, who were considered powerful in generating community awareness and change | “Encouraging young people to support their mates and stand up for mates, including when the young person is in the wrong.” Respondent 47, Practitioner “Improve gender equity at all facets of society. Media and societal advocates have a huge role to play in this.” Respondent 40, Service designer/manager |
National Outcome 2 – Relationships are respectful
Where are we now?
There was minimal data relating to what works in promoting respectful relationships. However, there was consensus that schools are an appropriate and important setting for consent and healthy relationships education for young people. Respondents asserted that in their current delivery, such programs are not adequately resourced and are not consistent in terms of the curriculum.
Respondents identified Love Bites as a promising intervention. Love Bites is a school-based relationships education program that provides young people with a safe environment to discuss and explore respectful relationships. Love Bites consists of two interactive workshops, “Relationship violence” and “Sex and relationships”, followed by creative workshops and community campaigns: “LOVE BITES education is focused on three critical areas for learning: knowledge: youth-led collaborative learning; attitudes: critical thinking and decision-making; and behaviours: problem solving and communication skills.” (Respondent 78, Practitioner and researcher)
The program was highly regarded by respondents as it “views young people as active participants who are able to make choices for themselves and their relationships when supported with information and opportunity for skill development” (Respondent 78, Practitioner and researcher).
Respondents also identified a lack of interventions to address young people who demonstrate abusive behaviours that have been modelled by caregivers, which can manifest as bullying behaviours with peers, at home with their family and/or in their intimate relationships.
Future directions
There were three possible areas identified as important future directions to promote respectful relationships, which again centred on young people: changes to the curriculum, better resourcing for consent and healthy relationships education, and interventions for young people to support building healthy relationships (Table 2).
Table 2: Future directions for promoting respectful relationships identified by respondents with exemplar quotes
Changes to curriculum
| Future direction | Respondent |
|---|---|
| Respondents identified embedding respectful relationships education in curriculums, including within early education, through a consistent national curriculum for primary, secondary and tertiary students | “More youth need to be exposed to the healthy relationships training called ‘Love Bites’ it’s very informative and really defines what a healthy relationship should look like. Often [domestic and family violence] is a repeated act that the perpetrator has seen happen as a form of getting things done, so they identify that this is normalized behaviour, if we can educate the youth before they are in relationships, they have a better understanding of how to be treated and what to expect.” Respondent 88, Service designer/manager |
Better resourcing for consent education
| Future direction | Respondent |
|---|---|
| Changes to curriculum must be accompanied by adequate resourcing to implement consent education effectively. In terms of adequate resourcing, one suggestion was to fund “violence prevention” practitioner positions in each region who could provide oversight and coordination for such initiatives | “Schools have now been formed into regional clusters to support them to carry out this initiative – each cluster needs a Violence Prevention Practitioner to provide a meaningful level of resourcing.” Respondent 50, Service designer/manager |
Interventions for children and young people to support building healthy relationships
| Future direction | Respondent |
|---|---|
| Respondents called for sufficient resourcing for interventions that provide therapy and other support for children and young people who engage in abusive behaviours that have been modelled by caregivers. Respondents indicated that this may include mentoring and other approaches that aim to provide role-modelling and build community connections for children and young people | “Get them into building relationships in the community to help with transition to adulthood.” Respondent 88, Service designer/manager |
National Outcome 3 – Aboriginal and Torres Strait Islander communities are strengthened
Where are we now?
Primarily respondents raised concerns about systemic issues that intersect with ongoing racism and discrimination experienced by Aboriginal and Torres Strait Islander peoples in Australia. Much of this centred on the criminal justice and child protection systems, particularly with regard to responses that are considered punitive and not trauma-informed or culturally safe.
Respondents cited concerns about high rates of Aboriginal and Torres Strait Islander children removed from families. Specifically, concerns centred on lack of collaboration with families and capability among the child protection workforce in terms of understanding how to work effectively with Aboriginal and Torres Strait Islander families. This also related to concerns around workforce understanding of the dynamics of family violence, as well as how this intersects with other forms of violence and trauma, including racism, intergenerational trauma and the ongoing legacy of colonisation:
Despite policy emphasising whole of family support, in practice there are often examples of interventions that are high-handed, do not involve collaboration with the family or explore alternatives to a punitive approach. Victim- and mother-blaming are still prevalent. There is little understanding of the patterns of behaviour that are involved with abuse and neglect and there continues to be a lack of awareness of issues and alternative approaches within the Aboriginal community. (Respondent 49, Practitioner)
Respondents also acknowledged the challenges for the child protection workforce, in terms of training, high rates of staff turnover and the need for ongoing support to manage burnout and vicarious trauma:
Child protection on its own as an intervention scheme is not helpful. Child protection is often involved after incidents of [family violence] where children are present. There is a lot of mistrust of the system, and it can seem punitive, which can make clients resistant to engagement. There is such a high workload within these agencies that it is nearly impossible for staff to spend any real time with clients. (Respondent 78, Practitioner and researcher)
By contrast, respondents reported that there are effective and culturally safe practices that have been developed and implemented through ACCOs and ACCHOs. These approaches are typically led by community, embedded with local contextual knowledge and leadership and delivery by Aboriginal and Torres Strait Islander staff: “There are good practices among ACCHOs or Aboriginal-led community responses to [family violence].” (Respondent 40, Service designer/manager)
Future directions
Respondents identified a number of promising approaches emphasising the need to prioritise self-determination and have solutions be led by Aboriginal and Torres Strait Islander communities and organisations (Table 3). Key to enabling this is adequate resourcing for sustainable, community-led and culturally safe responses:
Any future directions for supporting Aboriginal women should be culturally appropriate and safe, community-led and run by Aboriginal organisations and communities and should allow for Aboriginal decision making and self-determination. (Respondent 27, Practitioner)
Table 3: Future directions to better support Aboriginal and Torres Strait Islander communities identified by respondents with exemplar quotes
Workforce is key
| Future direction | Respondent |
|---|---|
| Respondents suggested ensuring cultural competence of mainstream staff as well as increasing the proportion of Aboriginal and Torres Strait Islander peoples through identified positions and training. Strengthening workforce capability will also support improved referral pathways between ACCHOs and mainstream services | “Comprehensive cultural awareness and safety training provided by local people for every new staff member. With refreshers provided every 12 months. Or even better develop a cultural safety framework. Utilise their Aboriginal staff in a more productive and meaningful way, not just consultation.” Respondent 78, Practitioner and researcher |
| Increasing competency and capability of all staff to enhance culturally safe responses. Importantly, respondents pointed out that this should not involve overburdening or delegating this responsibility to Aboriginal and Torres Strait Islander staff in mainstream services. It is the responsibility of mainstream services and non-Aboriginal staff to ensure their cultural competency | “Cultural competence of staff is not the responsibility of Aboriginal staff.” Respondent 59, Practitioner |
Better practice models and risk assessment tools
| Future direction | Respondent |
|---|---|
| Respondents indicated that models that work with Aboriginal and Torres Strait Islander families must consider biases and harm related to risk assessment tools that are not culturally responsive or valid | “Better risk assessment to assess … families who will benefit from additional support.” Respondent 40, Service designer/manager |
Whole-of-family approaches
| Future direction | Respondent |
|---|---|
| Respondents identified that whole-of-family approaches, in collaboration with multisectoral supports such as schools and health services, can be an effective way to support families to make holistic and lasting change | “Families need to be empowered in these process[es] to ensure there will be sustainable change that is realistic and achievable.” Respondent 78, Practitioner and researcher |
| Whole-of-family approaches must also be preventative, rather than reactive and/or punitive. This can also involve broader community work to address inequity, such as poverty, unemployment and housing | “Work harder at kinship care, keeping the child in the home with the parents … do preventative work in the community. The biggest issues [are] poverty, so reduce poverty.” Respondent 48, Practitioner |
Engage rather than marginalise men
| Future direction | Respondent |
|---|---|
| In addition to whole-of-family approaches, respondents valued working in a way that engages men and may include specific programs or supports that are aimed at reconnecting with culture and community through strengths-based approaches | “Aboriginal women say ‘we need something for our men, they are hurting too.” Respondent 35, Researcher |
| Respondents called for approaches that focus not just on reducing offending but also emphasise healing and connection to Country and culture. For example, an effective way to engage men is to support other men to be role models and leaders in their community | “Reductions in contact with the criminal justice system, reductions in alcohol and drug use, reduction in violence against partners and children, men standing up against violence in the community, men taking control of their lives and being strong role models, participating in on-country programs where they learn about being a good Aboriginal man and father.” Respondent 35, Researcher |
National Outcome 4 – Services meet the needs of women and children experiencing violence
Where are we now?
Respondents identified multiple systemic issues that contribute to service gaps and harm for victims and survivors. An overarching issue expressed by respondents was that the system is focused on single incidents and we need better understanding of and responses to patterns of abuse, including coercive control.
The most substantial gaps centred on resourcing insufficiencies, which drive and contribute to the reactivity in the system. There was consensus that resourcing is largely directed toward crisis responses and interventions, rather than early intervention or recovery. Further, there was criticism that resource constraints frequently manifested in interventions that are limited by eligibility criteria and duration, without sufficient follow-up measures in place.
Underlying these service gaps are issues of insecure, inflexible and insufficient funding, which respondents identified as a major issue in delivering services, as well as ensuring workforce capability and sustainability through longer-term funding and employment contracts. These issues are compounded in rural and remote areas, where there is a stark lack of services, especially for children and young people. Likewise, resourcing constraints are evident in the lack of culturally appropriate and accessible services for women who may experience intersecting forms of discrimination and oppression.
Respondents cited the health workforce capability as a strength, particularly in routine screening in health settings (e.g. maternal, early childhood, drug and alcohol, mental health and emergency), as well as risk screening in general practice. However, the effectiveness of this is constrained by a number of systemic factors such as clinicians’ knowledge of, or access to, clear referral pathways. Consequently, respondents identified that the health workforce requires ongoing support and education for staff to safely screen patients in these settings:
Better education for all staff who work in emergency on what is helpful and not helpful. It is really hard to change judgemental attitudes but protocols on what not to say or do in certain circumstances might be helpful. (Respondent 15, Practitioner)
Further, in health settings, the biomedical model is dominant. As such, respondents felt that the focus on physical incidents of violence without consideration or understanding of the psychosocial context can be problematic.
Respondents elaborated substantially on issues within the housing and child protection sectors. It was clear that respondents perceive that longstanding insufficiencies and deeply entrenched inequities in these systems cause harm and trauma for victims and survivors.
Housing
Multiple issues that centred on housing were described by respondents. These issues contribute to people remaining in, or returning to, unsafe circumstances, as well as traumatisation and re-traumatisation as a result of engaging with services and being unable to access appropriate housing support: “The horrendous housing situation in Australia is deterring women from leaving abusive relationships.” (Respondent 37, Service designer/manager)
There was acknowledgement that housing is a social determinant of health and that systemic issues preventing access to safe and affordable long-term housing greatly contribute to risk and harm for people experiencing violence: “Decades-long waiting list for community housing coupled with high rents and demand outstripping supply of rental properties means that finding sustainable long-term housing is becoming more difficult.” (Respondent 27, Practitioner)
Alongside widespread housing shortages, there are also substantial insufficiencies and bottlenecks in emergency accommodation.
After the 8-week tenancy, our women and children find it very difficult to find housing and at times, extend their lease. This prevents other women and children at serious threat from accessing safe crisis accommodation. It also means that women in transitional properties who are looking for long-term tenancies are finding it more difficult to move, again placing a bottleneck as some women move from crisis accommodation to transitional housing for three months before securing a tenancy. (Respondent 27, Practitioner)
Respondents elaborated on issues with emergency accommodation:
- Some accommodation has high levels of violence, which can be “scary and retraumatising and likely to prolong their suffering and delay recovery” (Respondent 15, Practitioner).
- Victims and survivors use hotels and motels for emergency accommodation, which are not universally accessible and are not suitable for children and families.
- There is a lack of options beyond emergency accommodation.
Conversely, some respondents argued there were no options for women after emergency accommodation:
- There seems to be a good amount of support with immediate crisis housing, but a lack of options for the next step, many women are left in hotels for months and months with no hope for finding safe and sustainable longer-term housing. (Respondent 52, Practitioner)
Respondents identified that these issues, which limit the safety, supply and suitability of housing, are forms of systems abuse that perpetuate trauma, increase risk, and constrain agency and choice. These issues are compounded by lack of supply and suitable housing options for LGBTQ+ communities, older persons, persons with disability or disabled persons, women without children and women with older children.
When placed in hotel cheap accommodation that is not safe and overcrowded for the family, this can place the family in a different type of harm [systems abuse] and they will return to the perpetrator. (Respondent 10, Practitioner)
The refuge I manage was not able to accommodate boys over the age of 14 for many years due to bathrooms being shared, recent refurbishment ensured all family rooms have private bathrooms enabling us to accommodate older boys … prior to being able to accept [older] aged boys we were experiencing women declining safe accommodation as they had to source other accommodation for their boys or leave them with the perpetrator. (Respondent 72, Service designer/manager)
Child protection
Respondents drew together a number of intersecting issues that centred on the child protection system. There was a sense that the system is unfairly punitive toward non-offending parents and that this drives mistrust and adverse outcomes. Respondents indicated that in practice, this frequently means that mothers are unfairly held to account for violence perpetrated by their partner and/or the children’s father: “The bulk of the pressure to act has been directed at victims of family violence. It’s the women’s parenting that has been pulled apart, not the man.” (Respondent 48, Practitioner)
One respondent framed this in the context of systems abuse, which not only harms victims and survivors and children, but ultimately discourages seeking help and support:
Removing children from women who are the non-offending parent is a collusion with the perpetrator and can be perceived [as] an extension of the violence inflicted by the perpetrator … A re-traumatising system does not encourage help-seeking behaviour. (Respondent 40, Service designer/manager)
To counter this, respondents emphasised the need for experienced workers who understand dynamics of domestic and family violence in the child protection workforce. Specifically, they outlined the need for more training for child protection workers in working with both perpetrators and non-offending parents:
… supporting the non-offending parent to keep her children safe through provision of safe housing, financial and practical resources as required, acknowledging the work the safe parent is doing to keep children safe, acknowledging and placing responsibility for the abuse with the offending parent. (Respondent 59, Practitioner)
Furthermore, workforce capability is impacted by high workloads and turnover of staff, which also contributes to issues around cultural competency and cultural safety for Aboriginal and Torres Strait Islander families:
Burnout is frequent and so there is a high turnover. This means new workers all the time, often not local. These workers often put themselves in culturally unsafe positions due to their lack of local knowledge. (Respondent 78, Practitioner and researcher)
Who is being left behind?
Respondents outlined broad systemic issues that have widespread impact. However, they also detailed more nuanced issues that disproportionately impact those who are likely to also be experiencing other forms of discrimination, oppression and barriers to accessing support.
Rather than viewing people in terms of discrete identities, respondents took an intersectional approach and identified specific systemic and service issues that must be considered in order to improve future responses for those experiencing ageism, racism, colonialism, ableism, religious prejudice, heteronormativity, homophobia, cis-sexism, transphobia and classism. Respondents elaborated on these systemic issues and described the nuanced and often less visible ways that these contribute to service gaps and harm for the following people, families and communities.
Children and young people
There was a strong sense that children and young people are not adequately considered in the context of their own rights, experiences and needs: “Children are often invisible in service delivery.” (Respondent 48, Practitioner)
Instead, children and young people seem to be treated as an adjunct to the situation or as bystanders, with one respondent noting that unless services “are specific to children and a child’s trauma, [they] do not focus on the impact on the child” (Respondent 89, Practitioner).
For example, children are often not named on intervention orders. Likewise, family law matters and arrangements for the care of children of separated families rarely centre the “voice of the child or [provide] instruction for children on how to remain safe when in custody of perpetrator” (Respondent 4, Researcher).
Often, children and young people are considered in relation to their parents or caregivers, which respondents related to traditional case management models that consider the “women to be the client and feel that they are not funded to provide services to children, or do not treat children as victim survivors in their own right” (Respondent 48, Practitioner).
Respondents also identified lack of services that specifically meet the needs of younger women who are victims and survivors: “Young women tend not to attend these general groups and are underrepresented as clients of specialist [domestic, family and sexual violence] services.” (Respondent 59, Practitioner)
For young people who use violence, respondents felt there needs to be greater recognition that they are likely also victims and survivors, which needs to inform service responses:
Violence is learnt, it can be unlearnt, but if you constantly label a young person as violent without understanding why or how the violence was used, then that [young person] will grow up into an adult who has learnt they are violent … We must acknowledge [a young person’s] vulnerability as a victim while simultaneously working with their use of violence. (Respondent 14, Practitioner)
Women who are incarcerated
Respondents pointed out that women are criminalised for offending in the context of violence, abuse and trauma, including for resisting violence:
[We] continue to punish women for behaviours in the context of [domestic and family violence] where men are “driving” the women’s behaviour, such as sex work, theft, drug possession [and] dealing … Also convicting victims of murder [or] assault when this may be a survival tactic in the face of overwhelming male-perpetrated [violence]. (Respondent 41, Practitioner)
Respondents also related this to the incompatibility of prison with addressing underlying trauma and providing the necessary conditions for women to be able to move forward in their lives:
… addressing the “anger” behaviours rather than the traumas which often underpin the “anger response”. Band-aiding the bigger and more complex issues, also blame[s] women for their trauma responses. (Respondent 41, Practitioner)
The majority of incarcerated women are there because of drug offences. In order to stay out of prison they need to avoid drugs and drug dealers, which is very difficult to do living amongst them. (Respondent 15, Practitioner)
Post-release, there are issues of inadequate housing and a need for more comprehensive throughcare support. Again, the restriction of agency and choice for women who are or have been incarcerated was identified as a key violation of rights and a barrier to women accessing effective support. For example, mandated counselling will not be effective if the woman has not been given a choice in how or if to engage: “Parole officer insisting on counselling when woman not wanting [to] or not ready.” (Respondent 15, Practitioner)
Women living in rural and remote communities
Some of the issues identified for rural and remote communities reflect broader systemic issues around resourcing and workforce capability. However, these issues are amplified in regions where there are insufficient services to meet the needs of rural and remote communities, which also constrains choice and accessibility for groups with specific needs.
1800RESPECT is a service available to people in remote or rural localities and can direct users to local services. It cannot replace or provide services in regions where they are inadequate or absent. (Respondent 88, Service designer/manager)
… services that can meet the needs of all people who need to use services in particular services that understand and respond to disability, [LGBTQ+] and cultural needs. (Respondent 39, Researcher)
Respondents also described the unique needs of rural and remote communities, the importance of the health sector in meeting these needs, and the need for more specialist services and emergency accommodation:
[Domestic and family violence] is more prevalent and has specific effects in rural and remote localities. These specific effects include access because of transport and distances, a lack of perpetrator accountability and other issues that discourage help-seeking such as privacy concerns and shame. (Respondent 49, Practitioner)
LGBTQ+ communities
Workforce capability was a major concern, with respondents citing lack of training for staff in mainstream and specialist domestic, family and sexual violence services regarding LGBTQ+ communities. This lack of capability in supporting LGBTQ+ communities also reflects a lack of societal knowledge and awareness more broadly, as well as the pervasive stereotypes and misunderstandings within society about domestic, family and sexual violence experienced by individuals in these communities. While training is important for the workforce, there is also a need for more LBGTQ+ specific services in mainstream healthcare services as well as specialist services, particularly in regional areas: “Currently support in regional New South Wales is limited to telesupports.” (Respondent 59, Practitioner)
Culturally and linguistically diverse women and communities
Respondents acknowledged that resourcing and workforce capability were key issues for culturally and linguistically diverse communities, with one saying that “mainstream service models are underfunded and resourced to respond appropriately to [culturally and linguistically diverse women]” (Respondent 23, Service designer/manager).
Respondents also identified that there is a lack of policy frameworks supporting women and perpetrators from culturally and linguistically diverse communities, as well as a lack of specialised support services: “There is not a clear policy on how to address specific cultural factors that mediate violence against women, especially against women from refugee and migrant background[s].” (Respondent 65, Researcher)
Respondents also pointed to policy issues that impact women on temporary visas and notably prevent access to social support such as emergency payments, income support and healthcare (e.g. through Medicare). This is a substantial barrier to women leaving their relationships as the services are inadequately resourced to support their needs, as described by the following:
As a refuge we are required to pay for everything and forgo rent, for sometimes 2+ years while the visa and court processes are taking place … [We] pay for everything and we are required to find support services (e.g. migration lawyers) that work pro bono. (Respondent 86, Service designer/manager)
Women with disability and disabled women
Respondents identified the lack of accessible services for women with disability and disabled women as a key issue:
… improved access to services, meeting the needs of all clients, ensuring equitable access, removing barriers to support … [For example], using Auslan interpreters for people with hearing impairments, making sure the service meets the requirements of people with disabilities and is accessible. (Respondent 59, Practitioner)
They also pointed to how limited service options constrain choice. This can be particularly harmful for victims and survivors who engage with multiple systems such as health, housing and employment. The National Disability Insurance Scheme (NDIS) was considered to be particularly problematic, as women face multiple barriers to accessing support through the scheme, as described by this respondent:
It is exhausting/emotionally draining and very worrying. People put in a lot of effort to be frustrated several times before they are finally accepted … I’ve had so many people say, “I can’t try again. It’s too hard.” I persuade them and they usually do. (Respondent 15, Practitioner)
It also places strain on services to provide resources and supports when clients have not been able to access them through the NDIS: “Our NGO service paid $200 to access an interpreter for a client with a hearing impairment as no funding was available.” (Respondent 59, Practitioner)
What is working?
There were four main approaches that respondents perceived to be working effectively:
- advocacy and coordination of support
- multi-agency responses
- therapeutic interventions
- interventions that are specifically for children and
young people.
Advocacy and coordination
Specific advocacy and coordinated care assists women to navigate options across sectors, which enables access to support but also minimises risk of “secondary systems abuse” (Respondent 23, Service designer/manager).
Respondents identified benefits of advocacy and coordinated care, for victims and survivors but also for workers who can face burnout brought about by systems failures. Advocacy and coordinated care are most effective when delivered by workers who hold a specific advocacy role, for example case management staff, with such roles embedded in organisational structures and policies.
In some settings, specific child advocacy can be effective for supporting older children, such that they are treated as clients in their own right and additional safety planning is tailored to their developmental needs: “The boys are linked into programs such as the police and citizens youth clubs and other support groups specific to young men and boys for positive male mentoring.” (Respondent 72, Service designer/manager)
One practitioner identified Legal Aid NSW’s Women’s Domestic Violence Court Advocacy Service (WDVCAS) as an example of an effective advocacy program. The WDVCAS is delivered through locally based, non-government service providers. The program provides information, advocacy and referrals to assist women and their children with their legal, social and welfare needs, including obtaining legal protection through applications for apprehended violence orders (AVOs) and providing referrals for services such as housing, counselling, financial assistance or health services.
Multi-agency responses
Respondents held multi-agency responses in high regard and identified current approaches that are considered to be promising, including co-location of services (e.g. Health Justice Partnerships) and the NSW Department of Communities and Justice Safer Pathways program. Such programs enable collaboration between services, with efficient information sharing to enhance safety and reduce re-traumatisation: “Safer Pathway provides a way for what I consider to be effective collaboration to happen but is more effective for cases rated as at serious threat.” (Respondent 49, Practitioner)
Therapeutic interventions
Trauma-informed therapeutic interventions were considered effective in promoting healing and recovery. Again, choice is vital, and the therapeutic relationship rather than therapeutic modality was considered by respondents to be particularly important. Respondents pointed to individual, family and group therapeutic interventions, as well as broader approaches to trauma recovery that address the embodied aspects of trauma, for example through yoga or similar.
… evidence-based therapies for trauma including complex trauma, developing secure attachments between non-offending parent and their child/ren … practices that recognise the complexity of each woman’s situation and assist them to identify their strengths, resources and coping skills while supporting them to make their own informed choices. (Respondent 30, Practitioner)
In addition to trauma-informed approaches, response-based practice was identified as an effective therapeutic way of working that frames victims’ and survivors’ responses within the context of violence and abuse, with one respondent noting: “Response-based practice has made a substantial difference to upholding dignity, locating responsibility for the person using violence and highlighting women’s resistance to violence.” (Respondent 27, Practitioner)
Likewise, therapeutic approaches that integrate trauma psychoeducation are destigmatising, and depathologise responses to trauma. This was considered to be effective in reducing victims’ and survivors’ sense of self-blame and shame.
By contrast, therapies that use exposure, requiring victims and survivors to revisit the details of the trauma, were considered potentially harmful if not undertaken appropriately and in conjunction with other therapeutic approaches: “Many clients have reported that they have found exposure therapy highly re-traumatising because it required them to repeatedly revisit the details of the trauma they experience.” (Respondent 50, Service designer/manager)
Respondents also cautioned that couples counselling and relationship services can be harmful if domestic, family and sexual violence is not recognised and understood, particularly in relationships where perpetrators use coercive control: “Couples and/or marriage counselling is meant to be for couples who are having relationship issues that do not involve using power and control behaviours over the other person.” (Respondent 28, Service designer/manager)
Family interventions described were those that work with parent(s) only or those that work with the whole family. Whole-of-family approaches were considered a promising model particularly to address reactivity, biases and harm in risk assessment and child protective services. In particular, there was support for therapeutic interventions that work with the non-offending parent to maintain a safe and stable home environment and to enable them “to continue being a capable primary carer for children, to overcome trauma and abuse” (Respondent 4, Researcher).
Family therapy brings a systemic approach whereby change created in one part of the system enables further change to take place. This approach takes into account the impact of early relational trauma, intergenerational trauma and disruption in attachment between family members: “In working with children, the system must also be considered i.e. family, school.” (Respondent 87, Service designer/manager)
One respondent described a narrative family therapy framework, in which change is made to the sense of meaning that the family brings to their experience: “The whole family is strengthened … to create new meaning and potentially a new narrative around the family, who they are and where they are heading.” (Respondent 89, Practitioner)
This respondent contrasted this framework with the dominant individual therapy paradigm, cognitive behavioural therapy (CBT), which focuses on the relationship between the thoughts, feelings and behaviours that someone has about themselves as an individual and their experience:
While [CBT] can have good effect with symptom management, it does not address deeper levels of meaning and experience. Furthermore, even though there is a trauma-focused CBT framework, it’s [sic] focus tends to be limited to the individual and their specific experience as opposed to their broader relational world. (Respondent 89, Practitioner)
Therapeutic interventions that are delivered in groups were considered effective in building connection and compassion through shared experiences. Furthermore, validation and support derived from group experiences can be helpful in rebuilding a sense of trust and increasing understanding of the complexity of domestic, family and sexual violence.
Typically, such interventions are delivered in a weekly format for a defined time period and consist of facilitated group discussion and education modules developed by specialist staff using evidence-based strategies. The interventions are delivered by trained facilitators “who have understanding on how coercive control behaviours influence women’s options and choices, [and] how women’s strengths and resistance are a way to reclaim back human rights.” (Respondent 27, Practitioner)
Access to group interventions is enabled by reducing barriers, such as providing them for free or at low cost for participants and providing onsite childcare. In some group interventions, additional individual counselling sessions and the support of a case worker are also offered.
Children and young people–specific interventions
For children and young people who are victims and survivors, respondents emphasised that effective interventions must overcome barriers to engagement by using innovative approaches that are responsive to their needs, such as art, music, play therapy and other somatic therapies (e.g. animal-assisted therapy). These interventions should address relational trauma and attachment, emotional regulation and awareness, and incorporate psychoeducation aimed at understanding “abusive behaviour [and] safety planning to know how to respond when unsafe situations occur” (Respondent 4, Researcher).
Additionally, “responses need to be developmentally appropriate, relational, trauma informed and cognisant of attachment processes [and] disruptions” (Respondent 89, Practitioner).
Brief interventions that can be delivered during periods of crisis were considered promising and can be useful in overcome lengthy wait times, in that they can be delivered to those on wait lists for long-term counselling. For example, the Bouverie Centre model offers free counselling services to children who have experienced family violence. The model includes child-centred single sessions as well as access to therapeutic group sessions. The single sessions are tailored to families in crisis who are unable to commit to or are on a waitlist for longer-term counselling:
The model has one children’s counsell[or] working with the child and another children’s counsellor working with the mother. Then they come together to engage in a facilitated conversation between mother (caregiver) and child … developing a safe space for the child to express their feelings and concerns. The process may be over a few sessions rather than one session depending on the individual’s circumstances including safety. (Respondent 37, Service designer/manager)
The purpose of the session is to provide an interim response for children who require longer-term counselling, in order to provide the caregiver and child some tools to support them in the short term until the immediate crisis is resolved. These types of approaches require therapists skilled in a number of different therapeutic models, including art therapy and play therapy. The therapist’s knowledge of family violence is critical to the success of the model and the whole of the organisation focuses on children not just as a model of practice but also in terms of creating an environment where children feel safe and “have a sense of ownership of the space” (Respondent 37, Service designer/manager).
Respondents identified examples of promising interventions for working with young people who use violence. For example, interventions for young people who engage in harmful sexual behaviour include Turning Corners and the Good Way Model, which was designed for young people with intellectual disability and a history of engaging in harmful sexual behaviour, but is also applicable to other young people who engage in sexual and other forms of violence. This model uses narrative therapy principles to assist young people to “develop a new sense of meaning as to who they are, their place in their world, their future options, their relationships with others” (Respondent 89, Practitioner).
Future directions
A number of promising approaches and interventions were identified by respondents to inform future directions (Table 4). There was acknowledgement that resourcing, workforce capability and enabling policy frameworks are key factors to be addressed across sectors and critical to this is adequate funding for services, with longer funding cycles and employment contracts to ensure workforce consistency and sustainability.
Table 4: Future directions to better support victims and survivors and children and young people experiencing violence identified by respondents with exemplar quotes
Adequate resourcing that is sustained, flexible and tailored to local contexts
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Long-term assistance to live [a] healthy life – everything is crisis related and focused on legal outcomes, not health and wellbeing.” Respondent 4, Researcher |
| “Longer-term interventions need to be available to people who have experienced family violence.” Respondent 30, Practitioner |
| “Access to income suqpport, especially for those who are on temporary visas.” Respondent 73, Practitioner |
| “Provision of appropriate and accredited interpreters.” Respondent 38, Service designer/manager |
| In custodial settings, there are multiple resourcing issues that need to be addressed to ensure better throughcare support, particularly for housing and employment In recognition that most women in prison have trauma histories, there is a duty of care to provide a trauma-informed environment that is conducive to recovery and healing | “A support worker who spends time with the client/prepares a resume/finds out what sort of work [the] woman would be comfortable doing and goes out to find opportunities. Offers support in the early days, perhaps negotiating short days to start with.” Respondent 15, Practitioner “Programs that allow animals in prisons, birds, dogs etc. Humanise the prison environment and encourage connectedness and care.” Respondent 41, Practitioner “Intensive support where desired for women leaving prison who have experienced and/or are at risk of domestic and family violence.” Respondent 59, Practitioner |
Enhanced workforce competency, capability and collaboration across sectors
| Future direction | Respondent |
|---|---|
| The health sector is an important resource, particularly in rural and remote regions. Respondents suggested increasing training for general practitioners (GPs), hospital staff and the allied health workforce – for example, expanding Multi-Agency Risk Assessment and Management Framework (MARAM) and/or Safe & Together training for these clinicians A promising Victorian example that may be appropriate for other states is the Strengthening Hospital Response to Family Violence, which educates healthcare workers to identify and care for women experiencing family violence | “Whole-of-hospital approach to educate staff in how to sensitively enquire about family violence and in what to do when a woman discloses. Led by the Royal Women’s Hospital, it is a program that builds capacity across all hospitals in Victoria.” Respondent 83, Service designer/manager |
| Respondents identified the need for:
| Further funding and training in this space to support same-sex perpetrators of [domestic and family violence] would be beneficial.” Respondent 2, Practitioner “Displaying signage that shows support for all community members, including rainbow flag, using pronouns on email signature.” Respondent 59, Practitioner |
| “Community education about sexual assault of older women. Ensuring older women and their advocates know they can speak out and be supported.” Respondent 94, Practitioner |
Address housing shortages, bottlenecks and accessibility issues
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Build more crisis accommodation that uses universal design principles, so these services are fully accessible for all women including women with a range of disabilities.” Respondent 39, Researcher |
| “More social housing, better funding for refuges, consideration of housing for perpetrators are some of the issues that remain unaddressed.” Respondent 49, Practitioner |
| “Education for real estate agents with property management services to reduce bias against women experiencing [domestic and family violence] and Start Safely packages, to sustain tenancies.” Respondent 27, Practitioner |
Addressing punitive approaches in child protection through early intervention and collaboration
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Best Beginnings is a home visiting service for families of new infants. It involves regular visits to your home by caring, trained professionals who provide support, advice, information, connections and practical help. The program is structured according to your needs. The aim is to improve child health and wellbeing, parent and family functioning and social support networks. Support can come from a range of professionals including nurses, teachers, social workers and psychologists.” Respondent 92, Service designer/manager |
| “Communication as basis for identifying capacity for change … through continual assessment and centring the child/ren’s voice … What I loved about this model was how it uses really user-friendly language, worries and concerns, hopes and dreams, what’s working well, what needs to change. It looks at the perspective of the parents, the perspective of the child and the perspective of the worker. As a risk assessment framework, it enables not only workers but parents too (once shown) how they can consider risks to their family and in particular the needs of their children.” Respondent 33, Researcher |
Better responses that meet the specific needs of children and young people
| Future direction | Respondent |
|---|---|
| Schools are an important setting to provide trauma-informed support for children and young people. School counsellors and psychologists are a central resource, however they are vastly underfunded such that children with more serious behavioural issues are prioritised for counselling support. Respondents suggested there is scope to provide enhanced training for all school staff to embed principles of trauma-informed practice in schools | “Children need to have escalated behavioural issues to receive counselling and then the focus is on their behaviour at the time (present) and not the behaviour they have been exposed to.” Respondent 4, Researcher “Trauma-informed training for teachers at schools.” Respondent 76, Practitioner |
| Respondents identified the need for:
| “Bringing a child-focused lens to family violence crisis care work.” Respondent 79, Practitioner “Different programs have different motivations and praxis, but those relevant to the [domestic and family violence] field focus on family relationships and issues such as values, attachment and connections to family members and community.” Respondent 49, Practitioner |
| “It labels young people as broken and that’s wrong, it’s just they need to learn how to appropriately and safely channel their expression.” Respondent 14, Practitioner |
| “A framework that understands that relationships can be triggering/frightening and that for some young people the only way to find safety is to use violence as a protective measure … that this is not an excuse for violence, but a context in which we can understand it.” Respondent 89, Practitioner |
| “Easier to access, break down the stigma and make them more ‘youth friendly.” Respondent 52, Practitioner “In places young people already access, as well as specialist domestic and family violence settings.” Respondent 59, Practitioner |
Mobilise telehealth and digitally enabled services
| Future direction | Respondent |
|---|---|
| Respondents believed that telehealth and digital services could overcome barriers faced by rural and remote communities, such as distance or lack of services. There is the potential to establish telehealth hubs to enhance accessibility, safety and privacy for clients | “Improving opportunities for women in rural or remote areas to access counselling e.g. if there are barriers to travel such as distance, work demands or childcare concerns.” Respondent 30, Practitioner |
Enabling policy frameworks
| Future direction | Respondent |
|---|---|
| Policy was consistently identified as an area that urgently needs attention and could incorporate principles of intersectionality | “Policy needs to be framed from an intersectional perspective to identify and respond to these complexities and funding, for example, for women with disabilities in rural and remote areas needs to be flexible so additional supports and services can be accessed without compromising safety.” Respondent 39, Researcher |
National Outcome 5 – Justice responses are effective
Where are we now?
Respondents identified several key issues that impact the effectiveness of justice responses. They centred on policing, prosecution and the family law courts.
Policing and prosecution
Respondents described shortcomings in policing that result in domestic, family and sexual violence not being responded to appropriately and being under-prosecuted. Respondents acknowledged that under-resourcing is a barrier to effective policing, for example in terms of delays in police response times. However, they also identified systemic issues around information sharing, victim blaming and workforce capability that thwart justice responses and harm victims and survivors. In particular, respondents described that policing responses can be traumatising for victims and survivors when police do not have the requisite knowledge and capability in responding to reports of domestic, family and sexual violence. This includes a lack of trauma-informed approaches, including inadequate and harmful responses reported by survey respondents, such as dismissive verbal and non-verbal responses, as well as not providing the appropriate physical environment and not
providing access to specialised policing units and staff:
Police responses to disclosures of [domestic, family and sexual violence] can be problematic when they are not [trauma and violence–]informed. We hear reports of police siding with perpetrators because they seem rational and calm when interviewed in response to an incident of [domestic, family and sexual violence] (in contrast to the victim/survivor who may be heightened and distressed). (Respondent 59, Practitioner)
Eyes were rolled, blame was implied for not making reports sooner, confidentiality was not established, safety was not ensured. (Respondent 74, Practitioner)
Victim/survivors are required to tell details of their stories in a physical space that is not supportive. (Respondent 7, Practitioner)
Reports of [domestic, family and sexual violence] are not necessarily taken seriously by the police and access to the specialised units is denied or the front desk officer demands to know the full story. (Respondent 15, Practitioner)
Many victim survivors are met with an abrupt and unkind manner by the police. Are sometimes made to feel like they are not believed or are victim blamed by the police. (Respondent 52, Practitioner)
Respondents specifically highlighted that those reporting sexual violence are frequently met with disbelief and victim-blaming attitudes when first reporting to police. One respondent felt that these re-traumatising experiences are evident across the journey that victims and survivors take through “the process of reporting, police statements, forensic examinations, investigating process and court process” (Respondent 52, Practitioner).
As respondents describe it, these initial adverse experiences are then followed with lengthy trial wait times, inadequate bail thresholds, low conviction rates and sentencing outcomes that respondents perceive to be “lenient”. These issues not only increase risks to victims and survivors but also deter people from making reports: “Women or children will do the right thing by going to the police and then the perpetrator is walking free again.” (Respondent 90, Practitioner)
These issues were partially attributed to under-resourcing and high workloads, particularly in relation to length of time taken for cases to be finalised. However, there was also a sense that, in some cases, delays can be an intentional strategy by defence lawyers:
It takes far too long for cases to come to court. This is partly because police are so under-resourced and the courts are very busy, but some thought needs to be given. Defence lawyers should not be allowed to get away with endless adjournments. (Respondent 15, Practitioner)
Court process to get to these outcomes takes a substantial amount of time. This amount of time often leads to victims reconciling with offender or no longer wishing to assist judicial process. (Respondent 57, Practitioner)
These issues with reporting and prosecution can also have adverse implications for victims and survivors seeking compensation. Furthermore, respondents considered that the evidentiary requirements of applications to New South Wales’s Victims Services for compensation are onerous and lead to significant delays in processing applications:
Changes to assessment process now requires victims to take the onus [in] providing medical and reporting evidence of [domestic, family and sexual violence] incidents (previously Victims Services gathered evidence on behalf of the victim, with consent). Evidentiary requirements are also cumbersome, as the requirement for medical evidence may in some instances not allow [victims and survivors] to apply for victims’ compensation because they have not reported incidents of violence, or they did not seek medical attention. (Respondent 27, Practitioner)
Family law courts
Much of the data relating to legal and court processes was concerned with systemic issues in the family law courts in Australia. Again, some of the issues identified related to resourcing, which contributes to lengthy wait times for cases to be heard by the courts. However, respondents also noted delays due to multiple adjournments, as well as the prohibitive costs of legal representation and the challenges for self-represented litigants:
Families may have to self-represent so experience poor outcomes as can’t afford a lawyer. Often violent men are given shared care when they should not [be] due to their violent behaviour. (Respondent 48, Practitioner)
Respondents described how, in their view, perpetrators weaponise court processes, such as adjournments and concealing assets, to enact abuse and coercive control:
[The family law courts are] used as an instrument to inflict maximum disruption and harm to women and children. (Respondent 54, Practitioner)
Perpetrators using violence often block therapeutic interventions [for children] as a way of maintaining power and control over mothers. (Respondent 59, Practitioner)
While respondents asserted that family law court proceedings and/or processes are frequently a source of re-traumatisation and systems abuse for victims and survivors, they also expressed how this system specifically harms children and disregards their voices. While Independent Children’s Lawyers should enable children’s voices to be heard, respondents lamented that in practice, Independent Children’s Lawyers, along with child and family assessors in family law court proceedings, frequently do not have sufficient capability or resources to make assessments in families where dynamics of abuse and violence are complex. A primary concern was that perpetrators are frequently granted access to children at the expense of their safety and wellbeing: “Courts give violent perpetrators chance after chance – and all too often award access to men who are terrorising their children.” (Respondent 15, Practitioner)
Following the commencement of the Australian Government’s court reform legislation, the Federal Circuit and Family Court of Australia commenced operation on 1 September 2021. The Court operates in all Australian states and territories, with the exception of Western Australia. The Australian Government’s reforms are intended to address many of the inefficiencies identified by respondents and to prevent adverse outcomes and harm for families. When first proposed by the Australian Government, the reforms faced opposition and criticism from key legal stakeholder groups centring on how adequately suited the proposed reforms were to addressing many of the factors that contribute to harm and poor outcomes, particularly around resourcing and training. The impact of these reforms on addressing these deeply entrenched systemic issues, particularly for those impacted by domestic, family and sexual violence, remains to be seen given the relatively recent
establishment of the Court:
The Family Court can and should do more to hold people using violence responsible and accountable instead of punishing victims [and] survivors for reporting violence and abuse and accusing them of “alienating” children from their fathers. (Respondent 59, Practitioner)
Future directions
Respondents identified a number of specialised approaches that have been implemented in some jurisdictions in Australia and elsewhere as promising future directions (Table 5). However, systemic issues of resourcing, workforce capability and multidisciplinary responses remain and are critical to addressing harm and poor outcomes in justice responses.
Table 5: Future directions to ensure justice responses are effective identified by respondents with exemplar quotes
Trauma- and violence-informed workforce training to improve outcomes at every stage of the justice process
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Increased training and monitoring of police responses. Following up with [domestic, family and sexual violence] victims and survivors to check in on the response received.” Respondent 59, Practitioner “Magistrates are making life-changing decisions about who children will live with and/or have visitation with based on reports written by professionals with little to no understanding of [domestic, family and sexual violence].” Respondent 59, Practitioner |
| “Children are sometimes consulted and may be represented in legal decisions however often are not communicated with after on outcomes of decisions and why their views and wishes may not have been the ultimate decision.” Respondent 4, Researcher |
Increased resourcing for specialised multidisciplinary responses within and across sectors of the justice system
| Future direction | Respondent |
|---|---|
| In policing, greater resourcing relates to increasing domestic, family and sexual violence liaison officers and specialised sexual violence support workers within stations to reduce risk of re-traumatisation and improve outcomes for victims and survivors | “Sexual assault teams, counselling and mental health support workers should be available at all police stations made available for victims [and] survivors making reports.” Respondent 74, Practitioner |
| Respondents called for guidelines and legislation for implementation of information-sharing platforms to reduce re-traumatisation and enhance efficiencies | “Information-sharing imperatives (legislation and guidelines) which lack any implementation platforms [are not useful].” Respondent 20, Service designer/manager |
Increased regulation and monitoring for Independent Children’s Lawyers, report writers and other child court experts
| Future direction | Respondent |
|---|---|
| Respondents proposed introducing minimum standards for Independent Children’s Lawyers, which include annual auditing of cases through an independent review process. This should include mechanisms for ongoing monitoring and evaluation to increase transparency and consistency of Independent Children’s Lawyers’ processes, assessments and outcomes | “Should be mandatory for them to speak to all professionals and services involved with the family and to see their client at least once.” Respondent 15, Practitioner |
| Likewise, respondents suggested training, regulation and monitoring of Court Child Experts and other family report writers (independent social workers or psychologists that conduct family assessments) | “An assessment should be carried out by a highly skilled social worker or psychologist and their recommendations listened to.” Respondent 15, Practitioner |
Specialised responses to better support victims and survivors, and children and young people
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Increasing children’s safety, holding people using violence accountable, lifting the burden off mother’s shoulders (currently they are required to manage their children’s safety, this causes a great deal of emotional stress and worry for many mothers and as their ex-partner’s behaviour is out of their control, it is actually an impossible, unmanageable task).” Respondent 59, Practitioner |
| “Ensuring fair and equitable access to legal advice and representation.” Respondent 59, Practitioner |
| “Many victim survivors either choose not to go through legal process or do make a police report but does not make it to court, or perpetrator found not guilty. By witnessing and/or restorative justice process, victims and survivors have an opportunity to have their voice heard and perpetrator to take responsibility.” Respondent 52, Practitioner |
| Respondents indicated that establishment of specialist family violence courts in Victoria, which adopt a victim-centred approach, could be promising for other jurisdictions. These are an outcome of Victoria’s Royal Commission into Family Violence | “As time goes on the knowledge and expertise of the magistrates should increase and better inform their decisions. They [courts] are intended to be a place where victims can feel secure that they will be understood and action taken to keep them safe. At this stage outcomes are still patchy, but one hopes they will improve.” Respondent 15, Practitioner) |
National Outcome 6 – Perpetrators stop their violence and are held to account
Where are we now
Similar to service responses for victims and survivors, respondents identified shortcomings in perpetrator responses that centre on insufficient services to meet demand, inadequate trauma-informed support for perpetrators and a lack of housing. These issues contribute to recidivism and also increase risks for victims and survivors: “Not providing any service to perpetrators is not effective.” (Respondent 15, Practitioner)
Moreover, responses are typically focused on averting immediate risk. There is a lack of long-term supports for perpetrators, which means there is little being done to generate lasting change:
The woman might be safe for now, but the male will perpetrate the same violence against his next partner and traumatise her children. (Respondent 15, Practitioner)
Little to no support … perpetrators are often victims first. (Respondent 88, Service designer/manager)
More specifically, respondents identified that initiatives addressing perpetrator accountability are variable across jurisdictions and that inadequate responses to breaches of court orders are highly problematic. One of the issues with intervention orders is that they typically only name the main victims and survivors. Respondents indicated that it would be beneficial to also include the victim’s and survivor’s wider support network, for example other family members or new partners who may be at risk from the perpetrator. Respondents also expressed the view that there need to be more stringent conditions on intervention orders and that breaches should be addressed with stronger penalties:
Messages are sent where this sort of contact is not allowed, sometimes threatening or abusive and the police note it, maybe have a talk to the perpetrator but do not breach, or if they do, the magistrate tells the perpetrator that if it happens again, the consequences will be severe – and the perpetrator gets the message that he can get away with anything. (Respondent 15, Practitioner)
The main interventions identified by respondents were therapeutic responses, where perpetrators are mandated to attend treatment, and group-based men’s behaviour change programs (MBCPs) to reduce recidivism. Various models of MBCPs were described, including MBCPs with case management, MBCPs with support for partners and MBCPs delivered in prison settings. Respondents identified that one of the strengths across various models of MBCPs was the approach taken by facilitators. They are mindful to maintain non-judgemental, non-coercive language and to work constructively with resistance:
Accredited behaviour change programs operate from a framework of gender disparity and hope to effect change by understanding the background of individuals and raising awareness of societal elements that contribute to men’s power and control leading to abuse. (Respondent 49, Practitioner)
MBCPs that combine varied approaches, such as motivational interviewing and case management, were considered to be sufficiently flexible in their approach to enable and engage participants with varied needs:
A combination of approaches [has] worked well to support change within the program – including narrative and strength-based approaches (to relate ethical choices back into men’s life experiences and to identify positive values that can be built upon). Motivational interviewing techniques are also used by facilitators, understanding that participants may be at different stages of change. A risk–needs–responsivity approach also underpins the program delivery – identifying clients[’] varied needs and dynamic risks and responding with appropriate interventions and responses including additional supports and referrals. The flexibility of case management assists participants with varied needs to remain engaged. (Respondent 2, Practitioner)
Further, case management can overcome barriers to accessing groups that have long waitlists or for men who need specific supports to enable them to be ready for group MBCP interventions:
Case-managed interventions allow increased flexibility to engage with men who may not be suitable for group (whether this is due to parental/employment responsibilities or other reasons such as mental health or substance misuse issues). (Respondent 2, Practitioner)
Groups like MBCPs are not always suitable, or the men need a lot of one-to-one group readiness work before attending the MBCP group. There are big wait lists for MBCPs, so case management could hold the men while they wait and reduce risk factors that may be contributing. (Respondent 48, Practitioner)
One respondent commented that there is a lack of understanding of MBCPs among magistrates, which leads to inappropriate sentencing:
There have been cases following a breach of [intervention orders] where magistrates have directed men [to MBCP]who have been assessed as either ineligible/unsuitable for [MBCP] interventions (e.g. clients being aggressive towards workers or demonstrating no interest in engaging/making any changes). (Respondent 2, Practitioner)
While respondents indicated that MBCPs can be effective, there were also concerns that they are not always culturally appropriate for Aboriginal and Torres Strait Islander men and men from culturally and linguistically diverse backgrounds: “MBCPs are not accessible to many men as their first language is not English.” (Respondent 48, Practitioner) Insufficient programs are available for LGBTQ+ communities.
Additionally, there can be variability in the accountability that is required of men who attend programs. This is key, both in terms of committing to attending the sessions and being held to account for their attitudes and behaviours: “Groups where they are not challenged on their ideas and behaviours … They can put in an appearance a couple of times and get away with saying they have attended.” (Respondent 15, Practitioner)
One respondent reflected on MBCPs delivered in prisons. They indicated that these can be ineffective at reducing recidivism as they need more psychoeducation, skill-building and focus on post-release supports: “Higher focus on emotional regulation … skills workshops, increased and extended supports upon release … Incarceration without rehabilitation is punitive and does not address the problem.” (Respondent 78, Practitioner and researcher)
Likewise, another respondent reflected that such programs need to be longer and more intensive, and include mentoring or peer support: “longer-term, group therapeutic program with a peer support element” (Respondent 87, Service designer/manager).
Some MBCPs have advocacy and other support for the men’s partners, which respondents indicated was a holistic and promising model:
Support and advocate with women their basic needs including safety planning, referral to others [sic] services and supports for themselves and their children. Case support aims to provide a framework where women are in control of decision-making, identify and direct what support they require. The outcome being that women will have an opportunity to be in control of their lives and become confident in seeking support and making decisions. (Respondent 28, Service designer/manager)
A whole-of-family response is vital to achieving safe outcomes – [MBCP with partner support] working closely throughout client engagement to assess and manage risk. (Respondent 2, Practitioner)
Likewise, for Aboriginal and Torres Strait Islander men, programs that are holistic and community led were considered to be most effective: “Interventions do not rely on the cognitive behaviour change approach but in men re-connecting with culture and community.” (Respondent 35, Researcher)
In contrast to MBCPs, respondents identified that many alternatives, such as moral reconation therapy groups and anger management groups, are ineffective. Respondents indicated such interventions can increase risk in some cases, particularly as they do not use a gender lens:
Sometimes courts accept an anger management group, but it is about power and control and male privilege, not anger management … it assumes the men can’t control their behaviour. (Respondent 48, Practitioner)
It is widely accepted in the men’s behaviour change field that men do not have an innate tendency to anger and its poor management is not what drives violence against women. It does not address power and control or the fact that men can be violent or controlling when not angry and that such behaviour is selectively deployed. (Respondent 49, Practitioner)
Likewise, respondents indicated that couples counselling can be ineffective and harmful, particularly when therapists do not have capability in recognising abusive and coercive behaviours:
Relationship counselling can be ineffective in cases where a power imbalance in the relationship is not addressed. An understanding of power and control and patterns of behaviour is necessary to promote a context where each partner has equity. Failure to account for this can lead to entrenched conduct and justification and further risk to vulnerable partners. (Respondent 49, Practitioner)
It is a space where abusers can use it to further abuse the victim. (Respondent 48, Practitioner)
In terms of early intervention, respondents identified gaps in responses to young people who use violence or are at risk of using violence. As respondents described it, there needs to be greater recognition that young people who use violence are frequently also victims and survivors who have had early adverse experiences and complex family dynamics. While diversionary interventions are promising, there also needs to be early intervention that focuses on promoting safety and wellbeing for these young people as opposed to focusing only on averting risk: “Diversion systems that expect young people to complete a three-month treatment program, or 10 sessions funded by Medicare, is [sic] simply inadequate.” (Respondent 14, Practitioner)
Future directions
Respondents identified promising future directions that expand the focus from averting risk to generating lasting behavioural change. While respondents felt it was important that justice responses are consistent and hold perpetrators to account, they also identified the need for more alternatives to criminal justice responses, including deterrence measures and strengthening therapeutic responses so that these better meet the diverse needs of perpetrators and families (Table 6).
Table 6: Future directions to stop perpetrators using violence and hold them to account identified by respondents with exemplar quotes
Address inconsistencies in holding perpetrators accountable
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Enforcing harsher penalties for those convicted of breaching [intervention orders].” Respondent 57, Practitioner “Police prosecuting any breach plus magistrates taking it seriously and imposing suitable consequences.” Respondent 15, Practitioner |
| “Close working relationship between [MBCP] providers and the criminal justice system (in progress at present) to increase understanding of program objectives and scope.” Respondent 2, Practitioner |
Investigation and implementation of promising deterrence measures to reduce risk of recidivism
| Future direction | Respondent |
|---|---|
| Respondents noted that deterrence devices, such as personal safety alarms, have shown promise in reducing recidivism and breaches of intervention orders | “Implementing as originally intended as a perpetrator deterrence device in conjunction with police, based on a pilot study … had a 98 per cent success rate in preventing AVO breaches for high-risk women.” Respondent 8, Practitioner |
Strengthen therapeutic interventions for perpetrators
| Future direction | Respondent |
|---|---|
| Respondents identified the need for:
| “Culturally sensitive family violence services for men (perpetrators) from a [culturally and linguistically diverse] background.” Respondent 48, Practitioner |
| “As with group work and case managed (face to face) meetings, remote working would support men who want to engage to address their choice to use abusive and violent behaviours – most likely via an online platform.” Respondent 2, Practitioner |
| “Counsellors have to be vigilant and call out the perpetrators when [they] try to normalise or trivialise their behaviour.” Respondent 16, Researcher “All psychologists and counsellors need to have raised awareness of the dangers of family violence and counselling with couples. They need raised awareness of how to identify signs/red flags of family violence.” Respondent 48, Practitioner |
| “It is co-facilitated by a male and a female to model effective and equal communication between males and females … Sometimes there is a corresponding female group which acts as a control group reporting on how and if change is occurring in the home.” Respondent 15, Practitioner |
| “Look to what works in other countries. Therapeutic court interventions work.” Respondent 14, Practitioner “In Victoria there is already a system including specific legislation [therapeutic treatment orders] and treatment services [Sexually Abusive Behaviours Treatment Service] that works in hand with the justice response.” Respondent 89, Practitioner |
Key themes
We generated five key themes that reflect workforce perceptions of what is needed to address domestic, family and sexual violence and better support victims and survivors, children and young people and perpetrators. These are contextualised and expanded with reference to literature that examines system and service responses to domestic, family and sexual violence.
Addressing upstream determinants of domestic, family and sexual violence
This theme points to the need for greater investment in addressing upstream determinants of violence and abuse. Enacting an upstream approach means addressing structural barriers that create and sustain multiple and intersecting forms of inequality, which are root causes of violence and abuse in our relationships, families, schools, workplaces and communities. In practical terms, respondents identified key social determinants that require an upstream approach, with the primary ones being poverty, equal participation in the workforce, and safe and affordable housing: “A public health approach is required”, including “a stronger focus and resources on prevention” (Respondent 46, Researcher).
Equal and fair participation in the workforce in Australia has the power to change structures, norms and practices that ultimately drive violence (Our Watch, 2022b). The gender pay gap in Australia is the result of gender inequality and perpetuates the devaluing, exclusion and marginalisation of women (Our Watch, 2022b). To address this, the social and economic factors facilitating the gender pay gap need to be addressed, as do attitudes towards women in the workplace. In 2017, the National Community Attitudes towards Violence against Women Survey (NCAS) found that 14 per cent of respondents did not believe women were as capable as men in politics, 14 per cent believed men were more capable bosses, 24 per cent did not see an issue with sexist jokes, 40 per cent felt women exaggerated inequality between men and women, and 10 per cent did not think discrimination against women in the workplace was an
issue (Webster et al., 2018).
Women are more likely than men to experience direct and indirect discrimination in the workplace because of pregnancy, breastfeeding, carer responsibilities or relationship status. Discrimination contributes to the factors facilitating the gender pay gap and sexual harassment in the workplace (Our Watch, 2022c). Sexual harassment includes any unwanted or unwelcome sexual behaviour that it is reasonable to assume will offend, humiliate or intimidate (Australian Human Rights Commission, 2022). Workplace sexual harassment is highly gendered. Between 2017 and 2018, 23 per cent of women were sexually harassed at work compared to 16 per cent of men, and the majority of perpetrators (four in five) were male (Gebicki et al., 2018). Some women are more vulnerable to sexual harassment in the workplace, including Aboriginal and Torres Strait Islander women, women with disability or disabled women, LGBTQ+ people and young women (18 to 24
years; Gebicki et al., 2018). Women are more likely to experience sexual harassment in workplaces that are
male -dominated (Gruber, 1998; Saunders & Easteal Am, 2013). This was demonstrated in a review of the treatment of women in the Australian Defence Force Academy, which found that 71 per cent of female cadets experienced sexual harassment, compared to 30 per cent of male cadets (Australian Human Rights Commission, 2011).
In addition to workplace harassment and discrimination, experiencing violence outside the workplace can directly or indirectly be a barrier to victims’ and survivors’ full and equal participation in the workforce (Moe & Bell, 2004). For some victims and survivors, experiencing violence is associated with unstable employment (Adams et al., 2012; Crowne et al., 2011; Moe & Bell, 2004; Staggs & Riger, 2005). This can be the result of abusive tactics that directly interfere with employment, such as harassing victims and survivors at their place of work, or interfering with the process of upskilling for or finding a job (Adams et al., 2012). Indirectly, the physical and mental health consequences of violence can lead to time off, frequent job changes and decreased job satisfaction (Crowne et al., 2011; Moe & Bell, 2004; Riger et al., 2004; Tolman & Wang, 2005). The impact of violence on job stability can persist long
after the abuse has ended (Crowne et al., 2011). Additionally, without a stable income, victims and survivors are less likely to have the economic resources required to leave a perpetrator (Adams et al., 2012; Cortis & Bullen, 2016). In Australia in 2020–21, 51 per cent of employers offered paid domestic violence leave, a fourfold increase from 2015 (Workplace Gender Equality Agency, 2022a). Not only does this type of leave provide victims and survivors with some financial stability when leaving a perpetrator, but when organisations adopt it, it represents their commitment to staff wellbeing and raises awareness of the impacts of violence on employment (Breckenridge et al., 2015).
Respondents’ views on housing are in line with literature that argues it is a key determinant in addressing domestic and family violence (Braaf & Meyering, 2011; Cortis & Bullen, 2015; Webster, 2016): “Housing is one of the biggest barriers to resolving the effects of [domestic and family violence] on victims.” (Respondent 49, Practitioner)
In 2020–21, 42 per cent of specialist homelessness service clients had experienced family or domestic violence (Australian Institute of Health and Welfare, 2021d). Since 2011–12, this number has increased annually (Australian Institute of Health and Welfare, 2021d). The majority of these clients were returning clients, and domestic and family violence was the main reason they were seeking support (Australian Institute of Health and Welfare, 2021d). Following domestic and family violence, loss of housing ownership, limited access to affordable social and private rental housing, and discrimination in the private rental market make it difficult for victims and survivors to access safe and affordable housing (Cortis & Bullen, 2015). Some victims and survivors do not have rental history or have poor rental history because of continued abuse or threats that require them to break leases and/or regularly relocate (Braaf & Meyering,
2011).
In line with the National Plan and the Fourth Action Plan, the Commonwealth Government introduced a “Keeping Women Safe in their Homes” initiative to enable women and children to remain in their home or a home of their choosing (Department of Social Services, 2021). The programs implemented as part of this initiative offer long-term and wrap-around support, case management and ongoing safety planning (Breckenridge et al., 2016). This departure from traditional crisis interventions is seen as a strength because victims and survivors are impacted by violence long after they leave the perpetrator (Breckenridge et al., 2016; Diemer et al., 2017). However, this initiative is only suitable for victims and survivors who will not be at risk of further violence by remaining in their home, and is not successful without proactive action from police and courts to monitor perpetrators and enforce protection orders (Breckenridge et al., 2016;
Diemer et al., 2017).
Reactivity and inequity in responses harms victims and survivors
This theme speaks to the need for systemic changes that address the full spectrum of prevention, early intervention, response, and recovery. Respondents emphasised that the system is set up to be reactive to incidents of violence, with less resourcing and capability for early intervention and prevention. This reactivity impacts, in particular, Aboriginal and Torres Strait Islander peoples and communities, with one respondent noting: “We have another stolen generation through Child Protection. We need to strengthen families, do more prevention community work … less reactive responses.” (Respondent 48, Practitioner)
Further, beyond crisis intervention responses that focus on immediate safety, respondents identified that there are gaps and bottlenecks in responses that focus more on long-term recovery and transitions. This largely relates to a lack of services and referral pathways, which is compounded in regional and remote areas and for people who face additional structural barriers to accessing support, including racism, ableism and ageism. The effect of this is that many perpetrators and victims and survivors are not able to effectively move forward from violence and abuse – the cycle repeats, with continued strain on crisis intervention services as well as the criminal justice, health and child protection systems. “[We need] a system that believes the [victim and survivor] has right to and provides safety and recovery.” (Respondent 10, Practitioner)
This theme also relates to issues of traumatisation, re-traumatisation and ineffective responses that harm victims and survivors. These systemic issues can also manifest in inadequate responses and lack of services for perpetrators, which ultimately increase harm and risk for victims and survivors.
Respondents acknowledged systemic issues are closely related to inadequate resourcing and limited funding, which results in narrow eligibility criteria for accessing services and rigid key performance indicators that are determined by funders and do not reflect community need. The implications of this in practice are long wait times and lack of choice, which are not only harmful but can also perpetuate trauma and deprive victims and survivors of agency:
As a worker I struggle sometimes getting in touch with [domestic, family and sexual violence] services, often nobody answers, needing to leave messages, sometimes days go by without a response. I can only imagine what this experience would be like for women calling for support … Also, the wait lists can be very long, I’ve had clients wait over one year for case management support. (Respondent 52, Practitioner)
It is vital that contact is made quite quickly and the [victim and survivor] does not have to wait. (Respondent 15, Practitioner)
Importantly, respondents linked these systemic issues around resourcing and workforce capability with poor coordination and inadequate responses that contribute to victims’ and survivors’ resource deprivation, isolation and traumatisation. This is consistent with workforce perspectives in the 2017 National Survey of Workers in the Domestic, Family and Sexual Violence Sectors (Cortis et al., 2018). Only 38 per cent of respondents felt their service was adequately staffed and four in five felt their services were inaccessible (Cortis et al., 2018). In particular, respondents felt there were limited service options for perpetrators, Aboriginal and Torres Strait Islander communities, young people, rural communities and people seeking housing support (Cortis et al., 2018).
Further, these reports of limited service options align with victim and survivor accounts (Evans & Feder, 2016; Kiamanesh & Hauge, 2019; Peckover, 2003; Robinson & Spilsbury, 2008). Victims and survivors who accessed specialist services reported access to support was difficult unless experiencing a crisis or homelessness (Evans & Feder, 2016). Resources such as shelter or informal support were rarely offered to victims and survivors despite disclosure and histories of mental health issues related to violence (Evans & Feder, 2016). Culturally and linguistically diverse women in a shelter reported that support services did not improve their situation because they were not tailored to their specific needs (Kiamanesh & Hauge, 2019). They described the help offered as a burden (Kiamanesh & Hauge, 2019). Similar results were seen in qualitative studies of victims and survivors accessing mainstream health
services (Peckover, 2003; Robinson & Spilsbury, 2008).
The traumatisation and re-traumatisation of victims and survivors and simultaneous deprivation of resources can lead to “loss spirals” (Schmidt, 2014). These can be considered in the context of conservation of resource theory, which is based on the idea that psychological reactions to stress such as trauma are related to accompanying social, economic and interpersonal resource loss or the threat of loss (Hobfoll, 2001; Hobfoll & Lilly, 1993; Schmidt, 2014). Trauma then exacerbates further loss, leading to these loss spirals (Hobfoll & Lilly, 1993; Schmidt, 2014). As such, individuals with fewer resources when they experience a stressor are more vulnerable to a greater and faster loss spiral (Hobfoll & Lilly, 1993; Schmidt, 2014). When services reinforce a stressor or deprive victims and survivors of resources, it replicates the context of violence and abuse and exacerbates loss spirals (Adams et al., 2008; Bybee &
Sullivan, 2002; Sullivan & Bybee, 1999; Sullivan et al., 2002). Equally, services that do support victims and survivors to access resources lessen the mental health impacts of violence and/or support recovery (Beeble et al., 2010; Coker et al., 2003; Schmidt, 2014).
There was much consideration of gender inequality by respondents, and how the impacts of gender inequality are not felt equally by all. Furthermore, binary notions of gender that are the foundations of gender inequality discourse are problematic and can disregard or marginalise the experiences of non-binary, gender-diverse or non-cisgender individuals. Moreover, respondents detailed systemic biases that impact those who experience multiple forms of discrimination and advocated that an intersectional lens must be applied to address systems abuse. While there is awareness that systems abuse disproportionately impacts those who experience intersecting axes of oppression, and intersectional approaches are referenced in policy and practice guidelines, this is largely still a poorly understood framework. As respondents identified, it is also not well operationalised in practice: “[We need] intersectional approaches to intervention – each survivor is
understood and what unique challenges they have because of systems that are, for example, racist or homophobic.” (Respondent 73, Practitioner)
This is indicative of the need for a trauma- and violence-informed system that considers the intersecting experiences of oppression, power and privilege. Trauma- and violence-informed care acknowledges that people who experience systemic inequities and structural violence will have experienced multiple and intersecting forms of trauma that extend beyond traumatic events or interpersonal trauma (Browne et al., 2017; Browne et al., 2012).
Critical to embedding trauma- and violence-informed approaches is recognition of the historical and contemporary violence of colonisation. This requires understanding trauma as intergenerational and influenced by systemic inequities and structural violence. As such, the focus is on validating and recognising strengths in the context of trauma and establishing lifelong healing as well as preventing re-traumatisation (Browne et al., 2017; Browne et al., 2012). Key to embedding trauma- and violence-informed care across the system is workforce capability, coordination and collaboration (Carlson et al., 2021; Cullen, Mackean, et al., 2021; Cullen et al., 2020). This can include strengthening partnerships, multisectoral responses and coordination, for example through streamlined information sharing between services and sectors or advocacy to influence policies or available services in a community (Browne et al., 2012).
Changing harmful understandings of domestic, family and sexual violence that can entrench victim blaming
This theme amalgamates respondents’ views that knowledge and cultural shifts are required to better conceptualise domestic, family and sexual violence, so that our understandings consider the intersection of violence within the broader context of structural and social determinants. Respondents asserted that harmful understandings of domestic, family and sexual violence contribute to victim blaming. In practice, this results in responses and outcomes that do not hold perpetrators to account for their use of violence and can further victimise and traumatise victims and survivors. In particular, respondents identified welfare and child protection frameworks that pathologise and harm victims and survivors:
Traditional welfare models often pathologise the victim and do not emphasise a rights-based approach. They may also collude with offenders. The criminal justice system has a significant role to play but these systems offer work counter to the needs of victim survivors. (Respondent 23, Service designer/manager)
There were concerns that such frameworks frequently blame non-offending parents, typically mothers, for not keeping children safe rather than focusing on the person using violence in the home:
When women come into the refuge space, they are supported with child protection services, amongst other services. But the perpetrator soon becomes invisible and it all becomes about her and her behaviour. Was she a protective mother? Does she have [mental health] issues that impact her parenting and is her [alcohol and drug] use damaging to the children. We should be pivoting back to the perpetrator. That is, how did his actions impact on her functioning and family ecology? (Respondent 86, Service designer/manager)
There was a nuanced relationship between perpetration and victim blaming when it comes to young people who use violence. Respondents indicated that young people’s actions are often not sufficiently conceptualised in the context of their history of experiencing violence and abuse. As one respondent put it, when young people are charged and prosecuted for their behaviour:
It is shaming and blaming and as a result feeds into the dynamics that have likely led that young person to engage in the violent behaviour … it is punitive and pays little mind to a young person’s developmental status or history of trauma. It does not in and of itself offer a young person a different way of being, the potential to develop a new way of relating. (Respondent 14, Practitioner)
Victim blaming and narrow conceptions of violence and abuse were also considered in the context of coercive control. Recent debates around the criminalisation of coercive control have shed much light on the challenges around understanding, identifying and responding to perpetrators and victims and survivors (Fitz-Gibbon et al., 2020; Smyth et al., 2021; Wangmann, 2020). One of the challenges with widespread community understanding of coercive control is the commonly held incident-based understanding of domestic, family and sexual violence that fails to consider the evolving, cumulative and individualised nature of coercive control (Joint Select Committee on Coercive Control, 2021; Smyth et al., 2021; Women’s Safety and Justice Taskforce, 2021). Another related challenge is the issue of misidentification of the primary victim and the risk of systems abuse by the perpetrator (Joint Select Committee on Coercive Control, 2021; Smyth et al.,
2021; Women’s Safety and Justice Taskforce, 2021): “The lack of recognition/prosecution for coercive control and an ability to evidence it often means women’s statements aren’t proceeded with and police/judicial practices don’t support women.” (Respondent 27, Practitioner)
In order to overcome these challenges, states that are criminalising coercive control have committed to ensuring public education on coercive control is a central element of the legislative process (Joint Select Committee on Coercive Control, 2021; Smyth et al., 2021; Women’s Safety and Justice Taskforce, 2021). However, there needs to be sufficient time, training and resourcing, and despite assurances to the contrary there are community concerns that legislation to criminalise coercive control has the potential to harm rather than protect victims and survivors. This relates to the known intersections between coercive control and other societal systems of oppression and violence, and in particular the disregard for, discrimination against and criminalisation of Aboriginal and Torres Strait Islander women.
An alternative model proposed by respondents to overcome systemic biases and misconceptions was the “social entrapment” model. The social entrapment model avoids victim blaming by recognising intersecting structural and social determinants that underpin the perpetrator’s ability to enact violence and the safety responses available to the victim (Douglas et al., 2021; Ptacek, 1999). Applying the social entrapment model as a framework to conceptualise experiences of violence has potential to promote holistic responses that better meet the needs of victims and survivors (Douglas et al., 2021; Ptacek, 1999; Tolmie et al., 2018). One respondent outlined key considerations in this model:
Understanding the pattern of harm over time, with an emphasis on coercive control … Realistically looking at what safety options exist, rather than assuming them … Seeing structural inequities as essential to understanding not only the victim’s circumstances and the perpetrator’s behaviour, but also the social response (the service system, options for safety, community attitudes, practitioner responses) as a whole. (Respondent 48, Practitioner)
In terms of service responses that address misconceptions and misattribution of blame, several respondents identified the Safe & Together model. A child-focused model, Safe & Together is based on three principles that prioritise the safety and wellbeing of children: keep children safe and together with non-offending parents; partner with the perpetrator and hold them accountable; intervene with the perpetrator to reduce risk and harm to children (Safe & Together Institute, 2020).
The critical components of the model involve gaining a deeper understanding of the patterns of coercive control and the harmful actions of the perpetrator; adverse impacts on the child; the role of substance use, mental health, culture and other socio-economic factors; and the protective role of the non-offending parent (Safe & Together Institute, 2020). This model originated in the United States and has been implemented in the United Kingdom, Scotland and Australia. The model (originally designed for child protection settings) has recently been adapted to the context of Australia’s family law system and the roles performed by those court officials and judicial officers with training delivered to judges, registrars and Court Child Experts within the Federal Circuit and Family Court of Australia. Safe & Together was highly regarded by respondents as it creates a shared language, understanding and collaborative practice aimed at supporting
the non-offending parent:
This child-centred model derives its name from the concept that children are best served when we can work toward keeping them safe and together with the non-offending parent (the adult domestic violence survivor). The model provides a framework for partnering with domestic violence survivors and intervening with domestic violence perpetrators in order to enhance the safety and wellbeing of children. (Respondent 48, Practitioner)
… recognised in Australia and internationally as a way to address siloing of information between services. It creates a common language and focus for all stakeholders including police, magistrates, family court, counsellors, [domestic violence] services, legal services and child protection. The perpetrator mapping tool shifts focus to the perpetrator. (Respondent 8, Practitioner)
Underpinned by the social entrapment model, Safe & Together averts victim blaming through a strengths-based approach that focuses on recognising and strengthening “the protective behaviours of the mother” (Respondent 52, Practitioner). Additionally, accountability for perpetrators is key and this is accompanied by practical supports to make meaningful change toward being a safe and capable parent: “Holding them accountable towards every step towards change, recognising unhealthy patterns.” (Respondent 33, Researcher)
Enabling choice and the right to self-determination
This theme draws on approaches that counter assertions within the previous three themes that systemic biases, inequities and victim blaming constrain choice and resourcefulness that are essential for victims and survivors. Indeed, respondents assert that the systems that are intended to enable safety and agency can entrench victims’ and survivors’ isolation, mistrust and helplessness.
[Victims and survivors] need to be treated with respect and made aware of their rights in order to help them recover. When this does not happen, they are mired in their sense of worthlessness. (Respondent 15, Practitioner)
While resourcing is an issue that constrains choice, respondents also pointed to widespread inconsistencies in access to supports that stem from limited and inconsistent access to appropriate information about rights and options. Respondents attributed this to shortcomings in workforce capability and knowledge, and this also reflects the need for broader systemic shifts toward trauma- and violence-informed responses, which promote choice, dignity and agency.
[We need] clearer information given to [victims and survivors] about the whole process so people can make informed choice[s]. (Respondent 52, Practitioner)
This perpetuates feeling of helplessness and just being someone things are done to rather than [an] adult with agency. (Respondent 15, Practitioner)
In order to enable choice for victims and survivors, gender sensitive and trauma- and violence-informed service models are essential (Oram et al., 2022). Respondents identified that the Victorian Centres Against Sexual Assault (CASA) is such a model, which seeks to enable victims’ and survivors’ choice and self-determination. Since 1990, 15 CASA have been established in Victoria to ensure victims and survivors of sexual assault and family violence have access to responsive, comprehensive and safe support and interventions. The services offered by CASA include 24-hour crisis care, advocacy, counselling, referrals and therapeutic treatment services for young people with sexually abusive behaviours. CASA are also involved in workforce development training, school safety programs and research projects.
The CASA model is underpinned by the victims’ rights model of justice, which acknowledges the link between rights, empowerment and long-term healing for victims and survivors of sexual assault. This model is non-punitive and focused on crime prevention and restorative justice (Roach, 1999). It is based on the idea that, when successful, it helps to foster stronger communities through a process of healing, compensation and restorative justice (Roach, 1999). Underpinned by this model, CASA work to centre and empower victims and survivors with rights and choices (Centres Against Sexual Assault Forum, 2014). They are also committed to collaborative decision-making and long-term healing (Centres Against Sexual Assault Forum, 2014). As one respondent describes it:
Knowledge and understanding of the individual, cultural, social and universal context of the lives of women and children is fundamental. The framework therefore acknowledges that CASAs respond to the presenting issues of sexual assault and to the victim[s’] and survivors[’] individual experience of it. This includes the emotional, psychological, developmental, economic and social consequences relating to the sexual assault. The CASA model places importance on the valuing of clients’ experience, strengths and skills. (Respondent 50, Service designer/manager)
Key to the CASA model is providing timely treatment and choice. The counselling and therapeutic models are centred around principles of feminist practice (Centres Against Sexual Assault Forum, 2014). These principles include empowering through choice and options, believing and validating experiences, reframing and reinterpreting abuse, and non-judgemental language. Equally, a central goal of the crisis care is facilitating victims’ and survivors’ choice and control over outcomes (Centres Against Sexual Assault Forum, 2014):
Regaining of control via informed decision making. Management of health issues that may arise as a consequence of being raped. Personal advocacy which diminishes the risk of secondary systems abuse … provided with information and is supported to implement decisions that she makes. (Respondent 23, Service designer/manager)
Through immediate delivery of services subsequent to a [sexual assault] the victim’s sense of control can start to be rebuilt. (Respondent 23, Service designer/manager)
Indeed, respondents emphasised how critical choice and self-determination are for victims and survivors. Importantly, respondents asserted that these can be further constrained for those for whom mainstream services do not adequately meet needs for cultural safety, inclusion and accessibility:
Ideally the service is trained in accessibility, cultural competency and inclusion. It is also important that referral pathways are in place for community-controlled services so groups such as Indigenous women or LGBTQI+ people have a choice which service to engage. (Respondent 49, Practitioner)
For Aboriginal and Torres Strait Islander communities, self-determination draws on decolonising approaches, which are critical to enabling community-owned and -led solutions. Respondents identified highly regarded approaches that take a decolonising approach and as such are grounded in self-determination. One respondent described how this is embedded within Marninwarntikura Women’s Resource Centre in Fitzroy Crossing, Kimberley, Western Australia:
Marnin is based on Bunuba country and works from within law and culture. It covers the spectrum of women’s needs, it has a legal service and a refuge, but places emphasis on community-led initiatives and strengthening culture. It engages Elders in a leadership role and focuses on intergenerational trauma rather than simply male power. It takes an explicitly decolonising approach … It ensures that cultural knowledge leads in the creation of interventions, there is a belief that culture must lead interventions. For example, decision-making often takes place on country, where Aboriginal knowledge takes precedence over mainstream knowledge. The various clan and language groups are all represented, often with women Elders in a leadership role. (Respondent 35, Researcher)
The importance of self-determination is seen in Aboriginal and Torres Strait Islander–led policy and reviews on what works in response to family violence (Carlson et al., 2021; VACCA et al., 2019; Victoria Department of Health and Human Services, 2018). State-based family violence policies such as Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families (Victoria Department of Health and Human Services, 2018) and the Nargneit Birrang framework (VACCA et al., 2019) centre self-determination as a guiding principle. The Nargneit Birrang framework is a Victorian holistic healing framework for family violence. Other key principles in
the Nargneit Birrang framework include safety as a priority; embedding culture, Country and community in healing; the past impacts on the present; trauma-informed healing; and resilience and hope (VACCA et al., 2019).
The importance of community-based and culturally safe services has been emphasised in policy, research and advocacy by Aboriginal and Torres Strait Islander scholars (Longbottom, 2019; Porter et al., 2021). A review of Aboriginal and Torres Strait Islander family violence programs found that self-determination is a key factor in healing (Carlson et al., 2021). A review examining what works in responses to family violence from the perspectives of Aboriginal and Torres Strait Islander women and communities similarly emphasised that Aboriginal and Torres Strait Islander peoples play a significant role in the development of effective and culturally safe responses (Olsen & Lovett, 2016). This was echoed in a qualitative study on the experiences of Aboriginal and Torres Strait Islander women’s engagement with legal and social family violence services (Langton et al., 2020). This study found that culturally safe care, that was appropriate and accessible,
was in most cases provided by Aboriginal and Torres Strait Islander–specific services (Langton et al., 2020).
Power of connection, collective healing and compassion
This theme emphasises that experiences of violence, abuse and trauma are unfortunately common, and our shared experiences bring opportunities for connection and compassion, which are fundamental to healing for individuals but also for collective healing. Respondents were clear that while there are systemic issues that can be powerful in enacting and compounding victims’ and survivors’ experiences of trauma, there are also systemic strengths that are powerful in generating healing and recovery.
For services and practitioners working with victims and survivors, creating a sense of safety through hearing and believing their experiences is imperative. This is especially true for those working with children and young people.
… to enhance personal safety and control, to enable people to process their trauma effectively … without further violence and without the economic and social disadvantage that can inhibit their recovery. (Respondent 87, Service designer/manager)
In terms of healing and recovery, one of the workforce’s main strengths lies in its relational capacity, with many members highly skilled in compassionate and trauma-informed responses. Building therapeutic relationships is a key aspect of healing from violence (Flasch et al., 2015; Sinko et al., 2021). This enables victims and survivors to feel safe, build support networks and cultivate a feeling of belonging (Sinko et al., 2021). Additionally, such relationships are akin to “walking beside” victims and survivors, which is important in not only preventing systems trauma and responding to crisis, but also in supporting healing in the longer term (Cullen, Stevenson, et al., 2021). This is echoed in a qualitative study of women with a history of sexual violence and mental health difficulties, in which women identified that their healing journey was enhanced by supportive counselling within holistic models of care that fostered a sense of
connection (Hegarty et al., 2017). As one respondent affirmed, the therapeutic relationship and providing the right support at the right time are critical in recovery and healing:
Rapport between therapist and client is vital. To go at client’s pace. Allow the client control – don’t try to force client to tell story too early … To introduce formal therapy when client ready, ideally graded exposure but it is important to recognise that many clients never reach this stage. (Respondent 15, Practitioner)
Respondents emphasised that therapeutic interventions focusing on embodied, relational and attachment approaches were important, as were narrative therapy approaches that enable victims and survivors to make sense of their experiences and integrate these within the narrative of their life experiences:
Trauma-focused CBT is better than traditional CBT. I’m not convinced it’s really the best way to go in the family violence/harmful sexual behaviour realm, as it does not take into account the impact of early relational trauma, intergenerational trauma, attachment disruption. (Respondent 89, Practitioner)
Current evidence supports a much broader approach to supporting trauma recovery, including yoga etc. (Respondent 8, Practitioner)
Further, respondents identified that psychoeducation is important in validating victims’ and survivors’ experiences of violence, abuse and trauma, as well as facilitating understanding of responses to trauma. This aligns with evidence that psychoeducation is a key point of best practice for complex trauma as it allows victims and survivors to understand how trauma has impacted their lives (Salter et al., 2020). Helpful psychoeducation topics include normalising responses to trauma, identifying and responding to triggers, naming and understanding abusive relationships and tactics, healthy relationships, and safety planning (Salter et al., 2020). “To provide psychoeducation on trauma – absolutely vital. To teach strategies to deal with intrusive thoughts and memories and to self-regulate.” (Respondent 15, Practitioner)
Respondents felt psychoeducation was particularly effective when delivered in a group format, as this enables collective healing that accompanies sharing of experiences. This is consistent with evidence that sharing stories can lead to feelings of validation and mutuality, especially when shared in a non-judgemental environment facilitated by peer workers and/or counsellors (Heywood et al., 2019). Indeed, advocates and peer workers who bring lived expertise are an important part of the workforce in promoting connection and healing through shared experiences.
The aims of the group were to support self-expression, relationship buildings to reduce isolation, increase feelings of empowerment and mastery through artmaking and stimulating different senses and curiosity. A strengths-based approach was deliberately adopted to broaden positive experiences without re-traumatisation. (Respondent 50, Service designer/manager)
The importance of collective healing is also emphasised in responses to Aboriginal and Torres Strait Islander peoples’ experiences of violence (Carlson et al., 2021; Olsen & Lovett, 2016). The focus in this context is on collective and family healing, with the aim of strengthening family relationships, community cohesion and connectedness to culture and Country (Carlson et al., 2021).
Promoting healing and recovery was viewed as a priority area for further research and service development. Respondents asserted that supporting the healing and recovery of victims and survivors, children and young people and people who use violence is important in averting intergenerational trauma, and is a key component of response and prevention.
Strengths and limitations
The findings from this study should be considered in light of its strengths and limitations. Firstly, the sample of 95 is a small representation of the workforce responding to domestic, family and sexual violence and under-represents key sectors and jurisdictions. Geographically, the majority of respondents are drawn from Victoria, Western Australia and New South Wales, with more than one third of respondents working in Victoria. This means that there was an emphasis on models of care and responses in these jurisdictions and limited insight into effective responses and contextual factors specific to other jurisdictions.
There were few respondents drawn from key sectors such as policing, clinical health services, legal services, disability services and Aboriginal and Torres Strait Islander organisations. Further, there were no respondents who identified as working in child protection, housing or LGBTQ+ specialist services. There were also few respondents whose work focused on primary prevention. This relates to the recruitment strategy, which, though purposive, relied on existing networks. Accordingly, more than half of respondents were drawn from services whose core business is addressing domestic, family and sexual violence. This has given substantial insight into the challenges and successes in these settings, and the perspectives of this workforce are rich with highly specialised expertise and knowledge of domestic, family and sexual violence. However, there was less insight into what works and is needed in more mainstream settings that are not specialised in
responding to domestic, family and sexual violence, or what works in primary prevention. Perhaps this partially reflects the siloing of services in Australia, and a broader recruitment strategy is certainly a consideration for future studies that wish to capture more diverse perspectives.
We sought to privilege the perspectives of the respondents, however reflexive thematic analysis is inherently linked to the experiences and interpretations of the research team. As such, the research team were mindful of our world views and how they are context-bound and may be reflected in the analysis. To enable a breadth of perspectives to shape the findings, the research team sought insight and guidance from key stakeholders and experts in domestic, family and sexual violence – firstly, from the Voices Advisory Committee, who provided valuable input into the study design, methods and interpretation of the findings; and secondly, from key stakeholders across state and territory jurisdictions as well as the Australian Government, who provided feedback on the findings and recommendations.
The online survey used an iterative qualitative approach with open-ended questions that enabled respondents some flexibility in how they responded. Unlike a fully qualitative approach, the online survey contained fixed, structured questions presented in standard order, which obviously differs from a flexible, semi-structured interview or focus group. A limitation of this is that it does not allow for conversation, observation, clarification or probing for more details. Despite this, there are several benefits to this approach. Online qualitative surveys are a cost-effective and efficient method for gathering perspectives from a large population. They are convenient for respondents, who can participate on their own terms, and the anonymity of the online format may have supported respondents to be candid and considered in their responses.
While respondents were able to choose the sections of the survey they responded to according to their expertise, some respondents indicated that the survey was unduly long and repetitive. Additionally, there were a large number of respondents not included in the analysis as they did not provide substantive responses to the qualitative questions, which may suggest that the requirements of the survey were perceived to be onerous, the time of year being a busy period, or the increased workload due to the impact of the COVID-19 pandemic on the sector. These factors are important considerations for further studies using this approach and additional piloting with the workforce is recommended.
Nonetheless, this dataset is richly detailed and gives unique perspectives and insights from a highly experienced workforce. Most respondents had worked in the sector for six or more years, with almost half having 10 or more years of experience. As a result, there is a depth of experience that provides important insights into the challenges of working in this complex sector. This is also reflected in the opportunities and priorities identified by the workforce, which comprehensively address intersecting issues of equity, accessibility and justice.
Conclusion and recommendations
This study explored the perspectives of the domestic, family and sexual violence workforce in Australia using an online qualitative survey. Richly imbued with lived expertise from those on the frontlines, the findings identify important priorities and opportunities for innovative responses that embrace complexity and enable choice and self-determination. Underpinned by sustainable resourcing, enabling policy and workforce strengthening, systemic strengths can generate powerful shifts toward addressing the full spectrum of prevention, early intervention, response and recovery. This study demonstrates the depth of insight and expertise in the Australian domestic, family and sexual violence workforce, whose knowledge of the complexities, strengths and challenges faced by the sector are invaluable in creating meaningful change. Their voices are a powerful call to action and signal the importance of centring lived experience and expertise in policy and
practice solutions.
A primary concern for the workforce was inadequate and short-term funding cycles, which prevent services from meeting demand and constrain capacity for collaboration and sustaining the workforce. Issues with resourcing also impact workforce competency and capability, which was identified by respondents as a barrier to effective collaboration and outcomes. Respondents indicated that there is a high degree of variability in the workforce capability and thereby recognised that responding to victims and survivors and holding perpetrators to account is highly variable in practice.
A number of areas of competency were identified for different sectors, indicating a need for comprehensive trauma- and violence-informed care training across health, justice and social services. As a framework, trauma- and violence-informed care provides a foundation for understanding domestic, family and sexual violence as well as the intersections with other forms of power, privilege and oppression. In particular, there is a need for greater capability in understanding and responding to the dynamics of abuse, the ways these intersect with other experiences of violence and trauma, and how this can manifest in different contexts.
Key recommendations
Our findings point to important opportunities and priorities for service and system improvement with recommendations across four key areas:
- Promote safer communities, workplaces, schools and homes.
- Enhance workforce competency, capability and collaboration across sectors.
- Break intergenerational cycles of violence and trauma by better supporting children and young people.
- Bring forth innovative solutions.
Promote safer communities, workplaces, schools and homes
Recommendations to promote safer communities, workplaces, schools and homes are underpinned by the recognition of domestic, family and sexual violence as a social determinant of health. Accordingly, these recommendations seek to ensure that domestic, family and sexual violence is addressed within the context of intersection with other social determinants, such as safe housing and communities; income equality; workforce participation; social inclusion and non-discrimination; and equitable access to justice, healthcare and social services.
Recommendation 1
Prioritise safe and affordable housing solutions by governments to address critical shortages and bottlenecks in emergency housing, as well as shortages in other short- and long-term housing. Universal design principles are essential to ensuring that housing solutions are appropriate and accessible for all.
Recommendation 2
Provide federally funded and accredited community bystander training to mobilise and equip individuals to recognise and respond to domestic, family and sexual violence. Training should be free and co-produced with lived expertise advocates.
Recommendation 3
Recognise the importance of workplaces and education settings for generating community change in knowledge, attitudes and behaviours. In educational settings, implementation of nationally consistent curricula on consent, healthy relationships and domestic, family and sexual violence must be supported, for example by funding local violence prevention practitioners to deliver additional training and support to schools.
In workplaces, violence prevention and anti-violence initiatives are important to enable a safe work environment for all, as is implementation of specific policies that have been developed to support victims and survivors, such as paid domestic violence leave policy. The implementation of such initiatives requires ongoing monitoring and evaluation to determine uptake and effectiveness.
Enhance workforce competency, capability and collaboration across sectors
Recommendation 4
Increase core funding for frontline services, with built-in mechanisms to account for consumer price index (CPI) and award wage increases, as well as flexible support packages and emergency funds, which can be mobilised rapidly to frontline services following disasters. Funding cycles should be a minimum of three to five years to ensure frontline services are sustained. Funding packages must allow for flexibility and tailoring to local contexts, with resourcing to introduce responses that have been shown to be effective in similar contexts as well as capacity to implement new and context-specific responses.
Recommendation 5
Develop nationally accredited workforce training that can be tailored to health, police, magistrates and child welfare, which draws on the social entrapment model of violence, and trauma- and violence-informed care. This training should be co-designed by those with professional and lived experience and expertise.
Recommendation 6
Mandate Safe & Together training for those working in child protection and related services including police, magistrates, judicial registrars and expert witnesses. Expand Safe & Together training to be accessible to those working with families across health, education, legal and related services.
Recommendation 7
Fund targeted research, that is led by Aboriginal and Torres Strait Islander peoples and communities, to investigate and implement decolonising approaches to enhance workforce competency and capability.
Break intergenerational cycles of violence and trauma by better supporting children and young people
Recommendations to address intergenerational cycles of violence and trauma by better supporting children and young people are underpinned by recognition of children and young people as victims and survivors in their own right. This should be embedded in policy and practice guidelines and must be accompanied by greater investment in child-specific interventions.
Recommendation 8
Fund targeted research to establish evidence of effectiveness of therapeutic interventions for young people who are victims and survivors and those who use violence.
Recommendation 9
Fund targeted research to establish evidence of effectiveness of promising whole-of-family approaches, which bring a child-focused lens, with a view to supporting expanded implementation.
Recommendation 10
Re-evaluate the roles, responsibilities and training needs of Independent Children’s Lawyers, family report writers and other child court experts to ensure that there are independent and robust assessments of a child’s best interests in circumstances of family violence and other safety concerns. This will help to inform decision-makers and provide an effective voice for children as victims and survivors in their own right.
Bring forth innovative solutions
Recommendation 11
Build on innovative and promising digital and telehealth solutions that emerged as innovations during the pandemic to improve equitable access to services, including use of interpreters. Consider hybrid and hub models for digitally enabled service delivery to regional and remote locations to enable outreach options and strengthen collaboration with local services.
Recommendation 12
Invest in implementation of secure platforms for operational information sharing that were advanced during the pandemic. This must be accompanied by legislation, guidelines, training and practice resources to support information sharing.
Recommendation 13
Invest in therapeutic interventions that are focused on long-term health, healing and recovery, such as trauma-specific services. This requires adequate resourcing of therapeutic interventions delivered by health services including ACCOs. An important component of this are alternatives to criminal justice responses, such as therapeutic court interventions, as well as prison throughcare programs and family restoration programs.
Author contributions
In collaboration with the Voices project team, Dominiek Coates and Maria Koleth designed the survey and managed the ethics, recruitment and data collection.
Dominiek Coates had principal oversight for the Voices project and provided detailed feedback for the initial data coding and thematic analysis.
Maria Koleth processed the resulting survey data and undertook the descriptive analyses of respondent demographics and initial coding of the qualitative data.
Natasha Walker drafted the background literature review section of the report and contributed to drafting the methods and discussion of findings, under the supervision of Patricia Cullen. Natasha further assisted in formatting, proofreading and adding references to the report.
Patricia Cullen led the thematic analysis with input from the Voices project team and the project’s advisory committee. Patricia led the drafting of the report and contributed to all sections of the report.
References
Adams, A. E., Sullivan, C. M., Bybee, D., & Greeson, M. R. (2008). Development of the Scale of Economic Abuse. Violence Against Women, 14(5), 563–588. https://doi.org/10.1177/1077801208315529
Adams, A. E., Tolman, R. M., Bybee, D., Sullivan, C. M., & Kennedy, A. C. (2012). The impact of intimate partner violence on low-income women’s economic well-being: The mediating role of job stability. Violence Against Women, 18(12), 1345–1367. https://doi.org/10.1177/1077801212474294
Australian Bureau of Statistics. (2017a). Personal Safety Survey 2016 (ABS cat. no. 4906.0.). ABS.
Australian Bureau of Statistics. (2017b). Personal Safety Survey, Australia: User Guide, 2016. https://www.abs.gov.au/ausstats/[email protected]/Lookup/4906.0.55.003main+features42016#Persondemo
Australian Domestic and Family Violence Death Review Network, & Australia’s National Research Organisation for Women’s Safety. (2022). Australian Domestic and Family Violence Death Review Network data report: Intimate partner violence homicides 2010–2018 (2nd ed.; Research report 03/2022). ANROWS.
Australian Human Rights Commission. (2011). Report on the Review into the Treatment of Women at the Australian Defence Force Academy: Phase 1 of the Review into the Treatment of Women in the Australian Defence Force. AHRC.
Australian Human Rights Commission. (2022). Sexual harassment. https://humanrights.gov.au/quick-guide/12096
Australian Institute of Health and Welfare. (2018). Family, domestic and sexual violence in Australia 2018 (Cat. no. FDV 2.). AIHW.
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story 2019 (Cat. no. FDV 3.). AIHW.
Australian Institute of Health and Welfare. (2021a). Australia’s youth: COVID-19 and the impact on young people. https://www.aihw.gov.au/reports/children-youth/covid-19-and-young-people
Australian Institute of Health and Welfare. (2021b). Child protection in Australia 2019–20 (Cat. no. CWS 78.). AIHW.
Australian Institute of Health and Welfare. (2021c). Family, domestic and sexual violence service responses in the time of COVID-19 (Cat no FDV 8.). https://www.aihw.gov.au/reports/domestic-violence/family-domestic-and-sexual-violence-service-respon/summary
Australian Institute of Health and Welfare. (2021d). Specialist homelessness services annual report 2020–21. https://www.aihw.gov.au/reports/homelessness-services/specialist-homelessness-services-annual-report/contents/summary
Ayre, J., Lum On, M., Webster, K., Gourley, M., & Moon, L. (2016). Examination of the burden of disease of intimate partner violence against women in 2011: Final report (ANROWS Horizons, Issue 06/2016). ANROWS.
Bedi, G., & Goddard, C. (2007). Intimate partner violence: What are the impacts on children? Australian Psychologist, 42(1), 66–77.
Beeble, M. L., Bybee, D., & Sullivan, C. M. (2010). The impact of resource constraints on the psychological well-being of survivors of intimate partner violence over time. Journal of Community Psychology, 38(8), 943–959. https://doi.org/10.1002/jcop.20407
Bevis, M., Atkinson, J., McCarthy, L., & Sweet, M. (2020). Kungas’ trauma experiences and effects on behaviour in Central Australia (Research report, 03/2020). ANROWS.
Blagg, H., Bluett-Boyd, N., & Williams, E. (2015). Innovative models in addressing violence against Indigenous women: State of knowledge paper (ANROWS Horizons, Issue 08). ANROWS.
Blagg, H., Williams, E., Cummings, E., Hovane, V., Torres-Carne, M., & Karen, N. W. (2018). Innovative models in addressing violence against Indigenous women: Final report (ANROWS Horizons, Issue 01). ANROWS.
Bolarinwa, O. (2015). Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger Postgrad Med J, 22(4), 195–201. https://doi.org/10.4103/1117-1936.173959
Boxall, H., Doherty, L., Lawler, S., Franks, C., & Bricknell, S. (2022). The “Pathways to intimate partner homicide” project: Key stages and events in male-perpetrated intimate partner homicide in Australia (Research report, 04/2022). ANROWS.
Braaf, R., & Meyering, I. (2011). Seeking security: Promoting women’s economic wellbeing following domestic violence. Australian Domestic and Family Violence Clearinghouse.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
Braun, V., Clarke, V., Hayfield, N., & Terry, G. (2018). Thematic analysis. In P. Liamputtong (Ed.), Handbook of research methods in health social sciences (pp. 1–18). Springer Singapore.
Breckenridge, J., Cale, J., Hameed, S., McCaskie, L., & Tzoumakis, S. (2015). Implementation of domestic violence clauses: An employer’s perspective. Gendered Violence Research Network, UNSW.
Breckenridge, J., Chung, D., Spinney, A., & Zufferey, C. (2016). National mapping and meta-evaluation outlining key features of effective “safe at home” programs that enhance safety and prevent homelessness for women and their children who have experienced domestic and family violence: State of knowledge (ANROWS Landscape, Issue 05/2015). ANROWS.
Brown, L. (2022). Identity-first language. Autistic Self Advocacy Network. https://autisticadvocacy.org/about-asan/identity-first-language/
Brown, S., Gartland, D., Woolhouse, H., & Giallo, R. (2015). Translating evidence from the maternal health study to inform policy and practice (Policy Brief 2). Murdoch Children’s Research Institute.
Browne, A. J., Varcoe, C., Lavoie, J., Smye, V., Wong, S. T., Krause, M., Tu, D., Godwin, O., Khan, K., & Fridkin, A. (2017). Enhancing health care equity with Indigenous populations: Evidence-based strategies from an ethnographic study. BMC Health Services Research, 16(1), 544. https://doi.org/10.1186/s12913-016-1707-9
Browne, A. J., Varcoe, C. M., Wong, S. T., Smye, V. L., Lavoie, J., Littlejohn, D., Tu, D., Godwin, O., Krause, M., Khan, K. B., Fridkin, A., Rodney, P., O’Neil, J., & Lennox, S. (2012). Closing the health equity gap: Evidence-based strategies for primary health care organizations. International Journal for Equity in Health, 11(1), 59. https://doi.org/10.1186/1475-9276-11-59
Brownridge, D., Taillieu, T., Tyler, K., Tiwari, A., Ko Ling, C., & Santos, S. (2011). Pregnancy and intimate partner violence: Risk factors, severity, and health effects. Violence Against Women, 17(7), 858–881. https://doi.org/10.1177/1077801211412547
Bruton, C., & Tyson, D. (2017). Leaving violent men: A study of women’s experiences of separation in Victoria, Australia. Australian & New Zealand Journal of Criminology, 51(3), 339–354. https://doi.org/10.1177/0004865817746711
Bryman, A. (2001). Social research methods. Oxford University Press.
Bybee, D. I., & Sullivan, C. M. (2002). The process through which an advocacy intervention resulted in positive change for battered women over time. American Journal of Community Psychology, 30(1), 103–132. https://doi.org/10.1023/A:1014376202459
Campo, M. (2015). Children’s exposure to domestic and family violence: Key issues and responses (Paper no. 36). Australian Institute of Family Studies.
Campo, M., Kaspiew, R., Moore, S., & Tayton, S. (2014). Children affected by domestic and family violence: A review of domestic and family violence prevention, early intervention and response services. Australian Institute of Family Studies.
Canadian Institutes of Health Research. (2018). Science is better with sex and gender: Strategic plan 2018–2023. https://publications.gc.ca/collections/collection_2019/irsc-cihr/MR4-32-2018-eng.pdf
Carlson, B., Day, M., & Farrelly, T. (2021). What works? Exploring the literature on Aboriginal and Torres Strait Islander healing programs that respond to family violence (Research report, 01/2021). ANROWS.
Centres Against Sexual Assault Forum. (2014). Victorian Centres Against Sexual Assault standards of practice (2nd ed.). https://static1.squarespace.com/static/5fa0db2b7ce66d7cda3bbe00/t/5fb757dcd5e88918f42e32e0/1605851103790/NASASV_Standards_2nd_Edition_2015.pdf
Child Family Community Australia. (2014). Effects of child abuse and neglect for adult survivors [CFCA resource sheet]. Australian Institute of Family Studies. https://aifs.gov.au/cfca/publications/effects-child-abuse-and-neglect-adult-survivors
Clark, N. (2014). Perseverance, determination and resistance: An Indigenous intersectional-based policy analysis of violence in the lives of Indigenous girls. In H. O (Ed.), An intersectionality-based policy analysis framework (pp. 26). Institute for Intersectionality Research and Policy, Simon Fraser University.
Coker, A. L., Watkins, K. W., Smith, P. H., & Brandt, H. M. (2003). Social support reduces the impact of partner violence on health: Application of structural equation models. Preventive Medicine, 37(3), 259–267. https://doi.org/10.1016/S0091-7435(03)00122-1
Commonwealth of Australia. (2019). National Women’s Health Strategy 2020–2030. Department of Health.
Commonwealth of Australia. (2021). Inquiry into family, domestic and sexual violence: Report. House of Representatives Standing Committee on Social Policy and Legal Affairs.
Cortis, N., Blaxland, M., Breckenridge, J., valentine, k., Mahoney, N., Chung, D., Cordier, R., Chen, Y.-w., & Green, D. (2018). National survey of workers in the domestic, family and sexual violence sectors: Final report. Social Policy Research Centre (UNSW).
Cortis, N., & Bullen, J. (2015). Building effective policies and services to promote women’s economic security following domestic violence: State of knowledge (ANROWS Landscapes, Issue 11/2015). ANROWS.
Cortis, N., & Bullen, J. (2016). Domestic violence and women’s economic security: Building Australia’s capacity for prevention and redress: Key findings and future directions (ANROWS Compass, Issue 06/2016). ANROWS.
Council of Australian Governments. (2015). National Outcome Standards for Perpetrator Interventions. COAG.
Council of Australian Governments. (2016). Third Action Plan 2016–2019 of the National Plan to Reduce Violence against Women and their Children 2010–2022. Department of Social Services.
Council of Australian Governments. (2019). Fourth Action Plan: National Plan to Reduce Violence against Women and their Children 2010–2022. COAG.
Council of Australian Governments Advisory Panel. (2010). National Plan to Reduce Violence Against Women and their Children 2010-2022. Council of Australian Governments.
Crabtree, B. F., & Miller, W. L. (1992). Doing qualitative research: Research methods for primary care (Vol. 3). Sage Publications.
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241–1299. https://doi.org/10.2307/1229039
Crowne, S. S., Juon, H. S., Ensminger, M., Burrell, L., McFarlane, E., & Duggan, A. (2011). Concurrent and long-term impact of intimate partner violence on employment stability. Journel of Interpersonal Violence, 26(6), 1282–1304. https://doi.org/10.1177/0886260510368160
Cullen, P., Mackean, T., Walker, N., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., Worner, F., & Longbottom, M. (2021). Integrating trauma and violence informed care in primary health care settings for First Nations women experiencing violence: a systematic review. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838020985571
Cullen, P., Mackean, T., Worner, F., Wellington, C., Longbottom, H., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., & Longbottom, M. (2020). Trauma and violence informed care through decolonising interagency partnerships: A complexity case study of Waminda’s model of systemic decolonisation. International Journal of Environmental Research and Public Health, 17(20), 7363. https://doi.org/10.3390/ijerph17207363
Cullen, P., Stevenson, S., Baffsky, R., & Walker, N. (2021). A new model of care for women experiencing trauma from domestic, family and sexual violence: Co-design report. University of New South Wales. https://womenshealthcentre.com.au/wp-content/uploads/2021/11/WTRC-Report_F-digital.pdf
Day, A., Casey, S., Gerace, A., Oster, C., & O’Kane, D. (2018). The forgotten victims: Prisoner experience of victimisation and engagement with the criminal justice system (Issue 01/2018). ANROWS.
Day, S., Mason, R., Lagosky, S., & Rochon, P. A. (2016). Integrating and evaluating sex and gender in health research. Health Research Policy and Systems, 14(1), 75. https://doi.org/10.1186/s12961-016-0147-7
Decker, M., McCauley, H. L., Phuengsamran, D., Janyam, S., Seage, G. R. 3rd, & Silverman, J. G. (2010). Violence victimisation, sexual risk and sexually transmitted infection symptoms among female sex workers in Thailand. Sexually Transmitted Infections, 86(3), 236–240. http://dx.doi.org/10.1136/sti.2009.037846
Decker, M. R., Pearson, E., Illangasekare, S. L., Clark, E., & Sherman, S. G. (2013). Violence against women in sex work and hiv risk implications differ qualitatively by perpetrator. BMC Public Health, 13(1), 876. https://doi.org/10.1186/1471-2458-13-876
Department for Victorian Communities. (2021). Family violence workforce census. Victorian Government. https://www.vic.gov.au/family-violence-workforce-census
Department of Health. (2018). National Women’s Health Strategy 2020–2030. Australian Government.
Department of Social Services. (2021). Keeping women safe in their homes. https://www.dss.gov.au/women-programs-services-reducing-violence/keeping-women-safe-in-their-homes
Department of Social Services. (2022). Draft National Plan to End Violence against Women and Children 2022–2032. https://engage.dss.gov.au/draft-national-plan-to-end-violence-against-women-and-children-2022-2032/
Didi, A., Soldatic, K., Frohmader, C., & Dowse, L. (2016). Violence against women with disabilities: Is Australia meeting its human rights obligations? Australian Journal of Human Rights, 22(1), 159–177. https://doi.org/10.1080/1323-238X.2016.11882162
Diemer, K., Humphreys, C., & Crinall, K. (2017). Safe at home? Housing decisions for women leaving family violence. Australian Journal of Social Issues, 52(1), 32–47. https://doi.org/10.1002/ajs4.5
Dillon, G., Hussain, R., Loxton, D., & Rahman, S. (2013). Mental and physical health and intimate partner violence against women: A review of the literature. International Journal of Family Medicine, 2013, 1–15. https://doi.org/10.1155/2013/313909
Douglas, H., Tarrant, S., & Tolmie, J. (2021). Social entrapment evidence: Understanding its role in self-defence cases involving intimate partner violence. University of New South Wales Law Journal, 44(1).
https://doi.org/10.53637/VJII7190
Edwards, K. M., Sylaska, K. M., & Neal, A. M. (2015). Intimate partner violence among sexual minority populations: A critical review of the literature and agenda for future research. Psychology of Violence, 5(2), 112–121. https://doi.org/10.1037/a0038656
Ehrensaft, M., Cohen, P., Brown, J., Smailes, E., Chen, H., & Johnson, J. G. (2003). Intergenerational transmission of partner violence: A 20-year prospective study. J Consult Clin Psychol, 71(4), 741–753. https://doi.org/10.1037/0022-006X.71.4.741
Ellonen, N., Piispa, M., Peltonen, K., & Oranen, M. (2013). Exposure to parental violence and outcomes of child psychosocial adjustment. Violence Vict(1), 3–15. https://doi.org/10.1891/0886-6708.28.1.3
Evans, M., & Feder, G. (2016). Help-seeking amongst women survivors of domestic violence: A qualitative study of pathways towards formal and informal support. Health Expectations, 19(1), 62–73. https://doi.org/10.1111/hex.12330
Family Violence Act 2004 (Cth).
Ferrer-Perez, V. A., Bosch-Fiol, E., Ferreiro-Basurto, V., Delgado-Alvarez, C., & Sánchez-Prada, A. (2020). Comparing implicit and explicit attitudes toward intimate partner violence against women. Front Psychol, 11, 2147. https://doi.org/10.3389/fpsyg.2020
Fitz-Gibbon, K., Walklate, S., & Meyer, S. (2020). Criminalisation of coercive control: Research brief. Monash Gender and Family Violence Prevention Centre. https://arts.monash.edu/__data/assets/pdf_file/0019/1530343/rb-coercive-control.pdf
Flasch, P., Murray, C. E., & Crowe, A. (2015). Overcoming abuse: A phenomenological investigation of the journey to recovery from past intimate partner violence. Journal of Interpersonal Violence, 32(22), 3373–3401. https://doi.org/10.1177/0886260515599161
Flood, M., & Fergus, L. (2008). An assault on our future: The impact of violence on young people and their relationships. White Ribbon Foundation. http://www.ncdsv.org/images/WhiteRibbon_AssaultOnOurFutureImpactOfViolence
OnYoungPeopleAndTheirRelationships_ExecSumm.pdf
Gebicki, C., Meagher, A., & Flax, G. (2018). Everyone’s business: Fourth national survey on sexual harassment in Australian workplaces. Australian Human Rights Commission. https://humanrights.gov.au/our-work/sex-discrimination/publications/everyones-business-fourth-national-survey-sexual
Government of South Australia. (2022). Discussion paper: Implementation considerations should coercive control be criminalised in South Australia. Attorney-General’s Department, SA Government.
Government of Western Australia. (2020). Path to safety: Western Australia’s Strategy to Reduce Family and Domestic Violence 2020–2030. Government of Western Australia, Department of Communities.
Grace, K. T., & Anderson, J. C. (2018). Reproductive coercion: A systematic review. Trauma, Violence & Abuse, 19(4), 371–390. https://doi.org/10.1177/1524838016663935
Gracia, E., Rodriguez, C. M., Martín-Fernández, M., & Lila, M. (2017). Acceptability of family violence: Underlying ties between intimate partner violence and child abuse. Journal of Interpersonal Violence, 35(17–18), 3217–3236. https://doi.org/10.1177/0886260517707310
Gruber, J. E. (1998). The impact of male work environments and organizational policies on women’s experiences of sexual harassment. Gender & Society, 12(3), 301–320. https://doi.org/10.1177/0891243298012003004
Hamby, S., & Grych, J. (2013). The web of violence: Exploring connections among different forms of interpersonal violence and abuse (13th ed.). Springer.
Hegarty, K., Tarzia, L., Rees, S., Fooks, A., Forsdike, K., Woodlock, D., Simpson, L., McCormack, C., & Amanatidis, S. (2017). Women’s Input into a Trauma-informed systems model of care in Health settings (The WITH study): Final report (ANROWS Horizons 02/2017). ANROWS.
Heise, L. L., & Kotsadam, A. (2015). Cross-national and multilevel correlates of partner violence: An analysis of data from population-based surveys. Lancet Global Health, 3(6), e332–e340. https://doi.org/10.1016/S2214-109X(15)00013-3
Herrero, J., Rodríguez, F. J., & Torres, A. (2017). Acceptability of partner violence in 51 societies: The role of sexism and attitudes toward violence in social relationships. Violence Against Women, 23(3), 351–367. https://doi.org/10.1177/1077801216642870
Heywood, I., Sammut, D., & Bradbury-Jones, C. (2019). A qualitative exploration of “thrivership” among women who have experienced domestic violence and abuse: Development of a new model. BMC women’s health, 19(1), 106. https://doi.org/10.1186/s12905-019-0789-z
Hill, A., Bourne, A., McNair, R., Carman, M., & Lyons, A. (2020). Private Lives 3: The health and wellbeing of LGBTIQ people in Australia (ARCSHS Monograph Series No. 122). Australian Research Centre in Sex, Health and Society, La Trobe University. https://www.latrobe.edu.au/__data/assets/pdf_file/0009/1185885/Private-Lives-3.pdf
Hill, A. O., Lyons, A., Jones, J., McGowan, I., Carman, M., Parsons, M., Power, J., & Bourne, A. (2021). Writing Themselves In 4: The health and wellbeing of LGBTQA+ young people in Australia (Monograph Series Number 124). Australian Research Centre in Sex, Health and Society, La Trobe University. https://www.latrobe.edu.au/__data/assets/pdf_file/0010/1198945/Writing-Themselves-In-4-National-report.pdf
Hobfoll, S. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing conservation of resources theory. Applied Psychology, 50(3), 337–421. https://doi.org/10.1111/1464-0597.00062
Hobfoll, S., & Lilly, R. (1993). Resource conservation as a strategy for community psychology. Journal of Community Psychology, 21(2), 128–148. https://doi.org/10.1002/1520-6629(199304)21:2<128::AID-JCOP2290210206>3.0.CO;2-5
Humphreys, C. (2007). Domestic violence and child protection: challenging directions for practice (Issues paper 13). Australian Domestic & Family Violence Clearinghouse.
Humphreys, C. (2008). Problems in the system of mandatory reporting of children living with domestic violence. Journal of Family Studies, 14(2–3), 228–239. https://doi.org/10.5172/jfs.327.14.2-3.228
Jaeger, M. E., & Rosnow, R. L. (1988). Contextualism and its implications for psychological inquiry. British Journal of Psychology, 79(1), 63–75.
James, L., Brody, D., & Hamilton, Z. (2013). Risk factors for domestic violence during pregnancy: A meta-analytic review. Violence Vict, 28(3), 359–380. https://doi.org/10.1891/0886-6708.VV-D-12-00034
Joint Select Committee on Coercive Control. (2021). Coercive control in domestic relationships (Report 1/57). Parliament of NSW. https://nla.gov.au/nla.obj-2969950536/view
Justice Health & Forensic Mental Health Network. (2017). Network patient health survey report 2015. Justice Health & Forensic Mental Health Network. https://www.justicehealth.nsw.gov.au/publications/2015_NHPS_FINALREPORT.pdf
Kaufman, K., & Little, L. (2003). Defining the boundaries of child neglect: When does domestic violence equate with parental failure to protect? Journal of Interpersonal Violence, 18(4), 338–355. https://doi.org/10.1177/0886260502250834
Kiamanesh, P., & Hauge, M.-I. (2019). “We are not weak, we just experience domestic violence”—Immigrant women’s experiences of encounters with service providers as a result of domestic violence. Child & Family Social Work, 24(2), 301–308. https://doi.org/10.1111/cfs.12615
KPMG. (2016). The cost of violence against women and their children in Australia. Department of Social Services.
Kulkarni, M., Graham-Bermann, S., Rauch, S., & Seng, J. (2011). Witnessing versus experiencing direct violence in childhood as correlates of adulthood PTSD. Journal of Interpersonal Violence, 26(6), 1264–1281. https://doi.org/10.1177/0886260510368159
Langenderfer-Magruder, L., Whitfield, D. L., Walls, N. E., Kattari, S. K., & Ramos, D. (2016). Experiences of intimate partner violence and subsequent police reporting among lesbian, gay, bisexual, transgender, and queer adults in Colorado: Comparing rates of cisgender and transgender victimization. J Interpers Violence, 31(5), 855–871. https://doi.org/10.1177/0886260514556767
Langton, M., Smith, K., Eastman, T., O’Neill, L., Cheesman, E., & Rose, M. (2020). Improving family violence legal and support services for Aboriginal and Torres Strait Islander women (Issue 25). ANROWS.
Longbottom, M. A. (2019). Balwalwanga Bhulungs: We are strong women [Unpublished thesis]. Wollotuka Institute, University of Newcastle.
Marie Stopes. (2020). Hidden forces: A white paper on reproductive coercion in contexts of family and domestic violence (2nd ed.). https://www.mariestopes.org.au/wp-content/uploads/Hidden-Forces-Second-Edition-.pdf
Meyer, S. R., Lasater, M. E., & García-Moreno, C. (2020). Violence against older women: A systematic review of qualitative literature. PLOS One, 15(9), e0239560. https://doi.org/10.1371/journal.pone.0239560
Moe, A. M., & Bell, M. P. (2004). Abject economics: The effects of battering and violence on women’s work and employability. Violence Against Women, 10(1), 29–55. https://doi.org/10.1177/1077801203256016
Muldoon, K. A., Deering, K. N., Feng, C. X., Shoveller, J. A., & Shannon, K. (2015). Sexual relationship power and intimate partner violence among sex workers with non-commercial intimate partners in a Canadian setting. AIDS Care, 27(4), 512–519. https://doi.org/10.1080/09540121.2014.978732
Myhill, A., & Hohl, K. (2016). The golden thread: Coercive control and risk assessment for domestic violence. Journal of Interpersonal Violence, 34, 4477–4497. https://doi.org/10.1177/0886260516675464
Nancarrow, H. (2010). Restorative justice for domestic family violence: hopes and fears of Indigenous and Non-Indigenous Australian women. In J. Ptacek (Ed.), Restorative justice and violence against women (pp. 123–149). Oxford University Press.
National Association of Services Against Sexual Violence. (2021). The standards of practice manual for services against sexual violence (3rd edition). https://static1.squarespace.com/static/5fa0db2b7ce66d7cda3bbe00/t/613583e1573d0042b238fd9b/1630897132183/Standards+of+Practice+Manual+for+Services+Against+
Sexual+Violence+3rd+Edition.PDF
Neave, M., Faulkner, P., & Nicholson, T. (2016). Royal Commission into Family Violence: Summary and recommendations (Parl Paper No 132). Victorian Government.
NSW Government. (2019). The case for change: Integrated prevention and response to violence, abuse and neglect in NSW Health. NSW Ministry of Health. https://www.health.nsw.gov.au/parvan/Publications/case-for-change.pdf
NSW Health. (2014). NSW Health workforce domestic violence survey. NSW Government. https://www.health.nsw.gov.au/parvan/DV/Documents/dv-workforce-survey-report.pdf
NSW Ministry of Health. (2019). The case for change: Integrated prevention and response to violence, abuse and neglect in NSW Health. NSW Government. https://www.health.nsw.gov.au/parvan/Publications/case-for-change.pdf
Olsen, A., & Lovett, R. (2016). Existing knowledge, practice and responses to violence against women in Australian Indigenous communities: State of knowledge paper (Issue 2/2016). ANROWS.
Oram, S., Fisher, H. L., Minnis, H., Seedat, S., Walby, S., Hegarty, K., Rouf, K., Angénieux, C., Callard, F., Chandra, P. S., Fazel, S., Garcia-Moreno, C., Henderson, M., Howarth, E., MacMillan, H. L., Murray, L. K., Othman, S., Robotham, D., Rondon, M. B., Sweeney, A., Taggart, D., & Howard, L. M. (2022). The Lancet Psychiatry Commission on Intimate Partner Violence and Mental Health: Advancing mental health services, research, and policy. Lancet Psychiatry, 9(6), 487–524. https://doi.org/10.1016/S2215-0366(22)00008-6
Our Watch. (2018). Changing the picture: A national resource to support the prevention of violence against Aboriginal and Torres Strait Islander women and their children. https://apo.org.au/sites/default/files/resource-files/2018-07/apo-nid182621.pdf
Our Watch. (2022a). The issue. https://www.ourwatch.org.au/the-issue/
Our Watch. (2022b). The power of the workplace. https://workplace.ourwatch.org.au/why-do-this-work/the-power-of-the-workplace/
Our Watch. (2022c). Understanding sexual harassment in workplaces. https://workplace.ourwatch.org.au/why-do-this-work/understanding-sexual-harassment-in-workplaces/#the-gendered-drivers-of-violence
Owen, S., & Carrington, K. (2015). Domestic violence service provision and the architecture of rural life: An Australian case study. Journal of Rural Studies, 39, 229–238. https://doi.org/10.1016/j.jrurstud.2014.11.004
Pathak, N., Dhairyawan, R., & Tariq, S. (2019). The experience of intimate partner violence among older women: A narrative review. Maturitas, 121, 63–75. https://doi.org/10.1016/j.maturitas.2018.12.011
Peckover, S. (2003). “I could have just done with a little more help”: An analysis of women’s help-seeking from health visitors in the context of domestic violence. Health & Social Care in the Community, 11(3), 275–282. https://doi.org/10.1046/j.1365-2524.2003.00423.x
People with Disability of Australia. (2019). What do I say? A guide to language about disability. https://pwd.org.au/wp-content/uploads/2019/08/PWDA_LanguageGuide_A5_WEB.pdf
Porter, A., Deslandes, A. L., McKinnon, C., & Longbottom, M. (2021). Women’s police stations in Australia: Would they work for “all” women? The Conversation. https://theconversation.com/womens-police-stations-in-australia-would-they-work-for-all-women-165873
Ptacek, J. (1999). Battered women in the courtroom: The power of judicial responses. Northeastern University Press.
Richards, K. (2011). Children’s exposure to domestic violence in Australia (no. 419). Australian Institute of Criminology.
Riger, S., Staggs, S. L., & Schewe, P. (2004). Intimate partner violence as an obstacle to employment among mothers affected by welfare reform. Journal of Social Issues, 60(4), 801–818. https://doi.org/10.1111/j.0022-4537.2004.00387.x
Roach, K. (1999). Four models of the criminal process. Journal of Criminal Law and Criminology, 89(671). https://doi.org/10.2307/1144140
Roberts, A. L., Gilman, S. E., Fitzmaurice, G., Decker, M. R., & Koenen, K. C. (2010). Witness of intimate partner violence in childhood and perpetration of intimate partner violence in adulthood. Epidemiology (Cambridge, Mass.), 21(6), 809–818. https://doi.org/10.1097/EDE.0b013e3181f39f03
Robinson, L., & Spilsbury, K. (2008). Systematic review of the perceptions and experiences of accessing health services by adult victims of domestic violence. Health & Social Care in the Community, 16(1), 16–30. https://doi.org/10.1111/j.1365-2524.2007.00721.x
Safe & Together Institute. (2020). Safe & Together model principles & critical components. https://safeandtogetherinstitute.com/safe-together/safe-together-overview/assumptions-principles-critical-components/
Salter, M. (2013). Multi-perpetrator domestic violence. Trauma, Violence, & Abuse, 15(2), 102–112. https://doi.org/10.1177/1524838013511542
Salter, M., Conroy, E., Dragiewicz, M., Burke, J., Ussher, J., Middleton, W., Vilenica, S., Martin Monzon, B., & Noack-Lundberg, K. (2020). “A deep wound under my heart”: Constructions of complex trauma and implications for women’s wellbeing and safety from violence (Research report, 12/2020). ANROWS. https://www.anrows.org.au/publication/a-deep-wound-under-my-heart-constructions-of-complex-trauma-and-implications-for-womens-wellbeing-and-safety-from-violence/
Saunders, S., & Easteal Am, P. (2013). The nature, pervasiveness and manifestations of sexual harassment in rural Australia: Does “masculinity” of workplace make a difference? Women’s Studies International Forum, 40, 121–131. https://doi.org/10.1016/j.wsif.2013.05.013
Schmidt, I. D. (2014). Addressing PTSD in low-income victims of intimate partner violence: Moving toward a comprehensive intervention. Soc Work, 59(3), 253–260.
Seib, C., Fischer, J., & Najman, J. M. (2009). The health of female sex workers from three industry sectors in Queensland, Australia. Social Science & Medicine, 68(3), 473–478. https://doi.org/10.1016/j.socscimed.2008.10.024
Shannon, K., Kerr, T., Bright, V., Gibson, K., & Tyndall, M. W. (2008). Drug sharing with clients as a risk marker for increased violence and sexual and drug-related harms among survival sex workers. AIDS Care, 20(2), 228–234. https://doi.org/10.1080/09540120701561270
Shannon, K., Kerr, T., Strathdee, S. A., Shoveller, J., Montaner, J. S., & Tyndall, M. W. (2009). Prevalence and structural correlates of gender based violence among a prospective cohort of female sex workers. BMJ, 339, b2939. https://doi.org/10.1136/bmj.b2939
Sharp-Jeffs, N., Kelly, L., & Klein, R. (2018). Long journeys toward freedom: The relationship between coercive control and space for action-measurement and emerging evidence. Violence Against Women, 24(2), 163–185. https://doi.org/10.1177/107780121668619
Sinko, L., James, R., & Hughesdon, K. (2021). Healing after gender-based violence: A qualitative metasynthesis using meta-ethnography. Trauma, Violence, & Abuse, 1524838021991305. https://doi.org/10.1177/1524838021991305
Smyth, C., Cullen, P., Breckenridge, J., Cortis, N., & valentine, k. (2021). COVID-19 lockdowns, intimate partner violence and coercive control. The Australian Journal of Social Issues. https://doi.org/10.1002/ajs4.162
Staggs, S. L., & Riger, S. (2005). Effects of intimate partner violence on low-income women’s health and employment. American Journal of Community Psychology, 36(1), 133–145. https://doi.org/10.1007/s10464-005-6238-1
Stark, E. (2007). Coercive control: How men entrap women in personal life. Oxford University Press.
Stark, E., & Hester, M. (2019). Coercive control: Update and review. Violence Against Women, 25(1), 81–104. https://doi.org/10.1177/1077801218816191
Stathopoulos, M., Quadara, A., Fileborn, B., & Clark, H. (2012). Addressing women’s victimisation histories in custodial settings (Issue no. 13). Australian Institute of Family Studies. https://aifs.gov.au/sites/default/files/publication-documents/i13_0.pdf
Sullivan, C. M., & Bybee, D. I. (1999). Reducing violence using community-based advocacy for women with abusive partners. Journal of Consulting and Clinical Psychology, 67(1), 43–53. https://doi.org/10.1037/0022-006X.67.1.43
Sullivan, C. M., Bybee, D. I., & Allen, N. E. (2002). Findings from a community-based program for battered women and their children. Journal of Interpersonal Violence, 17(9), 915–936. https://doi.org/10.1177/0886260502017009001
Szalacha, L. A., Hughes, T. L., McNair, R., & Loxton, D. (2017). Mental health, sexual identity, and interpersonal violence: Findings from the Australian Longitudinal Women’s Health Study. BMC Women’s Health, 17(1), 94. https://doi.org/10.1186/s12905-017-0452-5
The Equality Institute. (2017). Preventing and responding to family violence: Taking an intersectional approach to address violence in Australian communities. https://apo.org.au/sites/default/files/resource-files/2017-10/apo-nid185301.pdf
Tolman, R. M., & Wang, H. C. (2005). Domestic violence and women’s employment: Fixed effects models of three waves of women’s employment study data. Am J Community Psychol, 36(1–2), 147–158. https://doi.org/10.1007/s10464-005-6239-0
Tolmie, J., Smith, R., Short, J., Wilson, D., & Sach, J. (2018). Social entrapment: A realistic understanding of the criminal offending of primary victims of intimate partner violence. New Zealand Law Review, 2018, 181.
Trevillion, K., Hughes, B., Feder, G., Borschmann, R., Oram, S., & Howard, L. M. (2014). Disclosure of domestic violence in mental health settings: A qualitative meta-synthesis. International Review of Psychiatry, 26(4), 430–444. https://doi.org/10.3109/09540261.2014.924095
VACCA, ThinkPlace, & Family Safety Victoria. (2019). Nargneit Birrang: Aboriginal holistic healing framework for family violence. State of Victoria.
Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Quiazon, R., Block, K., & Warr, D. (2016). Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: The ASPIRE project (ANROWS Landscapes, Issue 12/2015). ANROWS.
Victoria Department of Health and Human Services. (2018). Dhelk Dja: Safe our way – Strong culture, strong peoples, strong families. Department of Health and Human Services.
Victoria Department of Premier and Cabinent. (2019). Victorian family violence data collection framework. State Government of Victoria.
Victorian Indigenous Taskforce. (2003). Victorian Indigenous Family Violence Task Force: Final report. Aboriginal Affairs Department for Victorian Communities. https://www.vgls.vic.gov.au/client/en_AU/search/asset/1162179/0
Walker, H., Freud, J., Ellis, R., Fraine, S., & Wilson, L. (2019). The prevalence of sexual revictimization: A meta-analytic review. Trauma, Violence, & Abuse, 20(1), 67–80. https://doi.org/10.1177/1524838017692364
Walker, N., Beek, K., Chen, H., Shang, J., Stevenson, S., Williams, K., Herzog, H., Ahmed, J., & Cullen, P. (2020). The experiences of persistent pain among women with a history of intimate partner violence: A systematic review. Trauma, Violence, & Abuse, 1524838020957989. https://doi.org/10.1177/1524838020957989
Walker, N., Mackean, T., Longbottom, M., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., Redfern, J., & Cullen, P. (2020). Responses to the primary health care needs of Aboriginal and Torres Strait Islander women experiencing violence: A scoping review of policy and practice guidelines. Health Promotion Journal of Australia. https://doi.org/10.1002/hpja.417
Wangmann, J. (2020). Coercive control as the context for intimate partner violence: The challenge for the legal system. In M. McMahon & P. McGorrery (Eds.), Criminalising coercive control (pp. 219–242). Springer.
Webster, K. (2016). A preventable burden: Measuring and addressing the prevalence and health impacts of intimate partner violence in Australian women: Key findings and future directions (ANROWS Compass, 07/2016). ANROWS.
Webster, K., Diemer, K., Honey, N., Mannix, S., Mickle, J., Morgan, J., Parkes, A., Politoff, V., Powell, A., Stubbs, J., & Ward, A. (2018). Australians’ attitudes to violence against women and gender equality: Findings from the 2017 National Community Attitudes towards Violence against Women Survey (NCAS) (Research report, 03/2018). ANROWS.
Willis, M. (2011). Non-disclosure of violence in Indigenous communities (Trends & Issues in Crime and Criminal Justice, no. 405). Australian Institute of Criminology.
Willoughby, M., Spittal, M. J., Borschmann, R., Tibble, H., & Kinner, S. A. (2020). Violence-related deaths among people released from prison: A data linkage study. Journal of Interpersonal Violence, 36(23–24), NP13229–NP13253. https://doi.org/10.1177/0886260520905546
Women’s Safety and Justice Taskforce. (2021). Options for legislating against coercive control and the creation of a standalone domestic violence offence: Discussion paper 1. https://www.womenstaskforce.qld.gov.au/__data/assets/pdf_file/0004/684913/WSJT-Discussion-paper-1-Options-for-legislating-against-coercive-control-and-the-creation-of-a-standaone-domestic-violence-offence.pdf
Workplace Gender Equality Agency. (2022a). Australia’s gender equality scorecard. https://www.wgea.gov.au/publications/australias-gender-equality-scorecard
Workplace Gender Equality Agency. (2022b). The gender pay gap. https://www.wgea.gov.au/the-gender-pay-gap
World Health Organization. (2014). Global status report on violence prevention. https://www.who.int/publications/i/item/9789241564793
World Health Organization. (2018). Elder abuse: Fact sheet. http://www.who.int/news-room/fact-sheets/detail/elder-abuse
World Health Organization. (2021). Violence against women. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
Appendix A:
Voices project advisory committee members
Dr Hayley Boxall (Australian Institute of Criminology)
The Healing Foundation
Heather Clarke (National Association of Services against Sexual Violence)
On the Line Australia
Louise Gottardo (Queensland Department of Justice and Attorney-General)
Emily Grant (WEAVERs panel)
Angela Hampton (Central Australian Aboriginal Congress)
ACON’s Sexual, Domestic and Family Violence Team
Sally Mills (Australian Institute of Health and Welfare)
Dr Astrid Perry (Settlement Services International)
Safiyah Salim (WA Health)
Officers from the Attorney-General’s Department
WA Department of Communities, Office for Prevention of Family and Domestic Violence
Amanda Wallace (WEAVERs panel)
Jacqui Watt (No to Violence)
Endnotes
- The social entrapment model avoids victim blaming by recognising intersecting structural and social determinants that underpin the perpetrator’s ability to enact violence and the safety responses available to the victim (Douglas et al., 2021; Ptacek, 1999). Back to reference ↑
- Safe & Together is based on three principles that prioritise the safety and wellbeing of children: keep children safe and together with non-offending parents; partner with the perpetrator and hold them accountable; intervene with the perpetrator to reduce risk and harm to children (Safe & Together Institute, 2020). Back to reference ↑
- Acknowledging the importance of preventing and responding to child sexual violence, the Australian Government has also established the National Office for Children’s Safety and provided initial funding for the National Centre for Action on Child Sexual Abuse. Back to reference ↑