
RESEARCH REPORT “I just felt like I was running around in a circle”: Listening to the voices of victims and perpetrators to transform responses to intimate partner violence
Professor Kelsey Hegarty
University of Melbourne
Dr Mandy McKenzie
University of Melbourne
Dr Elizabeth McLindon
University of Melbourne
Matt Addison
University of Melbourne
Dr Jodie Valpied
University of Melbourne
Dr Mohajer Hameed
University of Melbourne
Dr Minerva Kyei-Onanjiri
University of Melbourne
Dr Surriya Baloch
University of Melbourne
Associate Professor Kristin Diemer
University of Melbourne
Associate Professor Laura Tarzia
University of Melbourne
RESEARCH REPORT
ISSUE 22 | DECEMBER 2022
ANROWS acknowledgement
This material was produced with funding from the Australian Government Department of Social Services. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from the government, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government Department of Social Services. Thank you to our advisory committee: Hayley Boxall (Australian Institute of Criminology), Sally Mills (Australian Institute Health and Welfare), Angela Hampton (Central Australian Aboriginal Congress), Jacqui Watt (No to Violence), Safiyah Salim (WA Health), Emily Grant (WEAVERs group, University of Melbourne), Amanda Wallace (WEAVERs group, University of Melbourne), Heather Clarke (National Association of Services against Sexual Violence), Louise Gottardo (Queensland Departmentof Justice), Dr Astrid Perry (Settlement Services International), Dominiek Coates (ANROWS), and representatives from the Commonwealth Attorney-General’s Department, ACON’s Sexual, Domestic and Family Violence team, the WA Department of Communities, and the Office for Prevention of Family and Domestic Violence.
Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we live and work. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and emerging. We value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with First Nations peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2022

With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
ISBN: 978-1-922645-59-3 (paperback)
ISBN: 978-1-922645-60-9 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project 4AP.8 “Transforming responses to intimate partner and sexual violence: Listening to the voices of victims, perpetrators and services”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Plan Outcome 4 – Services meet the needs of women and their children experiencing violence and National Plan Outcome 6 – Perpetrators stop their violence and are held to account.
Suggested citation:
Hegarty, K., McKenzie, M., McLindon, E., Addison, M., Valpied, J., Hameed, M., Kyei-Onanjiri, M., Baloch, S., Diemer, K., & Tarzia, L. (2022). “I just felt like I was running around in a circle”: Listening to the voices of victims and perpetrators to transform responses to intimate partner violence (Research report, 22/2022). ANROWS.

The University of Melbourne
Parkville VIC 3010
Author acknowledgement
We gratefully acknowledge contributions made by all the participants who so generously participated in various phases of this project by sharing their experiences with us. We appreciate contributions made by Jacqueline Kuruppu and Kitty Novy who assisted with survey design. We thank members of the advisory committee established to support this project. They oversaw the general conduct of the research and assisted with recruitment and interpreting and disseminating the findings.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of people affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
ANROWS acknowledges that children and young people living in homes where domestic and family violence (DFV) is present are not simply “exposed” to DFV – they are experiencing it. There are no circumstances in which children and young people are exposed to DFV and are not also being impacted by this violence. Therefore, ANROWS will always default to using “experienced DFV” instead of “were exposed to DFV” or “witnessed DFV”. This language recognises that children experience DFV as victims in their own right, and also seeks to honour the voices of victims and survivors who have felt minimised, erased or unacknowledged as childhood survivors.
Please note that in this report, the authors have occasionally used the language of exposure and witnessing.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76).
Acronyms and abbreviations
Acronym / abbreviation
Definition
ACEs
Adverse childhood experiences
CALD
Culturally and linguistically diverse
CASr-SF
Composite Abuse Scale (Revised) Short Form
DV or IPV
Domestic violence or intimate partner violence
IPV and/or SV
Intimate partner violence and/or sexual violence
LGBTQ
Lesbian, gay, bisexual, trans and gender diverse, queer and questioning
PTSD
Post-traumatic stress disorder
SV
Sexual violence
Definitions and concepts
Concept
Definition
Child abuse
Child abuse refers to a range of physically, sexually and psychologically abusive and neglectful behaviours, including experiencing parental violence growing up. This study included questions about child abuse from the Adverse Childhood Experiences Scale and refers to abusive and harmful behaviour occurring before the age of 15 years, perpetrated by somebody over the age of 18 years, from within or outside the family (Felitti et al., 1998).
Family violence
Family violence refers to physically, sexually, emotionally or economically abusive behaviours by an intimate or non-intimate family member that may make a family member feel afraid for their safety or wellbeing (Australasian Legal Information Institute, 2008; Ellsberg & Heise, 2002). Family violence includes behaviour that children experience living in homes where domestic violence is occurring. “Family violence” is the term preferred by Australian Aboriginal and Torres Strait Islander peoples as better reflecting the experiences of extended families and communities (Olsen & Lovett, 2016). While family violence refers to abusive behaviour that can occur in families of diverse configurations, it is often used to describe behaviour by an intimate partner against his current or former partner and her children (Victorian Government, 2016).
Financial abuse
Financial abuse is a form of family violence that may include withholding money, controlling household finances or refusing to include a victim and survivor in financial decisions.
Intimate partner violence (IPV)
The World Health Organization (WHO) defines “intimate partner violence” (IPV) as “behaviour by an intimate partner that causes physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviours” (World Health Organization, 2013b, p. vii). This definition is inclusive of violence by current and former spouses and other intimate partners. The National Plan to Reduce Violence Against Women and their Children 2010–2022 (the National Plan) highlights that IPV is frequently characterised by “an ongoing pattern of behaviour … a range of tactics to exercise power and control over women and their children” (Council of Australian Governments, 2012, p. 2). IPV is used in this report instead of “domestic violence”, because, although they are commonly used interchangeably, the definition of domestic violence is broader to include other people who live in a domesticarrangement.
Intimate partner violence and/or sexual violence (IPV and/or SV)
In recognition of the common but often hidden experience of sexual violence (SV) within IPV as well as the prevalence of SV outside of intimate relationships, in this report we use the term “IPV and/or SV”. IPV and/or SV refers to instances where people have experienced IPV that may or may not have included SV by a partner or somebody else.
People who use violence and abuse
The terms “people who use violence and abuse” or “people who use IPV and/or SV” are employed within this report to refer to people of all genders who have perpetrated physical, sexual and/or psychological violence against an intimate partner. We employ inclusive language to refer to people who have used violence, but we nonetheless acknowledge that the prevalence and impacts of IPV and/or SV are not sex-asymmetrical (Indermaur, 2001; Kertesz et al., 2019). While many factors contribute to IPV and/or SV, research has long shown that chief among them is the power disparity between men and women as a result of women’s relative lack of access to resources and rigid gender roles linking masculinity with dominance (Flood & Pease, 2009; Our Watch & VicHealth, 2021). Interchangeable terms with “people who use violence and abuse” in this report include “perpetrator” and “people who use violence”.
Poly-victimisation
Poly-victimisation refers to the experience of more than one type of abuse across a person’s life course (Finkelhor et al., 2005). For example, a person who experienced abuse in childhood by a family member and was later victimised by an intimate partner in adulthood is a victim and survivor of poly-victimisation.
Psychological abuse
Psychological abuse refers to emotional, verbal, isolating, coercive and/or controlling behaviours by an intimate partner (Dokkedahl et al., 2022). Usually, psychological abuse encompasses a combination of behaviours that occur over time, and research suggests this type of violence is the most common form of IPV (Dokkedahl et al., 2022). Perpetrated either in person or via technology, psychological abuse may occur in combination with physical and sexual abuse or it may stand alone.
Reproductive coercion
Reproductive coercion is behaviour that interferes with the independent decision-making of a woman in relation to her reproductive health (Grace & Anderson, 2016). In this report, the term “reproductive coercion” is used to refer to the use of force or coercion to compel a woman to become or remain pregnant when she does not want to be (including by tampering with birth control), or to end a pregnancy against her wishes.
Sexual violence (SV)
The term “sexual violence” describes acts of a sexual nature carried out without consent and with force, fear, intimidation or coercion, including rape, attempted rape and other forced sexual activity by an intimate partner, acquaintance or stranger (World Health Organization 2012). For this report, SV does not include unwanted sexual touching or sexual harassment (Cox, 2015).
Technology-facilitated abuse
Technology-facilitated abuse indicates abusive behaviour that is perpetrated via a technological device (e.g. mobile phone, computer) by an intimate partner or someone in a dating relationship (Brown & Hegarty, 2021). Examples of technology-facilitated abuse include monitoring a person’s whereabouts using tracking software or distributing or threatening to distribute nude images or video without permission.
Victim and survivor
The term “victim and survivor” is used with reference to people with lived experience of IPV and/or SV (Elliott et al., 2005). This term was chosen for use throughout the report because it recognises both the harm caused by IPV and/or SV and the strength and resilience of people who have experienced these traumas and continue to survive. “Victim and survivor” is also the language used in the Fourth Action Plan 2019–2022 (Department of Social Services, 2019) of the National Plan. In this research, we are exploring the experiences of women victims and survivors, since they are the main people who experience IPV and/or SV. We acknowledge that children and young people can be victims and survivors in their own right. We also acknowledge that non-binary people and men are victims and survivors, but they were not the focus of this research.
Executive summary
“I just constantly felt like I was running around in a circle.”
(Victim and survivor participant)
“I need to have someone hear me and talk to me, not at me.”
(Male participant who had used IPV and/or SV)
Background
Intimate partner violence (IPV) and sexual violence (SV) are common issues in the community that have negative impacts on the health and wellbeing of women and children victims and survivors. Understanding patterns of abuse and violence and the help-seeking behaviours and needs of both those who experience IPV and/or SV and those people who use IPV and/or SV are needed to inform policy and practice. There has been limited in-depth data collected in Australia that can inform the policy and practice reform needed to support victims and survivors on their pathway to safety and healing, or to engage people who use IPV and/or SV to seek help for their abusive behaviours.
Aim and objectives
The “Voices” project explored:
- experiences of IPV and/or SV, including patterns of abuse and violence and service needs from the perspectives of women victims and survivors
- experiences and service needs of people who use IPV and/or SV against women.
We were interested in “what works” from the perspectives of women victims and survivors and from perpetrators in terms of service responses for themselves and their children.
Method
To gain a deep understanding, we used a mixed methods study, which included data from online surveys of 1,122 women victims and survivors and 563 people who had used IPV and/or SV against women. Interviews were also conducted with 30 women victims and survivors and eight people who had used IPV and/or SV (all male), drawn from the survey participants. Survey participants were recruited through social media and a commercial panel of people who registered for research studies. Participants were eligible if they answered yes to one of the questions in the boxes below.
Box 1: Victim and survivor survey screening items
In the last five years have you:
- Been afraid of a partner of ex-partner?
- Been controlled by a partner or ex-partner?
- Been physically hurt by a partner or ex-partner?
- Experienced unwanted sex by anyone, including a partner or ex-partner?
Box 2: People who use violence survey screening items
In the last five years have you:
- Been concerned about your behaviours in intimate relationships?
- Believed your behaviour has scared a partner or ex-partner?
- Sought help from anyone to address issues in your intimate relationships?
IPV and/or SV was measured using the Composite Abuse Scale (Revised)-Short Form (CASr-SF), which asks about 15 abusive behaviours. However, it’s important to note that participants who did not score on this measure may have experienced IPV and/or SV or used IPV and/or SV. Quantitative data was analysed using STATA and descriptive statistics. Interviews were transcribed and analysed using a thematic approach. Thematic analysis was also utilised to interpret qualitative data from open-ended questions in the survey.
Findings
Victims’ and survivors’ demographics, experiences and health impact
- Female participants were generally nationally representative of the Australian population of women, except more of them were from Victoria (33.4%), or were from Aboriginal and Torres Strait Islander background (7.8%) or reported difficulty managing on their available income (58.5%). There was less representation from women who were employed (59.3%) or were born overseas (18.1%) or for whom English was a second language (7.4%), which is not surprising given the survey was only available in English.
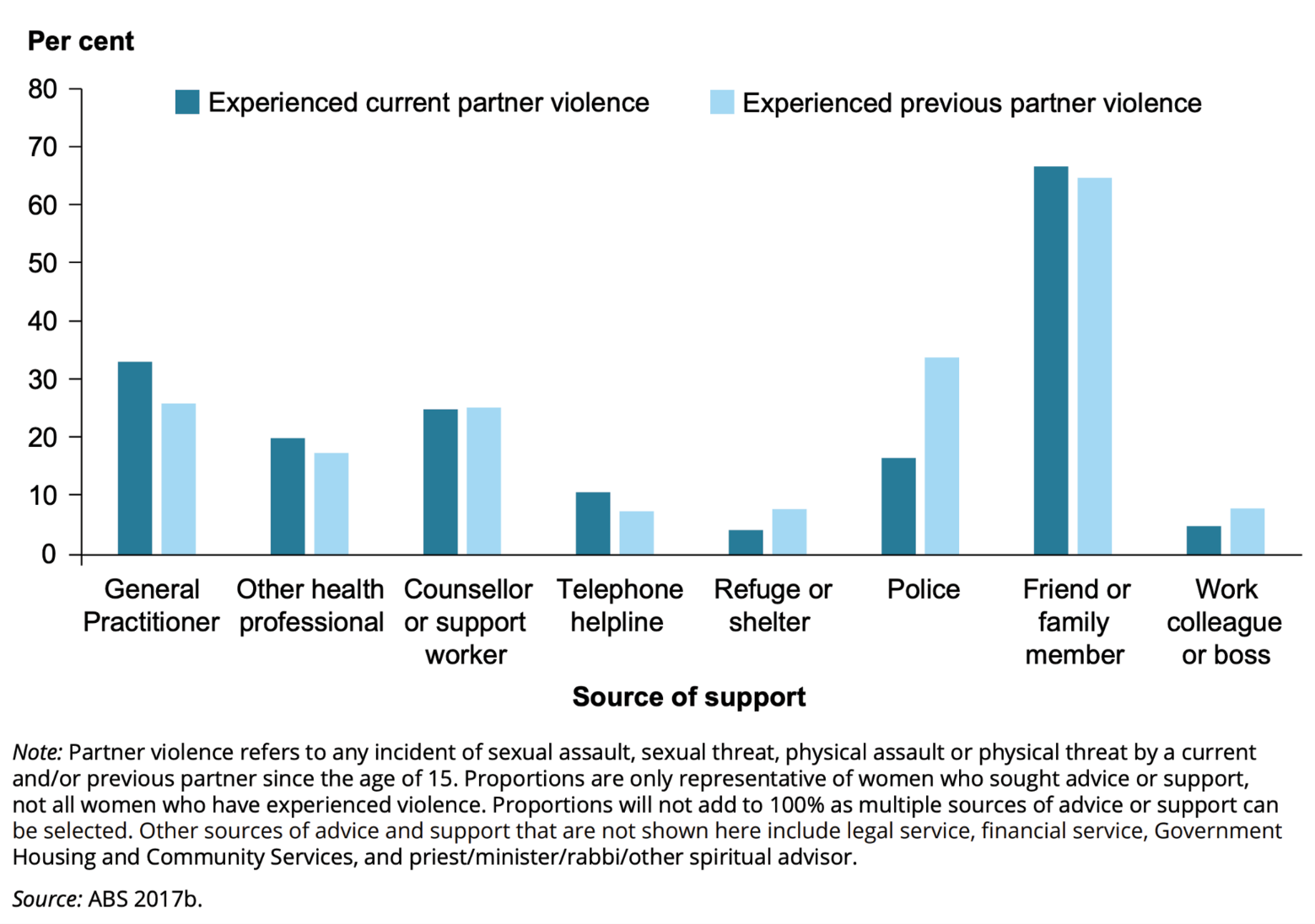
- Patterns of IPV and/or SV showed participants experienced multiple types of IPV rather than one type alone during their lifetime (see Figure 1). Of those women who experienced IPV (905), 60.5 per cent experienced technology-facilitated abuse, 32.9 per cent reproductive coercion and 40.7 per cent financial abuse.
Figure 1: Overlap of types of IPV
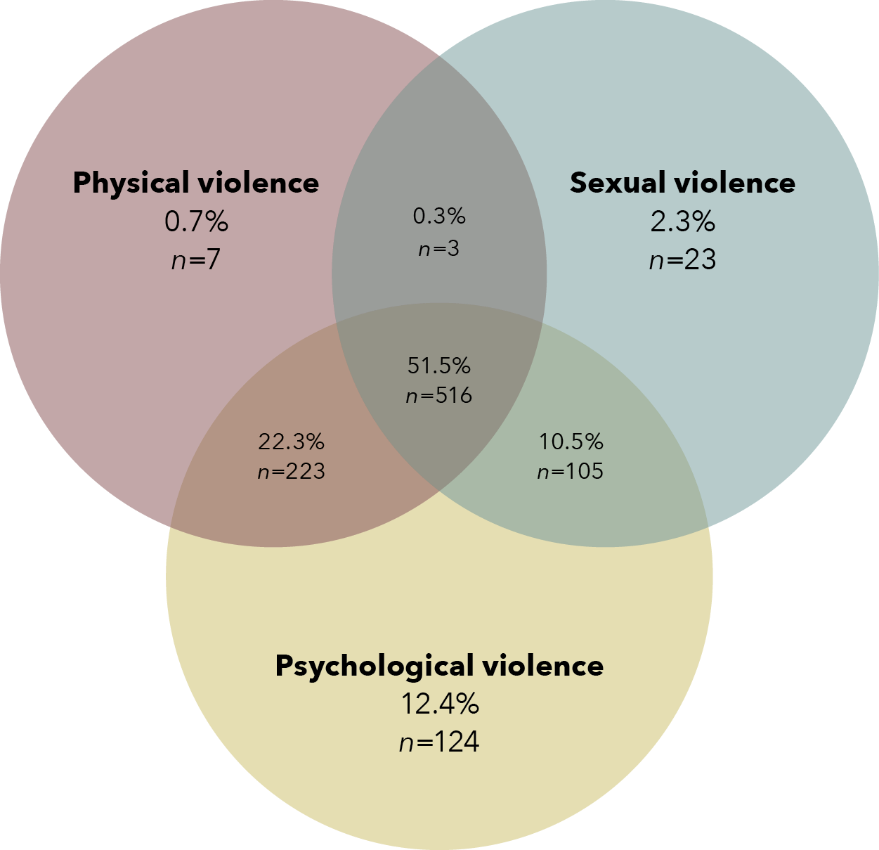
Data table for the figure above:
Type of IPV
Percentage
n
Physical violence
0.7%
7
Sexual violence
2.3%
23
Psychological violence
12.4%
124
Physical and sexual violence
0.3%
3
Physical and psychological violence
22.3%
223
Sexual and psychological violence
10.5%
105
Physical, sexual and psychological violence
51.5%
516
- The vast majority of participants were afraid of their partner or ex-partner (76.1% currently afraid; 80.7% afraid in the last 12 months; and 84.3% ever afraid).
- Poly-victimisation occurred across victims’ and survivors’ lifetimes, with 69.4 per cent experiencing child abuse.
- The burden of disease (see Figure 2) was high, with 71.2 per cent of victims and survivors experiencing probable post-traumatic stress disorder (PTSD), half experiencing other mental health issues (52.4% anxiety symptoms, 45.4% depression symptoms) and over one third affected by disability (39.2%) or rating their health as poor or fair (35.5%).
- These above patterns and health issues were more common in those from Aboriginal and Torres Strait Islander backgrounds and those who were unemployed or who had difficulty managing on their available income.
Figure 2: Percentage of participants with different health issues
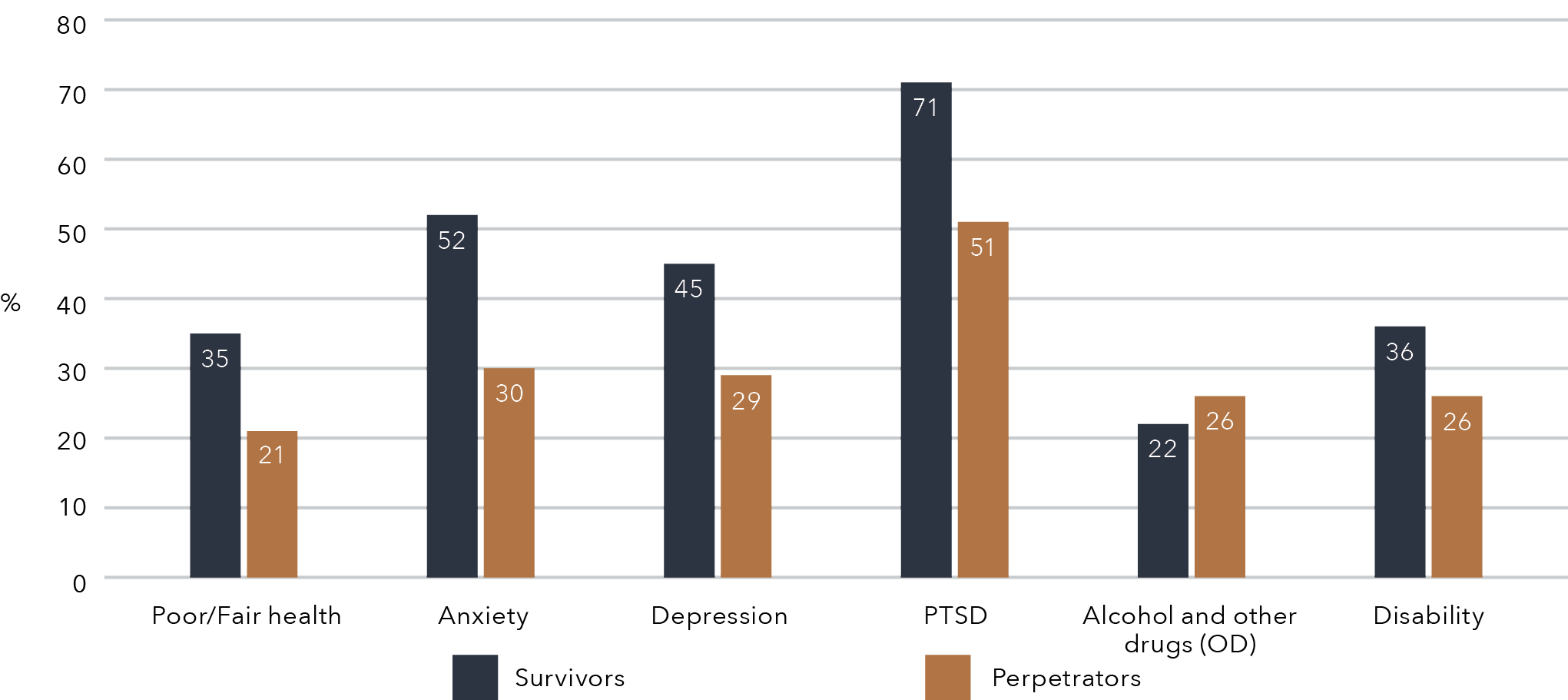
Data table for the figure above:
Health issue
Survivors
Perpetrators
Poor/Fair health
35
21
Anxiety
52
30
Depression
45
29
PTSD
71
51
Alcohol and other drugs (OD)
22
26
Disability
36
26
Demographics, experiences and health issues of people who use violence
- Participants (93.1% men, 5.7% women, 0.9% non-binary and 0.4% prefer not to say) were generally nationally representative of the Australian population, except more of them were aged between 18 and 39 years, were from Victoria (50.7%) or from an Aboriginal or Torres Strait Islander background (10.1%), or reported difficulty managing on their available income (39%). There was less representation from people who were employed (67.8%) or were married (38.1%).
- Over half (58.2%) of the participants reported having ever used IPV and/or SV on the CASr-SF measure, while 44 per cent identified they had ever made their partner feel afraid of them.
- Half of the participants experienced child abuse (47.6%) or PTSD (51.2%), one third experienced anxiety (30.4%) and depression (29%), and one in four reported excessive alcohol consumption (26.2%), living with disability (25.8%) or rated their health as fair or poor (21%; see Figure 2).
- These patterns and health issues were more common in those from Aboriginal and Torres Strait Islander backgrounds and those who were unemployed or who had difficulty managing on their available income.
- A higher proportion of participants held attitudes that were supportive of violence against women when compared to the Australian community (using the National Community Attitudes towards Violence against Women Survey; Webster et al., 2018).
Victims’ and survivors’ help-seeking behaviours
- One in five (21.5%) victims and survivors did not seek any source of formal help for their relationship issues.
- Help-seeking was most commonly sought from family and friends (64.4%) or a health professional (e.g. a psychologist/counsellor, general practitioner, nurse, social worker; 51.4%), with two thirds of victim and survivor participants finding these sources helpful (see Figure 6).
- Fewer participants sought help from specialist IPV and/or SV services (40.1%), police (31.1%) or legal services (19.3%).
Figure 3: Proportion of participants who sought help
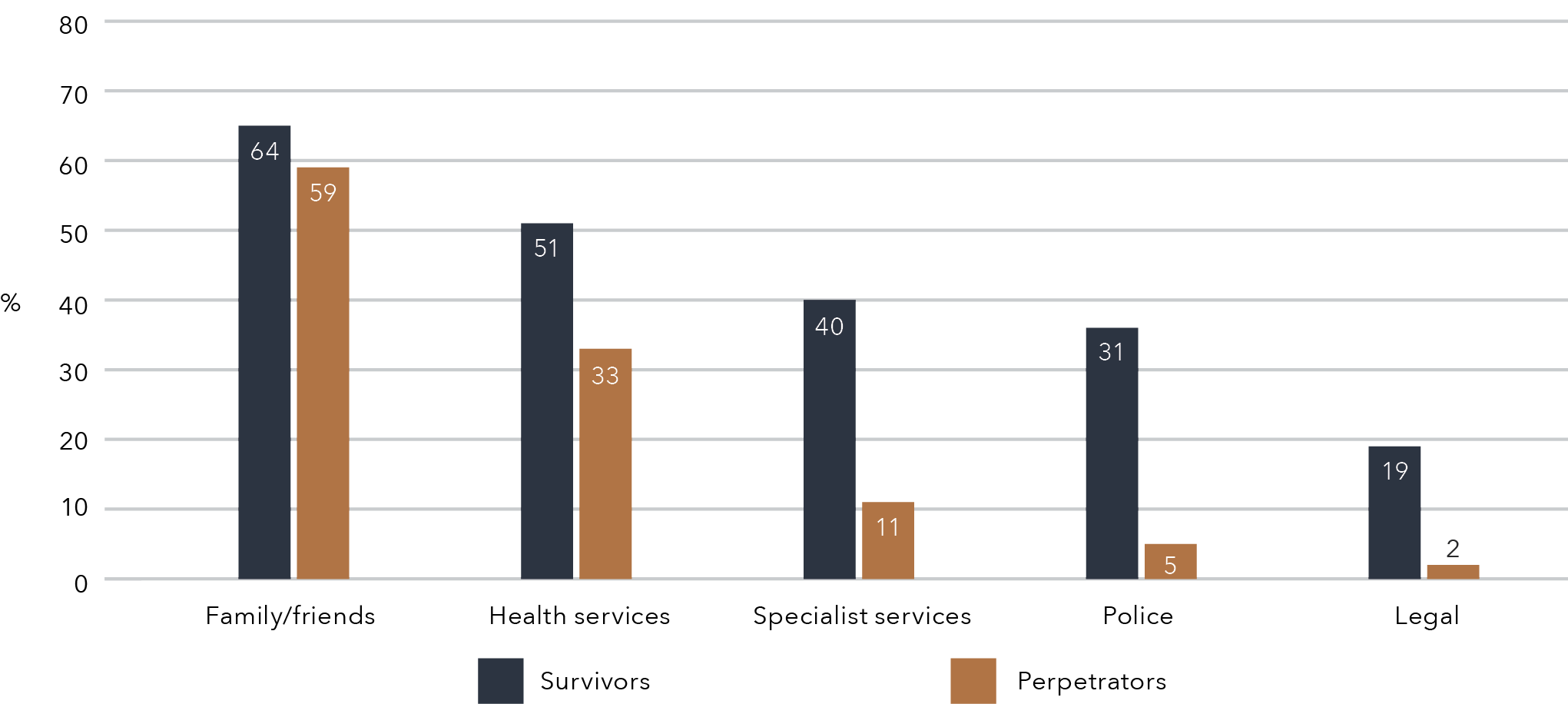
Data table for the figure above:
Participant group
Survivors
Perpetrators
Family/friends
64
59
Health services
51
33
Specialist services
40
11
Police
31
5
Legal
19
2
Help-seeking behaviours of people who use IPV and/or SV
- Almost one third (26.5%) of people who use IPV and/ or SV did not seek any source of help for relationship issues. Help-seeking was most commonly sought from family and friends (58.9%, including partners 31.7%) or a health professional (e.g. psychologist/counsellor, general practitioner, nurse, social worker; 33.3%), with two thirds of participants finding these sources helpful (see Figure 3).
- Fewer participants sought help from specialist IPV and/or SV services (10.8%, including telephone helplines 3.4%), police (4.7%) or legal services (2.3%).
Journeys of help-seeking for women victims and survivors
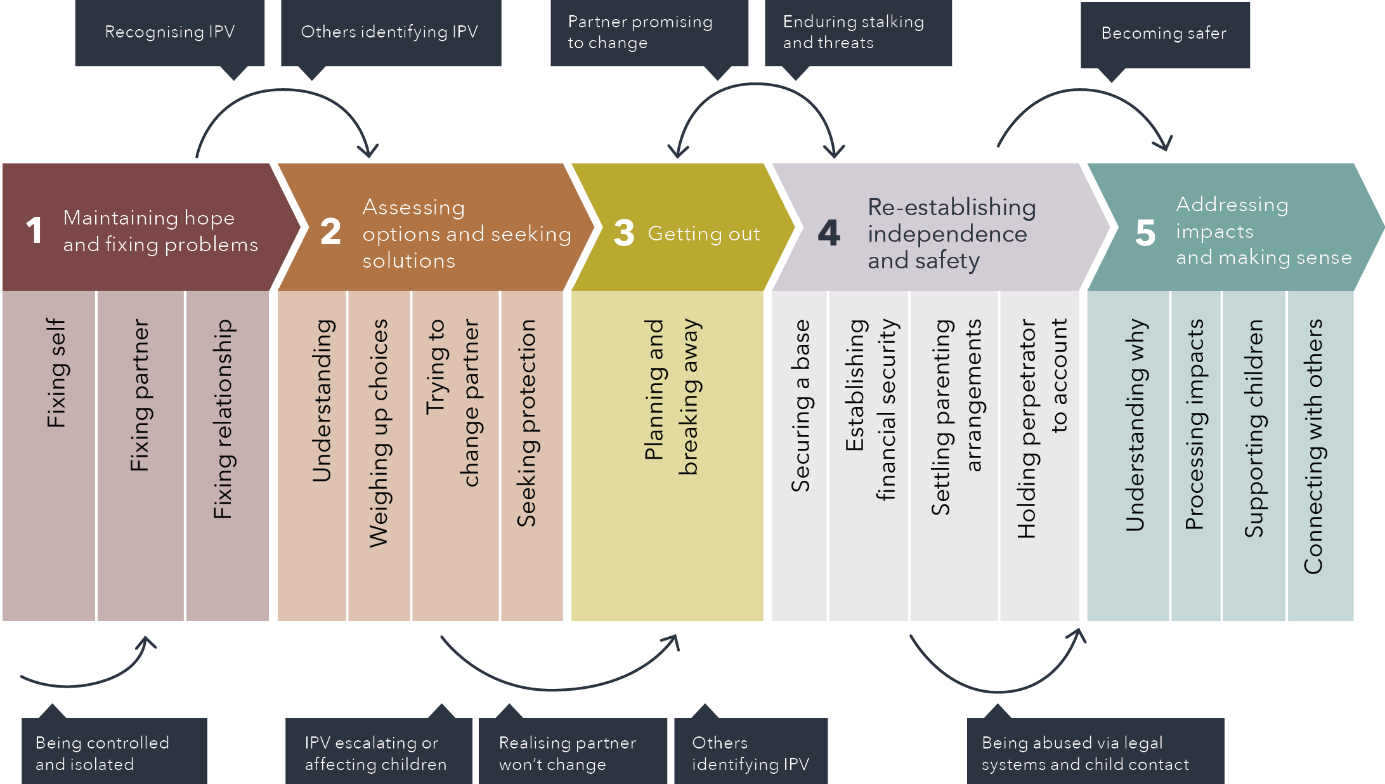
Based on the interview themes and timelines we created from interview data with 30 victim and survivor participants, we identified the following five key stages of help-seeking: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; establishing independence and safety; and addressing impacts and making sense. These stages reflected particular help-seeking needs or goals at different times. Each stage was triggered by critical turning points or changes in how women understood and experienced the abuse. Figure 4 provides a visual illustration of the different stages of participants’ help-seeking journeys and turning points for each stage. Although the stages we identified reflected common needs and turning pointsacross participants’ journeys, it is important to note that not every participant passed through each stage or progressed through stages in the linear order shown in the diagram. For example, many went through a cycle of getting out of the relationship and later returning.
Figure 4: Journeys to help-seeking for victims and survivors of IPV and/or SV
Text version of the figure above:
- Maintaining hope and fixing problems
- Fixing self
- Fixing partners
- Fixing relationship
- Assessing options and seeking solutions
- Understanding
- Weighing up choices
- Trying to change partner
- Seeking protection
- Getting out
- Planning and breaking away
- Re-establishing independence and safety
- Securing a base
- Establishing financial security
- Settling parenting arrangements
- Holding perpetrator to account
- Addressing impacts and making sense
- Understanding why
- Processing impacts
- Supporting children
- Connecting with others
Before step 1 to step 1:
- Being controlled and isolated
Between step 1 and 2:
- Recognising IPV
- Others identifying IPV
Between step 2 and 3
- IPV escalating or affecting children
- Realising partner won’t change
- Others identifying IPV
Between step 3 and 4
- Partner promising to change
- Enduring stalking and threats
Between step 4 and 5
- Behing abused via legal systems and child contact
- Becoming safer
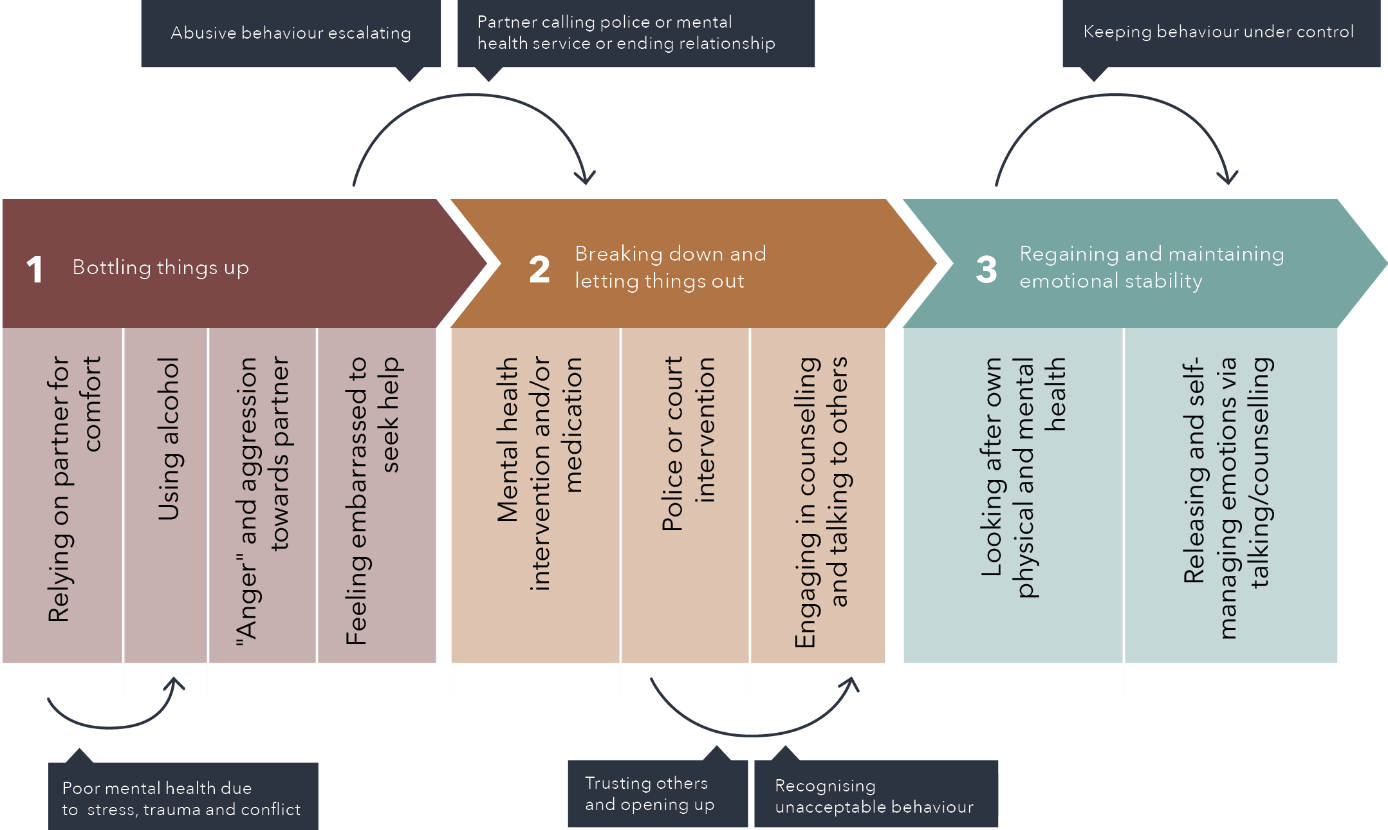
By analysing the themes and timelines regarding how the eight interview participants described their abusive behaviour and their journeys towards change, we identified the following three stages: bottling things up; breaking down and letting things out; and regaining and maintaining control. Figure 5 provides an illustration of these stages and the key turning points in participants’ journeys. The stages reflect the ways in which the eight interview participants framed their journeys of help-seeking to change their behaviour, and it is likely that their journeys were not as linear as the illustration suggests. It should also be noted that all of the interview participants were male, so their journeys may not reflect the help-seeking journeys of people of other genders who use IPV and/or SV against women.
Figure 5: Journeys to help-seeking for people who use violence
Text version of the figure above:
- Bottling things up
- Relying on partner for comfort
- Using alcohol
- “Anger” and aggression toward partner
- Feeling embarrassed to seek help
- Breading down and letting things out
- Mental health intervention and/or medication
- Police or court intervention
- Engaging in counselling and talking to others
- Regaining and maintaining emotional stability
- Looking after own physical and mental health
- Releasing and self-managing emotions via talking/counselling
Before step 1 to step 1:
- Poor mental health due to stress, trauma and conflict
Between steps 1 and 2:
- Abusive behaviour escalating
- Partner calling police or mental health service or ending relationship
Between steps 2 and 3:
- Trusting others and opening up
- Recognising unacceptable behaviour
Within Step 3:
- Keeping behaviour under control
Summary: Voices of victims and survivors of IPV and/or SV
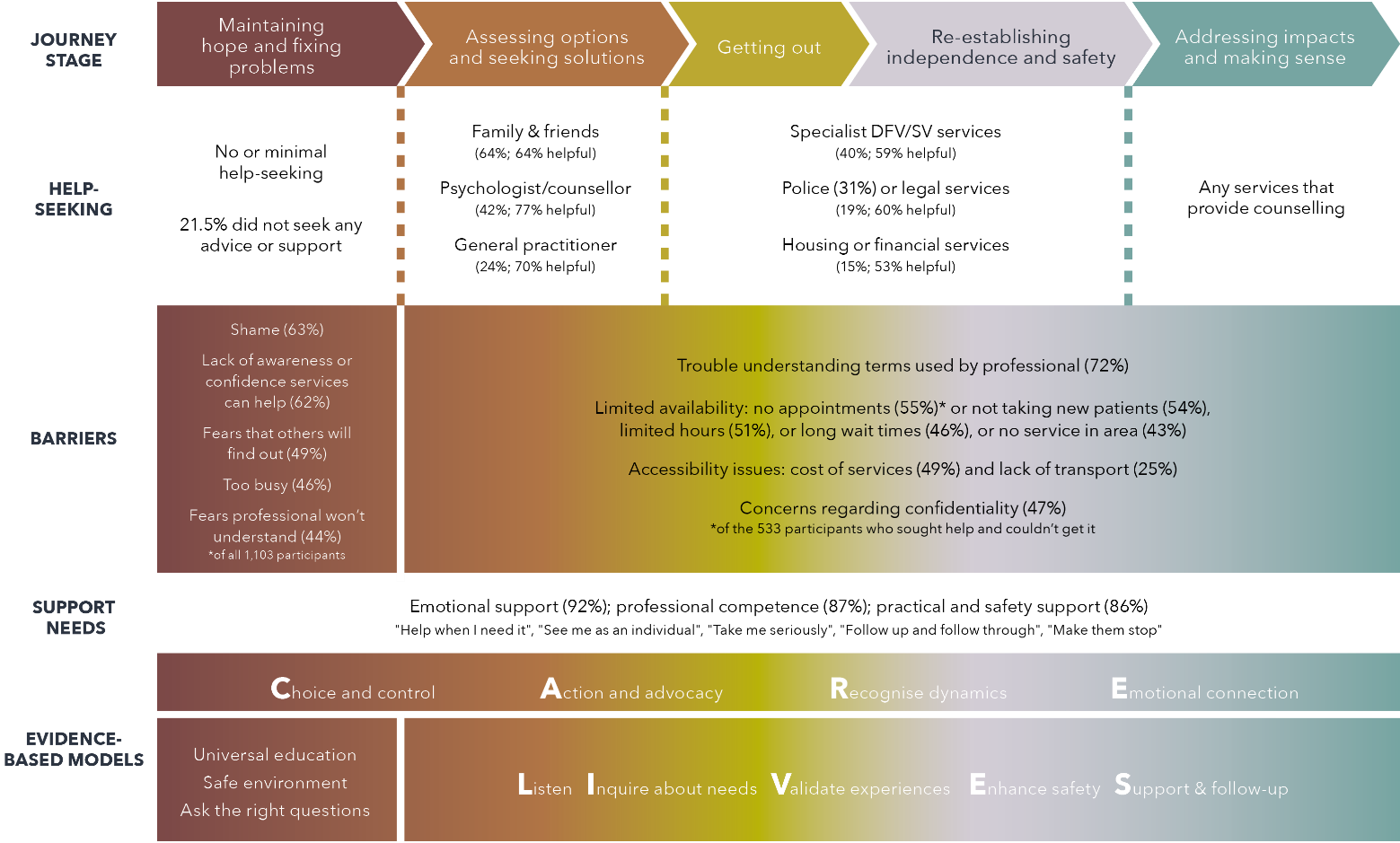
Figure 6 combines the results from the surveys and the interviews with victims and survivors. In the survey, the top three most cited barriers preventing help-seeking were as follows: feeling ashamed (63.2%); lack of awareness about a service that could help (62.1%); and concerns about confidentiality (49.5%). The vast majority of victims and survivors wanted professional competence to provide them with emotional, practical and safety support (see Figure 6).
Figure 6: Help-seeking, barriers, support needs and models for victims and survivors of IPV and/or SV
Text version of the figure above:
Journey stage
- Maintaining hope and fixing problems
- Assessing options and seeking solutions
- Getting out
- Re-establishing independence and safety
- Addressing impacts and making sense
Help-seeking
- Journey stage 1:
-
- No or minimal help-seeking. 21.5% did not seek any advice or support
- Journey stage 2:
-
- Family & Friends (64%; 64% helpful). Psychologist / counsellor (42%; 77% helpful)
- General practitioner (24%; 70% helpful)
- Journey stage 3 and 4:
-
- Specialist DFV/SV services (40%; 59% helpful)
- Police (31%) or legal services (19%; 60% helpful)
- Housing or financial services (15%; 53% helpful)
- Journey stage 5:
-
- Any services that provide counselling
Barriers
- Journey stage 1:
-
- Shame (63%)
- Lack of awareness of confidence services can help (62%)
- Fears that others will find out (49%)
- Too busy (46%)
- Fears professional won’t understand (44%) *of all 1,103 participants
- Journey stage 2 to 5:
-
- Trouble understanding terms used by professional (72%)
- Limited availability: no appointments (55%)* or not taking new patients (54%), limited hours (51%), or long wait times (46%), or no service in area ( 43%)
-
- * of the 533 participants who sought help and couldn’t get it
Support needs
- Emotional support (92%); professional competence (87%); practical and safety support (86%)
-
- “Help when I need it”, “See me as an individual”, ‘Take me seriously”, “Follow up and follow through”, “Make them stop”
- Journey stages 1 to 5:
-
- C.A.R.E – Choice and control, Action and advocacy, Recognise dynamics, Emotional connection
Evidence-based models
- Journey stage 1:
-
- Universal education
- Safe environment
- Ask the right questions
- Journey stages 2 to 5:
-
- L.I.V.E.S – Listen, Inquire about needs, Validate experiences, Enhance safety, Support & follow-up
Summary: Voices of people who use IPV and/or SV
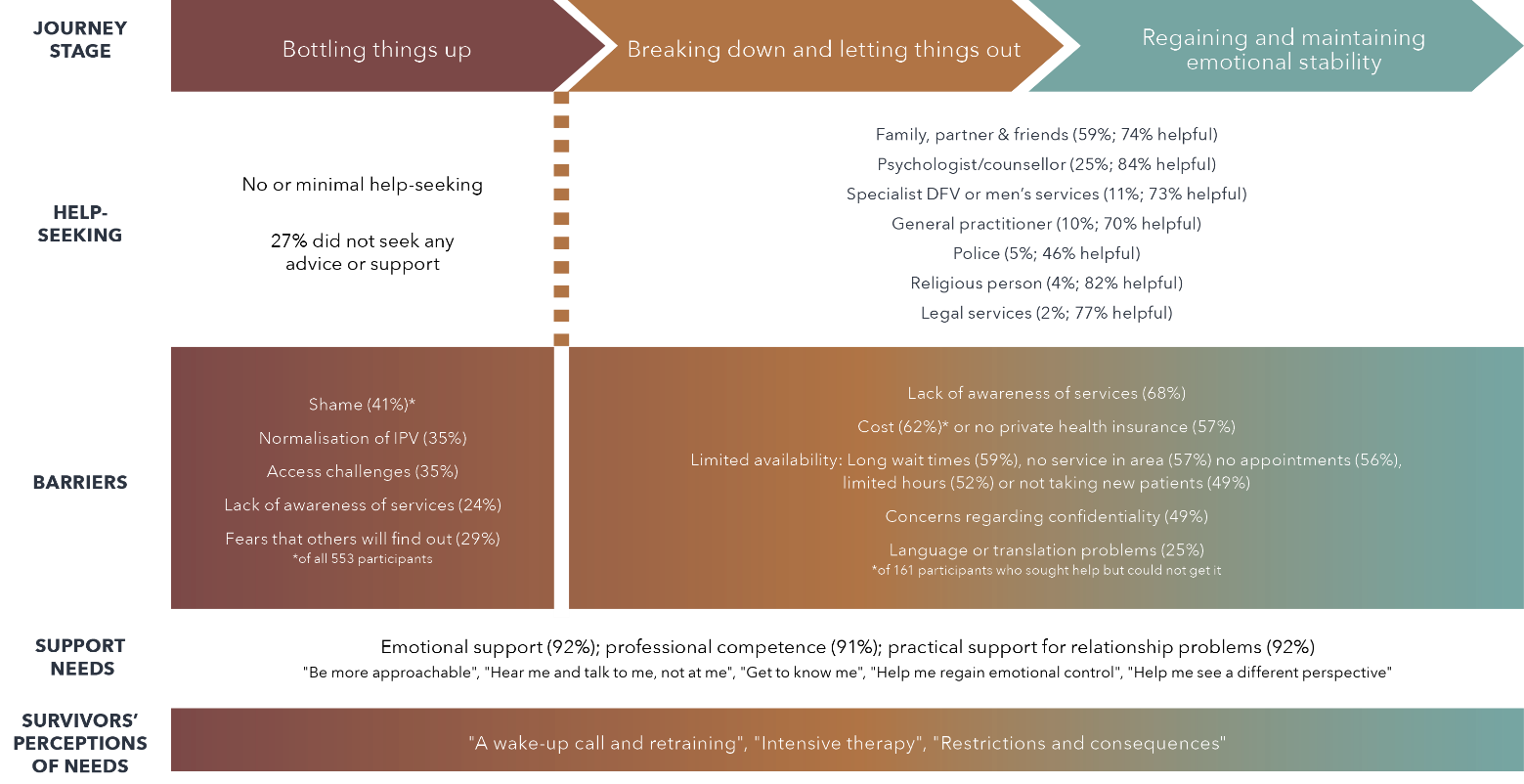
Figure 7 combines the results from the surveys and the interviews with people who use IPV and/or SV. The survey found that the most common barriers that prevented people who used IPV and/or SV from help-seeking were as follows: feeling ashamed (41.4%); a belief that violence is a normal part of a relationship (34.7%); access challenges (34.7%); concerns about confidentiality (29.3%); lack of awareness of services (23.9%); communication issues (22.1%); and not having the time to talk to someone (15.9%). The vast majority of perpetrator participants in the survey wanted professional competence and emotional and practical support for relationship problems. Figure 7 also includes key themes identified by victim and survivor survey participants about their perceptions of what people who use IPV and/or SV need in order to stop their use of violence and abuse. These were for the perpetrator to have “a wake-up call and retraining” to recognise their use ofIPV and/or SV; for them to have “intensive therapy”; and for there to be “restrictions and consequences” for their behaviour.
Figure 7: Help-seeking, barriers and support needs of people who use IPV and/or SV
Text version of the figure above:
Journey stage:
- Bottling things up
- Breaking down and letting things out
- Regaining and maintaining emotional stability
Help-seeking:
- Journey stage 1:
-
- No or minimal help-seeking
- 27% did not seek any advice or support
- Journey stages 2 and 3:
- Family, partner & friends (59%; 75% helpful)
- Psychologist / counsellor (25%; 84% helpful)
- Specialist DFV or men’s services (11%; 73% helpful)
- General practitioner (10%; 70% helpful)
- Police (5%; 46% helpful)
- Religious person (4%; 82% helpful)
- Legal services (2%; 77% helpful)
Barriers:
- Journey stage 1:
-
- Shame (41%) of all 554 participants
- Normalisation of IPV (35%)
- Access challenges (35%)
- Lack of awareness of services (24%)
- Fears that others will find out (29%)
- Journey stages 2 and 3:
- Lack of awareness of services (68%)
- Cost (62%) of 161 participants who sought help but could not get it or no private health insurance (57%)
- Limited availability: Long wait times (59%), no service in area (57%), no appointments (56%), limited hours (52%) or not taking new patients (49%)
- Concerns regarding confidentiality (49%)
- Language or translation problems (25%)
Support needs:
- Journey stags 1 to 3:
-
- Emotional support (92%)
- Professional competence (91%)
- Practical support for relationship problems (92%)
- “Be more approachable”, “Hear me and talk to me, not at me”, “Get to know me”, “Help me regain emotional control”, “Help me see a difference perspective”
Survivors’ perceptions of needs
- Journey stages 1 to 3:
-
- “A wake-up call and retraining”, “Intensive therapy”, “Restriction and consequences”
Implications for policy and practice
The recommendations below are derived from a synthesis of all the findings in the Voices project (see Figure 8). They highlight reform that is needed aimed at policy and practice levels for the community, social networks, early engagement services, system access and ongoing response services. They are particularly focused on areas that need the most reform or are less highlighted in the draft National Plan to End Violence against Women and Children 2022–2032 (the draft National Plan), which is still to be finalised at the time of writing. Individual policy briefs can be provided for any recommendations likely to be moved forward as part of this plan.
We have included in our recommendations some overarching principles for responses across the service system, including the need to:
- recognise the impacts of IPV and/or SV on children, by developing mechanisms for children’s voices to inform reforms and offering accessible therapeutic support for children
- respond to the diversity of the Australian community, by investing in responses tailored for people with diverse backgrounds and experiences of structural inequalities
- promote change, by offering sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
Across the Australian community, we recommend that the following be provided:
- universal education to assist community members to identify healthy and abusive behaviours in relationships
- enhanced public messaging to raise awareness of affordable and confidential supports available, including helplines for victims and survivors and people who use IPV and/or SV
- financial interventions (e.g. microfinancing) to alleviate financial distress for victims and survivors, so they can obtain the support and resources they need for their safety and wellbeing.
To improve the responses of members of the victim’s and survivor’s and the perpetrator’s social networks, we recommend the following approaches be developed and delivered:
- “allies training” for family, friends and community members to support victims and survivors, using the CARE model (Choice and control, Action and advocacy, Recognition and understanding, Emotional connection; Tarzia, Bohren, et al., 2020)
- “First responder healthy relationships first aid” for workplaces and faith-based organisations, using the LIVES model (Listen, Inquire about needs, Validate, Enhance safety, Support; (World Health Organization, 2013b)
- “engaging men” training for family, friends and community members so they can respond effectively to men who use IPV and/or SV.
To encourage victims and survivors and perpetrators to engage early in seeking professional help, we recommend:
- fostering professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- fostering the capacity of general practice, mental health and counselling services to engage people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
To improve the accessibility of the service system, we recommend:
- ongoing flexible service delivery (telehealth or online) across sectors for victims and survivors and people who use IPV and/or SV
- the resourcing of “care navigators” who can provide accessible and affordable long-term individual support and advocacy for victims and survivors
- accessible messaging to be provided about the limits of service confidentiality, to help address the barriers to accessing support.
To improve the ongoing support available for victims and survivors to address the impacts of IPV and/or SV, we recommend the following responses be resourced:
- Aboriginal and Torres Strait Islander–led centres for healing for all members of the family in each state, developed by local communities for local communities
- trauma- and violence-informed recovery and healing services in each state
- peer victim and survivor–led support groups in each state
- trauma- and violence-informed care from general practice and private mental health services to be funded through the Medicare Benefits Scheme.
Figure 8: Recommendations
Overarching principles
Recognise children:
Develop mechanisms for children’s voices to inform reforms and offer accessible therapeutic support for children.
Respond to diversity:
Invest in responses tailors for people with diverse backgrounds experiences of structural inequalities.
Promote change:
Offer sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
Community
Provide
- Universal education on healthy and abusive relationship behaviours
- Enhanced public messaging about available, affordable and confidential supports, including helplines for victims and survivors and people who use IPV and/or SV
- Financial interventions (eg. microfinancing) to alleviate financial distress for victims and survivors.
Social networks

Develop and deliver
- “Allies training” for family, friends and community using the CARE victim and survivor model
- “First responder healthy relationships first aid” for family, friends, workplaces, and faith-based organisations using the LIVES model
- “Engaging men” training for family and friends to engage effectively with men who use IPV and/or SV
Early engagement

Foster
- Professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- Capacity of general practice, mental health and counselling services to engage with people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
System access

Offer
- Ongoing flexible service delivery (telehealth/online) across sectors for victims and survivors and people who use IPV and/or SV
- “Care navigators” for pathways to accessible and affordable long-term support and advocacy for victims and survivors
- Accessible messaging about limits of confidentiality to overcome barriers to accessing support.
Ongoing response

Response
- Aboriginal and Torres Strait Islander-led centres for healing for all members of the family in each state
- Trauma- and violence-informed recovery and healing services in each state
- Peer victim and survivor-led support groups in each state
- Trauma- and violence- informed care through the Medicare Benefits Scheme for general practice and private mental health services
Conclusion
This mixed methods study has provided insights into the voices of victims and survivors and people who use IPV and/or SV across Australia in terms of what might assist them in their journeys to help-seeking and what support they value. The key role of family and friends and health services in early engagement is highlighted. Recommendations across the service system are suggested for policy and practice that are likely to advance the prevention and response to IPV and/or SV. We no longer want victims and survivors having to go around in circles to find support, as shown by this quote from an interview participant:
You get referred here, there, and everywhere. In the beginning you’re on so many phone calls, you can’t remember who you were talking to, where they’re from. You go through the same story hundreds of times, and you just get completely lost. You can’t remember any of it. Then with the practical assistance you get is very little to none. This person will go, “Oh no we can’t help you with that, but here, try this person”, and they’ll go, “Oh no we can’t do that, try this person”, and then you get referred back to where you started at. It’s really frustrating.
We also need to hear the voices of people who use IPV and/or SV, in order to know how to engage them in behaviour change, as shown by this quote from a survey participant:
Just feeling safe and heard during conversation. That would be the most important thing I would expect from a service or professional. Sometimes just hearing your thoughts said out loud is enough to realise what personal plan of action you must take to change your behaviour, which would hopefully be bolstered by the professionals’ help.
Part A:
Introduction
Part A provides an overview of the background, literature review and policy context for the project. We then discuss the research gaps this project is filling and describe the aims of the project. The next part, Part B, will provide detail of the methodology for the quantitative and qualitative aspects of the project. Findings are then divided into Part C with three sections on women who have experienced intimate partner violence (IPV) and/or sexual violence (SV), Part D with three sections on people who use IPV and/or SV and Part E on children’s experiences and support needs. Part F is the discussion, which provides a synthesis of what works from the perspective of victims and survivors and people who use IPV and/or SV. We conclude with implications for policy and practice.
Background
IPV and SV are major health and human rights issues (World Health Organization, 2013a). IPV is defined as any behaviour within an intimate relationship that causes physical, psychological or sexual harm (World Health Organization, 2013a). A feature of IPV is ongoing patterns of abusive behaviours and tactics used to control and take power away from women and their children (Council of Australian Governments, 2012, p. 2). SV is defined as any act (or attempted act) of a sexual nature perpetrated by one person against another without the victim’s consent (World Health Organization, 2013a). SV may occur at the hands of a partner or ex-partner but can also be perpetrated by family members, acquaintances or strangers. Men are more likely than women to use abuse and violence more frequently and severely so that female victims and survivors are more likely to fear for their lives, or to be injured or killed by a partner (World Health Organization, 2013a).
IPV has wide-ranging impacts on individuals, families and communities, including poor mental and physical health (Webster, 2016), injury, hospitalisation and loss of work productivity (PriceWaterhouseCoopers Australia, 2015; World Health Organization, 2013a). For women, IPV is the most common cause of injury (World Health Organization, 2013b) and causes half of female homicides in Australia (Shackelford & Mouzos, 2005). For men, using IPV is associated with increased alcohol and substance use, depression, suicidal thoughts, anxiety and low self-esteem (Oram et al., 2013). For children, IPV-related trauma is cumulative in impact and associated with social, behavioural, emotional and cognitive problems, persisting into adulthood (Felitti & Anda, 2010).
In Australia, one in six women have experienced physical or sexual violence by a current or previous partner since the age of 15. One in four women have experienced emotional abuse (Australian Institute of Health and Welfare, 2018). However, despite the high prevalence of IPV and SV, there is a dearth of research – including within the Australian context – exploring the nature of abuse from the perspectives of victims and perpetrators to enable tailored responses. In particular, more research is needed into the nature or patterns of abuse and violence that are non-physical – for example, sexual violence, financial control, emotional abuse, non-physical coercive control, technology-facilitated abuse and systems-facilitated violence (Ayre et al., 2016; Cortis & Bullen, 2016).
Further, we do not have detailed research on the help-seeking behaviours and service needs of victims and survivors, or those of people who use IPV and/or SV. The 2016 Australian-based Personal Safety Survey data (Australian Bureau of Statistics, 2016) indicate that most women seek help from friends or family members, followed by health practitioners and then police (Figure 9). Little is known, however, about their experiences accessing these supports and services, the barriers to help-seeking, what they want services to do, and what could be done better to promote more effective delivery of support. Almost nothing is known about the help-seeking behaviours of people who use IPV and/or SV or their service needs. This critical gap is a major focus of this report, as we sought to identify “what works” for women victims and survivors, and people who use IPV and/or SV in Australia. In the next section, we providean overview of the Australian literature to highlight specific gaps in our knowledge of help-seeking. More details about the literature review undertaken are in Appendix A.
Figure 9: Women’s help-seeking to formal and informal services (Australian Institute of Health and Welfare, 2018)
Data table for the figure above:
Service
Experienced current partner violence
Experienced previous partner violence
General practitioner
33.14%
25.88%
Other health professional
20.04%
17.51%
Counsellor or support worker
25.19%
25.25%
Telephone helpline
10.73%
7.42%
Refuge or shelter
4.26%
7.73%
Police
16.57%
33.93%
Friend or family member
66.75%
64.85%
Work colleague or boss
4.89%
7.89%
Note: Partner violence refers to any incident of sexual assault, sexual threat, physical assault or physical threat by a current and/or previous partner since the age of 15. Proportions are only representative of women who sought advice or support, not all women who have experienced violence. Proportions will not add to 100% as multiple sources of advice or support can be selected. Other sources of advice and support at not shown here including legal service, financial service, Government House and Community Services, and priest/minister/rabbi/other spiritual advisor.
Source: ABS 2017b
Overview of the literature on help-seeking for IPV and/or SV
We undertook a rapid systematic review of the peer-reviewed literature focused on the help-seeking behaviours and service needs of both victims and survivors of IPV and/or SV and people who use IPV and/or SV (see Appendix A for details). We identified relevant studies and reviews of the literature using a systematic search of key bibliographic databases (MEDLINE, Embase, PsycINFO, Cochrane Database, Applied Social Sciences Index and Abstracts: ASSIA, Web of Science, PsycArticles and Scopus). The search was conducted during September 2020, using relevant subject headings and key terms. This was informally updated in May 2022 to include more recent review articles. We also checked the reference lists of all included records to identify additional studies, and undertook hand-searching and communication with experts in the field to identify any further potentially relevant sources of data. All searches were filtered to 1 January 2010 onwards to findliterature related to contemporary service delivery.
The full search results are outlined in Appendix A. To provide context for our study, in the below sections we first summarise the primary studies (11 qualitative and four quantitative) undertaken in Australia between 2010 and 2020 and related to either women’s experiences of help-seeking after IPV and/or SV or help-seeking by people who use IPV/SV against women. Second, we outline the findings from recent systematic reviews (2020 onwards) focused on help-seeking by victims and survivors or perpetrators of IPV and/or SV.
Australian context 2010–2020
Overall, the evidence base in relation to the experiences and needs of women in Australia who have experienced IPV and/or SV is populated largely by qualitative studies (Day et al., 2018; Meyer & Stambe, 2021). These focused mainly on discrete aspects of help-seeking, for example disclosure experiences in particular settings, such as hospital emergency departments, general practice clinics, or the court system (Meyer, 2011; O’Doherty et al., 2016; Reisenhofer & Seibold, 2013); and the impact of particular contextual factors on help-seeking, such as rurality, migration status or being incarcerated (Day et al., 2018; Ghafournia & Easteal, 2019; Ragusa, 2016; Wendt et al., 2017). One study (Meyer, 2010a) examined how having children impacted on women’s help-seeking decisions in a small Queensland sample. Another Queensland study (Meyer, 2016) explored women’s experiences of victim-blaming when trying to access support after IPV. Morerecently, Tarzia and colleagues (2018) investigated women’s perceptions about online help-seeking, comparing their experiences to those who had sought help from a specially trained general practitioner. The findings suggested that preferences for help-seeking (online vs. face-to-face) were shaped by whether women prioritised a trusting relationship with a professional or autonomy and control over their help-seeking journey. Only one report was found that addressed women’s help-seeking experiences after SV (Hegarty et al., 2017), finding that women wanted to be heard, to be connected with a range of services, and to be helped to heal holistically.
Quantitative studies addressing women’s help-seeking in the Australian context were lacking. We found only three studies utilising cross-sectional surveys to explore help-seeking behaviours for IPV: one focused on postpartum women (Hooker et al., 2020), one on migrant women (Satyen et al., 2018), and one broader study on women’s decisions on whether and where to seek help (Meyer, 2010b). These studies suggest that women who had experienced IPV were more likely to use community and health services (Hooker et al., 2020) than women who had no IPV history, and that children witnessing IPV was the strongest predictor of initiating help-seeking (Meyer, 2010b). For Australian migrant women, many refrained from seeking help at all (Satyen et al., 2018). One study by Hegarty and colleagues (2013) found that women experiencing IPV sought help frequently, but from health or counselling services more than specialist IPV services. Severity of violence increasedthe likelihood of help-seeking. Limitations of these studies included a very low response rate to the surveys (Hooker et al., 2020) and a small sample size (Satyen et al., 2018).
No Australian studies were found exploring the help-seeking experiences or service needs of people who use IPV and/or SV.
Table 1: Characteristics of quantitative Australian-based studies exploring women’s help-seeking for IPV and/or SV
Authors
Aim and objectives
Design and data collection method
Participants
Data analysis
Summary of findings
Study quality and limitations
Hegarty et al., 2016
To explore associations between type and severity of IPV and health, quality of life and help-seeking
Baseline survey from randomised controlled trial
272 women recruited from general practices who had experienced IPV
Logistic regression
Women who had experienced severe or combined physical/emotional abuse were more likely than the other women to have visited a counsellor, social worker or psychologist in the past 12 months.
Participants also used healthcare services frequently but specialist domestic violence services infrequently
Sample may not be representative of all women attending primary care
Self-report measures
Hooker et al., 2020
To examine the help-seeking behaviour and perceived helpfulness of services in abused and non-abused postpartum women
Cross-sectional survey
2,621 women recruited from maternal and child health settings
Descriptive and interferential statistics
Women who had experienced IPV sought:
informal family support less frequently (81.3% compared with 92.4%, p < .001)
were more frequent users of hospital emergency departments (p = .03), nurse home visiting programs (p = .02) and some breastfeeding services (p = .001), compared with non-abused women
Very low response rate to survey (25%)
Respondents had a higher socio-economic status compared to non-responders
Meyer, 2010
To explore factors that influence victims’ decisions on whether and where to seek help
Australian national survey
2,276 women who had experienced IPV
Bivariate and multivariate analyses
While the presence of unborn children (i.e. pregnancy) had no effect on victims’ help-seeking decisions, children witnessing the abuse emerged as the strongest predictor of general and more formalised help-seeking decisions
Survey data only offer a snapshot of help-seeking decisions at one point in time
Satyen et al., 2018
To explore Australian migrant women’s help-seeking for IPV
Cross-sectional survey
130 migrant women who had experienced IPV
Descriptive and regression analysis
Most women who had experienced IPV indicated that they needed
help; however, many refrained from seeking it
Small sample size
Reluctance of women to seek help warrants further research
Table 2: Characteristics of qualitative Australian-based studies exploring women’s help-seeking for IPV and/or SV
Authors
Aim and objectives
Design and data collection method
Participants
Data analysis
Summary of findings
Study quality and limitations
Day et al., 2018
To explore help-seeking of women for IPV
Semi-structured interviews
22 women who had been incarcerated
Thematic analysis
Barriers to help-seeking included:
- fear of the police
- fear of having children removed
- attitudes of services towards ex-prisoners
- perceived lack of acknowledgement of IPV in prison
- Small sample size in one jurisdiction
Ghafournia & Easteal, 2019
To explore the help-seeking experiences of Muslim immigrant women who have experienced IPV
Semi-structured interviews
14 women who had experienced IPV
Thematic analysis
Barriers to help-seeking included:
- fear of repercussions (visa insecurity)
- desire to keep family together
- fear of child removal
- xenophobia/racism from services
- fear of judgement from community.
Women typically first accessed informal support. Formal support was found to be helpful but was only accessed at later stages
- Small sample size
- Women had already sought previous help
Meyer, 2010a
To explore women’s help-seeking for IPV when children are present
Semi-structured interviews
29 women who had experienced IPV in Qld
Thematic analysis
Barriers to help-seeking included:
stereotypical and victim-blaming attitudes along with a lack of understanding of the dynamics of IPV
fear of harm and loss of custody.
After disclosure, women felt trapped between expectations to protect their children by leaving the abusive partner and a reluctance on behalf of judges and magistrates to offer the necessary protection by including children on granted domestic violence orders (DVOs)
- Lack of diversity in sample
- Women had mostly experienced severe violence
Meyer, 2011
To explore women’s help-seeking through the criminal justice system after IPV
Semi-structured interviews
29 women who had experienced IPV in Qld
Thematic analysis
Barriers to help-seeking included:
- fear of gendered discrimination or lack of support from police
- fear of retribution from perpetrator
- lack of time to go through lengthy police reporting process
- feeling that help would not be provided if they did not leave
- court/magistrates lack understanding of dynamics of IPV
- reluctance to include children in DVOs
- Lack of diversity in sample
- Women had mostly experienced severe violence
Meyer, 2016
To explore women’s experiences seeking help after IPV
Semi-structured interviews
28 women who had experienced IPV in Qld
Thematic analysis
Women encountered blaming attitudes when seeking help from informal and general formal support sources
- Lack of diversity in sample
- Women had mostly experienced severe violence
Meyer & Stambe, 2021
To explore women’s help-seeking decisions and recovery from IPV
Semi-structured interviews
13 Indigenous women in regional Qld who had experienced IPV
Thematic analysis
- Help-seeking for IPV was complicated by social and cultural marginalisation, spiritual disconnectedness and the close-knit nature of regional Indigenous communities and related community expectations and to some extent community “monitoring”.
- Family is perceived as both a stressor and protective factor
- Small sample size in one regional jurisdiction
O’Doherty et al., 2016
To explore the impacts of abuse on identity and its role in help-seeking
Semi-structured interviews
14 women who had experienced IPV
Inductive/deductive thematic analysis
- Concealing one’s “abuse identity” was a barrier to help-seeking.
- Damage to identity caused by perpetrator tipped balance in favour of help-seeking.
- Positive response allows safe expression of abuse identity
- Convenience sample
- Participants recruited only from metropolitan areas
Ragusa, 2013
To explore legal help-seeking experiences of rural Australian women who experience IPV
Semi-structured interviews
36 women living in rural areas
Thematic analysis
Findings reveal that police and court responses reflect broader social inequalities and rurality exacerbates concerns such as anonymity and lack of service
- Small sample size and reliance on social service agency recommendations for selecting participants
Reisenhofer & Seibold, 2013
To explore emergency healthcare experiences of women who experience IPV
Semi-structured interviews
7 women who had experienced IPV and sought emergency or primary healthcare
Grounded theory
Barriers to help-seeking included:
- perpetrator always present
- fear and shame
- women wanted empathy and care rather than pity and blame
- Small sample size
Tarzia et al., 2018
To compare women’s experiences of help-seeking online with help-seeking face-to-face via a general practitioner
Semi-structured interviews
16 women who had experienced IPV (8 who had used online support and 8 face-to-face)
Thematic analysis
Women who value control in help-seeking journey may prefer online support for IPV, whereas women who value trust may prefer face-to-face support from a trained professional
- Small sample size
- Women recruited from 2 different projects so not a direct comparison of different support modalities
Wendt et al., 2017
To explore how geographical and social isolation impacts on help-seeking experiences among rural women
Semi-structured interviews
23 women
(6 Aboriginal)
Thematic analysis
Shame and embarrassment and social isolation (particularly for non-Aboriginal women) were main barriers. Geographical isolation was not a barrier
- Convenience sample
- Only women who had sought help were recruited
Recent reviews about help-seeking in a global context (2020–2022)
In May 2022, we informally updated our rapid review by undertaking a scan of the literature published since our initial review in 2020. We focused on review articles (such as systematic, narrative, integrative or scoping reviews; meta-analyses; meta-syntheses) summarising the literature from anywhere in the world. We identified 14 reviews on help-seeking by IPV and/or SV victims and survivors; one on the help-seeking of people who use IPV; and one addressing both victims and survivors and perpetrators of IPV. These have shed more light on the complexities and nuances of help-seeking for IPV and/or SV, particularly in relation to differing forms of IPV and help-seeking by people from marginalised populations.
Six of the reviews explored formal help-seeking, including the factors that facilitated or prevented help-seeking from service providers in the United States (Ravi et al., 2021; Robinson et al., 2020); the factors that silenced victims and survivors and prevented them from seeking formal help (Pokharel et al., 2020); and the factors that impacted disclosure and experiences of care within health settings (Heron & Eisma, 2021; Tarzia, Bohren, et al., 2020). Zinzow and colleagues (2021) explored the barriers to formal help-seeking for SV, situating these within an ecological framework. Two reviews comprehensively reviewed the qualitative literature on help-seeking for IPV in health settings (Heron & Eisma, 2021; Tarzia, Bohren, et al., 2020). The majority of the reviewed studies were assessed to be of good quality, though most were undertaken in Western countries and there was a lack of data from low- and-middle-income countries. Takentogether, these six reviews indicate that individual factors (particularly victim and survivor self-blame and concern about the impacts of disclosure on children or family) are important barriers to disclosing and seeking formal help, along with societal or structural factors, such as immigration policies, gender norms and pressures on women to present an image of a happy family (Heron & Eisma, 2021; Pokharel et al., 2020). The literature also identifies that how a potential disclosure recipient interacts with the victim and survivor plays a critical role in whether a victim and survivor discloses and/or continues to seek help. Receiving supportive responses from friends and family can be an important facilitator of formal help-seeking by victims and survivors (Ravi et al., 2021). Further, how healthcare providers and other services engage with victims and survivors – such as by being open and empathic, asking directly about abusive behaviours, and listening toand believing the victims and survivors – is critically important in facilitating help-seeking (Heron & Eisma, 2021; Ravi et al., 2021; Tarzia, Bohren, et al., 2020). Other key factors at the service level are the provider’s knowledge about IPV and the experiences of people from cultural, racial, sexual or other minorities; service accessibility (including location); and whether the provider caters for people with disability or those who speak different languages.
Recent reviews have further illuminated how marginalisation influences help-seeking. These include studies of the experiences of women who are South Asian (Sripada, 2021) and African American (Waller et al., 2021), and a study of victims and survivors with criminal backgrounds (Iratzoqui & Cohn, 2020). Consistent with the findings of the literature reviews discussed earlier, these reviews identify particular barriers to reporting IPV or seeking help for those from marginalised communities, including cultural stereotypes about African American women, which may become internalised (Waller et al., 2021), as well as a fear of negative responses from authorities or service providers for victims and survivors with criminal backgrounds (Iratzoqui & Cohn, 2020). Stigma and discrimination have also been identified as concerns for lesbian, gay, bisexual, trans and gender diverse, queer and questioning (LGBTQ) victims and survivors of IPV and/or SV(Edwards et al., 2022; Peitzmeier et al., 2020; Santoniccolo et al., 2021). Two recent systematic reviews of the help-seeking behaviours of sexual or gender minorities (one on IPV and one on SV) indicated a preference for relying on friends, family and other informal sources of support, while fear of being “outed”, homophobia and a heteronormative framing of relationships were barriers to using formal services (Santoniccolo et al., 2021). Similarly, a review of literature on IPV experiences of transgender people found experiences of discrimination when seeking help from services were common (Peitzmeier et al., 2020).
The literature also suggests that problematic behaviours are often normalised in relationships, which means victims and survivors do not identify them as abusive or feel that they have a legitimate reason to seek help (Pokharel et al., 2020). This may particularly be the case for women who are subjected to sexual forms of violence from a partner, according to the findings of a systematic review of 17 studies of SV by an intimate partner (Wright et al., 2021). Compared to other forms of IPV, experiencing SV by an intimate partner was associated with increased help-seeking from social, medical or legal services, yet also with decreased help-seeking from informal sources. The authors suggest the physical consequences of SV, such as pregnancies or sexually transmitted diseases, may prompt victims and survivors to seek formal help, while a social norm about keeping sexual relationships private may contribute to their reluctance to confide in family andfriends. A normalisation of abuse by a partner was also a barrier identified in a review of studies on help-seeking for elder abuse (Fraga Dominguez et al., 2021); the authors found that older victims and survivors were more likely to report abuse by a relative or paid caregiver than abuse by a partner.
Two recent reviews provide useful data on the help-seeking of people who use IPV (Calcia et al., 2021; Santoniccolo et al., 2021). A systematic review of qualitative studies on the experiences of perpetrators in accessing healthcare services identified six studies, reporting data on 125 participants, almost all of whom were male. A reluctance to admit their abusive behaviour to clinicians was commonly identified in studies, including a normalisation of the behaviour and minimising its impact or perceiving other personal issues were more of a priority in their lives. Other barriers were a concern about being blamed or not understood. Common triggers to help-seeking were the abuse escalating, the breakdown of their relationship or loss of contact with children, or legal intervention and other negative consequences. Participants reported engaging with a range of services, including GPs, drug and alcohol and mental health services, and often soughtreferrals for “anger management” programs. Finding a healthcare professional who listened non-judgementally facilitated disclosure of abusive behaviour and continued engagement with services. Calcia et al. (2021) also identified that for men in same-sex relationships, concerns that professionals lacked knowledge about their sexuality were barriers to disclosure. Similar findings were evident in a review on help-seeking in same-sex relationships by Santoniccolo et al. (2021). The authors found some studies included help-seeking by perpetrators (of all genders) as well as by victims and survivors. A lack of recognition of abuse perpetrated by women (both lesbian and heterosexual) was a barrier to seeking help, as was a perception that services would not understand same-sex relationships.
Evidence gaps
There are considerable gaps in the research literature about IPV and/or SV experiences – in particular, the nature and patterns of abuse and violence that are not just physical violence. For example, little is known about the nature and prevalence of financial control, emotional abuse, non-physical coercive control, technology-facilitated abuse, reproductive coercion and abuse, and systems-facilitated violence (for example intentionally drawing out litigation proceedings; Ayre et al., 2016; Cortis & Bullen, 2016; Our Watch, 2018a, 2018b; Partners for Prevention, 2020). We know little about how the patterns of violence vary between different cohorts – for example different demographic characteristics, women who stay with their partner and cohabiting/non-cohabiting perpetrators (Cox, 2015).
Furthermore, our review of the literature highlights that there remain some key evidence gaps around service experiences, needs and help-seeking of victims and survivors of IPV and/or SV. Although there is a fairly robust evidence base of good-quality qualitative research into women’s experiences of seeking help for IPV and support needs in health settings (Heron & Eisma, 2021; Tarzia, Bohren, et al., 2020) and the criminal justice system, there is less research on help-seeking in other contexts, such as specialist IPV services, children’s services, and financial or housing services (Australian Institute of Health and Welfare, 2018; Dowling & Morgan, 2019; Dowling et al., 2018; Humphreys & Healey, 2017). Importantly, there is a lack of research on women’s support needs at different time points and how their engagement with the service system unfolds over time, including when the abuse escalates orafter it ends (Harper, 2021; Wright et al., 2021). Furthermore, women who experience IPV and/or SV may have valuable insight or recommendations into the service needs of their partner or former partner (i.e. the perpetrator). This has not been the focus of any research across the service sector.
Although some systematic reviews (Iratzoqui & Cohn, 2020; Santoniccolo et al., 2021; Sripada, 2021) did address how marginalisation impacts help-seeking, in general we still have insufficient data on the experiences, service needs and help-seeking behaviours of specific vulnerable cohorts of women and their children. This includes women from culturally and linguistically diverse communities (CALD), those who are LGBTQ, Aboriginal and Torres Strait Islander women (Fiolet et al., 2019), women from rural communities, young (18 to 24 years old) and older women (over 65 years), and women who are socio-economically disadvantaged. While we know that many of these groups are at higher risk of violence, we know little about their unique experiences (Australian Institute of Health and Welfare, 2018; Ayre et al., 2016; Blagg et al., 2018; Cox, 2015; Dyson et al., 2017; Mitra-Kahn et al., 2016; Our Watch, 2017; Vaughan et al., 2016). There is an urgentneed for large-scale national research that allows for analysis of the experience and support needs of women with different demographic characteristics (Australian Institute of Health and Welfare, 2018; Cox, 2015; Dyson et al., 2017; Mitra-Kahn et al., 2016; Vaughan et al., 2016).
Developing insight into the service needs and experiences of perpetrators is another important area that requires urgent attention. It is critical that engagement of perpetrators with services and effective interventions be improved (Diemer et al., 2020; Gallant et al., 2017; Humphreys, Diemer, et al., 2019). Yet, it is unclear how this could best be achieved, since this is an area that has been largely neglected in extant research (Australian Institute of Health and Welfare, 2018; Humphreys & Campo, 2017). The Australian Institute of Health and Welfare (2018) calls for more research to develop insight into the outcomes and impacts of current service responses from the perspective of perpetrators, including health services, police and justice responses, and specialist services (Day et al., 2018; Day et al., 2019). Many of the available studies with perpetrators of IPV and/or SV have been undertaken with men participating in behaviour changeprograms, yet these programs only engage a subset of perpetrators, most of whom have been court-mandated to attend (Day et al., 2019; Tarzia, Forsdike, et al., 2020). In addition, a number of researchers have highlighted the importance of addressing the service needs of fathers who use violence, especially those who remain living together with their partner, and the need to build an evidence base around the development and outcomes of practice with this population (Diemer et al., 2020; Healey et al., 2018; Humphreys & Campo, 2017; Kaspiew et al., 2017).
Furthermore, during the COVID-19 pandemic, social isolation, psychological and financial stress, and unemployment may have exacerbated men’s use of violence in intimate relationships and created barriers to help-seeking from services (Bradbury‐Jones & Isham, 2020). Service provider reports suggest that women and children experiencing IPV had contact with friends and family members restricted as part of abuse tactics (Fitz-Gibbon et al., 2020). However, little research has been undertaken to date with victims and survivors of IPV and/or SV to explore their perspectives about how COVID-19 impacted their experiences of violence and their help-seeking.
In summary, there remains a need for further research into women victims’ and survivors’ experiences of IPV, particularly for non-physical forms, such as psychological abuse, financial abuse, or technology-facilitated abuse. There is also a dearth of research into women’s experiences of SV. In regard to help-seeking, although there is a good-quality qualitative evidence base focused on how health and criminal justice services respond to IPV, research is lacking across other facets of the service landscape. Again, help-seeking for SV is relatively under-represented in research across all settings. Major gaps exist around the experiences, support needs and help-seeking of people who use IPV and/or SV; it is critical that this be addressed in order to inform effective interventions and policies for perpetration of violence. This report contributes to filling this gap with data on experiences, barriers and enablers to help-seeking and support needs,and makes recommendations for policy and practice.
Policy context
The Australian Government is developing the National Plan to End Violence against Women and Children 2022–2032 (draft National Plan) to replace the existing National Plan. The draft plan has four pillars across prevention, early intervention, response and recovery. The current project is exploring help-seeking needs across the last three pillars for victims and survivors, children, and people who use IPV and/or SV. The National Summit on Women’s Safety statement from delegates called for the draft National Plan to prioritise listening, engaging and being informed by diverse lived experience, particularly that of victims and survivors. They also called for addressing men’s violence against women and children across all settings. This project is responding to these national policy contexts and can inform the development of specific strategies.
Aim of study
This collaborative project between Melbourne University and Australia’s National Research Organisation for Women’s Safety (ANROWS) aimed to provide in-depth insights into the experiences of different cohorts of people and to compare the experiences, service needs and help-seeking behaviours of these diverse cohorts. This is so as to enable tailored messaging and responses for people who experience or use IPV and/or SV.
Thus, this project aimed to gain insight into 1) the experiences of IPV and/or SV, including patterns of abuse and violence, and service needs from the perspectives of women victims; and 2) the experiences and service needs of people who use IPV and/or SV against women (please refer to key research questions below).
We aimed to understand:
- “what works” from the perspective of women victims and survivors in terms of service responses for themselves, their children and the perpetrator, and what their recommendations are for system improvement
- “what works” from the perspective of perpetrators in terms of service responses and what their recommendations are for system improvement.
Research questions
Specifically, we wanted to explore the following.
Victims and survivors
- What are the experiences and patterns of abuse and violence for Australian women victims and survivors over their lifetime?
- What is the association between patterns of abuse and demographic factors?
- How are adverse childhood experiences associated with victimisation for adult women?
- What are the help-seeking experiences, journeys to seeking help, and support needs of diverse women victims and survivors and their children following IPV and/or SV?
- What is the role of family and friends to support victims and survivors?
- What are women’s perspectives about the service needs of their partners who use IPV and/or SV?
- What are barriers to help-seeking and women’s expectations of service providers?
- How were victims and survivors impacted by COVID-19 and how can we safely reach victims and survivors during COVID-19 self-isolation?
People who use IPV and/or SV
- What are the patterns of abuse and violence from the perspective of perpetrators from different backgrounds?
- What is the association between patterns of abuse and demographic factors?
- What is the association of adverse childhood experiences, and attitudes to violence against women, with perpetration against adult women?
- How do perpetrators perceive the impact of violence on their family, including women and any children?
- What are diverse perpetrators’, help-seeking experiences, journeys to seeking help and support needs after use of IPV and/or SV?
- What is the role of family and friends to engage perpetrators in help-seeking?
- What are barriers to help-seeking and expectations of service providers working with people who use IPV and/or SV?
- How can we engage people who use violence to seek help during COVID-19 lockdowns/isolation?
The next part will outline the methodology used in the project and describe the ethical issues we addressed in the project.
Part B:
Methodology
Introduction
This part outlines the methods used for the surveys and the interviews, including recruitment, design and data analyses. This is followed by the ethical considerations of the project and how we synthesised the data to answer the research questions.
Surveys of women victims and survivors of, and people who use,
IPV and/or SV
The methods for the survey were the same for all participants, so below we outline how we recruited participants, as well as how data was collected and analysed.
Recruitment
The project utilised various participant recruitment strategies, including a range of social and traditional media channels to secure target participation, to drive awareness of the project and to sustain continued participation and interest throughout recruitment. Links to the online survey were distributed nationally between 27 January 2021 and 31 January 2022, via the project partners’ and advisory committee’s networks, membership lists and social media, including Facebook. Existing social media channels within Melbourne University and ANROWS were leveraged, while community groups and family violence organisations were asked to distribute the advertisement flyer. Participants for both surveys were recruited from across Australia. When reaching the sample size target for both surveys was proving difficult, we engaged the research company i-Link Research to assist. i-Link is a social and market research company with extensive experienceadministering online surveys to panel members across Australia (Boxall & Morgan, 2021). i-Link administers online research panels made up of people in Australian who have consented to receive information about a broad range of market and research surveys in which they can choose to participate. i-Link renumerates its panel member participants with “points” that can be redeemed as vouchers (M. Geagea, personal communication, 10 November 2021). Researchers at the University of Melbourne recruited 574 women victims and survivors and i-Link recruited 548 women victims and survivors. In terms of the recruitment of people who use IPV and/or SV, the researchers recruited 203 participants and i-Link recruited a further 360 participants.
Sample size
A sample size of 500 or more participants was determined in advance to be sufficient to detect meaningful differences between participants on variables of interest with at least 80 per cent power and a 5 per cent significance level.
Inclusion criteria
Inclusion criteria for the victim and survivor survey was women who spoke English and were aged 16 years and over. Women also needed to answer “yes” to at least one of four screening items about behaviours by a partner or ex-partner, date or stranger in the previous five years (Box 1).
The language and age criteria were the same for the people who use violence survey; however, participants could self-identify as any sex and needed to answer “yes” to at least one of three screening items about behaviours perpetrated against someone with whom they had been in an “intimate relationship” during the last five years (Box 2). By intimate relationship, we meant a current or former husband/wife, partner or boy/girlfriend for longer than one month.
Box 1: Victim and survivor survey screening items
In the last five years have you:
- Been afraid of a partner or ex-partner?
- Been controlled by a partner or ex-partner?
- Been physically hurt by a partner or ex-partner?
- Experienced unwanted sex by anyone, including a partner or ex-partner?
Box 2: People who use violence survey screening items
In the last five years have you:
- Been concerned about your behaviours in intimate relationships?
- Believe your behaviour has scared a partner or ex-partner?
- Sought help from anyone to address issues in your intimate relationships?
Data collection
Two online cross-sectional surveys were developed for women victims and survivors of IPV and/or SV and people who have used IPV and/or SV. Cross-sectional surveys are a robust method for reaching groups of people with quantitative questions about experience, particularly for sensitive and stigmatised research topics (Braun et al., 2020). Due to the anonymity of online surveys, they have been shown to result in more comfortable and candid participation for a greater number of people, while encompassing a broader range of views than in-person research methods (Burton & Blair, 1991). The surveys were developed in consultation with the project’s advisory committee, and were informed by survey theory, a review of the literature and an investigation of validated tools as well as the research team’s extensive experience in survey design and delivery with people who have experienced IPV and/or SV, and who have used IPV and/or SV (see Appendix Bfor the victim and survivor survey and Appendix C for the people who have used violence survey). The two English-language surveys were delivered online via the online survey platform Qualtrics. A range of standardised measures were incorporated (see Table 3). The survey was piloted with 11 people, which led to modifications of the wording and refined pathways through the survey.
Trauma-informed research design principles (Shimmin et al., 2017) were incorporated into both surveys, including that survey questions were optional due to their sensitive nature. An introductory sentence at the beginning of each section provided the purpose and overview of the section in an effort to assist participants with information about and control over the survey process. The surveys were regularly punctuated with contact details for support services and each page contained a quick exit link. The surveys took approximately 25 to 30 minutes to complete. Prior to survey completion, all participants were asked to read an information sheet. Consent was implied through returned surveys. Initially, participants who completed a survey were sent small ($30) gratis gift vouchers in recognition of their time and expertise. Vouchers had to be ceased when data integrity issues emerged (see “Methodological challenges” below).
Survey measures
For a summary of survey measures used, see Table 3.
Table 3: Survey measures
Variables
Included topics
Survey V/S | P
Source measure
Screening items for victims and survivors
Fear of partner, control/physical hurt by partner, unwanted sex by anyone during last five years
V/S
Adapted from ACTS (Hegarty et al., 2021)
Screening items for people who use violence and abuse
Concern about behaviours in relationship, having scared a partner, sought help to address relationship issues during last five years
P
Adapted from other SAFER Families research projects
Sociodemographics
Age, education, income (including financial hardship), Aboriginal and Torres Strait Islander status, and CALD status, sexual identity, location, housing, children to compare with the population
V/S | P
Adapted from Australian Bureau of Statistics (2016)
Adult lifetime IPV
Validated measure of 15 abusive behaviours; occurrence (yes/no) of behaviours since age 15 years by someone with whom relationship lasted longer than one month
Abuse categorised as psychological, sexual and/or physical (participants can belong to more than one category)
V/S
CASr-SF (Ford-Gilboe et al., 2016)
12-month IPV
Ibid.
If “yes” to abusive behaviour/s in adult lifetime, participant asked to score frequency of corresponding behaviour during last 12 months
V/S
CASr-SF (Ford-Gilboe et al., 2016)
Adult lifetime IPV perpetration
As above, adapted for use of 15 abusive behaviours since age 15 years against a partner of longer than one month
P
Adapted from CASr-SF (Ford-Gilboe et al., 2016)
12-month IPV perpetration
If “yes” to use of abusive behaviour/s in adult lifetime, participant asked to score frequency of use of corresponding behaviour during last 12 months
P
Adapted from CASr-SF (Ford-Gilboe et al., 2016)
Sexual violence and reproductive coercion
Sex obtained via coercion or threats and interference in autonomous decision-making over reproductive health by anyone (experience of same for V/S survey and perpetration of same for P survey)
V/S | P
Sexual violence items developed by the research team with some items adapted from US National Intimate Partner and Sexual Violence Survey (Black et al., 2010). Reproductive coercion items adapted from the Australian Longitudinal Women’s Health Survey (Commonwealth of Australia, 2020)
Child abuse
Adverse childhood experiences questionnaire
V/S | P
ACE scale (Felitti et al., 1998)
Physical and mental health
- Indicators of health/mental issues including:
- Physical health
- Anxiety and depression
- PTSD
- Hazardous alcohol consumption
V/S | P
SF-12 (Ware et al., 1996)
PHQ-4 (Kroenke et al., 2009)
Short Screening Scale for DSM-IV PTSD (Breslau et al., 1999)
FAST (Hodgson et al., 2002)
Help-seeking
Self-reported use of health, justice, counselling and specialised services used in other studies
V/S | P
Adapted from other SAFER Families research projects
Service barriers and values
Service needs, expectations and perspectives
V/S | P
Adapted from other SAFER Families research projects
COVID-19
Items to identify perceived impact and service needs
V/S | P
Adapted from other SAFER Families research projects
Attitudes
Measure of attitudes that support violence against women to compare with the population
V/S | P
(Webster et al., 2018)
Notes:
Survey V/S= Victim and survivor survey.
Survey P = People who use violence survey.
Data analysis
Quantitative data analyses were performed using STATA (Version 15.0; StataCorp, 2015). All data was checked and cleaned for errors and accuracy. Sociodemographic characteristics of participants were summarised, using the mean and standard deviation for continuous measures, and counts and percentages for categorical data. Descriptive statistics were used to compare mean help-seeking between groups. For binary outcomes, differences in proportions were tested using McNemar’s chi-square test and odds ratios with 95 per cent confidence intervals (CI) calculated using ratio of numbers of discordant pairs. General linear models with related measures were used to assess differences for continuous outcomes with 95 per cent CI and p-values. Mixed effects linear models were used to describe the relationship between continuous outcomes and the factors associated at the participant level (e.g. sexual orientation, rurality,migrant background). For binary outcomes, a fixed and random effects logistic model was used to describe the relationship between outcome and factors.
Missing data
As is common with a survey method, not all participants in this study answered all questions in the survey, which resulted in missing data. Missing data is the reason why the denominators and samples sizes for each variable vary. The survey contained sensitive questions, which are known to increase the risk of missing data (Kirkwood & Sterne, 2003). In some instances, participants were excluded from analysis, and this is specified in the table notes (e.g. participants who had never been in a relationship were excluded from answering questions about relationship violence). Imputation methods were used to replace missing data, depending on type of data and the reason for data loss.
Qualitative survey data
Participants were asked to provide written responses to a number of open-ended survey questions. Response lengths ranged from a single word to three or four sentences. We used thematic analysis to analyse the qualitative survey data. This was done by importing the written responses for each survey question in an Excel spreadsheet into the software program NVivo 12. We then coded the data and grouped codes under higher-order thematic categories that reflected common patterns within the dataset, relevant to each research question. We gave some consideration to the prevalence of responses associated with a theme as a way of reflecting on the strength of a pattern in the data (in describing the findings, we identify this by referring to “many” or “some” responses), though quantifying themes was not our primary aim. Our focus was primarily descriptive themes, with some attention to underlying (latent) meanings in the data.
For victims and survivors, for each qualitative survey question we coded the responses of a random sample of 500 participants out of a total of 1,122 participants. We coded only a sample of responses due to time constraints. Different participants would have provided different responses to each qualitative survey question, so a limitation of this approach is that the responses we coded may not have reflected the entire dataset of participants. For the qualitative survey data from people who used abuse or violence, we coded the responses of the 288 participants who identified that they had used IPV and/or SV across their adult lifetime (sample described in Table 19).
Interviews with women victims and survivors of, and people who use, IPV and/or SV
The aim of the qualitative phase was to help explain or elaborate on the quantitative results obtained in the survey, exploring the journeys to help-seeking. For this phase, we used in-depth interviews to provide a more complex and nuanced understanding of the needs of victims and survivors and of people who use IPV and/or SV and how their help-seeking changed over time (see Appendices D and E for interview schedules). We separately recruited victims and survivors and people who had used IPV and/or SV. However, we used similar methods for recruitment, data collection and analysis.
We separately sought approval for the interview phase of the study from the University of Melbourne Human Ethics Committee (approval no. 2021-21471-23926-4).
Recruitment
Participants for interviews were drawn from those who had completed the survey and had expressed interest in participating in further research at the end of the quantitative survey. Those who ticked “yes” to participating in this research were provided with a link that directed them to a new form where they filled out their contact details (first name, phone number and best time to contact them safely). Information sheets were provided to the participants.
A total of 299 women victims and survivors expressed interest in participating in interviews. We used purposive sampling to recruit a diverse sample of 30 women interview participants, based on their age, birthplace, Aboriginal and Torres Strait Islander status, their location in Australia (i.e. different states and territories, urban/rural areas) and parenting status. To recruit participants who had used IPV and/or SV, we contacted the first 30 people who had completed the survey and had expressed interest in participating in further research (out of a total of 185 people who had expressed interest). We only contacted the first 30 people due to time constraints. Eight of those we contacted responded and agreed to be interviewed. Others did not respond to our contact or responded but declined to participate or were unavailable within the timeframe for the interview phase.
First, we emailed potential participants using the safe contact details they had provided. We then sent interested participants the consent form and plain language statement. We spoke to them by phone to explain the study and answer any questions. In all recruitment and interview processes, we used established ethical protocols for research with victims and survivors of interpersonal violence (World Health Organization, 2016) to ensure participant safety (for instance, we referred to the research as a “relationships, health and wellbeing” study).
Data collection
The interviews were held via telephone or using Zoom (video conferencing software). The approximate duration of interviews was between 30 and 120 minutes for victims and survivors and between 28 and 60 minutes for people who had used IPV and/or SV. In part, the difference in interview lengths reflected that most victims and survivors described in detail their experiences of being subjected to abuse and their long journeys of seeking help, while interview participants who had used IPV and/or SV tended not to speak at length about their behaviour and frequently had less contact with supports and services. The interview style was informal and conversation-like, which facilitated the sharing of experiences and may have reduced some of the power differences that can occur in a formal research interview (Burgess-Proctor, 2015). We used a narrative approach, which aims to encourage interview participants to tell detailed stories about their personalexperiences (Riessman, 2008). This approach was more appropriate for our aims than using a more structured interview schedule, given that our focus was on inviting participants to tell their story in their own words about their support needs, how they sought help or support for the IPV and/or SV and how this changed over time. For our interviews with women victims and survivors, we asked two questions: “Can you tell me about when you first realised what you were experiencing in your relationship was not okay?” and “Can you take me through your experiences of seeking help or support?” For our interviews with people who had used IPV and/or SV, we asked: “Can you tell me when you first realised there was an issue with your behaviour in your intimate relationship(s)?” and “Can you take me through your experiences of speaking to people about your behaviour in your intimate relationships?” We then used probes to draw out further details of key events, responses andturning points.
At the end of each interview, we provided a resource card with information about other types of health services, such as mental health, in addition to services about violence. We also provided participant honorariums in the form of e-gift vouchers valued at AU$40 per participant as a token of appreciation for their time and contribution.
Data analysis
The audio from interviews was transcribed by a professional service. We de-identified the transcripts, removing names of people, places, specific services and dates. For the analysis, we used an inductive thematic approach to generate key themes and identify the range of responses across participants (Braun & Clarke, 2006, 2021). We coded interview transcripts, assisted by the qualitative data software package NVivo 12. We then grouped codes into broader interpretative themes, using an iterative process of moving back and forth between the descriptive codes (and associated quotes from transcripts) and interpretative codes as they developed. We held discussions about interpretative and overarching themes as a research team to promote a rigorous approach to the analysis.
We also constructed a timeline of each participant’s support and help-seeking journey (Kolar et al., 2015; Patterson et al., 2012). This assisted us to organise the narrative data from individual interviews and to identify changes over time. We used Microsoft Excel to create a timeline analysis table. The table included the turning point or trigger event (such as the abuse escalating), the participant’s help-seeking aim or need, the source they sought help from, and a brief description of the response (e.g. “emotional support” or “being judgemental”). We then compared the timelines across participants to identify similarities and differences in turning points, help-seeking needs/aims and sources of help. This enabled us to identify common stages of help-seeking over time, the turning points that led to them, and perceptions of the responses received at each stage. We did not return to participants to check the accuracy of the timelines, as we wereinterested in the story as was it told in the interview, rather than ensuring that every relevant event was recorded in order. However, a limitation of this method is that in some cases, data about important events or turning points may have not been included, so the stages of help-seeking we identified in our findings may not have accurately reflected the journeys of all participants.
It should be noted that in re-presenting participant interview data by using case studies and quotations, we used pseudonyms and removed any other potentially identifying details.
Ethical considerations
The topics of IPV and SV are sensitive and potentially confronting. It is vital that research be undertaken in a safe, ethical and trauma-informed way to ensure the wellbeing of participants. Consequently, all phases of this research underwent ethical review by the University of Melbourne’s Human Research Ethics Committee prior to commencement. Below, we outline some of the key ethical considerations for this research, and how these were mitigated.
Participant distress
Participant distress is a very real risk for any researcher working in this complex and sensitive field. Our survey contained numerous items asking about abusive behaviours, and the interviews required participants to recall their experiences of violence in detail as well as what happened when they sought help. Despite this, it is important to remember that experiencing strong emotions when recalling a traumatic event is not the same as being retraumatised. Indeed, studies do consistently indicate that women usually find participation in research to be an empowering and cathartic experience (Valpied et al., 2014).
Similarly, research with people who have perpetrated IPV and/or SV could also elicit strong emotional responses such as distress or shame. While studies indicate that people using IPV and/or SV can safely, openly and honestly engage in discussions about past behaviours and processes of change (McGinn et al., 2020; Sheehan et al., 2012), it is vital that proper precautions be put in place.
As with all research conducted by the Sexual and Family Violence team in the Department of General Practice, distress protocols have been developed to guide the response of researchers should a participant become upset during an interview. The protocol includes supportive listening, allowing the participant time to pause or stop the interview if they wish, and checking in with participants at the end of the interview. Consistent with a trauma-informed approach (Campbell et al., 2019) we prepared participants before interviews by describing the interview process in detail, including the kind of questions they would be asked. The interviewers also showed empathy and validated participants’ strengths (Campbell et al., 2019). Participants were provided with information about available support services.
The plain language statements included a list of support services that participants may access. Trained research assistants with experience in working with individuals who have experienced or used IPV and/or SV were involved in participant engagement and responding to any potential distress using the distress protocol. During survey completion, if for any reason the participant was distressed, there was an option for them to save and return to the survey at any later time.
Perpetrator awareness
For women, completing an online survey about IPV and/or SV could have increased their risk of being victimised if a partner were to discover their participation. To reduce the risk of harm because of completing the online survey, the following actions were undertaken to reduce perpetrator or other people’s awareness:
- Each page of the online survey had a “quick exit” button which led to a blank Google search engine page.
- Best practice advice about online safety was provided to the participants at the very beginning of the survey (e.g. clearing browser history and cache).
- The survey title and all emails about the survey did not explicitly mention “domestic violence”, “intimate partner violence” or “sexual violence”.
Similar precautions were taken for the interviews, with communication about the study referring to a “women’s health project”. If at any time an unknown person answered the telephone, no information was provided about the study.
Privacy
To ensure participants’ identifying information was not associated with their survey responses, the following actions were undertaken:
- If survey participants decided that they wanted to be involved in an interview, they were directed to a completely new form to input their details.
- Consent forms for interviews were stored in a different location to the participants’ interview audio recording and transcript.
- For interviews, the researchers always ensured that the participant was in a private location. Participants were informed that if they were interrupted and were not in a position to speak privately at any time during the interview, they could simply end the call.
- Resource cards given to participants contained information about other types of health services, such as mental health, in addition to services about violence.
- All transcripts were de-identified before analysis. Consistent with a trauma-informed approach (Campbell et al., 2019), we offered participants the opportunity to check their transcripts to remove any contextual information they felt could identify them.
Disclosure of criminal activity
There was a small risk that a participant might disclose illegal activities during their interview or make a threat to harm another person. Clear safety protocols were in place to guide the research team including de-escalation if necessary and contacting emergency services. Researchers were familiar with mandatory reporting guidelines regarding disclosure of child abuse. Fortunately, no illegal activities or contemporary child abuse were disclosed to the research team at any point during the project.
Researcher wellbeing
All the researchers involved in this study were highly experienced, either with a research background in IPV and/or SV, a clinical or counselling background, or a combination of both research and practice expertise. Team members were therefore aware of the importance of practicing good self-care during the study and had their own strategies in place to reduce the likelihood of vicarious trauma. Nonetheless, additional actions were taken to ensure that any member of the team who experienced feelings of distress was well-supported. We undertook weekly meetings where any concerns could be openly discussed and strategies or solutions workshopped with others. The two researchers conducting the interviews undertook additional debriefings with a senior member of the team on a regular basis to discuss specific issues relating to this phase of the research. Team members also had access to supervision on an ad hoc basis if needed. As Moran and Asquith (2020)have noted, emphasising how the research is contributing to positive change for victims and survivors of IPV and SV can help to compensate for some of the emotional challenges inherent in this work; this was something we frequently reflected on as a team.
Synthesis
The ANROWS team collaborated with the Melbourne University research team to appoint representatives of key organisations and services. The research team engaged with the advisory committee (16 members), which has wide representation from government, non-government and service organisations. The advisory committee provided feedback on the research design, survey instruments and findings to ensure that the research meets their priorities and will be useful for policy and practice. The advisory committee also assisted with providing contacts and networks for the recruitment of research participants and was consulted further about survey questions and the piloting of research instruments.
Methodological challenges
There were several specific challenges that occurred during this project that delayed progress and also required some new methods to be utilised. We became aware that some participants had been answering our online survey multiple times for the sake of receiving gift vouchers. As a result of this incident, we stopped sending gift vouchers to all participants, changing to a draw for iPads. We manually checked whether the data was genuine by going through data line by line using a variety of methods including IP addresses, length of time to complete and qualitative responses. We removed fraudulent responses. We only sent gift vouchers to participants who genuinely responded and completed the survey. We also further changed our processes to a brief screening survey that was unlikely to be able to be answered by computer and participants got a separate email with a new link to the survey which stopped all fraudulent responses. We are confident of thisbecause we checked the data very closely.
Summary
We undertook an online survey of adult women who had experienced IPV and/or SV and a survey of people who used IPV and/or SV against women. Participants were recruited via social media and traditional media channels. We cleaned the data and used descriptive statistics for our analysis of the quantitative survey data. We also analysed open-ended survey questions about experiences of help-seeking for IPV and/or SV and support needs. We held interviews with women victims and survivors and men who used IPV and/or SV. They were survey participants who had expressed interest in participating in an interview. We thematically analysed the interview data and constructed a timeline of each participant’s support and help-seeking journey.
Part C:
Key findings –
Victim and survivor experiences
The most helpful people I’ve spoken to are empathetic, non-judging and know where to [go] next. Especially in the early stages of leaving there’s so much fear and you need to know you are doing the right thing. It’s a very lonely road.
(Survey participant)
Introduction
This part is divided into three sections that integrate quantitative and qualitative findings from the perspective of the victims and survivors. The first section overviews participant characteristics and the nature, patterns and health impacts of IPV and/or SV, including the effects of the COVID-19 pandemic on experiences. This is followed by a section on help-seeking and service needs, including the effects of the COVID-19 pandemic on help-seeking. The final section describes support needs of victim and survivor participants.
1. Patterns and associations of abuse and violence
Sociodemographic characteristics
Overall, study participants were generally representative of the Australian population of women except for some specific demographic areas (see Table 4). The average age of victim and survivor participants was around 42 years, which represents a slightly higher mean age compared to the general Australian population. Among women in this study, most Australian states and territories had similar representation to the Australian population, except that a greater proportion of participants lived in Victoria (33.4%), while fewer lived in New South Wales (21.9%). A similar proportion of women participants to the general Australian population lived in a metropolitan area (71.5%).
Just under half the women (45.6%) were in a current relationship and 44.3 per cent were living with their partner. Of those in a relationship, the majority (94.8%) reported their partner as male, 3.8 per cent female and 1.4 per cent as non-binary. Approximately one in four (26.2%) participants were married, and three in four (75.7%) had children living at home with them.
Table 4 shows a comparison of specific demographic characteristics. This study recruited almost double the proportion of Aboriginal and Torres Strait Islander women (7.8%) compared to population figures, but a lower share of women born overseas (18.1%). A greater number of women participants had attained a trade, apprenticeship or diploma after high school (57%), or had attended university (43%), compared to the general population. Approximately three fifths of participants were employed (59.3%), a smaller proportion than the general Australian population. A greater percentage of women participants in this study held a Health Care Card (60%) or reported difficulty managing on their available income some or all of the time (58.5%) compared to the general population (Table4).
Table 4: Demographic characteristics of survivor women participants compared to the broader Australian population (N=1,122)
Age (years)
Characteristic
All participants
n (%)
Australian population (women) %a
18–29
231 (20.6)
18.6
30–39
298 (26.6)
14.7
40–49
265 (23.7)
12.9
50–59
191 (17.1)
12.4
60–69
99 (8.8)
10.9
70–79
32 (2.9)
7.8
80+
4 (0.4)
4.8
Current Australian state of residence (n=1,121)
Characteristic
All participants
n (%)
Australian population (women) %a
Australian Capital Territory
27 (2.4)
0.8
New South Wales
245 (21.9)
17.4
Victoria
375 (33.4)
13.4
Northern Territory
11 (1)
0.2
Queensland
239 (21.3)
10.5
Western Australia
111 (9.9)
5.2
Tasmania
32 (2.8)
1.4
South Australia
81 (7.2)
4.4
Lives in metropolitan area (n=1,117)
799 (71.5)
71
In current relationship (≥1 month length)
508 (45.6)
N/Ab
Lives with a partner
(male/female/spouse; n=1,122)
497 (44.3)
45
Sex of current partner (n=497)
N/A
Male
471 (94.8)
59.8
Female
19 (3.8)
7.1
Non-binary
1 (1.4)
17.3
Sexual orientation (n=1,070)
Characteristic
All participants
n (%)
Australian population (women) %a
Heterosexual
844 (78.9)
92
Bisexual
107 (10)
1.4
Lesbian
20 (1.9)
1.9
Queer
11 (1)
N/A
Pansexual
18 (1.7)
N/A
Asexual
13 (1.2)
N/A
Self-described
33 (3.1)
N/A
Not sure
24 (2.2)
0.8
Marital status (n=1,220)
Characteristic
All participants
n (%)
Australian population (women) %a
Never married
459 (41)
32
Married
294 (26.2)
30.6
Separated but not divorced
144 (12.9)
3.1
Divorced
200 (17.9)
7
Widowed
23 (2.1)
6
Children
746 (66.6)
43
1+ children living at home
565 (75.7)
49
Aboriginal and/or Torres Strait Islander
87 (7.8)
3.2
Born outside Australia
203 (18.1)
30
First language not English
83 (7.4)
21
Prior schooling
(n=1,060)
Attended school but finished prior to Year 12
295 (28.1)
10.5
Completed Year 12
734 (69.9)
79
Educational qualification
(n=1,050)
Trade/apprenticeship/diploma
598 (57)
26.5
University degree/higher degree
452 (43)
29
Employment and income (n=1,069)
Characteristic
All participants
n (%)
Australian population (women) %a
Employed
634 (59.3)
64.1
Not in employment
435 (40.7)
5.7
Has difficulty managing on available income
626 (58.5)
18.7
Health Care Card holder
641 (60)
52
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey item.
a Population data is weighted proportions from Australian Bureau of Statistics (2020);, values are percentages of women as a proportion of the total Australian population.
b Comparable data either not collected or available.
Twelve-month and lifetime experiences and patterns of IPV and/or SV
To understand the experiences of IPV and/or SV victims and survivors, the survey screened participants for IPV and/or SV using three items about specific acts of abuse by a partner or ex-partner in the last five years. One further item asked about SV perpetrated by anyone. Participants could answer with a simple “yes/no” response. Further, IPV and/or SV experiences of participants were collected via the short-form CASr-SF (Ford-Gilboe et al., 2016) for the last 12 months and lifetime, and experiences of child abuse were measured using the Adverse Childhood Experiences scale (Felitti et al., 1998; see “Methodology” further).
While not all participants reported experiencing IPV and/or SV when measured using the CASr-SF (Ford-Gilboe et al., 2016), the eligibility of all women to participate in the study was established through their positive response to one or more screening questions (see “Methodology” further). The screening questions indicated that the participant had experienced abuse and violence in a relationship (including casual relationships) in the last five years, and/or had experienced SV by anyone in the same timeframe. In this context, we chose to analyse the whole sample of women participants, rather than selecting out only the women who scored on the CASr-SF, and we refer to all participants in this section as “victims and survivors” (Ford-Gilboe et al., 2016).
IPV in the last 12 months
Three in four women participants (76.1%) were currently afraid of their partner or ex-partner, while 80.7 per cent reported that they had felt afraid of a partner during the previous 12 months (Table 5). Fear of a partner was a feature of most (between 86% and 100%) victim and survivor participants’ experiences regardless of the type of violence and abuse their partner had perpetrated against them in the last 12 months.
Table 5: Proportion of women who experienced IPV and/or SV during the last 12 months
Last 12 months
Types of IPV
n (%)
Afraid of partner or ex-partner in last 12 months (n=1,038)a
838 (80.7)
Currently afraid of partner or ex-partner (n=930)
708 (76.1)
IPV any category (CASr-SF; n=881)b
362 (41.1)
Physical
194 (23.6)
Sexual
190 (23.8)
Psychological
286 (38.5)
Total: 12-month fear of a partner and/or IPV (n=1,038)
861 (82.9)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed 12-month CASr-SF (Ford-Gilboe et al., 2016).
a Seventy-six participants were omitted because they had never been in a relationship for longer than one month.
b Participants could belong to more than one CASr-SF category.
The occurrence of combined categories of IPV was more prevalent than not; more women participants had experienced physical, sexual and psychological abuse (27.1%) than had experienced one or two IPV categories in the last 12 months (Figure 10). The second most common type of IPV women had experienced was psychological IPV not in combination with any other category of IPV (24.6%), followed by combined physical and psychological violence (16.9%). Physical and sexual IPV without psychological abuse was the least common category of IPV reported (3.9%).
Figure 10: Proportion of participants who experienced physical, sexual and psychological IPV in the last 12 months (n=361)
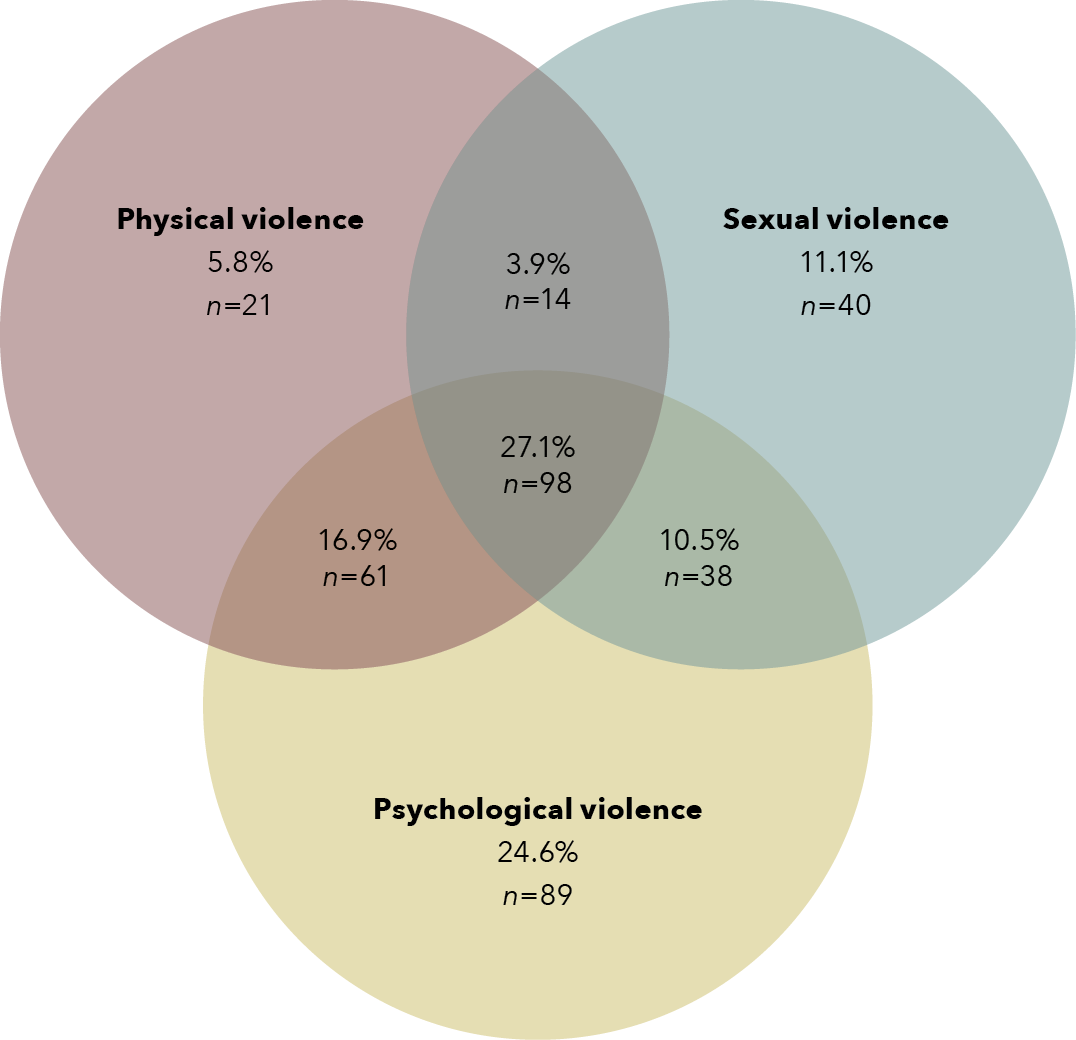
Data table for the figure above:
Type of violence
Percentage
n
Physical violence
5.8%
21
Sexual violence
11.1%
40
Psychological violence
24.6%
89
Physical and sexual violence
3.9%
14
Physical and psychological violence
16.9%
61
Sexual and psychological violence
24.6%
89
Physical, sexual and psychological violence
27.1%
98
Of those who had experienced IPV in the last 12 months (n=362), almost two thirds (60.8%) of victim and survivor participants had experienced technology-facilitated harassment, and around one in three (31.8%) had been financially abused by being kept from having access to a job or finances. The most commonly perpetrated acts of abuse reported were being told they were crazy, stupid or not good enough (84.8%); being blamed for causing the violent behaviour (83.4%); and the perpetrator trying to convince family, friends and children they were crazy or trying to turn those people against them (61.3%; Table 6).
The next section describes lifetime experiences.
Table 6: Proportion of women who experienced 12-month IPV and/or SV and type of abusive behaviour (n=362)
Abusive behavioursa
n (%)
Told me I was crazy, stupid or not good enough
307 (84.8)
Blamed me for causing their violent behaviour
302 (83.4)
Tried to convince my family, children or friends that I am crazy or tried to turn them against me
222 (61.3)
Harassed me by phone, text, email or using social media
220 (60.8)
Shook, pushed, grabbed or threw me
205 (56.6)
Kept me from seeing or talking to my family or friends
169 (46.7)
Made me perform sex acts that I did not want to perform
158 (43.6)
Forced or tried to force me to have sex
140 (38.7)
Followed me or hung around outside my home or work
134 (37)
Kept me from having access to a job, money or financial resources
115 (31.8)
Threatened to harm or kill me or someone close to me
111 (30.7)
Hit me with a fist or object, kicked or bit me
109 (30.1)
Choked me
95 (26.2)
Used or threatened to use a knife or gun or other weapon to harm me
79 (21.8)
Confined or locked me in a room or other space
51 (14.1)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed 12-month CASr-SF.
a Experienced these behaviours once or more during last 12 months.
IVP, SV and reproductive coercion since age 16 years
Of all victims and survivors who had experienced IPV and/or SV by a partner or ex-partner since the age of 16 years, 84.3 per cent had felt fear of their partner (Table 7) and for half (51.5%), their experience was of physical, sexual and psychological IPV (Figure 11). In fact, very few women participants (15.4%) reported the experience of one type of IPV in isolation (Figure 11). For example, only 3 per cent of victims and survivors had experienced physical or sexual IPV alone. Nearly one in three women participants (32.9%) had experienced their partner interfere with or force their independent decision-making about pregnancy, including 17.1 per cent having been forced to terminate a pregnancy and 15.3 per cent being forced into pregnancy (Table 7).
Table 7: Proportion of women who experienced IPV and/or SV across the adult lifetime since the age of 16 years
IPV and/or SV
n (%)
(n=1,046)
Total adult lifetime IPV, including fear, intimate partner SV and/or reproductive coercion
1,008 (96.4)
Afraid of partner or ex-partnera
882 (84.3)
(n=1,039)
IPV (scored using CASr-SF)
905 (87.1)
(n=1,036)
Sexual violence by an intimate partner
852 (82.5)
Forced sexual activity
701 (67.8)
Had unwanted sex with a partner due to fear
718 (69.4)
Forced to watch pornography
370 (35.8)
(n=1,035)
Reproductive coercion
341 (32.9)
Forced pregnancy
158 (15.3)
Prevented termination of pregnancy
102 (9.9)
Forced termination of pregnancy
177 (17.1)
Contraception interfered with or partner prevented use
139 (13.4)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed survey items.
a Seventy-six participants omitted because they had never been in a relationship for longer than one month.
Figure 11: Proportion of participants who had experienced physical, sexual and psychological IPV since the age of 16 (n=1,001)
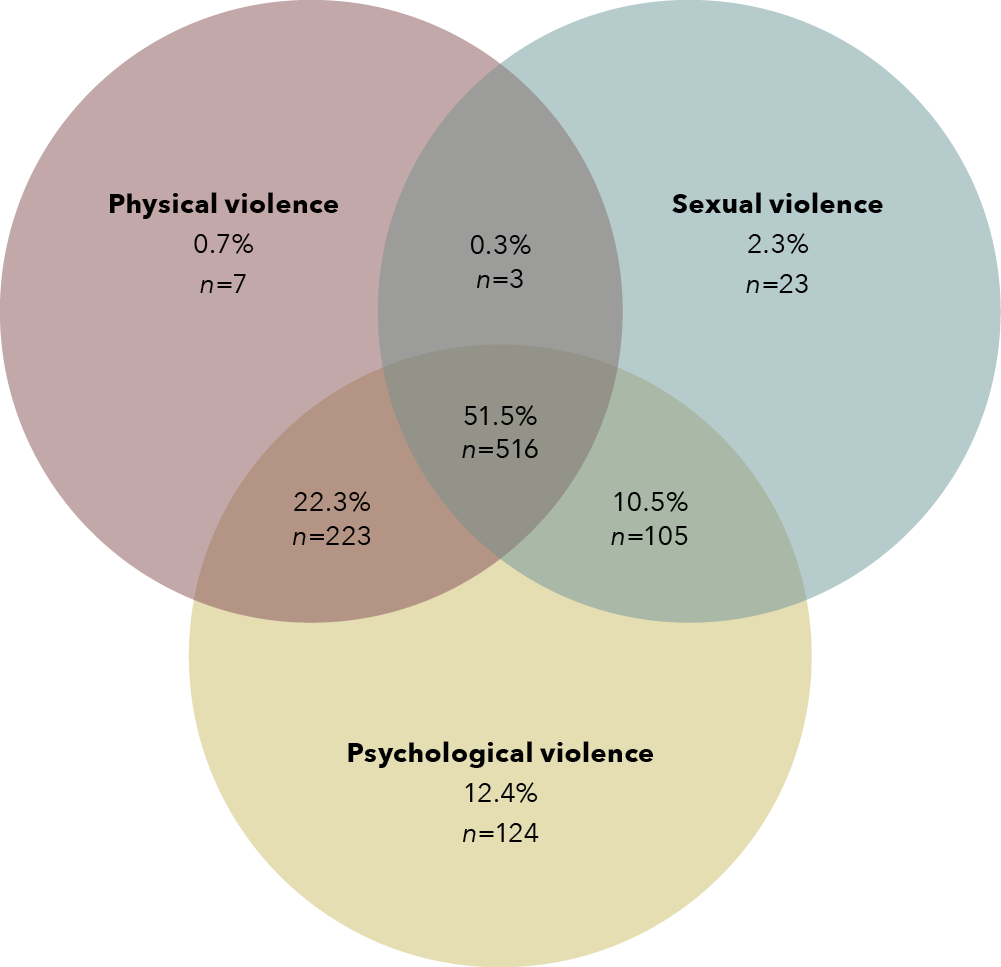
Data table for the figure above:
Type of violence
Percentage
n
Physical violence
0.7%
7
Sexual violence
2.3%
23
Psychological violence
12.4%
124
Physical and sexual violence
0.3%
3
Physical and psychological violence
22.3%
223
Sexual and psychological violence
10.5%
105
Physical, sexual and psychological violence
51.5%
516
Please note: n=1,001 includes all women who scored on any of three lifetime IPV categories of abuse using the CASr-SF, including emotional abuse and harassment.
The three most frequently reported acts of abuse across 905 victim and survivor participants were as follows: being told they were crazy, stupid, or not good enough (80.2%); being blamed for causing the violent behaviour (75.9%); and being shaken, pushed, grabbed or thrown (64%; Table 8). The most commonly reported experience of sexual violence was feeling forced to have unwanted sex with a partner due to fear (69.4%; Table 7). Almost two in three (60.5%) victim and survivor participants had experienced technology-facilitated harassment and 40.7 per cent had experienced financial abuse (Table 8).
Table 8: Proportion of women who experienced lifetime IPV and/or SV and type of abusive behaviour (n=905)
Abusive behavioursa
Adult lifetime
n (%)a
Told me I was crazy, stupid or not good enough
833 (80.2)
Blamed me for causing their violent behaviour
789 (75.9)
Shook, pushed, grabbed or threw me
665 (64)
Harassed me by phone, text, email or using social media
627 (60.5)
Tried to convince my family, children or friends that I am crazy or tried to turn them against me
625 (60.2)
Kept me from seeing or talking to my family or friends
587 (56.5)
Made me perform sex acts that I did not want to perform
570 (54.9)
Forced or tried to force me to have sex
562 (54.3)
Hit me with a fist or object, kicked or bit me
429 (41.3)
Kept me from having access to a job, money or financial resources
422 (40.7)
Threatened to harm or kill me or someone close to me
399 (38.4)
Choked me
352 (33.9)
Used or threatened to use a knife or gun or other weapon to harm me
295 (28.4)
Confined or locked me in a room or other space
221 (21.3)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed CASr-SF (Ford-Gilboe et al. 2016).
a Behaved in this way once or more during last 12 months.
Associations between patterns of abuse and sociodemographic characteristics
Looking at sociodemographic associations with combinations of abuse, women aged 25 to 45 years were over-represented as victims and survivors of poly-victimisation, including IPV in the last 12 months and IPV combined with sexual violence, reproductive coercion and child abuse (Table 9). Aboriginal and Torres Strait Islander women also indicated a higher prevalence of poly-victimisation across different forms of abuse compared to other women. Further, unemployed women were more likely than other women to have experienced IPV in combination with sexual violence and personal history of child abuse. Women who were not living with their partner at the time of completing the survey were less likely than other women to have experienced IPV in the last 12 months, whilemigrant women were less likely to report being a victim and survivor of poly-victimisation.
In brief:
Poly-victimisation against victims and survivors

Aboriginal and Torres Strait Islander women, women aged 25 to 45 years and unemployed women were overepresented as victims and survivors of IPV, SV and child abuse.

Migrant and young women were underrepresented as victims and survivors of poly-victimisation with multiple types of abuse.
Table 9: Proportion of women who experienced multiple abuse types, with sociodemographic factors
Sociodemographic factors
Experienced IPV in last 12 months (alone)
(n=1,039)
Experienced lifetime IPV and SV and reproductive coercion
(n=305)
Experienced lifetime IPV and SV and reproductive coercion and child abuse
(n=245)
All participants (n=1,122)
861 (82.9)
305 (29.2)
245 (21.8)
Age (years; n=1,120)
Up to 25 years (n=104)
84 (80.8)
20 (19.2)
16 (12.9)
25–45 years (n=516)
460 (89.2)
188 (36.3)
151 (27.4)
> 45 years (n=418)
317 (75.8)
97 (23)
78 (17.5)
Aboriginal and/or Torres Strait Islander (n=76)
71 (93.4)
98 (32.7)
31 (35.6)
Migrant background (n=192)
154 (80.2)
43 (22.4)
32 (14.7)
Same-sex partner (n=29)
27 (93.1)
8 (26.7)
8 (22.2)
Lives in non-metropolitan location (n=297)
238 (80.1)
98 (32.7)
79 (24.8)
Lives with disabilitya
330 (79.1)
136 (32.5)
119 (27.1)
Attended school but finished prior to Year 12 (n=301)
241 (80.1)
167 (30.2)
146 (24.4)
No university degree (n=552)
453 (82.1)
119 (29.7)
99 (22.8)
No employment (n=401)
314 (78.3)
207 (35.4)
168 (26.8)
Has difficulty managing on available income (n=584)
493 (84.2)
188 (32)
153 (23.9)
Health Care Card holder (n=588)
478 (81.3)
172 (29.4)
135 (21.6)
Not living with partner (n=580)
434 (74.8)
305 (29.2)
245 (21.8)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
% = represents the proportion of overall demographic group who have experienced the abuse category (IPV/sexual violence/reproductive coercion/child abuse).
a Lives with disability defined as participants who answered “yes” to living with a disability or chronic illness limiting daily activities including employment.
Adverse childhood experiences and victimisation in adulthood
There was a significant overlap for women participants between having experienced IPV and/or SV in adulthood and abuse during childhood. Two out of three (69.4%) participants had experienced physical, sexual or emotional abuse in childhood, and half (50.3%) had experienced four or more adverse experiences measured using the Adverse Childhood Experiences scale (Felitti et al., 1998); Table 10). Close to a quarter (23.8%) of women participants had grown up in a household where there was violence perpetrated against their mother. Among 12-month IPV and/or SV victim and survivor participants, 62 per cent had a history of child abuse, and for adult lifetime IPV and/or SV victims and survivors the proportion rose to 70.4 per cent who had experienced child abuse.This represented a more than fourfold increase in the predicted odds of reporting IPV and/or SV for victims and survivors who had a history of child abuse, indicating a life course effect of child abuse on adult relationships (OR 4.4, 95% CI 2.1 to 9.1).
Table 10: Proportion of women who experienced child abuse
Child abuse typea
Before age 15 years
(n=1,115)
Emotional neglect
626 (56.1)
Emotional abuse
616 (55.2)
Physical abuse
447 (40.1)
Sexual abuse
402 (36)
FV against mother growing up
266 (23.8)
Physical neglect
196 (17.6)
Total child abuse
774 (69.4)
Total ACE b score of 4+
561 (50.3)
Total child abuse and/or ACE>4
788 (70.7)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to child abuse survey items.
a Abusive behaviour before the age of 15 years by someone aged 18 plus years.
b Adverse Childhood Experiences scale (Felitti, 2019) score out of 10. Scores 4+ are associated with serious health and risk issues in adulthood (Felitti, 2019).
Health of victim and survivor participants
The burden of disease for participants was high, with health issues including (self-rated) poor health, long-term illness, mental health issues and/or hazardous alcohol consumption over-reported by victims and survivors compared to the general population (Breslau et al., 1999; Hodgson et al., 2002; Kroenke et al., 2009; Ware et al., 1996). Half of the victim and survivor participants met the core criteria for generalised anxiety disorder (52.4%; Kroenke et al., 2009), while three quarters of participants screened positive for PTSD (71.2%; Breslau et al., 1999). The proportion of participants reporting health issues increased as the types of abuse they had experienced increased. Table 11 demonstrates that victims and survivors whose IPV included sexual violence and reproductive coercion had higher rates of poor health across all health measures when compared to victims and survivors of IPV alone in the last 12 months. For victims and survivors oflifetime IPV and/or SV whose experience had also included childhood abuse, the prevalence of health issues rose higher again (Table 11).
Table 11: Proportion of women who experienced health and mental health issues by type of abuse and cumulative abuse
Mental health
Current health issue
All participants
(n=1,122)
IPV in last 12 months
(n=1,039)
Experienced lifetime IPV and SV and reproductive coercion
(n=305)
Experienced lifetime IPV and SV and reproductive coercion and child abuse
(n=245)
PTSD (n=1,120)
797 (71.2)
636 (73.4)
252 (82.6)
209 (85.3)
Anxiety (n=1,121)
587 (52.4)
481 (55.9)
196 (64.3)
167 (68.2)
Depression (n=1,121)
509 (45.4)
407 (47.3)
170 (55.7)
150 (61.2)
General health
Current health issue
All participants
IPV in last 12 months
Experienced lifetime IPV and SV and reproductive coercion
Experienced lifetime IPV and SV and reproductive coercion and child abuse
Lives with disability (n=1,121)
439 (39.2)
330 (38.3)
136 (44.6)
119 (48.6)
Poor to fair self-rated health (n=1,121)
398 (35.5)
310 (36)
125 (41)
111 (45.3)
Hazardous alcohol consumption (n=1,118)
239 (21.4)
173 (20.1)
77 (25.2)
64 (26.1)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
When looking at the experiences of victims and survivors as abuse in their lives accumulated, two groups of victims and survivors reported poorer health than other victims and survivors on a variety of measures: Aboriginal and Torres Strait Islander victims and survivors and those who have difficulty managing on their available income (Table 12). By contrast, migrant victims and survivors were less likely to experience a range of health and mental health issues compared to other victims and survivors.
Table 12: Proportion of women from diverse backgrounds who have experienced lifetime IPV and/or SV and health and mental health issues
Current health issues
All (lifetime) IPV and/or SV victims and survivors
(n=979)
Aboriginal and Torres Strait Islander victims and survivors
(n=71)
Migrant victims and survivors
(n=192)
Non-metro victims and survivors
(n=297)
Unemployed victims and survivors
(n=401)
Victims and survivors who have difficulty managing on available income
(n=584)
Victims and survivors not living with a partner
(n=580)
Poor to fair self-rated health (n=398)
366 (37.2)
25 (35)
49 (25.5)
103 (36.4)
200 (52.9)
256 (45.5)
198 (35.9)
Lives with disability
(n=439)
400 (40.9)
35 (49.3)
56 (31.6)
131 (46.3)
219 (57.9)
265 (47.2)
239 (43.3)
Anxiety (n=531)
531 (54.2)
49 (69)
82 (46.3)
150 (53)
272 (48.8)
344 (61.2)
292 (52.9)
Depression (n=509)
461 (47.1)
49 (69)
81 (45.8)
134 (47.3)
209 (55.3)
320 (56.9)
246 (44.6)
PTSD (n=797)
722 (73.7)
61 (85.9)
117 (66.1)
211 (74.6)
309 (81.7)
461 (82)
414 (75)
Excessive alcohol consumption (n=239)
199 (20.3)
32 (45.1)
27 (15.2)
58 (20.5)
72 (19)
117 (20.8)
87 (15.8)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all women who completed CASr-SF and responded to demographic and health survey items.
In brief
Health and mental health of victims and survivors

Aboriginal and Torres Strait Islander women, women who experience difficulty managing on their available income and unemployed women more frequently reported poor health issues.

Women not living with their partner less frequently reported poor health and mental health issues.
This section has provided insight into the patterns of IPV and/or SV experienced by women and associations with sociodemographic characteristics, health issues and service use. In the next section we examine qualitative survey data on the impact of the COVID-19 pandemic on IPV and/or SV for victims and survivors.
COVID-19 pandemic effects on women’s experiences
We asked women survey participants to provide written responses to the question: “How have your experiences in your adult intimate relationships changed during COVID-19 isolation?” Many simply commented “no change”. However, others reported the pandemic changed the abuse they experienced. We identified the following three themes from our analysis of participants’ comments.
Isolation fuelled and enabled the abuse
A key theme was that abuse or violence from a partner had first occurred during the pandemic and that COVID-19-related restrictions had amplified or enabled abusive behaviour. A key contributing factor for participants was having to spend more time with the perpetrator at home and being isolated from family and friends, which gave the perpetrator more opportunities to abuse and monitor them. The following quotes from two participants are examples:
I was a prisoner to the house. Because I couldn’t work he had total control. I did shopping on line so he knew what I spent etc. … he was happiest during lock down.
It was easier for my ex-partner to manipulate me when I was cut off from the outside world.
Many mentioned feeling “suffocated”, “imprisoned” and “trapped”, or commented that nowhere felt safe during the pandemic (for instance, “it was harder to find a safe space in and out of home”). However, it was not only women who were co-habiting who reported an escalation in the abuse. Some said the perpetrator having less access to them triggered monitoring behaviour from a distance:
During lockdowns contact was by phone however [the perpetrator] started to become possessive. Several messages a day, numerous phone calls. Was told to breach lockdown rules to travel to see, we lived in different towns (1.5 hours away). Constant checking up what I was up to.
Participants frequently linked the increased abuse with the perpetrator’s heightened stress levels due to a loss of employment, the pressures of home schooling and/or having fewer distractions or outlets.
[The abuse] escalated immensely during this time and compounded with our 2019 bushfire season and unemployment due to COVID-19. His drinking became out of control and subsequent verbal and emotional abuse, isolation and financial control became a daily occurrence instead of monthly.
Worse because more time together and harder to have a break, their increased stress, and being cut off from supports.
Being together more has brought out his anger and frustration without work as a distraction.
My partner became very unwell. She lost her business, as not being an Australian citizen, she hasn’t had money and we have had to live off one income. It has put us under so much stress, she was never violent before COVID-19.
Women also said that their partner’s constant presence and monitoring of them meant they struggled to take a break from them, to look after their own wellbeing or to make plans to escape:
[It’s] definitely worse during lockdowns – he can still access alcohol/cigarettes and all the things that fuel his behaviour – I was not able to access any support to assist with being away from the abuse such as gyms, yoga class etc.
[The pandemic] intensified the impact of behaviours, made me more isolated, made the household more tense as couldn’t leave the house, more difficult to safety plan/ leave.
Leaving the relationship was made more difficult because of the pandemic. This was not only due to the increased psychological pressure their partner put them under, but also because victims and survivors had fewer employment and housing options available during the pandemic:
[Relationships] changed by taking away many options. Remote learning means I can’t look for work when lockdowns happen often. No predictability as to if we will or won’t be in lockdown make planning for anything very hard. Delay in earning enough money, means no options to move away from the toxic environment. He was home more often, so walking on eggshells and avoiding conflict happened so much more. Plus keep the peace with him home and keeping kids quiet or calm during remote learning simply leads to depression from fatigue and toxic stress.
Limited rental market made it difficult to access my own accommodation when I left relationship.
Some participants who had separated from their partner reported that they were more vulnerable to stalking because public places were quieter:
… fearful as there are less people out and about and thus more opportunities for him to approach and harm me, which he has.
Additionally, some found that it was easier for their ex-partner to discover their home address:
I was advised not to let him in my house or let him know where we lived, but that became impossible under COVID-19 and led to the incident where he harmed my daughter.
Restrictions improved safety
Although most women reported negative impacts of COVID-19 restrictions, some participants said they felt the introduction of rules about curtailing social contacts had a positive impact on their safety. Women who were not living with their abusive partner or had separated from them reported that the restrictions enabled them to avoid contact with the perpetrator.
Felt a little safer not having to see ex at kids’ sport etc.
I have been able to use lockdown as an excuse to spend time by myself and not visit my current boyfriend every weekend.
I felt safer as I didn’t need to go into my work premises where he (or his family/friends) could be … [and] I feel safer at home as I know I’m unlikely to be being watched.
Some also mentioned that they appreciated periods of isolation as it helped them to recover from experiences of abuse:
I’ve been very isolated but used the time to retreat from the world to heal and break trauma bonds.
The pandemic was the tipping point for action
A considerable number of participants said COVID-19-related isolation both increased their partner’s abuse and their own awareness of it.
It put our abuser over the top of us, where previously he went to work so we had some relief. His behaviour escalated and mine and my children’s anxiety, anger, etc. escalated immensely. It was the tipping point for my awakening as to what was going on and that all the behaviours and physical manifestations I was seeing in my kids was due to his behaviour.
For some, this was a catalyst for their decision to end the relationship:
Intensified the behaviours to extreme breaking point. For me this was a good thing. Things got so bad that drastic urgent action needed to be taken. I think I would have had a back-and-forth relationship for years otherwise as I am concerned that he would have been able to charm or threaten me back into the relationship. However, things got so bad as a result of constant contact and his control over me during lockdown that it was so much easier to leave than stay.
I have become less tolerant of his bad behaviour – have hated not being able to have time away from him and it is the impetus for breaking up now.
Conclusion
This section has outlined the experiences of abuse and violence, the sociodemographic characteristics associated with IPV and/or SV, health impacts and the effects of the COVID-19 pandemic. The next section explores help-seeking in detail.
2. Help-seeking experiences of victims and survivors of IPV and/or SV
This section integrates the findings from the surveys and interviews with victims and survivors regarding who sought help from social, health, specialist, justice, housing and community services, and how helpful those supports were found to be. This section also documents barriers to help-seeking. The interviews explored the women’s journeys of seeking support and safety and how their engagement with the service system unfolded over time. Both informal and formal services were included, ranging from all sectors that could come in contact with victims and survivors. It should be remembered that one third of participants were from Victoria, a state where there has been a marked degree of reform across the system in the last five years.
Sources of help and perceptions of helpfulness
Victim and survivor participants were more likely to have sought support from a friend/s (54.3%) or family member/s (38.3%) than from a formal support service. More victim and survivor participants than not (64.4%) had accessed one or more formal sources of support at some time in the past, and overall 57.1 per cent of these participants rated the formal support services as helpful or very helpful (Figure 12; Table 13). Health services (psychologists, counsellors, GPs, allied health and family counselling) were the most common type of formal support service accessed, with51.4 per cent of victim and survivor participants having accessed one or more health professionals. Health services were also the most likely type of support to be experienced as being helpful, with 65.6 per cent of service user participants reporting this. Housing and financial services were the least likely services to be accessed for support, with 15.1 per cent of victim and survivor participants ever having used those types of services. One in five (21.5%) participants did not seek any form of advice or support from services (Table 13).
Figure 12: Proportion of women who accessed support for lifetime IPV and/or SV and types of support they accessed (n=1,111)
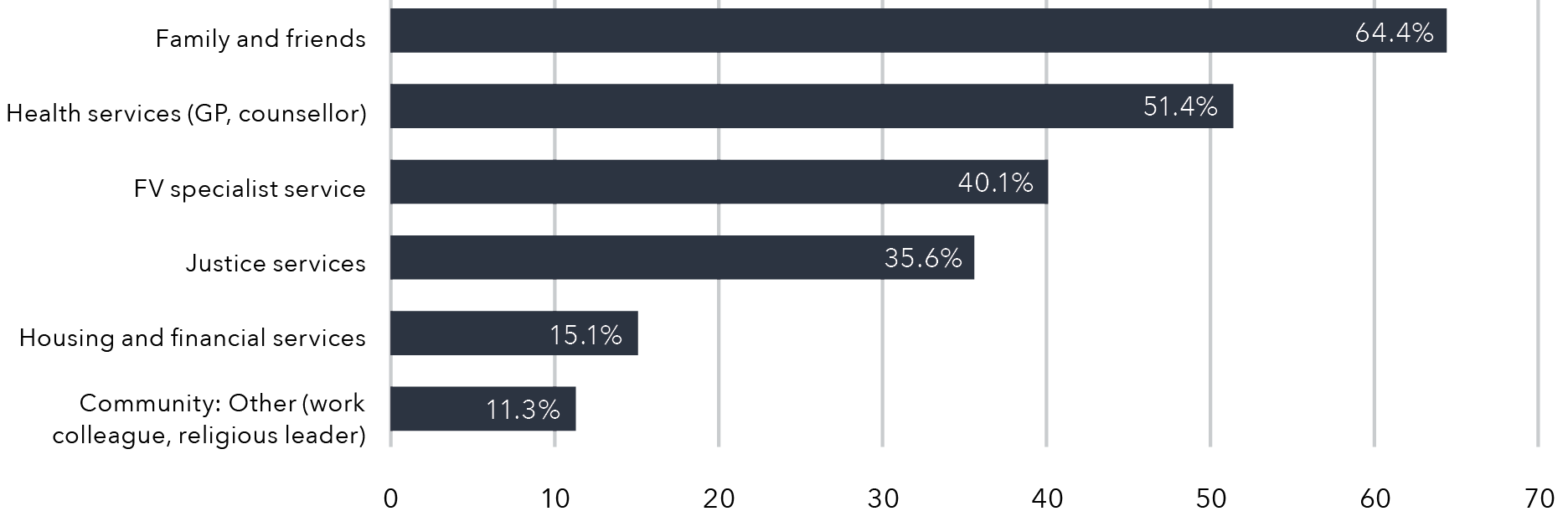
Data table for the figure above:
Type of support
Percentage
Family and friends
64.4%
Health services (GP, counsellor)
51.4%
RV specialist service
40.1%
Justice services
35.6%
Housing and financial services
15.1%
Community: Other (work colleague, religious leader)
11.3%
Table 13: Proportion of women who have sought help for IPV and/or SV and perceived helpfulness
Service/resource
Sought support
(n=1,111)
Found support helpful
n (%)a
Any source of help
872 (78.5%)
62%b
Family and friends (total)
714 (64.4)
64.3%c
Friend/s
603 (54.3)
399 (66.2)
Family members
426 (38.3)
284 (67.9)
Partner
90 (8.1)
53 (58.9)
Formal sources of support
715 (64.4)
59.6%
Health services (total)
571 (51.4)
65.6%
Psychologist or counsellor
469 (42.2)
354 (77.1)
General practitioner
268 (24.1)
182 (69.5)
Social worker (hospital/community health)
125 (11.2)
82 (66.1)
Family therapist
56 (5)
31 (56.4)
Nurse
49 (4.4)
27 (56.2)
Alcohol and/or drug worker
41 (3.7)
26 (68.4)
Specialist services (total)
446 (40.1)
65.6%
Domestic or family violence service
332 (29.9)
163 (63.7)
Telephone helpline (e.g. Lifeline, 1800 RESPECT)
258 (23.2)
Missing
Sexual assault service
108 (9.7)
71 (67.6)
Justice services (total)
396 (35.6)
53.9%
Police
346 (31.1)
166 (48)
Legal service (e.g. solicitor or legal aid)
214 (19.3)
128 (59.8)
Housing and financial services (total)
168 (15.1)
52.6%
Financial service (e.g. Centrelink)
138 (12.4)
69 (50)
Housing service
78 (7)
43 (55.1)
Community – other (total)
126 (11.3)
53%
Work colleague or boss
100 (9)
65 (65)
Priest/minister/rabbi or any other religious person
39 (3.5)
16 (41)
Did not seek advice or support
239 (21.5)
N/A
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to opt-in survey item about having spoken to someone about relationship issues, after experiencing violence and/or unwanted sexual encounters.
a Total number of participants who had accessed 1+ source of help (average proportion of all participants who found source of help helpful).
b Helpful/very helpful (median).
c Category % totals are an average of helpfulness across the sources of help within that category.
Help-seeking of women from diverse backgrounds
Some women participants were more or less likely than others to have accessed certain types of support (Table 14). Participants who were Aboriginal and Torres Strait Islander women, women who have difficulty managing on their available income, women aged 25 to 45 years, or those no longer living with their partner were all over-represented as users of informal and formal support compared with other women. Migrant women less often sought help from specialist services. Young women aged less than 25 years most often sought help from family and friends and less often from health and specialist services.
Table 14: Proportion of help-seeking by women from diverse backgrounds
Participants
Family and friends
Health services
Specialist services
Justice services
Housing /financial services
Community – other
Did not seek advice or support
n (%)
All participants (n=1,122)
714 (64.3)
571 (51.4)
446 (40.1)
396 (35.6)
168 (15.1)
126 (11.3)
239 (21.5)
Age (years; n=1,120)
Participants
Family and friends
Health services
Specialist services
Justice services
Housing /financial services
Community – other
Did not seek advice or support
n (%)
Up to 25 (n=104)
93 (75)
45 (36.3)
26 (21)
14 (11.3)
4 (3.2)
6 (4.8)
27 (21.8)
25–45 (n=516)
376 (68.6)
299 (54.6)
253 (46.2)
219 (40)
102 (18.6)
68 (12.4)
94 (17.1)
> 45 years (n=418)
244 (55.7)
226 (51.6)
166 (37.9)
162 (37)
62 (14.2)
52 (11.9)
118 (26.9)
Aboriginal and/or Torres Strait Islander (n=76)
58 (66)
44 (50.6)
43 (49.4)
35 (40.2)
15 (17.2)
6 (6.9)
13 (14.9)
Migrant background (n=192)
134 (61.7)
110 (50.7)
64 (29.5)
65 (29.9)
22 (10.1)
29 (13.4)
52 (24)
Same-sex partner (n=29)
24 (68.6)
18 (51.4)
16 (45.7)
11 (31.4)
7 (20)
4 (11.4)
4 (11.4)
Lives in non-metropolitan location (n=297)
199 (63.2)
169 (53.6)
142 (45.1)
122 (38.7)
53 (16.8)
35 (11.1)
60 (19.1)
Lives with disability (n=439)
272 (62.5)
242 (55.6)
187 (43)
163 (37.5)
76 (17.5)
48 (11)
97 (22.3)
Attended school but finished prior to Year 12 (n=301)
196 (60.1)
159 (48.8)
139 (42.6)
121 (37.1)
51 (15.6)
26 (8)
80 (24.5)
No university degree (n=552)
369 (61.7)
284 (47.5)
236 (39.5)
208 (34.8)
89 (14.9)
49 (8.2)
128 (21.4)
No employment (n=401)
258 (59.3)
213 (49)
165 (37.9)
149 (34.2)
74 (17)
34 (7.8)
115 (26.4)
Has difficulty managing on available income (n=584)
401 (64.1)
339 (54.1)
286 (45.7)
248 (39.6)
122 (19.5)
74 (11.8)
130 (20.8)
Health Care Card holder (n=588)
452 (66.3)
330 (51.5)
284 (44.3)
246 (38.4)
116 (18.1)
54 (8.4)
122 (19)
Not living with partner (n=580)
422 (68.3)
378 (61.2)
296 (47.9)
284 (45.9)
122 (19.7)
90 (14.6)
109 (17.6)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
The proportion (%) in this table represents the proportion of overall demographic group who have accessed help by category.
In brief:
Help-seeking victim and survivor participants

Aboriginal and Torres Strait Islander women and women who had difficulty managing on their available income more often sought support from specialists and justice services; women not living with their partner more often sought support from health, housing and financial services.

Migrant and young women less often sought support from specialist, justice, housing and financial services.
Barriers to help-seeking
Various personal, information and service barriers were identified by victim and survivor participants as affecting their access to services (Table 15). The top three most cited barriers preventing help-seeking were as follows: shame (63.2%); lack of awareness about a service that could help (62.1%); and concerns about confidentiality (49.5%).
Table 15: Proportion of women who have experienced IPV and/or SV who identified barriers to professional help-seeking (n=1,108)
Barriera
n (%)
Shame
700 (63.2)
I feel too ashamed to talk to anyone
590 (53.2)
I don’t want to talk to anyone about my partner’s behaviours, it is too personal
454 (41.2)
Lack of awareness of services that could help
688 (62.1)
I was uncertain who to see
508 (46.1)
I decided not to seek care as not sure it would be helpful
437 (39.7)
I don’t know of any service that might be able to help
403 (36.6)
Confidentiality
549 (49.5)
My friends or family will find out
443 (40)
The professional will tell others
359 (32.4)
Low priority/lack of time
515 (46.4)
I had too many personal or family responsibilities to seek help
403 (36.6)
I have no time to talk to someone about these things
285 (25.7)
Communication
485 (43.7)
The professional will not understand me
485 (43.8)
Normalisation of violence
394 (35.5)
My partner’s behaviour was a once-off. It won’t happen again
299 (27.1)
My partner’s behaviours are just a normal part of relationships. I don’t believe there is any need to see a professional about them
271 (24.5)
Access challenges
274 (24.7)
I have no access to transport to see someone
274 (24.7)
Cultural issues
173 (15.7)
My culture or religion is a barrier for me seeking help
173 (15.7)
Total participants who needed IPV and/or SV help, but were unable to get it
533 (48.1)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; maximum missing n=9.
a Barrier defined as those elements that participants said were “Moderately important”/“Very important”.
Close to one in two (48.1%) participants said there had been a time when they needed help for relationship issues or sexual assault but could not get it. Of these 533 participants, the top two service barriers they most frequently encountered that prevented them getting help were difficulty understanding the professional/worker and lack of available appointments (Figure 13).
Figure 13: Proportion of women who experienced service barriers that prevented them from accessing help (n=533)
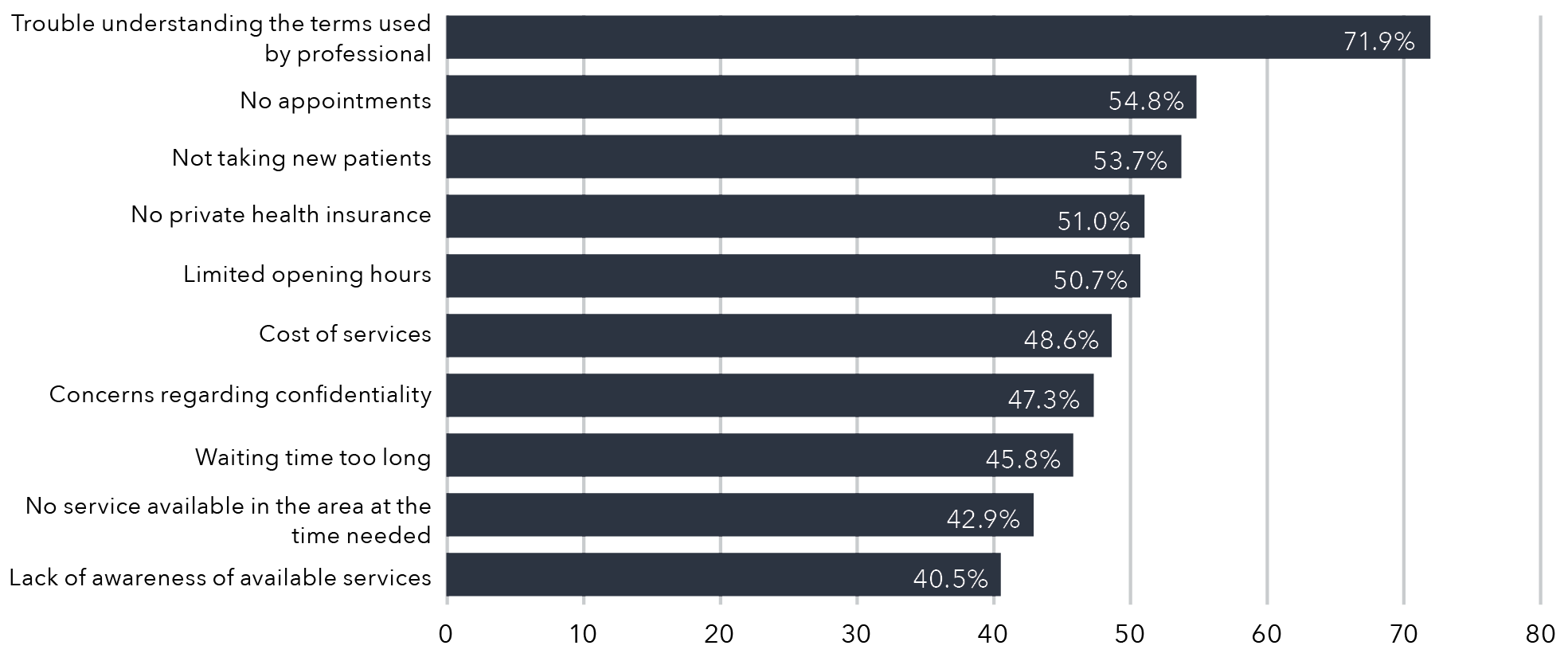
Data table for the figure above:
Barriers
Percentage
Trouble understanding the terms used by professional
71.9%
No appointments
54.8%
Not taking new patients
53.7%
No private health insurance
51.0%
Limited opening hours
50.7%
Cost of services
48.6%
Concerns regarding confidentiality
47.3%
Waiting time too long
45.8%
No services available in the area at the time needed
42.9%
Lack of awareness of available services
40.5%
Please note: 566 participants were omitted from this analysis because they had never been in the situation of needing help and being unable to get it.
The next section utilises the interview data to describe women’s journeys to seeking help.
Journeys to seeking help and support
To further illustrate the victim and survivor participants’ help-seeking journeys, we present the interview findings from the 30 women victims and survivors, which offer a deeper understanding of the survey responses.
Demographic profile of interview participants
Participants’ ages spanned between 19 and 62 years, with a median age of 38.5 years, and most participants (24) were aged between 20 and 59 (Table 16). They were living across Australia, with 24 of them living in the eastern states. Over a third (11 participants) were born overseas, with six born in countries in Asia (India, China, Hong Kong, Japan), and the remainder from the United Kingdom or countries in Europe or South America (Ecuador, Israel, United Kingdom, Greece). Two were Aboriginal. The majority were employed (21) and tertiary-educated (28). Half (14) were living with a disability or chronic illness that limited them from daily activities, including employment. Most had experienced IPV and/or SV from a male perpetrator while in a heterosexualrelationship, while three women had experienced abuse in a same-sex relationship. Two thirds (20) had children with the partner who used IPV. All were separated from the perpetrator at the time of the interview. Not all women responded to the survey sections where they identified the types of IPV and/or SV they had experienced, and the interview discussions did not focus on exploring the details of the IPV and/or SV. However, more than a third answered on the survey that they had experienced forms of physical and/or sexual violence from a partner.
Table 16: Interview participant demographic details (n=30)
Age (years)
Age
n
15–19
2
20–29
6
30–39
8
40–49
6
50–59
6
60–69
2
State/territory of residence
Age
n
Australian Capital Territory
2
New South Wales
4
Northern Territory
1
Queensland
7
South Australia
4
Tasmania
4
Victoria
7
Western Australia
1
Central theme: Carrying the burden alone
We first discuss the overall themes in the women’s stories of navigating the service system to address their partners’ abuse. We then explore how the women’s help-seeking unfolded over time.
Our analysis of the women’s narratives about their help-seeking journeys led to an interpretation of the overall experience as being one of “carrying the burden alone”. This was exemplified in a number of ways. In reflecting on their early experiences of abuse in their relationships, interview participants spoke of feeling responsible for their partner’s behaviour. For example, one woman said her partner had brainwashed her to believe his abuse of her was “my problem and my responsibility to fix”. In participants’ narratives of engaging with the service system, the main theme was that the responses they received had only reinforced that perception. Women felt that the onus was on them to manage the perpetrator’s behaviour and to keep themselves and their children safe. Although participants offered examples of responses that had been helpful at different times, they suggested that, overall, the service system had provided only short-termassistance, little protection, and minimal financial, material and emotional support. They felt services were under-resourced, and professionals were often disinclined or simply unable to engage meaningfully with their individual experiences. This perception was reflected in participants’ comments about feeling like “a number”, “just another victim” or that they “didn’t really matter at all”. They felt they were expected to curtail their freedoms to avoid the abuse and to manage the impacts on their own and their children’s mental health. Meanwhile, the perpetrator was subjected to little scrutiny and few restrictions, and in many cases was only emboldened by his or her contact with the service system.
To illustrate this central theme, we present three brief narratives of women’s journeys through the service system. The three narratives presented below illustrate women’s experiences of “carrying the burden alone”. Each of the women expressed that they felt the service system put the onus on them to manage the perpetrator’s abuse and to cope with its consequences. Fiona’s story highlights how a lack of intervention and information sharing by service providers leaves women feeling they are responsible for addressing the perpetrator’s behaviour on their own. Nella’s story speaks to the sense of loneliness women can feel when they are unable to trust services to offer effective support or to understand the dynamics of their individual experiences. Indeed, for many Aboriginal and Strait Islander women such as Nella, services can be not only unhelpful, but harmful. In Julia’s narrative, we can see how exhausting it is for women to have to constantly“go into battle” to protect themselves and their children, with little support to back them up.
“I’m the only one calling him out”: Fiona
Fiona said she noticed her partner’s aggressive outbursts were becoming more frequent, but she was constantly in “fight or flight mode” so it was hard to think clearly about what was going on. She spoke about her partner’s “anger issues” to their family’s GP, who referred him to a support service. However, she discovered her partner only attended one session then refused to continue. Fiona was upset that no one had informed her of this, and no one followed up with her partner:
The GP knew stuff was happening … but when you’re dealing with someone who acts like this in a family environment, you’re just kind of letting that person run wild with no follow-through. So, then all the onus is on me.
Fiona became particularly concerned about how her partner’s aggression was affecting their children. She confided her concerns to a supportive friend, who encouraged her to contact a DV hotline. The hotline helped by validating her concerns and providing practical tips, but Fiona said: “The support thereafter was a bit lacking. I just feel that they’ve not got the time. They’re just so under-resourced.”
The violence continued and there were occasions when Fiona had to flee the house with her children. Finally, she went to the police, which was a turning point in her leaving her partner. They arrested him and applied for a family violence order, so he wasn’t allowed back to their home. However, Fiona described the police’s approach to communicating with her as “very hands off”. They charged her partner with assault but failed to inform her they were doing so. While Fiona was ultimately glad charges had been laid, the police appeared to give little consideration to the ramifications for her safety; as she said, “any impact it [the assault charge] has on him, it goes back on me”.
Fiona’s partner breached the court order several times, with mixed responses from police. She found the criminal prosecution process extremely confusing: “You’ve got so many questions and concerns … but they’re already too busy onto the next [case].” She also attended family mediation with her partner to develop a parenting agreement. However, this was a frustrating experience. Even though the mediators privately told her they had noticed her partner’s manipulative behaviour, they did not directly confront him about it:
[I wish they would] tell him so that he knows, because he’s just walked out of here thinking that he’s still king pin and you’ve believed him … I’m the only one that calls him out on his behaviour … Nobody’s actually overseeing how that interaction is going and how that person’s behaving.
Fiona said she would like to understand what her legal and financial entitlements are but keeps “getting shipped off” to different services. She also wants to find a counsellor for emotional support, but in between trying to work, supporting her children and selling the home she shared with her partner, she has had to put her own needs “on the back burner”.
You feel alone”: Nella
Nella identified as Aboriginal and said her family had suffered from intergenerational trauma. As a child, she was removed and put into foster care. She said: “If we were a British family I probably never would have been taken away.” As a teenager, she became involved with a partner who was abusive. She sought help from a mental health hotline as she had not slept for days. However, she said: “When you’re under 18, if you talk to anyone about anything even vaguely negative, they call the cops.” The hotline reported her situation to the police, who arrived at her school and asked “invasive” questions. Based on prior experiences, Nella said she knew not to trust the police:
When you’re not a child of the chalk … that’s not a good idea to deal with cops … I said to them, “I’m not saying anything. I don’t talk to police. I’m not the one who committed a crime here so leave me alone.”
The risk of police involvement meant she felt unable to seek assistance until she was over the age of 18. Nella said, “when you can’t tell anyone you feel alone”. Her new partner and a friend were supportive, but she didn’t want to burden them by sharing the details of her abuse. Eventually, suffering nightmares and struggling to cope, she went to a youth mental health service. However, the counsellor seemed to hold her responsible for what had happened, suggesting she should “fight back … not get in the situation in the first place … not trust people … trust different people”. Nella said, “None of those solutions would have helped because I was already putting every single measure you could in place.”
The only way Nella was able to escape the abuse was to move cities and change her name. Now that she is over 18 and has found employment, she has been able to afford to pay for a psychologist to address the PTSD symptoms she experiences.
“Wearing the burden of being careful”: Julia
Julia’s partner was violent from early in their marriage. After he began directing his abuse at their children, she managed to leave him. She found a new home and kept the address from her ex-partner. Her children did not want to see their father because of his abuse. To protect them, Julia fought to obtain a family court order to stop her children being mandated to have contact with their father.
However, Julia said that even though the family court recognised her ex-partner’s abuse, there was no coordination or follow-through from the service system; instead, she had to “go and pick myself up … and tell my story again”. For example, she had difficulties getting local police to recognise the family court orders. Her ex-partner also began “playing games” with child support, which was another problem that she had to figure out how to address.
Julia said she believes her ex-partner likes to play games like “a cat and mouse. He is just going to continue to keep me on that edge” and every day it feels like she is “going into battle”. However, she can’t risk applying for a domestic violence protection order because she will need to provide her address, and she believes her ex-partner will not be deterred by another “piece of paper”. In the past she has had to push the police to act, but recently, they have recognised the risk she faces. The police have told her: “This is serious, you’re going to have to change, don’t have any patterns, don’t be on social media, don’t do anything.” But Julia said constantly having to be wary and restrict her freedoms has “ruined my life … why am I wearing the burden of being careful?” She can only leave the house at times of the day when her ex-partner is likely to be occupied, and she is unable to use social media, which has damaged herjob prospects and connections with others.
Julia has also faced difficulties getting medical and other services to understand her safety and privacy needs. She has sought counselling to help manage her constant anxiety, but the psychologist has told her that her symptoms can’t properly be treated while she remains unsafe.
Key responses at different stages in women’s help-seeking
Based on our analysis of the interview themes and the timelines we created from the interview data with 30 victim and survivor participants, we identified five key stages of help-seeking: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; establishing independence and safety; and addressing impacts and making sense. These stages reflected particular help-seeking needs or goals at different times. Each stage was triggered by critical turning points or changes in how women understood and experienced the abuse. Figure 14 provides a visual illustration of the different stages of participants’ help-seeking journeys and the turning points or changes in their experiences or understandings of the abuse at each stage.
It is important to note that while the stages reflected common needs and turning points across participants’ timelines of seeking help, not every participant passed through each stage in order (or at all). Additionally, there were often overlaps and loops back between the stages. For example, many women went through the stages of trying to get out of the relationship and re-establishing their independence and safety, but then returned to the relationship and to the stages of maintaining hope and/or assessing options. All of the participants we interviewed had eventually left the relationship, but for some it had taken many years. Despite ending the relationship, many were still subjected to ongoing abuse, threats and stalking by their ex-partner. Additionally, across every stage of their journeys, women prioritised supporting their children (i.e. not only in the addressing impacts and making sense stage). However, many said that once they and theirchildren had become safer (often after leaving the perpetrator), they began to seek out formal counselling and support programs for their children to address the trauma of the IPV and/or SV.
Figure 14: Key stages and turning points in victims’ and survivors’ help-seeking journeys
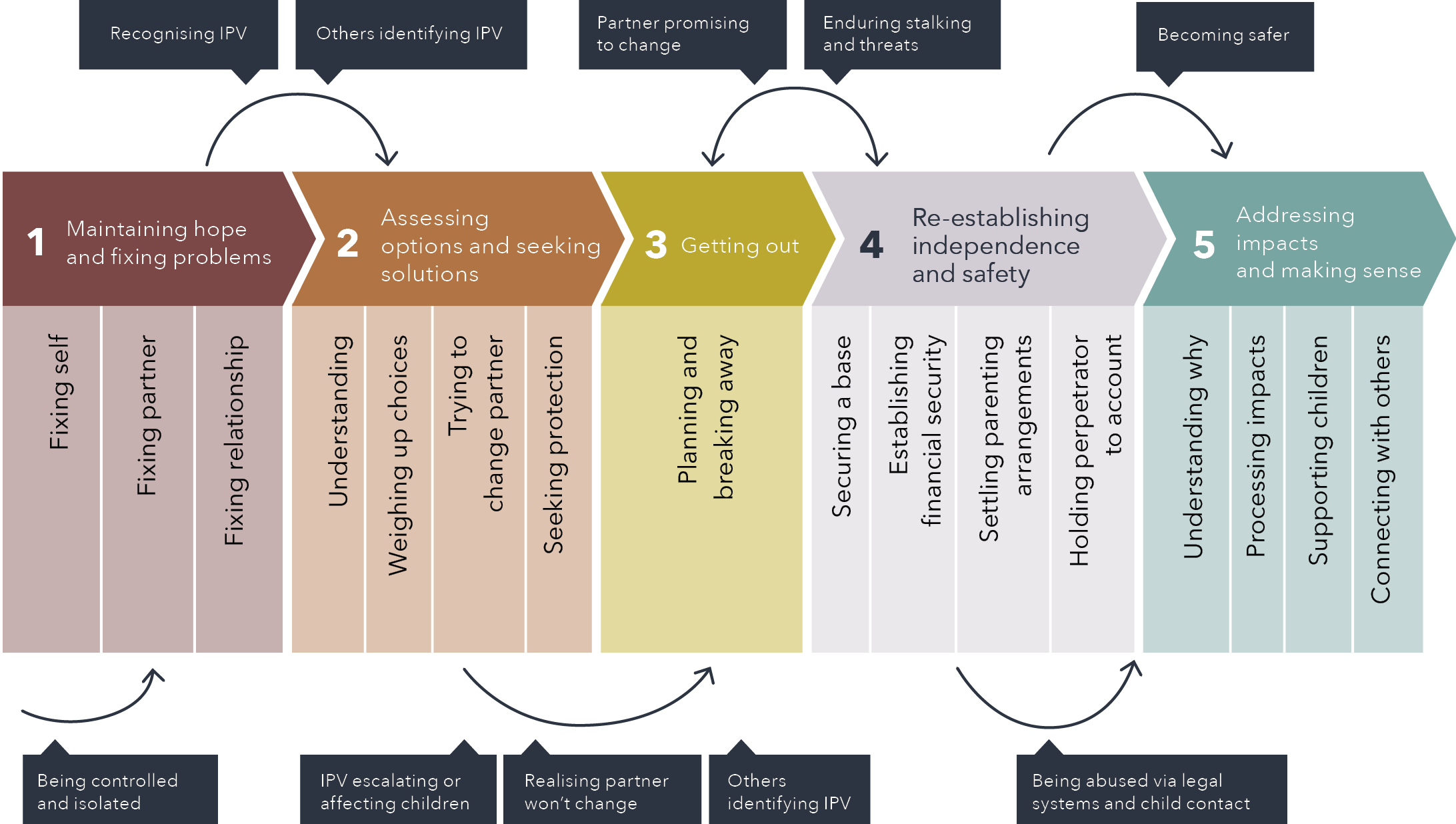
Text version of the figure above:
- Maintaining hope and fixing problems
- Fixing self
- Fixing partner
- Fixing relationship
- Assessing options and seeking solutions
- Understanding
- Weighing up choices
- Trying to change partner
- Seeking protection
- Getting out
- Planning and breaking away
- Re-establishing independence and safety
- Securing a base
- Establishing financial security
- Settling parenting arrangements
- Holding perpetrator to account
- Addressing impacts and making sense
- Understanding why
- Processing impacts
- Supporting children
- Connecting with others
Before step 1 to step 1:
- Being controlled and isolated
Between steps 1 and 2:
- Recognising IPV
- Others identifying IPV
Between steps 2 and 3:
- IPV escalating or affecting children
- Realising partner won’t change
- Others identifying IPV
Between steps 3 and 4:
- Partner promising to change
- Enduring stalking and threats
Between steps 4 and 5:
- Being abused via legal systems and child contact
- Becoming safer
In the following discussion, we explore the five stages of help-seeking in detail. We also draw on narrative and thematic data to identify helpful responses in each stage. As explained in the previous section, the women largely felt the service system had let them down and left them carrying the burden of managing their partner’s/ex-partner’s behaviour and coping with its impacts. However, participants also described key moments during their help-seeking journey when service providers responded in a way that made them feel supported and less alone. We provide examples of positive or pivotal responses at each stage of help-seeking, as well as examples of responses that were inadequate in meeting women’s needs. We use participant quotes to illustrate. For longer quotes we provide a participant number to indicate which interview participant is being quoted.
Stage 1:
Maintaining hope and fixing problems
In describing their early experiences of engaging with others about the abuse, many women spoke of unawareness and misdirected help-seeking. They recalled noticing manipulation, isolation and controlling behaviour from their partner, but did not fully acknowledge it as abusive and hoped the relationship would continue. When women were subjected to psychological or sexual forms of abuse, it was particularly difficult for them to recognise the behaviour as unacceptable.
In relation to their early help-seeking, women described approaching their family and friends, GPs, health professionals, psychologists, psychiatrists and relationship counsellors. Their aim was to maintain the relationship and to try to fix what they perceived to be causing the problem: their own mental health issues, their partner’s mental health or drug and alcohol use, or the communication in the relationship. For instance, one said: “I was like, my partner is an addict and I need to help them” (Participant 9). Another said: “I very much thought … he’s had a mental health crisis. Once he gets help for that, everything will be all right” (Participant 22).
During this stage of help-seeking, women said the following responses were helpful or pivotal in shifting their understanding of their situation.
“Someone cares”: Inquiring about wellbeing
For some women, having a professional take the time to directly ask about their emotional wellbeing and safety in their relationship was a significant turning point; it gave them an opportunity to open up about their experiences, and it demonstrated that someone else cared about what was happening to them. This was the case for one woman (Participant 6). She married her husband in India, but he became physically violent when they came to live with his family in Australia. She said in her culture it is unacceptable to leave a marriage, so all she felt she could do was “pamper” him in the hope he would change. His aggression escalated when their child was born. A neighbour became concerned and called the police. The police took her to stay with some extended family members but did not refer her to any DV support services.
It was only when the participant’s maternal and child health nurse directly asked her what was going on in her relationship that she felt able to disclose. The nurse had witnessed signs of abuse and had purposely followed up by making a private appointment to see her:
When [the nurse] said to me that “Are you okay and are you free and safe?” … I burst into tears, and I told her the whole story … She said, “When you came to me after … [your baby’s] health check, I knew something is wrong. I saw your husband was treating you very badly in front of me … I didn’t talk to you at that time because your husband was there with you … But I was just trying …to contact you if you are okay” … I was so happy, finally there is someone who cares about me, who cares about my daughter. (Participant 6)
“It’s not you”: Identifying the abuse
Almost a third of the women reported that an interaction with a service provider had been pivotal in transforming their perspective on their relationship. For instance, one woman (Participant 1) said her partner’s psychological abuse worsened when they moved to a regional property, as there was no one around to hear it. However, at the time, her partner manipulated her to think her own depression was the cause of his behaviour. She suggested the responses of a GP helped lift the burden of self-blame and led her to begin seeking help to end the abuse:
I thought there was something wrong with me, [I was] depressed … [My partner] keeps telling me I was psychotic … So, it felt like a bit of relief talking to the doctor because she said “Oh no, no, no. This is gaslighting. It’s not you. It’s perfectly normal to feel upset and depressed in this situation.” (Participant 1)
However, other women explained that their initial contacts with professionals had only reinforced the notion that they were responsible for their partner’s behaviour or the problems in their relationship. One said:
I was still seeing … his aggression as something that I was doing wrong that I could work on myself and change. [But] there was no suggestion [from the counsellor] that what I was facing wasn’t okay. She was giving me strategies … that I could try … I would have been so much better equipped earlier on if I had of understood that these behaviours were not okay, and they were not something that I could control … that would have made a significant difference. (Participant 3)
In some cases, health professionals had diagnosed women with a mental health disorder rather than exploring underlying causes of their symptoms:
[I] just ended up on a bunch of medication and going down this line of people thinking I had bipolar. So, I was like, this isn’t helping with me feeling that it’s not all in my head and not all my fault. (Participant 9)
A focus on psychopathology was particularly problematic for women who had already been diagnosed with a mental illness. For example, one said:
I actually never felt listened to because it was always about the schizophrenia. So, any concerns I raised were dismissed as symptoms of my mental disorder … It maintained the idea that I was the problem. (Participant 29)
Stage 2:
Assessing options and seeking solutions
Once each of the women recognised that their partner’s behaviour was unacceptable, their focus was understanding what was happening and how to address it. During this stage, the women sought advice and assistance from mental health services, counsellors, health professionals, domestic violence and sexual assault services, and their family and friends. Several also sought police protection during incidents of aggression from their partner or contacted police for advice. Some engaged with men’s mental health services and behaviour change programs in the hope that they could help to stop their partner’s abuse.
However, disclosing the abuse to others was not an easy thing and many said they were extremely wary about doing so. Some struggled to find a private moment to talk freely, particularly when their partner constantly monitored their communication with others. Several said they felt ashamed and feared being judged. For example, one said: “I was humiliated that I was in this relationship where I was being controlled by somebody else … I felt embarrassed to have to tell people” (Participant 8). Being in a same-sex relationship added another layer of concern for some women: “There’s already enough criticism of [same-sex relationships]. Then you don’t want to say, ‘Oh, by the way, I’m actually in an abusive relationship with my same-sex partner’” (Participant 9).
Women also feared that disclosing their mistreatment could result in unwanted interventions by others; as one participant said: “I was afraid … that someone would [be] silly enough to say something to him, which has happened, and it would make it worse for us” (Participant 10). A major concern for those with children was that they would be reported to child protection. For Aboriginal women, racial discrimination made this a significant risk:
[Being from] an Aboriginal family, I was always afraid that even if I was listened to, I would be seen as the problem and my children would be removed from my care. (Participant 29)
Yet despite these barriers, each of the women had managed to disclose the abuse to formal service providers, hoping that they could help them to explore their options and potential solutions. In some cases, confiding with others about the abuse was a positive or transformative experience for the women, while in other cases it only deterred them from further help-seeking.
“I’m not going to judge you”: Listening and showing empathy
In deciding whether to disclose and how much to share with professionals, women looked for signs that they could trust them to provide an understanding response. For example, one participant said that her therapist responded to her disclosure “in a way that says ‘It’s okay to bring that here. I’m not going to judge you.’” She reflected that it was critical that service providers demonstrated they cared and were prepared to listen:
It’s about creating that sense of openness to people’s experiences … Even [if services had] a sticker that said: “If you’re not safe, you can tell me.” Something like that [would help to facilitate disclosure]. (Participant 9)
Participants emphasised that what they needed at the point of disclosure was not anything complex – it was simply to be believed and listened to. For instance, one woman said the supportive response from her local police made a big difference:
Just that hand on the shoulder and saying, “We understand how awful this is and we believe that what you say occurred did occur.” Just small things, just “we believe you” and listen to you. (Participant 4)
They greatly valued service providers showing concern for their wellbeing, asking questions, and giving them time to talk. For example, one spoke to a pelvic floor psychologist about the sexual assaults by her partner:
[She] just listened, and she believed me … she didn’t question it happening, she just asked more questions to find out more. I think that was probably the biggest thing, is feeling heard. (Participant 17)
“Take me seriously”: Validating concerns and identifying risks
Having their concerns validated was critical, considering that, as one woman said, “When you’ve been controlled and manipulated, you doubt your own feelings” (Participant 1). While women appreciated validation from their family and friends, the perspective of a professional with expertise in the area was a major turning point in recognising that the problem was legitimate and important to address. This was reflected in the following comments from two participants:
Having it almost … justified by a professional [meant] … I felt like I wasn’t crazy, like I [hadn’t made] all of this stuff up in my head. (Participant 17)
[The police officer] took all the details, she listened, and she took me seriously. She said, “You’re at moderate risk” … I came away thinking, well jeez, if the police take it that seriously then it must be a mess … They see this every day, so they know what they’re talking about. (Participant 28)
Having an outsider tell them that they had noticed the abuse was also valuable in making women feel they were not the only person who saw it. One woman said it made a “huge” difference when she was contacted by the facilitator of the men’s behaviour change program her partner was attending:
[The facilitator] said “I’m concerned about you because I’m not seeing changes in [your partner] that I would have liked at this point” … Our mutual friends don’t get it because they’ve never seen him like that. I’m the only one. So, I appreciated that … There was a validation there … It was huge and at the end of that very short conversation, I thought, ooh, I might be ready [to leave]. (Participant 20)
However, women also received responses that discouraged them from further help-seeking. The terms used to describe abuse by an intimate partner were deterrents for some women. Several said they had been uncertain about whether they could access domestic violence or sexual assault services because their experiences of violence or abuse did not fit common stereotypes. For example, one young woman who was sexually assaulted by her partner said:
The reason why I didn’t reach out to any [domestic violence or sexual assault] services like that [was] because I wasn’t, quotation marks, “raped” … [and the term] domestic violence I’ve never … appl[ied] to my situation … [The term “domestic violence” is] quite mature … you often think of it being like a 40-year-old woman who’s been in a relationship for 20 years. (Participant 17)
Some women who were experiencing non-physical forms of abuse did contact domestic violence services; however, they said that the questions asked during risk assessment processes made them feel that their concerns were less valid. For example, one said:
[The DV counsellor asked me] “Do you feel scared?” – “Yes.” “Has he ever hit you?” – “No.” There would be like a little, “Okay, okay”, like I could see in their face or their body language, the more serious questions around sexual assault or physical violence. “Okay, we don’t have that situation here. I can just downgrade my concern a little bit.” Which didn’t help when I was questioning if [the abuse] was real. (Participant 20)
“We’ll go as fast or slow as you need”: Exploring options without pressure
A valuable response from service providers during this stage was providing information and exploring options without expecting women to act immediately. For example, one woman contacted a local police domestic violence liaison officer when she was considering reporting her partner’s sexual and physical assaults against her. She found her initial contacts with them “really supportive”:
[The officer] said “Look, there’s no pressure … we’ll go as fast or as slow as you need to” … She gave me lots of things to read … She was like, “Go online and have a look at this. There’s a … form that you can get” – she gave me options, and then was, like, “Ring back anytime.” (Participant 15)
In contrast, women frequently described directive advice as unhelpful, particularly when they were not emotionally ready or lacked the resources needed to act on the advice. For instance, one felt the well-intended approach she received from her friends and a DV service was not helpful because she was not ready to hear it:
[The domestic violence counsellor] said, “Right, let’s make a safety plan, I want you to have a packed bag in your car, I want you to do this, and this, and this” and I was like “What? I just need help figuring out what I’m going to do to get strong” … People saying things to me directly about “This is bad, and you need to get out” didn’t help at all … The message was probably okay but there wasn’t support to back it up. (Participant 20)
Another concern was a lack of emphasis on encouraging perpetrators to change their behaviour. Some women felt that the service system was predicated on an assumption that the best solution was the victim immediately ending the relationship with the perpetrator, but this was not practical in the long-term, particularly when children were involved. For example, one woman (Participant 19) said that she felt pressured by police and services to sever all contact with her partner. What she felt would be a better long-term solution for her children and herself was for her partner to be mandated to attend a residential program for his drug use and to have a dedicated male case worker who could hold him accountable for changing his behaviour. She was frustrated that during a protection order hearing, a magistrate denied her request to order her partner to attend a men’s behaviour change program. She reflected that in the end, separating from her partner hadonly caused her financial hardship and she and her children still had maintained contact with him because he was her children’s father. She said:
There’s so much emphasis on “Kick him out, get an IVO [intervention order], break up your family”, whereas looking back now I wish the support had been, “We’re going to take him out … he needs to go to rehab, he needs to get on top of this” … You’ve got to stop and think about the practicalities … [There’s] nothing that’s viable for a single parent … there’s not that support, to make sure that long term … there’s going to be genuine skills learned or other people helping hold people accountable for their behaviour … [So] it’s just going to keep happening … [And kicking him out and locking him up] doesn’t work for kids who … legally, are told they have to have access with the perpetrator … So, they’re leaving kids to just have to deal [with it]. (Participant 19)
“I would not have made it out alive”: Intervening when necessary
Some participants said they had needed service providers to step in to protect them, even when intervention was not what they had wanted at the time. This was particularly the case when women were in great danger but powerless to escape on their own, or when the perpetrator was manipulating them into making decisions that were not in their interests. For instance, one woman (Participant 30) said her partner had “brainwashed” her to stay in the relationship by promising he would change. She had spoken to a counsellor from a domestic violence service, and they supported her choice to stay. However, on reflection, she said she had needed the counsellor to “be a little harder” on her and help “extract” her from the hold her partner had over her. In the end, what had been helpful was the firm response of a police officer:
The first thing [my partner] wanted me to do, obviously, was to drop the intervention order. [But the police officer] just held his ground. He goes, “No. No, you’re not withdrawing them. What about if we change it to this, this and this?” … At the end of the day … I needed … somebody to question me on this request to withdraw charges … he wasn’t bullying or anything. He was just like a strong dad. (Participant 30)
Women suggested that when professionals stepped in, it was vital was that they had expertise in IPV and/or SV; took women’s concerns seriously; and provided timely responses, follow-up support and clear information. For example, one (Participant 10) said she was unable to disclose her partner’s violence because he constantly monitored her through the cameras he set up in their home. She feared that if police became involved, they would remove her children, or her partner would act on his threats to kill her. However, eventually the police intervened after a family member called a domestic violence hotline about her situation, and the hotline contacted the police. This ended up being a turning point that helped her escape. What made the difference was that the officers were skilled in DFV interventions, took her fears seriously and responded swiftly:
The police turned up on my doorstep to do a welfare check … Fortunately, the two officers were also child protection trained and they were fantastic. They separated us both … I was advised that they would have to tell [my partner] why they were there. I’m like … “I’m terrified … if you leave us here, when you leave, I am dead.” I honestly do not believe that I would have made it out alive if they had not taken us … He was arrested, taken immediately to the police station … We had enough time to gather a couple of things … then we were in the police station overnight … and then straight into safe accommodation. (Participant 10)
However, for other women, critical interventions were followed by poor communication or tardy or unsupportive responses from police, prosecutors and the courts. This only amplified their distress. For example, one woman (Participant 22) said the police took out a protection order and charged her partner with assault, even though she asked them not to. Although this improved her immediate safety, the lengthy delays, lack of agency, and humiliating and intrusive questioning she experienced in the criminal courts deeply traumatised her. She said of the criminal justice response: “It’s good that it’s in place, but … the amount of time it takes for these things to happen and the way the victims are treated needs to change.”
Stage 3: Getting out
When their partner’s abuse escalated or when women realised their partner was not going to change or that the abuse was affecting their children, women made the decision to leave. All of the women in the study had ultimately ended the relationship with their abusive partner, but for many it had been an extremely difficult process and had taken several attempts to do so. To seek help with getting out, women’s main service contacts were domestic violence services, police, Centrelink, housing and welfare organisations. They also relied on their friends and family for practical help with accommodation, childcare and financial assistance.
“Here are the steps you need to take”: Help to plan a safe escape
Once women had decided to end the relationship, they needed to figure out how to safely get away from their abusive partner, how to keep their children with them, where they could stay and how they could survive financially. However, many said they struggled to think clearly and to plan how to get out while coping with regular abuse. As one said: “[I needed] just somebody sitting down and practically talking through, here are the steps that you need to take to move, because you’re so exhausted … so overwhelmed” (Participant 20).
Domestic violence hotlines and services were frequently a source of valuable advice during this time, including practical tips for how to escape in an emergency:
[The DV service] made sure that I had plans and things in place … They helped me to understand that this person could be quite dangerous because his physical abuse was escalating … So, I did what I could and had things ready to grab if I had to get out quickly and park[ed] the car a certain way, so it was easy to get out. (Participant 1)
Some also found police helpful when they took their fears seriously and were ready to protect them:
I was encouraged … to give the details to the police and let them know what was happening. So should he escalate, they apparently can put an alert on the address. So, if they get a call from that address, it’s a priority, so I did that. (Participant 28)
“I’ve got nowhere to go”: Providing income and a secure place to stay
Although women found that information and safety planning advice was relatively easy to obtain, it was more challenging to find material assistance to leave, including a safe place to stay and a means to support themselves. Many were financially dependent on their partner, often because the partner had stopped them from working, controlled their finances, depleted their savings or accrued debts in their name.
When women were facing immediate danger, they found services were able to respond to their practical needs to help them escape. For instance, one woman (Participant 6) felt very vulnerable as she had little financial or family support in Australia and was profoundly grateful that refuge workers were able to provide her with short-term accommodation. They also assisted her to secure a rental property, legal advice, employment and childcare, and provided money to buy furniture when she found a house to rent. She said when she first contacted them:
[The DV counsellor] interviewed me … I said “I’ve got nowhere to go and I’ve got a little child … I’ve got no money, I’ve got nothing” … She assured me that we will be sending you a taxi [to a hotel] … When I got [there] I feel like, “Thank God I am safe” … They found a refuge for me … They gave me proper shelter … I had to pay nothing to them. There was so much good support … everything starts falling into a good place. (Participant 6)
However, many of the women who wanted to leave found that unless they were facing an imminent threat of physical harm, services were unable to offer any tangible help. For instance, one said:
I felt very alone and with a lack of support to actually get out of that situation. Just like, the DV [service] … counselled me for a bit on the phone and said, “This is what we can do. If you feel that you’re in immediate danger, we can remove you or … put you into a motel and then help you find a place” … [But] because I didn’t feel that I was in that situation, I was just left to “You need to leave, good luck.” (Participant 28)
Like other women, she could not afford private rental as a single parent and found there was a very long waiting list for public housing. The only advice services could offer her was to stay with family or friends, but she could not do so as no one she knew had room in their house to accommodate her and her children.
The lack of housing and a financial safety net meant many of the women and their children were trapped with their abuser for a prolonged period. A few were able to remain in their home and to obtain a protection order to force their partner to leave. Yet they found it difficult to obtain financial assistance to get the locks changed or to install security lights and cameras, which meant they could not feel safe.
Stage 4:
Re-establishing independence and safety
After separating from the perpetrator, most women had extensive engagement with various services and the legal system in order to establish a safe place to live and an independent income and to sort out parenting and property arrangements. The services they had contact with at this stage included DV services, Centrelink, welfare and housing services, financial counselling, police, child protection, criminal and family courts, mental health services, and child psychologists, as well as childcare and schools.
“Someone to bat for you”: Help navigating the service system
All of the participants described the service and legal system as disjointed and overwhelmingly confusing to navigate, particularly when they were already stressed and exhausted. They described feeling like they were on a “merry go round”, “running around in circles”, ‘or “flailing around with no clue”. For example, one said:
Nobody seems to know what anyone else can offer, it’s a guess. You get referred here, there, and everywhere. In the beginning you’re on so many phone calls, you can’t remember who you were talking to, where they’re from. You go through the same story hundreds of times, and you just get completely lost. You can’t remember any of it. Then with the practical assistance you get is very little to none. This person will go, “Oh, no we can’t help you with that, but here, try this person”, and they’ll go, “Oh, no, we can’t do that, try this person”, and then you get referred back to where you started at. (Participant 10)
It was difficult having to repeatedly disclose their abuse to different service providers because women felt it exposed them to being judged or disbelieved. One woman said:
It’s just confronting constantly having to tell the story over and over again … Vulnerability and constantly having to pour your heart out to people hoping that they were understanding your situation. (Participant 28)
In a few cases, participants found a professional who helped to lift the burden of working out how to access what they needed. One woman eventually found assistance from a worker from a Victorian DV service that was recently established to provide a coordinated response. She said this was invaluable, though it took seven months from when police referred her there to when the worker finally was able to contact her:
[The worker] was very supportive … She said, “Do financial counselling” [and] she got me in. She rang me constantly to see how I was doing and [to] just be an ear … It just felt like someone cared. (Participant 1)
For another woman, having a DV service guide her through the process of accessing legal protection was a turning point in becoming safer:
He’d taken the children and disappeared … I called [the DV service] highly distraught, and they were terrific. It was because of what they did in the moment of crisis … where they helped me to go to the police station, they supported me with the police, and the police took an application out on my behalf for an intervention order – that was life changing for me. (Participant 5)
However, like many others, she found longer-term support beyond a crisis response was not on offer. Instead, participants repeatedly described being left on their own to navigate a complex and seemingly uncaring system. Consequently, a major need at this stage of help-seeking was for a dedicated case worker who could advocate for women and guide them through the service system. The following examples from three participants illustrate this theme:
What would have really helped is someone just stepping up and saying that “We hear you; we see through how you’re presenting and understand why you’re being like you are.” Having that support person in place to go with you to Centrelink, housing, go with you into court. Just to bat for you. (Participant 4)
You need some sort of integrating liaison officer who’s assigned to you or something like that who can help do some of that coordination work and make sure you’re on track with things. (Participant 12)
If I had somebody who can be your advocate … and can walk you through the process. [Because] my head was in such a fog … A case worker of some description, who can go through things with you … rather than just being left on your own. (Participant 10)
“Tangible things”: Material and financial support
Many women struggled to afford basic items they and their children needed to survive, such as food, clothing, housing, transport and childcare. As the following quotes from two participants illustrate, a few managed to secure some financial help, but this was only short-term:
I actually found [child protection] to be really good … They assisted me to get my daughter into kindy [kindergarten], because I hadn’t been able to afford that previously because of his spending habits, but they wrote me a support letter so that I could get some kindy coverage at no cost for [a] period of time. (Participant 10)
[The domestic violence worker] was able to pay one of my electricity bills … [and] to give me some vouchers … so that I could actually go and buy myself a doona … and a few things that I needed. That was so helpful. Those tangible helpful things are lifesavers when you’re teetering. (Participant 1)
Yet, most discovered there was no consistent financial safety net to support them to regain their independence. One said:
As for financial help, there is zero out there. If you qualify and you get it done in time, there’s a $500 Centrelink emergency payment …[but] there’s nothing else out there really … [You can get a Salvos voucher] every couple of months if you’re lucky and if you can get through to them in the first place, because no one’s answering their phone anymore. So, you struggle. Can I feed my kid today? She needs some new clothes, what the hell do I do? … We’re going to stay with a family member temporarily, but that’s going to end and then where do we go after that? (Participant 10)
Seeing through the abuser’s tactics: Recognising and stopping the abuse
Most of the women (24 participants) were harassed or stalked by their ex-partner after they separated. Two thirds of those participants had contact with the police and the courts, often because they needed protection from ongoing threats and abuse. Several sought to hold the perpetrator accountable for previous violence or assaults through the criminal justice system. Women also sought to settle property and to establish safe parenting arrangements via the family courts.
Women occasionally described good responses from the criminal justice system. For example, one described the police as “fantastic” in explaining their processes and checking in on her wellbeing. In her case, firm legal action and incarceration had temporarily stopped the violence:
He is facing at least 22 different criminal charges related to the DV. He was arrested … and denied bail this time, thank God. [It] just was such a relief … To know that I can go for a walk to the park with my daughter and not have to worry about him pulling up on the side of road and trying to grab us or something. (Participant 11)
Another woman said it had been profoundly validating when a magistrate saw through her ex-partner’s tactics and took action to stop them. She believed what made the difference was that the magistrate and court professionals had been trained in recognising non-physical forms of IPV:
[The court staff are] very aware of all the tactics and the ploys … [The magistrate has] actually seen right through him. She’s highlighted exactly his behaviours. He was arrogant, rude, he spoke over the top … I felt vindicated by the judgment … Seeing that other people can see what I’m dealing with and they’re doing their best to protect me … that’s what’s given me a lot of hope. (Participant 1)
Yet on many occasions, rather than ending women’s experiences of abuse, the legal system had ignored or enabled them. A consistent theme was that police and courts did not recognise coercive controlling behaviour and non-physical forms of IPV. For example, one woman (Participant 13) believed getting legal protection would have been easier if there had been a “physical reason” for it. Her husband’s abuse was not physical; she said it was “not one big thing [but] lots and lots of little things”. He was highly controlling, intimidating and deliberately turned their child and their friends against her. However, she was told by the police that she was unlikely to get a protection order because proving the abuse in the courts would be “almost impossible”. The fact that she had not applied for a protection order was then used against her in the family court to imply that she had been lying about the abuse.
Several said they felt like they were being blamed for the abuse. One woman said the police asked her “What did you do? Have you been drinking?” (Participant 27) Another said police told her to withdraw sexual assault charges against her ex-partner because they were concerned that she had shared intimate texts with him during their relationship, so “a barrister would rip me apart and the jury wouldn’t believe me” (Participant 15).
Women also reported child protection authorities made them feel responsible for failing to protect their children from their partner’s abuse. For example, one said:
All of the weight of keeping your kids safe is on you … that’s the ironic thing, you call the police – doing the right thing, trying to protect yourself and your kids – and then the next thing you know … child protection are calling … questioning you as to why you’re not keeping your kids safe because … the perpetrator keeps breaching the order. (Participant 19)
Many described feeling retraumatised by how they were treated by legal professionals. A participant said the lawyer’s cross-examination of her in the courtroom was just like her partner’s abuse:
You have to sit there. You can only speak once you’re spoken to … you’re mocked, you’re ridiculed … your words are twisted around and thrown back at you. (Participant 3)
When charges were withdrawn or legal processes did not succeed, women felt the perpetrator was validated and “emboldened” in their abusive behaviour. One said her partner used the unsuccessful court case to proclaim to friends and family that “he was innocent … and I was a liar” (Participant 26). As a result of their experiences, many participants spoke of losing faith in the legal system. For example, one said:
Police [were] not helpful. My child lawyer wasn’t helpful, judge wasn’t helpful … My ex breached IVO a couple of times; police never listened to me. I showed them texts, I showed them videos … [So] I was like, I’m not going to call [police] at all … I’m better off shutting my mouth and … put[ting] the [home security] camera on. (Participant 6)
Similarly, many women said that they and their children were let down and unprotected by the family courts. Approximately half of the participants mentioned having contact with family court professionals, including judges, mediators, barristers and solicitors, independent children’s lawyers, family court report writers and other family law experts. A consistent theme was that family court professionals lacked an understanding of IPV, particularly non-physical forms of abuse. A common concern was a failure to recognise controlling and coercive behaviour and how it not only affected women’s safety and wellbeing but also undermined the safety and wellbeing of children. Participants also felt the prevailing processes, culture and assumptions within the family courts had worked against them – including a presumption of equal shared parental responsibility, unequal expectations of mothers and fathers, and jurisdictional conflicts between federal andstate/territory laws, and civil and criminal justice systems. For instance, one woman observed:
The family court has high expectations of mothers in terms of parenting and really low expectations of fathers … There doesn’t seem to be any real mechanisms to address … the behaviours of fathers that have been so destructive. (Participant 3)
Another said:
[The family court professionals] were virtually fuelling his sense of entitlement … the court report [writer] …was writing things like “The mother is a danger to the children by insisting that the children don’t have unsupervised contact with the father, because there is nothing wrong with him” … I mean, this man tried to kill me a number of times and I’ve gone to the police and given my statement … which was then passed onto the family court. [But] they dismissed it and then just took he and I as we presented. (Participant 4)
Further, women felt the family courts did not recognise how perpetrators were able to harness the system as a tactic of the abuse. For example, women said perpetrators would deny requests to move house or to access counselling for their children. One said:
Even though he’d been charged with intimidation and extortion and had an apprehended violence order, the parenting agreement was still skewed in his favour … in that I had all the responsibility, and he had the power of veto over my movements, the way the children were brought up and other stuff … So, my experience of the system is that often it increases the suffering and increases the ability for the abuser to victimise. (Participant 29)
Perpetrators also exploited any opportunity to delay proceedings. For example, one woman said during the COVID-19 pandemic when court hearings were held online, her ex-partner repeatedly claimed to have internet problems, so hearings had to be rescheduled. Another common tactic was to deliberately exhaust women’s financial resources by forcing them to respond to minor complaints:
He would just constantly take me to court … over the most trivial matters. [Like] if I didn’t FaceTime him at a certain time … I went and visited my family, oh, she didn’t have my consent to go do that. Just little things, and it was just on and on and on … I’m still paying off my debt. (Participant 11)
In some cases, professionals were aware of abuse but did nothing to address it. For example, one woman said a family court report writer witnessed aggression during a joint session:
[My ex-partner] got up and he grabbed the coffee table … and he was almost going to up-end it … but then he caught himself just in time … [The court report writer] saw it and I saw the fear in her eyes, and I tried to eyeball her, but she just kept her eyes fixed … She never mentioned that incident at all [in her report]. (Participant 5)
Several remained caught up in protracted litigation and felt powerless to escape. They described being engaged with the family courts as “like putting the washing machine with all the dirty laundry on an endless cycle” (Participant 8) or “like that Whac-a-Mole game … where you just wait for the next thing to pop up” (Participant 3).
Women were also concerned that their children were powerless in family court processes and had little opportunity to express their views. For example, one described how her children had only been allocated a brief session with a family consultant to talk about their experiences and views about contact with their father (who had perpetrated IPV). She said that for her children, “It must be so distressing to have your whole life being determined by people with very limited insight into their experience” (Participant 3).
Stage 5:
Addressing impacts and making sense
Once women had established some security and safety, they sought help to make sense of what had happened and to address the impacts of the abuse on their own and their children’s mental health. One participant explained that psychological support at this stage was important, because the mental health impacts became more apparent once the physical danger had ended: “The further away from the abuse you get, the more comes up … So, it doesn’t just get easier afterwards. It actually gets harder” (Participant 20).
During this stage, the women spoke to psychologists, psychiatrists, mental health services, GPs and health professionals, DV and sexual assault services, and peer support groups.
“Help to be a more whole person”: Ongoing counselling with someone who understands
Women wanted a counsellor who was knowledgeable about IPV and could help to piece together what had happened to them and why. One woman said:
The counsellor helped me to see why I’ve been making the choices I’ve been making … to understand why my memory was so bad, why I was so teary, why I was so all over the place. (Participant 1)
Women said a compassionate and understanding response was critically important. However, developing the trust required to share personal experiences and address the trauma of the abuse was a process that took time:
You have to go deeper and treat the root of it and being able to provide that safe environment … because. It’s extremely scary to go back to something that was really traumatic for you … [You need] someone that’s not going to quickly judge you or jump to conclusions. (Participant 2)
Considering this, women valued counsellors who could work with them over a considerable period. However, almost all of the participants had struggled to find such a service. Many said DV services could only provide crisis support:
[It’s] almost, unless you’re in real danger, it’s they don’t know what else they can do … [But] it’s not just the emergency or immediate danger … after you separate, [you need] some ongoing support. (Participant 13)
Some participants had accessed free counselling from a sexual assault service. They said this was helpful, but they were only offered a few sessions. For most, the only long-term option to address the trauma they had experienced was to pay for a private psychologist or counsellor. Some felt this was not a realistic choice because the Medicare rebate for counselling did not cover enough of the expense. For others, having the rebate made a huge difference:
I used to pay $120 an hour out of my own pocket to see good therapists, and now I can get the rebate it’s changed my life … It’s helped me be a more whole person, it’s helped me have better relationships, it’s helped me be a good parent. I could not have been a parent without this. (Participant 9)
Participants frequently reported that the psychologists and psychiatrists they saw had lacked expertise in IPV and/or SV. Several spoke of psychologists and counsellors having medicated their symptoms rather than treating the underlying trauma:
I went through all of this horrible process of been told I had a pretty serious mental health condition and thinking that that’s what it was … I lost about 35 kilograms … on lithium, which is what they put me on … I kept screaming at them. I’m like, I’m just trying to sort this crap that has happened to me out. (Participant 3)
Another common perception was that psychologists only offered “textbook” responses:
Counsellors wanted to go straight to some kind of solution, like “Have you been out for a walk to take your mind off it, have you tried breathing and relaxing exercises?” (Participant 15)
Others had found it difficult to find a counsellor who could relate to their cultural background. For instance, one woman born in India said she wished her counsellor had understood that in her culture it was not acceptable to talk about sexual matters, because it made it hard for her to disclose the sexual assaults she had experienced. Another woman was from a Chinese background and said she felt there was a lack of diversity among psychologists:
[Psychology is] a very privileged industry. It’s very white-based, and so … it’s just limiting … I just didn’t feel like any of these people had any real-world experiences with abuse. (Participant 2)
“You’re not alone”: Connecting with other victims and survivors
Another significant theme at this stage was a desire to connect with other victims and survivors of IPV and/or SV. Participants consistently said peer support would assist them to feel that they were “not alone” and were part of a larger community and a shared experience.
Some were able to join support groups facilitated by organisations, while others located support online. They said these were important sources of support and were particularly helpful in normalising and shifting the stigma of what they had experienced. This was illustrated by the following quotes from two participants:
You feel like you’re in a place where you’re safe and people understand what you’ve been through. (Participant 15)
Reading stories of women who had previously gone through it. I was like, “Oh, I’m actually not alone and what I have gone through is actually really terrible and my feelings are valid.” (Participant 30)
Participants from marginalised communities found being able to connect with others who shared similar backgrounds or experiences was particularly helpful. For instance, one participant said engaging with members of the Aboriginal community had “strengthened” her and had been more valuable than using “mainstream” services (Participant 29). Another woman said:
[The support group for victims and survivors of abuse in lesbian relationships] was important, because I felt like I wasn’t the only one … and that I could recover because other people had too … It breaks that silence, it reduces the stigma, it gives you a voice. (Participant 9)
However, several participants felt services did not offer enough peer support opportunities or did not seem to recognise their value. For instance, one said: “There’s only two or three [DV support groups] in the whole [city] … but they’re all packed and always full” (Participant 15). In another woman’s experience (Participant 16), the agency had only provided a group meet-up opportunity for women but had not used trained facilitators to promote deeper engagement: “They fill you up with a lot of junk food and not … really tell you what step you should take or not … really allow you to speak about things.” She was so concerned about the lack of available support that she voluntarily organised a group information session for Spanish-speaking women in her community who were experiencing IPV and/or SV. Another woman (Participant 5) felt agencies were too restrictive in controlling access to support groups, and that women did not want to go throughanother a “taxing, intensive process” to join them. She had also been involved as a volunteer in setting up a peer support group for women that was “open to anybody”. She said: “This is really work that the [DV] industry should be doing, but they’re not, so we’ve found that we need to fill the gap.”
Conclusion
In summary, from our analysis of interviews with 30 women who were victims and survivors of IPV and/or SV, we developed the following five non-linear and overlapping stages in their help-seeking journeys: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; re-establishing independence and safety; and addressing impacts and making sense. Each stage reflected the particular needs women had at different times. Although women described receiving some helpful responses at different stages, overall, many felt that they were “carrying the burden alone” in seeking support and safety for themselves and their children.
In the next section, we return to the qualitative data we collected in our survey and explore issues during the COVID-19 pandemic that victims and survivors experienced when accessing services.
COVID-19 pandemic impacts on access to services
We asked survey participants to provide written responses to a question about whether the COVID-19 pandemic had affected their access to support services. The majority commented that the pandemic had reduced their ability to obtain support, though some had found it made access easier. We identified the following four themes from participants’ responses.
Everywhere is full or closed
Closed doors, long waiting lists and increased demands on services was a significant theme. Many participants spoke of struggling to find any assistance at all from crisis services. For example:
I needed to leave the family home whilst pregnant but because of lockdown, there was nowhere to go. I was unable to access Centrelink as my application was held up due to JobKeeper [government welfare payments introduced during the pandemic]. Once I left it was difficult to navigate and find the right services as it was all via phone. I wasn’t able to get supports for my children.
It took so long to get the worker and support from the family violence agency, they didn’t even follow up how I am going etc., [which] was an unpleasant experience.
Legal processes changed and court hearings were also frequently delayed or deferred. Some women said this had benefitted the perpetrator:
My ex(s) has/have used it to stone wall and manipulate and take advantage of the backlog in the courts.
COVID-19 was used as a reason to prevent me from attending his court appearances for charges against me! I should be allowed to attend! Once again he’s protected, not me.
Several participants commented that the limited and delayed responses from agencies not only made them less safe, but also communicated to them that the service system did not deem their needs to be important.
It is SO hard to get appointments. Everything is full. It made me feel like I didn’t matter.
I escaped during COVID-19 in March 2020. I was not able to get assistance with housing as the shelters were full. Police were very little assistance as they were so busy, and I felt as though my situation was not “bad enough” for anyone to care much.
I have been waiting nearly two years to have security blinds installed on my home which were meant to help make me feel safe … this is how long the VOCAT [Victims of Crime Assistance Tribunal] system and Department of Housing think it’s OK to take when a domestic violence victim is involved.
Participants also expressed distress that the surge in demand for services left their children without access to support:
I spent many days completely at a loss and totally overwhelmed that I could not secure support for my kids when I first left because all service providers were full.
Few opportunities for private conversations
The increased presence of partners at home was a major barrier to seeking support for many women. Many struggled to find a way to contact services without their partner knowing:
Lockdown is hell. There is no way to find supports when you’re stuck with the person all of the time.
It was very lonely and could only access [services] when my now ex-husband left or if I went for a walk.
It has been difficult to privately talk to professionals without the partner being suspicious or able to overhear the conversation.
I had to pretend to go shopping or something to have Zoom counselling inside of the car.
Having children constantly present due to the requirement that they be schooled at home also made it challenging to reach out for support:
I’m at home with three small children. COVID-19 severely limits me having the children somewhere else so I can access services.
You don’t want your children to overhear what you are saying and there is no-where you can go to speak about it.
Engagement was less personal
A frequent comment was that online or phone contact felt “less personal” than face-to-face contact, and it was harder to open up to the service provider. Participants also expressed fears that sessions could be recorded or that others in the household may overhear:
Phone sessions [are] not the same because I’m not in my safe space in her office to really talk.
It’s very hard to talk to CASA [Centre Against Sexual Assault] on the phone instead of mentally preparing yourself as you would when speaking in person. I don’t always know what to even say.
The lack of continuity of care when using telehealth was another source of frustration:
All sterile over the phone, not always the same person so you’re forced to retell your story again and again. They call you on private numbers which a lot of abused women don’t answer for fear of who it is.
Further, it was difficult to engage children in counselling or legal processes via the phone or online:
My communication with support services was all done via telephone. I feel that it would have been more personal if we were able to meet the case manager/psychologist/ legal representatives in person, especially for children who interact/communicate better in person.
Current face to face restrictions are preventing me from accessing sessions for my kids in one on one and as a family (without perpetrator) as online sessions are just not effective with kids.
Participants also encountered problems in relation to court proceedings. Some reported that perpetrators claimed to have internet access issues, which was a tactic to delay court hearings. Other participants felt the lack of face-to-face contact disadvantaged them in court:
The magistrate/judge doesn’t get to see us in person, see the body language and other interactions that only happen in a face-to-face setting – all of which help to demonstrate the character of my ex-partner and the way he is towards me.
Greater flexibility and accessibility
On the other hand, a considerable number of participants suggested that accessing support was easier during the pandemic due to services being delivered online or via phone. Not having to attend in-person sessions saved time and money (as one said, “less expense involved, no driving/ parking tickets!”) and they could access service providers from outside of their local area or after hours:
[Services are] more accessible, especially when you have young children and can have a counselling session when they are asleep.
I live in a regional area where access to psychologists is limited, and they are mostly in my professional network. COVID-19 meant I could access a psychologist via telehealth.
[Access to services] has been better because I was depressed and sometimes would think twice for the travel to the clinic. Now it’s more convenient.
Some participants said they appreciated being able to access Medicare-funded telehealth counselling, which was a measure introduced by the Federal Government to address the mental health impacts of the pandemic.
Summary
This section overviewed the help-seeking strategies of victim and survivor participants. It was clear from our survey that they most often sought help first from friends and family, followed by health practitioners. Aboriginal and/or Torres Strait Islander women, those who had difficulty managing on their available income, and women aged between 25 and 45 years used informal and formal support more than other women. However, younger women were more likely than others to seek help from friends and family and tended not to seek help from specialist domestic violence or sexual assault services; similarly, migrant women less often sought help from specialist services. Barriers that affected help-seeking included shame and a lack of awareness of services that could help or a perception that the professional would not understand them. Concerns about confidentiality were also important barriers. Almost half of survey participants said that at times theywere unable to get the help they needed, and this was primarily due to a difficulty understanding the professional, a lack of available appointments or the cost of services. Participants’ perceptions of the helpfulness of formal service providers were mixed, though overall more than half rated the responses they received as helpful or very helpful.
Our interviews with 30 victims and survivors provided detailed data on their experiences of help-seeking and how their support needs changed over time. Our analysis showed that while most received valuable responses at different stages of their help-seeking journeys, overall, many felt alone in carrying the burden of addressing the IPV and/or SV. Participants often found that there was little ongoing support or material assistance available, with service providers being overburdened or not understanding their needs. The challenges that victims and survivors faced did not end once they had gotten out of the abusive relationship, with many being subjected to ongoing stalking and/or abuse via the legal system and child contact. Regardless of whether the abuse had ended or continued, most found rebuilding a sense of self and dealing with the traumatic impacts of the abuse on themselves and their children was a difficult and long-term process. However,their ability to recover was hindered by the lack of accessible counselling options and opportunities to connect with other survivors.
Data from our survey indicated that these problems were exacerbated during the pandemic. Many found it harder to access services, though some appreciated the availability of telehealth or online services as they afforded greater flexibility in accessing support.
In the next section we provide an overview of women’s support needs from services and from their family and friends.
3. Support needs of victims and survivors
This section integrates the quantitative and qualitative data to overview what victim and survivor participants were looking for in a service.
What do victims and survivors value in a service?
There was broad agreement among victim and survivor participants about what they valued in a service, and this was usually about how the professional made them feel (Table 17). Victim and survivor participants most valued the receipt of emotional support, including feeling listened to (91.7%); having someone to talk to (90.4%); and not feeling judged or put down (86.9%).
Table 17: Proportion of women who have experienced IPV and/or SV and what they value most in a service (n=688)
Service values
n (%)
Emotional support
672 (97.7)
Feeling listened to
631 (91.7)
Having someone to talk to
622 (90.4)
Not feeling judged or put down
598 (86.9)
Knowing that my story would be held in confidence by professional
594 (86.3)
The professional being interested in who I was as a person
564 (82)
Practical support
642 (93.3)
Given practical information about safety
593 (86.2)
Learning new ways to escape violence
534 (77.6)
Material support (e.g. getting access to accommodation)
495 (71.9)
Professional competency
596 (86.6)
The expertise of the professional
596 (86.6)
Notes:
Values are numbers (percentages) unless otherwise stated .
Denominators vary due to missing responses; base = all participants who responded to survey item.
239 participants omitted as they had never sought advice or support.
Expectations of services
The qualitative data we collected from our survey provides more descriptive data on what participants expected and needed from service providers. We asked women survey participants to provide written responses to two questions addressing their expectations from services. The first question asked: “If you think about your partner’s/ex-partner’s behaviours towards you, what do you think your greatest need is from a service or professional?” The second question asked them to complete the sentence “I wish that service providers …” We analysed a selection of their responses to each of these two questions and identified the following five themes, which describe what women victims and survivors need and want from services.
Take me seriously
A strong theme within the data was that women wanted service providers to take their experiences seriously. Women overwhelmingly wanted services to listen and for practitioners to believe them.
My greatest need is for services or professionals … to sit and listen. I can scream my problems from the roof top [and] get nowhere.
To be heard and acknowledged [is my greatest need]. To be believed. For them to tell you what they can offer/explain how they can help or support you rather than you having to request help without knowing what type of help is offered.
[My greatest need is] being believed. Having the police behave professionally and take the assault seriously.
For women who had experienced abuse from an intimate partner, it was important to receive reassurance that the abuse was not acceptable and that they were not responsible for their partner’s behaviour. Such responses helped to affirm that they were not irrational, crazy, exaggerating or imagining things.
[I need] someone to tell me that I am not crazy, and that this is not the way I should be treated.
[I need] validation that he is the problem not me.
[I need] reassurance that the events were unsafe and inappropriate and that the emotional damage is warranted. Reminder that I’m not weak or dramatic.
Help at the time when I need it
A significant theme was for services to be adequately resourced so they could respond when women needed them. Participants’ comments consistently reflected a perception that their support needs were not being fulfilled, with a mismatch between what they wanted and what was offered. A lack of accessibility and availability was one aspect that many women spoke about. They described encountering long waiting lists and limited availability for appointments when trying to access services:
I wish services helped me when I needed them and not months later and that I didn’t have to struggle so hard to find any help at all.
I wish service providers had shorter waiting times …
Participants wanted service providers to spend more time with them, so they could more carefully listen and explore their experiences and needs:
I wish service providers were more accessible and were able to have longer sessions, as it is very hard for me to open up. It takes a long time for me to be able to get the words out.
I wish service providers would take the time to listen rather than just offering up solution.
Many mentioned significant cost-barriers and a wish for more affordable therapeutic or legal services:
I wish service providers were free. I can’t afford to see my therapist.
I wish they could be available when I needed them and that they did not cost so much. I tried a psychologist once but even with my mental health plan it still cost $125 a session. I don’t have that kind of money.
Follow up and follow through
Many of the participants lamented the short-term and transient nature of most of the available service provision. Women felt that they had to contact multiple agencies to find assistance and found it difficult having to repeatedly tell their story. For example, one said, “I wish service providers provided actual practical assistance and stopped referring [me] to the next person and the next person.” They also said services were often not proactive about following up with them after, or between appointments. As one participant stated, “I wish service providers kept checking up on me.” Another similarly valued “consistency, checking in and actually following through”.
Instead, participants wished for enduring support and case management, preferably with someone to help them navigate the legal and service system in an ongoing way. For women who had experienced IPV and/or SV, they wanted to continue to receive support even after an abusive relationship had ended.
We need to have a support network to assist DV victims from the get-go – help with reporting, help with getting an intervention order … Someone needs to take the victim though the whole system.
I wish service providers would be more emotionally supportive with ongoing counselling/referrals once a victim leaves the relationship.
Ongoing specialist counselling to help manage both the trauma from past events and living with the continued risk.
Recognise me as an individual person
Women wanted services to better understand the complexity of their experiences and recognise that violence affects everyone differently. In the context of IPV and/or SV, participants wanted practitioners to improve their recognition of non-physical forms of abuse, including manipulative tactics used after separation:
I wish service providers realised more the hell of coercive control – that even in separation from the ex you are still wholly entrapped if they have access to your children.
I wish service providers had clear training on how to recognise controlling behaviour as the beginning of abusive cycles and the impacts it has on people.
Linked with this was a wish for greater empathy and understanding of how different victims and survivors respond to IPV and/or SV. For example, women wanted services to understand that not every victim and survivor can or wants to leave the relationship:
I wish service providers would not blame me for staying.
I wish service providers understood that not everybody wishes to uproot their lives and leave. Not everybody (especially older women) wants to risk starting again financially or be put in a vulnerable position – going from frying pan to fire – not having sufficient income, no superannuation or savings to start again.
Participants across the sample also wanted practitioners to avoid relying on stereotypes and assumptions and to better understand how abuse and violence affects women with different backgrounds, characteristics or circumstances:
I wish service providers would be less judgemental and factor in cultural differences.
I wish service providers knew that abuse happens to smart educated women too – I am a doctor.
I wish service providers were more accessible for LGBTIQ people experiencing violence.
I wish service providers would treat every client as a human … each client’s needs are different and even vulnerable, uneducated women are intellectual and deserve respect and for their voices to be heard, even when that takes longer than their allocated time.
A need for better access to services was frequently mentioned by victims and survivors with disability, those in rural or regional areas and those who spoke languages other than English. For instance:
I wish service providers can understand me better and if could, provide service in my first language.
I wish service providers could have more services for people with a disability and understand the barriers of people [with] disabilities needing to escape domestic violence.
Finally, women highlighted that the type of support could also vary from person to person. For instance, where some women wanted emotional support, counselling and someone to listen, others wanted more practical help with housing, finances and legal assistance:
I wish service providers could help me with somewhere to go.
I wish service providers could offer REAL assistance for everyday needs.
Make them stop
The final theme was a wish for services to take more action to address the perpetrator’s abusive behaviour. Participants mentioned both legal and police action, as well as therapeutic responses to promote behaviour change.
I wish service providers did more to protect and also address the perpetrators more instead of putting it all onto the victim.
I wish service providers … could do more legally, that they could have removed my partner.
I wish service providers stepped in and provided intensive and REAL support and rehabilitation for changing the negative behaviours … immediately.
Women wanted services to place greater responsibility and accountability onto the perpetrator. They wanted systems to prioritise and foreground their voices as victims and survivors rather than allowing the perpetrator’s voice to “dominate and control the narrative”.
I need the legal system to stop protecting abusers, giving them another platform to continue their abuse and drag out the legal process adding costs and stresses to the victim … He continues to gaslight, stalk, lie, abuse – all in a way that is acceptable to the courts.
[I need] someone to make him stop. To protect the kids and I. To take action against him.
Immediate action for them to tell the police, so his behaviour will no longer be tolerated by anyone.
The next section highlights the role of informal help.
Role of family and friends
The following section discusses our analysis of qualitative data from victims’ and survivors’ responses to two survey questions: “I wish that my family …” and “I wish that my friends …” Our analysis identified that “be on my side” was the central theme in women’s wishes regarding the role of their family and friends. Within this theme there were two sub-themes: “stick by me”, which was frequently connected to the role of friends; and “speak up, step up and step in”, which was mainly associated with the role of family members.
Be on my side
The main theme evident in women’s responses was a wish for family and friends to be “on their side” by supporting them and their view of the situation. This theme was evident in comments about wanting family and friends to “stand by me”, “back me”, and be “loyal” or “there for me”. Participants also gave examples of the things family and friends did that did not demonstrate being “on their side”. For instance, one said:
I wish that my family would be on my side and ask if I’m ok for once. Be there for me. Check on my mental health instead of blaming me for all that’s happened to me.
An important aspect of this theme was family and friends listening to them, believing them and understanding their perspective, rather than taking the perspective of the perpetrator. Participants wanted family and friends to see through the perpetrator and to understand what they were really like:
I wish that my family believed me … They found it easier to believe that I was lying rather than he was capable of the abusive behaviour.
I wish my family could see behind the mask of my partner.
I wish my friends didn’t think my husband was so amazing as he is in public.
Victims and survivors also wanted family and friends to try to understand their responses to the abuse, including the challenges they faced in leaving the perpetrator and managing the long-term impacts of the abuse. For instance:
I wish my family would understand why I have kept going back.
I wish my family could understand why I react the way I do and what might be going on behind closed doors even if I can’t tell them.
I wish that my family would understand that you don’t just “snap out” of trauma.
They also frequently expressed a wish that friends and family understood why it was difficult for them to stay in touch:
I wish my friends could be aware what my life is like. I’m sure they would then understand my huge periods of non-contact.
Participants repeatedly mentioned a wish not to be judged by friends and family. Concerns about judgement were typically focused on a perception that they had been “weak”, “stupid”, a “lost cause” or “a victim” for having stayed in the abusive relationship. For example, one said: “I wish my friends wouldn’t think I’m stupid for giving lots of chances”.
Also associated with having family and friends “on their side” was a wish not to be blamed for their partner’s abusive behaviour. It was notable that participants’ comments about receiving angry or blaming reactions tended to be connected to family members. This was evident in comments such as:
I wish my family would let go of their anger in my marrying that person. I feel doubly punished.
I wish that my family would stop thinking I provoked him in some way.
Victims and survivors also spoke of family members being disappointed in them or seeing them as a “failure”. For example, one said: “I wish that my family would stop caring about what other people think (other relatives or friends) and make me feel ashamed for what I went through.”
Stick by me
The sub-theme “stick by me” was linked to the responses of friends. Many participants expressed a wish that their friends would maintain a strong friendship with them; for example, one said, “I wish my friends would keep always being there for me and me for them.” However, participants’ responses suggested that damaged friendships and the loss of friends was a common experience. A frequent comment was that they wished their friends “didn’t give up” on, “cut off” or “abandon” them. For some, the perpetrator appeared to have directly undermined the friendship:
I wish friends hadn’t believed his lies. I lost all of them.
I wish that my friends hadn’t been removed from my life by his control and isolation.
I wish my friends didn’t believe the ex’s smear campaign.
For others, the loss of friendships occurred because their friends were upset with them for staying in the relationship:
I wish my friends didn’t abandon me as means to show disapproval for the relationship because it made me believe that I was crazy.
I wish friends didn’t judge me or ditch me when I returned back to the perpetrator.
I wish friends didn’t just run away because they “couldn’t stand watching this”.
Victims and survivors also wished their friends would be proactive in maintaining the friendship and would make an effort to reach out to them:
I wish my friends checked in on me more, instead of just waiting for me to call them.
I wish friends had regular scheduled catch ups or social events to maintain contact.
I wish friends were able to spend more time with me when I really needed it, but they were busy with their own families.
Step up, speak up and step in
The second sub-theme mainly related to victims’ and survivors’ family members and a wish that they could play an active role in looking after them. This theme was reflected in participants’ comments about wanting family members to “step up” and help with everyday tasks, finances or a place to stay:
I wish that my family [gave] practical support in managing day to day life, like having help with household tasks like cooking and cleaning, picking up kids from school, so we can focus on sorting out legal issues.
I wish that my family was rich (!) so we could escape and not need his child support.
I wish that my family would have let me stay with them and report everything to police and take a AVO against him for my safety.
Participants also expected that they should be able to rely on their family to act in their best interests. Several said they had wanted family members to raise their concerns with them when they noticed signs of abuse:
I wish that my family spoke up about how they felt about him.
I wish that my family had helped me earlier and been stronger in telling me things weren’t right and that I deserved better.
They also wished their family members were able to step in to protect them:
I wish that my family could make him leave me alone.
I wish that my family had been more honest and stopped me from getting married.
Speaking up and stepping in was also a response women wanted from their friends when they witnessed abusive behaviour. Several said they wished that friends would have called out abusive behaviour when they were bystanders to it. For example:
I wish that my friends pulled my partner up on their abusive behaviour … especially if present when it occurred.
Summary
In summary, victim and survivor survey participants wanted emotional and practical support from professionals who had expertise in the area. Our analysis of qualitative survey data found that they wanted formal service providers to take them seriously; help them at a time when they needed it; follow up and recognise their individual experiences; and take more action to make the perpetrator stop the abuse. In relation to informal support, they wanted their family and friends to be on their side, by sticking by them and stepping up through providing practical assistance, and to speak up when they witnessed abusive behaviour. The next part turns to the voices of people who use IPV and/or SV.
Part D:
Key findings –
The experiences of people who use violence
“It’s very hard to understand what behaviours are abusive/wrong, I often can’t understand why I’m wrong for a long time or until an event [occurs] after which it becomes clear.”
(Survey participant)
Introduction
This part is divided into three sections that integrate quantitative and qualitative findings from the perspective of people who use IPV and/or SV. The first section overviews participant characteristics, and the nature, patterns and associations of use of IPV and/or SV, including the effects of the COVID-19 pandemic on experiences. This is followed by a section on help-seeking and service needs, including the effects of the COVID-19 pandemic. The final section describes the support needs of people who use IPV and/or SV.
1. Patterns and associations of use of IPV and/or SV
Sociodemographic characteristics
Overall, participants who used violence were generally representative of the Australian population except for a few specific demographic areas of note. The majority of participants (93.1%) were men, 5.7 per cent were women, 0.9 per cent were non-binary and 0.4 per cent preferred to self-describe. Nearly two thirds of participants in this study were aged between 18 and 39 years, a higher proportion compared to the general Australian population (Table 18). Approximately double the percentage of Victorian residents responded to this survey compared to the general population. Similar to population figures, approximately three quarters (74%) of the people in this study were born in Australia and lived in a metropolitan area (78.7%). Of those participants who were in arelationship at the time of the survey, the majority had a female partner (94.4%), were married (38.1%) and had children at home (69.2%; Table 18).
The proportion of participants identifying as Aboriginal and/or Torres Strait Islander (10.1%) or who did not complete Year 12 (19.6%) was higher than in the general community. Approximately half (49.7%) of participants had completed a degree or higher degree, which was also higher than the general community (28.3%). Most participants were employed (67.8%), although many (39%) had difficulty managing on their available income some or all of the time, which was disproportionally high compared to the general community.
Table 18: Demographic characteristics of participants who completed survey about use of violence and abuse compared to the broader Australian population (N=563)
Age (years; n=562)
Characteristic
All participants n (%)
Australian population %a
18–29
194 (34.5)
19.8
30–39
158 (28.1)
14.7
40–49
78 (13.9)
12.8
50–59
132 (23.5)
12.2
Current Australian state of residence
Characteristic
All participants n (%)
Australian population %a
Australian Capital Territory
9 (1.6)
1
New South Wales
128 (22.8)
15.1
Northern Territory
1 (0.2)
0.5
Queensland
82 (14.6)
9.5
South Australia
26 (4.6)
3.7
Tasmania
6 (1.1)
1.2
Victoria
285 (50.7)
11.5
Western Australia
25 (4.4)
4.6
Lives in metropolitan area
441 (78.7)
71
In current relationship (≥1 month length)
320 (57.2)
**
Lives with partner
332 (56)
45
Not living with partner (male/female/spouse)
231 (41)
24
Sex of current partner (n=320)b
Characteristic
All participants n (%)
Australian population %a
Female
302 (94.4)
63.8
Non-binary
1 (0.3)
17.3
Prefer not to say
16 (5)
**
Sexual orientation (n=547)
Characteristic
All participants n (%)
Australian population %a
Heterosexual
457 (83.6)
92.8
Bisexual
46 (8.4)
0.8
Queer
8 (1.5)
**
Asexual
2 (0.4)
**
Self-described
7 (1.3)
**
Not sure
22 (4)
1
Marital status
Characteristic
All participants n (%)
Australian population %a
Never married
275 (48.9)
32
Married
214 (38.1)
30.6
Separated but not divorced
36 (6.4)
2.9
Divorced
33 (5.9)
7
Widowed
4 (0.7)
6
Children
240 (42.7)
43
1+ children living at home
166 (69.2)
49
Aboriginal and/or Torres Strait Islander
57 (10.1)
3.2
Born outside Australia
146 (26)
30
First language not English
90 (16)
21
Prior schooling (n=539)
Characteristic
All participants n (%)
Australian population %a
Attended school but finished prior to Year 12
106 (19.6)
10.5
Completed Year 12
436 (80.4)
79
Educational qualification (n=542)
Characteristic
All participants n (%)
Australian population %a
Trade/apprenticeship/diploma
202 (37.5)
32.8
University degree/higher degree
268 (49.7)
24
Employment and income (n=546)
Characteristic
All participants n (%)
Australian population %a
Employed
370 (67.8)
64.1
Not employed
176 (32.2)
5.7
Has difficulty managing on available income
213 (39)
18.7
Health Care Card holder
337 (61.7)
52
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey item.
** Comparable data either not collected or available.
a Population data is weighted proportions from Australian Bureau of Statistics (2020); values are proportion total Australian population.
b Male partner not reported; participants with male partner excluded from survey on IPV against women .
Twelve-month and lifetime experiences of use of violence and abuse
Interpretive note
To understand the experience of people who use violence and abuse, the survey screened participants for behaviours in their relationship using three items relating to feeling concerned about behaviours in a relationship, help-seeking for issues in a relationship and having made a partner feel afraid. These questions were designed to engage people who may not have identified their behaviour using the language of “domestic violence or abuse” but may still have felt worried about their behaviour. Participants could answer with a simple “yes/no” response. Abusive actions and behaviours of participants were measured using the short-form CASr-SF (Ford-Gilboe et al., 2016), altered to ask about behaviours used by participants against a partner, and experiences of child abuse were measured using the ACEs scale (Felitti et al., 1998; see “Methodology” earlier).
It is important to note that while not all participants reported using IPV and/or SV when measured using the CASr-SF (Ford-Gilboe et al., 2016), all participants completed screening questions (see “Methodology” further) indicating that they may have used abuse and violence in a relationship, which established their eligibility for the study. Further, analysis of the violence against women attitudes data indicated differences between all participants and general population attitudes but not meaningful attitudinal differences between people who reported as having used IPV and/or SV on the CASr-SF and those who had not (Table 26).
In analysing participants’ responses in the open-ended questions on the survey, it was evident that many did not see themselves or did not wish to characterise themselves as perpetrators. This was despite them having identified using forms of violent or abusive behaviour in other parts of the survey. For example, one responded by saying: “I am not convinced I am violent or abusive, I am a really good man”, and another said: “I’m not really a violent person by nature but sometimes I just get really angry.” Similarly, other participants rejected the characterisation because they had not used physical aggression. For example, one said: “I [am] mostly not violent, like I don’t hit her, it’s mostly verbal and I’ve tried all I can.” This suggested they did not perceive negative verbal or psychological behaviours to be as serious as physical abuse. Another common response was acknowledging some form of abuse but suggesting its impact was minimal or theirpartner mutually contributed to it. For instance, one participant said: “I’m not sure it can be classified as abuse. If so, it is a mild form of abuse she is willing to tolerate.”
For all of the reasons above, we chose to analyse the whole sample, rather than selecting out only the people who scored on the CASr-SF, and we refer to all participants in this section as “people who have used violence and abuse” (Ford-Gilboe et al., 2016).
Experiences and patterns of using IPV and/or SV in the past 12 months
In the last 12 months, 34.8 per cent of people in this study reported having used violence against a partner or ex-partner (as measured using 15 behaviours on the CASr-SF; Ford-Gilboe et al., 2016). Approximately one in four (26.7%) participants identified that they had made their partner feel afraid of them in the last 12 months, with slightly more than one in five (22.7%) saying their partner was currently afraid of them (Table 19). Approximately half of the participants who reported using any IPV in the last year said this was psychological in nature, while 44.4 per cent was sexual and 42 per cent physical.
Table 19: Proportion of people who had used violence against a partner during the last 12 months
Last 12 months
Types of IPV and/or SV
n (%)
Made partner feel currently afraid (n=427)a
97 (22.7)
Made partner feel afraid in last 12 months (n=491)
131 (26.7)
Used IPV (any; n=490)b
81 (16.5)
Physical
34 (7.1)
Sexual
36 (7.5)
Psychological (including technology-facilitated abuse)
45 (9.5)
Total 12-month made partner feel afraid and/or used violence against them (n=491)
171 (34.8)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed screening items and/or 12-month CASr-SF (Ford-Gilboe et al. 2016).
a 68 participants omitted because they had never been in a relationship longer than one month.
b Participants could belong to more than one CASr-SF category.
Table 20 displays the 12-month frequency of specific acts of abuse that were asked about in the survey. It indicates that the most common acts of IPV and/or SV were harassing one’s partner by phone, text, email or social media; telling one’s partner they were crazy, stupid or not good enough; and trying to convince the family or friends of one’s partner that they were crazy.
Table 20: Of people who had ever used violence, proportion of those who had used each behaviour in the last 12 months
Abusive behaviours
12-month use
n (%)a
Harassed partner by phone, text, email or using social media
74 (60)
Told partner they were crazy, stupid or not good enough
74 (54.4)
Tried to convince partner’s family or friends that they were crazy
29 (53.7)
Blamed a partner for causing their violent behaviour
73 (49.6)
Hit partner with a fist or object, kicked or bit them
21 (47.7)
Made partner perform sex acts that were unwanted
26 (47.3)
Kept partner from seeing or talking to family or friends
14 (46.7)
Forced or tried to force partner to have sex
20 (45.4)
Shook, pushed, grabbed or threw a partner
50 (45)
Choked partner
12 (42.8)
Kept partner from having access to a job, money or financial resources
11 (42.3)
Confined or locked partner in a room or other space
5 (41.7)
Used or threatened to use a knife or gun or other weapon to harm partner
9 (40.9)
Followed partner or hung around outside their home or work
25 (35.2)
Threatened to harm or kill partner or someone close to them
7 (30.4)
Total (one or more abusive behaviours; n=290)b
169 (58.3)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = 12-month proportion of participants who had used corresponding lifetime abusive behaviour measured using CASr-SF (Ford-Gilboe et al. 2016).
a Behaved in this way once or more during last 12 months as a proportion of people who had ever used each behaviour- see Table 22.
b 169/290 people used one or more abusive behaviours in the last 12 months.
Lifetime experiences of using violence and abuse
As above, while everyone who took part in the survey completed screening questions indicating that they may have used abuse and violence in a relationship, which established their eligibility for the study, just over half (58.2%) met the criteria for having used IPV during their adult lifetime on the CASr-SF (Ford-Gilboe et al., 2016). Of these 288 participants, three in four (75.7%) identified that their behaviour had caused their partner to feel afraid of them (Table 21). Approximately one in five (21.6%) participants had used sexual violence against a partner, and 19 had exerted coercion over their partner’s reproductive health and decision-making (4.7%)
Table 21: Proportion of people who have used violence against a partner across the adult lifetime (since the age of
16 years)
People who have used violence
n (%)
Have ever made partner feel afraid (n=495)
218 (44)
Perpetrated IPV (any; n=491)
171 (34.8)
Used SV against a partner or ex-partner (n=490)
106 (21.6)
Total IPV (including fear; n=495)
269 (54.3)
Reproductive coercion (n=490)
23 (4.7)
Total adult lifetime IPV, SV and/or reproductive coercion (n=495)
288 (58.2)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed CASr-SF and other abuse survey items.
Sixty-eight participants omitted because they had never been in a relationship for longer than one month.
The acts of abuse most frequently reported among participants were emotionally abusive and harassing behaviours, including blaming their partner for causing violent behaviour (29.9%); telling their partner they were crazy, stupid or not good enough (27.7%); and harassing their partner by phone, text, email or using social media (25.3%; Table 22).
Table 22: Proportion of people who have used lifetime violence and the type of abusive behaviour used (n=495)
Abusive behaviours
Adult lifetime n (%)
Blamed partner for causing their violent behaviour
147 (29.9)
Told partner they were crazy, stupid or not good enough
136 (27.7)
Harassed partner by phone, text, email or using social media
124 (25.3)
Shook, pushed, grabbed or threw partner
111 (22.6)
Followed partner or hung around outside their home or work
71 (14.5)
Made partner perform sex acts that were unwanted
55 (11.2)
Tried to convince partner’s family or friends that they were crazy
54 (11)
Forced or tried to force partner to have sex
44 (9)
Hit partner with a fist or object, kicked or bit them
44 (9)
Kept partner from seeing or talking to family or friends
30 (6.1)
Choked partner
28 (5.7)
Kept partner from having access to a job, money or financial resources
26 (5.3)
Threatened to harm or kill partner or someone close to them
23 (4.7)
Used or threatened to use a knife or gun or other weapon to harm partner
22 (4.5)
Confined or locked partner in a room or other space
12 (2.4)
Total (one or more abusive behaviours)
290 (59.1)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = adult lifetime proportion of participants who had used lifetime abuse measured using CASr-SF (Ford-Gilboe et al. 2016); maximum missing n=5.
Patterns of abuse and violence by people who use violence
Participants more frequently reported violence against a partner in the last 12 months if they were aged between 25 and 45 years, were Aboriginal and/or Torres Strait Islander, and told us they had difficulty managing on their available income (Table 23). Those same sociodemographic factors were associated with use of violence against a partner over the adult lifetime (since the age of 16 years). Those not living with a partner were under-represented among those who had used violence in the last 12 months. Youth was also associated with under-reporting abuse and violence across the adult lifetime (Table 23).
Table 23: Proportion of people who used violence in the last 12 months and across the adult lifetime with sociodemographic factors
Sociodemographic factors
Use of violence against a partner in last 12 months (n=171)
Use of violence against a partner (since the age of 16 years) (n=269)
All participants (n=562)
171 (34.8)
269 (54.3)
Age (years)
Sociodemographic factors
Use of violence against a partner in last 12 months (n=171)
Use of violence against a partner (since the age of 16 years) (n=269)
Up to 25 years (n=133)
33 (28)
51 (43.2)
25-45 years (n=267)
99 (43.2)
145 (63)
> 45 years (n=162)
39 (27.1)
73 (50)
Aboriginal/Torres Strait Islander (n=53)
29 (54.7)
39 (72.2)
Migrant background (n=152)
44 (33.6)
73 (55.7)
Lives in non-metropolitan location (n=98)
37 (37.8)
60 (61.2)
Attended school but finished prior to Year 12 (n=101)
36 (35.6)
60 (59.4)
No university degree (n=240)
80 (33.3)
132 (55)
No employment (n=160)
57 (35.6)
90 (56.2)
Has difficulty managing on available income (n=200)
77 (38.5)
122 (61)
Health Care Card holder (n=302)
99 (32.8)
163 (54)
Not living with partner (n=206)
58 (28.2)
112 (53.6)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
% = represents the proportion of overall demographic group who have used abuse.
Adverse childhood experiences and use of violence in adulthood
Physical, sexual and/or emotional abuse in childhood had been experienced by approximately one in two (47.6%) participants who had ever used IPV and/or SV (Table 24 and Figure 15). One in three (33.7%) participants had been physically abused or neglected before the age of 15, nearly one in five (17.3%) had been sexually abused and nearly half (47.2%) had been emotionally abused or neglected. Using logistic regression, the predicted odds of reporting the use of violence against a partner in the last 12 months were three times greater if a participant had experienced child abuse (OR 3, 95% CI 2 to 4.5), and 2.7 times greater if the participant had used violence against a partner since they were aged 16 years (OR 2.7 95% CI 1.8 to 3.8). This association betweenchild abuse and the use of IPV and/or SV in adulthood indicates a life course effect of violence in early life on later relationships.
Table 24: Proportion of people who have used violence who have experienced child abuse
Child abuse typea
Before age 15 years
(n=561)
Emotional abuse
210 (37.4)
Emotional neglect
183 (32.6)
Physical neglect
170 (30.4)
Physical abuse
170 (30.3)
Sexual abuse
97 (17.3)
FV against mother growing up
86 (15.3)
Total child abuse
267 (47.6)
Total ACEb score of 4+
153 (27.3)
Total child abuse and/or ACE>4
270 (48.1)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to child abuse survey items.
a Abusive behaviour before the age of 15 years by someone aged 18 plus years.
b ACEs scale (Felitti, 2019) score out of 10; scores 4+ are associated with serious health and risk issues in adulthood (Felitti, 2019).
Figure 15: Proportion of people who had used IPV and/or SV since the age of 16 and/or experienced child abuse before the age of 15 years (n=356)
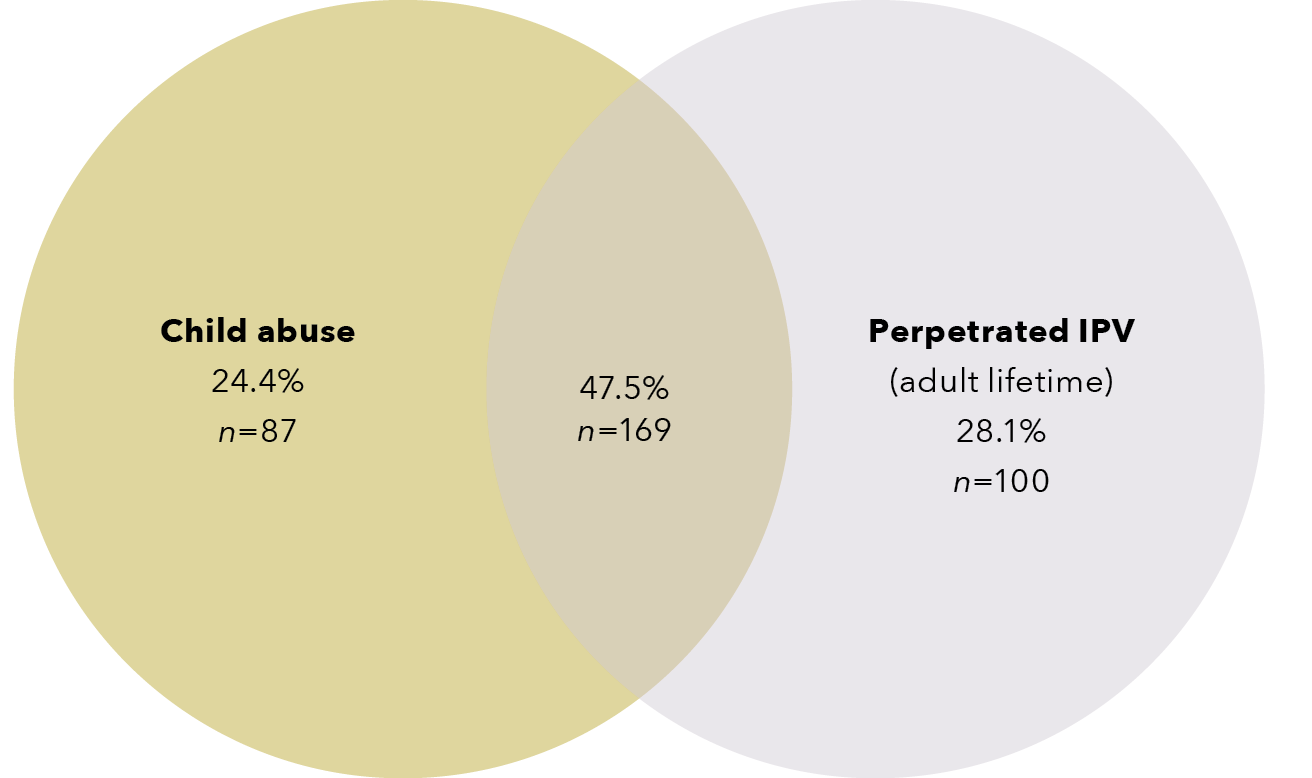
Data table for the figure above:
Category
Percentage
n
Child abuse
24.4%
87
Perpetrated IPV (adult lifetime)
28.1%
100
Child abuse and perpetrated IPV
47.5%
169
In Brief:
Use of violence and abuse findings

Aboriginal and Torres Strait Islander participants, participants aged 25–45 years, and those who had difficulty managing on their available income were over-represented as having used violence in the last 12 month and across the adult lifetime (since 16 years).
Participants who were not living with a partner were less likely to have used violence and abuse in the last 12 months. Younger participants (less than 25 years) were less likely to have used violence and abuse in the last 12 months and across the adult lifetime (since 16 years).

Participants who had experienced child abuse were three times more likely to use violence against a partner in adulthood.
Health experiences of participants who had used violence
Participants who had used violence against a partner in the last 12 months were more likely than those whose IPV and/or SV occurred more than 12 months ago to report poor health and mental health on a range of measures (Table 25). More than half (51.2 to 62.6%) of all participants screened positive for PTSD. Further, between one in four and one in three participants who had used violence and abuse reported poor to fair general health and long-term illness, and met the core criteria for anxiety, depression and/or hazardous alcohol consumption.
Table 25: Proportion of people who use violence and their experience of health and mental health issues, arranged by type of abuse and cumulative abuse
Mental health
Current health issues
All participants
(n=562)
Use of violence against a partner in last 12 months
(n=171)
Use of violence against a partner since the age of 16 years
(n=269)
PTSD
288 (51.2)
107 (62.6)
107 (62.6)
Anxiety
171 (30.4)
63 (36.8)
89 (33.1)
Depression
163 (29)
65 (38)
93 (34.6)
Hazardous alcohol consumption
137 (26.2)
47 (29.4)
71 (28.5)
General health
Current health issues
All participants
Use of violence against a partner in last 12 months
Use of violence against a partner since the age of 16 years
Lives with disability
145 (25.8)
53 (31)
87 (32.3)
Poor to fair self-rated health
118 (21)
47 (27.5)
68 (25.3)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
Attitudes towards violence against women
A higher proportion of participants in this study demonstrated attitudes that support violence against women when compared to the Australian community (using the National Community Attitudes towards Violence against Women Survey [NCAS] items; Webster et al., 2018). Across all 10 violence against women attitude items, a higher proportion of survey participants agreed with each statement when compared to the national Australian population (Table 26). Moreover, participants who met the criterion on the CASr-SF for having used IPV and/or SV displayed the highest proportion of attitudes that support violence against women. For example, 72 per cent agreed with the statement “Many women mistakenlyinterpret innocent remarks or acts as being sexist”, compared to 50 per cent of the general population; 56.9 per cent agreed that “Men should take control in relationships and be the head of the household”, compared to 16 per cent of the general population; and 28.5 per cent thought that “It is embarrassing for a man to have a job that is usually filled by a woman”, compared to just 6 per cent of the general Australian population (Table 26).
Table 26: Proportion of people who use violence who hold attitudes that support violence against women compared to the Australian population
Attitude
Participants who agreed with statement
(n=521)
Participants who had used lifetime IPV and/or SVa who agreed with statement
(n=246)
Australian comparisonb
N=17,500
Many women mistakenly interpret innocent remarks or acts as being sexist
358 (68.7)
177 (72)
50%
Many women exaggerate how unequally women are treated in Australia
334 (64.1)
162 (65.8)
40%
Many women fail to fully appreciate all that men do for them
310 (59.5)
155 (63)
36%
Women prefer a man to be in charge of the relationship
305 (58.5)
146 (59.3)
25%
Men should take control in relationships and be the head of the household
288 (55.3)
140 (56.9)
16%
On the whole, men make better political leaders than women
240 (46.1)
115 (46.7)
14%
In the workplace, men generally make more capable bosses than women
244 (46.8)
114 (46.3)
14%
I think there’s no harm in men making sexist jokes about women when they are among their male friends
210 (40.3)
118 (48)
24%
When a couple start dating, the woman should not be the one to initiate sex
201 (38.6)
94 (38.2)
10%
I think it is embarrassing for a man to have a job that is usually filled by a woman.
132 (25.3)
70 (28.5)
6%
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed the NCAS (Webster et al., 2018).
a Scored using the CASr-SF (Ford-Gilboe et al., 2016).
b Webster et al., 2018.
In Brief
The health and attitudes of participants who had used violence and abuse

Participants who had used violence against a partner recently were more likely than those whose IPV occurred longer than 12 months ago to report poor physical and mental health.

On every attitudinal measure, a higher proportion of participants indicated attitudes that support violence against women compared to the general Australian community.
This section has provided an overview of the patterns of abuse and violence used by survey participants, and how these were associated with their sociodemographic characteristics. In the next section we examine qualitative survey data on the impact of the COVID-19 pandemic on the use of IPV and/or SV.
The impact of the COVID-19 pandemic on IPV and/or SV
Survey participants who had used abuse or violence were asked to provide written responses to the question: “How have your experiences in your adult intimate relationships changed during COVID-19 isolation?” From our question, it was difficult to determine whether participants were referring to an abusive relationship or a non-abusive one. Consequently, we focused on comments that alluded to the participant’s behaviour towards a partner/ex-partner. In response to our question, most simply commented “no” or “no change”. However, others noticed that the pandemic had influenced their relationships and behaviour towards their partner.
Increased pressure triggered poor behaviour
While some participants felt the pandemic had been a time of personal growth, others admitted it had triggered problematic behaviour towards their partner. Many suggested this was due to having had less space and time away from their partner. For instance, several survey participants who identified that they had been physically aggressive towards a partner said that they had found it harder to control their emotions during the pandemic:
Worse – she’s in my face all the time and I get angrier.
More time together, less opportunity for space when either one of us is upset or feeling overwhelmed.
[It has been] harder to keep my temper in check.
Others suggested their poor behaviour had resulted from increased mental distress and financial pressures:
Increased isolation and severe stress due to finances has triggered a lot of my behaviours. Severe mental health deterioration for both my partner and I, lack of access to services.
Heightened feelings of depression and anxiety causing me to take it out on my partner.
Several indicated that the restrictions on how often they could see their partner created tensions in the relationship. Some suggested being unable to meet up with their partner caused problems in communicating effectively, which led to increased stress or feeling more insecure or worried about the relationship.
The pandemic provided time and space for self-reflection
A strong theme was that the pandemic prompted positive change. Many said the isolation afforded them more time to reflect on their problematic behaviour and the personal issues that may contribute to it. This was evident in the following comments:
Living alone during the COVID-19 isolation periods last year was immensely beneficial. I was already changing a number of things in my life and coming out of a hugely destructive working environment, so was already making the types of active changes to make myself a better partner. However, during the isolation period, I found myself actively assessing my life, how I act, and who I want to be. As an extrovert, I believe this may have been the first period in my entire life that I was actually able to engage in such reflection, and I believe it has sped my transformation.
My experiences have changed a lot. I spent countless hours thinking on how I can be a better husband. I spent hours thinking of how I can provide for my kids. I spent hours thinking on how I can talk to my wife and let her know how much I love her.
I’ve been actively avoiding intimate relationships so I could work on my own mental health and drug dependency issues.
Others said that spending more time in contact with a partner during COVID-related isolation had prompted self-reflection and change. For example, one participant who identified in the survey that she had been physically aggressive and had excessively contacted her partner and kept him from family and friends responded:
Firstly, I found that the relationship I did enter became very intense very quickly due to the fact we were legally only allowed to visit each other and no one else. I was in a short-lived relationship during COVID-19 which caused me to deeply self-reflect and take a break from dating to work on myself. COVID-19 has been a time of personal growth for me.
Some felt the reduced stress and pressure during isolation had enabled them to have a greater emotional control:
Surprisingly, our experiences have been better during isolation. A lot of my anxiety comes from being in public spaces. Being isolated has been a short-term fix for most of my anxiety issues and in turn I have had far better control on my frustration levels and reduced the amount of drinking I have had.
Summary
Our analysis of the survey data from over 500 participants (predominantly male) found that a third indicated they had been abusive or violent to a partner or ex-partner in the past 12 months, and more than half reported having used IPV and/or SV during their adult lifetime. Emotionally abusive or harassing behaviours were the most commonly reported forms of abuse used. Aboriginal and Torres Strait Islander participants and those who had difficulty managing on their available income were over-represented among those who had used violence or abuse, while participants aged under 25 were under-represented. Almost half of participants who used IPV and/or SV in the last 12 months had experienced abuse in childhood. Those who had used IPV and/or SV were also more likely than other participants to report having poor physical and mental health. Survey data indicated that a higher proportion of participants had attitudes that support violence against womencompared to the general Australian community. Our analysis of qualitative data from the survey suggested that for many, their use of IPV and/or SV escalated during the COVID-19 pandemic; however, some said the isolation allowed them more time to reflect on their problematic behaviour.
The next section explores the help-seeking experiences of people who use IPV and/or SV.
2. Help-seeking experiences of people who use IPV and/or SV
This section provides an overview of the help-seeking experiences of people who use IPV and/or SV, based on the survey data. In particular, it details from whom they sought help; how helpful it was; and the barriers to seeking help. The section also draws on the interview data to explore how people who use violence engage on journeys to seek help and the open-ended questions in the surveys to understand how participants felt the COVID-19 pandemic affected help-seeking. Both informal and formal services were included, ranging from all sectors that could come in contact with people who use violence or abuse. It should be remembered that half of the participants were from Victoria, a state where there has been a marked degree of reform across the system in the last five years.
Help-seeking experiences
Most participants (73.5%) had sought formal or informal advice or support from someone about their behaviour towards a partner (Table 27). Most often, the person to whom a participant spoke was a friend (45.4%), partner (31.7%) or family member (27.7%). Among the formal services that participants accessed for assistance, health services were the most frequently utilised (33.3%), followed by specialist family violence services (10.8%), and justice services (6.3%). More often than not, participants rated the service they had accessed as helpful (71.8%). Some services were deemed more helpful than others, with psychologists or counsellors (84.1%), religious people (81.8%) and family therapists (80.8%) the most positively rated.
Table 27: Proportion of people who have used abuse and violence, sources of help-seeking and perceived helpfulness
Service/resource
Sought support
(n=555)
Found support helpfula
Any source of help:
408 (73.5)
72.3b
Family and friends (total)
327 (58.9)
74.3c
Friend/s
252 (45.4)
194 (77)
Partner
176 (31.7)
134 (76.1)
Family member/s
154 (27.7)
111 (72.1)
Formal sources of support:
229 (41.3)
71.8
Health services (total)
185 (33.3)
74
Psychologist/counsellor
138 (24.9)
116 (84.1)
Family therapist
26 (4.7)
21 (80.8)
Nurse
12 (2.2)
9 (75)
General practitioner
58 (10.4)
40 (70.2)
Social worker (hospital, community health)
13 (2.3)
9 (69.2)
Alcohol or drug worker
19 (3.4)
11 (64.7)
Specialist services (total)
60 (10.8)
73.2
Men’s referral service
19 (3.4)
15 (78.9)
Behaviour change program
18 (3.2)
14 (77.8)
Domestic or family violence service
27 (4.9)
17 (63)
Telephone helpline (e.g. Lifeline, 1800RESPECT)
19 (3.4)
N/A
MensLine
15 (2.7)
N/A
Justice services (total)
35 (6.3)
61.5
Legal service (e.g. solicitor or legal aid)
13 (2.3)
10 (76.9)
Police
26 (4.7)
12 (46.1)
Community – other (total)
33 (5.9)
78.4
Priest/minister/rabbi or any other religious person
22 (4)
18 (81.8)
Work colleague or boss
12 (2.2)
9 (75)
Housing and financial services (total)
6 (1.1)
**
Financial service (e.g. Centrelink)
5 (0.9)
4 (**)
Housing service
1 (0.2)
1 (**)
Did not seek advice or support
147 (26.5)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to opt in survey item about having spoken to someone about behaviour in relationship.
** Small cell count prevented analysis.
a Helpful/very helpful (median).
b Total number of participants who had accessed 1+ service (average proportion of all participants who found service/s helpful).
c Category proportions are an average of helpfulness across the category.
Some groups of participants accessed services for advice and support more or less frequently than others (Table 28). While interpretive caution is required due to small cell counts in some cases, some between-group differences are still important to highlight. Aboriginal and Torres Strait Islander participants sought help more than other participants, especially among family and friends, specialist services and other community services. Participants who had attended school but left prior to Year 12 and those who had difficulty managing on their available income were also more frequent service-users. Migrant participants were less likely than other participants to have accessed services (Table 28).
Table 28: Proportion of help-seeking by people from diverse backgrounds
Age (years)
Demographic
Community – family and friends
n (%)
Health services
n (%)
Specialist services
n (%)
Justice services
n (%)
Community – other
n (%)
Did not seek advice or support
n (%)
All participants (n=562)
327 (58.9)
185 (33.3)
60 (10.8)
35 (6.3)
33 (5.9)
147 (26.5)
Up to 25 (n=133)
100 (75.2)
20 (15)
5 (3.8)
3 (2.3)
2 (1.5)
30 (22.6)
25–45 (n=267)
160 (60.2)
96 (36.1)
35 (13.2)
17 (6.4)
21 (7.9)
64 (24.1)
> 45 (n=162)
67 (42.9)
69 (44.2)
20 (12.8)
15 (9.6)
10 (6.4)
53 (34)
Aboriginal and/or Torres Strait Islander (n=53)
40 (71.4)
21 (37.5)
14 (25)
6 (10.7)
10 (17.9)
13 (23.2)
Migrant background (n=152)
91 (60.7)
39 (26)
9 (6)
4 (2.7)
7 (4.7)
42 (28)
Lives in non-metropolitan location (n=98)
61 (51.7)
48 (40.7)
16 (13.6)
10 (8.5)
9 (7.6)
32 (27.1)
Attended school but finished prior to Year 12 (n=101)
53 (50)
45 (42.4)
20 (18.9)
11 (10.4)
5 (4.7)
29 (27.4)
No university degree (n=240)
154 (56.8)
95 (35.1)
33 (12.2)
20 (7.4)
17 (6.3)
73 (26.9)
No employment (n=160)
108 (61.4)
63 (35.8)
18 (10.2)
17 (9.7)
11 (6.2)
44 (25)
Has difficulty managing on available income (n=200)
131 (61.5)
84 (39.4)
39 (11.6)
23 (10.8)
15 (7)
47 (22.1)
Health Care Card holder (n=302)
212 (62.9)
125 (37.1)
39 (11.6)
22 (6.5)
18 (5.3)
82 (24.3)
Not living with partner (n=206)
151 (66.8)
73 (32.3)
31 (13.7)
19 (8.4)
13 (5.7)
45 (19.9)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
The proportion (%) in this table represents the proportion of overall demographic group who have accessed help by category.
In brief:
Help-seeking of participants who had used violence and abuse

People whose income did not cover their needs and people aged 45 years and older accessed health services more than others; participants who left high school prior to Year 12 also accessed specialised services more than others; Aboriginal and Torres Strait Islander participants accessed both types of services more than others as well as seeking help from family/friends and other community services.

Migrant participants less often sought support from services compared to others.
Barriers to help-seeking
Participants who had used IPV and/or SV identified barriers to seeking help for their behaviour (Table 29). The most named barriers were as follows: feeling ashamed (41.4%); belief that violence is a normal part of a relationship (34.7%); access challenges (34.7%); concerns about confidentiality (29.3%); lack of awareness of services (23.9%); communication issues (22.1%); and not having the time to talk to someone (15.9%).
Table 29: Proportion of people who use violence who identify barriers to professional help-seeking (n=553)
Barriera
n (%)
Shame
229 (41.4)
I feel too ashamed to talk to anyone
143 (25.9)
I don’t want to talk to anyone about my behaviours; it is too personal
134 (24.3)
I don’t feel deserving of help
97 (17.5)
Normalisation of violence
192 (34.7)
My behaviour is just a normal part of relationships. I don’t believe there is any need to see a professional about them
141 (25.5)
My behaviour was a once-off. It won’t happen again
113 (20.5)
Access challenges
192 (34.7)
All available services are too expensive
164 (29.7)
No access to transport to see someone
80 (14.5)
Confidentiality
162 (29.3)
My friends or family will find out
128 (23.2)
The professional will tell others
87 (15.7)
Lack of awareness of services
132 (23.9)
I don’t know of any service that might be able to help
132 (23.9)
Communication
122 (22.1)
The professional will not understand me
122 (22.1)
Low priority/lack of time
88 (15.9)
I have no time to talk to someone about these things
88 (15.9)
Total participants who needed help and were unable to get it
161 (29.1)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses, maximum missing n=1.
a Barrier defined as those options that participants said were “Moderately important”/ “Very important”.
Among the 161 participants who had never sought advice or support for their behaviour in the past, the three most common service barriers they identified were a lack of awareness about available services (68.3%), the cost of services (62.1%) and long waiting times (59%; Table 30).
Table 30: Proportion of people who use violence and the service barriers that prevented their access to services (n=161)
Service barriers
n (%)
Lack of awareness of available services
110 (68.3)
Cost of services
100 (62.1)
Waiting time too long
95 (59)
No service available in the area at the time needed
92 (57.1)
No private health insurance
91 (56.9)
No appointments
90 (55.9)
Limited opening hours
84 (52.2)
Not taking new patients
79 (49.1)
Concerns regarding confidentiality
79 (49.1)
Language or translation problems
40 (25)
Notes:
392 participants were skipped from this item because they had not been in the situation of needing help and being unable to get it.
Denominators vary due to missing responses; maximum missing n=1.
Journeys to help-seeking
In this section we expand on the above survey findings to explore the findings from our interviews with eight people who acknowledged that they had used abuse or violence towards a partner. The research question that guided this part of the study was “What are people’s journeys in engaging with help for their use of IPV and/or SV?”
The interview participants were all male and aged between 43 and 71 years old, with a median of 55 years. Three were from Victoria, three from New South Wales and two from Western Australia. Three were born outside Australia (in India, the United Kingdom and Sudan). All identified problematic behaviour in relationships with female partners. In their previous survey responses, six of the participants said a partner had been afraid of them; four said they had continuously contacted or followed a partner; four had made threats to harm a partner; three had forced a partner into sex; and two said they had shaken, thrown, pushed or grabbed a partner. In their interviews, four said their partner had contacted the police about their behaviour and three of them had been subject to a protection order. Two were still in their relationship and six were separated from their partner.
The interviews with participants focused on their journeys engaging with help and support for their abusive behaviour. We undertook a thematic analysis of the interview data to help understand how they experienced this process of help-seeking. We begin by discussing the central theme in their stories that reflects their overall experience of seeking help to address their behaviour. We then provide three case studies from participants in order to illustrate this central theme. Following this, we discuss the key stages and turning points in participants’ journeys of engaging with help for their use of IPV and/or SV.
Central theme: Releasing emotions and regaining stability
In their interviews, all of the participants emphasised that they did not have disrespectful attitudes towards women and most claimed that they had never been physically violent. However, most did acknowledge using some form of problematic behaviour in their relationships. Some described their behaviour as “psychological aggression” or “emotional abuse”, while others spoke of their “anger” towards their partner without identifying what this meant in terms of their behaviour. A common belief among participants was that their abusive or violent behaviour did not reflect their conscious choices or their character, beliefs or attitudes. Instead, they suggested it was responsive and caused by strong emotions that had led them to temporarily lose control over their behaviour. They spoke of being overcome by anger (for example, one said “I couldn’t control my temper” [Participant 9]), powerful sexual drives and mental distress or illness (forinstance, one associated his violence with being “mentally unwell” and said it “felt like someone else had taken over my body”[Participant 2]). Some also indicated that a lack of sleep, high blood pressure and/or alcohol use had contributed to their actions.
Thus, based on the perceptions and experiences of participants, a central theme was that to stop their abusive behaviour they needed help to release their emotions and regain emotional stability. They suggested that what assisted them to not “bottle things up” was talking to counsellors and others, getting the right medication for their mental health, doing regular exercise and improving their physical health. The following three case studies illustrate this central theme in participants’ stories.
“I’ve just got to look after myself”: Brett
Brett explained in his interview that his job had been extremely stressful, and that he had developed PTSD as a result of his work. He said he could not sleep and was in “a mentally dark place that I just couldn’t … I didn’t have control of my emotions. I couldn’t control myself. So, my ex would always be walking on eggshells not to just disturb me.”
Brett said his employer gave him time off and pushed him to see a psychiatrist. He found it “cathartic” talking to professionals about his distress; however, at that stage, his medication was not working, and he was still “angry all the time” and “unbearable” to be around. His partner told him he needed to go to hospital and got him admitted. However, Brett said: “I tried to do the things that she asked me to do, but in the end it wasn’t enough.” Being hospitalised increased his anxiety and he did not feel comfortable to engage in therapy while he was there. His partner ended up leaving him, taking their children. Brett said: “On top of losing my family I lost my home, I lost my job, I got arrested many times and put through the court process … and I wasn’t allowed to see my [child] for some time.” His partner took out an intervention order and “was alleging all sorts of things that weren’t true”. Due to her allegations about himbreaching the order, he was mandated to attend a men’s behaviour change program. However, Brett said the program did not help. He said the other men in the group had disrespectful attitudes and “were all there because they’d punched the shit out of their missus or destroyed property”, and Brett felt he was different to them.
Brett said once he got the right help and felt motivated to change, things got better: “The medication started to work, and I felt more comfortable talking to [my psychiatrist and psychologist] … they help to guide you in the right direction. But, yeah, you’ve got to want to do it. If you don’t want to do the effort, put the effort in, nothing’s going to change.” The thing he said really helped his mental health and behaviour was getting physically fit:
Exercise is the thing that pushed me back [onto the right path]. So, when I don’t get it, through the lockdowns and all the last couple of years I couldn’t go to the gym, that was a fairly dark period. But now that we’re over them and I’m able to go to exercise … I’m fairly stable … I’ve just got to continue to look after myself.
“Someone I can talk to …instead of bottling it up”: Amar
Amar acknowledged that his partner had been afraid of him. In his interview he explained that a major cause of arguments was his wife’s reluctance to have sex after she had a baby:
I was in my prime, you know, raring to go all the time. That was a major problem … I pride myself on not going anywhere else but to my wife … But in saying that, I hurt myself doing that … it affected our relationship where I just tried to put the hard word on my wife all the time. She didn’t want it and we argued about it.
Amar said that what increased the conflict in his marriage was that he had suffered a “breakdown” because of work-related trauma. He left his job but struggled to find a new one because of the medication he was taking for his mental health. He said not being employed was difficult and caused arguments with his wife, because he had been brought up to believe “I should be the one earning the money”. He said he needed understanding and comfort from his wife but was not receiving it: “I just wanted to feel loved … I wanted my wife to cuddle me and have sex with me … I needed relief.”
Amar said he could not talk to his family because they thought he was “an asshole” and his child “thought I was being nasty on purpose to my wife”. He found it “embarrassing” to seek help because people would think “You’re a man … [so] harden up.” He became depressed and suicidal, and “ended up in a psychiatric ward … because I just couldn’t take it.” He found being hospitalised was a relief because he “didn’t have to worry about anything”. Amar said the main thing that had helped was finding a psychologist. The psychologist enabled him to talk freely and honestly because he did not feel judged: “He’s someone that I can talk to … instead of bottling it up… he knows everything about me. I don’t have to hide anything … because there is no ‘wrong way’ because it’s not against him.” He suggested that being able to release his emotions in counselling has prevented him from taking them out on his wife:
I tell [my psychologist] exactly how I feel … what I feel like doing. So, yeah, he knows a lot, and he has helped me because … it takes a lot off my mind when I talk to him about things, because now I think, well, I’m not going to go home and bottle it up … and then one day she may not put enough sugar in my coffee or something, and I’ll spit the dummy and let it all out … and have a go at her, you know. I don’t want to do that.
“I’ve emptied myself of all that hate and darkness”: Aaron
In his interview, Aaron spoke of the stress of his job and said he suffered work-related trauma and an assault during his employment. He explained that he had “carried” that trauma into his relationship and it affected his behaviour: “I was very, very psychologically violent to [my first wife]. I mean, very scary … I mean, I never hit her or anything, but it was psychological violence.” He was drinking excessively to cope, but that only made things worse: “I was still bottling up all of the things that had happened to me so that was still being pushed down with alcohol, so that was fuelling things.”
Aaron said he kept “just losing it … just getting more, just angrier and angrier and angrier”. Yet he felt unable to seek help because his workmates would see him as “weak”. He also did not know what services were available. He would try to speak to his GP but said that “all they’d do is say ‘Oh, you’re an alcoholic’”. Things “came to a head” when he threatened his partner with a knife. His partner called the police and a CAT (crisis assessment and treatment) team, and he was hospitalised. However, Aaron said the psychiatric hospital was “horrible”. He felt they did not diagnose him properly and the nurses had “no compassion”; they treated him like a violent alcoholic who “should be in prison”. Aaron described feeling trapped in a cycle of medication and drinking, which he said only fuelled his poor mental health and aggression:
I just felt like I was losing control of everything, and I didn’t know where to go … I was trying and trying not to drink. I was going to AA and I just found that didn’t work. I was on the medications and that was working but it was like I just couldn’t – it was like I was unable to actually explore my own baggage and trauma.
He ended up leaving his wife as he was “confused” about his feelings towards her and feared doing something “beyond regrettable”.
Aaron said this cycle shifted when he met his new partner, who made him feel “loved for the first time” and offered “a bit more stabilisation” in his life. His partner found a psychologist who supported him to disclose and process the trauma he experienced:
I felt so comfortable with [the psychologist] and so trusting of [him], that then I was able to open up more to him, which – then I was much more able to open up to my wife … I’ve actually talked to him about all of the trauma that I suffered in the army. It’s like the whole – I don’t need to drink anymore because I’ve actually emptied myself of all that hate and darkness.
Since seeing his psychologist, Aaron says he has changed significantly. What helped was receiving ongoing emotional support, as well as being directly challenged and prompted to focus on his motivation for change:
We were talking the other day about how when I first started coming to see him and how angry I was and where I am now in relation to that. It’s like leaps and bounds. But that’s probably because [he] tell[s] me off as well. So … we talk about a lot of – what I want to achieve out of this. Otherwise … if you don’t want anything, why are you here? So [he’s] direct but at the same time he makes you feel very relaxed and open.
The three narratives presented above illustrate the central theme that reflects participants’ journeys of seeking help for their use of IPV and/or SV: “releasing emotions and regaining stability”. Each of the participants suggested that they suffered a build-up of mental distress and “lost control” of their behaviour. Participants perceived that what helped them regain control was medication, counselling and/or improving their physical health. Next, we will discuss the main stages and turning points across interview participants’ stories of getting help for their behaviour.
Key stages in participants’ journeys
By analysing how the interview participants described their abusive behaviour and their journeys towards change, we identified three stages: bottling things up; breaking down and letting things out; and regaining and maintaining emotional stability. Figure 16 provides an illustration of these stages and the key turning points in participants’ journeys.
Figure 16: Key stages and turning points in participants’ journeys of engaging with help
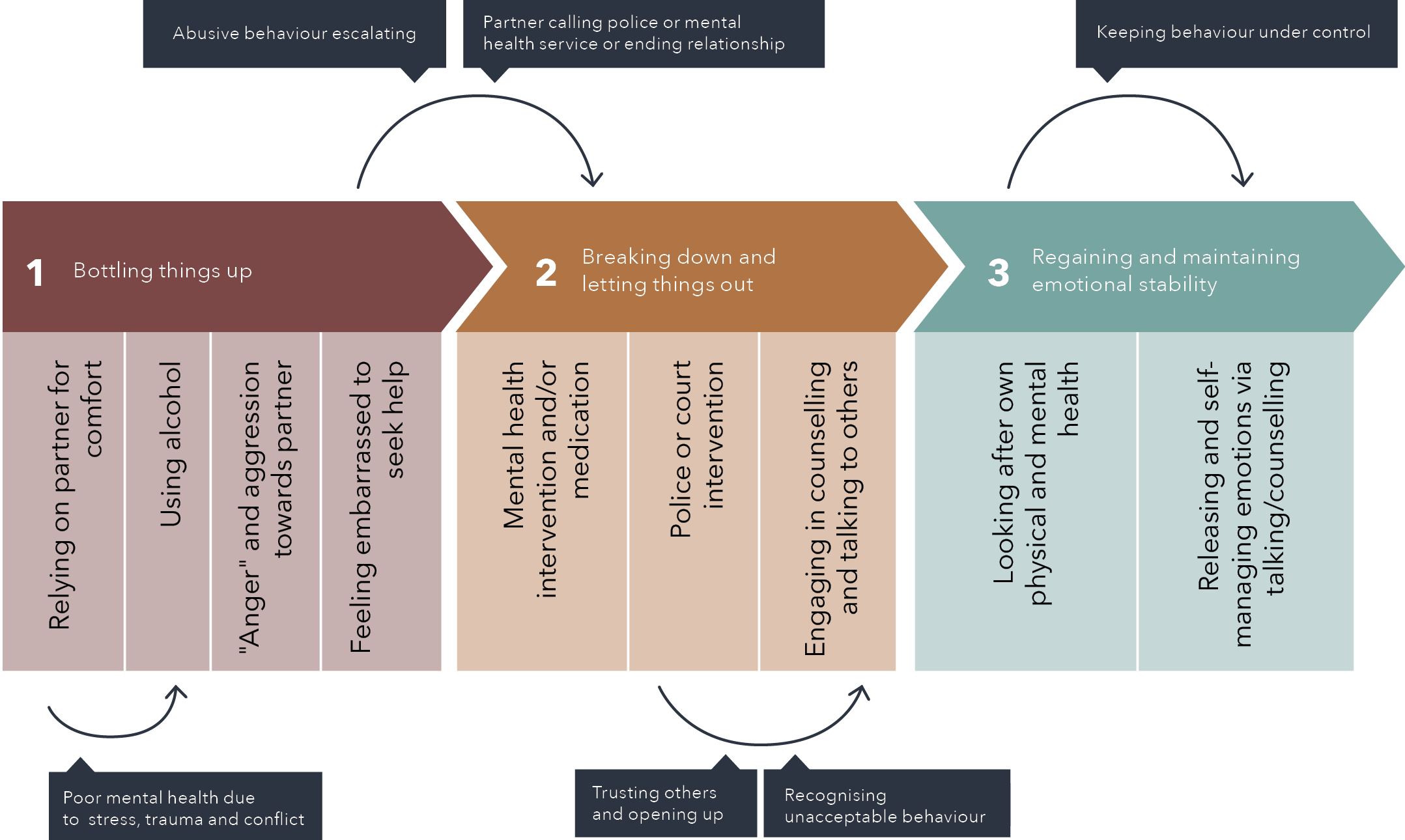
Text version of the figure above:
- Bottling things up
- Relying on partner for comfort
- Using alcohol
- “Anger” and aggression towards partner
- Feeling embarrassed to seek help
- Breaking down and letting things out
- Mental health and intervention and/or medication
- Police or court intervention
- Engaging in counselling and talking to others
- Regaining and maintaining emotional stability
- Looking after own physical and mental health
- Releasing and self-managing emotions via talking/counselling
Before step 1 to step 1
- Poor mental health due to stress, trauma and conflict
Between steps 1 and 2
- Abusive behaviour escalating
- Partner calling police or mental health service or ending relationship
Within step 2
- Trusting others and opening up
- Recognising unacceptable behaviour
Within step 3
- Keeping behaviour under control
Bottling things up
Participants suggested a build-up of stress, poor mental health and conflict in their lives and relationships had triggered their abusive behaviour. Four said they had suffered work-related stress, or a traumatic event related to their employment, and two said abuse they experienced during their childhood had resurfaced and affected their mental health. Some also indicated their partner had also contributed to conflicts and stress, because they were depressed, “hot tempered” or “antagonistic”, or refused to have sex with them. Two said their partner was emotionally or physically abusive towards them.
Participants spoke of “bottling things up”, “pushing things down” and/or using alcohol to cope with the mental distress they were experiencing. At this stage they did not seek help, either because they were so mentally unwell that they could not recognise their behaviour as a problem, they did not know where to turn, or they felt too embarrassed to talk to others. Being a man was described as a barrier to help-seeking as they felt they were expected to be “hard” and not express vulnerability. However, they suggested they believed they ought to be able to rely on their partner for emotional support and/or sexual comfort. Several expressed disappointment or resentment that their partner had not understood their suffering or had been unavailable due to her own problems (for example, one [Participant 2] said his partner became “a zombie” because she was taking medication for post-natal depression).
Breaking down and letting it out
Most participants said their engagement with services only occurred after they had reached a crisis point. The crisis was a mental health “breakdown” and/or their partner leaving them and taking their children. During this time, participants appeared to be motivated to engage with service providers to alleviate their mental distress. However, most did not instigate the help-seeking process themselves. Instead, the catalyst for their engagement with services was their partner/ex-partner ending the relationship and/or contacting police or mental health services about their behaviour. Four of the participants (including Brett, Amar and Aaron, as described in their case studies) spoke of being hospitalised after their partner had contacted mental health services or police. While they did not always perceive the intervention of mental health services as helpful, it opened the door to acknowledging their problems and gaining an understanding of theunderlying causes of their distress.
All the participants said they eventually found someone who gave them effective support. This source of help was a psychologist (for three participants); a GP (two participants); family and friends (two participants); a new partner (one participant); and a men’s health support group (one participant). What they said was important was receiving a non-judgemental and compassionate response and being able to develop a relationship of trust over time. Participants suggested such responses enabled them to “open up” and “let out” their emotions, rather than bottling them up and taking them out on their partner. They felt that releasing their feelings and getting the right medication and/or insight into the underlying causes of their problems improved their mental health and helped them change their behaviour towards their partner. Some said they also valued being offered advice on how to manage relationship dynamics, being challenged about theirbehaviour and being guided to focus on what they wanted to change in their life and their relationships (as illustrated in Aaron’s case study). The responses participants found unhelpful were immediately being made to feel criticised or judged, such as professionals labelling them a “violent thug”, or police or family courts automatically assuming that men are the abusers in relationships while women are not.
Regaining and maintaining emotional stability
Once they had recognised their emotional problems and found the right help, participants focused on “stabilising” themselves and keeping their mental health and emotions under control. They suggested this required continuous self-management. Participants (as illustrated in Brett’s case study) spoke of the importance of keeping up with exercise, doing yoga, eating healthily and getting sleep to prevent having further problems. For some (as described in Amar and Aaron’s case studies), supportive professionals played an ongoing role and they voluntarily returned for support whenever they needed help to maintain emotional control. For instance, one participant said:
If I cannot control the situation … then I go to see [my GP] … [he tells me to] keep out of the area … and go inside somewhere where nobody can disturb you … watching TV or listen to music … and your rage or anger will cool down. (Participant 8)
In this section, we have presented data from interview participants about how they perceived their use of IPV and/or SV and how they sought help over time to change their behaviour. In the discussion section of our report, we consider participants’ perceptions and experiences in light of current research evidence about how behaviour change occurs, including the importance of shifting the gender-based beliefs and attitudes that underpin the perpetration of IPV and/or SV.
The next section specifically looks at help-seeking during the COVID-19 pandemic by participants who used IPV and/or SV.
The impact of the COVID-19 pandemic on help-seeking
We also asked survey participants what impact, if any, the COVID-19 pandemic restrictions had on their access to support services for their behaviours in intimate relationships. Many said it had not impacted them or that they did not need to use support services. Others noted that it had altered their engagement with services.
It made getting support harder
A major theme was that it had been more difficult to access support services during the pandemic. Participants said they were unable to visit a professional in person because of restrictions or long waiting lists for counselling support. For example, one stated: “[My] psychologist was heavily booked throughout lockdown, so I wasn’t able to see them as often as I needed to.” Several commented that they missed out on accessing group-based programs; for instance, one said “I … wish that there were face to face support groups operating as it’s been very isolating.”
A number of participants described a lack of comfort engaging with services that were only offered via phone or online. They suggested that compared to face-to-face interactions, telehealth delivery felt impersonal, “distant” and “disconnected”. For example, one said:
Back when COVID-19 first came to fruition my weekly appointment with my drug and alcohol and relationship counsellor went from being face to face to over the phone. It never felt anywhere near as beneficial as my face-to-face appointments and as a result I stopped seeing them.
Participants said it was “tiring” and “harder to explain things” and they needed physical closeness to the service provider to “feel okay about being vulnerable”. For instance, one said in-person conversations “feel a lot more authentic/of value”, while another said telehealth counselling “doesn’t have the same impact as being in the same room”.
A lack of privacy at home was a key concern that made participants reluctant to use telehealth services:
I wasn’t comfortable with video chatting/phone calls during lockdown as it put me in earshot with my partner or neighbours.
It has made it more complex to access services in private, as I share a house with other people I don’t have complete privacy.
Greater convenience and awareness of services
For some participants, telehealth during the pandemic meant support services were more convenient to access. Participants said they appreciated not having to travel or being able to access services in other cities. For example, one said: “I actually quite enjoyed [counselling via telehealth], because we don’t have a car at the moment, so transport is sometimes an issue.” Another said they appreciated that “services in other cities or countries can be accessed from anywhere”.
Another benefit was that support services were more prominently advertised during the pandemic:
It made things easier! And a lot of services are getting heavily promoted which raises awareness of their existence.
Summary
Survey participants who had used abuse or violence mostly sought help from their friends, family members or partners, followed by a health professional. More often than not, they rated the informal or formal support they had accessed as helpful. Barriers to help-seeking included shame, the normalisation of violence, access challenges and confidentiality concerns. Some participants were unaware of services that could help or said they lacked access to affordable, available services. Our interviews with eight participants provided more detailed data about the help-seeking over time of people who had used IPV and/or SV. While most interview participants admitted using problematic behaviour in their relationships, they often minimised it as “anger” or said they were emotionally abusive but not physically violent. They suggested that strong emotions or poor mental health had led them to temporarily lose control over their behaviour, and a key theme wasthat they needed help with releasing their emotions and regaining control. We identified three key stages in how they described their journey to engaging with help: bottling things up; breaking down and letting things out; and regaining and maintaining emotional control. Our survey data from participants who used abuse or violence indicated that the COVID-19 pandemic made it more difficult for many to access support services to address their behaviour. However, for some participants, it had no effect or made it more convenient for them to seek support through the use of telehealth or online service delivery.
3. Support needs of people who use violence
This section integrates the survey findings and the qualitative findings on support needs from the perspective of people who use violence.
What do people who use violence value in a service?
For the 408 participants who had spoken to someone in the past, they most valued the following: learning new ways of dealing with relationship problems (92.4%); feeling listened to (91.9%), and the expertise of the professional (91.2%; Table 31).
The next section draws on qualitative data from the survey.
Table 31: Proportion of people who use violence and what they value most in a service (n=408)
Emotional support
Service values
n (%)
Feeling listened to
375 (91.9)
Knowing that my story would be held in confidence by professional
357 (87.5)
The professional being interested in who I was as a person
350 (85.8)
Not feeling judged or put down
349 (85.5)
Having someone to talk to
345 (84.6)
Professional competency
Service values
n (%)
The expertise of the professional
372 (91.2)
Practical support
Service values
n (%)
Learning new ways of dealing with relationship problems
377 (92.4)
Given practical information about how to increase safety
359 (88)
Material support (e.g. getting access to accommodation)
255 (62.5)
Other (participant open-text suggestions)
15 (3.7)
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey item.
155 participants were omitted as they had never sought advice or support.
Support needs and expectations of services
In this section we draw on qualitative data provided by participants, in answer to the following four open-ended survey questions about their support needs and expectations:
- What do you think you need the most to stop using violence and abuse?
- What do you think your greatest need is from a service or professional?
- What do you believe that professionals need to do differently to better help people in similar situations as you?
- I wish that service providers …
We combined the data from the questions in developing our analysis of the support needs of people who used IPV and/or SV. In analysing participants’ responses, it was evident that many did not see themselves as needing support for their use of violence or abuse as they did not wish to characterise themselves in this way. This was despite them having identified using forms of violent or abusive behaviour in other parts of the survey.
For participants who did acknowledge needing to address their use of violence and abuse, we identified three themes relating to their support needs: “Help to regain emotional control”; “Hear me and talk to me, not at me”; and “Help me see things from a different perspective”.
Help me regain emotional control
A common theme among participants was that their violence or abuse was caused by problems controlling their anger or other emotions. Many participants expressed this belief, including those who identified having used forms of physical and/or sexual violence, as well as psychological abuse or monitoring behaviours, such as following or continuously contacting a partner. Consequently, help with emotional regulation or “anger management” was seen as a key component to stopping their behaviour. For example:
I need to be more patient and be of low temper.
[I need] learning [on] how to deal with my own emotions and keep them under control.
I get frustrated/angry quickly over very minor things. Having a couple of drinks which really helps in reducing those outbursts but it is a really unhealthy pattern that is upsetting to both me and my partner. It also can lead to excessive drinking. I need help in breaking that chain and control my frustrations better.
I need [services] to help me manage my emotions and prevent them from getting to an uncontrollable state.
While some indicated poor anger control was part of their personality, others suggested that it was because they were dealing with difficult external circumstances. For example, to stop their abuse, one spoke of needing to “reduce stress from work”, and another said: “I think I need to be balanced financially, lack of finance makes me angry because it makes me feel less like a man.”
There was considerable interest among participants in receiving counselling to help process, release and regulate their emotions. For instance:
[My greatest need is] emotional support … I know my unhealthy behaviours and it is when I feel compelled to react to deep feelings of shame, insecurity, fear or pain that I would like support to process those deep feelings.
[I need] techniques on how to actively dissipate feelings of anger or frustration.
They also spoke of a need for “coaching” or guidance on how to improve their communication and reduce conflict with their partner. For example, one said: “[My greatest need is] learning skills to de-escalate an argument with my partner (i.e. moving into another room, tone of voice etc.).” Another said lessons in effective communication would help to stop a build-up of anger: “Being taught to be able to communicate what is bothering me in an effective manner [would help] so I don’t bottle it up and then explode.”
Many participants suggested that an underlying mental illness (such as anxiety, depression, or PTSD) made regulating their emotions difficult and caused their abusive behaviour. Thus, a frequent comment was that they needed professional treatment for their mental health problems in order to improve how they treated their partner. Many spoke of needing a diagnosis, medication and/or therapy:
[My greatest need is] regular sessions with my shrink to help me deal with my PTSD. My negative behaviours towards partners are, generally, unintentional and reactionary to PTSD.
[My greatest need is] a combination of therapy with an increase in daily stimulus for my mind. During the pandemic I became increasingly aggravated at the smallest components due to depression and under-stimulation, which is a difficult combination to overcome.
[My greatest need is professional help] dealing with anger and past trauma from the army.
Possibly [I need] a diagnosis of ADHD and then help to prevent my quickness to anger.
I’m on tablets now which are great, I don’t swear, yell or do anything.
However, there were other participants who suggested they could manage their emotions without external help. By far, the most common solution was to calm down by taking a break or “walking away” when they had conflicts with their partner. Another solution was to improve their general physical and emotional wellbeing so they could be more emotionally balanced. Participants identified various strategies they needed to use to increase their wellbeing, such as meditation or relaxation exercises, seeing friends, and going for walks. Reducing alcohol or drug consumption was also perceived to be helpful in regaining control. For example, one participant’s greatest need was:
Zero alcohol consumption, and a dedication to actually reading the one single quote that is 100% relevant, each and every morning. Even several times a day, as it is inspirational.
Help me see things from a different perspective
The second theme among participants’ responses was a need for a new way of thinking. Some said they wanted someone to teach them what a healthy relationship looked like and how to recognise their problematic behaviour. For instance:
[I need] explanations of poor behaviour and guidance for improvement and change.
[My greatest need is] having some sort of mentoring so that you can differentiate between right and wrong.
[My greatest need is] having a safe space to talk out my thoughts and feelings … to help me understand, see things from a different perspective and hopefully learn, grow and change my behaviours.
As well as help to identify poor behaviour, they also wanted support to understand their partner’s perspective. For example, one said:
[My greatest need is help to] learn how to regulate my own emotions, be responsible for my own actions and have better empathy/do a better job of perspective taking for my partner. Professionals that were non-judgemental and empathetic, but able to challenge me, have been really helpful.
Only a small number of participants indicated that they needed help to better understand how their behaviour was connected to gendered beliefs and attitudes. For instance, one said his greatest need from professionals was to help him understand “How are we supposed to be a man?”, because “Being respectful, and treating people equally can be a lonely path … In many settings, men are still required to ‘man up’, which seems to mean suppress your emotions, and stick to your guns”. However, most did not explicitly connect their behaviour to beliefs about masculinity or attitudes towards women. Despite this, a number of participants did refer to a need for help to change their “way of thinking” or their “mindset” in relation to how they thought about or valued their partner. For example:
My greatest need from a professional right now is for that person to listen to me and help me reshape the way I look, think and approach my wife and partner. I need advice on how to handle myself when I meet certain difficult situations in my relationship.
[My greatest need is] an effective way to control my mindset, so that any temptation to do “the wrong thing” can be shrugged away without too much effort.
I think I have to be shown ways to appreciate my wife rather than see her bad sides or flaws.
As is evident in some of the quotations above, several participants emphasised that in order to reflect on and change their perspective, they needed to feel the professional provided a “safe” or “non-judgemental” space for such a conversation. This need is discussed in the next theme.
Hear me and talk to me, not at me
An important theme that cut across participants’ responses was a need for a conversation with a professional who would listen and try to understand, rather than judge. This theme was encapsulated in the response of one participant, who said their greatest need was “to have someone hear me and talk to me, not at me”. Similarly, another said, “[My greatest need is for a professional to] be understanding and unpatronising and really just listen and provide good advice.”
Many felt that openly sharing their experiences and feelings with a counsellor could help them to explore what was causing their behaviour:
[My greatest need from services is for] understanding and compassion as well as strategies to find the root of the issues.
I have felt for a long time that I would most benefit from an open and honest conversation about my past with a professional therapist. [It] would help me process my experiences and actions, understand the factors that led to them, and ensure that they never happened in the future.
In order to open up, participants said they needed a professional who was approachable and non-judgemental. For instance, one suggested service providers should “make the atmosphere more friendly … first do some warm-up so that the patient can feel relaxed talking to the professional”. Others spoke of the importance of being reassured that the conversation would be confidential:
I would most value not feeling judged or intimidated by the professionals. This might mean being confident in the confidentiality of the session and also speaking to them in an informal setting or manner.
Participants frequently expressed uncertainty about whether professionals would report what they said to others and wanted clear confidentiality guidelines to help them feel comfortable to seek support. For instance, one participant said: “[I need] professionals to show more evidence that they will not disclose my private information.”
As well as wanting to be listened to, rather than talked “at”, participants also spoke of needing professionals to get to know them “as a person”. Many spoke of not wanting service providers to make assumptions or to offer “standardised” or “textbook” responses. For example:
The professionals need to understand that general advice may not be suitable in every case. There are different societal and cultural practices that must be taken into consideration when offering solutions.
I think some professionals need to take each person as having their own unique circumstance … Whilst it is beneficial for them to take their learnings and knowledge from other patients – it should never be the sole focus or influence decisions too heavily.
Similarly, some said they did not want professionals to automatically assume they were the problem:
[I wish that service providers would] not presume that I am at fault. Understand that people who feel hard done by often actually are.
Several expressed a wish for services to “understand men” better and not “stigmatise” them or push a “gender narrative” about the causes of abuse. For example:
[I wish that service providers] understood the problem is not always with men even if we are more likely to get violent.
Some felt gendered assumptions about men as abusers were barriers to seeking support:
One thing I believe would help is for professionals to be able to let men know they differentiate these types of experiences. I know of friends who wish to take similar proactive steps in changing their way of dealing with anger but, because of the stigma that domestic violence rightly has attached to it, feel they will get quickly identified as an abuser and not as someone who is actively trying to make themselves a better partner.
The next section explores the role of family and friends.
Role of family and friends
We asked people who used abuse or violence to provide their written responses to the survey questions “I wish that my family …” and “I wish that my friends …” The questions followed others about their use of abuse and violence, and we instructed participants that they should think about their relationship with their partner or ex-partner in answering the questions about what they wished for from family and friends. It was not always clear whether their survey responses were referring to how they wished their friends and family could respond to their use of abuse or violence or to general relationship or personal concerns. However, the data we collected from the survey provide a broad indication of how participants saw the role of family and friends in responding to intimate relationship issues. Based on our analysis of their responses, we identified the two themes: “Be willing to engage in a deeper conversation” and “Listen with an open mind”.
Be willing to engage in a deeper conversation
The main theme evident in participants’ responses was a wish that family and friends were more interested in having meaningful conversations about relationship or personal problems. For example, some wished their friends were more prepared to have emotionally supportive conversations:
I wish that my friends were more available and willing to have an emotional discussion about our vulnerabilities, to build a stronger deeper friendship.
I wish that my friends were more authentic and supportive, rather than only contacting me when I’m needed. I wish my friends would check up on me more often, especially since they know about my past mental health problems.
Others spoke of wanting greater engagement from family members. For example, one said: “I wish that my family can communicate with me deeply more often”. However, participants frequently suggested that their family and friends were not comfortable having serious conversations about relationships, emotional issues or sex. For example:
[I wish my friends] will learn to stop joking about everything.
[I wish that my family] didn’t make talking about sexual relationships taboo.
[I wish my friends] were more willing to talk about sexual violence and our role as men in preventing it.
Some indicated their family or friends did not know how to help and gave dismissive or unhelpful responses.
I wish that my family knew better how to respond to mental health/family violence/substance use issues. I wish they had taken my partner[’]s concerns more seriously and been far more proactive in reaching out to support her once I came clean to them about what had been going on.
[I wish my that family] had spent more time discussing feelings and how to cope with them, and not disregarded them or told me to “stop”.
Listen with an open mind
A second theme was the wish that when participants discussed relationship issues with family and friends they would have an open mind and try to understand, rather than responding with judgement or unwanted opinions. Participants frequently said they wanted family and friends to be more “neutral”. For example:
I wish that my friends who my wife has turned against me would realise that there are two sides to every story and give me a chance to explain to them, the other side.
I wish that my family would not make an uninformed judgement on my relationship and actively listen without bias. I wish that they would check in with me more to provide basic emotional support.
Many also expressed a wish that family and friends were “better at listening than giving advice”. For example:
[I wish that my family] would try to understand where I am coming from in any given situation before pushing their views on to me. Have more of an open mind.
[I wish that my family] would listen instead of trying to downplay a lot of what is being said to them. My issues are never big problems in their eyes and I always get a response like “you will work through it” or “I know someone who has it worse”. It isn’t helpful.
As well as receiving unsolicited advice, some participants did not like receiving unwanted interventions from friends or family. Several said they wanted friends or family to “respect boundaries” or stop “interfering in a negative way” in their relationships. For example:
I wish that my family keep their noses out of my business.
I wish that my family would stop judging and prying into my life.
In summary, our analysis of survey responses suggested that people who use IPV and/or SV are often interested in having in-depth conversations with their family and friends about their relationships and would like family and friends to listen with an open mind. Such conversations could potentially play an important role in helping to identify abusive behaviour and to support people on a pathway towards change. However, our findings also suggest that many people who use IPV and/or SV find it difficult to engage their family and friends in serious discussions and may receive responses that they perceive as dismissive or unhelpful.
Victims’ and survivors’ perspectives on helping people who use IPV and/or SV to stop
In this section we explore what helps people to stop using IPV and/or SV from a different viewpoint. We return to the survey data from victim and survivor participants to explore their experiences of their partner or ex-partner’s abuse and what had helped or would help to end it. We asked women victim and survivor survey participants to provide written responses to two questions: “If you think about your partner’s/ex-partner’s behaviours towards you, what do you think has been most helpful for your partner in helping them to stop using violence and abuse?” and “If you think about your partner’s/ex-partner’s behaviours towards you, what do you think your partner might need that would help your partner stop using violence and abuse?” We identified three key themes based on their responses to the first question: “Nothing was helpful”, “Removing myself” and “A fear of the consequences”.
Nothing was helpful
The predominant theme among participants was that nothing had helped their partner/ex-partner to cease their abuse. Participants typically expressed a deep pessimism that their partner/ex-partner would ever change. They frequently commented that the main problem was the perpetrator’s refusal to accept their behaviour as abusive. For example:
He doesn’t see he has a problem.
He thinks he’s the victim in it all.
Although some women believed that therapeutic approaches such as counselling or drug/alcohol programs had been helpful for their partners, many stated that their partner/ex-partner had resisted attempts to engage them in treatment or therapeutic interventions, even when they had been legally mandated to do so. For example, one said: “I had two IVOs [intervention orders] which he totally ignored … and he was apparently told to do an anger management course which he did not do.” Another participant similarly described: “I tried for two-and-a-half years in my court orders for him to do a Men’s Behavioural change program but he didn’t want to, so he didn’t.”
Others observed that even though their partner had attended treatment or had been subjected to legal intervention, it had failed to curb the abuse.
He went to rehab 3 times while we together purely to stay out of jail. I have a FVRO [family violence restraining order] in place, he’s breached it many times.
Some women felt that their partner had been able to trick service providers into believing that they had changed, or that their behaviour was less serious than it really was:
He sees psychologists and a psychiatrist who he doesn’t tell the full story around our separation to … so, he’s getting no help at all.
He did a men’s behaviour program and manipulated them.
Some women observed that the perpetrator’s behaviour had continued after they left the relationship or that the only thing that had altered was the type of abuse they used: “The abuse and violence has not stopped it has simply changed into systems and legal abuse and it continues today.” Participants also noticed that the perpetrator had then redirected their abuse towards their new partner: “He re-partnered 4 weeks after I finally left him and he’s the same with her.”
Removing myself
Although for some participants, leaving the relationship failed to stop their ex-partner’s abuse, for others, leaving reduced the abuse. While these participants observed that ending the relationship did not cause the perpetrator to change their mindset, it did mean that the perpetrator had fewer opportunities to target them:
I had to remove myself. One partner stalked me for three years till I left the country.
Me leaving [stopped the abuse] … he is still the same person as he was back then though … He still blames me for his abuse during our marriage and now he tries to undermine me to our children. But at least now I am not living with it daily.
The only thing keeping me safe is that he lives in another state.
I got rid of him – that is probably the biggest opportunity for him to decide to face himself – and get some help – but alas he has ignored this opportunity.
A fear of the consequences
Some participants indicated that legal responses such as police intervention or protection orders had been partially effective in reducing their partner or ex-partner’s abuse. For instance, one said: “Family court orders and the FVO [family violence order] have stopped his violence and abuse for the most part. It continues in other, less overt ways.” Another said: “Putting him in jail … but even that didn’t stop him until the 3rd time.”
Women commented that the major deterrent for the perpetrator after police intervention was the threat of further negative consequences, such as the loss of freedom or reputational damage:
Police intervention and threat of losing his job and reputation.
The threat he will go to jail next time he steps over that line. His fear of the consequences and Court.
Me telling him I will get an in-house AVO [apprehended violence order] on him. He cannot allow others to think he’s a monster.
Victims’ and survivors’ views on what would help stop the perpetrator’s abuse
In this section, we will discuss the key themes from our analysis of participants’ responses to the second question about what might help their partners.
As outlined in the previous section on victims’ and survivors’ survey responses on what had helped their partner/ex-partner, when asked about what they might need, many participants expressed great pessimism about their partner or ex-partner’s ability to change. This was reflected in comments that the only thing that would stop the abuse was if the perpetrator disappeared. For instance, some responded that what their partner/ex-partner needed was “a bullet”, “castration”, “a lobotomy”, and one commented that “his death is when the abuse will stop”. While we recognise and acknowledge these sentiments, in this section, we have focused on the other suggestions women made to help the perpetrator stop using violence.
A wake-up call and retraining
Many victims and survivors indicated that their partner or ex-partner refused to accept that they were abusive or violent. Thus, a major theme was that the perpetrator needed someone who could make them recognise that their behaviour was unacceptable and change the thinking and beliefs that underpinned it. For example, participants said the perpetrator needed:
… a wake-up call. He thought he was a victim because he couldn’t get us to do everything he wanted.
Some kind of wake-up call that would show him what an asshole he is when he drinks.
To be called out on their behaviour and shown the right way to treat a person.
Victims and survivors indicated that they were not in a position to be able to change their partner’s/ex-partner’s beliefs or behaviour. Instead, they needed someone external to them who had greater influence or power. They suggested male friends, professionals, community members and others who their partner or ex-partner respected and who could play an important role in calling out the problematic behaviour and attitudes. For example:
Perhaps if he had a male friend who could make him aware of his behaviour and lack of respect for women.
He needs to listen to a professional and get help as he thinks he is self-righteous and never wrong.
[What might help is] having people who he trusted or looked up to talk about his behaviour and its consequences.
[What might help is] being told by male health professionals and friends he respects that it is not okay.
[What might help is] more ads on TV supporting people calling out bad behaviour.
Participants also highlighted a need for intensive education programs to transform perpetrators’ beliefs about gender roles and relationships:
[He needs] MASSIVE retraining, addressing personality issues and his belief that he has the right to whatever he wants from his partner.
[They need] a course in how to treat a partner properly and therapy for their abuse as a child most of it is learnt behaviour, they need to be … taught different ways.
[They need] education that it is not ok to be controlling towards your wife.
“Intensive” therapy
Many participants suggested that significant personality and/or mental health problems contributed to the abuse or violence; however, their partner or ex-partner denied that they needed to seek help. Thus, a strong theme was that the perpetrator needed to be mandated or forced to engage in treatment or therapy and that any therapy needed to be intensive and ongoing. This was evident in participants’ comments that the perpetrator needed “strong”, “dedicated”, “extreme”, “serious”, or “continual” therapeutic interventions or “forced mental therapy”. For example, participants said:
[He needs] intensive therapy … it appears that he might have PTSD from previous experiences and a previous job role.
If he were ordered not to behave in an abusive way to either of us and if he were to be forced to see a psychologist for his behaviour and mental illnesses (all of which he denies), perhaps he could one day become a healthy father.
Victims’ and survivors’ responses also indicated that they felt a complex array of factors contributed to their partner or ex-partner’s behaviour. Thus, they suggested that a multi-pronged approach that addressed a combination of contributing factors could be helpful. This might include education, therapy for mental health and drug and alcohol use, and/or family or couples’ therapy. Responses included:
[What might help is] serious counselling. Mental health assessment. Anger management. Drug and alcohol counselling.
[What might help is] regular psychologist sessions, space to talk and mediate as a couple, alcohol and drug support.
Participants also emphasised that for therapy or treatment to be effective, the professional would need to understand victims’ and survivors’ experiences, and have expertise in challenging problematic attitudes or behaviour:
[He needs] an experienced anger management psychologist, not some half-arsed Medicare subsidised counsellor who just enables his behaviours in a group setting and never hears the side of the victim!
[My partner needs] counselling but where the counselling knows both sides because an individual can sugar coat their behaviour.
Hold them to account
Most victims and survivors suggested they had little hope that change would emerge spontaneously from within the perpetrator. Thus, a significant theme was those with power or authority needed to intervene, hold the perpetrator accountable and impose restrictions and/or consequences for abusive behaviour. For example, some highlighted legal interventions:
[He needs] further police intervention. Harsher restrictions. Police actually following up on the breaches. Checking he is abiding by his curfew.
What is needed is for coercive control to be illegal and for me to report him and for it to be taken seriously and for him to be warned about his behaviour.
Others suggested a therapeutic approach might help if professionals held the perpetrator accountable for making changes:
[My partner needs] to be heard just like anyone else. To be given the opportunity to talk through their behaviour and to make the changes that are needed. Also given the consequences of their actions if that behaviour continues.
[What might help is] actually having consequences for his actions and some alcohol abuse help.
Others felt incarceration was the only thing that would be effective. This was not only because it would force the perpetrator to have to confront their abuse but also because it meant they were no longer able to target the victim and survivor. For instance:
A prison cell is about all that would work.
I’m not with him anymore but jail [would help] so he doesn’t come out to do it again.
Overall, our analysis of survey responses found many women felt disillusionment and despair about ever being able to end their partner or ex-partner’s problematic behaviour towards them. A frequent comment was the perpetrator had minimised or denied the abuse and was resistant to seeking help. Some reported that their partner or ex-partner had attended therapy, behaviour change programs or substance use treatment, yet most reported that these responses had been ineffective, often because the perpetrator had not been held to account for making changes. The responses that were perceived to have had an impact in curtailing the abuse were the victim and survivor leaving the relationship or threatening to involve legal authorities. Participants felt that their partner needed someone who could make them recognise their behaviour was unacceptable, and that intensive therapy might be required, while holding them to account.
Summary
From the survey, the support needs of people who use violence included emotional and practical support delivered by a professional who they felt was competent. Participants wanted help regaining emotional control, to see things from a different perspective and for services to hear them and talk to them, not at them. From family and friends, perpetrators wanted a willingness to engage in deeper conversations and listen with an open mind. From victims’ and survivors’ perspectives, nothing was helpful other than removing themselves from the perpetrator’s reach. They thought if their partner could fear any consequences for their behaviour, something that was a wake-up call might turn their behaviours around. Finally, intensive therapy, while holding the partners to account, might also be helpful to stop them using abuse and violence.
Part E:
Children’s experiences and support needs
This part highlights what participants said about their children from the perspective of those who experience or use IPV and/or SV. The data is drawn from the open-ended survey questions with 500 victims and survivors and 288 people who used IPV and/or SV.
Victim and survivor perceptions
Victims and survivors who participated in the survey were asked to write about what had helped their children. Specifically, the question asked: “If you think about your partner’s/ex-partner’s behaviours towards you and your children, what has been most helpful for your children’s needs?” Below, we present our analysis of the themes evident in participants’ responses to the question with supporting quotations for each. Overall, our analysis suggests that many women felt there had been little assistance given to their children and that they were their children’s primary supporter and protector.
“The system has failed my children”
A major theme among participants’ responses was that no one had helped to protect or support their children. Many expressed that the service system had failed to adequately protect their children from the harmful impacts of the perpetrator’s behaviour. Feelings of powerlessness, frustration and despair were evident in many comments:
There is NO help, my child is repeatedly stating his father is going to kill him. Despite multiple notifications, we are yet to get any help.
The system has failed my kids. The police has failed my kids. We live in fear.
The children have not been helped at all. So many services enable ongoing abuse of them and me through coparenting … Everyone has been enablers. They don’t care. My [teenage] daughter was nearly choked by her dad – we have an AVO and family court orders suspended. But there were so many red flags and no one cared. Our case presented as high conflict couple … yet contact was tripled [by the court].
Linked with this theme was a perception that police, child protection and the family courts did not recognise that children were negatively affected by a perpetrator’s abuse of their mother:
I feel at a total loss in the existing system about how to do what’s best for my children. Australian family law assumes that intimate partner violence is only experienced by the survivor and that if the perpetrator was never violent towards children, then the children don’t need protection from him. I have felt too afraid and disempowered to act in their best interests.
I was unable to protect my children from their father[’]s
using them as pawns to distress me by neglecting and mistreating them. Police weren’t interested. Family court couldn’t get him to engage in mediation/counselling so that was that. Child protection said 12 was too old. If they were 5 they could investigate.
It was really hard to get anyone to believe my ex-partner hurt my child. Whilst in family court he said he only hurt the child accidentally, as I was using them as a human shield (breastfeeding a baby he went to kick me and got the baby in the head, there were other times etc.). I came across as erratic, because I felt like no one was listening and they were putting my child in danger.
Several participants said they became estranged from their children because they were not supported to stop the perpetrator’s damaging behaviour:
Nothing has helped. All the professionals abandoned us and I lost my children to him. I was able to get my oldest back recently after many years of separation.
A perception that children had been failed by the system was not only connected to the responses of courts or authorities. Many also said their children had been let down by the lack of therapeutic support to address the traumatic impacts of the abuse they had experienced. Limited availability and the expense of accessing counsellors with expertise in working with children was a significant concern; as one said: “There are not enough psychologists around to see children, the wait times are huge.” One participant commented that after four years, her children were still on a waiting list to see a free specialist counsellor.
Another problem that participants frequently identified was that the perpetrator was legally allowed to block their children’s access to support:
I see a counsellor who supports me to support my children, as they are unable to receive any direct support themselves (their father blocks any access to support).
I would never have coped had it not been for my daughter’s child psychologist. However, her father withdrew consent for her to continue her services (after my daughter disclosed family violence).
Other barriers were confidentiality issues and organisational policies, such as a requirement that children be safe and not living with the perpetrator in order to access counselling:
Not much [has helped my children]. My son won’t speak to anyone because his psychologist told his dad what they’d discussed and people didn’t believe him. Kids Helpline did not respond well.
A social worker from The Australian Childhood foundation [has helped]. But they cannot help unless you are no longer living with the perpetrator. And no help if the children still see them.
A mother who can support them
Participants suggested that their children’s wellbeing and safety was closely connected to their own; for instance, one commented that, “When mums feel unsafe and traumatised, our kids do too.” Thus, a key theme was that the main thing that helped and protected children was their mother being supported and free from the abuse. Two sub-themes were associated with this theme: “Me protecting them” and “Me being validated and supported”.
“Me protecting them”
A frequent perception among participants was that their own protective actions had improved their children’s wellbeing and safety. Many highlighted their decision to leave their partner and how they had tried to establish a secure and calm home environment:
Leaving my ex-husband was the best thing that I ever did for the protection of my children … I am hoping that when they are adults, I can explain what happened, and they will understand why I had to get them out of that household.
[What was most helpful for my children was] leaving him. Although this has also meant additional difficulties such as me being blamed (in conversation with the children by the abusive partner) for everything in the relationship that was not good … it also enabled the children to see who could provide them with a clean home, good meals, positive support for schooling … to see the contrast between what he said was true and what the reality … Separating meant when the children were with me I could focus on their needs and care.
Participants also spoke of protecting their children emotionally:
Standing my ground that I am the best and most reliable person in their lives and doing whatever I could to ensure this continued. Being flexible when the father let them down – i.e. being available to pick them up or whatever, no matter what. Being entirely reliable and supportive while they were forced to experience his lack of reliability.
However, leaving the perpetrator was not the only protective response that participants identified. Some commented that the only way to help protect their children was to comply with the perpetrator’s wishes, even though this had meant making a considerable sacrifice themselves. Participants mentioned a variety of strategies they were forced to use to keep their kids safe, including obeying the perpetrator’s demands, remaining in the relationship, and leaving but allowing the perpetrator to keep custody of their child.
Staying in the relationship was best to protect my children and avoid losing them.
Probably most helpful thing I did for my son is that I left without him so that he is safe even though he is with my ex-partner. Let my son to be aligned with his dad so that his enemy is just me.
Keeping the partner happy helps to keep the kids safe too.
“Me being validated and supported”
Participants frequently commented that being supported as a mother and a parent was what had been most helpful for their children. They suggested that they were in the best position to assist their children, but they could only do so if they maintained their own wellbeing. For instance, one said having emotional support meant she was able to support her children: “[What was most helpful for my children was] someone to listen to me to help reduce my anxiety which gives me more resilience to help the kids.”
The responses that participants said helped them to help their children included being believed and having their parenting validated, and assistance with safety planning, finances and managing the impacts of the abuse on their children:
[What was most helpful for my children was] me being supported and believed. Having the funds to hire a babysitter/activity person to give the children a change/break.
Me being supported to support them. Validation of my mothering which was impacted by family violence.
Counselling along with building our relationship again, giving them the power to choose or make some decisions to help them feel in control and lots of self-care.
We also asked survey participants about what could help their children, through the question: “If you think about your partner’s/ex-partner’s behaviours towards you and your children, what do you think services can do to best address your children’s needs?” We identified three themes: “Let them have a voice”, “Believe mothers instead of blaming them”, and “Recognise the impacts on children”.
Let them have a voice
The major theme evident in participants’ responses was that services needed to listen to children and prioritise children’s safety over the needs of the perpetrator. This included ensuring that the perpetrator’s needs and demands did not dominate decisions relating to child contact:
Services need to put the children’s voices at the forefront and put in place mechanisms that stop their voices from being drowned-out by the noise of an entitled, controlling and abusive male parent.
[Services need to] see him as the problem. Not force kids to go to their dad’s house if there has been abuse.
Participants emphasised the importance of hearing children’s views and wishes in relation to contact with the perpetrator. For example:
Listen to my child and empower him to speak up about what parenting arrangements suit him in future.
Actually, ask them how seeing their abuser makes them feel.
Believe mothers instead of blaming them
The second theme was that to best assist children, service providers needed to better support mothers. For example, one said: “Services need to support the one that is always there for them (nearly always the mother and certainly so in my case). DEFEND her when she needs it.”
Participants suggested they were willing and able to meet the needs of their children, but they needed material, legal and financial support to do so:
Services need to teach me how to ensure my experiences don’t affect them and their future relationships with others.
Services need to support mums like me with infrastructure and other needs – housing (I received no financial settlement and fell into extreme poverty).
Services need to help me with my mental health so they [children] can be loved properly.
Associated with this theme was a need to believe mothers, rather than blaming them for the abuse:
Stop blaming mothers. Hold perpetrator accountable and get him out of the house.
Believe your allegations. Victim blaming days should be long over by now.
Listen to mothers when they say they do not feel their child is safe.
There was also a strong perception that it was the perpetrator, rather than the victim and her children, who should suffer the consequences of the abuse:
Why do victims have to be uprooted and placed in shelters? … Funding should be going to police to give them more power to remove perpetrators and allow families, who are already traumatised, to remain in their homes.
Support children to address the impacts of IPV and/or SV
A third theme was that services needed to recognise that abuse by a partner not only affected the adult victim but could have traumatic impacts for children. Participants suggested children’s support needs were not adequately recognised by services. They emphasised that children needed psychologists and counsellors who had specialist expertise in IPV and abuse:
Psychologists need training in DV. My oldest daughter has had two psychologists who know nothing. One told her after 2 years of separation from a 32-year relationship that “mum and dad need to get over it. You[r] mother is wrong, she could have left.” The other has no idea of family dynamics.
[Services need to offer] counsellors, services and psychologists independent of the Family Law courts who understand DV and recognise that even though children weren’t directly abused or witnessed abuse of a parent, that abuse of a parent is emotional abuse and equally devastating to a child.
Greater access to low-cost children’s counsellors who could offer regular, long-term support was also highlighted:
Better access to child psychologists and more appointments available rather than once a month or every 2 months.
Give us counselling on how to deal with his ongoing behaviour. They will be mentally ruined by the time they’re 15.
Participants also suggested that the perpetrator should not be able to control the children’s access to therapeutic services:
Allow one parent to seek help for the children involved without the other[’]s permission. My ex has refused our children play therapy.
[Children need] services that don’t rely on both parents agreeing, my daughter needs counselling but because we co parent I have to tell him we are seeking support and get his approval. It’s crap.
[Children] need better access to support in school and I should not need both parents’ signatures for them to receive it.
Views of people who use IPV and/or SV on their children
To explore how people who had used violence or abuse perceived the support their children needed, we included the following two questions in our survey: “If you think about your behaviours towards your partner/ex-partner and children, how do you think your children have been affected?” and “If you think about your behaviours towards your partner/ex-partner, what do you think services can do to best address your children’s needs?”
Impact of IPV and/or SV on children
In response to our questions on the impact on children, it was evident that many felt their children were not significantly affected by the abusive behaviour. For example, one survey participant who acknowledged that he had been physically violent and was frequently verbally abusive said that he believed his children “are not affected too much by any of this”. Many expressed a belief their child/ren were unaffected because they had not seen any of the abuse or were too young to understand it. For example, one said “It’s not been obvious enough for them to notice”, and another said: “Counsellors have told us he is fine and he never witnessed [it].” Others said they had tried not to expose their children to their abusive behaviour. For example, one said: “I never raised my voice to my wife when the children were around”, and another commented: “Well, I don’t think it’s affecting him, at least we’ve tried our best to hide it from him.”
Other participants felt that their children had coped well and/or had managed to overcome any negative impacts of witnessing the abuse. The following comments from two participants illustrate this:
My son has been very resilient and forgiving for which I am blessed. He has also come out of it with a healthy respect for the women in his life and his expected behaviour towards them.
My irresponsibility with alcohol is something my daughter sees, and I do wonder what she’s thinking. Having said this, I don’t think it’s affected her much if at all.
However, some participants admitted that their abusive behaviour towards their partner had caused trauma or fear for their children. Several noticed that their children were upset or often afraid of being around them. For example:
I know my daughter is scared of me and I hear them cry when their mum and me fight.
They would have been worried and feeling helpless.
The kids were definitely wary around me when their mother lived with us. They became less so when she left.
My daughter wouldn’t understand but would be scared and become quiet.
Some expressed concern about how their children had been affected. For example:
[My children] have been afraid to confront me during times of anger, and this is saddening to me.
My kids will normally be traumatised but I will ensure I do everything to cancel that from their life and memory by showing love, empathy to my wife and kids.
Participants also expressed a fear that their children may suffer long-term consequences or replicate the same behaviour when they grew up. One said:
Whilst [my children] are only 7 and 5, which gives me a marginally pleasing mindset that they aren’t yet truly old enough to know exactly what is going on, I am seriously concerned that if I don’t sort myself out, their lives will be destined for failure, hardship, criminal offences etc.
Children’s support needs
Considering that many participants felt their children were not affected by their abusive behaviour, it was unsurprising that in response to our question about children’s support needs, a frequent comment was that their children did not need external support or help. However, some participants commented on what services could do to help their children and/or what they themselves could do. We identified the following two themes based on their responses.
Help me be a better parent
Some participants indicated that they needed to change in order to help their children. Although some indicated that they simply needed to be more careful about how they behaved in front of their children (for instance, one said he wanted to “reduce acts of violence in front of the child”), others identified a need for more substantial personal change. As one commented: “The more I can change my behaviour the better for everyone else.” This included becoming a better parent and role model, and repairing relationships with their partner and children:
[I need to] be a better father figure for them.
At the moment, I just want to focus on my wife and I making sure we become the best example for our kids in every way.
We are actually working at that currently, in fact I sent a letter of apology to my children in an effort of reconciliation (in conjunction with my counsellor).
A conversation and an explanation
The second theme was that children needed to have a reassuring conversation, in which they could share their feelings and be given an explanation for what was going on in their family. Some suggested that as a parent it was their role to engage in such a conversation, while others indicated their child needed a counsellor or someone external to the situation. For example:
[Services need to] give them a safe space to talk about their feelings and be heard.
[My children need] a service that gives them the confidentiality to speak freely and open up about how they feel.
[Services need to] talk to the children, ask them if they were okay.
Several commented that explaining why an adult might behave badly would be an important part of a supportive conversation.
[Services need to] explain to them that adults sometime are acting stupid.
[Services need to] just be supportive and explain that even grownups can get sick or do naughty things, but like all of us, can fix them!
Summary
There were stark differences between how victims and survivors view the impact of the violence and needs of the children compared to people who use IPV and/or SV. Victim and survivor participants frequently felt the system had failed their children who had been greatly impacted by their mother’s experience of IPV and/or SV, whereas many participants who had used IPV and/or SV did not identify a great impact on their children or any support needs for children arising from the IPV and/or SV.
Part F:
Discussion and implications for system improvement
Having people – not necessarily professional people – around you who believe in you and believe you … and are willing to support you through it all, I think that makes a huge difference.
(Victim and survivor participant)
Introduction
In this part we summarise the project findings for each group of participants and discuss them in the broader context of the literature. We highlight children’s needs and the impact of the COVID-19 pandemic. Drawing on the voices of women victims and survivors and people who use violence, as well as the available evidence base, we present integrated, whole-of-system recommendations to improve support and service engagement tailored to different stages of help-seeking.
Summary of findings in context
Women victims and survivors
We obtained survey data from 1,122 women who self-identified as having experienced IPV and/or SV in the previous five years. We also undertook in-depth qualitative interviews with 30 of these women. This data represents a valuable national snapshot of the abuse and violence experiences of women in Australia, highlighting patterns and types of violence and its impacts on health. Furthermore, both the quantitative and qualitative data illuminate their experiences of help-seeking, support needs and key areas where barriers to service delivery could be addressed.
Sociodemographic characteristics and experiences of IPV and/or SV
Our survey sample was largely representative of the broader Australian population of women in terms of age, education, location, marital status and whether they had children. Some key differences were that our sample was over-representative of Aboriginal and Torres Strait Islander women, but under-representative of women from migrant backgrounds as the survey was only available in English.
In terms of experiences of violence, over 80 per cent were currently afraid or had been afraid of a partner in the previous 12 months. Looking at lifetime experiences since age 16 years, poly-victimisation was common, particularly among Aboriginal and Torres Strait Islander women, women aged 25 to 45 years, and unemployed women, but less so among migrant women and younger women. Combined forms of IPV were commonly experienced (psychological, physical and/or sexual violence; 84.6%), highlighting the need to cease looking at one-dimensional types of abuse and rather to consider an overall pattern of abuse during a woman’s lifetime (Potter et al., 2020). Sexual violence was extremely common and often overlapped with psychological abuse, which is consistent with other research (Tarzia & Hegarty, 2022).
Of the women who reported IPV experiences, nearly one in three also reported experiencing reproductive coercion and abuse (RCA) which is higher than rates reported in other recent Australian research (Price et al., 2019). Almost all of the participants who had experienced RCA also reported combined physical, psychological and sexual violence, supporting the hypothesis that RCA is closely linked with fear and control in relationships (Tarzia & Hegarty, 2020). It is worth noting that one in three women experiencing IPV also reported technology-facilitated abuse and financial abuse in their lifetimes, highlighting the need to include these under-researched forms of IPV.
Child abuse and adverse childhood experiences were also common for two thirds of the victim and survivor participants, adding to the burden of trauma for women (Capaldi et al., 2012; Li et al., 2019). Overall, those who experienced abuse as a child and an adult had the highest health burden, and reported experiencing both mental health issues, poor general health and chronic conditions.
The vast majority of participants experienced PTSD, and two thirds experienced anxiety and depression, with half of participants living with disability or chronic illness limiting daily activities including employment (Figure 17). Aboriginal and Torres Strait Islander women and those who had difficulty managing on their available income had the highest burden (Blagg et al., 2022). The prevalence of health problems was consistent with the extant literature (Summers, 2022; World Health Organization, 2013a). In particular, the impacts of SV or reproductive coercion on women’s health were evident, highlighting the need for greater attention to be paid to these forms of violence (Tarzia, 2020; Tarzia & Hegarty, 2020). Aboriginal and Torres Strait Islander women andwomen who were unemployed or had difficulty managing on their available income also reported high rates of poor mental and physical health.
Figure 17: Percentage of participants (victims and survivors, and perpetrators) with health issues
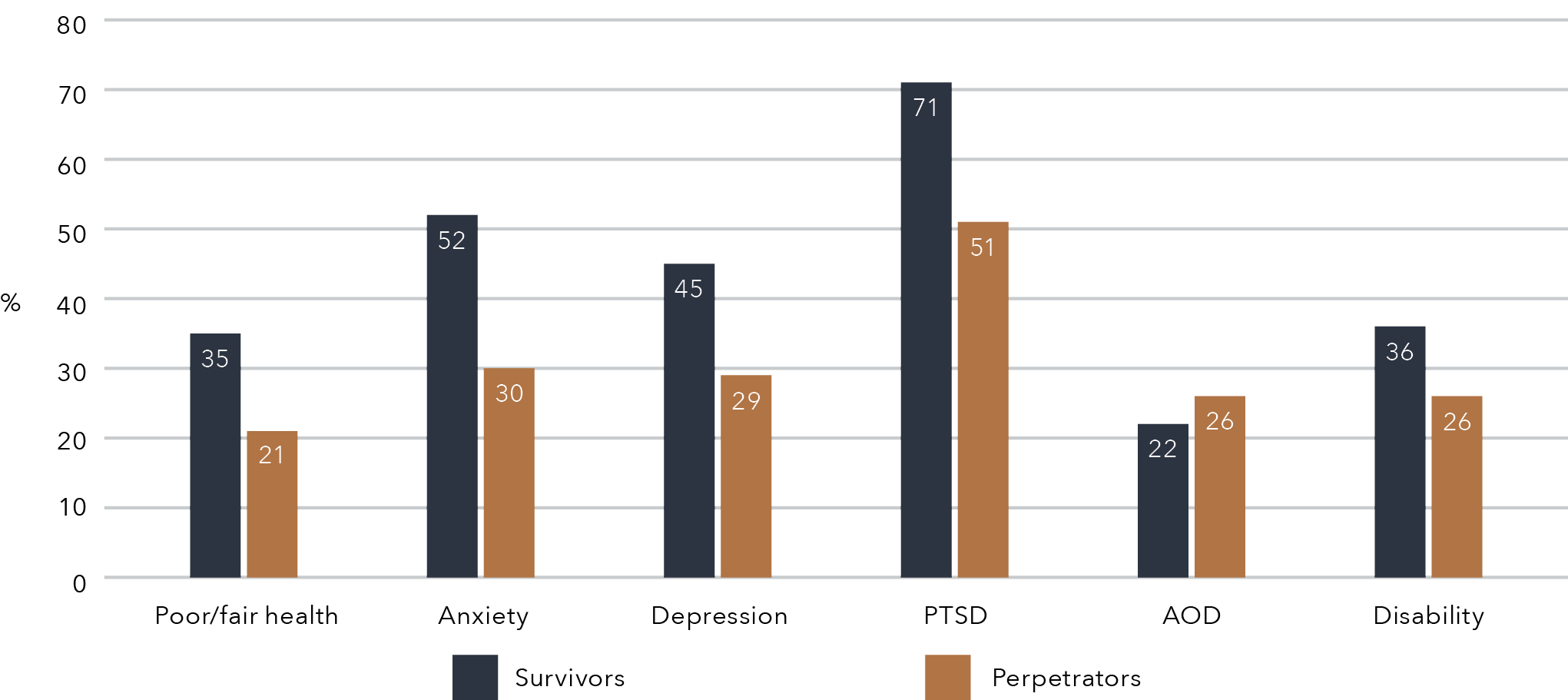
Data table for the figure above:
Health issues
Survivors
Perpetrators
Poor/fair health
35%
21%
Anxiety
52%
30%
Depression
45%
29%
PTSD
71%
51%
AOD
22%
26%
Disability
36%
26%
Figure 17 compares the health status of victim and survivor participants to those who used IPV and/or SV. It shows that a greater proportion of victims and survivors reported poor or fair health, anxiety, depression, PTSD or had a disability. The only factor that people who used IPV and/or SV reported slightly more was the use of alcohol or drugs, reported by 26 per cent, compared to 22 per cent of victims and survivors.
People who use IPV and/or SV
A key contribution of this project is that it is the first attempt nationally to capture the experiences of people who use IPV and/or SV. We obtained survey data from 563 people who self-identified as having caused a partner to be fearful and/or had used IPV and/or SV in the previous five years. We also undertook in-depth qualitative interviews with eight men drawn from the survey sample. The data we collected highlights patterns and types of violence and their associations with various health problems. Quantitative and qualitative data illuminates how people who use IPV and/or SV seek help, their support needs, and key areas where services could strengthen how they respond so that there is an appropriate balance of accountability with empathy.
Sociodemographic characteristics
The sample of people who had used violence was broadly representative of the Australian population in terms of being born in Australia, having children and living in a metropolitan area. The vast majority of the sample were men and most had a female partner. Some key areas of difference included age (with our sample being younger than the general population of men) and Aboriginal and Torres Strait Islander identity (nearly one in 10 participants in our sample). A larger proportion of participants had obtained a higher degree and more were currently employed compared with the broader population.
Despite having to indicate that they had used IPV and/or SV in order to be eligible for the study, only around half of participants met the criteria for having used IPV and/or SV during their adult lifetime, with 34 per cent reporting use of IPV and/or SV in the last 12 months. Just under one third of participants stated that they had made their partner afraid in the last 12 months, and almost three quarters had made a partner afraid at some point in their adult lives. Nearly 5 per cent of participants stated that they had perpetrated reproductive coercion – the first time Australian data has been collected on the perpetration of this form of violence.
Participants who were aged between 25 and 45 years, were Aboriginal and Torres Strait Islander or had difficulty managing on their available income were more likely to report perpetration of IPV and/or SV both over their lifetimes and within the previous 12 months. Younger participants were less likely to report use of violence.
Consistent with the literature (Kimber et al., 2018), child abuse experiences were frequently reported by those who had used IPV and/or SV. Participants who reported childhood abuse were three times more likely than other participants to perpetrate violence as an adult. Perpetration of IPV and/or SV was associated with poor general health, long-term illness, and other mental health problems, with stronger associations for those who had used violence more recently. Systematic reviews have similarly highlighted the associations between IPV perpetration and mental health problems (Oram et al., 2013), highlighting the need for early engagement through health settings.
The survey data from participants who used abuse or violence indicated that they had more violence against women–supportive attitudes compared with the broader Australian population, with those who met the criteria for IPV and/or SV perpetration reporting the strongest support for each negative attitudinal measure. This accords with other research showing that attitudes about gender and condoning or excusing violence are key drivers of violence against women (Webster et al., 2018).
Help-seeking of victims and survivors and people who use IPV and/or SV
The critical role of family and friends
Our survey data suggests that both women victims and survivors and people who use abuse or violence are most likely to seek help from their family or friends compared to formal support services (Figure 18). For victims and survivors, almost two thirds (64%) spoke about their abuse to family or friends, with younger women particularly likely to do so (Figure 18). Similar findings are evident in other Australian (Cox, 2016) and international studies (Sylaska & Edwards, 2014). Two thirds of women participants reported that the responses of family and friends were helpful.Similarly, more than half (59%) of the participants who used abuse or violence reported that they spoke to family or friends, and many (74%) found their responses helpful. Thus, family members and friends are in a critical position to provide assistance both to those subjected to IPV and/or SV and those who perpetrate it.
Our analysis of the victims’ and survivors’ open-ended survey responses provided some insight into the important role that family and friends can play in their help-seeking journeys. Fundamentally, women wanted their family and friends to be “on their side” and to understand their view of the situation, rather than taking the perspective of their abusive partner. An important aspect of this was listening, believing and validating the survivor, rather than judging them or their responses to the abuse. Similar findings have been identified in other studies with victims and survivors (McKenzie et al., 2022; Sylaska & Edwards, 2014; Taket et al., 2014; Trotter & Allen, 2009).
There were notable differences between what participants wanted from their family members and their friends. Victims and survivors frequently spoke of a wish for non-blaming responses from their family and described family members being disappointed or angry with them for the abuse. This may be because familial relationships are based on ongoing biological ties and an identification with one another. The behaviour of one family member may be seen to reflect on others, so family members may react more strongly and be more prepared to directly express blame if they perceive a victim has contributed to the abuse. In contrast to familial relationships, friendships tend to be voluntary and informal relationships that can be ended relatively easily (Rawlins, 2008), which may help to explain why the sub-theme “Stick by me” was associated with friends’ responses. Many participants spoke of wanting their friends to make an effort to maintain the friendship,and it was evident that for many, the perpetrator’s behaviour or how friends had responded to it had damaged the friendship. The sub-theme “step up, speak up and step in” was mainly associated with family members’ responses. Victims’ and survivors’ wish that family should “step up” when they needed them may reflect a social expectation that family members should be a reliable source of practical help, including assistance with finances or caring for children. The “speaking up” and “stepping in” aspects of the theme were connected with both family and friends and reflected a wish for family and friends to call out problematic behaviour or intervene if they witnessed it. Within the responses of victims and survivors about their wishes from family and friends were many examples of the kinds of reactions that they had received that they did not find helpful. It was evident that many experienced disbelief, blame or judgement from family and friends, and many spoke of theloss of friendships as a result of the abuse. This finding is consistent with other studies of victims and survivors, who frequently report receiving mixed responses from family and friends (McKenzie et al., 2022; Sylaska & Edwards, 2014; Taket et al., 2014; Trotter & Allen, 2009).
Many participants who used IPV and/or SV also indicated they were interested in having in-depth conversations with their family and friends about their relationships and wanted family and friends to listen with an open mind. Such conversations could potentially play an important role in helping to identify abusive behaviour and to support people on a pathway towards change. However, our findings also identified that many participants who used IPV found it difficult to engage their family and friends in serious discussions and often received responses that they perceived as dismissive or unhelpful. This accords with research with family and friends of perpetrators of IPV, who often report uncertainty in knowing how to respond (Latta & Goodman, 2011; McKenzie et al., 2022).
Together, our survey findings suggest guidance and education is needed for family and friends on how to be an ally for victims and survivors of IPV and how to respond effectively to someone who perpetrates IPV and/or SV. Unlike service providers, family and friends can be “on the side” of victims and survivors in an enduring way (Goodman & Smyth, 2011). Their emotional support and practical help can be critical as victims and survivors navigate a journey to safety and recovery from the abuse. Their responses also send powerful signals to the perpetrator as to whether or not their abusive behaviour is acceptable (Hydén, 2015; Klein, 2012). However, research indicates that often friends and family feel overwhelmed and unsure how to be helpful to victims and survivors (Gregory et al., 2017; McKenzie et al., 2022). They also struggle to know how to respond to a perpetrator of IPV and/or SV (Latta & Goodman, 2011; McKenzie et al., 2022). Thus,programs to equip family and friends to respond effectively to IPV and/or SV are essential in efforts to improve supports for victims and survivors and responses to perpetrators.
Formal help-seeking and journeys through the service system
Victim and survivor survey participants were more likely than those who used IPV and/or SV to seek support and legal assistance from formal service providers. For both groups, health professionals were the most frequently used formal source of help, being used by around half of the victims and survivors and a third of participants who used IPV and/or SV. This reiterates the key role that the health system plays in responding to IPV and/or SV and the importance of ensuring that practitioners are well-trained and ready to do this work (Garcia-Moreno et al., 2015; Oram et al., 2022) Victims and survivors less often also turned to specialist services (40%), police (31%) and legal services (19%), in contrast to participants who used IPV and/or SV (11%, 5% and 2% respectively). Figure 18 compares the proportion of participants who sought help from informal and formal supports.
Figure 18: Percentage of participants (victims and survivors, and perpetrators) who sought help
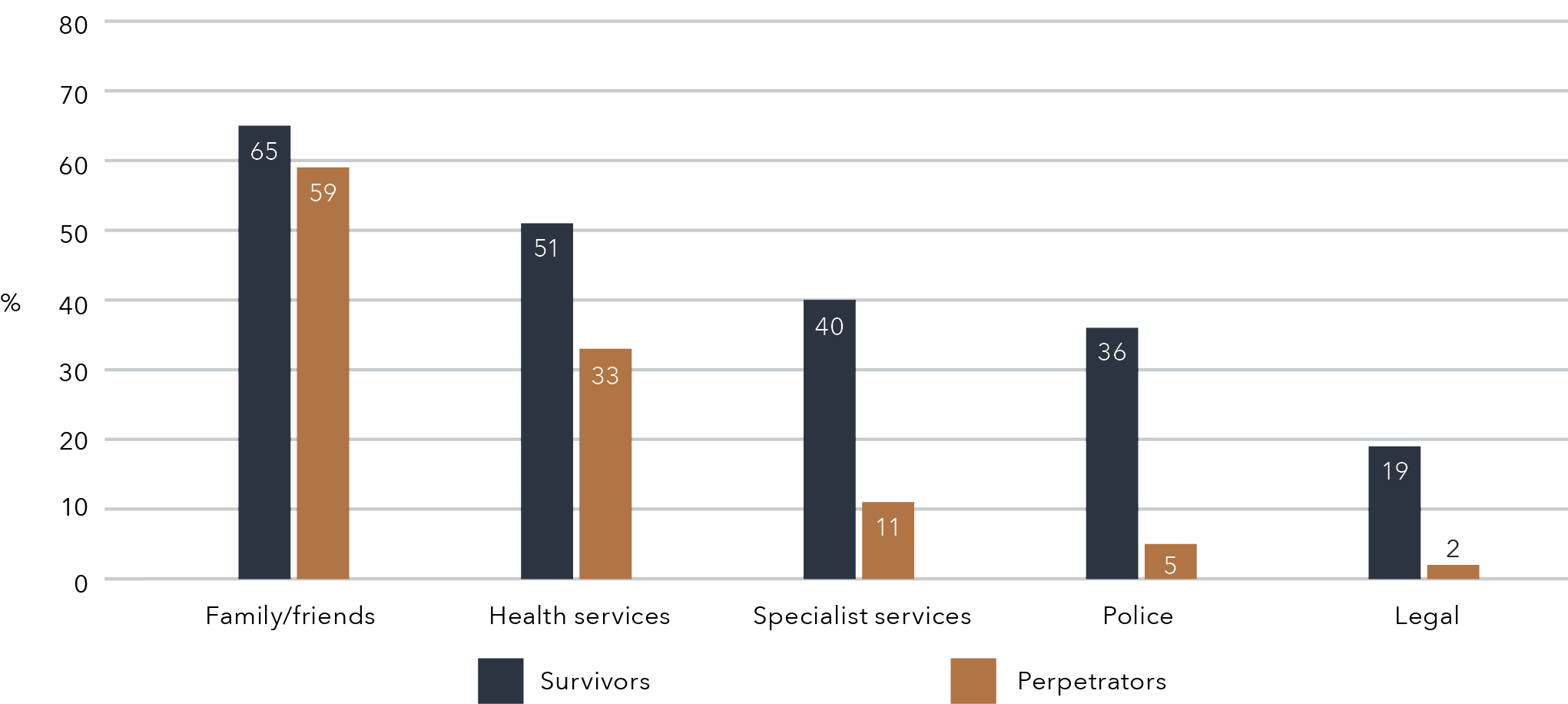
Data table for the figure above:
Type of help
Survivors
Perpetrators
Family/friends
65%
59%
Health services
51%
33%
Specialist services
40%
11%
Police
36%
5%
Legal
19%
2%
Help-seeking journeys through the service system for victims and survivors
As illustrated in Figure 18, most women victims and survivors had accessed at least one formal service (primarily health services), and more than half of them (59.6%) found their formal service contact helpful. Aboriginal and Torres Strait Islander women, women who had difficulty managing on their available income and women aged 25 to 45 years or no longer living with their partner were all over-represented as users of formal support compared with other women. This is likely to be because all these groups are more likely to experience a greater prevalence of IPV and/or SV (Australian Institute of Health and Welfare, 2018). Migrant and younger women were less likely to access formal support, which may suggest that there is greater stigma or additional barriersto accessing services for these groups of women (Tarzia et al., 2017; Vaughan et al., 2016).
Shame, lack of awareness about services or confidence in their ability to help were the most frequently reported barriers to accessing support. Women were also concerned about confidentiality. Nearly half of the participants said there had been a time they needed help for IPV and/or SV but could not get it, most commonly because of difficulty understanding the practitioner or a lack of available appointments. This communication barrier may partly explain the under-representation of migrant women in help-seeking via formal services.
Our analysis of help-seeking timelines and themes from our interviews with 30 victims and survivors provided a more nuanced insight into their help-seeking needs and their journeys through the service landscape. We identified five main stages of help-seeking: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; establishing independence and safety; and addressing impacts and making sense. These stages reflected victims’ and survivors’ particular needs or goals at different times. In the earlier stages, women needed empathetic listening, validation of their concerns, help to identify the abuse and options for support and safety. For many, the source of this help was a healthcare provider, such as a GP or mental health professional. However, not all victims and survivors received an empathic response when they sought help to understand the problems they were experiencing. Some described professionals focusingonly on mental health symptoms or diagnosis, while others said their abuse was misidentified as mutual conflict in the relationship. This highlights a critical need for health professionals to be competent to provide an effective first-line response.
Once women had recognised the abuse and sought to improve their safety, end the relationship or re-establish their independence, they frequently needed tangible and practical support – including housing, financial help and legal advice. However, they often found that there was little assistance available or that it was very complex to access. This finding underscores a need for greater government investment so that services can deliver the practical assistance that victims and survivors require to regain their safety, wellbeing and independence. Along with material help, a critical need was for someone to support, guide and advocate for victims and survivors as they navigated a very complex service system. Victims and survivors described already feeling overwhelmed by the abuse, and the long struggle to find assistance and having to repeatedly retell their story to different service providers only amplified their distress. Few found a professionalwho could act as an advocate to support them and “go into bat” for them to access the resources or legal protection they needed. Similar service gaps have been identified in the US (Campbell, 2021) and in the UK (Sullivan & Goodman, 2019).
Our interviews also identified that when women sought legal protection or to settle post-separation parenting or property arrangements, they were often left feeling that the perpetrator had only been emboldened in their abuse. Consistent with other Australian studies (Kaspiew et al., 2017), women reported that the family court in particular was an arena in which non-physical forms of IPV were misrecognised or minimised. There is an urgent need to foster increased competency in recognising and addressing IPV across the legal service system. Better recognition of coercive and controlling tactics is particularly pressing in the family courts to prevent perpetrators from using legal systems abuse and the deliberate manipulation of children to further harm a victim or survivor.
Women in our study also felt let down by a lack of accessible or appropriate help to recover from traumatic impacts and to make sense of the abuse they had experienced. They also felt psychologists and other mental health professionals tended to offer “textbook” responses, and it was difficult to locate a counsellor who was trauma-informed and IPV-trained. Similar findings have been identified in other studies with Australian victims and survivors (Marsden et al., 2021). Another important need that participants identified was to connect with other victims and survivors. Consistent with other research (Gregory et al., 2021; Osborn & Rajah, 2020), participants felt peer-based approaches reduced isolation and shifted the stigma of being victimised by a partner. However, opportunities for group-based support were limited and participants often felt service providers did not recognise the importance of peer support models.
Overall, the findings indicate that although women victims and survivors received support that was positive or helpful at different times, they felt they were “carrying the burden alone” in trying to address the abuse. The main message they felt the service system conveyed was that it was largely their responsibility to manage the perpetrator’s abuse and the consequences it had for themselves and their children. They perceived that the system was focused on crisis responses, while there was a lack of ongoing help to navigate through a maze of different services to find safety and recover from the IPV. There was also an emphasis on physical harm and immediate risks to safety, but less recognition of the impacts of other forms of abuse, including post-separation stalking and manipulation of the legal system and parenting arrangements. Similarly, women perceived that trauma-informed healing and recovery from the abuse they had experienced was not apriority for the service system. Services were overstretched and at each stage of their journey towards safety, victims and survivors did not always receive the legal, emotional or practical support they needed. Figure 19 illustrates women participants’ perceptions of the roadblocks and missed opportunities they encountered at each stage of their journey. Each of these contributed to a perception of being alone with the burden of ending and addressing the perpetrator’s abuse.
Yet, in women’s stories of help-seeking, there were also examples of responses from service providers that were positive or pivotal in meeting their support needs. Figure 20 illustrates the key responses at different stages that women perceived had made them and their children feel secure and supported.
Figure 19: Roadblocks and missed opportunities in victims’ and survivors’ journeys
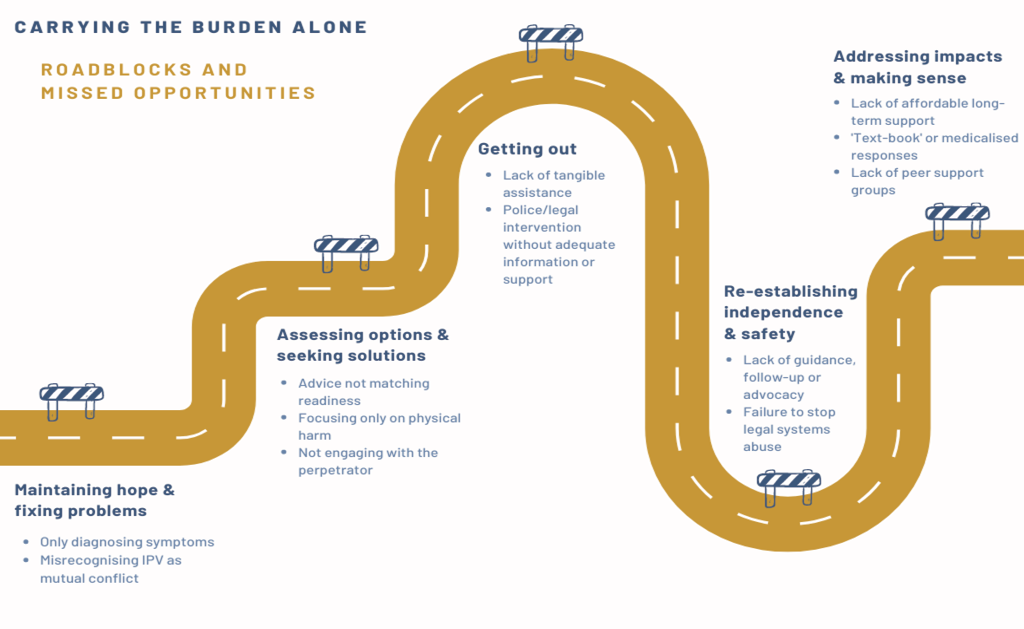
Text version of the figure above:
Carrying the Burden Alone
Roadblocks and Missed Opportunities
Maintaining hope & Fixing problems
- Only diagnosing symptoms
- Misrecognising IPV as mutual conflict
Assessing options and seeking solutions
- Advice not matching readiness
- Focusing only on physical harm
- Not engaging with the perpetrator
Getting out
- Lack of tangible assistance
- Police/legal intervention without adequate information or support
Re-establishing independence and safety
- Lack of guidance, follow-up or advocacy
- Failure to stop legal systems abuse
Addressing impacts and making sense
- Lack of affordable long-term support
- “Textbook” or medicalised response
- Lack of peer support groups
Figure 20: Positive or pivotal responses in victims’ and survivors’ journeys
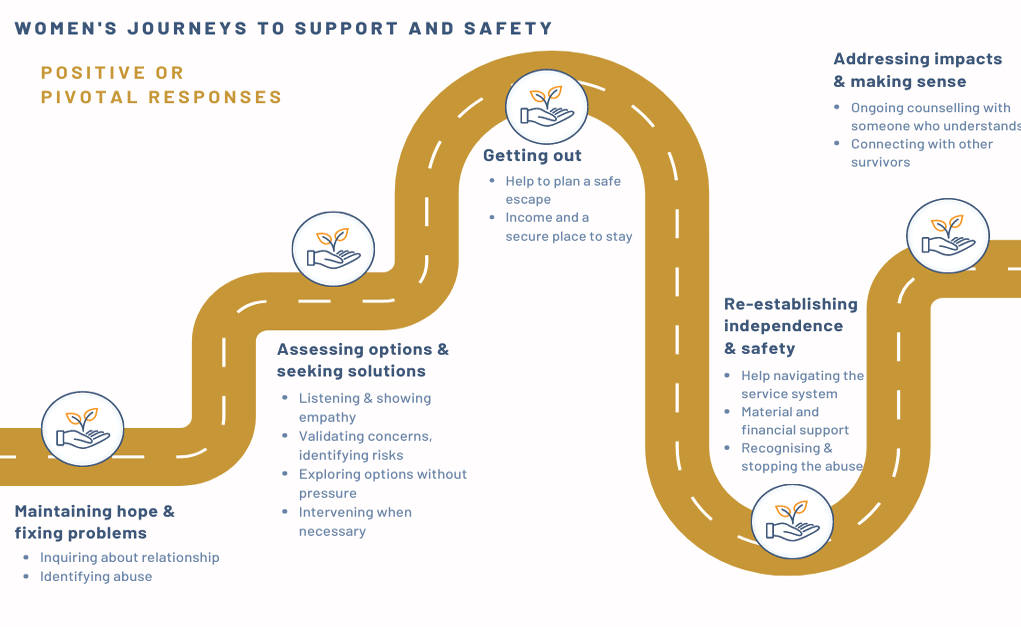
Text version of the figure above:
Women’s journeys to support and safety
Positive or pivotal responses
Maintaining hope & fixing problems
- Inquiring about relationships
- Identifying abuse
Assessing options & seeking solutions
- Listening & showing empathy
- Validating concerns, identifying risks
- Exploring options without pressure
- Intervening with necessary
Getting out
- Help to plan a safe escape
- Income and a secure place to stay
Re-establishing independence & safety
- Help navigating the service system
- Material and financial support
- Recognising and stopping the abuse
Addressing impacts and making sense
- Ongoing counselling with someone who understands
- Connecting with other survivors
Help-seeking journeys through the service system for people using IPV and/or SV
Slightly less than half of the survey participants (41%) had sought formal advice or support for their use of violence (Figure 18). As for the women victims and survivors, health services were the most frequently utilised avenue for formal support, with the majority finding these helpful. Specialist services and the justice system were less frequently accessed, most likely because they require identifying to some extent as a “perpetrator”. As the open-ended survey questions demonstrated, many of the participants strongly felt that they were not violent or abusive and therefore did not require support.
Aboriginal and Torres Strait Islander participants, those who had difficulty managing on available income, older participants, and those who had not completed Year 12 at school were over-represented among service users, whereas – as with the victims and survivors – participants from a migrant background were less likely to access formal services, highlighting the barriers these community members face (Segrave & Pfitzner, 2020; Vaughan et al., 2016).
Numerous barriers to accessing support were reported by participants using IPV and/or SV. Similar to the victims and survivors, shame was the most commonly reported barrier, followed by a belief that violence is a normal part of a relationship. Participants also reported access challenges similar to those described by victims and survivors, including concerns about confidentiality; lack of awareness of services; communication issues; and not having the time to talk to someone. For those participants who had sought help but been unable to get it, the most common barriers were lack of awareness about services; prohibitive costs; and long waiting times.
Our interview findings with men who had used violence similarly speak to the challenges around promoting early, effective help-seeking for perpetrators. We identified three stages across the men’s journeys through the service landscape: bottling things up; breaking down and letting things out; and regaining and maintaining control. Men’s support needs differed across each of these stages, with an overarching perception that they needed help to release and regain control of their emotions in order to stop using violence.
For most of the men, initial engagement with service providers occurred at a crisis point and was prompted by their partner deciding to leave them and/or contacting mental health services or the police. Participants felt this engagement was a catalyst for them to begin to change their problematic behaviour. The finding that help-seeking was prompted by a
“breaking point”, particularly relationship breakdown or a partner pushing them to engage with services, is consistent with other studies (Calcia et al., 2021; Davis et al., 2021). For example, a recent review of the literature on the help-seeking of perpetrators of IPV found that a perceived crisis and the threat of negative social outcomes (such as escalating abuse, criminal justice involvement, and a fear of losing or damaging relationships with children and partners) were common catalysts for their engagement with healthcare services (Calcia et al., 2021). Yet, if men’s motives are primarilyself-preservation or functional gain (such as regaining their relationship with their partner or avoiding legal sanctions), rather than deep personal reflection and transformation, then behaviour change may not be sustained (McGinn et al., 2020). Our findings help to demonstrate that the interventions of GPs, mental health professionals, police and others during times of crisis may be key initial steps to engage perpetrators on a “pathway towards accountability” (Campbell & Vlais, 2019). This accords with other Australian research that identifies that human services agencies, including mental health professionals, can play a key role in early interventions that help change abusive behaviours and violence-supportive attitudes (Chung et al., 2020).
As found in other research with men who have used IPV (Kelly & Westmarland, 2016), there was incongruence between participants’ reported behaviour in relationships and their self-perception. Almost all the participants suggested their abusive behaviour did not reflect their underlying beliefs or character, but was a reaction to external factors and circumstances, such as prior trauma and/or mental health problems, and/or a build-up of anger and strong emotions that were difficult to control. Thus, they framed the abuse as a “loss of control” that occurred when they were not rational and “not themselves”, rather than being a deliberate attempt at exerting control over their partner. In effect, this framing distanced them from responsibility for their behaviour. Further, although they suggested their mental distress and behaviour was problematic for themselves and their partner, they were reluctant to seek help. Masculinity was a barrier; manyattributed their help-seeking hesitancy to a perception that for men, vulnerability was shameful, which aligns with the quantitative survey findings. Taken together, this underscores the importance of shifting men’s perceptions that stigmatise help-seeking as “unmanly” and a reflection of personal weakness or failure (Levant, 2011; Vogel & Heath, 2016).
Support needs for victims and survivors of, and people who use, IPV and/or SV
Formal support needs of victims and survivors
Victim and survivor survey participants most valued the receipt of emotional support, including feeling listened to (91.7%), having someone to talk to (90.4%), and not feeling judged or put down (86.9%). These needs are consistent with evidence-based frameworks outlining recommended responses from services, such as LIVES (World Health Organization, 2014) and CARE (Tarzia, Bohren, et al., 2020).
Figure 21: LIVES recommendations for first-line response
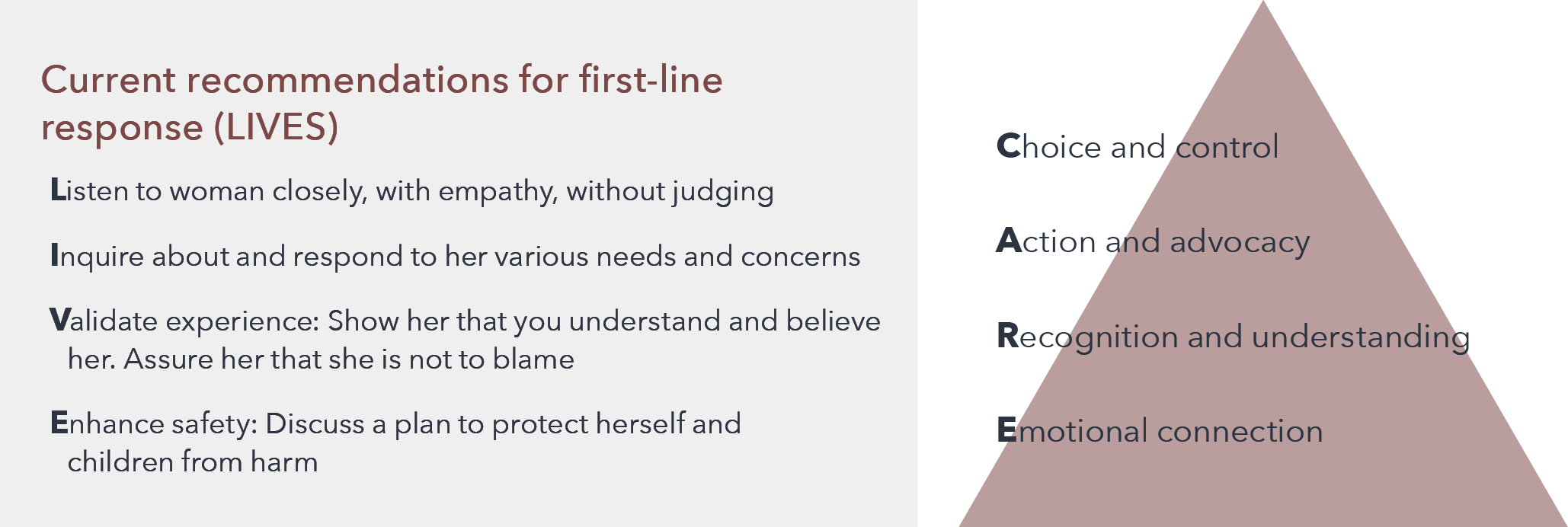
Text version of the figure above:
Current recommendations for the first-line response (LIVES)
- L – Listen to woman closely, with empathy, without judging
- I – Inquire about and respond to her various needs and concerns
- V – Validation experience: Show her that you understand and believe her. Assure her that she is not to blame
- E – Enhance safety: Discuss a plan to protect herself and children from harm
CARE
- C – Choice and control
- A – Action and advocacy
- R – Recognition and understanding
- E – Emotional connection
Similarly, the qualitative survey data highlighted women’s need to be taken seriously by service providers and have their concerns heard and validated. Women wanted support that was delivered empathetically, acknowledged them as individuals and was responsive to their particular needs. Yet, there was frequently a mismatch between what women wanted and what was offered. A lack of accessibility and availability was identified as a core problem across the service sector. Women described help not being available when they needed it, and they encountered long waiting lists and a limited availability of appointments when trying to access services. Participants also struggled with the fragmented and disconnected nature of the service sector. Many described challenges around having to access multiple services, being forced to repeatedly tell their stories, and feeling neglected after services were only available in the short term or service providersfailed to follow up with them. Finally, women were desperate for services to make the perpetrator stop the abuse. There was a sense of helplessness that services were unable or unwilling to hold the perpetrator accountable or to take meaningful action to keep women and their children safe. These themes were echoed across women’s stories of their help-seeking journeys, as identified by interview participants. Many said they felt alone in carrying the burden of addressing the abuse and recovering from its impacts on themselves and their children.
Support needs of Aboriginal and Torres Strait Islander women victims and survivors
Our survey identified that compared to other participants, Aboriginal and Torres Strait Islander women had a higher prevalence of experiencing multiple forms of victimisation in their lifetimes, including IPV, SV and child abuse. This is consistent with the findings of other studies (e.g. AIHW, 2018), and is influenced by intergenerational trauma, racism and discriminatory social policies and practices in the lives of Aboriginal and Torres Strait Islander women (Blagg et al., 2022). Survey participants who were Aboriginal and/or Torres Strait Islander were also over-represented as users of informal and formal supports (Fiolet et al., 2019). Other studies of Indigenous women globally identify a reluctance to seek formal help and a reliance on family and informal networks, though Indigenous women do seek formal help as a last resort in a crisis (as summarised in a review by Fiolet et al., 2019). This may have been the experience of participants inour study, or our findings may reflect Aboriginal and Torres Strait Islander women’s repeated attempts at help-seeking from different service providers over time. The higher rates of help-seeking by Aboriginal and Torres Strait Islander participants compared to other participants in our study may also relate to the impacts of social disadvantage. Other Australian studies have identified that women victims and survivors who were socially disadvantaged accessed more support than those in circumstances associated with social advantage (Cox, 2015). Our findings also show that those who had difficulty managing on available income were more likely to seek formal help.
Consistent with our findings, other research makes clear that Aboriginal and Torres Strait Islander women face considerable barriers in seeking appropriate support (Fiolet et al., 2019). Our interviews with Aboriginal and Torres Strait Islander women identified that fears of receiving racist responses and/or having their children removed from their care meant they were reluctant to engage with service providers and the legal system.
Aboriginal and Torres Strait Islander leaders have long identified the need for investment in community-led responses to domestic and family violence (Blagg et al., 2022; Carlson et al., 2021; Morgan et al., 2022). There has been a call for holistic healing approaches that recognise how the traumatic impacts of colonisation and systemic oppression of Aboriginal and Torres Strait Islander peoples shape women’s experiences of IPV and/or SV and their help-seeking (Blagg et al., 2022; Carlson et al., 2021). The importance of Aboriginal and Torres Strait Islander communities developing dedicated responses to abuse and violence has recently been acknowledged in the federal government’s draft National Plan. Our study lends further support for the need to resource community-led trauma- and healing-informed responses, given that our findings identify that Aboriginal and Torres Strait Islander women are at high risk of experiencing IPV and/or SV and facesignificant barriers in using mainstream support and legal services. Thus, we recommend that Aboriginal-led centres for healing be developed and be fully resourced in each state and territory.
Support needs for people who use IPV and/or SV
Participants in the survey suggested that their main support needs from services were learning new ways of dealing with relationship problems; feeling listened to; and having access to professional expertise. There was an expectation that the service provider would see them as an individual person and provide non-judgemental support.
Analysis of the open-text survey responses shed more light on the expectations and needs of people using violence. Participants said they wanted help to regain emotional control and reshape how they saw their behaviour and/or their partner, as described in the theme “help to see things from a new perspective”. Another important theme across participants’ responses was “hear me and talk to me, not at me”. This theme encapsulated a desire to have an open and honest conversation with a professional who listened, rather than lectured.
Consistent with the findings of a recent review (Calcia et al., 2021), our analysis of survey responses suggests that people who use IPV may be prepared to engage with support services to address their abuse. Although they had different perceptions about the kind of support they need, with some focusing on a need for help with emotional control and others wanting insight into how their thinking may contribute to their behaviour, participants consistently emphasised that they wanted someone they could open up to who could listen with empathy. Feeling listened to was also identified as a facilitator of disclosure of the use of IPV in other studies (Calcia et al., 2021). As mentioned in our discussion of findings from our interviews with people who used IPV, this highlights the importance of service providers – particularly health and mental health professionals – having the skills to engage empathically with people who use IPV, while encouraging themto take responsibility for their choices and change their behaviour.
Victims’ and survivors’ views of what perpetrators need to stop using IPV and/or SV
Some argue that compared to the person using violence, victims and survivors have a more “objective” perspective on the perpetrator’s behaviour (McGinn et al., 2016). Indeed, our analysis of open-ended survey responses from victims and survivors indicated that changing the perpetrator to stop their abuse would be a long and intensive process, and some felt that the perpetrator would never change. Many participants found that nothing had prompted the perpetrator to stop the abuse, other than the survivor ending the relationship and removing themselves from contact with the perpetrator. For some, legal consequences had curtailed the abuse to some extent. Similar findings were identified in a systematic review of studies with women whose partners attended behaviour change programs (McGinn et al., 2016). Some victims and survivors in our study felt change was possible and suggested that what the perpetrator needed was a “wake-up call” from others torecognise their problematic behaviour, intensive therapy to address underlying or contributing personal issues (along with contact with the victim and survivor to understand their side of the story), and strong mechanisms to hold them accountable for stopping the abuse.
Comparing the survey responses of people who used IPV and/or SV and the responses of victims and survivors, it was evident that there were some overlaps in participants’ perceptions of what was needed to change abusive behaviour. Both groups identified that therapy or counselling for the perpetrator may be beneficial, though victims and survivors emphasised such conversations needed to be undertaken in consultation with the victims and survivors and should be ongoing and intensive. Some victims and survivors said the perpetrator should be mandated to attend. In contrast, people who used IPV and/or SV suggested they were voluntarily prepared to seek help to help manage their emotions and/or gain insight into their behaviour. Similarly, while both groups of participants suggested that having others provide a new perspective on the abusive behaviour was important, victims and survivors suggested this change in thinking needed to be prompted byprofessionals, friends, family members and other community members (particularly men) intervening with the perpetrator and calling out their abusive behaviour. Victims and survivors also emphasised a need for professionals and authorities to hold the perpetrator to account by applying restrictions and legal consequences if they continued to use abuse or violence. Similar findings were identified by McGinn et al. (2020; 2016), who undertook a review of research on perpetrators’ perceptions of engaging in behaviour change programs, following an earlier review of victims’ and survivors’ experiences of men’s behaviour change programs. The authors found that perpetrators highlighted their internal motivations for change, while victims and survivors spoke of change being initiated by external forces and the importance of legal and other measures to hold the perpetrator accountable (McGinn et al., 2020; McGinn et al., 2016).
Our findings suggest that victims and survivors perceive that a range of external actors can play a role in holding the perpetrator responsible for their behaviour, including friends, family and other community members who can “call out” the abuse or violence; professionals who provide therapy or treatment; and police and courts that can implement restrictions and consequences. Thus, in our recommendations, we identify a need to build capacity across the community on how to effectively intervene, which will help create a “web of accountability” around the perpetrator (Chung et al., 2020). This includes training for family and friends and education to foster the competence of GPs, mental health services and other professionals to respond.
Children’s needs in the context of adult IPV and/or SV
Perceptions of women victims and survivors
Our analysis of open-ended survey responses indicated that women recognised that their children had been significantly affected by the IPV but felt legal and support services had failed to protect them or to address the impacts of the abuse on their children’s wellbeing. A key concern was the family courts enabling perpetrators to use children as pawns in the abuse or to block children’s access to support programs. The findings echo those of Kaspiew et al. (2017), who found that women frequently reported negative experiences in the Australian family courts and that their children’s safety and wellbeing was compromised as a result. Participants in our survey emphasised a connection between their children’s safety and their own and the importance of resourcing and supporting them so they could care for and protect their children. They also identified a lack of therapeutic support available to help their children deal with the trauma of
the abuse.
As other studies have identified, perpetrators of IPV often deliberately sabotage the relationship between mothers and their children as a tactic of their abuse (Humphreys, Kertesz, et al., 2019; Humphreys et al., 2015; Lévesque et al., 2021). However, historically, courts, child protection authorities and welfare professionals have often failed to recognise how IPV affects women’s abilities to parent and protect their children; instead, women have been judged and held responsible for the impacts of the IPV on their children (Humphreys, Kertesz, et al., 2019). The responses of victims and survivors in our survey make clear that partnering with mothers to support and protect their children is a critical approach to improve children’s safety and wellbeing. Survey participants identified that the best ways that children could be supported were by listening to and believing their mothers and helping mothers to obtain the legal protection, safe housingand financial support they needed to create a secure home for their children. However, participants also emphasised the importance of recognising that children have needs that are separate to those of their parents. Thus, other key themes in participants’ responses were a need for children to be given a voice in court proceedings and to have access to counselling or support programs to address the trauma of living with IPV.
Perceptions of people who use violence
In contrast to victim and survivor survey participants, those who used abuse or violence frequently felt that their children were unaffected by their abuse or violence and therefore did not need support to address it. However, some participants did identify signs of their children’s fear or distress, which is consistent with literature that consistently identifies that children’s emotional, social and behavioural development can be significantly impacted by IPV (Humphreys & Campo, 2017; Humphreys, Diemer, et al., 2019; Lamb et al., 2018). Recognition of the impacts on children is an important area for interventions to target, given that studies suggest concern about damaging or losing their relationships with children can be a key motivator for perpetrators to change their behaviour (Meyer, 2018). Encouragingly, some identified that getting support for themselves to be a better parent would be helpful for their children. Some surveyparticipants who had used IPV and/or SV also said that their children should have the opportunity to share their feelings with a professional and be given an explanation for the abusive behaviour.
The importance of support for children was a strong theme for victims and survivor participants, along with giving children a voice in court decisions. Thus, we recommend that a key principle across the service system is listening to children’s voices and offering children therapeutic support to address the impacts of the abuse and violence in their lives (see “Recommendations for policy and practice”). Further, considering that our findings and those of other studies (Li et al., 2020) suggest that people who use IPV and/or SV may be more likely than others to have experienced child abuse themselves, providing a timely early intervention to address experiences of abuse or violence in childhood may help prevent perpetration in later life.
The impacts of the COVID-19 pandemic
Women’s written responses to our survey questions about the impacts of the COVID-19 pandemic suggested that many of their experiences of abuse intensified during this period. This finding is consistent with other Australian (Boxall et al., 2020; Carrington et al., 2021; Morgan et al., 2022; Pfitzner et al., 2022) and international research (Piquero et al., 2021). An increase in abusive behaviour during the pandemic was also a key theme among survey participants who had used IPV and/or SV. While those participants suggested this escalation was due to external pressures on them, such as increased financial and mental stress, many victim and survivor participants connected it to them being socially isolated and trapped at home, affording the perpetrator more opportunities to target them.
While victims and survivors said their partner or ex-partner’s abuse had increased, they also said it was more difficult for them to access support and find safety. This accords with the findings of a recent Australian study, which showed that victims and survivors were less likely to report their abuse to the police when stay-at-home measures were introduced (Morgan et al., 2022). As other researchers have argued, social isolation, increased time spent at home with the perpetrator, the loss of employment and difficulties accessing services created a “perfect storm” that made many IPV victims and survivors vulnerable to escalating abuse (Usher et al., 2020). However, our analysis of survey responses also uncovered evidence of positive change in victims’ and survivors’ lives due to the pandemic. Some participants in our study suggested the emergence of the pandemic led them to acknowledge their partner’s mistreatment and to take action. Others saidthe increase in the availability of phone or telehealth services improved their access to support, particularly for those who had transportation difficulties, lived a long distance from services or needed support after hours. However, some felt that online or telehealth services were less personal or too risky or difficult to use with children or the perpetrator present in the home.
Similarly, for participants who used IPV and/or SV, there were some positive findings about the impacts of the COVID-19 pandemic. Some people reported that pandemic restrictions gave them more time to reflect on their behaviour towards their partner. Participants also said that they found it easier to seek help because support services were heavily advertised and/or became more convenient to use with the increase in video or telehealth service delivery.
Together, the survey findings from victims and survivors and people who used IPV and/or SV highlight that during times of extreme social turbulence, such as in a pandemic or a natural disaster, the delivery of support services for IPV and SV should be prioritised and increased. There is also a need to establish new and creative ways of delivering services, particularly when access to face-to-face support is restricted. An important finding was that even when lockdowns are not in place, telehealth and phone services can still provide an important alternative to in-person services for those who find it challenging to access services due to distance, transportation, or an inability to access services during business hours. This finding was echoed in a recent review of the literature on mental health interventions for IPV victims and survivors during COVID-19 (Su et al., 2021). However, researchers also caution that such responses should not replacetraditional face-to-face delivery, considering that some people face significant barriers accessing technology-based services, including those who are on a low income, experiencing homelessness, or living in areas where there is poor internet access (Baird et al., 2022). Further, our findings, along with other research (Pentaraki & Speake, 2020), show that when social restrictions are in place and women victims spend more time with the perpetrator or their children, it may be difficult or risky to access support via phone or online. It is also important to recognise that perpetrators may be able to remotely monitor a victim’s use of communication via technology, even when pandemic-related restrictions are not in place (Pentaraki & Speake, 2020). However, we recommend telehealth and online services should continue to be provided as an adjunct to face-to-face options, as they provide greater flexibility of access to support.
What works from the perspective of women in terms of service responses for themselves, their children and the perpetrator?
We have summarised our findings according to the help-seeking journeys women undertake and mapped what participants told us about what might work to improve the system overall and at different stages (Figure 22). It is clear that the normalisation of violence and abuse in relationships – particularly non-physical forms – is common across the community and can mean victims and survivors find it difficult to identify the abuse they are experiencing. Thus, universal education across the community may assist victims and survivors and people who use IPV and/or SV to recognise the signs of an abusive relationship, including sexual, psychological and other forms of abuse. Shame and a lack of awareness of the services that can assist are also major barriers to help-seeking, requiring greater promotion of the services that are available. Hence, we recommend increased community messaging about the availability of accessible and confidential support services,including national helplines for IPV and/or SV. Additionally, messaging should counter the victim-blaming attitudes that remain common in the Australian community, so that victims and survivors are supported, rather than judged, when they seek informal or formal assistance.
The program “Change that Lasts” in Wales is an example of a broad-based community response approach, similar to our recommendations. It consists of “Ask Me” training for “community ambassadors” to improve awareness, understanding and responses within the wider community; ”Trusted Professional Training” to enable non-specialist professionals to identify and respond better to victims and survivors and perpetrators; and ”Specialist Support Services Provision”, which involves needs-led, trauma-informed specialist services for victims and survivors. Finally, ”CLEAR” (Change that Lasts Early Awareness Raising) is a course working with those using abusive behaviours at an early stage (see ”Make a Change” box in the section on what works for perpetrators).
Given that both victims and survivors and people who use IPV and/or SV tend to rely on their family members and friends for help, there needs to be a greater focus on equipping family and friends to respond. Supportive responses from family and friends can also lead women to seek further help from service providers (Evans & Feder, 2016); thus, friends, family and other informal sources can play a critical role in early engagement in formal help-seeking. However, our findings suggested family members and friends were not always helpful or “on the side” of the victim and survivor. Hence, we have made recommendations for training for family and friends to be developed and made widely available online and through community groups so they can understand how to be an effective ally to a victim and survivor. In addition, training in “healthy relationship first aid” could be promoted in all workplaces and faith-based organisations to enable a helpfulfirst-line response.
Considering that health services, in particular general practice and private and public mental health services, were frequently used as sources of support for victims and survivors and for those who used IPV and/or SV, the upskilling of those professionals should be made a priority. Similar calls for action in the health and mental health sectors have been made by the WHO (2013b), the Lancet Psychiatry Commission (Oram et al., 2022) and the Medical Journal of Australia (Hegarty et al., 2022). There has been significant work in this area that demonstrates how the health system needs to be changed to deliver trauma- and violence-informed care (Hegarty et al., 2022).
Our findings also indicate that victims and survivors not only require improved responses from service providers, but also greater access to financial and material support. For example, our survey identified an association between unemployment and an increased likelihood of experiencing multiple types of abuse across the lifespan (such as child abuse, IPV and/or SV). Research suggests that being on a low income or experiencing unemployment is often a consequence of victimisation and, further, women’s financial insecurity may be exploited by a perpetrator as part of their abuse (Cortis & Bullen, 2016). Many women fall into poverty after separating from an abusive partner (Summers, 2022), which may help to explain why our survey identified an association between having an insufficient income and increased help-seeking from financial, justice and specialist services. Additionally, for victims and survivors, having difficulty managing on theiravailable income was associated with poorer physical and mental health, which may also have contributed to their increased levels of help-seeking from health services. Interview participants also highlighted that a lack of access to income narrowed their choices and prolonged the danger they faced, with some saying that a lack of financial support and accommodation meant they had to remain with or return to an abusive partner. Given these findings, it is essential that governments adequately fund the financial and income support victims and survivors need to leave abusive partners and re-establish their independence and safety.
Another critical need of victims and survivors who participated in our survey and interviews was for someone to support and advocate for them as they navigated the service system. This need has been identified elsewhere. For example, in the United States, Sullivan and Goodman (2019) highlighted the importance of trauma-informed advocacy – an approach that recognises the impacts of trauma on help-seeking and validates victims’ and survivors’ and partners with them to regain control over their lives. Such an approach differs to “case management” in that it emphasises a victim and survivor–led orientation. We suggest a similar approach needs to be adequately resourced in Australia. As discussed in our recommendations below, “care navigators” need to be appointed to ensure women have accessible long-term support and advocacy as they journey through the service system. As identified in a recent review, it is also important to recognise the complexity ofadvocacy work and the need to tailor interventions to women with differing backgrounds and needs (Rivas et al., 2019). Thus, it is critical to ensure care navigators are well resourced and provided with ongoing professional training and emotional support.
Our recommendations also highlight a need to shift the orientation of the domestic violence service system from crisis and immediate risk to a recognition of the long-term impacts of IPV. Victims and survivors in our study frequently reported a lack of accessible or affordable support to recover from the traumatic impacts of the abuse. Many also said that when they were able to access mental health services or other support, often service providers lacked the skills and understanding to meet their needs. Victim and survivor participants also emphasised the value of peer-based support from other survivors, which was profoundly helpful in reducing stigma and isolation. Thus, we not only recommend a need for professional competency for mental health service providers and the increased delivery of trauma recovery and healing services, but also the funding of group-based peer support models.
Together, our recommendations highlight that whole-of-system and whole-of-community change is needed, rather than altering specific aspects in isolation (such as the training of staff in specific sectors only). For victims and survivors, this will mean that rather than feeling alone in carrying the burden of addressing the abuse, they feel that no matter who they speak to about their experiences, they will receive a supportive and non-judgemental response.
Critically, the service system needs to have the skills and capacity to respond to the individual needs of victims and survivors with different experiences, circumstances and backgrounds (consistent with the theme “recognise me as an individual person”, identified in our analysis of qualitative survey data from victims and survivors). This requires an intersectional understanding of IPV and/or SV (Kulkarni, 2019), which recognises how victimisation and help-seeking are influenced by the impacts of marginalisation and oppression based on race, ethnicity, sexuality, age, ability, class, geography and other factors (Shimmin et al., 2017). It also requires an understanding of how the impacts of adverse or abusive experiences in childhood may be compounded by being subjected to IPV and/or SV in adulthood. This is important considering that many victims and survivors in our survey had multiple experiences of victimisation across the lifespan, which hasalso been found in other studies (Capaldi et al., 2012; Li et al., 2019). Several factors are key to sustaining a transformed approach across the service system and community: committed leadership; regular training (with mandatory attendance) of staff, from front-desk workers to those who see victims and survivors; on-site trainers; and clear referral pathways. We need a gender-responsive, culturally safe, trauma- and violence-informed, and contextually tailored system for all victims and survivors.
It is also important to acknowledge that while victims and survivors should be able to get the help they need, only focusing on improving help-seeking and providing support risks putting the onus on the victim and survivor to stop the abuse. Thus, a fundamental concern of policy and practice must be on strategies to end the use of violence by those who perpetrate it. In the next section, we summarise our findings on what may assist to stop the perpetration of IPV and/or SV.
“Make a Change” has been developed by Respect in partnership with Women’s Aid Federation England (inspired by the “Change That Lasts” approach described above in the victims and survivors section).
The model aims to address abusive behaviour at an earlier stage, before it becomes entrenched. It offers direct support to people who are concerned that their behaviour towards a partner or ex-partner has been controlling, frightening or harmful. It also provides separate and confidential support to their partners and/or ex-partners, and awareness-raising activities with local communities and training for professionals.
Figure 22: Summary of journeys and help-seeking for victims and survivors
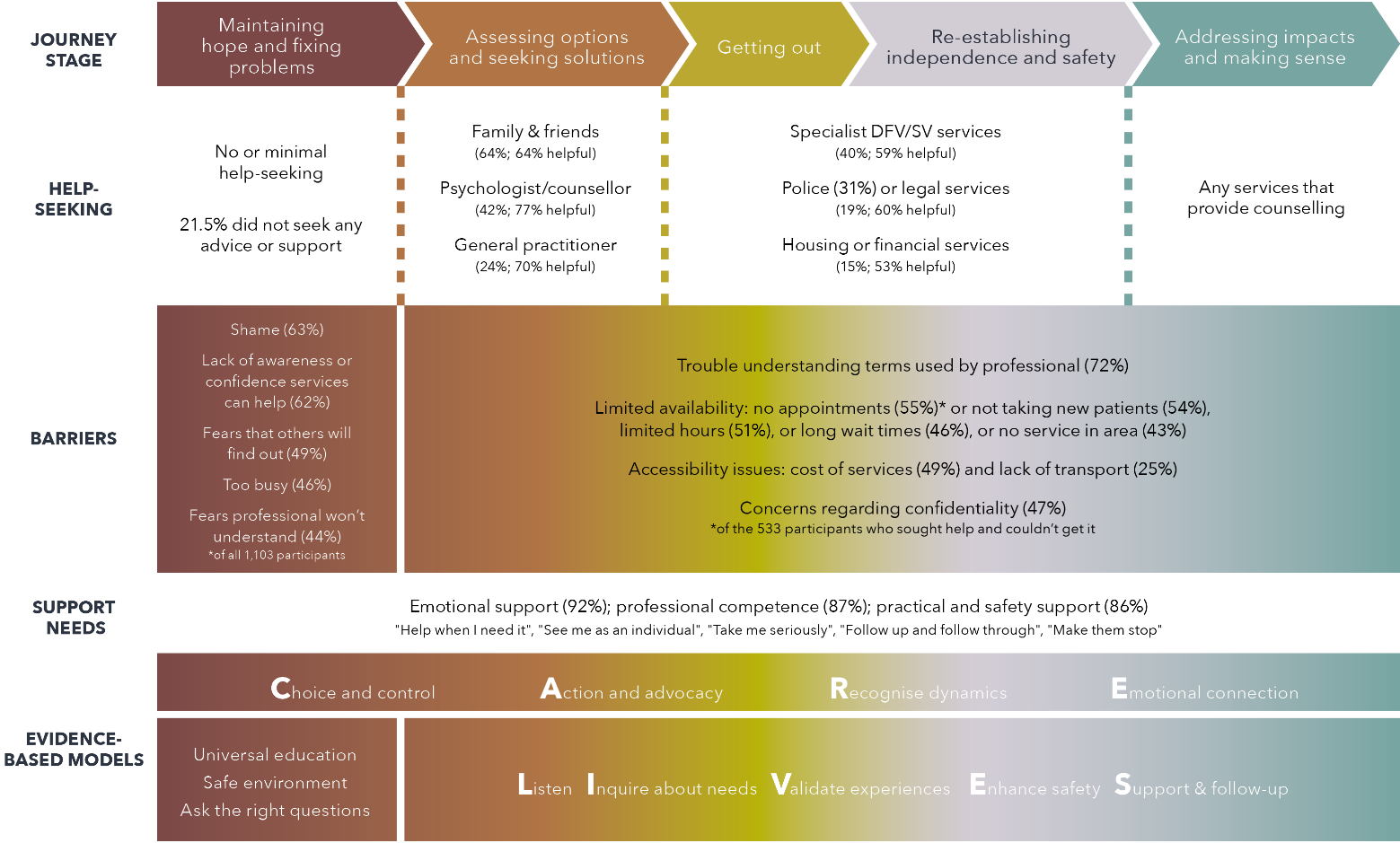
Text version of the figure above:
Journey stage
- Maintaining hope and fixing problems
- Assessing options and seeking solutions
- Getting out
- Re-establishing independence and safety
- Addressing impacts and making sense
Help-seeking
- Journey stage 1:
-
- No or minimal help-seeking. 21.5% did not seek any advice or support
- Journey stage 2:
-
- Family & Friends (64%; 64% helpful). Psychologist / counsellor (42%; 77% helpful)
- General practitioner (24%; 70% helpful)
- Journey stage 3 and 4:
-
- Specialist DFV/SV services (40%; 59% helpful)
- Police (31%) or legal services (19%; 60% helpful)
- Housing or financial services (15%; 53% helpful)
- Journey stage 5:
-
- Any services that provide counselling
Barriers
- Journey stage 1:
-
- Shame (63%)
- Lack of awareness of confidence services can help (62%)
- Fears that others will find out (49%)
- Too busy (46%)
- Fears professional won’t understand (44%) *of all 1,103 participants
- Journey stage 2 to 5:
-
- Trouble understanding terms used by professional (72%)
- Limited availability: no appointments (55%)* or not taking new patients (54%), limited hours (51%), or long wait times (46%), or no service in area ( 43%)
-
- * of the 533 participants who sought help and couldn’t get it
Support needs
- Emotional support (92%); professional competence (87%); practical and safety support (86%)
-
- “Help when I need it”, “See me as an individual”, ‘Take me seriously”, “Follow up and follow through”, “Make them stop”
- Journey stages 1 to 5:
-
- C.A.R.E – Choice and control, Action and advocacy, Recognise dynamics, Emotional connection
Evidence-based models
- Journey stage 1:
-
- Universal education
- Safe environment
- Ask the right questions
- Journey stages 2 to 5:
-
- L.I.V.E.S – Listen, Inquire about needs, Validate experiences, Enhance safety, Support & follow-up
What works from the perspective of perpetrators in terms of service responses?
For a summary of journeys and help-seeking for people who use IPV and/or SV, see Figure 23.
Figure 23: Summary of journeys and help-seeking for people who use IPV and/or SV
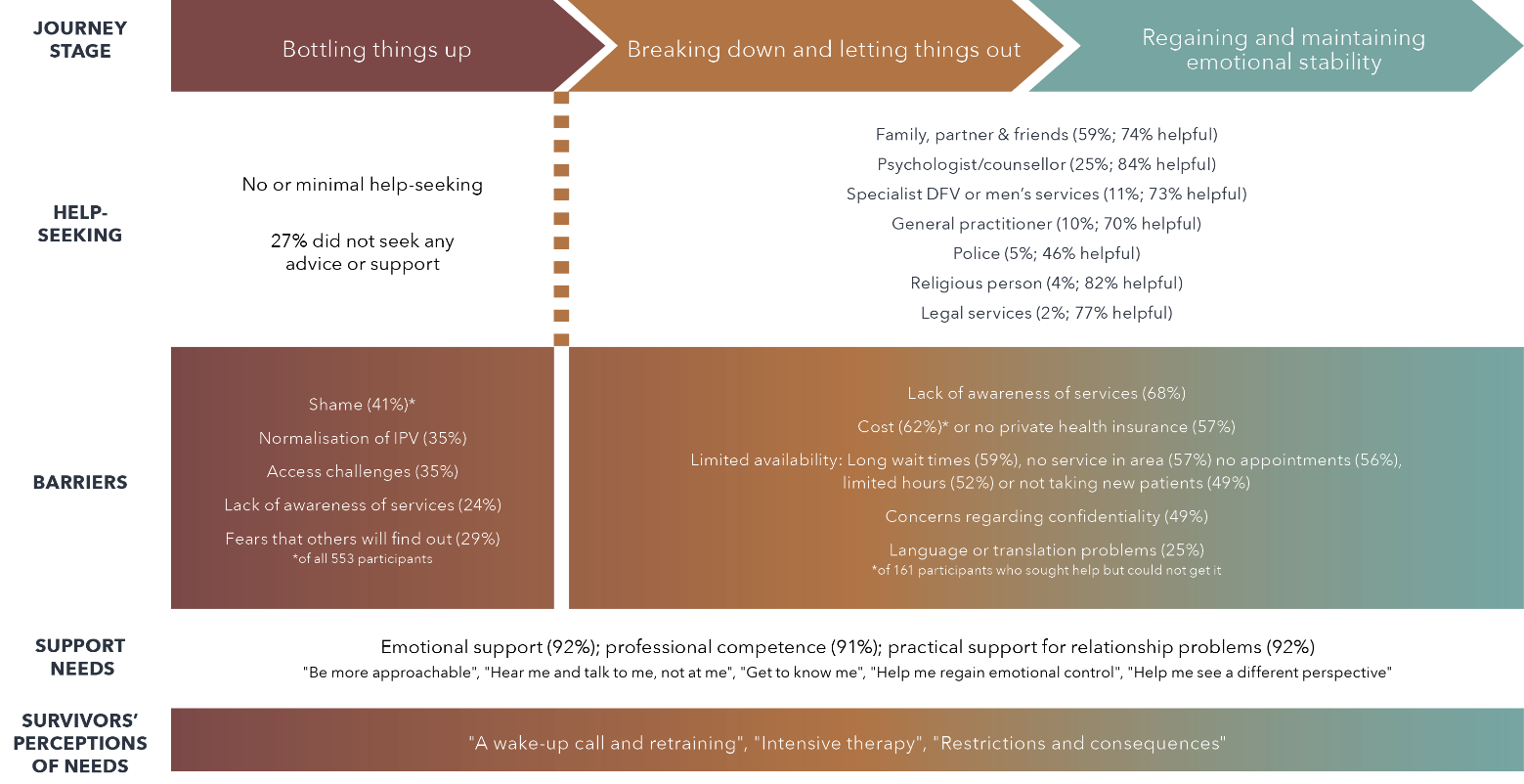
Text version of the figure above:
Journey stage:
- Bottling things up
- Breaking down and letting things out
- Regaining and maintaining emotional stability
Help-seeking:
- Journey stage 1:
-
- No or minimal help-seeking
- 27% did not seek any advice or support
- Journey stages 2 and 3:
- Family, partner & friends (59%; 75% helpful)
- Psychologist / counsellor (25%; 84% helpful)
- Specialist DFV or men’s services (11%; 73% helpful)
- General practitioner (10%; 70% helpful)
- Police (5%; 46% helpful)
- Religious person (4%; 82% helpful)
- Legal services (2%; 77% helpful)
Barriers:
- Journey stage 1:
-
- Shame (41%) of all 554 participants
- Normalisation of IPV (35%)
- Access challenges (35%)
- Lack of awareness of services (24%)
- Fears that others will find out (29%)
- Journey stages 2 and 3:
- Lack of awareness of services (68%)
- Cost (62%) of 161 participants who sought help but could not get it or no private health insurance (57%)
- Limited availability: Long wait times (59%), no service in area (57%), no appointments (56%), limited hours (52%) or not taking new patients (49%)
- Concerns regarding confidentiality (49%)
- Language or translation problems (25%)
Support needs:
- Journey stags 1 to 3:
-
- Emotional support (92%)
- Professional competence (91%)
- Practical support for relationship problems (92%)
- “Be more approachable”, “Hear me and talk to me, not at me”, “Get to know me”, “Help me regain emotional control”, “Help me see a difference perspective”
Survivors’ perceptions of needs
- Journey stages 1 to 3:
-
- “A wake-up call and retraining”, “Intensive therapy”, “Restriction and consequences”
We have summarised our findings according to the journeys described by interview participants who used IPV and/or SV. Against this, we have mapped what they told us about what might work to engage them to seek help for their behaviours (Figure 23). Similar to victims and survivors, universal education is required to assist people to recognise what is a healthy relationship and what is abuse. The “Make a Change” model in the United Kingdom provides a good example of a community education and early intervention program (see earlier box for more).
Shame and lack of awareness of services are major barriers requiring community messaging. A greater focus on family and friends might ensure we engage early with perpetrators and change the trajectory for women and theirchildren. Hence, we have made recommendations that involve “engaging men” training for family and friends and “healthy relationship first aid” training for all workplaces and faith-based organisations.
Further, general practice and private and public mental health services require upskilling on how to engage with people who use IPV and/or SV. The work in health systems is less advanced than in the victim and survivor space but is essential as it is where men go for the associated health issues they have. Professionals need to not only have skills to provide empathic support, but also to challenge people to critically reflect on how their emotional and psychological states and behaviours are connected to gendered beliefs and other discriminatory attitudes (such as racism, ableism and homophobia) that support the use of IPV. Although there is a paucity of evidence on the effectiveness of interventions for perpetrators in health settings (Forsdike et al., 2021; Tarzia, Forsdike, et al., 2020), recent Australian research indicates that respectful therapeutic alliances with perpetrators can be effective when professionals invite perpetrators toexplore a different way of being and when structures of accountability and processes for supporting victims and survivors are in place (Wendt et al., 2019). However, such work is complex, considering that such thought processes may have developed over a lifetime and are supported by dominant social constructions of masculinity (McGinn et al., 2020). It also requires considerable skill to explain the limits of confidentiality and to find a balance between engaging empathically while also maintaining the safety of others (Calcia et al., 2021).
There is a need for greater training to ensure all professionals can develop effective therapeutic alliances that not only support perpetrators, but can also act as part of a “web of accountability”, helping to monitor perpetrators’ risk over time, sharing information and working collaboratively to manage risk (Chung et al., 2020). It should also be noted that any increased investment in services for perpetrators should not be delivered by reducing funding to victim support services.
Strengths and limitations
A strength of the study was the large group of diverse participants who were able to be recruited to the study, although the survey was only available in the English language and to those who could access the internet. The combination of quantitative and qualitative methods enabled a rich narrative to be described of victim and survivor and perpetrator experiences of IPV and/or SV, and their help-seeking and support needs. Although this is the largest detailed study in Australia to undertake this exploration, participants may not represent the experiences or journeys of all those who experience or perpetrate IPV and/or SV, particularly people from diverse backgrounds.
Limitations for the survey methods were as follows:
- Data collection methods were inaccessible for people who do not know English, are not technologically literate and who have limited internet access.
- Having the survey only available online was not considerate of possible participants who have tracked internet usage.
- More respondents being from Victoria impacts results, as there are many statewide services, and the usefulness of these services can affect results in broader survey.
- The online nature meant we were unable to verify that people had not completed the survey twice (this was mitigated by checks for duplication on the data).
Limitations for the victim and survivor interviews were that all of the participants had left their partners at the time of the interviews and their journeys may not reflect the experiences of those still with their partners. Limitations for the perpetrator interviews were that the sample was small, and only comprised male, heterosexual and middle- or older-aged participants. Additionally, it may be difficult for people who use violence to fully acknowledge, share and reflect on their abusive behaviour with an interviewer whom they do not know. Using repeated interviews may assist participants to develop the rapport and trust that would support more open discussion.
Implications for research
It is important that future research exploring help-seeking for IPV and/or SV incorporates the following:
- methods that are inclusive of people who read another language other than English, who have literacy problems, and who do not have access to computers and internet
- more rigorous methods to avoid fraudulent responses ensuring participants cannot answer the survey multiple times
- further insight into engaging safely with people who use IPV and/or SV, victims and survivors still with their partners, non-binary and transgender people, and younger people
- better developed measures of perpetration of IPV and/or SV, tailored to people from diverse backgrounds
- more research on how to engage perpetrators in research
- more research directly with children about their help seeking and needs.
Recommendations for policy and practice
The implications for policy and practice are summarised in the recommendations below, which arose out of synthesis workshops that the team undertook based on the quantitative and qualitative data. We have included some overarching principles for responses across the service system. These include a need to:
- recognise the impacts of IPV and/or SV on children, by developing mechanisms for children’s voices to inform reforms and offering accessible therapeutic support for children
- respond to the diversity of the Australian community, by investing in responses tailored for people with diverse backgrounds and experiences of structural inequalities
- promote change, by offering sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
We developed these principles mostly by acknowledging what was absent or difficult to capture from our data. This included that the voices of children were not included in our study, although victim and survivor participants (and some participants who had used IPV and/or SV) highlighted that they wanted therapeutic interventions for their children and for children’s experiences of IPV and/or SV to be recognised and their voices heard by professionals across the service system. Also, although our sample of participants was reasonably diverse, we were unable to drill down to identify how specific responses should be tailored to people’s individual backgrounds, circumstances or experiences. Finally, there was less data about how to provide sustained support for people to change their use of IPV and/or SV.
Below we make recommendations at different levels including community, social networks, early engagement and system access, and for ongoing response (see Figure 24). Each of these targets a specific barrier or enabler that participants identified in the surveys or interviews.
Figure 24: Recommendations
Overarching principles
Recognise children:
Develop mechanisms for children’s voices to inform reforms and offer accessible therapeutic support for children.
Respond to diversity:
Invest in responses tailors for people with diverse backgrounds experiences of structural inequalities.
Promote change:
Offer sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
Community
Provide
- Universal education on healthy and abusive relationship behaviours
- Enhanced public messaging about available, affordable and confidential supports, including helplines for victims and survivors and people who use IPV and/or SV
- Financial interventions (eg. microfinancing) to alleviate financial distress for victims and survivors.
Social networks

Develop and deliver
- “Allies training” for family, friends and community using the CARE victim and survivor model
- “First responder healthy relationships first aid” for family, friends, workplaces, and faith-based organisations using the LIVES model
- “Engaging men” training for family and friends to engage effectively with men who use IPV and/or SV
Early engagement

Foster
- Professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- Capacity of general practice, mental health and counselling services to engage with people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
System access

Offer
- Ongoing flexible service delivery (telehealth/online) across sectors for victims and survivors and people who use IPV and/or SV
- “Care navigators” for pathways to accessible and affordable long-term support and advocacy for victims and survivors
- Accessible messaging about limits of confidentiality to overcome barriers to accessing support.
Ongoing response

Response
- Aboriginal and Torres Strait Islander-led centres for healing for all members of the family in each state
- Trauma- and violence-informed recovery and healing services in each state
- Peer victim and survivor-led support groups in each state
- Trauma- and violence- informed care through the Medicare Benefits Scheme for general practice and private mental health services
We recommend that the following be provided across the Australian community:
- universal education to assist community members to identify healthy and abusive behaviours in relationships
- enhanced public messaging to raise awareness of affordable and confidential supports available, including helplines for victims and survivors and people who use IPV and/or SV
- financial interventions (e.g. microfinancing) to alleviate financial distress for victims and survivors, so they can obtain the support and resources they need for their safety and wellbeing.
We recommend the following approaches be developed and delivered to improve how social networks respond to IPV and/or SV:
- “allies training” for family, friends and community members to support victims and survivors, using the CARE model (Choice and control, Action and advocacy, Recognition and understanding, Emotional connection; Tarzia, Bohren, et al., 2020)
- “first responder healthy relationships first aid” for workplaces and faith-based organisations, using the LIVES model (Listen, Inquire about needs, Validate, Enhance safety, Support; World Health Organization, 2013b)
- “engaging men” training for family, friends and community members so they can respond effectively to men who use IPV and/or SV.
To encourage victims and survivors and perpetrators to engage early in seeking professional help, we recommend:
- fostering professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- fostering the capacity of general practice, mental health and counselling services to engage people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
To improve the accessibility of the service system, we recommend:
- ongoing flexible service delivery (telehealth or online) across sectors for victims and survivors and people who use IPV and/or SV
- the resourcing of “care navigators” who can provide accessible and affordable long-term individual support and advocacy for victims and survivors
- accessible messaging to be provided about the limits of service confidentiality, to help address the barriers to accessing support.
To improve the ongoing support available to address the impacts of IPV and/or SV, we recommend the following responses be resourced:
- Aboriginal and Torres Strait Islander–led centres for healing for all members of the family in each state, developed by local communities for local communities
- trauma- and violence-informed recovery and healing services in each state
- peer victim and survivor–led support groups in each state
- trauma- and violence-informed care from general practice and private mental health services to be funded through the Medicare Benefits Scheme.
Conclusion
This mixed methods study has provided insights into the voices and experiences of victims and survivors, and people who use IPV and/or SV, across Australia as to what might assist them in their journeys to help-seeking and what support they value. It is one of the first studies to explore the support needs of those who use violence and abuse, and to contrast their perspectives with those of victims and survivors – including in relation to the needs of children in the aftermath of IPV and/or SV. The findings highlight the key role of family and friends and health services in early engagement. Based on our findings, we also make recommendations across the service system for policy and practice changes that can advance the prevention and response to IPV and/or SV. We no longer want victims and survivors having to go around in circles to find support, as shown by this quote from a study participant:
You get referred here, there, and everywhere. In the beginning you’re on so many phone calls, you can’t remember who you were talking to, where they’re from. You go through the same story hundreds of times, and you just get completely lost. You can’t remember any of it. Then with the practical assistance you get is very little to none. This person will go, “Oh no we can’t help you with that, but here, try this person”, and they’ll go, “Oh no we can’t do that, try this person”, and then you get referred back to where you started at. It’s really frustrating.
Critically, we need to end the use of IPV and/or SV by those who perpetrate it. To do so, we need to hear their voices in order to know how to engage them in behaviour change, as shown by this quote:
Just feeling safe and heard during conversation. That would be the most important thing I would expect from a service or professional. Sometimes just hearing your thoughts said out loud is enough to realise what personal plan of action you must take to change your behaviour, which would hopefully be bolstered by the professional’s help.
Author contributions
Kelsey Hegarty, Mandy McKenzie, Elizabeth McLindon and Laura Tarzia prepared this report. Mandy McKenzie undertook the victim and survivor interviews and analyses with Laura Tarzia. Matt Addison undertook the perpetrator interviews, and Mohajer Hameed and Minerva Kyei-Onanjiri oversaw the survey database. Jodie Valpied and Surriya Baloch assisted Elizabeth Mclindon with quantitative analyses, and Kristin Diemer assisted with survey design and interpretation of quantitative analyses.
References
Afrouz, R., Crisp, B. R., & Taket, A. (2020). Seeking help in domestic violence among Muslim women in Muslim-majority and non-Muslim-majority countries: A literature review. Trauma, Violence & Abuse, 21(3), 551–566. https://doi.org/10.1177/1524838018781102
Anyikwa, V. A. (2015). The intersections of race and gender in help-seeking strategies among a battered sample of low-income African American women. Journal of Human Behavior in the Social Environment, 25(8), 948–959. https://doi.org/10.1080/10911359.2015.1047075
Australian Bureau of Statistics. (2016). Personal Safety Survey. https://www.abs.gov.au/statistics/people/crime-and-justice/personal-safety-australia/latest-release
Australian Bureau of Statistics. (2020). Gender indicators, Australia. https://www.abs.gov.au/statistics/people/people-and-communities/gender-indicators-australia/latest-release#data-download
Australian Institute of Health and Welfare. (2018). Family, domestic and sexual violence in Australia 2018. Cat. no. FDV 2. https://www.aihw.gov.au/getmedia/d1a8d479-a39a-48c1-bbe2-4b27c7a321e0/aihw-fdv-02.pdf.aspx?inline=true
Ayre, J., Lum On, M., Webster, K., Gourley, M., & Moon, L. (2016). Examination of the burden of disease of intimate partner violence against women in 2011: Final report (ANROWS Horizons, Issue 06/2016). ANROWS. https://www.anrows.org.au/publication/examination-of-the-burden-of-disease-of-intimate-partner-violence-against-women-in-2011-final-report/
Baird, S. L., Tarshis, S., Messenger, C., & Falla, M. (2022). Virtual support and intimate partner violence services: A scoping review. Research on Social Work Practice. https://doi.org/10.1177/10497315221087232
Barrett, B. J., & Pierre, M. S. (2011). Variations in women’s help seeking in response to intimate partner violence: Findings from a Canadian population-based study. Violence Against Women, 17(1), 47–70. https://doi.org/10.1177/1077801210394273
Blagg, H., Hovane, V., Tulich, T., Raye, D., May, S., & Worrigal, T. (2022). Law, culture and decolonisation: The perspectives of Aboriginal Elders on family violence in Australia. Social and Legal Studies, 31(4), 535–558. https://doi.org/10.1177/09646639211046134
Blagg, H., Williams, E., Cummings, E., Hovane, V., Torres, M., & Woodley, K. N. (2018). Innovative models in addressing violence against Indigenous women (ANROWS Horizons, Issue 01/2018). ANROWS. https://www.anrows.org.au/publication/innovative-models-in-addressing-violence-against-indigenous-women-final-report/
Boxall, H., & Morgan, A. (2021). Experiences of coercive control among Australian women. Statistical Bulletin, 30. Australian Institute of Criminology. https://doi.org/10.52922/sb78108
Boxall, H., Morgan, A., & Brown, R. (2020). The prevalence of domestic violence among women during the COVID-19 pandemic. Statistical Bulletin, 28. Australian Institute of Criminology. https://www.aic.gov.au/sites/default/files/2020-07/sb28_prevalence_of_domestic_violence_among_women_during_covid-19_pandemic.pdf
Bradbury‐Jones, C., & Isham, L. (2020). The pandemic paradox: The consequences of COVID‐19 on domestic violence. Journal of Clinical Nursing, 29(13–14), 2017–2049. https://doi.org/10.1111/jocn.15296
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Braun, V., & Clarke, V. (2021). Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Counselling & Psychotherapy Research, 21(37–47). https://doi.org/10.1002/capr.12360
Braun, V., Clarke, V., Boulton, E., Davey, L., & McEvoy, C. (2020). The online survey as a qualitative research tool. International Journal of Social Research Methodology, 24(6), 641–654. https://doi.org/10.1080/13645579.2020.1805550
Breslau, N., Peterson, E. L., Kessler, R. C., & Schultz, L. R. (1999). Short screening scale for DSM-IV posttraumatic stress disorder. American Journal of Psychiatry, 156(6), 908–911. https://doi.org/10.1176/ajp.156.6.908
Brown, C., & Hegarty, K. (2021). Development and validation of the TAR scale: A measure of technology-facilitated abuse in relationships. Computers in Human Behavior Reports, 3(100059), 1–10. https://doi.org/10.1016/j.chbr.2021.100059
Burgess-Proctor, A. (2015). Methodological and ethical issues in feminist research with abused women: Reflections on participants’ vulnerability and empowerment. Women’s Studies International Forum, 48, 124–134. https://doi.org/10.1016/j.wsif.2014.10.014
Burton, S., & Blair, E. (1991). The power of survey design: A user’s guide for managing surveys, interpreting results and influencing respondents. Public Opinion Quarterly, 55(1), 50–79.
Calcia, M., Bedi, S., Howard, L., Lempp, H., & Oram, S. (2021). Healthcare experiences of perpetrators of domestic violence and abuse: A systematic review and meta-synthesis. BMJ Open, 11(5), e043183. https://doi.org/10.1177/1558689816651808
Campbell, C. (2021). When the personal is not political: Experiences of collective agency amongst participants in the domestic violence response in London, UK. Critical Public Health, 31(3), 280–292. https://doi.org/10.1080/09581596.2021.1874296
Campbell, E., & Vlais, R. (2019). Bringing pathways towards accountability together: Perpetrator experiences and system roles and responsibilities. Centre for Innovative Justice. https://cij.org.au/cms/wp-content/uploads/2018/08/bringing-pathways-towards-accountability-together-perpetrator-experiences-and-system-roles-and-responsibilities-170519.pdf
Campbell, R., Goodman-Williams, R., & Javorka, M. (2019). A trauma-informed approach to sexual violence research ethics and open science. Journal of Interpersonal Violence, 34(23–24), 4765–4793. https://doi.org/10.1177/0886260519871530
Capaldi, D., Knoble, N., Shortt, J., & Kim, H. (2012). A systematic review of risk factors for intimate partner violence. Partner Abuse, 3(2), 231–280. https://doi.org/10.1891/1946-6560.3.2.231
Carlson, B., Day, M., & Farrelly, T. (2021). What works? Exploring the literature on Aboriginal and Torres Strait Islander healing programs that respond to family violence (Research report, Issue 01/2021). https://www.anrows.org.au/publication/what-works-exploring-the-literature-on-aboriginal-and-torres-strait-islander-healing-programs-that-respond-to-family-violence/
Carrington, K., Morley, C., Warren, S., Ryan, V., Ball, M., Clarke, J., & Vitis, L. (2021). The impact of COVID‐19 pandemic on Australian domestic and family violence services and their clients. Australian Journal of Social Issues, 56(4), 539–558. https://doi.org/10.1002/ajs4.183
Chung, D., Upton-Davis, K., Cordier, R., Campbell, E., Wong, T., Salter, M., . . . Bissett, T. (2020). Improved accountability: The role of perpetrator intervention systems (Research report, Issue 20/2020). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2020/06/Chung-RR-Improved-Accountability.pdf
Cortis, N., & Bullen, J. (2016). Domestic violence and women’s economic security: Building Australia’s capacity for prevention and redress: Final report (ANROWS Horizons, Issue 05/2016). ANROWS. https://www.anrows.org.au/publication/domestic-violence-and-womens-economic-security-building-australias-capacity-for-prevention-and-redress-final-report/
Council of Australian Governments. (2012). National Implementation Plan for the First Action Plan 2010–2013: Building a strong foundation. https://www.dss.gov.au/sites/default/files/documents/09_2012/imp_plan_27092012.pdf
Cox, P. (2015). Violence against women in Australia: Additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey, 2012 (Rev ed.; ANROWS Horizons, Issue 01.01/2016). ANROWS. https://www.anrows.org.au/publication/violence-against-women-in-australia-additional-analysis-of-the-australian-bureau-of-statistics-personal-safety-survey-2012/
Davis, M., Fernandez, B., Jonson-Reid, M., & Kyriakakis, S. (2021). Pathways to seeking help from a partner abuse intervention program: A qualitative study of voluntary and non-court-mandated Latino men’s experiences. Journal of Interpersonal Violence, 36(21–22), 10454–10478. https://doi.org/10.1177/0886260519884680
Day, A., Gerace, A., Oster, C., O’Kane, D., & Casey, S. (2018). The views of women in prison about help-seeking for intimate partner violence: At the intersection of survivor and offender. Victims & Offenders, 13(7), 974–994. https://doi.org/10.1080/15564886.2018.1514339
Day, A., Vlais, R., Chung, D., & Green, D. (2019). Evaluation readiness, program quality and outcomes in men’s behaviour change programs (Research report, Issue 01/2019). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/04/Day-et-al-Evaluation-readiness-MBCPs-Research-report-01.2019.pdf
Department of Social Services. (2019). Fourth Action Plan of the National Plan to Reduce Violence against Women and their Children 2010–2022. https://www.dss.gov.au/sites/default/files/documents/08_2019/fourth_action-plan.pdf
Diemer, K., Humphreys, C., Fogden, L., Gallant, D., Spiteri-Staines, A., Bornemisza, A., & Vercoe, E. (2020). Helping fathers value their children: Three site independent evaluation 2017–2020. The University of Melbourne. https://vawc.com.au/wp-content/uploads/2020/05/2020-Caring-Dads-Final-Report-23-3-2020.pdf
Dokkedahl, S., Kirubakaran, R., Bech-Hansen, D., Kristensen, T., & Elklit, A. (2022). The psychological subtype of intimate partner violence and its effect on mental health: A systematic review with meta-analyses. Systematic Reviews, 11(163), 1–16. https://doi.org/10.1186/s13643-022-02025-z
Dowling, C., & Morgan, A. (2019). Predicting repeat domestic violence: Improving police risk assessment. Trends and Issues in Crime and Criminal Justice, 581. Australian Institute of Criminology. https://www.aic.gov.au/publications/tandi/tandi581
Dowling, C., Morgan, A., Boyd, C., & Voce, I. (2018). Policing domestic violence: A review of the evidence (AIC Reports, Issue 13). Australian Institute of Criminology. https://www.aic.gov.au/publications/rr/rr13
Dyson, S., Frawley, P., & Robinson, S. (2017). “Whatever it takes”: Access for women with disabilities to domestic and family violence services (ANROWS Horizons, Issue 05/2017). ANROWS. https://www.anrows.org.au/publication/whatever-it-takes-access-for-women-with-disabilities-to-domestic-and-family-violence-services-final-report/
Edwards, K. M., Mauer, V., Huff, M., Farquhar-Leicester, A., Sutton, T., & Ullman, S. (2022). Disclosure of sexual assault among sexual and gender minorities: A systematic literature review. Trauma, Violence & Abuse. https://doi.org/10.1177/15248380211073842
Elliott, D., Bjelajac, P., Fallor, R. D., Markoff, L. S., & Reed, B. G. (2005). Trauma-informed or trauma-denied: Principles and implementation of trauma-informed services for women. Journal of Community Psychology, 33(4), 461–477. https://doi.org/10.1002/jcop.20063
Ellsberg, M., & Heise, L. (2002). Bearing witness: Ethics in domestic violence research. Lancet, 359(9317), 1599–1604. https://doi.org/10.1016/S0140-6736(02)08521-5
Evans, M., & Feder, G. (2016). Help‐seeking amongst women survivors of domestic violence: A qualitative study of pathways towards formal and informal support. Health Expectations, 19(1), 62–73. https://doi.org/10.1111/hex.12330
Family Violence Protection Act 2008 (Vic).
Felitti, V., & Anda, R. (2010). The relationship of adverse childhood experiences to adult medical disease, psychiatric disorders and sexual behaviour: Implications for healthcare. In R. Lanius, E. Vermetten, & C. Pain (Eds.), The impact of early life trauma on health and disease (pp. 77–87). Cambridge University Press.
Felitti, V., Anda, R., Nordenberg, D., Williamson, D., Spitz, A., Edwards, V., . . . Marks, J. (1998). Relationship of childhood abuse and household dysfunction to many leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventative Medicine, 14, 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Femi-Ajao, O., Kendal, S., & Lovell, K. (2020). A qualitative systematic review of published work on disclosure and help-seeking for domestic violence and abuse among women from ethnic minority populations in the UK. Ethnicity & Health, 25(5), 732–746. https://doi.org/10.1080/13557858.2018.1447652
Finkelhor, D., Ormrod, R., Turner, H., & Hamby, S. (2005). Measuring poly-victimization using the juvenile victimization questionnaire. Child Abuse & Neglect, 29(11), 1297–1312. https://doi.org/doi.org/10.1016/j.chiabu.2005.06.005
Fiolet, R., Tarzia, L., Hameed, M., & Hegarty, K. (2019). Indigenous peoples’ help-seeking behaviors for family violence: A scoping review. Trauma, Violence & Abuse, 22(2), 370–380. https://doi.org/10.1177/1524838019852638
Fitz-Gibbon, K., Burley, J., & Meyer, S. (2020). How do we keep family violence perpetrators “in view” during the COVID-19 lockdown? The Conversation. https://theconversation.com/how-do-we-keep-family-violence-perpetrators-in-view-during-the-covid-19-lockdown-135942
Flood, M., & Pease, B. (2009). Factors influencing attitudes to violence against women. Trauma, Violence & Abuse, 10(2), 125–42. https://doi.org/10.1177/1524838009334131
Ford-Gilboe, M., Aathen, N., Varcoe, C., MacMillan, H., Scott-Storey, K., Mantler, T., . . . Perrin, N. (2016). Development of a brief measure of intimate partner violence experiences: The composite abuse scale (revised). BMJ Open, 6(12). https://doi.org/10.1136/bmjopen-2016-012824
Forsdike, K., Tarzia, L., Flood, M., Vlais, R., & Hegarty, K. (2021). “A lightbulb moment”: Using the theory of planned behavior to explore the challenges and opportunities for early engagement of Australian men who use violence in their relationships. Journal of Interpersonal Violence, 36(7–8), NP3889–NP3913. https://doi.org/10.1177/0886260518780778
Fraga Dominguez, S., Storey, J. E., & Glorney, E. (2021). Help-seeking behavior in victims of elder abuse: A systematic review. Trauma, Violence, & Abuse, 22(3), 466–480. https://doi.org/10.1177/1524838019860616
Gallant, D., Andrews, S., Humphreys, C., Diemer, K., Ellis, D., Burton, J., . . . Bamblett, A. (2017). Aboriginal men’s programs tackling family violence: A scoping review. Journal of Australian Indigenous Issues, 20(2), 48–68. https://static1.squarespace.com/static/596d8907b3db2b5b22158a4e/t/5d351cd1a472a70001e21851/1563761876804/Gallant+et+al+Aboriginal+ Men%27s+Programs+Scoping+Review.pdf
Garcia-Moreno, C., Hegarty, K., d’Oliveira, A., Koziol-McLain, J., Colombini, M., & Feder, G. (2015). The health-systems response to violence against women. Lancet, 385, 1567–1579. https://doi.org/10.1016/S0140-6736(14)61837-7
Ghafournia, N., & Easteal, P. (2019). Help-seeking experiences of immigrant domestic violence survivors in Australia: A snapshot of Muslim survivors. Journal of Interpersonal Violence, 36(19–20), 9008–9034. https://doi.org/10.1177/0886260519863722
Goodman, L., & Smyth, K. F. (2011). A call for a social network-oriented approach to services for survivors of intimate partner violence. Psychology of Violence, 1(2), 79–92. https://doi.org/10.1037/a0022977
Grace, K., & Anderson, J. (2016). Reproductive coercion: A systematic review. Trauma, Violence & Abuse, 19(4). https://doi.org/10.1177/1524838016663935
Gregory, A., Feder, G., Taket, A., & Williamson, E. (2017). Qualitative study to explore the health and well-being impacts on adults providing informal support to female domestic violence survivors. BMJ Open, 7(3), e014511. https://doi.org/10.1136/bmjopen-2016-014511
Gregory, A., Johnson, E., Feder, G., Campbell, J., Konya, J., & Perot, C. (2021). Perceptions of peer support for victim-survivors of sexual violence and abuse: An exploratory study with key stakeholders. Journal of Interpersonal Violence. https://doi.org/10.1177/08862605211007931
Hashimoto, N., Radcliffe, P., & Gilchrist, G. (2018). Help-seeking behaviors for intimate partner violence perpetration by men receiving substance use treatment: A mixed-methods secondary analysis. Journal of Interpersonal Violence, 36(7–8). https://doi.org/10.1177/0886260518770645
Healey, L., Humphreys, C., Tsantefski, M., Heward-Belle, S., & Mandel, D. (2018). Invisible practices: Intervention with fathers who use violence (Research to policy practice, Issue 04/2018). ANROWS. https://www.anrows.org.au/publication/invisible-practices-intervention-with-fathers-who-use-violence-key-findings-and-future-directions/
Hegarty, K., Andrews, S., & Tarzia, L. (2022). Transforming health systems to address gender-based violence in Australia. Medical Journal of Australia, 217(3), 159–166. https://doi.org/10.5694/mja2.51638
Hegarty, K., O’Doherty, L., Chondros, P., Valpied, J., Taft, A., Astbury, J., . . . Gunn, J. (2013). Effect of type and severity of intimate partner violence on women’s health and service use: Findings from a primary care trial of women afraid of their partners. Journal of Interpersonal Violence, 28(2), 273–294. https://doi.org/10.1177/0886260512454722
Hegarty, K., Spangaro, J., Kyei-Onanjiri, M., Valpied, J., Walsh, J., Chapman, J., & Koziol-McLain, J. (2021). Validity of the ACTS intimate partner violence screen in antenatal care: A cross sectional study. BMC Public Health, 2021(March 4). https://doi.org/10.21203/rs.3.rs-264487/v1
Hegarty, K., Tarzia, L., Rees, S., Fooks, A., Forsdike, K., Woodlock, D., . . . Amanatidis, S. (2017). Women’s input to a trauma-informed systems model of care in health settings: The WITH study (ANROWS Horizons, Issue 02/2017). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/WITH_Horizons_UPDATE_FINAL.pdf
Heron, R. L., & Eisma, M. C. (2021). Barriers and facilitators of disclosing domestic violence to the healthcare service: A systematic review of qualitative research. Health & Social Care in the Community, 29(3), 612–630. https://doi.org/10.1111/hsc.13282
Hodgson, R., Alwyn, T., John, B., Thom, B., & Smith, A. (2002). The FAST alcohol screening test. Alcohol and Alcoholism, 37(1), 61–66. https://doi.org/10.1093/alcalc/37.1.61
Hooker, L., Versteegh, L., Lindgren, H., & Taft, A. (2020). Differences in help-seeking behaviours and perceived helpfulness of services between abused and non-abused women: A cross-sectional survey of Australian postpartum women. Health & Social Care in the Community, 28(3), 958–968. https://doi.org/10.1111/hsc.12927
Hu, R., Xue, J., Lin, K., Sun, I. Y., Wu, Y., & Wang, X. (2020). The patterns and influencing factors of help-seeking decisions among women survivors of intimate partner violence in China. Journal of Family Violence, 36, 669–681. https://doi.org/10.1007/s10896-020-00145-5
Humphreys, C., & Campo, M. (2017). Fathers who use violence: Options for safe practice where there is ongoing contact with children (Child Family Community Australia information exchange, Issue 43). Australian Institute of Family Studies. https://aifs.gov.au/sites/default/files/publication-documents/fatherswho_useviolence-final-v2_0_0.pdf
Humphreys, C., Diemer, K., Bornemisza, A., Spiteri‐Staines, A., Kaspiew, R., & Horsfall, B. (2019). More present than absent: Men who use domestic violence and their fathering. Child & Family Social Work, 24(2), 321–329. https://doi.org/10.1111/cfs.12617
Humphreys, C., & Healey, L. (2017). PAThways and research into collaborative inter-agency practice: Collaborative work across the child protection and specialist domestic and family violence interface: Final report (ANROWS Horizons, Issue 03/2017). ANROWS. https://www.anrows.org.au/publication/pathways-and-research-into-collaborative-inter-agency-practice-collaborative-work-across-the-child-protection-and-specialist-domestic-and-family-violence-interface-the-patricia-project-final-report/
Humphreys, C., Kertesz, M., Healey, L., & Mandel, D. (2019). Shifting practice in domestic violence: Child protection workers partnering with mothers. In C. Zufferey & F. Buchanan (Eds.), Intersections of mothering (pp. 194–205). Routledge.
Humphreys, C., Thiara, R., Sharp, C., & Jones, J. (2015). Supporting the relationship between mothers and children in the aftermath of domestic violence. In C. Humphreys & N. Stanley (Eds.), Domestic violence and protecting children: New thinking and approaches (pp. 130–147). Jessica Kingsley Publishers.
Hydén, M. (2015). What social networks do in the aftermath of domestic violence. British Journal of Criminology, 55(6), 1040–1057. https://doi.org/10.1093/bjc/azv099
Indermaur, D. (2001). Young Australians and domestic violence. Trends and Issues in Crime and Criminal Justice, 195. Australian Institute of Criminology. https://www.aic.gov.au/publications/tandi/tandi195
Iratzoqui, A., & Cohn, E. G. (2020). The reporting and help‐seeking behaviors of domestic violence victims with criminal backgrounds. Sociology Compass, 14(4), e12771. https://doi.org/10.1111/soc4.12771
Kaspiew, R., Horsfall, B., Qu, L., Nicholson, J., Humphreys, C., Diemer, K., . . . Taft, A. (2017). Domestic and family violence and parenting: Mixed method insights into impact and support needs: Final report (ANROWS Horizons, Issue 04/2017). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/Parenting_Horizons_FINAL-1.pdf
Kelly, L., & Westmarland, N. (2016). Naming and defining “domestic violence”: Lessons from research with violent men. Feminist Review, 112(1), 113–127. https://doi.org/10.1057/fr.2015.52
Kertesz, M., Humphreys, C., Larance, L., Vicary, D., Spiteri-Staines, A., & Ovenden, G. (2019). Working with women who use force: A feasibility study protocol of the Positive (+) SHIFT group work programme in Australia. BMJ Open, 9(5), Article e027496. https://doi.org/10.1136/bmjopen-2018-027496
Kimber, M., Adham, S., Gill, S., McTavish, J., & MacMillan, H. (2018). The association between child exposure to intimate partner violence (IPV) and perpetration of IPV in adulthood: A systematic review. Child Abuse & Neglect, 76, 273–286. https://doi.org/10.1016/j.chiabu.2017.11.007
Kirkwood, B., & Sterne, J. (2003). Essential medical statistics (2nd ed.). Blackwell Science.
Klein, R. (2012). Responding to intimate violence against women: The role of informal networks. Cambridge University Press.
Kolar, K., Ahmad, F., Chen, L., & Erickson, P. (2015). Timeline mapping in qualitative interviews: A study of resilience with marginalized groups. International Journal of Qualitative Methods, 14(3), 13–32. https://doi.org/10.1177/160940691501400302
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Lowe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics, 50(6), 613–621. https://doi.org/10.1176/appi.psy.50.6.613
Kulkarni, S. (2019). Intersectional trauma-informed intimate partner violence (IPV) services: Narrowing the gap between IPV service delivery and survivor needs. Journal of Family Violence, 34, 55–64. https://doi.org/10.1007/s10896-018-0001-5
Lamb, K., Humphreys, C., & Hegarty, K. (2018). “Your behaviour has consequences”: Children and young people’s perspectives on reparation with their fathers after domestic violence. Children and Youth Services Review, 88, 164–169. https://doi.org/10.1016/j.childyouth.2018.03.013
Latta, R. E., & Goodman, L. (2011). Intervening in partner violence against women: A grounded theory exploration of informal network members’ experiences. Counseling Psychologist, 39(7), 973–1023. https://doi.org/10.1177/0011000011398504
Lelaurain, S., Graziani, P., & Lo Monaco, G. (2017). Intimate partner violence and help-seeking: A systematic review and social psychological tracks for future research. European Psychologist, 22(4), 263–281. https://doi.org/10.1027/1016-9040/a000304
Levant, R. F. (2011). Research in the psychology of men and masculinity using the gender role strain paradigm as a framework. American Psychologist, 66(8), 765–776. https://doi.org/10.1037/a0025034
Lévesque, S., Rousseau, C., Lessard, G., Bigaouette, M., Fernet, M., Valderrama, A., & Boulebsol, C. (2021). Qualitative exploration of the influence of domestic violence on motherhood in the perinatal period. Journal of Family Violence, 37(9), 275–287. https://doi.org/10.1007/s10896-021-00294-1
Li, S., Zhao, F., & Yu, G. (2019). Childhood maltreatment and intimate partner violence victimization: A meta-analysis. Child Abuse & Neglect, 88, 212–224. https://doi.org/10.1016/j.chiabu.2018.11.012
Li, S., Zhao, F., & Yu, G. (2020). A meta-analysis of childhood maltreatment and intimate partner violence perpetration. Aggression and Violent Behavior, 50, Article 101362. https://doi.org/10.1016/j.avb.2019.101362
Marsden, S., Humphreys, C., & Hegarty, K. (2021). Women survivors’ accounts of seeing psychologists: Harm or benefit? Journal of Gender-Based Violence, 5(1), 111–127. https://doi.org/10.1332/239868020X16040863370635
Martsolf, D. S., Draucker, C. B., Cook, C. B., Ross, R., & Stidham, A. W. (2010). A meta-summary of qualitative findings about professional services for survivors of sexual violence. Qualitative Report, 15(3), 489–506. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3153442/
McGinn, T., McColgan, M., & Taylor, B. (2020). Male IPV perpetrators’ perspectives on intervention and change: A systematic synthesis of qualitative studies. Trauma, Violence, & Abuse, 21(1), 97–112. https://doi.org/10.1177/1524838017742167
McGinn, T., Taylor, B., McColgan, M., & Lagdon, S. (2016). Survivor perspectives on IPV perpetrator interventions: A systematic narrative review. Trauma, Violence & Abuse, 17(3), 239–255. https://doi.org/10.1177/1524838015584358
McKenzie, M., Hegarty, K., Palmer, V., & Tarzia, L. (2022). “Walking on eggshells”: A qualitative study of how friends of young women experiencing intimate partner violence perceive their role. Journal of Interpersonal Violence, 37(9–10), NP7502–NP7527. https://doi.org/10.1177/0886260520969238
Meyer, S. (2010a). “Acting in the children’s best interest?”: Examining victims’ responses to intimate partner violence. Journal of Child & Family Studies, 20(4), 436–443. https://doi.org/10.1007/s10826-010-9410-7
Meyer, S. (2010b). Seeking help to protect the children?: The influence of children on women’s decisions to seek help when experiencing intimate partner violence. Journal of Family Violence, 25(8), 713–725. https://doi.org/10.1007/s10896-010-9329-1
Meyer, S. (2011). Seeking help for intimate partner violence: Victims’ experiences when approaching the criminal justice system for IPV-related support and protection in an Australian jurisdiction. Feminist Criminology, 6(4), 268–290. https://doi.org/10.1177/1557085111414860
Meyer, S. (2016). Still blaming the victim of intimate partner violence? Women’s narratives of victim desistance and redemption when seeking support. Theoretical Criminology, 20(1), 75–90. https://doi.org/10.1177/1362480615585399
Meyer, S. (2018). Motivating perpetrators of domestic and family violence to engage in behaviour change: The role of fatherhood. Child & Family Social Work, 23(1), 97–104. https://doi.org/https://doi.org/10.1111/cfs.12388
Meyer, S., & Stambe, R. M. (2021). Indigenous women’s experiences of domestic and family violence, help-seeking and recovery in regional Queensland. Australian Journal of Social Issues, 56(3), 443–458. https://doi.org/10.1002/ajs4.128
Mitra-Kahn, T., Newbigin, C., & Hardefeldt, S. (2016). Invisible women, invisible violence: Understanding and improving data on the experiences of domestic and family violence and sexual assault for diverse groups of women: State of knowledge paper (ANROWS Landscapes, Issue 01/2016). ANROWS. https://www.anrows.org.au/publication/invisible-women-invisible-violence-understanding-and-improving-data-on-the-experiences-of-domestic-and-family-violence-and-sexual-assault-for-diverse-groups-of-women-state-of-knowledge-paper/
Moran, R., & Asquith, N. (2020). Understanding the vicarious trauma and emotional labour of criminological research. Methodological Innovations, 13(2). https://doi.org/10.1177/2059799120926085
Morgan, A., Boxall, H., & Payne, J. L. (2022). Reporting to police by intimate partner violence victim-survivors during the COVID-19 pandemic. Journal of Criminology, 55(3). https://doi.org/10.1177/26338076221094845
Morgan, G., Butler, C., French, R., Creamer, T., Hillan, L., Ruggiero, E., . . . Trew, S. (2022). New ways for our families: Designing an Aboriginal and Torres Strait Islander cultural practice framework and system responses to address the impacts of domestic and family violence on children and young people (Research report, Issue 06/2022). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2022/04/Morgan-et-al-RR1_NewWaysOurFamilies.pdf
Morgan, K., Williamson, E., Hester, M., Jones, S., & Feder, G. (2014). Asking men about domestic violence and abuse in a family medicine context: Help seeking and views on the general practitioner role. Aggression and Violent Behavior, 19(6), 637–642. https://doi.org/10.1016/j.avb.2014.09.008
O’Doherty, L., Taft, A., McNair, R., & Hegarty, K. (2016). Fractured identity in the context of intimate partner violence: Barriers and opportunities to seeking help in health settings. Violence Against Women, 22(2), 225–248. https://doi.org/10.1177/1077801215601248
Olsen, A., & Lovett, R. (2016). Existing knowledge, practice and responses to violence against women in Australian Indigenous communities (ANROWS Landscapes, Issue 02/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/FINAL-02.16_3.2-AIATSIS-Landscapes-WEB-1.pdf
Oram, S., Fisher, H., Minnis, H., Seedat, S., Walby, S., Hegarty, K., . . . Howard , L. M. (2022). The Lancet Psychiatry Commision on intimate partner violence and mental health: Advancing mental health services, research, and policy. Lancet Psychiatry, 9(6), 487–524. https://doi.org/10.1016/S2215-0366(22)00008-6
Oram, S., Trevillion, K., Khalifeh, H., Feder, G., & Howard, L. (2013). Systematic review and meta-analysis of psychiatric disorder and the perpetration of partner violence. Epidemiology and Psychiatric Sciences, 23(4). https://doi.org/10.1017/S2045796013000450
Osborn, M., & Rajah, V. (2020). Understanding formal responses to intimate partner violence and women’s resistance processes: A scoping review. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838020967348
Our Watch. (2017). Primary prevention of family violence against people from LGBTI communities. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2019/11/07031955/Primary-Prevention-of-FV-against-LGBTI-people-Report-Accessible-PDF.pdf
Our Watch. (2018a). Changing the picture: Background paper: Understanding violence against Aboriginal and Torres Strait Islander women and their children. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2020/09/20231756/Changing-the-picture-Part-1-AA.pdf
Our Watch. (2018b). Changing the picture: A national resource to support the prevention of violence against Aboriginal and Torres Strait Islander women and their children. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2020/09/20231759/Changing-the-picture-Part-2-AA.pdf
Our Watch, & VicHealth. (2021). Change the story: A shared framework for the primary prevention of violence against women and their children in Australia. Our Watch. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2021/11/18101814/Change-the-story-Our-Watch-AA.pdf
Partners for Prevention. (2020). The UN multi-country study on men and violence in Asia and the Pacific. United Nations. http://www.partners4prevention.org/about-prevention/research/men-and-violence-study
Patterson, M., Markey, M., & Somers, J. (2012). Multiple paths to just ends: Using narrative interviews and timelines to explore health equity and homelessness. International Journal of Qualitative Methods, 11(2), 132–151. https://doi.org/10.1177/16094069120110020
Peitzmeier, S. M., Malik, M., Kattari, S. K., Marrow, E., Stephenson, R., Agénor, M., & Reisner, S. L. (2020). Intimate partner violence in transgender populations: Systematic review and meta-analysis of prevalence and correlates. American Journal of Public Health, 110(9), e1–e14. https://doi.org/10.2105/AJPH.2020.305774
Pentaraki, M., & Speake, J. (2020). Domestic violence in a COVID-19 context: Exploring emerging issues through a systematic analysis of the literature. Open Journal of Social Sciences, 8(10), 193–211. https://doi.org/10.4236/jss.2020.810013
Pfitzner, N., Fitz-Gibbon, K., & True, J. (2022). When staying home isn’t safe: Australian practitioner experiences of responding to intimate partner violence during COVID-19 restrictions. Journal of Gender-Based Violence, 6(2), 297–314. https://doi.org/10.1332/239868021X16420024310873
Piquero, A. R., Jennings, W. G., Jemison, E., Kaukinen, C., & Knaul, F. M. (2021). Domestic violence during the COVID-19 pandemic: Evidence from a systematic review and meta-analysis. Journal of Criminal Justice, 74, 101806. https://doi.org/10.1016/j.jcrimjus.2021.101806
Pokharel, B., Hegadoren, K., & Papathanassoglou, E. (2020). Factors influencing silencing of women who experience intimate partner violence: An integrative review. Aggression and Violent Behavior, 52, 101422. https://doi.org/10.1016/j.avb.2020.101422
Potter, L., Morris, R., Hegarty, K., Garcia- Moreno, C., & Feder, G. (2020). Categories and health impacts of intimate partner violence in the World Health Organization multi-country study on women’s health and domestic violence. International Journal of Epidemiology, 1–11. Advance online publication. https://doi.org/10.1093/ije/dyaa220
Price, E., Sharman, L., Douglas, H., Sheeran, N., & Dingle, G. (2019). Experiences of reproductive coercion in Queensland women. Journal of Interpersonal Violence, 37(5–6), NP2823–NP2843. https://doi.org/10.1177/0886260519846851
PriceWaterhouseCoopers Australia. (2015). A high price to pay: The economic case for preventing violence against women. https://www.pwc.com.au/pdf/a-high-price-to-pay.pdf
Ragusa, A. (2016). Rurality’s influence on women’s intimate partner violence experiences and support needed for escape and healing in Australia. Journal of Social Service Research, 43(2), 270–295. https://doi.org/10.1080/01488376.2016.1248267
Ravi, K., Robinson, S. R., & Voth Schrag, R. (2021). Facilitators of formal help-seeking for adult survivors of IPV in the United States: A systematic review. Trauma, Violence, & Abuse. https://doi.org/10.1177/1524838021995954
Rawlins, W. K. (2008). The compass of friendship: Narratives, identities, and dialogues. Sage Publications.
Reisenhofer, S., & Seibold, C. (2013). Emergency healthcare experiences of women living with intimate partner violence. Journal of Clinical Nursing, 22(15–16), 2253–2263. https://doi.org/10.1111/j.1365-2702.2012.04311.x
Riessman, C. (2008). Narrative methods for the human sciences. Sage.
Rivas, C., Vigurs, C., Cameron, J., & Yeo, L. (2019). A realist review of which advocacy interventions work for which abused women under what circumstances. Cochrane Database Syst Rev, 6, CD013135. https://doi.org/10.1002/14651858.CD013135.pub2
Robinson, S. R., Ravi, K., & Voth Schrag, R. (2020). A systematic review of barriers to formal help seeking for adult survivors of IPV in the United States, 2005–2019. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838020916254
Santoniccolo, F., Trombetta, T., & Rollè, L. (2021). The help-seeking process in same-sex intimate partner violence: A systematic review. Sexuality Research and Social Policy. https://doi.org/10.1007/s13178-021-00629-z
Satyen, L., Piedra, S., Ranganathan, A., & Golluccio, N. (2018). Intimate partner violence and help-seeking behavior among migrant women in Australia. Journal of Family Violence, 33(7), 447–456. https://doi.org/10.1007/s10896-018-9980-5
Satyen, L., Rogic, A. C., & Supol, M. (2019). Intimate partner violence and help-seeking behaviour: A systematic review of cross-cultural differences [Review]. Journal of Immigrant and Minority Health, 21(4), 879–892. https://doi.org/10.1007/s10903-018-0803-9
Segrave, M., & Pfitzner, N. (2020). Family violence and temporary visa holders during COVID-19. Monash. https://bridges.monash.edu/articles/online_resource/Family_violence_and_temporary_visa_holders_during_COVID-19/12987938
Shackelford, T. K., & Mouzos, J. (2005). Partner killing by men in cohabiting and marital relationships: A comparative, cross-national analysis of data from Australia and the United States. Journal of Interpersonal Violence, 20(10), 1310–1324. https://doi.org/10.1177/0886260505278606
Sheehan, K., Thakor, S., & Stewart, D. (2012). Turning points for perpetrators of intimate partner violence. Trauma, Violence & Abuse, 13(1), 30–40. https://doi.org/10.1177/1524838011426016
Shimmin, C., Wittmeier, K., Lavoie, J., Wicklund, E., & Sibley, K. (2017). Moving towards a more inclusive patient and public involvement in health research paradigm: The incorporation of a trauma-informed intersectional analysis. BMC Health Services Research, 17(539). https://doi.org/10.1186/s12913-017-2463-1
Sripada, P. (2021). Help-seeking behavior of South Asian women in domestic violence: A scoping review. Journal of Human Behavior in the Social Environment, 31(6), 729–750. https://doi.org/10.1080/10911359.2020.1811823
StataCorp. (2015). Stata Statistical Software: Release 15. https://www.stata.com
Strang, A., O’Brien, O., Sandilands, M., & Horn, R. (2020). Help-seeking, trust and intimate partner violence: Social connections amongst displaced and non-displaced Yezidi women and men in the Kurdistan region of northern Iraq. Conflict and Health, 14, 61. https://doi.org/10.1186/s13031-020-00305-w
Su, Z., McDonnell, D., Roth, S., Li, Q., Šegalo, S., Shi, F., & Wagers, S. (2021). Mental health solutions for domestic violence victims amid COVID-19: A review of the literature. Globalization and Health, 17(67). https://doi.org/10.1186/s12992-021-00710-7
Sullivan, C., & Goodman, L. (2019). Advocacy with survivors of intimate partner violence: What it is, what it isn’t, and why it’s critically important. Violence Against Women, 25(16), 2007–2023. https://doi.org/10.1177/1077801219875826
Summers, A. (2022). The choice: Violence or poverty. Paul Ramsay Foundation. https://paulramsayfoundation.org.au/wp-content/uploads/2022/07/TheChoice-violence-or-poverty-web.pdf
Sylaska, K. M., & Edwards, K. M. (2014). Disclosure of intimate partner violence to informal social support network members: A review of the literature. Trauma, Violence & Abuse, 15(1), 3–21. https://doi.org/10.1177/1524838013496335
Taket, A., O’Doherty, L., Valpied, J., & Hegarty, K. (2014). What do Australian women experiencing intimate partner abuse want from family and friends? Qualitative Health Research, 24(7), 983–996. https://doi.org/10.1177/1049732314540054
Tarzia, L. (2020). “It went to the very heart of who I was as a woman”: The invisible impacts of intimate partner sexual violence. Qualitative Health Research, 31(2), 287–297. https://doi.org/10.1177/1049732320967659
Tarzia, L., Bohren, M., Cameron, J., Garcia-Moreno, C., O’Doherty, L., Fiolet, R., . . . Hegarty, K. (2020). Women’s experiences and expectations after disclosure of intimate partner abuse to a healthcare provider: A qualitative meta-synthesis. BMJ Open, 10(11), e041339. https://doi.org/10.1136/bmjopen-2020-041339
Tarzia, L., Cornelio, R., Forsdike, K., & Hegarty, K. (2018). Women’s experiences receiving support online for intimate partner violence: How does it compare to face-to-face support from a health professional? Interacting With Computers, 30(5), 433–443. https://doi.org/doi.org/10.1093/iwc/iwy019
Tarzia, L., Forsdike, K., Feder, G., & Hegarty, K. (2020). Interventions in health settings for male perpetrators or victims of intimate partner violence. Trauma, Violence & Abuse, 21(1), 123–137. https://doi.org/10.1177/1524838017744772
Tarzia, L., & Hegarty, K. (2020). A conceptual re-evaluation of reproductive coercion: Centring intent, fear and control. BMC Reproductive Health, 18(87). https://doi.org/10.1186/s12978-021-01143-6
Tarzia, L., & Hegarty, K. (2022). “He’d tell me I was frigid and ugly and force me to have sex with him anyway”: Women’s experiences of co-occurring sexual violence and psychological abuse in heterosexual relationships. Journal of Interpersonal Violence, 1–21. https://doi.org/10.1177/08862605221090563
Tarzia, L., Iyer, D., Thrower, E., & Hegarty, K. (2017). “Technology doesn’t judge you”: Young Australian women’s views on using the internet and smartphones to address intimate partner violence. Journal of Technology in Human Services, 35(3), 199–218. https://doi.org/doi.org/10.1080/15228835.2017.1350616
Tengku Hassan, T. N. F., Ali, S. H., & Salleh, H. (2015). Patterns of help-seeking among women experiencing intimate partner violence in Malaysia. Asian Journal of Womens Studies, 21(1), 77–92. https://doi.org/10.1080/12259276.2015.1029226
Trotter, J. L., & Allen, N. E. (2009). The good, the bad, and the ugly: Domestic violence survivors’ experiences with their informal social networks. American Journal of Community Psychology, 43(3), 221–231. https://doi.org/10.1007/s10464-009-9232-1
Usher, K., Bhullar, N., Durkin, J., Gyamfi, N., & Jackson, D. (2020). Family violence and COVID‐19: Increased vulnerability and reduced options for support. International Journal of Mental Health Nursing, 29(4), 549–552. https://doi.org/10.1111/inm.12735
Valpied, J., Cini, A., O’Doherty, L., Taket, A., & Hegarty, K. (2014). “Sometimes cathartic. Sometimes quite raw”: Benefit and harm in an intimate partner violence trial. Aggression and Violent Behavior, 19(6), 673–685. https://doi.org/https://doi.org/10.1016/j.avb.2014.09.005
Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Block, K., . . . Warr, D. (2016). Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: The ASPIRE Project: Key findings and future directions (ANROWS Compass, Issue 08/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/01/Aspire_Compass_final.pdf
Victorian Government. (2016). Royal Commission into Family Violence: Summary and recommendations. https://www.parliament.vic.gov.au/file_uploads/1a_RFV_112ppA4_SummaryRecommendations.WEB_DXQyLhqv.pdf
Vogel, D. L., & Heath, P. J. (2016). Men, masculinities, and help-seeking patterns. In APA handbook of men and masculinities (pp. 685–707). American Psychological Association.
Waller, B. Y., Harris, J., & Quinn, C. R. (2021). Caught in the crossroad: An intersectional examination of African American women intimate partner violence survivors’ help seeking. Trauma, Violence, & Abuse, 23(4), 1235–1248. https://doi.org/10.1177/1524838021991303
Ware, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233. https://doi.org/10.1097/00005650-199603000-00003
Webster, K. (2016). A preventable burden: Measuring and addressing the prevalence and health impacts of intimate partner violence in Australian women (ANROWS Compass, Issue 07/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/01/28-10-16-BOD-Compass.pdf
Webster, K., Diemer, K., Honey, N., Mannix, S., Mickle, J., Morgan, J., . . . Ward, A. (2018). Australians’ attitudes to violence against women and gender equality: Findings from the 2017 National Community Attitudes Survey (NCAS). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/10/anr001-NCAS-report-WEB-1019.pdf
Wendt, S., Chung, D., Elder, A., Hendrick, A., & Hartwig, A. (2017). Seeking help for domestic and family violence: Exploring regional, rural, and remote women’s coping experiences: Final report (ANROWS Horizons, Issue 06/2017). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/RP.14.04_RWR_Horizons-FINAL-1709.pdf
Wendt, S., Seymour, K., Buchanan, F., Dolman, C., & Greenland, N. (2019). Engaging men who use violence: Invitational narrative approaches (Research report, Issue 05/2019). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/10/PI.17.12-Wendt-Invitational-Narrative-Therapies-ANROWS-Research-Report.pdf
World Health Organization (2012). Violence against women: Intimate partner violence and sexual violence against women. http://www.who.int/mediacentre/factsheets/fs239/en/index.html
World Health Organization. (2013a). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf
World Health Organization. (2013b). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. http://www.who.int/reproductivehealth/publications/violence/9789241548595/en/
World Health Organization. (2014). Health care for women subjected to intimate partner violence or sexual violence: A clinical handbook. http://apps.who.int/iris/bitstream/10665/136101/1/WHO_RHR_14.26_eng.pdf
World Health Organization. (2016). Ethical and safety recommendations for intervention research on violence against women. https://apps.who.int/iris/bitstream/handle/10665/251759/9789241510189-eng.pdf
Wright, E. N., Anderson, J., Phillips, K., & Miyamoto, S. (2021). Help-seeking and barriers to care in intimate partner sexual violence: A systematic review. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838021998305
Wu, E., El-Bassel, N., Gilbert, L., Sarfo, B., & Seewald, R. (2010). Criminal justice involvement and service need among men on methadone who have perpetrated intimate partner violence. Journal of Criminal Justice, 38(4), 835–840. https://doi.org/10.1016/j.jcrimjus.2010.05.012
Zinzow, H., Littleton, H., Muscari, E., & Sall, K. (2021). Barriers to formal help-seeking following sexual violence: Review from within an ecological systems framework. Victims & Offenders, 17(6), 893–918. https://doi.org/10.1080/15564886.2021.1978023
Appendix A:
Literature review 2010 to 2020
Search strategy and key terms
We undertook a rapid systematic review of the peer-reviewed literature focused on IPV and/or SV, help-seeking behaviours and service needs. We identified relevant studies and reviews of the literature using a systematic search of key bibliographic databases (MEDLINE, Embase, PsycINFO, Cochrane databases, Applied Social Sciences Index and Abstracts: ASSIA, Web of Science, PsycArticles and Scopus). The search was conducted during September 2020, using the subject headings and key terms shown in the table below. This was informally updated in May 2022 to include more recent systematic review articles. We also checked the reference lists of all included records to identify additional studies, and undertook hand-searching and communication with experts in the field to identify any further potentially relevant sources of data. All searches were filtered to 1 January 2010 onwards to find literature related to contemporary service delivery.
Women who experience IPV and/or SV
People who perpetrate IPV and/or SV against women
(Women OR Female) AND (Intimate partner violence OR battered women OR domestic violence OR spouse abuse OR family violence OR rape OR sexual victimisation OR sexual aggression OR sexual violence OR sexual coercion OR sexual assault) AND (Help seeking)
(Women OR female OR men OR male OR man) AND (Intimate partner violence OR perpetration OR domestic violence OR spouse abuse OR family violence OR Abuse and violence OR batter OR rape OR sexual perpetration OR sexual aggression OR sexual violence OR sexual coercion OR sexual assault) AND (Help seeking)
Inclusion/exclusion criteria
Inclusion was limited to studies where 1) participants were women aged 18 years and older who had experienced any type of IPV and/or SV or people aged 18 years and older who had perpetrated any type of IPV and/or SV against women; and 2) the data focused on help-seeking behaviours. We excluded studies exclusively exploring experiences of disclosure in response to routine or universal screening in health settings, since this is a provider-initiated interaction. Study types of interest included quantitative or qualitative primary studies (any methodology); systematic reviews or meta-analyses; and peer-reviewed reports. Opinion pieces, theoretical articles, books and theses were excluded.
Search results
As illustrated in the PRISMA flowchart below, our search yielded 863 results after duplicates were removed. After screening the titles and/or abstracts (863), 666 (titles) and 105 (abstracts) records were removed based on the exclusion criteria. Of the remaining 92 records, the full text was screened to determine whether they met the inclusion criteria.
PRISMA flowchart
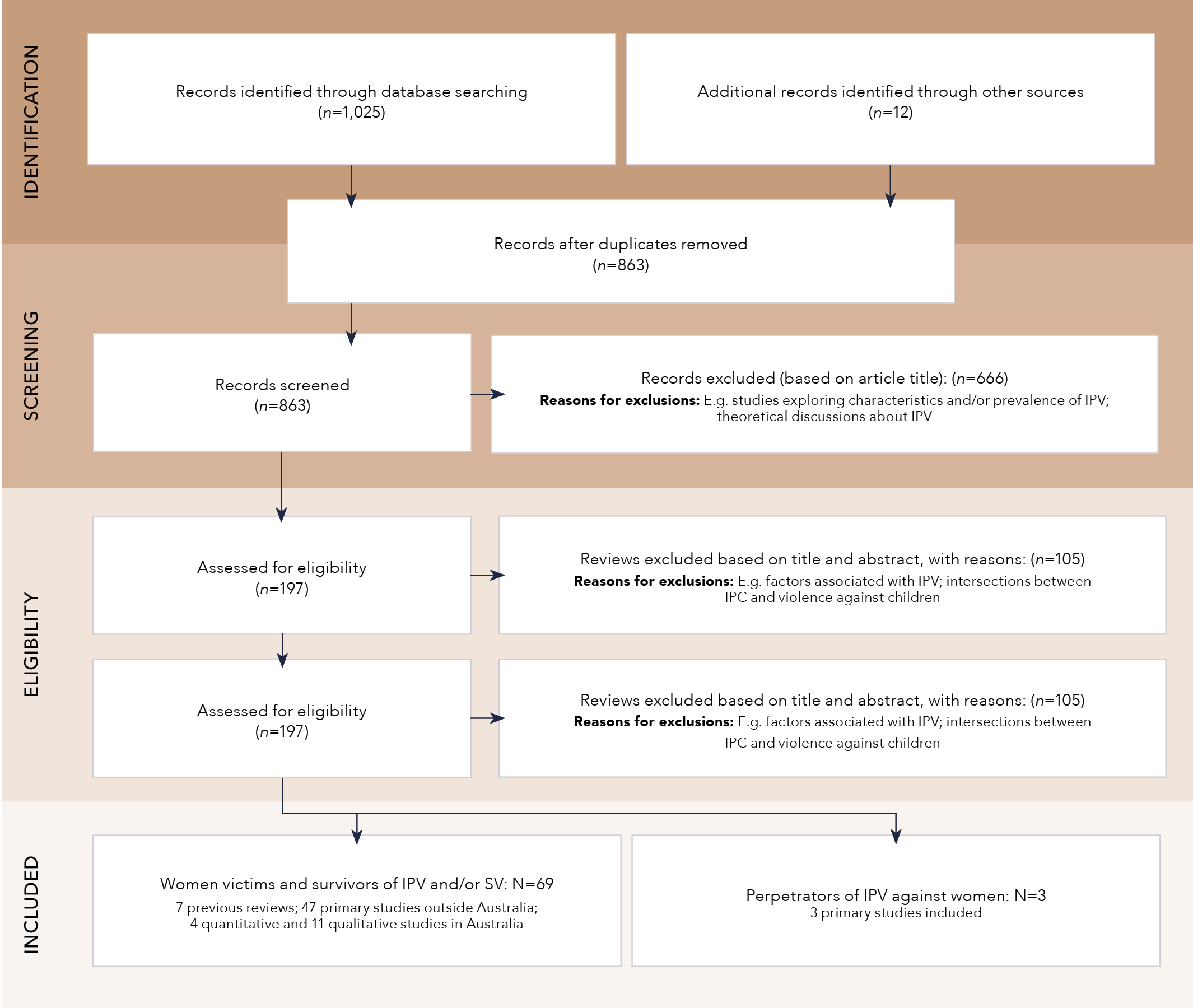
Text version of the figure above:
Identification:
- Records identified through database searching (n=1,035)
- Additional records identified through other sources (n=12)
Between Identification and Screening
- Records after duplicated removed (n=863)
Screening
- Records screened (n=863)
- Records excluded (based on article title): (n=666)
-
- Reasons for exclusions: E.g. studies exploring characteristics and/or prevalence of IPV; theoretical discussions about IPV
Eligibility
- Assessed for eligibility (n=197)
- Review excluded based on title and abstract, with reasons: (n=105)
-
- Reasons for exclusions: E.g. factors associated with IPV; intersections between IPC and violence against children
- Assessed for eligibility (n=197)
- Reviewed excluded based on title and abstract, with reasons: (n=105)
-
- Reasons for exclusions: E.g. factors associated with IPV; intersections between IPC and violence against children
Included
- Women victims and survivors of IPV and/or SV: N=69
-
- 7 previous reviews; 47 primary studies outside Australia; 4 quantitative and 11 qualitative studies in Australia
- Perpetrators of IPV against women: N=3
-
- 3 primary studies included
Help-seeking behaviours of IPV and/or SV victims and survivors
Overall, 69 records were related to women who experience IPV and/or SV (seven previous reviews; 47 primary studies outside Australia; four quantitative and 11 qualitative studies in Australia). Findings for the Australian context are reported in the main document.
In terms of women’s help-seeking for IPV more generally, 47 primary studies were based outside Australia, for example, in Canada (Barrett & Pierre, 2011), the United States (Anyikwa, 2015), Malaysia (Tengku Hassan et al., 2015), China (Hu et al., 2020) and Iraq (Strang et al., 2020). There were six global narrative reviews related to women’s help-seeking behaviours for experiences of IPV (Afrouz et al., 2020; Femi-Ajao et al., 2020; Fiolet et al., 2019; Lelaurain et al., 2017; Robinson et al., 2020; Satyen et al., 2019) and one review relating to help-seeking for SV (Martsolf et al., 2010). Not all the reviews focused exclusively on women, but women formed the vast majority of the participants. Characteristics of the included reviews are outlined in the Table A1.
Overall, the reviews were mostly limited to qualitative studies that explored barriers to IPV disclosure and help-seeking of women from culturally and linguistically diverse backgrounds. For example, for women from Black and minority ethnic populations, barriers to IPV disclosure included immigration status, unsupportive attitudes of staff within mainstream services and language-related barriers (Femi-Ajao et al., 2020), yet escalation of abuse and serious safety concerns for children were facilitators of help-seeking. In contrast, for Muslim women, maintaining family harmony, honour and reputation were among key barriers to IPV disclosure and help-seeking behaviours (Afrouz et al., 2020). A scoping review of global Indigenous studies found that Indigenous peoples are generally reluctant to engage in help-seeking behaviours for IPV due to shame, tight-knit communities, and inappropriate service responses causing mistrust and fear (Fiolet et al.,2019). For SV, Martsolf and colleagues (2010) found that victims and survivors wanted their abuse histories taken seriously and expected service providers to display professional competence and sensitivity. Fear of not being believed was a barrier to help-seeking, as were judgemental or dismissive responses.
In terms of study quality, many studies included in the above reviews were found to have major methodological limitations. For example, studies did not adequately describe methods of data collection and/or analysis, and had minimum or no consideration of ethical issues. Similarly, most quantitative studies included in Satyen et al.’s review (2019) were classified as having a high risk of bias due to sampling bias or recall bias.
Table A1: Characteristics of reviews exploring women’s help-seeking for IPV, 2010–2020
Study
Aim and objectives
Design
Included studies
No. of participants
Data synthesis
Summary of findings
Study quality and limitations
Femi-Ajao et al., 2020
To explore barriers to IPV disclosure; facilitators of help-seeking; and self-perceived impacts of IPV
Qualitative systematic review
4 qualitative studies (8 publications)
83 women (Black and minority ethnic populations)
Thematic analysis
Barriers to IPV disclosure:
- Immigration status, unsupportive attitudes of staff within mainstream services, language-related barriers
Facilitators of help-seeking:
- Escalation of abuse, safety of children
Impact of IPV:
Loss of identity, shame, denial of abuse, lack of choice as women
- Quality appraisal using CASP tool indicated major methodological weaknesses in the included studies (e.g. non-reliable methods, no consideration of ethical issues)
- Very small number of included studies limits the generalisability of the findings
Afrouz et al., 2020
To explore Muslim women’s barriers to IPV disclosure and help-seeking
Critical systematic review
21 (14 qualitative and mixed method, 6 quantitative, and 1 literature review)
567 Muslim women (qualitative studies)
Thematic analysis
Barriers to IPV disclosure and help-seeking:
- Perception of IPV as a private issue
- Maintain family harmony, honour and reputation
- Fear of abuser’s retaliation
- Financial issues post-divorce and separation
- Shame and embarrassment
- Quality appraisal using CASP tool indicated major methodological weaknesses in the included studies (e.g. no details about sampling procedures, data analysis, ethics, confidentiality or consent)
Fiolet et al., 2019
To explore the views Indigenous peoples have on help-seeking for IPV
Scoping review
15 studies (11 qualitative)
600 Indigenous women
Thematic analysis
Indigenous peoples are reluctant to engage in help-seeking behaviours:
- Barriers of shame, tight-knit communities, and inappropriate service responses causing mistrust and fear
- Turning to informal support networks, and help is sought when crisis point is reached
- Most participants were recruited from groups who were accessing services, so do not represent women who are not accessing services
- As a scoping review, no study appraisal was conducted
LeLaurain et al., 2017
To explore factors that facilitate or inhibit help-seeking for IPV
Systematic review
90 studies (47 qualitative or mixed methods)
Not reported
Barriers and facilitators to IPV help-seeking:
- Help-seeking is impacted by violence severity; environmental factors; issues relating to children; sociodemographic characteristics; social stigma; patriarchal norms; psychological costs of violence; feelings about partner; and religion
- Quality appraisal not undertaken
Martsolf et al., 2010
To explore how victims and survivors of SV utilise professional services
Systematic review and meta-summary
31 qualitative studies
1,024 total, 984 women
Qualitative meta-summary
Barriers and facilitators to SV help-seeking:
- Barriers included abuse not being taken seriously/dismissed; lack of professional competence; lack of sensitivity; not being believed
- Facilitators were the reverse of barriers
- Quality appraisal not undertaken
Robinson et al., 2020
To explore barriers to help-seeking from formal services for IPV survivors
Systematic review
29 (22 qualitative)
862 women living in US
Thematic analysis
Barriers to help seeking:
- Lack of awareness, access challenges, consequences of disclosure, lack of material resources, personal barriers, system failures
- Quality appraisal not undertaken
Satyen et al., 2019
To explore cross-cultural differences in help-seeking behaviour of women who have experienced IPV
Systematic review
17 (quantitative)
40,904
Narrative synthesis
- Help-seeking behaviour for IPV survivors is not uniform across cultural groups and sometimes within cultural groups
- Overall, Caucasian women were more likely to seek assistance from formal services such as mental health and social services
- Latina/Hispanic and African American women were more likely to utilise other types of formal supports such as hospital and law enforcement services
- Minority groups do not request help even from those close to them (e.g. family and friends)
- Most studies classified as high risk of bias (e.g. sampling bias, recall bias)
Notes: CASP = Critical Appraisal Skills Programme
Help-seeking by people who use IPV and/or SV, 2010–2020
Studies focused on the help-seeking behaviours of people who use violence are extremely limited. This is the case for self-identified perpetrators who have accessed services voluntarily, perpetrators who have been mandated into services, and perpetrators who have not been identified as such and use community and health services. Although there is some limited literature published prior to 2010, our search found only three studies focused on male perpetrators of IPV published between 2010 and 2020 (see Table A2). No relevant articles were found about women’s use of IPV and/or SV and their help-seeking behaviours, nor any articles that focused on the perpetration of IPV and/or SV.
In general, research undertaken to date on perpetrators of IPV has been primarily focused on assessing the efficacy of specific programs (for example, men’s behaviour change programs) rather than exploring perpetrator service needs or experiences overall. This may be in large part because the system is designed to respond to violence after it has occurred rather than trying to engage and tailor services to perpetrators before risk has escalated. Some limited exceptions include studies exploring the service needs of men attending programs to address both IPV and other co-occurring problems. For example, in a quantitative study of men attending a substance treatment program who had also used IPV, Wu et al. (2010) found that the majority of participants indicated a need for medical, employment, substance use, legal, psychological and family services. Service needs were heightened in the period following criminal justice system involvement. Althoughthe study suffered from some methodological limitations, the authors cautiously concluded that their findings are suggestive of the willingness of perpetrators to seek help, and that therefore efforts ought to focus on engaging men rather than mandating or coercing them into accessing services. A mixed-method study by Hashimoto and colleagues (2018) – also with men in substance use treatment – explored pathways and barriers to disclosure and help-seeking. They found that participants were more likely to disclose perpetration to family, friends or other informal supports, but to seek help from formal services such as health professionals. Barriers to disclosure included fear of child removal, shame and embarrassment, and normalisation or minimisation of their behaviours. Another mixed-method study with men attending general practices who had used or experienced IPV (Morgan et al., 2014) found that men wanted to be asked abouttheir use of violence and were more likely to seek support via friends and family or health settings. They also reported shame and a reluctance to receive difficult feedback as barriers to disclosure.
Table A2: Characteristics of studies exploring help-seeking for IPV perpetration
Study
Aim and objectives
Design
Included studies
No. of participants
Data synthesis
Summary of findings
Study quality and limitations
Hashimoto et al., 2018
To examine IPV perpetration disclosure and help-seeking among male IPV perpetrators receiving substance use treatment
Mixed method primary study
UK (substance use treatment)
170 men
(20 men for qualitative phase)
Thematic analysis and logistic regression
Men who disclosed IPV perpetration to both formal and informal resources had:
- significantly higher support for gender equitable norms
- dependent children
- been arrested for IPV
- perceived IPV as a crime
Barriers to disclosure and help-seeking for IPV perpetration:
- fear that their children would be taken into care by social services
- shame and embarrassment
- minimisation or normalisation of their behaviour
- Only men receiving substance use treatment were recruited
- 20/170 men did not answer the questions on help-seeking behaviours for IPV
Morgan et al., 2014
To explore male help-seeking practices in relation to IPV
Mixed method primary study (cross-sectional survey and interview)
UK (general practice)
1,368 men attending general practice (31 interviews)
Thematic analysis and descriptive statistics
Men were most likely to seek informal support from friends or family. The next most likely source of support was the family doctor
- Study only approached men attending general practice clinics
Wu et al., 2010
To explore help-seeking associations and barriers among men attending a methadone maintenance treatment program who had used IPV
Face-to-face structured interview
US
108 men
Logistic regression
Men expressed the need for support from medical, employment, substance use, legal, psychological and family services. These needs were heightened closer to time of involvement with criminal justice
- Small sample size and non-normal distributions limited analyses
- Only a sample of men already accessing services for substance misuse
Appendix B:
Survey (Victims and survivors)
Start of Block: Screening
Q265 Hello, thank you for taking an interest in the VOICES project. Before we start, we need to ask you some initial questions in order to understand whether the project is suited to you and your experiences. It should take approximately 2 minutes to complete. Upon completion of these initial questions, if the survey is a good match to you and your experiences, you will automatically proceed to the main survey. Participating in the survey will help us understand women’s experiences and need for services. Responses to the survey are strictly confidential. Your voice is important. If you have any questions, please contact the project team at voice_project@unimelb.edu.au. Remember there are resources available here if you need support at any time.
Q266 How do you identify?
- Male (1)
- Female (2)
- Non-binary (3)
- Prefer not to say (4)
- Prefer to self-identify (5) ________________________________________________
Q267 How old are you?
- 17 or younger (1)
- 18–24 (0)
- 25–34 (2)
- 35–44 (3)
- 45+ years (4)
Q268 What country do you live in?
- China (1)
- Australia (0)
- India (2)
- England (3)
- Indonesia (4)
- Canada (5)
- Other (6) ________________________________________________
Q269 How did you find this survey?
- Domestic violence service (1)
- Community service (2)
- Twitter (3)
- Instagram (4)
- Facebook (5)
- University of Melbourne student notices (6)
- Other (7) ________________________________________________
Q270 In the last five years have you ever… (Please select all that apply)
- Been afraid of a partner? (1)
- Been controlled by a partner? (2)
- Been physically hurt by a partner? (3)
- Experienced unwanted sex by anyone, including a partner? (4)
- None of the above (0)
Q271 The following question is asked to determine if you are a human or a robot…
Q272 What is 2+2?
- 6 (1)
- 8 (2)
- 4 (3)
Display This Question:
If How do you identify? = Female
Or How old are you? = 17 or younger
Or What country do you live in? = Australia
Or In the last five years have you ever… (please select all that apply) = None of the above
Or What is 2+2? = 4
Q276 We thank you for your interest in our project and for reading through the provided materials. As the present project is about adult women’s experiences of fear or violence within intimate partner relationships who live in Australia, one or more of your answers has made you ineligible for the current study. If you have any questions, please email the project team here: voice_project@unimelb.edu.au.
Remember, there are resources available here if you need support at any time.
Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed
End of Block: Screening
Start of Block: INTRO_BLOCK
Display This Question:
If How do you identify? = Female
And How old are you? = 17 or younger
And What country do you live in? = Australia
And In the last five years have you ever… (please select all that apply) = None of the above
And What is 2+2? = 4
Q1 Welcome to the VOICES Project survey. Thank you for answering our initial questions, it looks as if you are eligible to complete the survey. The VOICES Project aims to understand your experiences of abuse and violence during your lifetime and what supports you might need from services. Your answers will help us further understand how to best support women’s health and wellbeing.
This survey asks about some background information, health and wellbeing, domestic violence and unwanted sexual experiences, and how we can support women more effectively. Some of the questions are sensitive so there are resources available by clicking here. These resources will also be made available throughout the survey.
All information you give us in this survey is confidential. The survey will take approximately 30 minutes to complete. After completing the survey, you will be given the option to enter into a draw to win an iPad. The project team is based at the Safer Families Centre, The University of Melbourne and ANROWS. If you have any questions about the project, please email: voice_project@unimelb.edu.au.We recommend that you complete the survey in private, please click here for further advice on keeping safe online. Feel free take a break at any time. Remember, if you exit the survey and return later, as this survey is anonymous, you will only be returned to where you left off if you use the same device that you started the survey on.
How to fill in the survey:
Please read the questions carefully and follow the instructions. There are no right or wrong answers, just put what is right for you. Please select only one answer per question unless we state that you can answer more than one answer.
End of Block: INTRO_BLOCK
Start of Block: ABOUT_YOU
Q2 About You We will start this survey with a few quick questions about your background. These questions are important because they allow your answers to be compared with those of other people with a similar background to you, without identifying anybody.
Q3 Do you identify as a woman?
- Yes (1)
- No (0)
Display This Question:
If Do you identify as a woman? = No
Q4 We thank you for your interest in our project and for reading through the provided materials. As the present project is about women’s experiences, this makes you ineligible. Should you wish to speak with someone from the project team, please contact Jacqueline by emailing Voice_Project@unimelb.edu.au. Should you wish to speak with someone for support, resources are available. Please click here. Once again, we thank you for your time and interest in the VOICES Project.
Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed
Q5 What is your age in years?
Please write a number in the box.
________________________________________________________________
Q6 What is your postcode where you live most of the time?
________________________________________________________________
Q7 Were you born in Australia?
- Yes (1)
- No (0)
Display This Question:
If Were you born in Australia? = No
Q8 Which country were you born in? Please select one option.
- UK (1)
- New Zealand (2)
- China (3)
- Other (4)
- Sri Lanka (5)
- India (6)
- Italy (7)
- South Africa (8)
- Greece (9)
- Lebanon (10)
- Vietnam (11)
Display This Question:
If Were you born in Australia? = No
Q9 How long have you lived in Australia? Please write the number of years in the box below. If you are not sure, your best guess is fine.
________________________________________________________________
Display This Question:
If Were you born in Australia? = No
Q10 Are you…
- An Australian citizen? (1)
- On a permanent visa? (2)
- On a temporary visa? (3)
Q11 Is English your first language?
- Yes (1)
- No (0)
Q12 Do you identify as Aboriginal or Torres Strait Islander?
- Yes, Aboriginal (1)
- Yes, Torres Strait Islander (2)
- Yes, both Aboriginal and Torres Strait Islander (3)
- No, neither (4)
Q13 What is the gender of your current partner?
- Male (1)
- Female (2)
- Non-binary (3)
- Prefer not to disclose (4)
I do not have a current partner (5)
Q14 Who do you usually live with?
Please select all that apply.
- No one else (1)
- Your husband (2)
- Your male partner (3)
- Other relatives (7)
- Friends (8)
- Other (please specify) (9)
- Your female partner (10)
- Unrelated flat mate or co-tenant (4)
Q15 Do you have children?
- Yes (0)
- No (1)
Display This Question:
If Do you have children? = Yes
Q16 How many children are currently at home with you?
- No children (0)
- One child (1)
- Two children (2)
- Three children (3)
- Four or more children (4)
Q17 What is your present marital status?
This does not necessarily refer to your current living arrangement. Please select one option only.
- Never married (1)
- Widowed (2)
- Divorced (3)
- Separated but not divorced (4)
- Married (5)
Q18
This is the end of this section. When you feel ready, please click the next button to continue.
End of Block: ABOUT_YOU
Start of Block: HEALTH_WELLBEING
Q19
About your health and wellbeing This section is about how you’re feeling, both emotionally and physically. We are asking these questions because we are interested in how any relationship issues affects your emotional and physical wellbeing.
Q20 In general, would you say your health is:
- Excellent (1)
- Very good (2)
- Good (3)
- Fair (4)
- Poor (5)
Q21 Over the last 2 weeks, how often have you been bothered by the following problems?
Not at all (0)
Several days (1)
More than half the days (2)
Nearly every day (3)
Feeling nervous, anxious or on edge (1)
Not being able to stop or control worrying (2)
Feeling down, depressed, or hopeless (4)
Little interest or pleasure in doing things (5)
Q22 Do you have any long-term illness, health problem or disability, which limits your daily activities or the work you can do (including problems that are due to old age)?
- Yes (1)
- No (0)
Q23 Below are some statements about how you feel in yourself. Please read each statement and choose the response that most closely indicates how you have felt during the past month.
Yes (1)
No (0)
Do you avoid being reminded of experiences by staying away from certain places, people or activities? (1)
Have you lost interest in activities that were once important or enjoyable? (2)
Have you begun to feel more distant or isolated from other people? (3)
Do you find it hard to feel love or affection for other people? (4)
Have you begun to feel that there is no point in planning for the future? (5)
Have you had more trouble than usual falling or staying asleep? (6)
Do you become jumpy or easily startled by ordinary noise or movements? (7)
Q24 Because alcohol use can affect health, it is important that we ask you some questions about your use of alcohol. Your answers will remain confidential, so please be as accurate as possible. Try to answer the questions in terms of “standard drinks”.
Q25
Q26 For the following questions, please select the answer which best applies to your drinking in the last year.
Never (1)
Less than monthly (2)
Monthly (3)
Weekly (4)
Daily or almost daily (5)
How often do you have SIX or more drinks on one occasion? (1)
How often during the last year have you been unable to remember what happened the night before because you had been drinking? (2)
How often during the last year have you failed to do what was normally expected of you because of drinking? (3)
Q27 In the last year, has a relative or friend, doctor or other health worker been concerned about your drinking or suggested you cut down?
- No (0)
- Yes, on one occasion (1)
- Yes, on more than one occasion (2)
Q28
Thank you for the information you have provided so far, we have a good picture of your background and health. We are now moving into more sensitive childhood and relationships questions. When you feel ready, please click next to continue.
End of Block: HEALTH_WELLBEING
Start of Block: RELATIONSHIPS_ACE
Q29 About your childhood
The following questions are about possible experiences you may have had as a child (before the age of 18). Some questions may bring up distressing memories. If this happens, help is available. Please click here if you would like some support.
Q30 While you were growing up, during your first 18 years of life:
Did a parent or other adult in the household OFTEN … Swear at you, insult you, put you down, or humiliate you? OR Act in a way that made you afraid that you might be physically hurt?
- Yes (1)
- No (0)
Q31 Did a parent or other adult in the household OFTEN … Push, grab, slap, or throw something at you? OR Ever hit you so hard that you had marks or were injured?
- Yes (1)
- No (0)
Q32 Did an adult or person at least 5 years older than you EVER… Touch or fondle you or have you touch their body in a sexual way? OR Try to or actually have oral, anal, or vaginal sex with you?
- Yes (1)
- No (0)
Q33 These next questions are about possible experiences you may have had as a child (before the age of 18).
Did you OFTEN feel that … No one in your family loved you or thought you were important or special? OR Your family didn’t look out for each other, feel close to each other, or support each other?
- Yes (1)
- No (0)
Q34 Did you OFTEN feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? OR Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
- Yes (1)
- No (0)
Q35 Were your parents EVER separated or divorced?
- Yes (1)
- No (0)
Q36 These next questions are about possible experiences you may have had as a child (before the age of 18).
Was your mother or stepmother OFTEN pushed, grabbed, slapped, or had something thrown at her? OR SOMETIMES OR OFTEN kicked, bitten, hit with a fist, or hit with something hard? OR EVER repeatedly hit over at least a few minutes or threatened with a gun or knife?
- Yes (1)
- No (0)
Q37 Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
- Yes (1)
- No (0)
Q38 Was a household member depressed or mentally ill or did a household member attempt suicide?
- Yes (1)
- No (0)
Q39 Did a household member go to prison?
- Yes (1)
- No (0)
Q40
This is the end of this section. If any of these questions have been in any way distressing and you would like support, please click here. When you feel ready, please click the next button to continue.
End of Block: RELATIONSHIPS_ACE
Start of Block: RELATIONSHIPS_NCAS
Q41 About your relationships
This section asks you some personal questions about your attitudes towards relationships and your experiences in your relationships. The purpose of asking these questions is to understand your needs from services. Your responses are anonymous. We recognise that some of these questions may be sensitive for people, and if you would like support, it is available by clicking here.
Q42 Here are some statements about gender roles, stereotypes and gender equality. Thinking about Australian society generally, please indicate the degree to which you agree or disagree.
MANY women mistakenly interpret innocent remarks or acts as being sexist.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q43 MANY women exaggerate how unequally women are treated in Australia.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q44 MANY women fail to fully appreciate all that men do for them.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q45
Here are some statements about gender roles, stereotypes and gender equality. Thinking about Australian society generally, please indicate the degree to which you agree or disagree.
Women prefer a man to be in charge of the relationship.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q46 Men should take control in relationships and be the head of the household.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q47 On the whole, men make better political leaders than women.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q48 Here are some statements about gender roles, stereotypes, and gender equality. Thinking about Australian society generally, please indicate the extent to which you agree or disagree.
In the workplace, men generally make more capable bosses than women.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q49 I think there’s no harm in men making sexist jokes about women when they are among their male friends.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q50 When a couple start dating, the woman should not be the one to initiate sex.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q51 I think it is embarrassing for a man to have a job that is usually filled by a woman.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
End of Block: RELATIONSHIPS_NCAS
Start of Block: RELATIONSHIPS_CAS
Q52 These questions are about your experiences in adult intimate relationships. By “adult intimate relationship”, we mean a current or former husband/wife, partner or boy/girlfriend for longer than one month. Have you ever been in an adult intimate relationship? Since you were 16 years of age.
- Yes (1)
- No (0)
Skip To: End of Block If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship”… = No
Q53 Have you been in an adult intimate relationship in the past 12 months?
- Yes (1)
- No (0)
Skip To: Q103 If Have you been in an adult intimate relationship in the past 12 months? = No
Q54 Are you currently in an intimate relationship?
- Yes (1)
- No (0)
Skip To: Q56 If Are you currently in an intimate relationship? = No
Q55 Are you currently afraid of your partner or ex-partner?
- Yes (1)
- No (0)
Q56 Have you been afraid of any partner or ex-partner in the past 12 months?
- Yes (1)
- No (0)
Q57 Have you ever been afraid of any partner or ex-partner?
- Yes (1)
- No (0)
Q58 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Blamed me for causing their violent behaviour
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or form… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q59 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q60 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q61 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Shook, pushed, grabbed or threw me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q62 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q63 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q64 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner: Tried to convince my family, children or friends that I am crazy or tried to turn them against me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q65 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q66 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q67 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Used or threatened to use a knife or gun or other weapon to harm me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q68 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q69 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q70 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Made me perform sex acts that I did not want to perform
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q71 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q72 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q73 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Followed me or hung around outside my home or work
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q74 How often has this happened in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often has this happened in the past 12 months? = Once in the past 12 months
Or How often has this happened in the past 12 months? = A few times in the past 12 months
Or How often has this happened in the past 12 months? = Monthly
Or How often has this happened in the past 12 months? = Weekly
Or How often has this happened in the past 12 months? = Daily/almost daily
Q75 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q76 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Threatened to harm or kill me or someone close to me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q77 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q78 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q79 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Choked me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q80 How often did this happen in past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in past 12 months? = Once in the past 12 months
Or How often did this happen in past 12 months? = A few times in the past 12 months
Or How often did this happen in past 12 months? = Monthly
Or How often did this happen in past 12 months? = Weekly
Or How often did this happen in past 12 months? = Daily/almost daily
Q81 Who behaved in this way towards you? Please select all that apply.
A male partner/ex-partner (1)
A female partner/ex-partner (2)
Q82 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Forced or tried to force me to have sex
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q83 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q84 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q85 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Harassed me by phone, text, email or using social media
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q86 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q87 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q88 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Told me I was crazy, stupid or not good enough
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q89 How often has this happened in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often has this happened in the past 12 months? = Once in the past 12 months
Or How often has this happened in the past 12 months? = A few times in the past 12 months
Or How often has this happened in the past 12 months? = Monthly
Or How often has this happened in the past 12 months? = Weekly
Or How often has this happened in the past 12 months? = Daily/almost daily
Q90 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q91
We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Hit me with a fist or object, kicked or bit me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q92 How often has this happened in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often has this happened in the past 12 months? = Once in the past 12 months
Or How often has this happened in the past 12 months? = A few times in the past 12 months
Or How often has this happened in the past 12 months? = Monthly
Or How often has this happened in the past 12 months? = Weekly
Or How often has this happened in the past 12 months? = Daily/almost daily
Q93 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q94
We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner: Kept me from seeing or talking to my family or friends
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or form… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q95 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q96 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q97 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Confined or locked me in a room or other space
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q98 How often did this happen in the past 12 months?
Not in the past 12 months (0)
Once in the past 12 months (1)
A few times in the past 12 months (2)
Monthly (3)
Weekly (4)
Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q99 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q100
We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Kept me from having access to a job, money or financial resources
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q101 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q102 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q103 Are you currently afraid of your partner or ex-partner?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q104 Have you ever been afraid of any partner or ex-partner?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q105 We would like to know if you have ever experienced any of the actions listed below from any current or former partners.
Yes (1)
No (0)
Blamed me for causing their violent behaviour (1)
Shook, pushed, grabbed or threw me (4)
Tried to convince my family, children or friends that I am crazy or tried to turn them against me (5)
Used or threatened to use a knife or gun or other weapon to harm me (6)
Made me perform sex acts that I did not want to perform (7)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q106 We would like to know if you have ever experienced any of the actions listed below from any current or former partners.
Yes (1)
No (0)
Followed me or hung around outside my home or work (9)
Threatened to harm or kill me or someone close to me (18)
Choked me (10)
Forced or tried to force me to have sex (11)
Harassed me by phone, text, email or using social media (12)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q107 We would like to know if you have ever experienced any of the actions listed below from any current or former partners.
Yes (1)
No (0)
Told me I was crazy, stupid, or not good enough (13)
Hit me with a fist or object, kicked or bit me (14)
Kept me from seeing or talking to my family or friends (15)
Confined or locked me in a room or other space (16)
Kept me from having access to a job, money, or financial resources (17)
Q108 Thank you for all your answers so far. You are at the half-way point of the survey. Please remember that your answers will contribute to helping us make services better for everyone in the community. If at any time you would like to take a break you may do so and return to the place you are up to (as long as you use the same device). If you would like to speak to anyone about anything distressing that has arisen for you so far, please click here.
End of Block: RELATIONSHIPS_CAS
Start of Block: RELATIONSHIPS_SV+RC
Q109 The next questions are about unwanted sexual experiences. These experiences may have occurred inside or outside of an intimate relationship. Remember that the survey is anonymous. If you do not feel comfortable answering any of the questions, skip them and go on to the next question. In this questionnaire, when we talk about “sex” we mean any kind of sex (vaginal, anal, oral etc.)
Q110 Since the age of 15, has any man or woman ever forced you or tried to force you into sexual activity against your will?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q111 Has a current or previous partner ever physically forced you to have sex when you did not want to? Did this happen once, a few times or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q112 Have you ever had sex with a current or previous partner when you did not want to because you were afraid of what he might do? Did this happen once, a few times or many times?
Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q113 Has your current or previous partner ever forced to watch pornography when you did not want to? Did this happen once, a few times or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q114 Has a current or previous partner ever forced you to do something else sexual that you did not want to? Did this happen once, a few times or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q115 Has any current or past partner ever pressured, forced or threatened you to become pregnant?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q116 Has any current or past partner ever used threats, pressure or force to prevent you from terminating a pregnancy?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q117 Has any current or past partner ever pressured, forced or threatened you to terminate a pregnancy?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q118 Has any current or past partner ever interfered with contraception in order to get you pregnant when you did not want to be (e.g. disposed of contraception, tampered with contraception, prevented you from obtaining contraception)?
- Yes (1)
- No (0)
Q119
This is the end of this section. Thank you for taking the time to answer these questions, some of which may have been distressing. This is the end of the sensitive questions about experiences you have had in your relationships. Below is a breathing exercise that may reconnect you with where you are in this moment, here and now. If you are feeling distressed or anxious, click on this link for a grounding technique that may help you anchor back to the present. If you would like to speak to someone for support, click here for a list of support services.
When you feel ready, press the next button to continue taking the survey. We really appreciate your time.
Q120
End of Block: RELATIONSHIPS_SV+RC
Start of Block: HELP_Q1
Q121 Your views on services
This section asks you about your use of services in the community. This information may help us understand how people use services and where there may be gaps in your support needs.
Q122 Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? Please tick all that apply.
- Friend/s (1)
- Family member (18)
- Partner (19)
- General practitioner (2)
- Nurse (20)
- Psychologist or counsellor (3)
- Social worker (Hospital/community health) (4)
- Alcohol or drug worker (5)
- Family therapist (6)
- Other (please specify) (7) ________________________________________________
- Telephone helpline (e.g. Lifeline, 1800 RESPECT) (8)
- Domestic or family violence service (9)
- Sexual assault service (21)
- Police (10)
- Legal service (e.g. solicitor or legal aid) (11)
- Financial service (e.g. Centrelink) (12)
- Housing service (13)
- Work colleague or boss (14)
- Priest/minister/rabbi or any other religious person (15)
- I did not seek advice or support (17)
End of Block: HELP_Q1
Start of Block: HOW HELPFUL
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Friend/s
Q123 How helpful was your friend/s?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Family member
Q124 How helpful was your family member?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Partner
Q125 How helpful was your partner?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = General practitioner
Q126 How helpful was the general practitioner?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Nurse
Q127
How helpful was the nurse?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Psychologist or counsellor
Q128 How helpful was the psychologist or counsellor?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Social worker (Hospital/community health)
Q129 How helpful was the social worker (hospital or community based)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Alcohol or drug worker
Q130 How helpful was alcohol or drug worker?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? … = Family therapist
Q131 How helpful was the family therapist?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Telephone helpline (e.g. Lifeline, 1800 RESPECT)
Q132 How helpful was the telephone helpline (e.g. Lifeline, 1800RESPECT)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Domestic or family violence service
Q133 How helpful was the domestic or family violence service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Sexual assault service
Q134 How helpful was the sexual assault service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Police
Q135 How helpful was the police?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Legal service (e.g. solicitor or legal aid)
Q136 How helpful was the legal service (e.g. solicitor or legal aid)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Financial service (e.g. Centrelink)
Q137 How helpful was the financial service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Housing Service
Q138 How helpful was the housing service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Work colleague or boss
Q139 How helpful was your work colleague or boss?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Priest/minister/rabbi or any other religious person
Q140 How helpful was the priest/minister/rabbi or any other religious person?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Other (please specify)
Q141 How helpful was Q122/ChoiceTextEntryValue/?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
End of Block: HOW HELPFUL
Start of Block: BLOCK2_POPUP
Q142 Below is a list of reasons you may not have spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters. Please rate how important each is to your own situation.
I have no time to talk to someone about these things.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q143 I feel too ashamed to talk to anyone.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q144 The professional will not understand me.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q145 The professional will tell others.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q146 My friends or family will find out.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q147 My partner’s behaviours are just a normal part of relationships. I don’t believe there is any need to see a professional about them.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q148 My partner’s behaviour was a once-off. It won’t happen again.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q149 I have no access to transport to see someone.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q150 Below is a list of reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters. Please rate how important each is to your own situation.
I don’t know of any service that might be able to help.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q151 I don’t want to talk to anyone about my partner’s behaviours, it is too personal.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q152 I decided not to seek care as I’m not sure it would be helpful.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q153 I had too many personal or family responsibilities to seek help.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q154 I was uncertain who to see.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q155 My culture or religion is a barrier for me seeking help.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q156 Are there any other reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Are there any other reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters? Text Response Does Not Contain No
And Are there any other reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters? Text Response Is Not Empty
Q157 Please rate how important this is to your own situation.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q158 Was there a time that you needed help for relationship issues or unwanted sexual encounters but could not get it?
- Yes (1)
- No (0)
Display This Question:
If Was there a time that you needed help for relationship issues or unwanted sexual encounters but … = Yes
Q159 How much did each of the service barriers below prevent you from accessing help? Select one option per line.
Not at all (1)
A small amount (2)
Moderately (3)
Quite a lot (4)
Extremely (5)
Language or translation problems (1)
Cost (2)
Limited opening hours (3)
No service available in the area at the time needed (4)
Waiting time too long (5)
No appointments (6)
Not taking new patients (7)
Trouble understanding the terms used by the professional (8)
Lack of awareness of available services (9)
Concerns regarding confidentiality (10)
No private health insurance (11)
Other barriers (12)
End of Block: BLOCK2_POPUP
Start of Block: BLOCK1_POP UP
Q160 Reflecting on any contact or experiences you’ve had with services, what would you value most in a service? Please rate how important you think each of the factors below are.
Not feeling judged or put down
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q161 Knowing that whatever I said would be held in confidence by the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q162 The professional being interested in who I was as a person
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q163 Reflecting on any contact or experiences you’ve had with services, what would you value most in a service? Please rate how important you think each of the factors below are.
Feeling listened to by the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q164 Being given practical information about safety for myself and any children
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q165 The expertise of the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q166 Reflecting on any contact or experiences you’ve had with services, what would you value most in a service? Please rate how important you think each of the factors below are.
Learning new ways of escaping violence
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q167 Material support (e.g. getting access to accommodation)
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q168 Emotional support (having someone to talk to)
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q169 Knowing that whatever I said would be held in confidence by the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q170 Considering all the experiences you have had in talking to services about your partner’s behaviours, what do you believe that professionals need to do differently to better help people in similar situations as you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q171 Considering all the experiences you have had in talking to services about unwanted sexual encounters, what do you believe professionals need to do differently to better help people in similar situations as you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q172 The COVID-19 pandemic has changed the way we all access support services. What impact, if any, has it had on your access to support services for your behaviours in intimate relationships?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: BLOCK1_POP UP
Start of Block: HOW_HELPFUL_CONT
Q173 If you thought that your partner was close to using the behaviours you previously reported them using, how likely is it that you would seek help from the following people and services?
Very unlikely (1)
Unlikely (2)
Neither likely or unlikely (3)
Likely (4)
Very likely (5)
Friend (1)
Family member (20)
General practitioner (2)
Psychologist or counsellor (3)
Social worker (Hospital/community health) (4)
Alcohol or drug worker (5)
Family therapist (6)
Telephone helpline (e.g. Lifeline, 1800 RESPECT (7)
Domestic or family violence service (8)
Sexual assault service (19)
Police (10)
Legal service (e.g. solicitor or legal aid) (11)
Financial service (e.g. Centrelink) (12)
Housing service (13)
Work colleague or boss (14)
Priest/minister/rabbi or any other religious person (15)
I will not seek advice or support (17)
I would seek help from another not listed person (please specify) (18)
Q174 If you think about your partner’s/ex-partner’s behaviours towards you, what do you think your greatest need is from a service or professional?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have children? = Yes
Q175 If you think about your partner’s/ex-partner’s behaviours towards you and your children, what has been most helpful for your children’s needs?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have children? = Yes
Q176 If you think about your partner’s/ex-partner’s behaviours towards you and your children, what do you think services can do to best address your children’s needs?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q177 If you think about your partner’s/ex-partner’s behaviours towards you, what do you think has been most helpful for your partner in helping them to stop using violence and abuse?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q178 If you think about your partners’/ex-partner’s behaviours towards you, what do you think your partner might need that would help your partner stop using violence and abuse?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q179 How have your experiences in your adult intimate relationships changed during COVID-19 isolation?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q180 These next questions ask you to think about your relationship with your partner or ex-partner. Please complete the following sentences with the first words that come to mind. There are no right or wrong answers, just write what you feel.
I wish that my partner/ex-partner…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q181 I wish that service providers…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q182 I wish that my family…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q183 I wish that my friends…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q184
This is the end of this section. When you feel ready, please click the next button to continue with some further background questions.
End of Block: HOW_HELPFUL_CONT
Start of Block: MORE_ABOUT_YOU
Q185 More about you
This section asks more about your background and some personal details about education and finances. These questions are important because they allow your answers to be placed in a broader context, without identifying anybody. Please remember that all survey responses are anonymous.
Q186 Which of these most closely describes your sexual orientation?
- I am heterosexual (1)
- I am bisexual (2)
- I am lesbian (3)
- I am queer (4)
- I am pansexual (8)
- I am asexual (5)
- Not sure (7)
- I would prefer to self-describe (9) ________________________________________________
Q187 Which of the following best describes your prior schooling?
- Still at secondary school (1)
- Completed secondary school to end of Year 12 (2)
- Attended secondary school but did not complete Year 12 (3)
- Attended primary school only (4)
- Did not attend school (5)
Q188 What is your highest qualification since leaving school?
- Finished a degree or higher degree (1)
- Completed a diploma or certificate (2)
- Completed a trade apprenticeship or traineeship (3)
- Other (please specify) (4) ________________________________________________
Q189 Which of the following best describes your current occupational status?
- Part-time wage or salary earner (including self-employed) (1)
- Full-time wage or salary earner (including self-employed) (2)
- Unemployed, seeking work (3)
- Unemployed, not seeking work (4)
- Retired (5)
- Unpaid work (e.g. home duties, voluntary, carer) (6)
Q190 Do you hold a current Health Care Card?
- Yes (1)
- No (0)
Q191 How do you manage on your available income?
- Easily (1)
- Not too badly (2)
- Difficult some of the time (3)
- Difficult all of the time (4)
- Impossible (5)
Q192
This is the end of this section. There’s just one more section to go! When you feel ready, please click the next button to continue.
End of Block: MORE_ABOUT_YOU
Start of Block: FELT_COMPLETING
Q193 your views on this survey
This last section asks questions about how you felt while completing this survey to understand what it was like being involved in the VOICES project. Please select one box on each line.
Q194 I felt comfortable answering the questions about domestic violence and sexual violence in this survey.
- Strongly agree (1)
- Agree (2)
- Neither agree nor disagree (3)
- Disagree (4)
- Strongly disagree (5)
Q195 As a result of questions about domestic violence and sexual violence being asked in this survey, my feelings about my relationship are…
- More positive (1)
- Somewhat more positive (2)
- Unchanged (3)
- Somewhat more negative (4)
- More negative (5)
Q196 The questions I was asked in this survey made me feel that the problems in my relationship with my partner or ex-partner are my fault.
- Strongly disagree (1)
- Disagree (2)
- Neither disagree nor agree (3)
- Agree (4)
- Strongly agree (5)
Q197 As a result of being asked questions about domestic violence and sexual violence in this survey, my feelings about myself as a person are…
- Better (1)
- Somewhat better (2)
- About the same as before (3)
- Somewhat worse (4)
- Worse (5)
Q198 Responding to this survey has made me more open to dealing with possible problems in my relationship.
- Strongly disagree (1)
- Disagree (2)
- Neither agree nor disagree (3)
- Agree (4)
- Strongly agree (5)
Q199 I am glad to be a participant in the VOICES project.
- Strongly disagree (1)
- Disagree (2)
- Neither agree nor disagree (3)
- Agree (4)
- Strongly agree (5)
Q200 Please use the space below if there is anything else you would like to tell us about yourself or the survey.
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q201 Final thoughts
In your own words, what enables you to stay strong?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q202 Do you have any extra comments that you wish to make about any issues raised in the survey?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: FELT_COMPLETING
Start of Block: THANK_YOU
Q203
Make Sure You Click Submit!
This is the end of the survey. Thank you very much for the time and effort you have taken. When you click the submit button, your responses will be submitted anonymously. On the next page you can provide your contact details to enter in a draw to win an iPad in appreciation of your time. You can also tell us if you would like to participate in a follow up interview about your experiences and need for services. Thank you.
End of Block: THANK_YOU
Start of Block: Gift Voucher
Q257 Thank you for completing this survey and taking the time to assist us today.
Your participation will contribute to our understanding of how best to help and keep families safe. You will be given the option to enter into a draw to win an iPad in appreciation for your time and contribution. If you would like to enter the draw, please provide us with your name and best email address. Your name and email address will not be used for any other purposes; and your details will not be linked in any way to your survey responses.
Q258 Name
________________________________________________________________
Q259 Email address
________________________________________________________________
Q260 Together, with your help, we are trying to work out ways to improve the support and services women receive in relation to issues of domestic violence and sexual assault.
To achieve this goal, further research (e.g. interviews) on this topic may be required. Please tick yes if you would be happy to be contacted by the researchers for involvement in further research.
Your participation in further research is completely voluntary, and independent of the survey you have just completed. You can provide your details now but if you change your mind later, you are free to withdraw your interest without explanation when/if you are contacted for further research at some time in the future.
Q261 Would you like to participate in further research on this topic?
- Yes (1)
- No (2)
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q262 My first name is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q263 The best phone number(s) to safely contact me on is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q264 An alternative contact (e.g. email) is:
________________________________________________________________
End of Block: Gift Voucher
Appendix C:
Survey (People who use IPV and/or SV)
Start of Block: Screening
Q293 Hello, thank you for taking an interest in the VOICES project. Before we start, we need to ask you some initial questions in order to understand whether the project is suited to you and your experiences. It should take approximately 2 minutes to complete. Upon completion of these initial questions, if the survey is a good match to you and your experiences, you will automatically proceed to the main survey.
Participating in this survey will help us understand the experiences of people who are concerned about their behaviours in their intimate relationships and their need for services. Responses to the survey are strictly confidential. Your voice is important. Remember, there are resources available here if you need support at any time.
Q294 Have you had a partner in the last five years who identified as a woman?
- Yes (1)
- No (0)
Q295 How old are you?
- 17 or younger (1)
- 18–24 (0)
- 25–34 (2)
- 35–44 (3)
- 45+ (4)
Q296 What country do you live in?
- China (1)
- Australia (0)
- India (2)
- England (3)
- Indonesia (4)
- Canada (5)
- Other (6) ________________________________________________
Q297 How did you find this survey?
- Men’s referral service (1)
- Community service (2)
- Instagram (3)
- Twitter (4)
- Facebook (5)
- Gumtree (6)
- University of Melbourne student notices (7)
- Other (8) ________________________________________________
Q298 In the last five years have you ever… (please select all that apply)
- Been concerned about your behaviours in intimate relationships? (1)
- Believe your behaviour has scared a partner or ex-partner? (2)
- Sought help from anyone to address issues in your intimate relationships? (3)
- None of the above (0)
Q299 The following question is asked to determine if you are a human or a robot…
Q300 What is 2+2?
- 6 (1)
- 8 (2)
- 4 (3)
Display This Question:
If Have you had a partner in the last five years who identified as a woman? = No
Or How old are you? = 17 or younger
Or What country do you live in? = Australia
Or In the last five years have you ever… (please select all that apply) = None of the above
Or What is 2+2? = 4
Q304 We thank you for your interest in our project and for reading through the provided materials. As the present project is about experiences of fear and conflict in relationships with women living in Australia, one or more of your answers has made you ineligible for the current study. If you have any questions, please email the project team at: voice_project@unimelb.edu.au. Remember, there are resources available here if you need support at any time.
Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed
End of Block: Screening
Start of Block: intro
Display This Question:
If Have you had a partner in the last five years who identified as a woman? = Yes
And How old are you? = 17 or younger
And What country do you live in? = Australia
And In the last five years have you ever… (please select all that apply) = None of the above
And What is 2+2? = 4
Welcome to the VOICES Project survey Thank you for answering our initial questions, it looks as if you are eligible to complete the survey. The VOICES survey asks about some background information, your health and wellbeing, use of domestic violence and unwanted sexual experiences, and how we can support men, women and families more effectively. Some of the questions are sensitive so there are resources available by clicking here, these will be available throughout the survey. All information you give us in this survey is anonymous. The survey will take approximately 30 minutes to complete. After completing the survey, you will be given the option to enter into a draw to win an iPad.
The project team is based at the Safer Families Centre, The University of Melbourne and ANROWS. If you have any questions about the project, please email:voice_project@unimelb.edu.au.
We recommend that you complete the survey in private, please click here for further advice on keeping safe online. Feel free take a break at any time. Remember, if you exit the survey and return later, as this survey is anonymous, you will only be returned to where you left off if you use the same device that you started the survey on. How to fill in the survey Please read the questions carefully and follow the instructions. There are no right or wrong answers, just put what is right for you. Please select only one answer per question unless instructed otherwise.
End of Block: intro
Start of Block: About_you_block
Q2 About You We will start the survey with a few quick questions about your background. These questions are important because they allow your answers to be compared with those of other people with a similar background to you, without identifying anybody.
Q3 Have you ever had a partner who identified as a woman?
- Yes (1)
- No (0)
Display This Question:
If Have you ever had a partner who identified as a woman? = No
Q4 We thank you for your interest in our project and for reading through the provided materials. As the present project is about people who have been in relationships with women, this makes you ineligible. Should you wish to speak with someone from the project team, please contact Matt by emailing Voice_Project@unimelb.edu.au.
Should you wish to speak with someone for support, resources are available. Please click here. Once again, we thank you for your time and interest in the Voices Project.
Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed
Q5 What is your gender?
- Male (1)
- Female (2)
- Non-binary (3)
- Prefer to self-describe (4) ________________________________________________
Q6 What is your age in years?
________________________________________________________________
Q7 What is your postcode where you live most of the time?
________________________________________________________________
Q8 Were you born in Australia?
- Yes (1)
- No (0)
Display This Question:
If Were you born in Australia? = No
Q9 Which country were you born in?
- UK (1)
- New Zealand (2)
- China (3)
- India (4)
- Sri Lanka (5)
- Other (please specify) (6) ________________________________________________
- Italy (7)
- South Africa (8)
- Greece (9)
- Lebanon (10)
- Vietnam (11)
Display This Question:
If Were you born in Australia? = No
Q10 How long have you lived in Australia?
Please write the number of years in the box below. If you are not sure, your best guess is fine.
________________________________________________________________
Display This Question:
If Were you born in Australia? = No
Q11 Are you…
- An Australian citizen (1)
- On a permanent visa (2)
- On a temporary visa (3)
Q12 Is English your first language?
- Yes (1)
- No (0)
Q13 Do you identify as Aboriginal or Torres Strait Islander?
- Yes, Aboriginal (1)
- Yes, Torres Strait Islander (2)
- Yes, both Aboriginal and Torres Strait Islander (3)
- No, neither (4)
Q14 What is the gender of your current partner?
- Female (40)
- Non-binary (41)
- Prefer not to disclose (42)
- I do not have a current partner (43)
Q15 Who do you usually live with? Please select all that apply.
- No one else (1)
- Your wife (2)
- Your female partner (3)
- Your male partner (5)
- Other relatives (8)
- Friends (9)
- Unrelated flatmate or co-tenant (10)
- Other (please specify) (6) ________________________________________________
Q16 Do you have any children?
- Yes (1)
- No (0)
Display This Question:
If Do you have any children? = Yes
Q17 How many children are currently at home with you?
- No children (0)
- One child (1)
- Two children (2)
- Three children (3)
- Four or more children (4)
Q18 What is your present marital status?
This does not necessarily refer to your current living arrangement. Please select one option only.
- Never married (1)
- Widowed (2)
- Divorced (3)
- Separated but not divorced (4)
- Married (5)
Q19
This is the end of this section. When you feel ready, please click the next button to continue.
End of Block: About_you_block
Start of Block: Health_wellbeing_block
Q20 About your health and wellbeing This section is about how you’re feeling, both emotionally and physically. We are asking these questions because we are interested in how relationship issues affect your emotional and physical wellbeing.
Q21 In general, how would you say your health is? Please select one option only.
- Excellent (1)
- Very good (2)
- Good (3)
- Fair (4)
- Poor (5)
Q22 Over the last 2 weeks, how often have you been bothered by the following problems?
Please select one option on each line.
Not at all (0)
Several days (1)
More than half the days (2)
Nearly every day (3)
Little interest or pleasure in doing things (1)
Feeling down, depressed or hopeless (2)
Feeling nervous, anxious, or on edge (3)
Not being able to stop or control worrying (4)
Q23 Do you have any long-term illness, health problem or disability, which limits your daily activities or the work you can do (including problems that are due to old age)?
- Yes (1)
- No (0)
Q24 Below are some statements about how you feel in yourself. Please read each statement and choose the response that most closely indicates how you have felt during the past month.
Yes (1)
No (0)
Do you avoid being reminded of experiences by staying away from certain places, people or activities? (1)
Have you lost interest in activities that were once important or enjoyable? (2)
Have you begun to feel more distant or isolated from other people? (3)
Do you find it hard to feel love or affection for other people? (4)
Have you begun to feel that there is no point in planning for the future? (5)
Have you had more trouble than usual falling or staying asleep? (6)
Do you become jumpy or easily startled by ordinary noise or movements? (7)
Q25 Because alcohol use can affect health, it is important that we ask you some questions about your use of alcohol. Your answers will remain confidential, so please be as accurate as possible. Try to answer the questions in terms of “standard drinks”.
Q26
Display This Question:
If What is your gender? = Male
Or What is your gender? = Non-binary
Or What is your gender? = Prefer to self-describe
Q27 Please select the answer which best applies to your drinking in the last year.
Never (1)
Less than monthly (1)
Monthly (2)
Weekly (3)
Daily or almost daily (4)
How often do you have EIGHT or more drinks on one occasion? (1)
How often have you been unable to remember what happened the night before because you had been drinking? (2)
How often have you failed to do what was normally expected of you because of drinking? (3)
Display This Question:
If What is your gender? = Female
Q28 For the following questions, please select the answer which best applies to your drinking in the last year.
Never (0)
Less than monthly (1)
Monthly (2)
Weekly (3)
Daily or almost daily (4)
How often do you have SIX or more drinks on one occasion? (1)
How often during the last year have you been unable to remember what happened the night before because you had been drinking? (2)
How often during the last year have you failed to do what was normally expected of you because of drinking? (3)
Q29 In the last year, has a relative or friend, doctor or other health worker been concerned about your drinking or suggested you cut down?
- No (0)
- Yes, on one occasion (1)
- Yes, on more than one occasion (2)
Q30
Thank you for the information you have provided so far, we have a good picture of your background and health. We are now moving into more sensitive childhood and relationships questions. When you feel ready, please click next to continue.
End of Block: Health_wellbeing_block
Start of Block: ACES
Q31 About your childhood The following questions are about possible experiences you may have had as a child (before the age of 18). Some questions may bring up distressing memories. If this happens, support can be accessed by clicking here.
Q32 While you were growing up, during your first 18 years of life: Did a parent or other adult in the household OFTEN … Swear at you, insult you, put you down, or humiliate you? OR Act in a way that made you afraid that you might be physically hurt?
- Yes (1)
- No (0)
Q33 Did a parent or other adult in the household OFTEN … Push, grab, slap, or throw something at you? OR Ever hit you so hard that you had marks or were injured?
- Yes (1)
- No (0)
Q34 Did an adult or person at least 5 years older than you EVER… Touch or fondle you or have you touch their body in a sexual way? OR Try to or actually have oral, anal, or vaginal sex with you?
- Yes (1)
- No (0)
Q35 These next questions are about possible experiences you may have had as a child (before the age of 18). Did you OFTEN feel that … No one in your family loved you or thought you were important or special? OR Your family didn’t look out for each other, feel close to each other, or support each other?
- Yes (1)
- No (0)
Q36 Did you OFTEN feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? OR Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
- Yes (1)
- No (0)
Q37 Were your parents EVER separated or divorced?
- Yes (1)
- No (0)
Q38 These next questions are about possible experiences you may have had as a child (before the age of 18). Was your mother or stepmother: OFTEN pushed, grabbed, slapped, or had something thrown at her? OR SOMETIMES OR OFTEN kicked, bitten, hit with a fist, or hit with something hard? OR EVER repeatedly hit over at least a few minutes or threatened with a gun or knife?
- Yes (1)
- No (0)
Q39 Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
- Yes (1)
- No (0)
Q40 Was a household member depressed or mentally ill or did a household member attempt suicide?
- Yes (1)
- No (0)
Q41 Did a household member go to prison?
- Yes (1)
- No (0)
Q42
This is the end of this section. If any of these questions have been in any way distressing and you would like support, please click here. When you feel ready, please click the next button to continue.
End of Block: ACES
Start of Block: NCAS_Relationships
Q43 About your relationships
This section asks you some personal questions about your attitudes towards relationships and your experiences in your relationships. The purpose of asking these questions is to understand your needs from services. Your responses are anonymous. We recognise that some of these questions may be sensitive for people, and if you would like support, it is available by clicking here.
Q44 Here are some statements about gender roles, stereotypes and gender equality. Thinking about Australian society generally, please indicate the degree to which you agree or disagree. Please select one option per line.
Strongly disagree (1)
Somewhat disagree (2)
Somewhat agree (3)
Strongly agree (4)
Don’t know (5)
MANY women mistakenly interpret innocent remarks or acts as being sexist. (1)
MANY women exaggerate how unequally women are treated in Australia. (2)
MANY women fail to fully appreciate all that men do for them. (3)
Women prefer a man to be in charge of the relationship. (4)
Men should take control in relationships and be the head of the household. (5)
On the whole, men make better political leaders than women. (6)
In the workplace, men generally make more capable bosses than women. (7)
I think there’s no harm in men making sexist jokes about women when they are among their male friends. (8)
When a couple start dating, the woman should not be the one to initiate sex. (9)
I think it is embarrassing for a man to have a job that is usually filled by a woman. (10)
End of Block: NCAS_Relationships
Start of Block: CAS_SF_Relationships
Q45 These questions are about your experiences in adult intimate relationships. By “adult intimate relationship”, we mean a current or former husband/wife, partner, or boy/girlfriend for longer than one month.
Have you ever been in an adult intimate relationship (i.e. since the age of 16)?
- Yes (1)
- No (0)
Skip To: End of Block If These questions are about your experiences in adult intimate relationships. By ‘adult intimate re… = No
Q46 Have you been in an adult intimate relationship in the past 12 months?
- Yes (1)
- No (0)
Skip To: Q82 If Have you been in an adult intimate relationship in the past 12 months? = No
Q47 Are you currently in a relationship?
- Yes (1)
- No (0)
Display This Question:
If Are you currently in a relationship? = Yes
Q48 Do you believe, at times, your current partner becomes afraid of you?
- Yes (1)
- No (0)
Q49 Do you believe a partner has been afraid of you in the last 12 months?
- Yes (1)
- No (0)
Q50 Do you believe a partner has ever been afraid of you?
- Yes (1)
- No (0)
Q51 We would like to know if you have ever used any of the behaviours listed below towards any current or former partner or partners.
Q52 Have you ever blamed a partner for causing you to act abusively?
- Yes (1)
- No (0)
Display This Question:
If Have you ever blamed a partner for causing you to act abusively? = Yes
Q53 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q54 Have you ever shaken, thrown, pushed, or grabbed a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever shaken, thrown, pushed, or grabbed a partner? = Yes
Q55 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q56 Have you ever tried to convince a partner’s family or friends that they were crazy?
- Yes (1)
- No (0)
Display This Question:
If Have you ever tried to convince a partner’s family or friends that they were crazy? = Yes
Q57 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q58 Have you ever used or threatened to use a knife or gun or other weapon against a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever used or threatened to use a knife or gun or other weapon against a partner? = Yes
Q59 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q60 Have you ever made a partner perform sex acts that were unwanted?
- Yes (1)
- No (0)
Display This Question:
If Have you ever made a partner perform sex acts that were unwanted? = Yes
Q61 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q62 Have you ever followed a partner or hung around outside their home or work?
- Yes (1)
- No (0)
Display This Question:
If Have you ever followed a partner or hung around outside their home or work? = Yes
Q63 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q64 Have you ever threatened to harm or kill a partner or someone close to them?
- Yes (1)
- No (0)
Display This Question:
If Have you ever threatened to harm or kill a partner or someone close to them? = Yes
Q65 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q66 Have you ever choked a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever choked a partner? = Yes
Q67 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q68 Have you ever forced or tried to force a partner to have sex?
- Yes (1)
- No (0)
Display This Question:
If Have you ever forced or tried to force a partner to have sex? = Yes
Q69 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q70 Have you ever continuously called, texted, emailed, or contacted a partner using social media?
- Yes (1)
- No (0)
Display This Question:
If Have you ever continuously called, texted, emailed, or contacted a partner using social media? = Yes
Q71 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q72 Have you ever told a partner they were crazy, stupid or not good enough?
- Yes (1)
- No (0)
Display This Question:
If Have you ever told a partner they were crazy, stupid, or not good enough? = Yes
Q73 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q74 Have you ever hit a partner with a fist or object, kicked or bitten a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever hit a partner with a fist or object, kicked, or bit a partner? = Yes
Q75 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q76 Have you ever kept a partner from seeing family or friends?
- Yes (1)
- No (0)
Display This Question:
If Have you ever kept a partner from seeing family or friends? = Yes
Q77 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q78 Have you ever locked a partner in a room or other space?
- Yes (1)
- No (0)
Display This Question:
If Have you ever locked a partner in a room or other space? = Yes
Q79 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q80 Have you ever kept a partner from having access to a job, money or financial resources?
- Yes (1)
- No (0)
Display This Question:
If Have you ever kept a partner from having access to a job, money or financial resources? = Yes
Q81 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q82 Do you believe a partner or ex-partner is currently afraid of you?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q83 Do you believe a partner has ever been afraid of you?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q84 We would like to know if you have ever used any of the listed behaviours below towards any current or former partner or partners. Have you ever…
Yes (1)
No (0)
Blamed a partner for causing you to act abusively (1)
Shook, threw, pushed, or grabbed a partner (4)
Tried to convince a partner’s family or friends that they were crazy (5)
Used or threatened to use a knife or gun or other weapon against a partner (6)
Made a partner perform sex acts that were unwanted (7)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q85 We would like to know if you have ever used any of the listed behaviours below towards any current or former partner or partners. Have you ever…
Yes (1)
No (0)
Followed a partner or hung around outside their home or work (9)
Threatened to harm or kill a partner or someone close to them (18)
Choked a partner (10)
Forced or tried to force a partner to have sex (11)
Constantly called, texted, emailed, or contacted a partner using social media (12)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q86 We would like to know if you have ever used any of the listed behaviours below towards any current or former partner or partners. Have you ever…
Yes (1)
No (0)
Told a partner they were crazy, stupid or not good enough (13)
Hit a partner with a fist or object, kicked or bitten a partner (14)
Kept a partner from seeing family or friends (15)
Locked a partner in a room or other space (16)
Kept a partner from working or having access to resources (17)
Q87
Thank you for all your answers so far. You are at the half-way point of the survey. Please remember that your answers will contribute to helping us make services better for everyone in the community. If at any time you would like to take a break you may do so and return to the place you are up to (as long as you use the same device). If you would like to speak to anyone about anything distressing that has arisen for you so far please click here.
End of Block: CAS_SF_Relationships
Start of Block: UNMC_Relationships
Q88 Your relationships continued
This section is about unwanted sexual experiences. These experiences may have occurred inside or outside of an intimate relationship. In this particular survey, we are interested in hearing from people who have instigated unwanted sex. Remember that the survey is anonymous. If you do not feel comfortable answering any of the questions, skip them and go on to the next question. In this questionnaire, when we talk about “sex” we mean any kind of sex (vaginal, anal, oral etc.)
Q89 Since the age of 15, have you ever forced or tried to force someone into sexual activity?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q90 Have you ever physically forced a partner to have sex? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q91 Have you ever threatened or made a current or former partner afraid in some other way in order to get them to have sex with you? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q92 Have you ever forced a current or former partner to watch pornography with you? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q93 Have you forced a current or former partner to do something else sexual with you? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q94 Have you ever pressured, forced or threatened a partner to become pregnant?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By ‘adult intimate re… = Yes
Q95 Have you ever pressured, forced, or threatened a partner to prevent them from terminating a pregnancy?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q96
Have you ever interfered with contraception in order to get a partner pregnant (e.g. disposed of contraception, tampered with contraception, prevented a partner from obtaining contraception)?
- Yes (1)
- No (0)
Q97
This is the end of this section. Thank you for taking the time to answer these questions, some of which may have been distressing. This is the end of the sensitive questions about experiences you have had in your relationships. Below is a breathing exercise that may reconnect you with where you are in this moment, here and now. If you would like to speak to someone for support, click here for a list of support services.
When you feel ready, press the next button to continue taking the survey. We really appreciate your time.
Q98
End of Block: UNMC_Relationships
Start of Block: Contemplation_Ladder
Q99 Changing your behaviour and relationships
Now we would like to ask you about how you feel about making changes to your behaviour and relationships. Below are a number of statements about behaviour and relationship change. We are interested to know how you see change in your own life. Right now, you may not see a need for change, you may be thinking about change, or you may have already taken steps to make changes to your behaviour or relationship.
Q100 Please select the one statement about changing your behaviour that best reflects how you feel today.
- I don’t need to change my behaviour, but my partner does. (1)
- I haven’t thought about changing the way I act or my behaviour towards my partner. (2)
- I think both my partner and I need to change the way we act and behave. (3)
- I need to change my behaviour, but am unsure if I can. (4)
- I need to change my behaviour, but I am not ready. (5)
- I am starting to make changes to my behaviour to improve my relationships. (6)
- I have made changes to my behaviour, but I am worried about things slipping back. (7)
Q101 Please select the one statement about changing your relationship that best reflects how you feel today.
- I don’t think about making my relationship healthier. (1)
- Sometimes I think that my relationship could be healthier. (2)
- I would love to make my relationship healthier, but don’t know if I am ready. (3)
- I would love to make my relationship healthier, but I am not sure how. (4)
- I have made changes in my relationship to make it healthier, but I worry it won’t last. (5)
- I have made changes in my relationship to make it healthier, and I am confident it will stay this way. (6)
End of Block: Contemplation_Ladder
Start of Block: Help-seeking
Q102 Your views on services This section asks you about your use of services in the community. This information will help us understand how people use services, what might be missing from services, and ways that existing services can be improved. In particular, we are interested to know whether you have ever sought advice or support for any of the relationship issues explored in the previous sections.
Q103 Have you ever spoken to any of the following services about your behaviour/s in your relationship/s? Please tick all that apply.
- I did not seek advice or support. (531)
- Friend/s (508)
- Family member/s (509)
- Partner (510)
- General practitioner (511)
- Nurse (512)
- Psychologist or counsellor (513)
- Social worker (hospital/community health) (514)
- Alcohol or drug worker (515)
- Family therapist (516)
- Telephone helpline (e.g. Lifeline, 1800 RESPECT) (517)
- Domestic or family violence service (519)
- Police (520)
- Legal service (e.g. solicitor or legal aid) (521)
- Men’s behaviour change program (522)
- Men’s referral service (523)
- Mensline (532)
- Financial service (e.g. Centrelink) (524)
- Housing service (525)
- Work colleague or boss (526)
- Priest/minister/rabbi or any other religious person (527)
- Other (please specify) (518) ________________________________________________
End of Block: Help-seeking
Start of Block: How helpful
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Friend/s
Q104 How helpful was your friend/s?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Family member/s
Q105 How helpful was your family member?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = General practitioner
Q106 How helpful was the general practitioner?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Nurse
Q107 How helpful was the nurse?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Psychologist or Counsellor
Q108 How helpful was the psychologist or counsellor?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Social worker (Hospital/community health)
Q109 How helpful was the social worker (hospital or community based)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Alcohol or drug worker
Q110 How helpful was the alcohol or drug worker?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Family therapist
Q111 How helpful was the family therapist?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Other (please specify)
Q112 How helpful was the telephone helpline (e.g. Lifeline, 1800RESPECT)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Domestic or family violence service
Q113 How helpful was the domestic or family violence service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Police
Q114 How helpful was the police?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Legal service (e.g. solicitor or legal aid)
Q115 How helpful was the legal service (e.g. solicitor or legal aid)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Financial service (e.g. Centrelink)
Q116 How helpful was the financial service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Housing service
Q117 How helpful was the housing service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Work colleague or boss
Q118 How helpful was your work colleague or boss?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Priest/Minister/Rabbi or any other religious person
Q119 How helpful was the priest/minister/rabbi or any other religious person?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to Rany of the following services about your behaviour/s in your relationship… = Partner
Q120 How helpful was your partner?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever sRpoken to any of the following services about your behaviour/s in your relationship… = Men’s behaviour change program
Q121 Was the men’s behaviour change program court-ordered or voluntary?
- Court-ordered (1)
- Voluntary (2)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Men’s behaviour change program
Q122 How helpful was men’s behaviour change program?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = men’s referral service
Q123 How helpful was men’s referral service?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
End of Block: How helpful
Start of Block: Help_seeking_did_not_seek_advice
Q124 Below is a list of reasons why you may have not spoken to a professional or service about your behaviours. Please rate how important each is to your own situation. Please select one option per line.
Not at all important (1)
A little bit important (2)
Somewhat important (3)
Moderately important (4)
Very important (5)
I don’t feel deserving of help. (13)
I feel too ashamed to talk to anyone. (14)
The professional will not understand me. (15)
The professional will tell others. (16)
My friends or family will find out. (17)
My behaviours are just a normal part of relationships. I don’t believe there is any need to see a professional about them. (18)
My behaviour was a once-off. It won’t happen again. (19)
I have no access to transport to see someone. (20)
I have no time to talk to someone about these things. (21)
All the services that are available are too expensive. (22)
I don’t know of any service that might be able to help. (23)
I don’t want to talk to anyone about my behaviours, it is too personal. (24)
Q125 Was there a time when you needed help for your behaviour in relationships but could not get it?
- Yes (1)
- No (0)
Display This Question:
If Was there a time when you needed help for your behaviour in relationships but could not get it? = Yes
Q126 How important were each of the service barriers in preventing you from accessing services? Please select one option per line.
Not at all (1)
Slightly (2)
Moderately (3)
Very (4)
Extremely (5)
Language or translation problems (36)
Cost (37)
Limited opening hours (38)
No service available in the area at the time needed (39)
Waiting time too long (40)
No appointments (41)
Not taking new patients (42)
Lack of awareness of available services (43)
Concerns regarding confidentiality (44)
No private health insurance (45)
Other barriers: ___________ (46)
End of Block: Help_seeking_did_not_seek_advice
Start of Block: Help_seeking_How_important
Q127 Reflecting on any contact or experiences you’ve had with services, what would you say you value most in a service? Please rate how important you think each of the following factors are.
Not at all important (1)
A little important (2)
Moderately important (3)
Very important (4)
Extremely important (5)
Not feeling judged or put down (11)
Knowing that whatever I said would be held in confidence by the professional (12)
The professional being interested in who I was as a person (13)
Feeling listened to by the professional (14)
Being given practical information about how to increase safety (15)
The expertise of the professional (16)
Learning new ways of dealing with relationship problems (17)
Material support (e.g. getting access to accommodation) (18)
Emotional support (having someone to talk to) (19)
Other (please specify) (20)
Q128 Considering all the experiences you have had in talking to professionals (including GPs, counsellors, nurses etc) about these behaviours, what do you believe that professionals need to do differently to better help people in similar situations as you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q129 The COVID-19 pandemic has changed the way we all access support services. What impact, if any, has it had on your access to support services for your behaviours in intimate relationships?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: Help_seeking_How_important
Start of Block: Help_seeking_continued
Q130 If you thought you were close to using abusive behaviour/s in your relationship/s, how likely is it that you would seek help from the following people or services?
Very unlikely (1)
Unlikely (2)
Neither likely nor unlikely (3)
Likely (4)
Very likely (5)
Friend/s (35)
Family member/s (36)
Partner (37)
General practitioner (38)
Nurse (39)
Psychologist or counsellor (40)
Social worker (hospital/community health) (41)
Alcohol or drug worker (42)
Family therapist (43)
Telephone helpline(e.g. Lifeline, 1800 RESPECT) (44)
Domestic or family violence service (45)
Police (46)
Legal service (e.g. solicitor or legal aid) (47)
Men’s behaviour change program (48)
Men’s referral service (49)
Financial service (e.g. Centrelink) (50)
Housing service (51)
Work colleague or boss (52)
Priest/minister/rabbi or any other religious person (53)
Other (please specify) (54)
Q131 If you think about your behaviours towards your partner/ex-partner you told us about in previous sections, what do you think your greatest need is from a service or professional?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q132 If you think about your behaviours towards your partner/ex-partner, what do you think you need the most to stop using violence and abuse?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have any children? = Yes
Q133 If you think about your behaviours towards your partner/ex-partner and children, how do you think your children have been affected?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have any children? = Yes
Q134 If you think about your behaviours towards your partner/ex-partner, what do you think services can do to best address your children’s needs?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q135 If you think about your behaviours towards your partner/ex-partner, what do you think your partner’s/ex-partner’s greatest need is from a service or professional?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q136 How have your experiences in your adult intimate relationships changed during COVID-19 isolation?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q137 I wish…
These next questions ask you to think about your relationship with your partner or ex-partner. Please complete the following sentences with the first words that come to mind. There are no right or wrong answers, just write what you feel.
I wish that my partner/ex-partner…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q138 I wish that service providers…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q139 I wish that my family…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q140 I wish that my friends…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q141
This is the end of this section. When you feel ready, please click the next button to continue with some further background questions.
End of Block: Help_seeking_continued
Start of Block: More_about_you
Q142 More about you This section asks more about your background and some personal details about education and finances. These questions are important because they allow your answers to be placed in a broader context, without identifying anybody. Please remember that all survey responses are anonymous.
Q143 Which of these most closely describes your sexual orientation?
- I am heterosexual (0)
- I am bisexual (1)
- I am lesbian (2)
- I prefer to self-describe (3) ________________________________________________
- I am asexual (4)
- Not sure (6)
- I am queer (7)
Q144 Which of the following best describes your prior schooling?
- Still at secondary school (1)
- Completed secondary school to end of Year 12 (2)
- Attended secondary school but did not complete Year 12 (3)
- Attended primary school only (4)
- Did not attend school (5)
Q145 What is your highest qualification since leaving school?
- Finished a degree or higher degree (1)
- Completed a diploma or certificate (2)
- Completed a trade apprenticeship or traineeship (3)
- Other (please specify (4) ________________________________________________
Q146 Which of the following best describes your occupational status?
- Part-time wage or salary earner (including self-employed) (1)
- Full-time wage or salary earner (including self-employed) (2)
- Unemployed, seeking work (3)
- Unemployed, not seeking work (4)
- Retired (5)
- Unpaid work (e.g. home duties, voluntary, carer) (6)
Q147 Do you hold a current Health Care Card?
- Yes (1)
- No (0)
Q148 How do you manage on your available income?
- Easily (1)
- Not too badly (2)
- Difficult some of the time (3)
- Difficult all of the time (4)
- Impossible (5)
Q149 You are close to the end. Only a few more questions and you will be finished. When you feel ready, please click the next button to continue.
End of Block: More_about_you
Start of Block: How_you_felt_completing_this_survey
Q150 Your views on the survey
This last section asks questions how you felt while completing this survey to understand what it was like being involved in the VOICES project. Please select one box on each line.
Q151 I felt comfortable answering questions about domestic violence and sexual violence in this survey.
- Strongly agree (1)
- Agree (2)
- Neither agree nor disagree (3)
- Disagree (4)
- Strongly disagree (5)
Q152 As a result of questions about domestic violence and sexual violence being asked in this survey, my feelings about my relationship are…
- More positive (1)
- Somewhat more positive (2)
- Unchanged (3)
- Somewhat more negative (4)
- More negative (5)
Q153 The questions I was asked in this survey made me feel that the problems in my relationship with my partner or ex-partner are my fault.
- Strongly disagree (1)
- Disagree (2)
- Neither disagree nor agree (3)
- Agree (4)
- Strongly agree (5)
Q154 As a result of being asked questions about domestic violence and sexual violence in this survey, my feelings about myself as a person are…
- Better (1)
- Somewhat better (2)
- About the same as before (3)
- Somewhat worse (4)
- Worse (5)
Q155 Responding to this survey has made me more open to dealing with possible problems in my relationship.
- Strongly disagree (1)
- Disagree (2)
- Neither agree nor disagree (3)
- Agree (4)
- Strongly agree (5)
Q156 I am glad to be a participant in the VOICES project.
- Strongly disagree (1)
- Disagree (2)
- Neither disagree nor agree (3)
- Agree (4)
- Strongly agree (5)
Q157 Please use the space below if there is anything else you would like to tell us about yourself or the survey
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q158 Final thoughts: In your own words, what have you gained from participating in the VOICES project?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q159 Do you have any extra comments that you wish to make about any issues raised in the survey?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: How_you_felt_completing_this_survey
Start of Block: Thank You
Q160
Make sure you click submit!
This is the end of the survey. Thank you very much for the time and effort you have taken. When you click the submit button, your responses will be submitted confidentially.
On the next page you can provide your contact details if you like to enter into a draw to win an iPad, as an appreciation of your time and effort. You can also tell us if you would like to participate in a follow up interview about your experiences and need for services.
Thank you.
End of Block: Thank You
Start of Block: Gift Voucher
Q263 Thank you for completing this survey and taking the time to assist us today. Your participation will contribute to our understanding of how best to help and keep families safe. We would like to offer you the option to enter a draw to win an iPad in appreciation for your time and contribution. If you would like to enter the draw, please provide us with your name and best email address. Your name and email address will not be used for any other purposes.
Q265 Email address
________________________________________________________________
Q264 Name
________________________________________________________________
Q266 Together, with your help, we are trying to work out ways to improve the support and services women receive in relation to issues of domestic violence and sexual assault.
To achieve this goal, further research (e.g. interviews) on this topic may be required. Please tick yes if you would be happy to be contacted by the researchers for involvement in further research.
Your participation in further research is completely voluntary, and independent of the survey you have just completed. You can provide your details now but if you change your mind later, you are free to withdraw your interest without explanation when/if you are contacted for further research at some time in the future.
Q267 Would you like to participate in further research on this topic?
- Yes (1)
- No (2)
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q268 My first name is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q269 The best phone number(s) to safely contact me on is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q270 An alternative contact (e.g. email) is:
________________________________________________________________
End of Block: Gift Voucher
Appendix D:
Interview schedule
(Victims and survivors)
Questions
1. Can you tell me about when you first realised what you were experiencing in your relationship /(what you experienced from a sexual partner) was not OK?
2. Can you take me through your experiences of seeking help or support since having issues in your relationship/an unwanted sexual encounter?
Interviewer will use probes to explore:
- • What help or support participant was hoping for
- • What prompted them to talk to others or seek support
- • What seeking help was like for them
- • If there any help or support that they wanted or needed but did not receive.
3. How could a professional or service make it easier to seek help or support?
Appendix E:
Interview schedule
(People who use IPV and/or SV)
Questions:
Can you tell me when you first realised there was an issue with your behaviour in your intimate relationship(s)?
Interviewer probes
What were some “lightbulb” moments?
Who was involved in supporting you to realise something was wrong?
What happened when you realised something was wrong?
Can you take me through your experiences of speaking to people about your behaviour in your intimate relationships?
Interviewer probes
What help or support were you hoping for?
What kinds of professionals did you speak to?
Was there any help or support that you wanted or needed but didn’t receive?
Professor Kelsey Hegarty
University of Melbourne
Dr Mandy McKenzie
University of Melbourne
Dr Elizabeth McLindon
University of Melbourne
Matt Addison
University of Melbourne
Dr Jodie Valpied
University of Melbourne
Dr Mohajer Hameed
University of Melbourne
Dr Minerva Kyei-Onanjiri
University of Melbourne
Dr Surriya Baloch
University of Melbourne
Associate Professor Kristin Diemer
University of Melbourne
Associate Professor Laura Tarzia
University of Melbourne
RESEARCH REPORT
ISSUE 22 | DECEMBER 2022
ANROWS acknowledgement
This material was produced with funding from the Australian Government Department of Social Services. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from the government, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government Department of Social Services. Thank you to our advisory committee: Hayley Boxall (Australian Institute of Criminology), Sally Mills (Australian Institute Health and Welfare), Angela Hampton (Central Australian Aboriginal Congress), Jacqui Watt (No to Violence), Safiyah Salim (WA Health), Emily Grant (WEAVERs group, University of Melbourne), Amanda Wallace (WEAVERs group, University of Melbourne), Heather Clarke (National Association of Services against Sexual Violence), Louise Gottardo (Queensland Departmentof Justice), Dr Astrid Perry (Settlement Services International), Dominiek Coates (ANROWS), and representatives from the Commonwealth Attorney-General’s Department, ACON’s Sexual, Domestic and Family Violence team, the WA Department of Communities, and the Office for Prevention of Family and Domestic Violence.
Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we live and work. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and emerging. We value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with First Nations peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2022
![]()
With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
ISBN: 978-1-922645-59-3 (paperback)
ISBN: 978-1-922645-60-9 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project 4AP.8 “Transforming responses to intimate partner and sexual violence: Listening to the voices of victims, perpetrators and services”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Plan Outcome 4 – Services meet the needs of women and their children experiencing violence and National Plan Outcome 6 – Perpetrators stop their violence and are held to account.
Suggested citation:
Hegarty, K., McKenzie, M., McLindon, E., Addison, M., Valpied, J., Hameed, M., Kyei-Onanjiri, M., Baloch, S., Diemer, K., & Tarzia, L. (2022). “I just felt like I was running around in a circle”: Listening to the voices of victims and perpetrators to transform responses to intimate partner violence (Research report, 22/2022). ANROWS.
The University of Melbourne
Parkville VIC 3010
Author acknowledgement
We gratefully acknowledge contributions made by all the participants who so generously participated in various phases of this project by sharing their experiences with us. We appreciate contributions made by Jacqueline Kuruppu and Kitty Novy who assisted with survey design. We thank members of the advisory committee established to support this project. They oversaw the general conduct of the research and assisted with recruitment and interpreting and disseminating the findings.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of people affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
ANROWS acknowledges that children and young people living in homes where domestic and family violence (DFV) is present are not simply “exposed” to DFV – they are experiencing it. There are no circumstances in which children and young people are exposed to DFV and are not also being impacted by this violence. Therefore, ANROWS will always default to using “experienced DFV” instead of “were exposed to DFV” or “witnessed DFV”. This language recognises that children experience DFV as victims in their own right, and also seeks to honour the voices of victims and survivors who have felt minimised, erased or unacknowledged as childhood survivors.
Please note that in this report, the authors have occasionally used the language of exposure and witnessing.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76).
Acronyms and abbreviations
| Acronym / abbreviation | Definition |
|---|---|
| ACEs | Adverse childhood experiences |
| CALD | Culturally and linguistically diverse |
| CASr-SF | Composite Abuse Scale (Revised) Short Form |
| DV or IPV | Domestic violence or intimate partner violence |
| IPV and/or SV | Intimate partner violence and/or sexual violence |
| LGBTQ | Lesbian, gay, bisexual, trans and gender diverse, queer and questioning |
| PTSD | Post-traumatic stress disorder |
| SV | Sexual violence |
Definitions and concepts
| Concept | Definition |
|---|---|
| Child abuse | Child abuse refers to a range of physically, sexually and psychologically abusive and neglectful behaviours, including experiencing parental violence growing up. This study included questions about child abuse from the Adverse Childhood Experiences Scale and refers to abusive and harmful behaviour occurring before the age of 15 years, perpetrated by somebody over the age of 18 years, from within or outside the family (Felitti et al., 1998). |
| Family violence | Family violence refers to physically, sexually, emotionally or economically abusive behaviours by an intimate or non-intimate family member that may make a family member feel afraid for their safety or wellbeing (Australasian Legal Information Institute, 2008; Ellsberg & Heise, 2002). Family violence includes behaviour that children experience living in homes where domestic violence is occurring. “Family violence” is the term preferred by Australian Aboriginal and Torres Strait Islander peoples as better reflecting the experiences of extended families and communities (Olsen & Lovett, 2016). While family violence refers to abusive behaviour that can occur in families of diverse configurations, it is often used to describe behaviour by an intimate partner against his current or former partner and her children (Victorian Government, 2016). |
| Financial abuse | Financial abuse is a form of family violence that may include withholding money, controlling household finances or refusing to include a victim and survivor in financial decisions. |
| Intimate partner violence (IPV) | The World Health Organization (WHO) defines “intimate partner violence” (IPV) as “behaviour by an intimate partner that causes physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviours” (World Health Organization, 2013b, p. vii). This definition is inclusive of violence by current and former spouses and other intimate partners. The National Plan to Reduce Violence Against Women and their Children 2010–2022 (the National Plan) highlights that IPV is frequently characterised by “an ongoing pattern of behaviour … a range of tactics to exercise power and control over women and their children” (Council of Australian Governments, 2012, p. 2). IPV is used in this report instead of “domestic violence”, because, although they are commonly used interchangeably, the definition of domestic violence is broader to include other people who live in a domesticarrangement. |
| Intimate partner violence and/or sexual violence (IPV and/or SV) | In recognition of the common but often hidden experience of sexual violence (SV) within IPV as well as the prevalence of SV outside of intimate relationships, in this report we use the term “IPV and/or SV”. IPV and/or SV refers to instances where people have experienced IPV that may or may not have included SV by a partner or somebody else. |
| People who use violence and abuse | The terms “people who use violence and abuse” or “people who use IPV and/or SV” are employed within this report to refer to people of all genders who have perpetrated physical, sexual and/or psychological violence against an intimate partner. We employ inclusive language to refer to people who have used violence, but we nonetheless acknowledge that the prevalence and impacts of IPV and/or SV are not sex-asymmetrical (Indermaur, 2001; Kertesz et al., 2019). While many factors contribute to IPV and/or SV, research has long shown that chief among them is the power disparity between men and women as a result of women’s relative lack of access to resources and rigid gender roles linking masculinity with dominance (Flood & Pease, 2009; Our Watch & VicHealth, 2021). Interchangeable terms with “people who use violence and abuse” in this report include “perpetrator” and “people who use violence”. |
| Poly-victimisation | Poly-victimisation refers to the experience of more than one type of abuse across a person’s life course (Finkelhor et al., 2005). For example, a person who experienced abuse in childhood by a family member and was later victimised by an intimate partner in adulthood is a victim and survivor of poly-victimisation. |
| Psychological abuse | Psychological abuse refers to emotional, verbal, isolating, coercive and/or controlling behaviours by an intimate partner (Dokkedahl et al., 2022). Usually, psychological abuse encompasses a combination of behaviours that occur over time, and research suggests this type of violence is the most common form of IPV (Dokkedahl et al., 2022). Perpetrated either in person or via technology, psychological abuse may occur in combination with physical and sexual abuse or it may stand alone. |
| Reproductive coercion | Reproductive coercion is behaviour that interferes with the independent decision-making of a woman in relation to her reproductive health (Grace & Anderson, 2016). In this report, the term “reproductive coercion” is used to refer to the use of force or coercion to compel a woman to become or remain pregnant when she does not want to be (including by tampering with birth control), or to end a pregnancy against her wishes. |
| Sexual violence (SV) | The term “sexual violence” describes acts of a sexual nature carried out without consent and with force, fear, intimidation or coercion, including rape, attempted rape and other forced sexual activity by an intimate partner, acquaintance or stranger (World Health Organization 2012). For this report, SV does not include unwanted sexual touching or sexual harassment (Cox, 2015). |
| Technology-facilitated abuse | Technology-facilitated abuse indicates abusive behaviour that is perpetrated via a technological device (e.g. mobile phone, computer) by an intimate partner or someone in a dating relationship (Brown & Hegarty, 2021). Examples of technology-facilitated abuse include monitoring a person’s whereabouts using tracking software or distributing or threatening to distribute nude images or video without permission. |
| Victim and survivor | The term “victim and survivor” is used with reference to people with lived experience of IPV and/or SV (Elliott et al., 2005). This term was chosen for use throughout the report because it recognises both the harm caused by IPV and/or SV and the strength and resilience of people who have experienced these traumas and continue to survive. “Victim and survivor” is also the language used in the Fourth Action Plan 2019–2022 (Department of Social Services, 2019) of the National Plan. In this research, we are exploring the experiences of women victims and survivors, since they are the main people who experience IPV and/or SV. We acknowledge that children and young people can be victims and survivors in their own right. We also acknowledge that non-binary people and men are victims and survivors, but they were not the focus of this research. |
Executive summary
“I just constantly felt like I was running around in a circle.”
(Victim and survivor participant)
“I need to have someone hear me and talk to me, not at me.”
(Male participant who had used IPV and/or SV)
Background
Intimate partner violence (IPV) and sexual violence (SV) are common issues in the community that have negative impacts on the health and wellbeing of women and children victims and survivors. Understanding patterns of abuse and violence and the help-seeking behaviours and needs of both those who experience IPV and/or SV and those people who use IPV and/or SV are needed to inform policy and practice. There has been limited in-depth data collected in Australia that can inform the policy and practice reform needed to support victims and survivors on their pathway to safety and healing, or to engage people who use IPV and/or SV to seek help for their abusive behaviours.
Aim and objectives
The “Voices” project explored:
- experiences of IPV and/or SV, including patterns of abuse and violence and service needs from the perspectives of women victims and survivors
- experiences and service needs of people who use IPV and/or SV against women.
We were interested in “what works” from the perspectives of women victims and survivors and from perpetrators in terms of service responses for themselves and their children.
Method
To gain a deep understanding, we used a mixed methods study, which included data from online surveys of 1,122 women victims and survivors and 563 people who had used IPV and/or SV against women. Interviews were also conducted with 30 women victims and survivors and eight people who had used IPV and/or SV (all male), drawn from the survey participants. Survey participants were recruited through social media and a commercial panel of people who registered for research studies. Participants were eligible if they answered yes to one of the questions in the boxes below.
Box 1: Victim and survivor survey screening items
In the last five years have you:
- Been afraid of a partner of ex-partner?
- Been controlled by a partner or ex-partner?
- Been physically hurt by a partner or ex-partner?
- Experienced unwanted sex by anyone, including a partner or ex-partner?
Box 2: People who use violence survey screening items
In the last five years have you:
- Been concerned about your behaviours in intimate relationships?
- Believed your behaviour has scared a partner or ex-partner?
- Sought help from anyone to address issues in your intimate relationships?
IPV and/or SV was measured using the Composite Abuse Scale (Revised)-Short Form (CASr-SF), which asks about 15 abusive behaviours. However, it’s important to note that participants who did not score on this measure may have experienced IPV and/or SV or used IPV and/or SV. Quantitative data was analysed using STATA and descriptive statistics. Interviews were transcribed and analysed using a thematic approach. Thematic analysis was also utilised to interpret qualitative data from open-ended questions in the survey.
Findings
Victims’ and survivors’ demographics, experiences and health impact
- Female participants were generally nationally representative of the Australian population of women, except more of them were from Victoria (33.4%), or were from Aboriginal and Torres Strait Islander background (7.8%) or reported difficulty managing on their available income (58.5%). There was less representation from women who were employed (59.3%) or were born overseas (18.1%) or for whom English was a second language (7.4%), which is not surprising given the survey was only available in English.
- Patterns of IPV and/or SV showed participants experienced multiple types of IPV rather than one type alone during their lifetime (see Figure 1). Of those women who experienced IPV (905), 60.5 per cent experienced technology-facilitated abuse, 32.9 per cent reproductive coercion and 40.7 per cent financial abuse.
Figure 1: Overlap of types of IPV
Data table for the figure above:
| Type of IPV | Percentage | n |
|---|---|---|
| Physical violence | 0.7% | 7 |
| Sexual violence | 2.3% | 23 |
| Psychological violence | 12.4% | 124 |
| Physical and sexual violence | 0.3% | 3 |
| Physical and psychological violence | 22.3% | 223 |
| Sexual and psychological violence | 10.5% | 105 |
| Physical, sexual and psychological violence | 51.5% | 516 |
- The vast majority of participants were afraid of their partner or ex-partner (76.1% currently afraid; 80.7% afraid in the last 12 months; and 84.3% ever afraid).
- Poly-victimisation occurred across victims’ and survivors’ lifetimes, with 69.4 per cent experiencing child abuse.
- The burden of disease (see Figure 2) was high, with 71.2 per cent of victims and survivors experiencing probable post-traumatic stress disorder (PTSD), half experiencing other mental health issues (52.4% anxiety symptoms, 45.4% depression symptoms) and over one third affected by disability (39.2%) or rating their health as poor or fair (35.5%).
- These above patterns and health issues were more common in those from Aboriginal and Torres Strait Islander backgrounds and those who were unemployed or who had difficulty managing on their available income.
Figure 2: Percentage of participants with different health issues
Data table for the figure above:
| Health issue | Survivors | Perpetrators |
|---|---|---|
| Poor/Fair health | 35 | 21 |
| Anxiety | 52 | 30 |
| Depression | 45 | 29 |
| PTSD | 71 | 51 |
| Alcohol and other drugs (OD) | 22 | 26 |
| Disability | 36 | 26 |
Demographics, experiences and health issues of people who use violence
- Participants (93.1% men, 5.7% women, 0.9% non-binary and 0.4% prefer not to say) were generally nationally representative of the Australian population, except more of them were aged between 18 and 39 years, were from Victoria (50.7%) or from an Aboriginal or Torres Strait Islander background (10.1%), or reported difficulty managing on their available income (39%). There was less representation from people who were employed (67.8%) or were married (38.1%).
- Over half (58.2%) of the participants reported having ever used IPV and/or SV on the CASr-SF measure, while 44 per cent identified they had ever made their partner feel afraid of them.
- Half of the participants experienced child abuse (47.6%) or PTSD (51.2%), one third experienced anxiety (30.4%) and depression (29%), and one in four reported excessive alcohol consumption (26.2%), living with disability (25.8%) or rated their health as fair or poor (21%; see Figure 2).
- These patterns and health issues were more common in those from Aboriginal and Torres Strait Islander backgrounds and those who were unemployed or who had difficulty managing on their available income.
- A higher proportion of participants held attitudes that were supportive of violence against women when compared to the Australian community (using the National Community Attitudes towards Violence against Women Survey; Webster et al., 2018).
Victims’ and survivors’ help-seeking behaviours
- One in five (21.5%) victims and survivors did not seek any source of formal help for their relationship issues.
- Help-seeking was most commonly sought from family and friends (64.4%) or a health professional (e.g. a psychologist/counsellor, general practitioner, nurse, social worker; 51.4%), with two thirds of victim and survivor participants finding these sources helpful (see Figure 6).
- Fewer participants sought help from specialist IPV and/or SV services (40.1%), police (31.1%) or legal services (19.3%).
Figure 3: Proportion of participants who sought help
Data table for the figure above:
| Participant group | Survivors | Perpetrators |
|---|---|---|
| Family/friends | 64 | 59 |
| Health services | 51 | 33 |
| Specialist services | 40 | 11 |
| Police | 31 | 5 |
| Legal | 19 | 2 |
Help-seeking behaviours of people who use IPV and/or SV
- Almost one third (26.5%) of people who use IPV and/ or SV did not seek any source of help for relationship issues. Help-seeking was most commonly sought from family and friends (58.9%, including partners 31.7%) or a health professional (e.g. psychologist/counsellor, general practitioner, nurse, social worker; 33.3%), with two thirds of participants finding these sources helpful (see Figure 3).
- Fewer participants sought help from specialist IPV and/or SV services (10.8%, including telephone helplines 3.4%), police (4.7%) or legal services (2.3%).
Journeys of help-seeking for women victims and survivors
Based on the interview themes and timelines we created from interview data with 30 victim and survivor participants, we identified the following five key stages of help-seeking: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; establishing independence and safety; and addressing impacts and making sense. These stages reflected particular help-seeking needs or goals at different times. Each stage was triggered by critical turning points or changes in how women understood and experienced the abuse. Figure 4 provides a visual illustration of the different stages of participants’ help-seeking journeys and turning points for each stage. Although the stages we identified reflected common needs and turning pointsacross participants’ journeys, it is important to note that not every participant passed through each stage or progressed through stages in the linear order shown in the diagram. For example, many went through a cycle of getting out of the relationship and later returning.
Figure 4: Journeys to help-seeking for victims and survivors of IPV and/or SV
Text version of the figure above:
- Maintaining hope and fixing problems
- Fixing self
- Fixing partners
- Fixing relationship
- Assessing options and seeking solutions
- Understanding
- Weighing up choices
- Trying to change partner
- Seeking protection
- Getting out
- Planning and breaking away
- Re-establishing independence and safety
- Securing a base
- Establishing financial security
- Settling parenting arrangements
- Holding perpetrator to account
- Addressing impacts and making sense
- Understanding why
- Processing impacts
- Supporting children
- Connecting with others
Before step 1 to step 1:
- Being controlled and isolated
Between step 1 and 2:
- Recognising IPV
- Others identifying IPV
Between step 2 and 3
- IPV escalating or affecting children
- Realising partner won’t change
- Others identifying IPV
Between step 3 and 4
- Partner promising to change
- Enduring stalking and threats
Between step 4 and 5
- Behing abused via legal systems and child contact
- Becoming safer
By analysing the themes and timelines regarding how the eight interview participants described their abusive behaviour and their journeys towards change, we identified the following three stages: bottling things up; breaking down and letting things out; and regaining and maintaining control. Figure 5 provides an illustration of these stages and the key turning points in participants’ journeys. The stages reflect the ways in which the eight interview participants framed their journeys of help-seeking to change their behaviour, and it is likely that their journeys were not as linear as the illustration suggests. It should also be noted that all of the interview participants were male, so their journeys may not reflect the help-seeking journeys of people of other genders who use IPV and/or SV against women.
Figure 5: Journeys to help-seeking for people who use violence
Text version of the figure above:
- Bottling things up
- Relying on partner for comfort
- Using alcohol
- “Anger” and aggression toward partner
- Feeling embarrassed to seek help
- Breading down and letting things out
- Mental health intervention and/or medication
- Police or court intervention
- Engaging in counselling and talking to others
- Regaining and maintaining emotional stability
- Looking after own physical and mental health
- Releasing and self-managing emotions via talking/counselling
Before step 1 to step 1:
- Poor mental health due to stress, trauma and conflict
Between steps 1 and 2:
- Abusive behaviour escalating
- Partner calling police or mental health service or ending relationship
Between steps 2 and 3:
- Trusting others and opening up
- Recognising unacceptable behaviour
Within Step 3:
- Keeping behaviour under control
Summary: Voices of victims and survivors of IPV and/or SV
Figure 6 combines the results from the surveys and the interviews with victims and survivors. In the survey, the top three most cited barriers preventing help-seeking were as follows: feeling ashamed (63.2%); lack of awareness about a service that could help (62.1%); and concerns about confidentiality (49.5%). The vast majority of victims and survivors wanted professional competence to provide them with emotional, practical and safety support (see Figure 6).
Figure 6: Help-seeking, barriers, support needs and models for victims and survivors of IPV and/or SV
Text version of the figure above:
Journey stage
- Maintaining hope and fixing problems
- Assessing options and seeking solutions
- Getting out
- Re-establishing independence and safety
- Addressing impacts and making sense
Help-seeking
- Journey stage 1:
-
- No or minimal help-seeking. 21.5% did not seek any advice or support
- Journey stage 2:
-
- Family & Friends (64%; 64% helpful). Psychologist / counsellor (42%; 77% helpful)
- General practitioner (24%; 70% helpful)
- Journey stage 3 and 4:
-
- Specialist DFV/SV services (40%; 59% helpful)
- Police (31%) or legal services (19%; 60% helpful)
- Housing or financial services (15%; 53% helpful)
- Journey stage 5:
-
- Any services that provide counselling
Barriers
- Journey stage 1:
-
- Shame (63%)
- Lack of awareness of confidence services can help (62%)
- Fears that others will find out (49%)
- Too busy (46%)
- Fears professional won’t understand (44%) *of all 1,103 participants
- Journey stage 2 to 5:
-
- Trouble understanding terms used by professional (72%)
- Limited availability: no appointments (55%)* or not taking new patients (54%), limited hours (51%), or long wait times (46%), or no service in area ( 43%)
-
- * of the 533 participants who sought help and couldn’t get it
Support needs
- Emotional support (92%); professional competence (87%); practical and safety support (86%)
-
- “Help when I need it”, “See me as an individual”, ‘Take me seriously”, “Follow up and follow through”, “Make them stop”
- Journey stages 1 to 5:
-
- C.A.R.E – Choice and control, Action and advocacy, Recognise dynamics, Emotional connection
Evidence-based models
- Journey stage 1:
-
- Universal education
- Safe environment
- Ask the right questions
- Journey stages 2 to 5:
-
- L.I.V.E.S – Listen, Inquire about needs, Validate experiences, Enhance safety, Support & follow-up
Summary: Voices of people who use IPV and/or SV
Figure 7 combines the results from the surveys and the interviews with people who use IPV and/or SV. The survey found that the most common barriers that prevented people who used IPV and/or SV from help-seeking were as follows: feeling ashamed (41.4%); a belief that violence is a normal part of a relationship (34.7%); access challenges (34.7%); concerns about confidentiality (29.3%); lack of awareness of services (23.9%); communication issues (22.1%); and not having the time to talk to someone (15.9%). The vast majority of perpetrator participants in the survey wanted professional competence and emotional and practical support for relationship problems. Figure 7 also includes key themes identified by victim and survivor survey participants about their perceptions of what people who use IPV and/or SV need in order to stop their use of violence and abuse. These were for the perpetrator to have “a wake-up call and retraining” to recognise their use ofIPV and/or SV; for them to have “intensive therapy”; and for there to be “restrictions and consequences” for their behaviour.
Figure 7: Help-seeking, barriers and support needs of people who use IPV and/or SV
Text version of the figure above:
Journey stage:
- Bottling things up
- Breaking down and letting things out
- Regaining and maintaining emotional stability
Help-seeking:
- Journey stage 1:
-
- No or minimal help-seeking
- 27% did not seek any advice or support
- Journey stages 2 and 3:
- Family, partner & friends (59%; 75% helpful)
- Psychologist / counsellor (25%; 84% helpful)
- Specialist DFV or men’s services (11%; 73% helpful)
- General practitioner (10%; 70% helpful)
- Police (5%; 46% helpful)
- Religious person (4%; 82% helpful)
- Legal services (2%; 77% helpful)
Barriers:
- Journey stage 1:
-
- Shame (41%) of all 554 participants
- Normalisation of IPV (35%)
- Access challenges (35%)
- Lack of awareness of services (24%)
- Fears that others will find out (29%)
- Journey stages 2 and 3:
- Lack of awareness of services (68%)
- Cost (62%) of 161 participants who sought help but could not get it or no private health insurance (57%)
- Limited availability: Long wait times (59%), no service in area (57%), no appointments (56%), limited hours (52%) or not taking new patients (49%)
- Concerns regarding confidentiality (49%)
- Language or translation problems (25%)
Support needs:
- Journey stags 1 to 3:
-
- Emotional support (92%)
- Professional competence (91%)
- Practical support for relationship problems (92%)
- “Be more approachable”, “Hear me and talk to me, not at me”, “Get to know me”, “Help me regain emotional control”, “Help me see a difference perspective”
Survivors’ perceptions of needs
- Journey stages 1 to 3:
-
- “A wake-up call and retraining”, “Intensive therapy”, “Restriction and consequences”
Implications for policy and practice
The recommendations below are derived from a synthesis of all the findings in the Voices project (see Figure 8). They highlight reform that is needed aimed at policy and practice levels for the community, social networks, early engagement services, system access and ongoing response services. They are particularly focused on areas that need the most reform or are less highlighted in the draft National Plan to End Violence against Women and Children 2022–2032 (the draft National Plan), which is still to be finalised at the time of writing. Individual policy briefs can be provided for any recommendations likely to be moved forward as part of this plan.
We have included in our recommendations some overarching principles for responses across the service system, including the need to:
- recognise the impacts of IPV and/or SV on children, by developing mechanisms for children’s voices to inform reforms and offering accessible therapeutic support for children
- respond to the diversity of the Australian community, by investing in responses tailored for people with diverse backgrounds and experiences of structural inequalities
- promote change, by offering sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
Across the Australian community, we recommend that the following be provided:
- universal education to assist community members to identify healthy and abusive behaviours in relationships
- enhanced public messaging to raise awareness of affordable and confidential supports available, including helplines for victims and survivors and people who use IPV and/or SV
- financial interventions (e.g. microfinancing) to alleviate financial distress for victims and survivors, so they can obtain the support and resources they need for their safety and wellbeing.
To improve the responses of members of the victim’s and survivor’s and the perpetrator’s social networks, we recommend the following approaches be developed and delivered:
- “allies training” for family, friends and community members to support victims and survivors, using the CARE model (Choice and control, Action and advocacy, Recognition and understanding, Emotional connection; Tarzia, Bohren, et al., 2020)
- “First responder healthy relationships first aid” for workplaces and faith-based organisations, using the LIVES model (Listen, Inquire about needs, Validate, Enhance safety, Support; (World Health Organization, 2013b)
- “engaging men” training for family, friends and community members so they can respond effectively to men who use IPV and/or SV.
To encourage victims and survivors and perpetrators to engage early in seeking professional help, we recommend:
- fostering professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- fostering the capacity of general practice, mental health and counselling services to engage people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
To improve the accessibility of the service system, we recommend:
- ongoing flexible service delivery (telehealth or online) across sectors for victims and survivors and people who use IPV and/or SV
- the resourcing of “care navigators” who can provide accessible and affordable long-term individual support and advocacy for victims and survivors
- accessible messaging to be provided about the limits of service confidentiality, to help address the barriers to accessing support.
To improve the ongoing support available for victims and survivors to address the impacts of IPV and/or SV, we recommend the following responses be resourced:
- Aboriginal and Torres Strait Islander–led centres for healing for all members of the family in each state, developed by local communities for local communities
- trauma- and violence-informed recovery and healing services in each state
- peer victim and survivor–led support groups in each state
- trauma- and violence-informed care from general practice and private mental health services to be funded through the Medicare Benefits Scheme.
Figure 8: Recommendations
Overarching principles
Recognise children:
Develop mechanisms for children’s voices to inform reforms and offer accessible therapeutic support for children.
Respond to diversity:
Invest in responses tailors for people with diverse backgrounds experiences of structural inequalities.
Promote change:
Offer sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
Community
Provide
- Universal education on healthy and abusive relationship behaviours
- Enhanced public messaging about available, affordable and confidential supports, including helplines for victims and survivors and people who use IPV and/or SV
- Financial interventions (eg. microfinancing) to alleviate financial distress for victims and survivors.
Social networks
Develop and deliver
- “Allies training” for family, friends and community using the CARE victim and survivor model
- “First responder healthy relationships first aid” for family, friends, workplaces, and faith-based organisations using the LIVES model
- “Engaging men” training for family and friends to engage effectively with men who use IPV and/or SV
Early engagement
Foster
- Professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- Capacity of general practice, mental health and counselling services to engage with people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
System access
Offer
- Ongoing flexible service delivery (telehealth/online) across sectors for victims and survivors and people who use IPV and/or SV
- “Care navigators” for pathways to accessible and affordable long-term support and advocacy for victims and survivors
- Accessible messaging about limits of confidentiality to overcome barriers to accessing support.
Ongoing response
Response
- Aboriginal and Torres Strait Islander-led centres for healing for all members of the family in each state
- Trauma- and violence-informed recovery and healing services in each state
- Peer victim and survivor-led support groups in each state
- Trauma- and violence- informed care through the Medicare Benefits Scheme for general practice and private mental health services
Conclusion
This mixed methods study has provided insights into the voices of victims and survivors and people who use IPV and/or SV across Australia in terms of what might assist them in their journeys to help-seeking and what support they value. The key role of family and friends and health services in early engagement is highlighted. Recommendations across the service system are suggested for policy and practice that are likely to advance the prevention and response to IPV and/or SV. We no longer want victims and survivors having to go around in circles to find support, as shown by this quote from an interview participant:
You get referred here, there, and everywhere. In the beginning you’re on so many phone calls, you can’t remember who you were talking to, where they’re from. You go through the same story hundreds of times, and you just get completely lost. You can’t remember any of it. Then with the practical assistance you get is very little to none. This person will go, “Oh no we can’t help you with that, but here, try this person”, and they’ll go, “Oh no we can’t do that, try this person”, and then you get referred back to where you started at. It’s really frustrating.
We also need to hear the voices of people who use IPV and/or SV, in order to know how to engage them in behaviour change, as shown by this quote from a survey participant:
Just feeling safe and heard during conversation. That would be the most important thing I would expect from a service or professional. Sometimes just hearing your thoughts said out loud is enough to realise what personal plan of action you must take to change your behaviour, which would hopefully be bolstered by the professionals’ help.
Part A:
Introduction
Part A provides an overview of the background, literature review and policy context for the project. We then discuss the research gaps this project is filling and describe the aims of the project. The next part, Part B, will provide detail of the methodology for the quantitative and qualitative aspects of the project. Findings are then divided into Part C with three sections on women who have experienced intimate partner violence (IPV) and/or sexual violence (SV), Part D with three sections on people who use IPV and/or SV and Part E on children’s experiences and support needs. Part F is the discussion, which provides a synthesis of what works from the perspective of victims and survivors and people who use IPV and/or SV. We conclude with implications for policy and practice.
Background
IPV and SV are major health and human rights issues (World Health Organization, 2013a). IPV is defined as any behaviour within an intimate relationship that causes physical, psychological or sexual harm (World Health Organization, 2013a). A feature of IPV is ongoing patterns of abusive behaviours and tactics used to control and take power away from women and their children (Council of Australian Governments, 2012, p. 2). SV is defined as any act (or attempted act) of a sexual nature perpetrated by one person against another without the victim’s consent (World Health Organization, 2013a). SV may occur at the hands of a partner or ex-partner but can also be perpetrated by family members, acquaintances or strangers. Men are more likely than women to use abuse and violence more frequently and severely so that female victims and survivors are more likely to fear for their lives, or to be injured or killed by a partner (World Health Organization, 2013a).
IPV has wide-ranging impacts on individuals, families and communities, including poor mental and physical health (Webster, 2016), injury, hospitalisation and loss of work productivity (PriceWaterhouseCoopers Australia, 2015; World Health Organization, 2013a). For women, IPV is the most common cause of injury (World Health Organization, 2013b) and causes half of female homicides in Australia (Shackelford & Mouzos, 2005). For men, using IPV is associated with increased alcohol and substance use, depression, suicidal thoughts, anxiety and low self-esteem (Oram et al., 2013). For children, IPV-related trauma is cumulative in impact and associated with social, behavioural, emotional and cognitive problems, persisting into adulthood (Felitti & Anda, 2010).
In Australia, one in six women have experienced physical or sexual violence by a current or previous partner since the age of 15. One in four women have experienced emotional abuse (Australian Institute of Health and Welfare, 2018). However, despite the high prevalence of IPV and SV, there is a dearth of research – including within the Australian context – exploring the nature of abuse from the perspectives of victims and perpetrators to enable tailored responses. In particular, more research is needed into the nature or patterns of abuse and violence that are non-physical – for example, sexual violence, financial control, emotional abuse, non-physical coercive control, technology-facilitated abuse and systems-facilitated violence (Ayre et al., 2016; Cortis & Bullen, 2016).
Further, we do not have detailed research on the help-seeking behaviours and service needs of victims and survivors, or those of people who use IPV and/or SV. The 2016 Australian-based Personal Safety Survey data (Australian Bureau of Statistics, 2016) indicate that most women seek help from friends or family members, followed by health practitioners and then police (Figure 9). Little is known, however, about their experiences accessing these supports and services, the barriers to help-seeking, what they want services to do, and what could be done better to promote more effective delivery of support. Almost nothing is known about the help-seeking behaviours of people who use IPV and/or SV or their service needs. This critical gap is a major focus of this report, as we sought to identify “what works” for women victims and survivors, and people who use IPV and/or SV in Australia. In the next section, we providean overview of the Australian literature to highlight specific gaps in our knowledge of help-seeking. More details about the literature review undertaken are in Appendix A.
Figure 9: Women’s help-seeking to formal and informal services (Australian Institute of Health and Welfare, 2018)
Data table for the figure above:
| Service | Experienced current partner violence | Experienced previous partner violence |
|---|---|---|
| General practitioner | 33.14% | 25.88% |
| Other health professional | 20.04% | 17.51% |
| Counsellor or support worker | 25.19% | 25.25% |
| Telephone helpline | 10.73% | 7.42% |
| Refuge or shelter | 4.26% | 7.73% |
| Police | 16.57% | 33.93% |
| Friend or family member | 66.75% | 64.85% |
| Work colleague or boss | 4.89% | 7.89% |
Note: Partner violence refers to any incident of sexual assault, sexual threat, physical assault or physical threat by a current and/or previous partner since the age of 15. Proportions are only representative of women who sought advice or support, not all women who have experienced violence. Proportions will not add to 100% as multiple sources of advice or support can be selected. Other sources of advice and support at not shown here including legal service, financial service, Government House and Community Services, and priest/minister/rabbi/other spiritual advisor.
Source: ABS 2017b
Overview of the literature on help-seeking for IPV and/or SV
We undertook a rapid systematic review of the peer-reviewed literature focused on the help-seeking behaviours and service needs of both victims and survivors of IPV and/or SV and people who use IPV and/or SV (see Appendix A for details). We identified relevant studies and reviews of the literature using a systematic search of key bibliographic databases (MEDLINE, Embase, PsycINFO, Cochrane Database, Applied Social Sciences Index and Abstracts: ASSIA, Web of Science, PsycArticles and Scopus). The search was conducted during September 2020, using relevant subject headings and key terms. This was informally updated in May 2022 to include more recent review articles. We also checked the reference lists of all included records to identify additional studies, and undertook hand-searching and communication with experts in the field to identify any further potentially relevant sources of data. All searches were filtered to 1 January 2010 onwards to findliterature related to contemporary service delivery.
The full search results are outlined in Appendix A. To provide context for our study, in the below sections we first summarise the primary studies (11 qualitative and four quantitative) undertaken in Australia between 2010 and 2020 and related to either women’s experiences of help-seeking after IPV and/or SV or help-seeking by people who use IPV/SV against women. Second, we outline the findings from recent systematic reviews (2020 onwards) focused on help-seeking by victims and survivors or perpetrators of IPV and/or SV.
Australian context 2010–2020
Overall, the evidence base in relation to the experiences and needs of women in Australia who have experienced IPV and/or SV is populated largely by qualitative studies (Day et al., 2018; Meyer & Stambe, 2021). These focused mainly on discrete aspects of help-seeking, for example disclosure experiences in particular settings, such as hospital emergency departments, general practice clinics, or the court system (Meyer, 2011; O’Doherty et al., 2016; Reisenhofer & Seibold, 2013); and the impact of particular contextual factors on help-seeking, such as rurality, migration status or being incarcerated (Day et al., 2018; Ghafournia & Easteal, 2019; Ragusa, 2016; Wendt et al., 2017). One study (Meyer, 2010a) examined how having children impacted on women’s help-seeking decisions in a small Queensland sample. Another Queensland study (Meyer, 2016) explored women’s experiences of victim-blaming when trying to access support after IPV. Morerecently, Tarzia and colleagues (2018) investigated women’s perceptions about online help-seeking, comparing their experiences to those who had sought help from a specially trained general practitioner. The findings suggested that preferences for help-seeking (online vs. face-to-face) were shaped by whether women prioritised a trusting relationship with a professional or autonomy and control over their help-seeking journey. Only one report was found that addressed women’s help-seeking experiences after SV (Hegarty et al., 2017), finding that women wanted to be heard, to be connected with a range of services, and to be helped to heal holistically.
Quantitative studies addressing women’s help-seeking in the Australian context were lacking. We found only three studies utilising cross-sectional surveys to explore help-seeking behaviours for IPV: one focused on postpartum women (Hooker et al., 2020), one on migrant women (Satyen et al., 2018), and one broader study on women’s decisions on whether and where to seek help (Meyer, 2010b). These studies suggest that women who had experienced IPV were more likely to use community and health services (Hooker et al., 2020) than women who had no IPV history, and that children witnessing IPV was the strongest predictor of initiating help-seeking (Meyer, 2010b). For Australian migrant women, many refrained from seeking help at all (Satyen et al., 2018). One study by Hegarty and colleagues (2013) found that women experiencing IPV sought help frequently, but from health or counselling services more than specialist IPV services. Severity of violence increasedthe likelihood of help-seeking. Limitations of these studies included a very low response rate to the surveys (Hooker et al., 2020) and a small sample size (Satyen et al., 2018).
No Australian studies were found exploring the help-seeking experiences or service needs of people who use IPV and/or SV.
Table 1: Characteristics of quantitative Australian-based studies exploring women’s help-seeking for IPV and/or SV
| Authors | Aim and objectives | Design and data collection method | Participants | Data analysis | Summary of findings | Study quality and limitations |
|---|---|---|---|---|---|---|
| Hegarty et al., 2016 | To explore associations between type and severity of IPV and health, quality of life and help-seeking | Baseline survey from randomised controlled trial | 272 women recruited from general practices who had experienced IPV | Logistic regression | Women who had experienced severe or combined physical/emotional abuse were more likely than the other women to have visited a counsellor, social worker or psychologist in the past 12 months. Participants also used healthcare services frequently but specialist domestic violence services infrequently | Sample may not be representative of all women attending primary care Self-report measures |
| Hooker et al., 2020 | To examine the help-seeking behaviour and perceived helpfulness of services in abused and non-abused postpartum women | Cross-sectional survey | 2,621 women recruited from maternal and child health settings | Descriptive and interferential statistics | Women who had experienced IPV sought: informal family support less frequently (81.3% compared with 92.4%, p < .001) were more frequent users of hospital emergency departments (p = .03), nurse home visiting programs (p = .02) and some breastfeeding services (p = .001), compared with non-abused women | Very low response rate to survey (25%) Respondents had a higher socio-economic status compared to non-responders |
| Meyer, 2010 | To explore factors that influence victims’ decisions on whether and where to seek help | Australian national survey | 2,276 women who had experienced IPV | Bivariate and multivariate analyses | While the presence of unborn children (i.e. pregnancy) had no effect on victims’ help-seeking decisions, children witnessing the abuse emerged as the strongest predictor of general and more formalised help-seeking decisions | Survey data only offer a snapshot of help-seeking decisions at one point in time |
| Satyen et al., 2018 | To explore Australian migrant women’s help-seeking for IPV | Cross-sectional survey | 130 migrant women who had experienced IPV | Descriptive and regression analysis | Most women who had experienced IPV indicated that they needed | Small sample size Reluctance of women to seek help warrants further research |
Table 2: Characteristics of qualitative Australian-based studies exploring women’s help-seeking for IPV and/or SV
| Authors | Aim and objectives | Design and data collection method | Participants | Data analysis | Summary of findings | Study quality and limitations |
|---|---|---|---|---|---|---|
| Day et al., 2018 | To explore help-seeking of women for IPV | Semi-structured interviews | 22 women who had been incarcerated | Thematic analysis | Barriers to help-seeking included:
|
|
| Ghafournia & Easteal, 2019 | To explore the help-seeking experiences of Muslim immigrant women who have experienced IPV | Semi-structured interviews | 14 women who had experienced IPV | Thematic analysis | Barriers to help-seeking included:
Women typically first accessed informal support. Formal support was found to be helpful but was only accessed at later stages |
|
| Meyer, 2010a | To explore women’s help-seeking for IPV when children are present | Semi-structured interviews | 29 women who had experienced IPV in Qld | Thematic analysis | Barriers to help-seeking included: stereotypical and victim-blaming attitudes along with a lack of understanding of the dynamics of IPV fear of harm and loss of custody. After disclosure, women felt trapped between expectations to protect their children by leaving the abusive partner and a reluctance on behalf of judges and magistrates to offer the necessary protection by including children on granted domestic violence orders (DVOs) |
|
| Meyer, 2011 | To explore women’s help-seeking through the criminal justice system after IPV | Semi-structured interviews | 29 women who had experienced IPV in Qld | Thematic analysis | Barriers to help-seeking included:
|
|
| Meyer, 2016 | To explore women’s experiences seeking help after IPV | Semi-structured interviews | 28 women who had experienced IPV in Qld | Thematic analysis | Women encountered blaming attitudes when seeking help from informal and general formal support sources |
|
| Meyer & Stambe, 2021 | To explore women’s help-seeking decisions and recovery from IPV | Semi-structured interviews | 13 Indigenous women in regional Qld who had experienced IPV | Thematic analysis |
|
|
| O’Doherty et al., 2016 | To explore the impacts of abuse on identity and its role in help-seeking | Semi-structured interviews | 14 women who had experienced IPV | Inductive/deductive thematic analysis |
|
|
| Ragusa, 2013 | To explore legal help-seeking experiences of rural Australian women who experience IPV | Semi-structured interviews | 36 women living in rural areas | Thematic analysis | Findings reveal that police and court responses reflect broader social inequalities and rurality exacerbates concerns such as anonymity and lack of service |
|
| Reisenhofer & Seibold, 2013 | To explore emergency healthcare experiences of women who experience IPV | Semi-structured interviews | 7 women who had experienced IPV and sought emergency or primary healthcare | Grounded theory | Barriers to help-seeking included:
|
|
| Tarzia et al., 2018 | To compare women’s experiences of help-seeking online with help-seeking face-to-face via a general practitioner | Semi-structured interviews | 16 women who had experienced IPV (8 who had used online support and 8 face-to-face) | Thematic analysis | Women who value control in help-seeking journey may prefer online support for IPV, whereas women who value trust may prefer face-to-face support from a trained professional |
|
| Wendt et al., 2017 | To explore how geographical and social isolation impacts on help-seeking experiences among rural women | Semi-structured interviews | 23 women | Thematic analysis | Shame and embarrassment and social isolation (particularly for non-Aboriginal women) were main barriers. Geographical isolation was not a barrier |
|
Recent reviews about help-seeking in a global context (2020–2022)
In May 2022, we informally updated our rapid review by undertaking a scan of the literature published since our initial review in 2020. We focused on review articles (such as systematic, narrative, integrative or scoping reviews; meta-analyses; meta-syntheses) summarising the literature from anywhere in the world. We identified 14 reviews on help-seeking by IPV and/or SV victims and survivors; one on the help-seeking of people who use IPV; and one addressing both victims and survivors and perpetrators of IPV. These have shed more light on the complexities and nuances of help-seeking for IPV and/or SV, particularly in relation to differing forms of IPV and help-seeking by people from marginalised populations.
Six of the reviews explored formal help-seeking, including the factors that facilitated or prevented help-seeking from service providers in the United States (Ravi et al., 2021; Robinson et al., 2020); the factors that silenced victims and survivors and prevented them from seeking formal help (Pokharel et al., 2020); and the factors that impacted disclosure and experiences of care within health settings (Heron & Eisma, 2021; Tarzia, Bohren, et al., 2020). Zinzow and colleagues (2021) explored the barriers to formal help-seeking for SV, situating these within an ecological framework. Two reviews comprehensively reviewed the qualitative literature on help-seeking for IPV in health settings (Heron & Eisma, 2021; Tarzia, Bohren, et al., 2020). The majority of the reviewed studies were assessed to be of good quality, though most were undertaken in Western countries and there was a lack of data from low- and-middle-income countries. Takentogether, these six reviews indicate that individual factors (particularly victim and survivor self-blame and concern about the impacts of disclosure on children or family) are important barriers to disclosing and seeking formal help, along with societal or structural factors, such as immigration policies, gender norms and pressures on women to present an image of a happy family (Heron & Eisma, 2021; Pokharel et al., 2020). The literature also identifies that how a potential disclosure recipient interacts with the victim and survivor plays a critical role in whether a victim and survivor discloses and/or continues to seek help. Receiving supportive responses from friends and family can be an important facilitator of formal help-seeking by victims and survivors (Ravi et al., 2021). Further, how healthcare providers and other services engage with victims and survivors – such as by being open and empathic, asking directly about abusive behaviours, and listening toand believing the victims and survivors – is critically important in facilitating help-seeking (Heron & Eisma, 2021; Ravi et al., 2021; Tarzia, Bohren, et al., 2020). Other key factors at the service level are the provider’s knowledge about IPV and the experiences of people from cultural, racial, sexual or other minorities; service accessibility (including location); and whether the provider caters for people with disability or those who speak different languages.
Recent reviews have further illuminated how marginalisation influences help-seeking. These include studies of the experiences of women who are South Asian (Sripada, 2021) and African American (Waller et al., 2021), and a study of victims and survivors with criminal backgrounds (Iratzoqui & Cohn, 2020). Consistent with the findings of the literature reviews discussed earlier, these reviews identify particular barriers to reporting IPV or seeking help for those from marginalised communities, including cultural stereotypes about African American women, which may become internalised (Waller et al., 2021), as well as a fear of negative responses from authorities or service providers for victims and survivors with criminal backgrounds (Iratzoqui & Cohn, 2020). Stigma and discrimination have also been identified as concerns for lesbian, gay, bisexual, trans and gender diverse, queer and questioning (LGBTQ) victims and survivors of IPV and/or SV(Edwards et al., 2022; Peitzmeier et al., 2020; Santoniccolo et al., 2021). Two recent systematic reviews of the help-seeking behaviours of sexual or gender minorities (one on IPV and one on SV) indicated a preference for relying on friends, family and other informal sources of support, while fear of being “outed”, homophobia and a heteronormative framing of relationships were barriers to using formal services (Santoniccolo et al., 2021). Similarly, a review of literature on IPV experiences of transgender people found experiences of discrimination when seeking help from services were common (Peitzmeier et al., 2020).
The literature also suggests that problematic behaviours are often normalised in relationships, which means victims and survivors do not identify them as abusive or feel that they have a legitimate reason to seek help (Pokharel et al., 2020). This may particularly be the case for women who are subjected to sexual forms of violence from a partner, according to the findings of a systematic review of 17 studies of SV by an intimate partner (Wright et al., 2021). Compared to other forms of IPV, experiencing SV by an intimate partner was associated with increased help-seeking from social, medical or legal services, yet also with decreased help-seeking from informal sources. The authors suggest the physical consequences of SV, such as pregnancies or sexually transmitted diseases, may prompt victims and survivors to seek formal help, while a social norm about keeping sexual relationships private may contribute to their reluctance to confide in family andfriends. A normalisation of abuse by a partner was also a barrier identified in a review of studies on help-seeking for elder abuse (Fraga Dominguez et al., 2021); the authors found that older victims and survivors were more likely to report abuse by a relative or paid caregiver than abuse by a partner.
Two recent reviews provide useful data on the help-seeking of people who use IPV (Calcia et al., 2021; Santoniccolo et al., 2021). A systematic review of qualitative studies on the experiences of perpetrators in accessing healthcare services identified six studies, reporting data on 125 participants, almost all of whom were male. A reluctance to admit their abusive behaviour to clinicians was commonly identified in studies, including a normalisation of the behaviour and minimising its impact or perceiving other personal issues were more of a priority in their lives. Other barriers were a concern about being blamed or not understood. Common triggers to help-seeking were the abuse escalating, the breakdown of their relationship or loss of contact with children, or legal intervention and other negative consequences. Participants reported engaging with a range of services, including GPs, drug and alcohol and mental health services, and often soughtreferrals for “anger management” programs. Finding a healthcare professional who listened non-judgementally facilitated disclosure of abusive behaviour and continued engagement with services. Calcia et al. (2021) also identified that for men in same-sex relationships, concerns that professionals lacked knowledge about their sexuality were barriers to disclosure. Similar findings were evident in a review on help-seeking in same-sex relationships by Santoniccolo et al. (2021). The authors found some studies included help-seeking by perpetrators (of all genders) as well as by victims and survivors. A lack of recognition of abuse perpetrated by women (both lesbian and heterosexual) was a barrier to seeking help, as was a perception that services would not understand same-sex relationships.
Evidence gaps
There are considerable gaps in the research literature about IPV and/or SV experiences – in particular, the nature and patterns of abuse and violence that are not just physical violence. For example, little is known about the nature and prevalence of financial control, emotional abuse, non-physical coercive control, technology-facilitated abuse, reproductive coercion and abuse, and systems-facilitated violence (for example intentionally drawing out litigation proceedings; Ayre et al., 2016; Cortis & Bullen, 2016; Our Watch, 2018a, 2018b; Partners for Prevention, 2020). We know little about how the patterns of violence vary between different cohorts – for example different demographic characteristics, women who stay with their partner and cohabiting/non-cohabiting perpetrators (Cox, 2015).
Furthermore, our review of the literature highlights that there remain some key evidence gaps around service experiences, needs and help-seeking of victims and survivors of IPV and/or SV. Although there is a fairly robust evidence base of good-quality qualitative research into women’s experiences of seeking help for IPV and support needs in health settings (Heron & Eisma, 2021; Tarzia, Bohren, et al., 2020) and the criminal justice system, there is less research on help-seeking in other contexts, such as specialist IPV services, children’s services, and financial or housing services (Australian Institute of Health and Welfare, 2018; Dowling & Morgan, 2019; Dowling et al., 2018; Humphreys & Healey, 2017). Importantly, there is a lack of research on women’s support needs at different time points and how their engagement with the service system unfolds over time, including when the abuse escalates orafter it ends (Harper, 2021; Wright et al., 2021). Furthermore, women who experience IPV and/or SV may have valuable insight or recommendations into the service needs of their partner or former partner (i.e. the perpetrator). This has not been the focus of any research across the service sector.
Although some systematic reviews (Iratzoqui & Cohn, 2020; Santoniccolo et al., 2021; Sripada, 2021) did address how marginalisation impacts help-seeking, in general we still have insufficient data on the experiences, service needs and help-seeking behaviours of specific vulnerable cohorts of women and their children. This includes women from culturally and linguistically diverse communities (CALD), those who are LGBTQ, Aboriginal and Torres Strait Islander women (Fiolet et al., 2019), women from rural communities, young (18 to 24 years old) and older women (over 65 years), and women who are socio-economically disadvantaged. While we know that many of these groups are at higher risk of violence, we know little about their unique experiences (Australian Institute of Health and Welfare, 2018; Ayre et al., 2016; Blagg et al., 2018; Cox, 2015; Dyson et al., 2017; Mitra-Kahn et al., 2016; Our Watch, 2017; Vaughan et al., 2016). There is an urgentneed for large-scale national research that allows for analysis of the experience and support needs of women with different demographic characteristics (Australian Institute of Health and Welfare, 2018; Cox, 2015; Dyson et al., 2017; Mitra-Kahn et al., 2016; Vaughan et al., 2016).
Developing insight into the service needs and experiences of perpetrators is another important area that requires urgent attention. It is critical that engagement of perpetrators with services and effective interventions be improved (Diemer et al., 2020; Gallant et al., 2017; Humphreys, Diemer, et al., 2019). Yet, it is unclear how this could best be achieved, since this is an area that has been largely neglected in extant research (Australian Institute of Health and Welfare, 2018; Humphreys & Campo, 2017). The Australian Institute of Health and Welfare (2018) calls for more research to develop insight into the outcomes and impacts of current service responses from the perspective of perpetrators, including health services, police and justice responses, and specialist services (Day et al., 2018; Day et al., 2019). Many of the available studies with perpetrators of IPV and/or SV have been undertaken with men participating in behaviour changeprograms, yet these programs only engage a subset of perpetrators, most of whom have been court-mandated to attend (Day et al., 2019; Tarzia, Forsdike, et al., 2020). In addition, a number of researchers have highlighted the importance of addressing the service needs of fathers who use violence, especially those who remain living together with their partner, and the need to build an evidence base around the development and outcomes of practice with this population (Diemer et al., 2020; Healey et al., 2018; Humphreys & Campo, 2017; Kaspiew et al., 2017).
Furthermore, during the COVID-19 pandemic, social isolation, psychological and financial stress, and unemployment may have exacerbated men’s use of violence in intimate relationships and created barriers to help-seeking from services (Bradbury‐Jones & Isham, 2020). Service provider reports suggest that women and children experiencing IPV had contact with friends and family members restricted as part of abuse tactics (Fitz-Gibbon et al., 2020). However, little research has been undertaken to date with victims and survivors of IPV and/or SV to explore their perspectives about how COVID-19 impacted their experiences of violence and their help-seeking.
In summary, there remains a need for further research into women victims’ and survivors’ experiences of IPV, particularly for non-physical forms, such as psychological abuse, financial abuse, or technology-facilitated abuse. There is also a dearth of research into women’s experiences of SV. In regard to help-seeking, although there is a good-quality qualitative evidence base focused on how health and criminal justice services respond to IPV, research is lacking across other facets of the service landscape. Again, help-seeking for SV is relatively under-represented in research across all settings. Major gaps exist around the experiences, support needs and help-seeking of people who use IPV and/or SV; it is critical that this be addressed in order to inform effective interventions and policies for perpetration of violence. This report contributes to filling this gap with data on experiences, barriers and enablers to help-seeking and support needs,and makes recommendations for policy and practice.
Policy context
The Australian Government is developing the National Plan to End Violence against Women and Children 2022–2032 (draft National Plan) to replace the existing National Plan. The draft plan has four pillars across prevention, early intervention, response and recovery. The current project is exploring help-seeking needs across the last three pillars for victims and survivors, children, and people who use IPV and/or SV. The National Summit on Women’s Safety statement from delegates called for the draft National Plan to prioritise listening, engaging and being informed by diverse lived experience, particularly that of victims and survivors. They also called for addressing men’s violence against women and children across all settings. This project is responding to these national policy contexts and can inform the development of specific strategies.
Aim of study
This collaborative project between Melbourne University and Australia’s National Research Organisation for Women’s Safety (ANROWS) aimed to provide in-depth insights into the experiences of different cohorts of people and to compare the experiences, service needs and help-seeking behaviours of these diverse cohorts. This is so as to enable tailored messaging and responses for people who experience or use IPV and/or SV.
Thus, this project aimed to gain insight into 1) the experiences of IPV and/or SV, including patterns of abuse and violence, and service needs from the perspectives of women victims; and 2) the experiences and service needs of people who use IPV and/or SV against women (please refer to key research questions below).
We aimed to understand:
- “what works” from the perspective of women victims and survivors in terms of service responses for themselves, their children and the perpetrator, and what their recommendations are for system improvement
- “what works” from the perspective of perpetrators in terms of service responses and what their recommendations are for system improvement.
Research questions
Specifically, we wanted to explore the following.
Victims and survivors
- What are the experiences and patterns of abuse and violence for Australian women victims and survivors over their lifetime?
- What is the association between patterns of abuse and demographic factors?
- How are adverse childhood experiences associated with victimisation for adult women?
- What are the help-seeking experiences, journeys to seeking help, and support needs of diverse women victims and survivors and their children following IPV and/or SV?
- What is the role of family and friends to support victims and survivors?
- What are women’s perspectives about the service needs of their partners who use IPV and/or SV?
- What are barriers to help-seeking and women’s expectations of service providers?
- How were victims and survivors impacted by COVID-19 and how can we safely reach victims and survivors during COVID-19 self-isolation?
People who use IPV and/or SV
- What are the patterns of abuse and violence from the perspective of perpetrators from different backgrounds?
- What is the association between patterns of abuse and demographic factors?
- What is the association of adverse childhood experiences, and attitudes to violence against women, with perpetration against adult women?
- How do perpetrators perceive the impact of violence on their family, including women and any children?
- What are diverse perpetrators’, help-seeking experiences, journeys to seeking help and support needs after use of IPV and/or SV?
- What is the role of family and friends to engage perpetrators in help-seeking?
- What are barriers to help-seeking and expectations of service providers working with people who use IPV and/or SV?
- How can we engage people who use violence to seek help during COVID-19 lockdowns/isolation?
The next part will outline the methodology used in the project and describe the ethical issues we addressed in the project.
Part B:
Methodology
Introduction
This part outlines the methods used for the surveys and the interviews, including recruitment, design and data analyses. This is followed by the ethical considerations of the project and how we synthesised the data to answer the research questions.
Surveys of women victims and survivors of, and people who use,
IPV and/or SV
The methods for the survey were the same for all participants, so below we outline how we recruited participants, as well as how data was collected and analysed.
Recruitment
The project utilised various participant recruitment strategies, including a range of social and traditional media channels to secure target participation, to drive awareness of the project and to sustain continued participation and interest throughout recruitment. Links to the online survey were distributed nationally between 27 January 2021 and 31 January 2022, via the project partners’ and advisory committee’s networks, membership lists and social media, including Facebook. Existing social media channels within Melbourne University and ANROWS were leveraged, while community groups and family violence organisations were asked to distribute the advertisement flyer. Participants for both surveys were recruited from across Australia. When reaching the sample size target for both surveys was proving difficult, we engaged the research company i-Link Research to assist. i-Link is a social and market research company with extensive experienceadministering online surveys to panel members across Australia (Boxall & Morgan, 2021). i-Link administers online research panels made up of people in Australian who have consented to receive information about a broad range of market and research surveys in which they can choose to participate. i-Link renumerates its panel member participants with “points” that can be redeemed as vouchers (M. Geagea, personal communication, 10 November 2021). Researchers at the University of Melbourne recruited 574 women victims and survivors and i-Link recruited 548 women victims and survivors. In terms of the recruitment of people who use IPV and/or SV, the researchers recruited 203 participants and i-Link recruited a further 360 participants.
Sample size
A sample size of 500 or more participants was determined in advance to be sufficient to detect meaningful differences between participants on variables of interest with at least 80 per cent power and a 5 per cent significance level.
Inclusion criteria
Inclusion criteria for the victim and survivor survey was women who spoke English and were aged 16 years and over. Women also needed to answer “yes” to at least one of four screening items about behaviours by a partner or ex-partner, date or stranger in the previous five years (Box 1).
The language and age criteria were the same for the people who use violence survey; however, participants could self-identify as any sex and needed to answer “yes” to at least one of three screening items about behaviours perpetrated against someone with whom they had been in an “intimate relationship” during the last five years (Box 2). By intimate relationship, we meant a current or former husband/wife, partner or boy/girlfriend for longer than one month.
Box 1: Victim and survivor survey screening items
In the last five years have you:
- Been afraid of a partner or ex-partner?
- Been controlled by a partner or ex-partner?
- Been physically hurt by a partner or ex-partner?
- Experienced unwanted sex by anyone, including a partner or ex-partner?
Box 2: People who use violence survey screening items
In the last five years have you:
- Been concerned about your behaviours in intimate relationships?
- Believe your behaviour has scared a partner or ex-partner?
- Sought help from anyone to address issues in your intimate relationships?
Data collection
Two online cross-sectional surveys were developed for women victims and survivors of IPV and/or SV and people who have used IPV and/or SV. Cross-sectional surveys are a robust method for reaching groups of people with quantitative questions about experience, particularly for sensitive and stigmatised research topics (Braun et al., 2020). Due to the anonymity of online surveys, they have been shown to result in more comfortable and candid participation for a greater number of people, while encompassing a broader range of views than in-person research methods (Burton & Blair, 1991). The surveys were developed in consultation with the project’s advisory committee, and were informed by survey theory, a review of the literature and an investigation of validated tools as well as the research team’s extensive experience in survey design and delivery with people who have experienced IPV and/or SV, and who have used IPV and/or SV (see Appendix Bfor the victim and survivor survey and Appendix C for the people who have used violence survey). The two English-language surveys were delivered online via the online survey platform Qualtrics. A range of standardised measures were incorporated (see Table 3). The survey was piloted with 11 people, which led to modifications of the wording and refined pathways through the survey.
Trauma-informed research design principles (Shimmin et al., 2017) were incorporated into both surveys, including that survey questions were optional due to their sensitive nature. An introductory sentence at the beginning of each section provided the purpose and overview of the section in an effort to assist participants with information about and control over the survey process. The surveys were regularly punctuated with contact details for support services and each page contained a quick exit link. The surveys took approximately 25 to 30 minutes to complete. Prior to survey completion, all participants were asked to read an information sheet. Consent was implied through returned surveys. Initially, participants who completed a survey were sent small ($30) gratis gift vouchers in recognition of their time and expertise. Vouchers had to be ceased when data integrity issues emerged (see “Methodological challenges” below).
Survey measures
For a summary of survey measures used, see Table 3.
Table 3: Survey measures
| Variables | Included topics | Survey V/S | P | Source measure |
|---|---|---|---|
| Screening items for victims and survivors | Fear of partner, control/physical hurt by partner, unwanted sex by anyone during last five years | V/S | Adapted from ACTS (Hegarty et al., 2021) |
| Screening items for people who use violence and abuse | Concern about behaviours in relationship, having scared a partner, sought help to address relationship issues during last five years | P | Adapted from other SAFER Families research projects |
| Sociodemographics | Age, education, income (including financial hardship), Aboriginal and Torres Strait Islander status, and CALD status, sexual identity, location, housing, children to compare with the population | V/S | P | Adapted from Australian Bureau of Statistics (2016) |
| Adult lifetime IPV | Validated measure of 15 abusive behaviours; occurrence (yes/no) of behaviours since age 15 years by someone with whom relationship lasted longer than one month Abuse categorised as psychological, sexual and/or physical (participants can belong to more than one category) | V/S | CASr-SF (Ford-Gilboe et al., 2016) |
| 12-month IPV | Ibid. If “yes” to abusive behaviour/s in adult lifetime, participant asked to score frequency of corresponding behaviour during last 12 months | V/S | CASr-SF (Ford-Gilboe et al., 2016) |
| Adult lifetime IPV perpetration | As above, adapted for use of 15 abusive behaviours since age 15 years against a partner of longer than one month | P | Adapted from CASr-SF (Ford-Gilboe et al., 2016) |
| 12-month IPV perpetration | If “yes” to use of abusive behaviour/s in adult lifetime, participant asked to score frequency of use of corresponding behaviour during last 12 months | P | Adapted from CASr-SF (Ford-Gilboe et al., 2016) |
| Sexual violence and reproductive coercion | Sex obtained via coercion or threats and interference in autonomous decision-making over reproductive health by anyone (experience of same for V/S survey and perpetration of same for P survey) | V/S | P | Sexual violence items developed by the research team with some items adapted from US National Intimate Partner and Sexual Violence Survey (Black et al., 2010). Reproductive coercion items adapted from the Australian Longitudinal Women’s Health Survey (Commonwealth of Australia, 2020) |
| Child abuse | Adverse childhood experiences questionnaire | V/S | P | ACE scale (Felitti et al., 1998) |
| Physical and mental health |
| V/S | P | SF-12 (Ware et al., 1996) PHQ-4 (Kroenke et al., 2009) Short Screening Scale for DSM-IV PTSD (Breslau et al., 1999) FAST (Hodgson et al., 2002) |
| Help-seeking | Self-reported use of health, justice, counselling and specialised services used in other studies | V/S | P | Adapted from other SAFER Families research projects |
| Service barriers and values | Service needs, expectations and perspectives | V/S | P | Adapted from other SAFER Families research projects |
| COVID-19 | Items to identify perceived impact and service needs | V/S | P | Adapted from other SAFER Families research projects |
| Attitudes | Measure of attitudes that support violence against women to compare with the population | V/S | P | (Webster et al., 2018) |
Notes:
Survey V/S= Victim and survivor survey.
Survey P = People who use violence survey.
Data analysis
Quantitative data analyses were performed using STATA (Version 15.0; StataCorp, 2015). All data was checked and cleaned for errors and accuracy. Sociodemographic characteristics of participants were summarised, using the mean and standard deviation for continuous measures, and counts and percentages for categorical data. Descriptive statistics were used to compare mean help-seeking between groups. For binary outcomes, differences in proportions were tested using McNemar’s chi-square test and odds ratios with 95 per cent confidence intervals (CI) calculated using ratio of numbers of discordant pairs. General linear models with related measures were used to assess differences for continuous outcomes with 95 per cent CI and p-values. Mixed effects linear models were used to describe the relationship between continuous outcomes and the factors associated at the participant level (e.g. sexual orientation, rurality,migrant background). For binary outcomes, a fixed and random effects logistic model was used to describe the relationship between outcome and factors.
Missing data
As is common with a survey method, not all participants in this study answered all questions in the survey, which resulted in missing data. Missing data is the reason why the denominators and samples sizes for each variable vary. The survey contained sensitive questions, which are known to increase the risk of missing data (Kirkwood & Sterne, 2003). In some instances, participants were excluded from analysis, and this is specified in the table notes (e.g. participants who had never been in a relationship were excluded from answering questions about relationship violence). Imputation methods were used to replace missing data, depending on type of data and the reason for data loss.
Qualitative survey data
Participants were asked to provide written responses to a number of open-ended survey questions. Response lengths ranged from a single word to three or four sentences. We used thematic analysis to analyse the qualitative survey data. This was done by importing the written responses for each survey question in an Excel spreadsheet into the software program NVivo 12. We then coded the data and grouped codes under higher-order thematic categories that reflected common patterns within the dataset, relevant to each research question. We gave some consideration to the prevalence of responses associated with a theme as a way of reflecting on the strength of a pattern in the data (in describing the findings, we identify this by referring to “many” or “some” responses), though quantifying themes was not our primary aim. Our focus was primarily descriptive themes, with some attention to underlying (latent) meanings in the data.
For victims and survivors, for each qualitative survey question we coded the responses of a random sample of 500 participants out of a total of 1,122 participants. We coded only a sample of responses due to time constraints. Different participants would have provided different responses to each qualitative survey question, so a limitation of this approach is that the responses we coded may not have reflected the entire dataset of participants. For the qualitative survey data from people who used abuse or violence, we coded the responses of the 288 participants who identified that they had used IPV and/or SV across their adult lifetime (sample described in Table 19).
Interviews with women victims and survivors of, and people who use, IPV and/or SV
The aim of the qualitative phase was to help explain or elaborate on the quantitative results obtained in the survey, exploring the journeys to help-seeking. For this phase, we used in-depth interviews to provide a more complex and nuanced understanding of the needs of victims and survivors and of people who use IPV and/or SV and how their help-seeking changed over time (see Appendices D and E for interview schedules). We separately recruited victims and survivors and people who had used IPV and/or SV. However, we used similar methods for recruitment, data collection and analysis.
We separately sought approval for the interview phase of the study from the University of Melbourne Human Ethics Committee (approval no. 2021-21471-23926-4).
Recruitment
Participants for interviews were drawn from those who had completed the survey and had expressed interest in participating in further research at the end of the quantitative survey. Those who ticked “yes” to participating in this research were provided with a link that directed them to a new form where they filled out their contact details (first name, phone number and best time to contact them safely). Information sheets were provided to the participants.
A total of 299 women victims and survivors expressed interest in participating in interviews. We used purposive sampling to recruit a diverse sample of 30 women interview participants, based on their age, birthplace, Aboriginal and Torres Strait Islander status, their location in Australia (i.e. different states and territories, urban/rural areas) and parenting status. To recruit participants who had used IPV and/or SV, we contacted the first 30 people who had completed the survey and had expressed interest in participating in further research (out of a total of 185 people who had expressed interest). We only contacted the first 30 people due to time constraints. Eight of those we contacted responded and agreed to be interviewed. Others did not respond to our contact or responded but declined to participate or were unavailable within the timeframe for the interview phase.
First, we emailed potential participants using the safe contact details they had provided. We then sent interested participants the consent form and plain language statement. We spoke to them by phone to explain the study and answer any questions. In all recruitment and interview processes, we used established ethical protocols for research with victims and survivors of interpersonal violence (World Health Organization, 2016) to ensure participant safety (for instance, we referred to the research as a “relationships, health and wellbeing” study).
Data collection
The interviews were held via telephone or using Zoom (video conferencing software). The approximate duration of interviews was between 30 and 120 minutes for victims and survivors and between 28 and 60 minutes for people who had used IPV and/or SV. In part, the difference in interview lengths reflected that most victims and survivors described in detail their experiences of being subjected to abuse and their long journeys of seeking help, while interview participants who had used IPV and/or SV tended not to speak at length about their behaviour and frequently had less contact with supports and services. The interview style was informal and conversation-like, which facilitated the sharing of experiences and may have reduced some of the power differences that can occur in a formal research interview (Burgess-Proctor, 2015). We used a narrative approach, which aims to encourage interview participants to tell detailed stories about their personalexperiences (Riessman, 2008). This approach was more appropriate for our aims than using a more structured interview schedule, given that our focus was on inviting participants to tell their story in their own words about their support needs, how they sought help or support for the IPV and/or SV and how this changed over time. For our interviews with women victims and survivors, we asked two questions: “Can you tell me about when you first realised what you were experiencing in your relationship was not okay?” and “Can you take me through your experiences of seeking help or support?” For our interviews with people who had used IPV and/or SV, we asked: “Can you tell me when you first realised there was an issue with your behaviour in your intimate relationship(s)?” and “Can you take me through your experiences of speaking to people about your behaviour in your intimate relationships?” We then used probes to draw out further details of key events, responses andturning points.
At the end of each interview, we provided a resource card with information about other types of health services, such as mental health, in addition to services about violence. We also provided participant honorariums in the form of e-gift vouchers valued at AU$40 per participant as a token of appreciation for their time and contribution.
Data analysis
The audio from interviews was transcribed by a professional service. We de-identified the transcripts, removing names of people, places, specific services and dates. For the analysis, we used an inductive thematic approach to generate key themes and identify the range of responses across participants (Braun & Clarke, 2006, 2021). We coded interview transcripts, assisted by the qualitative data software package NVivo 12. We then grouped codes into broader interpretative themes, using an iterative process of moving back and forth between the descriptive codes (and associated quotes from transcripts) and interpretative codes as they developed. We held discussions about interpretative and overarching themes as a research team to promote a rigorous approach to the analysis.
We also constructed a timeline of each participant’s support and help-seeking journey (Kolar et al., 2015; Patterson et al., 2012). This assisted us to organise the narrative data from individual interviews and to identify changes over time. We used Microsoft Excel to create a timeline analysis table. The table included the turning point or trigger event (such as the abuse escalating), the participant’s help-seeking aim or need, the source they sought help from, and a brief description of the response (e.g. “emotional support” or “being judgemental”). We then compared the timelines across participants to identify similarities and differences in turning points, help-seeking needs/aims and sources of help. This enabled us to identify common stages of help-seeking over time, the turning points that led to them, and perceptions of the responses received at each stage. We did not return to participants to check the accuracy of the timelines, as we wereinterested in the story as was it told in the interview, rather than ensuring that every relevant event was recorded in order. However, a limitation of this method is that in some cases, data about important events or turning points may have not been included, so the stages of help-seeking we identified in our findings may not have accurately reflected the journeys of all participants.
It should be noted that in re-presenting participant interview data by using case studies and quotations, we used pseudonyms and removed any other potentially identifying details.
Ethical considerations
The topics of IPV and SV are sensitive and potentially confronting. It is vital that research be undertaken in a safe, ethical and trauma-informed way to ensure the wellbeing of participants. Consequently, all phases of this research underwent ethical review by the University of Melbourne’s Human Research Ethics Committee prior to commencement. Below, we outline some of the key ethical considerations for this research, and how these were mitigated.
Participant distress
Participant distress is a very real risk for any researcher working in this complex and sensitive field. Our survey contained numerous items asking about abusive behaviours, and the interviews required participants to recall their experiences of violence in detail as well as what happened when they sought help. Despite this, it is important to remember that experiencing strong emotions when recalling a traumatic event is not the same as being retraumatised. Indeed, studies do consistently indicate that women usually find participation in research to be an empowering and cathartic experience (Valpied et al., 2014).
Similarly, research with people who have perpetrated IPV and/or SV could also elicit strong emotional responses such as distress or shame. While studies indicate that people using IPV and/or SV can safely, openly and honestly engage in discussions about past behaviours and processes of change (McGinn et al., 2020; Sheehan et al., 2012), it is vital that proper precautions be put in place.
As with all research conducted by the Sexual and Family Violence team in the Department of General Practice, distress protocols have been developed to guide the response of researchers should a participant become upset during an interview. The protocol includes supportive listening, allowing the participant time to pause or stop the interview if they wish, and checking in with participants at the end of the interview. Consistent with a trauma-informed approach (Campbell et al., 2019) we prepared participants before interviews by describing the interview process in detail, including the kind of questions they would be asked. The interviewers also showed empathy and validated participants’ strengths (Campbell et al., 2019). Participants were provided with information about available support services.
The plain language statements included a list of support services that participants may access. Trained research assistants with experience in working with individuals who have experienced or used IPV and/or SV were involved in participant engagement and responding to any potential distress using the distress protocol. During survey completion, if for any reason the participant was distressed, there was an option for them to save and return to the survey at any later time.
Perpetrator awareness
For women, completing an online survey about IPV and/or SV could have increased their risk of being victimised if a partner were to discover their participation. To reduce the risk of harm because of completing the online survey, the following actions were undertaken to reduce perpetrator or other people’s awareness:
- Each page of the online survey had a “quick exit” button which led to a blank Google search engine page.
- Best practice advice about online safety was provided to the participants at the very beginning of the survey (e.g. clearing browser history and cache).
- The survey title and all emails about the survey did not explicitly mention “domestic violence”, “intimate partner violence” or “sexual violence”.
Similar precautions were taken for the interviews, with communication about the study referring to a “women’s health project”. If at any time an unknown person answered the telephone, no information was provided about the study.
Privacy
To ensure participants’ identifying information was not associated with their survey responses, the following actions were undertaken:
- If survey participants decided that they wanted to be involved in an interview, they were directed to a completely new form to input their details.
- Consent forms for interviews were stored in a different location to the participants’ interview audio recording and transcript.
- For interviews, the researchers always ensured that the participant was in a private location. Participants were informed that if they were interrupted and were not in a position to speak privately at any time during the interview, they could simply end the call.
- Resource cards given to participants contained information about other types of health services, such as mental health, in addition to services about violence.
- All transcripts were de-identified before analysis. Consistent with a trauma-informed approach (Campbell et al., 2019), we offered participants the opportunity to check their transcripts to remove any contextual information they felt could identify them.
Disclosure of criminal activity
There was a small risk that a participant might disclose illegal activities during their interview or make a threat to harm another person. Clear safety protocols were in place to guide the research team including de-escalation if necessary and contacting emergency services. Researchers were familiar with mandatory reporting guidelines regarding disclosure of child abuse. Fortunately, no illegal activities or contemporary child abuse were disclosed to the research team at any point during the project.
Researcher wellbeing
All the researchers involved in this study were highly experienced, either with a research background in IPV and/or SV, a clinical or counselling background, or a combination of both research and practice expertise. Team members were therefore aware of the importance of practicing good self-care during the study and had their own strategies in place to reduce the likelihood of vicarious trauma. Nonetheless, additional actions were taken to ensure that any member of the team who experienced feelings of distress was well-supported. We undertook weekly meetings where any concerns could be openly discussed and strategies or solutions workshopped with others. The two researchers conducting the interviews undertook additional debriefings with a senior member of the team on a regular basis to discuss specific issues relating to this phase of the research. Team members also had access to supervision on an ad hoc basis if needed. As Moran and Asquith (2020)have noted, emphasising how the research is contributing to positive change for victims and survivors of IPV and SV can help to compensate for some of the emotional challenges inherent in this work; this was something we frequently reflected on as a team.
Synthesis
The ANROWS team collaborated with the Melbourne University research team to appoint representatives of key organisations and services. The research team engaged with the advisory committee (16 members), which has wide representation from government, non-government and service organisations. The advisory committee provided feedback on the research design, survey instruments and findings to ensure that the research meets their priorities and will be useful for policy and practice. The advisory committee also assisted with providing contacts and networks for the recruitment of research participants and was consulted further about survey questions and the piloting of research instruments.
Methodological challenges
There were several specific challenges that occurred during this project that delayed progress and also required some new methods to be utilised. We became aware that some participants had been answering our online survey multiple times for the sake of receiving gift vouchers. As a result of this incident, we stopped sending gift vouchers to all participants, changing to a draw for iPads. We manually checked whether the data was genuine by going through data line by line using a variety of methods including IP addresses, length of time to complete and qualitative responses. We removed fraudulent responses. We only sent gift vouchers to participants who genuinely responded and completed the survey. We also further changed our processes to a brief screening survey that was unlikely to be able to be answered by computer and participants got a separate email with a new link to the survey which stopped all fraudulent responses. We are confident of thisbecause we checked the data very closely.
Summary
We undertook an online survey of adult women who had experienced IPV and/or SV and a survey of people who used IPV and/or SV against women. Participants were recruited via social media and traditional media channels. We cleaned the data and used descriptive statistics for our analysis of the quantitative survey data. We also analysed open-ended survey questions about experiences of help-seeking for IPV and/or SV and support needs. We held interviews with women victims and survivors and men who used IPV and/or SV. They were survey participants who had expressed interest in participating in an interview. We thematically analysed the interview data and constructed a timeline of each participant’s support and help-seeking journey.
Part C:
Key findings –
Victim and survivor experiences
The most helpful people I’ve spoken to are empathetic, non-judging and know where to [go] next. Especially in the early stages of leaving there’s so much fear and you need to know you are doing the right thing. It’s a very lonely road.
(Survey participant)
Introduction
This part is divided into three sections that integrate quantitative and qualitative findings from the perspective of the victims and survivors. The first section overviews participant characteristics and the nature, patterns and health impacts of IPV and/or SV, including the effects of the COVID-19 pandemic on experiences. This is followed by a section on help-seeking and service needs, including the effects of the COVID-19 pandemic on help-seeking. The final section describes support needs of victim and survivor participants.
1. Patterns and associations of abuse and violence
Sociodemographic characteristics
Overall, study participants were generally representative of the Australian population of women except for some specific demographic areas (see Table 4). The average age of victim and survivor participants was around 42 years, which represents a slightly higher mean age compared to the general Australian population. Among women in this study, most Australian states and territories had similar representation to the Australian population, except that a greater proportion of participants lived in Victoria (33.4%), while fewer lived in New South Wales (21.9%). A similar proportion of women participants to the general Australian population lived in a metropolitan area (71.5%).
Just under half the women (45.6%) were in a current relationship and 44.3 per cent were living with their partner. Of those in a relationship, the majority (94.8%) reported their partner as male, 3.8 per cent female and 1.4 per cent as non-binary. Approximately one in four (26.2%) participants were married, and three in four (75.7%) had children living at home with them.
Table 4 shows a comparison of specific demographic characteristics. This study recruited almost double the proportion of Aboriginal and Torres Strait Islander women (7.8%) compared to population figures, but a lower share of women born overseas (18.1%). A greater number of women participants had attained a trade, apprenticeship or diploma after high school (57%), or had attended university (43%), compared to the general population. Approximately three fifths of participants were employed (59.3%), a smaller proportion than the general Australian population. A greater percentage of women participants in this study held a Health Care Card (60%) or reported difficulty managing on their available income some or all of the time (58.5%) compared to the general population (Table4).
Table 4: Demographic characteristics of survivor women participants compared to the broader Australian population (N=1,122)
Age (years)
| Characteristic | All participants | Australian population (women) %a |
|---|---|---|
| 18–29 | 231 (20.6) | 18.6 |
| 30–39 | 298 (26.6) | 14.7 |
| 40–49 | 265 (23.7) | 12.9 |
| 50–59 | 191 (17.1) | 12.4 |
| 60–69 | 99 (8.8) | 10.9 |
| 70–79 | 32 (2.9) | 7.8 |
| 80+ | 4 (0.4) | 4.8 |
Current Australian state of residence (n=1,121)
| Characteristic | All participants | Australian population (women) %a |
|---|---|---|
| Australian Capital Territory | 27 (2.4) | 0.8 |
| New South Wales | 245 (21.9) | 17.4 |
| Victoria | 375 (33.4) | 13.4 |
| Northern Territory | 11 (1) | 0.2 |
| Queensland | 239 (21.3) | 10.5 |
| Western Australia | 111 (9.9) | 5.2 |
| Tasmania | 32 (2.8) | 1.4 |
| South Australia | 81 (7.2) | 4.4 |
| Lives in metropolitan area (n=1,117) | 799 (71.5) | 71 |
| In current relationship (≥1 month length) | 508 (45.6) | N/Ab |
| Lives with a partner | 497 (44.3) | 45 |
| Sex of current partner (n=497) | N/A | |
| Male | 471 (94.8) | 59.8 |
| Female | 19 (3.8) | 7.1 |
| Non-binary | 1 (1.4) | 17.3 |
Sexual orientation (n=1,070)
| Characteristic | All participants | Australian population (women) %a |
|---|---|---|
| Heterosexual | 844 (78.9) | 92 |
| Bisexual | 107 (10) | 1.4 |
| Lesbian | 20 (1.9) | 1.9 |
| Queer | 11 (1) | N/A |
| Pansexual | 18 (1.7) | N/A |
| Asexual | 13 (1.2) | N/A |
| Self-described | 33 (3.1) | N/A |
| Not sure | 24 (2.2) | 0.8 |
Marital status (n=1,220)
| Characteristic | All participants | Australian population (women) %a |
|---|---|---|
| Never married | 459 (41) | 32 |
| Married | 294 (26.2) | 30.6 |
| Separated but not divorced | 144 (12.9) | 3.1 |
| Divorced | 200 (17.9) | 7 |
| Widowed | 23 (2.1) | 6 |
| Children | 746 (66.6) | 43 |
| 1+ children living at home | 565 (75.7) | 49 |
| Aboriginal and/or Torres Strait Islander | 87 (7.8) | 3.2 |
| Born outside Australia | 203 (18.1) | 30 |
| First language not English | 83 (7.4) | 21 |
| Prior schooling | (n=1,060) | |
| Attended school but finished prior to Year 12 | 295 (28.1) | 10.5 |
| Completed Year 12 | 734 (69.9) | 79 |
| Educational qualification | (n=1,050) | |
| Trade/apprenticeship/diploma | 598 (57) | 26.5 |
| University degree/higher degree | 452 (43) | 29 |
Employment and income (n=1,069)
| Characteristic | All participants | Australian population (women) %a |
|---|---|---|
| Employed | 634 (59.3) | 64.1 |
| Not in employment | 435 (40.7) | 5.7 |
| Has difficulty managing on available income | 626 (58.5) | 18.7 |
| Health Care Card holder | 641 (60) | 52 |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey item.
a Population data is weighted proportions from Australian Bureau of Statistics (2020);, values are percentages of women as a proportion of the total Australian population.
b Comparable data either not collected or available.
Twelve-month and lifetime experiences and patterns of IPV and/or SV
To understand the experiences of IPV and/or SV victims and survivors, the survey screened participants for IPV and/or SV using three items about specific acts of abuse by a partner or ex-partner in the last five years. One further item asked about SV perpetrated by anyone. Participants could answer with a simple “yes/no” response. Further, IPV and/or SV experiences of participants were collected via the short-form CASr-SF (Ford-Gilboe et al., 2016) for the last 12 months and lifetime, and experiences of child abuse were measured using the Adverse Childhood Experiences scale (Felitti et al., 1998; see “Methodology” further).
While not all participants reported experiencing IPV and/or SV when measured using the CASr-SF (Ford-Gilboe et al., 2016), the eligibility of all women to participate in the study was established through their positive response to one or more screening questions (see “Methodology” further). The screening questions indicated that the participant had experienced abuse and violence in a relationship (including casual relationships) in the last five years, and/or had experienced SV by anyone in the same timeframe. In this context, we chose to analyse the whole sample of women participants, rather than selecting out only the women who scored on the CASr-SF, and we refer to all participants in this section as “victims and survivors” (Ford-Gilboe et al., 2016).
IPV in the last 12 months
Three in four women participants (76.1%) were currently afraid of their partner or ex-partner, while 80.7 per cent reported that they had felt afraid of a partner during the previous 12 months (Table 5). Fear of a partner was a feature of most (between 86% and 100%) victim and survivor participants’ experiences regardless of the type of violence and abuse their partner had perpetrated against them in the last 12 months.
Table 5: Proportion of women who experienced IPV and/or SV during the last 12 months
Last 12 months
| Types of IPV | n (%) |
|---|---|
| Afraid of partner or ex-partner in last 12 months (n=1,038)a | 838 (80.7) |
| Currently afraid of partner or ex-partner (n=930) | 708 (76.1) |
| IPV any category (CASr-SF; n=881)b | 362 (41.1) |
| Physical | 194 (23.6) |
| Sexual | 190 (23.8) |
| Psychological | 286 (38.5) |
| Total: 12-month fear of a partner and/or IPV (n=1,038) | 861 (82.9) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed 12-month CASr-SF (Ford-Gilboe et al., 2016).
a Seventy-six participants were omitted because they had never been in a relationship for longer than one month.
b Participants could belong to more than one CASr-SF category.
The occurrence of combined categories of IPV was more prevalent than not; more women participants had experienced physical, sexual and psychological abuse (27.1%) than had experienced one or two IPV categories in the last 12 months (Figure 10). The second most common type of IPV women had experienced was psychological IPV not in combination with any other category of IPV (24.6%), followed by combined physical and psychological violence (16.9%). Physical and sexual IPV without psychological abuse was the least common category of IPV reported (3.9%).
Figure 10: Proportion of participants who experienced physical, sexual and psychological IPV in the last 12 months (n=361)
Data table for the figure above:
| Type of violence | Percentage | n |
|---|---|---|
| Physical violence | 5.8% | 21 |
| Sexual violence | 11.1% | 40 |
| Psychological violence | 24.6% | 89 |
| Physical and sexual violence | 3.9% | 14 |
| Physical and psychological violence | 16.9% | 61 |
| Sexual and psychological violence | 24.6% | 89 |
| Physical, sexual and psychological violence | 27.1% | 98 |
Of those who had experienced IPV in the last 12 months (n=362), almost two thirds (60.8%) of victim and survivor participants had experienced technology-facilitated harassment, and around one in three (31.8%) had been financially abused by being kept from having access to a job or finances. The most commonly perpetrated acts of abuse reported were being told they were crazy, stupid or not good enough (84.8%); being blamed for causing the violent behaviour (83.4%); and the perpetrator trying to convince family, friends and children they were crazy or trying to turn those people against them (61.3%; Table 6).
The next section describes lifetime experiences.
Table 6: Proportion of women who experienced 12-month IPV and/or SV and type of abusive behaviour (n=362)
| Abusive behavioursa | n (%) |
|---|---|
| Told me I was crazy, stupid or not good enough | 307 (84.8) |
| Blamed me for causing their violent behaviour | 302 (83.4) |
| Tried to convince my family, children or friends that I am crazy or tried to turn them against me | 222 (61.3) |
| Harassed me by phone, text, email or using social media | 220 (60.8) |
| Shook, pushed, grabbed or threw me | 205 (56.6) |
| Kept me from seeing or talking to my family or friends | 169 (46.7) |
| Made me perform sex acts that I did not want to perform | 158 (43.6) |
| Forced or tried to force me to have sex | 140 (38.7) |
| Followed me or hung around outside my home or work | 134 (37) |
| Kept me from having access to a job, money or financial resources | 115 (31.8) |
| Threatened to harm or kill me or someone close to me | 111 (30.7) |
| Hit me with a fist or object, kicked or bit me | 109 (30.1) |
| Choked me | 95 (26.2) |
| Used or threatened to use a knife or gun or other weapon to harm me | 79 (21.8) |
| Confined or locked me in a room or other space | 51 (14.1) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed 12-month CASr-SF.
a Experienced these behaviours once or more during last 12 months.
IVP, SV and reproductive coercion since age 16 years
Of all victims and survivors who had experienced IPV and/or SV by a partner or ex-partner since the age of 16 years, 84.3 per cent had felt fear of their partner (Table 7) and for half (51.5%), their experience was of physical, sexual and psychological IPV (Figure 11). In fact, very few women participants (15.4%) reported the experience of one type of IPV in isolation (Figure 11). For example, only 3 per cent of victims and survivors had experienced physical or sexual IPV alone. Nearly one in three women participants (32.9%) had experienced their partner interfere with or force their independent decision-making about pregnancy, including 17.1 per cent having been forced to terminate a pregnancy and 15.3 per cent being forced into pregnancy (Table 7).
Table 7: Proportion of women who experienced IPV and/or SV across the adult lifetime since the age of 16 years
| IPV and/or SV | n (%) |
|---|---|
| Total adult lifetime IPV, including fear, intimate partner SV and/or reproductive coercion | 1,008 (96.4) |
| Afraid of partner or ex-partnera | 882 (84.3) |
| IPV (scored using CASr-SF) | 905 (87.1) |
| Sexual violence by an intimate partner | 852 (82.5) |
| Forced sexual activity | 701 (67.8) |
| Had unwanted sex with a partner due to fear | 718 (69.4) |
| Forced to watch pornography | 370 (35.8) |
| Reproductive coercion | 341 (32.9) |
| Forced pregnancy | 158 (15.3) |
| Prevented termination of pregnancy | 102 (9.9) |
| Forced termination of pregnancy | 177 (17.1) |
| Contraception interfered with or partner prevented use | 139 (13.4) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed survey items.
a Seventy-six participants omitted because they had never been in a relationship for longer than one month.
Figure 11: Proportion of participants who had experienced physical, sexual and psychological IPV since the age of 16 (n=1,001)
Data table for the figure above:
| Type of violence | Percentage | n |
|---|---|---|
| Physical violence | 0.7% | 7 |
| Sexual violence | 2.3% | 23 |
| Psychological violence | 12.4% | 124 |
| Physical and sexual violence | 0.3% | 3 |
| Physical and psychological violence | 22.3% | 223 |
| Sexual and psychological violence | 10.5% | 105 |
| Physical, sexual and psychological violence | 51.5% | 516 |
Please note: n=1,001 includes all women who scored on any of three lifetime IPV categories of abuse using the CASr-SF, including emotional abuse and harassment.
The three most frequently reported acts of abuse across 905 victim and survivor participants were as follows: being told they were crazy, stupid, or not good enough (80.2%); being blamed for causing the violent behaviour (75.9%); and being shaken, pushed, grabbed or thrown (64%; Table 8). The most commonly reported experience of sexual violence was feeling forced to have unwanted sex with a partner due to fear (69.4%; Table 7). Almost two in three (60.5%) victim and survivor participants had experienced technology-facilitated harassment and 40.7 per cent had experienced financial abuse (Table 8).
Table 8: Proportion of women who experienced lifetime IPV and/or SV and type of abusive behaviour (n=905)
| Abusive behavioursa | Adult lifetime |
|---|---|
| Told me I was crazy, stupid or not good enough | 833 (80.2) |
| Blamed me for causing their violent behaviour | 789 (75.9) |
| Shook, pushed, grabbed or threw me | 665 (64) |
| Harassed me by phone, text, email or using social media | 627 (60.5) |
| Tried to convince my family, children or friends that I am crazy or tried to turn them against me | 625 (60.2) |
| Kept me from seeing or talking to my family or friends | 587 (56.5) |
| Made me perform sex acts that I did not want to perform | 570 (54.9) |
| Forced or tried to force me to have sex | 562 (54.3) |
| Hit me with a fist or object, kicked or bit me | 429 (41.3) |
| Kept me from having access to a job, money or financial resources | 422 (40.7) |
| Threatened to harm or kill me or someone close to me | 399 (38.4) |
| Choked me | 352 (33.9) |
| Used or threatened to use a knife or gun or other weapon to harm me | 295 (28.4) |
| Confined or locked me in a room or other space | 221 (21.3) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed CASr-SF (Ford-Gilboe et al. 2016).
a Behaved in this way once or more during last 12 months.
Associations between patterns of abuse and sociodemographic characteristics
Looking at sociodemographic associations with combinations of abuse, women aged 25 to 45 years were over-represented as victims and survivors of poly-victimisation, including IPV in the last 12 months and IPV combined with sexual violence, reproductive coercion and child abuse (Table 9). Aboriginal and Torres Strait Islander women also indicated a higher prevalence of poly-victimisation across different forms of abuse compared to other women. Further, unemployed women were more likely than other women to have experienced IPV in combination with sexual violence and personal history of child abuse. Women who were not living with their partner at the time of completing the survey were less likely than other women to have experienced IPV in the last 12 months, whilemigrant women were less likely to report being a victim and survivor of poly-victimisation.
In brief:
Poly-victimisation against victims and survivors
Aboriginal and Torres Strait Islander women, women aged 25 to 45 years and unemployed women were overepresented as victims and survivors of IPV, SV and child abuse.
Migrant and young women were underrepresented as victims and survivors of poly-victimisation with multiple types of abuse.
Table 9: Proportion of women who experienced multiple abuse types, with sociodemographic factors
| Sociodemographic factors | Experienced IPV in last 12 months (alone) (n=1,039) | Experienced lifetime IPV and SV and reproductive coercion (n=305) | Experienced lifetime IPV and SV and reproductive coercion and child abuse (n=245) |
|---|---|---|---|
| All participants (n=1,122) | 861 (82.9) | 305 (29.2) | 245 (21.8) |
| Age (years; n=1,120) | |||
| Up to 25 years (n=104) | 84 (80.8) | 20 (19.2) | 16 (12.9) |
| 25–45 years (n=516) | 460 (89.2) | 188 (36.3) | 151 (27.4) |
| > 45 years (n=418) | 317 (75.8) | 97 (23) | 78 (17.5) |
| Aboriginal and/or Torres Strait Islander (n=76) | 71 (93.4) | 98 (32.7) | 31 (35.6) |
| Migrant background (n=192) | 154 (80.2) | 43 (22.4) | 32 (14.7) |
| Same-sex partner (n=29) | 27 (93.1) | 8 (26.7) | 8 (22.2) |
| Lives in non-metropolitan location (n=297) | 238 (80.1) | 98 (32.7) | 79 (24.8) |
| Lives with disabilitya | 330 (79.1) | 136 (32.5) | 119 (27.1) |
| Attended school but finished prior to Year 12 (n=301) | 241 (80.1) | 167 (30.2) | 146 (24.4) |
| No university degree (n=552) | 453 (82.1) | 119 (29.7) | 99 (22.8) |
| No employment (n=401) | 314 (78.3) | 207 (35.4) | 168 (26.8) |
| Has difficulty managing on available income (n=584) | 493 (84.2) | 188 (32) | 153 (23.9) |
| Health Care Card holder (n=588) | 478 (81.3) | 172 (29.4) | 135 (21.6) |
| Not living with partner (n=580) | 434 (74.8) | 305 (29.2) | 245 (21.8) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
% = represents the proportion of overall demographic group who have experienced the abuse category (IPV/sexual violence/reproductive coercion/child abuse).
a Lives with disability defined as participants who answered “yes” to living with a disability or chronic illness limiting daily activities including employment.
Adverse childhood experiences and victimisation in adulthood
There was a significant overlap for women participants between having experienced IPV and/or SV in adulthood and abuse during childhood. Two out of three (69.4%) participants had experienced physical, sexual or emotional abuse in childhood, and half (50.3%) had experienced four or more adverse experiences measured using the Adverse Childhood Experiences scale (Felitti et al., 1998); Table 10). Close to a quarter (23.8%) of women participants had grown up in a household where there was violence perpetrated against their mother. Among 12-month IPV and/or SV victim and survivor participants, 62 per cent had a history of child abuse, and for adult lifetime IPV and/or SV victims and survivors the proportion rose to 70.4 per cent who had experienced child abuse.This represented a more than fourfold increase in the predicted odds of reporting IPV and/or SV for victims and survivors who had a history of child abuse, indicating a life course effect of child abuse on adult relationships (OR 4.4, 95% CI 2.1 to 9.1).
Table 10: Proportion of women who experienced child abuse
| Child abuse typea | Before age 15 years (n=1,115) |
|---|---|
| Emotional neglect | 626 (56.1) |
| Emotional abuse | 616 (55.2) |
| Physical abuse | 447 (40.1) |
| Sexual abuse | 402 (36) |
| FV against mother growing up | 266 (23.8) |
| Physical neglect | 196 (17.6) |
| Total child abuse | 774 (69.4) |
| Total ACE b score of 4+ | 561 (50.3) |
| Total child abuse and/or ACE>4 | 788 (70.7) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to child abuse survey items.
a Abusive behaviour before the age of 15 years by someone aged 18 plus years.
b Adverse Childhood Experiences scale (Felitti, 2019) score out of 10. Scores 4+ are associated with serious health and risk issues in adulthood (Felitti, 2019).
Health of victim and survivor participants
The burden of disease for participants was high, with health issues including (self-rated) poor health, long-term illness, mental health issues and/or hazardous alcohol consumption over-reported by victims and survivors compared to the general population (Breslau et al., 1999; Hodgson et al., 2002; Kroenke et al., 2009; Ware et al., 1996). Half of the victim and survivor participants met the core criteria for generalised anxiety disorder (52.4%; Kroenke et al., 2009), while three quarters of participants screened positive for PTSD (71.2%; Breslau et al., 1999). The proportion of participants reporting health issues increased as the types of abuse they had experienced increased. Table 11 demonstrates that victims and survivors whose IPV included sexual violence and reproductive coercion had higher rates of poor health across all health measures when compared to victims and survivors of IPV alone in the last 12 months. For victims and survivors oflifetime IPV and/or SV whose experience had also included childhood abuse, the prevalence of health issues rose higher again (Table 11).
Table 11: Proportion of women who experienced health and mental health issues by type of abuse and cumulative abuse
Mental health
| Current health issue | All participants (n=1,122) | IPV in last 12 months (n=1,039) | Experienced lifetime IPV and SV and reproductive coercion (n=305) | Experienced lifetime IPV and SV and reproductive coercion and child abuse (n=245) |
|---|---|---|---|---|
| PTSD (n=1,120) | 797 (71.2) | 636 (73.4) | 252 (82.6) | 209 (85.3) |
| Anxiety (n=1,121) | 587 (52.4) | 481 (55.9) | 196 (64.3) | 167 (68.2) |
| Depression (n=1,121) | 509 (45.4) | 407 (47.3) | 170 (55.7) | 150 (61.2) |
General health
| Current health issue | All participants | IPV in last 12 months | Experienced lifetime IPV and SV and reproductive coercion | Experienced lifetime IPV and SV and reproductive coercion and child abuse |
|---|---|---|---|---|
| Lives with disability (n=1,121) | 439 (39.2) | 330 (38.3) | 136 (44.6) | 119 (48.6) |
| Poor to fair self-rated health (n=1,121) | 398 (35.5) | 310 (36) | 125 (41) | 111 (45.3) |
| Hazardous alcohol consumption (n=1,118) | 239 (21.4) | 173 (20.1) | 77 (25.2) | 64 (26.1) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
When looking at the experiences of victims and survivors as abuse in their lives accumulated, two groups of victims and survivors reported poorer health than other victims and survivors on a variety of measures: Aboriginal and Torres Strait Islander victims and survivors and those who have difficulty managing on their available income (Table 12). By contrast, migrant victims and survivors were less likely to experience a range of health and mental health issues compared to other victims and survivors.
Table 12: Proportion of women from diverse backgrounds who have experienced lifetime IPV and/or SV and health and mental health issues
| Current health issues | All (lifetime) IPV and/or SV victims and survivors (n=979) | Aboriginal and Torres Strait Islander victims and survivors (n=71) | Migrant victims and survivors (n=192) | Non-metro victims and survivors (n=297) | Unemployed victims and survivors (n=401) | Victims and survivors who have difficulty managing on available income (n=584) | Victims and survivors not living with a partner (n=580) |
|---|---|---|---|---|---|---|---|
| Poor to fair self-rated health (n=398) | 366 (37.2) | 25 (35) | 49 (25.5) | 103 (36.4) | 200 (52.9) | 256 (45.5) | 198 (35.9) |
| Lives with disability (n=439) | 400 (40.9) | 35 (49.3) | 56 (31.6) | 131 (46.3) | 219 (57.9) | 265 (47.2) | 239 (43.3) |
| Anxiety (n=531) | 531 (54.2) | 49 (69) | 82 (46.3) | 150 (53) | 272 (48.8) | 344 (61.2) | 292 (52.9) |
| Depression (n=509) | 461 (47.1) | 49 (69) | 81 (45.8) | 134 (47.3) | 209 (55.3) | 320 (56.9) | 246 (44.6) |
| PTSD (n=797) | 722 (73.7) | 61 (85.9) | 117 (66.1) | 211 (74.6) | 309 (81.7) | 461 (82) | 414 (75) |
| Excessive alcohol consumption (n=239) | 199 (20.3) | 32 (45.1) | 27 (15.2) | 58 (20.5) | 72 (19) | 117 (20.8) | 87 (15.8) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all women who completed CASr-SF and responded to demographic and health survey items.
In brief
Health and mental health of victims and survivors
Aboriginal and Torres Strait Islander women, women who experience difficulty managing on their available income and unemployed women more frequently reported poor health issues.
Women not living with their partner less frequently reported poor health and mental health issues.
This section has provided insight into the patterns of IPV and/or SV experienced by women and associations with sociodemographic characteristics, health issues and service use. In the next section we examine qualitative survey data on the impact of the COVID-19 pandemic on IPV and/or SV for victims and survivors.
COVID-19 pandemic effects on women’s experiences
We asked women survey participants to provide written responses to the question: “How have your experiences in your adult intimate relationships changed during COVID-19 isolation?” Many simply commented “no change”. However, others reported the pandemic changed the abuse they experienced. We identified the following three themes from our analysis of participants’ comments.
Isolation fuelled and enabled the abuse
A key theme was that abuse or violence from a partner had first occurred during the pandemic and that COVID-19-related restrictions had amplified or enabled abusive behaviour. A key contributing factor for participants was having to spend more time with the perpetrator at home and being isolated from family and friends, which gave the perpetrator more opportunities to abuse and monitor them. The following quotes from two participants are examples:
I was a prisoner to the house. Because I couldn’t work he had total control. I did shopping on line so he knew what I spent etc. … he was happiest during lock down.
It was easier for my ex-partner to manipulate me when I was cut off from the outside world.
Many mentioned feeling “suffocated”, “imprisoned” and “trapped”, or commented that nowhere felt safe during the pandemic (for instance, “it was harder to find a safe space in and out of home”). However, it was not only women who were co-habiting who reported an escalation in the abuse. Some said the perpetrator having less access to them triggered monitoring behaviour from a distance:
During lockdowns contact was by phone however [the perpetrator] started to become possessive. Several messages a day, numerous phone calls. Was told to breach lockdown rules to travel to see, we lived in different towns (1.5 hours away). Constant checking up what I was up to.
Participants frequently linked the increased abuse with the perpetrator’s heightened stress levels due to a loss of employment, the pressures of home schooling and/or having fewer distractions or outlets.
[The abuse] escalated immensely during this time and compounded with our 2019 bushfire season and unemployment due to COVID-19. His drinking became out of control and subsequent verbal and emotional abuse, isolation and financial control became a daily occurrence instead of monthly.
Worse because more time together and harder to have a break, their increased stress, and being cut off from supports.
Being together more has brought out his anger and frustration without work as a distraction.
My partner became very unwell. She lost her business, as not being an Australian citizen, she hasn’t had money and we have had to live off one income. It has put us under so much stress, she was never violent before COVID-19.
Women also said that their partner’s constant presence and monitoring of them meant they struggled to take a break from them, to look after their own wellbeing or to make plans to escape:
[It’s] definitely worse during lockdowns – he can still access alcohol/cigarettes and all the things that fuel his behaviour – I was not able to access any support to assist with being away from the abuse such as gyms, yoga class etc.
[The pandemic] intensified the impact of behaviours, made me more isolated, made the household more tense as couldn’t leave the house, more difficult to safety plan/ leave.
Leaving the relationship was made more difficult because of the pandemic. This was not only due to the increased psychological pressure their partner put them under, but also because victims and survivors had fewer employment and housing options available during the pandemic:
[Relationships] changed by taking away many options. Remote learning means I can’t look for work when lockdowns happen often. No predictability as to if we will or won’t be in lockdown make planning for anything very hard. Delay in earning enough money, means no options to move away from the toxic environment. He was home more often, so walking on eggshells and avoiding conflict happened so much more. Plus keep the peace with him home and keeping kids quiet or calm during remote learning simply leads to depression from fatigue and toxic stress.
Limited rental market made it difficult to access my own accommodation when I left relationship.
Some participants who had separated from their partner reported that they were more vulnerable to stalking because public places were quieter:
… fearful as there are less people out and about and thus more opportunities for him to approach and harm me, which he has.
Additionally, some found that it was easier for their ex-partner to discover their home address:
I was advised not to let him in my house or let him know where we lived, but that became impossible under COVID-19 and led to the incident where he harmed my daughter.
Restrictions improved safety
Although most women reported negative impacts of COVID-19 restrictions, some participants said they felt the introduction of rules about curtailing social contacts had a positive impact on their safety. Women who were not living with their abusive partner or had separated from them reported that the restrictions enabled them to avoid contact with the perpetrator.
Felt a little safer not having to see ex at kids’ sport etc.
I have been able to use lockdown as an excuse to spend time by myself and not visit my current boyfriend every weekend.
I felt safer as I didn’t need to go into my work premises where he (or his family/friends) could be … [and] I feel safer at home as I know I’m unlikely to be being watched.
Some also mentioned that they appreciated periods of isolation as it helped them to recover from experiences of abuse:
I’ve been very isolated but used the time to retreat from the world to heal and break trauma bonds.
The pandemic was the tipping point for action
A considerable number of participants said COVID-19-related isolation both increased their partner’s abuse and their own awareness of it.
It put our abuser over the top of us, where previously he went to work so we had some relief. His behaviour escalated and mine and my children’s anxiety, anger, etc. escalated immensely. It was the tipping point for my awakening as to what was going on and that all the behaviours and physical manifestations I was seeing in my kids was due to his behaviour.
For some, this was a catalyst for their decision to end the relationship:
Intensified the behaviours to extreme breaking point. For me this was a good thing. Things got so bad that drastic urgent action needed to be taken. I think I would have had a back-and-forth relationship for years otherwise as I am concerned that he would have been able to charm or threaten me back into the relationship. However, things got so bad as a result of constant contact and his control over me during lockdown that it was so much easier to leave than stay.
I have become less tolerant of his bad behaviour – have hated not being able to have time away from him and it is the impetus for breaking up now.
Conclusion
This section has outlined the experiences of abuse and violence, the sociodemographic characteristics associated with IPV and/or SV, health impacts and the effects of the COVID-19 pandemic. The next section explores help-seeking in detail.
2. Help-seeking experiences of victims and survivors of IPV and/or SV
This section integrates the findings from the surveys and interviews with victims and survivors regarding who sought help from social, health, specialist, justice, housing and community services, and how helpful those supports were found to be. This section also documents barriers to help-seeking. The interviews explored the women’s journeys of seeking support and safety and how their engagement with the service system unfolded over time. Both informal and formal services were included, ranging from all sectors that could come in contact with victims and survivors. It should be remembered that one third of participants were from Victoria, a state where there has been a marked degree of reform across the system in the last five years.
Sources of help and perceptions of helpfulness
Victim and survivor participants were more likely to have sought support from a friend/s (54.3%) or family member/s (38.3%) than from a formal support service. More victim and survivor participants than not (64.4%) had accessed one or more formal sources of support at some time in the past, and overall 57.1 per cent of these participants rated the formal support services as helpful or very helpful (Figure 12; Table 13). Health services (psychologists, counsellors, GPs, allied health and family counselling) were the most common type of formal support service accessed, with51.4 per cent of victim and survivor participants having accessed one or more health professionals. Health services were also the most likely type of support to be experienced as being helpful, with 65.6 per cent of service user participants reporting this. Housing and financial services were the least likely services to be accessed for support, with 15.1 per cent of victim and survivor participants ever having used those types of services. One in five (21.5%) participants did not seek any form of advice or support from services (Table 13).
Figure 12: Proportion of women who accessed support for lifetime IPV and/or SV and types of support they accessed (n=1,111)
Data table for the figure above:
| Type of support | Percentage |
|---|---|
| Family and friends | 64.4% |
| Health services (GP, counsellor) | 51.4% |
| RV specialist service | 40.1% |
| Justice services | 35.6% |
| Housing and financial services | 15.1% |
| Community: Other (work colleague, religious leader) | 11.3% |
Table 13: Proportion of women who have sought help for IPV and/or SV and perceived helpfulness
| Service/resource | Sought support (n=1,111) | Found support helpful n (%)a |
|---|---|---|
| Any source of help | 872 (78.5%) | 62%b |
| Family and friends (total) | 714 (64.4) | 64.3%c |
| Friend/s | 603 (54.3) | 399 (66.2) |
| Family members | 426 (38.3) | 284 (67.9) |
| Partner | 90 (8.1) | 53 (58.9) |
| Formal sources of support | 715 (64.4) | 59.6% |
| Health services (total) | 571 (51.4) | 65.6% |
| Psychologist or counsellor | 469 (42.2) | 354 (77.1) |
| General practitioner | 268 (24.1) | 182 (69.5) |
| Social worker (hospital/community health) | 125 (11.2) | 82 (66.1) |
| Family therapist | 56 (5) | 31 (56.4) |
| Nurse | 49 (4.4) | 27 (56.2) |
| Alcohol and/or drug worker | 41 (3.7) | 26 (68.4) |
| Specialist services (total) | 446 (40.1) | 65.6% |
| Domestic or family violence service | 332 (29.9) | 163 (63.7) |
| Telephone helpline (e.g. Lifeline, 1800 RESPECT) | 258 (23.2) | Missing |
| Sexual assault service | 108 (9.7) | 71 (67.6) |
| Justice services (total) | 396 (35.6) | 53.9% |
| Police | 346 (31.1) | 166 (48) |
| Legal service (e.g. solicitor or legal aid) | 214 (19.3) | 128 (59.8) |
| Housing and financial services (total) | 168 (15.1) | 52.6% |
| Financial service (e.g. Centrelink) | 138 (12.4) | 69 (50) |
| Housing service | 78 (7) | 43 (55.1) |
| Community – other (total) | 126 (11.3) | 53% |
| Work colleague or boss | 100 (9) | 65 (65) |
| Priest/minister/rabbi or any other religious person | 39 (3.5) | 16 (41) |
| Did not seek advice or support | 239 (21.5) | N/A |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to opt-in survey item about having spoken to someone about relationship issues, after experiencing violence and/or unwanted sexual encounters.
a Total number of participants who had accessed 1+ source of help (average proportion of all participants who found source of help helpful).
b Helpful/very helpful (median).
c Category % totals are an average of helpfulness across the sources of help within that category.
Help-seeking of women from diverse backgrounds
Some women participants were more or less likely than others to have accessed certain types of support (Table 14). Participants who were Aboriginal and Torres Strait Islander women, women who have difficulty managing on their available income, women aged 25 to 45 years, or those no longer living with their partner were all over-represented as users of informal and formal support compared with other women. Migrant women less often sought help from specialist services. Young women aged less than 25 years most often sought help from family and friends and less often from health and specialist services.
Table 14: Proportion of help-seeking by women from diverse backgrounds
| Participants | Family and friends | Health services | Specialist services | Justice services | Housing /financial services | Community – other | Did not seek advice or support n (%) |
|---|---|---|---|---|---|---|---|
| All participants (n=1,122) | 714 (64.3) | 571 (51.4) | 446 (40.1) | 396 (35.6) | 168 (15.1) | 126 (11.3) | 239 (21.5) |
Age (years; n=1,120)
| Participants | Family and friends | Health services | Specialist services | Justice services | Housing /financial services | Community – other | Did not seek advice or support n (%) |
|---|---|---|---|---|---|---|---|
| Up to 25 (n=104) | 93 (75) | 45 (36.3) | 26 (21) | 14 (11.3) | 4 (3.2) | 6 (4.8) | 27 (21.8) |
| 25–45 (n=516) | 376 (68.6) | 299 (54.6) | 253 (46.2) | 219 (40) | 102 (18.6) | 68 (12.4) | 94 (17.1) |
| > 45 years (n=418) | 244 (55.7) | 226 (51.6) | 166 (37.9) | 162 (37) | 62 (14.2) | 52 (11.9) | 118 (26.9) |
| Aboriginal and/or Torres Strait Islander (n=76) | 58 (66) | 44 (50.6) | 43 (49.4) | 35 (40.2) | 15 (17.2) | 6 (6.9) | 13 (14.9) |
| Migrant background (n=192) | 134 (61.7) | 110 (50.7) | 64 (29.5) | 65 (29.9) | 22 (10.1) | 29 (13.4) | 52 (24) |
| Same-sex partner (n=29) | 24 (68.6) | 18 (51.4) | 16 (45.7) | 11 (31.4) | 7 (20) | 4 (11.4) | 4 (11.4) |
| Lives in non-metropolitan location (n=297) | 199 (63.2) | 169 (53.6) | 142 (45.1) | 122 (38.7) | 53 (16.8) | 35 (11.1) | 60 (19.1) |
| Lives with disability (n=439) | 272 (62.5) | 242 (55.6) | 187 (43) | 163 (37.5) | 76 (17.5) | 48 (11) | 97 (22.3) |
| Attended school but finished prior to Year 12 (n=301) | 196 (60.1) | 159 (48.8) | 139 (42.6) | 121 (37.1) | 51 (15.6) | 26 (8) | 80 (24.5) |
| No university degree (n=552) | 369 (61.7) | 284 (47.5) | 236 (39.5) | 208 (34.8) | 89 (14.9) | 49 (8.2) | 128 (21.4) |
| No employment (n=401) | 258 (59.3) | 213 (49) | 165 (37.9) | 149 (34.2) | 74 (17) | 34 (7.8) | 115 (26.4) |
| Has difficulty managing on available income (n=584) | 401 (64.1) | 339 (54.1) | 286 (45.7) | 248 (39.6) | 122 (19.5) | 74 (11.8) | 130 (20.8) |
| Health Care Card holder (n=588) | 452 (66.3) | 330 (51.5) | 284 (44.3) | 246 (38.4) | 116 (18.1) | 54 (8.4) | 122 (19) |
| Not living with partner (n=580) | 422 (68.3) | 378 (61.2) | 296 (47.9) | 284 (45.9) | 122 (19.7) | 90 (14.6) | 109 (17.6) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
The proportion (%) in this table represents the proportion of overall demographic group who have accessed help by category.
In brief:
Help-seeking victim and survivor participants
Aboriginal and Torres Strait Islander women and women who had difficulty managing on their available income more often sought support from specialists and justice services; women not living with their partner more often sought support from health, housing and financial services.
Migrant and young women less often sought support from specialist, justice, housing and financial services.
Barriers to help-seeking
Various personal, information and service barriers were identified by victim and survivor participants as affecting their access to services (Table 15). The top three most cited barriers preventing help-seeking were as follows: shame (63.2%); lack of awareness about a service that could help (62.1%); and concerns about confidentiality (49.5%).
Table 15: Proportion of women who have experienced IPV and/or SV who identified barriers to professional help-seeking (n=1,108)
| Barriera | n (%) |
|---|---|
| Shame | 700 (63.2) |
| I feel too ashamed to talk to anyone | 590 (53.2) |
| I don’t want to talk to anyone about my partner’s behaviours, it is too personal | 454 (41.2) |
| Lack of awareness of services that could help | 688 (62.1) |
| I was uncertain who to see | 508 (46.1) |
| I decided not to seek care as not sure it would be helpful | 437 (39.7) |
| I don’t know of any service that might be able to help | 403 (36.6) |
| Confidentiality | 549 (49.5) |
| My friends or family will find out | 443 (40) |
| The professional will tell others | 359 (32.4) |
| Low priority/lack of time | 515 (46.4) |
| I had too many personal or family responsibilities to seek help | 403 (36.6) |
| I have no time to talk to someone about these things | 285 (25.7) |
| Communication | 485 (43.7) |
| The professional will not understand me | 485 (43.8) |
| Normalisation of violence | 394 (35.5) |
| My partner’s behaviour was a once-off. It won’t happen again | 299 (27.1) |
| My partner’s behaviours are just a normal part of relationships. I don’t believe there is any need to see a professional about them | 271 (24.5) |
| Access challenges | 274 (24.7) |
| I have no access to transport to see someone | 274 (24.7) |
| Cultural issues | 173 (15.7) |
| My culture or religion is a barrier for me seeking help | 173 (15.7) |
| Total participants who needed IPV and/or SV help, but were unable to get it | 533 (48.1) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; maximum missing n=9.
a Barrier defined as those elements that participants said were “Moderately important”/“Very important”.
Close to one in two (48.1%) participants said there had been a time when they needed help for relationship issues or sexual assault but could not get it. Of these 533 participants, the top two service barriers they most frequently encountered that prevented them getting help were difficulty understanding the professional/worker and lack of available appointments (Figure 13).
Figure 13: Proportion of women who experienced service barriers that prevented them from accessing help (n=533)
Data table for the figure above:
| Barriers | Percentage |
|---|---|
| Trouble understanding the terms used by professional | 71.9% |
| No appointments | 54.8% |
| Not taking new patients | 53.7% |
| No private health insurance | 51.0% |
| Limited opening hours | 50.7% |
| Cost of services | 48.6% |
| Concerns regarding confidentiality | 47.3% |
| Waiting time too long | 45.8% |
| No services available in the area at the time needed | 42.9% |
| Lack of awareness of available services | 40.5% |
Please note: 566 participants were omitted from this analysis because they had never been in the situation of needing help and being unable to get it.
The next section utilises the interview data to describe women’s journeys to seeking help.
Journeys to seeking help and support
To further illustrate the victim and survivor participants’ help-seeking journeys, we present the interview findings from the 30 women victims and survivors, which offer a deeper understanding of the survey responses.
Demographic profile of interview participants
Participants’ ages spanned between 19 and 62 years, with a median age of 38.5 years, and most participants (24) were aged between 20 and 59 (Table 16). They were living across Australia, with 24 of them living in the eastern states. Over a third (11 participants) were born overseas, with six born in countries in Asia (India, China, Hong Kong, Japan), and the remainder from the United Kingdom or countries in Europe or South America (Ecuador, Israel, United Kingdom, Greece). Two were Aboriginal. The majority were employed (21) and tertiary-educated (28). Half (14) were living with a disability or chronic illness that limited them from daily activities, including employment. Most had experienced IPV and/or SV from a male perpetrator while in a heterosexualrelationship, while three women had experienced abuse in a same-sex relationship. Two thirds (20) had children with the partner who used IPV. All were separated from the perpetrator at the time of the interview. Not all women responded to the survey sections where they identified the types of IPV and/or SV they had experienced, and the interview discussions did not focus on exploring the details of the IPV and/or SV. However, more than a third answered on the survey that they had experienced forms of physical and/or sexual violence from a partner.
Table 16: Interview participant demographic details (n=30)
Age (years)
| Age | n |
|---|---|
| 15–19 | 2 |
| 20–29 | 6 |
| 30–39 | 8 |
| 40–49 | 6 |
| 50–59 | 6 |
| 60–69 | 2 |
State/territory of residence
| Age | n |
|---|---|
| Australian Capital Territory | 2 |
| New South Wales | 4 |
| Northern Territory | 1 |
| Queensland | 7 |
| South Australia | 4 |
| Tasmania | 4 |
| Victoria | 7 |
| Western Australia | 1 |
Central theme: Carrying the burden alone
We first discuss the overall themes in the women’s stories of navigating the service system to address their partners’ abuse. We then explore how the women’s help-seeking unfolded over time.
Our analysis of the women’s narratives about their help-seeking journeys led to an interpretation of the overall experience as being one of “carrying the burden alone”. This was exemplified in a number of ways. In reflecting on their early experiences of abuse in their relationships, interview participants spoke of feeling responsible for their partner’s behaviour. For example, one woman said her partner had brainwashed her to believe his abuse of her was “my problem and my responsibility to fix”. In participants’ narratives of engaging with the service system, the main theme was that the responses they received had only reinforced that perception. Women felt that the onus was on them to manage the perpetrator’s behaviour and to keep themselves and their children safe. Although participants offered examples of responses that had been helpful at different times, they suggested that, overall, the service system had provided only short-termassistance, little protection, and minimal financial, material and emotional support. They felt services were under-resourced, and professionals were often disinclined or simply unable to engage meaningfully with their individual experiences. This perception was reflected in participants’ comments about feeling like “a number”, “just another victim” or that they “didn’t really matter at all”. They felt they were expected to curtail their freedoms to avoid the abuse and to manage the impacts on their own and their children’s mental health. Meanwhile, the perpetrator was subjected to little scrutiny and few restrictions, and in many cases was only emboldened by his or her contact with the service system.
To illustrate this central theme, we present three brief narratives of women’s journeys through the service system. The three narratives presented below illustrate women’s experiences of “carrying the burden alone”. Each of the women expressed that they felt the service system put the onus on them to manage the perpetrator’s abuse and to cope with its consequences. Fiona’s story highlights how a lack of intervention and information sharing by service providers leaves women feeling they are responsible for addressing the perpetrator’s behaviour on their own. Nella’s story speaks to the sense of loneliness women can feel when they are unable to trust services to offer effective support or to understand the dynamics of their individual experiences. Indeed, for many Aboriginal and Strait Islander women such as Nella, services can be not only unhelpful, but harmful. In Julia’s narrative, we can see how exhausting it is for women to have to constantly“go into battle” to protect themselves and their children, with little support to back them up.
“I’m the only one calling him out”: Fiona
Fiona said she noticed her partner’s aggressive outbursts were becoming more frequent, but she was constantly in “fight or flight mode” so it was hard to think clearly about what was going on. She spoke about her partner’s “anger issues” to their family’s GP, who referred him to a support service. However, she discovered her partner only attended one session then refused to continue. Fiona was upset that no one had informed her of this, and no one followed up with her partner:
The GP knew stuff was happening … but when you’re dealing with someone who acts like this in a family environment, you’re just kind of letting that person run wild with no follow-through. So, then all the onus is on me.
Fiona became particularly concerned about how her partner’s aggression was affecting their children. She confided her concerns to a supportive friend, who encouraged her to contact a DV hotline. The hotline helped by validating her concerns and providing practical tips, but Fiona said: “The support thereafter was a bit lacking. I just feel that they’ve not got the time. They’re just so under-resourced.”
The violence continued and there were occasions when Fiona had to flee the house with her children. Finally, she went to the police, which was a turning point in her leaving her partner. They arrested him and applied for a family violence order, so he wasn’t allowed back to their home. However, Fiona described the police’s approach to communicating with her as “very hands off”. They charged her partner with assault but failed to inform her they were doing so. While Fiona was ultimately glad charges had been laid, the police appeared to give little consideration to the ramifications for her safety; as she said, “any impact it [the assault charge] has on him, it goes back on me”.
Fiona’s partner breached the court order several times, with mixed responses from police. She found the criminal prosecution process extremely confusing: “You’ve got so many questions and concerns … but they’re already too busy onto the next [case].” She also attended family mediation with her partner to develop a parenting agreement. However, this was a frustrating experience. Even though the mediators privately told her they had noticed her partner’s manipulative behaviour, they did not directly confront him about it:
[I wish they would] tell him so that he knows, because he’s just walked out of here thinking that he’s still king pin and you’ve believed him … I’m the only one that calls him out on his behaviour … Nobody’s actually overseeing how that interaction is going and how that person’s behaving.
Fiona said she would like to understand what her legal and financial entitlements are but keeps “getting shipped off” to different services. She also wants to find a counsellor for emotional support, but in between trying to work, supporting her children and selling the home she shared with her partner, she has had to put her own needs “on the back burner”.
You feel alone”: Nella
Nella identified as Aboriginal and said her family had suffered from intergenerational trauma. As a child, she was removed and put into foster care. She said: “If we were a British family I probably never would have been taken away.” As a teenager, she became involved with a partner who was abusive. She sought help from a mental health hotline as she had not slept for days. However, she said: “When you’re under 18, if you talk to anyone about anything even vaguely negative, they call the cops.” The hotline reported her situation to the police, who arrived at her school and asked “invasive” questions. Based on prior experiences, Nella said she knew not to trust the police:
When you’re not a child of the chalk … that’s not a good idea to deal with cops … I said to them, “I’m not saying anything. I don’t talk to police. I’m not the one who committed a crime here so leave me alone.”
The risk of police involvement meant she felt unable to seek assistance until she was over the age of 18. Nella said, “when you can’t tell anyone you feel alone”. Her new partner and a friend were supportive, but she didn’t want to burden them by sharing the details of her abuse. Eventually, suffering nightmares and struggling to cope, she went to a youth mental health service. However, the counsellor seemed to hold her responsible for what had happened, suggesting she should “fight back … not get in the situation in the first place … not trust people … trust different people”. Nella said, “None of those solutions would have helped because I was already putting every single measure you could in place.”
The only way Nella was able to escape the abuse was to move cities and change her name. Now that she is over 18 and has found employment, she has been able to afford to pay for a psychologist to address the PTSD symptoms she experiences.
“Wearing the burden of being careful”: Julia
Julia’s partner was violent from early in their marriage. After he began directing his abuse at their children, she managed to leave him. She found a new home and kept the address from her ex-partner. Her children did not want to see their father because of his abuse. To protect them, Julia fought to obtain a family court order to stop her children being mandated to have contact with their father.
However, Julia said that even though the family court recognised her ex-partner’s abuse, there was no coordination or follow-through from the service system; instead, she had to “go and pick myself up … and tell my story again”. For example, she had difficulties getting local police to recognise the family court orders. Her ex-partner also began “playing games” with child support, which was another problem that she had to figure out how to address.
Julia said she believes her ex-partner likes to play games like “a cat and mouse. He is just going to continue to keep me on that edge” and every day it feels like she is “going into battle”. However, she can’t risk applying for a domestic violence protection order because she will need to provide her address, and she believes her ex-partner will not be deterred by another “piece of paper”. In the past she has had to push the police to act, but recently, they have recognised the risk she faces. The police have told her: “This is serious, you’re going to have to change, don’t have any patterns, don’t be on social media, don’t do anything.” But Julia said constantly having to be wary and restrict her freedoms has “ruined my life … why am I wearing the burden of being careful?” She can only leave the house at times of the day when her ex-partner is likely to be occupied, and she is unable to use social media, which has damaged herjob prospects and connections with others.
Julia has also faced difficulties getting medical and other services to understand her safety and privacy needs. She has sought counselling to help manage her constant anxiety, but the psychologist has told her that her symptoms can’t properly be treated while she remains unsafe.
Key responses at different stages in women’s help-seeking
Based on our analysis of the interview themes and the timelines we created from the interview data with 30 victim and survivor participants, we identified five key stages of help-seeking: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; establishing independence and safety; and addressing impacts and making sense. These stages reflected particular help-seeking needs or goals at different times. Each stage was triggered by critical turning points or changes in how women understood and experienced the abuse. Figure 14 provides a visual illustration of the different stages of participants’ help-seeking journeys and the turning points or changes in their experiences or understandings of the abuse at each stage.
It is important to note that while the stages reflected common needs and turning points across participants’ timelines of seeking help, not every participant passed through each stage in order (or at all). Additionally, there were often overlaps and loops back between the stages. For example, many women went through the stages of trying to get out of the relationship and re-establishing their independence and safety, but then returned to the relationship and to the stages of maintaining hope and/or assessing options. All of the participants we interviewed had eventually left the relationship, but for some it had taken many years. Despite ending the relationship, many were still subjected to ongoing abuse, threats and stalking by their ex-partner. Additionally, across every stage of their journeys, women prioritised supporting their children (i.e. not only in the addressing impacts and making sense stage). However, many said that once they and theirchildren had become safer (often after leaving the perpetrator), they began to seek out formal counselling and support programs for their children to address the trauma of the IPV and/or SV.
Figure 14: Key stages and turning points in victims’ and survivors’ help-seeking journeys
Text version of the figure above:
- Maintaining hope and fixing problems
- Fixing self
- Fixing partner
- Fixing relationship
- Assessing options and seeking solutions
- Understanding
- Weighing up choices
- Trying to change partner
- Seeking protection
- Getting out
- Planning and breaking away
- Re-establishing independence and safety
- Securing a base
- Establishing financial security
- Settling parenting arrangements
- Holding perpetrator to account
- Addressing impacts and making sense
- Understanding why
- Processing impacts
- Supporting children
- Connecting with others
Before step 1 to step 1:
- Being controlled and isolated
Between steps 1 and 2:
- Recognising IPV
- Others identifying IPV
Between steps 2 and 3:
- IPV escalating or affecting children
- Realising partner won’t change
- Others identifying IPV
Between steps 3 and 4:
- Partner promising to change
- Enduring stalking and threats
Between steps 4 and 5:
- Being abused via legal systems and child contact
- Becoming safer
In the following discussion, we explore the five stages of help-seeking in detail. We also draw on narrative and thematic data to identify helpful responses in each stage. As explained in the previous section, the women largely felt the service system had let them down and left them carrying the burden of managing their partner’s/ex-partner’s behaviour and coping with its impacts. However, participants also described key moments during their help-seeking journey when service providers responded in a way that made them feel supported and less alone. We provide examples of positive or pivotal responses at each stage of help-seeking, as well as examples of responses that were inadequate in meeting women’s needs. We use participant quotes to illustrate. For longer quotes we provide a participant number to indicate which interview participant is being quoted.
Stage 1:
Maintaining hope and fixing problems
In describing their early experiences of engaging with others about the abuse, many women spoke of unawareness and misdirected help-seeking. They recalled noticing manipulation, isolation and controlling behaviour from their partner, but did not fully acknowledge it as abusive and hoped the relationship would continue. When women were subjected to psychological or sexual forms of abuse, it was particularly difficult for them to recognise the behaviour as unacceptable.
In relation to their early help-seeking, women described approaching their family and friends, GPs, health professionals, psychologists, psychiatrists and relationship counsellors. Their aim was to maintain the relationship and to try to fix what they perceived to be causing the problem: their own mental health issues, their partner’s mental health or drug and alcohol use, or the communication in the relationship. For instance, one said: “I was like, my partner is an addict and I need to help them” (Participant 9). Another said: “I very much thought … he’s had a mental health crisis. Once he gets help for that, everything will be all right” (Participant 22).
During this stage of help-seeking, women said the following responses were helpful or pivotal in shifting their understanding of their situation.
“Someone cares”: Inquiring about wellbeing
For some women, having a professional take the time to directly ask about their emotional wellbeing and safety in their relationship was a significant turning point; it gave them an opportunity to open up about their experiences, and it demonstrated that someone else cared about what was happening to them. This was the case for one woman (Participant 6). She married her husband in India, but he became physically violent when they came to live with his family in Australia. She said in her culture it is unacceptable to leave a marriage, so all she felt she could do was “pamper” him in the hope he would change. His aggression escalated when their child was born. A neighbour became concerned and called the police. The police took her to stay with some extended family members but did not refer her to any DV support services.
It was only when the participant’s maternal and child health nurse directly asked her what was going on in her relationship that she felt able to disclose. The nurse had witnessed signs of abuse and had purposely followed up by making a private appointment to see her:
When [the nurse] said to me that “Are you okay and are you free and safe?” … I burst into tears, and I told her the whole story … She said, “When you came to me after … [your baby’s] health check, I knew something is wrong. I saw your husband was treating you very badly in front of me … I didn’t talk to you at that time because your husband was there with you … But I was just trying …to contact you if you are okay” … I was so happy, finally there is someone who cares about me, who cares about my daughter. (Participant 6)
“It’s not you”: Identifying the abuse
Almost a third of the women reported that an interaction with a service provider had been pivotal in transforming their perspective on their relationship. For instance, one woman (Participant 1) said her partner’s psychological abuse worsened when they moved to a regional property, as there was no one around to hear it. However, at the time, her partner manipulated her to think her own depression was the cause of his behaviour. She suggested the responses of a GP helped lift the burden of self-blame and led her to begin seeking help to end the abuse:
I thought there was something wrong with me, [I was] depressed … [My partner] keeps telling me I was psychotic … So, it felt like a bit of relief talking to the doctor because she said “Oh no, no, no. This is gaslighting. It’s not you. It’s perfectly normal to feel upset and depressed in this situation.” (Participant 1)
However, other women explained that their initial contacts with professionals had only reinforced the notion that they were responsible for their partner’s behaviour or the problems in their relationship. One said:
I was still seeing … his aggression as something that I was doing wrong that I could work on myself and change. [But] there was no suggestion [from the counsellor] that what I was facing wasn’t okay. She was giving me strategies … that I could try … I would have been so much better equipped earlier on if I had of understood that these behaviours were not okay, and they were not something that I could control … that would have made a significant difference. (Participant 3)
In some cases, health professionals had diagnosed women with a mental health disorder rather than exploring underlying causes of their symptoms:
[I] just ended up on a bunch of medication and going down this line of people thinking I had bipolar. So, I was like, this isn’t helping with me feeling that it’s not all in my head and not all my fault. (Participant 9)
A focus on psychopathology was particularly problematic for women who had already been diagnosed with a mental illness. For example, one said:
I actually never felt listened to because it was always about the schizophrenia. So, any concerns I raised were dismissed as symptoms of my mental disorder … It maintained the idea that I was the problem. (Participant 29)
Stage 2:
Assessing options and seeking solutions
Once each of the women recognised that their partner’s behaviour was unacceptable, their focus was understanding what was happening and how to address it. During this stage, the women sought advice and assistance from mental health services, counsellors, health professionals, domestic violence and sexual assault services, and their family and friends. Several also sought police protection during incidents of aggression from their partner or contacted police for advice. Some engaged with men’s mental health services and behaviour change programs in the hope that they could help to stop their partner’s abuse.
However, disclosing the abuse to others was not an easy thing and many said they were extremely wary about doing so. Some struggled to find a private moment to talk freely, particularly when their partner constantly monitored their communication with others. Several said they felt ashamed and feared being judged. For example, one said: “I was humiliated that I was in this relationship where I was being controlled by somebody else … I felt embarrassed to have to tell people” (Participant 8). Being in a same-sex relationship added another layer of concern for some women: “There’s already enough criticism of [same-sex relationships]. Then you don’t want to say, ‘Oh, by the way, I’m actually in an abusive relationship with my same-sex partner’” (Participant 9).
Women also feared that disclosing their mistreatment could result in unwanted interventions by others; as one participant said: “I was afraid … that someone would [be] silly enough to say something to him, which has happened, and it would make it worse for us” (Participant 10). A major concern for those with children was that they would be reported to child protection. For Aboriginal women, racial discrimination made this a significant risk:
[Being from] an Aboriginal family, I was always afraid that even if I was listened to, I would be seen as the problem and my children would be removed from my care. (Participant 29)
Yet despite these barriers, each of the women had managed to disclose the abuse to formal service providers, hoping that they could help them to explore their options and potential solutions. In some cases, confiding with others about the abuse was a positive or transformative experience for the women, while in other cases it only deterred them from further help-seeking.
“I’m not going to judge you”: Listening and showing empathy
In deciding whether to disclose and how much to share with professionals, women looked for signs that they could trust them to provide an understanding response. For example, one participant said that her therapist responded to her disclosure “in a way that says ‘It’s okay to bring that here. I’m not going to judge you.’” She reflected that it was critical that service providers demonstrated they cared and were prepared to listen:
It’s about creating that sense of openness to people’s experiences … Even [if services had] a sticker that said: “If you’re not safe, you can tell me.” Something like that [would help to facilitate disclosure]. (Participant 9)
Participants emphasised that what they needed at the point of disclosure was not anything complex – it was simply to be believed and listened to. For instance, one woman said the supportive response from her local police made a big difference:
Just that hand on the shoulder and saying, “We understand how awful this is and we believe that what you say occurred did occur.” Just small things, just “we believe you” and listen to you. (Participant 4)
They greatly valued service providers showing concern for their wellbeing, asking questions, and giving them time to talk. For example, one spoke to a pelvic floor psychologist about the sexual assaults by her partner:
[She] just listened, and she believed me … she didn’t question it happening, she just asked more questions to find out more. I think that was probably the biggest thing, is feeling heard. (Participant 17)
“Take me seriously”: Validating concerns and identifying risks
Having their concerns validated was critical, considering that, as one woman said, “When you’ve been controlled and manipulated, you doubt your own feelings” (Participant 1). While women appreciated validation from their family and friends, the perspective of a professional with expertise in the area was a major turning point in recognising that the problem was legitimate and important to address. This was reflected in the following comments from two participants:
Having it almost … justified by a professional [meant] … I felt like I wasn’t crazy, like I [hadn’t made] all of this stuff up in my head. (Participant 17)
[The police officer] took all the details, she listened, and she took me seriously. She said, “You’re at moderate risk” … I came away thinking, well jeez, if the police take it that seriously then it must be a mess … They see this every day, so they know what they’re talking about. (Participant 28)
Having an outsider tell them that they had noticed the abuse was also valuable in making women feel they were not the only person who saw it. One woman said it made a “huge” difference when she was contacted by the facilitator of the men’s behaviour change program her partner was attending:
[The facilitator] said “I’m concerned about you because I’m not seeing changes in [your partner] that I would have liked at this point” … Our mutual friends don’t get it because they’ve never seen him like that. I’m the only one. So, I appreciated that … There was a validation there … It was huge and at the end of that very short conversation, I thought, ooh, I might be ready [to leave]. (Participant 20)
However, women also received responses that discouraged them from further help-seeking. The terms used to describe abuse by an intimate partner were deterrents for some women. Several said they had been uncertain about whether they could access domestic violence or sexual assault services because their experiences of violence or abuse did not fit common stereotypes. For example, one young woman who was sexually assaulted by her partner said:
The reason why I didn’t reach out to any [domestic violence or sexual assault] services like that [was] because I wasn’t, quotation marks, “raped” … [and the term] domestic violence I’ve never … appl[ied] to my situation … [The term “domestic violence” is] quite mature … you often think of it being like a 40-year-old woman who’s been in a relationship for 20 years. (Participant 17)
Some women who were experiencing non-physical forms of abuse did contact domestic violence services; however, they said that the questions asked during risk assessment processes made them feel that their concerns were less valid. For example, one said:
[The DV counsellor asked me] “Do you feel scared?” – “Yes.” “Has he ever hit you?” – “No.” There would be like a little, “Okay, okay”, like I could see in their face or their body language, the more serious questions around sexual assault or physical violence. “Okay, we don’t have that situation here. I can just downgrade my concern a little bit.” Which didn’t help when I was questioning if [the abuse] was real. (Participant 20)
“We’ll go as fast or slow as you need”: Exploring options without pressure
A valuable response from service providers during this stage was providing information and exploring options without expecting women to act immediately. For example, one woman contacted a local police domestic violence liaison officer when she was considering reporting her partner’s sexual and physical assaults against her. She found her initial contacts with them “really supportive”:
[The officer] said “Look, there’s no pressure … we’ll go as fast or as slow as you need to” … She gave me lots of things to read … She was like, “Go online and have a look at this. There’s a … form that you can get” – she gave me options, and then was, like, “Ring back anytime.” (Participant 15)
In contrast, women frequently described directive advice as unhelpful, particularly when they were not emotionally ready or lacked the resources needed to act on the advice. For instance, one felt the well-intended approach she received from her friends and a DV service was not helpful because she was not ready to hear it:
[The domestic violence counsellor] said, “Right, let’s make a safety plan, I want you to have a packed bag in your car, I want you to do this, and this, and this” and I was like “What? I just need help figuring out what I’m going to do to get strong” … People saying things to me directly about “This is bad, and you need to get out” didn’t help at all … The message was probably okay but there wasn’t support to back it up. (Participant 20)
Another concern was a lack of emphasis on encouraging perpetrators to change their behaviour. Some women felt that the service system was predicated on an assumption that the best solution was the victim immediately ending the relationship with the perpetrator, but this was not practical in the long-term, particularly when children were involved. For example, one woman (Participant 19) said that she felt pressured by police and services to sever all contact with her partner. What she felt would be a better long-term solution for her children and herself was for her partner to be mandated to attend a residential program for his drug use and to have a dedicated male case worker who could hold him accountable for changing his behaviour. She was frustrated that during a protection order hearing, a magistrate denied her request to order her partner to attend a men’s behaviour change program. She reflected that in the end, separating from her partner hadonly caused her financial hardship and she and her children still had maintained contact with him because he was her children’s father. She said:
There’s so much emphasis on “Kick him out, get an IVO [intervention order], break up your family”, whereas looking back now I wish the support had been, “We’re going to take him out … he needs to go to rehab, he needs to get on top of this” … You’ve got to stop and think about the practicalities … [There’s] nothing that’s viable for a single parent … there’s not that support, to make sure that long term … there’s going to be genuine skills learned or other people helping hold people accountable for their behaviour … [So] it’s just going to keep happening … [And kicking him out and locking him up] doesn’t work for kids who … legally, are told they have to have access with the perpetrator … So, they’re leaving kids to just have to deal [with it]. (Participant 19)
“I would not have made it out alive”: Intervening when necessary
Some participants said they had needed service providers to step in to protect them, even when intervention was not what they had wanted at the time. This was particularly the case when women were in great danger but powerless to escape on their own, or when the perpetrator was manipulating them into making decisions that were not in their interests. For instance, one woman (Participant 30) said her partner had “brainwashed” her to stay in the relationship by promising he would change. She had spoken to a counsellor from a domestic violence service, and they supported her choice to stay. However, on reflection, she said she had needed the counsellor to “be a little harder” on her and help “extract” her from the hold her partner had over her. In the end, what had been helpful was the firm response of a police officer:
The first thing [my partner] wanted me to do, obviously, was to drop the intervention order. [But the police officer] just held his ground. He goes, “No. No, you’re not withdrawing them. What about if we change it to this, this and this?” … At the end of the day … I needed … somebody to question me on this request to withdraw charges … he wasn’t bullying or anything. He was just like a strong dad. (Participant 30)
Women suggested that when professionals stepped in, it was vital was that they had expertise in IPV and/or SV; took women’s concerns seriously; and provided timely responses, follow-up support and clear information. For example, one (Participant 10) said she was unable to disclose her partner’s violence because he constantly monitored her through the cameras he set up in their home. She feared that if police became involved, they would remove her children, or her partner would act on his threats to kill her. However, eventually the police intervened after a family member called a domestic violence hotline about her situation, and the hotline contacted the police. This ended up being a turning point that helped her escape. What made the difference was that the officers were skilled in DFV interventions, took her fears seriously and responded swiftly:
The police turned up on my doorstep to do a welfare check … Fortunately, the two officers were also child protection trained and they were fantastic. They separated us both … I was advised that they would have to tell [my partner] why they were there. I’m like … “I’m terrified … if you leave us here, when you leave, I am dead.” I honestly do not believe that I would have made it out alive if they had not taken us … He was arrested, taken immediately to the police station … We had enough time to gather a couple of things … then we were in the police station overnight … and then straight into safe accommodation. (Participant 10)
However, for other women, critical interventions were followed by poor communication or tardy or unsupportive responses from police, prosecutors and the courts. This only amplified their distress. For example, one woman (Participant 22) said the police took out a protection order and charged her partner with assault, even though she asked them not to. Although this improved her immediate safety, the lengthy delays, lack of agency, and humiliating and intrusive questioning she experienced in the criminal courts deeply traumatised her. She said of the criminal justice response: “It’s good that it’s in place, but … the amount of time it takes for these things to happen and the way the victims are treated needs to change.”
Stage 3: Getting out
When their partner’s abuse escalated or when women realised their partner was not going to change or that the abuse was affecting their children, women made the decision to leave. All of the women in the study had ultimately ended the relationship with their abusive partner, but for many it had been an extremely difficult process and had taken several attempts to do so. To seek help with getting out, women’s main service contacts were domestic violence services, police, Centrelink, housing and welfare organisations. They also relied on their friends and family for practical help with accommodation, childcare and financial assistance.
“Here are the steps you need to take”: Help to plan a safe escape
Once women had decided to end the relationship, they needed to figure out how to safely get away from their abusive partner, how to keep their children with them, where they could stay and how they could survive financially. However, many said they struggled to think clearly and to plan how to get out while coping with regular abuse. As one said: “[I needed] just somebody sitting down and practically talking through, here are the steps that you need to take to move, because you’re so exhausted … so overwhelmed” (Participant 20).
Domestic violence hotlines and services were frequently a source of valuable advice during this time, including practical tips for how to escape in an emergency:
[The DV service] made sure that I had plans and things in place … They helped me to understand that this person could be quite dangerous because his physical abuse was escalating … So, I did what I could and had things ready to grab if I had to get out quickly and park[ed] the car a certain way, so it was easy to get out. (Participant 1)
Some also found police helpful when they took their fears seriously and were ready to protect them:
I was encouraged … to give the details to the police and let them know what was happening. So should he escalate, they apparently can put an alert on the address. So, if they get a call from that address, it’s a priority, so I did that. (Participant 28)
“I’ve got nowhere to go”: Providing income and a secure place to stay
Although women found that information and safety planning advice was relatively easy to obtain, it was more challenging to find material assistance to leave, including a safe place to stay and a means to support themselves. Many were financially dependent on their partner, often because the partner had stopped them from working, controlled their finances, depleted their savings or accrued debts in their name.
When women were facing immediate danger, they found services were able to respond to their practical needs to help them escape. For instance, one woman (Participant 6) felt very vulnerable as she had little financial or family support in Australia and was profoundly grateful that refuge workers were able to provide her with short-term accommodation. They also assisted her to secure a rental property, legal advice, employment and childcare, and provided money to buy furniture when she found a house to rent. She said when she first contacted them:
[The DV counsellor] interviewed me … I said “I’ve got nowhere to go and I’ve got a little child … I’ve got no money, I’ve got nothing” … She assured me that we will be sending you a taxi [to a hotel] … When I got [there] I feel like, “Thank God I am safe” … They found a refuge for me … They gave me proper shelter … I had to pay nothing to them. There was so much good support … everything starts falling into a good place. (Participant 6)
However, many of the women who wanted to leave found that unless they were facing an imminent threat of physical harm, services were unable to offer any tangible help. For instance, one said:
I felt very alone and with a lack of support to actually get out of that situation. Just like, the DV [service] … counselled me for a bit on the phone and said, “This is what we can do. If you feel that you’re in immediate danger, we can remove you or … put you into a motel and then help you find a place” … [But] because I didn’t feel that I was in that situation, I was just left to “You need to leave, good luck.” (Participant 28)
Like other women, she could not afford private rental as a single parent and found there was a very long waiting list for public housing. The only advice services could offer her was to stay with family or friends, but she could not do so as no one she knew had room in their house to accommodate her and her children.
The lack of housing and a financial safety net meant many of the women and their children were trapped with their abuser for a prolonged period. A few were able to remain in their home and to obtain a protection order to force their partner to leave. Yet they found it difficult to obtain financial assistance to get the locks changed or to install security lights and cameras, which meant they could not feel safe.
Stage 4:
Re-establishing independence and safety
After separating from the perpetrator, most women had extensive engagement with various services and the legal system in order to establish a safe place to live and an independent income and to sort out parenting and property arrangements. The services they had contact with at this stage included DV services, Centrelink, welfare and housing services, financial counselling, police, child protection, criminal and family courts, mental health services, and child psychologists, as well as childcare and schools.
“Someone to bat for you”: Help navigating the service system
All of the participants described the service and legal system as disjointed and overwhelmingly confusing to navigate, particularly when they were already stressed and exhausted. They described feeling like they were on a “merry go round”, “running around in circles”, ‘or “flailing around with no clue”. For example, one said:
Nobody seems to know what anyone else can offer, it’s a guess. You get referred here, there, and everywhere. In the beginning you’re on so many phone calls, you can’t remember who you were talking to, where they’re from. You go through the same story hundreds of times, and you just get completely lost. You can’t remember any of it. Then with the practical assistance you get is very little to none. This person will go, “Oh, no we can’t help you with that, but here, try this person”, and they’ll go, “Oh, no, we can’t do that, try this person”, and then you get referred back to where you started at. (Participant 10)
It was difficult having to repeatedly disclose their abuse to different service providers because women felt it exposed them to being judged or disbelieved. One woman said:
It’s just confronting constantly having to tell the story over and over again … Vulnerability and constantly having to pour your heart out to people hoping that they were understanding your situation. (Participant 28)
In a few cases, participants found a professional who helped to lift the burden of working out how to access what they needed. One woman eventually found assistance from a worker from a Victorian DV service that was recently established to provide a coordinated response. She said this was invaluable, though it took seven months from when police referred her there to when the worker finally was able to contact her:
[The worker] was very supportive … She said, “Do financial counselling” [and] she got me in. She rang me constantly to see how I was doing and [to] just be an ear … It just felt like someone cared. (Participant 1)
For another woman, having a DV service guide her through the process of accessing legal protection was a turning point in becoming safer:
He’d taken the children and disappeared … I called [the DV service] highly distraught, and they were terrific. It was because of what they did in the moment of crisis … where they helped me to go to the police station, they supported me with the police, and the police took an application out on my behalf for an intervention order – that was life changing for me. (Participant 5)
However, like many others, she found longer-term support beyond a crisis response was not on offer. Instead, participants repeatedly described being left on their own to navigate a complex and seemingly uncaring system. Consequently, a major need at this stage of help-seeking was for a dedicated case worker who could advocate for women and guide them through the service system. The following examples from three participants illustrate this theme:
What would have really helped is someone just stepping up and saying that “We hear you; we see through how you’re presenting and understand why you’re being like you are.” Having that support person in place to go with you to Centrelink, housing, go with you into court. Just to bat for you. (Participant 4)
You need some sort of integrating liaison officer who’s assigned to you or something like that who can help do some of that coordination work and make sure you’re on track with things. (Participant 12)
If I had somebody who can be your advocate … and can walk you through the process. [Because] my head was in such a fog … A case worker of some description, who can go through things with you … rather than just being left on your own. (Participant 10)
“Tangible things”: Material and financial support
Many women struggled to afford basic items they and their children needed to survive, such as food, clothing, housing, transport and childcare. As the following quotes from two participants illustrate, a few managed to secure some financial help, but this was only short-term:
I actually found [child protection] to be really good … They assisted me to get my daughter into kindy [kindergarten], because I hadn’t been able to afford that previously because of his spending habits, but they wrote me a support letter so that I could get some kindy coverage at no cost for [a] period of time. (Participant 10)
[The domestic violence worker] was able to pay one of my electricity bills … [and] to give me some vouchers … so that I could actually go and buy myself a doona … and a few things that I needed. That was so helpful. Those tangible helpful things are lifesavers when you’re teetering. (Participant 1)
Yet, most discovered there was no consistent financial safety net to support them to regain their independence. One said:
As for financial help, there is zero out there. If you qualify and you get it done in time, there’s a $500 Centrelink emergency payment …[but] there’s nothing else out there really … [You can get a Salvos voucher] every couple of months if you’re lucky and if you can get through to them in the first place, because no one’s answering their phone anymore. So, you struggle. Can I feed my kid today? She needs some new clothes, what the hell do I do? … We’re going to stay with a family member temporarily, but that’s going to end and then where do we go after that? (Participant 10)
Seeing through the abuser’s tactics: Recognising and stopping the abuse
Most of the women (24 participants) were harassed or stalked by their ex-partner after they separated. Two thirds of those participants had contact with the police and the courts, often because they needed protection from ongoing threats and abuse. Several sought to hold the perpetrator accountable for previous violence or assaults through the criminal justice system. Women also sought to settle property and to establish safe parenting arrangements via the family courts.
Women occasionally described good responses from the criminal justice system. For example, one described the police as “fantastic” in explaining their processes and checking in on her wellbeing. In her case, firm legal action and incarceration had temporarily stopped the violence:
He is facing at least 22 different criminal charges related to the DV. He was arrested … and denied bail this time, thank God. [It] just was such a relief … To know that I can go for a walk to the park with my daughter and not have to worry about him pulling up on the side of road and trying to grab us or something. (Participant 11)
Another woman said it had been profoundly validating when a magistrate saw through her ex-partner’s tactics and took action to stop them. She believed what made the difference was that the magistrate and court professionals had been trained in recognising non-physical forms of IPV:
[The court staff are] very aware of all the tactics and the ploys … [The magistrate has] actually seen right through him. She’s highlighted exactly his behaviours. He was arrogant, rude, he spoke over the top … I felt vindicated by the judgment … Seeing that other people can see what I’m dealing with and they’re doing their best to protect me … that’s what’s given me a lot of hope. (Participant 1)
Yet on many occasions, rather than ending women’s experiences of abuse, the legal system had ignored or enabled them. A consistent theme was that police and courts did not recognise coercive controlling behaviour and non-physical forms of IPV. For example, one woman (Participant 13) believed getting legal protection would have been easier if there had been a “physical reason” for it. Her husband’s abuse was not physical; she said it was “not one big thing [but] lots and lots of little things”. He was highly controlling, intimidating and deliberately turned their child and their friends against her. However, she was told by the police that she was unlikely to get a protection order because proving the abuse in the courts would be “almost impossible”. The fact that she had not applied for a protection order was then used against her in the family court to imply that she had been lying about the abuse.
Several said they felt like they were being blamed for the abuse. One woman said the police asked her “What did you do? Have you been drinking?” (Participant 27) Another said police told her to withdraw sexual assault charges against her ex-partner because they were concerned that she had shared intimate texts with him during their relationship, so “a barrister would rip me apart and the jury wouldn’t believe me” (Participant 15).
Women also reported child protection authorities made them feel responsible for failing to protect their children from their partner’s abuse. For example, one said:
All of the weight of keeping your kids safe is on you … that’s the ironic thing, you call the police – doing the right thing, trying to protect yourself and your kids – and then the next thing you know … child protection are calling … questioning you as to why you’re not keeping your kids safe because … the perpetrator keeps breaching the order. (Participant 19)
Many described feeling retraumatised by how they were treated by legal professionals. A participant said the lawyer’s cross-examination of her in the courtroom was just like her partner’s abuse:
You have to sit there. You can only speak once you’re spoken to … you’re mocked, you’re ridiculed … your words are twisted around and thrown back at you. (Participant 3)
When charges were withdrawn or legal processes did not succeed, women felt the perpetrator was validated and “emboldened” in their abusive behaviour. One said her partner used the unsuccessful court case to proclaim to friends and family that “he was innocent … and I was a liar” (Participant 26). As a result of their experiences, many participants spoke of losing faith in the legal system. For example, one said:
Police [were] not helpful. My child lawyer wasn’t helpful, judge wasn’t helpful … My ex breached IVO a couple of times; police never listened to me. I showed them texts, I showed them videos … [So] I was like, I’m not going to call [police] at all … I’m better off shutting my mouth and … put[ting] the [home security] camera on. (Participant 6)
Similarly, many women said that they and their children were let down and unprotected by the family courts. Approximately half of the participants mentioned having contact with family court professionals, including judges, mediators, barristers and solicitors, independent children’s lawyers, family court report writers and other family law experts. A consistent theme was that family court professionals lacked an understanding of IPV, particularly non-physical forms of abuse. A common concern was a failure to recognise controlling and coercive behaviour and how it not only affected women’s safety and wellbeing but also undermined the safety and wellbeing of children. Participants also felt the prevailing processes, culture and assumptions within the family courts had worked against them – including a presumption of equal shared parental responsibility, unequal expectations of mothers and fathers, and jurisdictional conflicts between federal andstate/territory laws, and civil and criminal justice systems. For instance, one woman observed:
The family court has high expectations of mothers in terms of parenting and really low expectations of fathers … There doesn’t seem to be any real mechanisms to address … the behaviours of fathers that have been so destructive. (Participant 3)
Another said:
[The family court professionals] were virtually fuelling his sense of entitlement … the court report [writer] …was writing things like “The mother is a danger to the children by insisting that the children don’t have unsupervised contact with the father, because there is nothing wrong with him” … I mean, this man tried to kill me a number of times and I’ve gone to the police and given my statement … which was then passed onto the family court. [But] they dismissed it and then just took he and I as we presented. (Participant 4)
Further, women felt the family courts did not recognise how perpetrators were able to harness the system as a tactic of the abuse. For example, women said perpetrators would deny requests to move house or to access counselling for their children. One said:
Even though he’d been charged with intimidation and extortion and had an apprehended violence order, the parenting agreement was still skewed in his favour … in that I had all the responsibility, and he had the power of veto over my movements, the way the children were brought up and other stuff … So, my experience of the system is that often it increases the suffering and increases the ability for the abuser to victimise. (Participant 29)
Perpetrators also exploited any opportunity to delay proceedings. For example, one woman said during the COVID-19 pandemic when court hearings were held online, her ex-partner repeatedly claimed to have internet problems, so hearings had to be rescheduled. Another common tactic was to deliberately exhaust women’s financial resources by forcing them to respond to minor complaints:
He would just constantly take me to court … over the most trivial matters. [Like] if I didn’t FaceTime him at a certain time … I went and visited my family, oh, she didn’t have my consent to go do that. Just little things, and it was just on and on and on … I’m still paying off my debt. (Participant 11)
In some cases, professionals were aware of abuse but did nothing to address it. For example, one woman said a family court report writer witnessed aggression during a joint session:
[My ex-partner] got up and he grabbed the coffee table … and he was almost going to up-end it … but then he caught himself just in time … [The court report writer] saw it and I saw the fear in her eyes, and I tried to eyeball her, but she just kept her eyes fixed … She never mentioned that incident at all [in her report]. (Participant 5)
Several remained caught up in protracted litigation and felt powerless to escape. They described being engaged with the family courts as “like putting the washing machine with all the dirty laundry on an endless cycle” (Participant 8) or “like that Whac-a-Mole game … where you just wait for the next thing to pop up” (Participant 3).
Women were also concerned that their children were powerless in family court processes and had little opportunity to express their views. For example, one described how her children had only been allocated a brief session with a family consultant to talk about their experiences and views about contact with their father (who had perpetrated IPV). She said that for her children, “It must be so distressing to have your whole life being determined by people with very limited insight into their experience” (Participant 3).
Stage 5:
Addressing impacts and making sense
Once women had established some security and safety, they sought help to make sense of what had happened and to address the impacts of the abuse on their own and their children’s mental health. One participant explained that psychological support at this stage was important, because the mental health impacts became more apparent once the physical danger had ended: “The further away from the abuse you get, the more comes up … So, it doesn’t just get easier afterwards. It actually gets harder” (Participant 20).
During this stage, the women spoke to psychologists, psychiatrists, mental health services, GPs and health professionals, DV and sexual assault services, and peer support groups.
“Help to be a more whole person”: Ongoing counselling with someone who understands
Women wanted a counsellor who was knowledgeable about IPV and could help to piece together what had happened to them and why. One woman said:
The counsellor helped me to see why I’ve been making the choices I’ve been making … to understand why my memory was so bad, why I was so teary, why I was so all over the place. (Participant 1)
Women said a compassionate and understanding response was critically important. However, developing the trust required to share personal experiences and address the trauma of the abuse was a process that took time:
You have to go deeper and treat the root of it and being able to provide that safe environment … because. It’s extremely scary to go back to something that was really traumatic for you … [You need] someone that’s not going to quickly judge you or jump to conclusions. (Participant 2)
Considering this, women valued counsellors who could work with them over a considerable period. However, almost all of the participants had struggled to find such a service. Many said DV services could only provide crisis support:
[It’s] almost, unless you’re in real danger, it’s they don’t know what else they can do … [But] it’s not just the emergency or immediate danger … after you separate, [you need] some ongoing support. (Participant 13)
Some participants had accessed free counselling from a sexual assault service. They said this was helpful, but they were only offered a few sessions. For most, the only long-term option to address the trauma they had experienced was to pay for a private psychologist or counsellor. Some felt this was not a realistic choice because the Medicare rebate for counselling did not cover enough of the expense. For others, having the rebate made a huge difference:
I used to pay $120 an hour out of my own pocket to see good therapists, and now I can get the rebate it’s changed my life … It’s helped me be a more whole person, it’s helped me have better relationships, it’s helped me be a good parent. I could not have been a parent without this. (Participant 9)
Participants frequently reported that the psychologists and psychiatrists they saw had lacked expertise in IPV and/or SV. Several spoke of psychologists and counsellors having medicated their symptoms rather than treating the underlying trauma:
I went through all of this horrible process of been told I had a pretty serious mental health condition and thinking that that’s what it was … I lost about 35 kilograms … on lithium, which is what they put me on … I kept screaming at them. I’m like, I’m just trying to sort this crap that has happened to me out. (Participant 3)
Another common perception was that psychologists only offered “textbook” responses:
Counsellors wanted to go straight to some kind of solution, like “Have you been out for a walk to take your mind off it, have you tried breathing and relaxing exercises?” (Participant 15)
Others had found it difficult to find a counsellor who could relate to their cultural background. For instance, one woman born in India said she wished her counsellor had understood that in her culture it was not acceptable to talk about sexual matters, because it made it hard for her to disclose the sexual assaults she had experienced. Another woman was from a Chinese background and said she felt there was a lack of diversity among psychologists:
[Psychology is] a very privileged industry. It’s very white-based, and so … it’s just limiting … I just didn’t feel like any of these people had any real-world experiences with abuse. (Participant 2)
“You’re not alone”: Connecting with other victims and survivors
Another significant theme at this stage was a desire to connect with other victims and survivors of IPV and/or SV. Participants consistently said peer support would assist them to feel that they were “not alone” and were part of a larger community and a shared experience.
Some were able to join support groups facilitated by organisations, while others located support online. They said these were important sources of support and were particularly helpful in normalising and shifting the stigma of what they had experienced. This was illustrated by the following quotes from two participants:
You feel like you’re in a place where you’re safe and people understand what you’ve been through. (Participant 15)
Reading stories of women who had previously gone through it. I was like, “Oh, I’m actually not alone and what I have gone through is actually really terrible and my feelings are valid.” (Participant 30)
Participants from marginalised communities found being able to connect with others who shared similar backgrounds or experiences was particularly helpful. For instance, one participant said engaging with members of the Aboriginal community had “strengthened” her and had been more valuable than using “mainstream” services (Participant 29). Another woman said:
[The support group for victims and survivors of abuse in lesbian relationships] was important, because I felt like I wasn’t the only one … and that I could recover because other people had too … It breaks that silence, it reduces the stigma, it gives you a voice. (Participant 9)
However, several participants felt services did not offer enough peer support opportunities or did not seem to recognise their value. For instance, one said: “There’s only two or three [DV support groups] in the whole [city] … but they’re all packed and always full” (Participant 15). In another woman’s experience (Participant 16), the agency had only provided a group meet-up opportunity for women but had not used trained facilitators to promote deeper engagement: “They fill you up with a lot of junk food and not … really tell you what step you should take or not … really allow you to speak about things.” She was so concerned about the lack of available support that she voluntarily organised a group information session for Spanish-speaking women in her community who were experiencing IPV and/or SV. Another woman (Participant 5) felt agencies were too restrictive in controlling access to support groups, and that women did not want to go throughanother a “taxing, intensive process” to join them. She had also been involved as a volunteer in setting up a peer support group for women that was “open to anybody”. She said: “This is really work that the [DV] industry should be doing, but they’re not, so we’ve found that we need to fill the gap.”
Conclusion
In summary, from our analysis of interviews with 30 women who were victims and survivors of IPV and/or SV, we developed the following five non-linear and overlapping stages in their help-seeking journeys: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; re-establishing independence and safety; and addressing impacts and making sense. Each stage reflected the particular needs women had at different times. Although women described receiving some helpful responses at different stages, overall, many felt that they were “carrying the burden alone” in seeking support and safety for themselves and their children.
In the next section, we return to the qualitative data we collected in our survey and explore issues during the COVID-19 pandemic that victims and survivors experienced when accessing services.
COVID-19 pandemic impacts on access to services
We asked survey participants to provide written responses to a question about whether the COVID-19 pandemic had affected their access to support services. The majority commented that the pandemic had reduced their ability to obtain support, though some had found it made access easier. We identified the following four themes from participants’ responses.
Everywhere is full or closed
Closed doors, long waiting lists and increased demands on services was a significant theme. Many participants spoke of struggling to find any assistance at all from crisis services. For example:
I needed to leave the family home whilst pregnant but because of lockdown, there was nowhere to go. I was unable to access Centrelink as my application was held up due to JobKeeper [government welfare payments introduced during the pandemic]. Once I left it was difficult to navigate and find the right services as it was all via phone. I wasn’t able to get supports for my children.
It took so long to get the worker and support from the family violence agency, they didn’t even follow up how I am going etc., [which] was an unpleasant experience.
Legal processes changed and court hearings were also frequently delayed or deferred. Some women said this had benefitted the perpetrator:
My ex(s) has/have used it to stone wall and manipulate and take advantage of the backlog in the courts.
COVID-19 was used as a reason to prevent me from attending his court appearances for charges against me! I should be allowed to attend! Once again he’s protected, not me.
Several participants commented that the limited and delayed responses from agencies not only made them less safe, but also communicated to them that the service system did not deem their needs to be important.
It is SO hard to get appointments. Everything is full. It made me feel like I didn’t matter.
I escaped during COVID-19 in March 2020. I was not able to get assistance with housing as the shelters were full. Police were very little assistance as they were so busy, and I felt as though my situation was not “bad enough” for anyone to care much.
I have been waiting nearly two years to have security blinds installed on my home which were meant to help make me feel safe … this is how long the VOCAT [Victims of Crime Assistance Tribunal] system and Department of Housing think it’s OK to take when a domestic violence victim is involved.
Participants also expressed distress that the surge in demand for services left their children without access to support:
I spent many days completely at a loss and totally overwhelmed that I could not secure support for my kids when I first left because all service providers were full.
Few opportunities for private conversations
The increased presence of partners at home was a major barrier to seeking support for many women. Many struggled to find a way to contact services without their partner knowing:
Lockdown is hell. There is no way to find supports when you’re stuck with the person all of the time.
It was very lonely and could only access [services] when my now ex-husband left or if I went for a walk.
It has been difficult to privately talk to professionals without the partner being suspicious or able to overhear the conversation.
I had to pretend to go shopping or something to have Zoom counselling inside of the car.
Having children constantly present due to the requirement that they be schooled at home also made it challenging to reach out for support:
I’m at home with three small children. COVID-19 severely limits me having the children somewhere else so I can access services.
You don’t want your children to overhear what you are saying and there is no-where you can go to speak about it.
Engagement was less personal
A frequent comment was that online or phone contact felt “less personal” than face-to-face contact, and it was harder to open up to the service provider. Participants also expressed fears that sessions could be recorded or that others in the household may overhear:
Phone sessions [are] not the same because I’m not in my safe space in her office to really talk.
It’s very hard to talk to CASA [Centre Against Sexual Assault] on the phone instead of mentally preparing yourself as you would when speaking in person. I don’t always know what to even say.
The lack of continuity of care when using telehealth was another source of frustration:
All sterile over the phone, not always the same person so you’re forced to retell your story again and again. They call you on private numbers which a lot of abused women don’t answer for fear of who it is.
Further, it was difficult to engage children in counselling or legal processes via the phone or online:
My communication with support services was all done via telephone. I feel that it would have been more personal if we were able to meet the case manager/psychologist/ legal representatives in person, especially for children who interact/communicate better in person.
Current face to face restrictions are preventing me from accessing sessions for my kids in one on one and as a family (without perpetrator) as online sessions are just not effective with kids.
Participants also encountered problems in relation to court proceedings. Some reported that perpetrators claimed to have internet access issues, which was a tactic to delay court hearings. Other participants felt the lack of face-to-face contact disadvantaged them in court:
The magistrate/judge doesn’t get to see us in person, see the body language and other interactions that only happen in a face-to-face setting – all of which help to demonstrate the character of my ex-partner and the way he is towards me.
Greater flexibility and accessibility
On the other hand, a considerable number of participants suggested that accessing support was easier during the pandemic due to services being delivered online or via phone. Not having to attend in-person sessions saved time and money (as one said, “less expense involved, no driving/ parking tickets!”) and they could access service providers from outside of their local area or after hours:
[Services are] more accessible, especially when you have young children and can have a counselling session when they are asleep.
I live in a regional area where access to psychologists is limited, and they are mostly in my professional network. COVID-19 meant I could access a psychologist via telehealth.
[Access to services] has been better because I was depressed and sometimes would think twice for the travel to the clinic. Now it’s more convenient.
Some participants said they appreciated being able to access Medicare-funded telehealth counselling, which was a measure introduced by the Federal Government to address the mental health impacts of the pandemic.
Summary
This section overviewed the help-seeking strategies of victim and survivor participants. It was clear from our survey that they most often sought help first from friends and family, followed by health practitioners. Aboriginal and/or Torres Strait Islander women, those who had difficulty managing on their available income, and women aged between 25 and 45 years used informal and formal support more than other women. However, younger women were more likely than others to seek help from friends and family and tended not to seek help from specialist domestic violence or sexual assault services; similarly, migrant women less often sought help from specialist services. Barriers that affected help-seeking included shame and a lack of awareness of services that could help or a perception that the professional would not understand them. Concerns about confidentiality were also important barriers. Almost half of survey participants said that at times theywere unable to get the help they needed, and this was primarily due to a difficulty understanding the professional, a lack of available appointments or the cost of services. Participants’ perceptions of the helpfulness of formal service providers were mixed, though overall more than half rated the responses they received as helpful or very helpful.
Our interviews with 30 victims and survivors provided detailed data on their experiences of help-seeking and how their support needs changed over time. Our analysis showed that while most received valuable responses at different stages of their help-seeking journeys, overall, many felt alone in carrying the burden of addressing the IPV and/or SV. Participants often found that there was little ongoing support or material assistance available, with service providers being overburdened or not understanding their needs. The challenges that victims and survivors faced did not end once they had gotten out of the abusive relationship, with many being subjected to ongoing stalking and/or abuse via the legal system and child contact. Regardless of whether the abuse had ended or continued, most found rebuilding a sense of self and dealing with the traumatic impacts of the abuse on themselves and their children was a difficult and long-term process. However,their ability to recover was hindered by the lack of accessible counselling options and opportunities to connect with other survivors.
Data from our survey indicated that these problems were exacerbated during the pandemic. Many found it harder to access services, though some appreciated the availability of telehealth or online services as they afforded greater flexibility in accessing support.
In the next section we provide an overview of women’s support needs from services and from their family and friends.
3. Support needs of victims and survivors
This section integrates the quantitative and qualitative data to overview what victim and survivor participants were looking for in a service.
What do victims and survivors value in a service?
There was broad agreement among victim and survivor participants about what they valued in a service, and this was usually about how the professional made them feel (Table 17). Victim and survivor participants most valued the receipt of emotional support, including feeling listened to (91.7%); having someone to talk to (90.4%); and not feeling judged or put down (86.9%).
Table 17: Proportion of women who have experienced IPV and/or SV and what they value most in a service (n=688)
| Service values | n (%) |
|---|---|
| Emotional support | 672 (97.7) |
| Feeling listened to | 631 (91.7) |
| Having someone to talk to | 622 (90.4) |
| Not feeling judged or put down | 598 (86.9) |
| Knowing that my story would be held in confidence by professional | 594 (86.3) |
| The professional being interested in who I was as a person | 564 (82) |
| Practical support | 642 (93.3) |
| Given practical information about safety | 593 (86.2) |
| Learning new ways to escape violence | 534 (77.6) |
| Material support (e.g. getting access to accommodation) | 495 (71.9) |
| Professional competency | 596 (86.6) |
| The expertise of the professional | 596 (86.6) |
Notes:
Values are numbers (percentages) unless otherwise stated .
Denominators vary due to missing responses; base = all participants who responded to survey item.
239 participants omitted as they had never sought advice or support.
Expectations of services
The qualitative data we collected from our survey provides more descriptive data on what participants expected and needed from service providers. We asked women survey participants to provide written responses to two questions addressing their expectations from services. The first question asked: “If you think about your partner’s/ex-partner’s behaviours towards you, what do you think your greatest need is from a service or professional?” The second question asked them to complete the sentence “I wish that service providers …” We analysed a selection of their responses to each of these two questions and identified the following five themes, which describe what women victims and survivors need and want from services.
Take me seriously
A strong theme within the data was that women wanted service providers to take their experiences seriously. Women overwhelmingly wanted services to listen and for practitioners to believe them.
My greatest need is for services or professionals … to sit and listen. I can scream my problems from the roof top [and] get nowhere.
To be heard and acknowledged [is my greatest need]. To be believed. For them to tell you what they can offer/explain how they can help or support you rather than you having to request help without knowing what type of help is offered.
[My greatest need is] being believed. Having the police behave professionally and take the assault seriously.
For women who had experienced abuse from an intimate partner, it was important to receive reassurance that the abuse was not acceptable and that they were not responsible for their partner’s behaviour. Such responses helped to affirm that they were not irrational, crazy, exaggerating or imagining things.
[I need] someone to tell me that I am not crazy, and that this is not the way I should be treated.
[I need] validation that he is the problem not me.
[I need] reassurance that the events were unsafe and inappropriate and that the emotional damage is warranted. Reminder that I’m not weak or dramatic.
Help at the time when I need it
A significant theme was for services to be adequately resourced so they could respond when women needed them. Participants’ comments consistently reflected a perception that their support needs were not being fulfilled, with a mismatch between what they wanted and what was offered. A lack of accessibility and availability was one aspect that many women spoke about. They described encountering long waiting lists and limited availability for appointments when trying to access services:
I wish services helped me when I needed them and not months later and that I didn’t have to struggle so hard to find any help at all.
I wish service providers had shorter waiting times …
Participants wanted service providers to spend more time with them, so they could more carefully listen and explore their experiences and needs:
I wish service providers were more accessible and were able to have longer sessions, as it is very hard for me to open up. It takes a long time for me to be able to get the words out.
I wish service providers would take the time to listen rather than just offering up solution.
Many mentioned significant cost-barriers and a wish for more affordable therapeutic or legal services:
I wish service providers were free. I can’t afford to see my therapist.
I wish they could be available when I needed them and that they did not cost so much. I tried a psychologist once but even with my mental health plan it still cost $125 a session. I don’t have that kind of money.
Follow up and follow through
Many of the participants lamented the short-term and transient nature of most of the available service provision. Women felt that they had to contact multiple agencies to find assistance and found it difficult having to repeatedly tell their story. For example, one said, “I wish service providers provided actual practical assistance and stopped referring [me] to the next person and the next person.” They also said services were often not proactive about following up with them after, or between appointments. As one participant stated, “I wish service providers kept checking up on me.” Another similarly valued “consistency, checking in and actually following through”.
Instead, participants wished for enduring support and case management, preferably with someone to help them navigate the legal and service system in an ongoing way. For women who had experienced IPV and/or SV, they wanted to continue to receive support even after an abusive relationship had ended.
We need to have a support network to assist DV victims from the get-go – help with reporting, help with getting an intervention order … Someone needs to take the victim though the whole system.
I wish service providers would be more emotionally supportive with ongoing counselling/referrals once a victim leaves the relationship.
Ongoing specialist counselling to help manage both the trauma from past events and living with the continued risk.
Recognise me as an individual person
Women wanted services to better understand the complexity of their experiences and recognise that violence affects everyone differently. In the context of IPV and/or SV, participants wanted practitioners to improve their recognition of non-physical forms of abuse, including manipulative tactics used after separation:
I wish service providers realised more the hell of coercive control – that even in separation from the ex you are still wholly entrapped if they have access to your children.
I wish service providers had clear training on how to recognise controlling behaviour as the beginning of abusive cycles and the impacts it has on people.
Linked with this was a wish for greater empathy and understanding of how different victims and survivors respond to IPV and/or SV. For example, women wanted services to understand that not every victim and survivor can or wants to leave the relationship:
I wish service providers would not blame me for staying.
I wish service providers understood that not everybody wishes to uproot their lives and leave. Not everybody (especially older women) wants to risk starting again financially or be put in a vulnerable position – going from frying pan to fire – not having sufficient income, no superannuation or savings to start again.
Participants across the sample also wanted practitioners to avoid relying on stereotypes and assumptions and to better understand how abuse and violence affects women with different backgrounds, characteristics or circumstances:
I wish service providers would be less judgemental and factor in cultural differences.
I wish service providers knew that abuse happens to smart educated women too – I am a doctor.
I wish service providers were more accessible for LGBTIQ people experiencing violence.
I wish service providers would treat every client as a human … each client’s needs are different and even vulnerable, uneducated women are intellectual and deserve respect and for their voices to be heard, even when that takes longer than their allocated time.
A need for better access to services was frequently mentioned by victims and survivors with disability, those in rural or regional areas and those who spoke languages other than English. For instance:
I wish service providers can understand me better and if could, provide service in my first language.
I wish service providers could have more services for people with a disability and understand the barriers of people [with] disabilities needing to escape domestic violence.
Finally, women highlighted that the type of support could also vary from person to person. For instance, where some women wanted emotional support, counselling and someone to listen, others wanted more practical help with housing, finances and legal assistance:
I wish service providers could help me with somewhere to go.
I wish service providers could offer REAL assistance for everyday needs.
Make them stop
The final theme was a wish for services to take more action to address the perpetrator’s abusive behaviour. Participants mentioned both legal and police action, as well as therapeutic responses to promote behaviour change.
I wish service providers did more to protect and also address the perpetrators more instead of putting it all onto the victim.
I wish service providers … could do more legally, that they could have removed my partner.
I wish service providers stepped in and provided intensive and REAL support and rehabilitation for changing the negative behaviours … immediately.
Women wanted services to place greater responsibility and accountability onto the perpetrator. They wanted systems to prioritise and foreground their voices as victims and survivors rather than allowing the perpetrator’s voice to “dominate and control the narrative”.
I need the legal system to stop protecting abusers, giving them another platform to continue their abuse and drag out the legal process adding costs and stresses to the victim … He continues to gaslight, stalk, lie, abuse – all in a way that is acceptable to the courts.
[I need] someone to make him stop. To protect the kids and I. To take action against him.
Immediate action for them to tell the police, so his behaviour will no longer be tolerated by anyone.
The next section highlights the role of informal help.
Role of family and friends
The following section discusses our analysis of qualitative data from victims’ and survivors’ responses to two survey questions: “I wish that my family …” and “I wish that my friends …” Our analysis identified that “be on my side” was the central theme in women’s wishes regarding the role of their family and friends. Within this theme there were two sub-themes: “stick by me”, which was frequently connected to the role of friends; and “speak up, step up and step in”, which was mainly associated with the role of family members.
Be on my side
The main theme evident in women’s responses was a wish for family and friends to be “on their side” by supporting them and their view of the situation. This theme was evident in comments about wanting family and friends to “stand by me”, “back me”, and be “loyal” or “there for me”. Participants also gave examples of the things family and friends did that did not demonstrate being “on their side”. For instance, one said:
I wish that my family would be on my side and ask if I’m ok for once. Be there for me. Check on my mental health instead of blaming me for all that’s happened to me.
An important aspect of this theme was family and friends listening to them, believing them and understanding their perspective, rather than taking the perspective of the perpetrator. Participants wanted family and friends to see through the perpetrator and to understand what they were really like:
I wish that my family believed me … They found it easier to believe that I was lying rather than he was capable of the abusive behaviour.
I wish my family could see behind the mask of my partner.
I wish my friends didn’t think my husband was so amazing as he is in public.
Victims and survivors also wanted family and friends to try to understand their responses to the abuse, including the challenges they faced in leaving the perpetrator and managing the long-term impacts of the abuse. For instance:
I wish my family would understand why I have kept going back.
I wish my family could understand why I react the way I do and what might be going on behind closed doors even if I can’t tell them.
I wish that my family would understand that you don’t just “snap out” of trauma.
They also frequently expressed a wish that friends and family understood why it was difficult for them to stay in touch:
I wish my friends could be aware what my life is like. I’m sure they would then understand my huge periods of non-contact.
Participants repeatedly mentioned a wish not to be judged by friends and family. Concerns about judgement were typically focused on a perception that they had been “weak”, “stupid”, a “lost cause” or “a victim” for having stayed in the abusive relationship. For example, one said: “I wish my friends wouldn’t think I’m stupid for giving lots of chances”.
Also associated with having family and friends “on their side” was a wish not to be blamed for their partner’s abusive behaviour. It was notable that participants’ comments about receiving angry or blaming reactions tended to be connected to family members. This was evident in comments such as:
I wish my family would let go of their anger in my marrying that person. I feel doubly punished.
I wish that my family would stop thinking I provoked him in some way.
Victims and survivors also spoke of family members being disappointed in them or seeing them as a “failure”. For example, one said: “I wish that my family would stop caring about what other people think (other relatives or friends) and make me feel ashamed for what I went through.”
Stick by me
The sub-theme “stick by me” was linked to the responses of friends. Many participants expressed a wish that their friends would maintain a strong friendship with them; for example, one said, “I wish my friends would keep always being there for me and me for them.” However, participants’ responses suggested that damaged friendships and the loss of friends was a common experience. A frequent comment was that they wished their friends “didn’t give up” on, “cut off” or “abandon” them. For some, the perpetrator appeared to have directly undermined the friendship:
I wish friends hadn’t believed his lies. I lost all of them.
I wish that my friends hadn’t been removed from my life by his control and isolation.
I wish my friends didn’t believe the ex’s smear campaign.
For others, the loss of friendships occurred because their friends were upset with them for staying in the relationship:
I wish my friends didn’t abandon me as means to show disapproval for the relationship because it made me believe that I was crazy.
I wish friends didn’t judge me or ditch me when I returned back to the perpetrator.
I wish friends didn’t just run away because they “couldn’t stand watching this”.
Victims and survivors also wished their friends would be proactive in maintaining the friendship and would make an effort to reach out to them:
I wish my friends checked in on me more, instead of just waiting for me to call them.
I wish friends had regular scheduled catch ups or social events to maintain contact.
I wish friends were able to spend more time with me when I really needed it, but they were busy with their own families.
Step up, speak up and step in
The second sub-theme mainly related to victims’ and survivors’ family members and a wish that they could play an active role in looking after them. This theme was reflected in participants’ comments about wanting family members to “step up” and help with everyday tasks, finances or a place to stay:
I wish that my family [gave] practical support in managing day to day life, like having help with household tasks like cooking and cleaning, picking up kids from school, so we can focus on sorting out legal issues.
I wish that my family was rich (!) so we could escape and not need his child support.
I wish that my family would have let me stay with them and report everything to police and take a AVO against him for my safety.
Participants also expected that they should be able to rely on their family to act in their best interests. Several said they had wanted family members to raise their concerns with them when they noticed signs of abuse:
I wish that my family spoke up about how they felt about him.
I wish that my family had helped me earlier and been stronger in telling me things weren’t right and that I deserved better.
They also wished their family members were able to step in to protect them:
I wish that my family could make him leave me alone.
I wish that my family had been more honest and stopped me from getting married.
Speaking up and stepping in was also a response women wanted from their friends when they witnessed abusive behaviour. Several said they wished that friends would have called out abusive behaviour when they were bystanders to it. For example:
I wish that my friends pulled my partner up on their abusive behaviour … especially if present when it occurred.
Summary
In summary, victim and survivor survey participants wanted emotional and practical support from professionals who had expertise in the area. Our analysis of qualitative survey data found that they wanted formal service providers to take them seriously; help them at a time when they needed it; follow up and recognise their individual experiences; and take more action to make the perpetrator stop the abuse. In relation to informal support, they wanted their family and friends to be on their side, by sticking by them and stepping up through providing practical assistance, and to speak up when they witnessed abusive behaviour. The next part turns to the voices of people who use IPV and/or SV.
Part D:
Key findings –
The experiences of people who use violence
“It’s very hard to understand what behaviours are abusive/wrong, I often can’t understand why I’m wrong for a long time or until an event [occurs] after which it becomes clear.”
(Survey participant)
Introduction
This part is divided into three sections that integrate quantitative and qualitative findings from the perspective of people who use IPV and/or SV. The first section overviews participant characteristics, and the nature, patterns and associations of use of IPV and/or SV, including the effects of the COVID-19 pandemic on experiences. This is followed by a section on help-seeking and service needs, including the effects of the COVID-19 pandemic. The final section describes the support needs of people who use IPV and/or SV.
1. Patterns and associations of use of IPV and/or SV
Sociodemographic characteristics
Overall, participants who used violence were generally representative of the Australian population except for a few specific demographic areas of note. The majority of participants (93.1%) were men, 5.7 per cent were women, 0.9 per cent were non-binary and 0.4 per cent preferred to self-describe. Nearly two thirds of participants in this study were aged between 18 and 39 years, a higher proportion compared to the general Australian population (Table 18). Approximately double the percentage of Victorian residents responded to this survey compared to the general population. Similar to population figures, approximately three quarters (74%) of the people in this study were born in Australia and lived in a metropolitan area (78.7%). Of those participants who were in arelationship at the time of the survey, the majority had a female partner (94.4%), were married (38.1%) and had children at home (69.2%; Table 18).
The proportion of participants identifying as Aboriginal and/or Torres Strait Islander (10.1%) or who did not complete Year 12 (19.6%) was higher than in the general community. Approximately half (49.7%) of participants had completed a degree or higher degree, which was also higher than the general community (28.3%). Most participants were employed (67.8%), although many (39%) had difficulty managing on their available income some or all of the time, which was disproportionally high compared to the general community.
Table 18: Demographic characteristics of participants who completed survey about use of violence and abuse compared to the broader Australian population (N=563)
Age (years; n=562)
| Characteristic | All participants n (%) | Australian population %a |
|---|---|---|
| 18–29 | 194 (34.5) | 19.8 |
| 30–39 | 158 (28.1) | 14.7 |
| 40–49 | 78 (13.9) | 12.8 |
| 50–59 | 132 (23.5) | 12.2 |
Current Australian state of residence
| Characteristic | All participants n (%) | Australian population %a |
|---|---|---|
| Australian Capital Territory | 9 (1.6) | 1 |
| New South Wales | 128 (22.8) | 15.1 |
| Northern Territory | 1 (0.2) | 0.5 |
| Queensland | 82 (14.6) | 9.5 |
| South Australia | 26 (4.6) | 3.7 |
| Tasmania | 6 (1.1) | 1.2 |
| Victoria | 285 (50.7) | 11.5 |
| Western Australia | 25 (4.4) | 4.6 |
| Lives in metropolitan area | 441 (78.7) | 71 |
| In current relationship (≥1 month length) | 320 (57.2) | ** |
| Lives with partner | 332 (56) | 45 |
| Not living with partner (male/female/spouse) | 231 (41) | 24 |
Sex of current partner (n=320)b
| Characteristic | All participants n (%) | Australian population %a |
|---|---|---|
| Female | 302 (94.4) | 63.8 |
| Non-binary | 1 (0.3) | 17.3 |
| Prefer not to say | 16 (5) | ** |
Sexual orientation (n=547)
| Characteristic | All participants n (%) | Australian population %a |
|---|---|---|
| Heterosexual | 457 (83.6) | 92.8 |
| Bisexual | 46 (8.4) | 0.8 |
| Queer | 8 (1.5) | ** |
| Asexual | 2 (0.4) | ** |
| Self-described | 7 (1.3) | ** |
| Not sure | 22 (4) | 1 |
Marital status
| Characteristic | All participants n (%) | Australian population %a |
|---|---|---|
| Never married | 275 (48.9) | 32 |
| Married | 214 (38.1) | 30.6 |
| Separated but not divorced | 36 (6.4) | 2.9 |
| Divorced | 33 (5.9) | 7 |
| Widowed | 4 (0.7) | 6 |
| Children | 240 (42.7) | 43 |
| 1+ children living at home | 166 (69.2) | 49 |
| Aboriginal and/or Torres Strait Islander | 57 (10.1) | 3.2 |
| Born outside Australia | 146 (26) | 30 |
| First language not English | 90 (16) | 21 |
Prior schooling (n=539)
| Characteristic | All participants n (%) | Australian population %a |
| Attended school but finished prior to Year 12 | 106 (19.6) | 10.5 |
| Completed Year 12 | 436 (80.4) | 79 |
Educational qualification (n=542)
| Characteristic | All participants n (%) | Australian population %a |
| Trade/apprenticeship/diploma | 202 (37.5) | 32.8 |
| University degree/higher degree | 268 (49.7) | 24 |
Employment and income (n=546)
| Characteristic | All participants n (%) | Australian population %a |
| Employed | 370 (67.8) | 64.1 |
| Not employed | 176 (32.2) | 5.7 |
| Has difficulty managing on available income | 213 (39) | 18.7 |
| Health Care Card holder | 337 (61.7) | 52 |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey item.
** Comparable data either not collected or available.
a Population data is weighted proportions from Australian Bureau of Statistics (2020); values are proportion total Australian population.
b Male partner not reported; participants with male partner excluded from survey on IPV against women .
Twelve-month and lifetime experiences of use of violence and abuse
Interpretive note
To understand the experience of people who use violence and abuse, the survey screened participants for behaviours in their relationship using three items relating to feeling concerned about behaviours in a relationship, help-seeking for issues in a relationship and having made a partner feel afraid. These questions were designed to engage people who may not have identified their behaviour using the language of “domestic violence or abuse” but may still have felt worried about their behaviour. Participants could answer with a simple “yes/no” response. Abusive actions and behaviours of participants were measured using the short-form CASr-SF (Ford-Gilboe et al., 2016), altered to ask about behaviours used by participants against a partner, and experiences of child abuse were measured using the ACEs scale (Felitti et al., 1998; see “Methodology” earlier).
It is important to note that while not all participants reported using IPV and/or SV when measured using the CASr-SF (Ford-Gilboe et al., 2016), all participants completed screening questions (see “Methodology” further) indicating that they may have used abuse and violence in a relationship, which established their eligibility for the study. Further, analysis of the violence against women attitudes data indicated differences between all participants and general population attitudes but not meaningful attitudinal differences between people who reported as having used IPV and/or SV on the CASr-SF and those who had not (Table 26).
In analysing participants’ responses in the open-ended questions on the survey, it was evident that many did not see themselves or did not wish to characterise themselves as perpetrators. This was despite them having identified using forms of violent or abusive behaviour in other parts of the survey. For example, one responded by saying: “I am not convinced I am violent or abusive, I am a really good man”, and another said: “I’m not really a violent person by nature but sometimes I just get really angry.” Similarly, other participants rejected the characterisation because they had not used physical aggression. For example, one said: “I [am] mostly not violent, like I don’t hit her, it’s mostly verbal and I’ve tried all I can.” This suggested they did not perceive negative verbal or psychological behaviours to be as serious as physical abuse. Another common response was acknowledging some form of abuse but suggesting its impact was minimal or theirpartner mutually contributed to it. For instance, one participant said: “I’m not sure it can be classified as abuse. If so, it is a mild form of abuse she is willing to tolerate.”
For all of the reasons above, we chose to analyse the whole sample, rather than selecting out only the people who scored on the CASr-SF, and we refer to all participants in this section as “people who have used violence and abuse” (Ford-Gilboe et al., 2016).
Experiences and patterns of using IPV and/or SV in the past 12 months
In the last 12 months, 34.8 per cent of people in this study reported having used violence against a partner or ex-partner (as measured using 15 behaviours on the CASr-SF; Ford-Gilboe et al., 2016). Approximately one in four (26.7%) participants identified that they had made their partner feel afraid of them in the last 12 months, with slightly more than one in five (22.7%) saying their partner was currently afraid of them (Table 19). Approximately half of the participants who reported using any IPV in the last year said this was psychological in nature, while 44.4 per cent was sexual and 42 per cent physical.
Table 19: Proportion of people who had used violence against a partner during the last 12 months
Last 12 months
| Types of IPV and/or SV | n (%) |
|---|---|
| Made partner feel currently afraid (n=427)a | 97 (22.7) |
| Made partner feel afraid in last 12 months (n=491) | 131 (26.7) |
| Used IPV (any; n=490)b | 81 (16.5) |
| Physical | 34 (7.1) |
| Sexual | 36 (7.5) |
| Psychological (including technology-facilitated abuse) | 45 (9.5) |
| Total 12-month made partner feel afraid and/or used violence against them (n=491) | 171 (34.8) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed screening items and/or 12-month CASr-SF (Ford-Gilboe et al. 2016).
a 68 participants omitted because they had never been in a relationship longer than one month.
b Participants could belong to more than one CASr-SF category.
Table 20 displays the 12-month frequency of specific acts of abuse that were asked about in the survey. It indicates that the most common acts of IPV and/or SV were harassing one’s partner by phone, text, email or social media; telling one’s partner they were crazy, stupid or not good enough; and trying to convince the family or friends of one’s partner that they were crazy.
Table 20: Of people who had ever used violence, proportion of those who had used each behaviour in the last 12 months
| Abusive behaviours | 12-month use |
|---|---|
| Harassed partner by phone, text, email or using social media | 74 (60) |
| Told partner they were crazy, stupid or not good enough | 74 (54.4) |
| Tried to convince partner’s family or friends that they were crazy | 29 (53.7) |
| Blamed a partner for causing their violent behaviour | 73 (49.6) |
| Hit partner with a fist or object, kicked or bit them | 21 (47.7) |
| Made partner perform sex acts that were unwanted | 26 (47.3) |
| Kept partner from seeing or talking to family or friends | 14 (46.7) |
| Forced or tried to force partner to have sex | 20 (45.4) |
| Shook, pushed, grabbed or threw a partner | 50 (45) |
| Choked partner | 12 (42.8) |
| Kept partner from having access to a job, money or financial resources | 11 (42.3) |
| Confined or locked partner in a room or other space | 5 (41.7) |
| Used or threatened to use a knife or gun or other weapon to harm partner | 9 (40.9) |
| Followed partner or hung around outside their home or work | 25 (35.2) |
| Threatened to harm or kill partner or someone close to them | 7 (30.4) |
| Total (one or more abusive behaviours; n=290)b | 169 (58.3) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = 12-month proportion of participants who had used corresponding lifetime abusive behaviour measured using CASr-SF (Ford-Gilboe et al. 2016).
a Behaved in this way once or more during last 12 months as a proportion of people who had ever used each behaviour- see Table 22.
b 169/290 people used one or more abusive behaviours in the last 12 months.
Lifetime experiences of using violence and abuse
As above, while everyone who took part in the survey completed screening questions indicating that they may have used abuse and violence in a relationship, which established their eligibility for the study, just over half (58.2%) met the criteria for having used IPV during their adult lifetime on the CASr-SF (Ford-Gilboe et al., 2016). Of these 288 participants, three in four (75.7%) identified that their behaviour had caused their partner to feel afraid of them (Table 21). Approximately one in five (21.6%) participants had used sexual violence against a partner, and 19 had exerted coercion over their partner’s reproductive health and decision-making (4.7%)
Table 21: Proportion of people who have used violence against a partner across the adult lifetime (since the age of
16 years)
| People who have used violence | n (%) |
|---|---|
| Have ever made partner feel afraid (n=495) | 218 (44) |
| Perpetrated IPV (any; n=491) | 171 (34.8) |
| Used SV against a partner or ex-partner (n=490) | 106 (21.6) |
| Total IPV (including fear; n=495) | 269 (54.3) |
| Reproductive coercion (n=490) | 23 (4.7) |
| Total adult lifetime IPV, SV and/or reproductive coercion (n=495) | 288 (58.2) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed CASr-SF and other abuse survey items.
Sixty-eight participants omitted because they had never been in a relationship for longer than one month.
The acts of abuse most frequently reported among participants were emotionally abusive and harassing behaviours, including blaming their partner for causing violent behaviour (29.9%); telling their partner they were crazy, stupid or not good enough (27.7%); and harassing their partner by phone, text, email or using social media (25.3%; Table 22).
Table 22: Proportion of people who have used lifetime violence and the type of abusive behaviour used (n=495)
| Abusive behaviours | Adult lifetime n (%) |
|---|---|
| Blamed partner for causing their violent behaviour | 147 (29.9) |
| Told partner they were crazy, stupid or not good enough | 136 (27.7) |
| Harassed partner by phone, text, email or using social media | 124 (25.3) |
| Shook, pushed, grabbed or threw partner | 111 (22.6) |
| Followed partner or hung around outside their home or work | 71 (14.5) |
| Made partner perform sex acts that were unwanted | 55 (11.2) |
| Tried to convince partner’s family or friends that they were crazy | 54 (11) |
| Forced or tried to force partner to have sex | 44 (9) |
| Hit partner with a fist or object, kicked or bit them | 44 (9) |
| Kept partner from seeing or talking to family or friends | 30 (6.1) |
| Choked partner | 28 (5.7) |
| Kept partner from having access to a job, money or financial resources | 26 (5.3) |
| Threatened to harm or kill partner or someone close to them | 23 (4.7) |
| Used or threatened to use a knife or gun or other weapon to harm partner | 22 (4.5) |
| Confined or locked partner in a room or other space | 12 (2.4) |
| Total (one or more abusive behaviours) | 290 (59.1) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = adult lifetime proportion of participants who had used lifetime abuse measured using CASr-SF (Ford-Gilboe et al. 2016); maximum missing n=5.
Patterns of abuse and violence by people who use violence
Participants more frequently reported violence against a partner in the last 12 months if they were aged between 25 and 45 years, were Aboriginal and/or Torres Strait Islander, and told us they had difficulty managing on their available income (Table 23). Those same sociodemographic factors were associated with use of violence against a partner over the adult lifetime (since the age of 16 years). Those not living with a partner were under-represented among those who had used violence in the last 12 months. Youth was also associated with under-reporting abuse and violence across the adult lifetime (Table 23).
Table 23: Proportion of people who used violence in the last 12 months and across the adult lifetime with sociodemographic factors
| Sociodemographic factors | Use of violence against a partner in last 12 months (n=171) | Use of violence against a partner (since the age of 16 years) (n=269) |
|---|---|---|
| All participants (n=562) | 171 (34.8) | 269 (54.3) |
Age (years)
| Sociodemographic factors | Use of violence against a partner in last 12 months (n=171) | Use of violence against a partner (since the age of 16 years) (n=269) |
|---|---|---|
| Up to 25 years (n=133) | 33 (28) | 51 (43.2) |
| 25-45 years (n=267) | 99 (43.2) | 145 (63) |
| > 45 years (n=162) | 39 (27.1) | 73 (50) |
| Aboriginal/Torres Strait Islander (n=53) | 29 (54.7) | 39 (72.2) |
| Migrant background (n=152) | 44 (33.6) | 73 (55.7) |
| Lives in non-metropolitan location (n=98) | 37 (37.8) | 60 (61.2) |
| Attended school but finished prior to Year 12 (n=101) | 36 (35.6) | 60 (59.4) |
| No university degree (n=240) | 80 (33.3) | 132 (55) |
| No employment (n=160) | 57 (35.6) | 90 (56.2) |
| Has difficulty managing on available income (n=200) | 77 (38.5) | 122 (61) |
| Health Care Card holder (n=302) | 99 (32.8) | 163 (54) |
| Not living with partner (n=206) | 58 (28.2) | 112 (53.6) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
% = represents the proportion of overall demographic group who have used abuse.
Adverse childhood experiences and use of violence in adulthood
Physical, sexual and/or emotional abuse in childhood had been experienced by approximately one in two (47.6%) participants who had ever used IPV and/or SV (Table 24 and Figure 15). One in three (33.7%) participants had been physically abused or neglected before the age of 15, nearly one in five (17.3%) had been sexually abused and nearly half (47.2%) had been emotionally abused or neglected. Using logistic regression, the predicted odds of reporting the use of violence against a partner in the last 12 months were three times greater if a participant had experienced child abuse (OR 3, 95% CI 2 to 4.5), and 2.7 times greater if the participant had used violence against a partner since they were aged 16 years (OR 2.7 95% CI 1.8 to 3.8). This association betweenchild abuse and the use of IPV and/or SV in adulthood indicates a life course effect of violence in early life on later relationships.
Table 24: Proportion of people who have used violence who have experienced child abuse
| Child abuse typea | Before age 15 years |
|---|---|
| Emotional abuse | 210 (37.4) |
| Emotional neglect | 183 (32.6) |
| Physical neglect | 170 (30.4) |
| Physical abuse | 170 (30.3) |
| Sexual abuse | 97 (17.3) |
| FV against mother growing up | 86 (15.3) |
| Total child abuse | 267 (47.6) |
| Total ACEb score of 4+ | 153 (27.3) |
| Total child abuse and/or ACE>4 | 270 (48.1) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to child abuse survey items.
a Abusive behaviour before the age of 15 years by someone aged 18 plus years.
b ACEs scale (Felitti, 2019) score out of 10; scores 4+ are associated with serious health and risk issues in adulthood (Felitti, 2019).
Figure 15: Proportion of people who had used IPV and/or SV since the age of 16 and/or experienced child abuse before the age of 15 years (n=356)
Data table for the figure above:
| Category | Percentage | n |
|---|---|---|
| Child abuse | 24.4% | 87 |
| Perpetrated IPV (adult lifetime) | 28.1% | 100 |
| Child abuse and perpetrated IPV | 47.5% | 169 |
In Brief:
Use of violence and abuse findings
Aboriginal and Torres Strait Islander participants, participants aged 25–45 years, and those who had difficulty managing on their available income were over-represented as having used violence in the last 12 month and across the adult lifetime (since 16 years).
Participants who were not living with a partner were less likely to have used violence and abuse in the last 12 months. Younger participants (less than 25 years) were less likely to have used violence and abuse in the last 12 months and across the adult lifetime (since 16 years).
Participants who had experienced child abuse were three times more likely to use violence against a partner in adulthood.
Health experiences of participants who had used violence
Participants who had used violence against a partner in the last 12 months were more likely than those whose IPV and/or SV occurred more than 12 months ago to report poor health and mental health on a range of measures (Table 25). More than half (51.2 to 62.6%) of all participants screened positive for PTSD. Further, between one in four and one in three participants who had used violence and abuse reported poor to fair general health and long-term illness, and met the core criteria for anxiety, depression and/or hazardous alcohol consumption.
Table 25: Proportion of people who use violence and their experience of health and mental health issues, arranged by type of abuse and cumulative abuse
Mental health
| Current health issues | All participants (n=562) | Use of violence against a partner in last 12 months (n=171) | Use of violence against a partner since the age of 16 years (n=269) |
|---|---|---|---|
| PTSD | 288 (51.2) | 107 (62.6) | 107 (62.6) |
| Anxiety | 171 (30.4) | 63 (36.8) | 89 (33.1) |
| Depression | 163 (29) | 65 (38) | 93 (34.6) |
| Hazardous alcohol consumption | 137 (26.2) | 47 (29.4) | 71 (28.5) |
General health
| Current health issues | All participants | Use of violence against a partner in last 12 months | Use of violence against a partner since the age of 16 years |
|---|---|---|---|
| Lives with disability | 145 (25.8) | 53 (31) | 87 (32.3) |
| Poor to fair self-rated health | 118 (21) | 47 (27.5) | 68 (25.3) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
Attitudes towards violence against women
A higher proportion of participants in this study demonstrated attitudes that support violence against women when compared to the Australian community (using the National Community Attitudes towards Violence against Women Survey [NCAS] items; Webster et al., 2018). Across all 10 violence against women attitude items, a higher proportion of survey participants agreed with each statement when compared to the national Australian population (Table 26). Moreover, participants who met the criterion on the CASr-SF for having used IPV and/or SV displayed the highest proportion of attitudes that support violence against women. For example, 72 per cent agreed with the statement “Many women mistakenlyinterpret innocent remarks or acts as being sexist”, compared to 50 per cent of the general population; 56.9 per cent agreed that “Men should take control in relationships and be the head of the household”, compared to 16 per cent of the general population; and 28.5 per cent thought that “It is embarrassing for a man to have a job that is usually filled by a woman”, compared to just 6 per cent of the general Australian population (Table 26).
Table 26: Proportion of people who use violence who hold attitudes that support violence against women compared to the Australian population
| Attitude | Participants who agreed with statement (n=521) | Participants who had used lifetime IPV and/or SVa who agreed with statement (n=246) | Australian comparisonb N=17,500 |
|---|---|---|---|
| Many women mistakenly interpret innocent remarks or acts as being sexist | 358 (68.7) | 177 (72) | 50% |
| Many women exaggerate how unequally women are treated in Australia | 334 (64.1) | 162 (65.8) | 40% |
| Many women fail to fully appreciate all that men do for them | 310 (59.5) | 155 (63) | 36% |
| Women prefer a man to be in charge of the relationship | 305 (58.5) | 146 (59.3) | 25% |
| Men should take control in relationships and be the head of the household | 288 (55.3) | 140 (56.9) | 16% |
| On the whole, men make better political leaders than women | 240 (46.1) | 115 (46.7) | 14% |
| In the workplace, men generally make more capable bosses than women | 244 (46.8) | 114 (46.3) | 14% |
| I think there’s no harm in men making sexist jokes about women when they are among their male friends | 210 (40.3) | 118 (48) | 24% |
| When a couple start dating, the woman should not be the one to initiate sex | 201 (38.6) | 94 (38.2) | 10% |
| I think it is embarrassing for a man to have a job that is usually filled by a woman. | 132 (25.3) | 70 (28.5) | 6% |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who completed the NCAS (Webster et al., 2018).
a Scored using the CASr-SF (Ford-Gilboe et al., 2016).
b Webster et al., 2018.
In Brief
The health and attitudes of participants who had used violence and abuse
Participants who had used violence against a partner recently were more likely than those whose IPV occurred longer than 12 months ago to report poor physical and mental health.
On every attitudinal measure, a higher proportion of participants indicated attitudes that support violence against women compared to the general Australian community.
This section has provided an overview of the patterns of abuse and violence used by survey participants, and how these were associated with their sociodemographic characteristics. In the next section we examine qualitative survey data on the impact of the COVID-19 pandemic on the use of IPV and/or SV.
The impact of the COVID-19 pandemic on IPV and/or SV
Survey participants who had used abuse or violence were asked to provide written responses to the question: “How have your experiences in your adult intimate relationships changed during COVID-19 isolation?” From our question, it was difficult to determine whether participants were referring to an abusive relationship or a non-abusive one. Consequently, we focused on comments that alluded to the participant’s behaviour towards a partner/ex-partner. In response to our question, most simply commented “no” or “no change”. However, others noticed that the pandemic had influenced their relationships and behaviour towards their partner.
Increased pressure triggered poor behaviour
While some participants felt the pandemic had been a time of personal growth, others admitted it had triggered problematic behaviour towards their partner. Many suggested this was due to having had less space and time away from their partner. For instance, several survey participants who identified that they had been physically aggressive towards a partner said that they had found it harder to control their emotions during the pandemic:
Worse – she’s in my face all the time and I get angrier.
More time together, less opportunity for space when either one of us is upset or feeling overwhelmed.
[It has been] harder to keep my temper in check.
Others suggested their poor behaviour had resulted from increased mental distress and financial pressures:
Increased isolation and severe stress due to finances has triggered a lot of my behaviours. Severe mental health deterioration for both my partner and I, lack of access to services.
Heightened feelings of depression and anxiety causing me to take it out on my partner.
Several indicated that the restrictions on how often they could see their partner created tensions in the relationship. Some suggested being unable to meet up with their partner caused problems in communicating effectively, which led to increased stress or feeling more insecure or worried about the relationship.
The pandemic provided time and space for self-reflection
A strong theme was that the pandemic prompted positive change. Many said the isolation afforded them more time to reflect on their problematic behaviour and the personal issues that may contribute to it. This was evident in the following comments:
Living alone during the COVID-19 isolation periods last year was immensely beneficial. I was already changing a number of things in my life and coming out of a hugely destructive working environment, so was already making the types of active changes to make myself a better partner. However, during the isolation period, I found myself actively assessing my life, how I act, and who I want to be. As an extrovert, I believe this may have been the first period in my entire life that I was actually able to engage in such reflection, and I believe it has sped my transformation.
My experiences have changed a lot. I spent countless hours thinking on how I can be a better husband. I spent hours thinking of how I can provide for my kids. I spent hours thinking on how I can talk to my wife and let her know how much I love her.
I’ve been actively avoiding intimate relationships so I could work on my own mental health and drug dependency issues.
Others said that spending more time in contact with a partner during COVID-related isolation had prompted self-reflection and change. For example, one participant who identified in the survey that she had been physically aggressive and had excessively contacted her partner and kept him from family and friends responded:
Firstly, I found that the relationship I did enter became very intense very quickly due to the fact we were legally only allowed to visit each other and no one else. I was in a short-lived relationship during COVID-19 which caused me to deeply self-reflect and take a break from dating to work on myself. COVID-19 has been a time of personal growth for me.
Some felt the reduced stress and pressure during isolation had enabled them to have a greater emotional control:
Surprisingly, our experiences have been better during isolation. A lot of my anxiety comes from being in public spaces. Being isolated has been a short-term fix for most of my anxiety issues and in turn I have had far better control on my frustration levels and reduced the amount of drinking I have had.
Summary
Our analysis of the survey data from over 500 participants (predominantly male) found that a third indicated they had been abusive or violent to a partner or ex-partner in the past 12 months, and more than half reported having used IPV and/or SV during their adult lifetime. Emotionally abusive or harassing behaviours were the most commonly reported forms of abuse used. Aboriginal and Torres Strait Islander participants and those who had difficulty managing on their available income were over-represented among those who had used violence or abuse, while participants aged under 25 were under-represented. Almost half of participants who used IPV and/or SV in the last 12 months had experienced abuse in childhood. Those who had used IPV and/or SV were also more likely than other participants to report having poor physical and mental health. Survey data indicated that a higher proportion of participants had attitudes that support violence against womencompared to the general Australian community. Our analysis of qualitative data from the survey suggested that for many, their use of IPV and/or SV escalated during the COVID-19 pandemic; however, some said the isolation allowed them more time to reflect on their problematic behaviour.
The next section explores the help-seeking experiences of people who use IPV and/or SV.
2. Help-seeking experiences of people who use IPV and/or SV
This section provides an overview of the help-seeking experiences of people who use IPV and/or SV, based on the survey data. In particular, it details from whom they sought help; how helpful it was; and the barriers to seeking help. The section also draws on the interview data to explore how people who use violence engage on journeys to seek help and the open-ended questions in the surveys to understand how participants felt the COVID-19 pandemic affected help-seeking. Both informal and formal services were included, ranging from all sectors that could come in contact with people who use violence or abuse. It should be remembered that half of the participants were from Victoria, a state where there has been a marked degree of reform across the system in the last five years.
Help-seeking experiences
Most participants (73.5%) had sought formal or informal advice or support from someone about their behaviour towards a partner (Table 27). Most often, the person to whom a participant spoke was a friend (45.4%), partner (31.7%) or family member (27.7%). Among the formal services that participants accessed for assistance, health services were the most frequently utilised (33.3%), followed by specialist family violence services (10.8%), and justice services (6.3%). More often than not, participants rated the service they had accessed as helpful (71.8%). Some services were deemed more helpful than others, with psychologists or counsellors (84.1%), religious people (81.8%) and family therapists (80.8%) the most positively rated.
Table 27: Proportion of people who have used abuse and violence, sources of help-seeking and perceived helpfulness
| Service/resource | Sought support (n=555) | Found support helpfula |
|---|---|---|
| Any source of help: | 408 (73.5) | 72.3b |
| Family and friends (total) | 327 (58.9) | 74.3c |
| Friend/s | 252 (45.4) | 194 (77) |
| Partner | 176 (31.7) | 134 (76.1) |
| Family member/s | 154 (27.7) | 111 (72.1) |
| Formal sources of support: | 229 (41.3) | 71.8 |
| Health services (total) | 185 (33.3) | 74 |
| Psychologist/counsellor | 138 (24.9) | 116 (84.1) |
| Family therapist | 26 (4.7) | 21 (80.8) |
| Nurse | 12 (2.2) | 9 (75) |
| General practitioner | 58 (10.4) | 40 (70.2) |
| Social worker (hospital, community health) | 13 (2.3) | 9 (69.2) |
| Alcohol or drug worker | 19 (3.4) | 11 (64.7) |
| Specialist services (total) | 60 (10.8) | 73.2 |
| Men’s referral service | 19 (3.4) | 15 (78.9) |
| Behaviour change program | 18 (3.2) | 14 (77.8) |
| Domestic or family violence service | 27 (4.9) | 17 (63) |
| Telephone helpline (e.g. Lifeline, 1800RESPECT) | 19 (3.4) | N/A |
| MensLine | 15 (2.7) | N/A |
| Justice services (total) | 35 (6.3) | 61.5 |
| Legal service (e.g. solicitor or legal aid) | 13 (2.3) | 10 (76.9) |
| Police | 26 (4.7) | 12 (46.1) |
| Community – other (total) | 33 (5.9) | 78.4 |
| Priest/minister/rabbi or any other religious person | 22 (4) | 18 (81.8) |
| Work colleague or boss | 12 (2.2) | 9 (75) |
| Housing and financial services (total) | 6 (1.1) | ** |
| Financial service (e.g. Centrelink) | 5 (0.9) | 4 (**) |
| Housing service | 1 (0.2) | 1 (**) |
| Did not seek advice or support | 147 (26.5) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to opt in survey item about having spoken to someone about behaviour in relationship.
** Small cell count prevented analysis.
a Helpful/very helpful (median).
b Total number of participants who had accessed 1+ service (average proportion of all participants who found service/s helpful).
c Category proportions are an average of helpfulness across the category.
Some groups of participants accessed services for advice and support more or less frequently than others (Table 28). While interpretive caution is required due to small cell counts in some cases, some between-group differences are still important to highlight. Aboriginal and Torres Strait Islander participants sought help more than other participants, especially among family and friends, specialist services and other community services. Participants who had attended school but left prior to Year 12 and those who had difficulty managing on their available income were also more frequent service-users. Migrant participants were less likely than other participants to have accessed services (Table 28).
Table 28: Proportion of help-seeking by people from diverse backgrounds
Age (years)
| Demographic | Community – family and friends n (%) | Health services n (%) | Specialist services n (%) | Justice services n (%) | Community – other n (%) | Did not seek advice or support n (%) |
|---|---|---|---|---|---|---|
| All participants (n=562) | 327 (58.9) | 185 (33.3) | 60 (10.8) | 35 (6.3) | 33 (5.9) | 147 (26.5) |
| Up to 25 (n=133) | 100 (75.2) | 20 (15) | 5 (3.8) | 3 (2.3) | 2 (1.5) | 30 (22.6) |
| 25–45 (n=267) | 160 (60.2) | 96 (36.1) | 35 (13.2) | 17 (6.4) | 21 (7.9) | 64 (24.1) |
| > 45 (n=162) | 67 (42.9) | 69 (44.2) | 20 (12.8) | 15 (9.6) | 10 (6.4) | 53 (34) |
| Aboriginal and/or Torres Strait Islander (n=53) | 40 (71.4) | 21 (37.5) | 14 (25) | 6 (10.7) | 10 (17.9) | 13 (23.2) |
| Migrant background (n=152) | 91 (60.7) | 39 (26) | 9 (6) | 4 (2.7) | 7 (4.7) | 42 (28) |
| Lives in non-metropolitan location (n=98) | 61 (51.7) | 48 (40.7) | 16 (13.6) | 10 (8.5) | 9 (7.6) | 32 (27.1) |
| Attended school but finished prior to Year 12 (n=101) | 53 (50) | 45 (42.4) | 20 (18.9) | 11 (10.4) | 5 (4.7) | 29 (27.4) |
| No university degree (n=240) | 154 (56.8) | 95 (35.1) | 33 (12.2) | 20 (7.4) | 17 (6.3) | 73 (26.9) |
| No employment (n=160) | 108 (61.4) | 63 (35.8) | 18 (10.2) | 17 (9.7) | 11 (6.2) | 44 (25) |
| Has difficulty managing on available income (n=200) | 131 (61.5) | 84 (39.4) | 39 (11.6) | 23 (10.8) | 15 (7) | 47 (22.1) |
| Health Care Card holder (n=302) | 212 (62.9) | 125 (37.1) | 39 (11.6) | 22 (6.5) | 18 (5.3) | 82 (24.3) |
| Not living with partner (n=206) | 151 (66.8) | 73 (32.3) | 31 (13.7) | 19 (8.4) | 13 (5.7) | 45 (19.9) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey items.
The proportion (%) in this table represents the proportion of overall demographic group who have accessed help by category.
In brief:
Help-seeking of participants who had used violence and abuse
People whose income did not cover their needs and people aged 45 years and older accessed health services more than others; participants who left high school prior to Year 12 also accessed specialised services more than others; Aboriginal and Torres Strait Islander participants accessed both types of services more than others as well as seeking help from family/friends and other community services.
Migrant participants less often sought support from services compared to others.
Barriers to help-seeking
Participants who had used IPV and/or SV identified barriers to seeking help for their behaviour (Table 29). The most named barriers were as follows: feeling ashamed (41.4%); belief that violence is a normal part of a relationship (34.7%); access challenges (34.7%); concerns about confidentiality (29.3%); lack of awareness of services (23.9%); communication issues (22.1%); and not having the time to talk to someone (15.9%).
Table 29: Proportion of people who use violence who identify barriers to professional help-seeking (n=553)
| Barriera | n (%) |
|---|---|
| Shame | 229 (41.4) |
| I feel too ashamed to talk to anyone | 143 (25.9) |
| I don’t want to talk to anyone about my behaviours; it is too personal | 134 (24.3) |
| I don’t feel deserving of help | 97 (17.5) |
| Normalisation of violence | 192 (34.7) |
| My behaviour is just a normal part of relationships. I don’t believe there is any need to see a professional about them | 141 (25.5) |
| My behaviour was a once-off. It won’t happen again | 113 (20.5) |
| Access challenges | 192 (34.7) |
| All available services are too expensive | 164 (29.7) |
| No access to transport to see someone | 80 (14.5) |
| Confidentiality | 162 (29.3) |
| My friends or family will find out | 128 (23.2) |
| The professional will tell others | 87 (15.7) |
| Lack of awareness of services | 132 (23.9) |
| I don’t know of any service that might be able to help | 132 (23.9) |
| Communication | 122 (22.1) |
| The professional will not understand me | 122 (22.1) |
| Low priority/lack of time | 88 (15.9) |
| I have no time to talk to someone about these things | 88 (15.9) |
| Total participants who needed help and were unable to get it | 161 (29.1) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses, maximum missing n=1.
a Barrier defined as those options that participants said were “Moderately important”/ “Very important”.
Among the 161 participants who had never sought advice or support for their behaviour in the past, the three most common service barriers they identified were a lack of awareness about available services (68.3%), the cost of services (62.1%) and long waiting times (59%; Table 30).
Table 30: Proportion of people who use violence and the service barriers that prevented their access to services (n=161)
| Service barriers | n (%) |
|---|---|
| Lack of awareness of available services | 110 (68.3) |
| Cost of services | 100 (62.1) |
| Waiting time too long | 95 (59) |
| No service available in the area at the time needed | 92 (57.1) |
| No private health insurance | 91 (56.9) |
| No appointments | 90 (55.9) |
| Limited opening hours | 84 (52.2) |
| Not taking new patients | 79 (49.1) |
| Concerns regarding confidentiality | 79 (49.1) |
| Language or translation problems | 40 (25) |
Notes:
392 participants were skipped from this item because they had not been in the situation of needing help and being unable to get it.
Denominators vary due to missing responses; maximum missing n=1.
Journeys to help-seeking
In this section we expand on the above survey findings to explore the findings from our interviews with eight people who acknowledged that they had used abuse or violence towards a partner. The research question that guided this part of the study was “What are people’s journeys in engaging with help for their use of IPV and/or SV?”
The interview participants were all male and aged between 43 and 71 years old, with a median of 55 years. Three were from Victoria, three from New South Wales and two from Western Australia. Three were born outside Australia (in India, the United Kingdom and Sudan). All identified problematic behaviour in relationships with female partners. In their previous survey responses, six of the participants said a partner had been afraid of them; four said they had continuously contacted or followed a partner; four had made threats to harm a partner; three had forced a partner into sex; and two said they had shaken, thrown, pushed or grabbed a partner. In their interviews, four said their partner had contacted the police about their behaviour and three of them had been subject to a protection order. Two were still in their relationship and six were separated from their partner.
The interviews with participants focused on their journeys engaging with help and support for their abusive behaviour. We undertook a thematic analysis of the interview data to help understand how they experienced this process of help-seeking. We begin by discussing the central theme in their stories that reflects their overall experience of seeking help to address their behaviour. We then provide three case studies from participants in order to illustrate this central theme. Following this, we discuss the key stages and turning points in participants’ journeys of engaging with help for their use of IPV and/or SV.
Central theme: Releasing emotions and regaining stability
In their interviews, all of the participants emphasised that they did not have disrespectful attitudes towards women and most claimed that they had never been physically violent. However, most did acknowledge using some form of problematic behaviour in their relationships. Some described their behaviour as “psychological aggression” or “emotional abuse”, while others spoke of their “anger” towards their partner without identifying what this meant in terms of their behaviour. A common belief among participants was that their abusive or violent behaviour did not reflect their conscious choices or their character, beliefs or attitudes. Instead, they suggested it was responsive and caused by strong emotions that had led them to temporarily lose control over their behaviour. They spoke of being overcome by anger (for example, one said “I couldn’t control my temper” [Participant 9]), powerful sexual drives and mental distress or illness (forinstance, one associated his violence with being “mentally unwell” and said it “felt like someone else had taken over my body”[Participant 2]). Some also indicated that a lack of sleep, high blood pressure and/or alcohol use had contributed to their actions.
Thus, based on the perceptions and experiences of participants, a central theme was that to stop their abusive behaviour they needed help to release their emotions and regain emotional stability. They suggested that what assisted them to not “bottle things up” was talking to counsellors and others, getting the right medication for their mental health, doing regular exercise and improving their physical health. The following three case studies illustrate this central theme in participants’ stories.
“I’ve just got to look after myself”: Brett
Brett explained in his interview that his job had been extremely stressful, and that he had developed PTSD as a result of his work. He said he could not sleep and was in “a mentally dark place that I just couldn’t … I didn’t have control of my emotions. I couldn’t control myself. So, my ex would always be walking on eggshells not to just disturb me.”
Brett said his employer gave him time off and pushed him to see a psychiatrist. He found it “cathartic” talking to professionals about his distress; however, at that stage, his medication was not working, and he was still “angry all the time” and “unbearable” to be around. His partner told him he needed to go to hospital and got him admitted. However, Brett said: “I tried to do the things that she asked me to do, but in the end it wasn’t enough.” Being hospitalised increased his anxiety and he did not feel comfortable to engage in therapy while he was there. His partner ended up leaving him, taking their children. Brett said: “On top of losing my family I lost my home, I lost my job, I got arrested many times and put through the court process … and I wasn’t allowed to see my [child] for some time.” His partner took out an intervention order and “was alleging all sorts of things that weren’t true”. Due to her allegations about himbreaching the order, he was mandated to attend a men’s behaviour change program. However, Brett said the program did not help. He said the other men in the group had disrespectful attitudes and “were all there because they’d punched the shit out of their missus or destroyed property”, and Brett felt he was different to them.
Brett said once he got the right help and felt motivated to change, things got better: “The medication started to work, and I felt more comfortable talking to [my psychiatrist and psychologist] … they help to guide you in the right direction. But, yeah, you’ve got to want to do it. If you don’t want to do the effort, put the effort in, nothing’s going to change.” The thing he said really helped his mental health and behaviour was getting physically fit:
Exercise is the thing that pushed me back [onto the right path]. So, when I don’t get it, through the lockdowns and all the last couple of years I couldn’t go to the gym, that was a fairly dark period. But now that we’re over them and I’m able to go to exercise … I’m fairly stable … I’ve just got to continue to look after myself.
“Someone I can talk to …instead of bottling it up”: Amar
Amar acknowledged that his partner had been afraid of him. In his interview he explained that a major cause of arguments was his wife’s reluctance to have sex after she had a baby:
I was in my prime, you know, raring to go all the time. That was a major problem … I pride myself on not going anywhere else but to my wife … But in saying that, I hurt myself doing that … it affected our relationship where I just tried to put the hard word on my wife all the time. She didn’t want it and we argued about it.
Amar said that what increased the conflict in his marriage was that he had suffered a “breakdown” because of work-related trauma. He left his job but struggled to find a new one because of the medication he was taking for his mental health. He said not being employed was difficult and caused arguments with his wife, because he had been brought up to believe “I should be the one earning the money”. He said he needed understanding and comfort from his wife but was not receiving it: “I just wanted to feel loved … I wanted my wife to cuddle me and have sex with me … I needed relief.”
Amar said he could not talk to his family because they thought he was “an asshole” and his child “thought I was being nasty on purpose to my wife”. He found it “embarrassing” to seek help because people would think “You’re a man … [so] harden up.” He became depressed and suicidal, and “ended up in a psychiatric ward … because I just couldn’t take it.” He found being hospitalised was a relief because he “didn’t have to worry about anything”. Amar said the main thing that had helped was finding a psychologist. The psychologist enabled him to talk freely and honestly because he did not feel judged: “He’s someone that I can talk to … instead of bottling it up… he knows everything about me. I don’t have to hide anything … because there is no ‘wrong way’ because it’s not against him.” He suggested that being able to release his emotions in counselling has prevented him from taking them out on his wife:
I tell [my psychologist] exactly how I feel … what I feel like doing. So, yeah, he knows a lot, and he has helped me because … it takes a lot off my mind when I talk to him about things, because now I think, well, I’m not going to go home and bottle it up … and then one day she may not put enough sugar in my coffee or something, and I’ll spit the dummy and let it all out … and have a go at her, you know. I don’t want to do that.
“I’ve emptied myself of all that hate and darkness”: Aaron
In his interview, Aaron spoke of the stress of his job and said he suffered work-related trauma and an assault during his employment. He explained that he had “carried” that trauma into his relationship and it affected his behaviour: “I was very, very psychologically violent to [my first wife]. I mean, very scary … I mean, I never hit her or anything, but it was psychological violence.” He was drinking excessively to cope, but that only made things worse: “I was still bottling up all of the things that had happened to me so that was still being pushed down with alcohol, so that was fuelling things.”
Aaron said he kept “just losing it … just getting more, just angrier and angrier and angrier”. Yet he felt unable to seek help because his workmates would see him as “weak”. He also did not know what services were available. He would try to speak to his GP but said that “all they’d do is say ‘Oh, you’re an alcoholic’”. Things “came to a head” when he threatened his partner with a knife. His partner called the police and a CAT (crisis assessment and treatment) team, and he was hospitalised. However, Aaron said the psychiatric hospital was “horrible”. He felt they did not diagnose him properly and the nurses had “no compassion”; they treated him like a violent alcoholic who “should be in prison”. Aaron described feeling trapped in a cycle of medication and drinking, which he said only fuelled his poor mental health and aggression:
I just felt like I was losing control of everything, and I didn’t know where to go … I was trying and trying not to drink. I was going to AA and I just found that didn’t work. I was on the medications and that was working but it was like I just couldn’t – it was like I was unable to actually explore my own baggage and trauma.
He ended up leaving his wife as he was “confused” about his feelings towards her and feared doing something “beyond regrettable”.
Aaron said this cycle shifted when he met his new partner, who made him feel “loved for the first time” and offered “a bit more stabilisation” in his life. His partner found a psychologist who supported him to disclose and process the trauma he experienced:
I felt so comfortable with [the psychologist] and so trusting of [him], that then I was able to open up more to him, which – then I was much more able to open up to my wife … I’ve actually talked to him about all of the trauma that I suffered in the army. It’s like the whole – I don’t need to drink anymore because I’ve actually emptied myself of all that hate and darkness.
Since seeing his psychologist, Aaron says he has changed significantly. What helped was receiving ongoing emotional support, as well as being directly challenged and prompted to focus on his motivation for change:
We were talking the other day about how when I first started coming to see him and how angry I was and where I am now in relation to that. It’s like leaps and bounds. But that’s probably because [he] tell[s] me off as well. So … we talk about a lot of – what I want to achieve out of this. Otherwise … if you don’t want anything, why are you here? So [he’s] direct but at the same time he makes you feel very relaxed and open.
The three narratives presented above illustrate the central theme that reflects participants’ journeys of seeking help for their use of IPV and/or SV: “releasing emotions and regaining stability”. Each of the participants suggested that they suffered a build-up of mental distress and “lost control” of their behaviour. Participants perceived that what helped them regain control was medication, counselling and/or improving their physical health. Next, we will discuss the main stages and turning points across interview participants’ stories of getting help for their behaviour.
Key stages in participants’ journeys
By analysing how the interview participants described their abusive behaviour and their journeys towards change, we identified three stages: bottling things up; breaking down and letting things out; and regaining and maintaining emotional stability. Figure 16 provides an illustration of these stages and the key turning points in participants’ journeys.
Figure 16: Key stages and turning points in participants’ journeys of engaging with help
Text version of the figure above:
- Bottling things up
- Relying on partner for comfort
- Using alcohol
- “Anger” and aggression towards partner
- Feeling embarrassed to seek help
- Breaking down and letting things out
- Mental health and intervention and/or medication
- Police or court intervention
- Engaging in counselling and talking to others
- Regaining and maintaining emotional stability
- Looking after own physical and mental health
- Releasing and self-managing emotions via talking/counselling
Before step 1 to step 1
- Poor mental health due to stress, trauma and conflict
Between steps 1 and 2
- Abusive behaviour escalating
- Partner calling police or mental health service or ending relationship
Within step 2
- Trusting others and opening up
- Recognising unacceptable behaviour
Within step 3
- Keeping behaviour under control
Bottling things up
Participants suggested a build-up of stress, poor mental health and conflict in their lives and relationships had triggered their abusive behaviour. Four said they had suffered work-related stress, or a traumatic event related to their employment, and two said abuse they experienced during their childhood had resurfaced and affected their mental health. Some also indicated their partner had also contributed to conflicts and stress, because they were depressed, “hot tempered” or “antagonistic”, or refused to have sex with them. Two said their partner was emotionally or physically abusive towards them.
Participants spoke of “bottling things up”, “pushing things down” and/or using alcohol to cope with the mental distress they were experiencing. At this stage they did not seek help, either because they were so mentally unwell that they could not recognise their behaviour as a problem, they did not know where to turn, or they felt too embarrassed to talk to others. Being a man was described as a barrier to help-seeking as they felt they were expected to be “hard” and not express vulnerability. However, they suggested they believed they ought to be able to rely on their partner for emotional support and/or sexual comfort. Several expressed disappointment or resentment that their partner had not understood their suffering or had been unavailable due to her own problems (for example, one [Participant 2] said his partner became “a zombie” because she was taking medication for post-natal depression).
Breaking down and letting it out
Most participants said their engagement with services only occurred after they had reached a crisis point. The crisis was a mental health “breakdown” and/or their partner leaving them and taking their children. During this time, participants appeared to be motivated to engage with service providers to alleviate their mental distress. However, most did not instigate the help-seeking process themselves. Instead, the catalyst for their engagement with services was their partner/ex-partner ending the relationship and/or contacting police or mental health services about their behaviour. Four of the participants (including Brett, Amar and Aaron, as described in their case studies) spoke of being hospitalised after their partner had contacted mental health services or police. While they did not always perceive the intervention of mental health services as helpful, it opened the door to acknowledging their problems and gaining an understanding of theunderlying causes of their distress.
All the participants said they eventually found someone who gave them effective support. This source of help was a psychologist (for three participants); a GP (two participants); family and friends (two participants); a new partner (one participant); and a men’s health support group (one participant). What they said was important was receiving a non-judgemental and compassionate response and being able to develop a relationship of trust over time. Participants suggested such responses enabled them to “open up” and “let out” their emotions, rather than bottling them up and taking them out on their partner. They felt that releasing their feelings and getting the right medication and/or insight into the underlying causes of their problems improved their mental health and helped them change their behaviour towards their partner. Some said they also valued being offered advice on how to manage relationship dynamics, being challenged about theirbehaviour and being guided to focus on what they wanted to change in their life and their relationships (as illustrated in Aaron’s case study). The responses participants found unhelpful were immediately being made to feel criticised or judged, such as professionals labelling them a “violent thug”, or police or family courts automatically assuming that men are the abusers in relationships while women are not.
Regaining and maintaining emotional stability
Once they had recognised their emotional problems and found the right help, participants focused on “stabilising” themselves and keeping their mental health and emotions under control. They suggested this required continuous self-management. Participants (as illustrated in Brett’s case study) spoke of the importance of keeping up with exercise, doing yoga, eating healthily and getting sleep to prevent having further problems. For some (as described in Amar and Aaron’s case studies), supportive professionals played an ongoing role and they voluntarily returned for support whenever they needed help to maintain emotional control. For instance, one participant said:
If I cannot control the situation … then I go to see [my GP] … [he tells me to] keep out of the area … and go inside somewhere where nobody can disturb you … watching TV or listen to music … and your rage or anger will cool down. (Participant 8)
In this section, we have presented data from interview participants about how they perceived their use of IPV and/or SV and how they sought help over time to change their behaviour. In the discussion section of our report, we consider participants’ perceptions and experiences in light of current research evidence about how behaviour change occurs, including the importance of shifting the gender-based beliefs and attitudes that underpin the perpetration of IPV and/or SV.
The next section specifically looks at help-seeking during the COVID-19 pandemic by participants who used IPV and/or SV.
The impact of the COVID-19 pandemic on help-seeking
We also asked survey participants what impact, if any, the COVID-19 pandemic restrictions had on their access to support services for their behaviours in intimate relationships. Many said it had not impacted them or that they did not need to use support services. Others noted that it had altered their engagement with services.
It made getting support harder
A major theme was that it had been more difficult to access support services during the pandemic. Participants said they were unable to visit a professional in person because of restrictions or long waiting lists for counselling support. For example, one stated: “[My] psychologist was heavily booked throughout lockdown, so I wasn’t able to see them as often as I needed to.” Several commented that they missed out on accessing group-based programs; for instance, one said “I … wish that there were face to face support groups operating as it’s been very isolating.”
A number of participants described a lack of comfort engaging with services that were only offered via phone or online. They suggested that compared to face-to-face interactions, telehealth delivery felt impersonal, “distant” and “disconnected”. For example, one said:
Back when COVID-19 first came to fruition my weekly appointment with my drug and alcohol and relationship counsellor went from being face to face to over the phone. It never felt anywhere near as beneficial as my face-to-face appointments and as a result I stopped seeing them.
Participants said it was “tiring” and “harder to explain things” and they needed physical closeness to the service provider to “feel okay about being vulnerable”. For instance, one said in-person conversations “feel a lot more authentic/of value”, while another said telehealth counselling “doesn’t have the same impact as being in the same room”.
A lack of privacy at home was a key concern that made participants reluctant to use telehealth services:
I wasn’t comfortable with video chatting/phone calls during lockdown as it put me in earshot with my partner or neighbours.
It has made it more complex to access services in private, as I share a house with other people I don’t have complete privacy.
Greater convenience and awareness of services
For some participants, telehealth during the pandemic meant support services were more convenient to access. Participants said they appreciated not having to travel or being able to access services in other cities. For example, one said: “I actually quite enjoyed [counselling via telehealth], because we don’t have a car at the moment, so transport is sometimes an issue.” Another said they appreciated that “services in other cities or countries can be accessed from anywhere”.
Another benefit was that support services were more prominently advertised during the pandemic:
It made things easier! And a lot of services are getting heavily promoted which raises awareness of their existence.
Summary
Survey participants who had used abuse or violence mostly sought help from their friends, family members or partners, followed by a health professional. More often than not, they rated the informal or formal support they had accessed as helpful. Barriers to help-seeking included shame, the normalisation of violence, access challenges and confidentiality concerns. Some participants were unaware of services that could help or said they lacked access to affordable, available services. Our interviews with eight participants provided more detailed data about the help-seeking over time of people who had used IPV and/or SV. While most interview participants admitted using problematic behaviour in their relationships, they often minimised it as “anger” or said they were emotionally abusive but not physically violent. They suggested that strong emotions or poor mental health had led them to temporarily lose control over their behaviour, and a key theme wasthat they needed help with releasing their emotions and regaining control. We identified three key stages in how they described their journey to engaging with help: bottling things up; breaking down and letting things out; and regaining and maintaining emotional control. Our survey data from participants who used abuse or violence indicated that the COVID-19 pandemic made it more difficult for many to access support services to address their behaviour. However, for some participants, it had no effect or made it more convenient for them to seek support through the use of telehealth or online service delivery.
3. Support needs of people who use violence
This section integrates the survey findings and the qualitative findings on support needs from the perspective of people who use violence.
What do people who use violence value in a service?
For the 408 participants who had spoken to someone in the past, they most valued the following: learning new ways of dealing with relationship problems (92.4%); feeling listened to (91.9%), and the expertise of the professional (91.2%; Table 31).
The next section draws on qualitative data from the survey.
Table 31: Proportion of people who use violence and what they value most in a service (n=408)
Emotional support
| Service values | n (%) |
|---|---|
| Feeling listened to | 375 (91.9) |
| Knowing that my story would be held in confidence by professional | 357 (87.5) |
| The professional being interested in who I was as a person | 350 (85.8) |
| Not feeling judged or put down | 349 (85.5) |
| Having someone to talk to | 345 (84.6) |
Professional competency
| Service values | n (%) |
|---|---|
| The expertise of the professional | 372 (91.2) |
Practical support
| Service values | n (%) |
|---|---|
| Learning new ways of dealing with relationship problems | 377 (92.4) |
| Given practical information about how to increase safety | 359 (88) |
| Material support (e.g. getting access to accommodation) | 255 (62.5) |
| Other (participant open-text suggestions) | 15 (3.7) |
Notes:
Values are numbers (percentages) unless otherwise stated.
Denominators vary due to missing responses; base = all participants who responded to survey item.
155 participants were omitted as they had never sought advice or support.
Support needs and expectations of services
In this section we draw on qualitative data provided by participants, in answer to the following four open-ended survey questions about their support needs and expectations:
- What do you think you need the most to stop using violence and abuse?
- What do you think your greatest need is from a service or professional?
- What do you believe that professionals need to do differently to better help people in similar situations as you?
- I wish that service providers …
We combined the data from the questions in developing our analysis of the support needs of people who used IPV and/or SV. In analysing participants’ responses, it was evident that many did not see themselves as needing support for their use of violence or abuse as they did not wish to characterise themselves in this way. This was despite them having identified using forms of violent or abusive behaviour in other parts of the survey.
For participants who did acknowledge needing to address their use of violence and abuse, we identified three themes relating to their support needs: “Help to regain emotional control”; “Hear me and talk to me, not at me”; and “Help me see things from a different perspective”.
Help me regain emotional control
A common theme among participants was that their violence or abuse was caused by problems controlling their anger or other emotions. Many participants expressed this belief, including those who identified having used forms of physical and/or sexual violence, as well as psychological abuse or monitoring behaviours, such as following or continuously contacting a partner. Consequently, help with emotional regulation or “anger management” was seen as a key component to stopping their behaviour. For example:
I need to be more patient and be of low temper.
[I need] learning [on] how to deal with my own emotions and keep them under control.
I get frustrated/angry quickly over very minor things. Having a couple of drinks which really helps in reducing those outbursts but it is a really unhealthy pattern that is upsetting to both me and my partner. It also can lead to excessive drinking. I need help in breaking that chain and control my frustrations better.
I need [services] to help me manage my emotions and prevent them from getting to an uncontrollable state.
While some indicated poor anger control was part of their personality, others suggested that it was because they were dealing with difficult external circumstances. For example, to stop their abuse, one spoke of needing to “reduce stress from work”, and another said: “I think I need to be balanced financially, lack of finance makes me angry because it makes me feel less like a man.”
There was considerable interest among participants in receiving counselling to help process, release and regulate their emotions. For instance:
[My greatest need is] emotional support … I know my unhealthy behaviours and it is when I feel compelled to react to deep feelings of shame, insecurity, fear or pain that I would like support to process those deep feelings.
[I need] techniques on how to actively dissipate feelings of anger or frustration.
They also spoke of a need for “coaching” or guidance on how to improve their communication and reduce conflict with their partner. For example, one said: “[My greatest need is] learning skills to de-escalate an argument with my partner (i.e. moving into another room, tone of voice etc.).” Another said lessons in effective communication would help to stop a build-up of anger: “Being taught to be able to communicate what is bothering me in an effective manner [would help] so I don’t bottle it up and then explode.”
Many participants suggested that an underlying mental illness (such as anxiety, depression, or PTSD) made regulating their emotions difficult and caused their abusive behaviour. Thus, a frequent comment was that they needed professional treatment for their mental health problems in order to improve how they treated their partner. Many spoke of needing a diagnosis, medication and/or therapy:
[My greatest need is] regular sessions with my shrink to help me deal with my PTSD. My negative behaviours towards partners are, generally, unintentional and reactionary to PTSD.
[My greatest need is] a combination of therapy with an increase in daily stimulus for my mind. During the pandemic I became increasingly aggravated at the smallest components due to depression and under-stimulation, which is a difficult combination to overcome.
[My greatest need is professional help] dealing with anger and past trauma from the army.
Possibly [I need] a diagnosis of ADHD and then help to prevent my quickness to anger.
I’m on tablets now which are great, I don’t swear, yell or do anything.
However, there were other participants who suggested they could manage their emotions without external help. By far, the most common solution was to calm down by taking a break or “walking away” when they had conflicts with their partner. Another solution was to improve their general physical and emotional wellbeing so they could be more emotionally balanced. Participants identified various strategies they needed to use to increase their wellbeing, such as meditation or relaxation exercises, seeing friends, and going for walks. Reducing alcohol or drug consumption was also perceived to be helpful in regaining control. For example, one participant’s greatest need was:
Zero alcohol consumption, and a dedication to actually reading the one single quote that is 100% relevant, each and every morning. Even several times a day, as it is inspirational.
Help me see things from a different perspective
The second theme among participants’ responses was a need for a new way of thinking. Some said they wanted someone to teach them what a healthy relationship looked like and how to recognise their problematic behaviour. For instance:
[I need] explanations of poor behaviour and guidance for improvement and change.
[My greatest need is] having some sort of mentoring so that you can differentiate between right and wrong.
[My greatest need is] having a safe space to talk out my thoughts and feelings … to help me understand, see things from a different perspective and hopefully learn, grow and change my behaviours.
As well as help to identify poor behaviour, they also wanted support to understand their partner’s perspective. For example, one said:
[My greatest need is help to] learn how to regulate my own emotions, be responsible for my own actions and have better empathy/do a better job of perspective taking for my partner. Professionals that were non-judgemental and empathetic, but able to challenge me, have been really helpful.
Only a small number of participants indicated that they needed help to better understand how their behaviour was connected to gendered beliefs and attitudes. For instance, one said his greatest need from professionals was to help him understand “How are we supposed to be a man?”, because “Being respectful, and treating people equally can be a lonely path … In many settings, men are still required to ‘man up’, which seems to mean suppress your emotions, and stick to your guns”. However, most did not explicitly connect their behaviour to beliefs about masculinity or attitudes towards women. Despite this, a number of participants did refer to a need for help to change their “way of thinking” or their “mindset” in relation to how they thought about or valued their partner. For example:
My greatest need from a professional right now is for that person to listen to me and help me reshape the way I look, think and approach my wife and partner. I need advice on how to handle myself when I meet certain difficult situations in my relationship.
[My greatest need is] an effective way to control my mindset, so that any temptation to do “the wrong thing” can be shrugged away without too much effort.
I think I have to be shown ways to appreciate my wife rather than see her bad sides or flaws.
As is evident in some of the quotations above, several participants emphasised that in order to reflect on and change their perspective, they needed to feel the professional provided a “safe” or “non-judgemental” space for such a conversation. This need is discussed in the next theme.
Hear me and talk to me, not at me
An important theme that cut across participants’ responses was a need for a conversation with a professional who would listen and try to understand, rather than judge. This theme was encapsulated in the response of one participant, who said their greatest need was “to have someone hear me and talk to me, not at me”. Similarly, another said, “[My greatest need is for a professional to] be understanding and unpatronising and really just listen and provide good advice.”
Many felt that openly sharing their experiences and feelings with a counsellor could help them to explore what was causing their behaviour:
[My greatest need from services is for] understanding and compassion as well as strategies to find the root of the issues.
I have felt for a long time that I would most benefit from an open and honest conversation about my past with a professional therapist. [It] would help me process my experiences and actions, understand the factors that led to them, and ensure that they never happened in the future.
In order to open up, participants said they needed a professional who was approachable and non-judgemental. For instance, one suggested service providers should “make the atmosphere more friendly … first do some warm-up so that the patient can feel relaxed talking to the professional”. Others spoke of the importance of being reassured that the conversation would be confidential:
I would most value not feeling judged or intimidated by the professionals. This might mean being confident in the confidentiality of the session and also speaking to them in an informal setting or manner.
Participants frequently expressed uncertainty about whether professionals would report what they said to others and wanted clear confidentiality guidelines to help them feel comfortable to seek support. For instance, one participant said: “[I need] professionals to show more evidence that they will not disclose my private information.”
As well as wanting to be listened to, rather than talked “at”, participants also spoke of needing professionals to get to know them “as a person”. Many spoke of not wanting service providers to make assumptions or to offer “standardised” or “textbook” responses. For example:
The professionals need to understand that general advice may not be suitable in every case. There are different societal and cultural practices that must be taken into consideration when offering solutions.
I think some professionals need to take each person as having their own unique circumstance … Whilst it is beneficial for them to take their learnings and knowledge from other patients – it should never be the sole focus or influence decisions too heavily.
Similarly, some said they did not want professionals to automatically assume they were the problem:
[I wish that service providers would] not presume that I am at fault. Understand that people who feel hard done by often actually are.
Several expressed a wish for services to “understand men” better and not “stigmatise” them or push a “gender narrative” about the causes of abuse. For example:
[I wish that service providers] understood the problem is not always with men even if we are more likely to get violent.
Some felt gendered assumptions about men as abusers were barriers to seeking support:
One thing I believe would help is for professionals to be able to let men know they differentiate these types of experiences. I know of friends who wish to take similar proactive steps in changing their way of dealing with anger but, because of the stigma that domestic violence rightly has attached to it, feel they will get quickly identified as an abuser and not as someone who is actively trying to make themselves a better partner.
The next section explores the role of family and friends.
Role of family and friends
We asked people who used abuse or violence to provide their written responses to the survey questions “I wish that my family …” and “I wish that my friends …” The questions followed others about their use of abuse and violence, and we instructed participants that they should think about their relationship with their partner or ex-partner in answering the questions about what they wished for from family and friends. It was not always clear whether their survey responses were referring to how they wished their friends and family could respond to their use of abuse or violence or to general relationship or personal concerns. However, the data we collected from the survey provide a broad indication of how participants saw the role of family and friends in responding to intimate relationship issues. Based on our analysis of their responses, we identified the two themes: “Be willing to engage in a deeper conversation” and “Listen with an open mind”.
Be willing to engage in a deeper conversation
The main theme evident in participants’ responses was a wish that family and friends were more interested in having meaningful conversations about relationship or personal problems. For example, some wished their friends were more prepared to have emotionally supportive conversations:
I wish that my friends were more available and willing to have an emotional discussion about our vulnerabilities, to build a stronger deeper friendship.
I wish that my friends were more authentic and supportive, rather than only contacting me when I’m needed. I wish my friends would check up on me more often, especially since they know about my past mental health problems.
Others spoke of wanting greater engagement from family members. For example, one said: “I wish that my family can communicate with me deeply more often”. However, participants frequently suggested that their family and friends were not comfortable having serious conversations about relationships, emotional issues or sex. For example:
[I wish my friends] will learn to stop joking about everything.
[I wish that my family] didn’t make talking about sexual relationships taboo.
[I wish my friends] were more willing to talk about sexual violence and our role as men in preventing it.
Some indicated their family or friends did not know how to help and gave dismissive or unhelpful responses.
I wish that my family knew better how to respond to mental health/family violence/substance use issues. I wish they had taken my partner[’]s concerns more seriously and been far more proactive in reaching out to support her once I came clean to them about what had been going on.
[I wish my that family] had spent more time discussing feelings and how to cope with them, and not disregarded them or told me to “stop”.
Listen with an open mind
A second theme was the wish that when participants discussed relationship issues with family and friends they would have an open mind and try to understand, rather than responding with judgement or unwanted opinions. Participants frequently said they wanted family and friends to be more “neutral”. For example:
I wish that my friends who my wife has turned against me would realise that there are two sides to every story and give me a chance to explain to them, the other side.
I wish that my family would not make an uninformed judgement on my relationship and actively listen without bias. I wish that they would check in with me more to provide basic emotional support.
Many also expressed a wish that family and friends were “better at listening than giving advice”. For example:
[I wish that my family] would try to understand where I am coming from in any given situation before pushing their views on to me. Have more of an open mind.
[I wish that my family] would listen instead of trying to downplay a lot of what is being said to them. My issues are never big problems in their eyes and I always get a response like “you will work through it” or “I know someone who has it worse”. It isn’t helpful.
As well as receiving unsolicited advice, some participants did not like receiving unwanted interventions from friends or family. Several said they wanted friends or family to “respect boundaries” or stop “interfering in a negative way” in their relationships. For example:
I wish that my family keep their noses out of my business.
I wish that my family would stop judging and prying into my life.
In summary, our analysis of survey responses suggested that people who use IPV and/or SV are often interested in having in-depth conversations with their family and friends about their relationships and would like family and friends to listen with an open mind. Such conversations could potentially play an important role in helping to identify abusive behaviour and to support people on a pathway towards change. However, our findings also suggest that many people who use IPV and/or SV find it difficult to engage their family and friends in serious discussions and may receive responses that they perceive as dismissive or unhelpful.
Victims’ and survivors’ perspectives on helping people who use IPV and/or SV to stop
In this section we explore what helps people to stop using IPV and/or SV from a different viewpoint. We return to the survey data from victim and survivor participants to explore their experiences of their partner or ex-partner’s abuse and what had helped or would help to end it. We asked women victim and survivor survey participants to provide written responses to two questions: “If you think about your partner’s/ex-partner’s behaviours towards you, what do you think has been most helpful for your partner in helping them to stop using violence and abuse?” and “If you think about your partner’s/ex-partner’s behaviours towards you, what do you think your partner might need that would help your partner stop using violence and abuse?” We identified three key themes based on their responses to the first question: “Nothing was helpful”, “Removing myself” and “A fear of the consequences”.
Nothing was helpful
The predominant theme among participants was that nothing had helped their partner/ex-partner to cease their abuse. Participants typically expressed a deep pessimism that their partner/ex-partner would ever change. They frequently commented that the main problem was the perpetrator’s refusal to accept their behaviour as abusive. For example:
He doesn’t see he has a problem.
He thinks he’s the victim in it all.
Although some women believed that therapeutic approaches such as counselling or drug/alcohol programs had been helpful for their partners, many stated that their partner/ex-partner had resisted attempts to engage them in treatment or therapeutic interventions, even when they had been legally mandated to do so. For example, one said: “I had two IVOs [intervention orders] which he totally ignored … and he was apparently told to do an anger management course which he did not do.” Another participant similarly described: “I tried for two-and-a-half years in my court orders for him to do a Men’s Behavioural change program but he didn’t want to, so he didn’t.”
Others observed that even though their partner had attended treatment or had been subjected to legal intervention, it had failed to curb the abuse.
He went to rehab 3 times while we together purely to stay out of jail. I have a FVRO [family violence restraining order] in place, he’s breached it many times.
Some women felt that their partner had been able to trick service providers into believing that they had changed, or that their behaviour was less serious than it really was:
He sees psychologists and a psychiatrist who he doesn’t tell the full story around our separation to … so, he’s getting no help at all.
He did a men’s behaviour program and manipulated them.
Some women observed that the perpetrator’s behaviour had continued after they left the relationship or that the only thing that had altered was the type of abuse they used: “The abuse and violence has not stopped it has simply changed into systems and legal abuse and it continues today.” Participants also noticed that the perpetrator had then redirected their abuse towards their new partner: “He re-partnered 4 weeks after I finally left him and he’s the same with her.”
Removing myself
Although for some participants, leaving the relationship failed to stop their ex-partner’s abuse, for others, leaving reduced the abuse. While these participants observed that ending the relationship did not cause the perpetrator to change their mindset, it did mean that the perpetrator had fewer opportunities to target them:
I had to remove myself. One partner stalked me for three years till I left the country.
Me leaving [stopped the abuse] … he is still the same person as he was back then though … He still blames me for his abuse during our marriage and now he tries to undermine me to our children. But at least now I am not living with it daily.
The only thing keeping me safe is that he lives in another state.
I got rid of him – that is probably the biggest opportunity for him to decide to face himself – and get some help – but alas he has ignored this opportunity.
A fear of the consequences
Some participants indicated that legal responses such as police intervention or protection orders had been partially effective in reducing their partner or ex-partner’s abuse. For instance, one said: “Family court orders and the FVO [family violence order] have stopped his violence and abuse for the most part. It continues in other, less overt ways.” Another said: “Putting him in jail … but even that didn’t stop him until the 3rd time.”
Women commented that the major deterrent for the perpetrator after police intervention was the threat of further negative consequences, such as the loss of freedom or reputational damage:
Police intervention and threat of losing his job and reputation.
The threat he will go to jail next time he steps over that line. His fear of the consequences and Court.
Me telling him I will get an in-house AVO [apprehended violence order] on him. He cannot allow others to think he’s a monster.
Victims’ and survivors’ views on what would help stop the perpetrator’s abuse
In this section, we will discuss the key themes from our analysis of participants’ responses to the second question about what might help their partners.
As outlined in the previous section on victims’ and survivors’ survey responses on what had helped their partner/ex-partner, when asked about what they might need, many participants expressed great pessimism about their partner or ex-partner’s ability to change. This was reflected in comments that the only thing that would stop the abuse was if the perpetrator disappeared. For instance, some responded that what their partner/ex-partner needed was “a bullet”, “castration”, “a lobotomy”, and one commented that “his death is when the abuse will stop”. While we recognise and acknowledge these sentiments, in this section, we have focused on the other suggestions women made to help the perpetrator stop using violence.
A wake-up call and retraining
Many victims and survivors indicated that their partner or ex-partner refused to accept that they were abusive or violent. Thus, a major theme was that the perpetrator needed someone who could make them recognise that their behaviour was unacceptable and change the thinking and beliefs that underpinned it. For example, participants said the perpetrator needed:
… a wake-up call. He thought he was a victim because he couldn’t get us to do everything he wanted.
Some kind of wake-up call that would show him what an asshole he is when he drinks.
To be called out on their behaviour and shown the right way to treat a person.
Victims and survivors indicated that they were not in a position to be able to change their partner’s/ex-partner’s beliefs or behaviour. Instead, they needed someone external to them who had greater influence or power. They suggested male friends, professionals, community members and others who their partner or ex-partner respected and who could play an important role in calling out the problematic behaviour and attitudes. For example:
Perhaps if he had a male friend who could make him aware of his behaviour and lack of respect for women.
He needs to listen to a professional and get help as he thinks he is self-righteous and never wrong.
[What might help is] having people who he trusted or looked up to talk about his behaviour and its consequences.
[What might help is] being told by male health professionals and friends he respects that it is not okay.
[What might help is] more ads on TV supporting people calling out bad behaviour.
Participants also highlighted a need for intensive education programs to transform perpetrators’ beliefs about gender roles and relationships:
[He needs] MASSIVE retraining, addressing personality issues and his belief that he has the right to whatever he wants from his partner.
[They need] a course in how to treat a partner properly and therapy for their abuse as a child most of it is learnt behaviour, they need to be … taught different ways.
[They need] education that it is not ok to be controlling towards your wife.
“Intensive” therapy
Many participants suggested that significant personality and/or mental health problems contributed to the abuse or violence; however, their partner or ex-partner denied that they needed to seek help. Thus, a strong theme was that the perpetrator needed to be mandated or forced to engage in treatment or therapy and that any therapy needed to be intensive and ongoing. This was evident in participants’ comments that the perpetrator needed “strong”, “dedicated”, “extreme”, “serious”, or “continual” therapeutic interventions or “forced mental therapy”. For example, participants said:
[He needs] intensive therapy … it appears that he might have PTSD from previous experiences and a previous job role.
If he were ordered not to behave in an abusive way to either of us and if he were to be forced to see a psychologist for his behaviour and mental illnesses (all of which he denies), perhaps he could one day become a healthy father.
Victims’ and survivors’ responses also indicated that they felt a complex array of factors contributed to their partner or ex-partner’s behaviour. Thus, they suggested that a multi-pronged approach that addressed a combination of contributing factors could be helpful. This might include education, therapy for mental health and drug and alcohol use, and/or family or couples’ therapy. Responses included:
[What might help is] serious counselling. Mental health assessment. Anger management. Drug and alcohol counselling.
[What might help is] regular psychologist sessions, space to talk and mediate as a couple, alcohol and drug support.
Participants also emphasised that for therapy or treatment to be effective, the professional would need to understand victims’ and survivors’ experiences, and have expertise in challenging problematic attitudes or behaviour:
[He needs] an experienced anger management psychologist, not some half-arsed Medicare subsidised counsellor who just enables his behaviours in a group setting and never hears the side of the victim!
[My partner needs] counselling but where the counselling knows both sides because an individual can sugar coat their behaviour.
Hold them to account
Most victims and survivors suggested they had little hope that change would emerge spontaneously from within the perpetrator. Thus, a significant theme was those with power or authority needed to intervene, hold the perpetrator accountable and impose restrictions and/or consequences for abusive behaviour. For example, some highlighted legal interventions:
[He needs] further police intervention. Harsher restrictions. Police actually following up on the breaches. Checking he is abiding by his curfew.
What is needed is for coercive control to be illegal and for me to report him and for it to be taken seriously and for him to be warned about his behaviour.
Others suggested a therapeutic approach might help if professionals held the perpetrator accountable for making changes:
[My partner needs] to be heard just like anyone else. To be given the opportunity to talk through their behaviour and to make the changes that are needed. Also given the consequences of their actions if that behaviour continues.
[What might help is] actually having consequences for his actions and some alcohol abuse help.
Others felt incarceration was the only thing that would be effective. This was not only because it would force the perpetrator to have to confront their abuse but also because it meant they were no longer able to target the victim and survivor. For instance:
A prison cell is about all that would work.
I’m not with him anymore but jail [would help] so he doesn’t come out to do it again.
Overall, our analysis of survey responses found many women felt disillusionment and despair about ever being able to end their partner or ex-partner’s problematic behaviour towards them. A frequent comment was the perpetrator had minimised or denied the abuse and was resistant to seeking help. Some reported that their partner or ex-partner had attended therapy, behaviour change programs or substance use treatment, yet most reported that these responses had been ineffective, often because the perpetrator had not been held to account for making changes. The responses that were perceived to have had an impact in curtailing the abuse were the victim and survivor leaving the relationship or threatening to involve legal authorities. Participants felt that their partner needed someone who could make them recognise their behaviour was unacceptable, and that intensive therapy might be required, while holding them to account.
Summary
From the survey, the support needs of people who use violence included emotional and practical support delivered by a professional who they felt was competent. Participants wanted help regaining emotional control, to see things from a different perspective and for services to hear them and talk to them, not at them. From family and friends, perpetrators wanted a willingness to engage in deeper conversations and listen with an open mind. From victims’ and survivors’ perspectives, nothing was helpful other than removing themselves from the perpetrator’s reach. They thought if their partner could fear any consequences for their behaviour, something that was a wake-up call might turn their behaviours around. Finally, intensive therapy, while holding the partners to account, might also be helpful to stop them using abuse and violence.
Part E:
Children’s experiences and support needs
This part highlights what participants said about their children from the perspective of those who experience or use IPV and/or SV. The data is drawn from the open-ended survey questions with 500 victims and survivors and 288 people who used IPV and/or SV.
Victim and survivor perceptions
Victims and survivors who participated in the survey were asked to write about what had helped their children. Specifically, the question asked: “If you think about your partner’s/ex-partner’s behaviours towards you and your children, what has been most helpful for your children’s needs?” Below, we present our analysis of the themes evident in participants’ responses to the question with supporting quotations for each. Overall, our analysis suggests that many women felt there had been little assistance given to their children and that they were their children’s primary supporter and protector.
“The system has failed my children”
A major theme among participants’ responses was that no one had helped to protect or support their children. Many expressed that the service system had failed to adequately protect their children from the harmful impacts of the perpetrator’s behaviour. Feelings of powerlessness, frustration and despair were evident in many comments:
There is NO help, my child is repeatedly stating his father is going to kill him. Despite multiple notifications, we are yet to get any help.
The system has failed my kids. The police has failed my kids. We live in fear.
The children have not been helped at all. So many services enable ongoing abuse of them and me through coparenting … Everyone has been enablers. They don’t care. My [teenage] daughter was nearly choked by her dad – we have an AVO and family court orders suspended. But there were so many red flags and no one cared. Our case presented as high conflict couple … yet contact was tripled [by the court].
Linked with this theme was a perception that police, child protection and the family courts did not recognise that children were negatively affected by a perpetrator’s abuse of their mother:
I feel at a total loss in the existing system about how to do what’s best for my children. Australian family law assumes that intimate partner violence is only experienced by the survivor and that if the perpetrator was never violent towards children, then the children don’t need protection from him. I have felt too afraid and disempowered to act in their best interests.
I was unable to protect my children from their father[’]s
using them as pawns to distress me by neglecting and mistreating them. Police weren’t interested. Family court couldn’t get him to engage in mediation/counselling so that was that. Child protection said 12 was too old. If they were 5 they could investigate.
It was really hard to get anyone to believe my ex-partner hurt my child. Whilst in family court he said he only hurt the child accidentally, as I was using them as a human shield (breastfeeding a baby he went to kick me and got the baby in the head, there were other times etc.). I came across as erratic, because I felt like no one was listening and they were putting my child in danger.
Several participants said they became estranged from their children because they were not supported to stop the perpetrator’s damaging behaviour:
Nothing has helped. All the professionals abandoned us and I lost my children to him. I was able to get my oldest back recently after many years of separation.
A perception that children had been failed by the system was not only connected to the responses of courts or authorities. Many also said their children had been let down by the lack of therapeutic support to address the traumatic impacts of the abuse they had experienced. Limited availability and the expense of accessing counsellors with expertise in working with children was a significant concern; as one said: “There are not enough psychologists around to see children, the wait times are huge.” One participant commented that after four years, her children were still on a waiting list to see a free specialist counsellor.
Another problem that participants frequently identified was that the perpetrator was legally allowed to block their children’s access to support:
I see a counsellor who supports me to support my children, as they are unable to receive any direct support themselves (their father blocks any access to support).
I would never have coped had it not been for my daughter’s child psychologist. However, her father withdrew consent for her to continue her services (after my daughter disclosed family violence).
Other barriers were confidentiality issues and organisational policies, such as a requirement that children be safe and not living with the perpetrator in order to access counselling:
Not much [has helped my children]. My son won’t speak to anyone because his psychologist told his dad what they’d discussed and people didn’t believe him. Kids Helpline did not respond well.
A social worker from The Australian Childhood foundation [has helped]. But they cannot help unless you are no longer living with the perpetrator. And no help if the children still see them.
A mother who can support them
Participants suggested that their children’s wellbeing and safety was closely connected to their own; for instance, one commented that, “When mums feel unsafe and traumatised, our kids do too.” Thus, a key theme was that the main thing that helped and protected children was their mother being supported and free from the abuse. Two sub-themes were associated with this theme: “Me protecting them” and “Me being validated and supported”.
“Me protecting them”
A frequent perception among participants was that their own protective actions had improved their children’s wellbeing and safety. Many highlighted their decision to leave their partner and how they had tried to establish a secure and calm home environment:
Leaving my ex-husband was the best thing that I ever did for the protection of my children … I am hoping that when they are adults, I can explain what happened, and they will understand why I had to get them out of that household.
[What was most helpful for my children was] leaving him. Although this has also meant additional difficulties such as me being blamed (in conversation with the children by the abusive partner) for everything in the relationship that was not good … it also enabled the children to see who could provide them with a clean home, good meals, positive support for schooling … to see the contrast between what he said was true and what the reality … Separating meant when the children were with me I could focus on their needs and care.
Participants also spoke of protecting their children emotionally:
Standing my ground that I am the best and most reliable person in their lives and doing whatever I could to ensure this continued. Being flexible when the father let them down – i.e. being available to pick them up or whatever, no matter what. Being entirely reliable and supportive while they were forced to experience his lack of reliability.
However, leaving the perpetrator was not the only protective response that participants identified. Some commented that the only way to help protect their children was to comply with the perpetrator’s wishes, even though this had meant making a considerable sacrifice themselves. Participants mentioned a variety of strategies they were forced to use to keep their kids safe, including obeying the perpetrator’s demands, remaining in the relationship, and leaving but allowing the perpetrator to keep custody of their child.
Staying in the relationship was best to protect my children and avoid losing them.
Probably most helpful thing I did for my son is that I left without him so that he is safe even though he is with my ex-partner. Let my son to be aligned with his dad so that his enemy is just me.
Keeping the partner happy helps to keep the kids safe too.
“Me being validated and supported”
Participants frequently commented that being supported as a mother and a parent was what had been most helpful for their children. They suggested that they were in the best position to assist their children, but they could only do so if they maintained their own wellbeing. For instance, one said having emotional support meant she was able to support her children: “[What was most helpful for my children was] someone to listen to me to help reduce my anxiety which gives me more resilience to help the kids.”
The responses that participants said helped them to help their children included being believed and having their parenting validated, and assistance with safety planning, finances and managing the impacts of the abuse on their children:
[What was most helpful for my children was] me being supported and believed. Having the funds to hire a babysitter/activity person to give the children a change/break.
Me being supported to support them. Validation of my mothering which was impacted by family violence.
Counselling along with building our relationship again, giving them the power to choose or make some decisions to help them feel in control and lots of self-care.
We also asked survey participants about what could help their children, through the question: “If you think about your partner’s/ex-partner’s behaviours towards you and your children, what do you think services can do to best address your children’s needs?” We identified three themes: “Let them have a voice”, “Believe mothers instead of blaming them”, and “Recognise the impacts on children”.
Let them have a voice
The major theme evident in participants’ responses was that services needed to listen to children and prioritise children’s safety over the needs of the perpetrator. This included ensuring that the perpetrator’s needs and demands did not dominate decisions relating to child contact:
Services need to put the children’s voices at the forefront and put in place mechanisms that stop their voices from being drowned-out by the noise of an entitled, controlling and abusive male parent.
[Services need to] see him as the problem. Not force kids to go to their dad’s house if there has been abuse.
Participants emphasised the importance of hearing children’s views and wishes in relation to contact with the perpetrator. For example:
Listen to my child and empower him to speak up about what parenting arrangements suit him in future.
Actually, ask them how seeing their abuser makes them feel.
Believe mothers instead of blaming them
The second theme was that to best assist children, service providers needed to better support mothers. For example, one said: “Services need to support the one that is always there for them (nearly always the mother and certainly so in my case). DEFEND her when she needs it.”
Participants suggested they were willing and able to meet the needs of their children, but they needed material, legal and financial support to do so:
Services need to teach me how to ensure my experiences don’t affect them and their future relationships with others.
Services need to support mums like me with infrastructure and other needs – housing (I received no financial settlement and fell into extreme poverty).
Services need to help me with my mental health so they [children] can be loved properly.
Associated with this theme was a need to believe mothers, rather than blaming them for the abuse:
Stop blaming mothers. Hold perpetrator accountable and get him out of the house.
Believe your allegations. Victim blaming days should be long over by now.
Listen to mothers when they say they do not feel their child is safe.
There was also a strong perception that it was the perpetrator, rather than the victim and her children, who should suffer the consequences of the abuse:
Why do victims have to be uprooted and placed in shelters? … Funding should be going to police to give them more power to remove perpetrators and allow families, who are already traumatised, to remain in their homes.
Support children to address the impacts of IPV and/or SV
A third theme was that services needed to recognise that abuse by a partner not only affected the adult victim but could have traumatic impacts for children. Participants suggested children’s support needs were not adequately recognised by services. They emphasised that children needed psychologists and counsellors who had specialist expertise in IPV and abuse:
Psychologists need training in DV. My oldest daughter has had two psychologists who know nothing. One told her after 2 years of separation from a 32-year relationship that “mum and dad need to get over it. You[r] mother is wrong, she could have left.” The other has no idea of family dynamics.
[Services need to offer] counsellors, services and psychologists independent of the Family Law courts who understand DV and recognise that even though children weren’t directly abused or witnessed abuse of a parent, that abuse of a parent is emotional abuse and equally devastating to a child.
Greater access to low-cost children’s counsellors who could offer regular, long-term support was also highlighted:
Better access to child psychologists and more appointments available rather than once a month or every 2 months.
Give us counselling on how to deal with his ongoing behaviour. They will be mentally ruined by the time they’re 15.
Participants also suggested that the perpetrator should not be able to control the children’s access to therapeutic services:
Allow one parent to seek help for the children involved without the other[’]s permission. My ex has refused our children play therapy.
[Children need] services that don’t rely on both parents agreeing, my daughter needs counselling but because we co parent I have to tell him we are seeking support and get his approval. It’s crap.
[Children] need better access to support in school and I should not need both parents’ signatures for them to receive it.
Views of people who use IPV and/or SV on their children
To explore how people who had used violence or abuse perceived the support their children needed, we included the following two questions in our survey: “If you think about your behaviours towards your partner/ex-partner and children, how do you think your children have been affected?” and “If you think about your behaviours towards your partner/ex-partner, what do you think services can do to best address your children’s needs?”
Impact of IPV and/or SV on children
In response to our questions on the impact on children, it was evident that many felt their children were not significantly affected by the abusive behaviour. For example, one survey participant who acknowledged that he had been physically violent and was frequently verbally abusive said that he believed his children “are not affected too much by any of this”. Many expressed a belief their child/ren were unaffected because they had not seen any of the abuse or were too young to understand it. For example, one said “It’s not been obvious enough for them to notice”, and another said: “Counsellors have told us he is fine and he never witnessed [it].” Others said they had tried not to expose their children to their abusive behaviour. For example, one said: “I never raised my voice to my wife when the children were around”, and another commented: “Well, I don’t think it’s affecting him, at least we’ve tried our best to hide it from him.”
Other participants felt that their children had coped well and/or had managed to overcome any negative impacts of witnessing the abuse. The following comments from two participants illustrate this:
My son has been very resilient and forgiving for which I am blessed. He has also come out of it with a healthy respect for the women in his life and his expected behaviour towards them.
My irresponsibility with alcohol is something my daughter sees, and I do wonder what she’s thinking. Having said this, I don’t think it’s affected her much if at all.
However, some participants admitted that their abusive behaviour towards their partner had caused trauma or fear for their children. Several noticed that their children were upset or often afraid of being around them. For example:
I know my daughter is scared of me and I hear them cry when their mum and me fight.
They would have been worried and feeling helpless.
The kids were definitely wary around me when their mother lived with us. They became less so when she left.
My daughter wouldn’t understand but would be scared and become quiet.
Some expressed concern about how their children had been affected. For example:
[My children] have been afraid to confront me during times of anger, and this is saddening to me.
My kids will normally be traumatised but I will ensure I do everything to cancel that from their life and memory by showing love, empathy to my wife and kids.
Participants also expressed a fear that their children may suffer long-term consequences or replicate the same behaviour when they grew up. One said:
Whilst [my children] are only 7 and 5, which gives me a marginally pleasing mindset that they aren’t yet truly old enough to know exactly what is going on, I am seriously concerned that if I don’t sort myself out, their lives will be destined for failure, hardship, criminal offences etc.
Children’s support needs
Considering that many participants felt their children were not affected by their abusive behaviour, it was unsurprising that in response to our question about children’s support needs, a frequent comment was that their children did not need external support or help. However, some participants commented on what services could do to help their children and/or what they themselves could do. We identified the following two themes based on their responses.
Help me be a better parent
Some participants indicated that they needed to change in order to help their children. Although some indicated that they simply needed to be more careful about how they behaved in front of their children (for instance, one said he wanted to “reduce acts of violence in front of the child”), others identified a need for more substantial personal change. As one commented: “The more I can change my behaviour the better for everyone else.” This included becoming a better parent and role model, and repairing relationships with their partner and children:
[I need to] be a better father figure for them.
At the moment, I just want to focus on my wife and I making sure we become the best example for our kids in every way.
We are actually working at that currently, in fact I sent a letter of apology to my children in an effort of reconciliation (in conjunction with my counsellor).
A conversation and an explanation
The second theme was that children needed to have a reassuring conversation, in which they could share their feelings and be given an explanation for what was going on in their family. Some suggested that as a parent it was their role to engage in such a conversation, while others indicated their child needed a counsellor or someone external to the situation. For example:
[Services need to] give them a safe space to talk about their feelings and be heard.
[My children need] a service that gives them the confidentiality to speak freely and open up about how they feel.
[Services need to] talk to the children, ask them if they were okay.
Several commented that explaining why an adult might behave badly would be an important part of a supportive conversation.
[Services need to] explain to them that adults sometime are acting stupid.
[Services need to] just be supportive and explain that even grownups can get sick or do naughty things, but like all of us, can fix them!
Summary
There were stark differences between how victims and survivors view the impact of the violence and needs of the children compared to people who use IPV and/or SV. Victim and survivor participants frequently felt the system had failed their children who had been greatly impacted by their mother’s experience of IPV and/or SV, whereas many participants who had used IPV and/or SV did not identify a great impact on their children or any support needs for children arising from the IPV and/or SV.
Part F:
Discussion and implications for system improvement
Having people – not necessarily professional people – around you who believe in you and believe you … and are willing to support you through it all, I think that makes a huge difference.
(Victim and survivor participant)
Introduction
In this part we summarise the project findings for each group of participants and discuss them in the broader context of the literature. We highlight children’s needs and the impact of the COVID-19 pandemic. Drawing on the voices of women victims and survivors and people who use violence, as well as the available evidence base, we present integrated, whole-of-system recommendations to improve support and service engagement tailored to different stages of help-seeking.
Summary of findings in context
Women victims and survivors
We obtained survey data from 1,122 women who self-identified as having experienced IPV and/or SV in the previous five years. We also undertook in-depth qualitative interviews with 30 of these women. This data represents a valuable national snapshot of the abuse and violence experiences of women in Australia, highlighting patterns and types of violence and its impacts on health. Furthermore, both the quantitative and qualitative data illuminate their experiences of help-seeking, support needs and key areas where barriers to service delivery could be addressed.
Sociodemographic characteristics and experiences of IPV and/or SV
Our survey sample was largely representative of the broader Australian population of women in terms of age, education, location, marital status and whether they had children. Some key differences were that our sample was over-representative of Aboriginal and Torres Strait Islander women, but under-representative of women from migrant backgrounds as the survey was only available in English.
In terms of experiences of violence, over 80 per cent were currently afraid or had been afraid of a partner in the previous 12 months. Looking at lifetime experiences since age 16 years, poly-victimisation was common, particularly among Aboriginal and Torres Strait Islander women, women aged 25 to 45 years, and unemployed women, but less so among migrant women and younger women. Combined forms of IPV were commonly experienced (psychological, physical and/or sexual violence; 84.6%), highlighting the need to cease looking at one-dimensional types of abuse and rather to consider an overall pattern of abuse during a woman’s lifetime (Potter et al., 2020). Sexual violence was extremely common and often overlapped with psychological abuse, which is consistent with other research (Tarzia & Hegarty, 2022).
Of the women who reported IPV experiences, nearly one in three also reported experiencing reproductive coercion and abuse (RCA) which is higher than rates reported in other recent Australian research (Price et al., 2019). Almost all of the participants who had experienced RCA also reported combined physical, psychological and sexual violence, supporting the hypothesis that RCA is closely linked with fear and control in relationships (Tarzia & Hegarty, 2020). It is worth noting that one in three women experiencing IPV also reported technology-facilitated abuse and financial abuse in their lifetimes, highlighting the need to include these under-researched forms of IPV.
Child abuse and adverse childhood experiences were also common for two thirds of the victim and survivor participants, adding to the burden of trauma for women (Capaldi et al., 2012; Li et al., 2019). Overall, those who experienced abuse as a child and an adult had the highest health burden, and reported experiencing both mental health issues, poor general health and chronic conditions.
The vast majority of participants experienced PTSD, and two thirds experienced anxiety and depression, with half of participants living with disability or chronic illness limiting daily activities including employment (Figure 17). Aboriginal and Torres Strait Islander women and those who had difficulty managing on their available income had the highest burden (Blagg et al., 2022). The prevalence of health problems was consistent with the extant literature (Summers, 2022; World Health Organization, 2013a). In particular, the impacts of SV or reproductive coercion on women’s health were evident, highlighting the need for greater attention to be paid to these forms of violence (Tarzia, 2020; Tarzia & Hegarty, 2020). Aboriginal and Torres Strait Islander women andwomen who were unemployed or had difficulty managing on their available income also reported high rates of poor mental and physical health.
Figure 17: Percentage of participants (victims and survivors, and perpetrators) with health issues
Data table for the figure above:
| Health issues | Survivors | Perpetrators |
|---|---|---|
| Poor/fair health | 35% | 21% |
| Anxiety | 52% | 30% |
| Depression | 45% | 29% |
| PTSD | 71% | 51% |
| AOD | 22% | 26% |
| Disability | 36% | 26% |
Figure 17 compares the health status of victim and survivor participants to those who used IPV and/or SV. It shows that a greater proportion of victims and survivors reported poor or fair health, anxiety, depression, PTSD or had a disability. The only factor that people who used IPV and/or SV reported slightly more was the use of alcohol or drugs, reported by 26 per cent, compared to 22 per cent of victims and survivors.
People who use IPV and/or SV
A key contribution of this project is that it is the first attempt nationally to capture the experiences of people who use IPV and/or SV. We obtained survey data from 563 people who self-identified as having caused a partner to be fearful and/or had used IPV and/or SV in the previous five years. We also undertook in-depth qualitative interviews with eight men drawn from the survey sample. The data we collected highlights patterns and types of violence and their associations with various health problems. Quantitative and qualitative data illuminates how people who use IPV and/or SV seek help, their support needs, and key areas where services could strengthen how they respond so that there is an appropriate balance of accountability with empathy.
Sociodemographic characteristics
The sample of people who had used violence was broadly representative of the Australian population in terms of being born in Australia, having children and living in a metropolitan area. The vast majority of the sample were men and most had a female partner. Some key areas of difference included age (with our sample being younger than the general population of men) and Aboriginal and Torres Strait Islander identity (nearly one in 10 participants in our sample). A larger proportion of participants had obtained a higher degree and more were currently employed compared with the broader population.
Despite having to indicate that they had used IPV and/or SV in order to be eligible for the study, only around half of participants met the criteria for having used IPV and/or SV during their adult lifetime, with 34 per cent reporting use of IPV and/or SV in the last 12 months. Just under one third of participants stated that they had made their partner afraid in the last 12 months, and almost three quarters had made a partner afraid at some point in their adult lives. Nearly 5 per cent of participants stated that they had perpetrated reproductive coercion – the first time Australian data has been collected on the perpetration of this form of violence.
Participants who were aged between 25 and 45 years, were Aboriginal and Torres Strait Islander or had difficulty managing on their available income were more likely to report perpetration of IPV and/or SV both over their lifetimes and within the previous 12 months. Younger participants were less likely to report use of violence.
Consistent with the literature (Kimber et al., 2018), child abuse experiences were frequently reported by those who had used IPV and/or SV. Participants who reported childhood abuse were three times more likely than other participants to perpetrate violence as an adult. Perpetration of IPV and/or SV was associated with poor general health, long-term illness, and other mental health problems, with stronger associations for those who had used violence more recently. Systematic reviews have similarly highlighted the associations between IPV perpetration and mental health problems (Oram et al., 2013), highlighting the need for early engagement through health settings.
The survey data from participants who used abuse or violence indicated that they had more violence against women–supportive attitudes compared with the broader Australian population, with those who met the criteria for IPV and/or SV perpetration reporting the strongest support for each negative attitudinal measure. This accords with other research showing that attitudes about gender and condoning or excusing violence are key drivers of violence against women (Webster et al., 2018).
Help-seeking of victims and survivors and people who use IPV and/or SV
The critical role of family and friends
Our survey data suggests that both women victims and survivors and people who use abuse or violence are most likely to seek help from their family or friends compared to formal support services (Figure 18). For victims and survivors, almost two thirds (64%) spoke about their abuse to family or friends, with younger women particularly likely to do so (Figure 18). Similar findings are evident in other Australian (Cox, 2016) and international studies (Sylaska & Edwards, 2014). Two thirds of women participants reported that the responses of family and friends were helpful.Similarly, more than half (59%) of the participants who used abuse or violence reported that they spoke to family or friends, and many (74%) found their responses helpful. Thus, family members and friends are in a critical position to provide assistance both to those subjected to IPV and/or SV and those who perpetrate it.
Our analysis of the victims’ and survivors’ open-ended survey responses provided some insight into the important role that family and friends can play in their help-seeking journeys. Fundamentally, women wanted their family and friends to be “on their side” and to understand their view of the situation, rather than taking the perspective of their abusive partner. An important aspect of this was listening, believing and validating the survivor, rather than judging them or their responses to the abuse. Similar findings have been identified in other studies with victims and survivors (McKenzie et al., 2022; Sylaska & Edwards, 2014; Taket et al., 2014; Trotter & Allen, 2009).
There were notable differences between what participants wanted from their family members and their friends. Victims and survivors frequently spoke of a wish for non-blaming responses from their family and described family members being disappointed or angry with them for the abuse. This may be because familial relationships are based on ongoing biological ties and an identification with one another. The behaviour of one family member may be seen to reflect on others, so family members may react more strongly and be more prepared to directly express blame if they perceive a victim has contributed to the abuse. In contrast to familial relationships, friendships tend to be voluntary and informal relationships that can be ended relatively easily (Rawlins, 2008), which may help to explain why the sub-theme “Stick by me” was associated with friends’ responses. Many participants spoke of wanting their friends to make an effort to maintain the friendship,and it was evident that for many, the perpetrator’s behaviour or how friends had responded to it had damaged the friendship. The sub-theme “step up, speak up and step in” was mainly associated with family members’ responses. Victims’ and survivors’ wish that family should “step up” when they needed them may reflect a social expectation that family members should be a reliable source of practical help, including assistance with finances or caring for children. The “speaking up” and “stepping in” aspects of the theme were connected with both family and friends and reflected a wish for family and friends to call out problematic behaviour or intervene if they witnessed it. Within the responses of victims and survivors about their wishes from family and friends were many examples of the kinds of reactions that they had received that they did not find helpful. It was evident that many experienced disbelief, blame or judgement from family and friends, and many spoke of theloss of friendships as a result of the abuse. This finding is consistent with other studies of victims and survivors, who frequently report receiving mixed responses from family and friends (McKenzie et al., 2022; Sylaska & Edwards, 2014; Taket et al., 2014; Trotter & Allen, 2009).
Many participants who used IPV and/or SV also indicated they were interested in having in-depth conversations with their family and friends about their relationships and wanted family and friends to listen with an open mind. Such conversations could potentially play an important role in helping to identify abusive behaviour and to support people on a pathway towards change. However, our findings also identified that many participants who used IPV found it difficult to engage their family and friends in serious discussions and often received responses that they perceived as dismissive or unhelpful. This accords with research with family and friends of perpetrators of IPV, who often report uncertainty in knowing how to respond (Latta & Goodman, 2011; McKenzie et al., 2022).
Together, our survey findings suggest guidance and education is needed for family and friends on how to be an ally for victims and survivors of IPV and how to respond effectively to someone who perpetrates IPV and/or SV. Unlike service providers, family and friends can be “on the side” of victims and survivors in an enduring way (Goodman & Smyth, 2011). Their emotional support and practical help can be critical as victims and survivors navigate a journey to safety and recovery from the abuse. Their responses also send powerful signals to the perpetrator as to whether or not their abusive behaviour is acceptable (Hydén, 2015; Klein, 2012). However, research indicates that often friends and family feel overwhelmed and unsure how to be helpful to victims and survivors (Gregory et al., 2017; McKenzie et al., 2022). They also struggle to know how to respond to a perpetrator of IPV and/or SV (Latta & Goodman, 2011; McKenzie et al., 2022). Thus,programs to equip family and friends to respond effectively to IPV and/or SV are essential in efforts to improve supports for victims and survivors and responses to perpetrators.
Formal help-seeking and journeys through the service system
Victim and survivor survey participants were more likely than those who used IPV and/or SV to seek support and legal assistance from formal service providers. For both groups, health professionals were the most frequently used formal source of help, being used by around half of the victims and survivors and a third of participants who used IPV and/or SV. This reiterates the key role that the health system plays in responding to IPV and/or SV and the importance of ensuring that practitioners are well-trained and ready to do this work (Garcia-Moreno et al., 2015; Oram et al., 2022) Victims and survivors less often also turned to specialist services (40%), police (31%) and legal services (19%), in contrast to participants who used IPV and/or SV (11%, 5% and 2% respectively). Figure 18 compares the proportion of participants who sought help from informal and formal supports.
Figure 18: Percentage of participants (victims and survivors, and perpetrators) who sought help
Data table for the figure above:
| Type of help | Survivors | Perpetrators |
|---|---|---|
| Family/friends | 65% | 59% |
| Health services | 51% | 33% |
| Specialist services | 40% | 11% |
| Police | 36% | 5% |
| Legal | 19% | 2% |
Help-seeking journeys through the service system for victims and survivors
As illustrated in Figure 18, most women victims and survivors had accessed at least one formal service (primarily health services), and more than half of them (59.6%) found their formal service contact helpful. Aboriginal and Torres Strait Islander women, women who had difficulty managing on their available income and women aged 25 to 45 years or no longer living with their partner were all over-represented as users of formal support compared with other women. This is likely to be because all these groups are more likely to experience a greater prevalence of IPV and/or SV (Australian Institute of Health and Welfare, 2018). Migrant and younger women were less likely to access formal support, which may suggest that there is greater stigma or additional barriersto accessing services for these groups of women (Tarzia et al., 2017; Vaughan et al., 2016).
Shame, lack of awareness about services or confidence in their ability to help were the most frequently reported barriers to accessing support. Women were also concerned about confidentiality. Nearly half of the participants said there had been a time they needed help for IPV and/or SV but could not get it, most commonly because of difficulty understanding the practitioner or a lack of available appointments. This communication barrier may partly explain the under-representation of migrant women in help-seeking via formal services.
Our analysis of help-seeking timelines and themes from our interviews with 30 victims and survivors provided a more nuanced insight into their help-seeking needs and their journeys through the service landscape. We identified five main stages of help-seeking: maintaining hope and fixing problems; assessing options and seeking solutions; getting out; establishing independence and safety; and addressing impacts and making sense. These stages reflected victims’ and survivors’ particular needs or goals at different times. In the earlier stages, women needed empathetic listening, validation of their concerns, help to identify the abuse and options for support and safety. For many, the source of this help was a healthcare provider, such as a GP or mental health professional. However, not all victims and survivors received an empathic response when they sought help to understand the problems they were experiencing. Some described professionals focusingonly on mental health symptoms or diagnosis, while others said their abuse was misidentified as mutual conflict in the relationship. This highlights a critical need for health professionals to be competent to provide an effective first-line response.
Once women had recognised the abuse and sought to improve their safety, end the relationship or re-establish their independence, they frequently needed tangible and practical support – including housing, financial help and legal advice. However, they often found that there was little assistance available or that it was very complex to access. This finding underscores a need for greater government investment so that services can deliver the practical assistance that victims and survivors require to regain their safety, wellbeing and independence. Along with material help, a critical need was for someone to support, guide and advocate for victims and survivors as they navigated a very complex service system. Victims and survivors described already feeling overwhelmed by the abuse, and the long struggle to find assistance and having to repeatedly retell their story to different service providers only amplified their distress. Few found a professionalwho could act as an advocate to support them and “go into bat” for them to access the resources or legal protection they needed. Similar service gaps have been identified in the US (Campbell, 2021) and in the UK (Sullivan & Goodman, 2019).
Our interviews also identified that when women sought legal protection or to settle post-separation parenting or property arrangements, they were often left feeling that the perpetrator had only been emboldened in their abuse. Consistent with other Australian studies (Kaspiew et al., 2017), women reported that the family court in particular was an arena in which non-physical forms of IPV were misrecognised or minimised. There is an urgent need to foster increased competency in recognising and addressing IPV across the legal service system. Better recognition of coercive and controlling tactics is particularly pressing in the family courts to prevent perpetrators from using legal systems abuse and the deliberate manipulation of children to further harm a victim or survivor.
Women in our study also felt let down by a lack of accessible or appropriate help to recover from traumatic impacts and to make sense of the abuse they had experienced. They also felt psychologists and other mental health professionals tended to offer “textbook” responses, and it was difficult to locate a counsellor who was trauma-informed and IPV-trained. Similar findings have been identified in other studies with Australian victims and survivors (Marsden et al., 2021). Another important need that participants identified was to connect with other victims and survivors. Consistent with other research (Gregory et al., 2021; Osborn & Rajah, 2020), participants felt peer-based approaches reduced isolation and shifted the stigma of being victimised by a partner. However, opportunities for group-based support were limited and participants often felt service providers did not recognise the importance of peer support models.
Overall, the findings indicate that although women victims and survivors received support that was positive or helpful at different times, they felt they were “carrying the burden alone” in trying to address the abuse. The main message they felt the service system conveyed was that it was largely their responsibility to manage the perpetrator’s abuse and the consequences it had for themselves and their children. They perceived that the system was focused on crisis responses, while there was a lack of ongoing help to navigate through a maze of different services to find safety and recover from the IPV. There was also an emphasis on physical harm and immediate risks to safety, but less recognition of the impacts of other forms of abuse, including post-separation stalking and manipulation of the legal system and parenting arrangements. Similarly, women perceived that trauma-informed healing and recovery from the abuse they had experienced was not apriority for the service system. Services were overstretched and at each stage of their journey towards safety, victims and survivors did not always receive the legal, emotional or practical support they needed. Figure 19 illustrates women participants’ perceptions of the roadblocks and missed opportunities they encountered at each stage of their journey. Each of these contributed to a perception of being alone with the burden of ending and addressing the perpetrator’s abuse.
Yet, in women’s stories of help-seeking, there were also examples of responses from service providers that were positive or pivotal in meeting their support needs. Figure 20 illustrates the key responses at different stages that women perceived had made them and their children feel secure and supported.
Figure 19: Roadblocks and missed opportunities in victims’ and survivors’ journeys
Text version of the figure above:
Carrying the Burden Alone
Roadblocks and Missed Opportunities
Maintaining hope & Fixing problems
- Only diagnosing symptoms
- Misrecognising IPV as mutual conflict
Assessing options and seeking solutions
- Advice not matching readiness
- Focusing only on physical harm
- Not engaging with the perpetrator
Getting out
- Lack of tangible assistance
- Police/legal intervention without adequate information or support
Re-establishing independence and safety
- Lack of guidance, follow-up or advocacy
- Failure to stop legal systems abuse
Addressing impacts and making sense
- Lack of affordable long-term support
- “Textbook” or medicalised response
- Lack of peer support groups
Figure 20: Positive or pivotal responses in victims’ and survivors’ journeys
Text version of the figure above:
Women’s journeys to support and safety
Positive or pivotal responses
Maintaining hope & fixing problems
- Inquiring about relationships
- Identifying abuse
Assessing options & seeking solutions
- Listening & showing empathy
- Validating concerns, identifying risks
- Exploring options without pressure
- Intervening with necessary
Getting out
- Help to plan a safe escape
- Income and a secure place to stay
Re-establishing independence & safety
- Help navigating the service system
- Material and financial support
- Recognising and stopping the abuse
Addressing impacts and making sense
- Ongoing counselling with someone who understands
- Connecting with other survivors
Help-seeking journeys through the service system for people using IPV and/or SV
Slightly less than half of the survey participants (41%) had sought formal advice or support for their use of violence (Figure 18). As for the women victims and survivors, health services were the most frequently utilised avenue for formal support, with the majority finding these helpful. Specialist services and the justice system were less frequently accessed, most likely because they require identifying to some extent as a “perpetrator”. As the open-ended survey questions demonstrated, many of the participants strongly felt that they were not violent or abusive and therefore did not require support.
Aboriginal and Torres Strait Islander participants, those who had difficulty managing on available income, older participants, and those who had not completed Year 12 at school were over-represented among service users, whereas – as with the victims and survivors – participants from a migrant background were less likely to access formal services, highlighting the barriers these community members face (Segrave & Pfitzner, 2020; Vaughan et al., 2016).
Numerous barriers to accessing support were reported by participants using IPV and/or SV. Similar to the victims and survivors, shame was the most commonly reported barrier, followed by a belief that violence is a normal part of a relationship. Participants also reported access challenges similar to those described by victims and survivors, including concerns about confidentiality; lack of awareness of services; communication issues; and not having the time to talk to someone. For those participants who had sought help but been unable to get it, the most common barriers were lack of awareness about services; prohibitive costs; and long waiting times.
Our interview findings with men who had used violence similarly speak to the challenges around promoting early, effective help-seeking for perpetrators. We identified three stages across the men’s journeys through the service landscape: bottling things up; breaking down and letting things out; and regaining and maintaining control. Men’s support needs differed across each of these stages, with an overarching perception that they needed help to release and regain control of their emotions in order to stop using violence.
For most of the men, initial engagement with service providers occurred at a crisis point and was prompted by their partner deciding to leave them and/or contacting mental health services or the police. Participants felt this engagement was a catalyst for them to begin to change their problematic behaviour. The finding that help-seeking was prompted by a
“breaking point”, particularly relationship breakdown or a partner pushing them to engage with services, is consistent with other studies (Calcia et al., 2021; Davis et al., 2021). For example, a recent review of the literature on the help-seeking of perpetrators of IPV found that a perceived crisis and the threat of negative social outcomes (such as escalating abuse, criminal justice involvement, and a fear of losing or damaging relationships with children and partners) were common catalysts for their engagement with healthcare services (Calcia et al., 2021). Yet, if men’s motives are primarilyself-preservation or functional gain (such as regaining their relationship with their partner or avoiding legal sanctions), rather than deep personal reflection and transformation, then behaviour change may not be sustained (McGinn et al., 2020). Our findings help to demonstrate that the interventions of GPs, mental health professionals, police and others during times of crisis may be key initial steps to engage perpetrators on a “pathway towards accountability” (Campbell & Vlais, 2019). This accords with other Australian research that identifies that human services agencies, including mental health professionals, can play a key role in early interventions that help change abusive behaviours and violence-supportive attitudes (Chung et al., 2020).
As found in other research with men who have used IPV (Kelly & Westmarland, 2016), there was incongruence between participants’ reported behaviour in relationships and their self-perception. Almost all the participants suggested their abusive behaviour did not reflect their underlying beliefs or character, but was a reaction to external factors and circumstances, such as prior trauma and/or mental health problems, and/or a build-up of anger and strong emotions that were difficult to control. Thus, they framed the abuse as a “loss of control” that occurred when they were not rational and “not themselves”, rather than being a deliberate attempt at exerting control over their partner. In effect, this framing distanced them from responsibility for their behaviour. Further, although they suggested their mental distress and behaviour was problematic for themselves and their partner, they were reluctant to seek help. Masculinity was a barrier; manyattributed their help-seeking hesitancy to a perception that for men, vulnerability was shameful, which aligns with the quantitative survey findings. Taken together, this underscores the importance of shifting men’s perceptions that stigmatise help-seeking as “unmanly” and a reflection of personal weakness or failure (Levant, 2011; Vogel & Heath, 2016).
Support needs for victims and survivors of, and people who use, IPV and/or SV
Formal support needs of victims and survivors
Victim and survivor survey participants most valued the receipt of emotional support, including feeling listened to (91.7%), having someone to talk to (90.4%), and not feeling judged or put down (86.9%). These needs are consistent with evidence-based frameworks outlining recommended responses from services, such as LIVES (World Health Organization, 2014) and CARE (Tarzia, Bohren, et al., 2020).
Figure 21: LIVES recommendations for first-line response
Text version of the figure above:
Current recommendations for the first-line response (LIVES)
- L – Listen to woman closely, with empathy, without judging
- I – Inquire about and respond to her various needs and concerns
- V – Validation experience: Show her that you understand and believe her. Assure her that she is not to blame
- E – Enhance safety: Discuss a plan to protect herself and children from harm
CARE
- C – Choice and control
- A – Action and advocacy
- R – Recognition and understanding
- E – Emotional connection
Similarly, the qualitative survey data highlighted women’s need to be taken seriously by service providers and have their concerns heard and validated. Women wanted support that was delivered empathetically, acknowledged them as individuals and was responsive to their particular needs. Yet, there was frequently a mismatch between what women wanted and what was offered. A lack of accessibility and availability was identified as a core problem across the service sector. Women described help not being available when they needed it, and they encountered long waiting lists and a limited availability of appointments when trying to access services. Participants also struggled with the fragmented and disconnected nature of the service sector. Many described challenges around having to access multiple services, being forced to repeatedly tell their stories, and feeling neglected after services were only available in the short term or service providersfailed to follow up with them. Finally, women were desperate for services to make the perpetrator stop the abuse. There was a sense of helplessness that services were unable or unwilling to hold the perpetrator accountable or to take meaningful action to keep women and their children safe. These themes were echoed across women’s stories of their help-seeking journeys, as identified by interview participants. Many said they felt alone in carrying the burden of addressing the abuse and recovering from its impacts on themselves and their children.
Support needs of Aboriginal and Torres Strait Islander women victims and survivors
Our survey identified that compared to other participants, Aboriginal and Torres Strait Islander women had a higher prevalence of experiencing multiple forms of victimisation in their lifetimes, including IPV, SV and child abuse. This is consistent with the findings of other studies (e.g. AIHW, 2018), and is influenced by intergenerational trauma, racism and discriminatory social policies and practices in the lives of Aboriginal and Torres Strait Islander women (Blagg et al., 2022). Survey participants who were Aboriginal and/or Torres Strait Islander were also over-represented as users of informal and formal supports (Fiolet et al., 2019). Other studies of Indigenous women globally identify a reluctance to seek formal help and a reliance on family and informal networks, though Indigenous women do seek formal help as a last resort in a crisis (as summarised in a review by Fiolet et al., 2019). This may have been the experience of participants inour study, or our findings may reflect Aboriginal and Torres Strait Islander women’s repeated attempts at help-seeking from different service providers over time. The higher rates of help-seeking by Aboriginal and Torres Strait Islander participants compared to other participants in our study may also relate to the impacts of social disadvantage. Other Australian studies have identified that women victims and survivors who were socially disadvantaged accessed more support than those in circumstances associated with social advantage (Cox, 2015). Our findings also show that those who had difficulty managing on available income were more likely to seek formal help.
Consistent with our findings, other research makes clear that Aboriginal and Torres Strait Islander women face considerable barriers in seeking appropriate support (Fiolet et al., 2019). Our interviews with Aboriginal and Torres Strait Islander women identified that fears of receiving racist responses and/or having their children removed from their care meant they were reluctant to engage with service providers and the legal system.
Aboriginal and Torres Strait Islander leaders have long identified the need for investment in community-led responses to domestic and family violence (Blagg et al., 2022; Carlson et al., 2021; Morgan et al., 2022). There has been a call for holistic healing approaches that recognise how the traumatic impacts of colonisation and systemic oppression of Aboriginal and Torres Strait Islander peoples shape women’s experiences of IPV and/or SV and their help-seeking (Blagg et al., 2022; Carlson et al., 2021). The importance of Aboriginal and Torres Strait Islander communities developing dedicated responses to abuse and violence has recently been acknowledged in the federal government’s draft National Plan. Our study lends further support for the need to resource community-led trauma- and healing-informed responses, given that our findings identify that Aboriginal and Torres Strait Islander women are at high risk of experiencing IPV and/or SV and facesignificant barriers in using mainstream support and legal services. Thus, we recommend that Aboriginal-led centres for healing be developed and be fully resourced in each state and territory.
Support needs for people who use IPV and/or SV
Participants in the survey suggested that their main support needs from services were learning new ways of dealing with relationship problems; feeling listened to; and having access to professional expertise. There was an expectation that the service provider would see them as an individual person and provide non-judgemental support.
Analysis of the open-text survey responses shed more light on the expectations and needs of people using violence. Participants said they wanted help to regain emotional control and reshape how they saw their behaviour and/or their partner, as described in the theme “help to see things from a new perspective”. Another important theme across participants’ responses was “hear me and talk to me, not at me”. This theme encapsulated a desire to have an open and honest conversation with a professional who listened, rather than lectured.
Consistent with the findings of a recent review (Calcia et al., 2021), our analysis of survey responses suggests that people who use IPV may be prepared to engage with support services to address their abuse. Although they had different perceptions about the kind of support they need, with some focusing on a need for help with emotional control and others wanting insight into how their thinking may contribute to their behaviour, participants consistently emphasised that they wanted someone they could open up to who could listen with empathy. Feeling listened to was also identified as a facilitator of disclosure of the use of IPV in other studies (Calcia et al., 2021). As mentioned in our discussion of findings from our interviews with people who used IPV, this highlights the importance of service providers – particularly health and mental health professionals – having the skills to engage empathically with people who use IPV, while encouraging themto take responsibility for their choices and change their behaviour.
Victims’ and survivors’ views of what perpetrators need to stop using IPV and/or SV
Some argue that compared to the person using violence, victims and survivors have a more “objective” perspective on the perpetrator’s behaviour (McGinn et al., 2016). Indeed, our analysis of open-ended survey responses from victims and survivors indicated that changing the perpetrator to stop their abuse would be a long and intensive process, and some felt that the perpetrator would never change. Many participants found that nothing had prompted the perpetrator to stop the abuse, other than the survivor ending the relationship and removing themselves from contact with the perpetrator. For some, legal consequences had curtailed the abuse to some extent. Similar findings were identified in a systematic review of studies with women whose partners attended behaviour change programs (McGinn et al., 2016). Some victims and survivors in our study felt change was possible and suggested that what the perpetrator needed was a “wake-up call” from others torecognise their problematic behaviour, intensive therapy to address underlying or contributing personal issues (along with contact with the victim and survivor to understand their side of the story), and strong mechanisms to hold them accountable for stopping the abuse.
Comparing the survey responses of people who used IPV and/or SV and the responses of victims and survivors, it was evident that there were some overlaps in participants’ perceptions of what was needed to change abusive behaviour. Both groups identified that therapy or counselling for the perpetrator may be beneficial, though victims and survivors emphasised such conversations needed to be undertaken in consultation with the victims and survivors and should be ongoing and intensive. Some victims and survivors said the perpetrator should be mandated to attend. In contrast, people who used IPV and/or SV suggested they were voluntarily prepared to seek help to help manage their emotions and/or gain insight into their behaviour. Similarly, while both groups of participants suggested that having others provide a new perspective on the abusive behaviour was important, victims and survivors suggested this change in thinking needed to be prompted byprofessionals, friends, family members and other community members (particularly men) intervening with the perpetrator and calling out their abusive behaviour. Victims and survivors also emphasised a need for professionals and authorities to hold the perpetrator to account by applying restrictions and legal consequences if they continued to use abuse or violence. Similar findings were identified by McGinn et al. (2020; 2016), who undertook a review of research on perpetrators’ perceptions of engaging in behaviour change programs, following an earlier review of victims’ and survivors’ experiences of men’s behaviour change programs. The authors found that perpetrators highlighted their internal motivations for change, while victims and survivors spoke of change being initiated by external forces and the importance of legal and other measures to hold the perpetrator accountable (McGinn et al., 2020; McGinn et al., 2016).
Our findings suggest that victims and survivors perceive that a range of external actors can play a role in holding the perpetrator responsible for their behaviour, including friends, family and other community members who can “call out” the abuse or violence; professionals who provide therapy or treatment; and police and courts that can implement restrictions and consequences. Thus, in our recommendations, we identify a need to build capacity across the community on how to effectively intervene, which will help create a “web of accountability” around the perpetrator (Chung et al., 2020). This includes training for family and friends and education to foster the competence of GPs, mental health services and other professionals to respond.
Children’s needs in the context of adult IPV and/or SV
Perceptions of women victims and survivors
Our analysis of open-ended survey responses indicated that women recognised that their children had been significantly affected by the IPV but felt legal and support services had failed to protect them or to address the impacts of the abuse on their children’s wellbeing. A key concern was the family courts enabling perpetrators to use children as pawns in the abuse or to block children’s access to support programs. The findings echo those of Kaspiew et al. (2017), who found that women frequently reported negative experiences in the Australian family courts and that their children’s safety and wellbeing was compromised as a result. Participants in our survey emphasised a connection between their children’s safety and their own and the importance of resourcing and supporting them so they could care for and protect their children. They also identified a lack of therapeutic support available to help their children deal with the trauma of
the abuse.
As other studies have identified, perpetrators of IPV often deliberately sabotage the relationship between mothers and their children as a tactic of their abuse (Humphreys, Kertesz, et al., 2019; Humphreys et al., 2015; Lévesque et al., 2021). However, historically, courts, child protection authorities and welfare professionals have often failed to recognise how IPV affects women’s abilities to parent and protect their children; instead, women have been judged and held responsible for the impacts of the IPV on their children (Humphreys, Kertesz, et al., 2019). The responses of victims and survivors in our survey make clear that partnering with mothers to support and protect their children is a critical approach to improve children’s safety and wellbeing. Survey participants identified that the best ways that children could be supported were by listening to and believing their mothers and helping mothers to obtain the legal protection, safe housingand financial support they needed to create a secure home for their children. However, participants also emphasised the importance of recognising that children have needs that are separate to those of their parents. Thus, other key themes in participants’ responses were a need for children to be given a voice in court proceedings and to have access to counselling or support programs to address the trauma of living with IPV.
Perceptions of people who use violence
In contrast to victim and survivor survey participants, those who used abuse or violence frequently felt that their children were unaffected by their abuse or violence and therefore did not need support to address it. However, some participants did identify signs of their children’s fear or distress, which is consistent with literature that consistently identifies that children’s emotional, social and behavioural development can be significantly impacted by IPV (Humphreys & Campo, 2017; Humphreys, Diemer, et al., 2019; Lamb et al., 2018). Recognition of the impacts on children is an important area for interventions to target, given that studies suggest concern about damaging or losing their relationships with children can be a key motivator for perpetrators to change their behaviour (Meyer, 2018). Encouragingly, some identified that getting support for themselves to be a better parent would be helpful for their children. Some surveyparticipants who had used IPV and/or SV also said that their children should have the opportunity to share their feelings with a professional and be given an explanation for the abusive behaviour.
The importance of support for children was a strong theme for victims and survivor participants, along with giving children a voice in court decisions. Thus, we recommend that a key principle across the service system is listening to children’s voices and offering children therapeutic support to address the impacts of the abuse and violence in their lives (see “Recommendations for policy and practice”). Further, considering that our findings and those of other studies (Li et al., 2020) suggest that people who use IPV and/or SV may be more likely than others to have experienced child abuse themselves, providing a timely early intervention to address experiences of abuse or violence in childhood may help prevent perpetration in later life.
The impacts of the COVID-19 pandemic
Women’s written responses to our survey questions about the impacts of the COVID-19 pandemic suggested that many of their experiences of abuse intensified during this period. This finding is consistent with other Australian (Boxall et al., 2020; Carrington et al., 2021; Morgan et al., 2022; Pfitzner et al., 2022) and international research (Piquero et al., 2021). An increase in abusive behaviour during the pandemic was also a key theme among survey participants who had used IPV and/or SV. While those participants suggested this escalation was due to external pressures on them, such as increased financial and mental stress, many victim and survivor participants connected it to them being socially isolated and trapped at home, affording the perpetrator more opportunities to target them.
While victims and survivors said their partner or ex-partner’s abuse had increased, they also said it was more difficult for them to access support and find safety. This accords with the findings of a recent Australian study, which showed that victims and survivors were less likely to report their abuse to the police when stay-at-home measures were introduced (Morgan et al., 2022). As other researchers have argued, social isolation, increased time spent at home with the perpetrator, the loss of employment and difficulties accessing services created a “perfect storm” that made many IPV victims and survivors vulnerable to escalating abuse (Usher et al., 2020). However, our analysis of survey responses also uncovered evidence of positive change in victims’ and survivors’ lives due to the pandemic. Some participants in our study suggested the emergence of the pandemic led them to acknowledge their partner’s mistreatment and to take action. Others saidthe increase in the availability of phone or telehealth services improved their access to support, particularly for those who had transportation difficulties, lived a long distance from services or needed support after hours. However, some felt that online or telehealth services were less personal or too risky or difficult to use with children or the perpetrator present in the home.
Similarly, for participants who used IPV and/or SV, there were some positive findings about the impacts of the COVID-19 pandemic. Some people reported that pandemic restrictions gave them more time to reflect on their behaviour towards their partner. Participants also said that they found it easier to seek help because support services were heavily advertised and/or became more convenient to use with the increase in video or telehealth service delivery.
Together, the survey findings from victims and survivors and people who used IPV and/or SV highlight that during times of extreme social turbulence, such as in a pandemic or a natural disaster, the delivery of support services for IPV and SV should be prioritised and increased. There is also a need to establish new and creative ways of delivering services, particularly when access to face-to-face support is restricted. An important finding was that even when lockdowns are not in place, telehealth and phone services can still provide an important alternative to in-person services for those who find it challenging to access services due to distance, transportation, or an inability to access services during business hours. This finding was echoed in a recent review of the literature on mental health interventions for IPV victims and survivors during COVID-19 (Su et al., 2021). However, researchers also caution that such responses should not replacetraditional face-to-face delivery, considering that some people face significant barriers accessing technology-based services, including those who are on a low income, experiencing homelessness, or living in areas where there is poor internet access (Baird et al., 2022). Further, our findings, along with other research (Pentaraki & Speake, 2020), show that when social restrictions are in place and women victims spend more time with the perpetrator or their children, it may be difficult or risky to access support via phone or online. It is also important to recognise that perpetrators may be able to remotely monitor a victim’s use of communication via technology, even when pandemic-related restrictions are not in place (Pentaraki & Speake, 2020). However, we recommend telehealth and online services should continue to be provided as an adjunct to face-to-face options, as they provide greater flexibility of access to support.
What works from the perspective of women in terms of service responses for themselves, their children and the perpetrator?
We have summarised our findings according to the help-seeking journeys women undertake and mapped what participants told us about what might work to improve the system overall and at different stages (Figure 22). It is clear that the normalisation of violence and abuse in relationships – particularly non-physical forms – is common across the community and can mean victims and survivors find it difficult to identify the abuse they are experiencing. Thus, universal education across the community may assist victims and survivors and people who use IPV and/or SV to recognise the signs of an abusive relationship, including sexual, psychological and other forms of abuse. Shame and a lack of awareness of the services that can assist are also major barriers to help-seeking, requiring greater promotion of the services that are available. Hence, we recommend increased community messaging about the availability of accessible and confidential support services,including national helplines for IPV and/or SV. Additionally, messaging should counter the victim-blaming attitudes that remain common in the Australian community, so that victims and survivors are supported, rather than judged, when they seek informal or formal assistance.
The program “Change that Lasts” in Wales is an example of a broad-based community response approach, similar to our recommendations. It consists of “Ask Me” training for “community ambassadors” to improve awareness, understanding and responses within the wider community; ”Trusted Professional Training” to enable non-specialist professionals to identify and respond better to victims and survivors and perpetrators; and ”Specialist Support Services Provision”, which involves needs-led, trauma-informed specialist services for victims and survivors. Finally, ”CLEAR” (Change that Lasts Early Awareness Raising) is a course working with those using abusive behaviours at an early stage (see ”Make a Change” box in the section on what works for perpetrators).
Given that both victims and survivors and people who use IPV and/or SV tend to rely on their family members and friends for help, there needs to be a greater focus on equipping family and friends to respond. Supportive responses from family and friends can also lead women to seek further help from service providers (Evans & Feder, 2016); thus, friends, family and other informal sources can play a critical role in early engagement in formal help-seeking. However, our findings suggested family members and friends were not always helpful or “on the side” of the victim and survivor. Hence, we have made recommendations for training for family and friends to be developed and made widely available online and through community groups so they can understand how to be an effective ally to a victim and survivor. In addition, training in “healthy relationship first aid” could be promoted in all workplaces and faith-based organisations to enable a helpfulfirst-line response.
Considering that health services, in particular general practice and private and public mental health services, were frequently used as sources of support for victims and survivors and for those who used IPV and/or SV, the upskilling of those professionals should be made a priority. Similar calls for action in the health and mental health sectors have been made by the WHO (2013b), the Lancet Psychiatry Commission (Oram et al., 2022) and the Medical Journal of Australia (Hegarty et al., 2022). There has been significant work in this area that demonstrates how the health system needs to be changed to deliver trauma- and violence-informed care (Hegarty et al., 2022).
Our findings also indicate that victims and survivors not only require improved responses from service providers, but also greater access to financial and material support. For example, our survey identified an association between unemployment and an increased likelihood of experiencing multiple types of abuse across the lifespan (such as child abuse, IPV and/or SV). Research suggests that being on a low income or experiencing unemployment is often a consequence of victimisation and, further, women’s financial insecurity may be exploited by a perpetrator as part of their abuse (Cortis & Bullen, 2016). Many women fall into poverty after separating from an abusive partner (Summers, 2022), which may help to explain why our survey identified an association between having an insufficient income and increased help-seeking from financial, justice and specialist services. Additionally, for victims and survivors, having difficulty managing on theiravailable income was associated with poorer physical and mental health, which may also have contributed to their increased levels of help-seeking from health services. Interview participants also highlighted that a lack of access to income narrowed their choices and prolonged the danger they faced, with some saying that a lack of financial support and accommodation meant they had to remain with or return to an abusive partner. Given these findings, it is essential that governments adequately fund the financial and income support victims and survivors need to leave abusive partners and re-establish their independence and safety.
Another critical need of victims and survivors who participated in our survey and interviews was for someone to support and advocate for them as they navigated the service system. This need has been identified elsewhere. For example, in the United States, Sullivan and Goodman (2019) highlighted the importance of trauma-informed advocacy – an approach that recognises the impacts of trauma on help-seeking and validates victims’ and survivors’ and partners with them to regain control over their lives. Such an approach differs to “case management” in that it emphasises a victim and survivor–led orientation. We suggest a similar approach needs to be adequately resourced in Australia. As discussed in our recommendations below, “care navigators” need to be appointed to ensure women have accessible long-term support and advocacy as they journey through the service system. As identified in a recent review, it is also important to recognise the complexity ofadvocacy work and the need to tailor interventions to women with differing backgrounds and needs (Rivas et al., 2019). Thus, it is critical to ensure care navigators are well resourced and provided with ongoing professional training and emotional support.
Our recommendations also highlight a need to shift the orientation of the domestic violence service system from crisis and immediate risk to a recognition of the long-term impacts of IPV. Victims and survivors in our study frequently reported a lack of accessible or affordable support to recover from the traumatic impacts of the abuse. Many also said that when they were able to access mental health services or other support, often service providers lacked the skills and understanding to meet their needs. Victim and survivor participants also emphasised the value of peer-based support from other survivors, which was profoundly helpful in reducing stigma and isolation. Thus, we not only recommend a need for professional competency for mental health service providers and the increased delivery of trauma recovery and healing services, but also the funding of group-based peer support models.
Together, our recommendations highlight that whole-of-system and whole-of-community change is needed, rather than altering specific aspects in isolation (such as the training of staff in specific sectors only). For victims and survivors, this will mean that rather than feeling alone in carrying the burden of addressing the abuse, they feel that no matter who they speak to about their experiences, they will receive a supportive and non-judgemental response.
Critically, the service system needs to have the skills and capacity to respond to the individual needs of victims and survivors with different experiences, circumstances and backgrounds (consistent with the theme “recognise me as an individual person”, identified in our analysis of qualitative survey data from victims and survivors). This requires an intersectional understanding of IPV and/or SV (Kulkarni, 2019), which recognises how victimisation and help-seeking are influenced by the impacts of marginalisation and oppression based on race, ethnicity, sexuality, age, ability, class, geography and other factors (Shimmin et al., 2017). It also requires an understanding of how the impacts of adverse or abusive experiences in childhood may be compounded by being subjected to IPV and/or SV in adulthood. This is important considering that many victims and survivors in our survey had multiple experiences of victimisation across the lifespan, which hasalso been found in other studies (Capaldi et al., 2012; Li et al., 2019). Several factors are key to sustaining a transformed approach across the service system and community: committed leadership; regular training (with mandatory attendance) of staff, from front-desk workers to those who see victims and survivors; on-site trainers; and clear referral pathways. We need a gender-responsive, culturally safe, trauma- and violence-informed, and contextually tailored system for all victims and survivors.
It is also important to acknowledge that while victims and survivors should be able to get the help they need, only focusing on improving help-seeking and providing support risks putting the onus on the victim and survivor to stop the abuse. Thus, a fundamental concern of policy and practice must be on strategies to end the use of violence by those who perpetrate it. In the next section, we summarise our findings on what may assist to stop the perpetration of IPV and/or SV.
“Make a Change” has been developed by Respect in partnership with Women’s Aid Federation England (inspired by the “Change That Lasts” approach described above in the victims and survivors section).
The model aims to address abusive behaviour at an earlier stage, before it becomes entrenched. It offers direct support to people who are concerned that their behaviour towards a partner or ex-partner has been controlling, frightening or harmful. It also provides separate and confidential support to their partners and/or ex-partners, and awareness-raising activities with local communities and training for professionals.
Figure 22: Summary of journeys and help-seeking for victims and survivors
Text version of the figure above:
Journey stage
- Maintaining hope and fixing problems
- Assessing options and seeking solutions
- Getting out
- Re-establishing independence and safety
- Addressing impacts and making sense
Help-seeking
- Journey stage 1:
-
- No or minimal help-seeking. 21.5% did not seek any advice or support
- Journey stage 2:
-
- Family & Friends (64%; 64% helpful). Psychologist / counsellor (42%; 77% helpful)
- General practitioner (24%; 70% helpful)
- Journey stage 3 and 4:
-
- Specialist DFV/SV services (40%; 59% helpful)
- Police (31%) or legal services (19%; 60% helpful)
- Housing or financial services (15%; 53% helpful)
- Journey stage 5:
-
- Any services that provide counselling
Barriers
- Journey stage 1:
-
- Shame (63%)
- Lack of awareness of confidence services can help (62%)
- Fears that others will find out (49%)
- Too busy (46%)
- Fears professional won’t understand (44%) *of all 1,103 participants
- Journey stage 2 to 5:
-
- Trouble understanding terms used by professional (72%)
- Limited availability: no appointments (55%)* or not taking new patients (54%), limited hours (51%), or long wait times (46%), or no service in area ( 43%)
-
- * of the 533 participants who sought help and couldn’t get it
Support needs
- Emotional support (92%); professional competence (87%); practical and safety support (86%)
-
- “Help when I need it”, “See me as an individual”, ‘Take me seriously”, “Follow up and follow through”, “Make them stop”
- Journey stages 1 to 5:
-
- C.A.R.E – Choice and control, Action and advocacy, Recognise dynamics, Emotional connection
Evidence-based models
- Journey stage 1:
-
- Universal education
- Safe environment
- Ask the right questions
- Journey stages 2 to 5:
-
- L.I.V.E.S – Listen, Inquire about needs, Validate experiences, Enhance safety, Support & follow-up
What works from the perspective of perpetrators in terms of service responses?
For a summary of journeys and help-seeking for people who use IPV and/or SV, see Figure 23.
Figure 23: Summary of journeys and help-seeking for people who use IPV and/or SV
Text version of the figure above:
Journey stage:
- Bottling things up
- Breaking down and letting things out
- Regaining and maintaining emotional stability
Help-seeking:
- Journey stage 1:
-
- No or minimal help-seeking
- 27% did not seek any advice or support
- Journey stages 2 and 3:
- Family, partner & friends (59%; 75% helpful)
- Psychologist / counsellor (25%; 84% helpful)
- Specialist DFV or men’s services (11%; 73% helpful)
- General practitioner (10%; 70% helpful)
- Police (5%; 46% helpful)
- Religious person (4%; 82% helpful)
- Legal services (2%; 77% helpful)
Barriers:
- Journey stage 1:
-
- Shame (41%) of all 554 participants
- Normalisation of IPV (35%)
- Access challenges (35%)
- Lack of awareness of services (24%)
- Fears that others will find out (29%)
- Journey stages 2 and 3:
- Lack of awareness of services (68%)
- Cost (62%) of 161 participants who sought help but could not get it or no private health insurance (57%)
- Limited availability: Long wait times (59%), no service in area (57%), no appointments (56%), limited hours (52%) or not taking new patients (49%)
- Concerns regarding confidentiality (49%)
- Language or translation problems (25%)
Support needs:
- Journey stags 1 to 3:
-
- Emotional support (92%)
- Professional competence (91%)
- Practical support for relationship problems (92%)
- “Be more approachable”, “Hear me and talk to me, not at me”, “Get to know me”, “Help me regain emotional control”, “Help me see a difference perspective”
Survivors’ perceptions of needs
- Journey stages 1 to 3:
-
- “A wake-up call and retraining”, “Intensive therapy”, “Restriction and consequences”
We have summarised our findings according to the journeys described by interview participants who used IPV and/or SV. Against this, we have mapped what they told us about what might work to engage them to seek help for their behaviours (Figure 23). Similar to victims and survivors, universal education is required to assist people to recognise what is a healthy relationship and what is abuse. The “Make a Change” model in the United Kingdom provides a good example of a community education and early intervention program (see earlier box for more).
Shame and lack of awareness of services are major barriers requiring community messaging. A greater focus on family and friends might ensure we engage early with perpetrators and change the trajectory for women and theirchildren. Hence, we have made recommendations that involve “engaging men” training for family and friends and “healthy relationship first aid” training for all workplaces and faith-based organisations.
Further, general practice and private and public mental health services require upskilling on how to engage with people who use IPV and/or SV. The work in health systems is less advanced than in the victim and survivor space but is essential as it is where men go for the associated health issues they have. Professionals need to not only have skills to provide empathic support, but also to challenge people to critically reflect on how their emotional and psychological states and behaviours are connected to gendered beliefs and other discriminatory attitudes (such as racism, ableism and homophobia) that support the use of IPV. Although there is a paucity of evidence on the effectiveness of interventions for perpetrators in health settings (Forsdike et al., 2021; Tarzia, Forsdike, et al., 2020), recent Australian research indicates that respectful therapeutic alliances with perpetrators can be effective when professionals invite perpetrators toexplore a different way of being and when structures of accountability and processes for supporting victims and survivors are in place (Wendt et al., 2019). However, such work is complex, considering that such thought processes may have developed over a lifetime and are supported by dominant social constructions of masculinity (McGinn et al., 2020). It also requires considerable skill to explain the limits of confidentiality and to find a balance between engaging empathically while also maintaining the safety of others (Calcia et al., 2021).
There is a need for greater training to ensure all professionals can develop effective therapeutic alliances that not only support perpetrators, but can also act as part of a “web of accountability”, helping to monitor perpetrators’ risk over time, sharing information and working collaboratively to manage risk (Chung et al., 2020). It should also be noted that any increased investment in services for perpetrators should not be delivered by reducing funding to victim support services.
Strengths and limitations
A strength of the study was the large group of diverse participants who were able to be recruited to the study, although the survey was only available in the English language and to those who could access the internet. The combination of quantitative and qualitative methods enabled a rich narrative to be described of victim and survivor and perpetrator experiences of IPV and/or SV, and their help-seeking and support needs. Although this is the largest detailed study in Australia to undertake this exploration, participants may not represent the experiences or journeys of all those who experience or perpetrate IPV and/or SV, particularly people from diverse backgrounds.
Limitations for the survey methods were as follows:
- Data collection methods were inaccessible for people who do not know English, are not technologically literate and who have limited internet access.
- Having the survey only available online was not considerate of possible participants who have tracked internet usage.
- More respondents being from Victoria impacts results, as there are many statewide services, and the usefulness of these services can affect results in broader survey.
- The online nature meant we were unable to verify that people had not completed the survey twice (this was mitigated by checks for duplication on the data).
Limitations for the victim and survivor interviews were that all of the participants had left their partners at the time of the interviews and their journeys may not reflect the experiences of those still with their partners. Limitations for the perpetrator interviews were that the sample was small, and only comprised male, heterosexual and middle- or older-aged participants. Additionally, it may be difficult for people who use violence to fully acknowledge, share and reflect on their abusive behaviour with an interviewer whom they do not know. Using repeated interviews may assist participants to develop the rapport and trust that would support more open discussion.
Implications for research
It is important that future research exploring help-seeking for IPV and/or SV incorporates the following:
- methods that are inclusive of people who read another language other than English, who have literacy problems, and who do not have access to computers and internet
- more rigorous methods to avoid fraudulent responses ensuring participants cannot answer the survey multiple times
- further insight into engaging safely with people who use IPV and/or SV, victims and survivors still with their partners, non-binary and transgender people, and younger people
- better developed measures of perpetration of IPV and/or SV, tailored to people from diverse backgrounds
- more research on how to engage perpetrators in research
- more research directly with children about their help seeking and needs.
Recommendations for policy and practice
The implications for policy and practice are summarised in the recommendations below, which arose out of synthesis workshops that the team undertook based on the quantitative and qualitative data. We have included some overarching principles for responses across the service system. These include a need to:
- recognise the impacts of IPV and/or SV on children, by developing mechanisms for children’s voices to inform reforms and offering accessible therapeutic support for children
- respond to the diversity of the Australian community, by investing in responses tailored for people with diverse backgrounds and experiences of structural inequalities
- promote change, by offering sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
We developed these principles mostly by acknowledging what was absent or difficult to capture from our data. This included that the voices of children were not included in our study, although victim and survivor participants (and some participants who had used IPV and/or SV) highlighted that they wanted therapeutic interventions for their children and for children’s experiences of IPV and/or SV to be recognised and their voices heard by professionals across the service system. Also, although our sample of participants was reasonably diverse, we were unable to drill down to identify how specific responses should be tailored to people’s individual backgrounds, circumstances or experiences. Finally, there was less data about how to provide sustained support for people to change their use of IPV and/or SV.
Below we make recommendations at different levels including community, social networks, early engagement and system access, and for ongoing response (see Figure 24). Each of these targets a specific barrier or enabler that participants identified in the surveys or interviews.
Figure 24: Recommendations
Overarching principles
Recognise children:
Develop mechanisms for children’s voices to inform reforms and offer accessible therapeutic support for children.
Respond to diversity:
Invest in responses tailors for people with diverse backgrounds experiences of structural inequalities.
Promote change:
Offer sustained support for people to end their use of IPV and/or SV within a framework that balances empathy with accountability.
Community
Provide
- Universal education on healthy and abusive relationship behaviours
- Enhanced public messaging about available, affordable and confidential supports, including helplines for victims and survivors and people who use IPV and/or SV
- Financial interventions (eg. microfinancing) to alleviate financial distress for victims and survivors.
Social networks
Develop and deliver
- “Allies training” for family, friends and community using the CARE victim and survivor model
- “First responder healthy relationships first aid” for family, friends, workplaces, and faith-based organisations using the LIVES model
- “Engaging men” training for family and friends to engage effectively with men who use IPV and/or SV
Early engagement
Foster
- Professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- Capacity of general practice, mental health and counselling services to engage with people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
System access
Offer
- Ongoing flexible service delivery (telehealth/online) across sectors for victims and survivors and people who use IPV and/or SV
- “Care navigators” for pathways to accessible and affordable long-term support and advocacy for victims and survivors
- Accessible messaging about limits of confidentiality to overcome barriers to accessing support.
Ongoing response
Response
- Aboriginal and Torres Strait Islander-led centres for healing for all members of the family in each state
- Trauma- and violence-informed recovery and healing services in each state
- Peer victim and survivor-led support groups in each state
- Trauma- and violence- informed care through the Medicare Benefits Scheme for general practice and private mental health services
We recommend that the following be provided across the Australian community:
- universal education to assist community members to identify healthy and abusive behaviours in relationships
- enhanced public messaging to raise awareness of affordable and confidential supports available, including helplines for victims and survivors and people who use IPV and/or SV
- financial interventions (e.g. microfinancing) to alleviate financial distress for victims and survivors, so they can obtain the support and resources they need for their safety and wellbeing.
We recommend the following approaches be developed and delivered to improve how social networks respond to IPV and/or SV:
- “allies training” for family, friends and community members to support victims and survivors, using the CARE model (Choice and control, Action and advocacy, Recognition and understanding, Emotional connection; Tarzia, Bohren, et al., 2020)
- “first responder healthy relationships first aid” for workplaces and faith-based organisations, using the LIVES model (Listen, Inquire about needs, Validate, Enhance safety, Support; World Health Organization, 2013b)
- “engaging men” training for family, friends and community members so they can respond effectively to men who use IPV and/or SV.
To encourage victims and survivors and perpetrators to engage early in seeking professional help, we recommend:
- fostering professional and cultural competency in general practice, mental health and counselling services to deliver emotional and practical support to victims and survivors
- fostering the capacity of general practice, mental health and counselling services to engage people who use IPV and/or SV to seek further help and to challenge violence-supportive thinking and attitudes.
To improve the accessibility of the service system, we recommend:
- ongoing flexible service delivery (telehealth or online) across sectors for victims and survivors and people who use IPV and/or SV
- the resourcing of “care navigators” who can provide accessible and affordable long-term individual support and advocacy for victims and survivors
- accessible messaging to be provided about the limits of service confidentiality, to help address the barriers to accessing support.
To improve the ongoing support available to address the impacts of IPV and/or SV, we recommend the following responses be resourced:
- Aboriginal and Torres Strait Islander–led centres for healing for all members of the family in each state, developed by local communities for local communities
- trauma- and violence-informed recovery and healing services in each state
- peer victim and survivor–led support groups in each state
- trauma- and violence-informed care from general practice and private mental health services to be funded through the Medicare Benefits Scheme.
Conclusion
This mixed methods study has provided insights into the voices and experiences of victims and survivors, and people who use IPV and/or SV, across Australia as to what might assist them in their journeys to help-seeking and what support they value. It is one of the first studies to explore the support needs of those who use violence and abuse, and to contrast their perspectives with those of victims and survivors – including in relation to the needs of children in the aftermath of IPV and/or SV. The findings highlight the key role of family and friends and health services in early engagement. Based on our findings, we also make recommendations across the service system for policy and practice changes that can advance the prevention and response to IPV and/or SV. We no longer want victims and survivors having to go around in circles to find support, as shown by this quote from a study participant:
You get referred here, there, and everywhere. In the beginning you’re on so many phone calls, you can’t remember who you were talking to, where they’re from. You go through the same story hundreds of times, and you just get completely lost. You can’t remember any of it. Then with the practical assistance you get is very little to none. This person will go, “Oh no we can’t help you with that, but here, try this person”, and they’ll go, “Oh no we can’t do that, try this person”, and then you get referred back to where you started at. It’s really frustrating.
Critically, we need to end the use of IPV and/or SV by those who perpetrate it. To do so, we need to hear their voices in order to know how to engage them in behaviour change, as shown by this quote:
Just feeling safe and heard during conversation. That would be the most important thing I would expect from a service or professional. Sometimes just hearing your thoughts said out loud is enough to realise what personal plan of action you must take to change your behaviour, which would hopefully be bolstered by the professional’s help.
Author contributions
Kelsey Hegarty, Mandy McKenzie, Elizabeth McLindon and Laura Tarzia prepared this report. Mandy McKenzie undertook the victim and survivor interviews and analyses with Laura Tarzia. Matt Addison undertook the perpetrator interviews, and Mohajer Hameed and Minerva Kyei-Onanjiri oversaw the survey database. Jodie Valpied and Surriya Baloch assisted Elizabeth Mclindon with quantitative analyses, and Kristin Diemer assisted with survey design and interpretation of quantitative analyses.
References
Afrouz, R., Crisp, B. R., & Taket, A. (2020). Seeking help in domestic violence among Muslim women in Muslim-majority and non-Muslim-majority countries: A literature review. Trauma, Violence & Abuse, 21(3), 551–566. https://doi.org/10.1177/1524838018781102
Anyikwa, V. A. (2015). The intersections of race and gender in help-seeking strategies among a battered sample of low-income African American women. Journal of Human Behavior in the Social Environment, 25(8), 948–959. https://doi.org/10.1080/10911359.2015.1047075
Australian Bureau of Statistics. (2016). Personal Safety Survey. https://www.abs.gov.au/statistics/people/crime-and-justice/personal-safety-australia/latest-release
Australian Bureau of Statistics. (2020). Gender indicators, Australia. https://www.abs.gov.au/statistics/people/people-and-communities/gender-indicators-australia/latest-release#data-download
Australian Institute of Health and Welfare. (2018). Family, domestic and sexual violence in Australia 2018. Cat. no. FDV 2. https://www.aihw.gov.au/getmedia/d1a8d479-a39a-48c1-bbe2-4b27c7a321e0/aihw-fdv-02.pdf.aspx?inline=true
Ayre, J., Lum On, M., Webster, K., Gourley, M., & Moon, L. (2016). Examination of the burden of disease of intimate partner violence against women in 2011: Final report (ANROWS Horizons, Issue 06/2016). ANROWS. https://www.anrows.org.au/publication/examination-of-the-burden-of-disease-of-intimate-partner-violence-against-women-in-2011-final-report/
Baird, S. L., Tarshis, S., Messenger, C., & Falla, M. (2022). Virtual support and intimate partner violence services: A scoping review. Research on Social Work Practice. https://doi.org/10.1177/10497315221087232
Barrett, B. J., & Pierre, M. S. (2011). Variations in women’s help seeking in response to intimate partner violence: Findings from a Canadian population-based study. Violence Against Women, 17(1), 47–70. https://doi.org/10.1177/1077801210394273
Blagg, H., Hovane, V., Tulich, T., Raye, D., May, S., & Worrigal, T. (2022). Law, culture and decolonisation: The perspectives of Aboriginal Elders on family violence in Australia. Social and Legal Studies, 31(4), 535–558. https://doi.org/10.1177/09646639211046134
Blagg, H., Williams, E., Cummings, E., Hovane, V., Torres, M., & Woodley, K. N. (2018). Innovative models in addressing violence against Indigenous women (ANROWS Horizons, Issue 01/2018). ANROWS. https://www.anrows.org.au/publication/innovative-models-in-addressing-violence-against-indigenous-women-final-report/
Boxall, H., & Morgan, A. (2021). Experiences of coercive control among Australian women. Statistical Bulletin, 30. Australian Institute of Criminology. https://doi.org/10.52922/sb78108
Boxall, H., Morgan, A., & Brown, R. (2020). The prevalence of domestic violence among women during the COVID-19 pandemic. Statistical Bulletin, 28. Australian Institute of Criminology. https://www.aic.gov.au/sites/default/files/2020-07/sb28_prevalence_of_domestic_violence_among_women_during_covid-19_pandemic.pdf
Bradbury‐Jones, C., & Isham, L. (2020). The pandemic paradox: The consequences of COVID‐19 on domestic violence. Journal of Clinical Nursing, 29(13–14), 2017–2049. https://doi.org/10.1111/jocn.15296
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Braun, V., & Clarke, V. (2021). Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Counselling & Psychotherapy Research, 21(37–47). https://doi.org/10.1002/capr.12360
Braun, V., Clarke, V., Boulton, E., Davey, L., & McEvoy, C. (2020). The online survey as a qualitative research tool. International Journal of Social Research Methodology, 24(6), 641–654. https://doi.org/10.1080/13645579.2020.1805550
Breslau, N., Peterson, E. L., Kessler, R. C., & Schultz, L. R. (1999). Short screening scale for DSM-IV posttraumatic stress disorder. American Journal of Psychiatry, 156(6), 908–911. https://doi.org/10.1176/ajp.156.6.908
Brown, C., & Hegarty, K. (2021). Development and validation of the TAR scale: A measure of technology-facilitated abuse in relationships. Computers in Human Behavior Reports, 3(100059), 1–10. https://doi.org/10.1016/j.chbr.2021.100059
Burgess-Proctor, A. (2015). Methodological and ethical issues in feminist research with abused women: Reflections on participants’ vulnerability and empowerment. Women’s Studies International Forum, 48, 124–134. https://doi.org/10.1016/j.wsif.2014.10.014
Burton, S., & Blair, E. (1991). The power of survey design: A user’s guide for managing surveys, interpreting results and influencing respondents. Public Opinion Quarterly, 55(1), 50–79.
Calcia, M., Bedi, S., Howard, L., Lempp, H., & Oram, S. (2021). Healthcare experiences of perpetrators of domestic violence and abuse: A systematic review and meta-synthesis. BMJ Open, 11(5), e043183. https://doi.org/10.1177/1558689816651808
Campbell, C. (2021). When the personal is not political: Experiences of collective agency amongst participants in the domestic violence response in London, UK. Critical Public Health, 31(3), 280–292. https://doi.org/10.1080/09581596.2021.1874296
Campbell, E., & Vlais, R. (2019). Bringing pathways towards accountability together: Perpetrator experiences and system roles and responsibilities. Centre for Innovative Justice. https://cij.org.au/cms/wp-content/uploads/2018/08/bringing-pathways-towards-accountability-together-perpetrator-experiences-and-system-roles-and-responsibilities-170519.pdf
Campbell, R., Goodman-Williams, R., & Javorka, M. (2019). A trauma-informed approach to sexual violence research ethics and open science. Journal of Interpersonal Violence, 34(23–24), 4765–4793. https://doi.org/10.1177/0886260519871530
Capaldi, D., Knoble, N., Shortt, J., & Kim, H. (2012). A systematic review of risk factors for intimate partner violence. Partner Abuse, 3(2), 231–280. https://doi.org/10.1891/1946-6560.3.2.231
Carlson, B., Day, M., & Farrelly, T. (2021). What works? Exploring the literature on Aboriginal and Torres Strait Islander healing programs that respond to family violence (Research report, Issue 01/2021). https://www.anrows.org.au/publication/what-works-exploring-the-literature-on-aboriginal-and-torres-strait-islander-healing-programs-that-respond-to-family-violence/
Carrington, K., Morley, C., Warren, S., Ryan, V., Ball, M., Clarke, J., & Vitis, L. (2021). The impact of COVID‐19 pandemic on Australian domestic and family violence services and their clients. Australian Journal of Social Issues, 56(4), 539–558. https://doi.org/10.1002/ajs4.183
Chung, D., Upton-Davis, K., Cordier, R., Campbell, E., Wong, T., Salter, M., . . . Bissett, T. (2020). Improved accountability: The role of perpetrator intervention systems (Research report, Issue 20/2020). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2020/06/Chung-RR-Improved-Accountability.pdf
Cortis, N., & Bullen, J. (2016). Domestic violence and women’s economic security: Building Australia’s capacity for prevention and redress: Final report (ANROWS Horizons, Issue 05/2016). ANROWS. https://www.anrows.org.au/publication/domestic-violence-and-womens-economic-security-building-australias-capacity-for-prevention-and-redress-final-report/
Council of Australian Governments. (2012). National Implementation Plan for the First Action Plan 2010–2013: Building a strong foundation. https://www.dss.gov.au/sites/default/files/documents/09_2012/imp_plan_27092012.pdf
Cox, P. (2015). Violence against women in Australia: Additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey, 2012 (Rev ed.; ANROWS Horizons, Issue 01.01/2016). ANROWS. https://www.anrows.org.au/publication/violence-against-women-in-australia-additional-analysis-of-the-australian-bureau-of-statistics-personal-safety-survey-2012/
Davis, M., Fernandez, B., Jonson-Reid, M., & Kyriakakis, S. (2021). Pathways to seeking help from a partner abuse intervention program: A qualitative study of voluntary and non-court-mandated Latino men’s experiences. Journal of Interpersonal Violence, 36(21–22), 10454–10478. https://doi.org/10.1177/0886260519884680
Day, A., Gerace, A., Oster, C., O’Kane, D., & Casey, S. (2018). The views of women in prison about help-seeking for intimate partner violence: At the intersection of survivor and offender. Victims & Offenders, 13(7), 974–994. https://doi.org/10.1080/15564886.2018.1514339
Day, A., Vlais, R., Chung, D., & Green, D. (2019). Evaluation readiness, program quality and outcomes in men’s behaviour change programs (Research report, Issue 01/2019). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/04/Day-et-al-Evaluation-readiness-MBCPs-Research-report-01.2019.pdf
Department of Social Services. (2019). Fourth Action Plan of the National Plan to Reduce Violence against Women and their Children 2010–2022. https://www.dss.gov.au/sites/default/files/documents/08_2019/fourth_action-plan.pdf
Diemer, K., Humphreys, C., Fogden, L., Gallant, D., Spiteri-Staines, A., Bornemisza, A., & Vercoe, E. (2020). Helping fathers value their children: Three site independent evaluation 2017–2020. The University of Melbourne. https://vawc.com.au/wp-content/uploads/2020/05/2020-Caring-Dads-Final-Report-23-3-2020.pdf
Dokkedahl, S., Kirubakaran, R., Bech-Hansen, D., Kristensen, T., & Elklit, A. (2022). The psychological subtype of intimate partner violence and its effect on mental health: A systematic review with meta-analyses. Systematic Reviews, 11(163), 1–16. https://doi.org/10.1186/s13643-022-02025-z
Dowling, C., & Morgan, A. (2019). Predicting repeat domestic violence: Improving police risk assessment. Trends and Issues in Crime and Criminal Justice, 581. Australian Institute of Criminology. https://www.aic.gov.au/publications/tandi/tandi581
Dowling, C., Morgan, A., Boyd, C., & Voce, I. (2018). Policing domestic violence: A review of the evidence (AIC Reports, Issue 13). Australian Institute of Criminology. https://www.aic.gov.au/publications/rr/rr13
Dyson, S., Frawley, P., & Robinson, S. (2017). “Whatever it takes”: Access for women with disabilities to domestic and family violence services (ANROWS Horizons, Issue 05/2017). ANROWS. https://www.anrows.org.au/publication/whatever-it-takes-access-for-women-with-disabilities-to-domestic-and-family-violence-services-final-report/
Edwards, K. M., Mauer, V., Huff, M., Farquhar-Leicester, A., Sutton, T., & Ullman, S. (2022). Disclosure of sexual assault among sexual and gender minorities: A systematic literature review. Trauma, Violence & Abuse. https://doi.org/10.1177/15248380211073842
Elliott, D., Bjelajac, P., Fallor, R. D., Markoff, L. S., & Reed, B. G. (2005). Trauma-informed or trauma-denied: Principles and implementation of trauma-informed services for women. Journal of Community Psychology, 33(4), 461–477. https://doi.org/10.1002/jcop.20063
Ellsberg, M., & Heise, L. (2002). Bearing witness: Ethics in domestic violence research. Lancet, 359(9317), 1599–1604. https://doi.org/10.1016/S0140-6736(02)08521-5
Evans, M., & Feder, G. (2016). Help‐seeking amongst women survivors of domestic violence: A qualitative study of pathways towards formal and informal support. Health Expectations, 19(1), 62–73. https://doi.org/10.1111/hex.12330
Family Violence Protection Act 2008 (Vic).
Felitti, V., & Anda, R. (2010). The relationship of adverse childhood experiences to adult medical disease, psychiatric disorders and sexual behaviour: Implications for healthcare. In R. Lanius, E. Vermetten, & C. Pain (Eds.), The impact of early life trauma on health and disease (pp. 77–87). Cambridge University Press.
Felitti, V., Anda, R., Nordenberg, D., Williamson, D., Spitz, A., Edwards, V., . . . Marks, J. (1998). Relationship of childhood abuse and household dysfunction to many leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventative Medicine, 14, 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Femi-Ajao, O., Kendal, S., & Lovell, K. (2020). A qualitative systematic review of published work on disclosure and help-seeking for domestic violence and abuse among women from ethnic minority populations in the UK. Ethnicity & Health, 25(5), 732–746. https://doi.org/10.1080/13557858.2018.1447652
Finkelhor, D., Ormrod, R., Turner, H., & Hamby, S. (2005). Measuring poly-victimization using the juvenile victimization questionnaire. Child Abuse & Neglect, 29(11), 1297–1312. https://doi.org/doi.org/10.1016/j.chiabu.2005.06.005
Fiolet, R., Tarzia, L., Hameed, M., & Hegarty, K. (2019). Indigenous peoples’ help-seeking behaviors for family violence: A scoping review. Trauma, Violence & Abuse, 22(2), 370–380. https://doi.org/10.1177/1524838019852638
Fitz-Gibbon, K., Burley, J., & Meyer, S. (2020). How do we keep family violence perpetrators “in view” during the COVID-19 lockdown? The Conversation. https://theconversation.com/how-do-we-keep-family-violence-perpetrators-in-view-during-the-covid-19-lockdown-135942
Flood, M., & Pease, B. (2009). Factors influencing attitudes to violence against women. Trauma, Violence & Abuse, 10(2), 125–42. https://doi.org/10.1177/1524838009334131
Ford-Gilboe, M., Aathen, N., Varcoe, C., MacMillan, H., Scott-Storey, K., Mantler, T., . . . Perrin, N. (2016). Development of a brief measure of intimate partner violence experiences: The composite abuse scale (revised). BMJ Open, 6(12). https://doi.org/10.1136/bmjopen-2016-012824
Forsdike, K., Tarzia, L., Flood, M., Vlais, R., & Hegarty, K. (2021). “A lightbulb moment”: Using the theory of planned behavior to explore the challenges and opportunities for early engagement of Australian men who use violence in their relationships. Journal of Interpersonal Violence, 36(7–8), NP3889–NP3913. https://doi.org/10.1177/0886260518780778
Fraga Dominguez, S., Storey, J. E., & Glorney, E. (2021). Help-seeking behavior in victims of elder abuse: A systematic review. Trauma, Violence, & Abuse, 22(3), 466–480. https://doi.org/10.1177/1524838019860616
Gallant, D., Andrews, S., Humphreys, C., Diemer, K., Ellis, D., Burton, J., . . . Bamblett, A. (2017). Aboriginal men’s programs tackling family violence: A scoping review. Journal of Australian Indigenous Issues, 20(2), 48–68. https://static1.squarespace.com/static/596d8907b3db2b5b22158a4e/t/5d351cd1a472a70001e21851/1563761876804/Gallant+et+al+Aboriginal+ Men%27s+Programs+Scoping+Review.pdf
Garcia-Moreno, C., Hegarty, K., d’Oliveira, A., Koziol-McLain, J., Colombini, M., & Feder, G. (2015). The health-systems response to violence against women. Lancet, 385, 1567–1579. https://doi.org/10.1016/S0140-6736(14)61837-7
Ghafournia, N., & Easteal, P. (2019). Help-seeking experiences of immigrant domestic violence survivors in Australia: A snapshot of Muslim survivors. Journal of Interpersonal Violence, 36(19–20), 9008–9034. https://doi.org/10.1177/0886260519863722
Goodman, L., & Smyth, K. F. (2011). A call for a social network-oriented approach to services for survivors of intimate partner violence. Psychology of Violence, 1(2), 79–92. https://doi.org/10.1037/a0022977
Grace, K., & Anderson, J. (2016). Reproductive coercion: A systematic review. Trauma, Violence & Abuse, 19(4). https://doi.org/10.1177/1524838016663935
Gregory, A., Feder, G., Taket, A., & Williamson, E. (2017). Qualitative study to explore the health and well-being impacts on adults providing informal support to female domestic violence survivors. BMJ Open, 7(3), e014511. https://doi.org/10.1136/bmjopen-2016-014511
Gregory, A., Johnson, E., Feder, G., Campbell, J., Konya, J., & Perot, C. (2021). Perceptions of peer support for victim-survivors of sexual violence and abuse: An exploratory study with key stakeholders. Journal of Interpersonal Violence. https://doi.org/10.1177/08862605211007931
Hashimoto, N., Radcliffe, P., & Gilchrist, G. (2018). Help-seeking behaviors for intimate partner violence perpetration by men receiving substance use treatment: A mixed-methods secondary analysis. Journal of Interpersonal Violence, 36(7–8). https://doi.org/10.1177/0886260518770645
Healey, L., Humphreys, C., Tsantefski, M., Heward-Belle, S., & Mandel, D. (2018). Invisible practices: Intervention with fathers who use violence (Research to policy practice, Issue 04/2018). ANROWS. https://www.anrows.org.au/publication/invisible-practices-intervention-with-fathers-who-use-violence-key-findings-and-future-directions/
Hegarty, K., Andrews, S., & Tarzia, L. (2022). Transforming health systems to address gender-based violence in Australia. Medical Journal of Australia, 217(3), 159–166. https://doi.org/10.5694/mja2.51638
Hegarty, K., O’Doherty, L., Chondros, P., Valpied, J., Taft, A., Astbury, J., . . . Gunn, J. (2013). Effect of type and severity of intimate partner violence on women’s health and service use: Findings from a primary care trial of women afraid of their partners. Journal of Interpersonal Violence, 28(2), 273–294. https://doi.org/10.1177/0886260512454722
Hegarty, K., Spangaro, J., Kyei-Onanjiri, M., Valpied, J., Walsh, J., Chapman, J., & Koziol-McLain, J. (2021). Validity of the ACTS intimate partner violence screen in antenatal care: A cross sectional study. BMC Public Health, 2021(March 4). https://doi.org/10.21203/rs.3.rs-264487/v1
Hegarty, K., Tarzia, L., Rees, S., Fooks, A., Forsdike, K., Woodlock, D., . . . Amanatidis, S. (2017). Women’s input to a trauma-informed systems model of care in health settings: The WITH study (ANROWS Horizons, Issue 02/2017). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/WITH_Horizons_UPDATE_FINAL.pdf
Heron, R. L., & Eisma, M. C. (2021). Barriers and facilitators of disclosing domestic violence to the healthcare service: A systematic review of qualitative research. Health & Social Care in the Community, 29(3), 612–630. https://doi.org/10.1111/hsc.13282
Hodgson, R., Alwyn, T., John, B., Thom, B., & Smith, A. (2002). The FAST alcohol screening test. Alcohol and Alcoholism, 37(1), 61–66. https://doi.org/10.1093/alcalc/37.1.61
Hooker, L., Versteegh, L., Lindgren, H., & Taft, A. (2020). Differences in help-seeking behaviours and perceived helpfulness of services between abused and non-abused women: A cross-sectional survey of Australian postpartum women. Health & Social Care in the Community, 28(3), 958–968. https://doi.org/10.1111/hsc.12927
Hu, R., Xue, J., Lin, K., Sun, I. Y., Wu, Y., & Wang, X. (2020). The patterns and influencing factors of help-seeking decisions among women survivors of intimate partner violence in China. Journal of Family Violence, 36, 669–681. https://doi.org/10.1007/s10896-020-00145-5
Humphreys, C., & Campo, M. (2017). Fathers who use violence: Options for safe practice where there is ongoing contact with children (Child Family Community Australia information exchange, Issue 43). Australian Institute of Family Studies. https://aifs.gov.au/sites/default/files/publication-documents/fatherswho_useviolence-final-v2_0_0.pdf
Humphreys, C., Diemer, K., Bornemisza, A., Spiteri‐Staines, A., Kaspiew, R., & Horsfall, B. (2019). More present than absent: Men who use domestic violence and their fathering. Child & Family Social Work, 24(2), 321–329. https://doi.org/10.1111/cfs.12617
Humphreys, C., & Healey, L. (2017). PAThways and research into collaborative inter-agency practice: Collaborative work across the child protection and specialist domestic and family violence interface: Final report (ANROWS Horizons, Issue 03/2017). ANROWS. https://www.anrows.org.au/publication/pathways-and-research-into-collaborative-inter-agency-practice-collaborative-work-across-the-child-protection-and-specialist-domestic-and-family-violence-interface-the-patricia-project-final-report/
Humphreys, C., Kertesz, M., Healey, L., & Mandel, D. (2019). Shifting practice in domestic violence: Child protection workers partnering with mothers. In C. Zufferey & F. Buchanan (Eds.), Intersections of mothering (pp. 194–205). Routledge.
Humphreys, C., Thiara, R., Sharp, C., & Jones, J. (2015). Supporting the relationship between mothers and children in the aftermath of domestic violence. In C. Humphreys & N. Stanley (Eds.), Domestic violence and protecting children: New thinking and approaches (pp. 130–147). Jessica Kingsley Publishers.
Hydén, M. (2015). What social networks do in the aftermath of domestic violence. British Journal of Criminology, 55(6), 1040–1057. https://doi.org/10.1093/bjc/azv099
Indermaur, D. (2001). Young Australians and domestic violence. Trends and Issues in Crime and Criminal Justice, 195. Australian Institute of Criminology. https://www.aic.gov.au/publications/tandi/tandi195
Iratzoqui, A., & Cohn, E. G. (2020). The reporting and help‐seeking behaviors of domestic violence victims with criminal backgrounds. Sociology Compass, 14(4), e12771. https://doi.org/10.1111/soc4.12771
Kaspiew, R., Horsfall, B., Qu, L., Nicholson, J., Humphreys, C., Diemer, K., . . . Taft, A. (2017). Domestic and family violence and parenting: Mixed method insights into impact and support needs: Final report (ANROWS Horizons, Issue 04/2017). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/Parenting_Horizons_FINAL-1.pdf
Kelly, L., & Westmarland, N. (2016). Naming and defining “domestic violence”: Lessons from research with violent men. Feminist Review, 112(1), 113–127. https://doi.org/10.1057/fr.2015.52
Kertesz, M., Humphreys, C., Larance, L., Vicary, D., Spiteri-Staines, A., & Ovenden, G. (2019). Working with women who use force: A feasibility study protocol of the Positive (+) SHIFT group work programme in Australia. BMJ Open, 9(5), Article e027496. https://doi.org/10.1136/bmjopen-2018-027496
Kimber, M., Adham, S., Gill, S., McTavish, J., & MacMillan, H. (2018). The association between child exposure to intimate partner violence (IPV) and perpetration of IPV in adulthood: A systematic review. Child Abuse & Neglect, 76, 273–286. https://doi.org/10.1016/j.chiabu.2017.11.007
Kirkwood, B., & Sterne, J. (2003). Essential medical statistics (2nd ed.). Blackwell Science.
Klein, R. (2012). Responding to intimate violence against women: The role of informal networks. Cambridge University Press.
Kolar, K., Ahmad, F., Chen, L., & Erickson, P. (2015). Timeline mapping in qualitative interviews: A study of resilience with marginalized groups. International Journal of Qualitative Methods, 14(3), 13–32. https://doi.org/10.1177/160940691501400302
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Lowe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics, 50(6), 613–621. https://doi.org/10.1176/appi.psy.50.6.613
Kulkarni, S. (2019). Intersectional trauma-informed intimate partner violence (IPV) services: Narrowing the gap between IPV service delivery and survivor needs. Journal of Family Violence, 34, 55–64. https://doi.org/10.1007/s10896-018-0001-5
Lamb, K., Humphreys, C., & Hegarty, K. (2018). “Your behaviour has consequences”: Children and young people’s perspectives on reparation with their fathers after domestic violence. Children and Youth Services Review, 88, 164–169. https://doi.org/10.1016/j.childyouth.2018.03.013
Latta, R. E., & Goodman, L. (2011). Intervening in partner violence against women: A grounded theory exploration of informal network members’ experiences. Counseling Psychologist, 39(7), 973–1023. https://doi.org/10.1177/0011000011398504
Lelaurain, S., Graziani, P., & Lo Monaco, G. (2017). Intimate partner violence and help-seeking: A systematic review and social psychological tracks for future research. European Psychologist, 22(4), 263–281. https://doi.org/10.1027/1016-9040/a000304
Levant, R. F. (2011). Research in the psychology of men and masculinity using the gender role strain paradigm as a framework. American Psychologist, 66(8), 765–776. https://doi.org/10.1037/a0025034
Lévesque, S., Rousseau, C., Lessard, G., Bigaouette, M., Fernet, M., Valderrama, A., & Boulebsol, C. (2021). Qualitative exploration of the influence of domestic violence on motherhood in the perinatal period. Journal of Family Violence, 37(9), 275–287. https://doi.org/10.1007/s10896-021-00294-1
Li, S., Zhao, F., & Yu, G. (2019). Childhood maltreatment and intimate partner violence victimization: A meta-analysis. Child Abuse & Neglect, 88, 212–224. https://doi.org/10.1016/j.chiabu.2018.11.012
Li, S., Zhao, F., & Yu, G. (2020). A meta-analysis of childhood maltreatment and intimate partner violence perpetration. Aggression and Violent Behavior, 50, Article 101362. https://doi.org/10.1016/j.avb.2019.101362
Marsden, S., Humphreys, C., & Hegarty, K. (2021). Women survivors’ accounts of seeing psychologists: Harm or benefit? Journal of Gender-Based Violence, 5(1), 111–127. https://doi.org/10.1332/239868020X16040863370635
Martsolf, D. S., Draucker, C. B., Cook, C. B., Ross, R., & Stidham, A. W. (2010). A meta-summary of qualitative findings about professional services for survivors of sexual violence. Qualitative Report, 15(3), 489–506. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3153442/
McGinn, T., McColgan, M., & Taylor, B. (2020). Male IPV perpetrators’ perspectives on intervention and change: A systematic synthesis of qualitative studies. Trauma, Violence, & Abuse, 21(1), 97–112. https://doi.org/10.1177/1524838017742167
McGinn, T., Taylor, B., McColgan, M., & Lagdon, S. (2016). Survivor perspectives on IPV perpetrator interventions: A systematic narrative review. Trauma, Violence & Abuse, 17(3), 239–255. https://doi.org/10.1177/1524838015584358
McKenzie, M., Hegarty, K., Palmer, V., & Tarzia, L. (2022). “Walking on eggshells”: A qualitative study of how friends of young women experiencing intimate partner violence perceive their role. Journal of Interpersonal Violence, 37(9–10), NP7502–NP7527. https://doi.org/10.1177/0886260520969238
Meyer, S. (2010a). “Acting in the children’s best interest?”: Examining victims’ responses to intimate partner violence. Journal of Child & Family Studies, 20(4), 436–443. https://doi.org/10.1007/s10826-010-9410-7
Meyer, S. (2010b). Seeking help to protect the children?: The influence of children on women’s decisions to seek help when experiencing intimate partner violence. Journal of Family Violence, 25(8), 713–725. https://doi.org/10.1007/s10896-010-9329-1
Meyer, S. (2011). Seeking help for intimate partner violence: Victims’ experiences when approaching the criminal justice system for IPV-related support and protection in an Australian jurisdiction. Feminist Criminology, 6(4), 268–290. https://doi.org/10.1177/1557085111414860
Meyer, S. (2016). Still blaming the victim of intimate partner violence? Women’s narratives of victim desistance and redemption when seeking support. Theoretical Criminology, 20(1), 75–90. https://doi.org/10.1177/1362480615585399
Meyer, S. (2018). Motivating perpetrators of domestic and family violence to engage in behaviour change: The role of fatherhood. Child & Family Social Work, 23(1), 97–104. https://doi.org/https://doi.org/10.1111/cfs.12388
Meyer, S., & Stambe, R. M. (2021). Indigenous women’s experiences of domestic and family violence, help-seeking and recovery in regional Queensland. Australian Journal of Social Issues, 56(3), 443–458. https://doi.org/10.1002/ajs4.128
Mitra-Kahn, T., Newbigin, C., & Hardefeldt, S. (2016). Invisible women, invisible violence: Understanding and improving data on the experiences of domestic and family violence and sexual assault for diverse groups of women: State of knowledge paper (ANROWS Landscapes, Issue 01/2016). ANROWS. https://www.anrows.org.au/publication/invisible-women-invisible-violence-understanding-and-improving-data-on-the-experiences-of-domestic-and-family-violence-and-sexual-assault-for-diverse-groups-of-women-state-of-knowledge-paper/
Moran, R., & Asquith, N. (2020). Understanding the vicarious trauma and emotional labour of criminological research. Methodological Innovations, 13(2). https://doi.org/10.1177/2059799120926085
Morgan, A., Boxall, H., & Payne, J. L. (2022). Reporting to police by intimate partner violence victim-survivors during the COVID-19 pandemic. Journal of Criminology, 55(3). https://doi.org/10.1177/26338076221094845
Morgan, G., Butler, C., French, R., Creamer, T., Hillan, L., Ruggiero, E., . . . Trew, S. (2022). New ways for our families: Designing an Aboriginal and Torres Strait Islander cultural practice framework and system responses to address the impacts of domestic and family violence on children and young people (Research report, Issue 06/2022). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2022/04/Morgan-et-al-RR1_NewWaysOurFamilies.pdf
Morgan, K., Williamson, E., Hester, M., Jones, S., & Feder, G. (2014). Asking men about domestic violence and abuse in a family medicine context: Help seeking and views on the general practitioner role. Aggression and Violent Behavior, 19(6), 637–642. https://doi.org/10.1016/j.avb.2014.09.008
O’Doherty, L., Taft, A., McNair, R., & Hegarty, K. (2016). Fractured identity in the context of intimate partner violence: Barriers and opportunities to seeking help in health settings. Violence Against Women, 22(2), 225–248. https://doi.org/10.1177/1077801215601248
Olsen, A., & Lovett, R. (2016). Existing knowledge, practice and responses to violence against women in Australian Indigenous communities (ANROWS Landscapes, Issue 02/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/FINAL-02.16_3.2-AIATSIS-Landscapes-WEB-1.pdf
Oram, S., Fisher, H., Minnis, H., Seedat, S., Walby, S., Hegarty, K., . . . Howard , L. M. (2022). The Lancet Psychiatry Commision on intimate partner violence and mental health: Advancing mental health services, research, and policy. Lancet Psychiatry, 9(6), 487–524. https://doi.org/10.1016/S2215-0366(22)00008-6
Oram, S., Trevillion, K., Khalifeh, H., Feder, G., & Howard, L. (2013). Systematic review and meta-analysis of psychiatric disorder and the perpetration of partner violence. Epidemiology and Psychiatric Sciences, 23(4). https://doi.org/10.1017/S2045796013000450
Osborn, M., & Rajah, V. (2020). Understanding formal responses to intimate partner violence and women’s resistance processes: A scoping review. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838020967348
Our Watch. (2017). Primary prevention of family violence against people from LGBTI communities. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2019/11/07031955/Primary-Prevention-of-FV-against-LGBTI-people-Report-Accessible-PDF.pdf
Our Watch. (2018a). Changing the picture: Background paper: Understanding violence against Aboriginal and Torres Strait Islander women and their children. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2020/09/20231756/Changing-the-picture-Part-1-AA.pdf
Our Watch. (2018b). Changing the picture: A national resource to support the prevention of violence against Aboriginal and Torres Strait Islander women and their children. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2020/09/20231759/Changing-the-picture-Part-2-AA.pdf
Our Watch, & VicHealth. (2021). Change the story: A shared framework for the primary prevention of violence against women and their children in Australia. Our Watch. https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2021/11/18101814/Change-the-story-Our-Watch-AA.pdf
Partners for Prevention. (2020). The UN multi-country study on men and violence in Asia and the Pacific. United Nations. http://www.partners4prevention.org/about-prevention/research/men-and-violence-study
Patterson, M., Markey, M., & Somers, J. (2012). Multiple paths to just ends: Using narrative interviews and timelines to explore health equity and homelessness. International Journal of Qualitative Methods, 11(2), 132–151. https://doi.org/10.1177/16094069120110020
Peitzmeier, S. M., Malik, M., Kattari, S. K., Marrow, E., Stephenson, R., Agénor, M., & Reisner, S. L. (2020). Intimate partner violence in transgender populations: Systematic review and meta-analysis of prevalence and correlates. American Journal of Public Health, 110(9), e1–e14. https://doi.org/10.2105/AJPH.2020.305774
Pentaraki, M., & Speake, J. (2020). Domestic violence in a COVID-19 context: Exploring emerging issues through a systematic analysis of the literature. Open Journal of Social Sciences, 8(10), 193–211. https://doi.org/10.4236/jss.2020.810013
Pfitzner, N., Fitz-Gibbon, K., & True, J. (2022). When staying home isn’t safe: Australian practitioner experiences of responding to intimate partner violence during COVID-19 restrictions. Journal of Gender-Based Violence, 6(2), 297–314. https://doi.org/10.1332/239868021X16420024310873
Piquero, A. R., Jennings, W. G., Jemison, E., Kaukinen, C., & Knaul, F. M. (2021). Domestic violence during the COVID-19 pandemic: Evidence from a systematic review and meta-analysis. Journal of Criminal Justice, 74, 101806. https://doi.org/10.1016/j.jcrimjus.2021.101806
Pokharel, B., Hegadoren, K., & Papathanassoglou, E. (2020). Factors influencing silencing of women who experience intimate partner violence: An integrative review. Aggression and Violent Behavior, 52, 101422. https://doi.org/10.1016/j.avb.2020.101422
Potter, L., Morris, R., Hegarty, K., Garcia- Moreno, C., & Feder, G. (2020). Categories and health impacts of intimate partner violence in the World Health Organization multi-country study on women’s health and domestic violence. International Journal of Epidemiology, 1–11. Advance online publication. https://doi.org/10.1093/ije/dyaa220
Price, E., Sharman, L., Douglas, H., Sheeran, N., & Dingle, G. (2019). Experiences of reproductive coercion in Queensland women. Journal of Interpersonal Violence, 37(5–6), NP2823–NP2843. https://doi.org/10.1177/0886260519846851
PriceWaterhouseCoopers Australia. (2015). A high price to pay: The economic case for preventing violence against women. https://www.pwc.com.au/pdf/a-high-price-to-pay.pdf
Ragusa, A. (2016). Rurality’s influence on women’s intimate partner violence experiences and support needed for escape and healing in Australia. Journal of Social Service Research, 43(2), 270–295. https://doi.org/10.1080/01488376.2016.1248267
Ravi, K., Robinson, S. R., & Voth Schrag, R. (2021). Facilitators of formal help-seeking for adult survivors of IPV in the United States: A systematic review. Trauma, Violence, & Abuse. https://doi.org/10.1177/1524838021995954
Rawlins, W. K. (2008). The compass of friendship: Narratives, identities, and dialogues. Sage Publications.
Reisenhofer, S., & Seibold, C. (2013). Emergency healthcare experiences of women living with intimate partner violence. Journal of Clinical Nursing, 22(15–16), 2253–2263. https://doi.org/10.1111/j.1365-2702.2012.04311.x
Riessman, C. (2008). Narrative methods for the human sciences. Sage.
Rivas, C., Vigurs, C., Cameron, J., & Yeo, L. (2019). A realist review of which advocacy interventions work for which abused women under what circumstances. Cochrane Database Syst Rev, 6, CD013135. https://doi.org/10.1002/14651858.CD013135.pub2
Robinson, S. R., Ravi, K., & Voth Schrag, R. (2020). A systematic review of barriers to formal help seeking for adult survivors of IPV in the United States, 2005–2019. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838020916254
Santoniccolo, F., Trombetta, T., & Rollè, L. (2021). The help-seeking process in same-sex intimate partner violence: A systematic review. Sexuality Research and Social Policy. https://doi.org/10.1007/s13178-021-00629-z
Satyen, L., Piedra, S., Ranganathan, A., & Golluccio, N. (2018). Intimate partner violence and help-seeking behavior among migrant women in Australia. Journal of Family Violence, 33(7), 447–456. https://doi.org/10.1007/s10896-018-9980-5
Satyen, L., Rogic, A. C., & Supol, M. (2019). Intimate partner violence and help-seeking behaviour: A systematic review of cross-cultural differences [Review]. Journal of Immigrant and Minority Health, 21(4), 879–892. https://doi.org/10.1007/s10903-018-0803-9
Segrave, M., & Pfitzner, N. (2020). Family violence and temporary visa holders during COVID-19. Monash. https://bridges.monash.edu/articles/online_resource/Family_violence_and_temporary_visa_holders_during_COVID-19/12987938
Shackelford, T. K., & Mouzos, J. (2005). Partner killing by men in cohabiting and marital relationships: A comparative, cross-national analysis of data from Australia and the United States. Journal of Interpersonal Violence, 20(10), 1310–1324. https://doi.org/10.1177/0886260505278606
Sheehan, K., Thakor, S., & Stewart, D. (2012). Turning points for perpetrators of intimate partner violence. Trauma, Violence & Abuse, 13(1), 30–40. https://doi.org/10.1177/1524838011426016
Shimmin, C., Wittmeier, K., Lavoie, J., Wicklund, E., & Sibley, K. (2017). Moving towards a more inclusive patient and public involvement in health research paradigm: The incorporation of a trauma-informed intersectional analysis. BMC Health Services Research, 17(539). https://doi.org/10.1186/s12913-017-2463-1
Sripada, P. (2021). Help-seeking behavior of South Asian women in domestic violence: A scoping review. Journal of Human Behavior in the Social Environment, 31(6), 729–750. https://doi.org/10.1080/10911359.2020.1811823
StataCorp. (2015). Stata Statistical Software: Release 15. https://www.stata.com
Strang, A., O’Brien, O., Sandilands, M., & Horn, R. (2020). Help-seeking, trust and intimate partner violence: Social connections amongst displaced and non-displaced Yezidi women and men in the Kurdistan region of northern Iraq. Conflict and Health, 14, 61. https://doi.org/10.1186/s13031-020-00305-w
Su, Z., McDonnell, D., Roth, S., Li, Q., Šegalo, S., Shi, F., & Wagers, S. (2021). Mental health solutions for domestic violence victims amid COVID-19: A review of the literature. Globalization and Health, 17(67). https://doi.org/10.1186/s12992-021-00710-7
Sullivan, C., & Goodman, L. (2019). Advocacy with survivors of intimate partner violence: What it is, what it isn’t, and why it’s critically important. Violence Against Women, 25(16), 2007–2023. https://doi.org/10.1177/1077801219875826
Summers, A. (2022). The choice: Violence or poverty. Paul Ramsay Foundation. https://paulramsayfoundation.org.au/wp-content/uploads/2022/07/TheChoice-violence-or-poverty-web.pdf
Sylaska, K. M., & Edwards, K. M. (2014). Disclosure of intimate partner violence to informal social support network members: A review of the literature. Trauma, Violence & Abuse, 15(1), 3–21. https://doi.org/10.1177/1524838013496335
Taket, A., O’Doherty, L., Valpied, J., & Hegarty, K. (2014). What do Australian women experiencing intimate partner abuse want from family and friends? Qualitative Health Research, 24(7), 983–996. https://doi.org/10.1177/1049732314540054
Tarzia, L. (2020). “It went to the very heart of who I was as a woman”: The invisible impacts of intimate partner sexual violence. Qualitative Health Research, 31(2), 287–297. https://doi.org/10.1177/1049732320967659
Tarzia, L., Bohren, M., Cameron, J., Garcia-Moreno, C., O’Doherty, L., Fiolet, R., . . . Hegarty, K. (2020). Women’s experiences and expectations after disclosure of intimate partner abuse to a healthcare provider: A qualitative meta-synthesis. BMJ Open, 10(11), e041339. https://doi.org/10.1136/bmjopen-2020-041339
Tarzia, L., Cornelio, R., Forsdike, K., & Hegarty, K. (2018). Women’s experiences receiving support online for intimate partner violence: How does it compare to face-to-face support from a health professional? Interacting With Computers, 30(5), 433–443. https://doi.org/doi.org/10.1093/iwc/iwy019
Tarzia, L., Forsdike, K., Feder, G., & Hegarty, K. (2020). Interventions in health settings for male perpetrators or victims of intimate partner violence. Trauma, Violence & Abuse, 21(1), 123–137. https://doi.org/10.1177/1524838017744772
Tarzia, L., & Hegarty, K. (2020). A conceptual re-evaluation of reproductive coercion: Centring intent, fear and control. BMC Reproductive Health, 18(87). https://doi.org/10.1186/s12978-021-01143-6
Tarzia, L., & Hegarty, K. (2022). “He’d tell me I was frigid and ugly and force me to have sex with him anyway”: Women’s experiences of co-occurring sexual violence and psychological abuse in heterosexual relationships. Journal of Interpersonal Violence, 1–21. https://doi.org/10.1177/08862605221090563
Tarzia, L., Iyer, D., Thrower, E., & Hegarty, K. (2017). “Technology doesn’t judge you”: Young Australian women’s views on using the internet and smartphones to address intimate partner violence. Journal of Technology in Human Services, 35(3), 199–218. https://doi.org/doi.org/10.1080/15228835.2017.1350616
Tengku Hassan, T. N. F., Ali, S. H., & Salleh, H. (2015). Patterns of help-seeking among women experiencing intimate partner violence in Malaysia. Asian Journal of Womens Studies, 21(1), 77–92. https://doi.org/10.1080/12259276.2015.1029226
Trotter, J. L., & Allen, N. E. (2009). The good, the bad, and the ugly: Domestic violence survivors’ experiences with their informal social networks. American Journal of Community Psychology, 43(3), 221–231. https://doi.org/10.1007/s10464-009-9232-1
Usher, K., Bhullar, N., Durkin, J., Gyamfi, N., & Jackson, D. (2020). Family violence and COVID‐19: Increased vulnerability and reduced options for support. International Journal of Mental Health Nursing, 29(4), 549–552. https://doi.org/10.1111/inm.12735
Valpied, J., Cini, A., O’Doherty, L., Taket, A., & Hegarty, K. (2014). “Sometimes cathartic. Sometimes quite raw”: Benefit and harm in an intimate partner violence trial. Aggression and Violent Behavior, 19(6), 673–685. https://doi.org/https://doi.org/10.1016/j.avb.2014.09.005
Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Block, K., . . . Warr, D. (2016). Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: The ASPIRE Project: Key findings and future directions (ANROWS Compass, Issue 08/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/01/Aspire_Compass_final.pdf
Victorian Government. (2016). Royal Commission into Family Violence: Summary and recommendations. https://www.parliament.vic.gov.au/file_uploads/1a_RFV_112ppA4_SummaryRecommendations.WEB_DXQyLhqv.pdf
Vogel, D. L., & Heath, P. J. (2016). Men, masculinities, and help-seeking patterns. In APA handbook of men and masculinities (pp. 685–707). American Psychological Association.
Waller, B. Y., Harris, J., & Quinn, C. R. (2021). Caught in the crossroad: An intersectional examination of African American women intimate partner violence survivors’ help seeking. Trauma, Violence, & Abuse, 23(4), 1235–1248. https://doi.org/10.1177/1524838021991303
Ware, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233. https://doi.org/10.1097/00005650-199603000-00003
Webster, K. (2016). A preventable burden: Measuring and addressing the prevalence and health impacts of intimate partner violence in Australian women (ANROWS Compass, Issue 07/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/01/28-10-16-BOD-Compass.pdf
Webster, K., Diemer, K., Honey, N., Mannix, S., Mickle, J., Morgan, J., . . . Ward, A. (2018). Australians’ attitudes to violence against women and gender equality: Findings from the 2017 National Community Attitudes Survey (NCAS). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/10/anr001-NCAS-report-WEB-1019.pdf
Wendt, S., Chung, D., Elder, A., Hendrick, A., & Hartwig, A. (2017). Seeking help for domestic and family violence: Exploring regional, rural, and remote women’s coping experiences: Final report (ANROWS Horizons, Issue 06/2017). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/RP.14.04_RWR_Horizons-FINAL-1709.pdf
Wendt, S., Seymour, K., Buchanan, F., Dolman, C., & Greenland, N. (2019). Engaging men who use violence: Invitational narrative approaches (Research report, Issue 05/2019). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/10/PI.17.12-Wendt-Invitational-Narrative-Therapies-ANROWS-Research-Report.pdf
World Health Organization (2012). Violence against women: Intimate partner violence and sexual violence against women. http://www.who.int/mediacentre/factsheets/fs239/en/index.html
World Health Organization. (2013a). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf
World Health Organization. (2013b). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. http://www.who.int/reproductivehealth/publications/violence/9789241548595/en/
World Health Organization. (2014). Health care for women subjected to intimate partner violence or sexual violence: A clinical handbook. http://apps.who.int/iris/bitstream/10665/136101/1/WHO_RHR_14.26_eng.pdf
World Health Organization. (2016). Ethical and safety recommendations for intervention research on violence against women. https://apps.who.int/iris/bitstream/handle/10665/251759/9789241510189-eng.pdf
Wright, E. N., Anderson, J., Phillips, K., & Miyamoto, S. (2021). Help-seeking and barriers to care in intimate partner sexual violence: A systematic review. Trauma, Violence & Abuse. https://doi.org/10.1177/1524838021998305
Wu, E., El-Bassel, N., Gilbert, L., Sarfo, B., & Seewald, R. (2010). Criminal justice involvement and service need among men on methadone who have perpetrated intimate partner violence. Journal of Criminal Justice, 38(4), 835–840. https://doi.org/10.1016/j.jcrimjus.2010.05.012
Zinzow, H., Littleton, H., Muscari, E., & Sall, K. (2021). Barriers to formal help-seeking following sexual violence: Review from within an ecological systems framework. Victims & Offenders, 17(6), 893–918. https://doi.org/10.1080/15564886.2021.1978023
Appendix A:
Literature review 2010 to 2020
Search strategy and key terms
We undertook a rapid systematic review of the peer-reviewed literature focused on IPV and/or SV, help-seeking behaviours and service needs. We identified relevant studies and reviews of the literature using a systematic search of key bibliographic databases (MEDLINE, Embase, PsycINFO, Cochrane databases, Applied Social Sciences Index and Abstracts: ASSIA, Web of Science, PsycArticles and Scopus). The search was conducted during September 2020, using the subject headings and key terms shown in the table below. This was informally updated in May 2022 to include more recent systematic review articles. We also checked the reference lists of all included records to identify additional studies, and undertook hand-searching and communication with experts in the field to identify any further potentially relevant sources of data. All searches were filtered to 1 January 2010 onwards to find literature related to contemporary service delivery.
| Women who experience IPV and/or SV | People who perpetrate IPV and/or SV against women |
|---|---|
| (Women OR Female) AND (Intimate partner violence OR battered women OR domestic violence OR spouse abuse OR family violence OR rape OR sexual victimisation OR sexual aggression OR sexual violence OR sexual coercion OR sexual assault) AND (Help seeking) | (Women OR female OR men OR male OR man) AND (Intimate partner violence OR perpetration OR domestic violence OR spouse abuse OR family violence OR Abuse and violence OR batter OR rape OR sexual perpetration OR sexual aggression OR sexual violence OR sexual coercion OR sexual assault) AND (Help seeking) |
Inclusion/exclusion criteria
Inclusion was limited to studies where 1) participants were women aged 18 years and older who had experienced any type of IPV and/or SV or people aged 18 years and older who had perpetrated any type of IPV and/or SV against women; and 2) the data focused on help-seeking behaviours. We excluded studies exclusively exploring experiences of disclosure in response to routine or universal screening in health settings, since this is a provider-initiated interaction. Study types of interest included quantitative or qualitative primary studies (any methodology); systematic reviews or meta-analyses; and peer-reviewed reports. Opinion pieces, theoretical articles, books and theses were excluded.
Search results
As illustrated in the PRISMA flowchart below, our search yielded 863 results after duplicates were removed. After screening the titles and/or abstracts (863), 666 (titles) and 105 (abstracts) records were removed based on the exclusion criteria. Of the remaining 92 records, the full text was screened to determine whether they met the inclusion criteria.
PRISMA flowchart
Text version of the figure above:
Identification:
- Records identified through database searching (n=1,035)
- Additional records identified through other sources (n=12)
Between Identification and Screening
- Records after duplicated removed (n=863)
Screening
- Records screened (n=863)
- Records excluded (based on article title): (n=666)
-
- Reasons for exclusions: E.g. studies exploring characteristics and/or prevalence of IPV; theoretical discussions about IPV
Eligibility
- Assessed for eligibility (n=197)
- Review excluded based on title and abstract, with reasons: (n=105)
-
- Reasons for exclusions: E.g. factors associated with IPV; intersections between IPC and violence against children
- Assessed for eligibility (n=197)
- Reviewed excluded based on title and abstract, with reasons: (n=105)
-
- Reasons for exclusions: E.g. factors associated with IPV; intersections between IPC and violence against children
Included
- Women victims and survivors of IPV and/or SV: N=69
-
- 7 previous reviews; 47 primary studies outside Australia; 4 quantitative and 11 qualitative studies in Australia
- Perpetrators of IPV against women: N=3
-
- 3 primary studies included
Help-seeking behaviours of IPV and/or SV victims and survivors
Overall, 69 records were related to women who experience IPV and/or SV (seven previous reviews; 47 primary studies outside Australia; four quantitative and 11 qualitative studies in Australia). Findings for the Australian context are reported in the main document.
In terms of women’s help-seeking for IPV more generally, 47 primary studies were based outside Australia, for example, in Canada (Barrett & Pierre, 2011), the United States (Anyikwa, 2015), Malaysia (Tengku Hassan et al., 2015), China (Hu et al., 2020) and Iraq (Strang et al., 2020). There were six global narrative reviews related to women’s help-seeking behaviours for experiences of IPV (Afrouz et al., 2020; Femi-Ajao et al., 2020; Fiolet et al., 2019; Lelaurain et al., 2017; Robinson et al., 2020; Satyen et al., 2019) and one review relating to help-seeking for SV (Martsolf et al., 2010). Not all the reviews focused exclusively on women, but women formed the vast majority of the participants. Characteristics of the included reviews are outlined in the Table A1.
Overall, the reviews were mostly limited to qualitative studies that explored barriers to IPV disclosure and help-seeking of women from culturally and linguistically diverse backgrounds. For example, for women from Black and minority ethnic populations, barriers to IPV disclosure included immigration status, unsupportive attitudes of staff within mainstream services and language-related barriers (Femi-Ajao et al., 2020), yet escalation of abuse and serious safety concerns for children were facilitators of help-seeking. In contrast, for Muslim women, maintaining family harmony, honour and reputation were among key barriers to IPV disclosure and help-seeking behaviours (Afrouz et al., 2020). A scoping review of global Indigenous studies found that Indigenous peoples are generally reluctant to engage in help-seeking behaviours for IPV due to shame, tight-knit communities, and inappropriate service responses causing mistrust and fear (Fiolet et al.,2019). For SV, Martsolf and colleagues (2010) found that victims and survivors wanted their abuse histories taken seriously and expected service providers to display professional competence and sensitivity. Fear of not being believed was a barrier to help-seeking, as were judgemental or dismissive responses.
In terms of study quality, many studies included in the above reviews were found to have major methodological limitations. For example, studies did not adequately describe methods of data collection and/or analysis, and had minimum or no consideration of ethical issues. Similarly, most quantitative studies included in Satyen et al.’s review (2019) were classified as having a high risk of bias due to sampling bias or recall bias.
Table A1: Characteristics of reviews exploring women’s help-seeking for IPV, 2010–2020
| Study | Aim and objectives | Design | Included studies | No. of participants | Data synthesis | Summary of findings | Study quality and limitations |
|---|---|---|---|---|---|---|---|
| Femi-Ajao et al., 2020 | To explore barriers to IPV disclosure; facilitators of help-seeking; and self-perceived impacts of IPV | Qualitative systematic review | 4 qualitative studies (8 publications) | 83 women (Black and minority ethnic populations) | Thematic analysis | Barriers to IPV disclosure:
Facilitators of help-seeking:
Impact of IPV: Loss of identity, shame, denial of abuse, lack of choice as women |
|
| Afrouz et al., 2020 | To explore Muslim women’s barriers to IPV disclosure and help-seeking | Critical systematic review | 21 (14 qualitative and mixed method, 6 quantitative, and 1 literature review) | 567 Muslim women (qualitative studies) | Thematic analysis | Barriers to IPV disclosure and help-seeking:
|
|
| Fiolet et al., 2019 | To explore the views Indigenous peoples have on help-seeking for IPV | Scoping review | 15 studies (11 qualitative) | 600 Indigenous women | Thematic analysis | Indigenous peoples are reluctant to engage in help-seeking behaviours:
|
|
| LeLaurain et al., 2017 | To explore factors that facilitate or inhibit help-seeking for IPV | Systematic review | 90 studies (47 qualitative or mixed methods) | Not reported | Barriers and facilitators to IPV help-seeking:
|
| |
| Martsolf et al., 2010 | To explore how victims and survivors of SV utilise professional services | Systematic review and meta-summary | 31 qualitative studies | 1,024 total, 984 women | Qualitative meta-summary | Barriers and facilitators to SV help-seeking:
|
|
| Robinson et al., 2020 | To explore barriers to help-seeking from formal services for IPV survivors | Systematic review | 29 (22 qualitative) | 862 women living in US | Thematic analysis | Barriers to help seeking:
|
|
| Satyen et al., 2019 | To explore cross-cultural differences in help-seeking behaviour of women who have experienced IPV | Systematic review | 17 (quantitative) | 40,904 | Narrative synthesis |
|
|
Notes: CASP = Critical Appraisal Skills Programme
Help-seeking by people who use IPV and/or SV, 2010–2020
Studies focused on the help-seeking behaviours of people who use violence are extremely limited. This is the case for self-identified perpetrators who have accessed services voluntarily, perpetrators who have been mandated into services, and perpetrators who have not been identified as such and use community and health services. Although there is some limited literature published prior to 2010, our search found only three studies focused on male perpetrators of IPV published between 2010 and 2020 (see Table A2). No relevant articles were found about women’s use of IPV and/or SV and their help-seeking behaviours, nor any articles that focused on the perpetration of IPV and/or SV.
In general, research undertaken to date on perpetrators of IPV has been primarily focused on assessing the efficacy of specific programs (for example, men’s behaviour change programs) rather than exploring perpetrator service needs or experiences overall. This may be in large part because the system is designed to respond to violence after it has occurred rather than trying to engage and tailor services to perpetrators before risk has escalated. Some limited exceptions include studies exploring the service needs of men attending programs to address both IPV and other co-occurring problems. For example, in a quantitative study of men attending a substance treatment program who had also used IPV, Wu et al. (2010) found that the majority of participants indicated a need for medical, employment, substance use, legal, psychological and family services. Service needs were heightened in the period following criminal justice system involvement. Althoughthe study suffered from some methodological limitations, the authors cautiously concluded that their findings are suggestive of the willingness of perpetrators to seek help, and that therefore efforts ought to focus on engaging men rather than mandating or coercing them into accessing services. A mixed-method study by Hashimoto and colleagues (2018) – also with men in substance use treatment – explored pathways and barriers to disclosure and help-seeking. They found that participants were more likely to disclose perpetration to family, friends or other informal supports, but to seek help from formal services such as health professionals. Barriers to disclosure included fear of child removal, shame and embarrassment, and normalisation or minimisation of their behaviours. Another mixed-method study with men attending general practices who had used or experienced IPV (Morgan et al., 2014) found that men wanted to be asked abouttheir use of violence and were more likely to seek support via friends and family or health settings. They also reported shame and a reluctance to receive difficult feedback as barriers to disclosure.
Table A2: Characteristics of studies exploring help-seeking for IPV perpetration
| Study | Aim and objectives | Design | Included studies | No. of participants | Data synthesis | Summary of findings | Study quality and limitations |
|---|---|---|---|---|---|---|---|
| Hashimoto et al., 2018 | To examine IPV perpetration disclosure and help-seeking among male IPV perpetrators receiving substance use treatment | Mixed method primary study | UK (substance use treatment) | 170 men (20 men for qualitative phase) | Thematic analysis and logistic regression | Men who disclosed IPV perpetration to both formal and informal resources had:
Barriers to disclosure and help-seeking for IPV perpetration:
|
|
| Morgan et al., 2014 | To explore male help-seeking practices in relation to IPV | Mixed method primary study (cross-sectional survey and interview) | UK (general practice) | 1,368 men attending general practice (31 interviews) | Thematic analysis and descriptive statistics | Men were most likely to seek informal support from friends or family. The next most likely source of support was the family doctor |
|
| Wu et al., 2010 | To explore help-seeking associations and barriers among men attending a methadone maintenance treatment program who had used IPV | Face-to-face structured interview | US | 108 men | Logistic regression | Men expressed the need for support from medical, employment, substance use, legal, psychological and family services. These needs were heightened closer to time of involvement with criminal justice |
|
Appendix B:
Survey (Victims and survivors)
Start of Block: Screening
Q265 Hello, thank you for taking an interest in the VOICES project. Before we start, we need to ask you some initial questions in order to understand whether the project is suited to you and your experiences. It should take approximately 2 minutes to complete. Upon completion of these initial questions, if the survey is a good match to you and your experiences, you will automatically proceed to the main survey. Participating in the survey will help us understand women’s experiences and need for services. Responses to the survey are strictly confidential. Your voice is important. If you have any questions, please contact the project team at voice_project@unimelb.edu.au. Remember there are resources available here if you need support at any time.
Q266 How do you identify?
- Male (1)
- Female (2)
- Non-binary (3)
- Prefer not to say (4)
- Prefer to self-identify (5) ________________________________________________
Q267 How old are you?
- 17 or younger (1)
- 18–24 (0)
- 25–34 (2)
- 35–44 (3)
- 45+ years (4)
Q268 What country do you live in?
- China (1)
- Australia (0)
- India (2)
- England (3)
- Indonesia (4)
- Canada (5)
- Other (6) ________________________________________________
Q269 How did you find this survey?
- Domestic violence service (1)
- Community service (2)
- Twitter (3)
- Instagram (4)
- Facebook (5)
- University of Melbourne student notices (6)
- Other (7) ________________________________________________
Q270 In the last five years have you ever… (Please select all that apply)
- Been afraid of a partner? (1)
- Been controlled by a partner? (2)
- Been physically hurt by a partner? (3)
- Experienced unwanted sex by anyone, including a partner? (4)
- None of the above (0)
Q271 The following question is asked to determine if you are a human or a robot…
Q272 What is 2+2?
- 6 (1)
- 8 (2)
- 4 (3)
Display This Question:
If How do you identify? = Female
Or How old are you? = 17 or younger
Or What country do you live in? = Australia
Or In the last five years have you ever… (please select all that apply) = None of the above
Or What is 2+2? = 4
Q276 We thank you for your interest in our project and for reading through the provided materials. As the present project is about adult women’s experiences of fear or violence within intimate partner relationships who live in Australia, one or more of your answers has made you ineligible for the current study. If you have any questions, please email the project team here: voice_project@unimelb.edu.au.
Remember, there are resources available here if you need support at any time.
Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed
End of Block: Screening
Start of Block: INTRO_BLOCK
Display This Question:
If How do you identify? = Female
And How old are you? = 17 or younger
And What country do you live in? = Australia
And In the last five years have you ever… (please select all that apply) = None of the above
And What is 2+2? = 4
Q1 Welcome to the VOICES Project survey. Thank you for answering our initial questions, it looks as if you are eligible to complete the survey. The VOICES Project aims to understand your experiences of abuse and violence during your lifetime and what supports you might need from services. Your answers will help us further understand how to best support women’s health and wellbeing.
This survey asks about some background information, health and wellbeing, domestic violence and unwanted sexual experiences, and how we can support women more effectively. Some of the questions are sensitive so there are resources available by clicking here. These resources will also be made available throughout the survey.
All information you give us in this survey is confidential. The survey will take approximately 30 minutes to complete. After completing the survey, you will be given the option to enter into a draw to win an iPad. The project team is based at the Safer Families Centre, The University of Melbourne and ANROWS. If you have any questions about the project, please email: voice_project@unimelb.edu.au.We recommend that you complete the survey in private, please click here for further advice on keeping safe online. Feel free take a break at any time. Remember, if you exit the survey and return later, as this survey is anonymous, you will only be returned to where you left off if you use the same device that you started the survey on.
How to fill in the survey:
Please read the questions carefully and follow the instructions. There are no right or wrong answers, just put what is right for you. Please select only one answer per question unless we state that you can answer more than one answer.
End of Block: INTRO_BLOCK
Start of Block: ABOUT_YOU
Q2 About You We will start this survey with a few quick questions about your background. These questions are important because they allow your answers to be compared with those of other people with a similar background to you, without identifying anybody.
Q3 Do you identify as a woman?
- Yes (1)
- No (0)
Display This Question:
If Do you identify as a woman? = No
Q4 We thank you for your interest in our project and for reading through the provided materials. As the present project is about women’s experiences, this makes you ineligible. Should you wish to speak with someone from the project team, please contact Jacqueline by emailing Voice_Project@unimelb.edu.au. Should you wish to speak with someone for support, resources are available. Please click here. Once again, we thank you for your time and interest in the VOICES Project.
| Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed |
Q5 What is your age in years?
Please write a number in the box.
________________________________________________________________
Q6 What is your postcode where you live most of the time?
________________________________________________________________
Q7 Were you born in Australia?
- Yes (1)
- No (0)
Display This Question:
If Were you born in Australia? = No
Q8 Which country were you born in? Please select one option.
- UK (1)
- New Zealand (2)
- China (3)
- Other (4)
- Sri Lanka (5)
- India (6)
- Italy (7)
- South Africa (8)
- Greece (9)
- Lebanon (10)
- Vietnam (11)
Display This Question:
If Were you born in Australia? = No
Q9 How long have you lived in Australia? Please write the number of years in the box below. If you are not sure, your best guess is fine.
________________________________________________________________
Display This Question:
If Were you born in Australia? = No
Q10 Are you…
- An Australian citizen? (1)
- On a permanent visa? (2)
- On a temporary visa? (3)
Q11 Is English your first language?
- Yes (1)
- No (0)
Q12 Do you identify as Aboriginal or Torres Strait Islander?
- Yes, Aboriginal (1)
- Yes, Torres Strait Islander (2)
- Yes, both Aboriginal and Torres Strait Islander (3)
- No, neither (4)
Q13 What is the gender of your current partner?
- Male (1)
- Female (2)
- Non-binary (3)
- Prefer not to disclose (4)
I do not have a current partner (5)
Q14 Who do you usually live with?
Please select all that apply.
- No one else (1)
- Your husband (2)
- Your male partner (3)
- Other relatives (7)
- Friends (8)
- Other (please specify) (9)
- Your female partner (10)
- Unrelated flat mate or co-tenant (4)
Q15 Do you have children?
- Yes (0)
- No (1)
Display This Question:
If Do you have children? = Yes
Q16 How many children are currently at home with you?
- No children (0)
- One child (1)
- Two children (2)
- Three children (3)
- Four or more children (4)
Q17 What is your present marital status?
This does not necessarily refer to your current living arrangement. Please select one option only.
- Never married (1)
- Widowed (2)
- Divorced (3)
- Separated but not divorced (4)
- Married (5)
Q18
This is the end of this section. When you feel ready, please click the next button to continue.
End of Block: ABOUT_YOU
Start of Block: HEALTH_WELLBEING
Q19
About your health and wellbeing This section is about how you’re feeling, both emotionally and physically. We are asking these questions because we are interested in how any relationship issues affects your emotional and physical wellbeing.
Q20 In general, would you say your health is:
- Excellent (1)
- Very good (2)
- Good (3)
- Fair (4)
- Poor (5)
Q21 Over the last 2 weeks, how often have you been bothered by the following problems?
| Not at all (0) | Several days (1) | More than half the days (2) | Nearly every day (3) | |
|---|---|---|---|---|
| Feeling nervous, anxious or on edge (1) | ||||
| Not being able to stop or control worrying (2) | ||||
| Feeling down, depressed, or hopeless (4) | ||||
| Little interest or pleasure in doing things (5) |
Q22 Do you have any long-term illness, health problem or disability, which limits your daily activities or the work you can do (including problems that are due to old age)?
- Yes (1)
- No (0)
Q23 Below are some statements about how you feel in yourself. Please read each statement and choose the response that most closely indicates how you have felt during the past month.
| Yes (1) | No (0) | |
|---|---|---|
| Do you avoid being reminded of experiences by staying away from certain places, people or activities? (1) | ||
| Have you lost interest in activities that were once important or enjoyable? (2) | ||
| Have you begun to feel more distant or isolated from other people? (3) | ||
| Do you find it hard to feel love or affection for other people? (4) | ||
| Have you begun to feel that there is no point in planning for the future? (5) | ||
| Have you had more trouble than usual falling or staying asleep? (6) | ||
| Do you become jumpy or easily startled by ordinary noise or movements? (7) |
Q24 Because alcohol use can affect health, it is important that we ask you some questions about your use of alcohol. Your answers will remain confidential, so please be as accurate as possible. Try to answer the questions in terms of “standard drinks”.
Q25
Q26 For the following questions, please select the answer which best applies to your drinking in the last year.
| Never (1) | Less than monthly (2) | Monthly (3) | Weekly (4) | Daily or almost daily (5) | |
|---|---|---|---|---|---|
| How often do you have SIX or more drinks on one occasion? (1) | |||||
| How often during the last year have you been unable to remember what happened the night before because you had been drinking? (2) | |||||
| How often during the last year have you failed to do what was normally expected of you because of drinking? (3) |
Q27 In the last year, has a relative or friend, doctor or other health worker been concerned about your drinking or suggested you cut down?
- No (0)
- Yes, on one occasion (1)
- Yes, on more than one occasion (2)
Q28
Thank you for the information you have provided so far, we have a good picture of your background and health. We are now moving into more sensitive childhood and relationships questions. When you feel ready, please click next to continue.
End of Block: HEALTH_WELLBEING
Start of Block: RELATIONSHIPS_ACE
Q29 About your childhood
The following questions are about possible experiences you may have had as a child (before the age of 18). Some questions may bring up distressing memories. If this happens, help is available. Please click here if you would like some support.
Q30 While you were growing up, during your first 18 years of life:
Did a parent or other adult in the household OFTEN … Swear at you, insult you, put you down, or humiliate you? OR Act in a way that made you afraid that you might be physically hurt?
- Yes (1)
- No (0)
Q31 Did a parent or other adult in the household OFTEN … Push, grab, slap, or throw something at you? OR Ever hit you so hard that you had marks or were injured?
- Yes (1)
- No (0)
Q32 Did an adult or person at least 5 years older than you EVER… Touch or fondle you or have you touch their body in a sexual way? OR Try to or actually have oral, anal, or vaginal sex with you?
- Yes (1)
- No (0)
Q33 These next questions are about possible experiences you may have had as a child (before the age of 18).
Did you OFTEN feel that … No one in your family loved you or thought you were important or special? OR Your family didn’t look out for each other, feel close to each other, or support each other?
- Yes (1)
- No (0)
Q34 Did you OFTEN feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? OR Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
- Yes (1)
- No (0)
Q35 Were your parents EVER separated or divorced?
- Yes (1)
- No (0)
Q36 These next questions are about possible experiences you may have had as a child (before the age of 18).
Was your mother or stepmother OFTEN pushed, grabbed, slapped, or had something thrown at her? OR SOMETIMES OR OFTEN kicked, bitten, hit with a fist, or hit with something hard? OR EVER repeatedly hit over at least a few minutes or threatened with a gun or knife?
- Yes (1)
- No (0)
Q37 Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
- Yes (1)
- No (0)
Q38 Was a household member depressed or mentally ill or did a household member attempt suicide?
- Yes (1)
- No (0)
Q39 Did a household member go to prison?
- Yes (1)
- No (0)
Q40
This is the end of this section. If any of these questions have been in any way distressing and you would like support, please click here. When you feel ready, please click the next button to continue.
End of Block: RELATIONSHIPS_ACE
Start of Block: RELATIONSHIPS_NCAS
Q41 About your relationships
This section asks you some personal questions about your attitudes towards relationships and your experiences in your relationships. The purpose of asking these questions is to understand your needs from services. Your responses are anonymous. We recognise that some of these questions may be sensitive for people, and if you would like support, it is available by clicking here.
Q42 Here are some statements about gender roles, stereotypes and gender equality. Thinking about Australian society generally, please indicate the degree to which you agree or disagree.
MANY women mistakenly interpret innocent remarks or acts as being sexist.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q43 MANY women exaggerate how unequally women are treated in Australia.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q44 MANY women fail to fully appreciate all that men do for them.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q45
Here are some statements about gender roles, stereotypes and gender equality. Thinking about Australian society generally, please indicate the degree to which you agree or disagree.
Women prefer a man to be in charge of the relationship.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q46 Men should take control in relationships and be the head of the household.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q47 On the whole, men make better political leaders than women.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q48 Here are some statements about gender roles, stereotypes, and gender equality. Thinking about Australian society generally, please indicate the extent to which you agree or disagree.
In the workplace, men generally make more capable bosses than women.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q49 I think there’s no harm in men making sexist jokes about women when they are among their male friends.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q50 When a couple start dating, the woman should not be the one to initiate sex.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
Q51 I think it is embarrassing for a man to have a job that is usually filled by a woman.
- Strongly disagree (1)
- Somewhat disagree (2)
- Somewhat agree (3)
- Strongly agree (4)
- Don’t know (5)
End of Block: RELATIONSHIPS_NCAS
Start of Block: RELATIONSHIPS_CAS
Q52 These questions are about your experiences in adult intimate relationships. By “adult intimate relationship”, we mean a current or former husband/wife, partner or boy/girlfriend for longer than one month. Have you ever been in an adult intimate relationship? Since you were 16 years of age.
- Yes (1)
- No (0)
| Skip To: End of Block If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship”… = No |
Q53 Have you been in an adult intimate relationship in the past 12 months?
- Yes (1)
- No (0)
Skip To: Q103 If Have you been in an adult intimate relationship in the past 12 months? = No
Q54 Are you currently in an intimate relationship?
- Yes (1)
- No (0)
Skip To: Q56 If Are you currently in an intimate relationship? = No
Q55 Are you currently afraid of your partner or ex-partner?
- Yes (1)
- No (0)
Q56 Have you been afraid of any partner or ex-partner in the past 12 months?
- Yes (1)
- No (0)
Q57 Have you ever been afraid of any partner or ex-partner?
- Yes (1)
- No (0)
Q58 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Blamed me for causing their violent behaviour
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or form… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q59 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q60 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q61 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Shook, pushed, grabbed or threw me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q62 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q63 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q64 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner: Tried to convince my family, children or friends that I am crazy or tried to turn them against me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q65 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q66 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q67 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Used or threatened to use a knife or gun or other weapon to harm me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q68 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q69 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q70 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Made me perform sex acts that I did not want to perform
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q71 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q72 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q73 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Followed me or hung around outside my home or work
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q74 How often has this happened in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often has this happened in the past 12 months? = Once in the past 12 months
Or How often has this happened in the past 12 months? = A few times in the past 12 months
Or How often has this happened in the past 12 months? = Monthly
Or How often has this happened in the past 12 months? = Weekly
Or How often has this happened in the past 12 months? = Daily/almost daily
Q75 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q76 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Threatened to harm or kill me or someone close to me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q77 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q78 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q79 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Choked me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q80 How often did this happen in past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in past 12 months? = Once in the past 12 months
Or How often did this happen in past 12 months? = A few times in the past 12 months
Or How often did this happen in past 12 months? = Monthly
Or How often did this happen in past 12 months? = Weekly
Or How often did this happen in past 12 months? = Daily/almost daily
Q81 Who behaved in this way towards you? Please select all that apply.
A male partner/ex-partner (1)
A female partner/ex-partner (2)
Q82 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Forced or tried to force me to have sex
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q83 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q84 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q85 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Harassed me by phone, text, email or using social media
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q86 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q87 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q88 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Told me I was crazy, stupid or not good enough
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q89 How often has this happened in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often has this happened in the past 12 months? = Once in the past 12 months
Or How often has this happened in the past 12 months? = A few times in the past 12 months
Or How often has this happened in the past 12 months? = Monthly
Or How often has this happened in the past 12 months? = Weekly
Or How often has this happened in the past 12 months? = Daily/almost daily
Q90 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q91
We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Hit me with a fist or object, kicked or bit me
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q92 How often has this happened in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often has this happened in the past 12 months? = Once in the past 12 months
Or How often has this happened in the past 12 months? = A few times in the past 12 months
Or How often has this happened in the past 12 months? = Monthly
Or How often has this happened in the past 12 months? = Weekly
Or How often has this happened in the past 12 months? = Daily/almost daily
Q93 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q94
We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner: Kept me from seeing or talking to my family or friends
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or form… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q95 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q96 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q97 We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Confined or locked me in a room or other space
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q98 How often did this happen in the past 12 months?
Not in the past 12 months (0)
Once in the past 12 months (1)
A few times in the past 12 months (2)
Monthly (3)
Weekly (4)
Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q99 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Q100
We would like to know if you experienced any of the actions listed below from any current or former partner or partners. Have any of the following ever happened to you?
My partner or ex-partner:
Kept me from having access to a job, money or financial resources
- Yes (1)
- No (0)
Display This Question:
If We would like to know if you experienced any of the actions listed below from any current or former… = Yes
And Have you been in an adult intimate relationship in the past 12 months? = Yes
Q101 How often did this happen in the past 12 months?
- Not in the past 12 months (0)
- Once in the past 12 months (1)
- A few times in the past 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If How often did this happen in the past 12 months? = Once in the past 12 months
Or How often did this happen in the past 12 months? = A few times in the past 12 months
Or How often did this happen in the past 12 months? = Monthly
Or How often did this happen in the past 12 months? = Weekly
Or How often did this happen in the past 12 months? = Daily/almost daily
Q102 Who behaved in this way towards you? Please select all that apply.
- A male partner/ex-partner (1)
- A female partner/ex-partner (2)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q103 Are you currently afraid of your partner or ex-partner?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q104 Have you ever been afraid of any partner or ex-partner?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q105 We would like to know if you have ever experienced any of the actions listed below from any current or former partners.
| Yes (1) | No (0) | |
|---|---|---|
| Blamed me for causing their violent behaviour (1) | ||
| Shook, pushed, grabbed or threw me (4) | ||
| Tried to convince my family, children or friends that I am crazy or tried to turn them against me (5) | ||
| Used or threatened to use a knife or gun or other weapon to harm me (6) | ||
| Made me perform sex acts that I did not want to perform (7) |
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q106 We would like to know if you have ever experienced any of the actions listed below from any current or former partners.
| Yes (1) | No (0) | |
|---|---|---|
| Followed me or hung around outside my home or work (9) | ||
| Threatened to harm or kill me or someone close to me (18) | ||
| Choked me (10) | ||
| Forced or tried to force me to have sex (11) | ||
| Harassed me by phone, text, email or using social media (12) |
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q107 We would like to know if you have ever experienced any of the actions listed below from any current or former partners.
| Yes (1) | No (0) | |
|---|---|---|
| Told me I was crazy, stupid, or not good enough (13) | ||
| Hit me with a fist or object, kicked or bit me (14) | ||
| Kept me from seeing or talking to my family or friends (15) | ||
| Confined or locked me in a room or other space (16) | ||
| Kept me from having access to a job, money, or financial resources (17) |
Q108 Thank you for all your answers so far. You are at the half-way point of the survey. Please remember that your answers will contribute to helping us make services better for everyone in the community. If at any time you would like to take a break you may do so and return to the place you are up to (as long as you use the same device). If you would like to speak to anyone about anything distressing that has arisen for you so far, please click here.
End of Block: RELATIONSHIPS_CAS
Start of Block: RELATIONSHIPS_SV+RC
Q109 The next questions are about unwanted sexual experiences. These experiences may have occurred inside or outside of an intimate relationship. Remember that the survey is anonymous. If you do not feel comfortable answering any of the questions, skip them and go on to the next question. In this questionnaire, when we talk about “sex” we mean any kind of sex (vaginal, anal, oral etc.)
Q110 Since the age of 15, has any man or woman ever forced you or tried to force you into sexual activity against your will?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q111 Has a current or previous partner ever physically forced you to have sex when you did not want to? Did this happen once, a few times or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q112 Have you ever had sex with a current or previous partner when you did not want to because you were afraid of what he might do? Did this happen once, a few times or many times?
Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q113 Has your current or previous partner ever forced to watch pornography when you did not want to? Did this happen once, a few times or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q114 Has a current or previous partner ever forced you to do something else sexual that you did not want to? Did this happen once, a few times or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q115 Has any current or past partner ever pressured, forced or threatened you to become pregnant?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q116 Has any current or past partner ever used threats, pressure or force to prevent you from terminating a pregnancy?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q117 Has any current or past partner ever pressured, forced or threatened you to terminate a pregnancy?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate…” = Yes
Q118 Has any current or past partner ever interfered with contraception in order to get you pregnant when you did not want to be (e.g. disposed of contraception, tampered with contraception, prevented you from obtaining contraception)?
- Yes (1)
- No (0)
Q119
This is the end of this section. Thank you for taking the time to answer these questions, some of which may have been distressing. This is the end of the sensitive questions about experiences you have had in your relationships. Below is a breathing exercise that may reconnect you with where you are in this moment, here and now. If you are feeling distressed or anxious, click on this link for a grounding technique that may help you anchor back to the present. If you would like to speak to someone for support, click here for a list of support services.
When you feel ready, press the next button to continue taking the survey. We really appreciate your time.
Q120
End of Block: RELATIONSHIPS_SV+RC
Start of Block: HELP_Q1
Q121 Your views on services
This section asks you about your use of services in the community. This information may help us understand how people use services and where there may be gaps in your support needs.
Q122 Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? Please tick all that apply.
- Friend/s (1)
- Family member (18)
- Partner (19)
- General practitioner (2)
- Nurse (20)
- Psychologist or counsellor (3)
- Social worker (Hospital/community health) (4)
- Alcohol or drug worker (5)
- Family therapist (6)
- Other (please specify) (7) ________________________________________________
- Telephone helpline (e.g. Lifeline, 1800 RESPECT) (8)
- Domestic or family violence service (9)
- Sexual assault service (21)
- Police (10)
- Legal service (e.g. solicitor or legal aid) (11)
- Financial service (e.g. Centrelink) (12)
- Housing service (13)
- Work colleague or boss (14)
- Priest/minister/rabbi or any other religious person (15)
- I did not seek advice or support (17)
End of Block: HELP_Q1
Start of Block: HOW HELPFUL
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Friend/s
Q123 How helpful was your friend/s?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Family member
Q124 How helpful was your family member?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Partner
Q125 How helpful was your partner?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = General practitioner
Q126 How helpful was the general practitioner?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Nurse
Q127
How helpful was the nurse?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Psychologist or counsellor
Q128 How helpful was the psychologist or counsellor?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Social worker (Hospital/community health)
Q129 How helpful was the social worker (hospital or community based)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Alcohol or drug worker
Q130 How helpful was alcohol or drug worker?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? … = Family therapist
Q131 How helpful was the family therapist?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Telephone helpline (e.g. Lifeline, 1800 RESPECT)
Q132 How helpful was the telephone helpline (e.g. Lifeline, 1800RESPECT)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Domestic or family violence service
Q133 How helpful was the domestic or family violence service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Sexual assault service
Q134 How helpful was the sexual assault service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Police
Q135 How helpful was the police?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Legal service (e.g. solicitor or legal aid)
Q136 How helpful was the legal service (e.g. solicitor or legal aid)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Financial service (e.g. Centrelink)
Q137 How helpful was the financial service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Housing Service
Q138 How helpful was the housing service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Work colleague or boss
Q139 How helpful was your work colleague or boss?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Priest/minister/rabbi or any other religious person
Q140 How helpful was the priest/minister/rabbi or any other religious person?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
Did you seek advice or support from any of the following for relationship issues or after experiencing violence and/or unwanted sexual encounters? = Other (please specify)
Q141 How helpful was Q122/ChoiceTextEntryValue/?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
End of Block: HOW HELPFUL
Start of Block: BLOCK2_POPUP
Q142 Below is a list of reasons you may not have spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters. Please rate how important each is to your own situation.
I have no time to talk to someone about these things.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q143 I feel too ashamed to talk to anyone.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q144 The professional will not understand me.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q145 The professional will tell others.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q146 My friends or family will find out.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q147 My partner’s behaviours are just a normal part of relationships. I don’t believe there is any need to see a professional about them.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q148 My partner’s behaviour was a once-off. It won’t happen again.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q149 I have no access to transport to see someone.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q150 Below is a list of reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters. Please rate how important each is to your own situation.
I don’t know of any service that might be able to help.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q151 I don’t want to talk to anyone about my partner’s behaviours, it is too personal.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q152 I decided not to seek care as I’m not sure it would be helpful.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q153 I had too many personal or family responsibilities to seek help.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q154 I was uncertain who to see.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q155 My culture or religion is a barrier for me seeking help.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q156 Are there any other reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Are there any other reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters? Text Response Does Not Contain No
And Are there any other reasons you may have not spoken to a professional or service about your partner’s behaviours or unwanted sexual encounters? Text Response Is Not Empty
Q157 Please rate how important this is to your own situation.
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q158 Was there a time that you needed help for relationship issues or unwanted sexual encounters but could not get it?
- Yes (1)
- No (0)
Display This Question:
If Was there a time that you needed help for relationship issues or unwanted sexual encounters but … = Yes
Q159 How much did each of the service barriers below prevent you from accessing help? Select one option per line.
| Not at all (1) | A small amount (2) | Moderately (3) | Quite a lot (4) | Extremely (5) | |
|---|---|---|---|---|---|
| Language or translation problems (1) | |||||
| Cost (2) | |||||
| Limited opening hours (3) | |||||
| No service available in the area at the time needed (4) | |||||
| Waiting time too long (5) | |||||
| No appointments (6) | |||||
| Not taking new patients (7) | |||||
| Trouble understanding the terms used by the professional (8) | |||||
| Lack of awareness of available services (9) | |||||
| Concerns regarding confidentiality (10) | |||||
| No private health insurance (11) | |||||
| Other barriers (12) |
End of Block: BLOCK2_POPUP
Start of Block: BLOCK1_POP UP
Q160 Reflecting on any contact or experiences you’ve had with services, what would you value most in a service? Please rate how important you think each of the factors below are.
Not feeling judged or put down
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q161 Knowing that whatever I said would be held in confidence by the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q162 The professional being interested in who I was as a person
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q163 Reflecting on any contact or experiences you’ve had with services, what would you value most in a service? Please rate how important you think each of the factors below are.
Feeling listened to by the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q164 Being given practical information about safety for myself and any children
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q165 The expertise of the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q166 Reflecting on any contact or experiences you’ve had with services, what would you value most in a service? Please rate how important you think each of the factors below are.
Learning new ways of escaping violence
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q167 Material support (e.g. getting access to accommodation)
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q168 Emotional support (having someone to talk to)
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q169 Knowing that whatever I said would be held in confidence by the professional
- Not at all important (1)
- A little bit important (2)
- Somewhat important (3)
- Moderately important (4)
- Very important (5)
Q170 Considering all the experiences you have had in talking to services about your partner’s behaviours, what do you believe that professionals need to do differently to better help people in similar situations as you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q171 Considering all the experiences you have had in talking to services about unwanted sexual encounters, what do you believe professionals need to do differently to better help people in similar situations as you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q172 The COVID-19 pandemic has changed the way we all access support services. What impact, if any, has it had on your access to support services for your behaviours in intimate relationships?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: BLOCK1_POP UP
Start of Block: HOW_HELPFUL_CONT
Q173 If you thought that your partner was close to using the behaviours you previously reported them using, how likely is it that you would seek help from the following people and services?
| Very unlikely (1) | Unlikely (2) | Neither likely or unlikely (3) | Likely (4) | Very likely (5) | |
|---|---|---|---|---|---|
| Friend (1) | |||||
| Family member (20) | |||||
| General practitioner (2) | |||||
| Psychologist or counsellor (3) | |||||
| Social worker (Hospital/community health) (4) | |||||
| Alcohol or drug worker (5) | |||||
| Family therapist (6) | |||||
| Telephone helpline (e.g. Lifeline, 1800 RESPECT (7) | |||||
| Domestic or family violence service (8) | |||||
| Sexual assault service (19) | |||||
| Police (10) | |||||
| Legal service (e.g. solicitor or legal aid) (11) | |||||
| Financial service (e.g. Centrelink) (12) | |||||
| Housing service (13) | |||||
| Work colleague or boss (14) | |||||
| Priest/minister/rabbi or any other religious person (15) | |||||
| I will not seek advice or support (17) | |||||
| I would seek help from another not listed person (please specify) (18) |
Q174 If you think about your partner’s/ex-partner’s behaviours towards you, what do you think your greatest need is from a service or professional?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have children? = Yes
Q175 If you think about your partner’s/ex-partner’s behaviours towards you and your children, what has been most helpful for your children’s needs?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have children? = Yes
Q176 If you think about your partner’s/ex-partner’s behaviours towards you and your children, what do you think services can do to best address your children’s needs?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q177 If you think about your partner’s/ex-partner’s behaviours towards you, what do you think has been most helpful for your partner in helping them to stop using violence and abuse?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q178 If you think about your partners’/ex-partner’s behaviours towards you, what do you think your partner might need that would help your partner stop using violence and abuse?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q179 How have your experiences in your adult intimate relationships changed during COVID-19 isolation?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q180 These next questions ask you to think about your relationship with your partner or ex-partner. Please complete the following sentences with the first words that come to mind. There are no right or wrong answers, just write what you feel.
I wish that my partner/ex-partner…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q181 I wish that service providers…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q182 I wish that my family…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q183 I wish that my friends…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q184
This is the end of this section. When you feel ready, please click the next button to continue with some further background questions.
End of Block: HOW_HELPFUL_CONT
Start of Block: MORE_ABOUT_YOU
Q185 More about you
This section asks more about your background and some personal details about education and finances. These questions are important because they allow your answers to be placed in a broader context, without identifying anybody. Please remember that all survey responses are anonymous.
Q186 Which of these most closely describes your sexual orientation?
- I am heterosexual (1)
- I am bisexual (2)
- I am lesbian (3)
- I am queer (4)
- I am pansexual (8)
- I am asexual (5)
- Not sure (7)
- I would prefer to self-describe (9) ________________________________________________
Q187 Which of the following best describes your prior schooling?
- Still at secondary school (1)
- Completed secondary school to end of Year 12 (2)
- Attended secondary school but did not complete Year 12 (3)
- Attended primary school only (4)
- Did not attend school (5)
Q188 What is your highest qualification since leaving school?
- Finished a degree or higher degree (1)
- Completed a diploma or certificate (2)
- Completed a trade apprenticeship or traineeship (3)
- Other (please specify) (4) ________________________________________________
Q189 Which of the following best describes your current occupational status?
- Part-time wage or salary earner (including self-employed) (1)
- Full-time wage or salary earner (including self-employed) (2)
- Unemployed, seeking work (3)
- Unemployed, not seeking work (4)
- Retired (5)
- Unpaid work (e.g. home duties, voluntary, carer) (6)
Q190 Do you hold a current Health Care Card?
- Yes (1)
- No (0)
Q191 How do you manage on your available income?
- Easily (1)
- Not too badly (2)
- Difficult some of the time (3)
- Difficult all of the time (4)
- Impossible (5)
Q192
This is the end of this section. There’s just one more section to go! When you feel ready, please click the next button to continue.
End of Block: MORE_ABOUT_YOU
Start of Block: FELT_COMPLETING
Q193 your views on this survey
This last section asks questions about how you felt while completing this survey to understand what it was like being involved in the VOICES project. Please select one box on each line.
Q194 I felt comfortable answering the questions about domestic violence and sexual violence in this survey.
- Strongly agree (1)
- Agree (2)
- Neither agree nor disagree (3)
- Disagree (4)
- Strongly disagree (5)
Q195 As a result of questions about domestic violence and sexual violence being asked in this survey, my feelings about my relationship are…
- More positive (1)
- Somewhat more positive (2)
- Unchanged (3)
- Somewhat more negative (4)
- More negative (5)
Q196 The questions I was asked in this survey made me feel that the problems in my relationship with my partner or ex-partner are my fault.
- Strongly disagree (1)
- Disagree (2)
- Neither disagree nor agree (3)
- Agree (4)
- Strongly agree (5)
Q197 As a result of being asked questions about domestic violence and sexual violence in this survey, my feelings about myself as a person are…
- Better (1)
- Somewhat better (2)
- About the same as before (3)
- Somewhat worse (4)
- Worse (5)
Q198 Responding to this survey has made me more open to dealing with possible problems in my relationship.
- Strongly disagree (1)
- Disagree (2)
- Neither agree nor disagree (3)
- Agree (4)
- Strongly agree (5)
Q199 I am glad to be a participant in the VOICES project.
- Strongly disagree (1)
- Disagree (2)
- Neither agree nor disagree (3)
- Agree (4)
- Strongly agree (5)
Q200 Please use the space below if there is anything else you would like to tell us about yourself or the survey.
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q201 Final thoughts
In your own words, what enables you to stay strong?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q202 Do you have any extra comments that you wish to make about any issues raised in the survey?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: FELT_COMPLETING
Start of Block: THANK_YOU
Q203
Make Sure You Click Submit!
This is the end of the survey. Thank you very much for the time and effort you have taken. When you click the submit button, your responses will be submitted anonymously. On the next page you can provide your contact details to enter in a draw to win an iPad in appreciation of your time. You can also tell us if you would like to participate in a follow up interview about your experiences and need for services. Thank you.
End of Block: THANK_YOU
Start of Block: Gift Voucher
Q257 Thank you for completing this survey and taking the time to assist us today.
Your participation will contribute to our understanding of how best to help and keep families safe. You will be given the option to enter into a draw to win an iPad in appreciation for your time and contribution. If you would like to enter the draw, please provide us with your name and best email address. Your name and email address will not be used for any other purposes; and your details will not be linked in any way to your survey responses.
Q258 Name
________________________________________________________________
Q259 Email address
________________________________________________________________
Q260 Together, with your help, we are trying to work out ways to improve the support and services women receive in relation to issues of domestic violence and sexual assault.
To achieve this goal, further research (e.g. interviews) on this topic may be required. Please tick yes if you would be happy to be contacted by the researchers for involvement in further research.
Your participation in further research is completely voluntary, and independent of the survey you have just completed. You can provide your details now but if you change your mind later, you are free to withdraw your interest without explanation when/if you are contacted for further research at some time in the future.
Q261 Would you like to participate in further research on this topic?
- Yes (1)
- No (2)
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q262 My first name is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q263 The best phone number(s) to safely contact me on is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q264 An alternative contact (e.g. email) is:
________________________________________________________________
End of Block: Gift Voucher
Appendix C:
Survey (People who use IPV and/or SV)
Start of Block: Screening
Q293 Hello, thank you for taking an interest in the VOICES project. Before we start, we need to ask you some initial questions in order to understand whether the project is suited to you and your experiences. It should take approximately 2 minutes to complete. Upon completion of these initial questions, if the survey is a good match to you and your experiences, you will automatically proceed to the main survey.
Participating in this survey will help us understand the experiences of people who are concerned about their behaviours in their intimate relationships and their need for services. Responses to the survey are strictly confidential. Your voice is important. Remember, there are resources available here if you need support at any time.
Q294 Have you had a partner in the last five years who identified as a woman?
- Yes (1)
- No (0)
Q295 How old are you?
- 17 or younger (1)
- 18–24 (0)
- 25–34 (2)
- 35–44 (3)
- 45+ (4)
Q296 What country do you live in?
- China (1)
- Australia (0)
- India (2)
- England (3)
- Indonesia (4)
- Canada (5)
- Other (6) ________________________________________________
Q297 How did you find this survey?
- Men’s referral service (1)
- Community service (2)
- Instagram (3)
- Twitter (4)
- Facebook (5)
- Gumtree (6)
- University of Melbourne student notices (7)
- Other (8) ________________________________________________
Q298 In the last five years have you ever… (please select all that apply)
- Been concerned about your behaviours in intimate relationships? (1)
- Believe your behaviour has scared a partner or ex-partner? (2)
- Sought help from anyone to address issues in your intimate relationships? (3)
- None of the above (0)
Q299 The following question is asked to determine if you are a human or a robot…
Q300 What is 2+2?
- 6 (1)
- 8 (2)
- 4 (3)
Display This Question:
If Have you had a partner in the last five years who identified as a woman? = No
Or How old are you? = 17 or younger
Or What country do you live in? = Australia
Or In the last five years have you ever… (please select all that apply) = None of the above
Or What is 2+2? = 4
Q304 We thank you for your interest in our project and for reading through the provided materials. As the present project is about experiences of fear and conflict in relationships with women living in Australia, one or more of your answers has made you ineligible for the current study. If you have any questions, please email the project team at: voice_project@unimelb.edu.au. Remember, there are resources available here if you need support at any time.
| Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed |
End of Block: Screening
Start of Block: intro
Display This Question:
If Have you had a partner in the last five years who identified as a woman? = Yes
And How old are you? = 17 or younger
And What country do you live in? = Australia
And In the last five years have you ever… (please select all that apply) = None of the above
And What is 2+2? = 4
Welcome to the VOICES Project survey Thank you for answering our initial questions, it looks as if you are eligible to complete the survey. The VOICES survey asks about some background information, your health and wellbeing, use of domestic violence and unwanted sexual experiences, and how we can support men, women and families more effectively. Some of the questions are sensitive so there are resources available by clicking here, these will be available throughout the survey. All information you give us in this survey is anonymous. The survey will take approximately 30 minutes to complete. After completing the survey, you will be given the option to enter into a draw to win an iPad.
The project team is based at the Safer Families Centre, The University of Melbourne and ANROWS. If you have any questions about the project, please email:voice_project@unimelb.edu.au.
We recommend that you complete the survey in private, please click here for further advice on keeping safe online. Feel free take a break at any time. Remember, if you exit the survey and return later, as this survey is anonymous, you will only be returned to where you left off if you use the same device that you started the survey on. How to fill in the survey Please read the questions carefully and follow the instructions. There are no right or wrong answers, just put what is right for you. Please select only one answer per question unless instructed otherwise.
End of Block: intro
Start of Block: About_you_block
Q2 About You We will start the survey with a few quick questions about your background. These questions are important because they allow your answers to be compared with those of other people with a similar background to you, without identifying anybody.
Q3 Have you ever had a partner who identified as a woman?
- Yes (1)
- No (0)
Display This Question:
If Have you ever had a partner who identified as a woman? = No
Q4 We thank you for your interest in our project and for reading through the provided materials. As the present project is about people who have been in relationships with women, this makes you ineligible. Should you wish to speak with someone from the project team, please contact Matt by emailing Voice_Project@unimelb.edu.au.
Should you wish to speak with someone for support, resources are available. Please click here. Once again, we thank you for your time and interest in the Voices Project.
| Skip To: End of Survey If We thank you for your interest in our project and for reading through the provided materials. As… Is Displayed |
Q5 What is your gender?
- Male (1)
- Female (2)
- Non-binary (3)
- Prefer to self-describe (4) ________________________________________________
Q6 What is your age in years?
________________________________________________________________
Q7 What is your postcode where you live most of the time?
________________________________________________________________
Q8 Were you born in Australia?
- Yes (1)
- No (0)
Display This Question:
If Were you born in Australia? = No
Q9 Which country were you born in?
- UK (1)
- New Zealand (2)
- China (3)
- India (4)
- Sri Lanka (5)
- Other (please specify) (6) ________________________________________________
- Italy (7)
- South Africa (8)
- Greece (9)
- Lebanon (10)
- Vietnam (11)
Display This Question:
If Were you born in Australia? = No
Q10 How long have you lived in Australia?
Please write the number of years in the box below. If you are not sure, your best guess is fine.
________________________________________________________________
Display This Question:
If Were you born in Australia? = No
Q11 Are you…
- An Australian citizen (1)
- On a permanent visa (2)
- On a temporary visa (3)
Q12 Is English your first language?
- Yes (1)
- No (0)
Q13 Do you identify as Aboriginal or Torres Strait Islander?
- Yes, Aboriginal (1)
- Yes, Torres Strait Islander (2)
- Yes, both Aboriginal and Torres Strait Islander (3)
- No, neither (4)
Q14 What is the gender of your current partner?
- Female (40)
- Non-binary (41)
- Prefer not to disclose (42)
- I do not have a current partner (43)
Q15 Who do you usually live with? Please select all that apply.
- No one else (1)
- Your wife (2)
- Your female partner (3)
- Your male partner (5)
- Other relatives (8)
- Friends (9)
- Unrelated flatmate or co-tenant (10)
- Other (please specify) (6) ________________________________________________
Q16 Do you have any children?
- Yes (1)
- No (0)
Display This Question:
If Do you have any children? = Yes
Q17 How many children are currently at home with you?
- No children (0)
- One child (1)
- Two children (2)
- Three children (3)
- Four or more children (4)
Q18 What is your present marital status?
This does not necessarily refer to your current living arrangement. Please select one option only.
- Never married (1)
- Widowed (2)
- Divorced (3)
- Separated but not divorced (4)
- Married (5)
Q19
This is the end of this section. When you feel ready, please click the next button to continue.
End of Block: About_you_block
Start of Block: Health_wellbeing_block
Q20 About your health and wellbeing This section is about how you’re feeling, both emotionally and physically. We are asking these questions because we are interested in how relationship issues affect your emotional and physical wellbeing.
Q21 In general, how would you say your health is? Please select one option only.
- Excellent (1)
- Very good (2)
- Good (3)
- Fair (4)
- Poor (5)
Q22 Over the last 2 weeks, how often have you been bothered by the following problems?
Please select one option on each line.
| Not at all (0) | Several days (1) | More than half the days (2) | Nearly every day (3) | |
|---|---|---|---|---|
| Little interest or pleasure in doing things (1) | ||||
| Feeling down, depressed or hopeless (2) | ||||
| Feeling nervous, anxious, or on edge (3) | ||||
| Not being able to stop or control worrying (4) |
Q23 Do you have any long-term illness, health problem or disability, which limits your daily activities or the work you can do (including problems that are due to old age)?
- Yes (1)
- No (0)
Q24 Below are some statements about how you feel in yourself. Please read each statement and choose the response that most closely indicates how you have felt during the past month.
| Yes (1) | No (0) | |
|---|---|---|
| Do you avoid being reminded of experiences by staying away from certain places, people or activities? (1) | ||
| Have you lost interest in activities that were once important or enjoyable? (2) | ||
| Have you begun to feel more distant or isolated from other people? (3) | ||
| Do you find it hard to feel love or affection for other people? (4) | ||
| Have you begun to feel that there is no point in planning for the future? (5) | ||
| Have you had more trouble than usual falling or staying asleep? (6) | ||
| Do you become jumpy or easily startled by ordinary noise or movements? (7) |
Q25 Because alcohol use can affect health, it is important that we ask you some questions about your use of alcohol. Your answers will remain confidential, so please be as accurate as possible. Try to answer the questions in terms of “standard drinks”.
Q26
Display This Question:
If What is your gender? = Male
Or What is your gender? = Non-binary
Or What is your gender? = Prefer to self-describe
Q27 Please select the answer which best applies to your drinking in the last year.
| Never (1) | Less than monthly (1) | Monthly (2) | Weekly (3) | Daily or almost daily (4) | |
|---|---|---|---|---|---|
| How often do you have EIGHT or more drinks on one occasion? (1) | |||||
| How often have you been unable to remember what happened the night before because you had been drinking? (2) | |||||
| How often have you failed to do what was normally expected of you because of drinking? (3) |
Display This Question:
If What is your gender? = Female
Q28 For the following questions, please select the answer which best applies to your drinking in the last year.
| Never (0) | Less than monthly (1) | Monthly (2) | Weekly (3) | Daily or almost daily (4) | |
|---|---|---|---|---|---|
| How often do you have SIX or more drinks on one occasion? (1) | |||||
| How often during the last year have you been unable to remember what happened the night before because you had been drinking? (2) | |||||
| How often during the last year have you failed to do what was normally expected of you because of drinking? (3) |
Q29 In the last year, has a relative or friend, doctor or other health worker been concerned about your drinking or suggested you cut down?
- No (0)
- Yes, on one occasion (1)
- Yes, on more than one occasion (2)
Q30
Thank you for the information you have provided so far, we have a good picture of your background and health. We are now moving into more sensitive childhood and relationships questions. When you feel ready, please click next to continue.
End of Block: Health_wellbeing_block
Start of Block: ACES
Q31 About your childhood The following questions are about possible experiences you may have had as a child (before the age of 18). Some questions may bring up distressing memories. If this happens, support can be accessed by clicking here.
Q32 While you were growing up, during your first 18 years of life: Did a parent or other adult in the household OFTEN … Swear at you, insult you, put you down, or humiliate you? OR Act in a way that made you afraid that you might be physically hurt?
- Yes (1)
- No (0)
Q33 Did a parent or other adult in the household OFTEN … Push, grab, slap, or throw something at you? OR Ever hit you so hard that you had marks or were injured?
- Yes (1)
- No (0)
Q34 Did an adult or person at least 5 years older than you EVER… Touch or fondle you or have you touch their body in a sexual way? OR Try to or actually have oral, anal, or vaginal sex with you?
- Yes (1)
- No (0)
Q35 These next questions are about possible experiences you may have had as a child (before the age of 18). Did you OFTEN feel that … No one in your family loved you or thought you were important or special? OR Your family didn’t look out for each other, feel close to each other, or support each other?
- Yes (1)
- No (0)
Q36 Did you OFTEN feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? OR Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
- Yes (1)
- No (0)
Q37 Were your parents EVER separated or divorced?
- Yes (1)
- No (0)
Q38 These next questions are about possible experiences you may have had as a child (before the age of 18). Was your mother or stepmother: OFTEN pushed, grabbed, slapped, or had something thrown at her? OR SOMETIMES OR OFTEN kicked, bitten, hit with a fist, or hit with something hard? OR EVER repeatedly hit over at least a few minutes or threatened with a gun or knife?
- Yes (1)
- No (0)
Q39 Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
- Yes (1)
- No (0)
Q40 Was a household member depressed or mentally ill or did a household member attempt suicide?
- Yes (1)
- No (0)
Q41 Did a household member go to prison?
- Yes (1)
- No (0)
Q42
This is the end of this section. If any of these questions have been in any way distressing and you would like support, please click here. When you feel ready, please click the next button to continue.
End of Block: ACES
Start of Block: NCAS_Relationships
Q43 About your relationships
This section asks you some personal questions about your attitudes towards relationships and your experiences in your relationships. The purpose of asking these questions is to understand your needs from services. Your responses are anonymous. We recognise that some of these questions may be sensitive for people, and if you would like support, it is available by clicking here.
Q44 Here are some statements about gender roles, stereotypes and gender equality. Thinking about Australian society generally, please indicate the degree to which you agree or disagree. Please select one option per line.
| Strongly disagree (1) | Somewhat disagree (2) | Somewhat agree (3) | Strongly agree (4) | Don’t know (5) | |
|---|---|---|---|---|---|
| MANY women mistakenly interpret innocent remarks or acts as being sexist. (1) | |||||
| MANY women exaggerate how unequally women are treated in Australia. (2) | |||||
| MANY women fail to fully appreciate all that men do for them. (3) | |||||
| Women prefer a man to be in charge of the relationship. (4) | |||||
| Men should take control in relationships and be the head of the household. (5) | |||||
| On the whole, men make better political leaders than women. (6) | |||||
| In the workplace, men generally make more capable bosses than women. (7) | |||||
| I think there’s no harm in men making sexist jokes about women when they are among their male friends. (8) | |||||
| When a couple start dating, the woman should not be the one to initiate sex. (9) | |||||
| I think it is embarrassing for a man to have a job that is usually filled by a woman. (10) |
End of Block: NCAS_Relationships
Start of Block: CAS_SF_Relationships
Q45 These questions are about your experiences in adult intimate relationships. By “adult intimate relationship”, we mean a current or former husband/wife, partner, or boy/girlfriend for longer than one month.
Have you ever been in an adult intimate relationship (i.e. since the age of 16)?
- Yes (1)
- No (0)
| Skip To: End of Block If These questions are about your experiences in adult intimate relationships. By ‘adult intimate re… = No |
Q46 Have you been in an adult intimate relationship in the past 12 months?
- Yes (1)
- No (0)
Skip To: Q82 If Have you been in an adult intimate relationship in the past 12 months? = No
Q47 Are you currently in a relationship?
- Yes (1)
- No (0)
Display This Question:
If Are you currently in a relationship? = Yes
Q48 Do you believe, at times, your current partner becomes afraid of you?
- Yes (1)
- No (0)
Q49 Do you believe a partner has been afraid of you in the last 12 months?
- Yes (1)
- No (0)
Q50 Do you believe a partner has ever been afraid of you?
- Yes (1)
- No (0)
Q51 We would like to know if you have ever used any of the behaviours listed below towards any current or former partner or partners.
Q52 Have you ever blamed a partner for causing you to act abusively?
- Yes (1)
- No (0)
Display This Question:
If Have you ever blamed a partner for causing you to act abusively? = Yes
Q53 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q54 Have you ever shaken, thrown, pushed, or grabbed a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever shaken, thrown, pushed, or grabbed a partner? = Yes
Q55 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q56 Have you ever tried to convince a partner’s family or friends that they were crazy?
- Yes (1)
- No (0)
Display This Question:
If Have you ever tried to convince a partner’s family or friends that they were crazy? = Yes
Q57 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q58 Have you ever used or threatened to use a knife or gun or other weapon against a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever used or threatened to use a knife or gun or other weapon against a partner? = Yes
Q59 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q60 Have you ever made a partner perform sex acts that were unwanted?
- Yes (1)
- No (0)
Display This Question:
If Have you ever made a partner perform sex acts that were unwanted? = Yes
Q61 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q62 Have you ever followed a partner or hung around outside their home or work?
- Yes (1)
- No (0)
Display This Question:
If Have you ever followed a partner or hung around outside their home or work? = Yes
Q63 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q64 Have you ever threatened to harm or kill a partner or someone close to them?
- Yes (1)
- No (0)
Display This Question:
If Have you ever threatened to harm or kill a partner or someone close to them? = Yes
Q65 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q66 Have you ever choked a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever choked a partner? = Yes
Q67 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q68 Have you ever forced or tried to force a partner to have sex?
- Yes (1)
- No (0)
Display This Question:
If Have you ever forced or tried to force a partner to have sex? = Yes
Q69 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q70 Have you ever continuously called, texted, emailed, or contacted a partner using social media?
- Yes (1)
- No (0)
Display This Question:
If Have you ever continuously called, texted, emailed, or contacted a partner using social media? = Yes
Q71 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q72 Have you ever told a partner they were crazy, stupid or not good enough?
- Yes (1)
- No (0)
Display This Question:
If Have you ever told a partner they were crazy, stupid, or not good enough? = Yes
Q73 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q74 Have you ever hit a partner with a fist or object, kicked or bitten a partner?
- Yes (1)
- No (0)
Display This Question:
If Have you ever hit a partner with a fist or object, kicked, or bit a partner? = Yes
Q75 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q76 Have you ever kept a partner from seeing family or friends?
- Yes (1)
- No (0)
Display This Question:
If Have you ever kept a partner from seeing family or friends? = Yes
Q77 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q78 Have you ever locked a partner in a room or other space?
- Yes (1)
- No (0)
Display This Question:
If Have you ever locked a partner in a room or other space? = Yes
Q79 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Q80 Have you ever kept a partner from having access to a job, money or financial resources?
- Yes (1)
- No (0)
Display This Question:
If Have you ever kept a partner from having access to a job, money or financial resources? = Yes
Q81 How often did this happen in the last 12 months?
- Not in the last 12 months (0)
- Once in the last 12 months (1)
- A few times in the last 12 months (2)
- Monthly (3)
- Weekly (4)
- Daily/almost daily (5)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q82 Do you believe a partner or ex-partner is currently afraid of you?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q83 Do you believe a partner has ever been afraid of you?
- Yes (1)
- No (0)
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q84 We would like to know if you have ever used any of the listed behaviours below towards any current or former partner or partners. Have you ever…
| Yes (1) | No (0) | |
|---|---|---|
| Blamed a partner for causing you to act abusively (1) | ||
| Shook, threw, pushed, or grabbed a partner (4) | ||
| Tried to convince a partner’s family or friends that they were crazy (5) | ||
| Used or threatened to use a knife or gun or other weapon against a partner (6) | ||
| Made a partner perform sex acts that were unwanted (7) |
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q85 We would like to know if you have ever used any of the listed behaviours below towards any current or former partner or partners. Have you ever…
| Yes (1) | No (0) | |
|---|---|---|
| Followed a partner or hung around outside their home or work (9) | ||
| Threatened to harm or kill a partner or someone close to them (18) | ||
| Choked a partner (10) | ||
| Forced or tried to force a partner to have sex (11) | ||
| Constantly called, texted, emailed, or contacted a partner using social media (12) |
Display This Question:
If Have you been in an adult intimate relationship in the past 12 months? = No
Q86 We would like to know if you have ever used any of the listed behaviours below towards any current or former partner or partners. Have you ever…
| Yes (1) | No (0) | |
|---|---|---|
| Told a partner they were crazy, stupid or not good enough (13) | ||
| Hit a partner with a fist or object, kicked or bitten a partner (14) | ||
| Kept a partner from seeing family or friends (15) | ||
| Locked a partner in a room or other space (16) | ||
| Kept a partner from working or having access to resources (17) |
Q87
Thank you for all your answers so far. You are at the half-way point of the survey. Please remember that your answers will contribute to helping us make services better for everyone in the community. If at any time you would like to take a break you may do so and return to the place you are up to (as long as you use the same device). If you would like to speak to anyone about anything distressing that has arisen for you so far please click here.
End of Block: CAS_SF_Relationships
Start of Block: UNMC_Relationships
Q88 Your relationships continued
This section is about unwanted sexual experiences. These experiences may have occurred inside or outside of an intimate relationship. In this particular survey, we are interested in hearing from people who have instigated unwanted sex. Remember that the survey is anonymous. If you do not feel comfortable answering any of the questions, skip them and go on to the next question. In this questionnaire, when we talk about “sex” we mean any kind of sex (vaginal, anal, oral etc.)
Q89 Since the age of 15, have you ever forced or tried to force someone into sexual activity?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q90 Have you ever physically forced a partner to have sex? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q91 Have you ever threatened or made a current or former partner afraid in some other way in order to get them to have sex with you? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q92 Have you ever forced a current or former partner to watch pornography with you? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q93 Have you forced a current or former partner to do something else sexual with you? Did this happen once, a few times, or many times?
- Never (0)
- Once (1)
- A few times (2)
- Many times (3)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q94 Have you ever pressured, forced or threatened a partner to become pregnant?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By ‘adult intimate re… = Yes
Q95 Have you ever pressured, forced, or threatened a partner to prevent them from terminating a pregnancy?
- Yes (1)
- No (0)
Display This Question:
If These questions are about your experiences in adult intimate relationships. By “adult intimate relationship…” = Yes
Q96
Have you ever interfered with contraception in order to get a partner pregnant (e.g. disposed of contraception, tampered with contraception, prevented a partner from obtaining contraception)?
- Yes (1)
- No (0)
Q97
This is the end of this section. Thank you for taking the time to answer these questions, some of which may have been distressing. This is the end of the sensitive questions about experiences you have had in your relationships. Below is a breathing exercise that may reconnect you with where you are in this moment, here and now. If you would like to speak to someone for support, click here for a list of support services.
When you feel ready, press the next button to continue taking the survey. We really appreciate your time.
Q98
End of Block: UNMC_Relationships
Start of Block: Contemplation_Ladder
Q99 Changing your behaviour and relationships
Now we would like to ask you about how you feel about making changes to your behaviour and relationships. Below are a number of statements about behaviour and relationship change. We are interested to know how you see change in your own life. Right now, you may not see a need for change, you may be thinking about change, or you may have already taken steps to make changes to your behaviour or relationship.
Q100 Please select the one statement about changing your behaviour that best reflects how you feel today.
- I don’t need to change my behaviour, but my partner does. (1)
- I haven’t thought about changing the way I act or my behaviour towards my partner. (2)
- I think both my partner and I need to change the way we act and behave. (3)
- I need to change my behaviour, but am unsure if I can. (4)
- I need to change my behaviour, but I am not ready. (5)
- I am starting to make changes to my behaviour to improve my relationships. (6)
- I have made changes to my behaviour, but I am worried about things slipping back. (7)
Q101 Please select the one statement about changing your relationship that best reflects how you feel today.
- I don’t think about making my relationship healthier. (1)
- Sometimes I think that my relationship could be healthier. (2)
- I would love to make my relationship healthier, but don’t know if I am ready. (3)
- I would love to make my relationship healthier, but I am not sure how. (4)
- I have made changes in my relationship to make it healthier, but I worry it won’t last. (5)
- I have made changes in my relationship to make it healthier, and I am confident it will stay this way. (6)
End of Block: Contemplation_Ladder
Start of Block: Help-seeking
Q102 Your views on services This section asks you about your use of services in the community. This information will help us understand how people use services, what might be missing from services, and ways that existing services can be improved. In particular, we are interested to know whether you have ever sought advice or support for any of the relationship issues explored in the previous sections.
Q103 Have you ever spoken to any of the following services about your behaviour/s in your relationship/s? Please tick all that apply.
- I did not seek advice or support. (531)
- Friend/s (508)
- Family member/s (509)
- Partner (510)
- General practitioner (511)
- Nurse (512)
- Psychologist or counsellor (513)
- Social worker (hospital/community health) (514)
- Alcohol or drug worker (515)
- Family therapist (516)
- Telephone helpline (e.g. Lifeline, 1800 RESPECT) (517)
- Domestic or family violence service (519)
- Police (520)
- Legal service (e.g. solicitor or legal aid) (521)
- Men’s behaviour change program (522)
- Men’s referral service (523)
- Mensline (532)
- Financial service (e.g. Centrelink) (524)
- Housing service (525)
- Work colleague or boss (526)
- Priest/minister/rabbi or any other religious person (527)
- Other (please specify) (518) ________________________________________________
End of Block: Help-seeking
Start of Block: How helpful
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Friend/s
Q104 How helpful was your friend/s?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Family member/s
Q105 How helpful was your family member?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = General practitioner
Q106 How helpful was the general practitioner?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Nurse
Q107 How helpful was the nurse?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Psychologist or Counsellor
Q108 How helpful was the psychologist or counsellor?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Social worker (Hospital/community health)
Q109 How helpful was the social worker (hospital or community based)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Alcohol or drug worker
Q110 How helpful was the alcohol or drug worker?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Family therapist
Q111 How helpful was the family therapist?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Other (please specify)
Q112 How helpful was the telephone helpline (e.g. Lifeline, 1800RESPECT)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Domestic or family violence service
Q113 How helpful was the domestic or family violence service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Police
Q114 How helpful was the police?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Legal service (e.g. solicitor or legal aid)
Q115 How helpful was the legal service (e.g. solicitor or legal aid)?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Financial service (e.g. Centrelink)
Q116 How helpful was the financial service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Housing service
Q117 How helpful was the housing service?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Work colleague or boss
Q118 How helpful was your work colleague or boss?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Priest/Minister/Rabbi or any other religious person
Q119 How helpful was the priest/minister/rabbi or any other religious person?
- Not at all helpful (1)
- Somewhat unhelpful (2)
- Neither helpful nor unhelpful (3)
- Somewhat helpful (4)
- Very helpful (5)
Display This Question:
If Have you ever spoken to Rany of the following services about your behaviour/s in your relationship… = Partner
Q120 How helpful was your partner?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever sRpoken to any of the following services about your behaviour/s in your relationship… = Men’s behaviour change program
Q121 Was the men’s behaviour change program court-ordered or voluntary?
- Court-ordered (1)
- Voluntary (2)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = Men’s behaviour change program
Q122 How helpful was men’s behaviour change program?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
Display This Question:
If Have you ever spoken to any of the following services about your behaviour/s in your relationship… = men’s referral service
Q123 How helpful was men’s referral service?
- Not at all helpful (6)
- Somewhat unhelpful (7)
- Neither helpful nor unhelpful (8)
- Somewhat helpful (9)
- Very helpful (10)
End of Block: How helpful
Start of Block: Help_seeking_did_not_seek_advice
Q124 Below is a list of reasons why you may have not spoken to a professional or service about your behaviours. Please rate how important each is to your own situation. Please select one option per line.
| Not at all important (1) | A little bit important (2) | Somewhat important (3) | Moderately important (4) | Very important (5) | |
|---|---|---|---|---|---|
| I don’t feel deserving of help. (13) | |||||
| I feel too ashamed to talk to anyone. (14) | |||||
| The professional will not understand me. (15) | |||||
| The professional will tell others. (16) | |||||
| My friends or family will find out. (17) | |||||
| My behaviours are just a normal part of relationships. I don’t believe there is any need to see a professional about them. (18) | |||||
| My behaviour was a once-off. It won’t happen again. (19) | |||||
| I have no access to transport to see someone. (20) | |||||
| I have no time to talk to someone about these things. (21) | |||||
| All the services that are available are too expensive. (22) | |||||
| I don’t know of any service that might be able to help. (23) | |||||
| I don’t want to talk to anyone about my behaviours, it is too personal. (24) |
Q125 Was there a time when you needed help for your behaviour in relationships but could not get it?
- Yes (1)
- No (0)
Display This Question:
If Was there a time when you needed help for your behaviour in relationships but could not get it? = Yes
Q126 How important were each of the service barriers in preventing you from accessing services? Please select one option per line.
| Not at all (1) | Slightly (2) | Moderately (3) | Very (4) | Extremely (5) | |
|---|---|---|---|---|---|
| Language or translation problems (36) | |||||
| Cost (37) | |||||
| Limited opening hours (38) | |||||
| No service available in the area at the time needed (39) | |||||
| Waiting time too long (40) | |||||
| No appointments (41) | |||||
| Not taking new patients (42) | |||||
| Lack of awareness of available services (43) | |||||
| Concerns regarding confidentiality (44) | |||||
| No private health insurance (45) | |||||
| Other barriers: ___________ (46) |
End of Block: Help_seeking_did_not_seek_advice
Start of Block: Help_seeking_How_important
Q127 Reflecting on any contact or experiences you’ve had with services, what would you say you value most in a service? Please rate how important you think each of the following factors are.
| Not at all important (1) | A little important (2) | Moderately important (3) | Very important (4) | Extremely important (5) | |
|---|---|---|---|---|---|
| Not feeling judged or put down (11) | |||||
| Knowing that whatever I said would be held in confidence by the professional (12) | |||||
| The professional being interested in who I was as a person (13) | |||||
| Feeling listened to by the professional (14) | |||||
| Being given practical information about how to increase safety (15) | |||||
| The expertise of the professional (16) | |||||
| Learning new ways of dealing with relationship problems (17) | |||||
| Material support (e.g. getting access to accommodation) (18) | |||||
| Emotional support (having someone to talk to) (19) | |||||
| Other (please specify) (20) |
Q128 Considering all the experiences you have had in talking to professionals (including GPs, counsellors, nurses etc) about these behaviours, what do you believe that professionals need to do differently to better help people in similar situations as you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q129 The COVID-19 pandemic has changed the way we all access support services. What impact, if any, has it had on your access to support services for your behaviours in intimate relationships?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: Help_seeking_How_important
Start of Block: Help_seeking_continued
Q130 If you thought you were close to using abusive behaviour/s in your relationship/s, how likely is it that you would seek help from the following people or services?
| Very unlikely (1) | Unlikely (2) | Neither likely nor unlikely (3) | Likely (4) | Very likely (5) | |
|---|---|---|---|---|---|
| Friend/s (35) | |||||
| Family member/s (36) | |||||
| Partner (37) | |||||
| General practitioner (38) | |||||
| Nurse (39) | |||||
| Psychologist or counsellor (40) | |||||
| Social worker (hospital/community health) (41) | |||||
| Alcohol or drug worker (42) | |||||
| Family therapist (43) | |||||
| Telephone helpline(e.g. Lifeline, 1800 RESPECT) (44) | |||||
| Domestic or family violence service (45) | |||||
| Police (46) | |||||
| Legal service (e.g. solicitor or legal aid) (47) | |||||
| Men’s behaviour change program (48) | |||||
| Men’s referral service (49) | |||||
| Financial service (e.g. Centrelink) (50) | |||||
| Housing service (51) | |||||
| Work colleague or boss (52) | |||||
| Priest/minister/rabbi or any other religious person (53) | |||||
| Other (please specify) (54) |
Q131 If you think about your behaviours towards your partner/ex-partner you told us about in previous sections, what do you think your greatest need is from a service or professional?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q132 If you think about your behaviours towards your partner/ex-partner, what do you think you need the most to stop using violence and abuse?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have any children? = Yes
Q133 If you think about your behaviours towards your partner/ex-partner and children, how do you think your children have been affected?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Display This Question:
If Do you have any children? = Yes
Q134 If you think about your behaviours towards your partner/ex-partner, what do you think services can do to best address your children’s needs?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q135 If you think about your behaviours towards your partner/ex-partner, what do you think your partner’s/ex-partner’s greatest need is from a service or professional?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q136 How have your experiences in your adult intimate relationships changed during COVID-19 isolation?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q137 I wish…
These next questions ask you to think about your relationship with your partner or ex-partner. Please complete the following sentences with the first words that come to mind. There are no right or wrong answers, just write what you feel.
I wish that my partner/ex-partner…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q138 I wish that service providers…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q139 I wish that my family…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q140 I wish that my friends…
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q141
This is the end of this section. When you feel ready, please click the next button to continue with some further background questions.
End of Block: Help_seeking_continued
Start of Block: More_about_you
Q142 More about you This section asks more about your background and some personal details about education and finances. These questions are important because they allow your answers to be placed in a broader context, without identifying anybody. Please remember that all survey responses are anonymous.
Q143 Which of these most closely describes your sexual orientation?
- I am heterosexual (0)
- I am bisexual (1)
- I am lesbian (2)
- I prefer to self-describe (3) ________________________________________________
- I am asexual (4)
- Not sure (6)
- I am queer (7)
Q144 Which of the following best describes your prior schooling?
- Still at secondary school (1)
- Completed secondary school to end of Year 12 (2)
- Attended secondary school but did not complete Year 12 (3)
- Attended primary school only (4)
- Did not attend school (5)
Q145 What is your highest qualification since leaving school?
- Finished a degree or higher degree (1)
- Completed a diploma or certificate (2)
- Completed a trade apprenticeship or traineeship (3)
- Other (please specify (4) ________________________________________________
Q146 Which of the following best describes your occupational status?
- Part-time wage or salary earner (including self-employed) (1)
- Full-time wage or salary earner (including self-employed) (2)
- Unemployed, seeking work (3)
- Unemployed, not seeking work (4)
- Retired (5)
- Unpaid work (e.g. home duties, voluntary, carer) (6)
Q147 Do you hold a current Health Care Card?
- Yes (1)
- No (0)
Q148 How do you manage on your available income?
- Easily (1)
- Not too badly (2)
- Difficult some of the time (3)
- Difficult all of the time (4)
- Impossible (5)
Q149 You are close to the end. Only a few more questions and you will be finished. When you feel ready, please click the next button to continue.
End of Block: More_about_you
Start of Block: How_you_felt_completing_this_survey
Q150 Your views on the survey
This last section asks questions how you felt while completing this survey to understand what it was like being involved in the VOICES project. Please select one box on each line.
Q151 I felt comfortable answering questions about domestic violence and sexual violence in this survey.
- Strongly agree (1)
- Agree (2)
- Neither agree nor disagree (3)
- Disagree (4)
- Strongly disagree (5)
Q152 As a result of questions about domestic violence and sexual violence being asked in this survey, my feelings about my relationship are…
- More positive (1)
- Somewhat more positive (2)
- Unchanged (3)
- Somewhat more negative (4)
- More negative (5)
Q153 The questions I was asked in this survey made me feel that the problems in my relationship with my partner or ex-partner are my fault.
- Strongly disagree (1)
- Disagree (2)
- Neither disagree nor agree (3)
- Agree (4)
- Strongly agree (5)
Q154 As a result of being asked questions about domestic violence and sexual violence in this survey, my feelings about myself as a person are…
- Better (1)
- Somewhat better (2)
- About the same as before (3)
- Somewhat worse (4)
- Worse (5)
Q155 Responding to this survey has made me more open to dealing with possible problems in my relationship.
- Strongly disagree (1)
- Disagree (2)
- Neither agree nor disagree (3)
- Agree (4)
- Strongly agree (5)
Q156 I am glad to be a participant in the VOICES project.
- Strongly disagree (1)
- Disagree (2)
- Neither disagree nor agree (3)
- Agree (4)
- Strongly agree (5)
Q157 Please use the space below if there is anything else you would like to tell us about yourself or the survey
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q158 Final thoughts: In your own words, what have you gained from participating in the VOICES project?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
Q159 Do you have any extra comments that you wish to make about any issues raised in the survey?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: How_you_felt_completing_this_survey
Start of Block: Thank You
Q160
Make sure you click submit!
This is the end of the survey. Thank you very much for the time and effort you have taken. When you click the submit button, your responses will be submitted confidentially.
On the next page you can provide your contact details if you like to enter into a draw to win an iPad, as an appreciation of your time and effort. You can also tell us if you would like to participate in a follow up interview about your experiences and need for services.
Thank you.
End of Block: Thank You
Start of Block: Gift Voucher
Q263 Thank you for completing this survey and taking the time to assist us today. Your participation will contribute to our understanding of how best to help and keep families safe. We would like to offer you the option to enter a draw to win an iPad in appreciation for your time and contribution. If you would like to enter the draw, please provide us with your name and best email address. Your name and email address will not be used for any other purposes.
Q265 Email address
________________________________________________________________
Q264 Name
________________________________________________________________
Q266 Together, with your help, we are trying to work out ways to improve the support and services women receive in relation to issues of domestic violence and sexual assault.
To achieve this goal, further research (e.g. interviews) on this topic may be required. Please tick yes if you would be happy to be contacted by the researchers for involvement in further research.
Your participation in further research is completely voluntary, and independent of the survey you have just completed. You can provide your details now but if you change your mind later, you are free to withdraw your interest without explanation when/if you are contacted for further research at some time in the future.
Q267 Would you like to participate in further research on this topic?
- Yes (1)
- No (2)
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q268 My first name is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q269 The best phone number(s) to safely contact me on is:
________________________________________________________________
Display This Question:
If Would you like to participate in further research on this topic? = Yes
Q270 An alternative contact (e.g. email) is:
________________________________________________________________
End of Block: Gift Voucher
Appendix D:
Interview schedule
(Victims and survivors)
Questions
1. Can you tell me about when you first realised what you were experiencing in your relationship /(what you experienced from a sexual partner) was not OK?
2. Can you take me through your experiences of seeking help or support since having issues in your relationship/an unwanted sexual encounter?
Interviewer will use probes to explore:
- • What help or support participant was hoping for
- • What prompted them to talk to others or seek support
- • What seeking help was like for them
- • If there any help or support that they wanted or needed but did not receive.
3. How could a professional or service make it easier to seek help or support?
Appendix E:
Interview schedule
(People who use IPV and/or SV)
Questions:
Can you tell me when you first realised there was an issue with your behaviour in your intimate relationship(s)?
Interviewer probes
What were some “lightbulb” moments?
Who was involved in supporting you to realise something was wrong?
What happened when you realised something was wrong?
Can you take me through your experiences of speaking to people about your behaviour in your intimate relationships?
Interviewer probes
What help or support were you hoping for?
What kinds of professionals did you speak to?
Was there any help or support that you wanted or needed but didn’t receive?